 Celia B. González-Alcorta1
Celia B. González-Alcorta1 Adelina Alcorta-Garza2*Daneli Ruiz-Sánchez1Blanca Angélica Soto-Martínez1Fernando Alcorta-Núñez3Itzel Lidey Galaviz-Reynoso3Paola A. López-Sierra3Juan Francisco González-Guerrero4Oscar Vidal-Gutiérrez5
Adelina Alcorta-Garza2*Daneli Ruiz-Sánchez1Blanca Angélica Soto-Martínez1Fernando Alcorta-Núñez3Itzel Lidey Galaviz-Reynoso3Paola A. López-Sierra3Juan Francisco González-Guerrero4Oscar Vidal-Gutiérrez5- 1Oncology Service, Area of Radiooncology, University Center Against Cancer, University Hospital "José E. González", Universidad Autónoma de Nuevo León, Monterrey, Mexico
- 2Coordination of Psycho-Oncology and Liaison between Medicine and Palliative Care, University Center Against Cancer, University Hospital "José E. González", Universidad Autónoma de Nuevo León, Monterrey, Mexico
- 3Oncology Service, University Center Against Cancer, University Hospital "José E. González", Universidad Autónoma de Nuevo León, Monterrey, Mexico
- 4Oncology Service, Area of Medical Oncology and Radiooncology, University Center Against Cancer, University Hospital "José E. González", Universidad Autónoma de Nuevo León, Monterrey, Mexico
- 5Oncology Service, Area of Oncologic Surgery, University Center Against Cancer, University Hospital "José E. González", Universidad Autónoma de Nuevo León, Monterrey, Mexico
Background: Research on low-dose-rate (LDR) brachytherapy for gynecological cancer primarily examines treatment toxicity while overlooking aspects such as sexual desire, arousal, orgasm, satisfaction, and overall quality of life. We assessed sexual function and quality of life in patients with cervical and endometrial cancer before and after LDR brachytherapy, identifying factors related to sexual dysfunction and good quality of life 3–6 months after brachytherapy.
Materials and methods: We prospectively followed a cohort of patients with a histopathological diagnosis of cervical and endometrial cancer who were treated with LDR intracavitary brachytherapy (n = 139). The SyDSF-AP, FACT-G, PHQ-9, and PHQ-15 scales were collected using a self-administered questionnaire before and 3–6 months after treatment. The analysis included estimating incidence rates and conducting a binary multiple logistic regression.
Results: Sexual dysfunction was observed in 14.4% of individuals, with 30% already affected at baseline. Higher education was associated with a decreased likelihood of developing or maintaining sexual dysfunction (OR, 0.10; 95% CI, 0.01–0.97). Physical wellbeing improved after treatment, with scores increasing from 69.3 to 78.7 (p < 0.001; effect size = 0.34). The presence of moderate-to-severe somatic symptoms, major depression, and sexual dysfunction reduced the likelihood of starting or maintaining a good quality of life.
Conclusion: Over 10% of patients experienced sexual dysfunction, with physical wellbeing being the only area that showed improvement after treatment. Research in this area enhances awareness and understanding of how healthcare providers can better support sexual and health-related wellbeing.
Introduction
There are five main types of gynecological cancer: cervix, uterine (usually endometrial), ovarian, vaginal, and vulvar. The Global Cancer Observatory reported that cervical cancer was the fifth most common malignant disorder in 2022, with an incidence rate of 14.1%. Cervical cancer is the third most common cancer, and uterine cancer is fifth, with rates of 13.2% in Mexico and 22.5% in the United States. Cervical cancer is the leading cause of gynecologic cancer deaths worldwide, especially in low- and middle-income countries. Mexico has the highest mortality rate among gynecological cancers at 6.2% (1). It is standard for cervical cancer patients to receive brachytherapy after external beam radiation therapy. For endometrial cancer patients, it is used post-hysterectomy to target any remaining cancer cells. Additionally, patients with uterine cancer who cannot undergo surgery may also receive brachytherapy (2–4). Brachytherapy may cause early side effects such as pain, swelling, and vaginal bleeding (5, 6). Over time, it may affect the pelvic floor muscles, leading to urinary and anal incontinence (7, 8). Radiotherapy can damage the vaginal structure, resulting in shortened length, reduced lubrication, and decreased elasticity. As a result, patients may experience stenosis, dryness, and dyspareunia (9–11). Survivors of gynecological cancer frequently face psychological challenges, such as reduced libido, body image changes, and anxiety about sexual performance. They may also struggle with maintaining previous sexual roles, feeling emotionally distant from their partner, and concerns about their partner’s sexual interest after treatment (12, 13). All these physical, psychological, and social effects may significantly impact sexual and health-related quality of life.
Brachytherapy can involve a low-dose-rate (LDR) or a high-dose-rate (HDR) of radiation (14). The primary distinctions are the speed and intensity of radiation delivery; HDR provides a rapid and intense dose, whereas LDR offers a slower and more prolonged dose. The choice depends on the type and location of the cancer, the patient’s health, and access to specialized equipment. A pulsed dose rate (PDR) is another type of brachytherapy that delivers continuous pulses over several days, each lasting a few minutes per hour. It combines the physical benefits of HDR treatment with the radiobiological advantages of LDR therapy (15, 16). Its primary disadvantage is the need for a dedicated hospital room with a remote after-loading system. Over time, HDR has replaced LDR (17). However, access to HDR brachytherapy in Latin America and Mexico involves investing in healthcare infrastructure, improving training programs, and addressing healthcare disparities (18). Some studies have explored how HDR brachytherapy affects sexual function and quality of life in gynecological cancer patients (12, 19–21). In contrast, studies on LDR brachytherapy have primarily examined treatment toxicity, such as vaginal mucosal changes, vaginal stenosis, and pain, without addressing sexual desire, arousal, orgasm, satisfaction, or quality of life (22–25). Understanding the impact of LDR brachytherapy on sexual function and quality of life can help guide healthcare policies, funding, and education to address these critical issues for cancer survivors in regions operating LDR units.
This study aimed to evaluate sexual function and quality of life in cervical and endometrial cancer patients before and after LDR brachytherapy. We also identified factors related to sexual dysfunction and good quality of life 3–6 months post-treatment.
Materials and methods
We prospectively followed a cohort of patients with a histopathological diagnosis of cervical and endometrial cancer treated with LDR intracavitary brachytherapy between February 2020 and November 2022. Participants had to be at least 18 years old, without neurological or cognitive disorders, and have a confirmed diagnosis of cervical or endometrial cancer. They were selected consecutively from the oncology outpatient clinic of a tertiary public teaching hospital in Monterrey, Mexico (Figure 1). The loss rate was 35.3%. Responders and non-responders showed no significant differences in terms of age, education, marital status, occupation, origin, disease stage, surgery, external radiotherapy, chemotherapy, or brachytherapy sessions (p > 0.05). The sample size of 97 was determined based on an expected 50% incidence of sexual dysfunction (SyDSF-AP ≥ 2) 3–6 months after brachytherapy, with a 10% margin of error and 95% confidence level.
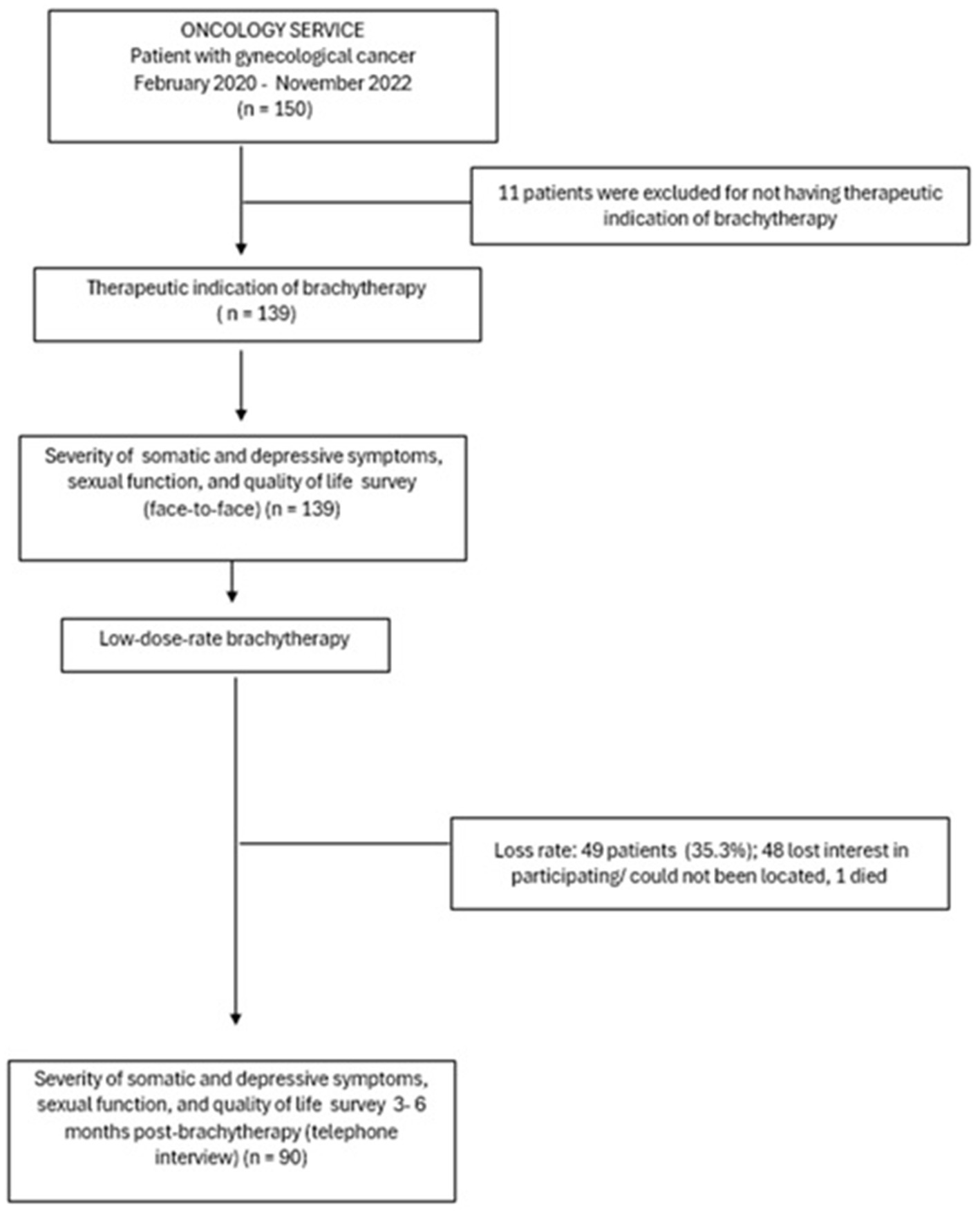
Figure 1. Study design.
