 Pernilla Sönnerfors1,2*
Pernilla Sönnerfors1,2* Petra Kristina Jacobson3,4†
Petra Kristina Jacobson3,4† Anders Andersson5,6
Anders Andersson5,6 Leif Hilding Bjermer7
Leif Hilding Bjermer7 Anders Blomberg8Heléne Blomqvist1,9
Anders Blomberg8Heléne Blomqvist1,9 Christer Janson10
Christer Janson10 Jonas S. Erjefält11Hans Lennart Persson3,4†
Jonas S. Erjefält11Hans Lennart Persson3,4† Ellen Tufvesson7
Ellen Tufvesson7 Åsa M. Wheelock1,9
Åsa M. Wheelock1,9 Carl Magnus Sköld1,9Annelie Behndig8†
Carl Magnus Sköld1,9Annelie Behndig8†- 1Department of Medicine Solna, Division of Immunology and Respiratory Medicine, Center for Molecular Medicine, Karolinska Institutet, Stockholm, Sweden
- 2Women’s Health and Allied Health Professionals Theme, Karolinska University Hospital, Stockholm, Sweden
- 3Department of Respiratory Medicine in Linköping, Linköping University, Linköping, Sweden
- 4Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden
- 5COPD Center, Department of Respiratory Medicine and Allergology, Sahlgrenska University Hospital, Gothenburg, Sweden
- 6COPD Center, Department of Internal Medicine and Clinical Nutrition, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
- 7Department of Clinical Sciences, Respiratory Medicine, Allergy and Palliative Medicine, Lund University, Lund, Sweden
- 8Department of Public Health and Clinical Medicine, Umeå University, Umeå, Sweden
- 9Department of Respiratory Medicine and Allergy, Karolinska University Hospital, Stockholm, Sweden
- 10Department of Medical Sciences, Respiratory, Allergy and Sleep Research, Uppsala University, Uppsala, Sweden
- 11Unit of Airway Inflammation, Department of Experimental Medicine Sciences, Lund University, Lund, Sweden
Introduction: Flexible bronchoscopy is regarded as a safe examination and is commonly used in the diagnostic work-up for lung diseases, but is also important in pulmonary research. We aimed to investigate participants’ experiences when undergoing bronchoscopy in a research setting.
Methods: Participants were recruited from the Swedish CArdioPulmonary bioImage Study (SCAPIS). A subset from this cohort (n = 45, mean age 60.5 years, 20 with normal lung function and 25 with chronic obstructive pulmonary disease, COPD) was selected for bronchoscopy. The procedure was explained both orally and in writing during a pre-procedure visit. The information included premedication, monitoring, local anesthesia, airway sampling [bronchoalveolar lavage (BAL), bronchial wash, and mucosal biopsies], and urine and blood samples. Questionnaires pre- and/or post-procedure were used to assess experiences and health impacts.
Results: In general, participants found the bronchoscopy procedure acceptable and only a few (18%) found it unpleasant. A majority (80%) reported their experience to be much better or as expected. Almost all participants (93%) were very satisfied with the information provided. Topical anesthesia was seen as more unpleasant (20%) than airway sampling (11%). Notably, more women and participants with normal lung function reported BAL as unpleasant. After the procedure, chills, fever, and hemoptysis were reported, but no serious adverse events occurred. Increased cough and phlegm were noted.
Conclusion: The present study, conducted by experienced bronchoscopists and healthcare teams, demonstrates that a bronchoscopy in a research setting in well-informed participants with normal lung function or COPD was well-tolerated.
1 Introduction
Flexible bronchoscopy is regarded as a safe examination method and is routinely used in the diagnostic work-up of lung diseases, but it is also important in pulmonary research. The side effects of bronchoscopy are primarily related to the procedure itself, such as bleeding, cough, and oxygen desaturation, but fever can also occur (1–4). The willingness to participate in research bronchoscopy is often high in resource-limited settings, due to the possibility of getting a free health check and showing gratitude to society (5). Younger age (<40 years), higher education level, a prior history of donating blood and having a chronic disease have been reported to increase the willingness to participate. The possibility of finding new treatments in the future has also been shown to increase motivation (6). However, it has also been shown that financial reward and altruism were highly motivating factors for healthy participants to participate in research studies (7). In a high-income setting, participants with chronic obstructive pulmonary disease (COPD) and asthma have also expressed a wish to help others and a hope to contribute to science. Also, personal benefits and a subjective feeling of being obligated to participate have been reported as factors (8). Well-trained recruiters, who can provide the participants with correct and trustworthy information, are essential, as trust in the researchers is an important factor in increasing the willingness to participate in medical research. Perceived risk of harm and fear of discomfort are major reasons for refusal to participate in health research (6, 8). Predictors of patients willing to participate in a second bronchoscopy are lower age, higher education, use of higher doses of anxiolytics and an inpatient setting (9).
Little is known about participants’ experiences of the procedures to undergo a bronchoscopy in a research setting, including their well-being on the following day. Knowledge of participants’ experiences of taking part in a research bronchoscopy might help optimize the recruitment process and the participant rate. Furthermore, to guide researchers in how to prepare participants and what to include in comprehensive information regarding the procedure might improve the overall experience. This study aimed to investigate the experiences of middle-aged participants with normal lung function and with COPD undergoing a bronchoscopy in a research setting.
