Abstract
Objective:
To determine the comparative effects and safety of traditional Chinese medicine (TCM) interventions based on meridian theory for pain relief in patients with primary dysmenorrhea (PD).
Methods:
This is a systematic review with network meta-analysis. Randomized controlled trials (RCTs) comparing meridian-based TCM interventions with waitlist, placebo, western medicine, and conventional therapies for PD pain. A SUCRA was used to estimate the probability ranking for the effects of interventions.
Results:
57 RCTs involving 3,903 participants and 15interventions were included. Thirty-two RCTs were rated as low risk of bias. A network diagram was drawn with 105 pairs of comparisons. Compared with NSAIDs and waitlist, significantly better effects were found in acupressure [SMD = −1.51, 95%CI (−2.91, −0.12)/SMD = −2.31, 95%CI (−4.61, −0.02)], warm needling [SMD = −1.43, 95%CI (−2.68, −0.18)/SMD = −2.23, 95%CI (−4.43, −0.03)], moxibustion [SMD = −1.21, 95%CI (−1.85, −0.57)/SMD = −2.10, 95%CI (−3.95, −0.07)], and acupuncture [SMD = −1.09, 95%CI (−1.62, −0.55)/SMD = −1.89, 95%CI (−3.67, −0.11)]. No adverse events were detected.
Conclusion:
For PD pain, the effects of acupressure, acupuncture, warm needling, and moxibustion were superior to those of NSAIDs and waitlist. Oral contraceptive pill, electro-acupuncture, acupressure, and warm needling demonstrated higher probabilities of being better interventions. More high-quality clinical trials are needed to provide more robust evidence of this network.
Systematic review registration:
PROSPERO CRD42022373312.
1 Introduction
Primary dysmenorrhea (PD) refers to the occurrence of menstrual cramps in the lower abdomen, without any identifiable pelvic pathology, with characteristic symptoms such as lower abdominal or pelvic pain, ranging from 8 h to 72 h and typically occurring at the onset of menstrual flow (1). Other associated symptoms include low back pain, headache, diarrhea, fatigue, nausea, or vomiting (2). The prevalence of PD varies from 50 to 90% (3). The exact causes remain unknown, leading to non-targeted treatments. Risk factors for PD include early age at menarche, heavy menstrual flow, nulliparity, family history of dysmenorrhea, and stress (4).
Systematic reviews and randomized controlled trials (RCTs) have shown that non-steroidal anti-inflammatory drugs (NSAIDs) (5, 6) and hormonal regulation through oral contraception (7) are significantly more effective for pain relief than placebo, and they are often used for symptom control (8). However, some women may not always find them effective or acceptable; for example, NSAIDs have undesirable side effects (6). Non-drug, non-surgical treatments for PD include transcutaneous electric nerve stimulation, behavior modification/relaxation, acupressure, acupuncture, spinal manipulation, topical heat, vitamin E, thiamine, fish oil, and herbal medicine (9). Only 26.7% of patients with PD have no experience with complementary and alternative medicine. Diet and homeopathy are the most frequently used methods from complementary and alternative medicine. In spite of the provision of information on efficacy, safety, and costs, patients choose methods based on earlier experience (10). Despite their popularity, evidence on the effectiveness of these nonpharmacologic therapies for PD is limited and inconsistent (11, 12).
Traditional Chinese medicine (TCM) interventions based on meridian theory can be an effective alternative approach for PD. Meridian is a system of conduits through which qi and blood circulate, connecting the bowels, viscera, extremities, superficial, organs, and tissues and making the body an organic whole. The meridian system includes 12 regular meridians, 8 extra meridians, 12 meridian divergence, 12 meridian sinews, 12 cutaneous vessels, and 15 collateral vessels (13). Meridian-based TCM interventions include acupuncture, acupressure, tuina, moxibustion, cupping, auricular therapy, electro-acupuncture, and scraping. These interventions may produce analgesic effects through the regulation of the hypothalamic–pituitary–ovarian axis, modulation of the immune system, and release of endogenous opioid peptides (14). Animal experiments have demonstrated that acupuncture may facilitate the release of central and peripheral neurotransmitters, modulation of immune function, and alleviation of uterine smooth muscle spasm (15, 16). Clinical trials have indicated that acupuncture may elicit analgesia by regulating serum levels of prostaglandins and ovarian hormones, facilitating the release of peripheral β-endorphin, improving the status of uterine artery blood flow, and alleviating uterine smooth muscle spasm (14). Similarly, moxibustion may modulate endocrine hormones, immune function, and nerve factors and enhance uterine microcirculation (17).
Numerous studies have investigated the efficacy of TCM interventions based on meridian theory for dysmenorrhea, including systematic reviews, RCTs, and case series. A systematic review of RCTs on acupuncture for PD reported that acupuncture provides superior pain relief (OR: 4.99; 95% CI: 2.82–8.82; 4 RCTs; I2 = 0%) and has fewer adverse events compared with NSAIDs (OR: 0.10; 95% CI: 0.02–0.44; 4 RCTs; I2 = 15%); however, evidence quality was low, and further research is needed to ascertain the effectiveness of acupuncture and acupressure (18). In an RCT of 152 subjects, moxibustion was found to have sustained and superior pain-relieving effects compared with drugs 3 months post-intervention (effect size: −0.87, 95% CI: −1.32 to −0.42, p < 0.001) measured by the visual analogue scale (VAS) (19). Acupressure on the SP6 meridian was found to be superior to placebo acupressure in relieving PD pain symptoms based on a VAS score (−4.935; 95% CI: [−15.757, 5.887]; p = 0.371) (20), whereas auricular therapy was found to be more effective than analgesics based on VAS scores (OR = 3.28, 95%CI: [1.37, 7.85], p = 0.008) (21). Although numerous studies have examined the effects of meridian-based TCM interventions for PD pain, no comparative analysis of their effectiveness has been conducted. Therefore, a comprehensive comparison of multiple TCM interventions based on meridian theory is required, as well as organization and collection of high-quality evidence.
Network meta-analysis (NMA) yields high-quality evidence, which can be used to evaluate the effects of multiple interventions and rank optimal intervention strategies (22). This study performed an NMA of RCTs on TCM interventions based on meridian theory for relieving pain in patients with PD, comparing the effects among interventions (TCM interventions based on meridian theory and eligible control interventions), and exploring the optimal one. The findings can provide evidence to help clinical workers and researchers understand the optimal protocol for pain management of PD.
2 Methods
This systematic review was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) (18), the PRISMA-2020 guidelines (19), and the extension statement for network meta-analysis (PRISMA-NMA) (20). The protocol was registered on PROSPERO (CRD42022373312).
2.1 Selection criteria
Studies had to fulfill the following criteria presented in PICOS tools (population, intervention, comparators, outcomes, and study design): (1) population: patients diagnosed with PD; (2) intervention: meridian-based TCM interventions including acupressure, acupuncture, moxibustion, tuina, electroacupuncture, warm needling, auricular therapy, and scraping therapy (Interventions should be singly used, so that their effects can be detected. Interventions related to Chinese herb, staging acupoint catgut embedment therapy, acupuncture point injection therapy, or combined TCM intervention were excluded.); (3) comparators: control group with waitlist, placebo, western medicine (e.g., NSAIDs and combined oral contraceptives), conventional therapy, or another type of meridian-based TCM interventions (Studies comparing two or more meridian-based TCM interventions were included. Usual care was excluded due to the variety of care content among different interventions and study settings.); (4) outcomes: studies that evaluated pain intensity using VAS or numerical rating scale (NRS); and (5) study design: RCTs.
2.2 Search strategy
We searched Ovid MEDLINE, Embase, Health Technology Assessment Database, Cochrane Central Register of Controlled Trials, Web of Science, Allied and Complementary Medicine, the China National Knowledge Infrastructure, Wanfang Data, PubMed, SinoMed, and CQVIP from database inception until 1 July 2023. The following keywords were used for our search: (massag* OR anmo OR acupress* OR tuina OR acupunct* OR electroacupunct* OR electro-acupunct* OR acupoint* OR meridia* OR auricular OR needl* OR moxibustion OR moxa) AND (dysmenorr* OR menstrua* pain OR period cramp OR period pain* OR menstrua* distress OR period distress OR menstrua* distress). To search the Chinese databases, we used the corresponding Chinese keywords. We did not impose any language restrictions (See Supplementary Appendix 1). We also scanned reference lists of relevant systematic reviews and clinical guidelines. Two authors (SCC and JYR) independently performed the literature search. Disagreements were resolved upon consultation and judgement by a third reviewer (WFY).
2.3 Data extraction
Two authors (SSC and LYP) independently screened the titles and abstracts of the retrieved studies, and the unrelated articles were removed. Thereafter, we reviewed the full texts of potentially relevant studies and extracted the data based on the selection criteria. The following data were extracted from the included RCTs in a predesigned data sheet: the first author’s name, publication year, characteristics of participants, sample size, diagnostic system, details of interventions, details of the control interventions, follow-up period, details of outcomes, and language. Basic information on the excluded studies was also extracted to provide a comprehensive reference to readers, with information on the original title, publication year, and reasons for exclusion. An additional reviewer (WFY) was consulted in the event of discrepancies between authors.
2.4 Quality assessment
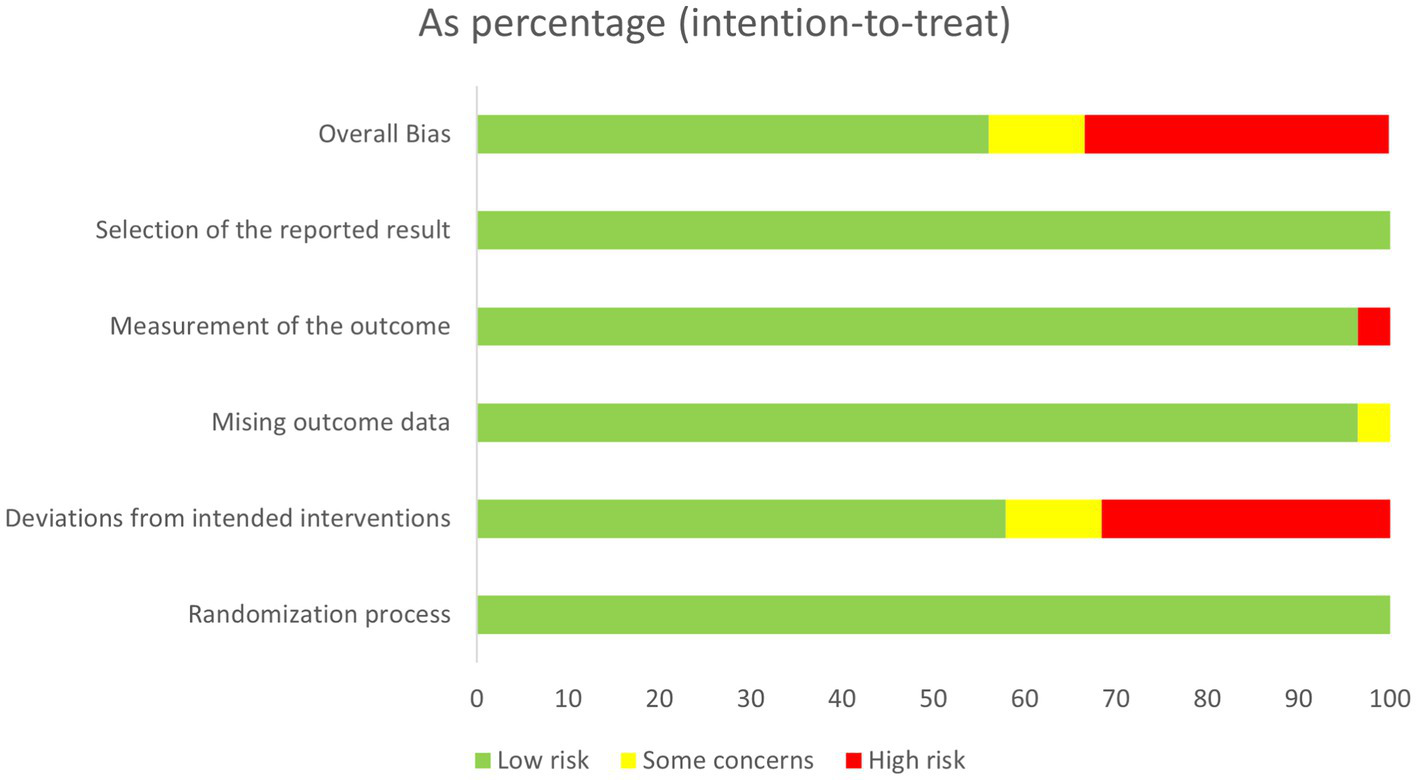
Two authors (SCC and LYP) performed the quality evaluation of included studies independently in accordance with Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (21). The risk of bias for trials was assessed using criteria in the Cochrane Risk of Bias version 2 (RoB 2) tool. We assessed potential bias related to five domains, namely, randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Each publication was identified as “high risk,” “low risk,” or “some concerns.” If there were any objections, they would be discussed or judged by a third researcher (WFY) to reach a consensus.
