 Irene López-Ferreruela1,2*
Irene López-Ferreruela1,2* Antonio Gimeno-Miguel3,4
Antonio Gimeno-Miguel3,4 Clara Laguna-Berna3,4
Clara Laguna-Berna3,4 Sara Malo2,4,5
Sara Malo2,4,5 Sara Castel-Feced2,6María José Rabanaque2,4,5
Sara Castel-Feced2,6María José Rabanaque2,4,5 Isabel Aguilar-Palacio2,4,5
Isabel Aguilar-Palacio2,4,5
- 1Torreramona Health Centre, Primary Care, Servicio Aragonés de Salud (SALUD), Zaragoza, Spain
- 2Grupo de Investigación en Servicios Sanitarios de Aragón (GRISSA), Fundación Instituto de Investigación Sanitaria de Aragón (IIS Aragón), Zaragoza, Spain
- 3EpiChron Research Group, Aragon Health Sciences Institute (IACS), IIS Aragón, Miguel Servet University Hospital, Zaragoza, Spain
- 4Research Network on Chronicity, Primary Care and Health Promotion (RICAPPS), Carlos III Health Institute (ISCIII), Madrid, Spain
- 5Department of Preventive Medicine and Public Health, University of Zaragoza, Zaragoza, Spain
- 6Department of Statistical Methods, University of Zaragoza, Zaragoza, Spain
Introduction: Secondary prevention after an acute myocardial infarction (AMI) has the objective of improving quality of life, minimizing recurrence, and reducing morbidity and mortality. Despite European guidelines highlighting the importance of cardiovascular risk factor (CVRF) management and optimal healthcare utilization, inequalities persist, particularly between genders. This study aims to identify and analyze gender inequalities in healthcare utilization and CVRF monitoring during the first year after AMI using real-world data (RWD).
Methods: An analytical study was conducted within the CARhES (CArdiovascular Risk factors for Health Services research) cohort in Aragon, Spain. The study population included 3,464 subjects who survived a first AMI and were followed for one full year after the event. Sociodemographic, anthropometric, clinical data, healthcare utilization, CVRF monitoring and pharmacological prescriptions, were extracted from the Aragon Health Service. Statistical analyses included chi-squared tests, Student's t-tests, and logistic regression, with Blinder-Oaxaca decomposition applied to explore possible explanatory factors for gender differences.
Results: Women represented 28.3% of the study population. Compared with men, they were older and had a higher morbidity burden. Primary care utilization was similar between genders; however, women had fewer cardiology visits (p < 0.001) and were less likely to achieve risk factor monitoring goals. Differences were also observed in pharmacological treatment, with women being less likely to receive beta-blockers, lipid modifying agents, and antiplatelet agents (p < 0.001). Several of these inequalities persisted after controlling for age. The Oaxaca decomposition showed that age and morbidity burden were the main contributors to gender disparities. In addition, socioeconomic status and place of residence played a role in health services utilization differences.
Conclusions: Gender inequalities are still present in post-AMI care and CVRF management, with women being more likely to receive less adequate treatment and management. Addressing these inequalities is crucial to ensuring equitable care and improving health outcomes for women.
1 Introduction
The primary objective of secondary prevention following an acute myocardial infarction (AMI) is to enhance patient's quality of life and to minimize recurrence, reduce morbidity and mortality rates (1–3). In order to obtain these outcomes, European guidelines emphasise the importance of following healthy lifestyle recommendations, effective management and monitoring of cardiovascular risk factors (CVRF), such as blood pressure, cholesterol, and glucose levels, and the appropriate use of recommended drugs, such as platelet aggregation inhibitors, beta-blockers, lipid modifying agents, renin–angiotensin–aldosterone system inhibitors and other comedications (4–6). Patients must be followed up properly, particularly during the first year after an AMI, in order to ensure the optimal utilization of healthcare services and the establishment of a positive, collaborative, and trusting therapeutic relationship that supports patient adherence, recovery, and commitment to their health (7).
Despite significant efforts to highlight the importance of CVRF management, a concerning number of patients fail to achieve the recommended targets (8).
In this context, recent evidence has suggested the existence of gender inequalities, defined as systematic, avoidable, and unjust differences in health status and healthcare access based on gender (9). Gender norms, roles, and power imbalances have been demonstrated to shape vulnerabilities to illness, influence health behaviours and care-seeking, and affect access to health services, treatment responses, and health outcomes (9).
As supported by research in cardiovascular disease, women are less likely than men to receive adequate risk factors assessment during secondary prevention and show poorer monitoring and achievement of key risk factors targets (such as glycated haemoglobin and lipoprotein cholesterol). They are also less likely to achieve guideline recommendations, including sufficient levels of physical activity, or being more frequently obese (1,8).
Moreover, gender inequalities have been documented even before healthcare contact. Qualitative studies have shown that women are more likely to misinterpret or minimize their symptoms, delay seeking medical attention, and experience greater uncertainty during the decision-making process, often attributing symptoms to non-cardiac causes and contributing to worse outcomes. Conversely, men have been shown to recognize the urgency of their symptoms and seek care earlier than women (10–12). These inequalities highlight gaps not only in preventive care, but throughout the entire care pathway.
Despite increasing awareness, research in this area remains limited. Additionally, the growing availability of real-world data (RWD), defined as routinely collected health information from sources such as electronic health records, administrative databases, or patient registries, presents a unique opportunity to enhance clinical research (13). When appropriately analysed, RWD can generate real-world evidence (RWE), providing valuable insights into healthcare utilization, treatment patterns, and outcomes in everyday clinical settings. This enables performing large-scale population secondary studies that can offer valuable evidence on gender inequalities in healthcare. Therefore, the objective of this study is to compare, describe and analyse, using RWD, the level of health services utilization and the monitoring of CVRFs between men and women during the first year after an AMI, in order to identify potential gender inequalities and explore their underlying causes.
2 Materials and methods
2.1 Study design
An analytical study based on observational population data was conducted within the CARhES (CArdiovascular Risk factors for hEalth Services research) cohort. This is an open, dynamic, population-based cohort of subjects aged 16 and older diagnosed with hypertension, diabetes mellitus, and/or dyslipidaemia in the Spanish region of Aragon (14).
2.2 Study population
For the purposes of this study, we included patients from the CARhES cohort who experienced a first recorded episode of AMI between 2017 and 2022 identified using the International Classification of Diseases (ICD-10) code I21. We excluded subjects with a prior diagnosis of AMI at the onset of cohort follow-up, as well as those who died during the index event. In order to analyse health services utilization and CVRF monitoring, we only included subjects with complete clinical and administrative data available for the 365 days following the AMI event. A detailed flowchart illustrating selection criteria of the study population is provided in Figure 1.
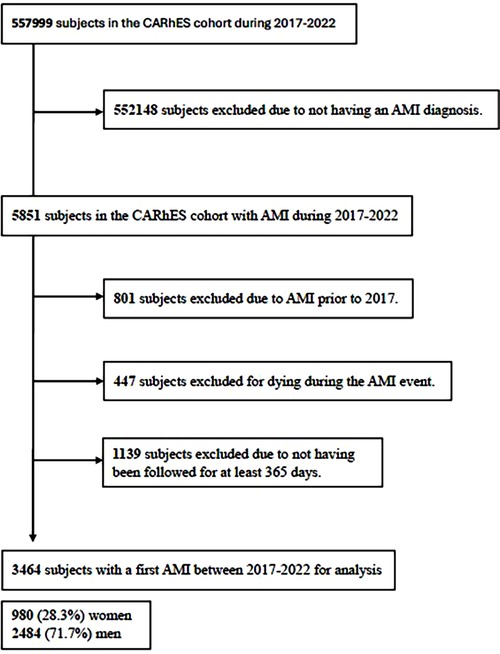
Figure 1. Study flowchart of subjects’ inclusion and exclusion for the study. CARhES, CArdiovascular Risk factors for hEalth Services research. AMI, acute myocardial infarction.
2.3 Data sources
The data used in this study were obtained from the CARhES cohort (14), a population-based, dynamic open cohort designed to analyse the impact of healthcare service use and pharmacological treatment on health outcomes in patients with CVRFs. The CARhES cohort is constructed using RWD, that is, routinely collected health information from clinical practice, including all individuals aged ≥16 years registered in the Aragón public health system (Spain) with a diagnosis of hypertension, diabetes mellitus, and/or dyslipidaemia since 2017. The cohort is subject to annual updates through data extractions.
This study constitutes a secondary analysis of anonymized RWD extracted from the BIGAN platform, which integrates multiple information systems of the Aragón Health Service (SALUD) for research and policy purposes. The integrated sources include the following: the user database (BDU) and adjusted morbidity groups (GMA) for demographic and clinical data; hospital discharge records (CMBD); specialist care data (CEX); primary care records (OMI-AP); emergency care data (PCH); and electronic pharmacy dispensing records (Receta Electrónica) for medication use. Collectively, these sources provide comprehensive information on patients' clinical profiles, socioeconomic conditions, and healthcare utilization. No additional instruments or patient-reported outcome measures were used; all data were obtained from routinely recorded clinical and administrative sources within the public health system.