2 Materials and methods
2.1 Study subjects
The study was based on the Swedish CArdioPulmonary bioImage Study (SCAPIS), a multi-center study investigating a population-based sample of the general Swedish population (n = 30,154) (10). Participants aged 50–75 years were screened and recruited based on smoking history and lung function to join the BRONCHO-SCAPIS study (n = 690)1 conducted at six university hospitals in Sweden from 2017 to 2023, with the primary aim to study COPD in never-smokers (11). In the present study, a total of 45 individuals were selected for bronchoscopy (Figure 1). Participants were divided into two study groups: participants with COPD (never-smokers and ex-smokers) and never-smokers with normal lung function. Participants with COPD had postbronchodilator (post-BD) forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) < 0.70 and FEV1/FVC z-score < −1.64 (<lower limit of normal, LLN) and FEV1 50–100% of predicted value. Participants with normal lung function had post-BD FEV1/FVC ≥ 0.75, FEV1/FVC z-score of ≥ LLN and FEV1 ≥ 90% of predicted value. Reference values used were from the European Community for Coal and Steel cohort (ECCS) (12), and for LLN (z-score), according to the Global Lung Initiative (GLI) (13). Participants who had smoked fewer than 100 cigarettes or 20 cigars in their lifetime and had not smoked at all in the past 2 years were defined as “never-smokers.” Participants with a prior history of tobacco smoking, who had at least 10 pack-years of tobacco smoking and had been more than 2 years since they stopped smoking, were referred to as “ex-smokers” in this study.
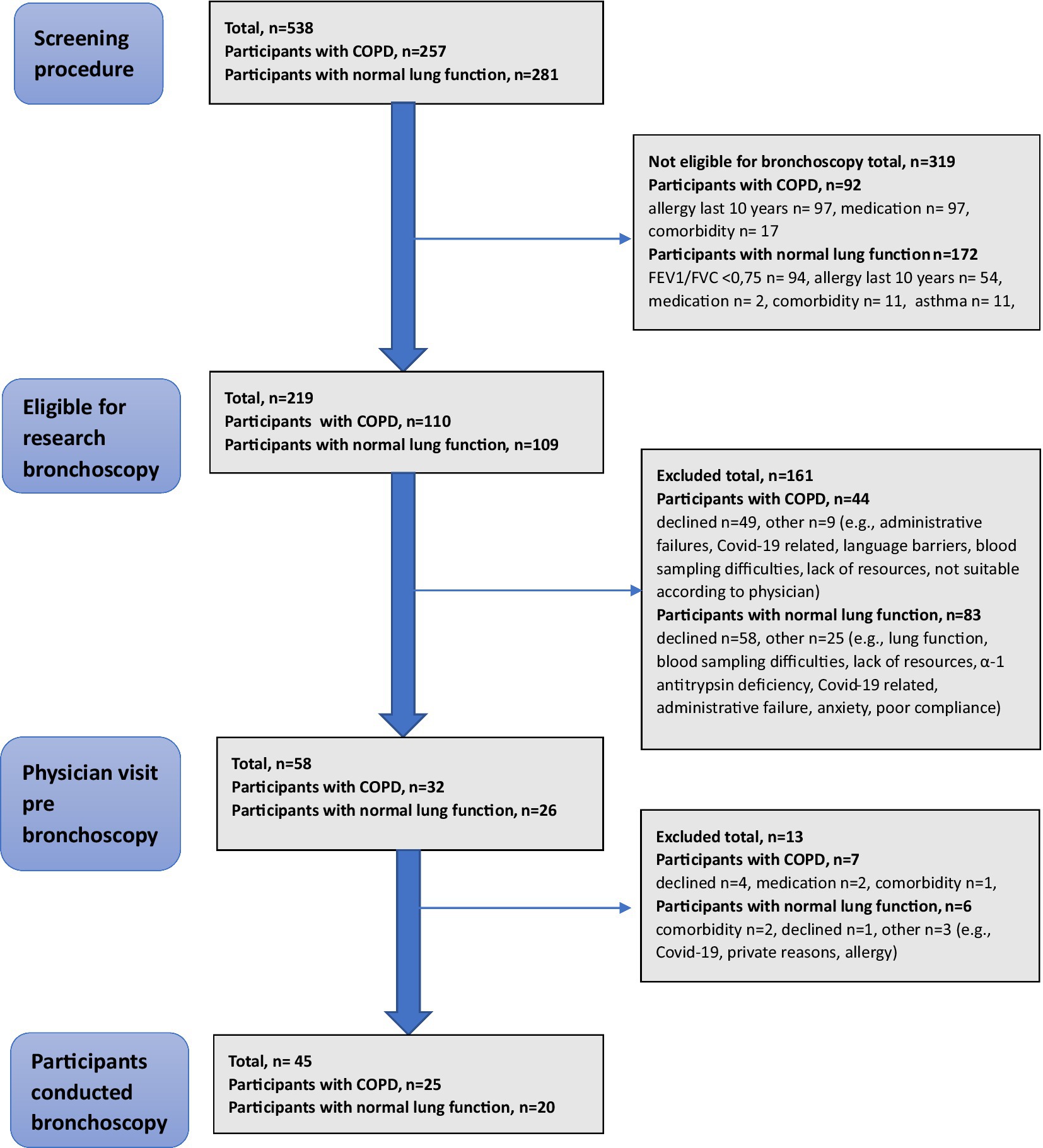
Figure 1. Flowchart of participants included in the BRONCHO-SCAPIS study undergoing research bronchoscopy.
Participants were excluded if they had an exacerbation requiring antibiotics or oral corticosteroids within 3 months or were using immunomodulating treatments. The participants were not allowed to use inhaled corticosteroids (ICS) for 3 months prior to bronchoscopy, and 1 month was required for common colds or viral upper airway infections. Other exclusion criteria included a history of significant cardiovascular diseases, coagulopathies, interstitial lung diseases, bronchiectasis, allergic eye/nose symptoms, and alcohol or drug abuse. A history of known causes of airway obstruction, such as alpha-1 antitrypsin deficiency or primary ciliary dyskinesia, was not allowed. In the study group with normal lung function, asthma was not allowed. Details of the exclusion criteria can be found in the Supplementary material.
2.2 Procedures before bronchoscopy
The study participants underwent three visits as part of the study protocol. The first visit was a screening visit, as previously described (11) for medical history, including respiratory symptoms, vital signs, routine blood tests, biobank samples and lung function tests. The participants received an economic compensation of 500 SEK (approximately 45 EUR or 50 USD) for the screening, along with 2,300 SEK (210 EUR and 230 USD) for the research bronchoscopy.
