 Francisco Illanes-Álvarez1,2,3†
Francisco Illanes-Álvarez1,2,3† Denisse Márquez-Ruiz1,2,3†
Denisse Márquez-Ruiz1,2,3† Sara Cuesta-Sancho1,2,4
Sara Cuesta-Sancho1,2,4 Irene Campaña-Gómez1,2
Irene Campaña-Gómez1,2 Andrés Martín-Aspas1,2Ismael Tinoco-Racero1,2,3‡
Andrés Martín-Aspas1,2Ismael Tinoco-Racero1,2,3‡ Mercedes Márquez-Coello2,3‡
Mercedes Márquez-Coello2,3‡ José-Antonio Girón-González1,2,3*‡
José-Antonio Girón-González1,2,3*‡- 1Servicio de Medicina Interna, Hospital Universitario Puerta del Mar, Cádiz, Spain
- 2Instituto para la Investigación e Innovación Biomédica de Cádiz (INIBiCA), Cádiz, Spain
- 3Facultad de Medicina, Universidad de Cádiz, Cádiz, Spain
- 4Mucosal Immunology Lab, Institute of Biomedicine and Molecular Genetics (IBGM, University of Valladolid-CSIC), Valladolid, Spain
Background: An increased prevalence of atherosclerosis has been observed in people living with HIV (PLWH). This study aimed to analyze levels of inflammatory, immune, endothelial, platelet, and coagulation parameters, as well as their relationship with subclinical atherosclerosis.
Methods: A total of 120 PLWH with chronic infection and undetectable HIV load, along with 30 age- and sex-matched controls (HIV-uninfected individuals), were selected. Serum levels of proinflammatory molecules, including interleukin 6 (IL-6), soluble CD163, and high-sensitivity C-reactive protein, were measured. Additionally, neutrophil extracellular traps (NET)-derived parameters (anti-nucleosome antibody titers and myeloperoxidase concentrations), activated T lymphocytes, endothelial (E-selectin, vascular cell adhesion molecule 1), platelet (P-selectin, Platelet factor 4) and coagulation (D-dimer) markers were assessed. Cardiovascular risk factors were evaluated using the REGICOR and ASCVD risk estimators. In a subset of 61 individuals (18 controls and 43 PLWH), subclinical atherosclerosis was assessed by carotid Doppler ultrasound.
Results: Levels of IL-6, sCD163, anti-nucleosome antibodies, and activated T lymphocytes were elevated in PLWH compared to controls. Likewise, serum levels of platelet factor 4 and D-dimer were higher in PLWH. Those PLWH with carotid atherosclerotic lesions exhibited higher REGICOR and ASCVD scores, as well as elevated IL-6 concentrations, compared to those PLWH without carotid atherosclerotic lesions. Multivariable analysis identified the REGICOR score and IL-6 serum levels as independent factors associated with atherosclerosis.
Conclusion: People living with HIV with long-term viral load control exhibit increased levels of inflammatory, immune, platelet and coagulation markers. Subclinical atherosclerosis in this population is independently influenced by both classic cardiovascular risk factors and inflammatory activation.
Introduction
An increased prevalence of cardiovascular diseases has been observed in people living with HIV (PLWH) compared to the general population, even in the era of effective antiretroviral therapy (ART) (1). As life expectancy in PLWH continues to rise due to sustained viral suppression and immune recovery, non-AIDS comorbidities, particularly cardiovascular diseases, have become a major cause of morbidity and mortality in this population. A better understanding of the mechanisms underlying vascular alterations in PLWH is critical, as this could expand therapeutic possibilities for these patients.
Multiple pathophysiological processes have been proposed to explain the increased cardiovascular risk in PLWH. Among them, endothelial dysfunction, platelet activation, and alterations in coagulation/fibrinolysis have been proposed as mechanisms contributing to this elevated risk (2). In this context, biomarkers such as high-sensitivity C-reactive protein (hsCRP), interleukin-6 (IL-6), and D-dimer have been widely used in large cohort studies and consistently associated with increased cardiovascular risk and mortality in PLWH (3). However, the behavior of these biomarkers in the specific setting of long-term viral suppression and immune restoration remains incompletely understood (4). In fact, findings from various studies have been inconsistent, potentially reflecting heterogeneity in study populations, including differences in ART (antiretroviral therapy) status, levels of viral replication, and degrees of immunosuppression (2, 5, 6). Furthermore, the potential interplay between these established inflammatory markers and emerging contributors —such as neutrophil extracellular traps (NETs)— has not yet been systematically explored.
Chronic immune activation and persistent systemic inflammation are additional mechanisms that may significantly contribute to the elevated prevalence and pathogenesis of cardiovascular disease in PLWH. This persistent immune activation is observed in PLWH even when viral loads are undetectable and current CD4+ T-cell counts are high (1). Elevated levels of inflammatory and immune activation markers have also been associated with increased mortality in this population (7).
Most research has focused on T lymphocytes and macrophages (8), while the role of polymorphonuclear neutrophils (PMNs) and their contribution through processes such as NETosis (formation of NETs, Neutrophil Extracellular Traps) (9, 10) has been underexplored. NETs are structures composed of DNA and proteins that can trap pathogens, but they have also been implicated in sterile inflammation and tissue damage. Notably, NETs have been associated with atherosclerotic plaque formation in the general population (11–13), and elevated NETs levels have been reported in PLWH (14), suggesting that neutrophil activation and NET formation may contribute to HIV-associated vascular disease and warrant further investigation.
In this context, this study had a twofold objective: first, to evaluate the possible presence of inflammatory –including that related to PMNs–, immune, endothelial, platelet, and coagulation activation in a homogenous cohort of PLWH with prolonged viral suppression and elevated CD4+ T cell/mm3 counts; second, to explore the association of these biological processes —alongside classical vascular risk factors (smoking, diabetes mellitus, arterial hypertension, hypercholesterolemia)— with subclinical atherosclerosis. By integrating these perspectives, we aim to advance a more comprehensive framework for understanding the multifactorial contributors to atherosclerosis in virologically suppressed PLWH, which could enhance cardiovascular risk stratification and guide targeted therapeutic interventions.
Materials and methods
Study design
This prospective observational study was conducted at the HIV outpatient clinics of Puerta del Mar University Hospital (Cádiz, Spain) between 2018 and 2023. We enrolled consecutive people living with HIV (PLWH) who attended routine follow-up visits during this period.
Eligible PLWH were adults (≥ 18 years) with chronic HIV infection who had maintained an undetectable plasma HIV viral load (< 50 copies/mL) for at least 12 months prior to inclusion, on stable antiretroviral therapy (ART). Patients with any active opportunistic infection, concomitant neoplasm, or other inflammatory conditions were excluded. Additional exclusion criteria included active substance abuse (cocaine, heroin, amphetamines), significant alcohol consumption (> 50 g/day), recent blood transfusions (within 30 days), or use of anti-inflammatory or immunosuppressive medications that could affect inflammatory markers.
The screening procedures for PLWH followed established national protocols (15).
A total of 120 PLWH meeting these criteria were included. Their ART regimens consisted of tenofovir alafenamide plus emtricitabine (64 patients, 53%) or abacavir plus lamivudine (56 patients, 47%), combined with rilpivirine (22 patients, 18%), integrase inhibitors (31 patients, 56%), or the protease inhibitor darunavir (31 patients, 26%).
The control group comprised 30 age- and sex-matched healthy individuals recruited from hospital staff and community volunteers during the same period. Controls were screened to exclude any history of HIV infection, cardiovascular disease, chronic inflammatory conditions, or use of medications affecting immune function.
All participants (PLWH and controls) were asymptomatic for cardiovascular or other target organ diseases (ischemic heart disease, cerebrovascular disease or lower extremity atherosclerosis) at inclusion.
Definitions
The duration of the HIV infection was established based on the first positive anti-HIV test. HIV replication was considered controlled when the viral load was below 50 copies/ml (Abbott RealTime HIV-1, Abbott Park, IL, United States).
