 Tianjiao Dai1,2*†Ying Zou2Hongbo Li3Wei Xu4Jing Luo2Lezheng Wang2Qiyue Sun2Lei Shi5Shaoxuan Ma2
Tianjiao Dai1,2*†Ying Zou2Hongbo Li3Wei Xu4Jing Luo2Lezheng Wang2Qiyue Sun2Lei Shi5Shaoxuan Ma2 Ye Liu1*
Ye Liu1*- 1School of Sport Science, Beijing Sport University, Beijing, China
- 2School of Rehabilitation, Jiangsu College of Nursing, Huai'an, China
- 3Department of Rehabilitation, Jinhu County People’s Hospital, Huai’an, China
- 4Department of Rehabilitation, Zhenjiang Hospital of Integrated Traditional Chinese and Western Medicine, Zhenjiang, China
- 5College of Physical Education, Yangzhou University, Yangzhou, China
Background: Stroke rehabilitation encompasses crucial components essential for the recovery process. This study aimed to investigate the knowledge, attitudes, and practices (KAP) of stroke patients regarding home-based exercise and psychological rehabilitation programs aimed at enhancing their physical and mental well-being, as well as alleviating depressive symptoms.
Methods: This study conducted a cross-sectional survey at 37 institutions from December 2023 to January 2024. The survey gathered demographic data and assessed KAP related to stroke rehabilitation through structured questionnaires.
Results: A total of 499 valid questionnaires were included in this study. Of these participants, 312 (62.5%) were male and 252 (50.5%) were aged over 60 years. The median [25.75%] knowledge, attitude, and practice scores were 9.03 (5.04) (possible range: 0–20), 33.19 (3.55) (possible range: 9–45), and 21.43 (4.49) (possible range: 6–30), respectively. Multivariate logistic regression showed that knowledge score (OR = 1.19, 95% CI: [1.13, 1.26], p < 0.001), attitude score (OR = 1.28, 95% CI: [1.19, 1.38], p < 0.001), employed (OR = 2.41, 95% CI: [1.15, 5.04], p = 0.020), retired (OR = 2.20, 95% CI: [1.20, 4.02], p = 0.011), and more than 3 years of duration of stroke (OR = 0.37, 95% CI: [0.16, 0.85], p = 0.019) were independently associated with practice. Structural equation modeling (SEM) showed that knowledge directly affected attitude (β = 0.407, p < 0.001), knowledge (β = 0.390, p < 0.001) and attitude (β = 0.461, p < 0.001) directly affected practice, and knowledge indirectly affected practice through attitude (β = 0.188, p = 0.007).
Conclusion: The study highlights that while stroke patients generally exhibit positive attitudes and practices toward home-based exercise and psychological rehabilitation, there remains a gap in their knowledge about these crucial interventions. Clinically, it is imperative to enhance educational strategies targeting stroke survivors, focusing on improving knowledge to further strengthen their rehabilitation outcomes and adherence to prescribed regimens.
Introduction
China, as the largest developing country in the world, is currently facing significant challenges in addressing the needs of its rapidly aging population. The average age of prevalent stroke patients in China is 66.4 years (1). Stroke, comprising ischemic and hemorrhagic types, is not only the second leading cause of death worldwide but also the foremost cause of mortality in China, home to the highest stroke burden globally (2–4). In individuals over 40, the standardized prevalence of stroke in China is 2.61%, with an incidence rate of 505.23 per 100,000 individuals, totaling approximately 17.8 million stroke patients (5). Furthermore, studies highlight significant psychosocial challenges faced by stroke patients, including prevalent anxiety and depression, experienced by 23 and 19% of patients, respectively, within the first 6 months post-stroke (6).
Effective stroke management primarily aims at reducing brain injury and enhancing patients’ recovery. The success of treatments heavily depends on the timely and accurate diagnosis by specialists, prompt initiation of treatment, and subsequent rehabilitation. Research indicates that the brain’s high plasticity allows for significant reductions in neurological deficits through immediate and long-term rehabilitation. However, the recovery process in post-stroke patients is notably varied due to factors such as the extent of the stroke, the degree of spontaneous regeneration, neuroplasticity, selected pharmacotherapy, and the adequacy of rehabilitation measures (7). Post-acute stroke rehabilitation typically incorporates two main models: Inpatient Rehabilitation (IR), which is provided within hospital settings, and Community Rehabilitation (CR), which includes outpatient services at clinics, day hospitals, or in the patient’s own home. Importably, the CR model features Early Supported Discharge (ESD), facilitating early hospital discharge with continued rehabilitation and support at home (8). Additionally, in China, there is a prevalent tradition of family-based rehabilitation, where family caregivers often take on the role of primary caregivers for stroke patients. This cultural practice underscores the integral role of familial support in the continuity of care and rehabilitation for stroke survivors.
The Knowledge, Attitude, and Practice (KAP) model is pivotal in public health, suggesting that individual behaviors are significantly influenced by one’s knowledge and attitudes. This approach is instrumental in examining health-related behaviors, where the assessment of knowledge and risk perception is frequently conducted through KAP surveys, shedding light on the intricate relationships between knowledge, attitudes, and behaviors (9–11). In China, which bears the heaviest global stroke burden and a significantly aging population, researching the KAP regarding Home-Based Exercise and Psychological Rehabilitation Programs among stroke patients is crucial. This study seeks to improve recovery outcomes and decrease morbidity by customizing interventions to the patients’ needs and the cultural framework, particularly focusing on the largely unexplored domain of family-supported home care predominant in China.
While a previous KAP study targeting family members of stroke survivors revealed relatively high scores in KAP questionnaires, it highlighted a gap in knowledge among caregivers in rural areas with lower education levels, making the patients more susceptible to potential complications of stroke (12). Despite this, there has been no similar research directly focusing on the patients. Therefore, this study aims to investigate the KAP of stroke patients concerning home-based exercise and psychological rehabilitation programs. The goal is to enhance their physical and mental well-being and alleviate symptoms of depression, which could lead to significant improvements in rehabilitation effectiveness and patient outcomes in this vital area.
Materials and methods
Study design and subjects
This cross-sectional study was conducted from December 2023 to January 2024 at 37 institutions and involved stroke patients as the research subjects. The study received approval from the Ethics Committee of Jinhu County People’s Hospital (LLSC 2023-LW-27), and all participants provided informed consent.
Inclusion criteria
Participants were included in the study if they:
1. Met the criteria set forth by the Fourth National Diagnostic Standards for Cerebrovascular Disease and were diagnosed with stroke through imaging tests such as CT or MRI.
2. Were in the subacute or recovery phase of stroke with stable conditions.
3. Possessed a sufficient level of education to understand the study procedures and could cooperate with the investigation.