A preprocedural clinical visit with a respiratory physician was arranged before the bronchoscopy as a second visit. Then, a detailed medical history was repeatedly taken, and a physical examination was performed. Current medications were documented in the medical record. Information about premedication, monitoring, topical anesthesia, airway sampling, and potential risks was given. An electrocardiogram (ECG) was performed, as well as a chest X-ray if not done during the last 3 months. Premedication for bronchoscopy was prescribed and blood samples were collected.
2.3 Bronchoscopy and sampling of the airways
On the day of the bronchoscopy, participants were fasting. Before the bronchoscopy, research samples were collected: blood (a total of 50 mL), urine and a mouthwash for analysis of mediators.
During bronchoscopy, participants were in the supine position and monitored for ECG, heart rate, and oxygen saturation (SaO2) by transcutaneous pulse oximetry. Supplemental oxygen (1–2 L/min) was administered via nasal prongs if deemed necessary by the bronchoscopist. Topical anesthesia was provided following local guidelines. Intravenous midazolam [2–3 (−5) mg] and robinul [0.2 (−0.4) mg] were administered before and during the procedure based on the physician’s clinical judgment. Additional doses of midazolam and/or alfentanil were administered during the procedure if required; alfentanil was given in doses of 0.25–0.5 mg. Bronchoscopy was performed by senior consultants, all with many years of experience, using a bronchoscope with an external diameter of 5 mm via an oral approach. During the bronchoscopy, the following airway samples were collected: Bronchial wash with three 10 mL aliquots of phosphate-buffered saline (PBS) at pH 7.4, pre-warmed to 37°C, administered in the right upper lobe for microbial culture. Bronchial brush samples were optional for the site, with up to five samples collected from the airway tree. A total of 10 endobronchial mucosal biopsy samples were obtained from the bronchial tree. Bronchoalveolar lavage (BAL) was performed with 180 mL of PBS, administered in the middle lobe in three 60 mL portions. After bronchoscopy, the participants fasted for 2.5 h and were then offered coffee or tea and a sandwich before leaving the hospital. At one study center, oral corticosteroids following bronchoscopy were given (n = 5) according to local guidelines. Each bronchoscopy procedure lasted approximately 30 min.
2.4 Questionnaires
Before and after the bronchoscopy procedure, a questionnaire of five questions regarding health status was completed. The questions were answered on a 6-item Likert scale (0–5), with higher scores indicating a worse health status. The questions addressed symptoms of cough, phlegm (mucus), wheeze, chest tightness and energy levels. The questionnaire was administered by a research nurse at the clinic on the morning of the bronchoscopy and was repeated by telephone the day after the bronchoscopy.
Another set of questions was developed to examine participants’ experience of undergoing a research bronchoscopy. These questions were tested in a pilot study on 15 healthy volunteers (14) before being used in the present study. All questions regarding participants’ experiences were answered by telephone the day after the bronchoscopy.
2.5 Statistical analysis
The Statistical Package for the Social Sciences (SPSS, IBM, New York, United States) was used for the analyses. The clinical characteristics were summarized using descriptive quantitative statistics and presented as numbers (n), per cent (%), median and interquartile range (IQR), or mean and standard deviation (SD). Subgroup analyses were conducted based on sex and lung function.
3 Results
3.1 Participants clinical characteristics
Of the 58 eligible participants who first accepted to participate and underwent a pre-bronchoscopy visit at the clinic, 13 were excluded due to later declining participation (n = 5), comorbidity (n = 3), medication not allowed (n = 2) or other reasons (COVID-19, allergy, private reasons, n = 3). Finally, a total of 45 participants performed bronchoscopy and were included in the data analysis. Of those, 25 had COPD (15 never-smokers and 10 ex-smokers) and 20 had normal lung function.
In all participants, age ranged from 54 to 72 years with a mean of 60.5 years (±4.6), and 44% were women. Most of the participants (89%) had no prior experience with bronchoscopy (Table 1). Their mean oxygen saturation was 97.6%, and their mean body mass index (BMI) was 26.4 kg/m2. Nearly all had a high education level (high school or college, university), most lived in detached or semi-detached houses, and most of them were still working (78%). A minority of participants reported respiratory symptoms (18%) during the last year, mostly wheezing. Some had a productive cough in the last year (24%), and only 4% reported chronic cough. In descending order, the most common comorbidities were hypertension, depression, sleep apnea, pet allergy, asthma, diabetes, and other heart diseases.