Brachytherapy parameters
The brachytherapy procedure adhered to institutional standards, and its delivery was homogeneous over time. Patients were hospitalized for the entire duration of the procedure. After thorough asepsis, a urinary catheter was inserted into the bladder and secured for physiological filling. Brachytherapy consisted of administering 20 to 60 Gy 5 mm below the vaginal surface using LDR cesium-137 sources. The dose rate ranged from 0.4 to 0.6 Gy/h (10–15 Gy/day). X-rays were used to estimate the doses according to the International Commission on Radiation Units and Measurements points, ensuring precise and effective radiation application. A Siemens Somatom computed tomography scanner from Siemens Healthineers was utilized for imaging evaluation during the treatment. Applicators were removed without anesthesia, and the sources were withdrawn after the required time. In patients receiving surgical treatment, chemotherapy, or external radiotherapy, brachytherapy should be administered at least 1 month after surgery or after 50% of the chemotherapy or external radiotherapy sessions have been completed. All patients were evaluated at 1-month post-treatment and between 3 and 6 months after therapy.
Standard protocols for cervical and endometrial cancer
The standard treatment for early-stage cervical cancer typically involves a surgical approach. If adverse characteristics are present, treatment may include chemotherapy (5 cycles of cisplatin) or external beam radiation (25 daily fractions), followed by two LDR treatments of 20 Gy to the mucosa. Advanced cervical cancer cases are treated with chemotherapy (5 cycles of cisplatin) and external beam radiation (25 daily fractions), followed by two LDR of 20 Gy to the mucosa. Three patients with stage IVB cervical cancer received LDR brachytherapy as a palliative measure after undergoing chemotherapy and presenting with active bleeding and pain. The standard treatment for early-stage endometrial cancer includes surgery, with or without LDR brachytherapy, depending on individual risk factors. Advanced cases are treated with surgery, chemotherapy (5 cycles of cisplatin), external beam radiation (25 daily fractions), and LDR (1–3 applications to the vaginal cuff). Unresectable cases are treated with chemotherapy (5 cycles of cisplatin) and external beam radiation (25 daily fractions), with or without LDR treatments or chemotherapy.
Study variables
Sexual function
It was measured using the Health and Feminine Sexual Dysfunction in Primary Care (SyDSF-AP) scale developed and validated in Spanish by Casas Aranda et al. (26). Sexual function was assessed based on the experience of symptoms in the past 3 months. The sexual function domain encompassed nine items regarding sexual satisfaction, sexual desire, sexual enjoyment, sexual arousal, dyspareunia, orgasm, sexual difficulties with a partner, the ability to live without sex, and feelings of depression or nervousness because of sexual problems (Cronbach’s alpha before and after brachytherapy = 0.56 and 0.60, respectively). The SyDSF-AP scale responses were on a 6-point Likert scale ranging from 0 (never) to 5 (always). The positively phrased questions were reversed so that a higher score indicated poor sexual function. The responses were averaged and categorized into the presence or absence of sexual dysfunction based on a cutoff point of ≥ 2 (equivalent to sometimes, often, almost always, and always). The classification of changes in status between the baseline measurement (before brachytherapy) and the second measurement taken 3–6 months after brachytherapy is shown in Supplementary file 1.
Quality of life
It was measured using the Functional Assessment of Cancer Therapy - General Scale (FACT-G) developed in 1993 for evaluating patients receiving cancer treatment (27) and validated in Spanish (28). It assessed the quality of life over the last 7 days and consisted of four dimensions: (a) physical wellbeing (e.g., “I lack energy”), with seven items (Cronbach’s alpha before and after brachytherapy = 0.86 and 0.82, respectively), (b) family and social wellbeing (e.g., “I receive emotional support from part of my family”), with seven items (Cronbach’s alpha before and after brachytherapy = 0.77 and 0.72, respectively), (c) emotional wellbeing (e.g., “I feel sad”), with six items (Cronbach’s alpha before and after brachytherapy = 0.74 and 0.71, respectively), and (d) functional wellbeing (e.g., “I sleep well”), with seven items (Cronbach’s alpha before and after brachytherapy = 0.81 and 0.78, respectively). FACT-G scale responses were provided on a 5-point Likert scale ranging from 0 (not at all) to 4 (very much). Negatively phrased questions were reversed so that a higher score indicated a better quality of life. The score was then transformed to a 0–100 scale, and the responses were averaged and categorized as follows: poor (0–25, equivalent to not at all and a little bit), fair (26–74, equivalent to somewhat), and good quality of life (75–100, equivalent to quite a bit and very much). The classification of the change in status between the baseline measurement (before brachytherapy) and the second measurement taken 3–6 months after brachytherapy is shown in Supplementary file 1.
Somatic and depressive symptom severity
This was assessed using two patient health questionnaires: the PHQ-15 (29) and the PHQ-9 (30). The PHQ-15 assessed physical problems that may have bothered the patient over the past 4 weeks, whereas the PHQ-9 evaluated depressive symptoms experienced in the previous 2 weeks. Both were available in Spanish (31, 32). The PHQ-15 consisted of 15 items, for example, “I have had stomach pain” (Cronbach’s alpha before and after brachytherapy = 0.85 and 0.83, respectively), with responses on a 3-point Likert scale ranging from 0 (not bothered at all) to 2 (bothered a lot). A higher score indicated a greater severity of somatic symptoms. The sum of the responses was categorized into minimal-mild (0–9) and moderate–severe (≥10). The PHQ-9 consisted of nine items, such as “I feel little interest or pleasure in doing things” (Cronbach’s alpha before and after brachytherapy = 0.82 and 0.73, respectively), with responses on a 4-point Likert scale ranging from 0 (never) to 3 (almost every day). A higher score indicated greater severity of depressive symptoms. The sum of the responses was categorized, with a score of ≥ 9 indicating major depression. This cutoff point was chosen because it demonstrated a sensitivity of 95% (29). The classification of the change in status between the baseline measurement (before brachytherapy) and the second measurement taken 3–6 months after brachytherapy is shown in Supplementary file 1.
Sociodemographic
Age, schooling, marital status, occupation, origin, and parity.
Procedures
Sexual function, quality of life, somatic and depressive symptom severity, and sociodemographic information were collected through a self-administered questionnaire before LDR-brachytherapy (basal measurement). At 3–6 months after brachytherapy, data were collected via telephone (second measurement). Medical files provided information on the patient’s history of diabetes, hypertension, and other health conditions. Brachytherapy characteristics (technique and number of sessions) and other treatments used, including surgery, external beam radiation, and chemotherapy, were recorded and analyzed. Additionally, data were collected regarding side effects and complications (gastrointestinal, genitourinary, fistula, colostomy, and nephrostomy), as well as the response to oncologic treatment (recurrence, progression, or persistence of cancer). The classification of disease stage followed the International Federation of Gynecology and Obstetrics.
Statistical analysis
Descriptive statistics, including means and standard deviations, were used for continuous variables, while frequency distributions were applied for categorical variables. The incidence of sexual dysfunction, good quality of life, moderate–severe somatic symptoms, and major depression was estimated based on the change from absence to presence (Supplementary file 1). The Wilcoxon signed-rank test for two related samples was used to compare the mean scores of the quality-of-life domains and the mean number of bothersome somatic and depressive symptoms. The effect size was estimated when the difference in the quality-of-life domain’s pre- and post-measurements was significant. Binary multiple logistic regression was used to examine risk factors for sexual dysfunction (dependent variable coded yes vs. no) and good quality of life (dependent variable coded yes vs. no) after LDR brachytherapy. In both models, age, education level, major depression, moderate–severe somatic symptoms, comorbidities, and side effects/complications were treated as independent variables. Disease stage and other treatments were used to serve as control variables. Odds ratios (OR) and 95% confidence intervals (CI) were estimated.
