 Nurshad Ali
Nurshad Ali- Department of Biochemistry and Molecular Biology, Shahjalal University of Science and Technology, Sylhet, Bangladesh
The COVID-19 outbreak is a great threat to public health worldwide. Lung injury is the main outcome of COVID-19 infection; however, damage can occur in other organs including the liver. Currently, limited data are available that link underlying liver injury with the severe SARS-CoV-2 infection. This review summarizes the available data on liver test abnormalities in COVID-19 patients; critically evaluates the possible causes of liver injury and provides recommendations for clinicians. In laboratory tests, serum levels of liver test markers notably transaminase, gamma-glutamyl transferase and total bilirubin were significantly higher in severe patients with COVID-19 infection. The use of certain drugs especially lopinavir and ritonavir showed an association with the progression of liver damage in severe cases. Available data suggest that liver injury in COVID-19 patients may result from direct effect by the virus, immune-mediated inflammation or drug-induced toxicity. Some studies demonstrated that COVID-19 patients with pre-existing liver disease are at higher risk for hospitalizations and mortality. Therefore, the impact of pre-existing liver disease on treatment and clinical outcomes of COVID-19 should be determined. Large-scale clinical studies are needed to identify the causes of liver injury in patients with COVID-19 infection.
Introduction
The COVID-19 pandemic poses a great challenge to the international healthcare system. Older adults and those at any age with hypertension, coronary heart disease and diabetes are at higher risk of SARS-CoV-2 infection and severe disease course (1, 2). Although the lung is the main target organ of SARS-CoV-2 infection; damage can occur in multiple organs. The liver is the vital organ in the human body and its exposure to the viral particles might be an additional concern for CVID-19 patients. Up to now, there is no strong evidence that the liver cells are exposed to SARS-CoV-2 in severe cases. Moreover, it remains unclear yet to what extent liver diseases are considerable risk factors of COVID-19 severity and mortality.
Liver impairment is an emerging concern with COVID-19, as it was observed with the similar coronavirus SARS. According to previous studies, up to 60% of patients had a liver impairment, with liver biopsy specimens suggesting viral nucleic acid and damage (3–5). In these studies authors noted that this might have been the result of drug-induced liver damage, given that the majority of the patients were treated with high doses of antibiotics, hepatotoxic antiviral drugs and steroids.
Some studies have reported the clinical features and laboratory test results associated with liver dysfunction in patients with COVID-19 infection (6–13). Although, pre-existing liver conditions have not been listed in most of these studies and the interaction of pre-existing liver disease with COVID-19 has not been investigated, which are major limitations in evaluating the underlying causes of liver injury in the severe disease course. However, the elevated levels of alanine aminotransferase and reduced platelet counts and reduced levels of albumin showed an association with higher fatality in COVID-19 patients (2). It is still unknown whether these laboratory analyses are an indicator of pre-existing hepatic diseases in severe patients, whether they rather mirror liver failure caused by the SARS-CoV-2 itself (14). Overreaction of the immune system may also contribute to disease progression and can lead to liver injury (15). Serum concentrations of pro-inflammatory cytokines, including C-reactive protein (CRP) TNF-α, IL-1β, and IL-6 were seen at elevated levels in most of the severe cases, indicating cytokine storm syndrome might be associated with the disease severity (16, 17). It is also considered that systemic infections might influence liver functions in a severe disease course. Further clinical studies can provide a better insight on liver damage in severe patients with SARS-CoV-2 infection. This review summarizes the available data on liver test abnormalities in COVID-19 patients; critically evaluates the possible causes of liver injury and provides recommendations for clinicians. Online databases including Google Scholar, PubMed, Scopus, and medRxiv were searched to identify relevant publications using relevant keywords.