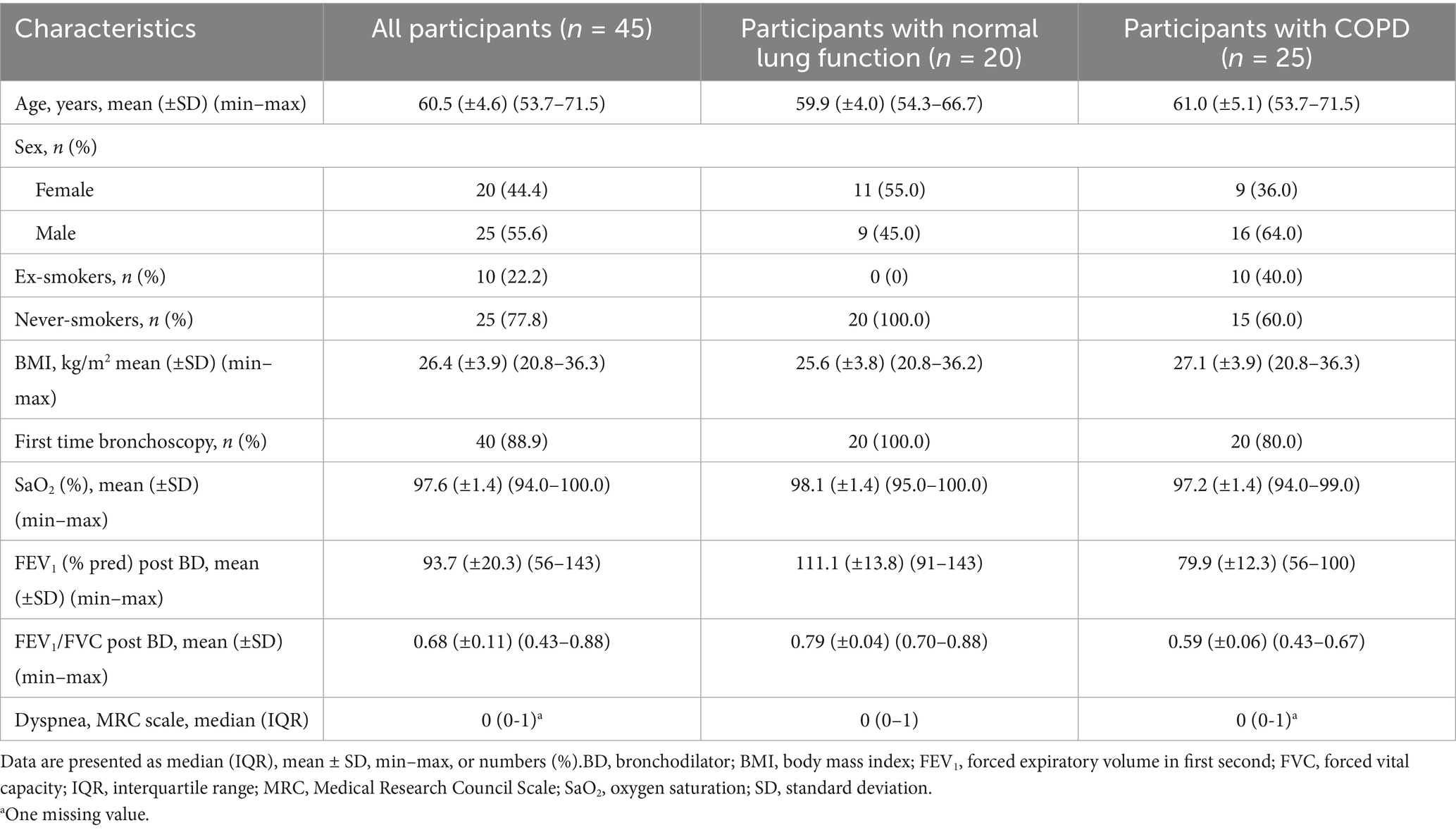
Table 1. Clinical characteristics of all participants who performed bronchoscopy, divided into those with normal lung function and those with COPD.
3.2 Experiences of bronchoscopy
Half of the participants found the overall experience of a research bronchoscopy a little unpleasant but okay (48%), simple (23%), or very simple (11%), and only 18% found it unpleasant. More women than men found it unpleasant (21% vs. 16%) and participants with normal lung function found it more unpleasant than participants with COPD (25% vs. 12%). Some experienced the bronchoscopy to be worse than expected (21%), but most of them found it to be better than expected (43%) or as expected (38%). The airway samplings were generally regarded as only a little unpleasant to very simple (89–91%). The samplings were found to be unpleasant or very unpleasant by more women than men (15% vs. 8%) and by more participants with normal lung function than participants with COPD (15% vs. 8%). Almost all participants experienced that the pre-medication had the intended effect (89%). Twenty per cent of all participants experienced receiving topical anesthesia as being unpleasant or very unpleasant, more among participants with normal lung function than among participants with COPD (25% vs. 16%). Participants were, to a large extent, satisfied with the information they received before the bronchoscopy.
By telephone interview, self-reported symptoms after bronchoscopy were chills (44%), fever (38%) and mild hemoptysis (32%). Half of the participants (53%) used paracetamol or ibuprofen after the procedure.
3.3 Reasons for participating in research bronchoscopy
Most participated in the research bronchoscopy to contribute to research (42%) or in combination with receiving a thorough examination of the lungs (38%). There were more women motivated by contributing to research than men (45% vs. 40%). Almost half of the participants (44%) were absolutely sure they would participate in a research bronchoscopy again if asked, another 44% said they might do it again, and only 11% would not participate again. Participants with normal lung function (15%) and women (20%) were the least interested in undergoing a research bronchoscopy again (Table 2).