Results
The mean age of the study population was 46.2 ± 12.7 years, and the mean number of pregnancies was 3.4 ± 1.7. The majority of participants were married or living with a partner, had a low level of education, were homemakers, and were primarily from the Northeastern states of Mexico, specifically Nuevo León and Tamaulipas. One in five patients had diabetes or hypertension, and more than 40% of the participants experienced gastrointestinal side effects (Table 1).
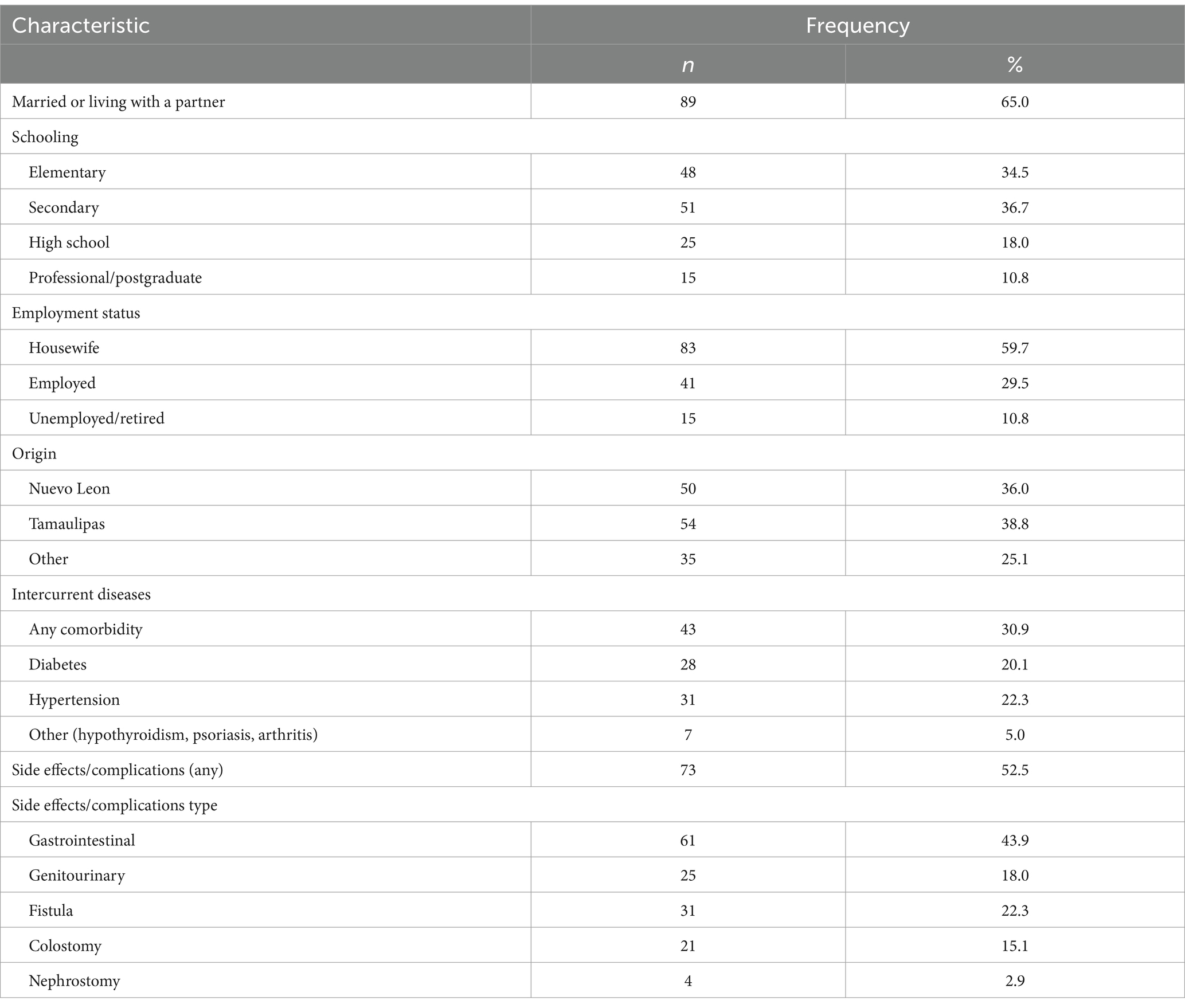
Table 1. Sociodemographic profile and intercurrent diseases (n = 139).
The disease stages were as follows: 20.4% stage IA or IB, 21.9% stage IIA or IIB, 10.9% stage IIIA or IIIB, 23.4% stage IIIC, and 23.4% stage IVA or IVB. The number of brachytherapy sessions was 2 for 82.7%, 1 for 15.1%, and 3 for 2.2%. The Fletcher technique predominated (61.8%), followed by colpostatos (33.1%) and mini-pelvis (5.1%). The frequency of other treatments received was surgery (36%), chemotherapy (71.9%), and external beam radiation (95.0%). The rates of cancer recurrence, progression, and persistence were 2.9, 5.8, and 10.8%, respectively. The mean number of bothersome somatic symptoms at 3–6 months was lower than before brachytherapy (8.3 ± 5.4 vs. 6.4 ± 4.2, p < 0.001). The mean number of depressive symptoms also decreased (7.2 ± 6.0 vs. 5.3 ± 5.1, p < 0.01). The incidence of moderate–severe somatic symptoms and major depression was 6.7%.
Sexual function
All patients who answered the questions regarding sexual function were sexually active. Sexual arousal and the ability to live without sex were the most frequently affected functions. There was no difference in the frequency of patients with dysfunctions before and after brachytherapy (p > 0.05) (Table 2). The incidence of sexual dysfunction (new cases after LDR brachytherapy) was 14.4%. Figure 2 (Sankey diagram) illustrates how participants’ sexual dysfunction status transitioned from the baseline measurement (before brachytherapy) to the second measurement at 3–6 months (after brachytherapy). Higher education was associated with a reduced risk of starting or maintaining sexual dysfunction following brachytherapy, independent of confounding factors (Table 3).
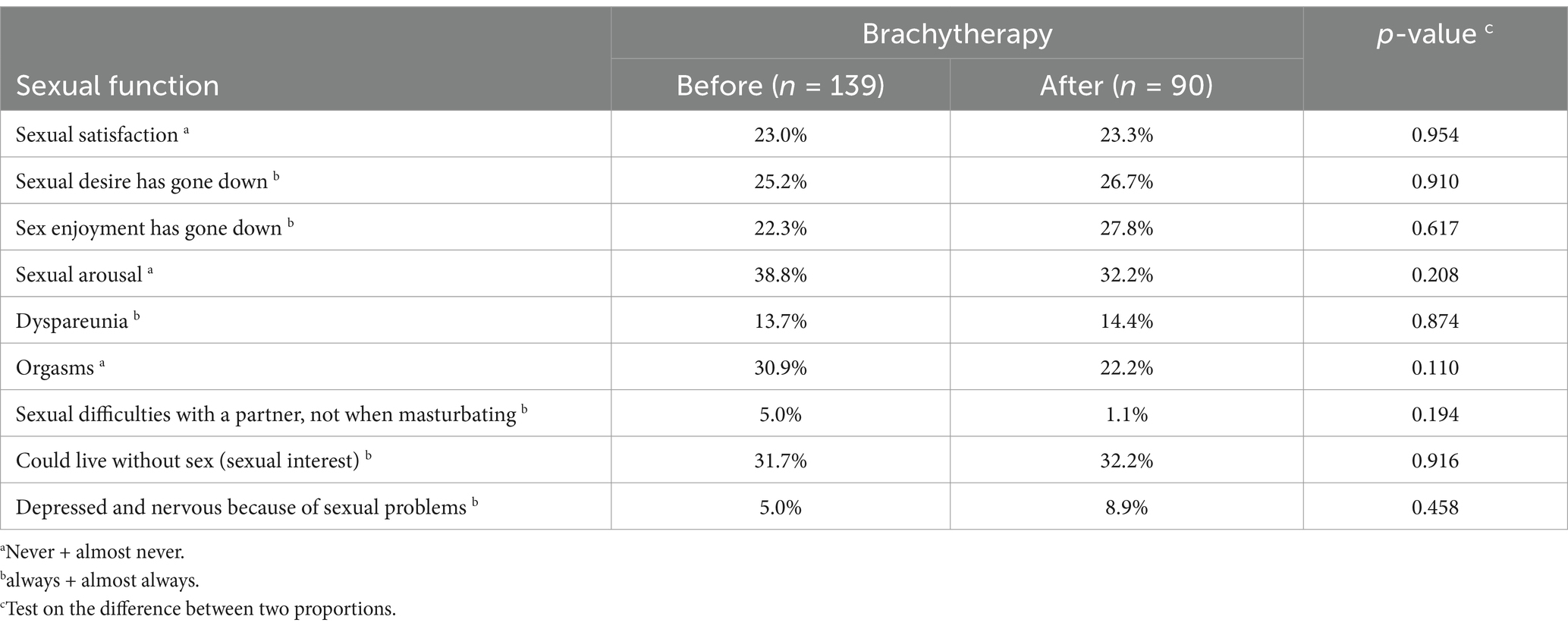
Table 2. Sexual function before and 3–6 months after LDR brachytherapy.
