 Blanca Álvarez-del Río1
Blanca Álvarez-del Río1 Laura Sánchez-de Prada1,2*Irene Arroyo-Hernantes2
Laura Sánchez-de Prada1,2*Irene Arroyo-Hernantes2 F. Javier Álvarez1,2,3,4Eduardo Tamayo1,2,3,4
F. Javier Álvarez1,2,3,4Eduardo Tamayo1,2,3,4 Eduardo Gutiérrez-Abejón1,2,4,5,6
Eduardo Gutiérrez-Abejón1,2,4,5,6- 1Facultad de Medicina, Universidad de Valladolid, Valladolid, Spain
- 2BioCritic, Grupo de investigación de Biomedicina en Cuidados Críticos, Valladolid, Spain
- 3Hospital Clínico Universitario de Valladolid, Valladolid, Spain
- 4Centro de Investigación Biomédica en Red de Enfermedades Infecciosas (CIBERINFEC), Instituto de Salud Carlos III, Madrid, Spain
- 5Dirección Técnica de Farmacia, Gerencia Regional de Salud de Castilla y León, Valladolid, Spain
- 6Facultad de Empresa y Comunicación, Universidad Internacional de la Rioja (UNIR), Logroño, Spain
Introduction: Pregnant women are considered a vulnerable group for COVID-19 with an increased risk for complications. The objective of this study is to describe in-hospital mortality, pregnancy outcomes, and direct hospital costs associated with COVID-19 in women at the time of childbirth.
Methods: This retrospective nationwide population-based registry study collects data on complications, outcomes, and direct hospital costs from women hospitalized for childbirth, recorded in the Minimum Basic Data Set obtained from the National Surveillance System for Hospital Data in Spain between 2020–2022. Hospitalization characteristics, complications related to pregnancy and childbirth, outcomes, and hospitalization costs are compared between COVID-19-positive and non-COVID-19 women at the time of childbirth.
Results: A total of 779,387 women were admitted between 2020 and 2022 with a record of childbirth in Spanish hospitals. Of these, 15,792 (2.06%) had COVID-19 at the time of delivery. These women had a longer length of stay (3.53 days), higher rates of intensive care unit (ICU) admission (2.53%), ventilation/intubation (0.91%), and in-hospital mortality (0.06%) (p < 0.0001). This group also exhibited higher rates of spontaneous premature onset of labor (7%) and postpartum hemorrhage (3.45%), as well as a higher rate of labor induction (6.27%) (p < 0.001). Additionally, a higher single stillbirth rate (0.73%) was found among COVID-19-positive women (p = 0.0002). A significant higher risk of postpartum hemorrhage (OR = 1.14), embolism (OR = 7.98), acute respiratory distress syndrome (OR = 35.5), temporary tracheostomy (OR = 4.89), ventilation/intubation (OR = 6.85), and single stillbirth (OR = 1.32) was found in COVID-19 women (p < 0.05). The mean cost per patient was €4,066.48, 25.06% higher than that for non-COVID-19 women (p < 0.0001). Stratification by age showed an increasing trend in costs with age, reaching €6,492.12 in women ≥45 years old, where the ICU admission rate reached 8.09%.
Conclusion: These findings show that COVID-19 at the time of childbirth occurs in 2 out of every 100 cases and increases the risk of complications related to pregnancy and childbirth, as well as mortality and hospitalization costs. These data are related to SARS-CoV-2 variants circulating from 2020–2022, and current variants could give different risks. Our evaluation should be useful for health authorities to allocate resources and professionals to implement preventive measures, such as vaccination and screening, due to the increased morbidity, mortality and costs in this group.
1 Introduction
COVID-19, caused by the novel severe acute respiratory syndrome coronavirus (SARS-CoV-2) emerged in 2019, resulting in a pandemic by March 2020 (1). The constant mutation of the virus and the emergence of new variants have challenged the countries worldwide in their attempt to control the pandemic (2, 3). By the end of 2022, nearly 730 million cases and 6.7 million deaths had been caused by the virus (4).
On one hand, pregnant women belong to high-risk group regarding COVID-19. Many studies have focused on deciphering the impact of COVID-19 infection on both mother and fetus at different stages (5, 6) which still remains uncertain. On the other hand, the pandemic has resulted in an unprecedent global health and macroeconomic crisis affecting countries worldwide (7, 8). Many studies have tried to assess the costs of COVID-19 hospitalizations and primary care (9), but none of them has focused on pregnancy and childbirth. Using nationwide records, the aim of this study is to evaluate the impact of COVID-19 infection on maternal morbidity, mortality, pregnancy outcomes, and its economic repercussion in Spain during 2020–2022.
2 Methods
2.1 Study design
We conducted a nationwide hospital registry-based retrospective cohort study on pregnant women with a record of delivery in Spanish hospitals (public and private) during three consecutive years, starting from the beginning of the SARS-CoV-2 pandemic (2020–2022).
Inclusion criteria involved all pregnancies with a record of childbirth during 2020–2022. Exclusion criteria involved not having a record of childbirth. Underlying conditions were not an exclusion criterion.
Data were obtained from the Minimum Basic Data Set (MBDS) (10) collected by the National Surveillance System for Hospital Data in Spain and published by the Ministry of Health with a two-year lag. The MBDS is a clinical and administrative database completed at the time of discharge, with an estimated coverage of 99.5% of public and private Spanish hospitals. It provides encrypted information following the International Classification of Diseases 10th Revision, Clinical Modification (ICD-10-CM) (11). The study was approved by the Ethics Review Board (CEIm Area de Salud Valladolid Este, reference study PI-22–2855), and informed consent was waived due to the anonymous nature of data contained in the MBDS. We followed the CHEERS reporting guideline.
2.2 Measures
Pregnant women with a record of childbirth during 2020–2022 were selected. Patients were then divided into two groups according to confirmed COVID-19 diagnosis following ICD-10-CM (11) codes B97.29 (“Other coronavirus as the cause of diseases classified elsewhere “), and U07.1 (“COVID-19, virus identified”)upon admission.
Variables collected included age, sex, length of stay (LoS), in-hospital mortality, admission to the intensive care unit (ICU), ICU, LoS, ICU mortality, mechanical ventilation and ventilatory assistance. Comorbidities, complications, and outcomes were identified (Table 1). Supplementary Table 1 provide the ICD-10-CM codes used to identify comorbidities and complications in the included patients.