4. Voluntarily agreed to participate in the study and signed the informed consent form.
Exclusion criteria
Individuals were excluded from the study if they:
1. Had Alzheimer’s disease.
2. Were diagnosed with malignant tumors, severe cardiovascular diseases, or significant liver and kidney dysfunction.
3. Had a long-term dependency on sedative drugs or were alcohol-dependent.
4. Had a family history of mental disorders.
Questionnaire introduction
The questionnaire was meticulously designed with references to guidelines and relevant literature (13–16), incorporating input from five experts in clinical rehabilitation. The preliminary version underwent a small-scale pilot test (40 copies) to assess reliability, which was determined to be 0.914. The finalized version of the questionnaire was composed in Chinese and comprised four dimensions covering a total of 38 items: 12 items on basic information, 10 on knowledge, 9 on attitudes, and 7 on practices (See Supplementary questionnaire).
For scoring, the knowledge dimension used a three-point scale: “Very familiar” (2 points), “Have heard of it” (1 point), and “Unclear” (0 points), with total scores ranging from 0 to 20. Attitudes were measured on a five-point Likert scale; items A1-A4 and A6-A8 gaged positive attitudes and scored from 5 (strongly agree) to 1 (strongly disagree), whereas A5 and A9 assessed negative attitudes and scored inversely from 1 to 5, with the overall attitude score spanning 9 to 45 points. Practice items P1-P6 also utilized a five-point Likert scale, scoring from 5 (completely meets) to 1 (completely does not meet), with the score range for this dimension being 6 to 30. Item P7 was a multiple-choice question designed to identify the sources of current knowledge. A scoring threshold of over 70% was set for each dimension to classify adequate knowledge, positive attitudes, and proactive practices (17).
The questionnaire was made available electronically through the “Questionnaire Star” platform (Changsha Ranxing Information Technology Co., Ltd.). It was distributed in 37 tertiary and secondary specialty hospital departments across 13 cities in Jiangsu Province (See Supplementary Table S1) via QR codes in patients’ WeChat and QQ groups. Paper versions were also distributed in rehabilitation training halls and were filled out voluntarily. Assistance was provided to some patients who were unable to use mobile devices or handle writing tools, either by a family member or a therapist. A total of 106 responses were collected electronically, and 396 via paper. After corrections for suspected errors made through telephone or direct therapist contact, and the exclusion of two for incomplete responses, 500 valid questionnaires were retained. The data were compiled into an Excel spreadsheet and reviewed for completeness, consistency, and validity by the research team.
Sample size calculation:
The sample size for this cross-sectional study was determined using the standard formula for minimum sample size in prevalence studies (18):
For this calculation:
The significance level (𝛼) is set at 0.05, giving a Z value of 1.96.
The margin of error (𝛿) is 0.05.
The estimated proportion (𝑝) is 0.5, assuming maximum variability.
Using these parameters, the required sample size (𝑛) is calculated to be 384. To account for a typical questionnaire response rate of 80%, the final sample size needed is adjusted to at least 480 questionnaires to ensure sufficient data for robust analysis.
Statistical analysis
Data analysis was conducted using R 4.3.2 and Stata 18.0 (Stata Corporation, College Station, TX, USA). Continuous data are presented as means and standard deviations (SD), while categorical data are expressed as n (%). Continuous variables underwent a normality test, with the t-test for normally distributed data and the Wilcoxon Mann–Whitney test for non-normally distributed data when comparing two groups. For three or more groups with normally distributed continuous variables and uniform variance, ANOVA was used for comparisons, while the Kruskal-Wallis test was employed for non-normally distributed data. Univariate and multivariate logistic regression were performed to explore the risk factors associated with K, A, and P, with 70% of the total score was used as the cut-off value. Univariate variables with p < 0.05 were enrolled in multivariate regression. Structural equation modeling (SEM) was utilized to explore the relationships between knowledge (K), attitude (A), and practice (P). Model fit was evaluated using root mean square error of approximation (RMSEA), incremental fit index (IFI), Tucker–Lewis index (TLI), and comparative fit index (CFI). A two-sided p-value less than 0.05 was considered statistically significant.
Result
In this study, we initially collected 502 questionnaires, from which we removed three due to irregularities: two from the attitude section and one from question 8 in the baseline section. This resulted in 499 valid questionnaires, achieving a validity rate of 99.40%. The internal consistency of both the total scale and its subscales was confirmed as being high, with a Cronbach’s alpha of 0.901 for the total scale, and 0.904, 0.804, and 0.836 for the knowledge, attitude, and practice sections, respectively.
Among the 499 stroke patients who participated in the study, 312 (62.5%) were male, 252 (50.5%) were over 60 years old, 249 (49.9%) lived in the city, 215 (43.1%) had junior high school education or below, 256 (51.3%) had monthly per capita income of less than 5,000 yuan, only 92 (18.5%) could take care of themselves, 301 (60.3%) had stroke for less than 1 year, 301 (60.3%) had exercise habit before onset, 448 (89.8%) were positive and optimistic before onset. The median [25.75%] knowledge, attitude, and practice scores were 9.03 (5.04) (possible range: 0–20), 33.19 (3.55) (possible range: 9–45), and 21.43 (4.49) (possible range: 6–30), respectively. Participants’ knowledge scores were more likely to vary depending on: residence (p < 0.001), education (p < 0.001), work status (p < 0.001), monthly per capita income (p < 0.001), marital status (p = 0.036), and whether have exercise habits before the onset of the disease (p < 0.001). Meanwhile, their attitude scores were more likely to vary across residence (p = 0.028), duration of stroke (p = 0.013), whether have exercise habits before the onset of the disease (p = 0.003), and whether positive and optimistic before the onset of the disease (p = 0.005). Furthermore, their practice scores were more likely to vary depending on: residence (p = 0.02), education (p = 0.011), work status (p = 0.03), whether have exercise habits before the onset of the disease (p < 0.001), and whether positive and optimistic before the onset of the disease (p = 0.046) (Table 1).