Prevalence of Liver Function Test Abnormalities in COVID-19 Patients
Several studies have demonstrated the different degrees of elevated liver test markers in COVID-19 patients, mainly reported by alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma-glutamyl transferase (GGT) levels accompanied by moderately elevated prothrombin time (PT), and total bilirubin (TB) levels (6–13, 17–27). However, there are limited numbers of studies that have specifically investigated the clinical characteristics of liver failure in COVID-19 patients. The available reports on liver function tests in COVID-19 patients are listed in Table 1. Of these studies, an increasing trend for liver enzymes has been observed in severe/non-survivor patients. The prevalence of elevated ALT, AST, and GGT were up to 82, 75, and 72%, respectively. A recent study reported 76.3% of liver test abnormalities and 21.5% of liver injury among hospitalized COVID-19 patients (6). Serum levels of ALT, AST, GGT and TB were significantly higher (p < 0.01) in ICU admitted severe patients than non-severe patients (6). In that study, 26.7% of patients with liver test abnormalities showed a progression to severe pneumonia. The abnormal liver tests were more pronounced in patients within 2 weeks of hospitalization. The liver injury was significantly higher in severe patients than non-severe patients. The authors also noted that patients in hepatocyte type had significantly higher odds for progression to severe COVID-19. In another study, concentrations of ALT, AST, GGT, ALP, and TB were markedly higher in deceased patients than in recovered patients (19). About 52% of deceased patients and 16% who recovered had elevated AST levels (19). In a retrospective study, the levels of ALT, AST, GGT, and TB, showed statistically significant elevation in severe COVID-19 patients compared with that in mild patients (27). ALT and AST abnormalities were also found at least two times higher in severe patients than non-severe patients (13). Moreover, a large cohort study including 1,099 patients, reported an elevated level of ALT and AST (28.1 and 39.4%, respectively) in severe patients than non-severe patients (19.8 and 18.2%, respectively) (8). Similarly, the prevalence of elevated AST in ICU patients (62%) was higher than non-ICU patients (25%) (28). Furthermore, in another publication, AST abnormalities were found lower in patients before the onset of symptoms than the patients did diagnose after the onset of symptoms (9). Other studies, however, reported different results. For example, Wu et al. did not find significant differences in liver function tests when compared to mild cases with severe cases (26). Another study consisted of 339 elderly COVID-19 patients and reported no evident differences in ALT levels between death and survival (25). Therefore, researchers also argue that though liver function tests abnormalities are common in COVID-19 patients, liver functions impairment maybe not a prominent feature of COVID-19 (27). However, the major studies clearly indicated increased liver dysfunctions in severe COVID-19 patients, though clinically significant liver failure has rarely been described.