2.4 Variables
In this study, the variables were grouped into two main categories: general patient characteristics at the time of the event (such as socio-demographic, anthropometric and clinical characteristics) and patient management variables, which included health service utilization, CVRF monitoring, and pharmacological treatment during the first year following AMI. The sex/gender variable was also included, as a key factor for analysing potential gender-based differences in care and outcomes.
2.4.1 General patient characteristics
2.4.1.1 Sociodemographic variables
Sociodemographic and anthropometric data were recorded at the time of the event. This included age, gender, nationality (classified as Spanish or immigrant), area of residence (urban or rural, according to the basic healthcare area in which the subject resided), institutionalisation in a nursing home, and socioeconomic status. Socioeconomic status was defined according to the income category of the subject. This included pensioners with income below 18,000€ per year and free pharmacy, pensioners with income above 18,000€ per year, unemployed, subjects with active employment with income below 18,000€ per year, active with income above 18,000€ per year, and other status (including mutual, special conditions or uninsured subjects).
2.4.1.2 Anthropometric variables
Weight (kg) and height (cm) were recorded to calculate the body mass index (BMI), defined as weight in kilograms divided by the height in metres squared, and then categorized in accordance with the World Health Organization (WHO) classification (15). A BMI lower than 18.5 kg/m2 was defined as underweight, while a normal range was established between 18.5 kg/m2 and 24.9 kg/m2. A BMI between 25 kg/m2 and 29.9 kg/m2 was defined as overweight, and a BMI of 30 kg/m2 or above was defined as obese.
2.4.1.3 Clinical characteristics
In terms of clinical information, we obtained several variables from the Morbidity adjusted groups (GMA). This is an information source that includes all medical diagnoses available in primary care, emergencies and hospital discharge records (Minimum Basic Data Set of Hospital Discharges) (16). It provides a description of the main comorbidities of each subject, a numeral quantification of their chronic pathologies, the subject's complexity, which is defined by the analysis of several resource utilization variables, such as mortality, risk of hospitalization, primary care visits, or prescriptions, linked to diagnoses, and their morbidity burden, obtained from the aggregation of the patient's different diagnoses.
Additionally, CVRF that were required for inclusion in the CARhES cohort (hypertension, diabetes mellitus and dyslipidemia) were registered.
2.4.2 Patient management variables
2.4.2.1 Health services utilization
In order to measure health services utilization among our population, the number of visits recorded in the database was quantified. From this basis, it was calculated the proportion of subjects who had visited at least once the primary care services, including general practitioner and nurse and specialist healthcare. In specialist healthcare, we specifically evaluated visits to cardiologist, endocrinologist, vascular surgeon, nephrologist and ophthalmologist, hospital admission and the emergency room use in the year following AMI.
2.4.2.2 CVRF monitoring
CVRF monitoring was assessed by monitoring the proportion of subjects who had at least one measurement for each of the following measures: blood pressure, capillary blood glucose, glycosylated haemoglobin (HbA1c), cholesterol values in blood tests, waist circumference, electrocardiogram (ECG), influenza vaccination and diabetic foot risk measured, as well as their self-report on adequate nutrition, physical activity and adherence to treatment.
2.4.2.3 Pharmacological treatment
Pharmacological treatment was selected in accordance with the recommendations set out in the European guidelines (4–6),identified by anatomical therapeutic chemical (ATC)-code, version 2024 (17), and defined based on prescriptions registered during the study year. This data does not reflect actual dispensation or therapy initiation. Pharmacological burden was included, defined as the number of different pharmacological subgroups that the individual was prescribed and dispensed during the study year. So, we included antihypertensive drugs (ATC-code C02), diuretics (C03), beta-blockers (C07) (all beta-blocking agents and combinations), calcium channel blockers (CCBs) (C08), angiotensin-converting enzyme inhibitors (ACE-I)/angiotensin receptor blocker (ARB) (C09), lipid modifying agents (C10), antiplatelets agents (B01AC), vitamin K antagonist (B01AA), direct thrombin inhibitors (B01AE) and direct factor Xa inhibitors (B01AF). The proportion of subjects who received at least one prescription for the selected drugs in the year following AMI was calculated.
2.4.3 Sex and gender
In our study, the variable measured was biological sex, as recorded in the health information systems. However, for analytical and interpretative purposes, the term gender is used, acknowledging that it encompasses a broader set of socio-cultural norms, roles, and behaviours that influence health outcomes. Furthermore, gender intersects with other axes of inequality, including socioeconomic status, place of residence, and access to care.
Although it is not always possible to disentangle the effects of sex and gender, the use of the term gender inequality reflects the intention to consider the structural and behavioural dimensions beyond biology. The assessment of gender inequality was conducted through a comparative analysis of frequency data and a subsequent calculation of adjusted rates. This approach was undertaken under the assumption that men and women should have equal access to healthcare services and similar levels of CVRFs monitoring. Any statistically significant deviation from this expected equality was interpreted as an indication of gender inequality.
2.5 Statistical analyses
Sociodemographic and baseline clinical characteristics of the subjects studied were described using counts and proportions for categorical variables and means with standard deviation (SD) for continuous variables. Bivariate analyses between men and women were performed using Pearson's Chi-squared test, and we compared means between groups using Student's T-test. Bivariate logistic regression analyses were conducted to investigate gender-based differences in patient management variables that had been previously defined. The threshold for statistical significance was set at P < 0.05. When statistically significant gender-based differences were identified, the Blinder-Oaxaca decomposition method was applied (18). A twofold decomposition was conducted using the Oaxaca R library and reference regression coefficients, which were calculated from a pooled regression model (19). Variables such as age, socioeconomic status, area of residence (urban or rural), and morbidity burden were examined to determine their contribution to the observed differences. This analytical approach enables the quantification of the extent to which observed gender differences can be attributed to measurable variables, and how much remains unexplained. Specifically, it decomposes the mean outcome differences between two groups into an explained fraction—linked to differences in observed characteristics—and an unexplained fraction, which may reflect the differential effects of those variables, unmeasured confounders, behavioural or structural inequalities, or potential discrimination (20). This method provides a nuanced understanding of the mechanisms underlying gender disparities in healthcare. All statistical analyses were performed using R 4.3.3. (R Core Team, 2022) a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/) (21) and JAMOVI (version 2.4) [Computer Software) Retrieved from https://www.jamovi.org (22).
2.6 Ethical aspects
This study is based on data from the CARhES cohort, whose protocol was approved by the Clinical Research Ethics Committee of Aragon (CEICA PI21/148). The research was conducted in accordance with local legislation and institutional requirements. As the study involved the retrospective analysis of anonymized, population-based data with no direct contact or interaction with participants, the requirement for written informed consent was waived by the Ethics Committee.
3 Results
3.1 General characteristics of the study population
The study population included a total of 3,464 subjects who had experienced a first AMI during 2017–2022, with a minimum follow-up of one year. Of these, 980 (28.30%) were women, and 2,482 (71.70%) were men.
As presented in Table 1, women were significantly older at the time of the event (75.26 years) compared to men (67.23 years). The majority of the population were pensioners <18,000€, with significant differences (p < 0.001) observed between men (41.79%) and women (67.45%). 2,471 subjects (71.33%) lived in urban areas. A greater proportion of women (10.92%) were institutionalized in nursing homes compared to men (4.31%).
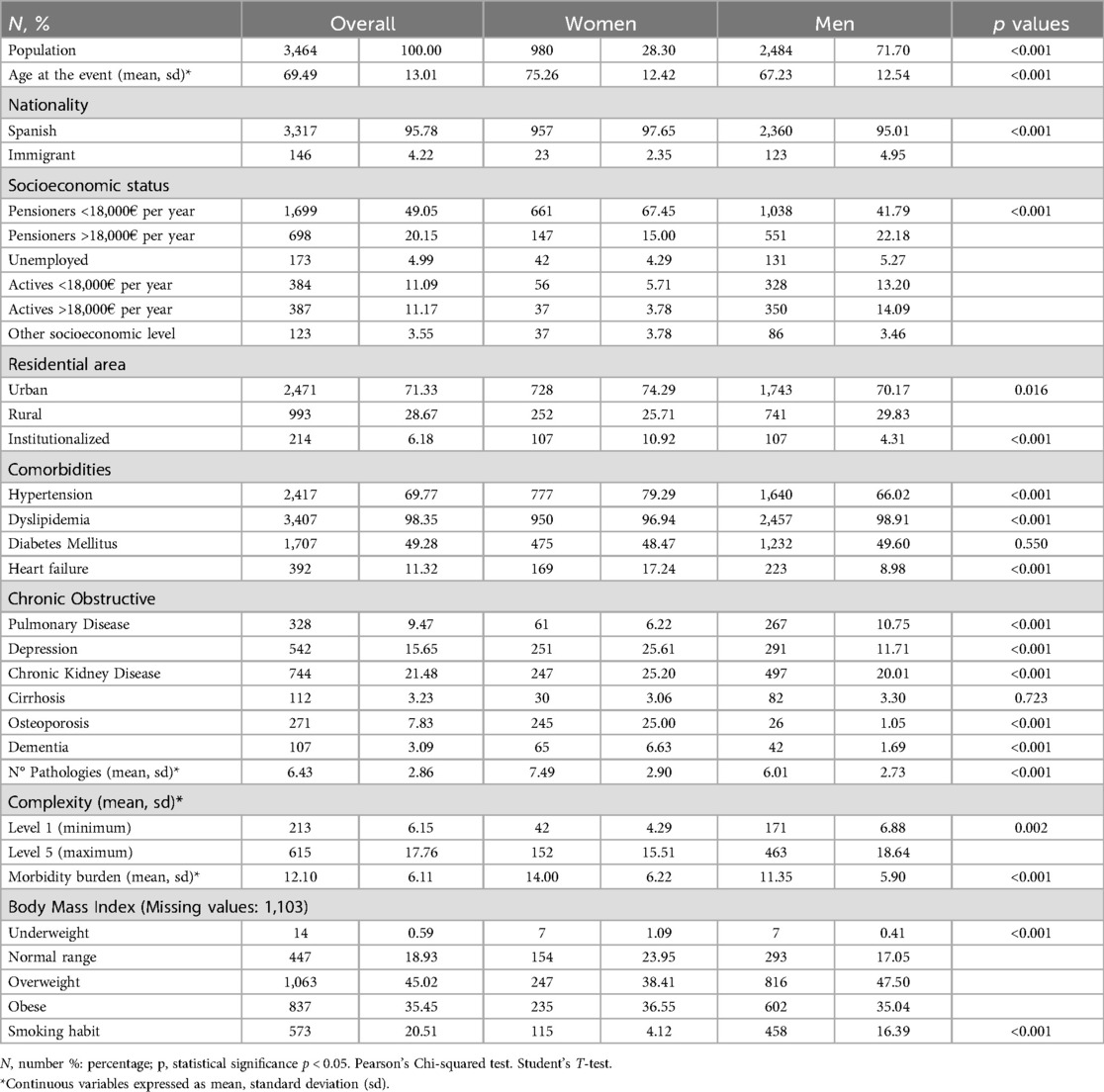
Table 1. General patient characteristics (socio-demographic, clinical and anthropometric). Results overall and stratified by gender.