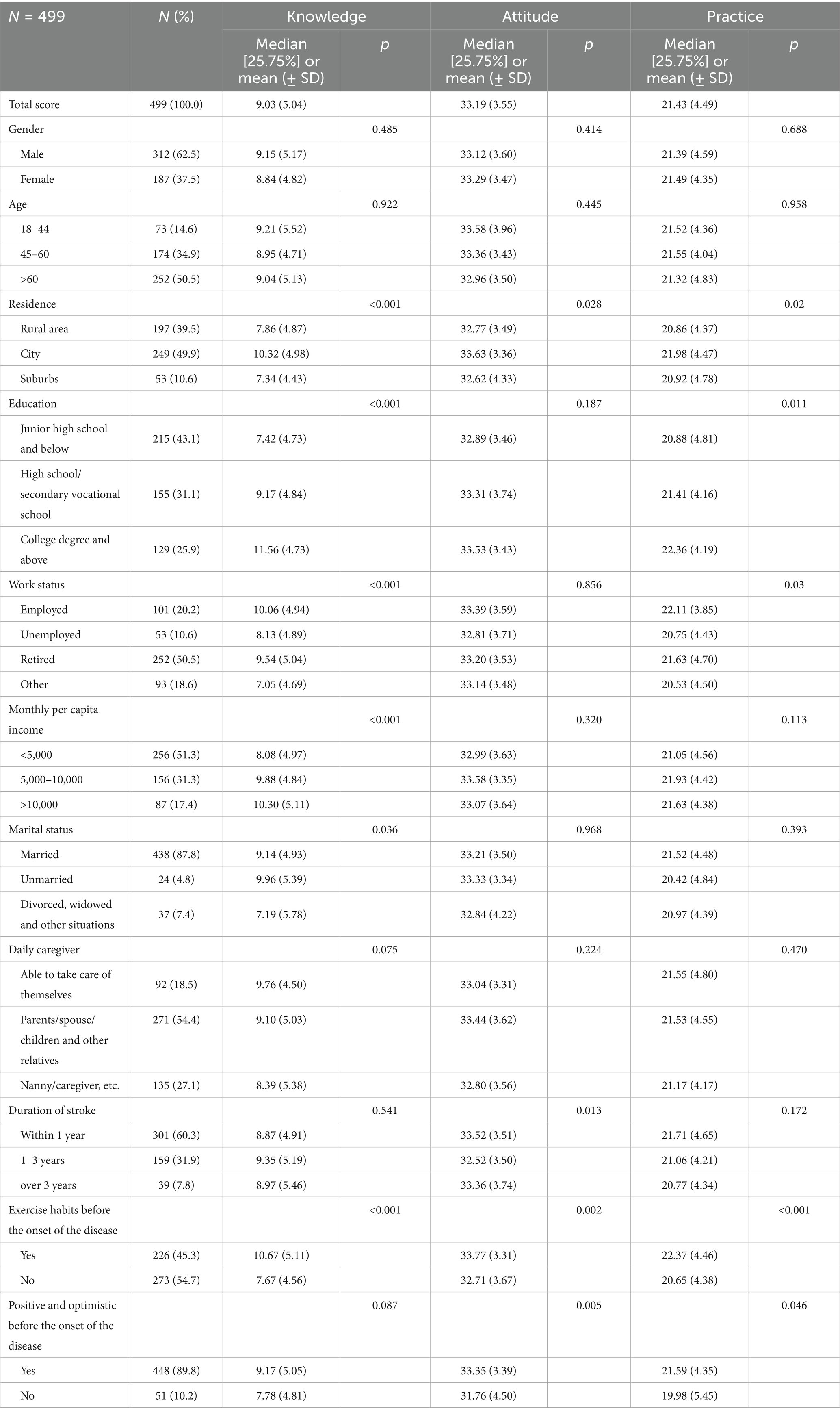
Table 1. Demographic characteristics.
The distribution of knowledge dimension revealed that the question with the highest number of participants choosing the “Very familiar” option was “Smoking, drinking, high blood pressure, diabetes, coronary heart disease, dyslipidemia, atrial fibrillation, etc. may induce or worsen stroke.” (K2), with 31.7%. The question with the highest number of participants choosing the “Have heard about it” option was “For stroke patients with mild depression/anxiety and other complications, the medical staff’s psychological rehabilitation program (including reasonable short-term exercise during the day, light music before bed to help sleep, deep breathing training, etc.) can effectively improve the patient’s quality of life.” (K9), with 55.5%. The question with the highest number of participants choosing the “Unclear” option was “Aquatic exercise therapy (i.e., hydrotherapy exercise) can effectively improve the physical function and activity participation ability of stroke patients.” (K7), with 45.9% (Supplementary Table S2).
Responses to the attitude dimension showed that 34.1% fully trusted the therapeutic, exercise, and psychological interventions provided to them by their doctors and caregivers, and were able to strictly implement them (A3), and 53.5% believed that they could adhere to the recommended programs in the long term (A7). When it comes to whether they were interested in learning about the relevant knowledge (A1), 23.6% were neutral. It is noteworthy that 18.6% strongly agreed and 31.9% agreed that their family members no longer value their opinions after the disease, that their presence in the family is diminishing, and that they are often discriminated against by other people on the road (A9) (Supplementary Table S3).
Responses to the practice dimension showed that 34.7% do not necessarily communicate the correct exercise rehabilitation program to their friends and relatives and strictly implement it with them (P3), 32.9% do not necessarily seek help from doctors/nursing staff when their psychological state is not good (P5), 19.4% seldom learn the relevant knowledge (P1), and 15.2% seldom give psychological support treatment program to their friends and relatives when they find the same psychological condition (P6) (Supplementary Table S4). When it comes to sources of knowledge about stroke and related exercise intervention and psychological intervention programs (P7), doctors and caregivers were reported by 89% of participants, followed by real-life cases around them (46.5%) (Supplementary Table S5).
In the correlation analysis, significant positive correlations were found between knowledge and attitude (r = 0.308, p = 0.002), knowledge and practice (r = 0.497, p < 0.001), and attitude and practice (r = 0.502, p < 0.001), respectively (Supplementary Table S6).
The number of participants above the cut-off value of knowledge, attitude, and practice score were 273 (54.7%), 272 (54.5%), and 255 (51.1%), respectively (Supplementary Table S7). Multivariate logistic regression showed that being college degree and above (OR = 3.36, 95% CI: [1.82, 6.22], p < 0.001), retired (OR = 2.22, 95% CI: [1.27, 3.90], p = 0.005), unmarried (OR = 3.79, 95% CI: [1.06, 13.64], p = 0.041), able to take care of themselves (OR = 2.47, 95% CI: [1.31, 4.65], p = 0.005), and without exercise habits before the onset of the disease (OR = 0.48, 95% CI: [0.32, 0.72], p < 0.001) were independently associated with knowledge (Table 2). Concurrently, knowledge score (OR = 1.12, 95% CI: [1.07, 1.16], p < 0.001) and 1–3 years of duration of stroke (OR = 0.59, 95% CI: [0.39, 0.89], p = 0.012) were independently associated with attitude (Table 3). Furthermore, knowledge score (OR = 1.19, 95% CI: [1.13, 1.26], p < 0.001), attitude score (OR = 1.28, 95% CI: [1.19, 1.38], p < 0.001), employed (OR = 2.41, 95% CI: [1.15, 5.04], p = 0.020), retired (OR = 2.20, 95% CI: [1.20, 4.02], p = 0.011), and more than 3 years of duration of stroke (OR = 0.37, 95% CI: [0.16, 0.85], p = 0.019) were independently associated with practice (Table 4).
