 Rebecca Hasseli1,2†
Rebecca Hasseli1,2† Frank Hanses3†Melanie Stecher4Christof Specker5
Frank Hanses3†Melanie Stecher4Christof Specker5 Tobias Weise6
Tobias Weise6 Stefan Borgmann7Martina Hasselberger8Bernd Hertenstein9Martin Hower10Bimba F. Hoyer11Carolin Koll4Andreas Krause12Marie von Lilienfeld-Toal13
Stefan Borgmann7Martina Hasselberger8Bernd Hertenstein9Martin Hower10Bimba F. Hoyer11Carolin Koll4Andreas Krause12Marie von Lilienfeld-Toal13 Hanns-Martin Lorenz14
Hanns-Martin Lorenz14 Uta Merle15Susana M. Nunes de Miranda16
Uta Merle15Susana M. Nunes de Miranda16 Mathias W. Pletz17Anne C. Regierer18Jutta G. Richter19,20Siegbert Rieg21Christoph Roemmele22Maria M. Ruethrich13Tim Schmeiser23
Mathias W. Pletz17Anne C. Regierer18Jutta G. Richter19,20Siegbert Rieg21Christoph Roemmele22Maria M. Ruethrich13Tim Schmeiser23 Hendrik Schulze-Koops24Anja Strangfeld18
Hendrik Schulze-Koops24Anja Strangfeld18 Maria J.G.T. Vehreschild25Florian Voit26
Maria J.G.T. Vehreschild25Florian Voit26 Reinhard E. Voll27Jörg Janne Vehreschild4,28
Reinhard E. Voll27Jörg Janne Vehreschild4,28 Ulf Müller-Ladner2*
Ulf Müller-Ladner2* Alexander Pfeil29*
Alexander Pfeil29*- 1Section of Rheumatology and Clinical Immunology, Department of Internal Medicine D, University Hospital Münster, Münster, Germany
- 2Department of Rheumatology and Clinical Immunology, Justus-Liebig University Giessen, Giessen, Germany
- 3Emergency Department and Department for Infectious Diseases and Infection Control, University Hospital Regensburg, Regensburg, Germany
- 4Department I of Internal Medicine, University of Cologne, Faculty of Medicine and University Hospital Cologne, Cologne, Germany
- 5Department of Rheumatology and Clinical Immunology, KEM Kliniken Essen-Mitte, Essen, Germany
- 6Biocontrol Jena, Jena, Germany
- 7Department of Infectious Diseases and Infection Control, Ingolstadt Hospital, Ingolstadt, Germany
- 8Klinikum Passau, Passau, Germany
- 9Klinikum Bremen-Mitte, Bremen, Germany
- 10Department of Pneumology, Infectious Diseases, Internal Medicine and Intensive Care, Klinikum Dortmund GmbH, Dortmund, Germany
- 11Department for Rheumatology and Clinical Immunology, University of Schleswig-Holstein, Kiel, Germany
- 12Department of Rheumatology, Clinical Immunology and Osteology, Immanuel Hospital Berlin, Berlin, Germany
- 13Department of Hematology and Medical Oncology, University Hospital Jena, Jena, Germany
- 14Department of Internal Medicine V, University of Heidelberg, Heidelberg, Germany
- 15Department of Gastroenterology and Infectious Diseases, Heidelberg University Hospital, Heidelberg, Germany
- 16Department of Medicine II, University of Freiburg, Freiburg, Germany
- 17Institute for Infectious Diseases and Infection Control, Jena University Hospital, Jena, Germany
- 18Epidemiology Unit, German Rheumatism Research Center Berlin, Berlin, Germany
- 19Department of Rheumatology, University Hospital Düsseldorf, Medical Faculty of Heinrich-Heine-University, Düsseldorf, Germany
- 20Hiller Research Center, University Hospital Düsseldorf, Medical Faculty of Heinrich-Heine-University, Düsseldorf, Germany
- 21Division of Infectious Diseases, Department of Medicine II, University of Freiburg, Freiburg, Germany
- 22Department of Gastroenterology, Faculty of Medicine, University of Augsburg, Augsburg, Germany
- 23Private Practice, Cologne, Germany
- 24Division of Rheumatology and Clinical Immunology, Department of Internal Medicine IV, University of Munich, Munich, Germany
- 25Department of Internal Medicine, Infectious Diseases, University Hospital Frankfurt, Goethe University Frankfurt, Frankfurt am Main, Germany
- 26Department of Internal Medicine II, School of Medicine, University Hospital Rechts Der Isar, Technical University of Munich, Munich, Germany
- 27Department of Rheumatology and Clinical Immunology, Faculty of Medicine, Medical Center-University of Freiburg, University of Freiburg, Freiburg, Germany
- 28Department II of Internal Medicine, Hematology/Oncology, Goethe University, Frankfurt, Germany
- 29Department of Internal Medicine III, University Hospital Jena, Jena, Germany
Objectives: To investigate, whether inflammatory rheumatic diseases (IRD) inpatients are at higher risk to develop a severe course of SARS-CoV-2 infections compared to the general population, data from the German COVID-19 registry for IRD patients and data from the Lean European Survey on SARS-CoV-2 (LEOSS) infected patients covering inpatients from the general population with SARS-CoV-2 infections were compared.
Methods: 4310 (LEOSS registry) and 1139 cases (IRD registry) were collected in general. Data were matched for age and gender. From both registries, 732 matched inpatients (LEOSS registry: n = 366 and IRD registry: n = 366) were included for analyses in total.
Results: Regarding the COVID-19 associated lethality, no significant difference between both registries was observed. Age > 65°years, chronic obstructive pulmonary disease, diabetes mellitus, rheumatoid arthritis, spondyloarthritis and the use of rituximab were associated with more severe courses of COVID-19. Female gender and the use of tumor necrosis factor-alpha inhibitors (TNF-I) were associated with a better outcome of COVID-19.
Conclusion: Inflammatory rheumatic diseases (IRD) patients have the same risk factors for severe COVID-19 regarding comorbidities compared to the general population without any immune-mediated disease or immunomodulation. The use of rituximab was associated with an increased risk for severe COVID-19. On the other hand, the use of TNF-I was associated with less severe COVID-19 compared to the general population, which might indicate a protective effect of TNF-I against severe COVID-19 disease.
Highlights:
• The risk of infection with SARS-CoV-2 might be higher in patients with inflammatory rheumatic disease compared to the general population.
• The data of two German nationwide registries revealed no increased COVID-19 associated lethality in inflammatory rheumatic diseases.
• The use of tumor necrosis factor-alpha inhibitors was associated with a better outcome of severe COVID-19 disease (odds ratio of 0.5; 95% CI 0.2 to 0.9).
Introduction
In December 2019, the first cases of patients with unexplained pneumonia were reported in Wuhan, China (1), which was identified in January 2020 as an infection with SARS-CoV-2. At the same time, first cases of COVID-19 were reported in Germany (2). Since March 2020, a global pandemic SARS-CoV-2 has been declared (2). The highest fatality rate was observed in elderly and multi-morbid persons (3). Patients with autoimmune disease were expected to harbour an increased risk for severe COVID-19, especially under the treatment with glucocorticoids (4, 5). In addition, disease activity of inflammatory rheumatic diseases (IRD) was associated with more severe COVID-19 compared to patients with sustained remission (6). Further, IRD patients under treatment with rituximab revealed a poor outcome of COVID-19 (6–9). For some patient groups (e.g., patients with oncological morbidities), a worse outcome of COVID-19 has been described compared to non-pre-diseased patients (10). Some data suggested an increased risk for IRD-patients to develop severe COVID-19, such as COVID-19 related pneumonia, compared to the general population (11, 12). Especially in patients with rheumatoid arthritis and systemic vasculitis, a higher risk for severe COVID-19 could be observed (12).
As disease activity of IRD plays a crucial role regarding COVID-19, severity and different healthcare systems might have an influence on this aspect. The aim of this study was to investigate whether inpatients with IRD are at higher risk to poor outcomes of COVID-19 compared to the general population in Germany. In addition, the question was whether IRD could be considered as a comorbidity increasing the risk for severe COVID-19 and if so, whether specific types of disease-modifying antirheumatic drugs (DMARD) were contributing factors.
Materials and methods
Data from the German COVID-19 registry for patients with IRD1 and data from the Lean European Open Survey on SARS-CoV-2 infected patients (LEOSS registry)2 obtained between March 2020 until January 2021 were analysed. Patients with IRD and SARS-CoV-2 infection were included in the ongoing IRD registry by their rheumatologists (13). The LEOSS cohort includes cases of SARS-CoV-2 infections in the general German population (14). Here data were entered by treating physicians, study nurses and other medical staff. In both registries, participating centres included both academic and non-academic clinics throughout Germany.
Data and missing values of patients with immune-mediated inflammatory diseases, cancer, a history of cancer, organ transplantation or immunomodulatory/immunosuppressive treatment (including glucocorticoids) were excluded for further analyses from both cohorts due to the known poorer outcomes of patients with SARS-CoV-2 infection (details see Figure 1). As in LEOSS, mainly COVID-19 inpatients were reported, our analysis focussed on COVID-19 inpatients only from both registries.