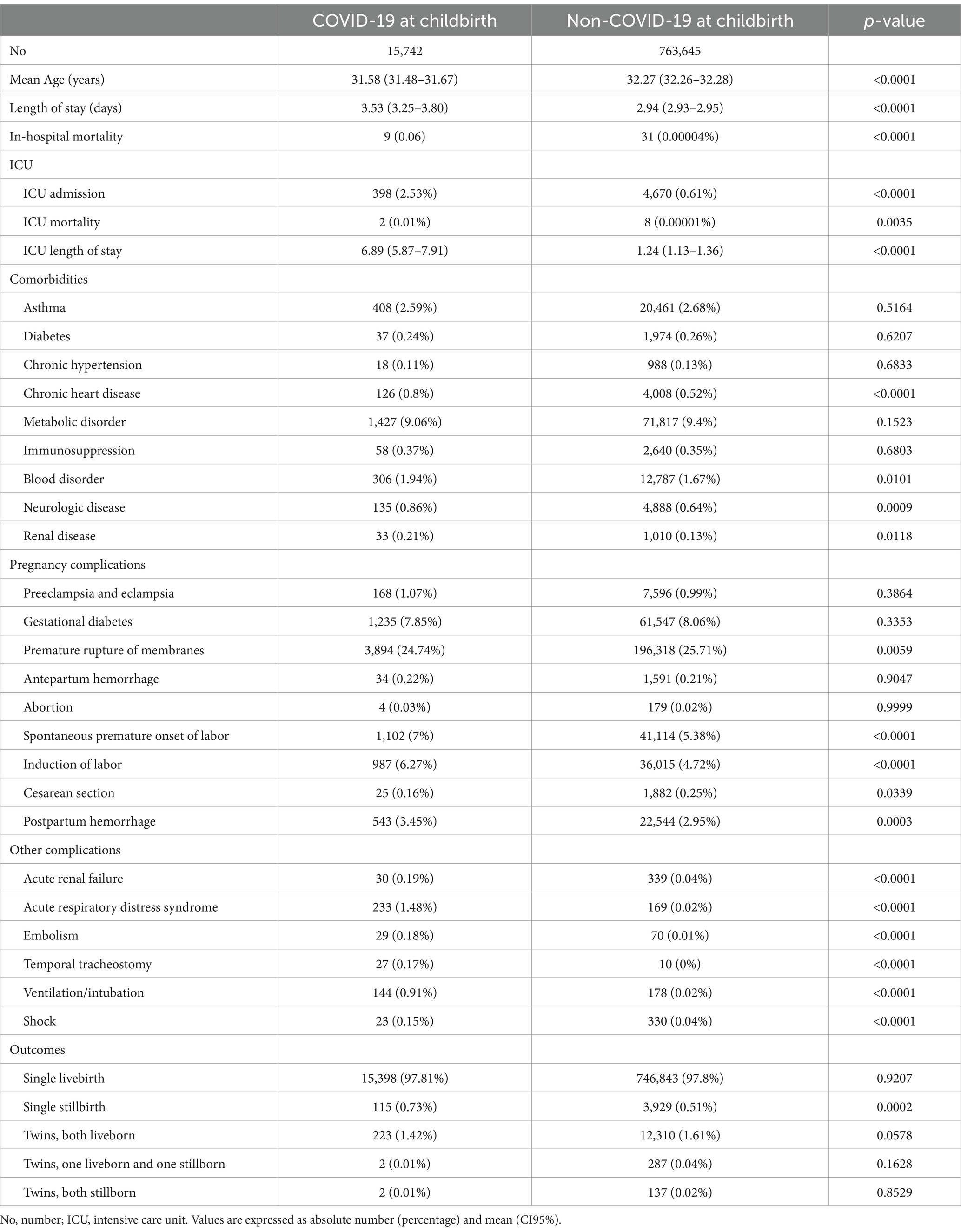
Table 1. Characteristics of hospitalized women at childbirth based on COVID-19 infection during 2020–2022.
Hospital costs were calculated using all patient refined diagnosis-related groups (APR-DRG) data extracted from the MBDS. The DRG weights and costs are derived from a representative sample of hospitals that perform analytic accounting in our country and are periodically collected in the Spanish Record of Hospital Costs. Costs calculated through the APR-DRG are adjusted for severity and mortality risk based on patient characteristics, secondary diagnosis and procedures performed during the stay. It also takes into consideration type of hospital and number of beds to estimate costs individually. Additionally, the Spanish Record of Hospital Costs has data of individual costs at discharge since 2008 which allows to have updated data on weight and costs based on actual costs and real healthcare practice in the Spanish system (12). These costs were disaggregated by year, based on age groups (<20, 20–24, 25–29,30–34, 35–39, 40–45, >45 years old), ICU-admission, and autonomous regions. All costs were expressed in euros (€). The annual inflation was calculated used the INE tool and represented a 6.5% in 2021 and 12.1% in 2022 compared to 2020 (13). The annual currency equivalence between 2020–2022 was 1€ = 1.1261$ United States dollars (USD) (14).
2.3 Statistical analysis
Patients not fulfilling inclusion criteria were excluded. Results were reported as mean with 95% confidence interval (CI95%) for continuous variables. and as frequencies and percentages for categorical variables. According to data distribution, non-parametric tests were used. Differences between groups were assessed using Student T-test, Mann–Whitney U-test and Kruskal-Wallis adjusted with Bonferroni correction for multiple comparisons (α = 0.05) for continuous variables when appropriate. In order to adjust for cofounders, first an univariate regression was performed for each variable, using the presence or absence of COVID-19 as the response variable. Then, significant variables from the univariate analysis were then included in a multivariate regression. In the multivariate analysis, a stepwise procedure was applied to retain only the significant variables. Odds Ratio (OR) with the 95% Confidence Interval (CI95%) were calculated. Significance was considered at p < 0.05. All statistical analysis was conducted with R software version 4.3.2.
3 Results
3.1 Sample characteristics
A total of 779,387 women were admitted between 2020 and 2022 with a record of delivery in Spanish hospitals; of these, 15,792 (2.06%) had COVID-19 at the time of delivery. The prevalence was 1.24, 1.06 and 3.73% in 2020, 2021, and 2022, respectively. The mean age was 31.6 years old in COVID-19 patients and 32.3 years in non-COVID-19 patients (Table 1). Age distribution of patients has been represented in Figure 1.