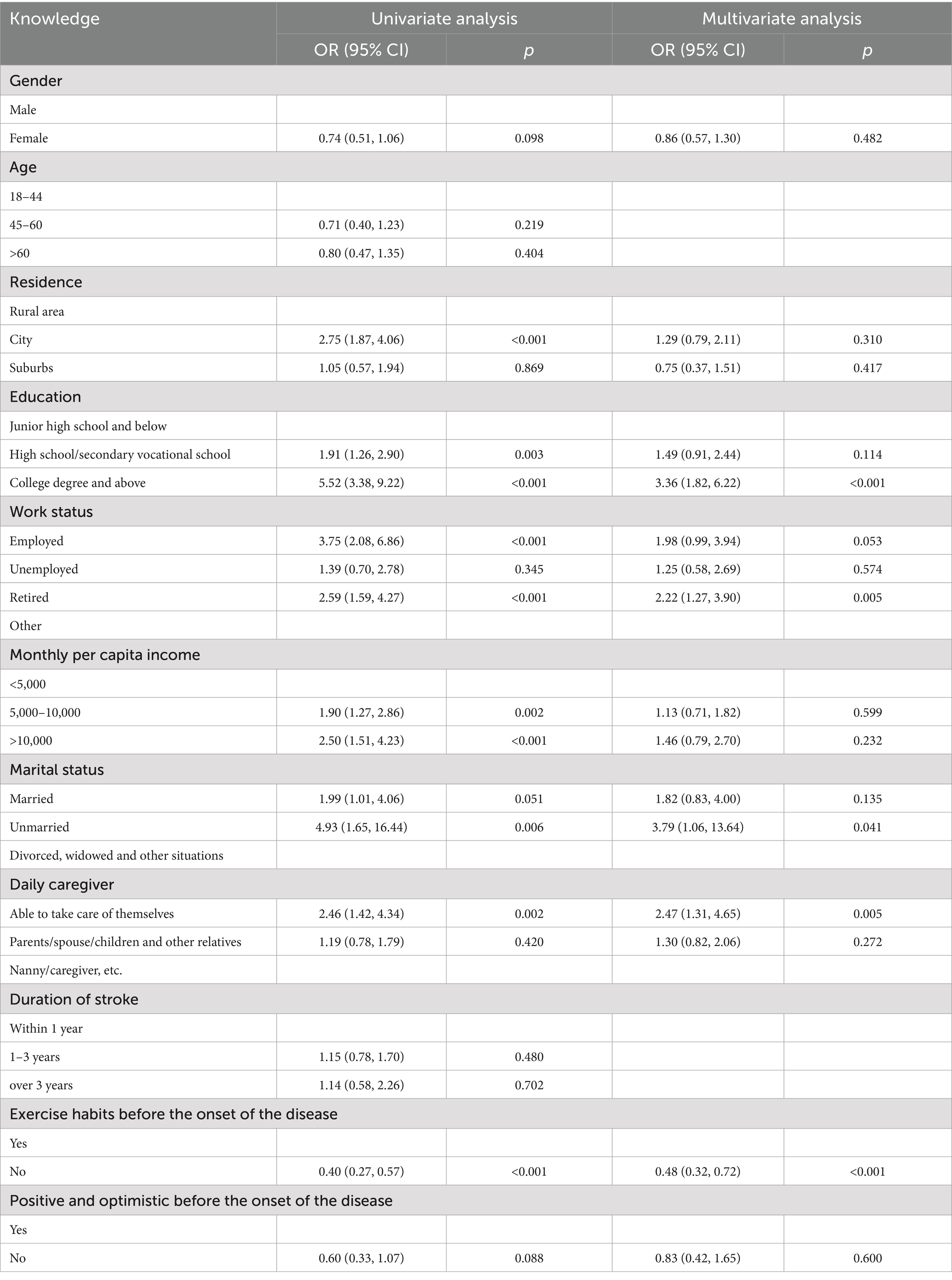
Table 2. Univariate and multivariate logistic regression analysis for knowledge.
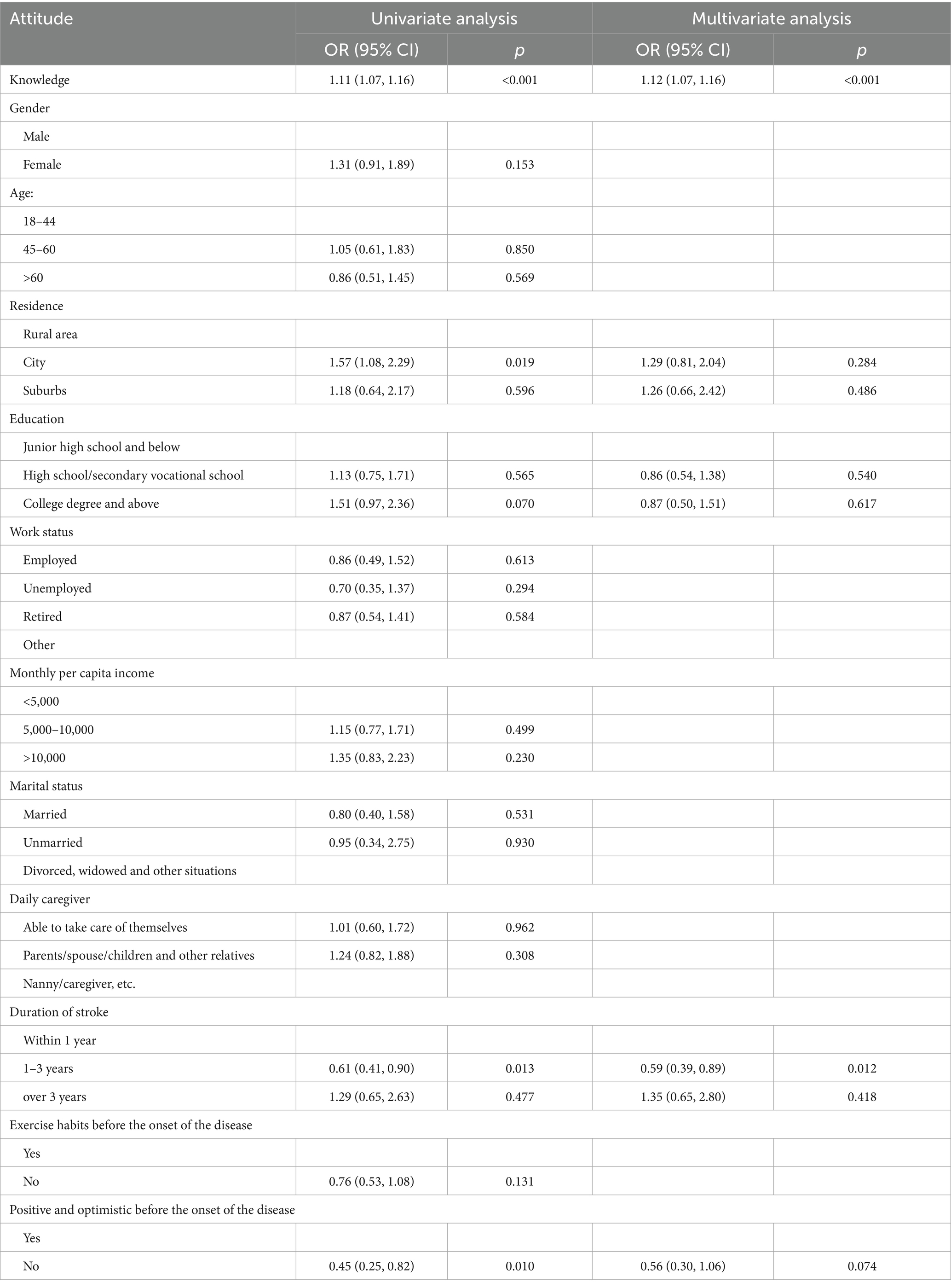
Table 3. Univariate and multivariate logistic regression analysis for attitudes.