While dyslipidemia was the most prevalent CVRF overall, with a slightly higher prevalence among men, hypertension was significantly more common in women. Among the comorbidities analyzed, all conditions (except cirrhosis and chronic obstructive pulmonary disease) were more prevalent in women (p < 0.001). Women exhibited a significantly higher number of pathologies, more affected systems, and a greater overall morbidity burden compared to men (p < 0.001). Conversely, men had higher rates of overweight and obesity and had a higher prevalence of smoking (p < 0.001) (Table 1).
3.2 Health services utilization
Nearly all participants (99.86%) had at least one primary care visit within the first year after AMI (Table 2). Women were more likely to visit nurse practitioners (93.67% vs. 91.77%) and specialists such as endocrinologists and ophthalmologists (p < 0.001),while men had significantly more visits to cardiologists (p < 0.001). Hospital admissions by all the causes were significantly higher in women (35.10% vs. 30.76%), while emergency room use was similar between genders (Table 2).
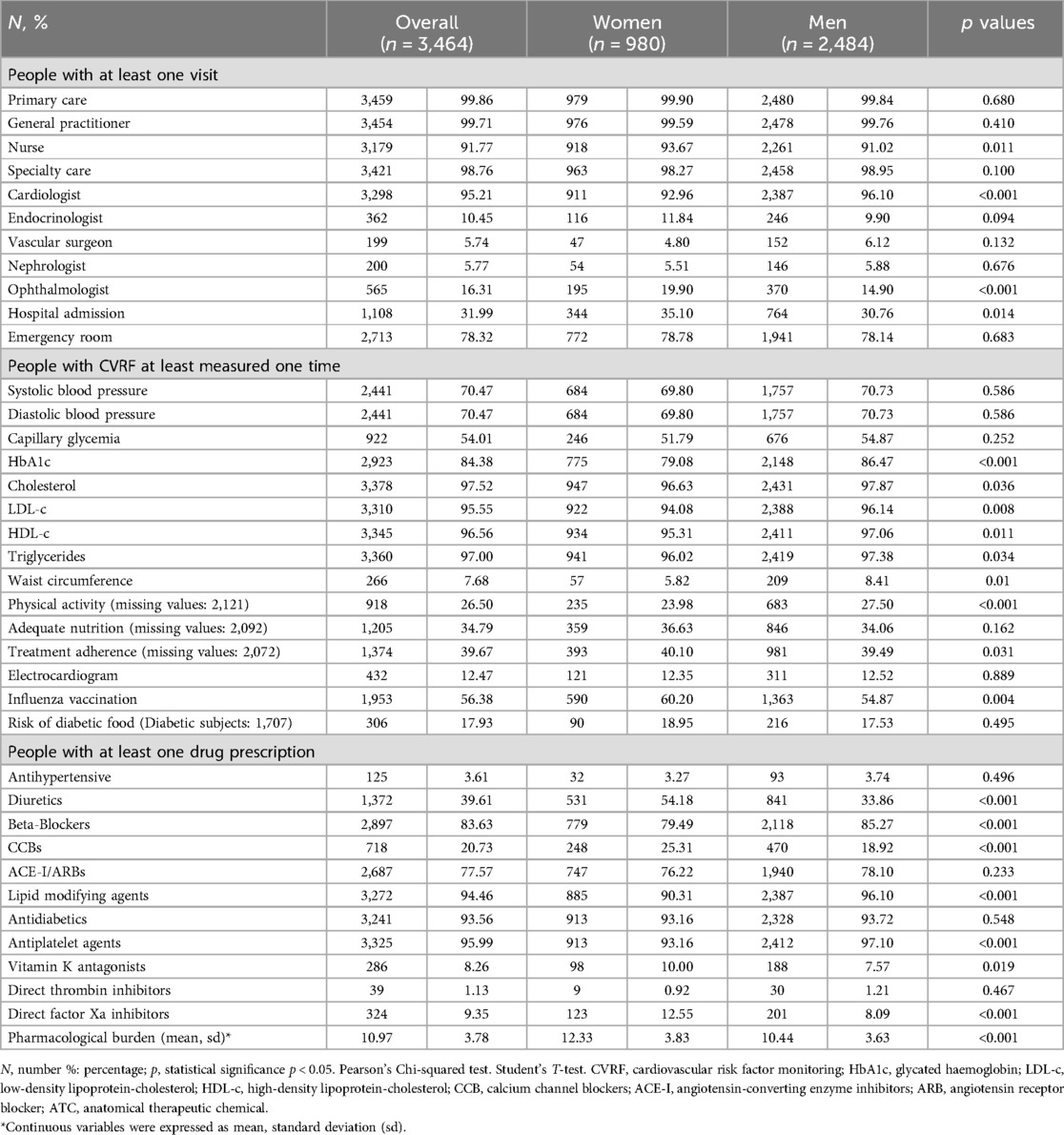
Table 2. Patient management: health services utilization, risk factors monitoring and pharmacological treatment.
3.3 CVRF monitoring
Men had higher rates of monitoring for several CVRFs (Table 2), including glycated hemoglobin (HbA1c), low-density lipoprotein cholesterol (LDL-c), and high-density lipoprotein cholesterol (HDL-c). Total cholesterol, triglycerides and waist circumference were also monitored more frequently among men, with smaller differences. Engagement with physical activity was reported more frequently by men (p < 0.001), while women were more likely to receive influenza vaccinations (p = 0.004). No significant differences were found in nutritional habits or treatment adherence (Table 2).
3.4 Pharmacological treatment
Men were more likely to receive the main guideline-recommended drugs, including beta-blockers, lipid modifying agents, and antiplatelet agents (p < 0.001) (Table 2). However, women were more frequently prescribed some concomitant medications, such as diuretics, CCBs, vitamin K antagonists, and direct Factor Xa inhibitors (p < 0.001), and showed a higher overall pharmacological burden (p < 0.001).
3.5 Multivariate analyses
Logistic regression analyses, shown in Table 3, revealed significant gender differences. After age adjustment, logistic regression indicated that most gender differences in health services were no longer statistically significant, with the exception of endocrinologist visits, which remained higher for women (adjusted Odds Ratio: 1.41, 95% Confidence Interval: 1.10–1.80). Significant gender differences remained in CVRFs monitoring: women were less likely to achieve optimal blood pressure levels, HbA1c levels, and waist circumference measurements. They also had lower odds of reporting regular physical activity (adjusted OR: 0.67, 95% CI: 0.52–0.87). Differences in lipid profiles and influenza vaccination were narrowed after adjustment for age. After adjusting for age, women continued to have lower odds of receiving beta-blockers, lipid modifying agents, and antiplatelet agents. In contrast, they were significantly more likely to be prescribed diuretics.
