 Jorge Andrade-Sierra1,2*
Jorge Andrade-Sierra1,2* Jorge Carlos Andrade-Martínez1Elsa Angélica Fuentes-López1
Jorge Carlos Andrade-Martínez1Elsa Angélica Fuentes-López1 Enrique Rojas-Campos3Víctor Martínez-Mejía1Eduardo González-Espinoza1
Enrique Rojas-Campos3Víctor Martínez-Mejía1Eduardo González-Espinoza1 Ernesto German Cardona-Muñoz1
Ernesto German Cardona-Muñoz1 José Ignacio Cerrillos-Gutiérrez1Luis Alberto Evangelista-Carrillo1Miguel Medina-Pérez1
José Ignacio Cerrillos-Gutiérrez1Luis Alberto Evangelista-Carrillo1Miguel Medina-Pérez1 Moisés Cruz-Landino1
Moisés Cruz-Landino1 Adriana Banda-López1
Adriana Banda-López1 Alejandra Guillermina Miranda-Díaz2J. Ahuixotl Gutiérrez Aceves1
Alejandra Guillermina Miranda-Díaz2J. Ahuixotl Gutiérrez Aceves1 Jorge Andrade-Ortega2
Jorge Andrade-Ortega2 Kevin Javier Arellano-Arteaga4
Kevin Javier Arellano-Arteaga4 Antonio de Jesús Andrade-Ortega2Laura Elizabeth Aguilar Fletes1Gerardo González-Correa1Priscila Preciado1Joel E. Verdugo-Correa1
Antonio de Jesús Andrade-Ortega2Laura Elizabeth Aguilar Fletes1Gerardo González-Correa1Priscila Preciado1Joel E. Verdugo-Correa1 Héctor Leonardo Pazarín-Villaseñor4
Héctor Leonardo Pazarín-Villaseñor4 Ana Luisa Corona-Nakamura5
Ana Luisa Corona-Nakamura5 Mauricio Carvallo-Venegas1
Mauricio Carvallo-Venegas1- 1Department of Nephrology and Organ Transplant Unit, Specialties Hospital, National Western Medical Centre, Mexican Institute of Social Security, Guadalajara, Mexico
- 2Department of Physiology, University Health Sciences Center, University of Guadalajara, Guadalajara, Mexico
- 3Medical Research Unit in Renal Diseases, Specialties Hospital, National Western Medical Centre, Mexican Institute of Social Security, Guadalajara, Mexico
- 4Department of Internal Medicine, Hospital Civil de Guadalajara “Dr. Juan I. Menchaca”, Guadalajara, Mexico
- 5Department of Infectology, Specialties Hospital, National Western Medical Centre, Mexican Institute of Social Security, Guadalajara, Mexico
After kidney transplantation, UTI are the most common infection concern and can cause acute renal injury (AKI) in allografts. However, long-term allograft function, loss, and mortality risk are inconsistent. A retrospective cohort research of 1,341 kidney transplant recipients (KTR) from January 2014 to March 2019 assessed UTI incidence, risk factors, and consequences on AKI and allograft function in the first year. All first-year post-transplant UTI patients were recorded. Third-generation cephalosporin (1 gr, two doses) and 500 mg intravesical amikacin were given to all patients 1 day before surgery. After that, patients had TMP-SMX (160/800 mg qd) for 3–4 months to prevent Pneumocystis jirovecii pneumonia, and the main immunosuppressive regimen was mycophenolate mofetil, prednisone and a Calcineurin inhibitors. The UTI incidence was 42.5%. Escherichia coli was the most common causal bacteria, accounting for a significant amount of strains of Extended-spectrum beta-lactamase (ESBL) and AKI occurred more in the first and second UTI. Our analysis showed risk factors of anti-thymocyte globulin (ATG) use (RR 1.52; p = 0.032), double J catheter (RR 1.9; p = 0.004), and urinary tract abnormalities (RR 1.92; p = 0.007). Although UTI was common and associated with AKI, it did not affect allograft function at 12 months post-transplantation.
Introduction
Urinary tract infection (UTI) is the most common infectious complication in kidney transplant recipients (KTR) (1–4), with a cumulative incidence of up to 53.7% during the first year (4), and prevalence rates ranging from 7.3 to 75% (5). Lack of uniformity in the diagnostic criteria, immunosuppression variability, and differences in the use of antimicrobial prophylaxis can explain the variation in prevalence (5–7). Known risk factors include: older age, female sex, obesity, diabetes, urinary tract abnormalities, systemic diseases, deceased kidney donor, time on dialysis, use of a urethral stent, allograft dysfunction, hepatitis C infection, cytomegalovirus (CMV) infection, over-immunosuppression, and chronic kidney disease (CKD) itself, which leads to functional alterations in the urinary tract (such as reduced antibacterial properties of urine, loss of the urothelial protective mucosa, and immunological changes associated with uremia) (5, 8–14). Gram-negative microorganisms account for more than 70% of UTIs, with Escherichia coli (E-coli) being the most common pathogen (30–80%) (5, 10, 15, 16). A challenging, unfortunate problem with UTIs is the presence of multi-drug resistant (MDR) infections, which arise due to the inadequate use of prophylaxis or treatment of asymptomatic bacteriuria (AB), allograft dysfunction, and the presentation of recurrent and nosocomial UTI (17, 18). It is currently estimated that one in every ten KTR develops a UTI caused by an Extended-spectrum beta-lactamase producing Enterobacteriaceae (ESBL-PE), carrying a risk of recurrence three times greater with a clinical impact of causing acute kidney injury (AKI) that can lead to long-term changes in allograft function, allograft loss, and high mortality; although underlying causes remain unclear (19–29).
Patients and methods
A retrospective cohort study included 1,341 kidney transplant recipients from January 2014 to March 2019, conducted in the Transplant Division of the Specialties Hospital at the National Western Medical Center of the Mexican Institute of Social Security in Guadalajara, Jalisco, Mexico. All patients receiving kidney transplantation from a living (related or known) or deceased donor, with any immunosuppressive regimen, were included and followed up for a minimum of 1 year (monitoring every week for 1 month, every 15 days for the subsequent 3 months, and then monthly for 8 months). Multiorgan recipients, any patients who lost their graft immediately due to surgical complications or hyperacute rejection within the first week post-transplantation, those with primary non-function of the allograft, patients who died within the first month after transplant, and those with incomplete information in the electronic records during the follow-up year were not included in this cohort. Conventional prophylaxis, according to our hospital attention protocol, was 500 mg intravesical amikacin prior to surgery, which was administered to all patients, plus a third generation cephalosporin (cefotaxime 1 g IV or ceftriaxone 1 gr IV, two doses each) prior to surgery. All patients received prophylactic dose of 160 mg trimethoprim and 800 mg sulfamethoxazole qd for 3 to 4 months post-transplantation to prevent Pneumocystis jirovecii pneumonia.
The following data were collected: recipient’s age, sex, history of diabetes mellitus or hypertension, anthropometric characteristics, anatomical alterations in the pre-transplant urinary tract, non-functioning native kidneys, residual uresis, etiology of chronic kidney disease, type and duration of kidney replacement therapy, duration of bladder catheterization, or indwelling urethral catheter, immunosuppression (induction, maintenance and desensitization therapies) and number of bacterial UTI.