The GRADEpro Guideline Development Tool web page was employed to assess the evidence for the quality of outcome indicators including five degrading factors: risk of bias, inconsistency, indirectness, imprecision, and publication bias (23). On the basis of these variables, the software generates a GRADE rating of “high,” “moderate,” “low,” or “very low” to reflect the certainty of the reported effect. A summary of findings (SoF) table was generated for a given comparison of interventions to provide key information concerning the magnitudes of relative and absolute effects of the interventions examined, the amount of available evidence, and the quality of available evidence (21).
2.5 Statistical analysis
Standard mean difference (SMD) with a 95% confidence interval (CI) was used to estimate the effect sizes of NRS or VAS. Variation was expected between the original studies. To make the results more conservative, a random effects model was used rather than a fixed effects model. The statistical heterogeneity in each pairwise comparison was assessed using inconsistency index tests or Chi-square test or I2 statistic test (I2 > 30% or p-value <0.1 indicating inconsistency). Additionally, sensitivity analysis was conducted to verify the robustness of the results and test the source of heterogeneity in each RCT. Three-armed RCTs were transformed into two-armed pairs to clearly present the effects of comparisons. For the studies that reported the mean and standard deviation of effect changes in the interventions, we calculated the data at the endpoint of the intervention period using the current data.
An NMA with a Bayesian framework using Statistics and Data Science (STATA) software was conducted to assess the outcomes of different interventions (24). Network diagrams were used to present the results: (1) each node represents an exercise intervention; (2) the size of the node indicates the sample size of the subjects who performed this intervention; (3) if there are no line segments between each node, then indirect comparisons will be made between the nodes; if there are line segments, then direct comparisons will be made between the nodes; (4) the thickness of the line segments between the nodes indicates the original study sample size; and (5) the size of the nodes and the thickness of the line segments are positively correlated with the number (25). The surface under the cumulative ranking curve (SUCRA) is the probability each intervention has of being among the best of those in the network; the SUCRA values range from 0 to 1, with large values representing high intervention ranking probabilities (26). NMA results were visualized using forest plots. A funnel plot was generated to examine possible publication bias.
3 Results
3.1 Literature search
Our search yielded a total of 3,080 potentially eligible citations, among which 704 remained after the removal of duplicates and irrelevant records. Of the remaining citations, 86 studies were obtained by reading the titles and abstracts. After the full text of these records was screened, 57 studies were included for network analysis. The PRISMA flow diagram describing the inclusion process is presented in Figure 1. Supplementary Appendix 2 shows the details of the excluded studies from full-text screening.
Figure 1

PRISMA Flow Chart.
3.2 Description of included studies
As shown in Table 1, the included 57 RCTs were published between 2011 and 2022 and included 3,903 participants. The included participants’ age ranged from 14 years to 39 years. The sample size of the included RCTs was from 20 to 208. Besides the eligibility on age, disease duration, and intervention use records, most RCTs screened and included participants by using pain rating scales (57 studies), including VAS and NRS. Eight types of meridian-based TCM interventions were reported among the included RCTs, namely, acupuncture (n = 865) (31, 32, 35–37, 41, 44, 46, 50–56, 58, 62–65, 68, 70), acupressure (n = 285) (27, 28, 30, 33, 34, 71, 72, 79), auricular therapy (n = 35) (57), electro-acupuncture (n = 66) (34, 47), moxibustion (n = 651) (29, 38–40, 42–44, 48–50, 61, 62, 66, 67, 74, 77), scraping therapy (n = 30) (69), tuina (n = 57) (45, 54), and warm needling (n = 151) (41, 59, 60, 78). The most commonly involved meridians included conception vessel (CV), spleen meridian (SP), stomach meridian (ST), and governor vessel (GV). Four types of control interventions were reported, namely, health education (27), waitlist (35, 81), placebo (sham interventions) (28–30, 32, 33, 56, 72, 82), and conventional medicine (oral contraceptive pill and NSAIDs) (31, 36–40, 42, 43, 45–49, 51–53, 55, 57–61, 63–71, 73–80, 83). Pain outcome measures included VAS and NRS. One RCT used both VAS and NRS (29), 3 used NRS only (36, 59, 69), and the other 53 used VAS only. The treatment period ranged from 30 min to 3 months, and the follow-up period ranged from 3 h to 6 months. Twelve RCTs were published in English and 45 were in Chinese.
Table 1
| NO. | First author (year) |
Age (mean, range) | Sample size (I/C) |
Inclusion criteria |
Exclusion criteria | Diagnostic system | Treatment | Control | Outcome measure (pain) |
Treatment/ follow-up period | Language |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Chen (2015) (27) | NR, NR | 129 (65/64) | - Women ≤25y - VAS ≥ 4 |
- Receiving pain medication in the recent 4 h - had a surgery for low back pain |
NR | Acupressure (SP6, BL32, Lv3) | Health education | - VAS | 1 m / 12 m | English |
| 2 | Dincer (2023) (28) | NR, NR | 67 (34/33) | - Women ≥18y - VAS ≥ 4 - Regular menstrual period of 3-8d with an interval of 21-35d |
- Having pelvic disease, operation, infection, physical or mental illness, NSAIDs allergy - receiving COC |
NR | Acupressure (SP6) | Sham acupressure (SP6) |
- VAS | 3 m / 1 m | English |
| 3 | Gao (2015) (29) | NR, NR | 56 (28/28) | - Nursing students - 17-25y - Regular menstrual cycles 21-35d and length 3-7d |
- Having received hormonal therapy in the past 6 m - Receiving analgesics during the study period - With SDM, systemic or gynecologic disease |
NR | Moxibustion (CV4, CV8) |
Sham moxibustion (CV4, CV8) | - NRS - VAS |
2 m / NR | English |
| 4 | Kashefi (2010) (30) | NR, 18–26 |
86 (43/43) | - Iranian single female college students - 18-28y - VAS ≥ 4 - regular menstrual cycles |
- Having recent stressful events - Having history of gynecological disease or SDM - receiving pain medication before each menstrual period and 3 h after intervention |
NR | Acupressure (SP6) | Sham acupressure | - VAS | 2 m / NR | English |
| 5 | Kiran (2013) (31) | 21, NR | 35 (11/24) | - Women aged 15–40y - Severe persist pain before/during menstruation - Being referred to the outpatient clinic of obstetrics |
-Having irregular menstrual cycles or SDM |
- Based on self-reported severe | Acupuncture (HT7, PC6, LI4, LI10, SP6, LR3, ST36, GB26, SP15, CV19) | NSAIDs (naproxen sodium) | - VAS | 3 m / 12 m | English |
| 6 | Liu (2022) (32) | NR, NR | 47 (22/19) | - Women aged 18–30y with at least 1y history of PDM - VAS ≥ 4 - Regular menstrual cycle 27-32d - No hormones or centrally acting drugs in the past 6 m |
- Having SDM or severe chronic diseases - Being pregnant, prepared for pregnancy/breastfeeding - Receiving acupuncture, analgesic medication in the past 3 m |
- Society of Obstetricians and Gynecologists of Canada’s diagnostic criteria | Acupuncture (SP6) | Sham acupuncture (SP6) | - VAS | 3 m / NR | English |
| 7 | Mirbagher-Ajorpaz (2011) (33) | 22, NR | 30 (15/15) | - Women aged 18-30y - Regular menstrual cycles - VAS ≥ 3 |
- Being pregnant - Having SDM |
- Based on history and then by exclusion of probable pathologies | Acupressure (SP6) | Light touch (SP6) | - VAS | 30 min / 3 h | English |
| 8 | Qorbanalipour (2018) (34) | NR, NR | 64 (31/33) | - Virgin girls aged 18-26y - At least 2y of regular menstruation between 21-35d |
- With SDM, history of pelvic organs surgery, itching, abnormal secretions - Using any other drugs for health problems in the past 6 m - with a history of smoking or alcohol use |
- Diagnosis from a gynecologist | Electro-acupuncture (SP4, SP6) | Acupressure (SP4, SP6) | - VAS | 2 m / 1 m | English |
| 9 | Shetty (2018) (35) | NR, 17–23 | 60 (30/30) | - Women with PDM for at least 1y - Regular menstrual cycles 28 ± 7d |
- With SDM or any systemic psychiatric illness - Receiving intrauterine devices and medicine for PDM in the past 6 m |
NR | Acupuncture (KI3, SP8, ST25, ST29, ST30, ST36, CV4, CV6, BL62, HT7, LI4, PC6) |
Waitlist | - VAS | 2 m / 1 m | English |
| 10 | Sriprasert (2015) (36) | NR, 18–35 | 52 (27/25) | - With PDM within the previous 3 months - NRS ≥ 5 - VMSS ≥2 |
- With contraindication to COC/acupuncture and abnormal gynecologic conditions - Underlying gynecologic conditions associated with DM |
- Diagnosis from a gynecologist | Acupuncture (CV6, CV3, SP8, SP6) | Oral contraceptive pill | - NRS | 3 m / NR | English |
| 11 | Wang (2019) (37) | NR, NR | 62 (31/31) | - Women aged 18-35y with PDM - VAS ≥ 4 - Normal menstrual cycles 28 ± 7d in recent 3 m |
- With SDM or serious diseases - Being pregnant or during lactation - Receiving any other treatment for PDM in recent 2wk - Having a history of delivery |
- PDM Consensus Guideline -The revised Chinese National Guideline |
Acupuncture (BL54, ST28) | NSAIDs (ibuprofen) | -VAS | 3 m / NR | English |
| 12 | Yang (2017) (38) | NR, NR | 152 (76/76) | - Women aged 18-35y with PDM (pattern of congealing cold with blood stasis) - VAS ≥ 4 -Regular menstrual cycles 28 ± 7d |
- Being during lactation, pregnant, or plan to get pregnant - With SDM - Receiving PGSI, drugs and moxibustion in recent 2wk |
- Society of Obstetricians and Gynecologists of Canada’s Clinical Guideline of PDM | Moxibustion (CV4, CV8, SP6) | NSAIDs (ibuprofen) | - VAS | 3 m / 3 m | English |
| 13 | Ding (2021) (39) | NR, 14–35 |
312 (104/104/104) | - With PDM (pattern of congealing cold with blood stasis) - Aged 14-35y |
- Having SDM - Having severe primary diseases - Receiving any treatment in the recent 2wk |
NR | Moxibustion (BL23) | NSAIDs (fenbide) | -VAS | 4 m / NR | Chinese |
| 14 | Wan (2022) (40) | NR, 18–30 | 60 (30/30) | - Diagnosed with PDM - Single and non-pregnant female aged 18-30y |
- With primary diseases, irregular menstrual cycles, contraindications of moxibustion - Receiving any treatment in the recent 1 m |
- Diagnosis criteria of PDM in Gynecology in Chinese Medicine - PDM diagnostic criteria by Obstetrics and Gynecology |
Moxibustion (GV14, GV2) | NSAIDs (ibuprofen) | -VAS | 3 m / NR | Chinese |
| 15 | Liu (2019) (41) | NR, 19–27 | 64 (32/32) | - Diagnosed with PDM - VAS > 4 |
- Being pregnant or lactating - With SDM or serious primary diseases - Receiving any treatment in the recent 1 m |
- Diagnosis criteria of PDM in Gynecology in Chinese Medicine | Warn needling (BL32) |
Acupuncture (CV4、SP6, SP8, EX-B8、ST28) | -VAS | 3 m/ NR | Chinese |
| 16 | Liu (2018) (42) | NR, 18–30 | 86 (13/13) | - Non-pregnant female aged 18-30y -With a disease duration 0.5-5y -With regular menstrual cycles |