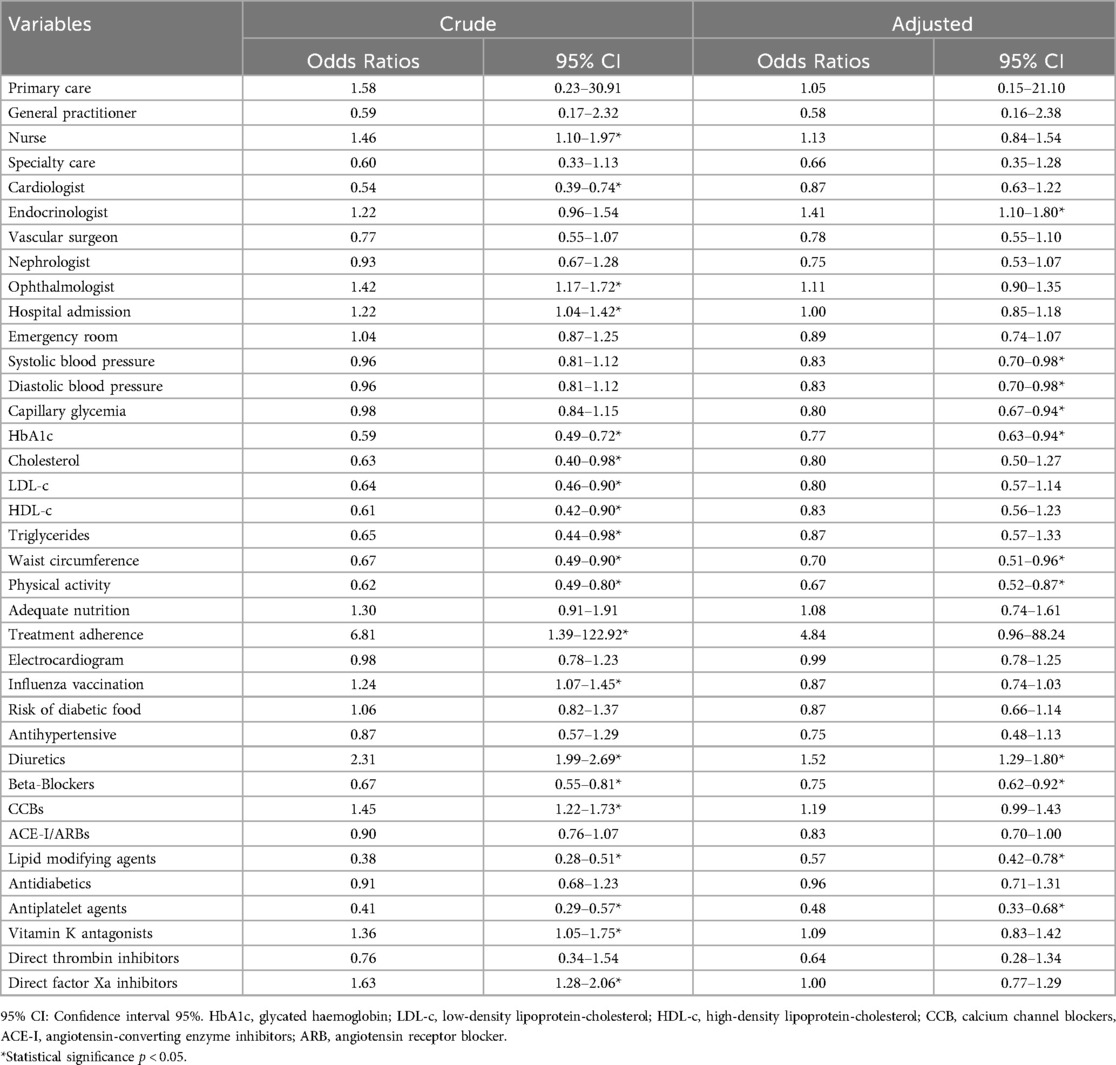
Table 3. Crude and age-adjusted odds ratios for health services utilization, risk factors monitoring control and pharmacological treatment in women compared with men.
3.6 Oaxaca–Blinder decomposition analysis
The Oaxaca-Blinder decomposition analyses assessed the contribution of observed variables to gender inequalities. So, variables with negative values reduced the observed inequalities, while those with positive values increased them (Figuress 2, 3). Complete data from the OAXACA decomposition analyses, such as the explained fraction of the models and the contribution of each variable, can be found in the Supplementary Tables S1 and S2.
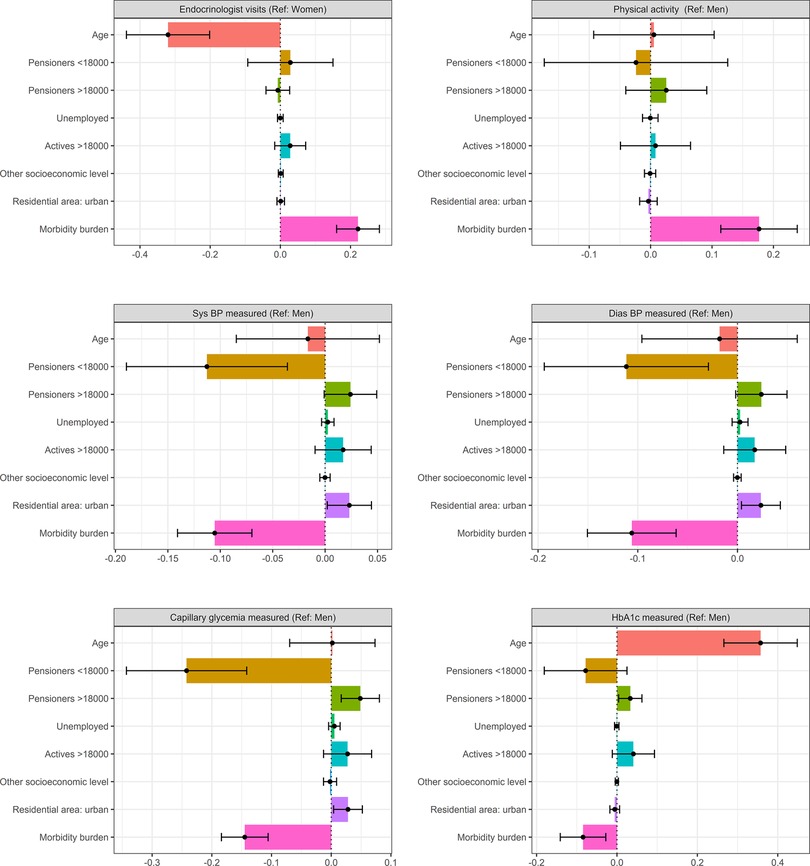
Figure 2. Decomposition of gender inequalities in healthcare utilization and CVRF monitoring. Oaxaca decomposition analyses. CVRF, cardiovascular risk factor; Ref, reference (gender taken as reference category); Sys BP, systolic blood pressure; Dias BP, diastolic blood pressure; HbA1c, glycated haemoglobin; categories of reference: actives <18,000, rural residence.
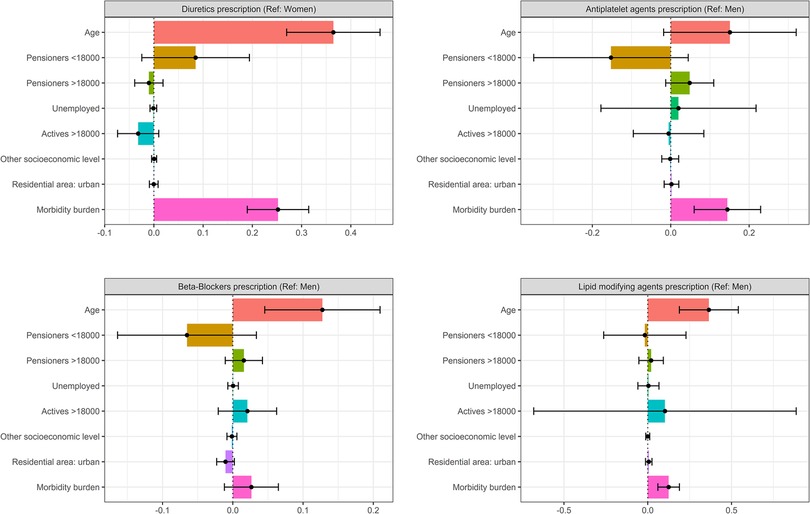
Figure 3. Decomposition of gender inequalities in treatment prescribing patterns. Oaxaca decomposition analyses. CVRF, cardiovascular risk factor; Ref, reference (gender taken as reference category); Sys BP, systolic blood pressure; Dias BP, diastolic blood pressure; HbA1c, glycated haemoglobin; categories of reference: actives <18000, rural residence.
Regarding healthcare utilization, the OAXACA analysis revealed that only 19.74% of the observed gender inequalities in endocrinology visits were explained by the variables included in the model, with age and morbidity burden being the main contributing factors. The lower age of men mitigated these inequalities, while the lower morbidity burden of men with respect to women increased the existing differences.
Concerning physical activity, which was more reported in men, the lower morbidity burden of men was the main explanatory factor of these gender differences, along with their higher socioeconomic status. However, being a low-income pensioner, seemed to mitigate these differences, while age did not seem to influence gender differences.
In terms of CVRF monitoring, the explained fraction varied from 63.15% for HbA1c to 38.78% for physical activity. The explanatory variables in the model exhibited different effects on each of the CVRF studied. With regard to blood pressure, which was less monitored in women, the factors that contributed most to increasing gender inequalities were urban residence and high socioeconomic status, considering actives <18,000€ as reference. In contrast, the older age of women, being a low-income pensioner, and their higher morbidity burden in this study reduced these differences. A similar explanatory pattern was observed for capillary glycemia measurement, except that age did not appear to be associated with variations in gender differences observed. For HbA1c measurement, the factors more associated with increased gender inequalities were age, as the main contributing factor, and high socioeconomic status. In contrast, being a low-income pensioner and morbidity burden appeared to reduce these inequalities.
