 Josephine Mistegård1
Josephine Mistegård1 Bjorn Gudbjornsson2
Bjorn Gudbjornsson2 Ulla Lindqvist3Leena Laasonen4Leif Ejstrup5Mona Ståhle6Lars Iversen1*
Ulla Lindqvist3Leena Laasonen4Leif Ejstrup5Mona Ståhle6Lars Iversen1*- 1Department of Dermatology, Aarhus University Hospital, Aarhus, Denmark
- 2Faculty of Medicine, Centre for Rheumatology Research, Landspitali University Hospital, University of Iceland, Reykjavik, Iceland
- 3Department of Medical Sciences, Rheumatology, Uppsala University, Uppsala, Sweden
- 4Helsinki Medical Imaging Center, Helsinki University Central Hospital, Helsinki, Finland
- 5Department of Rheumatology, Odense University Hospital, Odense, Denmark
- 6Dermatology Division, Department of Medicine, Karolinska Institutet, Stockholm, Sweden
Objective: Psoriatic arthritis mutilans (PAM) is the most severe phenotype of psoriatic arthritis due to excessive bone erosion causing joint destruction and decreased functional capacity. The aim of this study was to investigate the prevalence of comorbidities among patients with PAM and the association between comorbidities and joint involvement.
Methods: A total of 66 patients aged ≥18 years from the Nordic countries with past or present psoriasis along with at least one mutilated joint were included in the present study.
Results: The median number of comorbid conditions per patient was 1 [interquartile range (IQR) 0–2] and 16.7% reported three or more comorbidities. The most frequent comorbidity was hypertension (36.4%). The median number of mutilated joints per patient was 3 (IQR 1–8.3; range 1–38).
Conclusion: Two thirds of the patients with PAM reported comorbid conditions and the most frequent was hypertension which affected more than a third of the patients. However, this study was unable to detect any association between comorbidities and the severity of PAM.
Introduction
Psoriatic arthritis (PsA) is an inflammatory musculoskeletal disease affecting 20–30% of patients with psoriasis (1–3). In the majority of patients with PsA, skin affection precedes arthritis by several years (4). PsA is characterized by synovial and entheseal inflammation along with extraarticular manifestations, such as nail lesions and uveitis (4, 5). Variable clinical presentations have given rise to five PsA subtypes: arthritis in the distal interphalangeal joints, asymmetric oligoarthritis, symmetric polyarthritis, axial spondyloarthritis, and psoriatic arthritis mutilans (PAM) (6). Any of these subtypes may be present in different combinations and the disease pattern may change over time (4, 7).
PAM is the most severe clinical subtype of PsA and is characterized by digital telescoping termed “opera-glass finger,” resulting in loss of function of the affected joint (6). The study of PAM has been impeded by the lack of internationally accepted classification criteria. However, attempts have been made in order to define PAM (8). Due to inconsistent classification criteria, reports on the prevalence of PAM vary widely with estimates ranging from 0.6 to 21% among patients with PsA (4, 6, 9–13). Meanwhile, the Nordic PAM Study reported a prevalence of nearly four cases per million inhabitants in the Nordic population (14). However, arthritis mutilans, may also occur along with rheumatoid arthritis, chronic reactive arthritis, and juvenile arthritis (15). Most previous reports of PAM are serial case reports and only few reports have included more than ten patients (3, 14, 16–19).
The pathogenesis of the different PsA phenotypes is still not fully understood. Genetic factors associated with psoriatic disease have become more clearly defined and may contribute to our understanding of the different clinical presentations of PsA (5, 20). Moreover, psoriatic disease is associated with a number of comorbidities. For example, metabolic syndrome is more prominent in patients with PsA than in the general population (21, 22). Also, the risk of cardiovascular disease (CVD) is increased among patients with PsA (22, 23). Shared inflammatory pathways, proinflammatory cytokine release and adhesion molecule expression may contribute to this association. Tumor necrosis factor (TNF)-α has been associated with endothelial dysfunction, and interleukin (IL)-17A has been associated with increased expression of adhesion and pro-inflammatory molecules associated with CVD (24, 25). Furthermore, it is well-established that the risk of mental comorbidities, such as depression and anxiety is higher among patients with psoriasis than in the general population (26–28). This may, in part, be caused by the psychosocial difficulties associated with having psoriasis but may also be related to overlapping mechanisms. The level of the proinflammatory cytokines IL-1 and IL-6 are increased in patients with both PsA and depression, indicating involvement of the same inflammatory process in both diseases (26). In addition, other inflammatory disorders, such as chronic obstructive pulmonary disease (COPD) and inflammatory bowel disease (IBD) are more prevalent among patients with PsA than among the general population (29–32).
Given its severe rheumatic manifestation, PAM may be associated with a higher inflammatory burden than other PsA phenotypes. The aim of this study was to investigate the prevalence of comorbidities among patients with PAM in the Nordic PAM Study and to explore the association between these comorbidities and joint involvement.