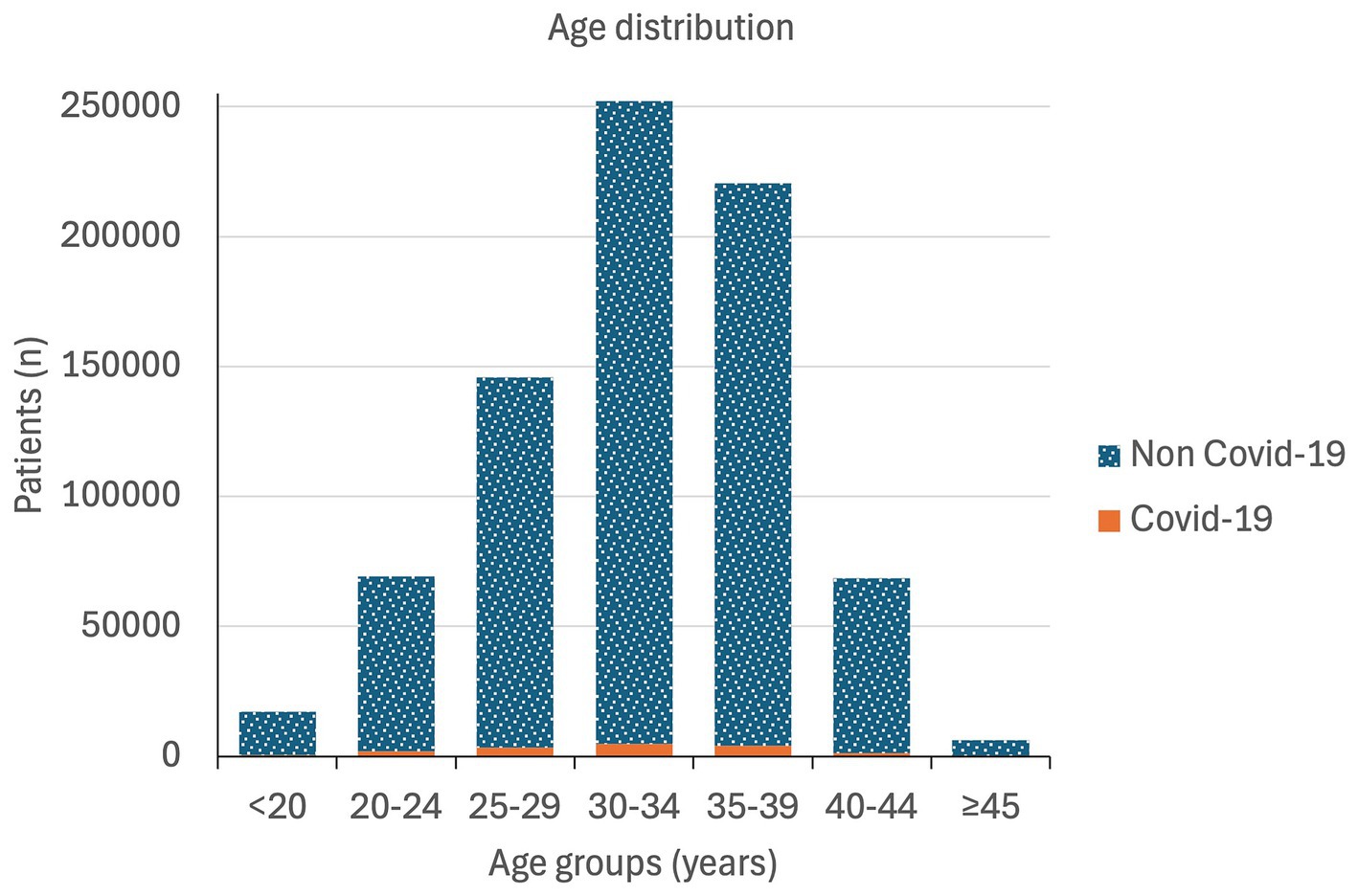
Figure 1. Age distribution of pregnant women at childbirth in Spain during 2020–2022.
3.2 Clinical characteristics and outcomes
Admission characteristics of both groups are described in Table 1. Pregnant women with COVID-19 at the time of delivery had significantly higher in-hospital mortality (0.06%) and LoS (3.53 days). A total of 2.53% of the women presenting with COVID-19 had to be admitted to the ICU and ICU mortality reached 0.01%. The mean ICU LoS was 6.89 days, and the ventilation/intubation rate was 0.91%. All of these variables significantly higher when compared to non-COVID-19 pregnant women (p < 0.0001) (Table 1).
Significant differences were observed in comorbidities, with higher rates of heart disease (0.8%), blood disorders (1.94%), neurological disorders (0.86%), and renal disease (0.21%) in the COVID-19 group (p < 0.05). Regarding complications, patients with COVID-19 exhibited significantly higher rates of acute renal failure (0.19%), acute respiratory distress syndrome (1.48%), embolism (0.18%), temporary tracheostomy (0.17%), ventilation/intubation (0.91%), and shock (0.15%) (p < 0.0001). Additionally, higher rates of pregnancy complications were observed in the COVID-19 group, including spontaneous preterm labor (7%), postpartum hemorrhage (3.45%), and labor induction (6.27%) (p < 0.001). Furthermore, a higher rate of single stillbirth (0.73%) was observed in COVID-19 patients (p = 0.0002) (Table 1).
The results of the multivariate model showed no significant association of comorbidities with the risk of COVID-19 (Supplementary Table 2). It can be observed that COVID-19 pregnant women were more likely to experience complications including acute respiratory distress syndrome (OR = 35.5), an embolism (OR = 7.98), a temporal tracheostomy (OR = 4.89) or the need of ventilation/intubation (OR = 6.85) (p < 0.05). However, the risk of cesarean section (OR = 0.64) or shock (OR = 0.29) was lower in this group (p < 0.05). The risk of postpartum hemorrhage (OR = 1.14) and single stillbirth were also significantly increased in the COVID-19 women (OR = 1.32) (p = 0.0051) (Figure 2).
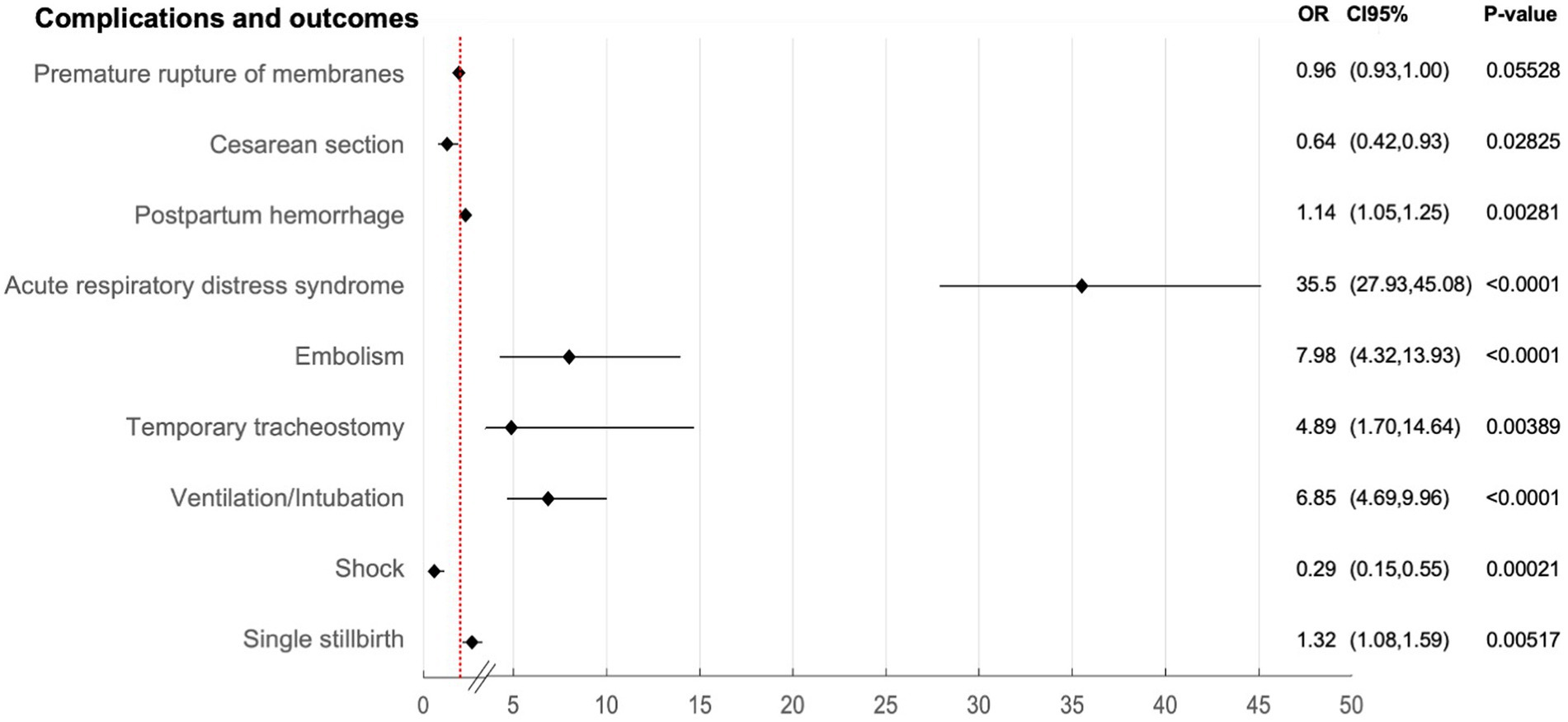
Figure 2. Association between COVID-19 in pregnant women at childbirth and complications and outcomes in Spain during 2020–2022.
