Abstract
Background and aims:
The management of Helicobacter pylori (H. pylori) in patients with inflammatory bowel disease (IBD) presents a common clinical dilemma. While standard guidelines recommend H. pylori eradication to prevent gastric pathology, emerging evidence suggests a potential complex relationship with IBD. This study aims to critically evaluate this relationship through an updated systematic review and meta-analysis to inform clinical decision-making.
Methods:
A comprehensive literature search on four major databases, PubMed, Embase, Medline, and Web of Science, was conducted, and all records before July 10th, 2025, were retrieved for screening. Pooled odds ratios (OR) with 95% confidence intervals (CIs) were calculated using STATA 18 software and a random-effects model (Restricted Maximum Likelihood, REML). Subgroup analyses, meta-regression, heterogeneity, sensitivity, and publication bias analyses were performed.
Results:
Analysis of 44 studies involving 14,100 IBD patients and 291,352 controls revealed a significantly lower prevalence of H. pylori infection in IBD patients compared to controls (13.48% vs. 10.87%; OR: 0.43, 95% CI: 0.35–0.53, p < 0.01). This negative association was particularly strong for Crohn’s disease (OR: 0.36, 95%CI: 0.28–0.45) and in Eastern populations (OR: 0.34, 95%CI: 0.26–0.40). Heterogeneity was high (I2 = 84.93%), but sensitivity analysis confirmed the robustness of the findings. No significant publication bias was detected.
Conclusion:
This meta-analysis demonstrates a significant negative association between H. pylori infection and IBD, particularly in patients with Crohn’s disease and those of Eastern population. Furthermore, H. pylori may exert a potential immunomodulatory role in IBD.
Systematic review registration:
https://www.crd.york.ac.uk/PROSPERO/view/CRD42024567688, CRD42024567688.
1 Introduction
The management of Helicobacter pylori infection in patients with inflammatory bowel disease (IBD) represents a growing clinical challenge. IBD is a chronic inflammatory condition of the gastrointestinal tract that requires long-term management (1, 2). The highest incidence rate of the disease occurs in early adulthood (3). The three major forms of IBD are Crohn’s disease (CD), Ulcerative colitis (UC), and IBD unclassified (IBDU). Currently, the definitive etiology of IBD is still unknown. However, genetic susceptibility of the host, intestinal microbiota, other environmental factors (e.g., diet, smoking, and physiological stress), and immunological abnormalities are aspects generally associated with the onset of IBD. Common controlling medications to stop the disease from developing into active phase, including 5-aminosalicylates, steroids, Immunosuppressive drugs, and biological agents (monoclonal antibodies, etc.), only target the inflammatory process and are often unsatisfactory in their results.
H. pylori infection can lead to upper gastrointestinal disorders, including chronic gastritis, peptic ulcer disease, gastric mucosa-associated lymphoid tissue (MALT) lymphoma, and gastric cancer (4). The Kyoto global consensus on H. pylori gastritis advocates eradication therapy for all infected individuals unless there are competing considerations, despite potential adverse effects including obesity, allergy, and perturbation of the intestinal microbiota (5).
The potential protective effect of H. pylori for IBD has been suspected after a series of observational studies spanning nearly three decades. Ormand et al. were the first to examine the relationship between H. pylori infection and different forms of gastritis, including Crohn’s Disease, in 1991 (6). In 1994, El-Omar et al. explicitly revealed a lower prevalence of H. pylori among IBD patients (7). The most recently published study related to the topic was by Garka-Pakulska et al., who took it a step further by comparing the endoscopic presentation between H. pylori positive and negative individuals with IBD (8).
The abundance of original studies has provided a valuable opportunity for statistical analysis. Several systematic reviews and meta-analyses exploring a possible connection between H. pylori and IBD have been published (9–19), with one in 2023 analyzing the situation in the child population. Most of these favored a potential protective role of H. pylori, except for the aforementioned pediatric study, which reported no significant correlation between H pylori infection and IBD (11). The objective of this systematic review and meta-analysis is to address this clinical question by providing an updated, comprehensive assessment of the relationship between H. pylori infection and IBD, incorporating the most recent evidence to guide clinical decision-making.
2 Methods
This systematic review and meta-analysis was conducted and reported under the requirements of the 2020 Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement (20). The protocol of this study was registered in the International Prospective Register of Systematic Reviews, PROSPERO, registration ID CRD42024567688.
2.1 Search strategy
Literature search was performed in four major medical-related databases: PubMed, Embase, Medline, and Web of Science, with language restricted to English and all records dated before July 10th, 2025, retrieved for screening. The search syntax was constructed based on Medical Subject Headings (MeSH) and relevant free words, including but not limited to ‘Crohn Disease’, ‘Crohn’s disease’, ‘Crohn’s Enteritis’, ‘Regional Enteritis’, ‘Granulomatous Enteritis’, ‘Terminal Ileitis’, ‘Colitis, Ulcerative’, ‘Idiopathic Proctocolitis’, ‘Ulcerative Colitis’, ‘Colitis Gravis’, ‘Inflammatory Bowel Diseases’, ‘Helicobacter pylori’, ‘Helicobacter nemestrinae’, and ‘Campylobacter pylori’, connected by Boolean operators. Supplementary material S1 provides the complete search syntax used for all databases.
2.2 Study selection
Observational studies regarding the association between H. pylori infection and IBD (CD, UC, or IBDU) were selected meticulously by two reviewers (Y. S. and Y. B.) who were trained on the eligibility criteria using EndNote X9 (Clarivate, London). The “find duplicates” function in EndNote X9 was utilized before the two reviewers independently reinspected the whole list of entries manually for any duplicates. Independent screening of the articles based on the relevance of the title, abstract, and full text was performed by the two reviewers, with any disagreements in the opinion were settled by consulting another senior reviewer (J. Z.) and consensus.