- With SDM - Having severe primary diseases - Receiving analgesics 24 h prior to treatment |
- Society of Obstetricians and Gynecologists of Canada’s Clinical Guideline of PDM | Moxibustion (lumbosacral and lower abdomen) | NSAIDs (Meloxicam) | -VAS | 3 m / NR | Chinese |
| 17 | Ye (2022) (43) | NR, NR |
74 (37/37) | - With PDM (pattern of congealing cold with blood stasis) - No treatment in the past 30d - Aged 15-35y - Regular menstrual cycles |
- Being pregnant or during lactation - Having injuries or infection in the skin, or psychiatric disorders |
- Chinese Obstetrics and Gynecology (3rd edition) - Obstetrics and Gynecology (8th edition) - Gynecology in Chinese Medicine (10th edition) |
Moxibustion (CV4, CV3, EX-CA1) | NSAIDs (ibuprofen) | - VAS | 3 m / 3 m | Chinese |
| 18 | Wu (2009) (44) | NR, 14–30 | 66 (33/33) | - With PDM (pattern of congealing cold with blood stasis) - women aged 14-30y |
- With SDM - Lactating women with physical or psychiatric disorders - Receiving any related treatment |
- Obstetrics and Gynecology (7th edition) - Clinical Research Guidance for New Drug of Chinese Medicine (1994) - Gynecology in Chinese Medicine (2nd edition) |
Moxibustion (CV4, EX-CA1) | Acupuncture (EX-CA1, CV4) |
- VAS | 3 m / 3 m | Chinese |
| 19 | Tang (2012) (45) | NR, 20–23 | 60 (30/30) | - With PDM (pattern of congealing cold with blood stasis) - Aged 15-30y - VAS ≥ 4 -Regular menstrual cycles 28 ± 7d |
- Being pregnant or during lactation - With primary diseases or chronic infectious diseases - Having received any analgesics or sedatives in the recent 2wks |
- Clinical Research Guidance on New Drug of Chinese Medicine for DM - Obstetrics and Gynecology (7th edition) - Gynecology in Chinese Medicine |
Tuina
(Spine pinching) |
NSAIDs (ibuprofen) | - VAS | 3 m / 1 m | Chinese |
| 20 | Chang (2020) (46) | NR, NR | 90 (45/45) | - With PDM (pattern of congealing cold with blood stasis) - aged 20-45y |
- Being pregnant or during lactation - With primary diseases, infectious diseases, or malignant tumor - Having received any treatment in the recent 3 m |
- Accurate Diagnosis and Coding of Obstetrics and Gynecology Disease - Exploration and Analysis of TCM Differentiation and Treatment of PDM |
Acupuncture (CV6, CV4, SP6, ST29) |
NSAIDs (ibuprofen) | - VAS | 3 m / NR | Chinese |
| 21 | Zhang (2017) (47) | NR, 12–39 | 70 (35/35) | - With PDM | - Being pregnant or during lactation - With SDM, psychiatric disorders, injuries, or infection on the sites for needling - Having taken analgesics treatment |
- Obstetrics and Gynecology - Diagnostic efficacy of standard TCM Syndrome |
Electroacupuncture (LI4, SP10, ST36, CV3, BL26, SP8) |
NSAIDs (ibuprofen) | - VAS | 3 m / 6 m | Chinese |
| 22 | Zhang (2020) (48) | NR, 18–30 | 100 (50/50) | - Non-pregnant female aged 18-30y with PDM -VAS ≥ 4 - With regular menstrual cycles |
- With SDM or severe primary diseases - Receiving contraceptives in recent 1y - Receiving drugs or supplements for fatigue during treatment |
- Obstetrics and Gynecology (6th edition) | Moxibustion (CV4, SP6) | NSAIDs (ibuprofen) | - VAS | 3 m / NR | Chinese |
| 23 | Zhang (2019) (49) | NR, 18–28 | 60 (30/30) | - With PDM (pattern of congealing cold with blood stasis) - With regular menstrual cycles 28 ± 7d - Not receiving analgesics, sedatives or hormonal drugs 2wks prior to treatment |
- Being pregnant or during lactation - With SDM, severe primary diseases, or contraindications of moxibustion - Having received contraceptives, intra-uterine device, or planning to become pregnant within 6 m |
- Clinical Research Guidance on New Drug of Chinese Medicine for DM - Obstetrics and Gynecology |
Moxibustion (CV3, ST36, SP10, SP6, SP8) |
NSAIDs (ibuprofen) | -VAS | 3 m / NR | Chinese |
| 24 | Zhang (2020) (50) | 23.16, 16–35 | 60 (30/30) | - Female aged 12-35y with PDM (pattern of congealing cold with blood stasis) - With regular menstrual period lasting 3-7d with interval of 21-35d - Not received any treatment for PDM in the recent 3 m |
- Being pregnant or during lactation - With severe diseases or psychiatric disorders - Having received contraceptives or intra-uterine device - Being allergic to ginger |
- Obstetrics and Gynecology (9th edition) - Diagnostic efficacy of standard TCM Syndrome (2017) - Gynecology in Chinese Medicine |
Moxibustion (BL31, BL32, BL 33, BL34) | Acupuncture (CV3, SP6, SP8, BL32, EX-B8, CV4, ST29) | - VAS | 3 m / 3 m | Chinese |
| 25 | Peng (2012) (51) | NR, 18–30 | 60 (30/30) | - Single female aged 18-35y with PDM | - With severe diseases, contraindications of ibuprofen/acupuncture | - Diagnostic efficacy of standard TCM Syndrome | Acupuncture (SP8, KI5) | NSAIDs (ibuprofen) | - VAS | 3 m / NR | Chinese |
| 26 | Cao (2011) (52) | NR, 15–28 | 60 (30/30) | - Non-pregnant female aged 15-35y with PDM - VAS ≥ 4 - With a 6-12 m disease duration -Regular menstrual cycles 28 ± 7 days |
- With SDM, severe primary diseases, or contraindications of acupuncture - Having received any treatment for PDM within 1 m |
- Society of Obstetricians and Gynecologists of Canada’s Clinical Guideline of PDM - Clinical Research Guidance for New Drug of Chinese Medicine - Gynecology in Chinese Medicine |
Acupuncture (EX-B8, BL32, SP8) | NSAIDs (ibuprofen) | - VAS | 3 m / 3 m | Chinese |
| 27 | Cao (2014) (53) | NR, 16–27 | 62 (31/31) | - With PDM for more than 3 consecutive menstrual cycles - Aged 16-35y - With regular menstrual cycles 28 ± 7 days |
- With SDM or severe diseases - Medical staffs participating in this study - having received any treatment in the recent 15d |
- Clinical Research of TCM Gynecology - Therapy of Acupuncture and Moxibustion Course - Obstetrics and Gynecology - Chinese Obstetrics and Gynecology |
Acupuncture (BL54, ST28) | NSAIDs (ibuprofen) | - VAS | 3 m / NR | Chinese |
| 28 | Zhu (2020) (54) | NR, NR | 60 (27/33) | - VAS ≥ 6 - Non-pregnant female aged 18-35y |
-With severe diseases or SDM - With DM due to sacroiliac joint dislocation -Receive any treatment for DM in the recent 1 m |
NR |
Tuina
(rubbing, kneading, trembling, pushing, grasping) |
Acupuncture (CV3, SP8, ST29, BL32, CV4, EX-B8, SP6) | - VAS | 3 m / NR | Chinese |
| 29 | Zhu (2015) (55) | NR, NR | 66 (33/33) | - Non-pregnant female aged 16-28y with PDM - With regular menstrual cycles 28 ± 7d |
- With SDM - During lactation - With severe diseases - Having received analgesics or hormonal drugs in the recent 2 wks |
- Obstetrics and Gynecology (6th edition) - Clinical Research Guidance on New Drug of Chinese Medicine for DM (1993) |
Acupuncture (CV4, CV6, CV12, CV10, KI13, EX-CA1) |
NSAIDs (ibuprofen) | -VAS | 3 m / 1 m | Chinese |
| 30 | Li (2014) (56) | NR, NR | 20 (10/10) | - Nonpregnant female aged 19-30y with PDM - VAS ≥ 4 / CMSS ≥10 - With regular menstrual cycles 28 ± 7d and feel pain within 48 h of menstruation |
- With other diseases - With previous experience of needling - Having received any analgesics in 1wk prior to treatment |
- Guidelines for Clinical Research on New Chinese Medicines for DM - Obstetrics and Gynecology |
Acupuncture (SP6) | Sham acupuncture (SP6) | -VAS | 8 min / NR | Chinese |
| 31 | Li (2017) (57) | 19, 18–20 | 70 (35/35) | - Women aged18-45y with PDM - regular menstrual cycles 28 ± 7 days - Not received any other treatment |
- With SDM, severe physical, or psychiatric disorders - Being pregnant or during lactation |
- Criteria for Diagnosis and Treatment of TCM Syndrome - Obstetrics and Gynecology |
Auricular therapy (TF2, CO18, TF4, CO12) |
NSAIDs (ibuprofen) | - VAS | 3 m / NR | Chinese |
| 32 | Lin (2019) (58) | NR, NR | 62 (30/32) | - Women aged18-30y - With PDM (pattern of congealing cold with blood stasis) - With regular menstrual cycles 28 ± 7d |
- With severe primary diseases or psychiatric disorders - Having received any treatment for PDM in the recent 1 m |
- Society of Obstetricians and Gynecologists of Canada’s Clinical Guideline of PDM - Diagnostic and Curative Criteria for Gynecological Diseases in TCM |
Acupuncture (SP6, CV4, GV4, CV3, SP6, BL23) | NSAIDs (ibuprofen) | - VAS | 3 m / 3 m | Chinese |
| 33 | Lin (2020) (59) | NR, NR | 110 (55/55) | - Women aged15-35y with PDM -Regular menstrual cycles 28 ± 7 days |
- Being pregnant or during lactation - With SDM, severe primary diseases, or psychiatric disorders - Having receive any treatment in the recent 1 m |
- Obstetrics and Gynecology - Gynecology in Chinese Medicine |
Warm needling (EX-CA1, CV4, ST36, SP6) |
NSAIDs (ibuprofen) | - NRS | 3 m / NR | Chinese |
| 34 | Lin (2020) (60) | NR, 19–32 | 66 (33/33) | - Nonpregnant female aged 18-35y with PDM - Regular menstrual cycles 28 ± 7 days |
- With primary diseases or infection - Having received contraceptives or intra-uterine device - Once received endocrine-related medication or injection |
- Clinical Research Guidance for New Drug of Chinese Medicine - Obstetrics and Gynecology (8th edition) - Gynecology in Chinese Medicine |
Warm needling (EX-B8, GV14, BL17) |
NSAIDs (fenbide) | - VAS | 3 m / 3 m | Chinese |
| 35 | Liang (2021) (61) | NR, NR | 60 (30/30) | - Nonpregnant female aged 16-32y with PDM -VAS ≥ 4 - Menarche over 2y with regular menstrual cycles 28 ± 7 days - Abdominal pain in the period |
- With contraindications of ibuprofen - With severe primary diseases and hypertension - Receive any treatment for DM |
- Obstetrics and Gynecology (8th edition) - Gynecology in Chinese Medicine (9th edition) - Clinical Research Guidance for New Drug of Chinese Medicine |
Moxibustion (CV8) | NSAIDs (ibuprofen) | - VAS | 3 m / 3 m | Chinese |
| 36 | Fan (2014) (62) | NR, 18–35 | 60 (30/30) | - Women aged 18-35y with PDM (pattern of congealing cold with blood stasis) - VAS ≥ 4 - Regular menstrual cycles 28 ± 7 d |
- Being pregnant or during lactation - With SDM, severe primary diseases, psychiatric disorders, or contraindications of moxibustion - Received drugs for DM in the recent 2wks |
- Clinical Research Guidance for New Drug of Chinese Medicine - Diagnostic efficacy of standard TCM Syndrome |
Moxibustion (CV4, CA7) | Acupuncture (CV4, CA7) | - VAS | 3 m / 3 m | Chinese |
| 37 | Tang (2015) (63) | NR, 18–27 | 60 (30/30) | - Regular menstrual cycles 28 ± 7 days with PDM | - With severe primary diseases or psychiatric disorders - Taking analgesics before or during treatment |
- Clinical Research Guidance for New Drug of Chinese Medicine - Obstetrics and Gynecology |
Acupuncture (SP6, SP8, CV4, LI4) |
NSAIDs (ibuprofen) | - VAS | 3–6 m / NR | Chinese |
| 38 | Wen (2021) (64) | NR, 17–34 | 60 (30/30) | - Women aged16-35y - With PDM (pattern of congealing cold/ qi stagnation with blood stasis) -regular menstrual cycles 28 ± 7 d |
-With SDM, bleeding tendencies, or coagulation disorders - Having received any treatment for PDM in the recent 3 m |
- Gynecology in Chinese Medicine - Diagnosis of Obstetrics and Gynecology Diseases |
Acupuncture (LR3, BL18, LR6, CV4) | NSAIDs (ibuprofen) | -VAS | 3 m / 3 m | Chinese |
| 39 | Wang (2019) (65) | 25.26, 15–35 | 60 (30/30) | - Women aged18-35y with PDM - Not received any treatment in the recent 1 m |