Methods
Patients were identified as part of The Nordic PAM Study initiated in 2009 to investigate PAM in the Nordic countries. Data collection has previously been described in detail (14, 17, 33–35). The study included patients from Denmark, Iceland, Norway and Sweden. Patients were identified in collaboration with specialist societies of dermatology and rheumatology and patient associations in each country. Included patients met the following inclusion criteria: (I) able and willing to give written informed consent; (II) age ≥18 years; (III) past or present psoriasis (skin or nails) diagnosed by a dermatologist; (IV) presence of clinical arthritis of the PAM type verified by a rheumatologist; and (V) radiological findings of severe erosive arthritis, e.g., pencil-in-cup or gross osteolysis of the bones. Patients meeting any classification criteria for any other rheumatic joint disease were excluded from the study. At present 70 patients have been included in the study. However, four patients were excluded from the present analysis due to missing information on joint involvement, leaving a cohort of 66 patients with PAM. The current inclusion is depicted in Figure 1 (14). The latest patient was included in April 2014. Cohort characteristics have been described previously and patient demographics of the present cohort are presented in Table 1 (14, 33, 35).
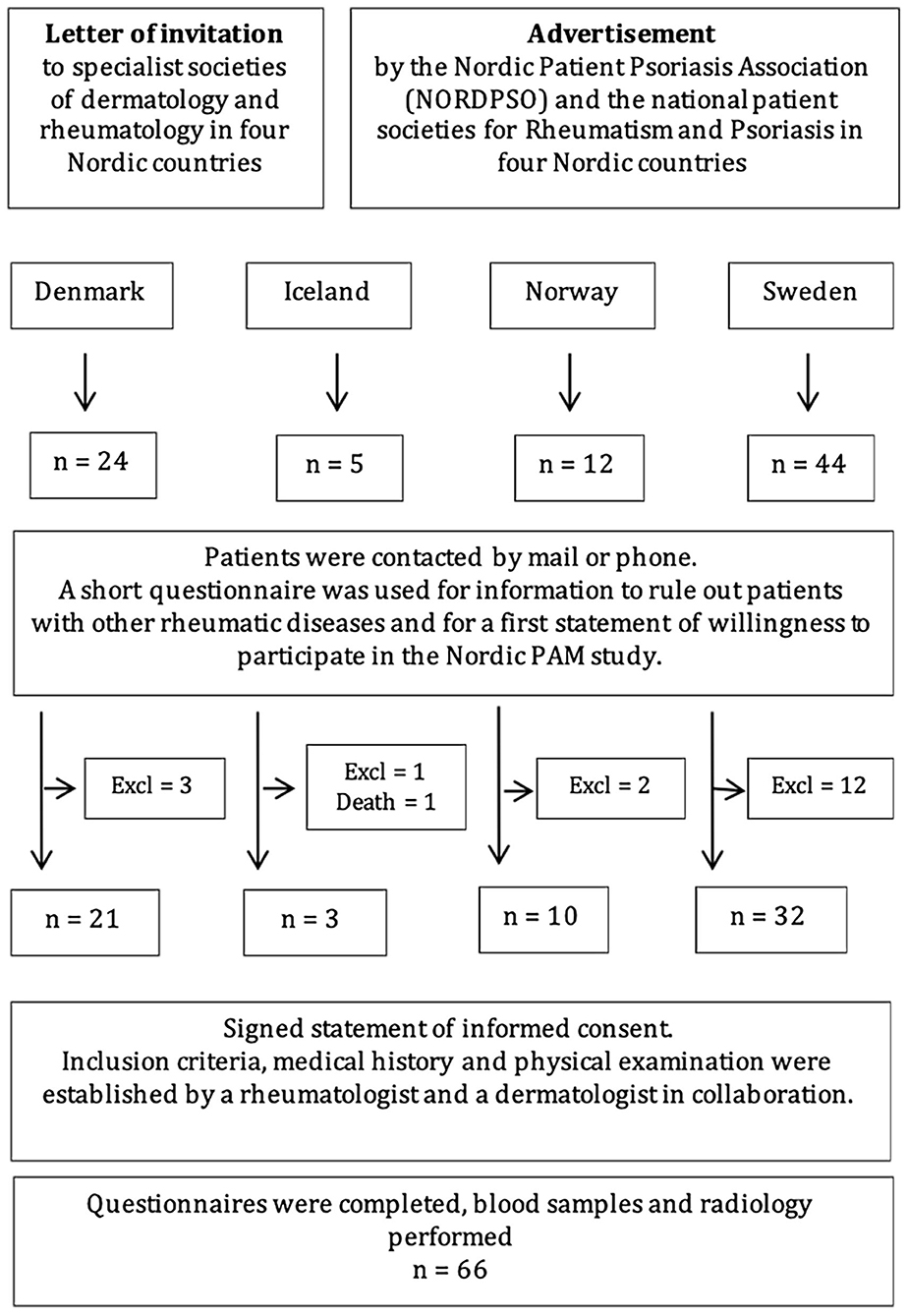
Figure 1. STROBE flowchart of the recruitment and inclusion process.