Increased serum concentration of intestinal fatty acid-binding protein (I-FABP) was indicative of gut barrier disruption (16). Bacterial translocation was assessed by measuring plasma 16S ribosomal RNA (16S rRNA) levels (17).
Markers of inflammatory activation included serum concentrations of interleukin (IL)-6, soluble CD163 (sCD163) and high sensitivity C-reactive protein (hsCRP). Serum titers of anti-nucleosome IgG antibodies (AnuA-IgG) and serum levels of myeloperoxidase (MPO) were indicative of NET formation. Serum levels of DNAse I were analyzed as the main enzyme responsible for NET degradation (18). Activated CD4+ and CD8+ T lymphocytes were identified by the co-expression of HLA-DR and CD38 on their membranes. Markers of vascular activation included serum concentrations of vascular cell adhesion molecule 1 (VCAM-1) and E-selectin. Platelet activation was assessed through levels of P-selectin and chemokine (C-X-C motif) ligand 4/Platelet factor 4 (CXCL4/PF4). D-dimer concentration was used to assess coagulation/fibrinolysis.
Participants who smoked more than 10 cigarettes per day were considered smokers. Diagnostic criteria for dyslipidemia, diabetes mellitus, arterial hypertension, and cardiovascular or cerebrovascular disease followed the latest clinical guidelines from the Spanish Society of Atherosclerosis (19). Patients were categorized using two vascular risk assessment tools: the Framingham scale adapted for the Spanish population (REGICOR) (20) and the American College of Cardiology’s cardiovascular risk scale (ASCVD risk estimator) (21). The REGICOR scale includes age, sex, smoking status, diagnosis of diabetes mellitus, serum levels of total cholesterol and high-density lipoprotein cholesterol, as well as systolic and diastolic arterial pressure. The ASCVD risk estimator additionally considers race, low-density lipoprotein cholesterol, and the use of antihypertensive medications, statins or aspirin, and has been recommended for use in patients with HIV infection.
Study schedule
The study protocol included: (1) collection of clinical history, nadir CD4+ T cell count, and duration of undetectable HIV load; (2) CD4+ T cell count at study inclusion; (3) peripheral blood sampling for analysis of bacterial translocation, inflammatory and immune parameters, as well as vascular and platelet activation and coagulation/fibrinolysis markers; (4) peripheral blood sampling for measurement of cholesterol, LDL-cholesterol, HDL-cholesterol, triglyceride concentrations, total cholesterol/HDL ratio, and glycemia; (5) in a subgroup of consecutive individuals (18 controls and 43 PLWH), carotid Doppler ultrasound was performed.
A comparison of the results for activated lymphocytes and parameters of inflammatory, vascular, and platelet activation, as well as ultrasound-Doppler findings, was conducted between controls and PLWH.
16S rDNA levels analysis
16S rDNA was extracted using the QIAamp DNA Blood Mini Kit (QIAgen, Hilden, Germany) with modifications to the manufacturer’s protocol. Briefly, plasma was obtained by centrifuging blood samples collected in ethylenediaminetetraacetic acid (EDTA) tubes at 2,500 g for 15 min at room temperature. The plasma was then frozen at −80°C until use. For extraction, 1 ml plasma was mixed with 15 μl of proteinase K and 1 ml of buffer AL, followed by a 30 min incubation at 56°C. Subsequently, 1 ml of 100% ethanol was added, and the mixture was incubated at room temperature for 10 min. The content was then processed through a spin column in multiple centrifugation steps. Washing steps were performed using 1 ml of buffer AW1 and 1 ml of buffer AW2, with elution carried out using 25 μl of buffer AE. The eluate underwent a 5 min incubation at 56°C, followed by centrifugation at 10,000 rpm for 30 s, re-collection, and a final centrifugation at 10,000 rpm for 1 min.
The 16S rDNA region of Escherichia coli was amplified in a CFX Connect Real-Time PCR System (CFX Connect Real-Time PCR System, Bio-Rad Laboratories, Inc. CA, United States) using the following primers: 16S F 5′-AGA-GTT-TGA-TCA-TGG-CTC-AG-3′ and 16S R 5′-ACC-GCC-ACT-GCT-GCT-GGC-AC-3′ (IDT, Coralville, Iowa, United States) (22). A standard curve was generated from an E. coli colony, provided by the Microbiology Department of Puerta del Mar University Hospital. After heat shock (90°C for 10 min and 10°C for 10 min) and centrifugation, the supernatant was collected and the concentration was measured with a Qubit fluorimeter and the Qubit™ dsDNA HS Assay Kit (Invitrogen, Thermo Scientific, Waltham, MA, Uinited States). Samples were run in duplicates, and their concentrations were determined using the standard curve generated from serial dilutions of the colony. All procedures were performed in a biological safety horizontal flow hood.
Microbial translocation markers, proinflammatory molecules, DNAse I, vascular- and platelet-related parameters, and D-dimer concentration
Serum was obtained by centrifuging blood samples collected in pyrogen-free heparinized tubes (Biofreeze, Costar, United States) at 2,500 g for 15 min at room temperature, with centrifugation performed immediately after blood extraction, in order to minimize potential changes in cytokine concentrations. The serum was then frozen at −80°C until its use.
Quantikine Human Immunoassays (R&D, Minneapolis, MN, United States) were used to quantify serum concentrations of I-FABP, IL-6, sCD163, hsCRP, MPO, VCAM-1, E-selectin, P-selectin, and PF4, following the indications of the manufacturer. Serum concentrations of anti-nucleosome IgG antibodies were measured using the Human anti-nucleosome antibody IgG (AnuA-IgG) ELISA Kit (MyBioSource, San Diego, CA, United States). DNAse I concentrations were determined with the Human DNase-I (deoxyribonuclease I) ELISA Kit (Biomatik, Wilmington, DE, United States). Plasma D-dimer concentration was analyzed by immunoassay using the D-Dimer HS 500 kit (Instrumentation Laboratory, Bedford, MA, United States). The samples were run in duplicate.
T-Cell immune phenotypes
Fresh blood samples collected in pyrogen-free heparinized tubes with EDTA (Biofreeze, Costar, United States) were used for flow cytometry. Stained cells were acquired on a BD FACSCanto™ II flow cytometer using BD FACSDiva™ Software (BD Biosciences, San Jose, CA, United States), and the resulting data were subsequently analyzed with FlowJo™ Software (BD Biosciences, San Jose, CA, United States). Activated CD4+ and CD8+ T lymphocytes (HLA-DR+CD38+) were identified using a multi-step gating strategy. Initially, viable cells were identified using the FVS510 viability marker (BD Biosciences, San Jose, CA, United States). From this population, lymphocytes were selected based on their characteristic forward (FSC-A) and side (SSC-A) scatter. Then, the CD3+ population was selected (clone SK7, BD Biosciences, San Jose, CA, United States), and it was further divided into CD4+ (clone SK3, BD Biosciences, San Jose, CA, United States) and CD8+ (clone SK1, BD Biosciences, San Jose, CA, United States) populations. Finally, activated T cells were defined within each CD4+ and CD8+ subset by the co-expression of activation markers CD38+ (clone HB-7, BD Biosciences, San Jose, CA, United States) and HLA-DR+ (clone L243, BD Biosciences, San Jose, CA, United States) (Supplementary Figure 1). In each case, 300,000 cells were acquired. Fluorescence minus one (FMO) controls were used to confirm staining specificity and distinguish the sample from background.