- Being pregnant or lactation - With irregular menstrual cycles - With severe primary disease - Having received analgesics or hormonal drugs |
- Obstetrics and Gynecology (8th edition) - Criteria for Diagnosis and Treatment of TCM Syndrome |
Acupuncture (CV12, CV10, CV6, CV4, ST24, ST26, GB31) | NSAIDs (ibuprofen) | - VAS | 3 m / 3 m | Chinese |
| 40 | Wang (2018) (66) | NR, NR | 120 (60/60) | - Women aged 15-28y - VAS ≥ 4 - With regular menstrual cycles - Not received medicine in the recent 1wk |
- Being pregnant or during lactation - With SDM, severe primary diseases, psychiatric disorders, pelvic inflammation, or organic disorders - Using other intervention for DM |
- Obstetrics and Gynecology - Guidelines for Clinical Research on New Chinese Medicines for DM - Diagnostic efficacy of standard TCM Syndrome |
Moxibustion (CV4, SP6, BL32) |
NSAIDs (ibuprofen) | - VAS | 3 m / NR | Chinese |
| 41 | Bai (2018) (67) | NR, 16–33 | 80 (40/40) | - With PDM (pattern of congealing cold with blood stasis) -VAS ≥ 4 - Regular menstrual cycles 28 ± 7 d |
- Being pregnant or during lactation -With SDM -With serious medical diseases |
- Obstetrics and Gynecology - Therapy of Acupuncture and Moxibustion Course |
Moxibustion (BL31, BL32, BL33, BL34) | NSAIDs (ibuprofen) | - VAS | 3 m / NR | Chinese |
| 42 | Sheng (2019) (68) | NR, NR | 72 (36/36) | - Women aged 16-35y with PDM - With regular menstrual period of 3-7d with an interval of 21-35d - Not receive analgesics, sedatives or hormonal drugs prior to treatment |
- Being pregnant or during lactation - With SDM, severe primary diseases, or contraindications of acupuncture - Receiving PDM medicine or intra-uterine devices - Having received oral prostaglandin synthase inhibitors within 2wks |
- Evidence-based Clinical Practice Guideline of Acupuncture and Moxibustion for PDM - Gynecology in Chinese Medicine - Criteria for Diagnosis and Treatment of TCM Symptom |
Acupuncture (SP8, EX-B8, SP6, BL32, EPC6) | NSAIDs (ibuprofen) | - VAS | 3 m / 3 m | Chinese |
| 43 | Shi (2022) (69) | NR, 19–28 | 60 (30/30) | - With PDM of cold damp pattern - Nonpregnant female aged 16-28y - With regular menstrual cycles 28 ± 7 |
- With SDM, serious diseases of vital organs, blood and circulatory systems, or psychiatric disorders - Having received analgesics in the recent 2 m |
- Obstetrics and Gynecology (9th edition) - Clinical Research Guidance for New Drug of Chinese Medicine |
Scraping therapy (GV4, EX-B8, CV6, CV2) | NSAIDs (ibuprofen) | - NRS | 3 m / NR | Chinese |
| 44 | Shi (2017) (70) | NR, NR | 44 (22/22) | - With PDM (pattern of congealing cold with blood stasis) - Nonpregnant female aged 18-35y - VAS = 5–9 - With regular menstrual cycles 21-35d - Disease duration ≥3 m |
- With SDM, prolonged illness, weakness, emaciation, or severe diseases - Injuries or infection on the sites for acupuncture - Having received any treatment in the recent 1 m |
- Obstetrics and Gynecology (8th edition) - Gynecology in Chinese Medicine |
Acupuncture (CV6, CV4, SP6) | NSAIDs (ibuprofen) | - VAS | 3 m / NR | Chinese |
| 45 | Lou (2020) (71) | NR, NR | 60 (30/30) | - With PDM (pattern of congealing cold with blood stasis) - Single and nonpregnant female aged 16-35y - With regular menstrual cycles 28 ± 7d |
- With SDM, organic disorders, or psychiatric disorders - With contraindications to ibuprofen or acupuncture - Having received any treatment in the recent 1 m |
- Obstetrics and Gynecology (7th edition) - Diagnostic efficacy of standard TCM Syndrome - Gynecology in Chinese Medicine (2nd edition) |
Acupressure (FV, CV, BV, CV6, EX-CA1, SP10, ST34, ST36, SP6) | NSAIDs (ibuprofen) | - VAS | 3 m / NR | Chinese |
| 46 | Zhai (2020) (72) | NR, 18–30 | 78 (39/39) | - Nonpregnant female aged 18-30y with PDM - VAS > 2 - With regular menstrual cycles 28 ± 7d - Not received any treatment for PDM |
- Being pregnant, in lactation - once experienced miscarriage and stillbirth - With severe primary diseases or psychiatric disorders -Having taken analgesics in the recent 24 h |
NR | Acupressure (carpus-ankle) |
Sham acupressure | - VAS | 30 min / NR | Chinese |
| 47 | Xiao (2016) (73) | NR, 12–30 | 60 (30/30) | - With PDM (pattern of congealing cold/ qi stagnation with blood stasis) -Nonpregnant female aged 12-30y |
- With SDM, severe primary diseases, or psychiatric disorders - having received contraceptives, intra-uterine device, or planning to become pregnant |
- Gynecology in Chinese Medicine - Obstetrics and Gynecology |
Acupuncture (ST25, ST26, ST27, ST28, CV4, CV3) | NSAIDs (ibuprofen) | -VAS | 3 m / 3 m | Chinese |
| 48 | Fan (2021) (74) | NR, 18–35 | 60 (30/30) | - nonpregnant or nonlactating women aged 18-35y with PDM (pattern of congealing cold/ qi stagnation with blood stasis) - with regular menstrual cycles 28 ± 7d |
- with severe primary diseases or contraindications of moxibustion - having received contraceptives or intra-uterine device - having received any treatment in the recent 1 m |
- Society of Obstetricians and Gynecologists of Canada’s Clinical Guideline of PDM - Gynecology in Chinese Medicine |
Moxibustion (CV6, CV4, ST36) |
NSAIDs (ibuprofen) | - VAS | 3 m / 3 m | Chinese |
| 49 | Jia (2017) (75) | NR, NR | 120 (60/60) | - female aged 16-30y with PDM - VAS > 3 - With regular menstrual period of 3-7d and an interval of 21-35d - Not received analgesics, sedatives or hormonal drugs in the recent 1wk |
- Being pregnant or during lactation - With SDM, severe primary diseases, psychiatric disorders, or contraindications of acupuncture - Using intra-uterine device and medicine for DM in the recent 1 m |
- Evidence-based Clinical Practice Guideline of Acupuncture and Moxibustion for PDM - Gynecology in Chinese Medicine (7th edition) |
Acupuncture (SP8, EX-B8, SP6, BL32, PC6) |
NSAIDs (ibuprofen) | - VAS | 6 m / NR | Chinese |
| 50 | Hao (2018) (76) | NR, 16–35 | 60 (30/30) | - Female aged 15-35y with PDM - VAS ≥ 3 -With regular menstrual cycles 28 ± 7d |
- Being pregnant or during lactation - With SDM, severe primary diseases, psychiatric disorders, or contraindications of acupuncture |
- Obstetrics and Gynecology - Gynecology in Chinese Medicine |
Acupuncture (SP6, ST36, LI4, PC6, RN8) |
NSAIDs (ibuprofen) | -VAS | 3 m / NR | Chinese |
| 51 | Guo (2021) (77) | NR, NR | 82 (41/41) | - With PDM (pattern of congealing cold with blood stasis) - Aged 15-35y - VAS ≥ 6 |
- Being pregnant or during lactation - With SDM, severe diseases, and contraindications to moxibustion - Having received treatment for DM in the recent 2 m |
- Obstetrics and Gynecology - Gynecology in Chinese Medicine |
Moxibustion (CV8, CV2, CV4, CV6, ST36) |
NSAIDs (ibuprofen) | - VAS | 3 m / 1 m | Chinese |
| 52 | Zhong (2017) (78) | NR, NR | 64 (33/31) | - Female with PDM (pattern of congealing cold with blood stasis) - Menarche over 1y |
- With severe primary diseases or psychiatric disorders | NR | Warm needling (CV4, ST29, SP6) |
NSAIDs (Ibuprofen) | - VAS | 3 m / NR | Chinese |
| 53 | Chen (2011) (79) | NR, NR | 60 (30/30) | - Single and nonpregnant female aged 15-32y with PDM 6 m-15y - VAS ≥ 4 - with regular menstrual cycles 28 ± 7d |
- With SDM, severe primary diseases, or organic disorders - with contraindication of aspirin - having received any analgesics in the recent 24 h |
- Society of Obstetricians and Gynecologists of Canada’s Clinical Guideline of PDM - Diagnostic efficacy of standard TCM Syndrome |
Acupressure (CV6, CV4, ST25, SP8) |
NSAIDs (ibuprofen) | - VAS | 3 m / NR | Chinese |
| 54 | Chen (2014) (80) | NR, NR | 80 (40/40) | - With PDM - Not receive analgesics or hormonal drugs 3 m prior to treatment |
- With SDM, severe primary diseases, or drugs allergy | -Diagnostic efficacy of standard TCM Syndrome | Acupuncture (SP8, CV3, SP6, KI3) | NSAIDs (ibuprofen) | -VAS | 3 m / NR | Chinese |
| 55 | Chen (2022) (81) | NR, 20–28 | 42 (21/21) | - Nonpregnant female aged 18-30y with PDM - VAS ≥ 4 - with regular menstrual cycles 28 ± 7d |
- With SDM, severe primary diseases, or contraindications to magnetic resonance imaging - Having taken medicine1m prior to treatment |
- Society of Obstetricians and Gynecologists of Canada’s No.345 PDM Consensus Guideline | Acupuncture (SP6, CV4) | Waitlist | - VAS | 3 m / NR | Chinese |
| 56 | Han (2015) (82) | NR, NR | 60 (30/30) | - Nonpregnant female aged 19-24y with PDM - VAS ≥ 4 - CMSS ≥1 - with regular menstrual cycles 28 ± 7d |
- Being pregnant or during lactation - With severe primary diseases or psychiatric disorders - Medical staff participating in this study - Having received acupuncture or analgesics 1wk prior to treatment |
- Clinical Research Guidance for New Drug of Chinese Medicine - Obstetrics and Gynecology |
Acupuncture (SP6) | Sham acupuncture (SP6) | - VAS | 3 m / NR | Chinese |
| 57 | Wei (2019) (83) | NR, NR | 86 (43/43) | - Nonpregnant female aged 18-30y with PDM - VAS ≥ 4 - disease duration ≥3 m |
- With SDM, irregular menstrual cycles, severe primary diseases, or contraindications of ibuprofen/acupuncture | - Obstetrics and Gynecology - Clinical Research Guidance for New Drug of Chinese Medicine |
Acupuncture (BL31, BL32, BL33, BL34) | NSAIDs (ibuprofen) | - VAS | 3 m / 3 m | Chinese |
Characteristics of the included studies.
I, intervention group; C, control group; NSAID, nonsteroidal anti-inflammatory drug; VAS, visual analogue scale; NR, not reported; PDM, primary dysmenorrhea: SDM, secondary dysmenorrhea; DM, dysmenorrhea; VMSS, verbal multidimensional scoring; COC, combined oral contraceptive pill; PGSI, prostaglandin synthetase inhibitor; CMSS, Cox menstrual symptom scale; MPQ, McGill pain questionnaire; BPI, brief pain inventory; TCM, traditional Chinese medicine.
3.3 Risk of bias
Figure 2 presents a summary of the methodological quality of the included studies. Thirty-two RCTs were rated as low risk of bias (28, 31, 33, 34, 36, 39–43, 46, 47, 49, 51, 56, 59, 61–66). Nineteen studies were rated as high risk of bias due to the application of inappropriate data analysis methods (27, 29, 30, 32, 45, 48, 50, 54, 55, 57, 58, 60, 68, 71, 72, 81, 83) or unblinding of the outcome assessors (35, 81). The remaining six studies were rated as having certain concerns because of the insufficient information on data analysis methods (37, 38, 44, 52, 53, 77) or the high dropout rate (57, 75).
Figure 2
Summary of risk of bias (RoB) of the included studies.
3.4 Network diagram
A network diagram was drawn based on 15 interventions, including 3,903 participants. A total of 105 pairs of comparisons were formed (including 18 pairs of direct comparisons and 87 pairs of indirect comparisons). Nineteen RCTs reported a comparison between acupuncture and NSAIDs, and 12 RCTs reported the comparison between moxibustion and NSAIDs. Direct comparisons between 9 pairs of comparisons occurred only once. Among these interventions, NSAIDs had the largest sample size (n = 1,426), followed by acupuncture (n = 865), moxibustion (n = 651), and warm needling (n = 151). The data are shown in Figure 3. (Supplementary Appendix 3).