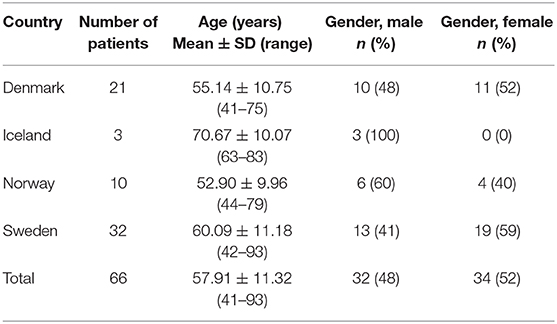
Table 1. Demographics of patients included in the Nordic PAM Study.
Clinical Examination and Data Collection
All patients who met the inclusion criteria underwent clinical evaluation by board-certified specialists in rheumatology and dermatology. The extent of joint involvement was assessed according to the 66/68 American College of Rheumatology (ACR) joint count for swelling and for tenderness. This joint count includes both the proximal interphalangeal (PIP) and the distal interphalangeal (DIP) joints of hands and feet. The presence of joint deformities, joint mutilation, dactylitis, and enthesitis was registered. A joint was considered mutilated in the presence of both clinical manifestation of PAM and joint destruction characterized by osteolysis on X-ray evaluation. Joints were radiographed at inclusion if the most recent previous radiographs had been made more than 3 months prior to inclusion. X-rays were evaluated by a radiologist and the findings have been reported elsewhere (34, 35). Information on current and past history of comorbid medical illness was obtained by the investigators as part of a semi-structured interview. Listed comorbidities included cancer, diabetes mellitus, COPD, IBD, cerebral insult, hypertension, acute myocardial infarct, heart failure, other autoimmune disease, infectious disease requiring hospitalization, and others. For each patient, the type, number, onset date, and potential current symptoms and required treatment were registered for the reported comorbidities. The investigators reviewed the patients' medication list in order to verify the reported comorbidities.
Data Analysis
All patient data were coded at inclusion. Continuous data were expressed as mean ± standard deviation (SD) for normally distributed data, and non-normally distributed data were expressed as median with interquartile range (IQR). Normality was assessed by plotting histograms and performing the D'Agostino-Person normality test. Categorical variables were analyzed using descriptive statistics and reported as frequency (n, %). The descriptive statistical analysis was done in Microsoft Excel 2019. Fischer's exact test was performed in 2 × 2 tables to investigate the association between the number of comorbid conditions and the number of affected joints. This test and the D'Agostino-Person test were carried out in GraphPad Prism 8.
Ethical Issues
Written informed consent was obtained from all study participants. The bioethics committee and data protection authorities of all four countries approved the study protocol.
Results
Joint Involvement
The median number of tender joints per patient was 1 (IQR 0–7) ranging from 0 to 35, and the median number of swollen joints per patient was 1 (IQR 0–3) ranging from 0 to 16. The median number of deformed joints per patient was 0.5 (IQR 0–12.5) ranging from 0 to 59 (Figure 2). In accordance with the inclusion criteria, all included patients had a minimum of one mutilated joint. The median number of mutilated joints per patient was 3 (IQR 1–8.3) ranging from 1 to 38, with 39.4% of patients presenting five or more and 19.7% presenting ten or more mutilated joints (Figure 3).
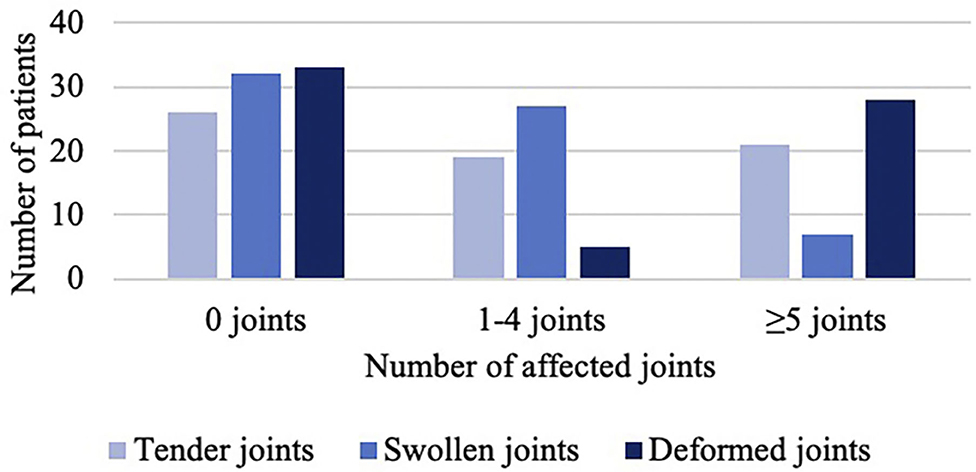
Figure 2. Number of tender, swollen, and deformed joints.