Evaluation of the carotid artery
Patients and controls underwent ultrasound measurements of carotid intima-media thickness (CIMT) using a Toshiba F31 device, equipped with a linear probe UST-5413 (4–11 MHz). Individuals were examined in the supine position, with their head turned 45° away from the side being studied. Three carotid segments were studied: the common carotid artery (1 cm proximal to bifurcation), the carotid bulb, and the internal carotid artery (1 cm distal to bifurcation). Using computer software with automatic edge detection integrated in the device, the maximum and mean values of the CIMT were measured for each segment, considering the average intimate-media thickness across all zones. The atheromatous plaque was defined as: (a) Focal thickening of the wall at least 50% higher than the surrounding wall. (b) Focal thickening of the wall that penetrates 0.5 mm in the lumen. (c) Localized area with a CIMT of more than 1.5 mm that penetrates the lumen and that is identified differentiated from the surrounding area. Carotid lesion was defined as a CIMT value exceeding 0.9 mm and/or the presence of plaques (23). The cut-off point set in the present study (0.9 mm) follows the consensus of the American Society of Echocardiography, which suggests that CIMT values at or above the 75th percentile of a reference population indicate increased cardiovascular risk (24); this value was 0.88 mm in a sample of the Spanish reference population (25).
Statistics
Data were expressed as absolute numbers (percentage) or as median values [25–75 interquartile range (IQR)]. Categorical variables were compared using the chi-square test or Fisher’s exact test. The Mann-Whitney U test was used to compare quantitative variables from two independent groups. For comparison of three or more independent groups, Kruskal-Wallis test was used. Spearman rank correlation tests were performed to evaluate associations between two variables. A two-tailed p-value of < 0.05 was considered to be significant.
Multivariable analysis of factors associated with the presence of carotid lesion was performed using binary logistic regression. A stepwise backward elimination approach was applied, starting with all candidate variables and sequentially removing those with the least statistical significance. The independent variables included were age, sex, duration of undetectable HIV load, and those selected from bivariate regression analysis using a cutoff p-value of < 0̃.1.
SPSS 22.0 statistical software package (SPSS Inc., Chicago, IL, United States) was used to perform these analyses.
Results
The demographic and immune characteristics, as well as the cardiovascular indexes of PLWH and controls, are shown in Table 1.
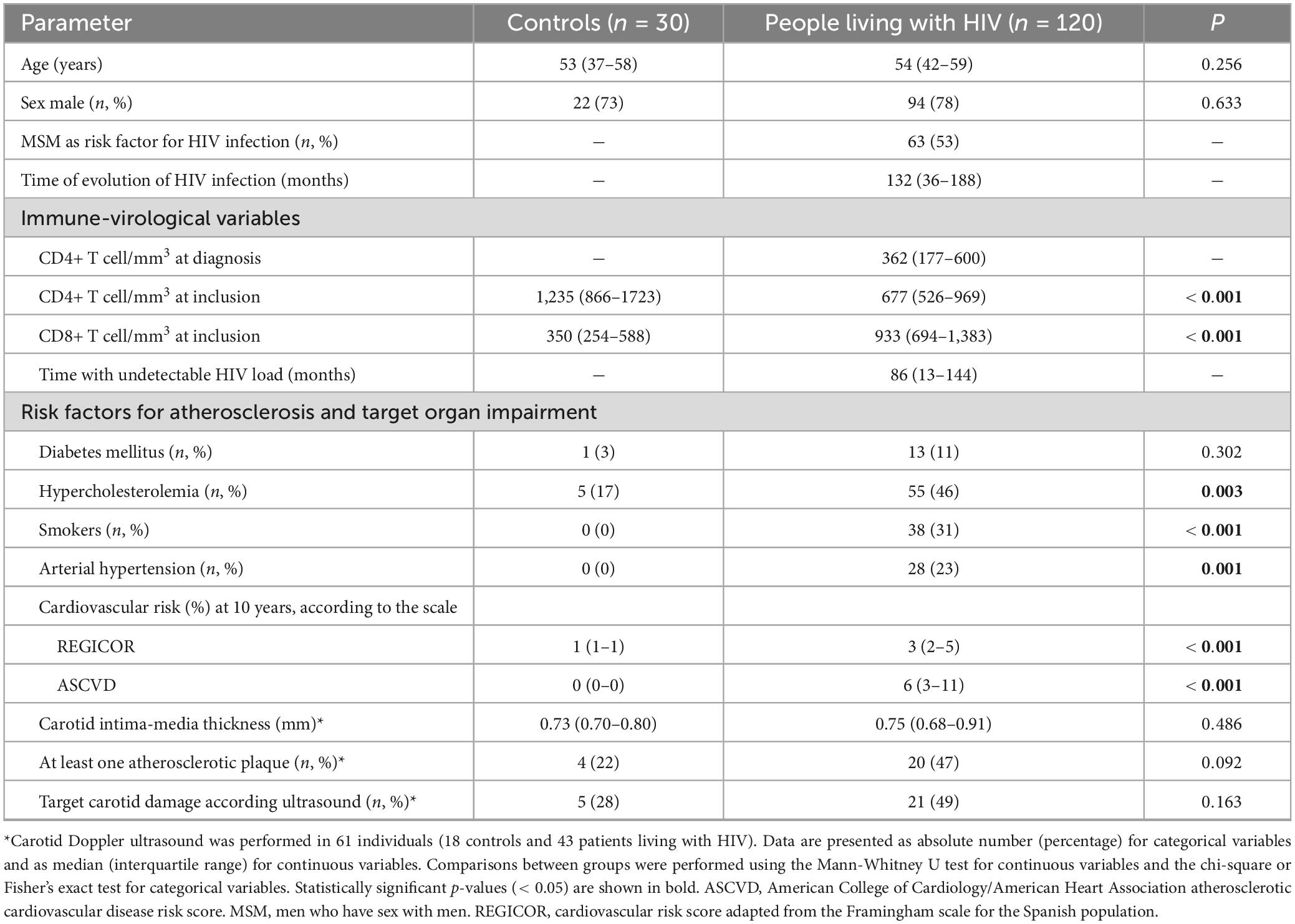
Table 1. Demographic, clinical, immunological, and cardiovascular risk characteristics of controls and people living with HIV.
Intestinal barrier permeability and bacterial translocation
Intestinal permeability (measured by serum I-FABP concentration) and bacterial translocation (measured by 16S rDNA values) were significantly higher in PLWH compared to controls (Table 2).
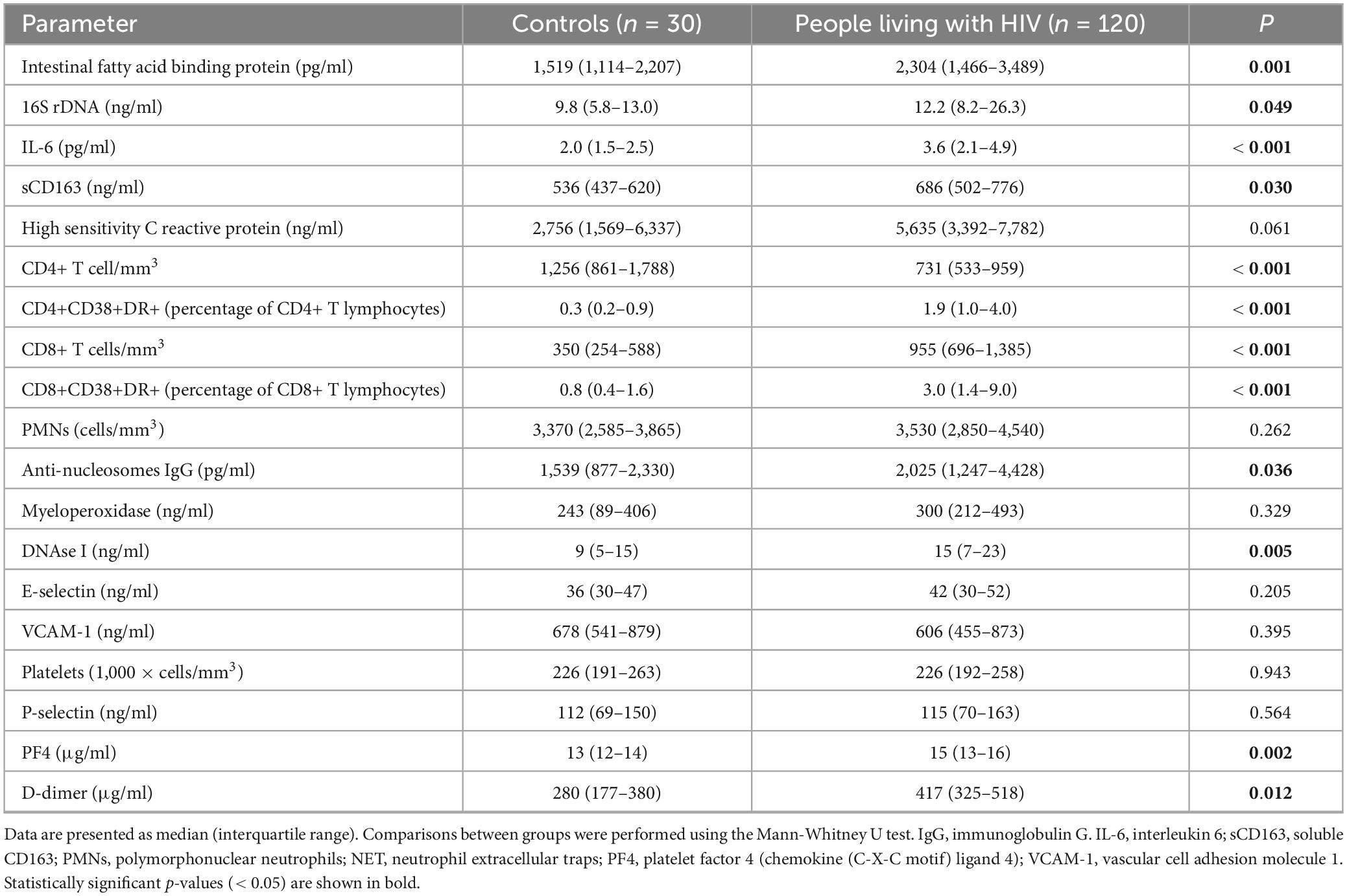
Table 2. Gut barrier integrity, bacterial translocation, and inflammatory, immune, vascular, platelet, and coagulation parameters in controls and chronically treated people living with HIV.