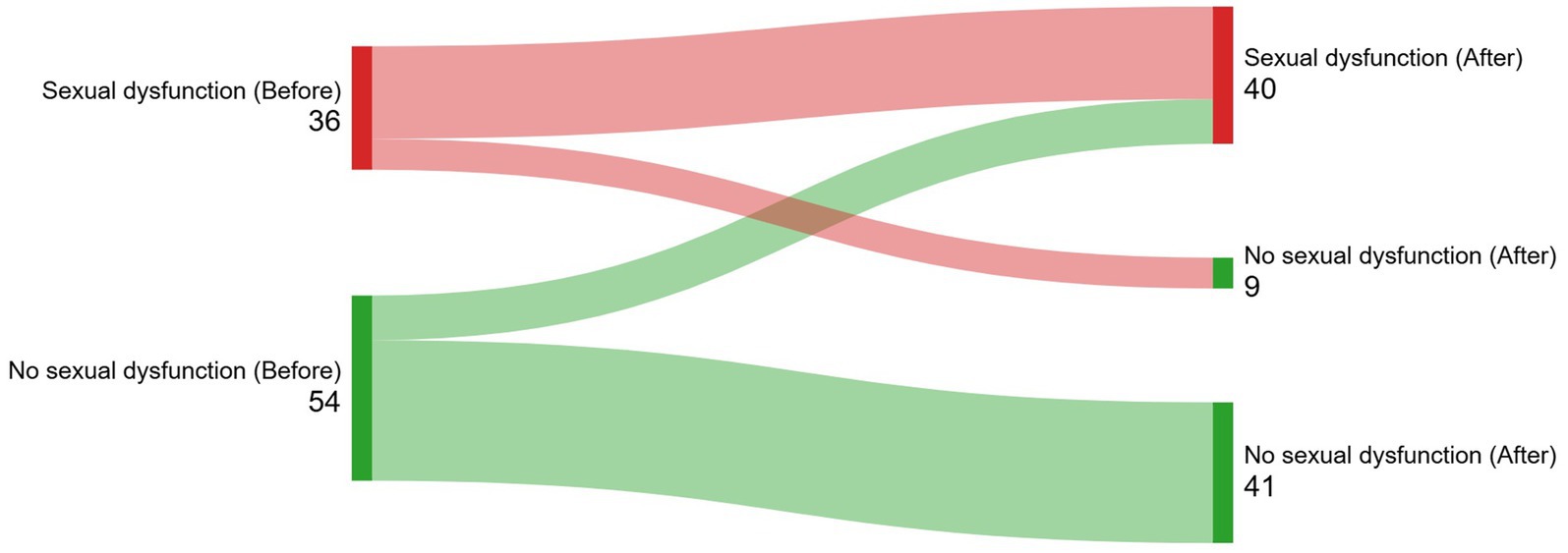
Figure 2. (Sankey diagram). Illustration of how participants’ sexual dysfunction status transitioned from the baseline measurement (before brachytherapy) to the second measurement at 3–6 months (after brachytherapy).
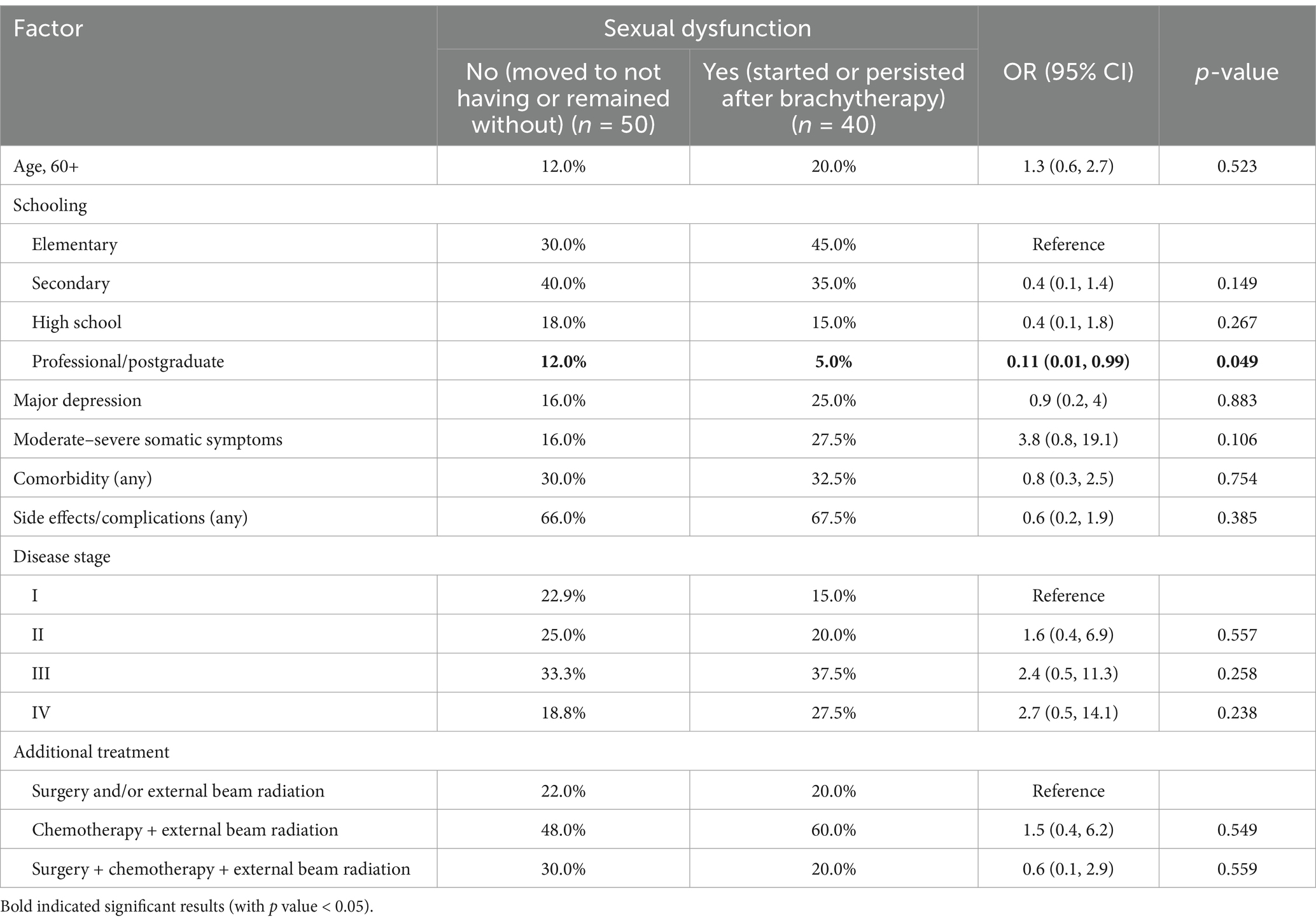
Table 3. Risk factors for sexual dysfunction 3–6 months after LDR brachytherapy.
Quality of life
Physical wellbeing improved 3–6 months after brachytherapy (69.3 ± 24.1 vs. 78.7 ± 20.2, p < 0.001; effect size = 0.34). Emotional health was the most affected area, showing no improvement in wellbeing, remaining either poor or fair (Table 4). The incidence of good quality of life was 28.2% (new cases after LDR brachytherapy). Figures 3–5 (Sankey diagrams) illustrate the transition in participants’ overall and domain-specific quality of life statuses from the baseline measurement (before brachytherapy) to the second measurement taken 3–6 months after brachytherapy. Sexual dysfunction, major depression, and moderate–severe somatic symptoms reduced the likelihood of starting or maintaining a good quality of life after brachytherapy, independent of confounding factors (Table 5). Multivariate analysis showed only chemotherapy as a factor associated with a specific domain of quality of life: physical well-being (OR, 0.24; 95% CI, 0.06-0.94).
