 Jorge Lima1
,2
*
†
Jorge Lima1
,2
*
†
 João Guerreiro3
†
João Guerreiro3
†
 Miguel Ângelo-Dias2
Sofia Silvério Serra4
Teresa Costa4
Natália Marto5
João Feldman de Pinho6
João Costa3
Rodrigo Ruano7
Gonçalo Silva Duarte3
,8
Miguel Ângelo-Dias2
Sofia Silvério Serra4
Teresa Costa4
Natália Marto5
João Feldman de Pinho6
João Costa3
Rodrigo Ruano7
Gonçalo Silva Duarte3
,8
- 1Department of Obstetrics and Gynecology, High-Risk Pregnancy Center, Hospital da Luz Lisboa, Lisbon, Portugal
- 2Comprehensive Health Research Centre–CHRC, NOVA Medical School, Faculdade de Ciências Médicas, NMS, FCM, Universidade NOVA de Lisboa, Lisbon, Portugal
- 3Laboratory of Clinical Pharmacology and Therapeutics, Faculdade de Medicina, Universidade de Lisboa, Lisbon, Portugal
- 4Library, NOVA Medical School, Faculdade de Ciências Médicas, NMS, FCM, Universidade NOVA de Lisboa, Lisbon, Portugal
- 5Department of Clinical Pharmacology, Hospital da Luz Lisboa, Lisbon, Portugal
- 6Department of Reproductive Endocrinology and Infertility at the Reproductive Centers of America, New York, NY, United States
- 7Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Miami and Jackson Memorial Hospital, Miami, FL, United States
- 8Clinical Pharmacology Unit, Unidade Local de Saúde Santa Maria, Lisbon, Portugal
Background: Approximately 50% of cases of recurrent pregnancy loss (RPL) remain unexplained, and there is a lack of consensus concerning the effective treatments for idiopathic RPL. We used network meta-analyses to evaluate the efficacy of several prophylactic therapeutic interventions used in women with idiopathic RPL.
Materials and methods: We conducted a systematic literature search using several databases from their inceptions to 20 July 2023. References from key articles were also manually searched. Randomized controlled trials assessing the efficacy and safety of any prophylactic intervention that were conducted in adult women with RPL were included. Studies with known causes of RPL were excluded. Two reviewers independently extracted data and assessed the risk of bias. Primary outcomes were live births and miscarriage rates. Secondary outcomes included serious adverse/adverse events and trial discontinuation. The network meta-analyses used a Bayesian hierarchical model with direct and indirect comparisons. Rank probabilities (assessed by surface under the cumulative ranking curve [SUCRA]) and certainty of evidence (assessed by Grading Recommendations Assessment, Development, and Evaluation [GRADE]) were also assessed.
Results: Thirty-eight studies (6,379 participants) were evaluated. No statistically significant differences in live birth rates among the interventions were found. The three best-ranked interventions for this outcome were prednisone plus progesterone plus aspirin (83%), leukocyte immune therapy (74%), and prednisolone (65%). Women who were treated with progesterone plus human chorionic gonadotrophin (instead of a placebo) presented an increase in miscarriage odds (odds ratio [OR] 3.83, 95% credible intervals [CrIs] 1.04–14.38). The three best-ranked interventions for miscarriage rate were prednisone plus progesterone plus aspirin (SUCRA = 81%), hydroxychloroquine (SUCRA = 79%), and intralipid (SUCRA = 65%). Overall, under placebo, 59% (95% confidence interval [CI] 51–67; I2 = 92%) of participants underwent successful live births, and 35% (95% CI 30–42, I2 = 86%) underwent miscarriages. We found no evidence of statistically significant differences between interventions (the top three interventions were low-molecular-weight heparin, granulocyte colony-stimulating factor, and leukocyte immune therapy) in those who discontinued trial participation.
Conclusion: Our results suggest that none of the analyzed interventions led to improvements in the live birth rate or a reduction in the miscarriage rate in women with idiopathic RPL.
Systematic review registration: https://www.crd.york.ac.uk/prospero, identifier CRD42023455668.
Introduction
Recurrent pregnancy loss (RPL) is defined as the failure of two or more clinical pregnancies before the point of fetal viability (up to 24 weeks of gestation). RPL presents a significant clinical challenge (1, 2). The prevalence of RPL has been reported as ranging from 0.8 to 3%, depending on population demographics, criteria for defining RPL, and the time of the study (3–8). The prevalence of RPL is nonetheless difficult to estimate due to challenges in obtaining accurate data concerning the number of experienced losses and the at-risk population of women, including all women of fertile age or those attempting to conceive. In addition, international guidelines vary in terms of their RPL definitions, with some of these guidelines defining it as two or more consecutive or non-consecutive pregnancy losses up to the 24th week of gestation (1, 2, 9), while others set the threshold at three or more losses up to the 14th (10) or 24th week (11). Therefore, such a lack of consensus can be challenging when comparing studies. However, clinicians are encouraged to use their clinical discretion to recommend extensive evaluation after two first-trimester miscarriages if the suspicion of a pathological nature of the losses is present.
Various causes and risk factors for RPL have been identified, including advanced maternal age, a history of multiple miscarriages, maternal distress, parental chromosomal abnormalities, uterine anatomical disorders, antiphospholipid syndrome, inherited thrombophilia, thyroid disorders, and environmental factors (12–16). However, approximately 50% of cases remain unexplained or idiopathic (1, 2, 11, 17). Such cases present a significant psychological burden for couples and healthcare providers (18). Since no evidence-based solutions for these women are available, treatment of these cases often involves empirical use of different treatment strategies, including acetylsalicylic acid, progesterone, corticosteroids, low-molecular-weight heparin (LMWH), intravenous immunoglobulin G (IVIG), lipid emulsion, and leukocyte immune therapy (19–21).
Despite thorough evaluations to identify presumptive risk factors and pathophysiologic mechanisms, physicians often fail to identify a specific target to direct a specific therapeutic intervention or prophylaxis for idiopathic RPL. Consequently, patients are often exposed to treatments based on theoretical hypotheses without proven efficacy (22).
Importantly, high-quality evidence regarding the therapeutic interventions of women with idiopathic RPL is scarce, and the current literature is insufficient to recommend any specific intervention for idiopathic RPL (1, 19). Furthermore, no systematic reviews and network meta-analyses (NMA) of randomized controlled trials (RCTs) have been published in which a comparison of the efficacy of the different therapeutic interventions used in women with idiopathic RPL may be particularly useful in assisting the clinical decision-making management options. Despite various proposed interventions, a lack of consensus exists concerning effective treatments for idiopathic RPL, thus emphasizing the need for this comprehensive network meta-analysis. Therefore, in this study, we used comprehensive NMA to evaluate the efficacy of various prophylactic therapeutic interventions for women with idiopathic RPL.
Materials and methods
Protocol and registration
This systematic review and NMA followed the Preferred Reporting Items Extension for Network Meta-Analyses (PRISMA-NMA; the checklist is presented in Supplementary Table S1) (23) guidelines and was registered with PROSPERO (ID: CRD42023455668) (24).
As a systematic review and NMA only involved the use of previously published data, no formal ethics approval or informed consent was required.
Data sources
A systematic literature search was conducted using the PubMed, EMBASE, Cochrane Library, Scopus, and Web of Science databases from their inceptions to 20 July 2023. The search strategy included terms related to idiopathic recurrent pregnancy loss and therapeutic interventions (see Supplementary Table S2). References from the most relevant studies were hand-screened to identify any eventual missing publications not retrieved by the electronic search.
Eligibility criteria and study selection
Inclusion criteria were RCTs that assessed the efficacy and safety of therapeutic interventions in adult women (>18 years) with idiopathic RPL.
RPL was defined as the loss of two or more clinical pregnancies before 24 weeks of gestation.
We excluded studies that included women with known diagnosed causes of RPL, including advanced maternal age (namely ≥40 years of age), parental chromosomal abnormalities, uterine anatomical disorders, inherited and/or acquired thrombophilia, thyroid disorders, and environmental factors. We also excluded cross-over trials due to the irrelevant nature of their study designs in the context of this review.
We imposed no restrictions on the number of recruited participants, number of recruitment centers, regional area, language, or year of publication. Unpublished studies (such as conference proceedings and poster or oral presentations) were also eligible for inclusion.
Two reviewers (GSD and JG) independently assessed all titles and abstracts of the retrieved search articles. Two reviewers (GSD and JG) conducted the selection of full-text articles for inclusion independently, and a third independent reviewer (JL) resolved any disagreements.
Data collection process and data items
From each study meeting the inclusion criteria, two reviewers (GSD and JG) independently analyzed and collected information on study authors, year of publication, primary outcome of each RCT, median or mean age of participants, RPL definition, and treatment arms (therapeutic intervention and dose). Disagreements were resolved after discussion with a third reviewer (JL). When more information was needed, the corresponding authors of the included studies were contacted to obtain or confirm data.
Primary and secondary outcome measures
Primary outcomes were the live birth and miscarriage rates. Secondary outcomes were serious adverse and adverse events and trial discontinuation.
We applied the International Council for Harmonization of Technical Requirements for Pharmaceuticals for Human Use (ICH) definitions of serious adverse events and adverse events (25).
Assessment of risk of bias within individual studies
Two reviewers (GSD and JG) independently evaluated the trial-level risk of bias using the Cochrane risk of bias tool for randomized trials (26). Disagreements were resolved after a discussion with a third reviewer (JC). Each trial’s overall risk of bias was divided into high or low risk.
Statistical analyses
The NMA involved both direct and indirect comparisons and was performed using a Bayesian hierarchical model (binomial modeling with a rate logit link function) supplemented with a Markov chain Monte Carlo approach (27, 28). We performed 10,000 adaptation steps followed by 100,000 iterations with a thinning factor of 10. All potential scale reduction factors were less than 1.05, indicating good convergence.
We constructed a network diagram for each outcome to illustrate all comparisons between therapeutic interventions. Each intervention was represented as a separate node, and the comparisons between interventions were depicted as links connecting these nodes. Node sizes corresponded to the number of participants who received an intervention, and connection sizes corresponded to the number of trials within a given comparison. Different doses of the same intervention were clustered into a single node.
For all models, we used vague prior distributions for all trial baselines and relative treatment or class effects and specifically selected normal distributions with a mean of 0 and a variance of 1002. For the random treatment effects models, we applied a minimally informative uniform prior distribution for the between-study heterogeneity parameter. For exchangeable-class models, we used a uniform (0, 5) prior distribution for the within-class standard deviation.
Fixed-, random-, and unrelated mean effects models were applied to each outcome and compared regarding the total residual deviances and the total number of data points to select the model that best fits the data. All outcomes were analyzed as binary variables using log odds ratios (log ORs), a binomial likelihood, and a complementary log–log (cloglog) link function. The outcomes were reported as odds ratios (ORs) with 95% confidence intervals (CIs) or 95% credible intervals (CrIs) as applicable. Heterogeneity between the included studies was evaluated using the heterogeneity index (I2) statistic and τ2 (tau-squared) value. A τ2 value greater than 0.5% indicated high statistical heterogeneity. Potential inconsistencies between direct and indirect evidence were assessed using the node-splitting method. To rank the therapeutic interventions, we used the surface under the cumulative ranking curve (SUCRA), for which higher values indicate a higher probability that a given intervention is associated with a better outcome. Publication bias was assessed using Peter’s test. Statistical significance was considered as p < 0.05 for all analyses. All statistical analyses were performed in R (version 4.3.2, R Foundation for Statistical Computing, Vienna, Austria) using the ‘gemtc’ package (version 0.8–7, GitHub, Inc., San Francisco, CA).
Assessment of certainty of evidence
The Grading of Recommendations Assessments, Development, and Evaluation (GRADE) approach was used to assess the certainty of the evidence for the outcomes of live birth and miscarriage rates and trial discontinuation of this NMA (29). Judgments concerning the certainty of evidence were obtained for several domains: (1) risk bias within studies, (2) indirectness, (3) inconsistency, and (4) imprecision. Supplementary Tables S3–S5 list all details of the GRADE assessment for each outcome.
Results
Study selection
Figure 1 depicts the PRISMA 2020 flow diagram for the systematic review process and study selection.