The inclusion criteria for studies were as follows: (1)The study was an observational study of a cohort, case–control, or cross-sectional design, carried out not on an entirely pediatric population; (2) The study included patients with the diagnosis of IBD, including CD, UC, and IBDU; (3) The status of H. pylori infection of study subjects were detected using one of the following techniques: urease breath test(UBT), rapid urease test(RUT), polymerase chain reaction(PCR), stool antigen testing, serological examination with enzyme-linked immunosorbent assay(ELISA), histology, or culture; (4) H. pylori infection status was reported in either numbers of infected individuals or OR with 95% CI; (5) The study was published as a peer-reviewed full text article. Exclusion criteria comprised study that: (1) performed on animal models or cell strains; (2) included primarily a pediatric population; (3) without the availability of the complete data; (4) not in the English language; (5) of publication types of conference proceedings, comments, letters, editorials.
2.3 Data extraction
Reviewers (Y. S. and Y. B.) independently extracted the data using a pre-designed Microsoft Excel sheet. Disagreements were settled by consulting another senior reviewer (J. Z.) and consensus. The first author’s family name, journal title, article title, country, region, the time of publication for each study, the definition of IBD adopted in the study, the categories of IBD, the detection methods for H. pylori, the sample size of each study, the age of participants, and study outcome (numbers, or ORs with 95% CI) were extracted.
2.4 Risk of bias assessment
Risk of bias assessment was performed by reviewers (Y. S. and Y. B.) using the Newcastle-Ottawa-Scale (NOS), a judgment framework based on the selection of the study groups, and the measurement of the exposure status, with a maximum of 9 stars. A study that scored 7 stars or higher was defined as high quality. Any disagreements in the assessment result were settled by consulting the senior reviewer (J. Z.) and consensus.
2.5 Data analysis
Data were analyzed using STATA 18 (StataCorp LP, College Station, Texas). Odds ratio (OR) with a 95% confidence interval (CI) was adopted as the effect measure for all meta-analyses. Heterogeneity was measured with the Cochrane Q p-value and the Higgins I2 statistics (21). Significant heterogeneity was defined as a Cochrane Q p-value < 0.05 or Higgins I2 > 50%. Considering the original studies varied greatly in various aspects, including the demographical composition of subjects, subtypes and definition of IBD, and H. pylori testing methods, a random-effect model was used as a default for data synthesis. Statistical significance was defined as a p-value less than 0.05. Sensitivity analyses were conducted by excluding low-quality studies and those with a sample size of less than 100, and a leave-one-out sensitivity analysis was additionally performed to evaluate the robustness of the pooled results. Meta-analysis and leave-one-out sensitivity analysis results were visually presented with forest plots. Data were stratified according to: (a) IBD subtype; (b) Study design; (c) Age stratification; (d) Age difference; (e) Ethnicity; (f) H. pylori detection method; (g) Definition of IBD; (h) Quality based on the risk of bias; and (i) Source of control, to enable subgroup analyses and meta-regression to determine the underlying source of heterogeneity. Difference between subgroups was analyzed with the test of group differences in STATA. Publication bias was assessed visually with a funnel plot and quantitatively with Egger’s test.
3 Results
3.1 Study selection
Database search yielded 6,951 entries (Figure 1). After removing 2,234 duplicates, 4,717 entries with unique titles were screened. 137 studies investigating the relation between H. pylori infection and IBD were retrieved for their potential eligibility. Of these, 46 studies met the inclusion criteria. After carefully reviewing the original studies, two studies conducted by Sonnenberg et al. were found to have potentially overlapping sample populations with another two and were therefore excluded (22, 23). Thus, 44 studies with complete full-text articles and available data were finally included.
Figure 1

PRISMA flow diagram of the current systematic review and meta-analysis (Comprehensive search of the databases was completed on July 10th, 2025).
3.2 Characteristics of the included studies
The 44 included studies all had a case–control design. Total case and control numbers were 14,100 and 291,352, respectively. Among these, 36 studies included CD (7, 8, 24–56), 29 included UC (7, 26–29, 31–33, 37, 38, 40–42, 45, 47–50, 53–63), and 5 included IBDU (40, 50, 54, 56, 64). Due to the scarcity of original studies analyzing IBDU as an individual entity, statistics of studies conducted on Microscopic Colitis (MC) have been included and merged to the IBD unclassified group due to its unique characteristics, which share some similarities with IBDU. Two studies conducted by Sonnenberg et al. had overlapping sample populations, and was therefore excluded (22, 23). Two studies did not differentiate between the subtypes of IBD (65, 66). Two studies included by Oliveira et al. shared the same control group of 76 individuals (44, 60). The majority of studies (24/44) were conducted on the Western population, with 12 on the Eastern population, 8 on the other population. IBD was defined using a reliable medical registry in 26 studies and colonoscopy/biopsy in 14. Four studies did not detail the definition of IBD in the respective settings. Regarding the ascertainment of H. pylori infection, 15 of the included studies incorporated UBT into the testing scheme, 2 adopted stool antigen testing, 17 included invasive testing methods that required endoscopic biopsy, and 16 utilized serology. Nine studies used more than one detection methods for H. pylori. The general information of the included studies is listed in Table 1.