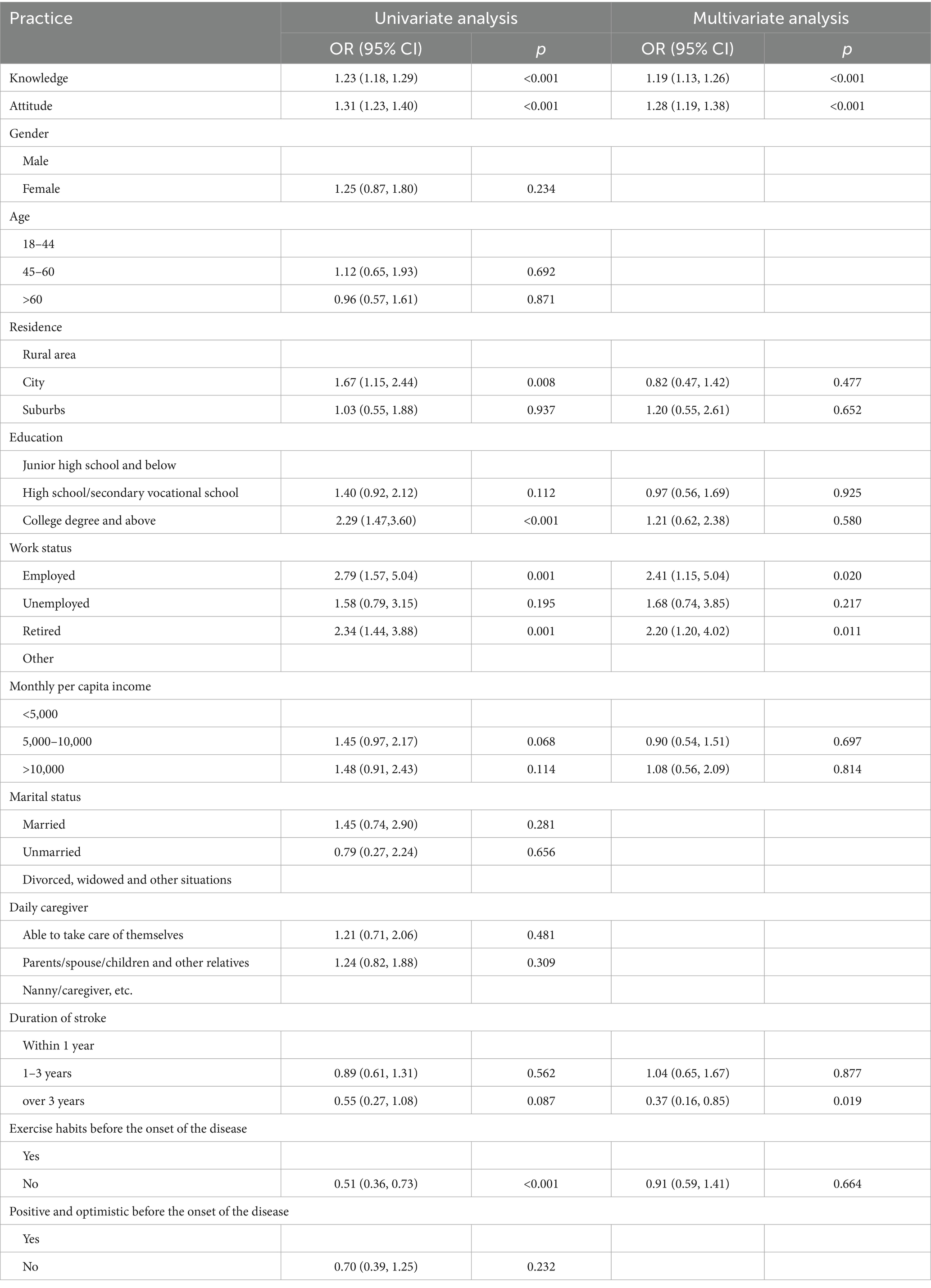
Table 4. Univariate and multivariate logistic regression analysis for practices.
The fit indices of the SEM model reached the desired range, indicating good model fit results (Supplementary Table S8) based on normal SEM model assumptions (Supplementary Table S9), the results of analysis of direct and indirect effects showed that knowledge directly affected attitude (β = 0.407, p < 0.001), knowledge (β = 0.390, p < 0.001) and attitude (β = 0.461, p < 0.001) directly affected practice, and knowledge indirectly affected practice through attitude (β = 0.188, p = 0.007) (Table 5; Figure 1).
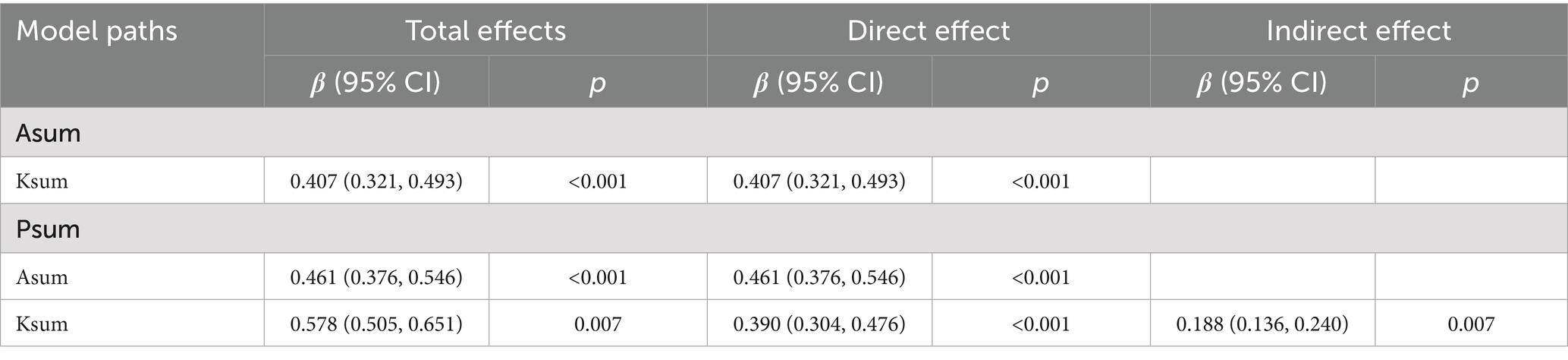
Table 5. SEM model direct effect and indirect effect analysis results.