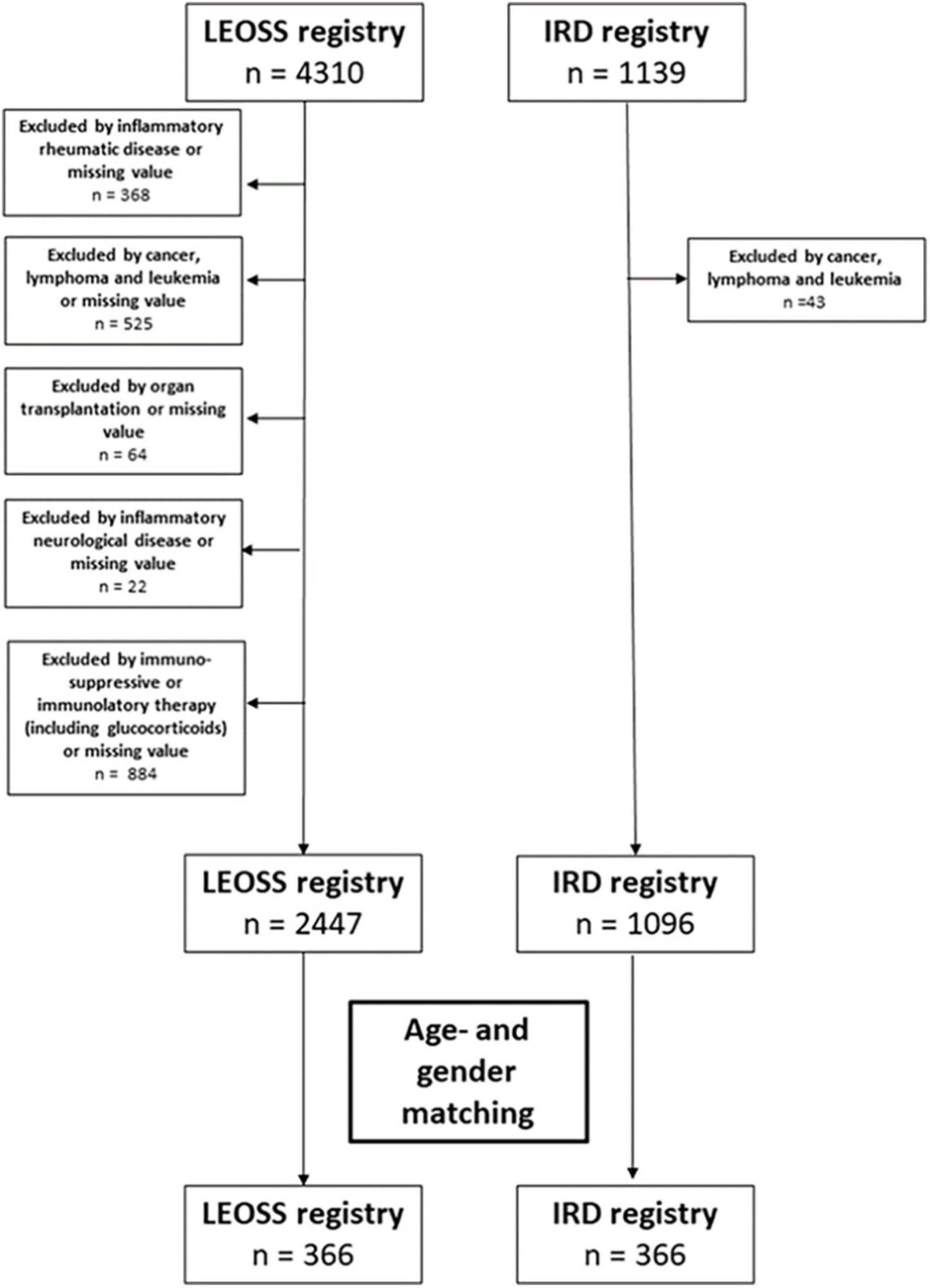
Figure 1. Flowchart regarding the excluded patients or missing value for matching of the patients from both registries.
For comparison, age-matching and gender-matching were used, as these two variables have been shown to strongly impact on the course of COVID-19. For age and gender a 1:1 matching was performed.
Statistical analyses
Completed cases were reviewed and queried in case of missing or inconsistent data. Statistical computations were performed using the programming language Python (version 3.10.0) and the additional packages numpy (version 1.22.3), pandas (version 1.4.1), scipy (version 1.8.0), scikit-learn (version 1.1.2), statsmodels (version 0.13.2), matplotlib (version 3.5.1), and seaborn (version 0.11.2). The use of the individual packages is structured as follows: performing basic numerical operations (numpy), processing of tabular data (pandas), testing group differences between both registries (scipy), ordinal logistic regression modeling (statsmodels), multiple imputation of missing values (sklearn) and data visualisation (matplotlib, seaborn).
The respective statistical significance level of group differences between both registries (see Tables 1(5) were calculated using the Mann-Whitney U test (scipy.stats.mannwhitneyu) for continuous variables as well as the Chi-Square test (scipy.stats.chi2_contingency) for categorical variables. P-values <0.05 were considered significant.
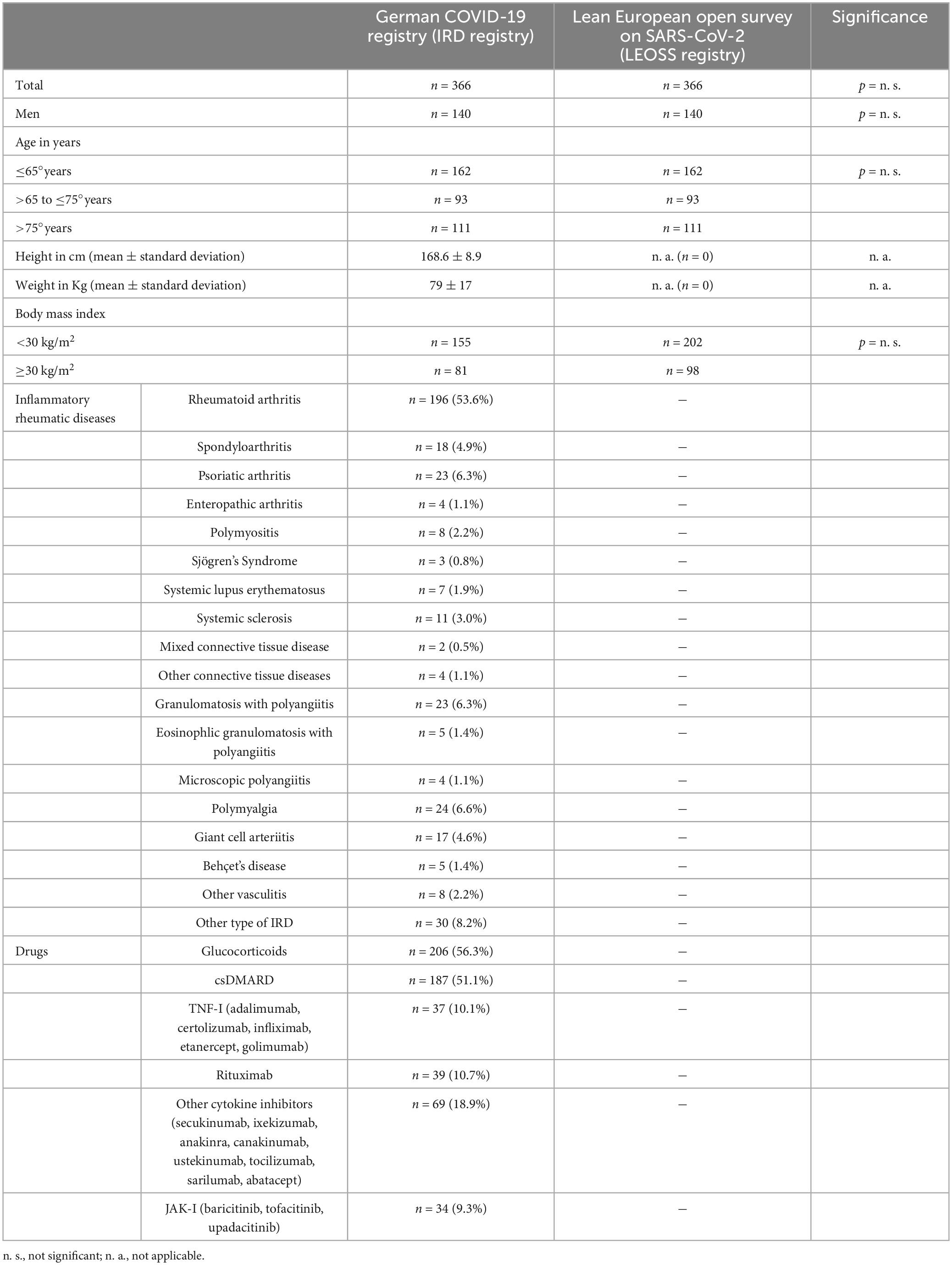
Table 1. Baseline characterisitca (n. s., not significant; n. a., not applicable).
Ordinal logistic regression analyses
Within the ordinal logistic regressions (statsmodels.miscmodels.ordinal_model.OrderedModel) the COVID-19 severity status was used as the outcome of interest. The COVID-19 severity status was defined using ascending levels: (0) hospitalisation, (1) oxygen administration/non-invasive ventilation and (2) invasive ventilation / extracorporal membrane oxygenation (ECMO) / death. The escalation in COVID-19 severity is assumed to be equidistant between the levels.