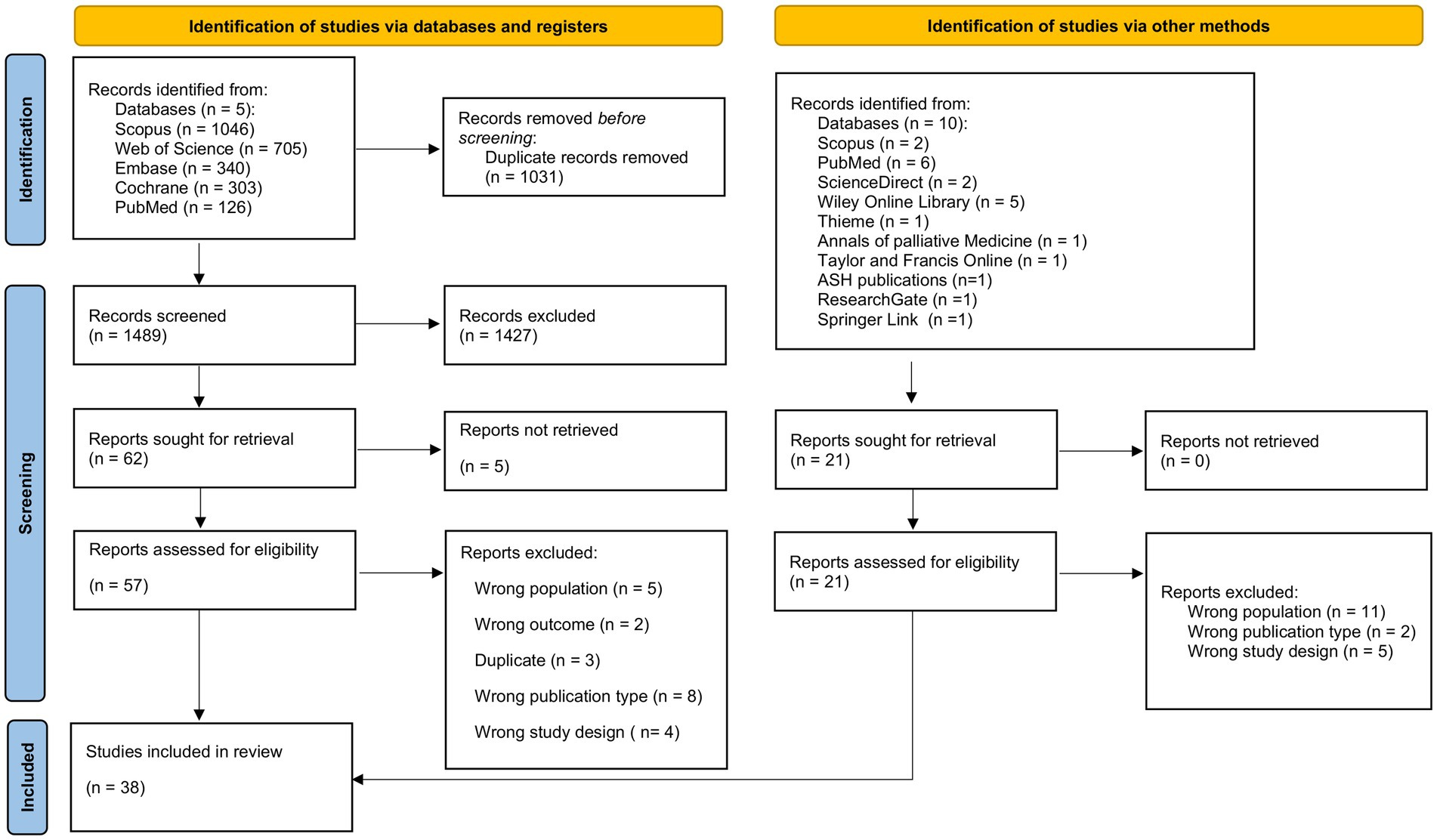
Figure 1. Preferred reporting items for systemic reviews and meta-analyses (PRISMA) 2020 flow diagram of systematic review process and study selection.
Our database search yielded 2,520 records, and after manually searching reference lists, we found an additional 21 records. We excluded 1,031 duplicates and 1,427 other records based on title and abstract screening. Five records were not retrieved, and after the review of 57 full-text articles, 22 studies were excluded due to wrong sample population (n = 5), wrong outcome (n = 2), duplicate (n = 3), wrong publication type (n = 8), and wrong study design (n = 4). In total, 38 RCTs (30–67) fulfilled all inclusion criteria and were included in our systematic review (Figure 1).
General characteristics of the studies
A total of 38 RCTs (30–67) with 6,379 participants were included in this study. Study characteristics are detailed in Table 1. The included studies were published between 1993 and 2022, and all were available in full-text format.
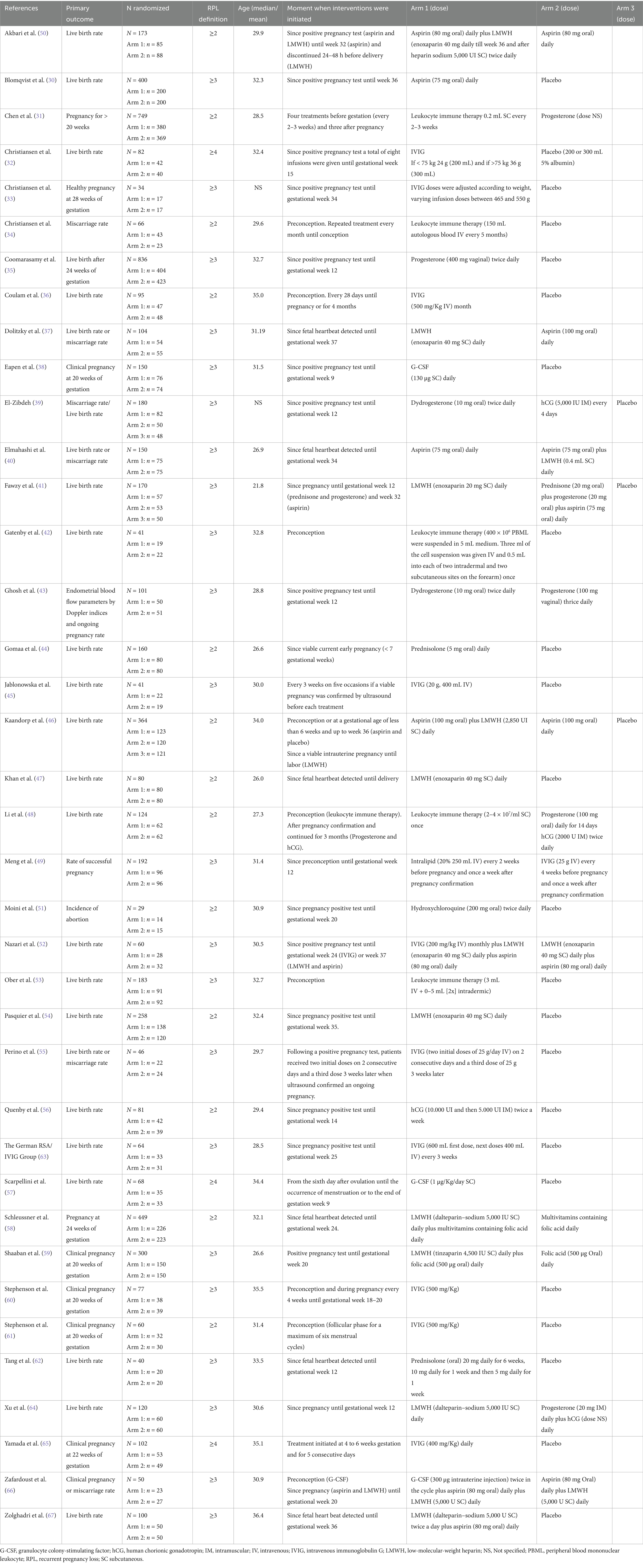
Table 1. Characteristics of the included studies.
Among these 38 articles, 13 (31, 34, 36, 44, 46–48, 50, 51, 54, 56, 58, 61) defined RPL as two or more miscarriages, 22 (30, 33, 35, 37–43, 45, 49, 52, 53, 55, 59, 60, 62–64, 66, 67) as three or more miscarriages, and three (32, 57, 65) as four or more miscarriages (Table 1).
Overall, the included studies included the following active interventions: (1) aspirin; (2) aspirin plus LMWH; (3) granulocyte colony-stimulating factor (G-CSF); (4) G-CSF plus aspirin plus LMWH; (5) human chorionic gonadotropin (hCG); (6) hydroxychloroquine; (7) intralipid; (8) IVIG; (9) IVIG plus LMWH plus aspirin; (10) leukocyte immune therapy; (11) LMWH; (12) prednisolone; (13) prednisone plus progesterone plus aspirin; (14) progesterone; (15) progesterone plus hCG (Table 1).
Participant ages ranged from 21.8 to 36.4 years on average. RCTs were generally two-arm trials (n = 35) (30–38, 40, 42–45, 47–67), with a smaller number being three-arm trials (n = 3) (39, 41, 46). The two most frequently studied therapeutic interventions were IVIG (n = 9) (32, 33, 36, 45, 55, 60, 61, 63, 65) and LMWH (n = 5) (37, 41, 47, 54, 64) (Table 1).
RCTs were not found to assess the efficacy and safety of levothyroxine, folic acid, multivitamins, clomiphene citrate, sitagliptin, metformin, and vitamin D for RPL (Table 1).
Risk of bias within individual studies
From the 38 included RCTs, 16 (41%) (31, 39, 40, 45–50, 52, 53, 58–60, 64, 67) were rated as having a high risk of bias. The main domains contributing to the bias rating were the risk of performance and detection bias. However, we also assessed six trials at a high (45, 49, 60) or unclear (46, 53, 59) risk of attrition bias (Table 2).

Table 2. Risk of bias assessment within individual studies according to the Cochrane risk of bias tool for randomized trials.
Model properties
Overall, we applied an NMA for the three outcomes: (1) live birth rate, (2) miscarriage rate, and (3) trial discontinuation. Despite being unable to conduct NMA due to a lack of data regarding both serious adverse and adverse events, we present the available data regarding these outcomes in Supplementary Tables S6, S7, respectively.
Supplementary Tables S8–S10 detail the model fit for each outcome. For all outcomes, only the random-effect models had similar total residual deviances when compared with the total number of data points, indicating an adequate fit of the results (Supplementary Tables S8–S10). Therefore, the results presented throughout this review pertain exclusively to the random-effects models.
The pairwise meta-analyses for live birth and miscarriage rates and trial discontinuation are presented in Figures 2–4, respectively. Regarding heterogeneity in pairwise meta-analysis, we found moderate-to-high levels of heterogeneity as reflected by high levels of tau2 and/or I2 in four of 14 contrasts in the NMA of live birth rate (aspirin versus aspirin plus LMWH [two trials], G-CSF versus placebo [two trials], LMWH versus placebo [five trials], and aspirin plus LMWH versus placebo [two trials]). In the miscarriage rate NMA, we found moderate-to-high levels of heterogeneity in five of 18 contrasts (leukocyte immune therapy versus placebo [two trials], progesterone versus placebo [two trials], G-CSF versus placebo [two trials], LMWH versus placebo [five trials], and aspirin plus LMWH versus placebo [two trials]). No contrasts in the NMA of trial discontinuations were found. Moreover, regarding heterogeneity, the between-study standard deviations across all outcomes were considered acceptable (Figures 2–4). Regarding inconsistency, the parameter estimates were similar for both the random effects and unrelated mean effects models, and considerable overlap in the 95% CrIs was observed (Supplementary Tables S8–S10). This finding suggests no evidence of global inconsistency in the network.
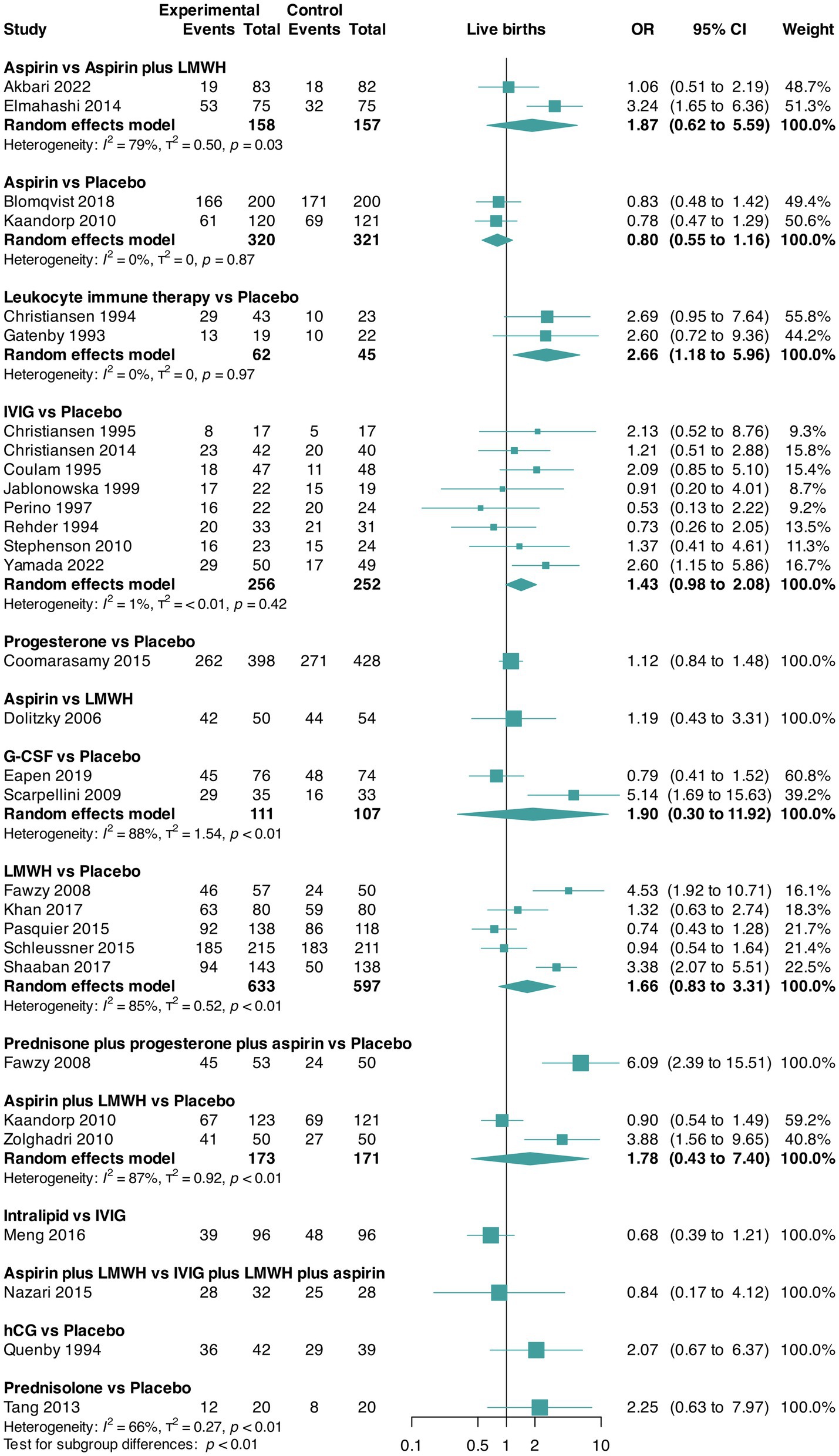
Figure 2. Pairwise meta-analysis for the outcome live birth rate. CI, confidence interval; G-CSF, granulocyte colony-stimulating factor; hCG, human chorionic gonadotropin; IVIG, intravenous immunoglobulin G; LMWH, low-molecular-weight heparin; OR, odds ratio.