Regarding drug prescription, the explained fraction of observed gender differences varied across the pharmacological groups analyzed. The explanatory fraction of the model was high in diuretics and lipid modifying agents (more than 50%) while the explanatory factor of beta-blockers and antiplatelet agents was low, suggesting the influence of additional factors not considered in the model. As shown in Figuress 2, 3, age and morbidity burden were the main factors contributing to gender inequalities in the prescribing of guideline-recommended drugs. Regarding age, the older age of women was related with increasing gender differences in the prescription of antiplatelets, beta-blockers and lipid modifying agents. On the contrary, the younger age of men seemed to increase prescription differences in diuretics. Regarding socioeconomic status, none of the categories analysed showed a statistically significant effect on drug prescription, but it was possible to observe some associations. In the case of antiplatelets and beta-blockers, the high frequency of women that were pensioners with low income reduced the inequalities observed. In the case of diuretics, with a higher prescription in women, the lower frequency of men with low income increased the differences. Finally, the morbidity burden increased the observed differences in all the drugs considered. The lower morbidity burden of men increased the differences observed in men and women in the prescription of diuretics. On the other hand, the higher morbidity burden of women increased the differences in the prescription of antiplatelets, beta-blockers and lipid-modifying agents.
4 Discussion
4.1 Sociodemographic and clinical profile differences
In our population following a first AMI, men and women had different socioeconomic and clinical characteristics. Women were older, more frequently institutionalized, and had higher morbidity burden and lower socioeconomic status. These factors are essential in order to comprehend the observed inequalities in healthcare utilization, CVRF monitoring, and treatment.
4.2 Healthcare service utilization
Nearly all patients had at least one primary care visit within the first year after AMI, as expected, since primary care is the principal setting for health care follow-up (23). However, women visited primary care nurses more frequently than men, as described in the literature (24–26) and may be due to differences in health-seeking behaviors or greater awareness of prevention (24). In this sense, a study by Vallejo-Torres et al. found that nurse utilization was associated with older age, female gender, the presence of more chronic conditions, and lower socioeconomic status (26) which is in line with our results.
In terms of specialist care, women were more likely to visit endocrinologists but had lower overall rates of visits to other specialists, particularly cardiologists, as the evidence shows (24,27). Our prior scoping review (28) suggested that this lower referral rate to cardiology may be related to an androgenic bias in cardiovascular care and under-recognition of the disease in women by both patients and healthcare providers (27,28), as well as, lower awareness of CVD, less social support, or lower socioeconomic status (29).
After adjusting for age, only endocrinologists' visits remained significant. Oaxaca decomposition attributed this to women's higher morbidity burden, which increased the observed differences.
This could be partly explained by the higher prevalence of endocrine disorders in women, particularly postmenopausal and elderly, such as thyroid disease, osteoporosis, or hormonal imbalances (30–32), which. often coexist with other comorbidities that increase cardiovascular risk and complicate disease management (33–36). In contrast, men's younger age helped reduce the differences observed. However, the association between age and referral patterns in older women is complex, and may be influenced by unmeasured factors such as race or marital status (37).
Hospital admissions were more frequent among women, however, became not significant after adjusting for age. These findings are consistent with previous studies (38,39), suggesting that while unadjusted data may show higher admission rates among women, factors such as age and other social determinants play a significant role in the observed differences.
4.3 CVRF monitoring
Gender inequalities in CVRF monitoring were pronounced. Men had a higher frequency of recorded risk factor monitoring, including blood pressure, glycemic control (HbA1c), and cholesterol levels (8, 40–42). These findings align with existing literature suggesting a potential gender bias in management, with women receiving less frequent CVRF monitoring and more conservative treatments, despite being older and having a higher morbidity burden (43). Urban residence increased gender inequalities in CVRF management, which could be explained by differences in access to health care. Rural areas often have shorter waiting lists and greater availability of primary care services (44–47). The relationship between socioeconomic status and gender inequalities in health outcomes is somewhat controversial. We observed a reduction in gender inequalities in blood pressure, capillary glycemia, and HbA1C control associated with lower socioeconomic status in women. This could be related to the fact that women with lower socioeconomic status in our population were older and had a higher burden of disease, leading them to visit primary care more frequently. As a result, their CVRFs were monitored more regularly, narrowing the gap between men and women. Some authors support this explanation (48,49). Conversely, other studies suggest that lower socioeconomic status may limit women's CVRFs monitoring, thereby increasing gender inequalities (50,51). Also, other studies have associated higher socioeconomic status with better CVRF monitoring and greater access to health care, highlighting the complexity of this relationship (29,52,53).
For HbA1c measurement, age has an important role in increasing existing inequalities, which has been related with the older age of women (54–57). In terms of lifestyle practices, women reported greater adherence to healthy lifestyle recommendations, such as proper diet and immunizations. This is consistent with existing literature (58–63). For physical activity, consistent with what has been reported in the literature (60,61,64,65), women in our study were less likely to report practicing physical activity than men. Oaxaca analysis identified that morbidity burden and high socioeconomic status increased gender inequalities in physical activity practice, whereas lower income reduced inequalities. As has been widely described, gender, age and socioeconomic status are known to be important determinants of physical activity (66). While higher income has been associated with greater physical activity (67), in low-income settings, men and women have shown to face similar barriers to physical activity, reducing gender inequalities (68). In addition, chronic health conditions negatively impact physical activity levels, with women experiencing greater reductions, further widening inequalities (69).
4.4 Pharmacological treatment
Women were less likely to be prescribed guideline-recommended medications and were more likely to receive adjunctive therapies, as diuretics. These results are consistent with the literature (8,28,41,42,70,71). The Oaxaca analysis showed that older age and higher morbidity burden were the main factors contributing to this gender inequalities. This is in line with some studies that have found strong associations between age, morbidity burden and greater risk of exacerbations, leading to under-prescription of the pharmacological groups studied, increasing gender inequalities (24,48,72–74). Similarly, the large international PRAISE registry (75) reported lower prescription rates of guideline-recommended therapies in women following acute coronary syndromes. However, it also found that female gender was not associated with an increased risk of adverse outcomes, including bleeding, highlighting the need for more intensive, evidence-based treatment strategies in women based on their clinical profile rather than gender alone. The analysis of socioeconomic status reveals complex interactions with gender disparities in the prescribing patterns of guideline-recommended medications, as explored in our previous research (70). While higher socioeconomic status is generally associated with reduced gender disparities (29,52,76), our study found that lower income subjects, particularly older women with a higher morbidity burden, experienced a narrowing of these disparities in the prescription of antiplatelets and beta-blockers, although this association was not statistically significant. This suggests that women in our population may receive more clinical attention, leading to more equitable prescribing patterns of guideline-recommended therapies (48,50,77).
Regarding diuretic prescription, our findings align with existing research associating lower socioeconomic status with higher diuretic prescription rates among women, which could be associated with the management of multiple comorbidities (78). Studies indicate that women with low socioeconomic status are more susceptible to polypharmacy, with diuretics frequently prescribed as part of a prescribing cascade (79). Additionally, diuretic use tends to increase with the overall number of medications prescribed, which corresponds to the greater morbidity burden observed in our study population (80).
4.5 Strengths and limitations
One of the major strengths of this study is the use of the CARhES cohort, a population cohort of RWD from the Aragon Health Service. This increases the internal validity of the study by ensuring a representative study population at the regional level.
In addition, a key strength of our study is the use of the Oaxaca-Blinder decomposition method to examine gender inequalities. This analytical approach allows us to separate observed gender differences into two components: an explained fraction, attributable to measurable variables, and an unexplained fraction, which may reflect differential effects of these characteristics, structural or behavioural inequalities, or potential discrimination (20). When we apply this method from a gender perspective, our analysis provides a more nuanced and comprehensive understanding of the mechanisms underlying inequalities in the use of services and management of CVD.
Nonetheless, certain limitations need to be acknowledged. A limitation of using registered diagnoses is the potential for diagnostic bias in CVD, as it excludes undiagnosed subjects. As highlighted in the literature (43,72), this issue could be particularly relevant for women because of potential underdiagnosis related to the nonrecognition of their symptoms in previous clinical guidelines. Another potential limitation of the study is the exclusion of patients who died during the index event, which may introduce survival bias. While the mortality rates were comparable between sexes, women represented a slightly higher proportion of the deceased and were, on average, older. No significant sex differences were observed in terms of morbidity burden or number of chronic conditions. However, the exclusion of these cases may have led to an underrepresentation of more severe female cases. Furthermore, the established follow-up period of one year may have further contributed to survival bias, as it excludes patients with shorter survival, potentially affecting older and more vulnerable subjects, particularly women. This decision was made to ensure a consistent observation period for all participants, thus minimising variability in follow-up duration and enabling reliable analysis of post-AMI care. Another limitation is the lack of information regarding the actual reason for the patient's visit. As a result, we cannot confirm whether consultations were directly related to the AMI episode. Finally, data on key lifestyle parameters, such as adequate diet, physical activity, smoking, or adherence to treatment, are underreported in electronic health records, as we have shown in our results. Nevertheless, we have chosen to present this information to highlight both their potential impact and the significant gaps in information registration.