The presence of post-transplantation UTIs was documented by clinical evaluation (dysuria, urinary urgency, pain over allograft, chills or fever), pathological urinalysis and systemic inflammatory response with confirmation by urine culture, were registered. In relation to taking urine cultures, our protocol is as follows: after antisepsis of the perineum and/or glands with sterile materials, a mid-stream sample in a sterile receptacle is obtained for the analysis, and the culture medium used was Blood Agar and Mac-Conkey Agar. As per our hospital protocol, in the case of clinical suspicion of complications, all patients undergo ultrasound or kidney tomography to rule out complications (obstruction or collections), all of which were recorded. Urodynamic studies were not registered in any patient. Antibiotic treatment, as well as modifications and duration of treatment, were recorded. Lastly, the serum creatinine (SCr) levels that were determined during the patient’s routine follow-up and during each episode of UTI were recorded.
Definitions
We aimed to adhere to current UTI guidelines and considered the following definitions, although these definitions were adjusted depending on the information obtained from patient records or in the electronic files. Additionally, we excluded AB from this analysis.
Urinary tract infections (UTI)
Urinary tract infections defined by clinical evaluation (dysuria, urinary urgency, pain over allograft, chills or fever) and pathological urinalysis; or, as the presence of bacteria in the urine with ≥105 CFU/mL in the presence of local and/or systemic signs or symptoms of infection. All UTIs that were uncomplicated (dysuria, frequency, or urinary urgency and the absence of fever or pain over allograft) and complicated (fever or bacteremia with one or more of the following symptoms: pain over allograft, lumbar pain, chills) were registered and analyzed concurrently, and we did not differentiate between lower and upper UTI.
Recurrent urinary tract infections (RUTI)
Recurrent urinary tract infections defined as (≥2 UTI episodes per year) new episodes of infection in the same patient, with or without bacterial isolation in a culture, obtained two to 4 weeks after the completion of the previous treatment.
Acute kidney injury (AKI)
Acute kidney injury defined solely as an increase of more than 30% in SCr compared to baseline values during the UTIs episode infections.
Immunosuppression characteristics
Immunosuppression management was carried out according to the protocols at our center: immunosuppression induction was based on basiliximab (BSL) 20 mg at 0- and 4-days post-transplant, or anti-thymocyte globulin (ATG) at a dose of 1 mg/kg/day (accumulated dosage 4 mg/kg).
Maintenance immunosuppression was based on mycophenolate mofetil (MMF) 1.5 to 2 g/day, tacrolimus (TAC) 0.12 mg/Kg/day or cyclosporine A (CsA) 4 mg/Kg/day (with dose adjustment according to serum levels), and prednisone (PDN) of 1 mg/kg/day starting from transplantation, with a reduction in dose to achieve 0.1 mg/kg/day by the third post-transplant month. Desensitization therapies before transplantation were conducted according to protocol, with three plasma exchanges (plasmapheresis) and/or immunoglobulin at 200 mg/kg/day administered on alternating days, along with rituximab at 375 mg/m2 (one or two doses with a 15-day interval), or immunoglobulin at 200 mg/kg/day for 3 days and rituximab at 375 mg/m2, based on medical discretion.
Statistical analysis
Data are presented as mean ± standard deviation or median (percentiles 25–75%), and numbers and percentages where appropriate. Chi-squared test or Fisher’s exact test were used to compare proportions. The unpaired Student t-test was used to compare continuous variables between groups, and the Mann–Whitney U-test was used to compare continuous variables with non-normal distribution. Logistic regression was applied individually to each variable. All episodes of UTIs were modeled in the logistic regression. Statistically significant variables in the univariate analysis were introduced in a multivariate model based on forward stepwise logistic regression to identify independent risk factors for UTI. Associations are represented using relative risk (RR) with a 95% confidence interval (95% CI). All results with a value of p < 0.05 were considered statistically significant. Statistical analysis was performed with SPSS™ software, version 22 (SPSS, Inc., Chicago, IL).
Ethical considerations
The present research complies with the Ethical Principles for Medical Research in Human Beings as stipulated in the Declaration of Helsinki 64th General Assembly, Fortaleza, Brazil, October 2013; in addition to adhering to the standards of good clinical practices. All operations followed the General Health Legal Guidelines for Health Care Research in Mexico, 2nd Title, in Ethical Aspects for Human Research in Human Beings, Chapter 1, Article 17. All patients signed the informed consent forms in the presence of witnesses. The local Ethics and Research Committee accepted the study (R-2017-1301-103).
Results
A total of 1,341 recipients were included in this cohort with a minimum follow-up of 1 year. During the study period, 556 patients (42.5%) developed at least one episode of bacterial UTI: a first episode occurred in 523 patients (39%), a second episode in 241 patients (18%), and a third episode in 121 patients (9%). Based on whether or not they developed a UTI, patients were divided into two groups, the characteristics of which are presented in Table 1. Most patients were young, male, and received their first transplant from a living donor. The incidence of UTI was higher in recipients with a history of diabetes mellitus and pre-transplant anatomical abnormalities of the urinary tract (Table 1). Occurrence of UTI was more prevalent in patients using a double-J catheter and in those who had a Foley catheter for five or more days. A total of 88.4% received maintenance immunosuppression with TAC/MMF/PDN, and 62% underwent induction therapy with ATG (see Table 2).