Inflammatory and immune activation parameters
Serum concentrations of inflammatory activation markers (IL-6, sCD163 and AnuA-IgG) were elevated in PLWH, with hsCRP levels also approaching statistical significance. The concentrations of DNAse I were likewise higher in this group, while serum MPO levels were similar between PLWH and controls (Table 2). Furthermore, the proportion of activated CD4+ and CD8+ T cells was significantly higher in PLWH (Table 2).
A significant negative correlation was detected between the duration of undetectable HIV viral load and AnuA-IgG titers (r = −0.327, p < 0.001) (Figure 1). When only individuals with more than 18 months of undetectable viral load were analyzed, the negative correlation between duration of viral suppression and AnuA-IgG titers remained significant (r = −0.267, p = 0.021). Likewise, the correlation between time with undetectable viral load and anti-nucleosomes IgG concentration persisted when the sample was stratified based on whether the age of PLWH was younger (r = −0.301, p = 0.024) or older (r = −0.285, p = 0.042) than their median age (54 years). These findings highlight the robustness of the association between reduced AnuA-IgG titers and prolonged viral suppression.
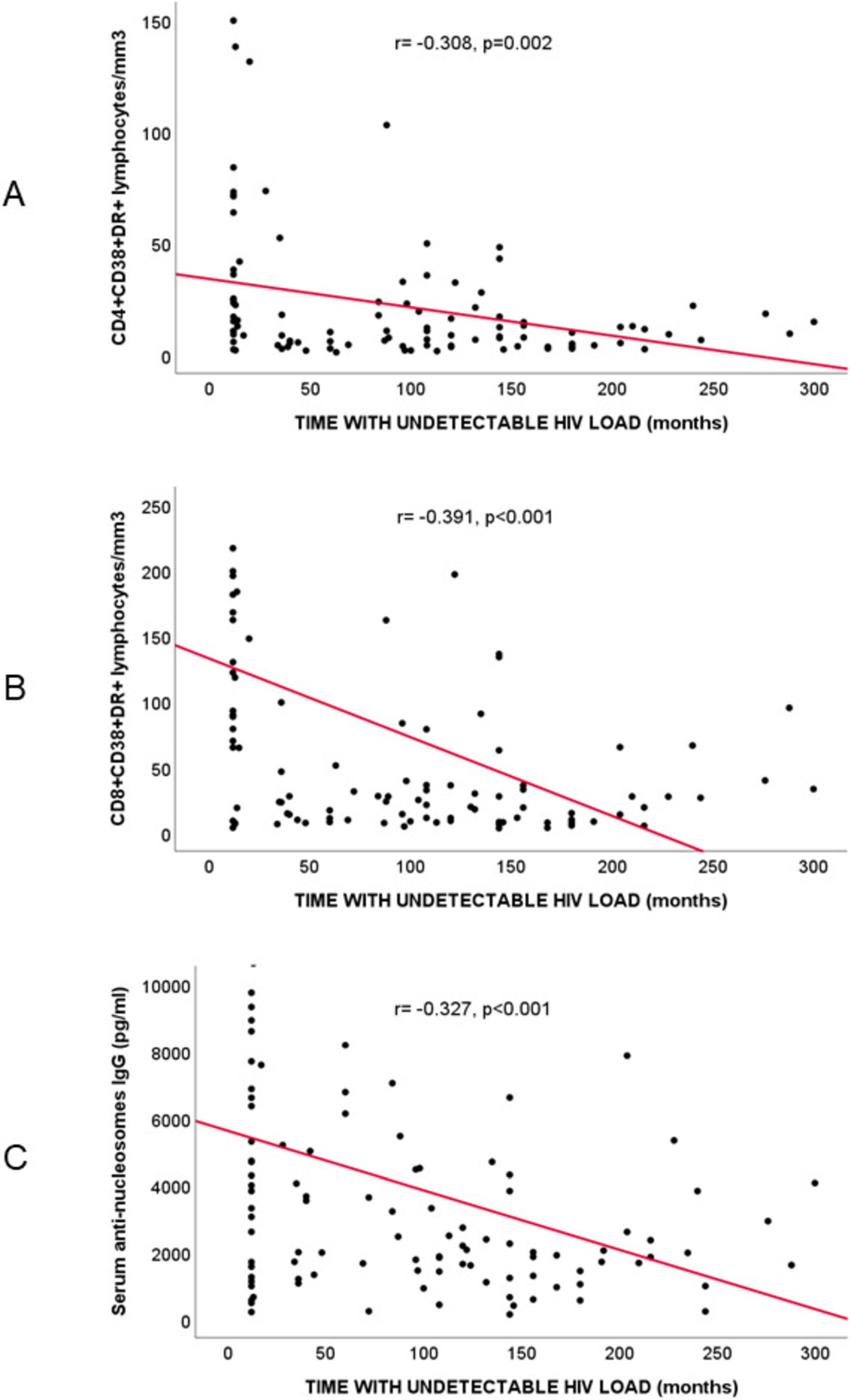
Figure 1. Spearman’s correlation analysis in people living with HIV (n = 120) between time with undetectable HIV viral load (months) and: (A) activated CD4+ T lymphocytes (CD4+CD38+DR+T lymphocytes/mm3; r = –0.308, p = 0.002); (B) activated CD8+ T lymphocytes (CD8+CD38+DR+T lymphocytes/mm3; r = –0.391, p < 0.001); (C) serum anti-nucleosome IgG titers (pg/ml; r = –0.327, p < 0.001).
Vascular and platelet activation markers and D-dimer levels
No significant differences were observed in serum E-selectin or VCAM-1 concentrations between PWLH and controls. Likewise, serum concentration of P-selectin was similar in both groups; however, a significant increase of PF4 was detected in PLWH. D-dimer concentration was also significantly higher in PLWH compared to controls (Table 2).
Atherosclerosis-related measures. Relationship with other inflammatory parameters
The 10 years cardiovascular risk, calculated using both the REGICOR and the ASCVD scales prior to carotid Doppler ultrasound, was significantly higher in PLWH.