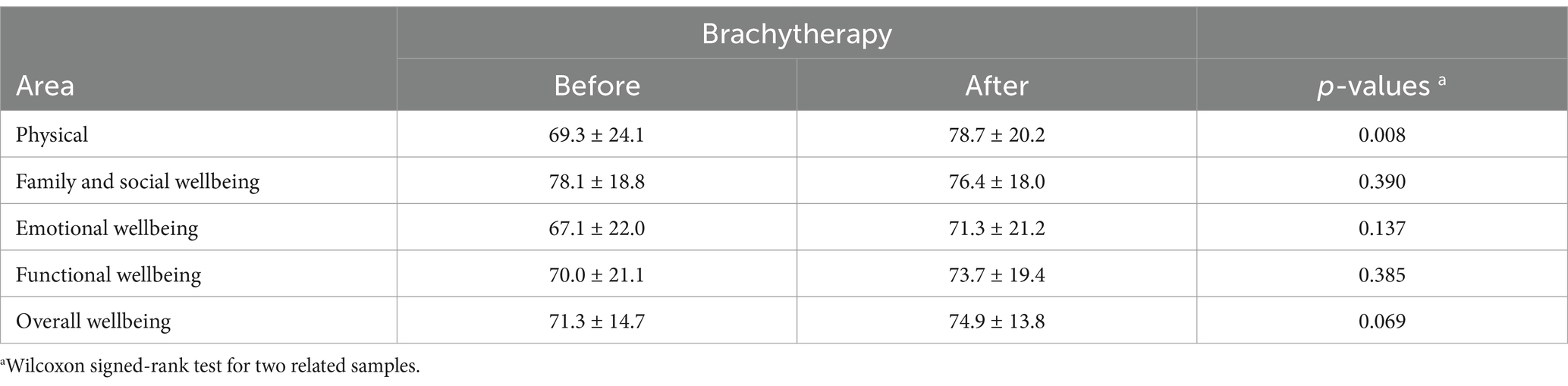
Table 4. Quality of life before and 3–6 months after LDR brachytherapy (n = 90).
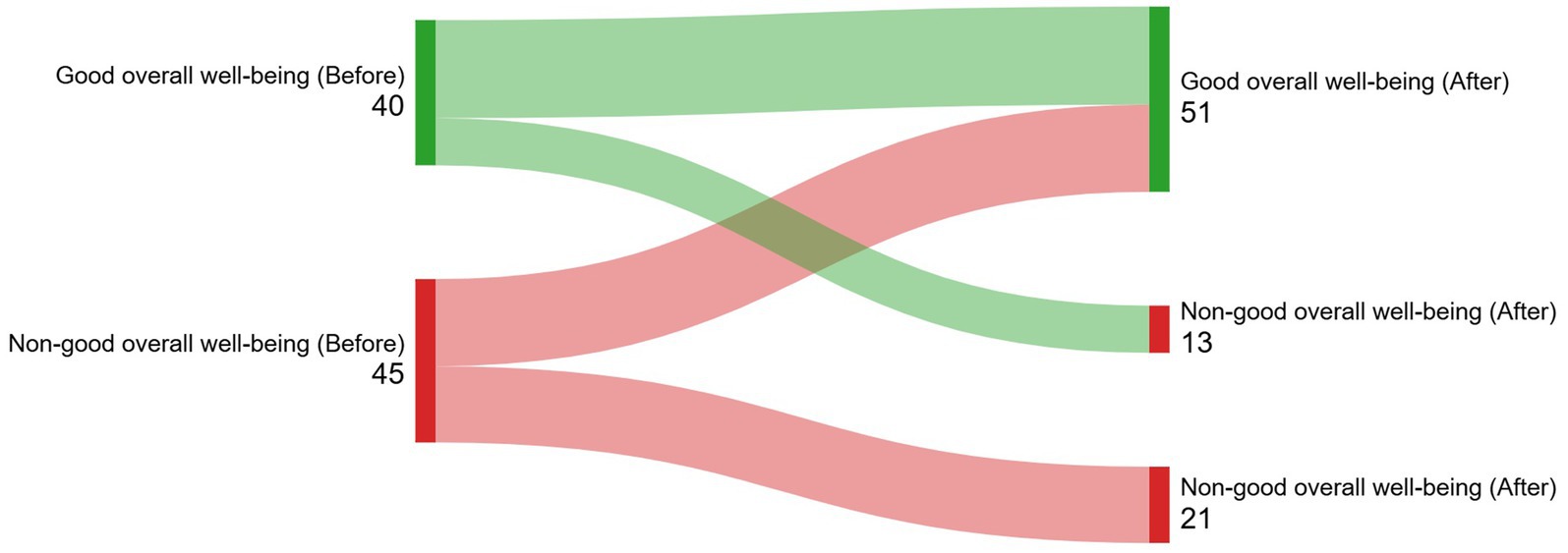
Figure 3. (Sankey diagram). Illustration of how participants’ overall wellbeing status transitioned from the baseline measurement (before brachytherapy) to the second measurement taken 3-6 months after brachytherapy.
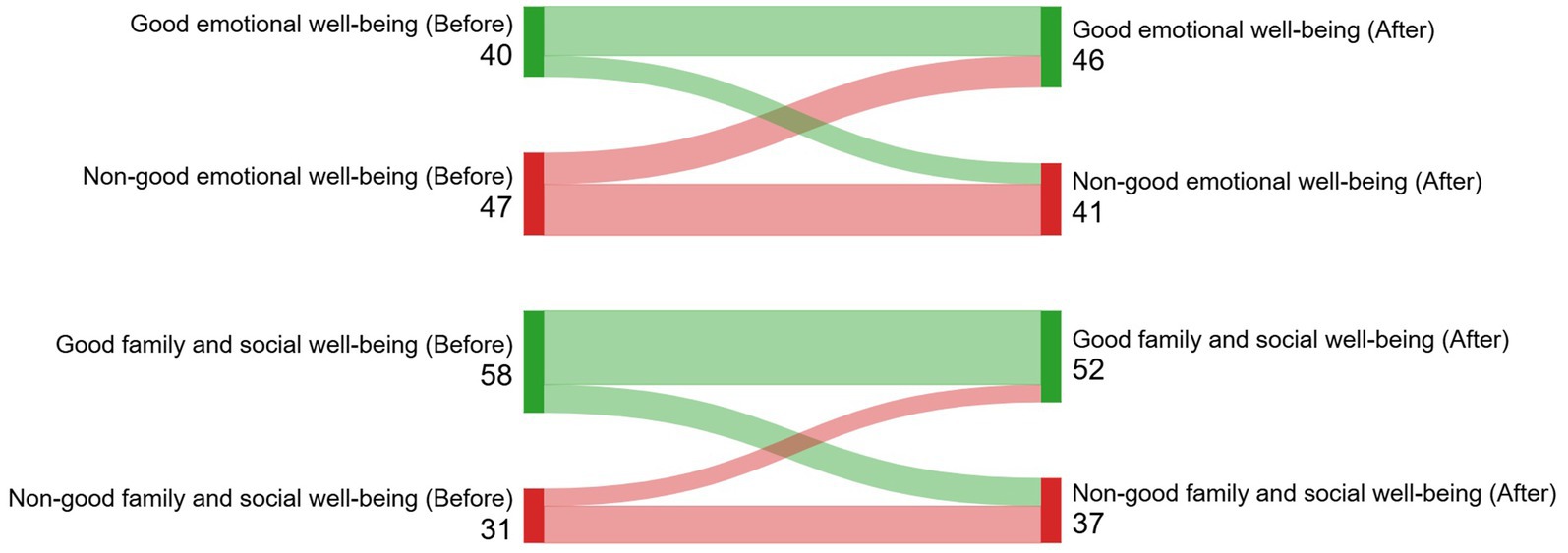
Figure 4. (Sankey diagram). Illustration of how participants’ emotional, family, and social wellbeing status transitioned from the baseline measurement (before brachytherapy) to the second measurement taken 3-6 months after brachytherapy.
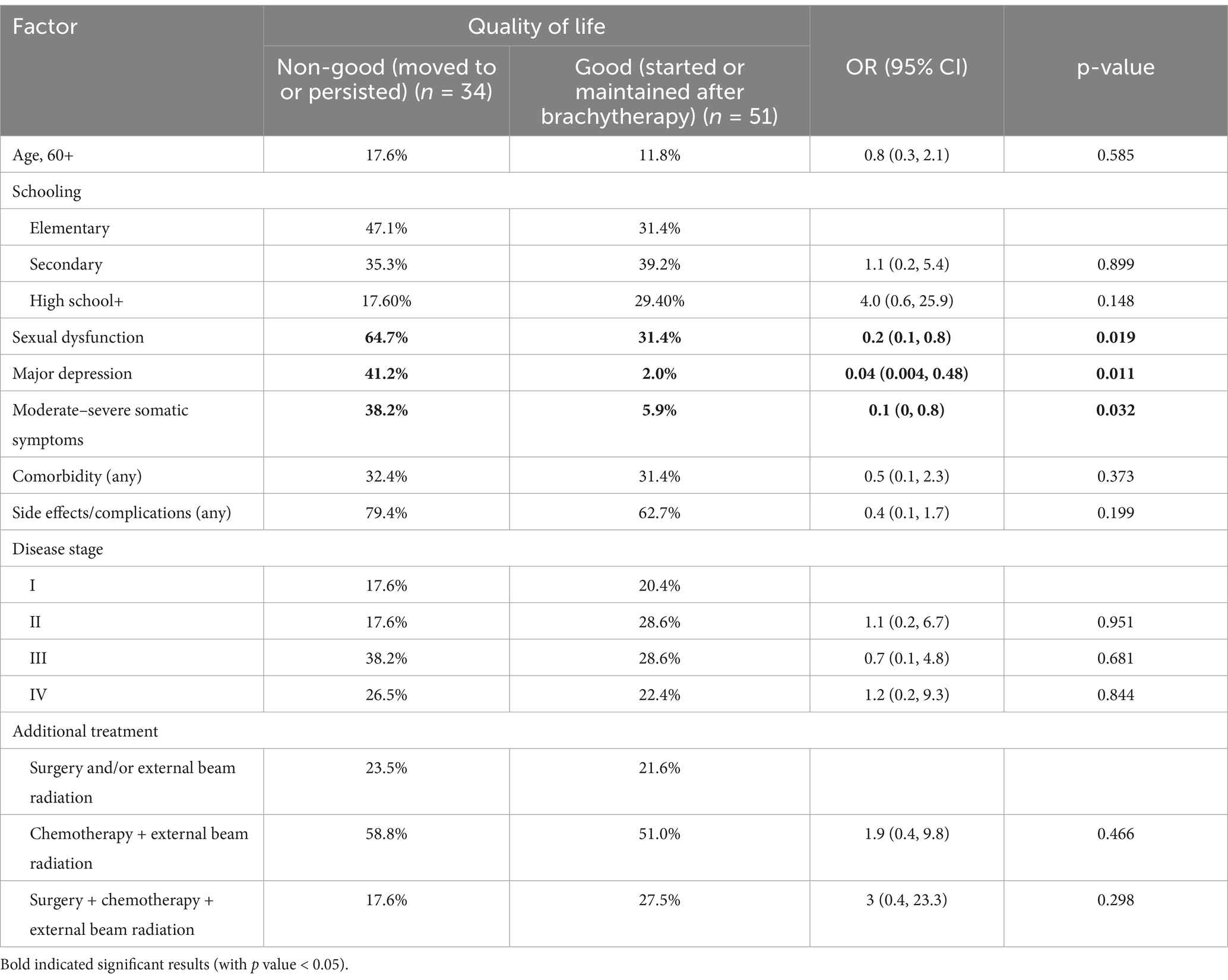
Table 5. Risk factors for good quality of life 3–6 months after LDR brachytherapy.