3.3 COVID-19 hospitalization related costs in pregnant women at childbirth
The total cost of admissions for pregnant women with COVID-19 disease at the time of delivery was €64 million (€64,014,477), with a mean cost per patient of €4,066.48. This was significantly higher that the €3,251.59 per patient spent on non-COVID-19 patients (p < 0.0001) (Table 2). Admission to the ICU represented a higher mean cost per patient (€13,629.35) compared to non-COVID-19 women (€4,563.58) (p < 0.0001) (Table 2).
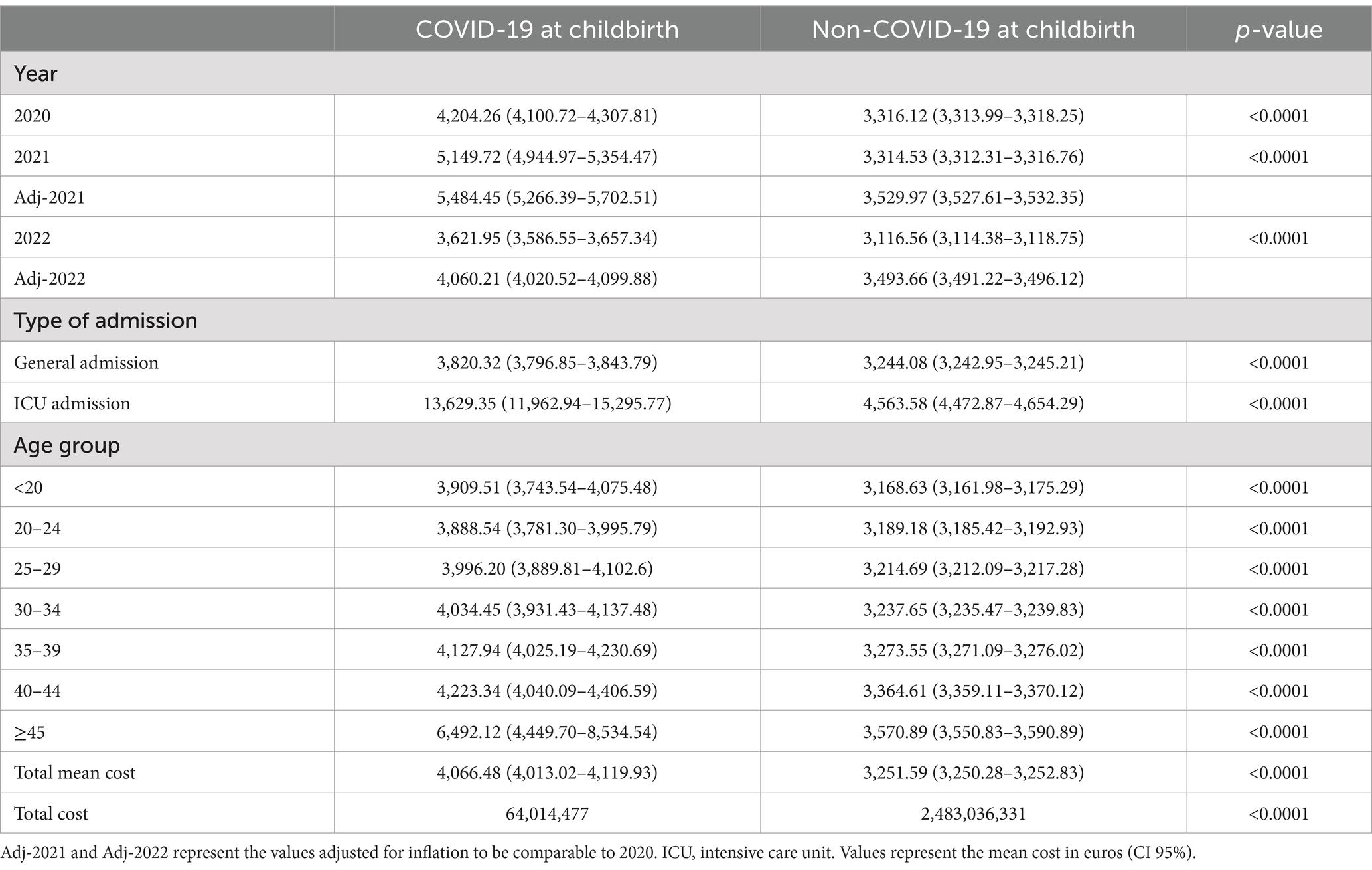
Table 2. Mean cost per patient (€) of hospitalization at childbirth in Spanish population based on COVID-19 infection during 2020–2022.
Age distribution showed an increasing trend in expenditure per patient with age, which was significantly higher in COVID-19 patients compared to those without COVID-19 in the same age range (p < 0.0001) (Figure 3). ICU admission, shown in Figure 4, presented an increasing trend with age in non-COVID-19 patients. However, for COVID-19 patients, ICU admission showed an increasing trend starting from the 25–29 age range, but higher rates were found in patients under 20 years old.