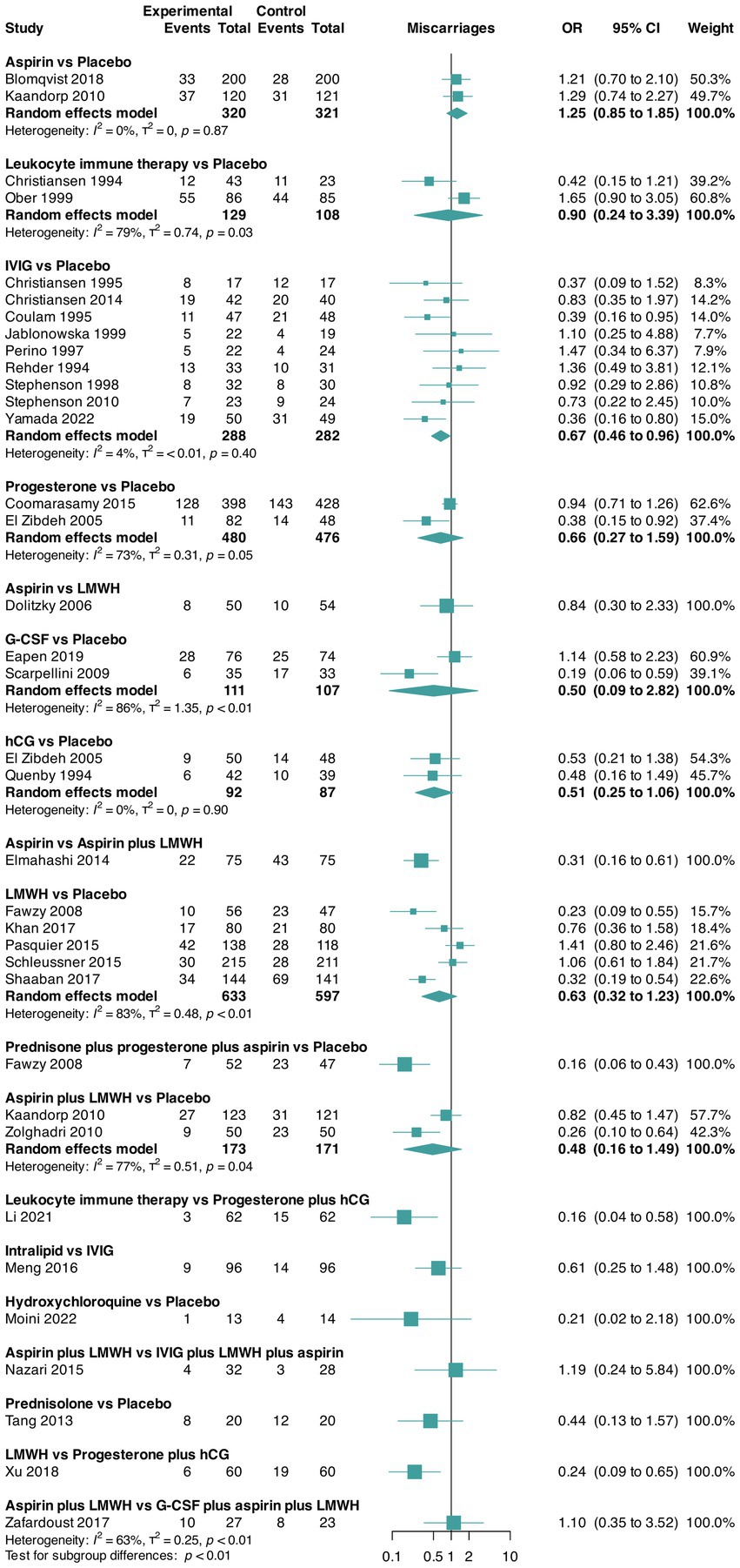
Figure 3. Pairwise meta-analysis for the outcome miscarriage rate. CI, confidence interval; G-CSF, granulocyte colony-stimulating factor; hCG, human chorionic gonadotropin; IVIG, intravenous immunoglobulin G; LMWH, low-molecular-weight heparin; OR, odds ratio.
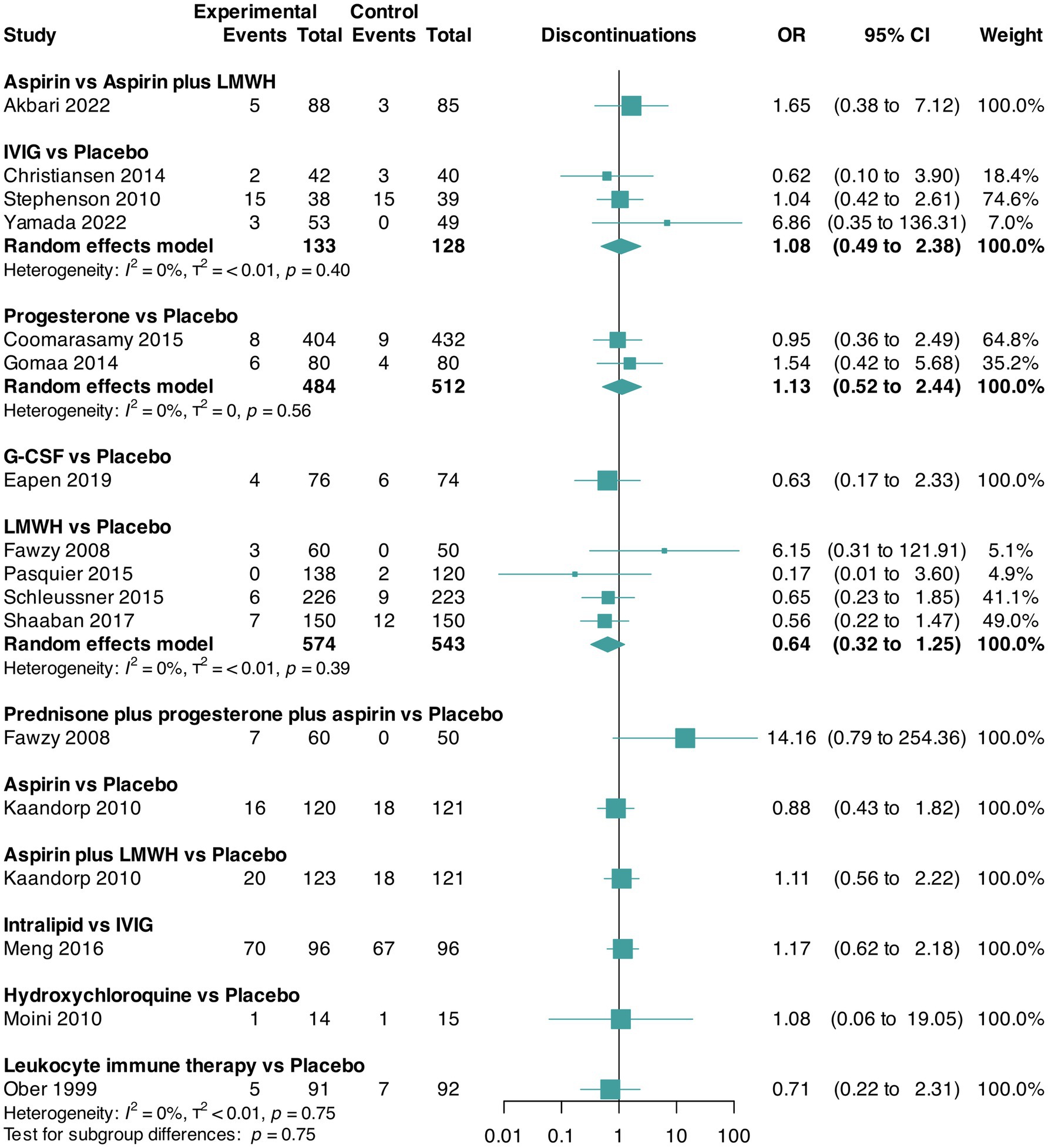
Figure 4. Pairwise meta-analysis for the outcome trial discontinuation. CI, confidence interval; G-CSF, granulocyte colony-stimulating factor; IVIG, intravenous immunoglobulin G; LMWH, low-molecular-weight heparin; OR, odds ratio.
Regarding inconsistency between direct and indirect evidence, node-split models suggest inconsistency in the comparison of placebo versus aspirin in both the outcomes live birth rate (Supplementary Figure S1) and miscarriage rate (Supplementary Figures S2, S3). Node-split analysis was not possible for the trial discontinuation outcome because of the network geometry for this outcome.
Live birth rate
The network plot with the comparisons between the therapeutic interventions for live birth rate is shown in Figure 5.
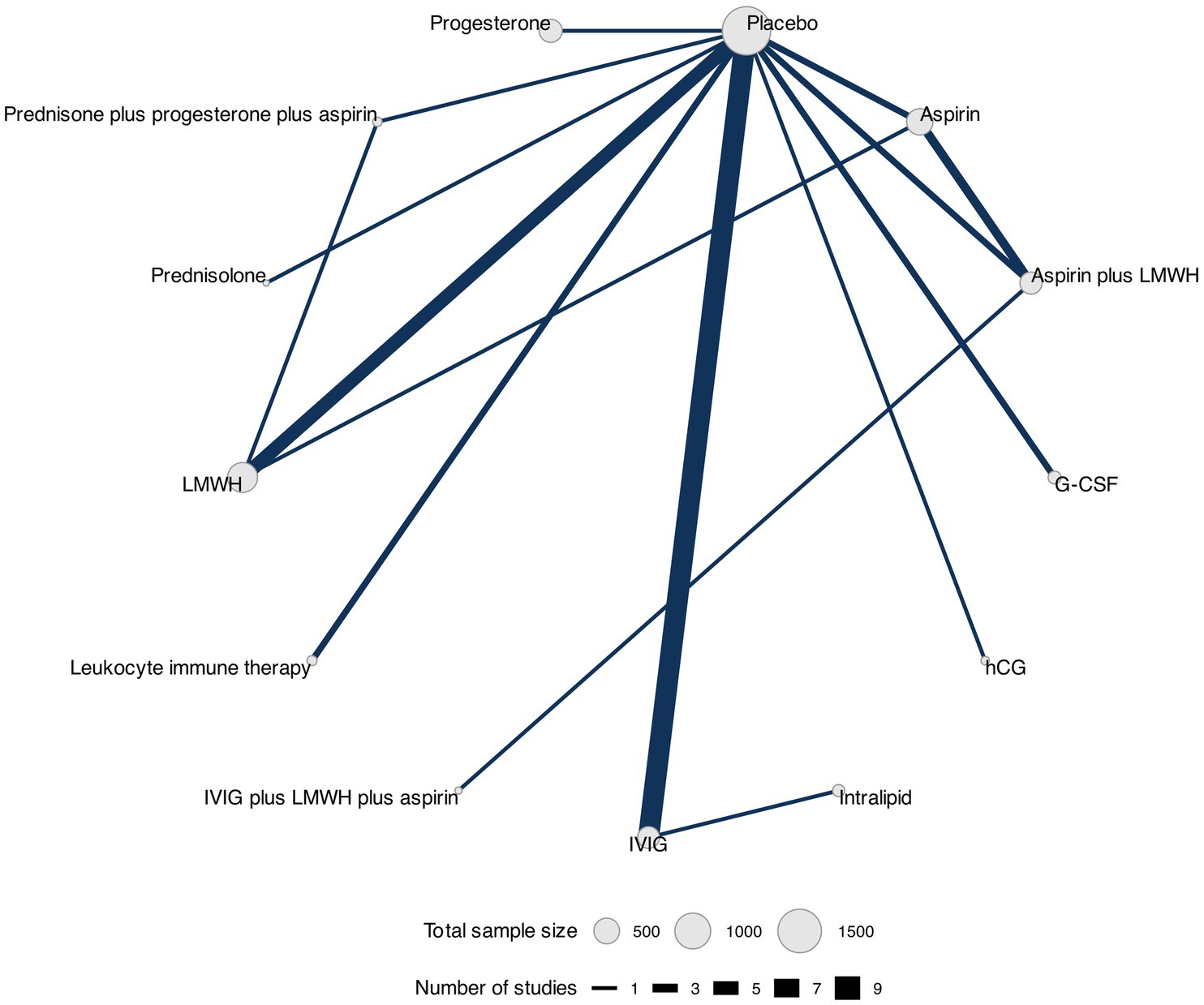
Figure 5. Network plot for live birth rate. Network plot showing comparisons in live birth rate between nodes (gray circles) in which each node represents a therapeutic intervention. The size of each node is proportional to the total number of participants assigned to that intervention, while the width of each connecting line is proportional to the number of studies conducting head-to-head comparisons between the two nodes.