Table 1
| Author | Publishing year | Journal | Region | NOS Score | IBD diagnosis | Type | Hp diagnosis method | Case | Control | Total |
|---|---|---|---|---|---|---|---|---|---|---|
| El-Omar et al. (7) | 1994 | Gut | UK | 6 | Not Mentioned | CD/UC | Serology/14C-UBT/histology | 110 | 100 | 210 |
| Halme et al. (33) | 1996 | Journal of Clinical Pathology | Finland | 7 | Registry/Medical Record | CD/UC | Serology | 200 | 100 | 300 |
| Meining et al. (34) | 1997 | Scandinavian Journal of Gastroenterology | Germany | 6 | Colonoscopy & Biopsy | CD | Histology | 36 | 36 | 72 |
| Oberhuber et al. (35) | 1997 | Gastroenterology | Germany | 6 | Registry/Medical Record | CD | Histology | 75 | 193 | 268 |
| Parente et al. (61) | 1997 | Scandinavian Journal of Gastroenterology | Italy | 7 | Registry/Medical Record | CD/UC | Serology | 216 | 216 | 432 |
| M. J. Wagtmans et al. (36) | 1997 | Scandinavian Journal of Gastroenterology | Netherlands | 7 | Registry/Medical Record | CD | Serology | 386 | 277 | 663 |
| D’Incà et al. (26) | 1998 | Digestive Diseases and Sciences | Italy | 6 | Registry/Medical Record | CD/UC | Histology | 108 | 43 | 151 |
| Duggan et al. (29) | 1998 | Gut | UK | 7 | Registry/Medical Record | CD/UC | Serology | 257 | 174 | 431 |
| Parente et al. (37) | 2000 | American Journal of Gastroenterology | Italy | 7 | Registry/Medical Record | CD/UC | 13C-UBT/histology | 220 | 141 | 361 |
| Pearce et al. (38) | 2000 | European Journal of Gastroenterology & Hepatology | UK | 5 | Registry/Medical Record | CD/UC | Serology/13C-UBT | 93 | 40 | 133 |
| Matsumura et al. (39) | 2001 | Journal of Gastroenterology | Japan | 5 | Registry/Medical Record | CD | Serology | 90 | 525 | 615 |
| Väre et al. (40) | 2001 | Scandinavian Journal of Gastroenterology | Finland | 7 | Registry/Medical Record | CD/UC/IBDU | Serology | 296 | 70 | 366 |
| Feeney et al. (31) | 2002 | European Journal of Gastroenterology and Hepatology | UK | 6 | Registry/Medical Record | CD/UC | Serology | 276 | 276 | 552 |
| Piodi et al. (41) | 2003 | Journal of Clinical Gastroenterology | Italy | 7 | Registry/Medical Record | CD/UC | 13C-UBT | 72 | 72 | 144 |
| Prónai et al. (42) | 2004 | Helicobacter | Hungary | 6 | Registry/Medical Record | CD/UC | 13C-UBT | 133 | 200 | 333 |
| Oliveira et al. (60) | 2004 | Journal of clinical microbiology | Brazil | 5 | Colonoscopy & Biopsy | UC | Serology/13C-UBT | 42 | 74 | 116 |
| Moriyama et al. (43) | 2005 | Alimentary Pharmacology & Therapeutics | Japan | 7 | Registry/Medical Record | CD | 13C-UBT | 29 | 7 | 36 |
| Oliveira et al. (44) | 2006 | Helicobacter | Brazil | 6 | Colonoscopy & Biopsy | CD | Serology/13C-UBT | 43 | 74 | 117 |
| Ando et al. (24) | 2008 | Journal of Gastroenterology and Hepatology | Japan | 7 | Not Mentioned | CD | 13C-UBT/Histology | 38 | 12 | 50 |
| Ando et al. (45) | 2008 | Digestion | Japan | 6 | Not Mentioned | UC/CD | 13C-UBT | 52 | 26 | 78 |