The independent variable “rheumatic disease activity” exhibited a small number of missing values (n = 27), which were derived by multiple imputation (sklearn.impute.KNNImputer) (15). The independent variable body mass index “BMI” was not considered in multivariate ordinal logistic regression due to high number of missing values (n = 196) in both registries. Multicollinearity between the independent variables was quantified using variance inflation factors (statsmodels.stats.outliers_influence.variance_inflation_factor). All independent variables (n = 23) considered in multiple ordinal logistic regression exhibited variance inflation factors <5 (16).
Due to the low prevalence of individual rheumatological diagnoses, selected diagnoses were combined into groups: “Sjögren’s Syndrome,” “Systemic Lupus Erythematosus,” “Systemic Sclerosis,” “Mixed Connective Tissue Disease,” “Polymyositis,” and “Other Connective Tissue diseases” were combined to the “Connective Tissue Diseases (CTD).” “Granulomatosis with Polyangiitis,” “Eosinophilic Granulomatosis with Polyangiitis,” “Microscopic Polyangiitis,” “Giant Cell Arteriitis,” “Polymyalgia Rheumatica,” “Behçet’s Disease,” and “Other Vasculitis” were combined to the “Vasculitides.” “Ankylosing spondylitis,” “Psoriatic arthritis” and “Enteropathic arthritis” were combined to “Spondyloarthritis” (SpA). RA represents the largest group within rheumatologic diagnoses and was included as a separate individual group in the analysis.
Univariate ordinal logistic regression was used to assess the individual association between the COVID-19 severity outcome (dependent variable) and the respective independent variable (Figure 1A). Multivariate ordinal logistic regression was used to assess the independent associations between the COVID-19 severity outcome and all independent variables (n = 23) considered in the analysis (Figure 1B). Results were reported as odd ratios (OR) including their respective 95% confidence intervals (CI). P-values were reported to describe the significance of the respective independent variable’s influence on the COVID-19 severity outcome. P-values <0.05 were considered significant (marked bold and colored blue, see Figure 2).
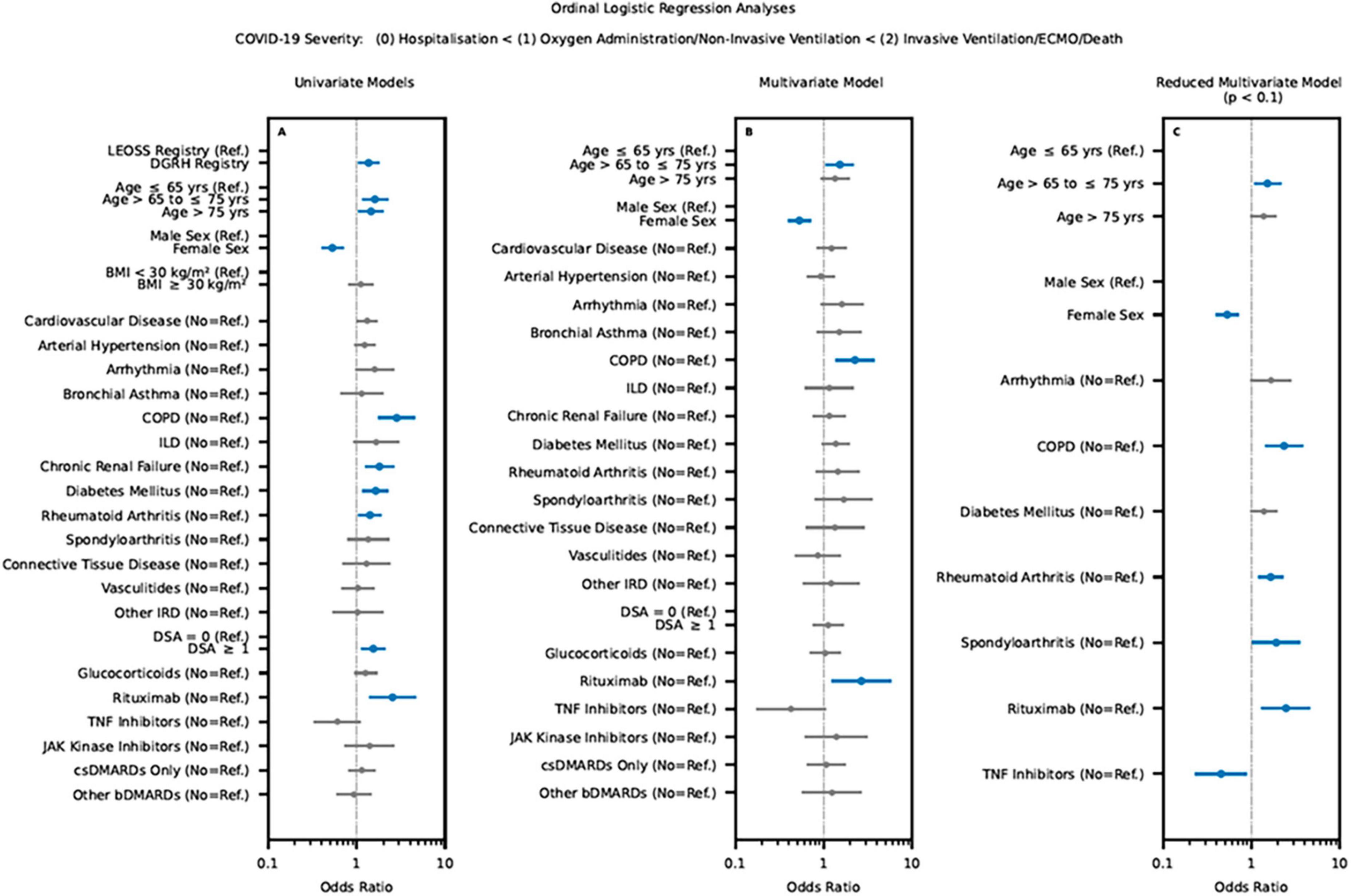
Figure 2. Results of the univariate (A) and multivariate regression analysis (B,C) for the verification of comorbidities, IRD and rheumatic treatment on the outcome of COVID-19 infection based on the LEOSS Registry and IRD registry. Significant independent variable’s influence (p-values <0.05) on the COVID-19 severity outcome marked bold and colored blue. (LEOSS Registry, Lean European Open Survey on SARS-CoV-2; BMI, body mass index; COPD, chronic obstructive pulmonary disease; ILD, interstitial lung disease; IRD, inflammatory rheumatic diseases; DSA, disease activity; bDMARD biological disease-modifying antirheumatic drugs, csDMARD, conventional synthetic disease-modifying antirheumatic drug; TNF Inhibitors, tumor necrosis factor-alpha inhibitors).
In order to reduce model complexity, the obtained multivariate ordinal logistic regression model was iteratively reduced by pruning the independent variable exhibiting lowest significance and re-evaluating the reduced model. This backward elimination procedure was repeated until all remaining independent variables exhibited p-values <0.1. This threshold was set to retain potentially confounding variables with a strong influence on the model. Only p-values <0.05 were considered significant (marked bold and colored blue, see Figure 2).
Results
Baseline characteristics
From March 2020 to January 2021, 4310 cases (LEOSS registry) and 1139 cases (IRD registry) of SARS-COV-2 infection were reported. After performing the exclusion criteria and focusing on COVID-19 inpatients, matched pairs by age and gender were developed, consequently 732 patients (LEOSS registry: n = 366 and IRD registry: n = 366) were subsequently available for analysis.
In the IRD registry, (196/366, 53.6%) of the patients were diagnosed with rheumatoid arthritis, followed by psoriatic arthritis (23/366, 6.3%) and SpA (18/366, 4.9%). The use of glucocorticoids was reported in 206/366 (56.3%) of IRD patients, 51.1% (187/366) were treated with conventional synthetic (cs) DMARDs, 10.1% (37/366) with Tumor Necrosis Factor-alpha Inhibitors (TNF-I), 10.7% (39/366) with rituximab, 18.9% (69/366) with other cytokine inhibitors, and 9.3% (34/366) with Janus kinase inhibitors (JAK-I). At time of SARS-CoV-2 infection, 7.0% (25/366) of IRD patients did not receive any immunomodulatory therapy (see Table 1).
Comorbidities
Arterial hypertension was the most common comorbidity in both registries (IRD registry: 53.8% vs. LEOSS: 54.4%). Regarding other cardiovascular diseases and arrhythmia, significantly more patients were reported in LEOSS as compared to the IRD registry (cardiovascular diseases: 60.4 vs. 26.8%, arrhythmia: 13.7 vs. 2.5%, p < 0.001). The IRD registry revealed significantly more patients with chronic kidney disease (20.8% vs. 13.4%; p < 0.05), pulmonary arterial hypertension (3.8% vs. 0.3%; p < 0.01), and interstitial lung disease (7.9% vs. 3.6%, p < 0.05). Concerning bronchial asthma, chronic obstructive pulmonary disease, liver cirrhosis, the use of alcohol and active smoking, no significant differences between the registries were observed (see Table 2).