Data for this outcome were reported in 28 RCTs (30, 32–38, 40–42, 45–47, 49, 50, 52, 54–60, 62, 63, 65, 67) (4,598 participants) that compared 13 interventions. Two RCTs were three-arm trials (41, 46) (Figure 2).
The network meta-analysis showed no statistically significant differences in live birth rates among the interventions (Table 3 and Supplementary Figure S4). The best-ranked interventions (according to the SUCRA, where higher values indicate more certainty that the intervention is the best-ranked in the comparison), as shown in Table 4, were prednisone plus progesterone plus aspirin (SUCRA = 83%), leukocyte immune therapy (SUCRA = 74%), and prednisolone (SUCRA = 65%). We did not find evidence of publication bias for this outcome (Peters test, p = 0.088), and the certainty of evidence of the relative treatment effects varied from low to moderate (Supplementary Table S3).
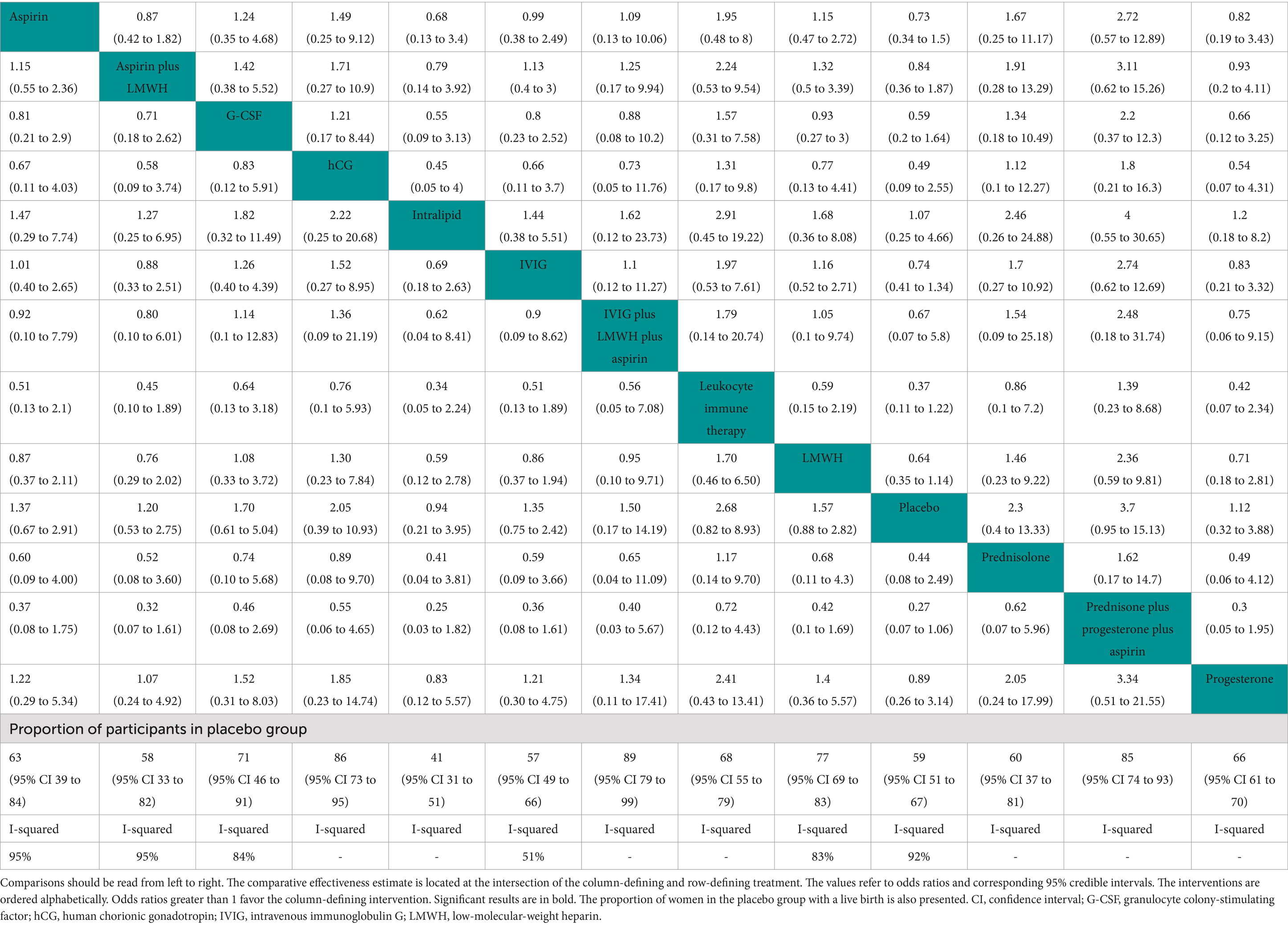
Table 3. League table showing the comparisons for the efficacy of each therapeutic intervention for live birth rate.
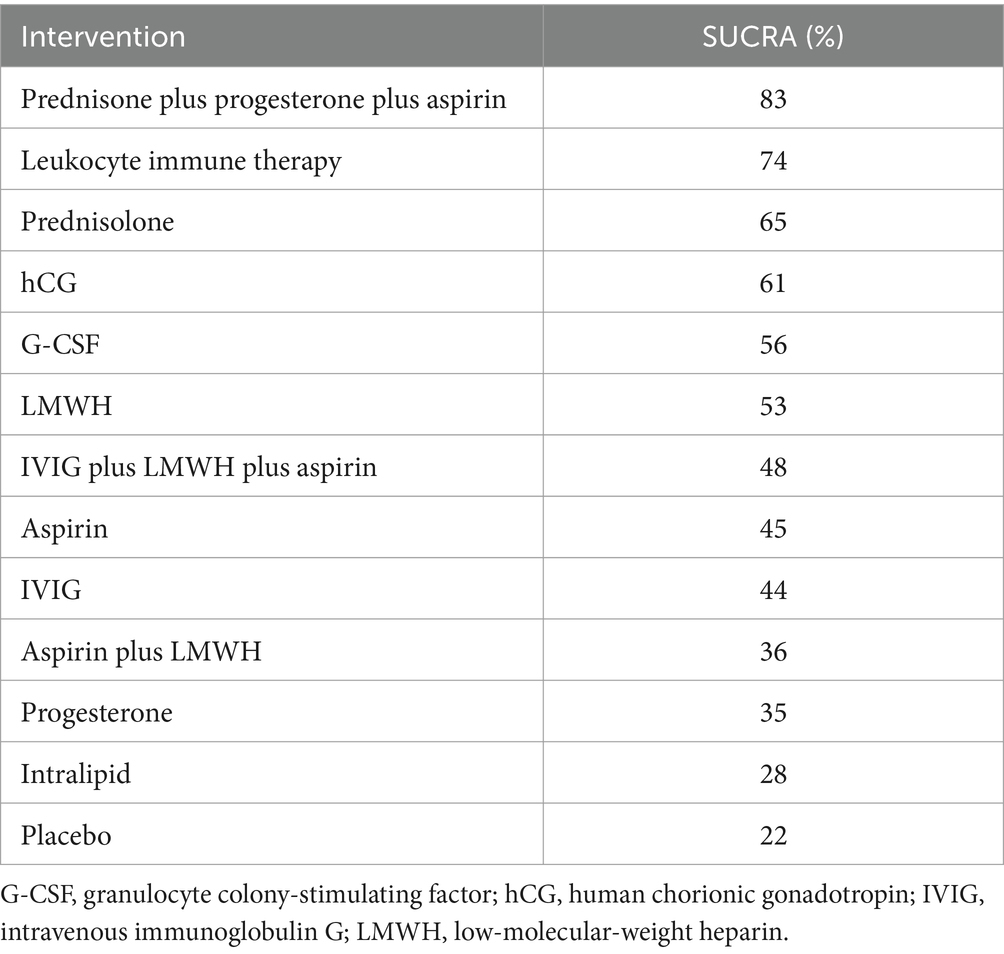
Table 4. Surface under the cumulative ranking curve (SUCRA) scores for live birth rate, expressed as a percentage, with higher values indicating a higher probability of an intervention being associated with a better outcome.
Based on 23 trials, the proportion of participants in the placebo group with a successful live birth was 59% (95% CI 51–67; I2 = 92%) (30, 32–36, 38, 41, 42, 45–47, 54–60, 62, 63, 65, 67) (Table 3).
Miscarriage rate
The network plot showing the comparisons between therapeutic interventions for miscarriage rate is shown in Figure 6.
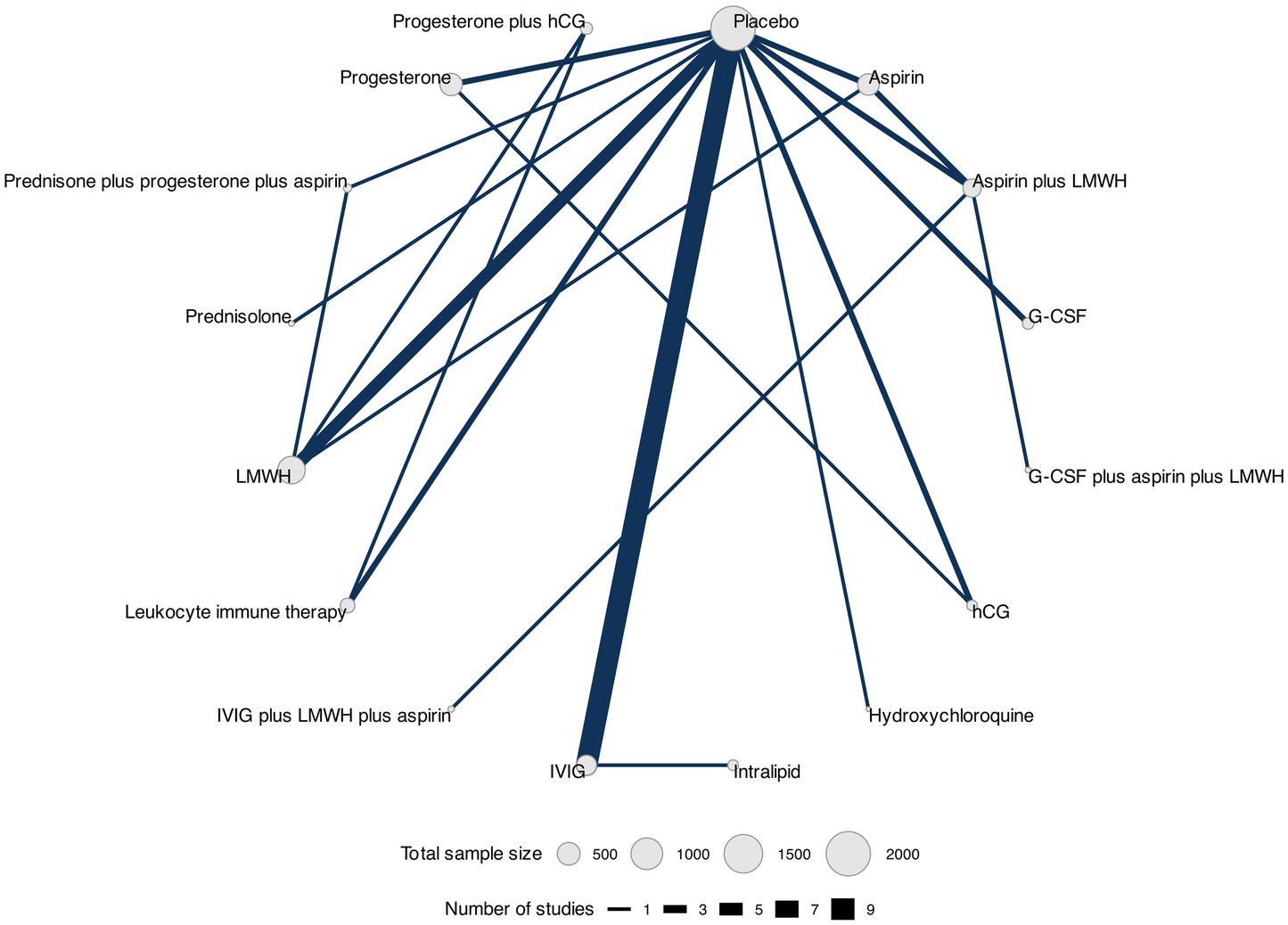
Figure 6. Network plot for miscarriage rate. Network plot showing comparisons in miscarriage rate between nodes (gray circles), each representing a therapeutic intervention. The size of each node is proportional to the total number of participants assigned to the intervention, and the width of each connecting line is proportional to the number of studies that have performed head-to-head comparisons between the two nodes.
Data for this outcome were reported in 33 RCTs (30, 32–41, 45–49, 51–67) (5,125 participants) that compared 16 interventions. Three RCTs were three-arm trials (39, 41, 46) (Figure 3).
Overall, we found evidence of statistically significant differences between a single intervention versus placebo, namely, progesterone plus hCG, which presented increased odds of miscarriage (OR 3.83, 95% CrIs 1.04–14.38) as shown in Table 5 and Supplementary Figure S5. The three best-ranked interventions in terms of miscarriage rate (according to the SUCRA, where higher values indicate more certainty that the intervention is the best-ranked in the comparison) were prednisone plus progesterone plus aspirin (SUCRA = 81%), hydroxychloroquine (SUCRA = 79%), and intralipid (SUCRA = 65%) as shown in Table 6. We did not find evidence of publication bias for this outcome (Peters test, p = 0.065), and the certainty of evidence of the relative treatment effects varied from very low and low to moderate (Supplementary Table S4).