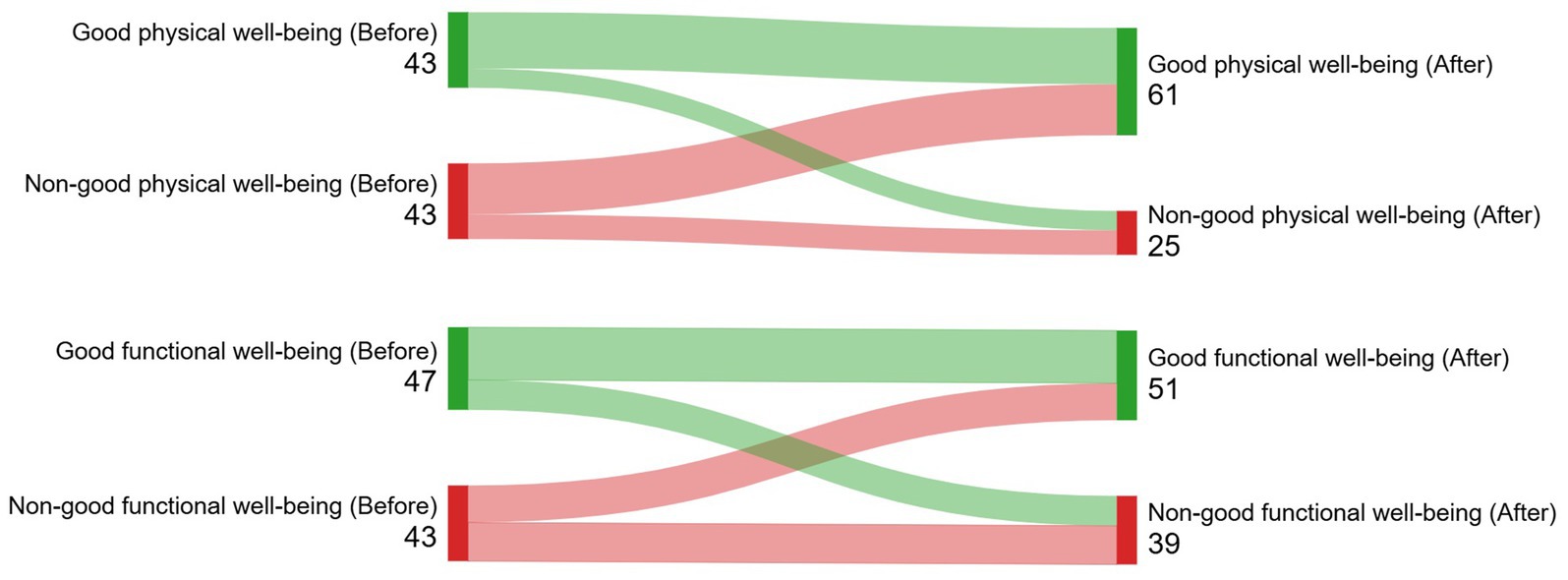
Figure 5. (Sankey diagram). Illustration of how participants’ physical and functional wellbeing status transitioned from the baseline measurement (before brachytherapy) to the second measurement taken 3-6 months after brachytherapy.
Discussion
We estimated sexual dysfunction and quality of life before and after LDR brachytherapy in patients with cervical and endometrial cancer in a region where HDR brachytherapy units are not widely available. Sexual dysfunction was present in 44.4% of the study population (14.4% were new cases and 30% were prevalent cases). Roberts et al. (33) reported that 62.5% of endometrial and cervical cancer patients experienced at least one sexual difficulty after completing brachytherapy, chemotherapy, or external radiotherapy for more than 8 months. In the general population, female sexual problems affect up to 43% of women (34). Three areas of sexual dysfunction frequently overlap: interest/arousal, orgasmic, and genital-pelvic pain or penetration (35). We found that sexual interest and sexual arousal were the most frequent dysfunctions both before and after brachytherapy. Zomkowski et al. (19) reported a negative effect on lubrication (p = 0.05) and desire (p = 0.06) 7 days after completing HDR treatment. Kirchheiner et al. (20) documented less sexual activity than did a healthy population at baseline and 3 months after a combination of HDR, external beam radiotherapy, and chemotherapy. Studies have shown that patients with cervical and endometrial cancer experience more dysfunctions in terms of sexual arousal and orgasm intensity than healthy individuals do, along with entry dyspareunia (36, 37). Sexual dysfunction is a common issue among patients with cervical and endometrial cancer due to a combination of physical (fatigue and chronic pain), psychological (body image issues and fear of recurrence), and cultural factors (rights to enjoy a full sexual life, willingness to discuss sexual health concerns, and seek help). We have not yet studied how cervical and endometrial cancer relates to changes in body image and sexual dysfunction. Future studies should investigate this area further, as gynecological cancer treatments may lead to significant changes in body perception. Women may avoid or have less frequent sex because they fear that it could cause a recurrence of cancer or because they or their partners are concerned that cancer could be transmitted through sexual activity (38). We found that women with higher education levels had a lower risk of sexual dysfunction after brachytherapy, which is consistent with the findings of previous studies (39, 40). Women with higher levels of education often express more significant concern about their sexuality than women with lower levels of education do (41). Higher-educated women may feel more culturally empowered to discuss sexual issues openly. Access to care also contributes to the problem of sexual dysfunction due to the absence or insufficient availability of sexual health counseling or therapy services. Furthermore, women with cervical and endometrial cancer may not seek healthcare regarding their sexual function because they feel uncomfortable discussing their sex life with healthcare providers. Healthcare providers, for their part, may also feel uncomfortable talking about sexual health due to a lack of training, fear of offending or embarrassing the patient, underestimation of the incidence/prevalence of sexual dysfunction, and a lack of knowledge about the impact of sexual dysfunction on the wellbeing of patients with cervical and endometrial cancer. Patients with gynecologic cancer should receive counseling on how to cope with anticipated changes in sexual functioning. Addressing sexual dysfunction in patients with cervical and endometrial cancer requires a multidisciplinary approach, including medical treatment, psychological support, and counseling (34, 42).
Physical wellbeing significantly improved after LDR brachytherapy, with a difference of +9.4 compared to baseline. The physical domain is related to treatment side effects, which may negatively influence the quality of life. We found that the mean number of bothersome somatic symptoms at 3–6 months was lower than before, which may explain the improvement in physical wellbeing. Zomkowski et al. (19) reported no improvement in overall wellbeing 7 days after HDR brachytherapy but noted improvements in specific symptoms, including appetite, diarrhea, and constipation. Emotional health was the most affected area and remained unchanged, similar to previous reports (19, 20). Family and social wellbeing ranked high both before and after brachytherapy. This contrasts with the findings of Zomkowski et al. (19), who found that social wellbeing was the second most affected area, with no significant change between measurements. Kirchheiner et al. (20) reported that social functioning was low at baseline but improved, reaching a level comparable to that of the reference population within the first 6 months. These results underscore the importance of examining short-term quality-of-life effects across different populations to inform the planning of targeted interventions. The incidence of moderate–severe somatic symptoms and major depression was low (6.7%). Both reduced the likelihood of an overall good quality of life in addition to sexual dysfunction. Depression can exacerbate physical symptoms such as pain, fatigue, and sleep disturbances, severely impacting daily functioning and quality of life. It can overshadow positive experiences and reduce overall life satisfaction. Effective management of depression through therapy, medication, or a combination of both can significantly improve quality of life. It is crucial to conduct psychological assessments and gather a comprehensive medical history to identify women who may be at higher risk of developing depressive disorders during or after treatment. Strengthening social support networks and encouraging social engagement can also help mitigate the negative impact of depression. Sexual health in cancer patients is a crucial marker of quality of life, and information should be provided to patients about the sexual consequences of surgery. It is essential to identify which patients may suffer from sexual health issues to help improve their quality of life. Therefore, sexual function should be assessed regularly (34). Supportive care interventions assist patients in addressing sexual dysfunction issues and enhancing their wellbeing.