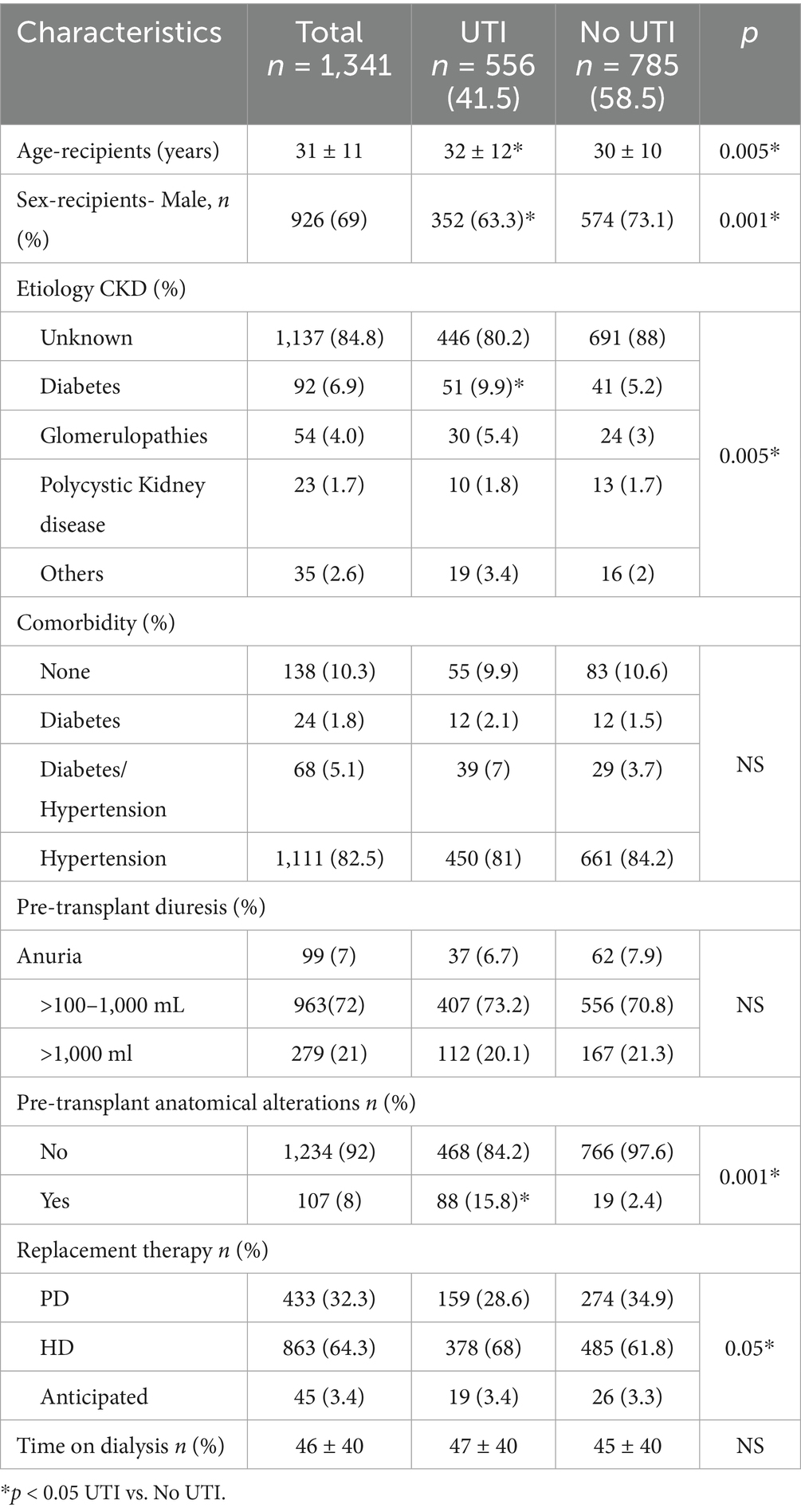
Table 1. Demographic characteristics.
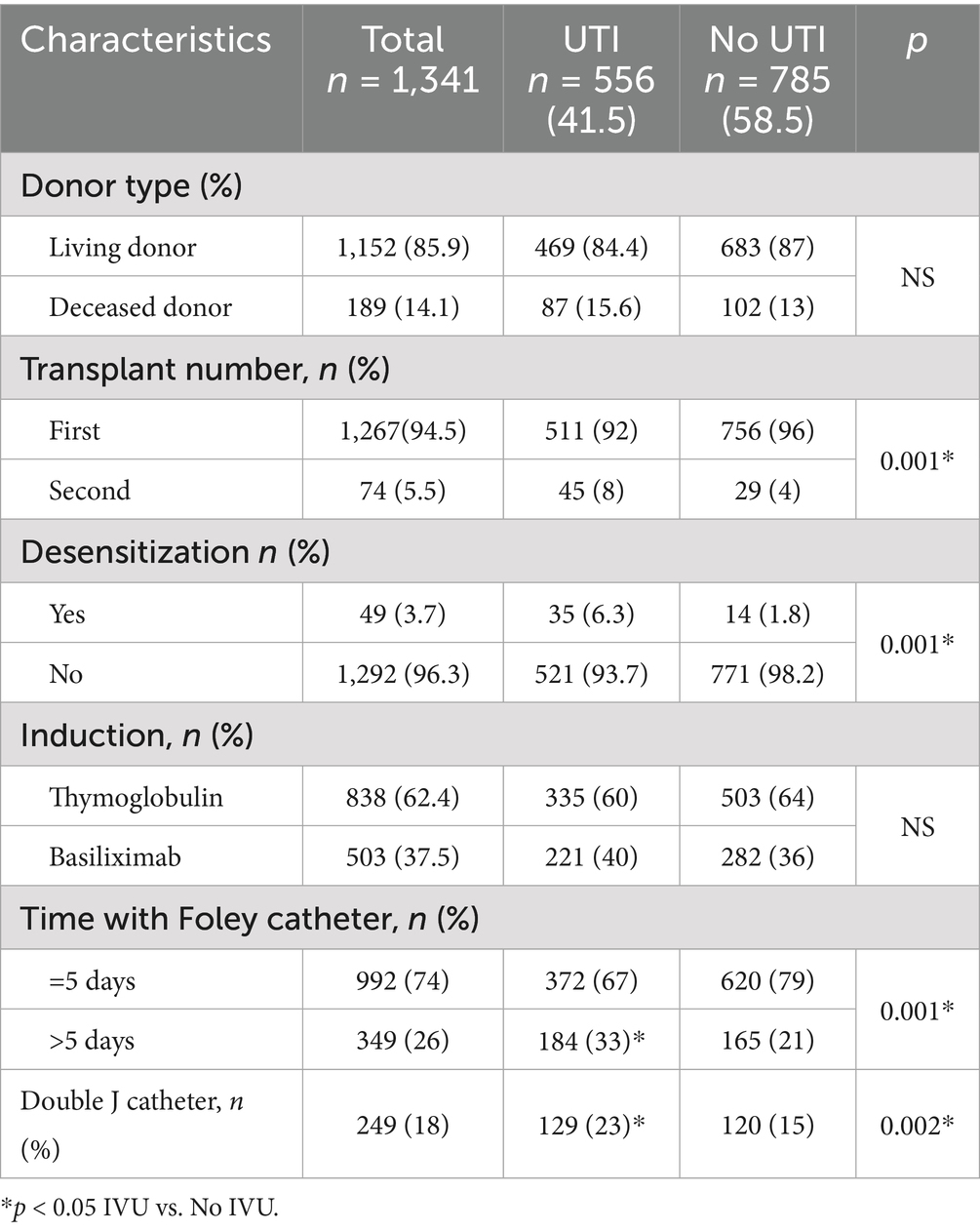
Table 2. Transplant characteristics.
We found that AKI occurred in 54.6% of patients who experienced at least one episode of UTI, with the majority of cases occurring in the first month post transplantation. Both the first and second UTI episode, 52 and 3%, occurred at 30 days and were related with AKI (Table 3) The most frequently isolated infectious pathogen in the first two UTI episodes was E. coli, with a significant percentage of Extended-spectrum beta-lactamase (ESBL) strains (Table 4). During the first UTI episode, E. coli was isolated in 51% of cases (22.5% Spp. and 29% ESBL), while E. faecalis was identified in 21.6% of cases (Table 4). According to our center’s antimicrobial susceptibility patterns, carbapenems were used to treat the first and second episodes in 75.4 and 67.8% of cases, respectively and due to the detection of multi-resistant bacteria (Pseudomonas spp., E. faecalis, A. baumanni, etc.) and the severity of the cases, piperacillin/tazobactam was used in the third episode at 54.7% compared to 26.5% for carbapenems. Most recorded bacteria were resistant to quinolones and trimethoprim/sulfamethoxazole. Anatomical abnormalities [RR 1.92, 95% confidence interval (CI) 1.30–3.0], double J catheter (RR 1.9, 95% CI 1.93–2.91), and the use of ATG, were independent variables associated with at least one episode of bacterial UTI (Table 5). At the end of follow up, kidney allograft function was evaluated solely based on SCr; according to the presence, or not, of UTI, and no significant differences were noted. In individuals with a single UTI, SCr levels were higher at 12 months (Tables 6, 7). Urological complications (urethral stenosis, urethral obstruction, and urinary leakage) were recorded with low frequency in the present cohort, which made their analysis unfeasible.