| Laharie et al. (46) | 2009 | Alimentary Pharmacology & Therapeutics | France | 6 | Colonoscopy & Biopsy | CD | PCR | 73 | 92 | 165 |
| Lidar et al. (47) | 2009 | Contemporary Challenges in Autoimmunity | Italy | 8 | Not Mentioned | IBD | Serology | 119 | 98 | 217 |
| Song et al. (48) | 2009 | The Korean journal of gastroenterology | Korea | 7 | Registry/Medical Record | CD/UC | UBT | 316 | 316 | 632 |
| Cheul Ho Hong et al. (63) | 2009 | The Korean journal of gastroenterology | Korea | 6 | Colonoscopy & Biopsy | UC/CD | Histology | 80 | 41 | 121 |
| Garza- González et al. (32) | 2010 | International Journal of Immunogenetics | Mexico | 7 | Registry/Medical Record | CD/UC | Serology | 44 | 75 | 119 |
| Koskela et al. (64) | 2011 | Scandinavian Journal of Gastroenterology | Finland | 7 | Colonoscopy & Biopsy | IBDU | Histology | 72 | 60 | 132 |
| J. M. Thomson et al. (59) | 2011 | PLoS ONE | UK | 6 | Registry/Medical Record | UC | FISH | 57 | 49 | 106 |
| Zhang et al. (49) | 2011 | Journal of Clinical Microbiology | China | 7 | Colonoscopy & Biopsy | CD/UC | 13C-UBT | 208 | 416 | 624 |
| Sonnenberg et al. (50) | 2012 | Alimentary Pharmacology and Therapeutics | USA | 7 | Registry/Medical Record | CD/UC/IBDU | Histology | 1,064 | 64,451 | 65,515 |
| Jin et al. (58) | 2013 | International Journal of Medical Sciences | China | 7 | Colonoscopy & Biopsy | UC | 14C-UBT/histology | 153 | 121 | 274 |
| Xiang et al. (51) | 2013 | World Journal of Gastroenterology | China | 6 | Colonoscopy & Biopsy | CD | 14C-UBT/Culture | 229 | 248 | 477 |
| M. Ram et al. (65) | 2013 | Clinical Chemistry and Laboratory Medicine | Europe | 6 | Registry/Medical Record | IBD | Serology | 119 | 245 | 364 |
| Magalhã es-Costa et al. (27) | 2014 | Arquivos de Gastroenterologia | Brazil | 7 | Colonoscopy & Biopsy | CD/UC | Histology | 57 | 26 | 83 |
| Farkas et al. (30) | 2016 | Journal of Crohn’s and Colitis | Hungary/ Hong Kong | 6 | Registry/Medical Record | CD | Histology | 180 | 189 | 369 |
| Mansour et al. (62) | 2018 | World Journal of Clinical Cases | Egypt | 6 | Registry/Medical Record | UC | Histology | 30 | 30 | 60 |
| Rosania et al. (55) | 2018 | Journal of Gastrointestinal and Liver Diseases | Germany | 7 | Registry/Medical Record | CD/UC | Serology | 127 | 254 | 381 |
| Sonnenberg et al. (54) | 2018 | Colorectal Disease | USA | 6 | Registry/Medical Record | CD/UC/IBDU | Histology | 7,684 | 220,822 | 228,506 |
| R. Sayar et al. (66) | 2019 | Caspian Journal of Internal Medicine | Iran | 7 | Colonoscopy & Biopsy | IBD | Serology | 60 | 120 | 180 |
| M. Varas Lorenzo et al. (56) | 2019 | Eurasian Journal of Medicine and Oncology | Spain | 5 | Registry/Medical Record | CD/UC/IBDU | 13C-UBT | 95 | 20 | 115 |
| J. Ostrowski et al. (52) | 2021 | Scientific Reports | Poland | 6 | Registry/Medical Record | CD | RUT/Sequencing | 24 | 19 | 43 |
| Ding et al. (28) | 2021 | Plos One | China | 7 | Registry/Medical Record | CD/UC | Serology | 260 | 520 | 780 |