5 Conclusions
Our study showed the existence of gender inequalities in post-AMI care, particularly in CVRFs monitoring and pharmacological treatment., Women visited more frequently primary care nurses and endocrinologists, while men visited more cardiologists. CVRFs were less frequently monitored in women, although they had better adherence to preventive and lifestyle behaviors. In addition, the main guidelines recommended drugs were prescribed to women less frequently. These inequalities were mainly explained by age, morbidity burden and socioeconomic status. Specifically, older age and higher comorbidity burden among women resulted in lower prescription of recommended drugs. Conversely, older age, lower income, and higher morbidity burden appeared to reduce differences in CVRF monitoring. However, a significant part of the observed differences remained unexplained, suggesting the presence of underlying systemic or structural biases in care delivery.
5.1 Research implications
It is important to assess whether factors such as age or comorbidities justify the reduced care observed or, on the contrary, reflect bias in clinical decisions.
Raising awareness of gender differences is essential to ensure equitable care. For example, better recording of CVRFs and lifestyle habits in health records is key to improving personalized care. Clinical practice guidelines must incorporate a gender-sensitive approach to ensure equitable and personalized care, as current recommendations do not fully address the differentiated healthcare needs of women, contributing to treatment inequities. Beyond clinical practice, these findings point to wider systemic challenges, including potential barriers that women face in accessing cardiovascular care as explored in our previous scoping review (28) and by Giordano et al. (11). Several social and cultural factors—like unrecognized symptoms, caregiving duties, fear of being a burden, low income, limited education, and reduced autonomy—can delay or prevent women with AMI from getting timely care. The establishment of follow-up protocols or structured monitoring programs, especially in primary care, can reduce the gender gap and improve health outcomes.
Finally, gender analysis is complex and closely linked to other social factors, making it hard to explain all the causes of disparities. This highlights the need for more research using an intersectional approach.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving human participants were approved by the Ethics Committee for Clinical Research in Aragon (CEICA PI21/148). All procedures were conducted in accordance with applicable local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement for written informed consent from participants or their legal guardians/next of kin because the study used retrospective, anonymized data from the CARhES cohort. The research involved no direct contact or interaction with individuals. The study protocol was reviewed and approved by the Ethics Committee for Clinical Research in Aragon (CEICA PI21/148), and complied with all relevant ethical and legal standards.
Author contributions
IL-F: Writing – review & editing, Formal analysis, Methodology, Data curation, Writing – original draft, Investigation, Conceptualization. AG-M: Conceptualization, Methodology, Writing – review & editing, Supervision. CL-B: Conceptualization, Writing – review & editing, Formal analysis, Methodology, Data curation. SM: Conceptualization, Supervision, Writing – review & editing, Funding acquisition, Methodology. SC-F: Data curation, Formal analysis, Writing – review & editing, Methodology. MR: Supervision, Funding acquisition, Writing – review & editing. IA-P: Funding acquisition, Methodology, Writing – review & editing, Supervision, Writing – original draft, Conceptualization.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study has been funded by Health Institute Carlos III (ISCIII) through the research grants FIS PI22/01193 and co-financed by the European Union through the European Regional Development Fund (ERDF) “A way of making Europe”. It was also funded by B09_23R Grupo de Investigación en Servicios Sanitarios de Aragón (GRISSA) from “Convocatoria de subvenciones destinadas a fomentar la actividad investigadora de los grupos de investigación reconocidos por la Administración de la Comunidad de Aragón” (Aragón Government). GRISSA is part of the Department of Employment, Science and Universities of the Government of Aragón (Spain).
Acknowledgments
We acknowledge the use of Chat GPT 4, a generative AI technology, for language checks in this manuscript.
Conflict of interest
The authors declare that this research was conducted independently, with no interests that could be perceived as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. We acknowledge the use of Chat GPT 4, a generative AI technology, for language checks in this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgwh.2025.1605400/full#supplementary-material
Abbreviations
AMI, acute myocardial infarction; CVRFs, cardiovascular risk factors; CVD, cardiovascular disease; RWD, real-world data; CARhES, CArdiovascular Risk factors for hEalth Services research; ICD, international Classification of Diseases; BMI, body mass index; WHO, World Health Organization; HbA1C, haemoglobin A1c; ATC, anatomical therapeutic chemical; CCBs, calcium channel blockers; ACE-I, angiotensin-converting enzyme inhibitors; ARBs, or angiotensin receptor blockers; SD, standard deviation; N, number; %, percentage; p, statistical significance p < 0.05; LDL-C, (low-density lipoprotein-cholesterol; HDL-C, high-density lipoprotein-cholesterol; OR, odds ratio; CI, confidence Interval; Sys BP, systolic blood pressure; Dias BP, diastolic blood pressure.
References
1. Hyun K, Negrone A, Redfern J, Atkins E, Chow C, Kilian J, et al. Gender difference in secondary prevention of cardiovascular disease and outcomes following the survival of acute coronary syndrome. Hear Lung Circ. (2021) 30(1):121–7. doi: 10.1016/j.hlc.2020.06.026
2. Perel P, Avezum A, Huffman M, Pais P, Rodgers A, Vedanthan R, et al. Reducing premature cardiovascular morbidity and mortality in people with atherosclerotic vascular disease the world heart federation roadmap for secondary prevention of cardiovascular disease. Glob Heart. (2015) 10(2):99–110. doi: 10.1016/j.gheart.2015.04.003
3. Ergatoudes C, Thunström E, Rosengren A, Björck L, Bengtsson Boström K, Falk K, et al. Long-term secondary prevention of acute myocardial infarction (SEPAT)—guidelines adherence and outcome. BMC Cardiovasc Disord. (2016) 16(1):1–8. doi: 10.1186/s12872-016-0400-6
4. Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, et al. 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J [Internet]. (2020) 41(3):407–77. doi: 10.1093/eurheartj/ehz425
5. Byrne RA, Rossello X, Coughlan JJ, Barbato E, Berry C, Chieffo A, et al. 2023 ESC guidelines for the management of acute coronary syndromes. Eur Heart J. (2023) 44(38):3720–826. doi: 10.1093/eurheartj/ehad191
6. Alfonso F, Sionis A, Bueno H, Ibáñez B, Sabaté M, Cequier Á, et al. Comentarios a la guía ESC 2017 sobre el tratamiento del infarto agudo de miocardio en pacientes con elevación del segmento ST. Rev Española Cardiol. (2017) 70(12):1039–45. doi: 10.1016/j.recesp.2017.10.049
7. Lizcano-Álvarez Á, Carretero-Julián L, Talavera-Saez A, Cristóbal-Zárate B, Cid-Expósito M, Alameda-Cuesta A. Intensive nurse-led follow-up in primary care to improve self-management and compliance behaviour after myocardial infarction. Nurs Open. (2023) 10(8):5211–24. doi: 10.1002/nop2.1758
8. Vynckier P, Ferrannini G, Ryden L, Jankowski P, De Backer T, Gevaert S, et al. Gender gap in risk factor control of coronary patients far from closing: results from the European Society of Cardiology EUROASPIRE V registry. Eur J Prev Cardiol. (2022) 29(2):344–51. doi: 10.1093/eurjpc/zwaa144
9. World Health Organization. Gender and health. Available online at: https://www.who.int/health-topics/gender (Accessed May 25, 2025).
10. Isaksson RM, Brulin C, Eliasson M, Näslund U, Zingmark K. Prehospital experiences of older men with a first myocardial infarction: a qualitative analysis within the northern Sweden MONICA study. Scand J Caring Sci. (2011) 25(4):787–97. doi: 10.1111/j.1471-6712.2011.00896.x
11. Giordano V, Mercuri C, Simeone S, Rea T, Virgolesi M, Nocerino R, et al. Behavioral delays in seeking care among post-acute myocardial infarction women: a qualitative study following percutaneous coronary intervention. Front Glob Women’s Heal. (2025) 6(February):1–18. doi: 10.3389/fgwh.2025.1501237
12. Isaksson RM, Brulin C, Eliasson M, Näslund U, Zingmark K. Older women’s prehospital experiences of their first myocardial infarction. J Cardiovasc Nurs. (2013) 28(4):360–9. doi: 10.1097/JCN.0b013e31824bcebc
13. US Food and Drug Administration. Real-World Evidence (2022). Available at: https://www.fda.gov/science-research/science-and research-specialtopics/real-world-evidence (Accessed March 7, 2024).
14. Aguilar-Palacio I, Rabanaque M, Castel S, Maldonado L, González-García J, Compés L, et al. Cohort profile: the CArdiovascular risk factors for hEalth services research (CARhES) cohort study. Int J Epidemiol. (2024) 53(2):dyae015. doi: 10.1093/ije/dyae015
15. WHO. Obesity: Preventing and Managing the Global Epidemic. Report of a wHO Consultation. wHO Technical Report Series 894. Geneva: World Health Organization (2000).
16. Ministerio de Sanidad consumo y bienestar Social. Informe del proyecto de Estratificación de la Población por Grupos de Morbilidad Ajustados (GMA) en Sist Nac Salud (2018). 33–9.