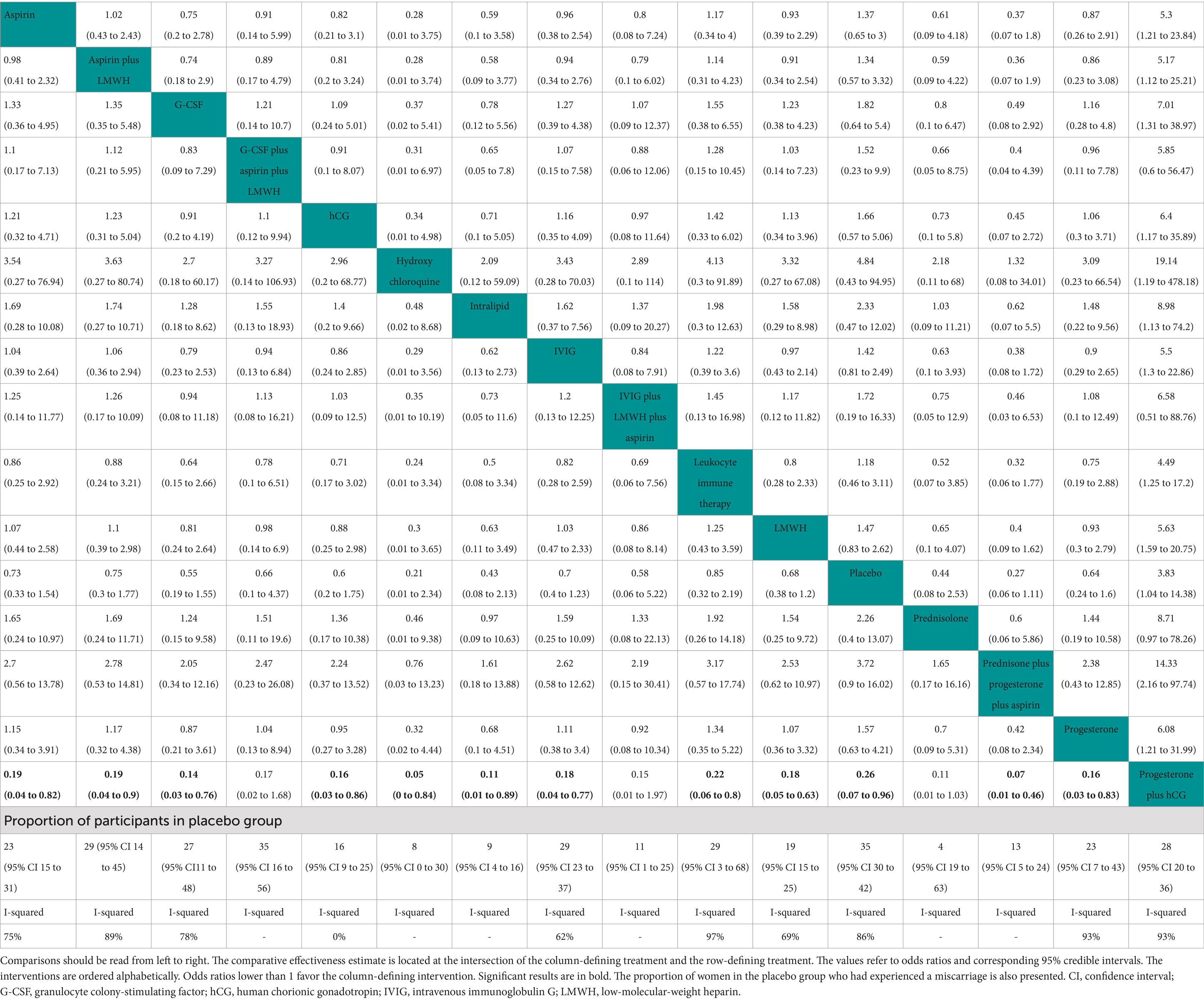
Table 5. League table showing the comparisons for the efficacy of each therapeutic intervention for miscarriage rate.
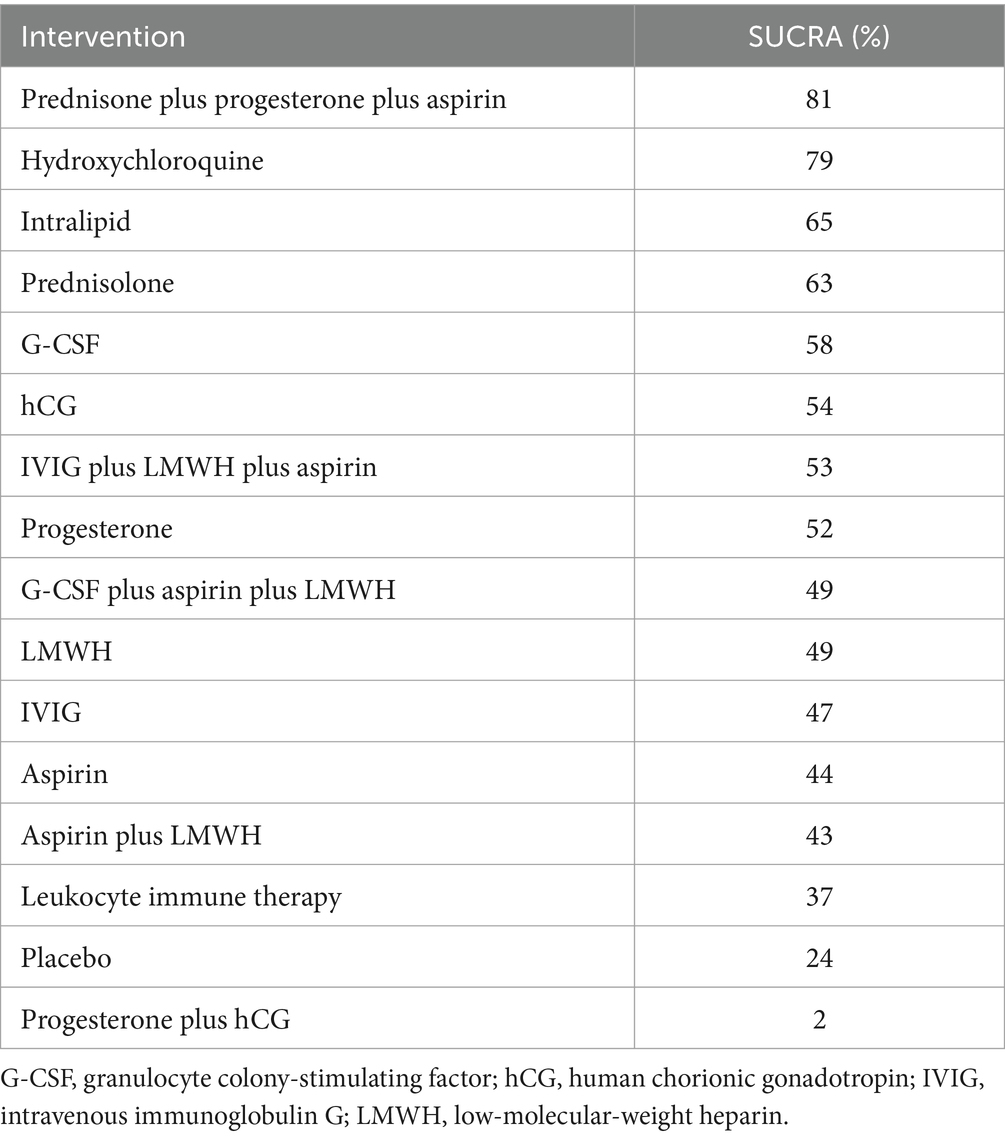
Table 6. Surface under the cumulative ranking curve (SUCRA) scores for miscarriage rate, expressed as a percentage, with higher values indicating a higher probability of an intervention being associated with a better outcome.
Based on 26 trials, the proportion of participants in the placebo group who underwent a miscarriage was 35% (95% CI 30–42; I2 = 86%) (30, 32–36, 38, 39, 41, 45–47, 51, 53–63, 65, 67) (Table 5).
Trial discontinuation
The network plot showing the comparisons between therapeutic interventions for trial discontinuation is shown in Figure 7.
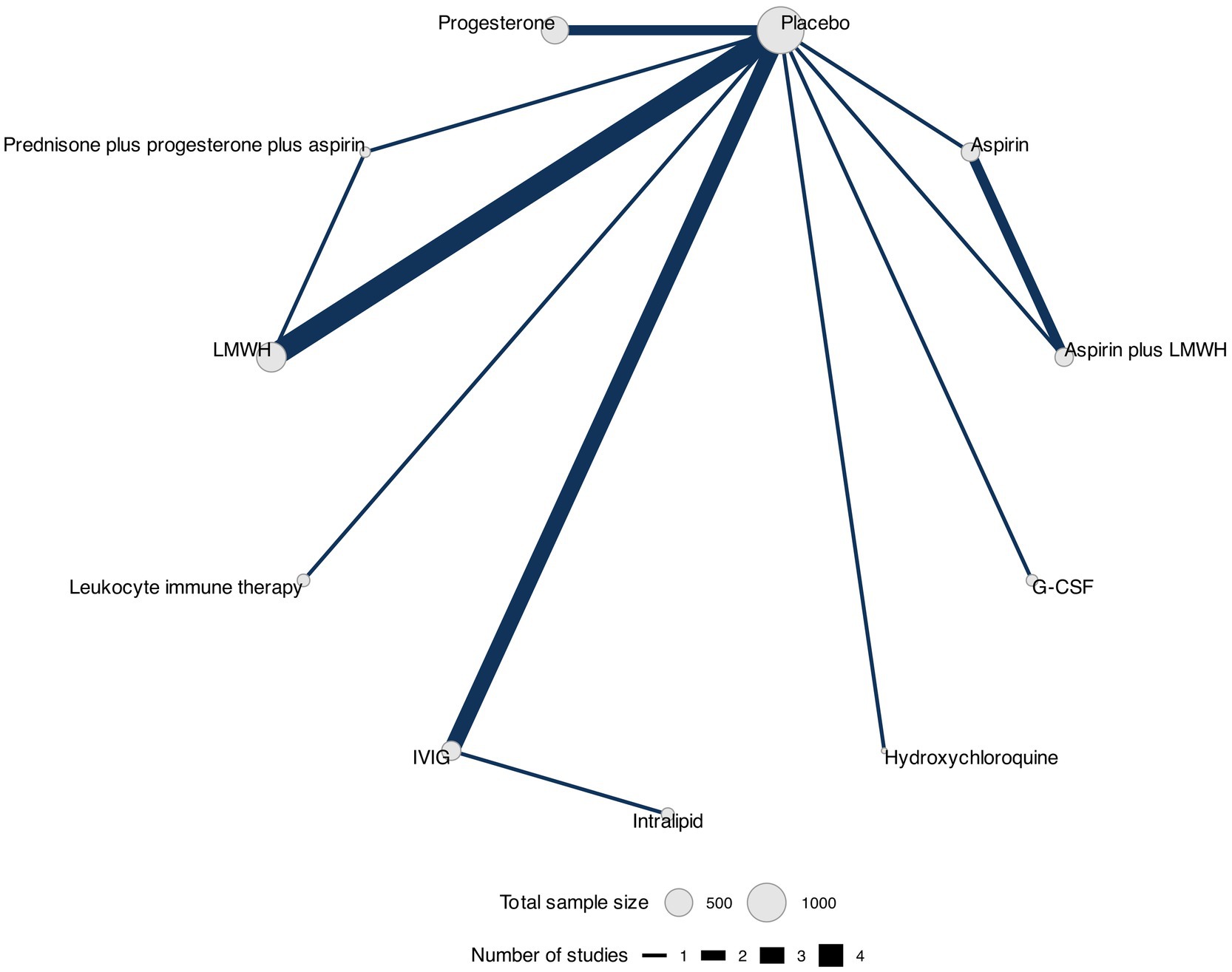
Figure 7. Network plot for trial discontinuation. Network plot showing comparisons in trial discontinuation between nodes (gray circles), each representing a therapeutic intervention. The size of each node is proportional to the total number of participants assigned to the intervention, and the width of each connecting line is proportional to the number of studies that have performed head-to-head comparisons between the two nodes.
Data for this outcome were reported in 15 RCTs (32, 35, 38, 41, 44, 46, 49–51, 53, 54, 58–60, 65) (3,525 participants) that compared 11 interventions. Two RCTs were three-arm trials (41, 46) (Figure 4).
We found no evidence of statistically significant differences between interventions in patients who discontinued participating in the trial (Table 7 and Supplementary Figure S6). The three best-ranked interventions regarding trial discontinuation were LMWH (SUCRA = 74%), G-CSF (SUCRA = 72%), and leukocyte immune therapy (SUCRA = 68%) as shown in Table 8. We did not find any evidence of publication bias for this outcome (Peters test, p = 0.32), and the certainty of evidence of the relative treatment effects varied from low to moderate (Supplementary Table S5).