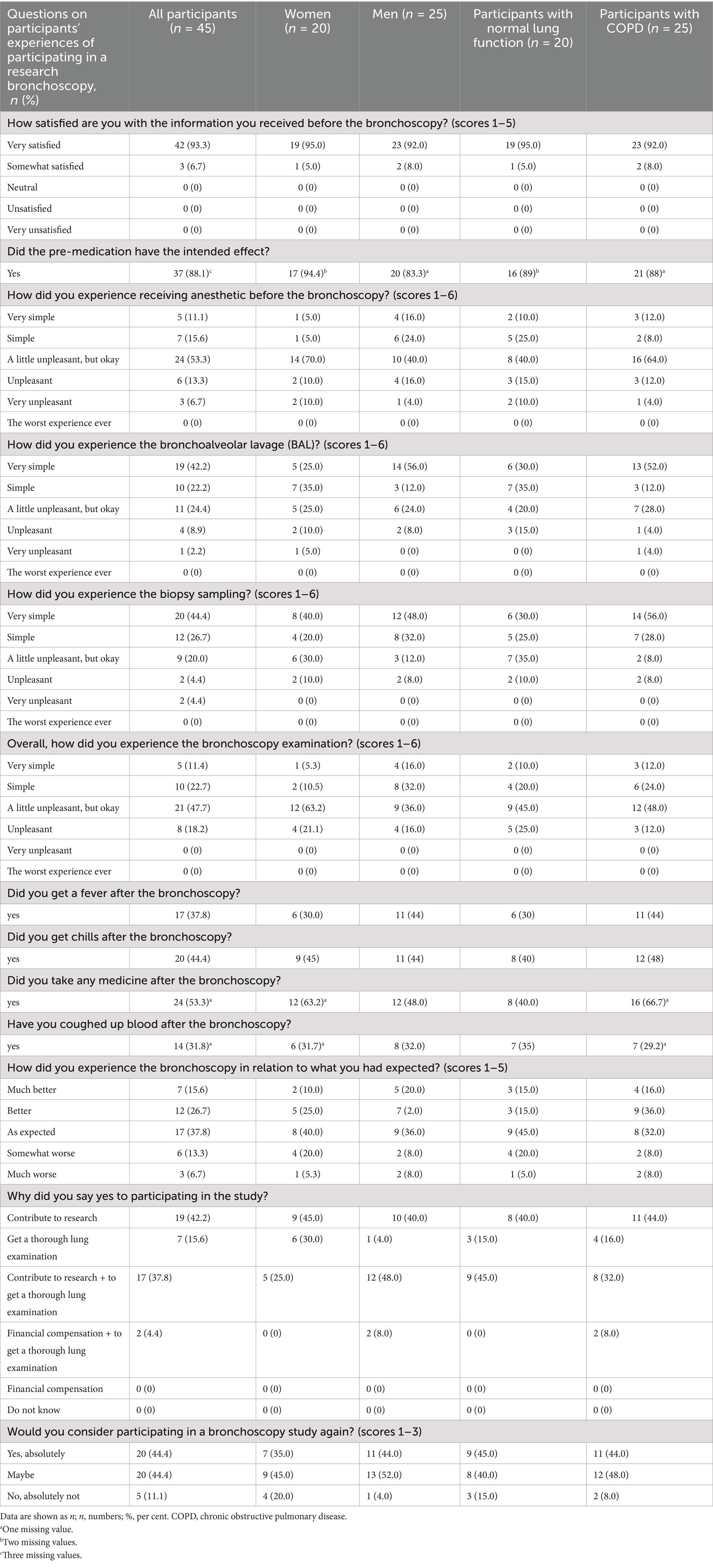
Table 2. Participants’ experiences of participating in research bronchoscopy divided into women versus men, and participants with normal lung function versus COPD.
3.4 Impact of research bronchoscopy
The participant’s health status did not change after bronchoscopy regarding wheezing, chest tightness and energy levels (Table 3). However, increased cough and phlegm were reported. There were no differences found regarding cough, tightness/pressure of the chest, or wheeze in the chest between participants with normal lung function and participants with COPD before and after bronchoscopy. Participants with normal lung function reported more phlegm after bronchoscopy compared to participants with COPD.
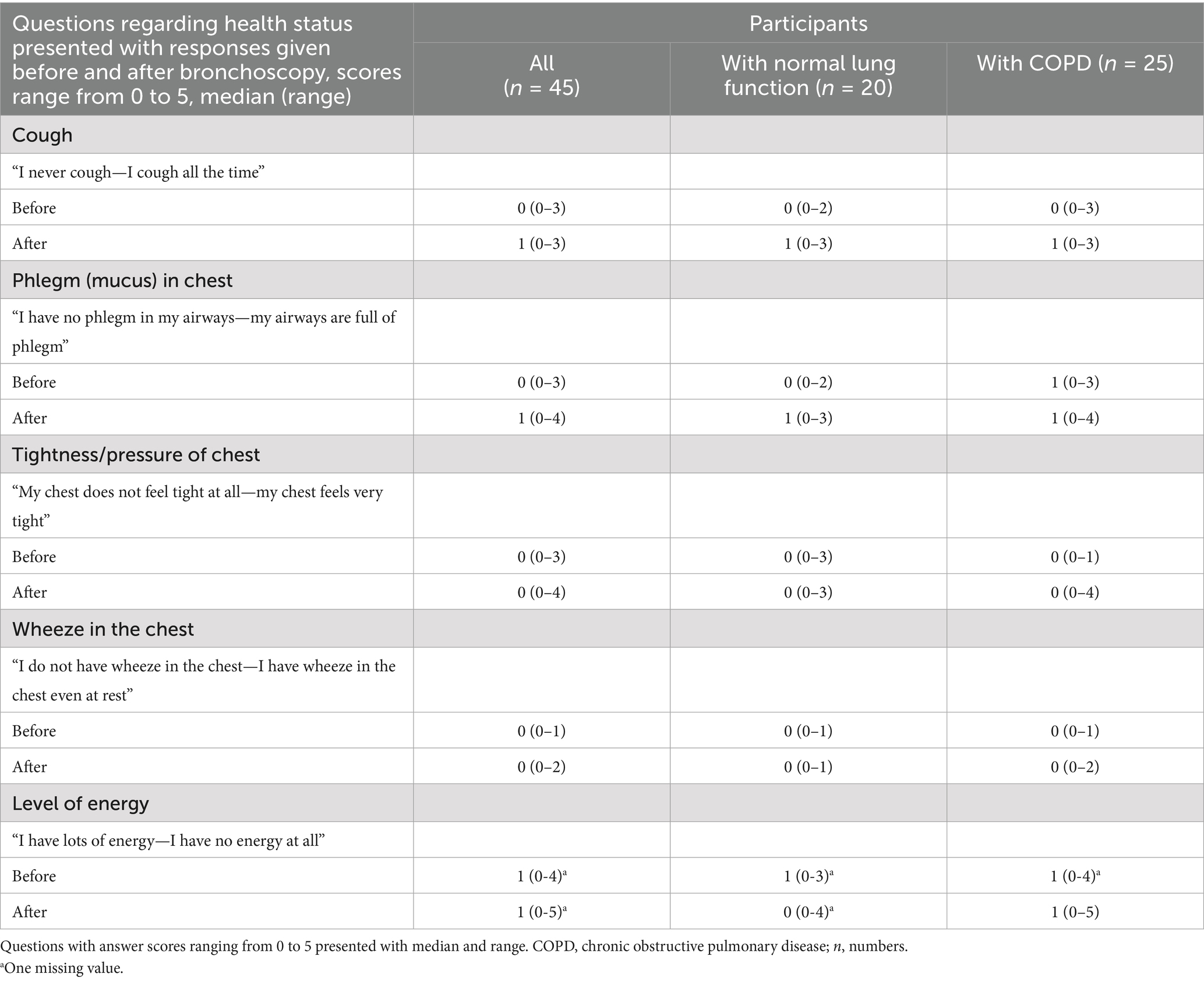
Table 3. Health status before and after a research bronchoscopy, shown for all participants and divided into groups of participants with normal lung function or COPD.