Figure 3
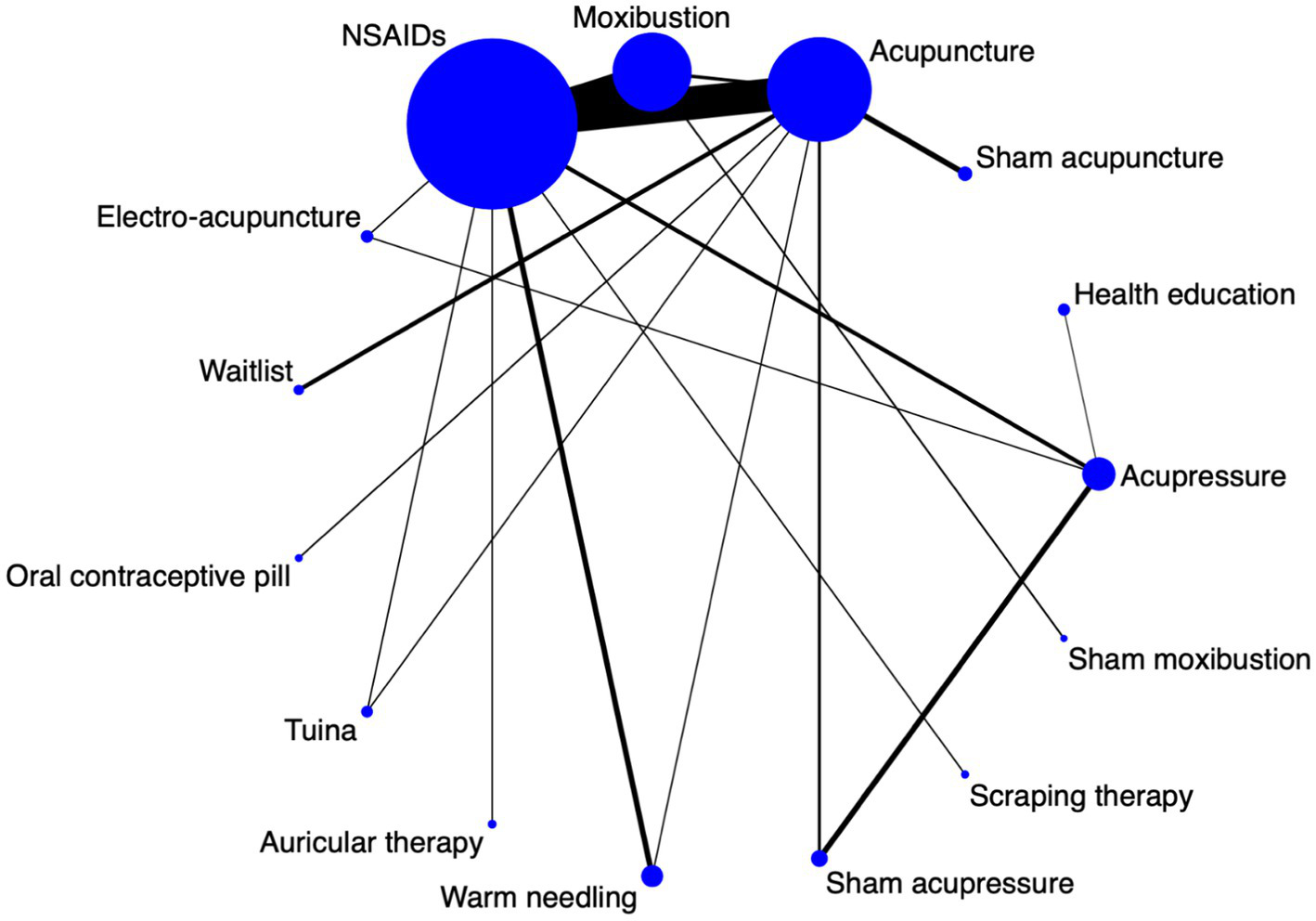
A network diagram for all interventions.
3.5 Heterogeneity and inconsistency test
Conceptual heterogeneity and inconsistency were low across the network given that all the included studies had the same study design, participants, and outcomes. Statistical heterogeneity was high in several pairwise comparisons (Supplementary Appendix 4). Supplementary Appendix 5 shows the detailed information on the local inconsistency test. A node-splitting test was conducted for local inconsistency analysis, and 19 pairs of mixed comparisons (including direct and indirect) were analyzed. The results showed no statistical inconsistency in each pair of direct comparison. Sensitivity analysis indicated that the findings were robust (Supplementary Appendix 6).
3.6 NMA
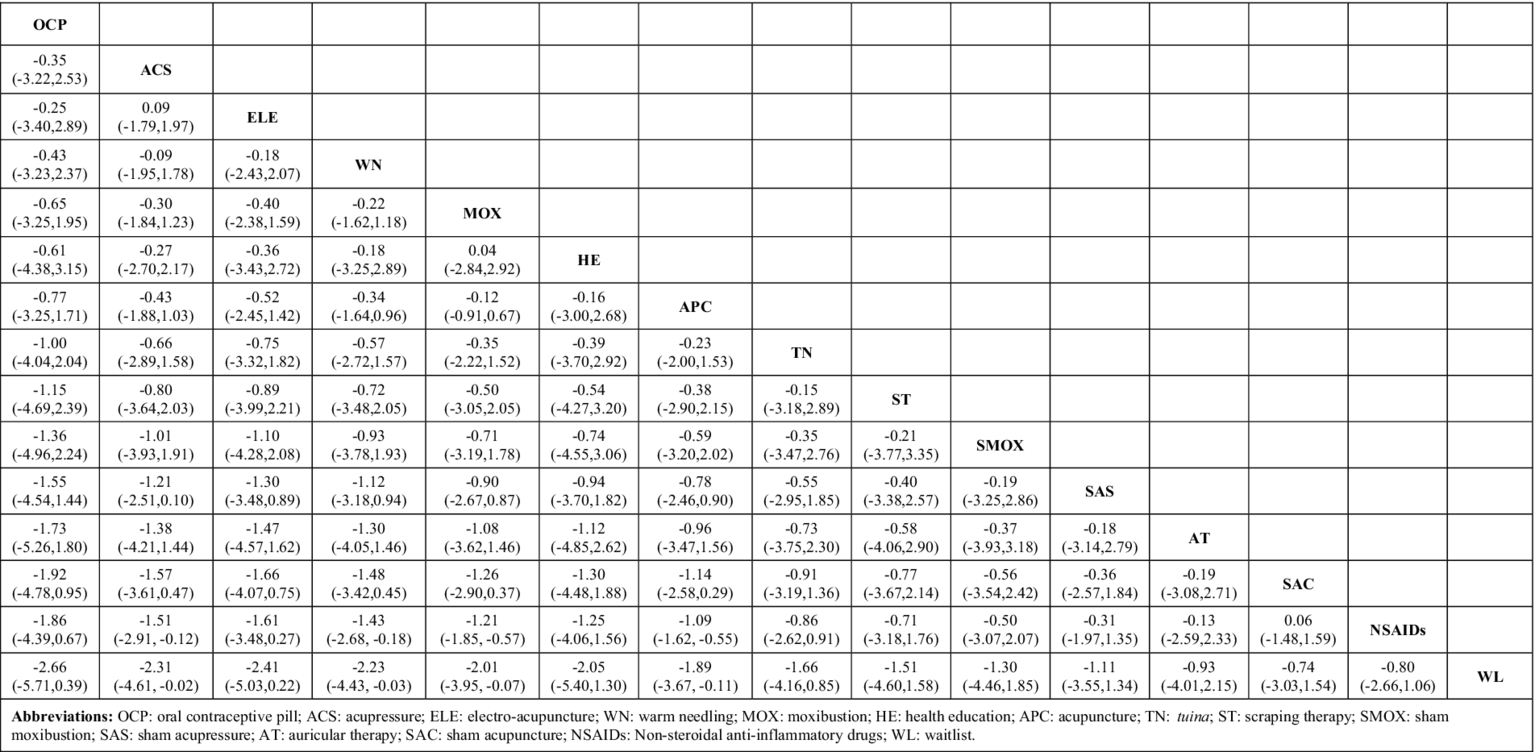
As shown in Figure 4, the estimated effect of the NMA for each intervention on relieving PD pain was generated. Compared with NSAIDs and waitlist, significantly better effects were found in acupressure [SMD = −1.51, 95% CI (−2.91, −0.12)/SMD = −2.31, 95% CI (−4.61, −0.02)], warm needling [SMD = −1.43, 95% CI (−2.68, −0.18)/SMD = −2.23, 95% CI (−4.43, −0.03)], moxibustion [SMD = −1.21, 95% CI (−1.85, −0.57)/SMD = −2.10, 95% CI (−3.95, −0.07)], and acupuncture [SMD = −1.09, 95% CI (−1.62, −0.55)/SMD = −1.89, 95% CI (−3.67, −0.11)].
Figure 4
The network meta-analysis for all interventions.
3.7 Probability ranking
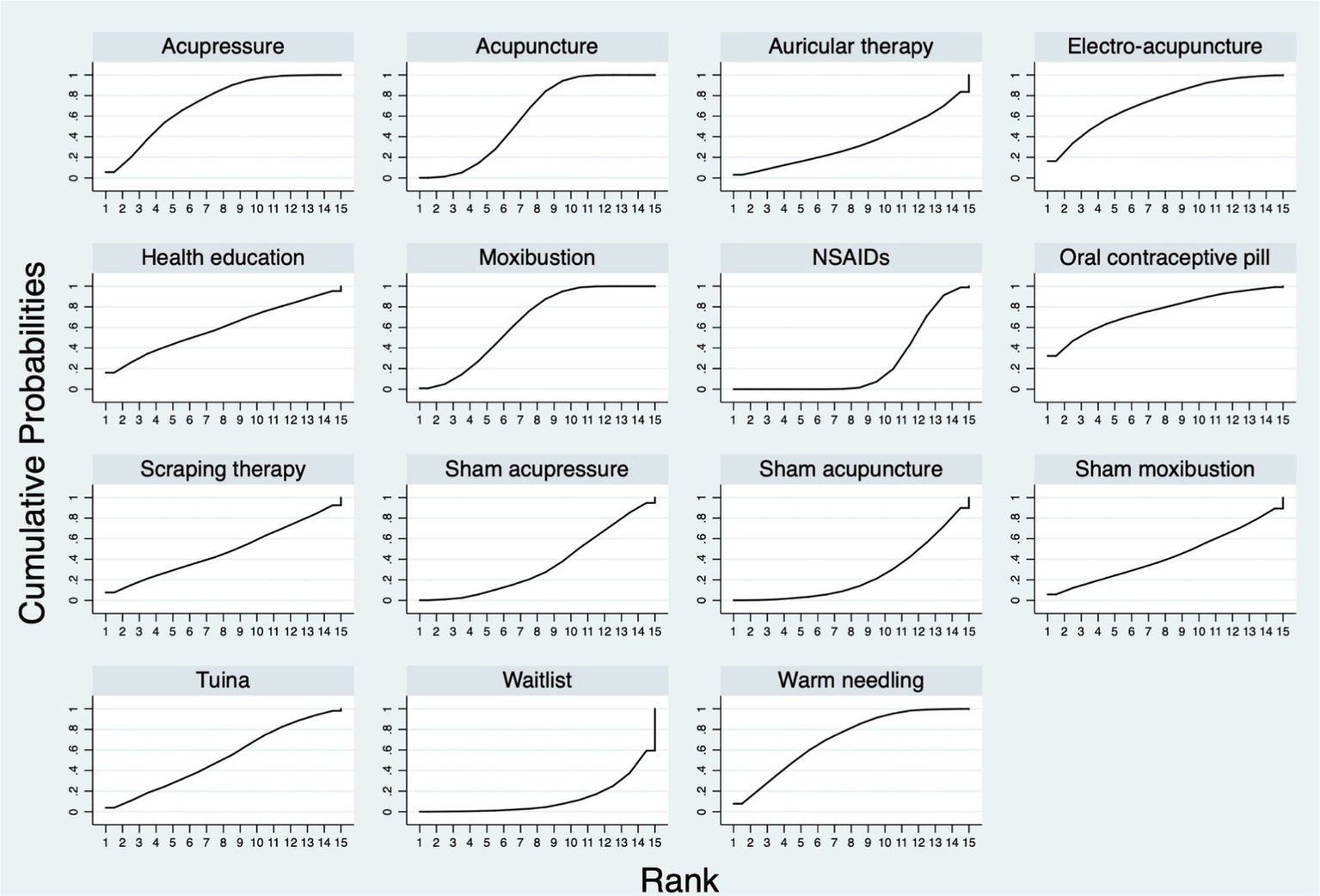
Figure 5 shows the SUCRA probability ranking for the different treatment effects of all interventions. For the 15 interventions, the SUCRA value predicted the possibility of different interventions as the best treatment on the management of PD pain, and the ranking was as follows: oral contraceptive pill (75.8%), electro-acupuncture (73.0%), acupressure (72.9%), warm needling (70.6%), moxibustion (64.9%), acupuncture (60.0%), health education (59.7%), tuina (52.3%), scarping therapy (48.0%), sham moxibustion (43.1%), sham acupressure (34.8%), auricular therapy (34.1%), sham acupuncture (24.9%), NSAIDs (23.9%), and waitlist (12.1%).