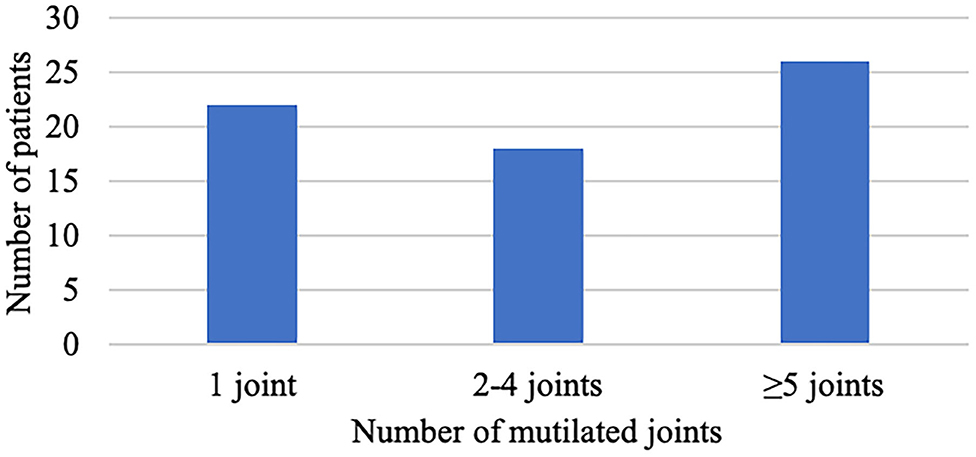
Figure 3. Number of mutilated joints.
Comorbidities
Comorbid conditions were reported by 65.2% of the participants. The median number of self-reported comorbid conditions per patient was 1 (IQR 0–2). A current or past history of two or more comorbidities was reported by 33.3% of the patients, and 16.7% reported three or more comorbidities (Figure 4A). Having two or more comorbidities was equally frequent among men and women (11:11). The most frequent comorbidity was hypertension requiring medical treatment (36.4%), followed by infectious diseases requiring hospitalization (28.8%) and other autoimmune diseases (12.1%) (Figure 4B).
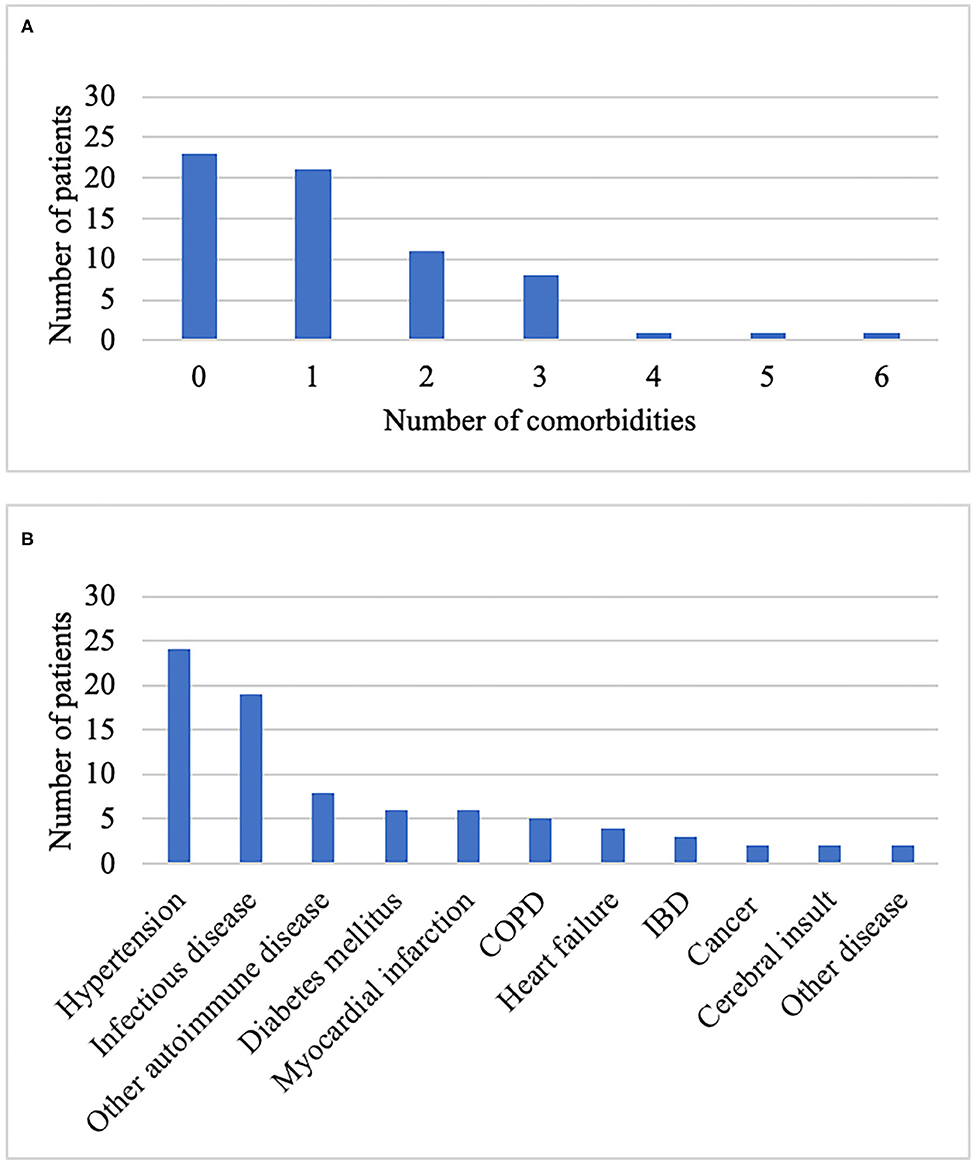
Figure 4. Comorbidities among participants in the Nordic PAM study (n = 66). (A) Number of comorbidities per participant. (B) Type of comorbidity. COPD, chronic obstructive pulmonary disease; IBD, inflammatory bowel disease.