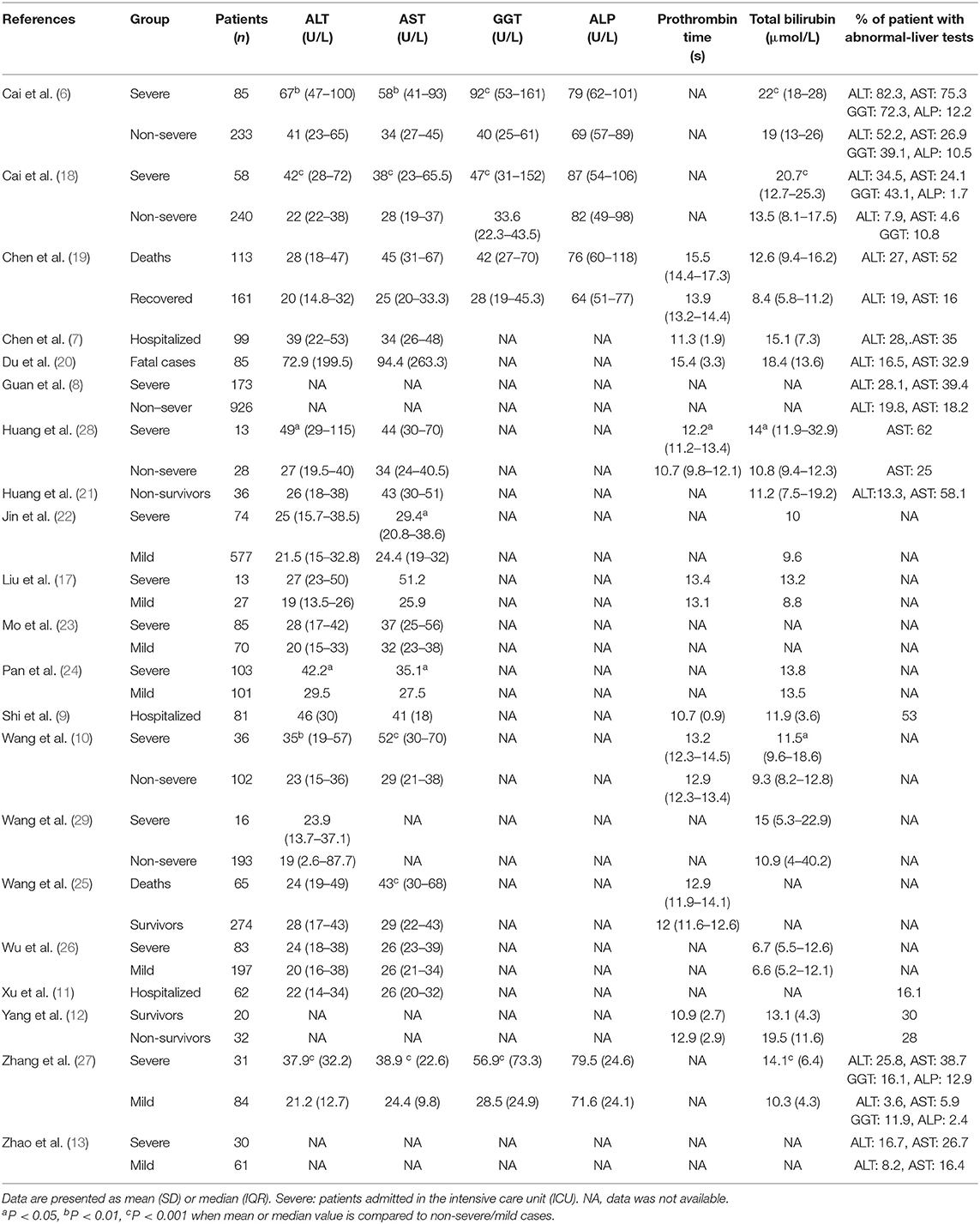
Table 1. Liver function test abnormalities in COVID-19 patients.
Possible Effects of Drugs on Liver Function in Covid-19 Patients
It is also possible that the drugs used in the treatment are associated with liver injury in COVI19 patients. For example, the use of multiple drugs, such as antibiotics, antivirals, antipyretics and analgesics, and traditional Chinese medicine may cause liver injury in COVID-19 patients (30). Yet, there is no clear evidence that the liver dysfunctions during hospitalization are completely drug-induced in severe patients with COVI-19 infection. In a recent study, the liver biopsy specimen of a patient who died from COVID-19 showed elevated liver enzymes that could be the partial effects of drugs used in the treatment, and the liver dysfunction may be occurred because of sepsis and shock (6). It has been indicated that angiotensin II receptor blockers and ACE-inhibitors drugs may inhibit liver functions in COVID-19 patients (6). In that study, elevated levels of liver enzymes were observed among participants who used ACE-Is/ARBs drugs during hospitalization, though; the elevation was not significant with those who did not use these drugs (6). The authors also observed that the drugs lopinavir and ritonavir contributed significantly to liver test abnormalities and liver injury. These drugs increased the odds of liver injury by four-fold (p < 0.001). Moreover, using antibiotics in the treatment also showed an association with the increased prevalence of liver test abnormalities in the regression model; however in other models this association was not significant (6). Another study showed 55.4% of liver injuries after treatment with lopinavir and ritonavir, suggesting possible drug-induced liver damage in COVID-19 patients (30). A randomized controlled trial reported gastrointestinal adverse events in COVID-19 patients, who received lopinavir-ritonavir in the treatment (31). However, no remarkable differences were observed in the levels of liver test markers (ALT and AST) between the lopinavir-ritonavir group and standard care group of COVID-19 patients. Hydroxychloroquine, an antimalarial agent has not been associated with liver injury in COVID-19; however, it should be used with caution to avoid any harmful effects. Future studies would be worth conducting in determining the possible effects of drugs on liver function in COVID-19 patients.