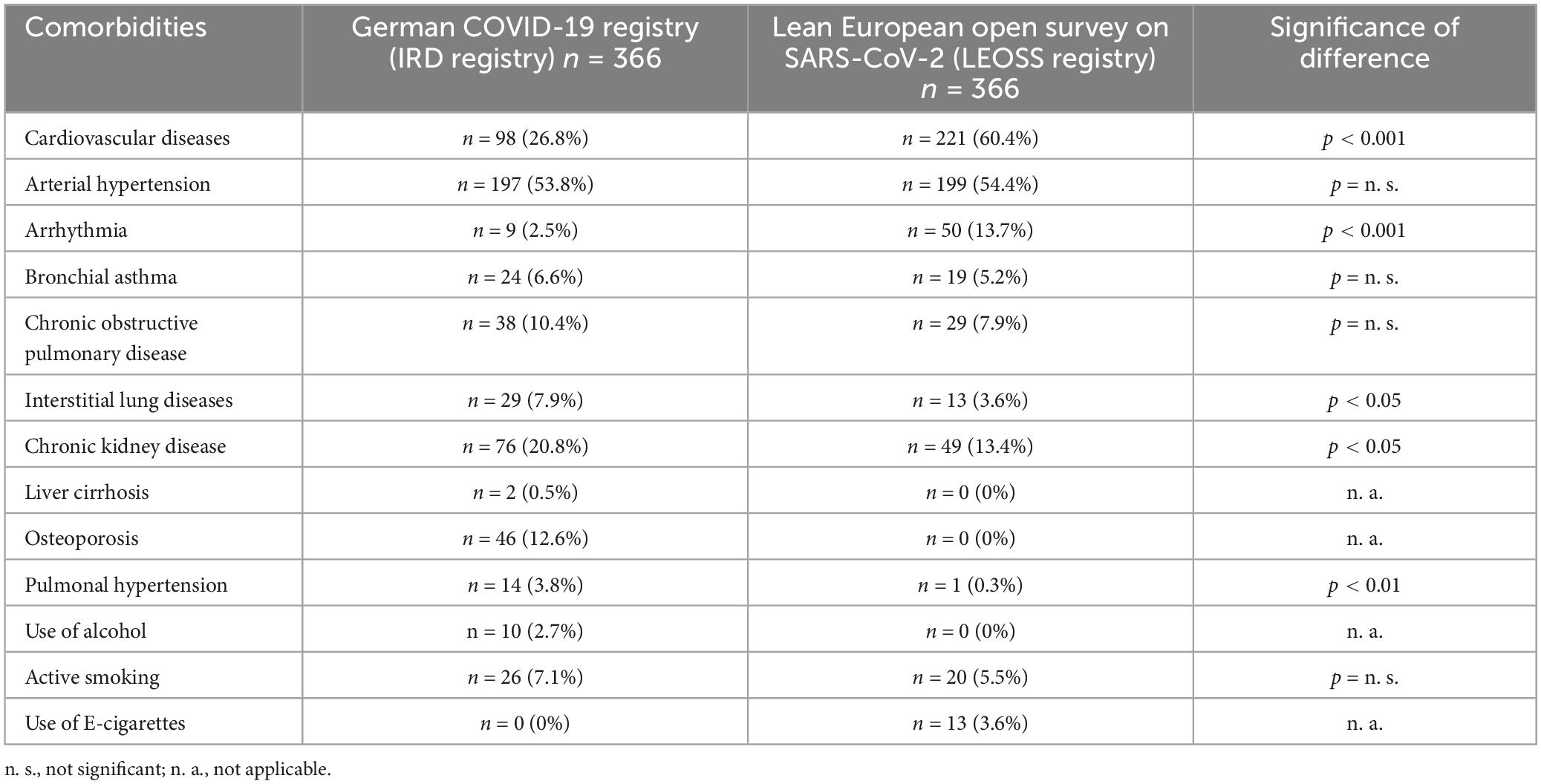
Table 2. Comorbidities.
COVID-19 related symptoms
In IRD patients, significantly more COVID-19 related symptoms were reported compared to the general population (Table 3). Most commonly were fever (IRD registry 70.2%, LEOSS registry 38.8%; p < 0.001), cough (IRD registry 62.3%, LEOSS registry 39.6%; p < 0.001), dyspnoea (IRD registry 55.2%, LEOSS registry 30.6%; p < 0.001), myalgia (IRD registry 27.9%, LEOSS registry 7.9%; p < 0.001), loss of appetite (IRD registry 24.6%, LEOSS registry 6.3%; p < 0.001), dysgeusia (IRD registry 19.9%, LEOSS registry 6.6%; p < 0.001), headache (IRD registry 18.0%, LEOSS registry 9.3%; p < 0.001), diarrhoea (IRD registry 15.8%, LEOSS registry 9.6%; p < 0.05), and anosmia (IRD registry 15.6%, LEOSS registry 4.9%; p < 0.001) (see Table 3).
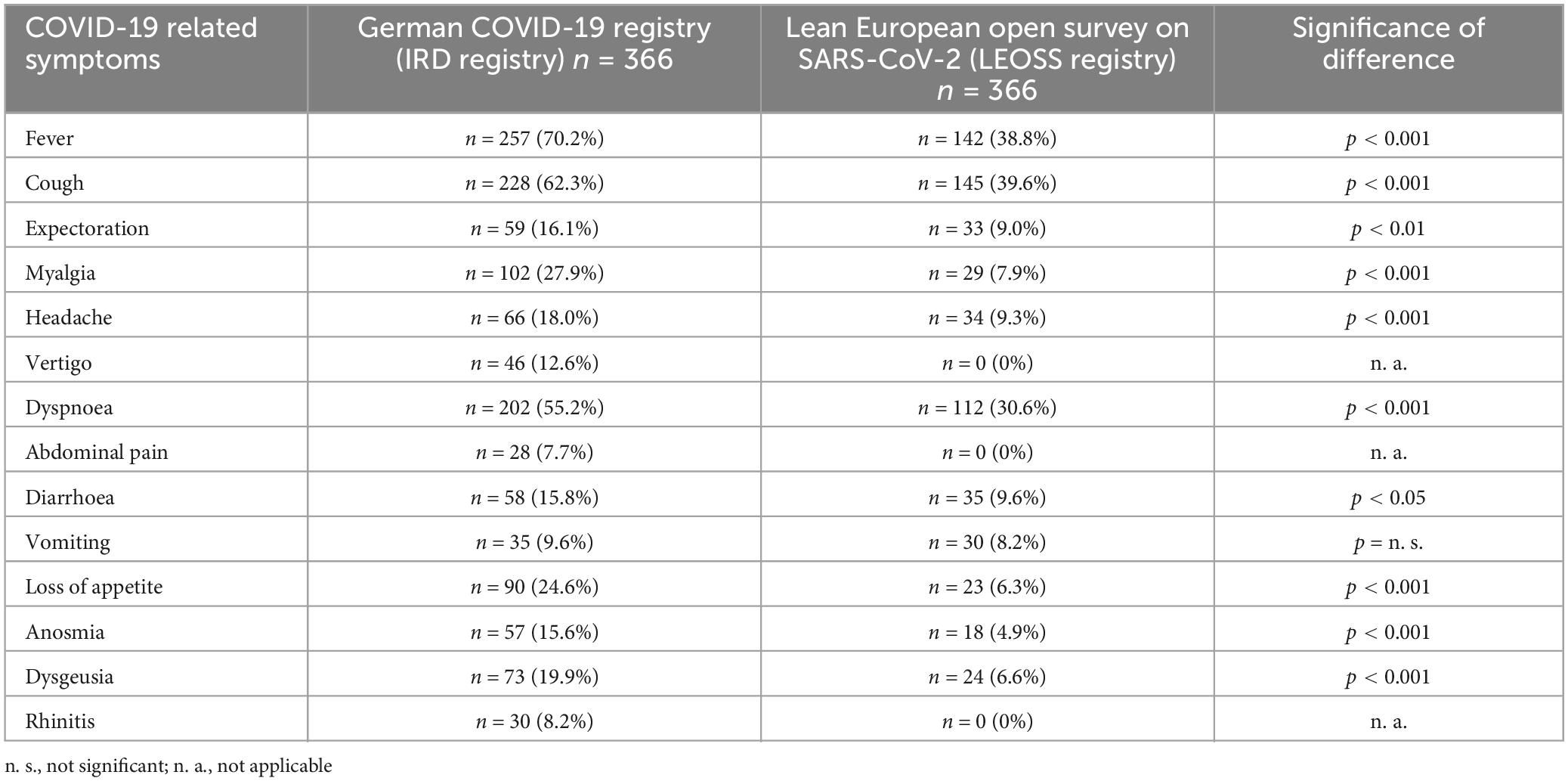
Table 3. Symptoms of COVID-19-infection.
COVID-19 related complications
The following complications were documented in the IRD registry: 16.9% concomitant infection, 13.7% acute respiratory distress syndrome and 9.0% sepsis. In the LEOSS registry, primarily concomitant infections (14.8%) were reported (see Table 4).