Any side effect may potentially impact sexual function and quality of life in women with gynecological cancer. We found that one out of two patients experienced a side effect, and gastrointestinal and genitourinary complications were frequent, occurring in 44 and 18% of patients, respectively. Chronic abdominal pain and cramping can make sexual activity uncomfortable or painful. Bloating, excessive gas, and bowel urgency may also cause physical discomfort during intimacy, especially when accompanied by urinary and anal incontinence complications. However, we did not observe a significant impact of these or other side effects on the patient’s sexual function and quality of life. Intensity, frequency, and side-effect management may have affected the results. Unfortunately, we did not have detailed information on the severity of the side effects. It would be interesting to continue this line of research to clarify the reasons for this lack of association. While the study focuses on the impact of LDR brachytherapy, we recognize that sexual function and quality of life may also be influenced by additional treatments, including surgery, chemotherapy, and external beam radiotherapy. Therefore, they were considered as control variables in the multivariate analysis, and the results for sexual function and quality of life were adjusted accordingly. We noticed no significant impact of additional treatments on the patient’s sexual function and overall quality of life as assessed by standardized questionnaires in this study. Chemotherapy was the only treatment associated with a reduction in physical wellbeing. Supportive care interventions can help patients manage chemotherapy side effects, thereby improving their overall wellbeing.
Study limitations
Cultural factors such as shyness and embarrassment could have influenced sexual function responses, leading to the underestimation of sexual dysfunction rates. Feelings of shame can act as a bias in surveys of sexuality by influencing how participants perceive, recall, and report their sexual experiences, leading to misreporting. On the other hand, there is also the possibility that the sample was biased toward women who were more comfortable discussing sex, which affects the generalizability of the results. Additionally, we did not include a healthy comparison group, and it would be interesting to consider one in future studies. Several patients expressed interest in learning more about their treatment and its potential impact on sexual function. These patients received counseling from a health professional trained to guide and educate them on preventing or improving their sexual function. Expanding this area into a line of research to compare the impact of such health promotion would be valuable. The therapeutic regimens were heterogeneous; however, we were unable to analyze population subgroups, such as brachytherapy combined with radiotherapy vs. brachytherapy combined with surgery, due to the small sample sizes. The majority of patients lacked health insurance and belonged to an economically vulnerable social class; therefore, the results cannot be generalized to patients in middle- and high-socioeconomic statuses with private healthcare. Additionally, there is a recognized bias toward urban residents, as the majority of participants live in the metropolitan area of Monterrey, Mexico. Future studies should include residents of rural areas to evaluate whether the results differ based on area of residence.
Conclusion
This study focused on a Mexican population from the northeast of the country. It was the first to assess sexual function and quality of life before and 3–6 months after LDR brachytherapy in a cohort of patients with cervical and endometrial cancer. More than 1 in 10 patients developed sexual dysfunction, and 3 in 10 experienced it before treatment. Physical wellbeing was the only quality of life that significantly improved after treatment. Higher education decreases the risk of starting or maintaining sexual dysfunction. Conversely, moderate–severe somatic symptoms, major depression, and sexual dysfunction adversely affect the ability to achieve or maintain a good quality of life after brachytherapy. Research in this area helps increase awareness and understanding of how healthcare providers can better support sexual and health-related wellbeing.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics, Biosafety, and Research Committees of the Dr. José Eleuterio González Hospital of the Autonomous University of Nuevo León, Mexico (CI22-00242). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CG-A: Conceptualization, Methodology, Writing – original draft. AA-G: Conceptualization, Methodology, Formal analysis, Writing – review & editing. DR-S: Investigation, Supervision, Writing – review & editing. BS-M: Investigation, Supervision, Writing – review & editing. FA-N: Data curation, Software, Writing – review & editing. IG-R: Investigation, Supervision, Writing – review & editing. PL-S: Investigation, Supervision, Writing – review & editing. JG-G: Investigation, Writing – review & editing. OV-G: Project administration, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted without any commercial or financial relationships that could potentially create a conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1584141/full#supplementary-material
References
1. International Agency for Research on Cancer. (2024) Cancer Today. Population factsheets. Available online at:. (https://gco.iarc.who.int/today/en/fact-sheets-populations#countries)
2. Chargari, C, Deutsch, E, Blanchard, P, Gouy, S, Martelli, H, Guérin, F, et al. Brachytherapy: an overview for clinicians. CA Cancer J Clin. (2019) 69:386–401. doi: 10.3322/caac.21578
3. Holschneider, CH, Petereit, DG, Chu, C, Hsu, I-C, Ioffe, YJ, Klopp, AH, et al. Brachytherapy: a critical component of primary radiation therapy for cervical cancer. Brachytherapy. (2019) 18:123–32. doi: 10.1016/j.brachy.2018.11.009
4. The University of Texas MD Anderson Cancer Center. (2024) Brachytherapy. Available online at:. (https://www.mdanderson.org/treatment-options/brachytherapy.html)
5. Chen, J, Zhang, N, Liu, Y, Han, D, Mao, Z, Yang, W, et al. Analysis of applicator insertion related acute side effects for cervical Cancer treated with brachytherapy. Front Oncol. (2021) 11:7052. doi: 10.3389/fonc.2021.677052
6. Hannoun-Levi, J-M, Chand-Fouche, M-E, Gautier, M, Dejean, C, Marcy, M, and Fouche, Y. Interstitial preoperative high-dose-rate brachytherapy for early stage cervical cancer: dose–volume histogram parameters, pathologic response and early clinical outcome. Brachytherapy. (2013) 12:148–55. doi: 10.1016/j.brachy.2012.04.007
7. Greear, G, Lefkowits, C, Parrillo, LM, and Flynn, BJ. Incontinence, voiding dysfunction, and other urologic complications after radiotherapy for gynecologic malignancies. Curr Bladder Dysfunct Rep. (2016) 11:88–97. doi: 10.1007/s11884-016-0354-7
8. Hazewinkel, MH, Sprangers, MAG, van der Velden, J, van der Vaart, CH, Stalpers, LJA, Burger, MPM, et al. Long-term cervical cancer survivors suffer from pelvic floor symptoms: a cross-sectional matched cohort study. Gynecol Oncol. (2010) 117:281–6. doi: 10.1016/j.ygyno.2010.01.034
9. Barcellini, A, Dominoni, M, Dal Mas, F, Biancuzzi, H, Venturini, SC, Gardella, B, et al. Sexual health dysfunction after radiotherapy for gynecological Cancer: role of physical rehabilitation including pelvic floor muscle training. Front Med. (2022) 8:813352. doi: 10.3389/fmed.2021.813352
10. Delishaj, D, Barcellini, A, D’Amico, R, Ursino, S, Pasqualetti, F, Fumagalli, IC, et al. Vaginal toxicity after high-dose-rate endovaginal brachytherapy: 20 years of results. J Contemp Brachytherapy. (2018) 10:559–66. doi: 10.5114/jcb.2018.79713
11. Stinesen Kollberg, K, Waldenström, A-C, Bergmark, K, Dunberger, G, Rossander, A, Wilderäng, U, et al. Reduced vaginal elasticity, reduced lubrication, and deep and superficial dyspareunia in irradiated gynecological cancer survivors. Acta Oncol. (2015) 54:772–9. doi: 10.3109/0284186X.2014.1001036