Figure 5
The probability ranking for all the interventions.
3.8 Safety
Information on the safety of different interventions was collected and assessed based on adverse events reported in RCTs. Nineteen RCTs reported adverse events on acupuncture, warm needling, NSAIDs, and sham acupressure. For acupuncture and warm needling, adverse events included local bleeding or hematoncus (8 RCTs) (36, 37, 51, 53, 58, 60, 68, 73), headache or myalgia (1 RCT) (36), fever (1 RCT) (36), nausea (1 RCT) (46), and nervousness in the first treatment session (1 RCT) (71). Adverse events of NSAIDs incorporated gastrointestinal symptoms (13 RCTs) (36, 37, 46, 48, 51–53, 65, 68, 69, 73, 75, 83), vaginal bleeding (1 RCT) (36), weight gain (1 RCT) (36), breast engorgement (1 RCT) (36), hypermenorrhea (1 RCT) (48), rash (1 RCT) (52), and dizziness and tinnitus (3 RCTs) (68, 73, 83). An RCT also reported that the analgesic effect of medication faded away with repetitive use in some cases (31). An RCT mentioned that 3 participants dropped out from the sham acupressure control group due to severe pain (30, 72), whereas another RCT reported that 2 participants dropped out from the sham acupressure group without providing the specific reasons (30). Details on the adverse events of the interventions are in Supplementary Appendix 7.
3.9 Certainty of evidence
The evidence quality of all 18 comparisons was evaluated by GRADEpro. High-quality evidence was found in two comparisons on PD pain symptoms, namely, acupuncture versus placebo and electroacupuncture versus NSAIDs. The evidence quality was evaluated as moderate in six comparisons: acupressure versus placebo, moxibustion versus NSAIDs, moxibustion versus acupuncture, tunia versus acupuncture, warm needling versus NSAIDs, and scraping therapy versus NSAIDs. The evidence quality of the rest of the 10 comparisons was evaluated as low or very low. The most common reason for downgrading the evidence quality was imprecision, followed by high heterogeneity and high risk of bias. Details of the SoF table are in Supplementary Appendix 8.
3.10 Publication bias
The publication bias is shown in Appendix 9. The results showed that the studies were roughly symmetrical around the center line. Egger’s test (p = 0.162) showed no significant risk of publication bias as well.
4 Discussion
Numerous clinical trials and systematic reviews have investigated the effects of meridian-based TCM interventions for PD pain and suggested that these interventions can reduce PD pain intensity, duration, and related symptoms, with relatively few adverse events. However, this work is the first study to quantitatively summarize and compare the effects of the meridian-based TCM interventions via NMA. In PD pain management, the effects of acupressure, acupuncture, and moxibustion were superior to those of NSAIDs and waitlist; acupressure was more effective than placebo; and warm needling was superior to both NSAIDs and waitlist.
Previous reviews have evaluated the effects of meridian-based TCM interventions for PD pain and found similar results to this study. A systematic review of acupuncture-related therapies (acupuncture, acupoint injection, acupressure, and moxibustion) for PD indicated that acupuncture was significantly more effective than placebo (WMD = −0.57, 95% CI [−0.76, −0.38]) and NSAIDs (WMD = −0.19, 95% CI [−0.37, −0.01]) in PD pain management, and acupressure was more effective than placebo (WMD = −0.91, 95% CI [−1.78, −0.04]). Nevertheless, the reliability of their review may be compromised because it included a combination of randomized and non-randomized trials with fewer interventions, trials, and comparisons. Moreover, most of the studies included were deemed low in methodology (84). Another systematic review on the effects and safety of acupuncture and moxibustion for PD demonstrated that acupuncture (MD = −1.93; 95% CI [−2.80, −1.06]) and moxibustion (MD = −2.67; 95% CI [−4.96, −0.38]) are more effective in managing PD pain than the control via VAS; however, the review combined all control interventions as one for their meta-analysis (85). Similarly, Jiang et al. conducted a systematic review of RCTs on acupressure for PD and reported that acupressure is better at improving pain with VAS compared with placebo or waitlist (MD: −1.41, 95% CI [−1.61, −1.21]), but the study found no difference in pain relief between acupressure and NSAIDs. This discrepancy may be due to the small number of RCTs with modest sample included, which hindered the detection of treatment effects in their systematic review (86). The present study’s findings suggested that electroacupuncture may be an optimal intervention strategy for PD pain; however, direct comparisons among interventions were few based on a limited number of studies.
For safety issues, the current study provided evidence that meridian-based TCM interventions are safe with no severe adverse events for the treatment of PD, and the reported adverse events focused on acupuncture and warm needling. These results were in accordance with previous studies (33, 84, 85). Fainting, hematoma or bleeding, sticking of needle, and needling sensation after acupuncture are common situations during acupuncture treatment in clinics or research (87). These situations might be related to irregular acupressure practice of practitioners, participants’ mental and physical conditions, and participant–practitioner interactions (88). All the abovementioned adverse events are mild and can be handled well under appropriate management. A systematic review examining the adverse events of meridian-based TCM interventions between 2000 and 2011 (117 studies, 25 countries, and 294 cases with adverse events in acupuncture) emphasized the significance of acupuncture practice guidelines (89). Therefore, to minimize adverse events, practitioners should strictly follow the operation guidelines, observe the situation of patients, and communicate with them actively during acupuncture treatment. Standard reporting form can be adopted in future studies to systematically document the occurrence and severity of AE (90).
The good statistical consistency observed in the NMA suggested that the variation in the treatment effects of the meridian-based TCM interventions is predictable and not due to chance (91). However, the statistical heterogeneity in the pairwise comparisons within the NMA is high. Several appropriate statistical methods were applied to identify the sources of heterogeneity. Sensitivity analysis indicated the robustness of the overall results of the meta-analysis (92). Publication bias was suggested from the funnel plot and Egger’s test. Considering that the overall methodological quality of the included studies was high, the high statistical heterogeneity observed in the pairwise comparisons could be attributed to the variability in sample size or the different durations of intervention among various studies (93). The heterogeneity may also arise from differences in demographic characteristic of participants with PD among the study populations (94). Future systematic reviews may limit the age range of the participants, define the optimal information size (for example, 400 as suggested by GRADEpro handbook) (95), and set the treatment duration and frequency. Special attention should be paid to the clinical trials with a large effect size but a small sample size (96, 97).
For the quality of methodology of the included studies, factors that led to high risk of bias included the application of inappropriate data analysis methods, unblinding of the outcome assessors, insufficient information on data analysis methods, and high dropout rate. The factors that rated down the evidence quality of this study by GRADEpro contained imprecision, high heterogeneity, and risk of bias. Further RCTs should give particular emphasis on these several domains, applying the intention-to-treat approach for data analysis to eliminate or reduce bias in treatment effects arising from missing data (98), blinging the outcome assessors to reduce detection bias (99), reporting the results completely to avoid selective reporting bias (e.g., selective outcome reporting, selective analysis reporting, and lack of reporting of adverse events and dropout reasons) (100), and making sure that the sample size has the power to demonstrate the smallest effect of intervention (101).
4.1 Implication
The findings of this study can implicate PD patients, healthcare providers, researchers, and policy makers. The study provides a potential ranking of the effects of multiple interventions (e.g., meridian-based TCM interventions and conventional western medicine) for relieving PD pain, as well as their adverse events. The information could be a reference for PD patients when choosing interventions. Health care providers may use the findings to inform their clinical decisions and improve patient outcomes. Researchers may find some research gaps from the findings. For example, the results indicated that acupressure, moxibustion, and warm needling may also have significant effects on PD pain, but relevant evidence is very limited. More clinical trials can be conducted to examine their effects on PD pain management. Researchers could further explore the effects of meridian-based TCM interventions on other outcomes in patients with PD. Policy makers in the field of women’s health may focus on the safety and potential effects of meridian-based TCM interventions and highlight the importance of integrating these interventions into clinical practice guidelines and health care policies.
4.2 Strength
The present study has several strengths. First, the study strictly defined the inclusion criteria, and the overall methodological quality of the included studies was high. Second, we limited the outcome as PD pain, providing a clear and specific research question that allowed for a focused assessment of the current evidence. Third, evidence of both effects and adverse events was collected, enabling readers to obtain knowledge of meridian-based TCM interventions on PD pain. Additionally, the review included studies published in both English and Chinese, which increased the generalizability of the findings and avoided potential language bias.
4.3 Limitation
Several limitations of this study should be acknowledged. First, as a result of the diversity of intervention types, the number of studies using the same interventions in some direct comparisons was relatively small. Besides, the duration of the interventions varied across the included studies, which may affect the effects of the interventions. These factors may subsequently influence the reliability of the findings. Second, the study only focused on the severity of PD pain as the sole outcome. Evidence on the effects of meridian-related interventions on other associated symptoms such as menstrual blood flow, sleep quality, and mood was not reviewed. Lastly, the statistical heterogeneity observed among different comparisons was high, suggesting the presence of substantial variability in the results and limiting the generalizability of the findings.
5 Conclusion
For the management of PD pain, the effects of acupressure, acupuncture, warm needling, and moxibustion were superior to those of NSAIDs and waitlist. Furthermore, based on probability ranking, oral contraceptive pill, electro-acupuncture, acupressure, and warm needling demonstrated higher probabilities of being better interventions. Meridian-based TCM interventions are safe, and no severe related adverse events were detected. More high-quality clinical trials are needed to provide more robust evidence of this NMA.
Statements
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
Author contributions
S-CC: Conceptualization, Formal analysis, Methodology, Writing – original draft. J-YR: Methodology, Writing – review & editing. BZ: Formal analysis, Writing – original draft. L-YP: Formal analysis, Writing – original draft. LZ: Writing – review & editing. S-LL: Formal analysis, Writing – original draft. K-PW: Writing – review & editing. H-XO: Writing – review & editing. W-FY: Writing – review & editing. Q-WF: Conceptualization, Writing – review & editing. B-QC: Writing – review & editing, Conceptualization.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1453609/full#supplementary-material
References
1.
Dawood MY . Primary dysmenorrhea: advances in pathogenesis and management. Obstetr Gynecol. (2006) 108:428–41. doi: 10.1097/01.AOG.0000230214.26638.0c
2.
Proctor M Farquhar C . Diagnosis and management of dysmenorrhoea. BMJ. (2006) 332:1134–8. doi: 10.1136/bmj.332.7550.1134
3.
Polat A Celik H Gurates B Kaya D Nalbant M Kavak E et al . Prevalence of primary dysmenorrhea in young adult female university students. Arch Gynecol Obstet. (2009) 279:527–32. doi: 10.1007/s00404-008-0750-0
4.
Akshatha K Shilpa D . Dysmenorrhoea. Obst Gynaecol Reprod Med. (2019) 29:286–91. doi: 10.1016/j.ogrm.2019.06.002
5.
Daniels S Robbins J West CR Nemeth MA . Celecoxib in the treatment of primary dysmenorrhea: results from two randomized, double-blind, active- and placebo-controlled, crossover studies. Clin Ther. (2009) 31:1192–208. doi: 10.1016/j.clinthera.2009.06.003
6.
Marjoribanks J Proctor ML Farquhar C . Nonsteroidal anti-inflammatory drugs for primary dysmenorrhoea. Cochrane Database Syst Rev. (2003) 4:CD001751. doi: 10.1002/14651858.CD001751
7.
Wong CL Farquhar C Roberts H Proctor M Wong CL . Oral contraceptive pill for primary dysmenorrhoea. Cochrane Database Syst Rev. (2009) 2010:CD002120–CD20. doi: 10.1002/14651858.CD002120.pub3
8.
Vercellini P Viganò P Somigliana E . The role of the levonorgestrel-releasing intrauterine device in the management of symptomatic endometriosis. Curr Opin Obstet Gynecol. (2005) 17:359–65. doi: 10.1097/01.gco.0000175353.03061.7f
9.
Khan KS Champaneria R Latthe PM . How effective are non-drug, non-surgical treatments for primary dysmenorrhoea?BMJ. (2012) 344:e3011. doi: 10.1136/bmj.e3011
10.