4 Discussion
The overall experience of undergoing a bronchoscopy in a research setting was generally considered tolerable, with only a few participants finding it unpleasant and most reported their experience to be much better or as expected. Participants were largely satisfied with the information they received before the bronchoscopy. The sampling procedures were mostly perceived as either slightly unpleasant or very simple. Notably, more women than men reported the samplings as unpleasant or very unpleasant, as did more participants with normal lung function compared to those with COPD.
Bronchoscopy is a safe procedure with a low complication rate (15). In this study, the participants reported chills, fever, and mild hemoptysis. The post-bronchoscopy complications were in accordance with previous reports (1), but somewhat difficult to fully compare since definitions of complications and discomfort vary between studies. Complications previously reported in patients undergoing bronchoscopy include a number of symptoms and signs such as hypoxia, pneumothorax, tachycardia, hemorrhage (9), coughing, hemodynamic changes and panic/subject unease (2, 9). Almost all participants experienced the intended effects of the pre-medication, but because of that, some participants could have been too “tired” to recall the procedure when asked about their experiences. This has been addressed in a qualitative study on participants with severe COPD, where half of them were unaware due to sedation during the bronchoscopy, and their reflections were mostly positive. They talked about drifting away and described being “knocked out” by the drugs and not remembering what happened (16). The tiredness could be challenging when answering the questions regarding their experiences, as they might not be fully aware of the various aspects of the procedure while sedated. It has been shown in a study on participants with COPD that those undergoing bronchoscopy with conscious sedation were often fully aware of the procedure. Many remembered feeling discomfort, especially from coughing and choking, which caused them distress (16). Discomfort during the bronchoscopy procedure has been shown to be an important factor affecting patient satisfaction (3).
In this study, the participants received pre-medication with midazolam and intravenous glycopyrronium and additional doses of midazolam and/or alfentanil when needed, according to the bronchoscopist’s clinical judgment. A greater comfort and satisfaction for patients has been described when the bronchoscopy was performed intubated under monitored anesthesia compared to when the bronchoscopy was performed under only topical anesthesia (4). This was also recognized in the present study as 88% experienced effect of the pre-medication, even though some (20%) had an unpleasant or very unpleasant experience of receiving the topical anesthesia. In a recent pilot study on healthy volunteers, research bronchoscopies without sedation were investigated. It was shown that minimizing the need for sedation by only using topical anesthesia has the potential to improve patient safety and enhance the tolerability of the procedure (17), which might also improve participants’ recollection of the procedure. Participants were mostly very satisfied with the information given before the bronchoscopy, and only 20% found the experience to be worse than expected. The importance of participants’ knowledge regarding the procedure has been shown to be significant. Providing adequate and relevant information about the bronchoscopy procedure, including illustrations and pictures, has been shown to help to reduce potential anxiety and improve the tolerability of participants (18, 19). Reducing the duration of the procedure is another crucial aspect that influences the patient’s comfort (19). This study limited the procedure to approximately 30 min. Study participants have previously expressed concerns about the bronchoscopy procedure being time-consuming and interrupting their work schedule (5).
Most participants expressed a desire to contribute to research, a motive that was particularly prevalent among women. Previous research on bronchoscopy has shown that altruistic motives are more common in women than in men (8). In the present study, more women were unwilling to participate in further research bronchoscopy than men. This reluctance may stem from the fact that women experienced the bronchoscopy procedure more negatively than they had anticipated. They also found receiving the topical anesthesia more difficult compared to the men. A moderate level of anxiety before the procedure has also been shown to be more common among women than men (3). Fear of discomfort and concerns about study participation have been noted as common reasons for individuals who are eligible but choose not to participate in a research bronchoscopy (8).
There were some differences between the subgroups when it came to their experiences of the procedure. Only a small number found the administration of topical anesthesia unpleasant or very unpleasant, with a higher percentage of participants with normal lung function reporting discomfort compared to those with COPD. The airway sampling was also perceived as more unpleasant among those with normal lung function compared to those with COPD. The reason participants with COPD experienced less discomfort is unknown, but it is possible that they are more used to having respiratory symptoms. The willingness to return for a research bronchoscopy was high, with participants with COPD being the most motivated. Willingness to return for a research bronchoscopy was also addressed in another study, where the participants with COPD were slightly less willing to return for another research bronchoscopy than those in the control group (76% vs. 84%) (2), which was opposite to the present results. A review has, however, shown no difference between these groups regarding the willingness to repeat bronchoscopy (20).
A strength of this study was that the bronchoscopy procedure was performed by experienced bronchoscopists and healthcare teams, which limits variability in procedure performance and enables comparison despite several study sites and several bronchoscopists. The experience of the physician performing the bronchoscopy has also been shown to be an important factor in reducing the number of complications (21). In the present study, there were no serious complications reported, which was seen as a strength, but this could be because the participants with COPD included in this study had milder airflow limitation than in other studies (2, 8). Also, more never-smoking participants with COPD, who often have milder symptoms (22), were included in this study. It might influence participants’ fear and concerns positively before undergoing a research bronchoscopy to know that the bronchoscopist is experienced, but previous studies have found no correlation between patient satisfaction and the bronchoscopist’s experience (23).