The most frequently reported infectious diseases requiring hospitalization were pneumonia (n = 5) and skin infection due to staphylococci (n = 3). Autoimmune diseases included thyroid disease (n = 5), uveitis (n = 2), and lung fibrosis (n = 1). The reported cases of cancer were non-melanoma skin cancers (n = 2).
Correlation Between Comorbidity and the Severity of the Joint Disease
Fischer's exact test was performed to evaluate the probability of patients having one or more comorbidities in case of one or more tender joints, swollen joints, or deformed joints. Furthermore, Fisher's exact test was used to evaluate the likelihood of patients having one or more comorbidities in case of more than two mutilated joints. This test found no correlation between the number of comorbidities and the number of affected joints (Supplementary Figures 1–4).
Discussion
The Nordic PAM Study offers a unique opportunity to further investigate this rare and disabling disease, since this is presently one of the largest cohorts of patients with PAM worldwide. To the authors' knowledge, the present study is the first study to investigate the prevalence and profile of comorbidities among patients suffering from PAM. The results are in line with previously published studies describing the comorbidity profile among patients with PsA.
Recent studies of comorbidities among patients with PsA reported a median of two comorbid conditions per patient. More than a third of these patients had three or more comorbidities and some patients reported up to 12 comorbid conditions (36, 37). In the present study of patients with PAM, the median number of self-reported comorbid conditions per patient was one comorbidity and some patients reported up to six comorbidities. One third of the patients with PAM reported a current or past history of two or more comorbidities, and one fifth reported three or more comorbidities. PsA has an impact on quality of life, which is directly related to disease activity and structural damage of the joints. However, increased comorbidity burden has also been independently associated with decreased functional capacity. This considered, detection and control of comorbid conditions among patients with PsA may serve to improve quality of life in this group of patients (38).
Hypertension is frequent among patients with PsA and similar to the frequency found among patients with PAM in the present study (36, 37). This is consistent with other studies suggesting an increased prevalence of metabolic syndrome among patients with PsA compared with the general population (21, 22, 39, 40). Frequencies of diabetes mellitus and CVD are also similar between patients with PAM and patients with PsA in general (36, 37). Yet, heterogeneity in the definition and categorization of comorbidities hampers direct comparison between studies. Since the preparation of the Nordic PAM Study protocol, it has been well-established that the risk of mental comorbidities, such as depression and anxiety is higher among patients with psoriatic disease than among the general population (26–28). These are some of the most frequent comorbidities among patients with PsA, affecting approximately one third of the patients (36, 37). Data on mental illness were not collected in the Nordic PAM Study, which may very well have contributed to the relatively low reported number of comorbidities in the Nordic PAM Study. PAM is the most severe PsA phenotype and seriously affects social functioning and quality of life. Thus, mental illness may be expected more frequently among patients with PAM than among patients suffering from other PsA subtypes (33).
As described initially, many studies have indicated that the variable clinical presentations of psoriatic disease may be related to the severity of the inflammatory burden. In this context, skin severity has been described to be correlated with joint activity; thus, patients with higher skin severity are two times more likely to have increased joint involvement (41). Moreover, comorbid conditions in the form of depression and anxiety along with hypertension and diabetes mellitus are described more frequently among patients suffering from both psoriasis in the skin and PsA than among patients with only psoriasis in the skin (27, 28). In addition, studies have found that cardiovascular risk factors are more strongly associated with severe psoriasis than with mild psoriasis (28, 42). In the present study, we analyzed the correlation between the severity of the joint affection and comorbidities by applying Fisher's exact test. This test found no association either between the number of comorbidities and chronic alterations in the form of mutilated or deformed joints or between the number of comorbidities and present inflammatory alterations at the time of inclusion in the form of tender or swollen joints. Hence, this study was unable to confirm the association that other studies have suggested.