People living with HIV who underwent carotid Doppler ultrasound were divided into two groups based on the presence (n = 21) or absence (n = 22) of carotid lesions. The 10 years cardiovascular risk was significantly higher in those with carotid lesions than in those without. Furthermore, PLWH with carotid atherosclerotic lesions exhibited significantly higher IL-6 concentrations and PMN/mm3 counts compared to those without such lesions (Table 3).
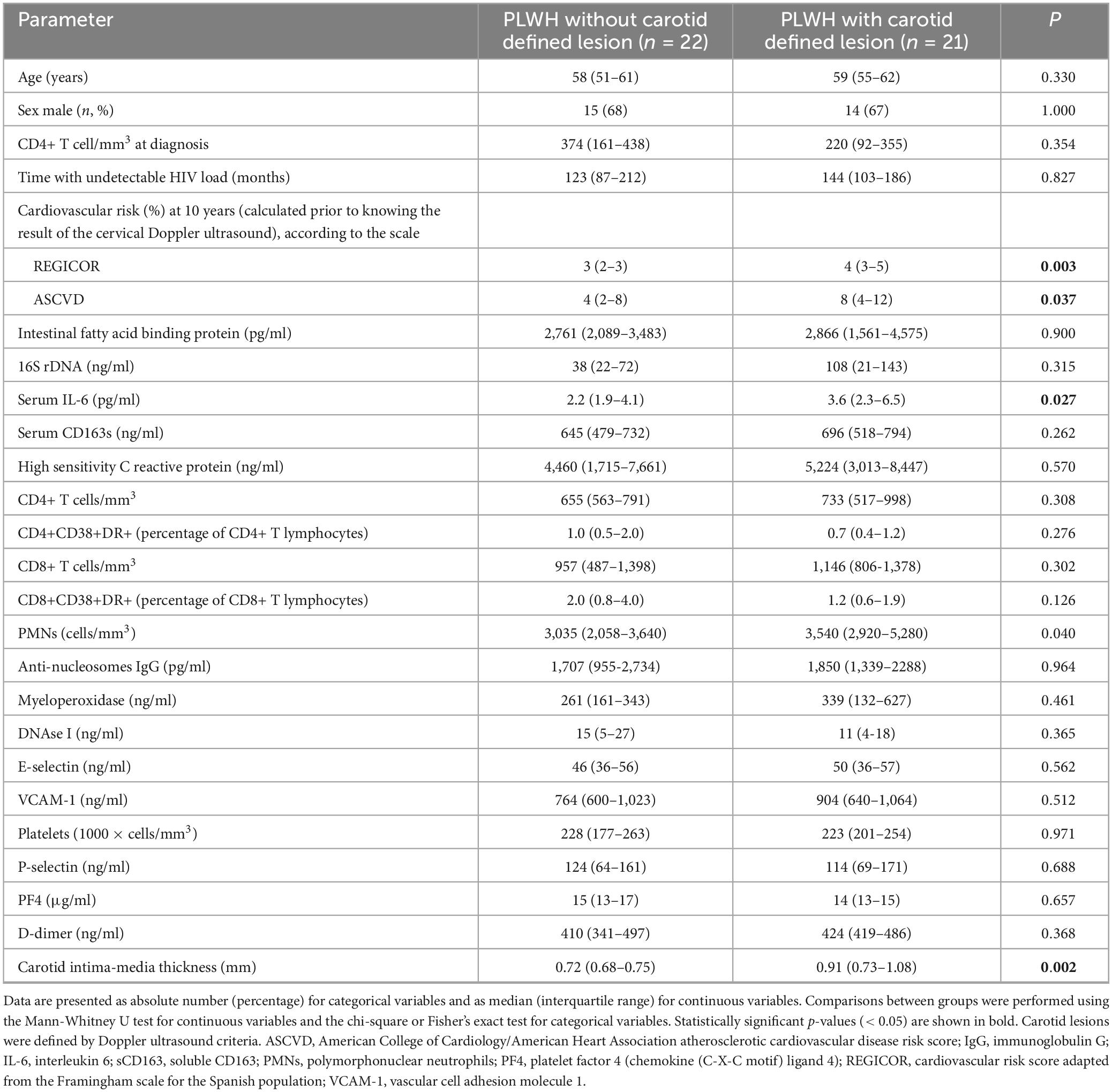
Table 3. Gut barrier integrity, bacterial translocation and inflammatory, immune, vascular, and platelet parameters in chronically treated people living with HIV, grouped by the presence or absence of carotid lesions.
Binary logistic regression analysis identified the REGICOR index and serum IL-6 concentration as independent parameters associated with the presence of carotid lesions (Table 4).
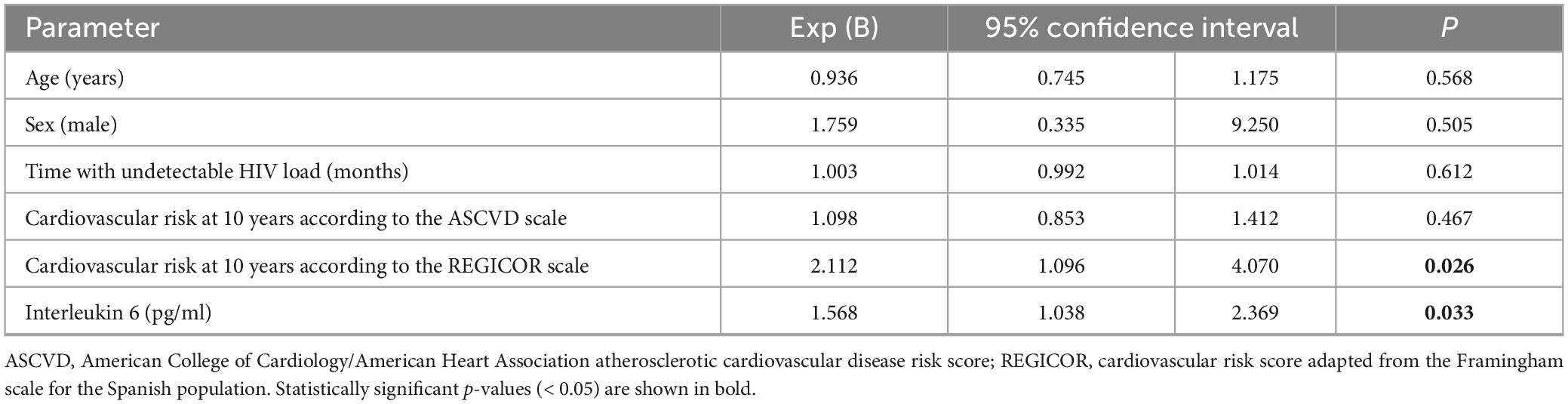
Table 4. Parameters independently associated with subclinical carotid atherosclerosis in people living with HIV (PLWH) (binary logistic regression).
Discussion
Previous studies have shown that PLWH have a higher prevalence of atherosclerosis (26). To further analyze the possible pathogenic factors contributing to this increased prevalence, the present work evaluated a range of markers —specifically those related to inflammatory, immune, endothelial, platelet, and coagulation activation— and their possible influence on the accelerated development of atherosclerosis in a selected and homogeneous cohort of patients with well-controlled viral replication over an extended period. This population, characterized by high CD4+ T cell counts and a low incidence of opportunistic infections, provides an optimal model for examining non-AIDS comorbidities, with cardiovascular disease emerging as a primary concern (1).
Consistent with other authors (27), our results suggest that increased intestinal permeability and persistent bacterial antigenic stimulation are present in these individuals, even after prolonged control of HIV viral replication. Bacterial translocation contributes to chronic immune activation —a hallmark of HIV infection— and is considered a central driver of persistent inflammation and immune activation in PLWH (27, 28).