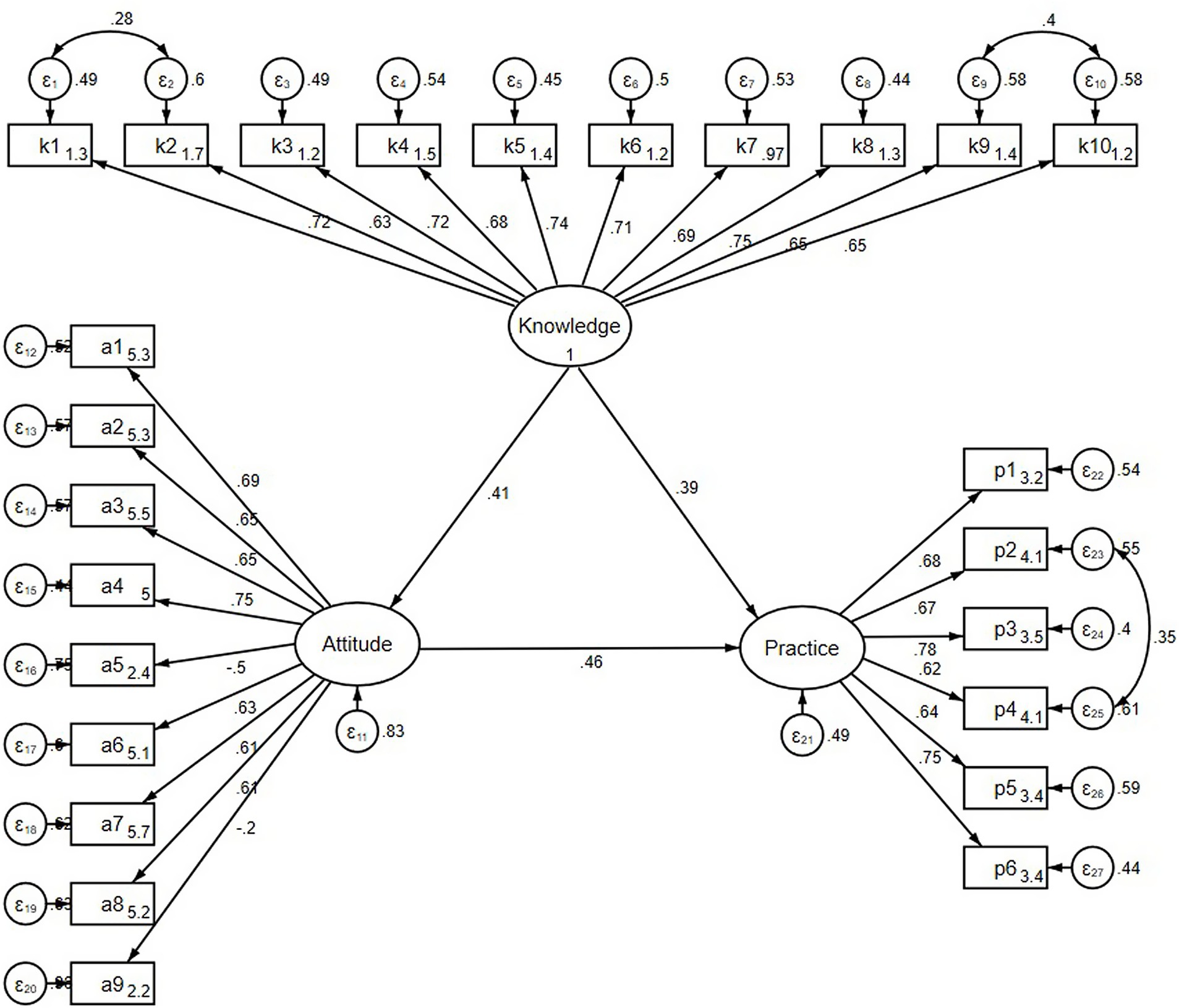
Figure 1. SEM model results of KAP.
Discussion
The study indicates that while stroke patients generally exhibit a positive attitude toward home-based rehabilitation, their knowledge and practice levels remain suboptimal, highlighting a critical gap in stroke recovery programs.
Notably, the study revealed significant disparities in knowledge, attitude, and practice scores based on demographic factors such as residence, education, and prior exercise habits, suggesting that these variables play a crucial role in influencing rehabilitation outcomes. For instance, urban residents displayed higher scores in all three domains compared to their rural counterparts, a pattern that aligns with findings from other studies highlighting urban areas’ better access to health information and resources (19). These differences were substantiated by the multivariate logistic regression results, affirming the robust impact of residence on rehabilitation outcomes.
Educational attainment emerged as a critical determinant, with individuals holding a college degree or higher exhibiting superior knowledge and practice scores. This association is supported by literature indicating that higher education levels correlate with better health literacy, which in turn enhances engagement with health-promoting behaviors (20). The positive influence of employment status on rehabilitation engagement reflects the broader societal role of employment in providing structure and access to resources that facilitate health maintenance (21). Furthermore, the multivariate logistic regression results supported these findings, showing a significant prediction of higher knowledge levels by educational attainment and employment status.
Interestingly, having pre-stroke exercise habits was significantly associated with better outcomes across all KAP domains. This observation is corroborated by research suggesting that pre-existing exercise routines may enhance individuals’ resilience (22). Moreover, multivariate logistic regression reinforced these findings, indicating that factors such as being able to take care of oneself significantly predict better knowledge, which in turn influences attitudes and practices toward stroke rehabilitation.
The findings from our study using multivariate logistic regression, correlation analyses, and SEM collectively demonstrate the profound interconnectedness between KAP in the context of stroke rehabilitation, confirming that enhancements in one domain could lead to improvements in others. This is consistent with the previous study that informed patients are more likely to have positive attitudes toward their treatment options, which enhances adherence to prescribed practices (23). These findings suggest that interventions aimed at enhancing knowledge could be particularly beneficial, as increased knowledge not only uplifts attitudes but also promotes healthier practices.