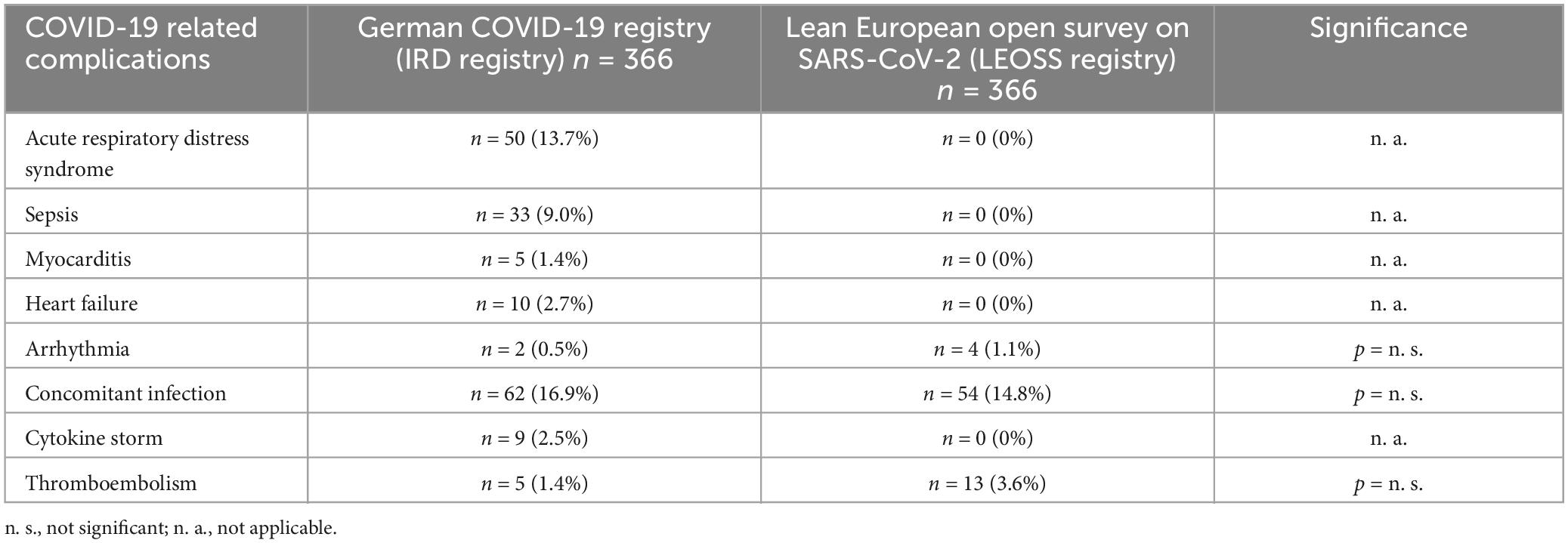
Table 4. Complications of COVID-19-infection.
COVID-19 related lethality
Regarding COVID-19 related lethality, no significant difference could be observed in both registries (IRD registry 16.9%, LEOSS registry 15.0%; p = n.s., Table 5). Oxygen administration and non-invasive ventilation (NIV) were reported significantly (p < 0.001) more frequent in IRD patients (oxygen administration 72.1% and NIV 11.5%) compared to data of the LEOSS registry (oxygen administration 51.6% and NIV 1.1%). Concerning invasive ventilation (IRD registry 18.3%; LEOSS registry 15.3%; p = n.s.) and ECMO (each 3.8%), no significant differences were found (see Table 5).
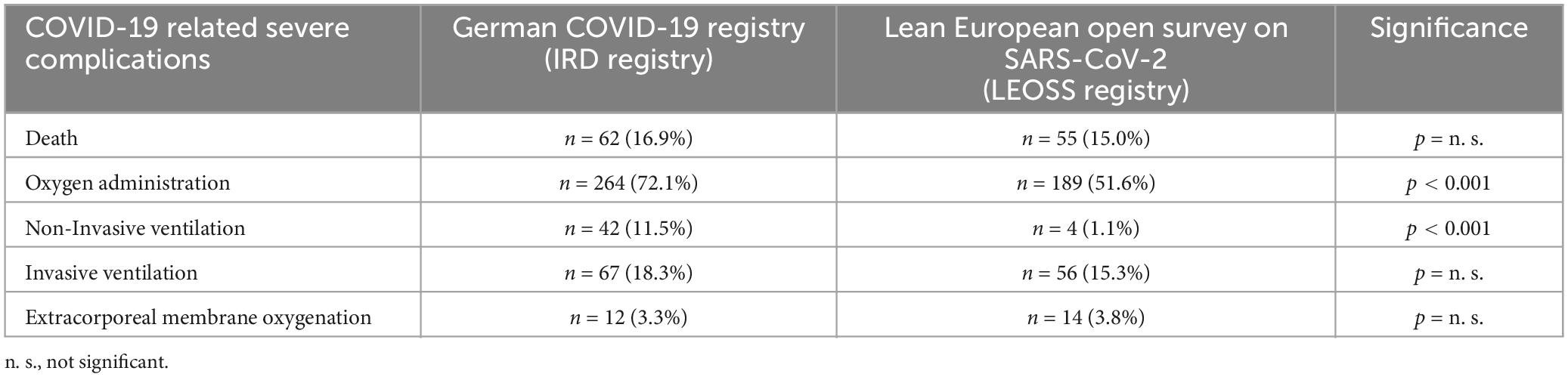
Table 5. COVID-19 related severe complications.
COVID-19 outcome analysis
In the univariate ordinal logistic regression, age > 65°years [odds ratio (OR) of 1.6, 95% confidence interval (CI) 1.1 to 2.2], cardiovascular disease (OR of 1.3; 95% CI 1.0 to 1.7), arrhythmia (OR of 1.6; 95% CI 1.0 to 2.6), chronic obstructive pulmonary disease (OR of 2.8; 95% CI 1.7 to 4.6), chronic renal failure (OR of 1.8; 95% CI 1.2 to 2.6), diabetes mellitus (OR of 1.6; 95% CI 1.2 to 2.3) and rituximab (OR of 2.5; 95% CI 1.4 to 4.7) were significantly associated with severe COVID-19. Female patients (OR of 0.5; 95% CI 0.4 to 0.7) showed a significant lower risk for severe COVID-19 compared to males. Regarding arterial hypertension, bronchial asthma, interstitial lung diseases, active smoking, type of IRD, IRD disease activity, use of glucocorticoids, TNF-I, JAK-I, csDMARDs (monotherapy), and other cytokine inhibitors [biological (b) DMARD], no significant association to COVID-19 severity could be identified (see Figure 2A). Compared to sustained remission/low disease activity, moderate/high disease activity was associated with an increased risk for poor COVID-19 outcome (OR of 1.6; 95% 1.2 to 2.1).
Multivariate ordinal logistic regression (excluding body mass index) revealed a significant increased risk for severe COVID-19 in older patients (age > 65 years: OR of 1.5, 95% CI 1.1 to 2.2), patients with chronic obstructive pulmonary disease (OR of 2.3; 95% CI 1.4 to 3.7) or patients treated with rituximab (OR of 2.6; 95% CI 1.3 to 5.1) (see Figure 2B). On the other hand, female gender was associated with lower risk for severe COVID-19 (OR of 0.5; 95% CI 0.4 to 0.7). Although univariate logistic regression model showed an increased association with severe COVID-19 in the case of moderate/high disease activity, this was not statistically confirmed in the multivariate ordinal logistic regression (OR of 1.1, 95% CI 0.8 to 1.7).
Regarding obtained multivariate ordinal logistic regression model after stepwise elimination, similar results could be detected regarding the impact of age (age > 65 years: OR of 1.5, 95% CI 1.1 to 2.1) and chronic obstructive pulmonary disease (OR of 2.3; 95% CI 1.4 to 3.8). In addition, further factors associated with severe COVID-19 were identified: chronic obstructive pulmonary disease (OR of 2.3; 95% CI 1.4 to 3.8), rheumatoid arthritis (OR of 1.6; 95% CI 1.2 to 2.3), SpA (OR of 1.9; 95% CI 1.0 to 3.5) and the use of rituximab (OR of 2.4; 95% CI 1.3 to 4.6). In contrast, female gender (OR of 0.5; 95% CI 0.4 to 0.7) and the use of TNF-I (OR of 0.5; 95% CI 0.2 to 0.9) were associated with a better outcome of COVID-19 inpatients (see Figure 2C).
COVID-19 outcome sub-analysis inflammatory rheumatic diseases
In the IRD registry, only cardiovascular disease (OR of 1.3; 95% CI 1.0 to 2.6), chronic obstructive pulmonary disease (OR of 4.9; 95% CI 2.5 to 9.7) and rituximab (OR of 2.4; 95% CI 1.3 to 4.6) were significantly associated with severe COVID-19 in the univariate ordinal logistic regression analysis. The use of TNF-I revealed a significant better COVID-19 outcome (OR of 0.5; 95% CI 0.2 to 0.9) (details see Figure 3A).