There are still no internationally accepted diagnostic criteria for this rare variant of PsA. Therefore, an inclusion criterion in the Nordic PAM Study was the presence of both clinical manifestation of PAM and confirmation of joint destruction characterized by osteolysis on X-ray evaluation.
Information on comorbidities was collected by the investigators as part of a semi-structured interview and verified through a review of the patients' medication list. The investigators registered the type, number, onset date, and potential current symptoms and required treatment for each reported comorbidity. Access to all parts of the patients' electronic medical file was not permitted in the study protocol. The use of a semi-structured interview may in this case have caused underreporting of comorbidities and thereby underestimation of the number of comorbidities among patients with PAM.
In conclusion, comorbidities are common among patients with PAM as two thirds of the participants in the Nordic PAM Study reported comorbid conditions. The most frequent comorbidity was hypertension which affected more than one third of the participants. This knowledge is important for diagnostic and therapeutic purposes alike, as knowledge of comorbidities may serve to ensure sufficient treatment and improved prognosis for patients suffering from PAM. The present study found no association between severity of joint affection and number of comorbidities. Future studies may focus on further evaluation of the significance of the inflammatory burden in the pathogenesis of the various PsA phenotypes.
Data Availability Statement
The data analyzed in this study is subject to the following licenses/restrictions: the datasets contain personally identifiable information and has therefore not been published in accordance with Danish legislation. Requests to access these datasets should be directed to Lars Iversen,bGFycy5pdmVyc2VuQGNsaW4uYXUuZGs=.
Ethics Statement
The study protocol was approved by the Bioethics Committee and Data Protection Authorities of Denmark, Iceland, Norway and Sweden. The study participants provided their written informed consent to participate in this study.
Author Contributions
JM, BG, UL, LL, LE, MS, and LI contributed to the design and implementation of the research, to the analysis of the results, and to the writing of the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors thank all patients who participated in the study; Thomas Ternowitz, Department of Dermatology, Stavanger University Hospital, Norway, for collecting Norwegian data; Kerstin Berg, Karolinska Institutet, Stockholm, Sweden, for data handling; and finally, NORDPSO for their economic support of the Nordic PAM Study.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2021.629741/full#supplementary-material
References
1. Alinaghi F, Calov M, Kristensen LE, Gladman DD, Coates LC, Jullien D, et al. Prevalence of psoriatic arthritis in patients with psoriasis: a systematic review and meta-analysis of observational and clinical studies. J Am Acad Dermatol. (2019) 80:251–65.e19. doi: 10.1016/j.jaad.2018.06.027
2. Mease PJ, Gladman DD, Papp KA, Khraishi MM, Thaçi D, Behrens F, et al. Prevalence of rheumatologist-diagnosed psoriatic arthritis in patients with psoriasis in European/North American dermatology clinics. J Am Acad Dermatol. (2013) 69:729–35. doi: 10.1016/j.jaad.2013.07.023
3. Reich K, Krüger K, Mössner R, Augustin M. Epidemiology and clinical pattern of psoriatic arthritis in Germany: a prospective interdisciplinary epidemiological study of 1511 patients with plaque-type psoriasis. Br J Dermatol. (2009) 160:1040–7. doi: 10.1111/j.1365-2133.2008.09023.x
4. Gladman DD, Antoni C, Mease P, Clegg DO, Nash P. Psoriatic arthritis: epidemiology, clinical features, course, and outcome. Ann Rheum Dis. (2005) 64:ii14–7. doi: 10.1136/ard.2004.032482
5. Veale DJ, Fearon U. The pathogenesis of psoriatic arthritis. Lancet. (2018) 391:2273–84. doi: 10.1016/S0140-6736(18)30830-4
6. Moll JM, Wright V. Psoriatic arthritis. Semin Arthritis Rheum. (1973) 3:55–78. doi: 10.1016/0049-0172(73)90035-8
7. Love TJ, Gudbjornsson B, Gudjonsson JE, Valdimarsson H. Psoriatic arthritis in Reykjavik, Iceland: prevalence, demographics, and disease course. J Rheumatol. (2007) 34:2082–8.
8. Chandran V, Gladman DD, Helliwell PS, Gudbjörnsson B. Arthritis mutilans: a report from the GRAPPA 2012 annual meeting. J Rheumatol. (2013) 40:1419–22. doi: 10.3899/jrheum.130453
9. Jones SM, Armas JB, Cohen MG, Lovell CR, Evison G, McHugh NJ. Psoriatic arthritis: outcome of disease subsets and relationship of joint disease to nail and skin disease. Br J Rheumatol. (1994) 33:834–9. doi: 10.1093/rheumatology/33.9.834
10. Madland TM, Apalset EM, Johannessen AE, Rossebö B, Brun JG. Prevalence, disease manifestations, and treatment of psoriatic arthritis in Western Norway. J Rheumatol. (2005) 32:1918–22.