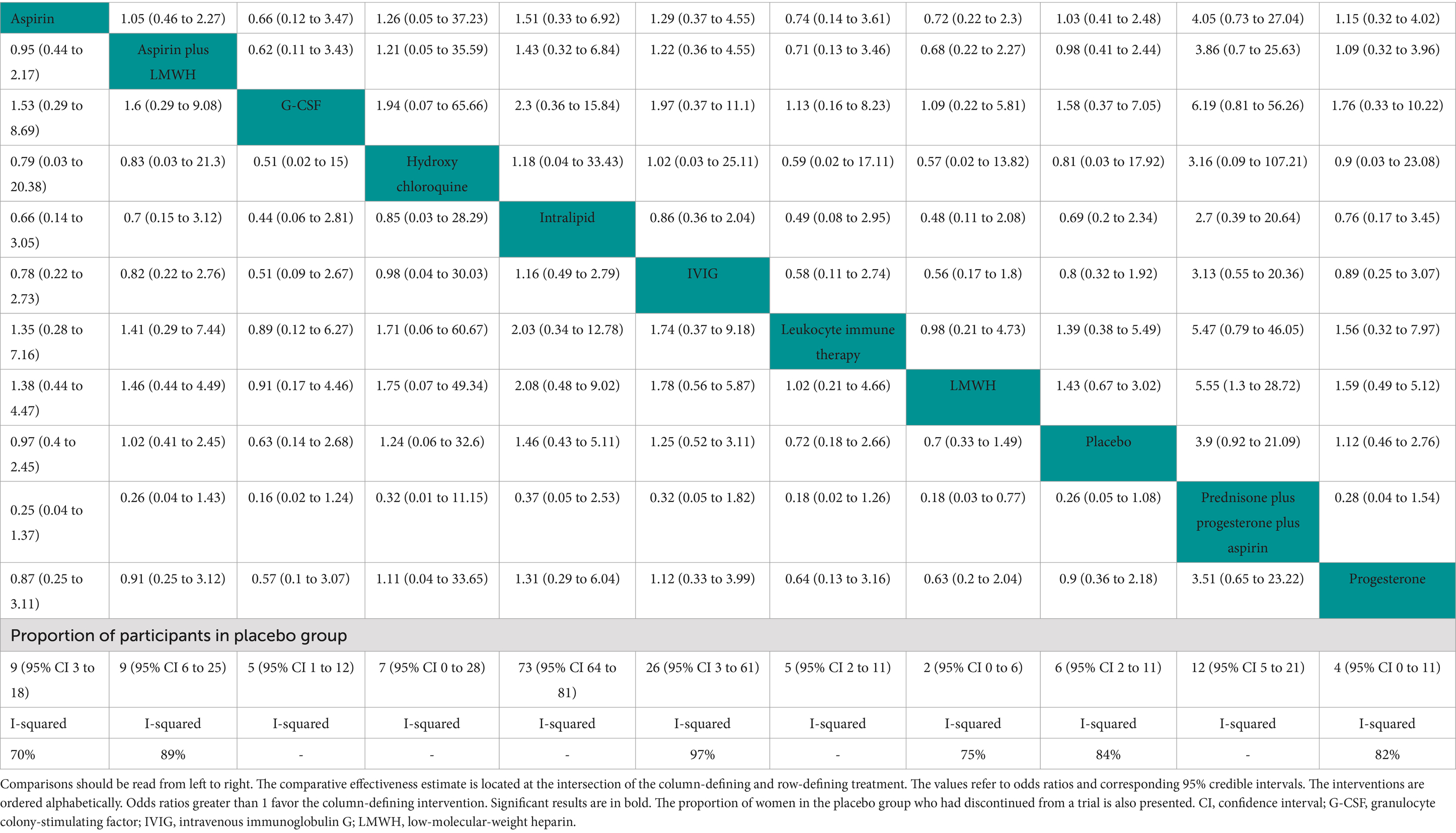
Table 7. League table showing the comparisons for the efficacy of each therapeutic intervention for trial discontinuation
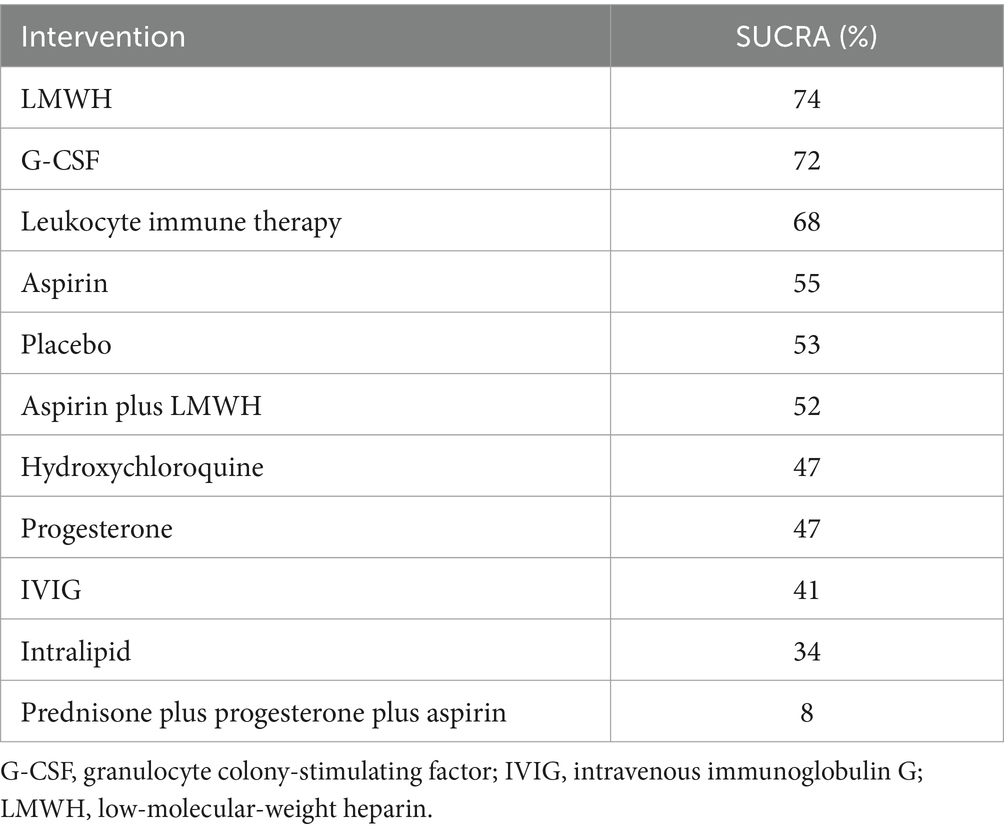
Table 8. Surface under the cumulative ranking curve (SUCRA) scores for trial discontinuation, expressed as a percentage, with higher values indicating a higher probability of an intervention being associated with a better outcome.
Based on 13 trials, 6% of the participants in the placebo group discontinued the trials (95% CI 2–11, I2 = 84%) (32, 35, 38, 41, 44, 46, 51, 53, 54, 58–60, 65) (Table 7).
Discussion
We applied NMA to compare the efficacy of several prophylactic therapeutic interventions in women with idiopathic RPL by synthesizing data from published RCTs. The primary outcomes included live birth and miscarriage rates, and the secondary outcomes were serious adverse/adverse events and trial discontinuation.
No significant differences between any of the interventions, including the placebo, were found concerning live birth rates. Nevertheless, based on this outcome, prednisone plus progesterone plus aspirin (first), leukocyte immune therapy (second), and prednisolone (third) were ranked among the top three interventions in terms of best live birth rates.
Regarding miscarriage rates, only progesterone plus hCG showed significant differences compared to other interventions, including placebos, as this treatment combination produced an increase in the odds of miscarriage. The three best-ranked interventions regarding this outcome were prednisone plus progesterone plus aspirin (first), hydroxychloroquine (second), and intralipid (third).
Regarding secondary outcomes, due to a lack of data concerning serious adverse/adverse events, we could not apply NMA to these outcomes.
Regarding trial discontinuations, we did not find statistically significant differences between the interventions assessed. This finding may reflect an equivalent tolerability to all assessed interventions in this specific population, which includes women who are highly motivated to adhere to a therapeutic option. However, the results do not reflect the totality of the available data. Following the standard recommendations for NMA, we excluded data from trials with no events in any trial arm.
The present analysis is comprehensive and introduces the idea of reevaluating the effects of different management therapeutic intervention options on both live birth and miscarriage rates and adverse events associated with the therapeutic interventions in women with idiopathic RPL. Furthermore, the certainty of evidence of the relative treatment effects varied from low to moderate for the live birth rate and trial discontinuation outcomes and from very low to moderate for the miscarriage rate outcome. These results emphasize the need for additional studies addressing the efficacy of therapeutic interventions used in idiopathic RPL in clinical trial settings. Our analysis found no significant improvements in live birth rates with any intervention, a finding that underscores the need for further research into effective therapies for idiopathic RPL.
This review was the first NMA that included data from published RCTs. Our review presents a thorough comparison of the efficacy of several therapeutic interventions in women with idiopathic RPL.
An earlier systematic review and meta-analyses examined the effects of different therapeutic interventions on live birth rates and adverse events associated with the interventions in women with idiopathic RPL (19). In these meta-analyses, the authors searched for RCTs until 2017 and included 21 studies (3,984 patients) assessing the effect of acetylsalicylic acid, LMWH, progesterone, IVIG, and leukocyte immune therapy in women who underwent three or more idiopathic RPL (19). The results from these meta-analyses indicated that no significant differences were found in live birth rates between the different therapeutic interventions, except for leukocyte immune therapy (risk ratio [RR] 1.8, 95% CI 1.34–2.41) and the use of progesterone initiated in the luteal phase (RR 1.18, 95% CI 1.09–1.27), which may be effective in improving live birth rates.(19) In contrast to our review and NMA, which included 38 eligible studies (6,379 participants), the authors did not include any RCT in which the intervention included corticosteroids, hydroxychloroquine, intralipid, G-CSF, and/or hCG. Furthermore, no serious adverse events or side effects were reported for the interventions analyzed in this meta-analysis (19). In contrast, in our study, conducting an NMA was not possible due to the scarcity of data regarding both serious adverse/adverse events in the included RCTs.
Using this network approach, which allows direct and indirect comparisons and subsequent ranking of the therapeutic interventions, we did not find any effective intervention that was capable of improving the live birth rate or reducing the miscarriage rate in women with idiopathic RPL. In contrast, we found evidence of statistically significant differences between the placebo and a single intervention, namely, progesterone combined with hCG, which was associated with an increase in the odds of miscarriage (OR 3.83, 95% CrIs 1.04–14.38).
Unfortunately, despite numerous advances in this field, several pregnancies still end in miscarriage; thus, no satisfactory explanation can be provided to approximately 50% of women with idiopathic RPL (1, 2, 11, 17). Therefore, a high number of women with idiopathic RPL are often exposed to therapeutic interventions based on theoretical hypotheses without proven efficacy (22). On the other hand, the prognosis is often favorable, and approximately two-thirds of women with a history of RPL may be able to undergo a subsequent pregnancy that results in a live birth even without therapeutic intervention and after being referred to a specialist (68).
Many empirical therapies aimed at reducing pro-inflammatory states and natural killer cell activity have been based on recent theories suggesting that immunological incompatibility at the maternal–fetal interface contributes to the pathophysiology of RPL (69, 70). The results of our NMA agree with other systematic reviews and meta-analyses that demonstrate that most of these immune therapies, which include corticosteroids, aspirin, LMWH, progesterone, hydroxychloroquine, IVIG, leukocyte immune therapy, intralipids, G-CSF, and tumor necrosis factor-alpha (TNF-α) antagonists, provide no significant and consistent beneficial effects over placebos in improving the live birth rates in women with RPL (19, 71–77).
Study strengths include a comprehensive search strategy and robust statistical analyses. We chose this recently described methodology in which data from randomized comparisons were combined to provide an internally consistent set of estimates while respecting the randomization of the evidence. This method may be a particularly useful tool in clinical decision-making scenarios. We believe that our NMA presents several additional strengths. To date, no systematic review and NMA of RCTs comparing the efficacy of therapeutic interventions for women with idiopathic RPL has been designed. We followed the PRISMA-NMA guidelines, and all results were reported according to the respective checklist (23). We conducted an extensive literature search with several updates to include all eligible trials containing high-quality data. Two independent reviewers extracted data and assessed the risk of bias using the Cochrane risk of bias tool. Discrepancies were resolved through discussion with a third reviewer. To attain the highest quality of evidence, this review included only RCTs, and the certainty of the generated evidence was assessed using the GRADE approach (29). We consider the inclusion of our team, which consisted of obstetricians, clinical pharmacologists, and librarians, as crucial for enhancing the integrity of our results and further validating the robustness of our network meta-analysis.
We acknowledge some limitations in our NMA. Two of the meta-analysis models assessed, namely, live birth rate and miscarriage rate, exhibited moderate-to-high levels of statistical heterogeneity, which may limit the generalizability of the findings. This heterogeneity likely stems from multiple factors, including variations in study design, different trial methodologies, and the complex interplay of genetic, immunological, and environmental influences on RPL. The presence of statistical heterogeneity underscores the need for caution when interpreting our results as the effectiveness of interventions may vary considerably depending on patient characteristics and study context. While subgroup analyses and meta-regression techniques can help explore potential sources of heterogeneity, they do not fully resolve the underlying uncertainty. Moreover, the sparse numbers of studies for each intervention in our systematic review preclude us from a rigorous assessment of this phenomenon. Future research should focus on identifying and characterizing specific subgroups of RPL patients to improve the precision and homogeneity of subsequent studies. In addition, the use of standardized definitions of RPL, rigorous study designs, and detailed reporting of patient characteristics will be essential for minimizing heterogeneity in future research and improving the reliability of findings in this complex field.