A limitation worth recognizing was that the questionnaires used to assess participants’ experiences have not been validated in a research setting, although pilot tested. Questions used to assess health status were modified from the COPD Assessment Test (CAT), which is validated in COPD (24). The absence of formal validation may impact the reliability and interpretation of the findings. Future research would benefit from employing fully validated questionnaires. Adopting a qualitative study approach could provide a deeper understanding of participants’ experiences (25). Another limitation might be that participants answered questions by telephone the day after the bronchoscopy procedure, which may also reduce their ability to remember details of the procedure. However, a telephone interview is common practice when it comes to distributing questionnaires about participants’ experiences. When recruiting participants for the present study, the current restrictions due to the COVID-19 pandemic limited the number of participants available or willing to participate. To obtain a representative sample, the inclusion period was prolonged, but during this time, some participants declined to participate despite showing an initial interest. Due to the lack of follow-ups on participants’ reasons for declining, this information remains unknown, which is considered a limitation. The limited number of participants is also a limitation, as a larger group would have enabled more general conclusions.
5 Conclusion
The present study shows participants’ experiences of a bronchoscopy in a research setting, including well-informed participants, experienced bronchoscopists and experienced healthcare teams, to be tolerable for participants both with normal lung function and with COPD.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by The Swedish Ethical Review Board in Stockholm Dnr 2016-841-31/2. The study was designed and conducted following the Declaration of Helsinki (26). The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
PS: Software, Writing – review & editing, Writing – original draft, Formal analysis, Validation, Data curation, Project administration. PJ: Writing – review & editing, Software, Writing – original draft, Formal analysis, Data curation, Validation, Investigation. AA: Methodology, Conceptualization, Investigation, Validation, Writing – review & editing. LB: Validation, Writing – review & editing, Conceptualization. ABl: Methodology, Validation, Investigation, Writing – review & editing, Conceptualization. HB: Project administration, Validation, Data curation, Writing – review & editing, Investigation, Software. CJ: Software, Investigation, Writing – review & editing, Supervision, Conceptualization, Formal analysis, Data curation, Validation. JE: Validation, Writing – review & editing, Investigation, Conceptualization. HP: Supervision, Investigation, Conceptualization, Validation, Writing – review & editing. ET: Conceptualization, Writing – review & editing, Investigation, Validation. ÅW: Conceptualization, Validation, Writing – review & editing. CS: Data curation, Validation, Writing – review & editing, Methodology, Supervision, Investigation, Conceptualization. ABe: Writing – review & editing, Writing – original draft, Investigation, Formal analysis, Conceptualization, Validation, Methodology.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The study was supported by the Swedish Heart and Lung Foundation (grant number 20160090) and through the Regional Agreement on Medical Training and Clinical Research (ALF) between Stockholm County Council and Karolinska Institutet (grant numbers FoUI-951900, FoUI-971259). The founders did not engage in study design, data collection, or data analysis.
Acknowledgments
We would like to acknowledge all the participants in this study, the individuals involved in the BRONCHO-SCAPIS research team, and those involved in the bronchoscopy procedures.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1648729/full#supplementary-material
Abbreviations
BAL, Bronchoalveolar lavage; BMI, Body Mass Index; BD, Bronchodilator; COPD, Chronic obstructive pulmonary disease; ECG, Electrocardiogram; FEV1, Forced expiratory volume in first second; FVC, Forced vital capacity; ICS, Inhaled corticosteroids; IQR, Interquartile range; MRC, Medical Research Council; n, Numbers; PBS, Phosphate-buffered saline; SaO2, Oxygen saturation; SD, Standard deviation; SPSS, The Statistical Package for the Social Sciences.
Footnotes
References
1. Stahl, DL, Richard, KM, and Papadimos, TJ. Complications of bronchoscopy: a concise synopsis. Int J Crit Illn Inj Sci. (2015) 5:189–95. doi: 10.4103/2229-5151.164995
2. Leiten, EO, Eagan, TML, Martinsen, EMH, Nordeide, E, Husebø, GR, Knudsen, KS, et al. Complications and discomfort after research bronchoscopy in the MicroCOPD study. BMJ Open Respir Res. (2020) 7:e000449. doi: 10.1136/bmjresp-2019-000449
3. Karewicz, A, Faber, K, Karon, K, Januszewska, K, Ryl, J, Korczynski, P, et al. Evaluation of patients' satisfaction with bronchoscopy procedure. PLoS One. (2022) 17:e0274377. doi: 10.1371/journal.pone.0274377
4. Huang, CT, Chou, RJ, Hu, GN, Lee, TC, Tsai, YJ, and Ho, CC. Patient experience with bronchoscopy: topical versus monitored anesthesia. BMC Pulm Med. (2024) 24:164. doi: 10.1186/s12890-024-02954-6
5. Kaawa-Mafigiri, D, Nsereko, M, Odie, M, and Johnson, JL. Perceptions about and reasons for participation in research bronchoscopy in Uganda: a qualitative analysis. PLoS One. (2023) 18:e0293174. doi: 10.1371/journal.pone.0293174
6. Bouida, W, Grissa, MH, Zorgati, A, Beltaief, K, Boubaker, H, Sriha, A, et al. Willingness to participate in health research: Tunisian survey. BMC Med Ethics. (2016) 17:47. doi: 10.1186/s12910-016-0131-3
7. Doshi, MS, Kulkarni, SP, Ghia, CJ, Gogtay, NJ, and Thatte, UM. Evaluation of factors that motivate participants to consent for non-therapeutic trials in India. J Med Ethics. (2013) 39:391–6. doi: 10.1136/medethics-2012-100755
8. Martinsen, EMH, Eagan, TML, Leiten, EO, Nordeide, E, Bakke, PS, Lehmann, S, et al. Motivation and response rates in bronchoscopy studies. Multidiscip Respir Med. (2019) 14:14. doi: 10.1186/s40248-019-0178-3
9. Aljohaney, AA. Levels and predictors of patient satisfaction during flexible bronchoscopy procedures. Niger J Clin Pract. (2023) 26:508–14. doi: 10.4103/njcp.njcp_545_20
10. Bergström, G, Berglund, G, Blomberg, A, Brandberg, J, Engström, G, Engvall, J, et al. The Swedish CArdioPulmonary BioImage study: objectives and design. J Intern Med. (2015) 278:645–59. doi: 10.1111/joim.12384
11. Sönnerfors, P, Jacobson, PK, Andersson, A, Behndig, A, Bjermer, L, Blomberg, A, et al. The challenges of recruiting never-smokers with chronic obstructive pulmonary disease from the large population-based Swedish CArdiopulmonary bioImage study (SCAPIS) cohort. Eur Clin Respir J. (2024) 11:2372903. doi: 10.1080/20018525.2024.2372903
12. Quanjer, PH, Tammeling, GJ, Cotes, JE, Pedersen OFPeslin, R, and Yernault, JC. Lung volumes and forced ventilatory flows. Eur Respir J Suppl. (1993) 16:5–40. doi: 10.1183/09041950.005s1693
13. Stanojevic, S, Quanjer, P, Miller, MR, and Stocks, J. The global lung function initiative: dispelling some myths of lung function test interpretation. Breathe. (2013) 9:462–74. doi: 10.1183/20734735.012113
14. Eriksson Ström, J, and Behndig, A. Willingness to Participate in Research Bronchoscopy. Poster at the Swedish Lung Congress; Gothenburg: Umeå University, (2015).