Possible Mechanisms of Liver Injury in Covid-19 Infection
It is speculated that liver injury in patients with SARS-CoV-2 infection may have occurred by directly the virus itself (32). Presence of diarrhea in 2–10% of patients, and SARS-CoV-2 RNA in blood and stools of patients with COVID-19 (33), indicating a possible viral inclusion in the liver (15). A recent review demonstrated that both SARS-CoV-2 and SARS-CoV use angiotensin-converting enzyme 2 (ACE2) receptor to enter the target host cell (10), which then subsequently infects the upper respiratory tract and lung cells. In pathological studies, patients with SARS showed the viral presence in their liver tissue at a low level (34), however, patients with MERS, virus were not detected in their liver tissue (35). Serum GGT, a potential diagnostic marker for cholangiocyte injury has been found at increased levels up to 72% in severe COVID-19 patients (6, 15). A preliminary study reported that the ACE2 receptor is abundantly expressed in cholangiocytes (36); suggesting that SARS-CoV-2 might bind to ACE2-positive cholangiocytes and cause liver dysfunction (15). Nonetheless, viral inclusions were not identified in the liver tissue of a patient who died from COVID-19 (37). Apart from these observations, it is also assumed that antiviral drugs used for the treatment might be linked with liver damage in COVID-19 patients (6, 15). Although, it remains unclear to what extent viruses or drugs are associated with liver injury in severe disease courses. Dysregulation of the innate immune response may be another important aspect of liver injury in COVID-19. So, the possible pathways that can be associated with liver damage in COVID-19 patients are (i) immune-mediated inflammation, such as cytokines storm and pneumonia-related hypoxia, (ii) Direct cytotoxicity because of active viral replication in the liver cells, (iii) Drug-induced liver damage: initially recommend antiviral drugs including lopinavir/ritonavir, chloroquine, remdesivir, tocilizumab, uminefovir, being potentially hepatotoxic in severe patients, (iv) Reactivation of pre-existing hepatic disease: patients with previous chronic hepatic disease are more vulnerable to hepatic damage from this viral infection, (v) Possible reactivation of hepatitis B virus with some biological drugs such as tocilizumab and baricitinib that may lead to liver dysfunction. Moreover, it is also unknown whether SARS -CoV−2 infection enhances cholestasis in patients with underlying cholestatic hepatic diseases. More mechanistic studies regarding virus entry and replication in liver cells and the potential consequences of drugs in the liver are required.
Covid-19 Patients With Pre-Existing Liver Disease
Data on pre-existing liver disease in COVID-19 would be worth in evaluating the underlying causes of liver damage in severe disease courses. However, limited information is available on the interaction between pre-existing liver disease and COVID-19. A recent study examined the effects of pre-existing liver disease on outcomes in a large cohort of COVID-19 patients (n = 2,780) in the USA (38). The authors observed a higher proportion of comorbidities (diabetes 48% and hypertension 68%) in patients with liver disease. Fatty liver disease and non-alcoholic steatohepatitis (42%) were more frequent among patients with pre-existing liver disease. Importantly, the mortality rate was significantly higher (p < 0.001) in patients with pre-existing liver disease than patients without liver disease and the relative risk was markedly higher in patients with cirrhosis (p < 0.001) (38). Moreover, patients with pre-existing liver disease required increased hospitalization. Another recent study reported a high mortality rates from COVID-19 among patients with chronic liver disease and cirrhosis (39). The authors demonstrated that patients with liver cirrhosis could result in decompensation of the liver and mortality. Patients with cirrhosis had poor outcomes with an overall mortality rate of 40%. Those with decompensated cirrhosis had a mortality rate between 43 and 63%, compared with 12% for patients with hepatic disease but without cirrhosis (39). In that investigation, there were many COVID-19 positive patients who had no respiratory problems, suggesting that patients with chronic liver disease should get priority for COVID-19 testing even in the absence of typical COVID-19 symptoms. The probable reasons for poor outcomes in COVID-19 with pre-existing liver disease require further investigation; however, it seems that there is interplay between local liver injury and systemic disturbances (38).