Most included studies did not provide data regarding serious adverse and/or adverse events; therefore, we could not assess the adverse events of the analyzed therapeutic interventions. Nevertheless, we presented the available data regarding these outcomes. In addition, the inclusion of studies with small samples could have raised the risk of bias in our NMA. Although we defined RPL as two or more clinically diagnosed miscarriages before 24 gestational weeks in this NMA, the heterogeneity of definitions and criteria applied by international guidelines for RPL in the different included RCTs can be considered a study limitation. The time at which the therapeutic interventions were initiated and their duration also differed in the included RCTs. Finally, our results were established based on both direct and indirect comparisons. Prospective RCTs should focus on direct comparisons of different therapeutic interventions, and future RCTs may further confirm the results of this NMA.
Furthermore, as already mentioned, the certainty of evidence of the relative treatment effects varied from low to moderate for the live birth rate and trial discontinuation outcomes and from very low to moderate for the miscarriage rate outcome, thus strengthening the urgent need for additional studies on the efficacy of therapeutic interventions used for idiopathic RPL in clinical trial settings.
Conclusion
RPL is a traumatic life event that affects women’s health. An increasing number of work-up and therapeutic options are being offered to women with this highly heterogeneous condition. Our NMA suggests that none of the analyzed therapeutic interventions, including placebo, led to improvements in live birth rates or reductions in miscarriage rates in women with idiopathic RPL. This study highlights the lack of effective interventions for improving live birth rates in women with idiopathic RPL and emphasizes the need for continued research in this area. Additional studies on the efficacy of therapeutic interventions used in idiopathic RPL in clinical trial settings are urgently needed and must include investigating potential adverse events associated with these interventions. Future studies should focus on large-scale RCTs by directly comparing these interventions and assessing long-term outcomes.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
Author contributions
JL: Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing. JG: Conceptualization, Investigation, Visualization, Writing – original draft. MÂ-D: Conceptualization, Investigation, Visualization, Writing – review & editing. SS: Conceptualization, Data curation, Writing – review & editing. TC: Conceptualization, Data curation, Writing – review & editing. NM: Conceptualization, Writing – review & editing. JP: Conceptualization, Validation, Writing – review & editing. JC: Conceptualization, Formal analysis, Software, Validation, Writing – review & editing. RR: Conceptualization, Writing – review & editing. GD: Conceptualization, Data curation, Formal analysis, Methodology, Software, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study in the context of the “Women’s Health and Maternal Fetal Research Group” was partially co-financed by Hospital da Luz Lisboa under the initiative “Luz Investigação.” The sponsor did not have any role in the study design, in the collection, analysis, and interpretation of data, in the report’s writing, and in the decision to submit the article for publication.
Acknowledgments
The authors would like to acknowledge Sofia Nunes, PhD (Scientific ToolBox Consulting, Lisbon, Portugal), for providing medical writing assistance and technical editing.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1569819/full#supplementary-material
Abbreviations
CI, confidence interval; CrI, credible interval; G-CSF, granulocyte colony-stimulating factor; GRADE, Grading Recommendations Assessment, Development, and Evaluation; hCG, human chorionic gonadotropin; ICH, International Council for Harmonization of Technical Requirements for Pharmaceuticals for Human Use; IVIG, intravenous immunoglobulin G; LMWH, low-molecular-weight heparin; NMA, network meta-analyses; OR, odds ratio; PRISMA-NMA, Preferred Reporting Items Extension for Network Meta-Analyses; RCTs, randomized controlled trials; RPL, recurrent pregnancy loss; RR, risk ratio; SUCRA, surface under the cumulative ranking curve.
References
1. Eshre Guideline Group on RPLBender Atik, R, Christiansen, OB, Elson, J, Kolte, AM, Lewis, S, et al. ESHRE guideline: recurrent pregnancy loss: an update in 2022. Hum Reprod Open. (2023) 2023:hoad002. doi: 10.1093/hropen/hoad002
2. de Assis, V, Giugni, CS, and Ros, ST. Evaluation of recurrent pregnancy loss. Obstet Gynecol. (2024) 143:645–59. doi: 10.1097/AOG.0000000000005498
3. Stray-Pedersen, B, and Lorentzen-Styr, AM. The prevalence of toxoplasma antibodies among 11, 736 pregnant women in Norway. Scand J Infect Dis. (1979) 11:159–65. doi: 10.3109/inf.1979.11.issue-2.12
4. Sugiura-Ogasawara, M, Suzuki, S, Ozaki, Y, Katano, K, Suzumori, N, and Kitaori, T. Frequency of recurrent spontaneous abortion and its influence on further marital relationship and illness: the Okazaki cohort study in Japan. J Obstet Gynaecol Res. (2013) 39:126–31. doi: 10.1111/j.1447-0756.2012.01973.x
5. Stephenson, MD. Frequency of factors associated with habitual abortion in 197 couples. Fertil Steril. (1996) 66:24–9.
6. Ford, HB, and Schust, DJ. Recurrent pregnancy loss: etiology, diagnosis, and therapy. Rev. Obstet Gynecol. (2009) 2:76–83.
7. Larsen, EC, Christiansen, OB, Kolte, AM, and Macklon, N. New insights into mechanisms behind miscarriage. BMC Med. (2013) 11:154. doi: 10.1186/1741-7015-11-154
8. Alberman, E. The epidemiology of repeated abortion In: F Sharp and RW Beard, editors. Early pregnancy loss. London: Springer (1988). 9–17.
9. Practice Committee of the American Society for Reproductive Medicine. Electronic address, a. a. o. Definitions of infertility and recurrent pregnancy loss: a committee opinion. Fertil Steril. (2020) 113:533–5. doi: 10.1016/j.fertnstert.2019.11.025
10. Delabaere, A, Huchon, C, Lavoue, V, Lejeune, V, Iraola, E, Nedellec, S, et al. Definition of pregnancy losses: standardization of terminology from the French National College of obstetricians and gynecologists (CNGOF). J Gynecol Obstet Biol Reprod (Paris). (2014) 43:756–63. doi: 10.1016/j.jgyn.2014.09.010
11. Regan, L, Rai, R, Saravelos, S, and Li, TCRoyal College of Obstetricians and Gynaecologists. Recurrent miscarriage green-top guideline no. 17. BJOG. (2023) 130:e9–e39. doi: 10.1111/1471-0528.17515
12. Branch, DW, Gibson, M, and Silver, RM. Clinical practice. Recurrent miscarriage. N Engl J Med. (2010) 363:1740–7. doi: 10.1056/NEJMcp1005330
13. Jeve, YB, and Davies, W. Evidence-based management of recurrent miscarriages. J Hum Reprod Sci. (2014) 7:159–69. doi: 10.4103/0974-1208.142475
14. Arias-Sosa, LA, Acosta, ID, Lucena-Quevedo, E, Moreno-Ortiz, H, Esteban-Perez, C, and Forero-Castro, M. Genetic and epigenetic variations associated with idiopathic recurrent pregnancy loss. J Assist Reprod Genet. (2018) 35:355–66. doi: 10.1007/s10815-017-1108-y
15. Quenby, S, Gallos, ID, Dhillon-Smith, RK, Podesek, M, Stephenson, MD, Fisher, J, et al. Miscarriage matters: the epidemiological, physical, psychological, and economic costs of early pregnancy loss. Lancet. (2021) 397:1658–67. doi: 10.1016/S0140-6736(21)00682-6
16. Turesheva, A, Aimagambetova, G, Ukybassova, T, Marat, A, Kanabekova, P, Kaldygulova, L, et al. Recurrent pregnancy loss etiology, risk factors, diagnosis, and management. Fresh look into a full box. J Clin Med. (2023) 12:1–26. doi: 10.3390/jcm12124074
17. Daya, S, and Stephenson, MD. Frequency of factors associated with habitual abortion in 197 couples. Fertil Steril. (1996) 66:24–9. doi: 10.1016/s0015-0282(16)58382-4
18. Kolte, AM, Olsen, LR, Mikkelsen, EM, Christiansen, OB, and Nielsen, HS. Depression and emotional stress is highly prevalent among women with recurrent pregnancy loss. Hum Reprod. (2015) 30:777–82. doi: 10.1093/humrep/dev014
19. Rasmark Roepke, E, Hellgren, M, Hjertberg, R, Blomqvist, L, Matthiesen, L, Henic, E, et al. Treatment efficacy for idiopathic recurrent pregnancy loss - a systematic review and meta-analyses. Acta Obstet Gynecol Scand. (2018) 97:921–41. doi: 10.1111/aogs.13352
20. Jauniaux, E, Farquharson, RG, Christiansen, OB, and Exalto, N. Evidence-based guidelines for the investigation and medical treatment of recurrent miscarriage. Hum Reprod. (2006) 21:2216–22. doi: 10.1093/humrep/del150
21. Diejomaoh, MF. Recurrent spontaneous miscarriage is still a challenging diagnostic and therapeutic quagmire. Med Princ Pract. (2015) 24:38–55. doi: 10.1159/000365973
22. Matthiesen, L, Kalkunte, S, and Sharma, S. Multiple pregnancy failures: an immunological paradigm. Am J Reprod Immunol. (2012) 67:334–40. doi: 10.1111/j.1600-0897.2012.01121.x
23. Hutton, B, Salanti, G, Caldwell, DM, Chaimani, A, Schmid, CH, Cameron, C, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. (2015) 162:777–84. doi: 10.7326/M14-2385
24. Lima, J., Duarte, G. S., Ângelo-Dias, M., Serra, S. S., Dias, S. S., and Marto, N. (2023). Interventions to improve live birth rate in women with idiopathic recurrent pregnancy loss: A systematic review and network meta-analysis. PROSPERO 2023 CRD42023455668 Available online at: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023455668 (Accessed September 1, 2024).