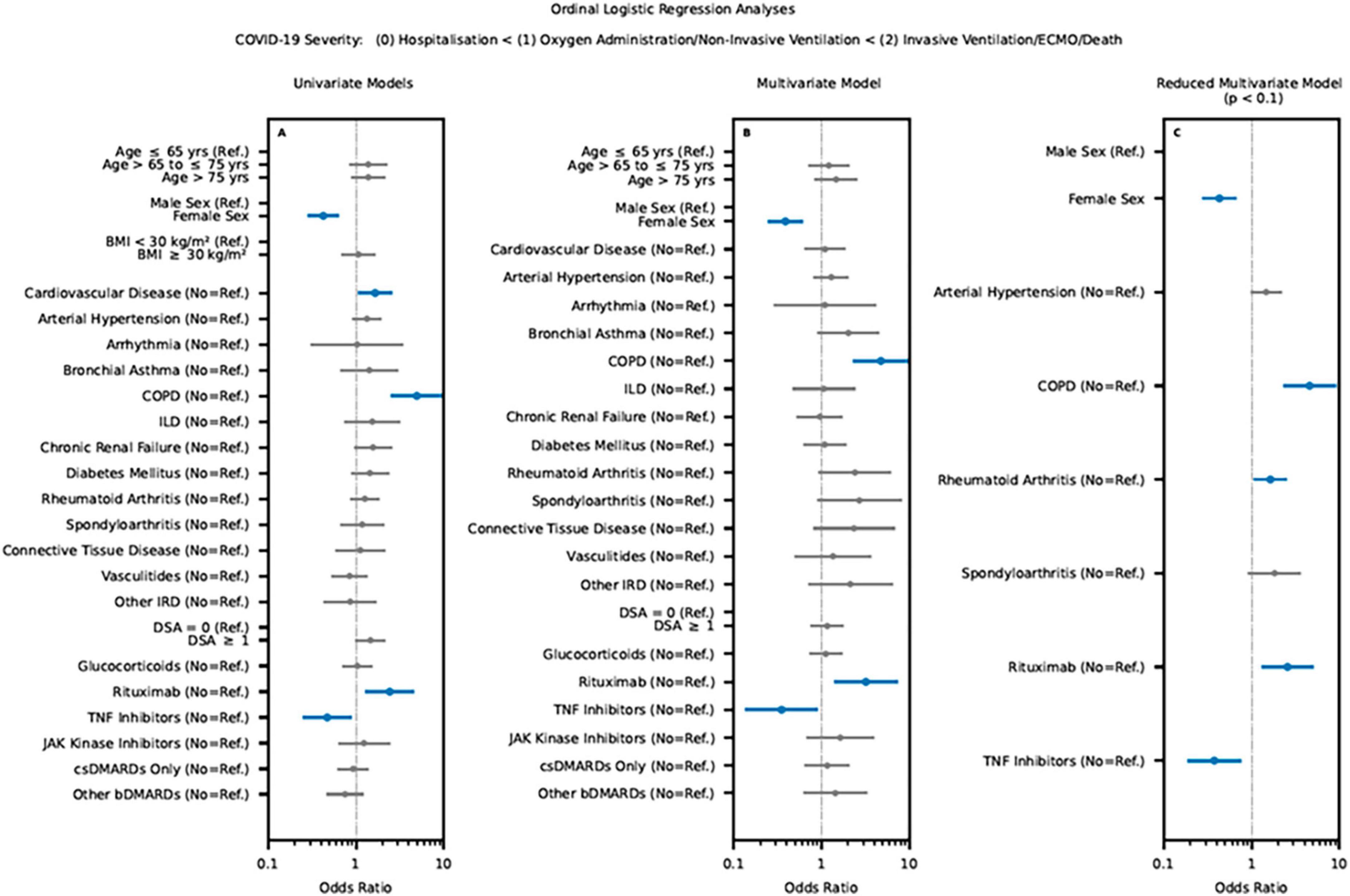
Figure 3. Results of the univariate (A) and multivariate regression (B,C) sub-analysis for the IRD cohort on the outcome of COVID-19 infection using the data of the IRD registry (significant variable were marked bold and colored blue. LEOSS Registry, Lean European Open Survey on SARS-CoV-2; BMI, body mass index; COPD, Chronic obstructive pulmonary disease; ILD, interstitial lung disease; IRD, inflammatory rheumatic diseases; DSA, disease activity; bDMARD, biological disease-modifying antirheumatic drugs; csDMARD, conventional synthetic disease-modifying antirheumatic drug; TNF inhibitors, tumor necrosis factor-alpha inhibitors).
An equivalent result was observed for the multivariate model (details see Figure 3B).
Regarding the reduced multivariate model chronic obstructive pulmonary disease (OR of 4.5; 95% CI 2.3 to 9.1), rheumatoid arthritis (OR of 1.6; 95% CI 1.1 to 2.5) and rituximab (OR of 2.6; 95% CI 1.3 to 5.0) showed a poor COVID-19 outcome. A better COVID-19 outcome was observed for female gender (OR of 0.4; 95% CI 0.3 to 0.7) and TNF-I (OR of 0.4; 95% CI 0.2 to 0.8) (see Figure 3C).
Discussion
The aim of this study was to evaluate whether IRD inpatients harbour a higher risk for a poor outcome of SARS-CoV-2 infections compared to the general population and to add evidence whether immunomodulatory treatment has an impact on the outcome of COVID-19.
For both registries, arterial hypertension was shown to be the most common comorbidity in patients with COVID-19 infection (IRD registry: 53.8% and LEOSS registry: 54.4%). A previous published study showed a lower rate of arterial hypertension (33%) in IRD-patients (4). In our study the comorbidity arterial hypertension had an association with hospitalization. Furthermore, 27.7% of non-hospitalized IRD patients had arterial hypertension compared to 43.6% of the hospitalized ones without invasive and 61.5% of the hospitalized ones with invasive ventilation. Additionally, it should be noted that chronic kidney disease or interstitial lung disease were more frequently detected as comorbidities in IRD patients. Both, chronic kidney disease (odds ratio 1.8) and interstitial lung disease (odds ratio 2.0) were associated with a worse outcome of COVID-19 as individual parameter, although no increased mortality was demonstrated for the IRD patients. Furthermore, 7.1% of patients in the IRD registry smoked compared to 5.5% of patients in the LEOSS registry. The prevalence of smoking in both registries is lower than the smoking prevalence in Germany (2019: 23.8%) (17). A similar result can be shown for the harmful use of alcohol (Germany 2019: 3.1%; IRD registry: 2.7% and LEOSS registry: 0%) (17).
Regarding symptoms of COVID-19, our IRD patients presented significantly more frequently with fever (IRD registry: 70.2% and LEOSS: 38.8%), respiratory symptoms including cough (IRD registry: 62.3% and LEOSS: 39.6%) and dyspnoea (IRD registry: 55.2% and LEOSS: 30.6%). These results are comparable to previously published data (4, 6).
For COVID-19 related death, no significant differences were observed in our cohorts, although IRD patients were significantly more frequently treated with oxygen administration (IRD registry: 72.1% and LEOSS: 51.6%) and non-invasive ventilation (IRD registry: 11.5% and LEOSS: 1.1%) compared to the LEOSS cohort.
This study confirmed known risk factors such as age, male gender in both cohorts. Regarding immunomodulatory therapies rituximab was a significant risk factor for a severe course and poor outcome of COVID-19 in IRD patients, whereas the use of TNF-I was associated with a significantly better outcome in IRD patients, even when compared to the general population without any immune-mediated disease or immunomodulatory treatment. This is an important finding of our analysis, as most of the studies investigating the impact of TNF-I were performed only in IRD patients without employing any comparison to the general population/control group (6, 18, 19). Although the mechanism of SARS-CoV-2 associated hyperinflammation is not fully understood, it is already known that increased TNF concentration in the serum is associated with COVID-19 related organ damage and worse outcome (20). Therefore, blocking of TNF might inhibit COVID-19 related organ damage. A case series already reported beneficial effects of TNF-I in the context of COVID-19 (21) and further studies are ongoing investigating the association of TNF-I and COVID-19 related outcome (22). Reports from the early phase of the pandemic from Wuhan (China) and Boston (USA) reported significant higher risk for severe COVID-19 in IRD patients compared to non-IRD patients, although there was no significant higher rate of death (23, 24). Our data are in accordance with these data, as the COVID-19 related lethality was similar in both registries.
Strengths and limitations
The strength of our study is the collaboration of two large nationwide registries. Compared to previous studies, data of our study derives from one country with patients treated within the same healthcare system. In addition, until December 2021 (the time period taken for this analysis) no COVID-19 vaccines were available, ruling out the influence of vaccination. To our knowledge, this is the largest study comparing IRD patients to the general population without any immune-mediated diseases, and without any immunomodulatory treatment with detailed clinical information. This allows proper estimation of the role or type of IRD and of immunomodulatory treatments in the context of COVID-19. As the data derived from a phase of the pandemic without any available antiviral treatment, there were no differences in specific COVID-19 treatments.
Limitations of this study include the risk of reporting bias because the registries used convenience sampling. However, our data are in accordance with previous published data, even analysis of health record network, suggesting that reporting bias was not a substantial bias of this study. Although the case report forms were similar, the data were not completely uniform. For example, comorbidities, pre-existing medication were recorded slightly differently across both registries. For this reason, no analysis of former medication was performed. Another limitation concerns the small number of patients who received specific types of immunomodulatory treatment, such as JAK-I. Only few patients with nicotine use were reported which might also be due to reporting bias. For this reason, no conclusion could be drawn regarding the effect of these immunomodulatory treatments and nicotine use in the context of COVID-19. As a further limitation, it should be pointed out, that the study covers the first two waves of the pandemic. SARS-CoV-2 variants and SARS-CoV-2 infection has been changed over time as well as in the clinical presentation of patients. Nevertheless, the study provides an insight into the disease process in patients with IRD and immunosuppressive/immunomodulatory therapy.
Conclusions
In conclusion, risk factors for increased severity of SARS-CoV-2 infection known for the general population, such as age, male gender, and certain chronic conditions, play a similar role in patients with IRD. Although, chronic kidney disease and interstitial lung disease showed an increased risk for severe COVID-19 compared to the general population, no higher risk for COVID-19 related death could be observed in IRD patients. Regarding treatment, rituximab was associated with worse outcome of COVID-19 and most importantly, our data show that treatment with TNF-I was associated with better outcome of COVID-19 compared to the herewith untreated control group, indicating a protective effect of TNF-inhibition against severe COVID-19 disease during the first two waves of pandemic.
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics statement
The COVID-19 registry for IRD patients has been approved by the ethics committee of the Justus-Liebig-University Giessen (#52-50), Germany. Approval for the LEOSS registry was obtained by the applicable local ethics committees of all participating centers and registered at the German Clinical Trails Register (DRKS, No. DRKS00021145). For the present analysis, we included data from March 2020 to January 2021. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because an analysis of anonymized data from two registries was carried out, where it was not necessary to obtain patient consent due to the ethics votes and the regulations in Germany.