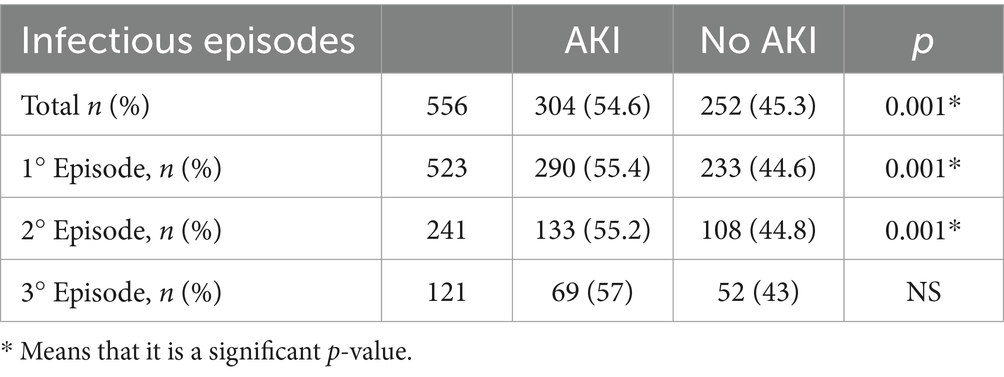
Table 3. Urinary tract infection episodes and their association with acute kidney injury (AKI).
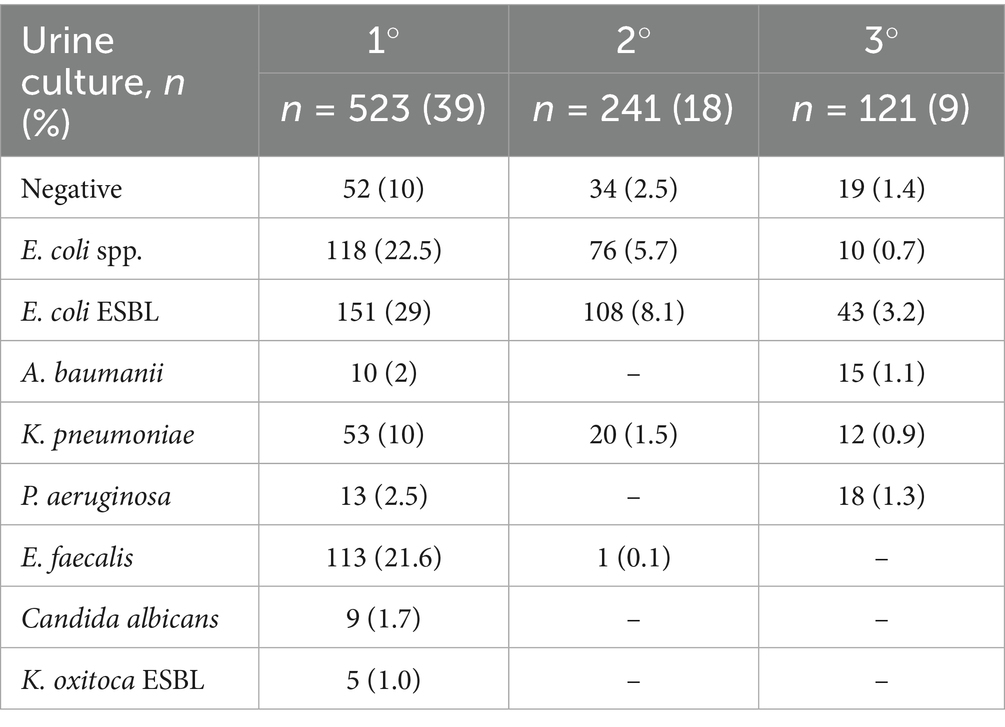
Table 4. Frequency of microorganisms isolated in urine cultures.
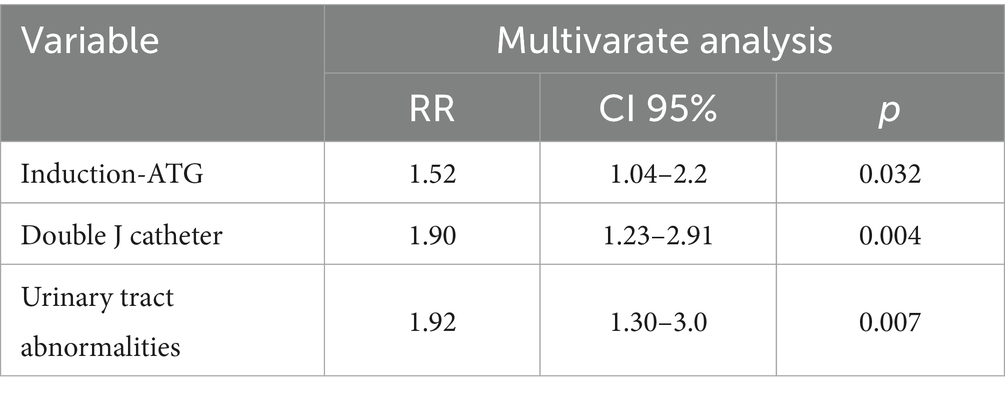
Table 5. Logistics regression analysis showing variables associated with at least one episode of bacterial UTI.
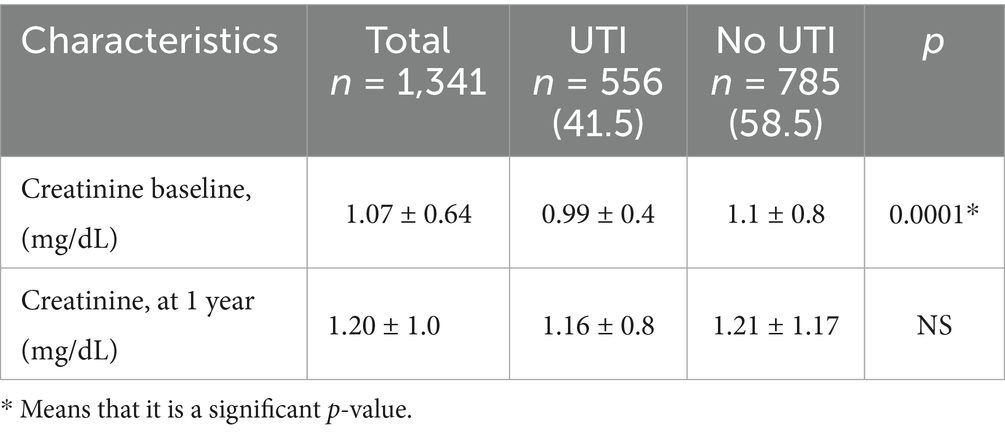
Table 6. Kidney function according to the presence of UTI.