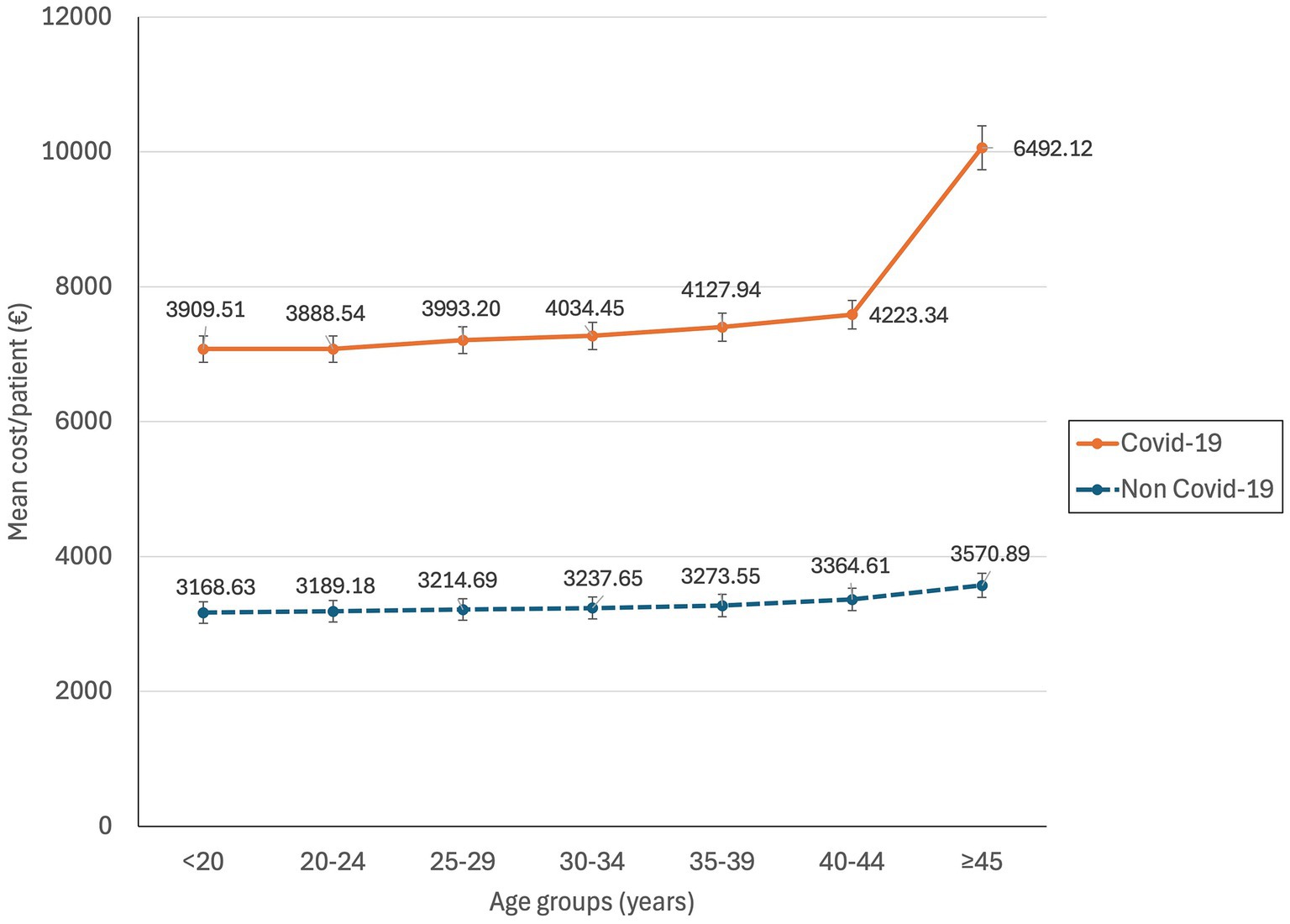
Figure 3. Mean cost per patient of hospitalization at childbirth according to age and COVID-19 infection in Spain during 2020–2022.
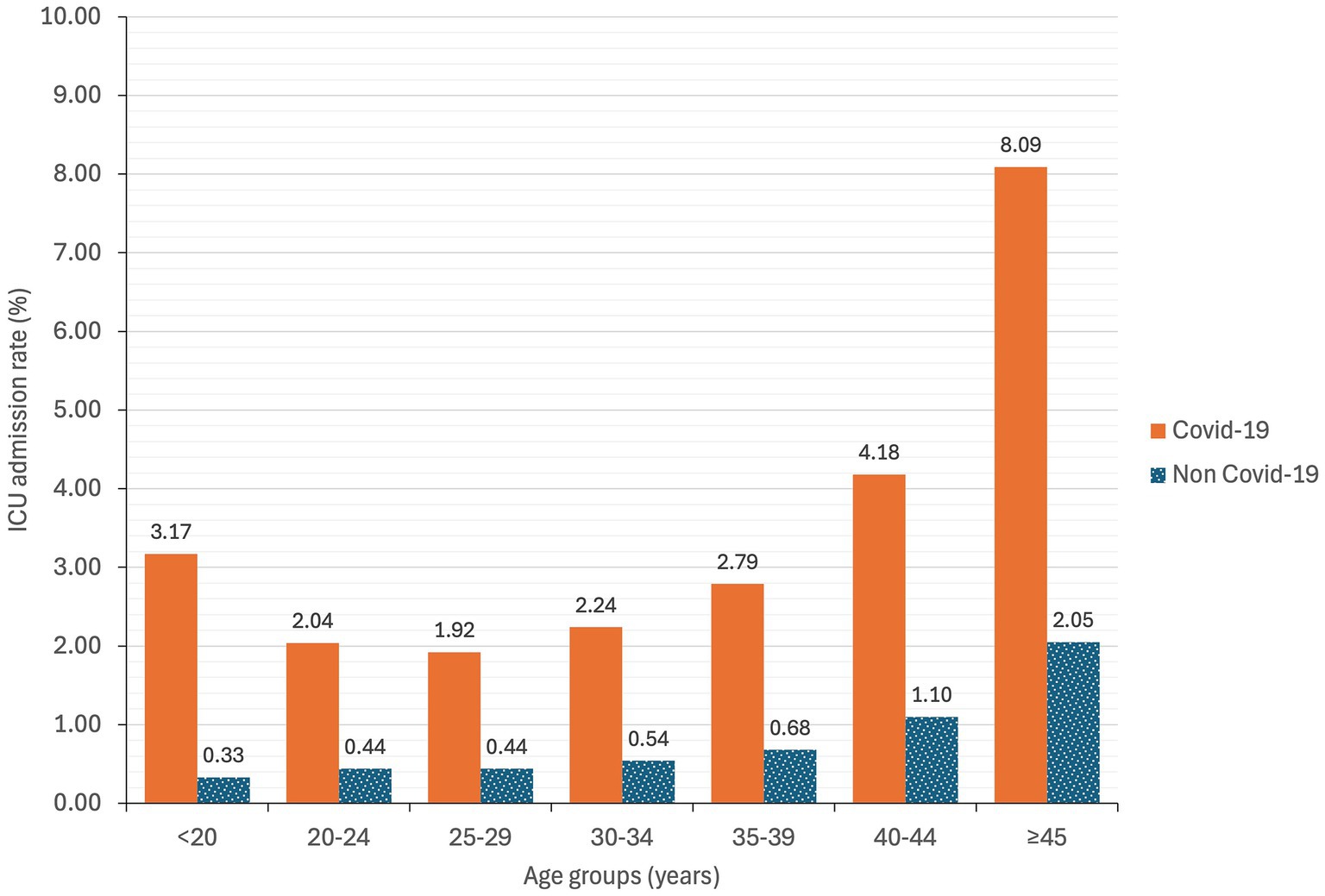
Figure 4. ICU admission rate of hospitalization at childbirth based on age groups and COVID-19 infection in Spain during 2020–2022.