Likewise, increased lymphocyte activation and higher concentrations of IL-6 and sCD163 were observed in PLWH, supporting the hypothesis that chronic inflammation is a key mediator of HIV-associated cardiovascular risk (29). Inflammatory markers derived from PMNs have been insufficiently studied in this context. In this study, an indirect measure of NETs was used —specifically, the immune response to nucleosomes released during NETosis (AnuA-IgG titers)—, which was found to be elevated in PLWH, suggesting the presence of circulating nucleosomes derived from NETs. Serum concentrations of DNAse I were also increased in PLWH, probably as a compensatory mechanism to control the excessive NETosis detected in this group.
Previous authors had analyzed NET formation in a heterogeneous sample of PLWH, reporting elevated serum concentration of citrullinated histone H3 (H3Cit), but not cell-free DNA, as indirect measures of NET formation, regardless of HIV viral load status (14). These measurements were also conducted in our work, but the high variability of the results obtained (data not shown) led to their exclusion from the final analysis. Interestingly, serum levels of the other marker of NETs studied, MPO, was similar between PLWH and controls. This finding leads us to hypothesize that MPO, and possibly other enzymes secreted by PMNs, might be trapped within these neutrophilic networks, rendering them less detectable in serum. Together, these findings suggest that NETosis may be active in virologically suppressed PLWH and could contribute to vascular inflammation.
Furthermore, the concentration of anti-nucleosome antibodies was negatively correlated with the duration of undetectable HIV viral load, suggesting that longer periods of viral replication control are associated with reduced activation of PMNs. This correlation persisted even when the analysis was restricted to PLWH with more than 18 months of controlled viral load, supporting the potential protective effect of long-term viral suppression on inflammatory homeostasis.
While endothelial dysfunction and platelet and coagulation activation have been proposed as mechanisms contributing to cardiovascular risk in PLWH (2), our findings challenge their role in patients receiving prolonged ART. HIV infection and endothelial activation can induce the shedding of cellular adhesion molecules such as E-selectin and VCAM-1 (30, 31). Given the persistent inflammatory state observed in these individuals, it would be expected that endothelial activation would also persist. However, no evidence of ongoing endothelial activation, as measured by serum concentrations of adhesion molecules E-selectin and VCAM-1, was found in PLWH. Prospective studies have shown that after 1 year of ART, the concentration of endothelial activation molecules tends to normalize (5), which supports our findings. However, we cannot exclude the possibility of endothelial activation mediated by other markers or pathways not assessed in this work (32).
Similarly, in our work, P-selectin concentrations—an indicator of platelet-endothelial interaction—did not differ between PLWH and controls, consistent with previous reports showing decreased P-selectin levels following 12 months of ART (6). In contrast, the serum concentration of PF4, a parameter not previously analyzed in PLWH, was increased in our cohort. PF4 is the most abundant protein in platelet alpha granules (33) and serves as both a marker of platelet activation and a mediator of tissue fibrosis (32). These findings suggest that, beyond platelet dysfunction, potential tissue fibrosis (arterial or cardiac) may contribute to cardiovascular events in PLWH.
Finally, our results confirmed elevated D-dimer concentrations in PLWH, a marker that has been independently associated with mortality in individuals with controlled HIV replication (3). This finding underscores the persistent hypercoagulable state in virologically suppressed patients and highlights the need for ongoing monitoring of thrombotic risk.
Taken together, our results demonstrate that even after a prolonged period of controlled viral replication due to ART (median, 86 months), PLWH continue to exhibit alterations in intestinal permeability, persistent inflammatory and immune activation, and disturbances in platelet activation and the coagulation/fibrinolysis system. These factors may synergistically promote atherogenesis.
Previous studies have shown that HIV infection is associated with accelerated progression of carotid atherosclerosis (34). In our study, carotid ultrasound revealed that nearly half of the cohort (49%) had carotid injury, a proportion similar to that reported in a recent Spanish series (35), despite a low estimated 10 years cardiovascular risk according to the REGICOR scale (score of 3). It is important to emphasize that the selected individuals had no clinical signs of cardiovascular or cerebrovascular disease. These findings are striking and consistent with observations in the general population (36), where carotid atherosclerosis is detected in a higher percentage of individuals classified as having a low-moderate cardiovascular risk based on standard risk scales.
A comprehensive assessment was conducted to evaluate potential factors contributing to the increased incidence in PLWH. These included the previously mentioned inflammatory, vascular, platelet and coagulation factors, along with classic cardiovascular risk factors, assessed using two established risk tools: the REGICOR scale (Framingham scale adapted for the Spanish population) (37) and the ASCVD risk estimator (38). Both the REGICOR and ASCVD scores were significantly higher in PLWH with carotid lesions, highlighting the role of classic cardiovascular risk factors, which may be exacerbated by lifestyle habits (39) or ART (40), in this population. Furthermore, PLWH with carotid atherosclerosis showed greater inflammatory activation, as evidenced by elevated serum IL-6 concentrations, compared to those without arterial injury. Multivariable analysis confirmed that both cardiovascular risk factors (as reflected by the REGICOR score) and inflammatory activation (measured by IL-6 levels) were independently associated with the presence of atherosclerotic lesions in PLWH. These findings support a model in which HIV-related chronic inflammation synergizes with conventional risk factors to accelerate atherosclerosis, even in clinically stable patients.
Interleukin-6 is a proinflammatory cytokine released by multiple immune cells, including PMNs, macrophages, lymphocytes, and endothelial cells (41). It is recognized as one of the key initiators of the atherosclerosis process (42), and its levels are known to be increased in PLWH (43). Furthermore, IL-6 has demonstrated prognostic value for overall mortality in PLWH (16, 44–46). Notably, studies have shown that IL-6 is an independent predictor of cardiovascular disease in PLWH, regardless of traditional atherosclerotic risk factors (47, 48). In the REPRIEVE (Reinforced Vascular Event Prevention in HIV) randomized trial, coronary artery disease detected by computed tomography was independently associated with IL-6 levels in PLWH (46). However, the relative contribution of endothelial, platelet, or coagulation factors was not assessed in any of these studies.
In summary, our analysis revealed that, in addition to classical cardiovascular risk factors, IL-6 is independently associated with the presence of subclinical atherosclerosis in PLWH with long-term controlled viral replication, underscoring the relevance of IL-6 as both a marker and a potential therapeutic target in the management of HIV-associated cardiovascular disease. In contrast, other HIV-related factors, such as duration of infection or CD4+ T lymphocyte counts at diagnosis or inclusion, were not identified as independent contributors to the atherosclerotic process. Therefore, our study reinforces the need to integrate inflammatory biomarkers into cardiovascular risk assessment for PLWH, moving beyond traditional risk scores to better identify those at risk of vascular disease. Since current clinical guidelines are mostly based on the general population, there is an urgent need for strategies specifically targeting HIV-related inflammation.
Limitations
Cardiovascular risk factors were defined according to the guidelines in place at the start of the study (19). Smoking was defined as the consumption of more than 10 cigarettes/day. This criterion differs from more recent definitions that consider any tobacco use. Additionally, the observational and single-center nature of the study may limit the generalizability of the results. Nevertheless, the homogeneity of our cohort and the comprehensive analysis of immuno-inflammatory and vascular markers strengthen the relevance of these findings for PLWH with durable viral suppression.
In conclusion, this study identified significant activation of inflammatory and immune cells, including PMNs, in PLWH with prolonged viral suppression. This immune activation was associated with subclinical atherosclerosis, highlighting its potential role in cardiovascular risk in this population. Additionally, evidence of platelet and coagulation activation was observed. Importantly, the presence of subclinical atherosclerosis was independently influenced by both traditional cardiovascular risk factors and inflammatory activation. These findings support the integration of inflammatory biomarker analysis into the clinical evaluation of PLWH to enable earlier detection and management of atherosclerosis.
Data availability statement
The original contributions presented in this study are included in this article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki, local legislation, and institutional requirements. The project was approved by the Comité Coordinador de Ética de la Investigación Biomédica de Andalucía (PI-0128-2018-2, Consejería de Salud de la Junta de Andalucía, Spain). All participants provided their written informed consent prior to inclusion in the study.