| Ali et al. (57) | 2022 | Heliyon | Palestine | 7 | Colonoscopy & Biopsy | UC | stool antigen test (SAT) | 35 | 105 | 140 |
| Graca-Pakulska et al. (8) | 2023 | Scientific reports | Poland | 6 | Registry/Medical Record | CD | RUT | 62 | 199 | 261 |
| Alotaibi et al. (53) | 2025 | BMC Gastroenterology | Saudi Arabia | 7 | Colonoscopy & Biopsy | CD/UC | stool antigen test (SAT) | 180 | 180 | 360 |
| Total | 14,100 | 291,352 | 305,452 |
Main characteristics of the included studies in this meta-analysis on Helicobacter pylori infection and IBD.
IBD, Inflammatory Bowel Diseases; Hp, Helicobacter pylori; Ag, Antigen; CD, Crohn’s Disease; UC, Ulcerative Colitis; IBDU, Inflammatory Bowel Diseases Unclassified; UBT, Urease Breath Test; RUT, Rapid Urease Test; PCR, Polymerase Chain Reaction; FISH, Fluorescence In Situ Hybridization.
3.3 Risk of bias assessment result
All included studies were subject to the risk of bias assessment with the Newcastle-Ottawa-Scale (NOS). The overall quality of the recruited studies was satisfactory, with 40 studies scoring over 6 stars (40/44, 90.91%) and half (22/44, 50.00%) scoring 7 stars or higher. When leave-one-out sensitivity analyses were conducted, all the results remained significant in both the overall and stratified analyses, indicating statistical robustness.
3.4 Association between Helicobacter pylori infection and IBD
The total study sample included 14,100 patients with IBD and 291,352 non-IBD controls. The population in most of the studies were middle-aged individuals. Data synthesis revealed a negative association between H. pylori infection and the condition of IBD (pooled OR:0.43, 95%CI: 0.35–0.53, p < 0.01; Figure 2A). Heterogeneity was high (I2 = 84.93%). The statistical robustness of the meta-analysis of H. pylori infection and IBD in the target population was proven with leave-one-out sensitivity analysis (Figure 2B).
Figure 2
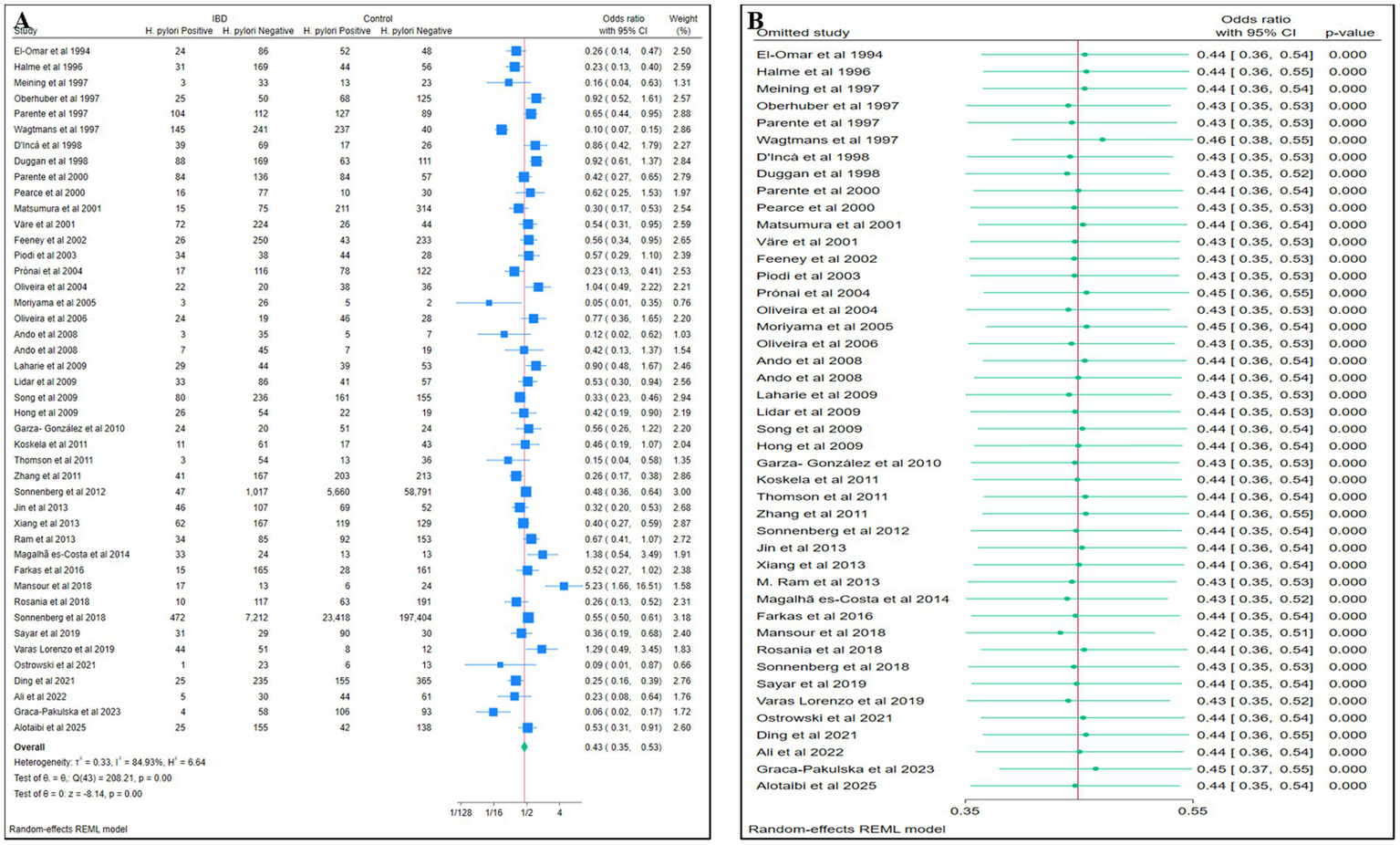
(A) Forest plots of the meta-analysis of H. pylori infection and IBD. (B) Leave-one-out sensitivity analysis.
3.5 Subgroup analyses
To explore potential sources of heterogeneity, we performed subgroup analyses across 9 dimensions, calculating pooled odds ratios (ORs) with 95% confidence intervals (CIs) and heterogeneity metrics (Cochrane’s Q, τ2, I2). Differences between subgroups were tested, and leave-one-out sensitivity analyses were conducted.
A negative association between H. pylori infection and IBD was consistently observed across all subgroups (Figure 3; Table 2). This association was strongest in CD (pooled OR: 0.36, 95% CI: 0.28–0.45), followed by UC (pooled OR: 0.51, 95% CI: 0.38–0.69) and IBDU (pooled OR: 0.54, 95% CI: 0.48–0.61). Heterogeneity was high in the CD and UC subgroups but substantially lower in the IBDU subgroup.
Figure 3
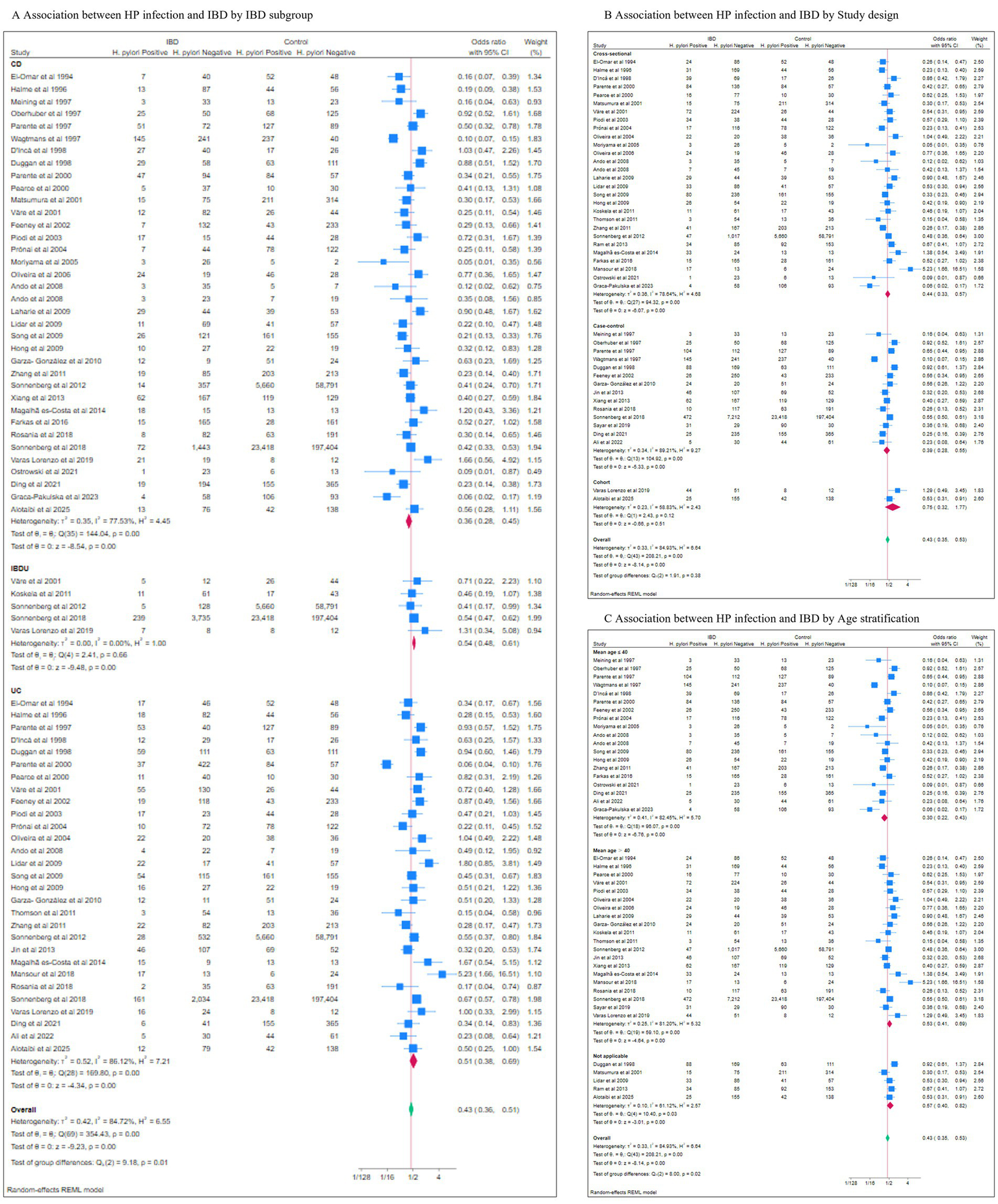
The results of different subgroup of analysis. (A) IBD subgroup; (B) Study design; (C) Age stratification.