Author contributions
RH: Writing – original draft, Writing – review & editing. FH: Writing – review & editing, Investigation. MS: Investigation, Data curation, Validation, Writing – original draft. CS: Writing – original draft, Writing – review & editing. TW: Writing – original draft, Writing – review & editing, Data curation, Validation. SB: Writing – review & editing, Investigation. MHa: Investigation, Writing – review & editing. BHe: Investigation, Writing – review & editing. MHo: Investigation, Writing – review & editing. BHo: Investigation, Writing – review & editing. CK: Writing – review & editing, Data curation, Formal Analysis, Methodology, Validation. AK: Investigation, Writing – review & editing. ML-T: Investigation, Writing – review & editing. H-MT: Investigation, Writing – review & editing. UM: Investigation, Writing – review & editing. SM: Investigation, Writing – review & editing. MP: Investigation, Writing – review & editing. AR: Investigation, Writing – review & editing, Data curation, Formal Analysis. JR: Writing – review & editing, Investigation. SR: Investigation, Writing – review & editing. CR: Investigation, Writing – review & editing. MR: Investigation, Writing – review & editing. TS: Investigation, Writing – review & editing. HS-K: Investigation, Writing – review & editing. AS: Investigation, Writing – review & editing. MV: Investigation, Writing – review & editing. FV: Investigation, Writing – review & editing. RV: Investigation, Writing – review & editing. JV: Investigation, Writing – review & editing, Conceptualization, Methodology, Project administration. UM-L: Conceptualization, Investigation, Methodology, Writing – review & editing, Supervision, Writing – original draft. AP: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The IRD registry was funded, in part, by the German Society for Rheumatology. The LEOSS study was supported by the German Center for Infection Research (DZIF) and the Willy Robert Pitzer Foundation.
Acknowledgments
All authors express the deep gratitude to all study teams supporting the LEOSS study. We thank all physicians and personnel involved in the documentation of the cases in the DGRh registry: Fredrik Albach, Annette Alberding, Tobias Alexander, Rieke Alten, Susanne Amann, Christopher Amberger, Michaela Amberger, Bianka Andermann, Nils Anders, Ioana Andreica, Jan Andresen, Nikolaos Andriopoulos, Peer Aries, Martin Aringer, Uta Arndt, Sarah Avemarg, Marina Backhaus, Christoph Baerwald, Erich Bärlin, Nora Bartholomä, Hans Bastian, Michael Bäuerle, Jutta Bauhammer, Dr Christine Baumann, Heidemarie Becker, Klaus Becker, Michaela Bellm, Sylvia Berger, Gerhard Birkner, Norbert Blank, Daniel Blendea, Hans Bloching, Stephanie Böddeker, Susanne Bogner, Martin Bohl-Bühler, Sebastian Böltz, Ilka Bösenberg, Nicole Böttcher, Jan Brandt-Jürgens, Matthias Braun, Matthias Braunisch, Jan Phillip Bremer, Matthias Broll, Andreas Bruckner, Veronika Brumberger, Martin Brzank, Sahra Büllesfeld, Sandra Burger, Gamal Chehab, Michaela Christenn, Dr Anne Claußnitzer, Kirsten de Groot, Elvira Decker, Frank Demtröder, Jacqueline Detert, Rainer Dörfler, Ines Dornacher, Elke Drexler, Edmund Edelmann, Roman Eder, Christina Eisterhues, Dr Andreas Engel, Joachim Michael Engel, Brigitte Erbslöh-Möller, Miriam Feine, Martin Feuchtenberger, Christoph Fiehn, Rebecca Fischer-Betz, Professor Dr Martin Fleck, Stefanie Freudenberg, Christian Fräbel, Petra Fuchs, Regina Gaissmaier, Ino Gao, Oliver Gardt, Georg Gauler, Katrin Geißler, Joachim Georgi, Jasmin Gilly, Yannik Gkanatsas, Cornelia Glaser, Agnes Gniezinski-Schwister, Rahel Gold, Norman Görl, Karl-Heinz Göttl, Beate Göttle, Anett Gräßler, Ricardo Grieshaber-Bouyer, Gisela Grothues, Mathias Grünke, Elizabeth Guilhon de Araujo, Florian Günther, Mirjam Haag, Linda Haas, Anna Haas-Wöhrle, Denitsa Hadjiski, Hildrun Haibel, Till Ole Hallmann-Böhm, Urs Hartmann, Charlotte S. Hasenkamp, Maura-Maria Hauf, Matthias Hauser, Nicole Heel, Liane Hein, Reinhard Hein, Claudia Hendrix, Jörg Henes, Karen Herlyn, Walter Hermann, Peter Herzer, Andrea Himsel, Guido Hoese, Paula Hoff, Marie-Therese Holzer, Johannes Hornig, Melanie Huber, Georg Hübner, Ole Hudowenz, Axel Hueber, Verena Hupertz, Elke Iburg, Annette Igney-Oertel, Steffen Illies, Annett M. Jacobi, Ilona Jandova, Christiane Jänicke, Sebastian T. Jendrek, Anne Johannes, Aaron Juche, Sarah Kahl, Ludwig Kalthoff, Wiebke Kaluza-Schilling, Eleni Kampylafka, Antje Kangowski, Andreas Kapelle, Kirsten Karberg, Dorothee Kaudewitz, Bernd Oliver Kaufmann, Gernot Keyßer, Nayereh Khoshraftar-Yazdi, Matthias Kirchgässner, Matthias Kirrstetter, Birgit Kittel, Christoph Kittel, Julia Kittler, Arnd Kleyer, Claudia Klink, Barbara Knau, Christian Kneitz, Anna Knothe, Katrin Köchel, Benjamin Köhler, Peter Korsten, Magdolna Kovacs, Dietmar Krause, Gabi Kreher, Rene Kreutzberger, Eveline Krieger-Dippel, Klaus Krüger, Brigitte Krummel-Lorenz, Martin Krusche, Holger Kudela, Christoph Kuhn, Kerstin Kujath, Reiner Kurthen, Rolf Kurzeja, Peter Kvacskay, Peter Lamprecht, Sabine Langen, Heiko Lantzsch, Petra Lehmann, Nicolai Leuchten, Christian Löffler, Dorothea Longerich-Scheuß, Gitta Lüdemann, Thomas Lutz, Vanessa Maerz, Hartmut Mahrhofer, Ingeborg Maier, Karin Manger, Elisabeth Märker-Hermann, Anette Märtz, Hanin Matar, Johannes Mattar, Sebastian Maus, Ursula Mauß-Etzler, Regina Max, Florian Meier, Adelheid Melzer, Carlos Meneses, Hans-Jürgen Menne, Helga Merwald-Fraenk, Claudia Metzler, Sabine Mewes, Harriet Morf, Harald Mörtlbauer, Markus Mortsch, Burkhard Muche, Niels Murawski, Antoine Murray, Jana Naumann, Anabell Nerenheim, Joachim Neuwirth, Phuong Nguyen, Stine Niehus, Martin Nielsen, Matthias Noehte, Dirk Nottarp, Dieter Nüvemann, Wolfgang Ochs, Sarah Ohrndorf, Jürgen Olk, Silke Osiek, Filiz Özden, Bettina Panzer, Alina Patroi, Ulrich Pfeiffer, Dorothea Pick, Marta Piechalska, Matthias Pierer, I. Pohlenz, Mikhail Protopopov, Almut Pulla, Michael Purschke, Judith Rademacher, Wolf Raub, Jürgen Rech, Sabine Reckert, Anke Reichelt de Tenorio, Christiane Reindl, Annja Reisch, Gabriela Riemekasten, Markus Rihl, Viale Rissom, Karin Rockwitz, Maike Rösel, Markus Röser, Christoph Rossmanith, Ekkehard Röther, Fabian Röther, Maria Roth-Szadorski, Martin Rudwaleit, Petra Saar, Jasemine Saech, Oliver Sander, Eva Sandrock, Ertan Saracbasi-Zender, Michael Sarholz, Christoph Schäfer, Kerstin Schäfer, Martin Scheel, Stefan Schewe, Hermine Schibinger, Magnus Schiebel, Andreas Schieweck-Güsmer, Susanne Schinke, Ulrike Schlenker, Daniel Schlittenhardt, Marc Schmalzing, Verena Schmitt, Matthias Schmitt-Haendle, Sebastian Schnarr, Dieter Schöffel, Michaela Scholz, Jutta Schönherr, Ulrich Schoo, Judith Schreiber, Anna-Sophie Schübler, Florian Schuch, Ilka Schwarze, Carola Schwerdt, Eva Seipelt, Matthias Sekura, Jörg Sensse, Nyamsuren Sentis, Christine Seyfert, Ondrej Sglunda, Naheed Sheikh, Iris Sievert, David Simon, Marta Sluszniak, Katharina Sokoll, Sigrid Sonn, Susanna Späthling-Mestekemper, Lydia Spengler, Gerald Stapfer, Nicolai Steinchen, Mirko Steinmüller, Karen Steveling, Karin Stockdreher, Helga Streibl, Johannes Strunk, Mechthild Surmann, ngo H. Tarner, Stefanie Tatsis, Astrid Thiele, Jan Thoden, Anika Tuleweit, Peter Vaith, Inka Vallbracht-Ackermann, Susanne Veerhoff, Nils Venhoff, Anita Viardot, Lisa Vinnemeier-Laubenthal, Markus Voglau, Marcus von Deimling, Cay-Benedict von der Decken, Heike von Löwis, Marisa Walther, Sven Weidner, Martin Weigelt, Stefan Weiner, Jutta Weinerth, Angela Weiß, Martin Welcker, Stephanie Werner, Dirk Wernicke, Franziska Wiesent, Peter Willeke, Lea Winau, Hans Wisseler, Matthias Witt, Stefan Wolf, Nina Wysocki, Panagiota Xanthouli, Monika Zaus, Markus Zeisbrich, and Silke Zinke.