Author contributions
FI-Á: Formal Analysis, Investigation, Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review and editing. DM-R: Formal Analysis, Investigation, Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review and editing. SC-S: Formal Analysis, Methodology, Validation, Visualization, Writing – original draft, Writing – review and editing. IC-G: Investigation, Methodology, Writing – original draft, Writing – review and editing. AM-A: Investigation, Methodology, Writing – original draft, Writing – review and editing. IT-R: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. MM-C: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. JG-G: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Consejería de Salud de la Junta de Andalucía, Spain, Iniciativa Territorial Integrada 2014–2020 para la provincia de Cádiz (No PI-0076-2017); by Instituto de Salud Carlos III, Acción Estratégica en Salud 2019 and 2023 (No PI19/01361 and PI23/01605), Spain. Co-financed by the European Regional Development Fund (FEDER).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1621765/full#supplementary-material
References
1. Zicari S, Sessa L, Cotugno N, Ruggiero A, Morrocchi E, Concato C, et al. Immune activation, inflammation, and Non-AIDS Co-morbidities in HIV-infected patients under long-term ART. Viruses. (2019) 11:200. doi: 10.3390/v11030200
2. Obare L, Temu T, Mallal S, Wanjalla C. Inflammation in HIV and its impact on atherosclerotic cardiovascular disease. Circ Res. (2024) 134:1515–45. doi: 10.1161/CIRCRESAHA.124.323891
3. Saumoy M, Fernandez A, Tiraboschi J, Peñafiel J, Sánchez-Quesada J, Vega J, et al. Biomarkers of inflammation and coagulation predict non-AIDS-defining events in a prospective cohort of virologically suppressed people living with HIV. HIV Med. (2025) 26:849–57. doi: 10.1111/hiv.70017
4. Dirajlal-Fargo S, Funderburg N. HIV and cardiovascular disease: The role of inflammation. Curr Opin HIV AIDS. (2022) 17:286–92. doi: 10.1097/COH.0000000000000755
5. Calza L, Magistrelli E, Danese I, Colangeli V, Borderi M, Bon I, et al. Changes in serum markers of inflammation and endothelial activation in HIV-infected antiretroviral naive patients starting A treatment with abacavir-lamivudine or tenofovir-emtricitabine plus efavirenz. Curr HIV Res. (2016) 14:61–70. doi: 10.2174/1570162x1401151102143222
6. O’Halloran J, Dunne E, Gurwith M, Lambert J, Sheehan G, Feeney E, et al. The effect of initiation of antiretroviral therapy on monocyte, endothelial and platelet function in HIV-1 infection. HIV Med. (2015) 16:608–19. doi: 10.1111/hiv.12270
7. Hunt P, Lee S, Siedner M. Immunologic biomarkers, morbidity, and mortality in treated HIV infection. J Infect Dis. (2016) 214(Suppl):S44–50. doi: 10.1093/infdis/jiw275
8. Márquez M, Romero-Cores P, Montes-Oca M, Martín-Aspas A, Soto-Cárdenas M, Guerrero F, et al. Immune activation response in chronic HIV-infected patients: Influence of Hepatitis C virus coinfection. PLoS One. (2015) 10:e0119568. doi: 10.1371/journal.pone.0119568
9. Kolaczkowska E, Kubes P. Neutrophil recruitment and function in health and inflammation. Nat Rev Immunol. (2013) 13:159–75. doi: 10.1038/nri3399
10. Saitoh T, Komano J, Saitoh Y, Misawa T, Takahama M, Kozaki T, et al. Neutrophil extracellular traps mediate a host defense response to human immunodeficiency virus-1. Cell Host Microbe. (2012) 12:109–16. doi: 10.1016/j.chom.2012.05.015
11. Megens R, Vijayan S, Lievens D, Döring Y, van Zandvoort M, Grommes J, et al. Presence of luminal neutrophil extracellular traps in atherosclerosis. Thromb Haemost. (2012) 107:597–8. doi: 10.1160/TH11-09-0650
12. Borissoff J, Joosen I, Versteylen M, Brill A, Fuchs T, Savchenko A, et al. Elevated levels of circulating DNA and chromatin are independently associated with severe coronary atherosclerosis and a prothrombotic state. Arterioscler Thromb Vasc Biol. (2013) 33:2032–40. doi: 10.1161/ATVBAHA.113.301627
13. Oklu R, Stone J, Albadawi H, Watkins M. Extracellular traps in lipid-rich lesions of carotid atherosclerotic plaques: Implications for lipoprotein retention and lesion progression. J Vasc Interv Radiol. (2014) 25:631–4. doi: 10.1016/j.jvir.2013.12.567
14. Park J, Dean L, Heckl J, Gangcuangco L, Pedro T, Tallquist M, et al. Low-density granulocytes display immature cells with enhanced NET formation in people living with HIV. Sci Rep. (2023) 13:13282. doi: 10.1038/s41598-023-40475-0
15. GESIDA. Documento de Consenso de GeSIDA - Panel de Expertos de GESIDA Respecto al Tratamiento Antirretroviral en Adultos Infectados Por El Virus de la Inmunodeficiencia Humana (Actualización enero 2025). (2025). Available online at: https://gesida-seimc.org/ (accessed April 21, 2025).
16. Hunt P, Sinclair E, Rodriguez B, Shive C, Clagett B, Funderburg N, et al. Gut epithelial barrier dysfunction and innate immune activation predict mortality in treated HIV infection. J Infect Dis. (2014) 210:1228–38. doi: 10.1093/infdis/jiu238
17. Abad-Fernández M, Vallejo A, Hernández-Novoa B, Díaz L, Gutiérrez C, Madrid N, et al. Correlation between different methods to measure microbial translocation and its association with immune activation in long-term suppressed HIV-1-infected individuals. J Acquir Immune Defic Syndr. (2013) 64:149–53. doi: 10.1097/QAI.0b013e31829a2f12
18. Lauková L, Konečná B, Janovičová Ľ, Vlková B, Celec P. Deoxyribonucleases and their applications in biomedicine. Biomolecules. (2020) 10:1036. doi: 10.3390/biom10071036
19. Ruiz-García A, Arranz-Martínez E, Morón-Merchante I, Pascual-Fuster V, Tamarit J, Trias-Villagut F, et al. Consensus document of the Spanish Society of Arteriosclerosis (SEA) for the prevention and treatment of cardiovascular disease in type 2 diabetes mellitus. Clin Investig Arterioscler. (2018) 30(Suppl 1):1–19. doi: 10.1016/j.arteri.2018.06.006
20. Marrugat J, D’Agostino R, Sullivan L, Elosua R, Wilson P, Ordovas J, et al. An adaptation of the Framingham coronary heart disease risk function to European Mediterranean areas. J Epidemiol Community Health. (2003) 57:634–8. doi: 10.1136/jech.57.8.634
21. Goff D, Lloyd-Jones D, Bennett G, Coady S, D’Agostino R, Gibbons R, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. (2014) 129:S49–73. doi: 10.1161/01.cir.0000437741.48606.98
22. Such J, Francés R, Muñoz C, Zapater P, Casellas J, Cifuentes A, et al. Detection and identification of bacterial DNA in patients with cirrhosis and culture-negative, nonneutrocytic ascites. Hepatology. (2002) 36:135–41. doi: 10.1053/jhep.2002.33715
23. Mancia G, Kreutz R, Brunström M, Burnier M, Grassi G, Januszewicz A, et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Associa. J Hypertens. (2023) 41:1874–2071. doi: 10.1097/HJH.0000000000003480