Table 2
| Subgroups | No. of studies | No. of cases | No. of controls | Q | p value | τ2 | I2(%) | OR 95%CI | p value | Test of group difference (P) |
|---|---|---|---|---|---|---|---|---|---|---|
| All studies | 44 | 14,100 | 291,352 | 208.21 | <0.01 | 0.33 | 84.93 | 0.43 (0.35,0.53) | <0.01 | |
| IBD subtype | 0.01 | |||||||||
| CD | 36 | 4,954 | 290,549 | 144.04 | <0.01 | 0.35 | 77.53 | 0.36 (0.28,0.45) | <0.01 | |
| UC | 29 | 4,756 | 289,056 | 169.80 | <0.01 | 0.52 | 86.12 | 0.51 (0.38,0.69) | <0.01 | |
| IBDU | 5 | 4,211 | 285,423 | 2.41 | 0.66 | 0.00 | 0.00 | 0.54 (0.48,0.61) | <0.01 | |
| Study design | 0.38 | |||||||||
| Cross-sectional | 28 | 3,987 | 67,715 | 94.32 | <0.01 | 0.36 | 78.64 | 0.44 (0.33,0.57) | <0.01 | |
| Case–control | 14 | 9,838 | 223,437 | 104.92 | <0.01 | 0.34 | 89.21 | 0.39 (0.28,0.55) | <0.01 | |
| Cohort | 2 | 275 | 200 | 2.43 | 0.12 | 0.23 | 58.83 | 0.75 (0.32,1.77) | 0.51 | |
| Age stratification | 0.02 | |||||||||
| Mean age ≤ 40 | 19 | 2,734 | 3,232 | 96.07 | <0.01 | 0.41 | 82.45 | 0.30 (0.22,0.43) | <0.01 | |
| Mean age > 40 | 20 | 10,601 | 286,898 | 59.10 | <0.01 | 0.25 | 81.20 | 0.53 (0.41,0.69) | <0.01 | |
| Not applicable | 5 | 765 | 1,222 | 10.40 | 0.03 | 0.10 | 61.12 | 0.43 (0.35,0.53) | <0.01 | |
| Age difference | 0.64 | |||||||||
| Age matched | 35 | 13,435 | 290,532 | 164.42 | <0.01 | 0.25 | 82.89 | 0.42 (0.34,0.51) | <0.01 | |
| Control group is older | 9 | 665 | 820 | 38.82 | <0.01 | 0.86 | 85.25 | 0.50 (0.25,0.97) | 0.04 | |
| Ethnicity | 0.08 | |||||||||
| Western | 24 | 11,816 | 288,233 | 122.09 | <0.01 | 0.28 | 85.00 | 0.46 (0.36,0.59) | <0.01 | |
| Eastern | 12 | 1931 | 2,482 | 15.66 | 0.15 | 0.01 | 16.19 | 0.34 (0.28,0.40) | <0.01 | |
| Others | 8 | 353 | 647 | 41.48 | <0.01 | 1.53 | 87.57 | 0.57 (0.22,1.45) | 0.24 | |
| HP detection method | 0.80 | |||||||||
| Serology | 16 | 2,695 | 3,164 | 97.91 | <0.01 | 0.32 | 81.16 | 0.42 (0.31,0.58) | <0.01 | |
| Non-serology | 28 | 11,405 | 288,188 | 100.99 | <0.01 | 0.37 | 85.79 | 0.45 (0.34,0.59) | <0.01 | |
| Definition of IBD | 0.48 | |||||||||
| Registry/medical record | 26 | 11,449 | 225,072 | 168.41 | <0.01 | 0.53 | 90.76 | 0.42 (0.31,0.58) | <0.01 | |
| Colonoscopy/Biopsy | 14 | 2,332 | 66,044 | 29.51 | <0.01 | 0.11 | 57.47 | 0.48 (0.38,0.62) | <0.01 | |
| Not specified | 4 | 319 | 236 | 4.83 | 0.18 | 0.11 | 37.30 | 0.34 (0.20,0.58) | <0.01 | |
| Quality based on the risk of bias | 0.24 | |||||||||
| High quality (≥7stars) | 22 | 4,409 | 67,811 | 105.18 | <0.01 | 0.25 | 78.60 | 0.39 (0.30,0.50) | <0.01 | |
| Fair quality (≤6stars) | 22 | 9,691 | 223,541 | 76.94 | <0.01 | 0.45 | 86.09 | 0.50 (0.36,0.69) | <0.01 | |
| Source of control | 0.05 | |||||||||
| Healthy | 19 | 2,802 | 2,937 | 93.59 | <0.01 | 0.37 | 81.94 | 0.35 (0.25,0.48) | <0.01 | |
| Other with-out IBD | 25 | 11,298 | 288,415 | 84.97 | <0.01 | 0.25 | 81.64 | 0.52 (0.41,0.66) | <0.01 | |
The results of different subgroup analysis.