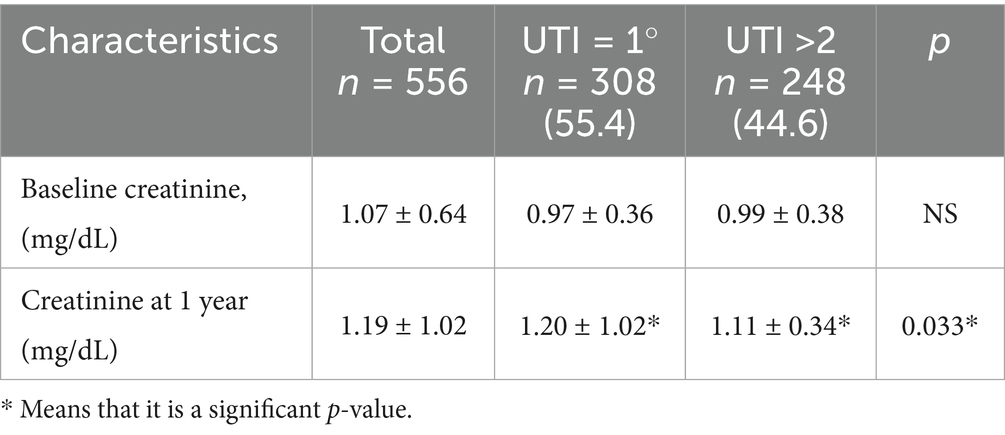
Table 7. Renal function according to the number of UTI episodes.
Discussion
UTI is one of the most prevalent infections during the post-transplant period, leading to undesirable outcomes, especially due to its association with AKI (27, 30), which contributes to reduced kidney function over time, lower allograft survival rates, and increased mortality (20–29).
In our study, the incidence of UTIs among patients with at least one episode was 41.5%, whereas it was 39% for those with only a single first episode, consistent with prior reports (4, 5, 12, 16, 23, 25, 31). Similarly, Arabi et al. (25) reported 35%, in patients followed for just 6 months. The timing of the initial UTI episode in our cohort (within the first 30 days post-transplant) aligns with previous research (12, 24, 25, 32).
Although some studies report similar or higher UTI rates, these often involve older patients, deceased donors, or cases with delayed graft function —factors known to increase incidence (29, 31, 33). In contrast, our cohort included only 15% deceased donors and did not report delayed graft function, making direct risk assessment challenging.
Notably, compared to other young populations receiving living donor transplants, such as those described by Khedr et al. (34), who reported a 27.3% incidence, our study found a higher rate of UTIs; however, their analysis was limited by a small sample size and inclusion of other infection types.
It is noteworthy that, 63.3% of UTI cases in our cohort occurred in male patients, which contrasts with previous studies that have identified female sex as a significant risk factor for UTI (5, 12, 16, 24, 25, 31). Beyond sex-related differences, several other risk factors for UTIs in KRT have been identified. For example the diabetic nephropathy exhibited a higher incidence of UTI in our cohort, consistent with previous studies identifying diabetes and diabetic nephropathy as risk factors (5, 14, 35).
However, diabetic nephropathy was not found to be an independent predictor in our analysis.
Urinary tract abnormalities are a well-established risk factor for UTI (5, 25), as evidenced by their association with at least one UTI episode when considered collectively in our cohort, although individual pathologies could not be analyzed due to the small sample size.
In our center, the use of a double J catheter—another documented risk factor for UTI. — (5, 25, 36, 37) is reserved for cases where urinary tract abnormalities or perioperative anatomical complexity, to prevent major urological complications such as urinary leakage or obstruction. Although less than a quarter of patients received a double J catheter, this was a significant risk predictor (RR 1.90; CI: 1.23–2.91, p < 0.004).
The literature indicates that early (14–21 days) (25, 36, 38–40), or even very early (<7 days) (41), removal of the double J catheter reduces infection risk without significantly increasing urological complications, in our center we opted for delayed removal (6–8 weeks) due to the specific clinical indications that initially warranted catheter placement, prioritizing the prevention of major urological complications in these complex cases.
Regarding Foley catheters, although previous studies have not found significant differences in UTI rates based on early or prolonged removal (42, 43). In our cohort we observed a higher incidence of UTIs with long-term use (>5 days). However, our analysis did not identify this as a significant risk factor, in contrast to other reports (5).
On the other hand, it is recognized that intensified immunosuppressive therapy increases UTIs. Although ATG is increasingly used in higher-risk or deceased donor transplants due to its efficacy in reducing AR (44), it does not improve outcomes in living donor transplants and increases viral and bacterial infections (13, 45, 46).
Although some studies do not consistently identify BSL or ATG as risk factors for UTIs (4, 16, 22, 25, 34), other research reports a higher risk associated with ATG (13, 45, 47). In a cohort study conducted at our institution, we previously established an association between the development of CMV and low-dose ATG (48).
Now, compared to BSL, we still observe a significant rate of UTI, supporting research showing that higher ATG accumulation increases the incidence of UTIs.
Li, S. et al., found that UTI incidence dropped to 5% from 19.8% when ATG accumulation was less than 6.34 mg/kg (13). At our center found that even with, low doses (4 mg) had more UTIs than BSL.
A significant aspect of UTI is its association with AKI, which can lead to allograft loss and increased mortality in KTR (27, 49, 50). In our cohort, over 50% of UTIs were linked to AKI, consistent with previous reports (27, 30, 51).
Notably, we did not differentiate between urosepsis and other complicated UTIs, which may explain the high incidence observed.
While the long-term impact of UTI-related allograft dysfunction remains debated—some studies report no significant deterioration, while others observe worse outcomes (19–26, 28)—we did not find evidence of allograft function decline at follow-up, even among patients with recurrent UTIs similar to other reports (20, 22, 23, 52–54), likely due to prompt antibiotic treatment.
While Sánchez et al. (53), observed a negative effect—particularly when analyzing complicated and recurrent UTIs—other studies, such as Ariza-Heredia et al. (20), found no significant difference in kidney function between recipients with or without UTI, although a tendency toward graft deterioration was noted when radioisotope were used.
This highlights the ongoing controversy regarding the long-term consequences of UTIs on graft outcomes.
Lastly, although rising antibiotic resistance is a concern, our center’s use of carbapenems is justified by local bacterial sensitivity and rapid patient recovery, including from AKI.
Limited pathogen data prevented recurrence analysis, but the frequent use of carbapenems underscores the need for ongoing monitoring and prevention strategies against multidrug-resistant bacteria.
Our research has some limitations: this retrospective study was single-center. Both upper and lower urinary tract infections and complicated (urosepsis) and simple UTI episodes were not distinguished, which could have affected AKI incidence and kidney function results. A lack of long-term follow-up and histopathology data (protocol biopsies) limited the study’s capacity to objectively assess the influence of UTIs on AR and chronic allograft damage.
Despite these limitations, the huge sample size and important UTI epidemiology data from Mexico’s (55) most active kidney transplant referral facility make our study strong.
In conclusion, this study demonstrates a high incidence of UTIs among KTR, significantly associated with the development of AKI. However, no deterioration in allograft function was observed at the end of follow-up. Over-immunosuppression with ATG, the presence of a double-J catheter, and pre-existing urinary tract abnormalities were confirmed as key risk factors for UTI.