The results indicate a significant variance in patients’ familiarity with various aspects of stroke, ranging from etiology to rehabilitation techniques. Notably, many patients reported being ‘unclear’ about critical rehabilitation practices such as early sports rehabilitation, aquatic exercise therapy, and specific psychological treatment programs. To address these gaps, targeted educational initiatives should be developed, emphasizing the practical application of rehabilitation techniques in everyday life. For example, utilizing popular social media platforms in China, like WeChat and Douyin, could disseminate bite-sized, easily digestible information about stroke rehabilitation. Additionally, interactive webinars hosted by healthcare professionals can offer in-depth discussions and Q&A sessions to reinforce understanding and application of the knowledge (24, 25).
The attitudes of stroke patients toward their recovery process show a generally positive inclination, but concerns about the effectiveness of long-term adherence to rehabilitation programs and fear of relapse indicate areas needing attention. Similar to previous findings, where patients’ confidence in rehabilitation positively correlated with their recovery outcomes, our study highlights the need for enhancing patients’ trust and commitment to prescribed interventions (26). To improve this, regular motivational interviewing sessions could be integrated into routine care, where healthcare providers reinforce the benefits of sustained rehabilitation efforts and address any misconceptions. Furthermore, creating patient-led support groups, particularly on platforms, where experiences and tips can be shared, may strengthen patients’ resolve and normalize their experiences, enhancing their attitudes toward ongoing care (27, 28).
In practice, while some patients regularly engage with their rehabilitation protocols, a significant number report not adhering strictly to the prescribed activities, especially in terms of sharing and implementing exercise and psychological plans with others. This reflects previous findings, which emphasized the role of social support in improving rehabilitation adherence (29). To enhance practical application, hospitals could partner with community centers to organize regular, supervised exercise sessions that also serve social functions, encouraging communal participation. Additionally, leveraging technology, such as developing a dedicated app that offers step-by-step guidance and tracking for rehabilitation exercises and psychological practices, could help patients maintain regular practice. Promotional campaigns through WeChat, where success stories and educational content are shared, could also increase engagement and compliance (30, 31).
This study has several limitations that warrant mention. First, the cross-sectional design limits our ability to establish causality between the observed knowledge, attitudes, and practices and patient outcomes, suggesting that longitudinal studies are needed to track changes over time. Second, the data were collected from a single institution, which may limit the generalizability of the findings to other settings or populations. Lastly, the reliance on self-reported measures for assessing knowledge, attitudes, and practices may introduce response biases, as participants could overestimate their compliance or understanding of rehabilitation protocols.
Conclusion
In conclusion, stroke patients exhibit a notable disparity between their generally positive attitudes and the sufficient practices toward home-based exercise and psychological rehabilitation, despite their relatively insufficient knowledge on the subject. To enhance the effectiveness of stroke rehabilitation, healthcare providers should focus on educational interventions that increase knowledge, as this is strongly correlated with improved attitudes and practices among patients.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving humans were approved by this study was approved by the Ethic Committee of Jinhu County People’s Hospital (LLSC 2023-LW-27). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
TD: Data curation, Funding acquisition, Methodology, Writing – original draft, Writing – review & editing. YZ: Project administration, Resources, Writing – original draft, Writing – review & editing. HL: Resources, Supervision, Writing – original draft, Writing – review & editing. WX: Resources, Investigation, Writing – original draft, Writing – review & editing. JL: Data curation, Visualization, Writing – original draft, Writing – review & editing. LW: Investigation, Writing – original draft, Writing – review & editing. QS: Investigation, Writing – original draft, Writing – review & editing. LS: Data curation, Writing – original draft, Writing – review & editing. SM: Data curation, Writing – original draft, Writing – review & editing. YL: Conceptualization, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by Medical Research Project of Jiangsu Commission of Health (Z2021051) to TD and Excellent University Key Young Teacher Programme of Jiangsu Province to TD.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1598489/full#supplementary-material
References
1. Wang, W, Jiang, B, Sun, H, Ru, X, Sun, D, Wang, L, et al. Prevalence, incidence, and mortality of stroke in China: results from a nationwide population-based survey of 480 687 adults. Circulation. (2017) 135:759–71. doi: 10.1161/CIRCULATIONAHA.116.025250
2. GBD 2016 Stroke Collaborators. Global, regional, and national burden of stroke, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. (2019) 18:439–58. doi: 10.1016/S1474-4422(19)30034-1
3. Wu, S, Wu, B, Liu, M, Chen, Z, Wang, W, Anderson, CS, et al. Stroke in China: advances and challenges in epidemiology, prevention, and management. Lancet Neurol. (2019) 18:394–405. doi: 10.1016/S1474-4422(18)30500-3
4. Zhou, M, Wang, H, Zeng, X, Yin, P, Zhu, J, Chen, W, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2019) 394:1145–58. doi: 10.1016/S0140-6736(19)30427-1
5. Guo, L, Wang, J, Wu, Q, Li, X, Zhang, B, Zhou, L, et al. Clinical study of a wearable remote rehabilitation training system for patients with stroke: randomized controlled pilot trial. JMIR Mhealth Uhealth. (2023) 11:e40416. doi: 10.2196/40416
6. Choi, S, and Kim, D. Effects of combining cognitive behavioral therapy with bilateral upper limb training in stroke patients: a randomized controlled trial. Occup Ther Int. (2022) 2022:1–9. doi: 10.1155/2022/4688113
7. Szelenberger, R, Kostka, J, Saluk-Bijak, J, and Miller, E. Pharmacological interventions and rehabilitation approach for enhancing brain self-repair and stroke recovery. Curr Neuropharmacol. (2020) 18:51–64. doi: 10.2174/1570159X17666190726104139