IBD, Inflammatory Bowel Diseases; CD, Crohn’s Disease; UC, Ulcerative Colitis; IBDU, Inflammatory Bowel Diseases Unclassified; OR, Odds Ratio; CI, Confidence Interval; HP, Helicobacter pylori.
Stratified analyses by study design, age stratification, age matching, ethnicity, H. pylori detection method, IBD definition, study quality and control source consistently revealed stable negative associations (Table 2). Notably, the association was significantly stronger in studies with younger populations (mean age ≤ 40; OR: 0.30, 95% CI: 0.22–0.43) than in those with older participants (mean age > 40; OR: 0.53, 95% CI: 0.41–0.69; p = 0.02 for subgroup difference). Study design did not significantly modify the effect (p = 0.38). The age-matched subgroup showed an effect size similar to the overall analysis (pooled OR: 0.42, 95% CI: 0.34–0.51, p < 0.01), with no significant between-subgroup difference (p = 0.64). Higher heterogeneity was observed in subgroups with older controls.
Negative association was observed in both Western (pooled OR: 0.46, 95% CI: 0.36–0.59, p < 0.01) and Eastern (pooled OR: 0.34, 95% CI: 0.28–0.40, p < 0.01) populations, but not in the “Others” category (pooled OR: 0.57, 95% CI: 0.22–1.45, p = 0.24). Heterogeneity was notably low in the Eastern subgroups.
When comparing serology-based detection of H. pylori with other methods, the serology subgroup exhibited a marginally stronger negative association (pooled OR: 0.42, 95% CI: 0.31–0.58, p < 0.01) than the non-serology subgroup (pooled OR: 0.45, 95% CI: 0.34–0.59, p < 0.01). Heterogeneity remained high in both, though sensitivity analyses confirmed result stability (Figure 4).
Figure 4
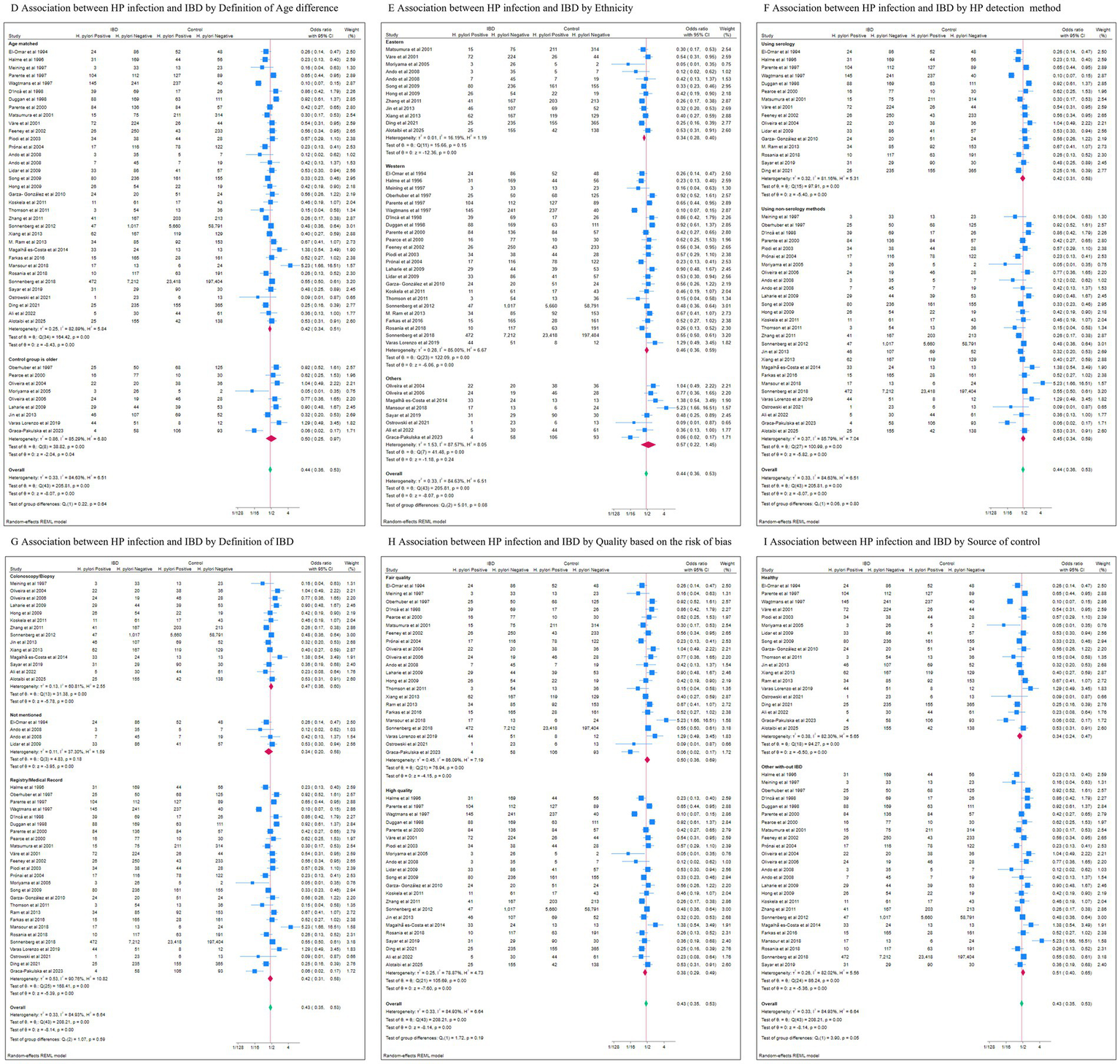
The results of different subgroup of analysis. (D) Age difference; (E) Ethnicity; (F) HP detection method; (G) Definition of IBD; (H) Quality based on the risk of bias; (I) Source of control.