These findings highlight the need for long-term monitoring to better understand the true impact of UTIs on graft function and patient outcomes.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Local ethics and research comitee R-2017-1301-103. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JA-S: Visualization, Investigation, Validation, Conceptualization, Methodology, Supervision, Writing – original draft, Resources, Writing – review & editing. JA-M: Visualization, Validation, Conceptualization, Supervision, Writing – review & editing, Investigation. EF-L: Investigation, Writing – review & editing, Validation, Visualization. ER-C: Methodology, Conceptualization, Software, Investigation, Writing – review & editing, Writing – original draft, Formal analysis. VM-M: Supervision, Writing – review & editing, Conceptualization, Visualization, Validation. EG-E: Supervision, Writing – review & editing, Conceptualization, Validation, Visualization. EC-M: Methodology, Supervision, Software, Writing – review & editing, Visualization, Validation. JC-G: Validation, Visualization, Conceptualization, Writing – review & editing, Investigation. LE-C: Investigation, Writing – review & editing, Validation, Supervision, Visualization, Conceptualization. MM-P: Validation, Visualization, Writing – review & editing, Supervision, Investigation. MC-L: Conceptualization, Validation, Writing – review & editing, Supervision, Visualization. AB-L: Supervision, Investigation, Writing – review & editing, Visualization, Validation. AM-D: Writing – review & editing, Conceptualization, Supervision, Visualization, Validation. JG: Supervision, Validation, Visualization, Writing – review & editing. JoA-O: Writing – review & editing, Conceptualization, Supervision, Visualization, Validation. KA-A: Investigation, Writing – review & editing, Validation, Visualization, Supervision. AA-O: Validation, Visualization, Conceptualization, Writing – review & editing, Supervision. LA: Supervision, Investigation, Validation, Writing – review & editing, Visualization. GG-C: Visualization, Supervision, Investigation, Writing – review & editing, Validation. PP: Writing – review & editing, Validation, Supervision, Investigation, Visualization. JV-C: Investigation, Validation, Writing – review & editing, Visualization, Supervision. HP-V: Software, Visualization, Writing – review & editing, Validation, Supervision, Investigation. AC-N: Investigation, Validation, Writing – review & editing, Methodology, Conceptualization, Visualization. MC-V: Writing – review & editing, Methodology, Supervision, Investigation, Visualization, Validation.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1606224/full#supplementary-material
References
1. Sommerer, C, Schröter, I, Gruneberg, K, Schindler, D, Behnisch, R, Morath, C, et al. Incidences of infectious events in a renal transplant cohort of the German Center of Infectious Diseases (DZIF). Open Forum Infect Dis. (2022) 9:ofac243. doi: 10.1093/ofid/ofac243
2. van Delden, C, Stampf, S, Hirsch, HH, Manuel, O, Meylan, P, Cusini, A, et al. Burden and timeline of infectious diseases in the first year after solid organ transplantation in the Swiss transplant cohort study. Clin Infect Dis. (2020) 71:e159–69. doi: 10.1093/cid/ciz1113
3. Agrawal, A, Ison, MG, and Danziger-Isakov, L. Long-term infectious complications of kidney transplantation. Clin J Am Soc Nephrol. (2022) 17:286–95. doi: 10.2215/CJN.15971020
4. Jackson, KR, Motter, JD, Bae, S, Kernodle, A, Long, JJ, Werbel, W, et al. Characterizing the landscape and impact of infections following kidney transplantation. Am J Transplant. (2021) 21:198–207. doi: 10.1111/ajt.16106
5. Hosseinpour, M, Pezeshgi, A, Mahdiabadi, MZ, Sabzghabaei, F, Hajishah, H, and Mahdavynia, S. Prevalence and risk factors of urinary tract infection in kidney recipients: a meta-analysis study. BMC Nephrol. (2023) 24:284. doi: 10.1186/s12882-023-03338-4
6. Hollyer, I, and Ison, MG. The challenge of urinary tract infections in renal transplant recipients. Transpl Infect Dis. (2018) 20:e12828. doi: 10.1111/tid.12828
7. Fiorentino, M, Pesce, F, Schena, A, Simone, S, Castellano, G, and Gesualdo, L. Updates on urinary tract infections in kidney transplantation. J Nephrol. (2019) 32:751–61. doi: 10.1007/s40620-019-00585-3
8. Wu, X, Dong, Y, Liu, Y, Li, Y, Sun, Y, Wang, J, et al. The prevalence and predictive factors of urinary tract infection in patients undergoing renal transplantation: a meta-analysis. Am J Infect Control. (2016) 44:1261–8. doi: 10.1016/j.ajic.2016.04.222
9. Tawab, KA, Gheith, O, Al Otaibi, T, Nampoory, N, Mansour, H, Halim, MA, et al. Recurrent urinary tract infection among renal transplant recipients: risk factors and Long-term outcome. Exp Clin Transplant. (2017) 15:157–63. doi: 10.6002/ect.2016.0069
10. McAteer, J, and Tamma, PD. Diagnosing and managing urinary tract infections in kidney transplant recipients. Infect Dis Clin N Am. (2024) 38:361–80. doi: 10.1016/j.idc.2024.03.008
11. Antonelli, TS, Mantovani, MDS, Carvalho, NC, Archangelo, TE, Minicucci, MF, Ferreira Filho, SP, et al. Body fat predicts urinary tract infection in kidney transplant recipients: a prospective cohort study. J Nephrol. (2024) 37:1551–62. doi: 10.1007/s40620-024-01922-x
12. Dziri, S, Azzabi, A, Tlili, G, Sahtout, W, Soumaya, BN, Wafa, S, et al. Prevalence and predictive factors of urinary tract infection in kidney transplant recipients: a 10-year study. Exp Clin Transplant. (2024) 22:285–9. doi: 10.6002/ect.MESOT2023.P96
13. Li, S, Wang, Z, Dong, Z, Cao, Y, and Wang, H. Cumulative rabbit anti-human thymocyte globulin dose to recipient weight during the peri-operative period is an independent risk factor for early postoperative urinary tract infection after kidney transplantation. Ren Fail. (2024) 46:2414841. doi: 10.1080/0886022X.2024.2414841
14. Krohmals, S, de Terwangne, C, Devresse, A, Goffin, E, Darius, T, Buemi, A, et al. Diabetes mellitus as a risk factor for complicated urinary tract infections in kidney transplant recipients. J Clin Med. (2025) 14:618. doi: 10.3390/jcm14020618
15. Vidal, E, Torre-Cisneros, J, Blanes, M, Montejo, M, Cervera, C, Aguado, JM, et al. Bacterial urinary tract infection after solid organ transplantation in the RESITRA cohort. Transpl Infect Dis. (2012) 14:595–603. doi: 10.1111/j.1399-3062.2012.00744.x