Munstedt K Riepen T . Patients' decisions regarding the treatment of primary dysmenorrhoea. Complement Ther Med. (2019) 45:1–6. doi: 10.1016/j.ctim.2019.05.016
11.
Proctor ML Murphy PA Pattison HM Suckling J Farquhar CM . Behavioural interventions for primary and secondary dysmenorrhoea. Cochrane Database Syst Rev. (2007) 3:CD002248. doi: 10.1002/14651858.CD002248.pub3
12.
Osayande AS Mehulic S . Diagnosis and initial management of dysmenorrhea. Am Fam Physician. (2014) 89:341–6. PMID:
13.
World Health Organization . Regional Office for the Western Pacific. WHO international standard terminologies on traditional medicine in the Western Pacific RegionWHO Regional Office for the Western Pacific (2007). Available at: https://iris.who.int/handle/10665/206952 (Accessed August, 2024).
14.
Song QY Zhou YL Zhou B Chen XY Zhang RY Chen YJ . Study progress on the mechanism of acupuncture for primary dysmenorrhea. World J Acupunct Moxibustion. (2021) 313:227–32. doi: 10.1016/j.wjam.2021.05.016
15.
Qin Y Guo MW Lan Y Wang YF Wang S Ji MX et al . Effect of electroacupuncture of "Hegu" (LI4) and "Zusanli" (ST36) on intestinal sensitivity and motility in irritable bowel syndrome rats. Zhen Ci Yan Jiu. (2020) 45:293–8. doi: 10.13702/j.1000-0607.190743
16.
Qin ZY Ling H Xia XH Meng L Wu ZJ . Effects of electroacupuncture of Sanyinjiao (SP 6) on genito-endocrine in patients with perimenopausal syndrome. Zhen Ci Yan Jiu. (2007) 32:255–9. PMID:
17.
Pan S Wang S Li J Yuan H Xue X Liu Y et al . Moxibustion for primary dysmenorrhea: an adjuvant therapy for pain relief. Evid Based Complement Alternat Med. (2022) 2022:1–14. doi: 10.1155/2022/6864195
18.
Moher D Liberati A Tetzlaff J Altman DG PRISMA Group . Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. Ann Intern Med. (2009) 151:264–69. doi: 10.1136/bmj.b2535
19.
Page MJ McKenzie JE Bossuyt PM Boutron I Hoffmann TC Mulrow CD et al . Updating guidance for reporting systematic reviews: development of the PRISMA 2020 statement. J Clin Epidemiol. (2021) 134:103–12. doi: 10.1016/j.jclinepi.2021.02.003
20.
Chen MN Chien LW Liu CF . Acupuncture or acupressure at the sanyinjiao (sp6) acupoint for the treatment of primary dysmenorrhea: A meta-analysis. Evid Based Complement Alternat Med. (2013) 2013:493038. doi: 10.1155/2013/493038
21.
Kong X Fang H Li X Zhang Y Guo Y . Effects of auricular acupressure on dysmenorrhea: A systematic review and meta-analysis of randomized controlled trials. Front Endocrinol (Lausanne). (2023) 5:1016222. doi: 10.3389/fendo.2022.1016222
22.
Higgins JPT Thomas J Chandler J Cumpston M Li T Page MJ et al . (eds.). Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023). (2023). Available from www.training.cochrane.org/handbook (Accessed August, 2024).
23.
Guyatt GH Oxman AD Kunz R Vist GE Falck-Ytter Y Schünemann HJ et al . Rating quality of evidence and strength of recommendations: what is "quality of evidence" and why is it important to clinicians?BMJ. (2008) 336:995–8. doi: 10.1136/bmj.39490.551019.BE
24.
van Valkenhoef G Lu G de Brock B Hillege H Ades AE Welton NJ . Automating network meta-analysis. Res Synth Methods. (2012) 3:285–99. doi: 10.1002/jrsm.1054
25.
Chaimani A Higgins JPT Mavridis D Spyridonos P Salanti G . Graphical tools for network meta-analysis in STATA. PLoS One. (2013) 8:e76654. doi: 10.1371/journal.pone.0076654
26.
Salanti G Ades A Ioannidis JP . Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorial. J Clin Epidemiol. (2011) 64:163–71. doi: 10.1016/j.jclinepi.2010.03.016
27.
Chen HM Wang HH Chiu MH Hu HM . Effects of acupressure on menstrual distress and low back pain in dysmenorrheic young adult women: an experimental study. Pain Manag Nurs. (2015) 16:188–97. doi: 10.1016/j.pmn.2014.06.002
28.
Dincer Y Oskay U . The Effect of Acupressure Applied to Sanyinjiao (SP6) on Primary Dysmenorrhea. Altern Ther Health Med. (2023) 29:16–22.
29.
Gao J Wang Q Xian S Feng YM Cao WX Ye JY et al . The effect of moxibustion on alleviating menstrual pain in a population of young nursing students: a prospective randomized cross-over pilot study. Complement Ther Med. (2015) 23:773–81. doi: 10.1016/j.ctim.2015.08.005
30.
Kashefi F Ziyadlou S Khajehei M Ashraf AR Reza Fadaee A Jafari P . Effect of acupressure at the Sanyinjiao point on primary dysmenorrhea: a randomized controlled trial. Complement Ther Clin Pract. (2010) 16:198–202. doi: 10.1016/j.ctcp.2010.04.003
31.
Kiran G Gumusalan Y Ekerbicer HC Kiran H Coskun A Arikan DC . A randomized pilot study of acupuncture treatment for primary dysmenorrhea. Eur J Obstet Gynecol Reprod Biol. (2013) 169:292–5. doi: 10.1016/j.ejogrb.2013.02.016
32.
Liu LY Li X Tian ZL Zhang Q Shen ZF Wei W et al . Acupuncture modulates the frequency-specific functional connectivity density in primary dysmenorrhea. Front Neurosci. (2022) 16:1–12. doi: 10.3389/fnins.2022.917721
33.
Mirbagher-Ajorpaz N Adib-Hajbaghery M Mosaebi F . The effects of acupressure on primary dysmenorrhea: a randomized controlled trial. Complement Ther Clin Pract. (2011) 17:33–6. doi: 10.1016/j.ctcp.2010.06.005
34.
Qorbanalipour K Ghaderi F Jafarabadi MA . Comparison of the effects of acupressure and electroacupuncture in primary dysmenorrhea: a randomized controlled trial. Int J Women’s Health Reprod Sci. (2018) 6:471–6. doi: 10.15296/ijwhr.2018.78
35.
Shetty GB Shetty B Mooventhan A . Efficacy of acupuncture in the Management of Primary Dysmenorrhea: a randomized controlled trial. JAMS J Acupuncture Meridian Stud. (2018) 11:153–8. doi: 10.1016/j.jams.2018.04.001
36.
Sriprasert I Suerungruang S Athilarp P Matanasarawoot A Teekachunhatean S . Efficacy of acupuncture versus combined Oral contraceptive pill in treatment of moderate-to-severe dysmenorrhea: a randomized controlled trial. Evidence-based complement Alt Med. (2015) 2015:1–10. doi: 10.1155/2015/735690
37.
Wang H Cao Y Jin X Yan M Wang J Li R et al . Effect of an acupuncture technique of penetrating through zhibian (BL54) to shuidao (ST28) with long needle for pain relief in patients with primary dysmenorrhea: a randomized controlled trial. Pain Res Manag. (2019) 2019:7978180. doi: 10.1155/2019/7978180
38.
Yang M Chen X Bo L Lao L Chen J Yu S et al . Moxibustion for pain relief in patients with primary dysmenorrhea: a randomized controlled trial. PLoS One. (2017) 12:e0170952. doi: 10.1371/journal.pone.0170952
39.
Ding LP Liu H Hu XW . Effect of mixed Moxibustion on pain and serum hormone levels of primary dysmenorrhea of cold coagulation and stasis type (in Chinese). Chin Med Mod Dist Educ China. (2021) 19:59–61. doi: 10.3969/j.issn.1672-2779.2021.07.023
40.
Wan KM Huang H Gen LL Tang LM Hu XW Zhou GX et al . Clinical observation of long snake-like moxibustion in treating primary dysmenonrrheal with deficiency of qi and blood (in Chinese). Chinese Medicine Moderen Distance Education of China. (2022) 20:131–33. doi: 10.3969/j.issn.1672-2779.2022.04.051
41.
Liu XP . Observation on treating primary dysmenorrhea of the hanshi ningzhi type by warm acupuncture at bl32 (in Chinese). Clin J Chin Med. (2019) 11:108–10. doi: 10.3969/j.issn.1674-7860.2019.08.042
42.
Liu Y Li Y . Evaluation on clinical efficacy of spaced ginger moxibustion for primary dysmenorrhea with colddamp stagnation (in Chinese). Mod J Integ Trad Chin Western Med. (2018) 27:850–2. doi: 10.3969/j.issn.1008-849.2018.08.015
43.
Ye ZY . Observation of clinical efficacy of heat-sensitive ginger-partitioned moxibustion in the treatment of cold blood stasis type of dysmenorrhea (in Chinese) [master’s thesis]. Jiangxi, China: Jiangxi University of Chinese Medicine. (2022)
44.
Wu F . Clinical observation on ginger-isolated moxibustion treatment with primary dysmenorrhea casued by cold and blood stagnation (in Chinese) [master’s thesis]. Sichuan, China: Chengdu University of Traditional Chinese Medicine. (2009).
45.
Tang N . The clinical observation of immediate analgesic effect of choropractic thearpy to the patients of congestive primary dysmenorrhea (in Chinese) [master’s thesis]. Shandong, China: Shandong University of Traditional Chinese Medicine. (2012).
46.
Chang JY Long DH Yu X Zhang L . Effect of periodic acupuncture and moxibustion on the pain degree frequency and symptoms of patients with primary dysmenorrhea with cold coagulation and blood stasis (in Chinese). World Journal of Integrated Traditional and Western Medicine (2020) 15:1315–18. doi: 10.13935/j.cnki.sjzx.200731
47.
Zhang Y . Clinical reserach of electro-acupuncture in treatment of primary dysmenorrhea (in chinese). Journal of Hunei University of Chinese Medicine (2017) 19:80–82. doi: 10.3969/j.issn.1008-987x.2017.06.21
48.
Zhang WW Wang L Qu L . Clinical observation of moxibustion with immediate effect in treating primary dysmenorrhea (in chinese). Journal of Guangzhou University of Traditional Chinese Medicine. (2020) 37:1091–94. doi: 10.13359/j.cnki.gzxbtcm.2020.06.018
49.
Zhang YH . The study of thunder-fire moxibustion in treating primary dysmenorrhea of cold-coagulation-stasis type (in Chinese) [master’s thesis]. Guangdong, China: Guangzhou University of Chinese Medicine. (2019).
50.
Zhang HZ . Clinical study of moxibustion on baliao point in treating primary dysmenorrhea with cold coagulation and blood stasis type (in Chinese) [master’s thesis]. Shandong, China: Shandong University of Traditional Chinese Medicine. (2020).
51.
Peng MH . Clinical observation on treating primary dysmenorrhea by acupuncture xi acupoints of three foot yin meridians (in Chinese) [master’s thesis]. Guangdong, China: Guangzhou University of Chinese Medicine. (2012).
52.
Cao Y . Acupuncture clinical analysis of primary dysmenorrhea (in Chinese) [master’s thesis]. Heilongjiang, China: Heilongjiang University of Chinese Medicine. (2011).
53.
Cao YX . The clinical research about primay dysmenorrhea treated by penetrating method from zhibian (b54) to shuidao (st28) (in Chinese) [master’s thesis]. Shanxi, China: Shanxi University of Chinese Medicine. (2014).
54.
Zhu L . Clinical observation on the treatment of dysmenorrhea caused by cold coagulation and blood stasis by wenjing tongluo massage technique (in Chinese) [master thesis]. Yunnan, China: Yunnan University of Chinese Medicine. (2020).
55.
Zhu Y . The clinical effect to primary dysmenorrhoea with adominal acupuncture (in Chinese) [master’s thesis]. Guangdong, China: Guangzhou University of Chinese Medicine. (2015).
56.
Li H . To study the functional regions of acupuncture at sanyinjiao(sp6) treatment on primary dysmenorrhea (in Chinese) [master’s thesis]. Henan, China: Henan University of Chinese Medicine. (2014).
57.
Li Z Qu JH Wang YZ Ma XP Song XL Li JC et al . Efficacy of press needles to the auricular point in treating primary dysmenorrhea of air force women soldiers (in Chinese). Med J of Air Force (2017) 33:306–07+42.
58.