Conflict of interest
TW was employed by company Biocontrol Jena.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
bDMARD, biological disease-modifying antirheumatic drug; BMI, body mass index; CI, confidence interval; COPD, Chronic obstructive pulmonary disease; COVID-19, coronavirus disease 2019; csDMARD, conventional synthetic disease-modifying antirheumatic drug; DMARD, disease-modifying antirheumatic drug; DSA, disease activity; ECMO, extracorporal membrane oxygenation; ILD, interstitial lung disease; IRD, inflammatory rheumatic diseases; IRD registry, German COVID-19 registry; JAK-I, Janus kinase inhibitors; LEOSS registry, Lean European Open Survey on SARS-CoV-2; n. a., not applicable; n. s., not significant; OR, Odds Ratio; SARS-CoV-2, Severe acute respiratory syndrome Coronavirus 2; SpA, Spondyloarthritis; TNF-I, Tumour necrosis factor-alpha inhibitors.
Footnotes
References
1. Ye Q, Wang B, Mao J, Fu J, Shang S, Shu Q, et al. Epidemiological analysis of COVID-19 and practical experience from China. J Med Virol. (2020) 92:755–69.
3. Onder G, Rezza G, Brusaferro S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA. (2020) 323:1775–6.
4. Hasseli R, Mueller-Ladner U, Hoyer B, Krause A, Lorenz H, Pfeil A, et al. Older age, comorbidity, glucocorticoid use and disease activity are risk factors for COVID-19 hospitalisation in patients with inflammatory rheumatic and musculoskeletal diseases. RMD Open. (2021) 7:e001464.
5. Akiyama S, Hamdeh S, Micic D, Sakuraba A. Prevalence and clinical outcomes of COVID-19 in patients with autoimmune diseases: a systematic review and meta-analysis. Ann Rheum Dis. (2021) 80:384–91.
6. Regierer A, Hasseli R, Schäfer M, Hoyer B, Krause A, Lorenz H, et al. TNFi is associated with positive outcome, but JAKi and rituximab are associated with negative outcome of SARS-CoV-2 infection in patients with RMD. RMD Open. (2021) 7:e001896. doi: 10.1136/rmdopen-2021-001896
7. Schulze-Koops H, Krueger K, Vallbracht I, Hasseli R, Skapenko A. Increased risk for severe COVID-19 in patients with inflammatory rheumatic diseases treated with rituximab. Ann Rheum Dis. (2021) 80:e67.
8. Strangfeld A, Schäfer M, Gianfrancesco M, Lawson-Tovey S, Liew J, Ljung L, et al. Factors associated with COVID-19-related death in people with rheumatic diseases: results from the COVID-19 global rheumatology alliance physician-reported registry. Ann Rheum Dis. (2021) 80:930–42.
9. Schulze-Koops, H, Krueger K, Vallbracht I, Hasseli R, Skapenko A. Treatment of patients with inflammatory rheumatic diseases with rituximab should be carefully considered during the SARS-CoV-2/COVID-19 pandemic. Response to: ‘persistence of rT-PCR-SARS-CoV-2 infection and delayed serological response, as a possible effect of rituximab according to the hypothesis of Schulze-Koops et al’ by Benucci, et al. Ann Rheum Dis. (2020). doi: 10.1136/annrheumdis-2020-218686 [Epub ahead of print].
10. Rüthrich M, Giessen-Jung C, Borgmann S, Classen A, Dolff S, Grüner B, et al. COVID-19 in cancer patients: clinical characteristics and outcome-an analysis of the LEOSS registry. Ann Hematol. (2021) 100:383–93. doi: 10.1007/s00277-020-04328-4
11. Chiriboga K, Pipitone O, Jones C, Greenberg B, Jones J. Risk of COVID-19 infection and hospitalization in patients with inflammatory rheumatic disease compared with the general population. J Clin Rheumatol. (2022) 28:e629–32.
12. Cordtz R, Lindhardsen J, Soussi B, Vela J, Uhrenholt L, Westermann R, et al. Incidence and severeness of COVID-19 hospitalization in patients with inflammatory rheumatic disease: a nationwide cohort study from Denmark. Rheumatology (Oxford). (2021) 60:Si59–67. doi: 10.1093/rheumatology/keaa897
13. Hasseli R, Mueller-Ladner U, Schmeiser T, Hoyer B, Krause A, Lorenz H, et al. National registry for patients with inflammatory rheumatic diseases (IRD) infected with SARS-CoV-2 in Germany (ReCoVery): a valuable mean to gain rapid and reliable knowledge of the clinical course of SARS-CoV-2 infections in patients with IRD. RMD Open. (2020) 6:e001332. doi: 10.1136/rmdopen-2020-001332
14. Pilgram L, Schons M, Jakob C, Claßen A, Franke B, Tscharntke L, et al. [The COVID-19 pandemic as an opportunity and challenge for registries in health services research: lessons learned from the lean European open survey on SARS-CoV-2 infected patients (LEOSS)]. Gesundheitswesen. (2021) 83:S45–53. doi: 10.1055/a-1655-8705
16. James GW, Hastie T, Tibshirani R. In Introduction to Statistical Learning: With Applications in R. Berlin: Springer (2013).
17. Die Drogenbeauftragte der Bundesregierung. Drogen– und Suchtbericht. (2019). Available online at: https://www.bundesdrogenbeauftragter.de/assets/Service/DSB_2019_mj_barr.pdf (accessed January 15, 2024).
18. Izadi Z, Brenner E, Mahil S, Dand N, Yiu Z, Yates M, et al. Association between tumor necrosis factor inhibitors and the risk of hospitalization or death among patients with immune-mediated inflammatory disease and COVID-19. JAMA Netw Open. (2021) 4:e2129639.
19. Sparks J, Wallace Z, Seet A, Gianfrancesco M, Izadi Z, Hyrich K, et al. Associations of baseline use of biologic or targeted synthetic DMARDs with COVID-19 severity in rheumatoid arthritis: results from the COVID-19 global rheumatology alliance physician registry. Ann Rheum Dis. (2021) 80:1137–46.
20. Del Valle D, Kim-Schulze S, Huang H, Beckmann N, Nirenberg S, Wang B, et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat Med. (2020) 26:1636–43.
21. Stallmach A, Kortgen A, Gonnert F, Coldewey S, Reuken P, Bauer M. Infliximab against severe COVID-19-induced cytokine storm syndrome with organ failure-a cautionary case series. Crit Care. (2020) 24:444. doi: 10.1186/s13054-020-03158-0
22. Goodsall T, Costello S, Bryant R. COVID-19 and implications for thiopurine use. Med J Aust. (2020) 212:490-490.e1.
23. D’Silva K, Jorge A, Cohen A, McCormick N, Zhang Y, Wallace Z, et al. COVID-19 outcomes in patients with systemic autoimmune rheumatic diseases compared to the general population: a US multicenter, comparative cohort study. Arthritis Rheumatol. (2021) 73:914–20. doi: 10.1002/art.41619
Keywords: inflammatory rheumatic diseases, COVID-19, general population, tumor necrosis factor-alpha inhibitors, severe disease
Citation: Hasseli R, Hanses F, Stecher M, Specker C, Weise T, Borgmann S, Hasselberger M, Hertenstein B, Hower M, Hoyer BF, Koll C, Krause A, von Lilienfeld-Toal M, Lorenz H-M, Merle U, Nunes de Miranda SM, Pletz MW, Regierer AC, Richter JG, Rieg S, Roemmele C, Ruethrich MM, Schmeiser T, Schulze-Koops H, Strangfeld A, Vehreschild MJGT, Voit F, Voll RE, Vehreschild JJ, Müller-Ladner U and Pfeil A (2024) The protective effect of tumor necrosis factor-alpha inhibitors in COVID-19 in patients with inflammatory rheumatic diseases compared to the general population—A comparison of two German registries. Front. Med. 11:1332716. doi: 10.3389/fmed.2024.1332716
Received: 03 November 2023; Accepted: 12 February 2024;
Published: 06 March 2024.
Edited by:
Peter Mandl, Medical University of Vienna, AustriaReviewed by:
Paul Studenic, Medical University of Vienna, AustriaMehmet Soy, Altınbaş University, Türkiye
Copyright © 2024 Hasseli, Hanses, Stecher, Specker, Weise, Borgmann, Hasselberger, Hertenstein, Hower, Hoyer, Koll, Krause, von Lilienfeld-Toal, Lorenz, Merle, Nunes de Miranda, Pletz, Regierer, Richter, Rieg, Roemmele, Ruethrich, Schmeiser, Schulze-Koops, Strangfeld, Vehreschild, Voit, Voll, Vehreschild, Müller-Ladner and Pfeil. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexander Pfeil, YWxleGFuZGVyLnBmZWlsQG1lZC51bmktamVuYS5kZQ==
†These authors have contributed equally to this work