8. Walters, R, Collier, JM, Braighi Carvalho, L, Langhorne, P, Katijjahbe, MA, Tan, D, et al. Exploring post acute rehabilitation service use and outcomes for working age stroke survivors (≤65 years) in Australia, UK and South East Asia: data from the international AVERT trial. BMJ Open. (2020) 10:e035850. doi: 10.1136/bmjopen-2019-035850
9. Aerts, C, Revilla, M, Duval, L, Paaijmans, K, Chandrabose, J, Cox, H, et al. Understanding the role of disease knowledge and risk perception in shaping preventive behavior for selected vector-borne diseases in Guyana. PLoS Negl Trop Dis. (2020) 14:e0008149. doi: 10.1371/journal.pntd.0008149
10. Liao, L, Feng, H, Jiao, J, Zhao, Y, and Ning, H. Nursing assistants' knowledge, attitudes and training needs regarding urinary incontinence in nursing homes: a mixed-methods study. BMC Geriatr. (2023) 23:39. doi: 10.1186/s12877-023-03762-z
11. Mumena, WA. Maternal knowledge, attitude and practices toward free sugar and the associations with free sugar intake in children. Nutrients. (2021) 13:4403. doi: 10.3390/nu13124403
12. Farpour, H, Mashhadiagha, A, Edrisi, F, and Farpour, S. Knowledge, attitude, and practice regarding stroke potential complications among stroke survivors' family members in shiraz, Iran. Turk J Phys Med Rehabil. (2023) 69:83–8. doi: 10.5606/tftrd.2022.9512
13. Billinger, SA, Arena, R, Bernhardt, J, Eng, JJ, Franklin, BA, Johnson, CM, et al. Physical activity and exercise recommendations for stroke survivors: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2014) 45:2532–53. doi: 10.1161/STR.0000000000000022
14. Gittler, M, and Davis, AM. Guidelines for adult stroke rehabilitation and recovery. JAMA. (2018) 319:820–1. doi: 10.1001/jama.2017.22036
15. Winstein, CJ, Stein, J, Arena, R, Bates, B, Cherney, LR, Cramer, SC, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2016) 47:e98–e169. doi: 10.1161/STR.0000000000000098
16. Zhang, T, Zhao, J, Li, X, Bai, Y, Wang, B, Qu, Y, et al. Chinese Stroke Association guidelines for clinical management of cerebrovascular disorders: executive summary and 2019 update of clinical management of stroke rehabilitation. Stroke Vasc Neurol. (2020) 5:250–9. doi: 10.1136/svn-2019-000321
17. He, J, Yang, W, He, Q, Tang, Y, Wang, Y, Wang, G, et al. Chinese pregnant women's knowledge, attitude, and practice of self-protection against coronavirus disease 2019 during the post-pandemic period: a structural equation modeling-based survey. Int J Disaster Risk Reduct. (2023) 87:103559. doi: 10.1016/j.ijdrr.2023.103559
18. Charan, J, and Biswas, T. How to calculate sample size for different study designs in medical research? Indian J Psychol Med. (2013) 35:121–6. doi: 10.4103/0253-7176.116232
19. Zhang, QN, and Lu, HX. Knowledge, attitude, practice and factors that influence the awareness of college students with regards to breast cancer. World J Clin Cases. (2022) 10:538–46. doi: 10.12998/wjcc.v10.i2.538
20. Negesa, LB, Magarey, J, Rasmussen, P, and Hendriks, JML. Patients' knowledge on cardiovascular risk factors and associated lifestyle behaviour in Ethiopia in 2018: a cross-sectional study. PLoS One. (2020) 15:e0234198. doi: 10.1371/journal.pone.0234198
21. Yuldashev, M, Khalikov, U, Nasriddinov, F, Ismailova, N, Kuldasheva, Z, and Ahmad, M. Impact of foreign direct investment on income inequality: evidence from selected Asian economies. PLoS One. (2023) 18:e0281870. doi: 10.1371/journal.pone.0281870
22. Apóstolo, J, Dixe, MDA, Bobrowicz-Campos, E, Areosa, T, Santos-Rocha, R, Braúna, M, et al. Effectiveness of a combined intervention on psychological and physical capacities of frail older adults: a cluster randomized controlled trial. Int J Environ Res Public Health. (2019) 16:3125. doi: 10.3390/ijerph16173125
23. Biyazin, T, Taye, A, and Belay, Y. Patient satisfaction with surgical informed consent at Jimma medical center, Ethiopia. BMC Med Ethics. (2022) 23:103. doi: 10.1186/s12910-022-00841-5
24. Ahn, AB, Kulhari, S, Karimi, A, Sundararajan, S, and Sajatovic, M. Readability of patient education material in stroke: a systematic literature review. Top Stroke Rehabil. (2024) 31:345–60. doi: 10.1080/10749357.2023.2259177
25. Szmuda, T, Alkhater, A, Albrahim, M, Alquraya, E, Ali, S, Dunquwah, RA, et al. YouTube as a source of patient information for stroke: a content-quality and an audience engagement analysis. J Stroke Cerebrovasc Dis. (2020) 29:105065. doi: 10.1016/j.jstrokecerebrovasdis.2020.105065
26. Gustavsson, C, and von Koch, L. Pain self-management intervention supports successful attainment of self-selected rehabilitation goals-secondary analysis of a randomized controlled trial. Health Expect. (2022) 25:1157–67. doi: 10.1111/hex.13469
27. Allegue, DR, Kairy, D, Higgins, J, Archambault, PS, Michaud, F, Miller, WC, et al. A personalized home-based rehabilitation program using Exergames combined with a Telerehabilitation app in a chronic stroke survivor: mixed methods case study. JMIR Serious Games. (2021) 9:e26153. doi: 10.2196/26153
28. Patel, K, Auton, MF, Watkins, CL, Sutton, CJ, Benedetto, V, Hackett, ML, et al. Delivering motivational interviewing early post stroke: standardisation of the intervention. Disabil Rehabil. (2022) 44:3453–8. doi: 10.1080/09638288.2020.1864035
29. Choukou, MA, Olatoye, F, Urbanowski, R, Caon, M, and Monnin, C. Digital health technology to support health care professionals and family caregivers caring for patients with cognitive impairment: scoping review. JMIR Ment Health. (2023) 10:e40330. doi: 10.2196/40330
30. Jin, Z, Zhu, L, Zhou, S, and Lu, C. Managing post-stroke fatigue using a Mobile health called iHealth after intracerebral hemorrhage. J Multidiscip Healthc. (2024) 17:2389–97. doi: 10.2147/JMDH.S465902
31. Kumar, A, Khurana, D, Pattanaik, S, Kumar, M, Kaur, S, Krishnan, NC, et al. A mobile application-based post-stroke care strategy for survivors and their caregivers for prevention and management of post-stroke complications - "stroke home care:" development and feasibility. J Neurosci Rural Pract. (2024) 15:217–26. doi: 10.25259/JNRP_411_2023
Keywords: knowledge, attitude, practice, stroke, patient, home-based exercise, psychological rehabilitation programs
Citation: Dai T, Zou Y, Li H, Xu W, Luo J, Wang L, Sun Q, Shi L, Ma S and Liu Y (2025) Stroke patients’ knowledge, attitudes, and practices regarding home-based exercise and psychological rehabilitation programs. Front. Med. 12:1598489. doi: 10.3389/fmed.2025.1598489
Edited by:
Giorgio Scivoletto, Santa Lucia Foundation (IRCCS), ItalyReviewed by:
Julie Lynn Schwertfeger, United States Department of Veterans Affairs, United StatesAkshatha Nayak, Kasturba Medical College, Mangalore, India
Copyright © 2025 Dai, Zou, Li, Xu, Luo, Wang, Sun, Shi, Ma and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tianjiao Dai, ZGFpX3RqQGpzY24uZWR1LmNu; Ye Liu, bGl1eWVfdGdAMTYzLmNvbQ==
†ORCID: Tianjiao Dai, orcid.org/0000-0002-8251-1749