Additionally, we performed a regional analysis of the mean cost per patient and ICU admission (Supplementary Figure 1; Supplementary Table 3). In almost every region, the mean cost per patient and ICU admission was significantly higher in COVID-19 patients.
4 Discussion
In our national study we found that 2.06% of pregnant women at the time of childbirth had COVID-19 infection. These women presented higher LoS, 4 times higher ICU admission rates, and 45 times higher ventilation/intubation rates. Although in-hospital mortality was quite infrequent (0.06%), it was 1,500 times higher compared to non-COVID-19 pregnant women. Regarding complications, we found higher rates of spontaneous premature onset of labor and postpartum hemorrhage, as well as higher induction of labor rates. Outcomes also showed a higher rate of single stillbirth (0.73%). Critically ill COVID-19 patients could lead to fetal hypoxia and stillbirth (15), which explains the need for labor induction in these cases. These results align with previous studies that found higher morbidity and mortality among pregnant women with COVID-19, as well as worse outcomes (16–21).
Regarding comorbidities, obesity or at least one risk factor have been associated with an increased risk of maternal death and ICU admission (22). In our study, both groups exhibited similar rates of risk factors in general, without any risk factor to be associated with an increased risk of COVID-19 in the multivariate analysis.
Numerous studies have examined both general and pregnancy-related complications associated with COVID-19. Several have reported an increased risk of gestational diabetes (23–25) while several reviews and meta-analyses have indicated a higher risk of preeclampsia (26, 27) in pregnant women infected with SARS-CoV-2. In contrast, our findings revealed an elevated risk of acute respiratory distress syndrome and embolism, which is consistent with the increased incidence of thrombotic events observed in these patients (28).
Furthermore, prior studies have reported higher rates of premature rupture of membranes (29, 30) preterm delivery (31, 32) and stillbirth (30–32) which are consistent with our observations. A national study conducted in England reported a lower prevalence of COVID-19 at childbirth (1.03%) and stillbirth (0.34%), but a higher rate of preterm deliveries (12.1%) compared to our data. That study also identified a stronger association of stillbirth (OR = 2.21) and preterm deliveries (OR = 2.17) with COVID-19 (33). Although we did not find a stronger association with preterm delivery, our results showed an increased risk of postpartum hemorrhage and stillbirth in women with COVID-19. These findings are consistent with prior reports and may be linked to inflammatory responses, coagulopathy, and changes in the placenta (34).
These discrepancies may be attributable to differences in study periods, particularly as our analysis involved three years since the beginning of the pandemic, during which different variants have circulated. Although vaccination status was not available for the participants in our study, COVID-19 vaccination during pregnancy has been shown to be safe and may help reduce risks and adverse outcomes (35).
Previous studies have assessed the direct costs of COVID-19 care in different contexts (9, 36, 37). However, this is the first study focusing on the increase in costs that COVID-19 can result in during hospitalization at childbirth. We found a higher mean cost per patient in general admission (3,820.32 €) as well as for ICU admission (13,629.35 €) in COVID-19 women compared to those admitted without COVID-19. The increased cost of COVID-19 at childbirth is likely related to the higher risk of complications and poorer outcomes in this specific population. Therefore, costs would involve longer stays and different treatment approaches required for those with COVID-19 which would entail higher resource use. These differences have remained consistent over the years. A higher mean cost was found in 2021 (5,149.72 €) for COVID-19 pregnant patients, which could be explained by the emergence of the Delta variant, which led to an increase in severity of cases (38, 39).
Additionally, the mean cost by age showed an increasing trend peaking in the population over 44 years old, with a mean cost per patient of 6,492.12€. The ICU admission rate also peaks in the over 44 years old group, reaching an 8.09%. These findings align with previous studies suggesting that older age is a risk factor for illness severity in pregnant women with COVID-19 (5, 6, 18). Finally, all regions showed a significant increase in the mean cost per patient for COVID-19 women at childbirth compared to those without COVID-19.
Our study is not without limitations. First, this is a retrospective study based on the Spanish MBDS; therefore, there could be coding errors and missing data. However, COVID-19 codes have been shown to have high sensitivity and specificity in other countries (40). Also, due to its retrospective nature, confounding factors were uncontrolled, and causal inference cannot be established. Second, cost estimates in the MBDS are calculated through diagnosis-related groups, a well-stablished American cost-estimation system (41). Third, the data is available with a two-year lag, therefore only data up to 2022 is available and this could change with new COVID-19 variants.
On the other hand, the strengths of our study include its nationwide scope, covering all childbirths recorded in the Spanish population over three years. The extensive data collected by the MBDS allowed us to evaluate the impact of COVID-19 on pregnant women at childbirth from multiple perspectives including the economic impact which to our knowledge has not been previously addressed.
To conclude COVID-19, affecting 2.06% of women at childbirth was associated with increased morbidity and mortality, including higher ICU admission rates, LoS and ventilation/intubation rates. It was also associated with complications related to pregnancy and childbirth and outcomes, such as spontaneous premature onset of labor, postpartum hemorrhage, higher induction of labor rates, and single stillbirth. The cost of these outcomes represents a 25.06% increase in the mean expenditure per patient. These data are related to SARS-CoV-2 variants circulating from 2020–2022, and current variants could give different risks. However, these differences underscore the need for specific preventive measures, such as vaccination and screening, and for strengthening resources to care for this vulnerable population. The findings provide a solid foundation for future public health strategies and clinical management during pandemics.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found at: the datasets presented in this article are not readily available because the MDBS is the property of the Ministry of Health. Therefore, any researcher can request the data related to this article from the Ministry of Health by email (aWNtYmRAbXNzc2kuZXM=), by fax (+34915964111), or by mail (Instituto de Información Sanitaria, Área de Información y Estadísticas Asistenciales, Ministerio de Sanidad, Consumo y Bienestar Social. Paseo del Prado 18–20; 28071 Madrid, Spain). Requests to access the datasets should be directed to Ministry of Health by fulfilling an application detailing the ICD-10 codes and periods needed.
Ethics statement
The studies involving humans were approved by Ethics Review Board CEIm Area de Salud Valladolid Este (reference study PI 22-2855). The studies were conducted in accordance with the national legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because informed consent was waived due to the anonymous nature of data used in the study.