17. WHO Collaborating Centre for Drug Statistics Methodology. ATC classification index with DDDs. Oslo, Norway (2024).
18. Oaxaca RL. Male-female wage differentials in urban labour markets. Int Econ Rev. (1973) 14(3):693–709. doi: 10.2307/2525981
19. Hlavac M. oaxaca: Blinder-Oaxaca Decomposition in R. R package version 0.1.5 (2022). Available online at: https://CRAN.R-project.org/package=oaxaca https://cran.rproject. org/web/packages/oaxaca/vignettes/oaxaca.pdf (Accessed February 01, 2025).
20. Rahimi E, Hashemi Nazari SS. A detailed explanation and graphical representation of the Blinder-Oaxaca decomposition method with its application in health inequalities. Emerg Themes Epidemiol. (2021) 18:12. doi: 10.1186/s12982-021-00100-9
21. R Core Team. R: A Language and environment for statistical computing. (Version 4.1) [Computer software] (2022). Available online at: https://cran.r-project.org (R packages accessed from CRAN snapshot 2023-04-07).
22. The jamovi project. jamovi. (Version 2.4) [Computer Software] (2023). Available online at: https://www.jamovi.org (Accessed February 01, 2025).
23. Talha KM, Hammonds K, Alhamdow A, Bennett MM, Bomar JVA, Ettlinger JA, et al. Healthcare resource utilization following acute myocardial infarction findings from RECORD-MI registry. Am J Cardiol. (2024) 232:1–7. doi: 10.1016/j.amjcard.2024.08.034
24. Gutiérrez AG, Poblador-Plou B, Prados-Torres A, Laiglesia FJR, Gimeno-Miguel A. Sex differences in comorbidity, therapy, and health services’ use of heart failure in Spain: evidence from real-world data. Int J Environ Res Public Health. (2020) 17:2136. doi: 10.3390/ijerph17062136
25. Montayre J, Liu MF, Calma KRB, Zhao IY, Ho MH. Nurse visit utilization and blood pressure control: a multi-cohort study in New Zealand. Public Health Nurs. (2022) 39(6):1181–7. doi: 10.1111/phn.13095
26. Vallejo-Torres L, Morris S. Factors associated with the use of primary care services: the role of practice nurses. Eur J Heal Econ. (2011) 12(4):373–81. doi: 10.1007/s10198-010-0251-5
27. Nanna MG, Wang TY, Xiang Q, Goldberg AC, Robinson JG, Roger VL, et al. Sex differences in the use of statins in community practice: patient and provider assessment of lipid management registry. Circ Cardiovasc Qual Outcomes. (2019) 12(8):1–10. doi: 10.1161/CIRCOUTCOMES.118.005562
28. López Ferreruela I, Obón Azuara B, Malo Fumanal S, Rabanaque Hernández MJ, Aguilar-Palacio I. Gender inequalities in secondary prevention of cardiovascular disease: a scoping review. Int J Equity Health. (2024) 23:146. doi: 10.1186/s12939-024-02230-3
29. Venditti V, Bleve E, Morano S, Filardi T. Gender-Related factors in medication adherence for metabolic and cardiovascular health. Metabolites. (2023) 13(1087):1–26. doi: 10.3390/metabo13101087
30. Thomas CC, Zeytinoglu M. Primary care endocrinology in the adult woman. Obstet Gynecol Clin North Am. (2016) 43(2):325–46. doi: 10.1016/j.ogc.2016.01.005
31. Bensenor IM, Olmos RD, Lotufo PA. Hypothyroidism in the elderly: diagnosis and management. Clin Interv Aging. (2012) 7:97–111. doi: 10.2147/CIA.S23966
32. Liu Y, Shan Z, Cheng M, Cao CX, Cao XP, Chen P, et al. Expert consensus on diagnosis and treatment for elderly with thyroid diseases in China (2021). Aging Med. (2021) 4(2):70–92. doi: 10.1002/agm2.12165
33. Ifthikhar MB, Dhamotharaswamy K. Correlation of hypothyroidism with age and comorbidities among women: a cross-sectional study. J Pharmacol Pharmacother. (2024) 15(3):336–42. doi: 10.1177/0976500X241266077
34. Kim J, Prasitlumkum N, Randhawa S, Banerjee D. Association between subclinical hypothyroidism and incident hypertension in women: a systematic review and meta-analysis. J Clin Med. (2021) 10(15):21–3. doi: 10.3390/jcm10153318
35. Zhu Y, Xu F, Shen J, Liu Y, Bi C, Liu J, et al. Prevalence of thyroid dysfunction in older Chinese patients with type 2 diabetes—a multicenter cross-sectional observational study across China. PLoS One. (2019) 14(5):1–14. doi: 10.1371/journal.pone.0216151
36. Meng Z, Liu M, Zhang Q, Liu L, Song K, Tan J, et al. Gender and age impacts on the association between thyroid function and metabolic syndrome in Chinese. Med (United States). (2015) 94(50):1–9. doi: 10.1097/MD.0000000000002193
37. El Ayadi H, Desai A, Jones RE, Mercado E, Williams M, Rooks B, et al. Referral rates vary widely between family medicine practices. J Am Board Fam Med. (2021) 34(6):1183–8. doi: 10.3122/jabfm.2021.06.210213
38. Lam L, Ahn HJ, Okajima K, Schoenman K, Seto TB, Shohet RV, et al. Gender differences in the rate of 30-day readmissions after percutaneous coronary intervention for acute coronary syndrome. Women’s Heal Issues. (2019) 29(1):17–22. doi: 10.1016/j.whi.2018.09.002
39. Haddadin F, Beydoun H, Sabharwal B, Rzechorzek W, Khandaker M, Munoz Estrella A, et al. Differences in social hardships in women and men with acute myocardial infarction: impact on 30-day readmission. Women’s Heal Reports. (2022) 3(1):437–42. doi: 10.1089/whr.2021.0150
40. Naicker K, Liddy C, Singh J, Taljaard M, Hogg W. Quality of cardiovascular disease care in Ontario’s primary care practices: a cross sectional study examining differences in guideline adherence by patient sex. BMC Fam Pract. (2014) 15:123. doi: 10.1186/1471-2296-15-123
41. Rachamin Y, Grischott T, Rosemann T, Meyer MR. Inferior control of low-density lipoprotein cholesterol in women is the primary sex difference in modifiable cardiovascular risk: a large-scale, cross-sectional study in primary care. Atherosclerosis. (2021) 324:141–7. doi: 10.1016/j.atherosclerosis.2021.02.024
42. Zhao M, Woodward M, Vaartjes I, Millett ERC, Klipstein-Grobusch K, Hyun K, et al. Sex differences in cardiovascular medication prescription in primary care: a systematic review and meta-analysis. J Am Heart Assoc. (2020) 9(11):e014742. doi: 10.1161/JAHA.119.014742
43. Möller-Leimkühler AM. Gender differences in cardiovascular disease and comorbid depression. Dialogues Clin Neurosci. (2007) 9(1):71–83. doi: 10.31887/DCNS.2007.9.1/ammoeller
44. McIntyre D, Chow CK. Waiting time as an indicator for health services under strain: a narrative review. Inquiry. (2020) 57:46958020910305. doi: 10.1177/0046958020910305
45. Sanz Tolosana E, Oliva Serrano J, Sanz Tolosana E, Oliva Serrano J. La percepción local del acceso a los servicios de salud en las áreas rurales. El caso del pirineo navarro. An Sist Sanit Navar. (2021) 44(2):185–94. doi: 10.23938/assn.0945
46. Portero de la Cruz S, Cebrino J. Rural-urban differences in common mental disorders, functional limitation and social support among adults with cancer: a population-based study in Spain. J Clin Med. (2022) 11(10):2742. doi: 10.3390/jcm11102742
47. Chen X, Orom H, Hay JL, Waters EA, Schofield E, Li Y, et al. Differences in rural and urban health information access and use. J Rural Health. (2019) 35(3):405–17. doi: 10.1111/jrh.12335
48. Jenkins KR, Ofstedal MB. The association between socioeconomic status and cardiovascular risk factors among middle-aged and older men and women. Women Health. (2014) 54(1):15–34. doi: 10.1080/03630242.2013.858098
49. Bijlsma-Rutte A, Rutters F, Elders PJM, Bot SDM, Nijpels G. Socio-economic status and HbA1c in type 2 diabetes: a systematic review and meta-analysis. Diabetes Metab Res Rev. (2018) 34(6):e3008. doi: 10.1002/dmrr.3008
50. Lindley KJ, Aggarwal NR, Briller JE, Davis MB, Douglass P, Epps KC, et al. Socioeconomic determinants of health and cardiovascular outcomes in women: JACC review topic of the week. J Am Coll Cardiol. (2021) 78(19):1919–29. doi: 10.1016/j.jacc.2021.09.011
51. Wang Y, Tian A, Wu C, Lu J, Chen B, Yang Y, et al. Influence of socioeconomic gender inequality on sex disparities in prevention and outcome of cardiovascular disease: data from a nationwide population cohort in China. J Am Heart Assoc. (2023) 12(20):e030203. doi: 10.1161/JAHA.123.030203