11. Nossent JC, Gran JT. Epidemiological and clinical characteristics of psoriatic arthritis in northern Norway. Scand J Rheumatol. (2009) 38:251–5. doi: 10.1080/03009740802609558
12. Torre Alonso JC, Rodriguez Perez A, Arribas Castrillo JM, Ballina Garcia J, Riestra Noriega JL, Lopez Larrea C. Psoriatic arthritis (PA): a clinical, immunological and radiological study of 180 patients. Br J Rheumatol. (1991) 30:245–50. doi: 10.1093/rheumatology/30.4.245
13. Veale D, Rogers S, Fitzgerald O. Classification of clinical subsets in psoriatic arthritis. Br J Rheumatol. (1994) 33:133–8. doi: 10.1093/rheumatology/33.2.133
14. Gudbjornsson B, Ejstrup L, Gran JT, Iversen L, Lindqvist U, Paimela L, et al. Psoriatic arthritis mutilans (PAM) in the Nordic countries: demographics and disease status. The Nordic PAM study. Scand J Rheumatol. (2013) 42:373–8. doi: 10.3109/03009742.2013.771211
15. Jadon DR, Shaddick G, Tillett W, Korendowych E, Robinson G, Waldron N, et al. Psoriatic arthritis mutilans: characteristics and natural radiographic history. J Rheumatol. (2015) 42:1169–76. doi: 10.3899/jrheum.150083
16. Marsal S, Armadans-Gil L, Martínez M, Gallardo D, Ribera A, Lience E. Clinical, radiographic and HLA associations as markers for different patterns of psoriatic arthritis. Rheumatology (Oxford). (1999) 38:332–7. doi: 10.1093/rheumatology/38.4.332
17. Nikamo P, Gudbjornsson B, Laasonen L, Ejstrup L, Iversen L, Lindqvist U, et al. HLA-B*27 is significantly enriched in Nordic patients with psoriatic arthritis mutilans. Clin Exp Rheumatol. (2020). [Epub ahead of print].
18. Rodriguez-Moreno J, Bonet M, Del Blanco-Barnusell J, Castaño C, Clavaguera T, Mateo-Soria L, et al. Mutilating/resorptive arthritis. A study of 24 patients in a series of 360 patients with psoriatic arthritis. Reumatol Clin. (2013) 9:38–41. doi: 10.1016/j.reuma.2012.06.015
19. Tan YM, Østergaard M, Doyle A, Dalbeth N, Lobo M, Reeves Q, et al. MRI bone oedema scores are higher in the arthritis mutilans form of psoriatic arthritis and correlate with high radiographic scores for joint damage. Arthritis Res Ther. (2009) 11:R2. doi: 10.1186/ar2586
20. FitzGerald O, Haroon M, Giles JT, Winchester R. Concepts of pathogenesis in psoriatic arthritis: genotype determines clinical phenotype. Arthritis Res Ther. (2015) 17:115. doi: 10.1186/s13075-015-0640-3
21. Eder L, Chandran V, Cook R, Gladman DD. The risk of developing diabetes mellitus in patients with psoriatic arthritis: a cohort study. J Rheumatol. (2017) 44:286–91. doi: 10.3899/jrheum.160861
22. Ferguson LD, Siebert S, McInnes IB, Sattar N. Cardiometabolic comorbidities in RA and PsA: lessons learned and future directions. Nat Rev Rheumatol. (2019) 15:461–74. doi: 10.1038/s41584-019-0256-0
23. Castañeda S, Martín-Martínez MA, González-Juanatey C, Llorca J, García-Yébenes MJ, Pérez-Vicente S, et al. Cardiovascular morbidity and associated risk factors in Spanish patients with chronic inflammatory rheumatic diseases attending rheumatology clinics: baseline data of the CARMA Project. Semin Arthritis Rheum. (2015) 44:618–26. doi: 10.1016/j.semarthrit.2014.12.002
24. Armstrong EJ, Krueger JG. Lipoprotein metabolism and inflammation in patients with psoriasis. Am J Cardiol. (2016) 118:603–9. doi: 10.1016/j.amjcard.2016.05.060
25. Hot A, Lenief V, Miossec P. Combination of IL-17 and TNFalpha induces a pro-inflammatory, pro-coagulant and pro-thrombotic phenotype in human endothelial cells. Ann Rheum Dis. (2012) 71:768–76. doi: 10.1136/annrheumdis-2011-200468
26. Koo J, Marangell LB, Nakamura M, Armstrong A, Jeon C, Bhutani T, et al. Depression and suicidality in psoriasis: review of the literature including the cytokine theory of depression. J Eur Acad Dermatol Venereol. (2017) 31:1999–2009. doi: 10.1111/jdv.14460
27. McDonough E, Ayearst R, Eder L, Chandran V, Rosen CF, Thavaneswaran A, et al. Depression and anxiety in psoriatic disease: prevalence and associated factors. J Rheumatol. (2014) 41:887–96. doi: 10.3899/jrheum.130797
28. Tekin HG, Wu JJ, Burge R, Birt J, Egeberg A. Burden and disease characteristics of patients with psoriatic arthritis: a population-based cross-sectional study. J Rheumatol. (2019) 46:716–20. doi: 10.3899/jrheum.180670