16. Olenski, S, Scuderi, C, Choo, A, et al. Urinary tract infections in renal transplant recipients at a quaternary care Centre in Australia. BMC Nephrol. (2019) 20:479. doi: 10.1186/s12882-019-1666-6
17. Sabé, N, Maristany, M, Tuells, M, Favà, A, Melilli, E, Tubau, F, et al. Risk factors and outcomes of acute graft pyelonephritis with bacteremia due to multidrug-resistant gram-negative Bacilli among kidney transplant recipients. J Clin Med. (2022) 11:3165. doi: 10.3390/jcm11113165
18. Coussement, J, Kamar, N, Matignon, M, Weekers, L, Scemla, A, Giral, M, et al. Antibiotics versus no therapy in kidney transplant recipients with asymptomatic bacteriuria (BiRT): a pragmatic, multicentre, randomized, controlled trial. Clin Microbiol Infect. (2021) 27:398–405. doi: 10.1016/j.cmi.2020.09.005
19. Naik, AS, Dharnidharka, VR, Schnitzler, MA, Brennan, DC, Segev, DL, Axelrod, D, et al. Clinical and economic consequences of first-year urinary tract infections, sepsis, and pneumonia in contemporary kidney transplantation practice. Transpl Int. (2016) 29:241–52. doi: 10.1111/tri.12711
20. Ariza-Heredia, EJ, Beam, EN, Lesnick, TG, Cosio, FG, Kremers, WK, and Razonable, RR. Impact of urinary tract infection on allograft function after kidney transplantation. Clin Transpl. (2014) 28:683–90. doi: 10.1111/ctr.12366
21. Gangula, RS, Eshwarappa, M, Rajashekar, R, Reddy, H, Prabhu, PP, Siddaiah, GM, et al. Effect of urinary tract infection on the outcome of the allograft in patients with kidney transplantation. J Bras Nefrol. (2024) 46:e20240002. doi: 10.1590/2175-8239-JBN-2024-0002en
22. Papasotiriou, M, Savvidaki, E, Kalliakmani, P, Papachristou, E, Marangos, M, Fokaefs, E, et al. Predisposing factors to the development of urinary tract infections in renal transplant recipients and the impact on the long-term graft function. Ren Fail. (2011) 33:405–10. doi: 10.3109/0886022X.2011.568137
23. Camargo, LF, Esteves, AB, Ulisses, LR, Rivelli, GG, and Mazzali, M. Urinary tract infection in renal transplant recipients: incidence, risk factors, and impact on graft function. Transplant Proc. (2014) 46:1757–9. doi: 10.1016/j.transproceed.2014.05.006
24. Ooms, L, IJ, J, Voor In 't Holt, A, Betjes, M, Vos, M, and Terkivatan, T. Urinary tract infections after kidney transplantation: a risk factor analysis of 417 patients. Ann Transplant. (2017) 22:402–8. doi: 10.12659/aot.903249
25. Arabi, Z, Al Thiab, K, Altheaby, A, Aboalsamh, G, Kashkoush, S, Almarastani, M, et al. Urinary tract infections in the first 6 months after renal transplantation. Int J Nephrol. (2021) 2021:1–8. doi: 10.1155/2021/3033276
26. Auglienė, R, Dalinkevičienė, E, Kuzminskis, V, Jievaltas, M, Peleckaitė, L, Gryguc, A, et al. Factors influencing renal graft survival: 7-year experience of a single center. Medicina (Kaunas). (2017) 53:224–32. doi: 10.1016/j.medici.2017.07.003
27. Królicki, T, Bardowska, K, Kudla, T, Królicka, A, Letachowicz, K, Mazanowska, O, et al. Acute kidney injury secondary to urinary tract infection in kidney transplant recipients. Sci Rep. (2022) 12:10858. doi: 10.1038/s41598-022-15035-7
28. Hamilton, AD, and Praetorius, HA. Reduced graft survival in renal transplant patients with urinary tract infections - a meta-analysis. Dan Med J. (2024) 71:A06230424. doi: 10.61409/A06230424
29. Brune, JE, Dickenmann, M, Wehmeier, C, Sidler, D, Walti, L, Golshayan, D, et al. Impact of different urinary tract infection phenotypes within the first year post-transplant on renal allograft outcomes. Am J Transplant. (2022) 22:1823–33. doi: 10.1111/ajt.17026
30. Shendi, AM, Wallis, G, Painter, H, Harber, M, and Collier, S. Epidemiology and impact of bloodstream infections among kidney transplant recipients: a retrospective single-center experience. Transpl Infect Dis. (2018) 20. doi: 10.1111/tid.12815
31. Moein, M, Garn, RM, Settineri, J, and Saidi, R. Urinary tract infection 1 year after kidney transplant: effect on kidney transplant outcomes. Exp Clin Transplant. (2023) 21:556–61. doi: 10.6002/ect.2023.0057
32. Bahrami, A, Shams, SF, Eidgahi, ES, Lotfi, Z, Sheikhi, M, and Shakeri, S. Epidemiology of infectious complications in renal allograft recipients in the first year after transplant. Exp Clin Transplant. (2017) 15:631–5. doi: 10.6002/ect.2016.0068
33. Ye, Q, Wu, L, Zhu, B, Zhang, G, Yang, B, Jin, P, et al. Risk factors for urinary tract infection in kidney transplantation from brain death donor and its role in graft function. Zhong Nan Da Xue Xue Bao Yi Xue Ban. (2021) 46:1220–6. doi: 10.11817/j.issn.1672-7347.2021.200666
34. Khedr, L, Teama, N, and El Sharkawy, M. Infections in the first year of living related kidney transplantation in a young transplant cohort. BMC Nephrol. (2023) 24:328. doi: 10.1186/s12882-023-03379-9
35. Ozawa, K, Takai, M, Taniguchi, T, Kawase, M, Takeuchi, S, Kawase, K, et al. Diabetes mellitus as a predictive factor for urinary tract infection for patients treated with kidney transplantation. Medicina (Kaunas). (2022) 58:1488. doi: 10.3390/medicina58101488
36. Arabi, Z, Al Thiab, K, Altheaby, A, Tawhari, M, Aboalsamh, G, Almarastani, M, et al. The impact of timing of stent removal on the incidence of UTI, recurrence, symptomatology, resistance, and hospitalization in renal transplant recipients. J Transp Secur. (2021) 2021:1–8. doi: 10.1155/2021/3428260
37. Mosqueda, AO, Hernández, EEL, Morales, GC, Navarro, LJM, Bonilla, JPH, Moreno, EO, et al. Association between the placement of a double-J catheter and the risk of urinary tract infection in renal transplantation recipients: a retrospective cohort study of 1038 patients. Transplant Proc. (2021) 53:1927–32. doi: 10.1016/j.transproceed.2021.05.002
38. Yahav, D, Green, H, Eliakim-Raz, N, Mor, E, and Husain, S. Early double J stent removal in renal transplant patients to prevent urinary tract infection - systematic review and meta-analysis of randomized controlled trials. Eur J Clin Microbiol Infect Dis. (2018) 37:773–8. doi: 10.1007/s10096-017-3173-7
39. Thompson, ER, Hosgood, SA, Nicholson, ML, and Wilson, CH. Early versus late ureteric stent removal after kidney transplantation. Cochrane Database Syst Rev. (2018) 1:CD011455. doi: 10.1002/14651858.CD011455.pub2