24. Stein J, Korcarz C, Hurst R, Lonn E, Kendall C, Mohler E, et al. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: A consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascul. J Am Soc Echocardiogr. (2008) 21:90–3. doi: 10.1016/j.echo.2007.11.011
25. Grau M, Subirana I, Agis D, Ramos R, Basagaña X, Martí R, et al. Carotid intima-media thickness in the Spanish population: Reference ranges and association with cardiovascular risk factors. Rev Esp Cardiol. (2012) 65:1086–93. doi: 10.1016/j.recesp.2012.04.026
26. Post W, Budoff M, Kingsley L, Palella F, Witt M, Li X, et al. Associations between HIV infection and subclinical coronary atherosclerosis. Ann Intern Med. (2014) 160:458–67. doi: 10.7326/M13-1754
27. Jiang W, Lederman M, Hunt P, Sieg S, Haley K, Rodriguez B, et al. Plasma levels of bacterial DNA correlate with immune activation and the magnitude of immune restoration in persons with antiretroviral-treated HIV infection. J Infect Dis. (2009) 199:1177–85. doi: 10.1086/597476
28. Cuesta-Sancho S, Márquez-Ruiz D, Illanes-Álvarez F, Campaña-Gómez I, Martín-Aspas A, Trujillo-Soto M, et al. Expression profile of microRNAs related with viral infectivity, inflammatory response, and immune activation in people living with HIV. Front Microbiol. (2023) 14:1136718. doi: 10.3389/fmicb.2023.1136718
29. Avagimyan A, Pogosova N, Kakturskiy L, Sheibani M, Urazova O, Trofimenko A, et al. HIV-related atherosclerosis: State-of-the-art-review. Curr Probl Cardiol. (2023) 48:101783. doi: 10.1016/j.cpcardiol.2023.101783
30. Broos K, Feys H, De Meyer S, Vanhoorelbeke K, Deckmyn H. Platelets at work in primary hemostasis. Blood Rev. (2011) 25:155–67. doi: 10.1016/j.blre.2011.03.002
31. Poredos P, Poredos A, Gregoric I. Endothelial dysfunction and its clinical implications. Angiology. (2021) 72:604–15. doi: 10.1177/0003319720987752
32. Zaldivar M, Pauels K, von Hundelshausen P, Berres M, Schmitz P, Bornemann J, et al. CXC chemokine ligand 4 (Cxcl4) is a platelet-derived mediator of experimental liver fibrosis. Hepatology. (2010) 51:1345–53. doi: 10.1002/hep.23435
33. Liu Z, Li L, Zhang H, Pang X, Qiu Z, Xiang Q, et al. Platelet factor 4(PF4) and its multiple roles in diseases. Blood Rev. (2024) 64:101155. doi: 10.1016/j.blre.2023.101155
34. Bravo C, Moon J, Davy K, Kaplan R, Anastos K, Rodriguez C, et al. Association of HIV and HCV infection with carotid artery plaque echomorphology in the MACS/WIHS combined cohort study. Stroke. (2024) 55:651–9. doi: 10.1161/STROKEAHA.123.043922
35. Saumoy M, Di Yacovo S, Pérez S, Sánchez-Quesada J, Valdivielso J, Subirana I, et al. Carotid atherosclerosis in virologically suppressed HIV patients: Comparison with a healthy sample and prediction by cardiovascular risk equations. HIV Med. (2021) 22:581–91. doi: 10.1111/hiv.13093
36. Fernández-Friera L, Peñalvo J, Fernández-Ortiz A, Ibañez B, López-Melgar B, Laclaustra M, et al. Prevalence, vascular distribution, and multiterritorial extent of subclinical atherosclerosis in a middle-aged cohort: The PESA (Progression of Early Subclinical Atherosclerosis) Study. Circulation. (2015) 131:2104–13. doi: 10.1161/CIRCULATIONAHA.114.014310
37. Marrugat J, Vila J, Baena-Díez J, Grau M, Sala J, Ramos R, et al. [Relative validity of the 10-year cardiovascular risk estimate in a population cohort of the REGICOR study]. Rev Esp Cardiol. (2011) 64:385–94. doi: 10.1016/j.recesp.2010.12.011
38. Feinstein M, Nance R, Drozd D, Ning H, Delaney J, Heckbert S, et al. Assessing and refining myocardial infarction risk estimation among patients with human immunodeficiency virus: A study by the centers for AIDS research network of integrated clinical systems. JAMA Cardiol. (2017) 2:155–62. doi: 10.1001/jamacardio.2016.4494
39. Rasmussen L, Helleberg M, May M, Afzal S, Kronborg G, Larsen C, et al. Myocardial infarction among Danish HIV-infected individuals: Population-attributable fractions associated with smoking. Clin Infect Dis. (2015) 60:1415–23. doi: 10.1093/cid/civ013
40. Brown T, Cole S, Li X, Kingsley L, Palella F, Riddler S, et al. Antiretroviral therapy and the prevalence and incidence of diabetes mellitus in the multicenter AIDS cohort study. Arch Intern Med. (2005) 165:1179–84. doi: 10.1001/archinte.165.10.1179
41. Scheller J, Chalaris A, Schmidt-Arras D, Rose-John S. The pro- and anti-inflammatory properties of the cytokine interleukin-6. Biochim Biophys Acta. (2011) 1813:878–88. doi: 10.1016/j.bbamcr.2011.01.034
42. Hemmat N, Ebadi A, Badalzadeh R, Memar M, Baghi H. Viral infection and atherosclerosis. Eur J Clin Microbiol Infect Dis. (2018) 37:2225–33. doi: 10.1007/s10096-018-3370-z
43. Hsue P, Waters D. HIV infection and coronary heart disease: Mechanisms and management. Nat Rev Cardiol. (2019) 16:745–59. doi: 10.1038/s41569-019-0219-9
44. Danesh J, Kaptoge S, Mann A, Sarwar N, Wood A, Angleman S, et al. Long-term interleukin-6 levels and subsequent risk of coronary heart disease: Two new prospective studies and a systematic review. PLoS Med. (2008) 5:e78. doi: 10.1371/journal.pmed.0050078
45. Wada N, Bream J, Martínez-Maza O, Macatangay B, Galvin S, Margolick J, et al. Inflammatory biomarkers and mortality risk among HIV-suppressed men: A multisite prospective cohort study. Clin Infect Dis an Off Publ Infect Dis Soc Am. (2016) 63:984–90. doi: 10.1093/cid/ciw409
46. Hoffmann U, Lu M, Foldyna B, Zanni MV, Karady J, Taron J, et al. Assessment of coronary artery disease with computed tomography angiography and inflammatory and immune activation biomarkers among adults With HIV eligible for primary cardiovascular prevention. JAMA Netw Open. (2021) 4:e2114923. doi: 10.1001/jamanetworkopen.2021.14923
47. Duprez D, Neuhaus J, Kuller L, Tracy R, Belloso W, De Wit S, et al. Inflammation, coagulation and cardiovascular disease in HIV-infected individuals. PLoS One. (2012) 7:e44454. doi: 10.1371/journal.pone.0044454
Keywords: HIV, proinflammatory cytokines, endothelial activation, platelet activation, atherosclerosis, cardiovascular risk factors
Citation: Illanes-Álvarez F, Márquez-Ruiz D, Cuesta-Sancho S, Campaña-Gómez I, Martín-Aspas A, Tinoco-Racero I, Márquez-Coello M and Girón-González J-A (2025) Persistent inflammatory activation in people living with HIV. Involvement in atherosclerosis. Front. Med. 12:1621765. doi: 10.3389/fmed.2025.1621765
Received: 01 May 2025; Accepted: 16 June 2025;
Published: 11 July 2025.
Edited by:
Vivek P Chavda, L. M. College of Pharmacy, IndiaReviewed by:
Nicholas Funderburg, The Ohio State University, United StatesAshot Avagimyan, Yerevan State Medical University, Armenia
Copyright © 2025 Illanes-Álvarez, Márquez-Ruiz, Cuesta-Sancho, Campaña-Gómez, Martín-Aspas, Tinoco-Racero, Márquez-Coello and Girón-González. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José-Antonio Girón-González, am9zZWFudG9uaW8uZ2lyb25AdWNhLmVz
†These authors have contributed equally to this work
‡These authors have contributed equally to this work and share last authorship