Author contributions
BÁ-dR: Conceptualization, Investigation, Validation, Writing – original draft, Writing – review & editing. LS-d: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. IA-H: Data curation, Formal analysis, Writing – review & editing. FÁ: Conceptualization, Funding acquisition, Supervision, Writing – review & editing. ET: Conceptualization, Funding acquisition, Resources, Supervision, Writing – review & editing. EG-A: Conceptualization, Investigation, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by Centro de Investigación Biomédica en Red de Enfermedades Infecciosas (Group CB21/13/00051), Instituto de Salud Carlos III (Co-funded by European Regional Development Fund/European Social Fund A way to make Europe/Investing in your future). The funding centers have no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Acknowledgments
The Instituto de Información Sanitaria, Area de Información y Estadísticas Asistenciales, Ministerio de Sanidad (Ministry of Health) of Spain provided access to the Conjunto Mínimo Básico de Datos (Minimum Basic Data Set) used in this study. BÁ-DR belongs to the PhD program “Investigación en Ciencias de la Salud” under the direction of Eduardo Tamayo and Eduardo Gutiérrez-Abejón.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1548245/full#supplementary-material
References
1. World Health Organization (WHO). (2023) Coronavirus disease (COVID-19) pandemic. Available online at: https://www.who.int/europe/emergencies/situations/covid-19#:~:text=Cases%20of%20novel%20coronavirus%20(nCoV,pandemic%20on%2011%20March202020 (Accessed October 12, 2024)
3. World Health Organization (WHO). (2022) One year since the emergence of the COVID-19 virus variant omicron. Available online at: https://www.who.int/news-room/feature-stories/detail/one-year-since-the-emergence-of-omicron (Accessed October 12, 2024)
4. World Health Organisation (WHO). (2023) WHO coronavirus (COVID-19) dashboard. Available online at: https://covid19.who.int/ (Accessed May 10, 2023)
5. Brandt, JS, Hill, J, Reddy, A, Schuster, M, Patrick, HS, Rosen, T, et al. Epidemiology of coronavirus disease 2019 in pregnancy: risk factors and associations with adverse maternal and neonatal outcomes. Am J Obstet Gynecol. (2021) 224:389.e1–9. doi: 10.1016/j.ajog.2020.09.043
6. Galang, RR, Newton, SM, Woodworth, KR, Griffin, I, Oduyebo, T, Sancken, CL, et al. Risk factors for illness severity among pregnant women with confirmed severe acute respiratory syndrome coronavirus 2 infection—surveillance for emerging threats to mothers and babies network, 22 state, local, and territorial health departments, 29 march 2020–5 march 2021. Clin Infect Dis. (2021) 73:S17–23. doi: 10.1093/cid/ciab432
7. Martin, FM, Sánchez, JM, and Wilkinson, O. The economic impact of COVID-19 around the world. Review. (2023) 105:74–88. doi: 10.20955/r.105.74-88
8. Sun, M, Yan, S, Cao, T, and Zhang, J. The impact of COVID-19 pandemic on the world’s major economies: based on a multi-country and multi-sector CGE model. Front Public Health. (2024) 12:12. doi: 10.3389/fpubh.2024.1338677
9. Richards, F, Kodjamanova, P, Chen, X, Li, N, Atanasov, P, Bennetts, L, et al. Economic burden of COVID-19: a systematic review. ClinicoEcon Outcomes Res. (2022) 14:293–307. doi: 10.2147/CEOR.S338225
10. Spanish Ministry of Health. (2022) Specialized care register (SCR-MBDS). Activity and results of hospitalizations in Spain. Available online at: https://pestadistico.inteligenciadegestion.sanidad.gob.es/publicoSNS/N/rae-cmbd/rae-cmbd (Accessed December 12, 2022)
11. Spanish Ministry of Health. (2020) ICD-10 regulations. MBDS. COVID-19 coding regulations. Available online at: https://www.sanidad.gob.es/estadEstudios/estadisticas/normalizacion/CIE10/PREGUNTAS_UT_Covid_19_ms_070420202.pdf (Accessed December 12, 2022)
12. Ministerio de Sanidad. (2022) Registro de Altas de los Hospitales Generales del Sistema Nacional de Salud. CMBD Norma Estatal. Available online at: https://www.sanidad.gob.es/estadEstudios/estadisticas/cmbd.htm (Accessed March 24, 2025)
13. INE. (2025) Actualización de rentas con el IPC general (sistema IPC base 2021) para periodos anuales completos. Available online at: https://www.ine.es/calcula/calcula.do (Accessed March 26, 2025)
14. European Central Bank. (2024) Eurosystem policies and exchange rates. Available online at: https://www.ecb.europa.eu/stats/policy_and_exchange_rates/euro_reference_exchange_rates/html/eurofxref-graph-usd.en.html (Accessed September 27, 2024)
15. Schwartz, DA, Avvad-Portari, E, Babál, P, Baldewijns, M, Blomberg, M, Bouachba, A, et al. Placental tissue destruction and insufficiency from COVID-19 causes stillbirth and neonatal death from hypoxic-ischemic injury. Arch Pathol Lab Med. (2022) 146:660–76. doi: 10.5858/arpa.2022-0029-SA
16. Metz, TD, Clifton, RG, Hughes, BL, Sandoval, GJ, Grobman, WA, Saade, GR, et al. Association of SARS-CoV-2 infection with serious maternal morbidity and mortality from obstetric complications. JAMA. (2022) 327:748–59. doi: 10.1001/jama.2022.1190
17. Jering, KS, Claggett, BL, Cunningham, JW, Rosenthal, N, Vardeny, O, Greene, MF, et al. Clinical characteristics and outcomes of hospitalized women giving birth with and without COVID-19. JAMA Intern Med. (2021) 181:714–7. doi: 10.1001/jamainternmed.2020.9241
18. Allotey, J, Fernandez, S, Bonet, M, Stallings, E, Yap, M, Kew, T, et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: living systematic review and meta-analysis. BMJ. 370:m3320. doi: 10.1136/bmj.m3320
19. Male, V. SARS-CoV-2 infection and COVID-19 vaccination in pregnancy. Nat Rev Immunol. (2022) 22:277–82. doi: 10.1038/s41577-022-00703-6
20. Marchand, G, Patil, AS, Masoud, AT, Ware, K, King, A, Ruther, S, et al. Systematic review and meta-analysis of COVID-19 maternal and neonatal clinical features and pregnancy outcomes up to June 3, 2021. AJOG Global Reports. (2022) 2:100049. doi: 10.1016/j.xagr.2021.100049