Management and Challenges of Liver Injury During Covid-19 Infection
Although, there is no direct evidence on liver failure in COVID-19 patients without pre-existing liver disease; several measures should be considered for all patients with COVID-19 during hospitalization. For example, individuals who are at high risk of hepatitis A infection should maintain personal hygiene and avoid large gatherings during this pandemic. Presently there is no evidence that people with hepatitis B and hepatitis C are at higher risk of infections. However, people living with hepatitis B and C should follow a healthy lifestyle and should also continue their regular treatments if they are affected by COVID-19 infection. People with pre-existing liver disease or after liver transplantation should follow the same preventive measures being followed by people with other medical conditions to avoid getting sick with or spreading COVID-19 infection. Moreover, attention should be paid to older people with severe medical conditions including liver test abnormalities as they are at higher risk of becoming severely ill from this infection. In addition, (i) the liver test markers should be measured and monitored regularly for all COVID-19 patients, (ii) Serologic testing for hepatitis B and C should take into consideration for COVID-19 patients during the measure of liver test biochemistries, (iii) Up to now, data are missing on the safety of drugs used for the treatment of COVID-19 patients with liver dysfunction, therefore, the detrimental effects of drugs on the liver injury during the treatment should be monitored and assessed frequently.
Conclusions and Recommendations
Abnormal liver function test markers are more common in patients with severe COVID-infection. Available study findings support the hypothesis that liver injury might be associated with severe outcomes in COVID-19 patients. However, there is still lacks important data on larger studies to determine causality between COVID-19 and liver damage. The mechanism of liver injury in COVID-19 infection is not well-understood yet and seems to be multifactorial. The patients with advanced hepatic disease and those after liver transplantation are at high risk of progression to severe disease course. Therefore, it is recommended to identify and care for patients with chronic liver disease with priority within the limited healthcare resources. COVID-19 patients with liver injury are advised to be treated with drugs that are able to inhibit inflammatory responses and protect liver functions. In addition, the detrimental effects of certain drugs on the liver injury during hospitalization should be monitored and evaluated regularly. Attention should also pay toward modulating innate immune dysfunction in severe cases. Moreover, the effects of pre-existing liver disease on treatment and clinical outcomes of COVID-19 should be determined. Future research should focus on the potential causes of liver damage in severe patients with COVID-19 infection.
Author Contributions
The author confirms being the sole contributor of this work and has approved it for publication.
Conflict of Interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Yang J, Zheng Y, Gou X, Pu K, Chen Z, Guo Q, et al. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: a systematic review and meta-analysis. Int J Infect Dis. (2020) 94:91–5. doi: 10.1016/j.ijid.2020.03.017
2. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. (2020) 395:1054–62. doi: 10.1016/S0140-6736(20)30566-3
3. Lee N, Hui D, Wu A, Chan P, Cameron P, Joynt GM, et al. A major outbreak of severe acute respiratory syndrome in Hong Kong. N Engl J Med. (2003) 348:1986–94. doi: 10.1056/NEJMoa030685
4. Peiris J, Lai S, Poon L, Guan Y, Yam L, Lim W, et al. Coronavirus as a possible cause of severe acute respiratory syndrome. Lancet. (2003) 361:1319–25. doi: 10.1016/S0140-6736(03)13077-2
5. Tsang KW, Ho PL, Ooi GC, Yee WK, Wang T, Chan-Yeung M, et al. A cluster of cases of severe acute respiratory syndrome in Hong Kong. N Engl J Med. (2003) 348:1977–85. doi: 10.1056/NEJMoa030666
6. Cai Q, Huang D, Yu H, Zhu Z, Xia Z, Su Y, et al. COVID-19: abnormal liver function tests. J Hepatol. (2020). doi: 10.1016/j.jhep.2020.04.006. [Epub ahead of print].
7. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. (2020) 395:507–13. doi: 10.1016/S0140-6736(20)30211-7
8. Guan W, Ni Z, Hu Y, Liang W, Ou C, He J, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. (2020) 382:1708–20. doi: 10.1056/NEJMoa2002032
9. Shi H, Han X, Jiang N, Cao Y, Alwalid O, Gu J, et al. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: a descriptive study. Lancet Infect Dis. (2020) 20:425–34. doi: 10.1016/S1473-3099(20)30086-4
10. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. (2020) 323:1061. doi: 10.1001/jama.2020.1585
11. Xu X-W, Wu X-X, Jiang X-G, Xu K-J, Ying L-J, Ma C-L, et al. Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: retrospective case series. BMJ. (2020) 368:m606. doi: 10.1136/bmj.m606
12. Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Resp Med. (2020) 8:475–81. doi: 10.1016/S2213-2600(20)30079-5
13. Zhao X-Y, Xu X-X, Yin H-S, Hu Q-M, Xiong T, Tang Y-Y, et al. Clinical characteristics of patients with 2019 coronavirus disease in a non-Wuhan area of Hubei Province, China: a retrospective study. BMC Infect Dis. (2020) 20:311. doi: 10.1186/s12879-020-05010-w
14. Boettler T, Newsome PN, Mondelli MU, Maticic M, Cordero E, Cornberg M, et al. Care of patients with liver disease during the COVID-19 pandemic: EASL-ESCMID position paper. JHEP Rep. (2020) 2:100113. doi: 10.1016/j.jhepr.2020.100113
15. Zhang C, Shi L, Wang F-S. Liver injury in COVID-19: management and challenges. Lancet Gastroenterol Hepatol. (2020) 5:428–30. doi: 10.1016/S2468-1253(20)30057-1
16. Ali N. Elevated level of C-reactive protein may be an early marker to predict risk for severity of COVID-19. J Med Virol. (2020) 26097. doi: 10.1002/jmv.26097. [Epub ahead of print].
17. Liu J, Li S, Liu J, Liang B, Wang X, Wang H, et al. Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients. EBioMedicine. (2020) 55:10276. doi: 10.1016/j.ebiom.2020.102763
18. Cai Q, Huang D, Ou P, Yu H, Zhu Z, Xia Z, et al. COVID-19 in a designated infectious diseases hospital outside Hubei Province, China. Allergy. (2020) 14309. doi: 10.1111/all.14309. [Epub ahead of print].
19. Chen T, Wu D, Chen H, Yan W, Yang D, Chen G, et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study. BMJ. (2020) 368:m1091. doi: 10.1136/bmj.m1091
20. Du Y, Tu L, Zhu P, Mu M, Wang R, Yang P, et al. Clinical features of 85 fatal cases of COVID-19 from Wuhan. A retrospective observational study. Am J Respir Crit Care Med. (2020) 201:1372–9. doi: 10.1164/rccm.202003-0543OC
21. Huang Y, Yang R, Xu Y, Gong P. Clinical characteristics of 36 non-survivors with COVID-19 in Wuhan, China. Infect Dis. (2020) 395:497–506. doi: 10.1101/2020.02.27.20029009
22. Jin X, Lian J-S, Hu J-H, Gao J, Zheng L, Zhang Y-M, et al. Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms. Gut. (2020) 69:1002–9. doi: 10.1136/gutjnl-2020-32092
23. Mo P, Xing Y, Xiao Y, Deng L, Zhao Q, Wang H, et al. Clinical characteristics of refractory COVID-19 pneumonia in Wuhan, China. Clin Infect Dis. (2020) ciaa270. doi: 10.1093/cid/ciaa270
24. Pan L, Mu M, Yang P, Sun Y, Wang R, Yan J, et al. Clinical characteristics of COVID-19 patients with digestive symptoms in Hubei, China: a descriptive, cross-sectional, multicenter study. Am J Gastroenterol. (2020) 115:620. doi: 10.14309/ajg.0000000000000620
25. Wang L, He W, Yu X, Hu D, Bao M, Liu H, et al. Coronavirus disease 2019 in elderly patients: characteristics and prognostic factors based on 4-week follow-up. J Infect. (2020) 80:639–45. doi: 10.1016/j.jinf.2020.03.019
26. Wu J, Li W, Shi X, Chen Z, Jiang B, Liu J, et al. Early antiviral treatment contributes to alleviate the severity and improve the prognosis of patients with novel coronavirus disease (COVID-19). J Intern Med. (2020) 288:128–38. doi: 10.1111/joim.13063
27. Zhang Y, Zheng L, Liu L, Zhao M, Xiao J, Zhao Q. Liver impairment in COVID-19 patients: a retrospective analysis of 115 cases from a single centre in Wuhan city, China. Liver Int. (2020) 14455. doi: 10.1111/liv.14455. [Epub ahead of print].
28. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
29. Wang G, Wu C, Zhang Q, Wu F, Yu B, Lv J, et al. C-reactive protein level may predict the risk of COVID-19 aggravation. Open Forum Infect Dis. (2020) 7:ofaa153. doi: 10.1093/ofid/ofaa153
30. Cai Q, Huang D, Ou P, Yu H, Zhu Z, Xia Z, et al. COVID-19 in a designated infectious diseases hospital outside Hubei Province, China. Public Global Health. (2020). doi: 10.1101/2020.02.17.20024018. [Epub ahead of print].
31. Cao B, Wang Y, Wen D, Liu W, Wang J, Fan G, et al. A trial of lopinavir–ritonavir in adults hospitalized with severe Covid-19. N Engl J Med. (2020) 382:1787–99. doi: 10.1056/NEJMoa2001282
32. Garrido I, Liberal R, Macedo G. Review article: COVID-19 and liver disease-what we know on 1st May 2020. Aliment Pharmacol Ther. (2020) 52:267–75. doi: 10.1111/apt.15813
33. Yeo C, Kaushal S, Yeo D. Enteric involvement of coronaviruses: is faecal–oral transmission of SARS-CoV-2 possible? Lancet Gastroenterol Hepatol. (2020) 5:335–7. doi: 10.1016/S2468-1253(20)30048-0
34. Chau T-N, Lee K-C, Yao H, Tsang T-Y, Chow T-C, Yeung Y-C, et al. SARS-associated viral hepatitis caused by a novel coronavirus: report of three cases. Hepatology. (2004) 39:302–10. doi: 10.1002/hep.20111
35. Alsaad KO, Hajeer AH, Al Balwi M, Al Moaiqel M, Al Oudah N, Al Ajlan A, et al. Histopathology of middle east respiratory syndrome coronovirus (MERS-CoV) infection - clinicopathological and ultrastructural study. Histopathology. (2018) 72:516–24. doi: 10.1111/his.13379
36. Chai X, Hu L, Zhang Y, Han W, Lu Z, Ke A, et al. Specific ACE2 expression in cholangiocytes may cause liver damage after 2019-nCoV infection. bioRxiv [preprint]. (2020). doi: 10.1101/2020.02.03.931766
37. Xu Z, Shi L, Wang Y, Zhang J, Huang L, Zhang C, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Resp Med. (2020) 8:420–2. doi: 10.1016/S2213-2600(20)30076-X
38. Singh S, Khan A. Clinical characteristics and outcomes of COVID-19 among patients with pre-existing liver disease in United States: a multi-center research network study. Gastroenterology. (2020). doi: 10.1053/j.gastro.2020.04.064. [Epub ahead of print].
39. Moon AM, Webb GJ, Aloman C, Armstrong MJ, Cargill T, Dhanasekaran R, et al. High mortality rates for SARS-CoV-2 infection in patients with pre-existing chronic liver disease and cirrhosis: Preliminary results from an international registry. J Hepatol. (2020). doi: 10.1016/j.jhep.2020.05.013. [Epub ahead of print].
Keywords: SARS-CoV-2, COVID-19, liver enzymes, liver disease, liver injury
Citation: Ali N (2020) Relationship Between COVID-19 Infection and Liver Injury: A Review of Recent Data. Front. Med. 7:458. doi: 10.3389/fmed.2020.00458
Received: 13 May 2020; Accepted: 09 July 2020;
Published: 21 July 2020.
Edited by:
Francesco Marotta, ReGenera R&D International for Aging Intervention, ItalyReviewed by:
Amin Talebi Bezmin Abadi, Tarbiat Modares University, IranDipen Vyas, Biorg, Inc., United States
Copyright © 2020 Ali. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nurshad Ali, bnVyX3J1YmRAeWFob28uY29t; bmFsaS1ibWJAc3VzdC5lZHU=
†ORCID: Nurshad Ali orcid.org/0000-0003-1649-0887