29. Bernstein CN, Wajda A, Blanchard JF. The clustering of other chronic inflammatory diseases in inflammatory bowel disease: a population-based study. Gastroenterology. (2005) 129:827–36. doi: 10.1053/j.gastro.2005.06.021
30. Cohen AD, Dreiher J, Birkenfeld S. Psoriasis associated with ulcerative colitis and Crohn's disease. J Eur Acad Dermatol Venereol. (2009) 23:561–5. doi: 10.1111/j.1468-3083.2008.03031.x
31. Gergianaki I, Tsiligianni I. Chronic obstructive pulmonary disease and rheumatic diseases: a systematic review on a neglected comorbidity. J Comorb. (2019) 9:2235042x18820209. doi: 10.1177/2235042X18820209
32. Li WQ, Han JL, Chan AT, Qureshi AA. Psoriasis, psoriatic arthritis and increased risk of incident Crohn's disease in US women. Ann Rheum Dis. (2013) 72:1200–5. doi: 10.1136/annrheumdis-2012-202143
33. Lindqvist U, Gudbjornsson B, Iversen L, Laasonen L, Ejstrup L, Ternowitz T, et al. Disease activity in and quality of life of patients with psoriatic arthritis mutilans: the Nordic PAM Study. Scand J Rheumatol. (2017) 46:454–60. doi: 10.1080/03009742.2017.1278787
34. Laasonen L, Gudbjornsson B, Ejstrup L, Iversen L, Ternowitz T, Ståhle M, et al. Radiographic development during three decades in a patient with psoriatic arthritis mutilans. Acta Radiol Open. (2015) 4:2058460115588098. doi: 10.1177/2058460115588098
35. Laasonen L, Lindqvist U, Iversen L, Ejstrup L, Jonmundsson T, Ståhle M, et al. Radiographic scoring systems for psoriatic arthritis are insufficient for psoriatic arthritis mutilans: results from the Nordic PAM Study. Acta Radiol Open. (2020) 9:2058460120920797. doi: 10.1177/2058460120920797
36. Baviere W, Deprez X, Houvenagel E, Philippe P, Deken V, Flipo RM, et al. Association between comorbidities and quality of life in psoriatic arthritis: results from a multicentric cross-sectional study. J Rheumatol. (2020) 47:369–76. doi: 10.3899/jrheum.181471
37. Sinnathurai P, Buchbinder R, Hill C, Lassere M, March L. Comorbidity in psoriatic arthritis and rheumatoid arthritis. Intern Med J. (2018) 48:1360–8. doi: 10.1111/imj.14046
38. Fernández-Carballido C, Martín-Martínez MA, García-Gómez C, Castañeda S, González-Juanatey C, Sánchez-Alonso F, et al. Impact of comorbidity on physical function in patients with ankylosing spondylitis and psoriatic arthritis attending rheumatology clinics: results from a cross-sectional study. Arthritis Care Res (Hoboken). (2020) 72:822–8. doi: 10.1002/acr.23910
39. Haroon M, Gallagher P, Heffernan E, FitzGerald O. High prevalence of metabolic syndrome and of insulin resistance in psoriatic arthritis is associated with the severity of underlying disease. J Rheumatol. (2014) 41:1357–65. doi: 10.3899/jrheum.140021
40. Haroon M, Rafiq Chaudhry AB, Fitzgerald O. Higher prevalence of metabolic syndrome in patients with psoriatic arthritis: a comparison with a control group of noninflammatory rheumatologic conditions. J Rheumatol. (2016) 43:463–4. doi: 10.3899/jrheum.150757
41. Mease PJ, Etzel CJ, Huster WJ, Muram TM, Armstrong AW, Lisse JR, et al. Understanding the association between skin involvement and joint activity in patients with psoriatic arthritis: experience from the Corrona Registry. RMD Open. (2019) 5:e000867. doi: 10.1136/rmdopen-2018-000867
Keywords: psoriasis, arthritis, mutilans, comorbidity, multinational study
Citation: Mistegård J, Gudbjornsson B, Lindqvist U, Laasonen L, Ejstrup L, Ståhle M and Iversen L (2021) Comorbidities in a Cohort of 66 Patients With Psoriatic Arthritis Mutilans—Results From the Nordic PAM Study. Front. Med. 8:629741. doi: 10.3389/fmed.2021.629741
Received: 17 November 2020; Accepted: 12 January 2021;
Published: 04 February 2021.
Edited by:
George Bertsias, University of Crete, GreeceReviewed by:
Santos Castañeda, Hospital de La Princesa, SpainWarren Fong, Singapore General Hospital, Singapore
Copyright © 2021 Mistegård, Gudbjornsson, Lindqvist, Laasonen, Ejstrup, Ståhle and Iversen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lars Iversen, bGFycy5pdmVyc2VuQGNsaW4uYXUuZGs=