40. Krzos, PM, Nguyen, CT, Kane, B, Krishnamoorthy, S, Kristof, TW, Reynolds, LF, et al. Evaluation of a ureteral stent removal protocol in adult kidney transplant recipients. Open Forum Infect Dis. (2024) 11:ofae510. doi: 10.1093/ofid/ofae510
41. Cai, JF, Wang, W, Hao, W, Sun, ZJ, Su, LL, Li, X, et al. Meta-analysis of early versus late ureteric stent removal after kidney transplantation. Transplant Proc. (2018) 50:3411–5. doi: 10.1016/j.transproceed.2018.08.033
42. Bezherano, I, and Kayler, LK. Timing of urinary catheter removal following kidney transplantation: a retrospective study. Kidney Med. (2022) 4:100484. doi: 10.1016/j.xkme.2022.100484
43. Akbari, R, Rahmani Firouzi, S, and Akbarzadeh-Pasha, A. Old habits die hard; does early urinary catheter removal affect kidney size, bacteriuria and UTI after renal transplantation? J Renal Inj Prev. (2017) 6:43–8. doi: 10.15171/jrip.2017.08
44. Hafeez, MS, Haq, MU, Bakhthiyar, SS, Azhar, K, Awan, AAY, Ramana Murthy, BV, et al. Outcomes after anti-thymocyte globulin vs basiliximab induction before deceased donor kidney transplants. Transpl Immunol. (2022) 75:101733. doi: 10.1016/j.trim.2022.101733
45. Huang, HF, Zhou, JY, Xie, WQ, Wu, JY, Deng, H, and Chen, JH. Basiliximab versus rabbit antithymocyte globulin as induction therapy for living-related renal transplantation: a single-center experience. Int Urol Nephrol. (2016) 48:1363–70. doi: 10.1007/s11255-016-1307-y
46. Kim, SJ, Rhu, J, Yoo, H, Kim, K, Lee, KW, and Park, JB. Outcome comparison between low-dose rabbit anti-thymocyte globulin and basiliximab in low-risk living donor kidney transplantation. J Clin Med. (2020) 9:1320. doi: 10.3390/jcm9051320
47. Pham, C, Kuten, SA, Knight, RJ, Nguyen, DT, Graviss, EA, and Gaber, AO. Assessment of infectious complications in elderly kidney transplant recipients receiving induction with anti-thymocyte globulin vs basiliximab. Transpl Infect Dis. (2020) 22:e13257. doi: 10.1111/tid.13257
48. Andrade-Sierra, J, Heredia-Pimentel, A, Rojas-Campos, E, Ramírez Flores, D, Cerrillos-Gutierrez, JI, Miranda-Díaz, AG, et al. Cytomegalovirus in renal transplant recipients from living donors with and without valganciclovir prophylaxis and with immunosuppression based on anti-thymocyte globulin or basiliximab. Int J Infect Dis. (2021) 107:18–24. doi: 10.1016/j.ijid.2021.04.032
49. Filiponi, TC, Requião-Moura, L, Tonato, EJ, Carvalho, A, e, A, and de, M. Hospital admission following acute kidney injury in kidney transplant recipients is associated with a negative impact on graft function after 1-year. PLoS One. (2015) 10:e0138944. doi: 10.1371/journal.pone.0138944
50. Fiorentino, M, Bagagli, F, Deleonardis, A, Stasi, A, Franzin, R, Conserva, F, et al. Acute kidney injury in kidney transplant patients in intensive care unit: from pathogenesis to clinical management. Biomedicines. (2023) 11:1474. doi: 10.3390/biomedicines11051474
51. Rice, JC, Peng, T, Kuo, YF, Pendyala, S, Simmons, L, Boughton, J, et al. Renal allograft injury is associated with urinary tract infection caused by Escherichia coli bearing adherence factors. Am J Transplant. (2006) 6:2375–83. doi: 10.1111/j.1600-6143.2006.01471.x
52. Fiorante, S, Fernandez-Ruiz, M, Lopez-Medrano, F, Lizasoain, M, Lalueza, A, Morales, JM, et al. Acute graft pyelonephritis in renal transplant recipients: incidence, risk factors and long-term outcome. Nephrol Dial Transplant. (2011) 26:1065–73. doi: 10.1093/ndt/gfq531
53. Sánchez, MPR, Rubio, DCA, Luna, IM, Padilla, PKG, Villamizar, KMC, González, CAG, et al. Impact of complicated urinary tract infection on renal graft function. Transplant Proc. (2020) 52:1173–7. doi: 10.1016/j.transproceed.2020.01.066
54. Fiorante, S, Lopez-Medrano, F, Lizasoain, M, Lalueza, A, Juan, RS, Andrés, A, et al. Systematic screening and treatment of asymptomatic bacteriuria in renal transplant recipients. Kidney Int. (2010) 78:774–81. doi: 10.1038/ki.2010.286
55. Gobierno de México. Available online at: https://www.gob.mx/cenatra/documentos/estadisticas-50060 (Accessed July 03, 2025).
Glossary
UTI - Urinary tract infections
KTR - Kidney transplant recipients
CMV - Cytomegalovirus
CKD - Chronic kidney disease
E-coli - Escherichia coli
MDR - Multi-drug resistance
AB - Asymptomatic bacteriuria
CFU - Colony-forming units
ESBL-PE - Extended-spectrum beta-lactamase producing Enterobacteriaceae
AKI - Acute kidney injury
SCr - Serum creatinine
RUTI - Recurrent urinary tract infections
BSL - Basiliximab
ATG - Thymoglobulin
MMF - Mycophenolate mofetil
TAC - Tacrolimus
CsA - Cyclosporine A
PDN - Prednisone
ESBL - Extended-spectrum beta-lactamase
AR - Acute rejection
Keywords: urinary tract infection (UTI), kidney function, acute kidney injury (AKI), immunosupresion, kidney tranplantation
Citation: Andrade Sierra J, Andrade-Martínez JC, Fuentes-López EA, Rojas-Campos E, Martínez-Mejía V, González-Espinoza E, Cardona-Muñoz EG, Cardona-Muñoz JI, Evangelista-Carrillo LA, Medina-Pérez M, Cruz-Landino M, Banda-Lopez A, Miranda-Díaz AG, Gutiérrez Aceves JA, Andrade-Ortega J, Arellano Arteaga KJ, Andrade-Ortega AJ, Aguilar Fletes LE, González-Correa G, Preciado P, Verdugo-Correa JE, Pazarín-Villaseñor HL, Corona-Nakamura AL and Carvallo-Venegas M (2025) A five-year retrospective study focused on urinary tract infections in kidney transplant recipients in the current era of immunosuppression. Front. Med. 12:1606224. doi: 10.3389/fmed.2025.1606224
Edited by:
Benedetta Chiodini, Queen Fabiola Children’s University Hospital, BelgiumReviewed by:
Gaurav Gupta, Virginia Commonwealth University, United StatesTomasz Porazko, Opole University, Poland
Copyright © 2025 Andrade-Sierra, Andrade-Martínez, Fuentes-López, Rojas-Campos, Martínez-Mejía, González-Espinoza, Cardona-Muñoz, Cerrillos-Gutiérrez, Evangelista-Carrillo, Medina-Pérez, Cruz-Landino, Banda-López, Miranda-Díaz, Gutiérrez Aceves, Andrade-Ortega, Arellano-Arteaga, Andrade-Ortega, Aguilar Fletes, González-Correa, Preciado, Verdugo-Correa, Pazarín-Villaseñor, Corona-Nakamura and Carvallo-Venegas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jorge Andrade-Sierra, am9yZ19hbmRyYWRlQGhvdG1haWwuY29t