12. de Freitas, CE, dos Anjos, GG, Caroline Andrade Oliveira, A, da Silva, PV, Christina Moura Barbosa Castro RCesar De Almeida, P, et al. Effects of brachytherapy on quality of life and functionality in the treatment of cervix cancer. Cogitare Enferm. (2022) 27:1–11. doi: 10.5380/ce.v27i0.86926
13. Abbott-Anderson, K, and Kwekkeboom, KL. A systematic review of sexual concerns reported by gynecological cancer survivors. Gynecol Oncol. (2012) 124:477–89. doi: 10.1016/j.ygyno.2011.11.030
14. American Cancer Society. (2024) Getting internal radiation therapy (Brachytherapy). Avaiable online at:. (https://www.cancer.org/cancer/managing-cancer/treatment-types/radiation/internal-radiation-therapy-brachytherapy.html)
15. Polo, A. Pulsed dose rate brachytherapy. Clin Transl Oncol. (2008) 10:324–33. doi: 10.1007/s12094-008-0208-7
16. Annede, P, Dumas, I, Schernberg, A, Tailleur, A, Fumagalli, I, Bockel, S, et al. Radiobiological optimization comparison between pulse-dose-rate and high-dose-rate brachytherapy in patients with locally advanced cervical cancer. Brachytherapy. (2019) 18:370–7. doi: 10.1016/j.brachy.2018.12.009
17. Abdel-Wahab, M, Grover, S, Zubizarreta, EH, and Polo Rubio, JA. Addressing the burden of cervical cancer through IAEA global brachytherapy initiatives. Brachytherapy. (2020) 19:850–6. doi: 10.1016/j.brachy.2020.07.015
18. Maldonado Magos, F, Lozano Ruíz, FJ, Pérez Álvarez, SI, Garay Villar, O, Cárdenas Pérez, C, Bautista Hernández, MY, et al. Radiation oncology in Mexico: current status according to Mexico’s radiation oncology certification board. Rep Pract Oncol Radiother. (2020) 25:840–5. doi: 10.1016/j.rpor.2020.06.002
19. Zomkowski, K, Toryi, AM, Sacomori, C, Dias, M, and Sperandio, FF. Sexual function and quality of life in gynecological cancer pre- and post-short-term brachytherapy: a prospective study. Arch Gynecol Obstet. (2016) 294:833–40. doi: 10.1007/s00404-016-4099-5
20. Kirchheiner, K, Pötter, R, Tanderup, K, Lindegaard, JC, Haie-Meder, C, Petrič, P, et al. Health-related quality of life in locally advanced cervical Cancer patients after definitive Chemoradiation therapy including image guided adaptive brachytherapy: an analysis from the EMBRACE study. Int J Radiat Oncol. (2016) 94:1088–98. doi: 10.1016/j.ijrobp.2015.12.363
21. Facondo, G, Vullo, G, De Sanctis, V, Vitiello, C, Nieddu, L, Alfò, M, et al. Quality of life and sexual functioning among endometrial cancer patients treated with one week adjuvant high-dose-rate vaginal brachytherapy schedule. J Contemp Brachytherapy. (2022) 14:341–6. doi: 10.5114/jcb.2022.119198
22. Haie-Meder, C, Kramar, A, Lambin, P, Lancar, R, Scalliet, P, Bouzy, J, et al. Analysis of complications in a prospective randomized trial comparing two brachytherapy low dose rates in cervical carcinoma. Int J Radiat Oncol. (1994) 29:953–60. doi: 10.1016/0360-3016(94)90388-3
23. Autorino, R, Tagliaferri, L, Campitelli, M, Smaniotto, D, Nardangeli, A, Mattiucci, GC, et al. EROS study: evaluation between high-dose-rate and low-dose-rate vaginal interventional radiotherapy (brachytherapy) in terms of overall survival and rate of stenosis. J Contemp Brachytherapy. (2018) 10:315–20. doi: 10.5114/jcb.2018.77953
24. Zuliani, AC, Cairo, AA, Barros Esteves, SC, Santos Watanabe, CC, de Oliveira, CM, and de Souza, GA. Adjuvant radiotherapy in early stage endometrial cancer. Rev Assoc Med Bras. (2011) 57:438–42. doi: 10.1590/S0104-42302011000400019
25. Blanchard, P, Monnier, L, Dumas, I, Morice, P, Pautier, P, Duvillard, P, et al. Low-dose-rate definitive brachytherapy for high-grade vaginal intraepithelial neoplasia. Oncologist. (2011) 16:182–8. doi: 10.1634/theoncologist.2010-0326
26. Casas Aranda, I, Guirao Sánchez, L, García-Giralda Ruiz, L, Alfaro González, JV, Sandoval Martínez, C, and García-Giralda Ruiz, FJ. SyDSF-AP: un cuestionario de 21 ítems para aproximarnos a la salud sexual y detectar las disfunciones sexuales femeninas en Atención Primaria. Med Fam Semergen. (2007) 33:9–13. doi: 10.1016/S1138-3593(07)73836-4
27. Cella, DF, Tulsky, DS, Gray, G, Sarafian, B, Linn, E, Bonomi, A, et al. The functional assessment of Cancer therapy scale: development and validation of the general measure. J Clin Oncol. (1993) 11:570–9. doi: 10.1200/JCO.1993.11.3.570
28. Dapueto, JJ, Francolino, C, Gotta, I, Levin, R, Alonso, I, Barrios, E, et al. Evaluation of the functional assessment of Cancer therapy-general questionnaire (FACT-G) in a south American Spanish speaking population. Psychooncology. (2001) 10:88–92.
29. Kroenke, K, Spitzer, RL, and Williams, JBW. The PHQ-15: validity of a new measure for evaluating the severity of somatic symptoms. Psychosom Med. (2002) 64:258–66. doi: 10.1097/00006842-200203000-00008
30. Kroenke, K, Spitzer, RL, and Williams, JBW. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
31. Ros Montalbán, S, Comas Vives, A, and Garcia-Garcia, M. Validation of the Spanish version of the PHQ-15 questionnaire for the evaluation of physical symptoms in patients with depression and/or anxiety disorders: DEPRE-SOMA study. Actas Esp Psiquiatr. (2010) 38:345–57.
32. Saldivia, S, Aslan, J, Cova, F, Vicente, B, Inostroza, C, and Rincón, P. Propiedades psicométricas del PHQ-9 (Patient Health Questionnaire) en centros de atención primaria de Chile. Rev Med Chile. (2019) 147:53–60. doi: 10.4067/S0034-98872019000100053
33. Roberts, K, Chong, T, Hollands, E, Tan, J, Mohan, GRKA, and Cohen, PA. Screening for sexual health concerns in survivors of gynecological cancer. Support Care Cancer. (2020) 28:599–605. doi: 10.1007/s00520-019-04872-4
34. Boa, R, and Grénman, S. Psychosexual health in gynecologic cancer. Int J Gynecol Obstet. (2018) 143:147–52. doi: 10.1002/ijgo.12623
35. Del Pup, L, Villa, P, Amar, ID, Bottoni, C, and Scambia, G. Approach to sexual dysfunction in women with cancer. Int J Gynecol Cancer. (2019) 29:630–4. doi: 10.1136/ijgc-2018-000096
36. Aerts, L, Enzlin, P, Verhaeghe, J, Poppe, W, Vergote, I, and Amant, F. Long-term sexual functioning in women after surgical treatment of cervical Cancer stages IA to IB: a prospective controlled study. Int J Gynecol Cancer. (2014) 24:1527–34. doi: 10.1097/IGC.0000000000000236
37. Aerts, L, Enzlin, P, Verhaeghe, J, Poppe, W, Vergote, I, and Amant, F. Sexual functioning in women after surgical treatment for endometrial Cancer: a prospective controlled study. J Sex Med. (2015) 12:198–209. doi: 10.1111/jsm.12764
38. Spagnoletti, BRM, Bennett, LR, Keenan, C, Shetty, SS, Manderson, L, McPake, B, et al. What factors shape quality of life for women affected by gynaecological cancer in south, south east and east Asian countries? A critical review. Reprod Health. (2022) 19:70. doi: 10.1186/s12978-022-01369-y
39. Jaafarpour, M, Khani, A, Khajavikhan, J, and Suhrabi, Z. Female sexual dysfunction: prevalence and risk factors. J Clin Diagnostic Res. (2013) 7:2877–80. doi: 10.7860/JCDR/2013/6813.3822
40. Lo, SS-T, and Kok, W-M. Sexual behavior and symptoms among reproductive age Chinese women in Hong Kong. J Sex Med. (2014) 11:1749–56. doi: 10.1111/jsm.12508
41. Thapa, N, Maharjan, M, Xiong, Y, Jiang, D, Nguyen, T-P, Petrini, MA, et al. Impact of cervical cancer on quality of life of women in Hubei, China. Sci Rep. (2018) 8:11993. doi: 10.1038/s41598-018-30506-6
Keywords: sexual dysfunction, quality of life, low-dose-rate, brachytherapy, cervical and endometrial cancer
Citation: González-Alcorta CB, Alcorta-Garza A, Ruiz-Sánchez D, Soto-Martínez BA, Alcorta-Núñez F, Galaviz-Reynoso IL, López-Sierra PA, González-Guerrero JF and Vidal-Gutiérrez O (2025) Sexual dysfunction and quality of life in cervical and endometrial cancer patients before and after low-dose-rate brachytherapy: a cohort study. Front. Med. 12:1584141. doi: 10.3389/fmed.2025.1584141
Edited by:
Andrea Giannini, Umberto 1 Hospital, ItalyReviewed by:
Elena Groff, Veneto Institute of Oncology (IRCCS), ItalyPooriwat Muangwong, Chiang Mai University, Thailand
Giuseppe Facondo, Ospedale Santa Maria della Misericordia di Udine, Italy
Copyright © 2025 González-Alcorta, Alcorta-Garza, Ruiz-Sánchez, Soto-Martínez, Alcorta-Núñez, Galaviz-Reynoso, López-Sierra, González-Guerrero and Vidal-Gutiérrez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adelina Alcorta-Garza, YWRlYWxjb3J0YUBnbWFpbC5jb20=