25. ICH Expert Working Group. International council for harmonisation of technical requirements for pharmaceuticals for human use, ICH Topic E 2 A: clinical safety data management: definitions and standards for expedited reporting (1995)
26. Higgins, JPT, Altman, DG, Gøtzsche, PC, Jüni, P, Moher, D, Oxman, AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. (2011) 343:d5928. doi: 10.1136/bmj.d5928
27. Dias, S, Sutton, AJ, Ades, AE, and Welton, NJ. Evidence synthesis for decision making 2: a generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med Decis Mak. (2013) 33:607–17. doi: 10.1177/0272989X12458724
28. van Ravenzwaaij, D, Cassey, P, and Brown, SD. A simple introduction to Markov chain Monte-Carlo sampling. Psychon Bull Rev. (2018) 25:143–54. doi: 10.3758/s13423-016-1015-8
29. Brignardello-Petersen, R, Mustafa, RA, Siemieniuk, RAC, Murad, MH, Agoritsas, T, Izcovich, A, et al. GRADE approach to rate the certainty from a network meta-analysis: addressing incoherence. J Clin Epidemiol. (2019) 108:77–85. doi: 10.1016/j.jclinepi.2018.11.025
30. Blomqvist, L, Hellgren, M, and Strandell, A. Acetylsalicylic acid does not prevent first-trimester unexplained recurrent pregnancy loss: a randomized controlled trial. Acta Obstet Gynecol Scand. (2018) 97:1365–72. doi: 10.1111/aogs.13420
31. Chen, JL, Yang, JM, Huang, YZ, and Li, Y. Clinical observation of lymphocyte active immunotherapy in 380 patients with unexplained recurrent spontaneous abortion. Int Immunopharmacol. (2016) 40:347–50. doi: 10.1016/j.intimp.2016.09.018
32. Christiansen, OB, Larsen, EC, Egerup, P, Lunoee, L, Egestad, L, and Nielsen, HS. Intravenous immunoglobulin treatment for secondary recurrent miscarriage: a randomised, double-blind, placebo-controlled trial. BJOG. (2014) 122:500–8. doi: 10.1111/1471-0528.13192
33. Christiansen, OB, Mathiesen, O, Husth, M, Rasmussen, KL, Ingerslev, HJ, Lauritsen, JG, et al. Placebo-controlled trial of treatment of unexplained secondary recurrent spontaneous abortions and recurrent late spontaneous abortions with i. v. Immunoglobulin. Hum Reprod. (1995) 10:2690–5. doi: 10.1093/oxfordjournals.humrep.a135769
34. Christiansen, OB, Mathiesen, O, Husth, M, Lauritsen, JG, and Grunnet, N. Placebo-controlled trial of active immunization with third party leukocytes in recurrent miscarriage. Acta Obstet Gynecol Scand. (1994) 73:261–8. doi: 10.3109/00016349409023451
35. Coomarasamy, A, Williams, H, Truchanowicz, E, Seed, PT, Small, R, Quenby, S, et al. A randomized trial of progesterone in women with recurrent miscarriages. N Engl J Med. (2015) 373:2141–8. doi: 10.1056/NEJMoa1504927
36. Coulam, CB, Krysa, L, Stern, JJ, and Bustillo, M. Intravenous immunoglobulin for treatment of recurrent pregnancy loss. Am J Reprod Immunol. (1995) 34:333–7. doi: 10.1111/j.1600-0897.1995.tb00960.x
37. Dolitzky, M, Inbal, A, Segal, Y, Weiss, A, Brenner, B, and Carp, H. A randomized study of thromboprophylaxis in women with unexplained consecutive recurrent miscarriages. Fertil Steril. (2006) 86:362–6. doi: 10.1016/j.fertnstert.2005.12.068
38. Eapen, A, Joing, M, Kwon, P, Tong, J, Maneta, E, De Santo, C, et al. Recombinant human granulocyte-colony stimulating factor in women with unexplained recurrent pregnancy losses: a randomized clinical trial. Hum Reprod. (2019) 34:424–32. doi: 10.1093/humrep/dey393
39. El-Zibdeh, MY. Dydrogesterone in the reduction of recurrent spontaneous abortion. J Steroid Biochem Mol Biol. (2005) 97:431–4. doi: 10.1016/j.jsbmb.2005.08.007
40. Elmahashi, MO, Elbareg, AM, Essadi, FM, Ashur, BM, and Adam, I. Low dose aspirin and low-molecular-weight heparin in the treatment of pregnant Libyan women with recurrent miscarriage. BMC Res Notes. (2014) 7:23. doi: 10.1186/1756-0500-7-23
41. Fawzy, M, Shokeir, T, El-Tatongy, M, Warda, O, El-Refaiey, AA, and Mosbah, A. Treatment options and pregnancy outcome in women with idiopathic recurrent miscarriage: a randomized placebo-controlled study. Arch Gynecol Obstet. (2008) 278:33–8. doi: 10.1007/s00404-007-0527-x
42. Gatenby, PA, Cameron, K, Simes, RJ, Adelstein, S, Bennett, MJ, Jansen, RP, et al. Treatment of recurrent spontaneous abortion by immunization with paternal lymphocytes: results of a controlled trial. Am J Reprod Immunol. (1993) 29:88–94. doi: 10.1111/j.1600-0897.1993.tb00571.x
43. Ghosh, S, Chattopadhyay, R, Goswami, S, Chaudhury, K, Chakravarty, B, and Ganesh, A. Assessment of sub-endometrial blood flow parameters following dydrogesterone and micronized vaginal progesterone administration in women with idiopathic recurrent miscarriage: a pilot study. J Obstet Gynaecol Res. (2014) 40:1871–6. doi: 10.1111/jog.12456
44. Gomaa, MF, Elkholy, AG, El-Said, MM, and Abdel-Salam, NE. Combined oral prednisolone and heparin versus heparin: the effect on peripheral NK cells and clinical outcome in patients with unexplained recurrent miscarriage. A double-blind placebo randomized controlled trial. Arch Gynecol Obstet. (2014) 290:757–62. doi: 10.1007/s00404-014-3262-0
45. Jablonowska, B, Selbing, A, Palfi, M, Ernerudh, J, Kjellberg, S, and Lindton, B. Prevention of recurrent spontaneous abortion by intravenous immunoglobulin: a double-blind placebo-controlled study. Hum Reprod. (1999) 14:838–41. doi: 10.1093/humrep/14.3.838
46. Kaandorp, SP, Goddijn, M, van der Post, JA, Hutten, BA, Verhoeve, HR, Hamulyak, K, et al. Aspirin plus heparin or aspirin alone in women with recurrent miscarriage. N Engl J Med. (2010) 362:1586–96. doi: 10.1056/NEJMoa1000641
47. Khan, ES, Basharat, A, Jamil, M, Ayub, S, and Khan, MA. Preventive role of low-molecular-weight heparin in unexplained recurrent pregnancy loss. S Afr J Obstet Gynaecol. (2017) 23:17–9. doi: 10.7196/SAJOG.2017.v23i1.1112
48. Li, J, Gu, Y, Zhang, S, Ju, B, and Wang, J. Effect of prepregnancy lymphocyte active immunotherapy on unexplained recurrent miscarriage, pregnancy success rate, and maternal-infant outcome. Biomed Res Int. (2021) 2021:7878752. doi: 10.1155/2021/7878752
49. Meng, L, Lin, J, Chen, L, Wang, Z, Liu, M, Liu, Y, et al. Effectiveness and potential mechanisms of intralipid in treating unexplained recurrent spontaneous abortion. Arch Gynecol Obstet. (2016) 294:29–39. doi: 10.1007/s00404-015-3922-8
50. Mohammad-Akbari, A, Mohazzab, A, Tavakoli, M, Karimi, A, Zafardoust, S, Zolghadri, Z, et al. The effect of low-molecular-weight heparin on live birth rate of patients with unexplained early recurrent pregnancy loss: a two-arm randomized clinical trial. J Res Med Sci. (2022) 27:78. doi: 10.4103/jrms.jrms_81_21
51. Moini, A, Sepidarkish, M, Dehpour, AR, Rabiei, M, Abiri, A, and Pirjani, R. The effect of hydroxychloroquine on pregnancy outcomes in patients with unexplained recurrent pregnancy loss: a placebo-controlled study "pilot study". J Obstet Gynaecol. (2022) 42:3471–6. doi: 10.1080/01443615.2022.2141615
52. Nazari, Z, Ghaffari, J, and Ebadi, A. Comparison of the effect of aspirin and heparin with or without intravenous immunoglobulin in treatment of recurrent abortion with unknown etiology: a clinical study. J Nat Sci Biol Med. (2015) 6:17–21. doi: 10.4103/0976-9668.166054
53. Ober, C, Karrison, T, Odem, RR, Barnes, RB, Branch, DW, Stephenson, MD, et al. Mononuclear-cell immunisation in prevention of recurrent miscarriages: a randomised trial. Lancet. (1999) 354:365–9. doi: 10.1016/S0140-6736(98)12055-X
54. Pasquier, E, de Saint Martin, L, Bohec, C, Chauleur, C, Bretelle, F, Marhic, G, et al. Enoxaparin for prevention of unexplained recurrent miscarriage: a multicenter randomized double-blind placebo-controlled trial. Blood. (2015) 125:2200–5. doi: 10.1182/blood-2014-11-610857
55. Perino, A, Vassiliadis, A, Vucetich, A, Colacurci, N, Menato, G, Cignitti, M, et al. Short-term therapy for recurrent abortion using intravenous immunoglobulins: results of a double-blind placebo-controlled Italian study. Hum Reprod. (1997) 12:2388–92. doi: 10.1093/humrep/12.11.2388
56. Quenby, S, and Farquharson, RG. Human chorionic gonadotropin supplementation in recurring pregnancy loss: a controlled trial. Fertil Steril. (1994) 62:708–10. doi: 10.1016/s0015-0282(16)56992-1
57. Scarpellini, F, and Sbracia, M. Use of granulocyte colony-stimulating factor for the treatment of unexplained recurrent miscarriage: a randomised controlled trial. Hum Reprod. (2009) 24:2703–8. doi: 10.1093/humrep/dep240
58. Schleussner, E, Kamin, G, Seliger, G, Rogenhofer, N, Ebner, S, Toth, B, et al. Low-molecular-weight heparin for women with unexplained recurrent pregnancy loss: a multicenter trial with a minimization randomization scheme. Ann Intern Med. (2015) 162:601–9. doi: 10.7326/M14-2062
59. Shaaban, OM, Abbas, AM, Zahran, KM, Fathalla, MM, Anan, MA, and Salman, SA. Low-molecular-weight heparin for the treatment of unexplained recurrent miscarriage with negative antiphospholipid antibodies: a randomized controlled trial. Clin Appl Thromb Hemost. (2017) 23:567–72. doi: 10.1177/1076029616665167
60. Stephenson, MD, Kutteh, WH, Purkiss, S, Librach, C, Schultz, P, Houlihan, E, et al. Intravenous immunoglobulin and idiopathic secondary recurrent miscarriage: a multicentered randomized placebo-controlled trial. Hum Reprod. (2010) 25:2203–9. doi: 10.1093/humrep/deq179
61. Stephenson, MD, Dreher, K, Houlihan, E, and Wu, V. Prevention of unexplained recurrent spontaneous abortion using intravenous immunoglobulin: a prospective, randomized, double-blinded, placebo-controlled trial. Am J Reprod Immunol. (1998) 39:82–8. doi: 10.1111/j.1600-0897.1998.tb00339.x
62. Tang, AW, Alfirevic, Z, Turner, MA, Drury, JA, Small, R, and Quenby, S. A feasibility trial of screening women with idiopathic recurrent miscarriage for high uterine natural killer cell density and randomizing to prednisolone or placebo when pregnant. Hum Reprod. (2013) 28:1743–52. doi: 10.1093/humrep/det117
63. The German RSA/IVIG Group. Intravenous immunoglobulin in the prevention of recurrent miscarriage. The German RSA/IVIG group. Br J Obstet Gynaecol. (1994) 101:1072–7. doi: 10.1111/j.1471-0528.1994.tb13584.x
64. Xu, GL, Hu, XF, Han, YM, and Wei, AW. Clinical efficacy of low molecular heparin on unexplained recurrent spontaneous abortion. Clin Lab. (2018) 64:1037–40. doi: 10.7754/Clin.Lab.2018.180130
65. Yamada, H, Deguchi, M, Saito, S, Takeshita, T, Mitsui, M, Saito, T, et al. Intravenous immunoglobulin treatment in women with four or more recurrent pregnancy losses: a double-blind, randomised, placebo-controlled trial. EClinicalMedicine. (2022) 50:101527. doi: 10.1016/j.eclinm.2022.101527
66. Zafardoust, S, Akhondi, MM, Sadeghi, MR, Mohammadzadeh, A, Karimi, A, Jouhari, S, et al. Efficacy of intrauterine injection of granulocyte colony stimulating factor (G-CSF) on treatment of unexplained recurrent miscarriage: a pilot rct study. J Reprod Infertil. (2017) 18:379–85.
67. Zolghadri, J, Ahmadpour, F, Momtahan, M, Tavana, Z, and Foroughinia, L. Evaluation of the efficacy of aspirin and low molecular weight heparin in patients with unexplained recurrent spontaneous abortions. Iran Red Crescent Med J. (2010) 12:548–52.
68. Lund, M, Kamper-Jorgensen, M, Nielsen, HS, Lidegaard, O, Andersen, AM, and Christiansen, OB. Prognosis for live birth in women with recurrent miscarriage: what is the best measure of success? Obstet Gynecol. (2012) 119:37–43. doi: 10.1097/AOG.0b013e31823c0413
69. Alecsandru, D, Barrio, A, Garrido, N, Aparicio, P, Pellicer, A, Moffett, A, et al. Parental human leukocyte antigen-C allotypes are predictive of live birth rate and risk of poor placentation in assisted reproductive treatment. Fertil Steril. (2020) 114:809–17. doi: 10.1016/j.fertnstert.2020.05.008
70. Alexandrova, M, Manchorova, D, and Dimova, T. Immunity at maternal-fetal interface: KIR/HLA (Allo)recognition. Immunol Rev. (2022) 308:55–76. doi: 10.1111/imr.13087
71. Wong, LF, Porter, TF, and Scott, JR. Immunotherapy for recurrent miscarriage. Cochrane Database Syst Rev. (2014) 2014:CD000112. doi: 10.1002/14651858.CD000112.pub3
72. Dan, S, Wei, W, Yichao, S, Hongbo, C, Shenmin, Y, Jiaxiong, W, et al. Effect of prednisolone administration on patients with unexplained recurrent miscarriage and in routine intracytoplasmic sperm injection: a meta-analysis. Am J Reprod Immunol. (2015) 74:89–97. doi: 10.1111/aji.12373
73. Egerup, P, Lindschou, J, Gluud, C, Christiansen, OB, and Immu Re, MIPDSG. The effects of intravenous immunoglobulins in women with recurrent miscarriages: a systematic review of randomised trials with meta-analyses and trial sequential analyses including individual patient data. PLoS One. (2015) 10:e0141588. doi: 10.1371/journal.pone.0141588
74. Mekinian, A, Cohen, J, Alijotas-Reig, J, Carbillon, L, Nicaise-Roland, P, Kayem, G, et al. Unexplained recurrent miscarriage and recurrent implantation failure: is there a place for immunomodulation? Am J Reprod Immunol. (2016) 76:8–28. doi: 10.1111/aji.12493
75. Saccone, G, Schoen, C, Franasiak, JM, Scott, RT Jr, and Berghella, V. Supplementation with progestogens in the first trimester of pregnancy to prevent miscarriage in women with unexplained recurrent miscarriage: a systematic review and meta-analysis of randomized, controlled trials. Fertil Steril. (2017) 107:e433:430–438.e3. doi: 10.1016/j.fertnstert.2016.10.031
76. Devall, AJ, Papadopoulou, A, Podesek, M, Haas, DM, Price, MJ, Coomarasamy, A, et al. Progestogens for preventing miscarriage: a network meta-analysis. Cochrane Database Syst Rev. (2021) 2021:CD013792. doi: 10.1002/14651858.CD013792.pub2
Keywords: network meta-analysis, therapeutic interventions, idiopathic recurrent pregnancy loss, systematic review, live birth rate, miscarriage rate
Citation: Lima J, Guerreiro J, Ângelo-Dias M, Serra SS, Costa T, Marto N, de Pinho JF, Costa J, Ruano R and Duarte GS (2025) Efficacy of therapeutic interventions for idiopathic recurrent pregnancy loss: a systematic review and network meta-analysis. Front. Med. 12:1569819. doi: 10.3389/fmed.2025.1569819
Edited by:
Panicos Shangaris, King’s College London, United KingdomReviewed by:
Gaetano Riemma, University of Campania Luigi Vanvitelli, ItalyKrishna Mantravadi, Oasis Fertility, India
Copyright © 2025 Lima, Guerreiro, Ângelo-Dias, Serra, Costa, Marto, de Pinho, Costa, Ruano and Duarte. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jorge Lima, am9yZ2VyYW1vc2xpbWFAc2Fwby5wdA==
†These authors have contributed equally to this work and share first authorship