15. Li, C, Zhu, T, Ma, D, Chen, Y, and Bo, L. Complications and safety analysis of diagnostic bronchoscopy in COPD: a systematic review and meta-analysis. Expert Rev Respir Med. (2022) 16:555–65. doi: 10.1080/17476348.2022.2056023
16. Saxon, C, Fulbrook, P, Fong, KM, and Ski, CF. High-risk respiratory patients' experiences of bronchoscopy with conscious sedation and analgesia: a qualitative study. J Clin Nurs. (2018) 27:2740–51. doi: 10.1111/jocn.14120
17. Kellogg, D 3rd, Maselli, D, Proud, K, Arnett, E, Schlesinger, LS, and Peters, JI. Bronchoscopy without sedation in healthy volunteers: a viable approach for research. CHEST Pulm. (2024) 2:100075. doi: 10.1016/j.chpulm.2024.100075
18. McCallum, AD, Nyirenda, D, Lora, W, Khoo, SH, Sloan, DJ, Mwandumba, HC, et al. Perceptions of research bronchoscopy in Malawian adults with pulmonary tuberculosis: a cross-sectional study. PLoS One. (2016) 11:e0165734. doi: 10.1371/journal.pone.0165734
19. Kareem, RS, Baram, A, and Saeed, SR. Importance of pre-procedure counselling in patients undergoing flexible bronchoscopy. Indian J Otolaryngol Head Neck Surg. (2023) 75:1894–9. doi: 10.1007/s12070-023-03767-5
20. Leiten, EO, Martinsen, EM, Bakke, PS, Eagan, TM, and Grønseth, R. Complications and discomfort of bronchoscopy: a systematic review. Eur Clin Respir J. (2016) 3:33324. doi: 10.3402/ecrj.v3.33324
21. Stather, DR, MacEachern, P, Chee, A, Dumoulin, E, and Tremblay, A. Trainee impact on procedural complications: an analysis of 967 consecutive flexible bronchoscopy procedures in an interventional pulmonology practice. Respiration. (2013) 85:422–8. doi: 10.1159/000346650
22. Yang, IA, Jenkins, CR, and Salvi, SS. Chronic obstructive pulmonary disease in never-smokers: risk factors, pathogenesis, and implications for prevention and treatment. Lancet Respir Med. (2022) 10:497–511. doi: 10.1016/S2213-2600(21)00506-3
23. Hirose, T, Okuda, K, Ishida, H, Sugiyama, T, Kusumoto, S, Nakashima, M, et al. Patient satisfaction with sedation for flexible bronchoscopy. Respirology. (2008) 13:722–7. doi: 10.1111/j.1440-1843.2008.01311.x
24. Jones, PW, Harding, G, Berry, P, Wiklund, I, Chen, WH, and Kline, LN. Development and first validation of the COPD assessment test. Eur Respir J. (2009) 34:648–54. doi: 10.1183/09031936.00102509
25. Graneheim, UH, and Lundman, B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. (2004) 24:105–12. doi: 10.1016/j.nedt.2003.10.001
Keywords: research bronchoscopy, participants’ experiences, airway sampling, research setting, patient information
Citation: Sönnerfors P, Jacobson PK, Andersson A, Bjermer LH, Blomberg A, Blomqvist H, Janson C, Erjefält JS, Persson HL, Tufvesson E, Wheelock ÅM, Sköld CM and Behndig A (2025) Swedish study participants undergoing research bronchoscopy – a tolerable or unpleasant experience? Front. Med. 12:1648729. doi: 10.3389/fmed.2025.1648729
Edited by:
Somchai Amornyotin, Mahidol University, ThailandReviewed by:
Fumi Kobayashi, Kyorin Daigaku Inokashira Toshokan, JapanDilan Akyurt, Anatolia Hospital, Türkiye
Copyright © 2025 Sönnerfors, Jacobson, Andersson, Bjermer, Blomberg, Blomqvist, Janson, Erjefält, Persson, Tufvesson, Wheelock, Sköld and Behndig. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pernilla Sönnerfors, cGVybmlsbGEuc29ubmVyZm9yc0BraS5zZQ==
†ORCID: Petra Kristina Jacobson, orcid.org/0000-0001-8550-2568
Hans Lennart Persson, orcid.org/0000-0002-5700-7284
Annelie Behndig, orcid.org/0000-0002-1533-9002