21. Cruz Melguizo, S, de la Cruz, CM, Carmona Payán, P, Abascal-Saiz, A, Pintando Recarte, P, González Rodríguez, L, et al. Pregnancy outcomes and SARS-CoV-2 infection: the Spanish obstetric emergency group study. Viruses. (2021) 13:853. doi: 10.3390/v13050853
22. La Verde, M, Riemma, G, Torella, M, Cianci, S, Savoia, F, Licciardi, F, et al. Maternal death related to COVID-19: a systematic review and meta-analysis focused on maternal co-morbidities and clinical characteristics. Int J Gynecol Obstet. (2021) 154:212–9. doi: 10.1002/ijgo.13726
23. Rhou, YJJ, Elhindi, J, Melov, SJ, Cheung, NW, and Pasupathy, D. Indirect effects of the COVID-19 pandemic on risk of gestational diabetes and factors contributing to increased risk in a multiethnic population: a retrospective cohort study. BMC Pregnancy Childbirth. (2023) 23:341. doi: 10.1186/s12884-023-05659-6
24. Karimi, L, Makvandi, S, Vahedian-Azimi, A, Sathyapalan, T, and Sahebkar, A. Effect of COVID-19 on mortality of pregnant and postpartum women: a systematic review and Meta-analysis. J Pregnancy. (2021) 2021:1–33. doi: 10.1155/2021/8870129
25. La Verde, M, Torella, M, Riemma, G, Narciso, G, Iavarone, I, Gliubizzi, L, et al. Incidence of gestational diabetes mellitus before and after the Covid-19 lockdown: a retrospective cohort study. J Obstet Gynaecol Res. (2022) 48:1126–31. doi: 10.1111/jog.15205
26. Mendoza, M, Garcia-Ruiz, I, Maiz, N, Rodo, C, Garcia-Manau, P, Serrano, B, et al. Pre-eclampsia-like syndrome induced by severe COVID-19: a prospective observational study. BJOG. (2020) 127:1374–80. doi: 10.1111/1471-0528.16339
27. Conde-Agudelo, A, and Romero, R. SARS-CoV-2 infection during pregnancy and risk of preeclampsia: a systematic review and meta-analysis. Am J Obstet Gynecol. (2022) 226:68–89.e3. doi: 10.1016/j.ajog.2021.07.009
28. Bikdeli, B, Krishnathasan, D, Khairani, CD, Bejjani, A, Davies, J, Porio, N, et al. Low absolute risk of thrombotic and cardiovascular events in outpatient pregnant women with COVID-19. Thromb Res. (2024) 237:209–15. doi: 10.1016/j.thromres.2024.02.021
29. Capobianco, G, Saderi, L, Aliberti, S, Mondoni, M, Piana, A, Dessole, F, et al. COVID-19 in pregnant women: a systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol. (2020) 252:543–58. doi: 10.1016/j.ejogrb.2020.07.006
30. Akhtar, H, Patel, C, Abuelgasim, E, and Harky, A. COVID-19 (SARS-CoV-2) infection in pregnancy: a systematic review. Gynecol Obstet Investig. (2020) 85:295–306. doi: 10.1159/000509290
31. Wei, SQ, Bilodeau-Bertrand, M, Liu, S, and Auger, N. The impact of COVID-19 on pregnancy outcomes: a systematic review and meta-analysis. Can Med Assoc J. (2021) 193:E540–8. doi: 10.1503/cmaj.202604
32. Dubey, P, Reddy, SY, Manuel, S, and Dwivedi, AK. Maternal and neonatal characteristics and outcomes among COVID-19 infected women: an updated systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol. (2020) 252:490–501. doi: 10.1016/j.ejogrb.2020.07.034
33. Gurol-Urganci, I, Jardine, JE, Carroll, F, Draycott, T, Dunn, G, Fremeaux, A, et al. Maternal and perinatal outcomes of pregnant women with SARS-CoV-2 infection at the time of birth in England: national cohort study. Am J Obstet Gynecol. (2021) 225:522.e1–522.e11. doi: 10.1016/j.ajog.2021.05.016
34. Mullins, E, Hudak, ML, Banerjee, J, Getzlaff, T, Townson, J, Barnette, K, et al. Pregnancy and neonatal outcomes of COVID-19: coreporting of common outcomes from PAN-COVIDand AAP-SONPM registries. Ultrasound Obstet Gynecol. (2021) 57:573–81. doi: 10.1002/uog.23619
35. De Rose, DU, Salvatori, G, Dotta, A, and Auriti, C. SARS-CoV-2 vaccines during pregnancy and breastfeeding: a systematic review of maternal and neonatal outcomes. Viruses. (2022) 14:539. doi: 10.3390/v14030539
36. Álvarez-del Río, B, Sánchez-de Prada, L, Álvaro-Meca, A, Martín-Fernández, M, Álvarez, FJ, Tamayo, E, et al. Prevalence and cost of hospitalized patients with asymptomatic COVID-19 in 2020 in Spain. Front Public Health. (2023) 11:11. doi: 10.3389/fpubh.2023.1229561
37. Álvarez-Del Río, B, Sánchez-de Prada, L, Álvaro-Meca, A, Martín-Fernández, M, Álvarez, FJ, Tamayo, E, et al. Economic burden of the 2020 COVID-19 hospitalizations in Spain. JAMA Netw Open. (2023) 6:e2250960. doi: 10.1001/jamanetworkopen.2022.50960
38. Morris, C, Doshi, H, and Liu, WF. Impact of COVID-19 in pregnancy on maternal and perinatal outcomes during the Delta variant period: a comparison of the Delta and pre-delta time periods, 2020–2021. Matern Health Neonatol Perinatol. (2024) 10:20. doi: 10.1186/s40748-024-00189-1
39. Poisson, M, Sibiude, J, Mosnino, E, Koual, M, Landraud, L, Fidouh, N, et al. Impact of variants of SARS-CoV-2 on obstetrical and neonatal outcomes. J Gynecol Obstet Hum Reprod. (2023) 52:102566. doi: 10.1016/j.jogoh.2023.102566
40. Kadri, SS, Gundrum, J, Warner, S, Cao, Z, Babiker, A, Klompas, M, et al. Uptake and accuracy of the diagnosis code for COVID-19 among US hospitalizations. JAMA. (2020) 324:2553–4. doi: 10.1001/JAMA.2020.20323
Keywords: COVID-19, pregnancy, childbirth, delivery, hospital direct costs, costs per patient, Spain, costs
Citation: Álvarez-del Río B, Sánchez-de Prada L, Arroyo-Hernantes I, Álvarez FJ, Tamayo E and Gutiérrez-Abejón E (2025) Nationwide analysis of COVID-19 complications, outcomes, and costs of childbirth in Spain. Front. Med. 12:1548245. doi: 10.3389/fmed.2025.1548245
Edited by:
Domenico Umberto De Rose, Bambino Gesù Children’s Hospital (IRCCS), ItalyReviewed by:
Arzu Bilge Tekin, Martyr Dr. İlhan Varank Sancaktepe Training and Research Hospital, TürkiyeMarco La Verde, Università degli Studi della Campania “Luigi Vanvitelli”, Italy
Copyright © 2025 Álvarez-del Río, Sánchez-de Prada, Arroyo-Hernantes, Álvarez, Tamayo and Gutiérrez-Abejón. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Laura Sánchez-de Prada, bGF1cmEuc2FuY2hlei5wcmFkYUB1dmEuZXM=