Lin LX . Clinical obervation on treatment of primary dysmenorrhea of cold coagulation and blood stasis type with filiform-fire needle (in Chinese) [master’s thesis]. Guangdong, China: Guangzhou University of Chinese Medicine. (2019).
59.
Lin WM Wu JS Lin LX . Observation on the therapeutic effect of warm acupuncture on primary dysmenorrhea (in Chinese). Chinese and Foreign Medical Research. (2020) 18:124–26. doi: 10.14033/j.cnki.cfmr.2020.16.050
60.
Lin GH . Clinical observation on treatment of primary dysmenorrhea of cold congealing and blood stasis type by warming acupuncture and moxibustion on 17 vertebrae (in Chinese) [master’s thesis]. Fujian, China: Fujian Univeristy of Traditional Chinese Medicine. (2020).
61.
Liang RF . Clinical observation and mechanism of treating primary dysmenorrhea with qijiao moxibustion (in Chinese) [master’s thesis]. Guangdong, China: Guangzhou University Of Chinese Medicine. (2021).
62.
Fan CH . Ginger moxibustion treatment of blood stasis type of dysmenorrhea haemorrhealogical nature of clinical research (in Chinese) [doctoral thesis]. Guangdong, China: Guangzhou University Of Chinese Medicine. (2014).
63.
Tang XM Liu XC . The acupuncture in the treatment of primary dysmenorrhea for 30 cases. Chin Med Mod Dist Educ China. (2015) 13:83–84. doi: 10.3969/j.issn.1672-2779.2015.22.045
64.
Wen SQ . Clinical observation on the treatment of primary dysmenorrhea with qi stagnation and blood stasis based on the principle of “the liver is the precondition for women” (in Chinese) [master’s thesis]. Liaoning, China: Liaoning University of Traditional Chinese Medicine. (2021).
65.
Wang DF . Clinical study of treatment in primary dysmenorrhea by abdominal acupuncture (in Chinese) [master’s thesis]. Guangxi, China: Guangxi University of Chinese Medicine (2019).
66.
Wang LY Chen HP . Clinical observation of 60 cases of primary dysmenorrhea treated with wheat-grain size cone moxibustion (in Chinese). J Chin Med. (2018) 50:174–76. doi: 10.13457/j.cnki.jncm.2018.07.052
67.
Bai MP Yang YF Lao JX Li ZY Chen SG . Clinical efficacy of heavy moxibustion at the eight acupoints in the treatment of cold-damp stagnation type of moderate to severe primary dysmenorrhea (in Chinese). J Emerg Tradit Chin Med. (2018) 11:2026–28. doi: 10.3969/j.issn.1004-745X.2018.11.043
68.
Sheng ML . Clinical effect of acupuncure on primary dysmenorrhea: A randomized, controlled trial (in Chinese) [master’s thesis]. Heilongjiang, China: Heilongjiang University of Chinese Medicine. (2019).
69.
Shi AD . Clinical study on the treatment of primary dysmenorrhea with cold dampness syndrome by holographic meridian copper-bian scraping method and its influence on prostaglandins (in Chinese) [master’s thesis]. Guangxi, China: Guangxi University of Chinese Medicine. (2022).
70.
Shi ZH Guo YJ . Immediate analgesic effect of warming needle Moxibustion for primary dysmenorrhea (in Chinese). Acta Chin Med. (2017) 32:1343–46. doi: 10.16368/j.issn.1674-8999.2017.07.354
71.
Lou S . A radomized controlled study on the treatment of primary dysmenorrhea od cold coagulation and blood staisi type by wentong chong abdominal massage (in Chinese) [master’s thesis]. Tianjin, China: Tianjin University of Traditional Chinese Medicine. (2020).
72.
Zhai SJ . Immediate analgesic effect of an acupressure wrist-ankle strap simulating wrist-ankle acupuncture stimulation on primary dysmenorrhea in young women: A randomized controlled trial (in Chinese) [master’s thesis]. Shanghai University of Traditional Chinese Medicine. (2020).
73.
Xiao Y . The clinical effect observation on the treatment of primary dysmenorrhea with abdominal meridians acupuncture as the main method (in Chinese) [master’s thesis]. Yunnan, China: Yunnan University of Chinese Medicine. (2016).
74.
Fan CH . Clinical study on the treatment of cold blood stasis type primary dysmenorrhea with thunder fire moxibustion (in Chinese) [master’s thesis]. Guangdong, China: Guangzhou University of Chinese Medicine. (2021).
75.
Jia F . Clinical observation on 120 cases of primary dysmenorrhea treated by acupuncture (in Chinese) [master’s thesis]. Heilongjiang, China: Heilongjiang University of Chinese Medicine. (2017).
76.
Hao CC Wang X . Observation on acupuncture and moxibustion in treatment of primary dysmenorrhea of cold - stagnation and blood - stasis type (in Chinese). Chinese Archives of Traditional Chinese Medicine. (2018) 36:659–62. doi: 10.13193/j.issn.1673-7717.2018.03.034
77.
Guo LM Zhou YB Kong XJ Zhou CH Liu B . Effect of thunder - fire moxibustion therapy for clinical symptoms and serum prostaglandin f2α in patients with primary dysmenorrhea of cold coagulation and blood stasis (in Chinese). Hebei, China: Hebei Journal Traditional Chinese Medicine. (2021) 43:1367–70+74.
78.
Zhong Y Wei YL . Warm needling for primary dysmenorrhea of cold-dampness stagnation syndrome (in Chinese). Chinese Manipulation & Rehabilitation Medicine. (2017) 8:32–33+37. doi: 10.19787/j.issn.1008-1879.2017.21.015
79.
Chen Y Shang GD Fu GB Jin T . Effect of massage on hemodynamics parameters of uterine artery and serum prostaglandin in treating patients with primary dysmenorrhea (in Chinese). Chin J Integr Med. (2011) 31:1355–58.
80.
Chen CL Deng C . Clinical observation of primary dysmenorrhea treated by acupuncture (in Chinese). J New Chin Med. (2014) 46:161–62. doi: 10.13457/j.cnki.jncm.2014.07.075
81.
Chen L Guo XL Yu SY Wei W Shen ZF Zhao GL et al . Effect of acupuncture on brain functional connectivity strength in patients with primary dysmenorrhea (in Chinese). Chinese Acupuncture & Moxibustion. (2022) 42:863–70. doi: 10.13703/j.0255-2930.20210826-k0004
82.
Han Y Zhou YL Guo XH Liu YJ Li H Chen XY . Analgesic effect on primary dysmenorrheal treated with conventional and sham acupucture at sanyinjiao (in Chinese). Chinese Acupuncture & Moxibustion. (2015) 35:318–22. doi: 10.13703/j.0255-2930.2015.04.002
83.
Wei YH Li WJ Fan HX . Immediate and long-term analgesic effect of baliao points daoqi method in treating primary dysmenorrhea (in Chinese). Acta Chinese Medicine. (2019) 34:2687–91. doi: 10.16368/j.issn.1674-8999.2019.12.616
84.
Yang H Liu CZ Chen X Ma LX Xie JP Guo NN et al . Systematic review of clinical trials of acupuncture-related therapies for primary dysmenorrhea. Acta obstetricia et gynecologica Scandinavica. (2008) 87:1114–22. doi: 10.1080/00016340802443798
85.
Liu W Wang CC Lee KH Ma X Kang TL . Efficacy and safety of acupuncture and or Moxibustion for managing primary dysmenorrhea: a systematic review and meta-analysis. Clin Nurs Res. (2022) 31:1362–75. doi: 10.1177/10547738221086984
86.
Jiang HR Ni S Li JL Liu MM Li J Cui XJ et al . Systematic review of randomized clinical trials of acupressure therapy for primary dysmenorrhea. Evid Based Complement Alternat Med. (2013) 2013:1–9. doi: 10.1155/2013/169692
87.
Zhang F Sun M Han S Shen X Luo Y Zhong D et al . Acupuncture for primary dysmenorrhea: an overview of systematic reviews. Evid Based Complement Alternat Med. (2018) 2018:8791538–11. doi: 10.1155/2018/8791538
88.
Chung KF Yeung WF Kwok CW Yu YM . Risk factors associated with adverse events of acupuncture: a prospective study. Acupunct Med. (2014) 32:455–62. doi: 10.1136/acupmed-2014-010635
89.
Xu S Wang L Cooper E Zhang M Manheimer E Berman B et al . Adverse events of acupuncture: a systematic review of case reports. Evid Based Complement Alternat Med. (2013) 2013:1–15. doi: 10.1155/2013/581203
90.
Chung KF Yeung WF Yu YM Kwok CW Zhang SP Zhang ZJ . Adverse events related to acupuncture development and testing of a rating scale. Clin J Pain. (2015) 31:922–8. doi: 10.1097/AJP.0000000000000189
91.
White IR Barrett JK Jackson D Higgins JPT . Consistency and inconsistency in network meta-analysis: model estimation using multivariate meta-regression. Res Synth Methods. (2012) 3:111–25. doi: 10.1002/jrsm.1045
92.
Marušić MF Fidahić M Cepeha CM Farcaș LG Tseke A Puljak L . Methodological tools and sensitivity analysis for assessing quality or risk of bias used in systematic reviews published in the high-impact anesthesiology journals. BMC Med Res Methodol. (2020) 20:121. doi: 10.1186/s12874-020-00966-4
93.
Higgins J Thompson S Deeks J Altman D . Statistical heterogeneity in systematic reviews of clinical trials: a critical appraisal of guidelines and practice. J Health Serv Res Policy. (2002) 7:51–61. doi: 10.1258/1355819021927674
94.
Viechtbauer W . Hypothesis tests for population heterogeneity in meta-analysis. Brit J Math Statist Psychol. (2007) 60:29–60. doi: 10.1348/000711005X64042
95.
Guyatt GH Oxman AD Kunz R Brozek J Alonso-Coello P Rind D et al . GRADE guidelines 6. Rating the quality of evidence—imprecision. J Clin Epidemiol. (2011) 64:1283–93. doi: 10.1016/j.jclinepi.2011.01.012
96.
IntHout J Ioannidis JPA Borm GF Goeman JJ . Small studies are more heterogeneous than large ones: a meta-meta-analysis. J Clin Epidemiol. (2015) 68:860–9. doi: 10.1016/j.jclinepi.2015.03.017
97.
Zhang Z Xu X Ni H . Small studies may overestimate the effect sizes in critical care meta-analyses: a meta-epidemiological study. Crit Care. (2013) 17:R2–2. doi: 10.1186/cc11919
98.
Del Re AC Maisel NC Blodgett JC Finney JW . Intention-to-treat analyses and missing data approaches in pharmacotherapy trials for alcohol use disorders. BMJ Open. (2013) 3:–e003464. doi: 10.1136/bmjopen-2013-003464
99.
Probst P Grummich K Heger P Zaschke S Knebel P Ulrich A et al . Blinding in randomized controlled trials in general and abdominal surgery: protocol for a systematic review and empirical study. Syst Rev. (2016) 5:48–8. doi: 10.1186/s13643-016-0226-4
100.
Moher D Hopewell S Schulz KF Montori V Gøtzsche PC Devereaux PJ et al . CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. J Clin Epidemiol. (2010) 63:e1–e37. doi: 10.1016/j.jclinepi.2010.03.004
101.
Sedgwick P . Randomised controlled trials: the importance of sample size. BMJ. (2015) 350:h1586. doi: 10.1136/bmj.h1586
Summary
Keywords
primary dysmenorrhea, TCM, Chinese medicine, acupuncture, acupressure, moxibustion, tuina , warm needling
Citation
Chen S-C, Ruan J-Y, Zhang B, Pang L-Y, Zhong L, Lin S-L, Wong K-P, Ouyang H-X, Yeung W-F, Fu Q-W and Chen B-Q (2024) Traditional Chinese medicine interventions based on meridian theory for pain relief in patients with primary dysmenorrhea: a systematic review and network meta-analysis. Front. Med. 11:1453609. doi: 10.3389/fmed.2024.1453609
Received
23 June 2024
Accepted
14 August 2024
Published
05 September 2024
Volume
11 - 2024
Edited by
Cristina Secosan, Victor Babes University of Medicine and Pharmacy, Romania
Reviewed by
Coroleuca Catalin, Clinical Hospital of Obstetrics and Gynecology Prof. Dr. Panait Sârbu, Romania
Razvan Ciortea, County Emergency Hospital Cluj-Napoca, Romania
Updates
Copyright
© 2024 Chen, Ruan, Zhang, Pang, Zhong, Lin, Wong, Ouyang, Yeung, Fu and Chen.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bo-Qian Chen, 20193113175@stu.gzucm.edu.cn; Qin-Wei Fu, fuqinweitcm@163.com
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.