52. Tetzlaff J, Geyer S, Westhoff-Bleck M, Sperlich S, Epping J, Tetzlaff F. Social inequalities in mild and severe myocardial infarction: how large is the gap in health expectancies? BMC Public Health. (2021) 21(1):1–10. doi: 10.1186/s12889-021-10236-7
53. Seidel-Jacobs E, Ptushkina V, Strassburger K, Icks A, Kuss O, Burkart V, et al. Socio-economic inequalities in glycaemic control in recently diagnosed adults with type 1 and type 2 diabetes. Diabet Med. (2022) 39(7):e14833. doi: 10.1111/dme.14833
54. McCormick TA, Adams JL, Lee EA, Emptage NP, Palmer-Toy DE, Martin JP, et al. Age-Dependent hemoglobin A1c therapeutic targets reduce diabetic medication changes in the elderly. EGEMS (Wash DC). (2019) 7(1):46. doi: 10.5334/egems.303
55. American Diabetes Association Professional Practice Committee. 13. Older adults: standards of care in diabetes—2024. Diabetes Care. (2024) 47(Suppl 1):S244–57. doi: 10.2337/dc24-S013
56. Liñana-Granell C, Romero-Del Barco R, Mercadal-Orfila B. Glycemic control in the elderly patient with type 2 diabetes mellitus treated with antidiabetics. Rev Ofil·Ilaphar. (2022) 32(1):29–33. doi: 10.4321/s1699-714x2022000100
57. Gómez-Huelgas R, Gómez Peralta F, Rodríguez Mañas L, Formiga F, Puig Domingo M, Mediavilla Bravo JJ, et al. Tratamiento de la diabetes mellitus tipo 2 en el paciente anciano. Rev Clin Esp. (2018) 218(2):74–88. doi: 10.1016/j.rce.2017.12.003
58. Feraco A, Gorini S, Camajani E, Filardi T, Karav S, Cava E, et al. Gender differences in dietary patterns and physical activity: an insight with principal component analysis (PCA). J Transl Med. (2024) 22:1112. doi: 10.1186/s12967-024-05965-3
59. De Smedt D, De Bacquer D, De Sutter J, Dallongeville J, Gevaert S, De Backer G, et al. The gender gap in risk factor control: effects of age and education on the control of cardiovascular risk factors in male and female coronary patients. The EUROASPIRE IV study by the European Society of Cardiology. Int J Cardiol. (2016) 209:284–90. doi: 10.1016/j.ijcard.2016.02.015
60. Maleki A, Haghjoo M, Ghaderi M. The impact of gender differences on healthy lifestyle and its subscales among patients with coronary artery disease. Res Cardiovasc Med. (2016) 5(4):1–6. doi: 10.5812/cardiovascmed.32995
61. Setny M, Jankowski P, Kaminski K, Gasior Z, Haberka M, Czarnecka D, et al. Secondary prevention of coronary heart disease in Poland: does sex matter? Results from the POLASPIRE survey. Polish Arch Intern Med. (2022) 132(3):22. doi: 10.20452/pamw.16179
62. Hiller J, Schatz K, Drexler H. Gender influence on health and risk behavior in primary prevention: a systematic review. J Public Health. (2017) 25:339–49. doi: 10.1007/s10389-017-0798-z
63. Jayawardana S, Esquivel M, Orešković T, Mossialos E. Gender differences in COVID-19 preventative measures and vaccination rates in the United States: a longitudinal survey analysis. Vaccine. (2024) 42(23):126044. doi: 10.1016/j.vaccine.2024.06.012
64. Minges KE, Strait KM, Owen N, Dunstan DW, Camhi SM, Lichtman J, et al. Gender differences in physical activity following acute myocardial infarction in adults: a prospective, observational study. Eur J Prev Cardiol. (2017) 24(2):192–203. doi: 10.1177/2047487316679905
65. Perera S, Aslam A, Stehli J, Kaye D, Layland J, Nicholls SJ, et al. Gender differences in healthy lifestyle adherence following percutaneous coronary intervention for coronary artery disease. Hear Lung Circ. (2021) 30(1):e37–40. doi: 10.1016/j.hlc.2020.06.024
66. Bauman AE, Reis RS, Sallis JF, Wells JC, Loos RJ, Martin BW. Correlates of physical activity: why are some people physically active and others not? Lancet. (2012) 380(9838):258–71. doi: 10.1016/S0140-6736(12)60735-1
67. Ricardo LIC, Wendt A, Costa CDS, Mielke GI, Brazo-Sayavera J, Khan A, et al. Gender inequalities in physical activity among adolescents from 64 global south countries. J Sport Health Sci. (2022) 11(4):509–20. doi: 10.1016/j.jshs.2022.01.007
68. Sfm C, Van Cauwenberg J, Maenhout L, Cardon G, Lambert EV, Van Dyck D. Inequality in physical activity, global trends by income inequality and gender in adults. Int J Behav Nutr Phys Act. (2020) 17:142. doi: 10.1186/s12966-020-01039-x
69. Leite GS, Lucena Alves CP, Leão OAA, Crochemore-Silva I. Gender, ethnicity, and socioeconomic inequalities in physical activity throughout the life course: a systematic review of cohort studies. J Phys Act Health. (2024) 21(12):1276–85. doi: 10.1123/jpah.2024-0313
70. López-Ferreruela I, Malo S, Obón-Azuara B, Rabanaque MJ, Gamba A, Castel-Feced S, et al. Gender inequalities in prescribing and initiation patterns of guideline-recommended drugs after acute myocardial infarction. BMC Public Health. (2025) 25:185. doi: 10.1186/s12889-025-21396-1
71. Sotorra-Figuerola G, Ouchi D, García-Sangenís A, Giner-Soriano M, Morros R. Pharmacological treatment after acute coronary syndrome: baseline clinical characteristics and gender differences in a population-based cohort study. Aten Primaria. (2022) 54(1):102157. doi: 10.1016/j.aprim.2021.102157
72. Abrahamyan L, Sahakyan Y, Wijeysundera HC, Krahn M, Rac VE. Gender differences in utilization of specialized heart failure clinics. J Women’s Heal. (2018) 27(5):623–9. doi: 10.1089/jwh.2017.6461
73. Dagan M, Dinh DT, Stehli J, Tan C, Brennan A, Warren J, et al. Sex disparity in secondary prevention pharmacotherapy and clinical outcomes following acute coronary syndrome. Eur Hear J Qual Care Clin Outcomes. (2022) 8(4):420–8. doi: 10.1093/ehjqcco/qcab007
74. Setny M, Jankowski P, Krzykwa A, Kamiński KA, Gąsior Z, Haberka M, et al. Management of dyslipidemia in women and men with coronary heart disease: results from polaspire study. J Clin Med. (2021) 10(12):2594. doi: 10.3390/jcm10122594
75. Spadafora L, Mohammadi T, Bernardi M, Testa A, Tun HN, D'Ascenzo F, et al. Appraising features and outlook of women and men discharged after an acute coronary syndrome: evidence from the 23,700-patient PRAISE international registry. Panminerva Med. (2023) 65(4):454–60. doi: 10.23736/S0031-0808.23.04909-1
76. Virani SS, Woodard LD, Ramsey DJ, Urech TH, Akeroyd JM, Shah T, et al. Gender disparities in evidence-based statin therapy in patients with cardiovascular disease. Am J Cardiol. (2015) 115(1):21–6. doi: 10.1016/j.amjcard.2014.09.041
77. Schultz WM, Kelli HM, Lisko JC, Varghese T, Shen J, Sandesara P, et al. Socioeconomic Status and cardiovascular outcomes: challenges and interventions. Circulation. (2018) 137(20):2166–78. doi: 10.1161/CIRCULATIONAHA.117.029652
78. Singh H, Johnson ML. Prescribing patterns of diuretics in multi-drug antihypertensive regimens. J Clin Hypertens (Greenwich). (2005) 7(2):81–7; quiz 88–9. doi: 10.1111/j.1524-6175.2005.03922.x
79. Rochon PA, Li J, O'Mahony D, Onder G, Petrovic M, Sternberg SA, et al. The impact of age, sex, and gender on polypharmacy and potential prescribing cascades: lessons from five databases. J Am Geriatr Soc. (2025) 73(2):520–32. doi: 10.1111/jgs.19282
Keywords: gender inequalities, delivery of healthcare, healthcare utilization, cardiovascular risk factors, myocardial infarction, secondary prevention, real-world data
Citation: López-Ferreruela I, Gimeno-Miguel A, Laguna-Berna C, Malo S, Castel-Feced S, José Rabanaque M and Aguilar-Palacio I (2025) When gender matters: inequalities in health services utilization and risk factors monitoring after acute myocardial infarction. Front. Glob. Women's Health 6:1605400. doi: 10.3389/fgwh.2025.1605400
Received: 3 April 2025; Accepted: 11 June 2025;
Published: 26 June 2025.
Edited by:
Elena Marbán-Castro, Women in Global Health Spain, SpainReviewed by:
Luigi Spadafora, Sapienza University of Rome, ItalyVincenza Giordano, Policlinico Tor Vergata, Italy
Fadoum Hassan, National health fund, Djibouti
Copyright: © 2025 López-Ferreruela, Gimeno-Miguel, Laguna-Berna, Malo, Castel-Feced, José Rabanaque and Aguilar-Palacio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Irene López-Ferreruela, aXJlbmUuaWxmQGhvdG1haWwuY29t