Most included studies defined IBD using either Registry/Hospital Record or Colonoscopy/Biopsy. Although the colonoscopy/biopsy subgroup was associated with lower heterogeneity, the effect sizes in both subgroups were comparable (Colonoscopy/Biopsy subgroup: pooled OR: 0.48, 95% CI: 0.38–0.62, p < 0.01; Registry/Medical Record subgroup: pooled OR: 0.42, 95% CI: 0.31–0.58, p < 0.01), with no statistically significant between-subgroup difference (p = 0.48).
A stronger negative association and lower heterogeneity level were observed in the high-quality subgroup (pooled OR: 0.39, 95% CI: 0.30–0.50, p < 0.01) compared to the fair-quality subgroup (pooled OR: 0.50, 95% CI: 0.36–0.69, p < 0.01). Similarly, studies using healthy controls demonstrated stronger negative association (pooled OR: 0.35, 95% CI: 0.25–0.48, p < 0.01) than those using non-IBD controls (pooled OR: 0.52, 95% CI: 0.41–0.66, p < 0.01), with a borderline significant subgroup difference (p = 0.05).
Despite extensive stratification, the definitive source of overall heterogeneity remained unexplained. Marked reductions in heterogeneity were observed in subgroups defined by Eastern ethnicity, IBDU diagnosis, colonoscopy-based IBD confirmation, and higher study quality. This pattern suggests that the observed heterogeneity stems from a combination of biological and methodological factors.
3.6 Meta-regression
Meta-regression analysis identified age stratification and control source as significant modifiers of the association between H. pylori infection and IBD: studies with participants aged > 40 years showed a significantly higher effect size (OR = 1.73, 95%CI: 1.13–2.62, p = 0.01), and those using non-IBD controls had a borderline significant higher effect size (OR = 1.48, 95%CI:0.99–2.21, p = 0.05). No significant differences were observed in other variables including IBD subtype, study design, ethnicity, and H. pylori detection method (Table 3).
Table 3
| Subgroups | No. of studies | No. of cases | No. of controls | OR | 95%CI | p value | Egger’s test p value |
|---|---|---|---|---|---|---|---|
| All studies | 44 | 14,100 | 291,352 | 0.72 | |||
| IBD subtype | |||||||
| CD | 36 | 4,954 | 290,549 | 0.69 | 0.48,1.00 | 0.53 | 0.69 |
| UC | 29 | 4,756 | 289,056 | reference | 0.82 | ||
| IBDU | 5 | 4,211 | 285,423 | 1.13 | 0.54,2.36 | 0.74 | 0.64 |
| Study design | |||||||
| Cross-sectional | 28 | 3,987 | 67,715 | reference | 0.57 | ||
| Case–control | 14 | 9,838 | 223,437 | 0.09 | 0.58.1.39 | 0.64 | 0.16 |
| Cohort | 2 | 275 | 200 | 1.76 | 0.64,4.85 | 0.27 | NA |
| Age stratification | |||||||
| Mean age ≤ 40 | 19 | 2,734 | 3,232 | reference | 0.31 | ||
| Mean age > 40 | 20 | 10,601 | 286,898 | 1.73 | 1.13,2.62 | 0.01 | 0.67 |
| Not applicable | 5 | 765 | 1,222 | 1.81 | 0.97,3.34 | 0.06 | 0.28 |
| Age difference | |||||||
| Age matched | 35 | 13,435 | 290,532 | Reference | 0.66 | ||
| Control group is older | 9 | 665 | 820 | 1.27 | 0.76,2.13 | 0.36 | 0.13 |
| Ethnicity | |||||||
| Western | 24 | 11,816 | 288,233 | 0.70 | 0.45,1.11 | 0.13 | 0.94 |
| Eastern | 12 | 1931 | 2,482 | Reference | 0.41 | ||
| Others | 8 | 353 | 647 | 1.31 | 0.73,2.33 | 0.36 | 0.54 |
| HP detection method | |||||||
| Serology | 16 | 2,695 | 3,164 | Reference | 0.96 | ||
| Non-serology | 28 | 11,405 | 288,188 | 1.05 | 0.69,1.59 | 0.79 | 0.39 |
| Definition of IBD | |||||||
| Registry/medical record | 26 | 11,449 | 225,072 | 1.16 | 0.74,1.81 | 0.52 | 0.59 |
| Colonoscopy/Biopsy | 14 | 2,332 | 66,044 | Reference | 0.86 | ||
| Not specified | 4 | 319 | 236 | 0.77 | 0.35,1.69 | 0.51 | 0.49 |
| Quality based on the risk of bias | |||||||
| High quality (≥7stars) | 22 | 4,409 | 67,811 | 1.29 | 0.87,1.93 | 0.20 | 0.26 |
| Fair quality (≤6stars) | 22 | 9,691 | 223,541 | Reference | 0.54 | ||
| Source of control | |||||||
| Healthy | 19 | 2,802 | 2,937 | Reference | 0.65 | ||
| Other with-out IBD | 25 | 11,298 | 288,415 | 1.48 | 0.99,2.21 | 0.05 | 0.20 |
The results of meta-regression and publication bias assessment.
IBD, Inflammatory Bowel Diseases; CD, Crohn’s Disease; UC, Ulcerative Colitis; IBDU, Inflammatory Bowel Diseases Unclassified; OR, Odds Ratio; CI, Confidence Interval; HP, Helicobacter pylori.
3.7 Assessment of publication bias
Publication bias was assessed for the overall set of included studies and for each subgroup. Although the funnel plot appeared slightly asymmetric (Figure 5), Egger’s test revealed no statistically significant evidence of publication bias in the overall analysis (p = 0.72) or in any of the subgroup analyses (Table 3).
Figure 5
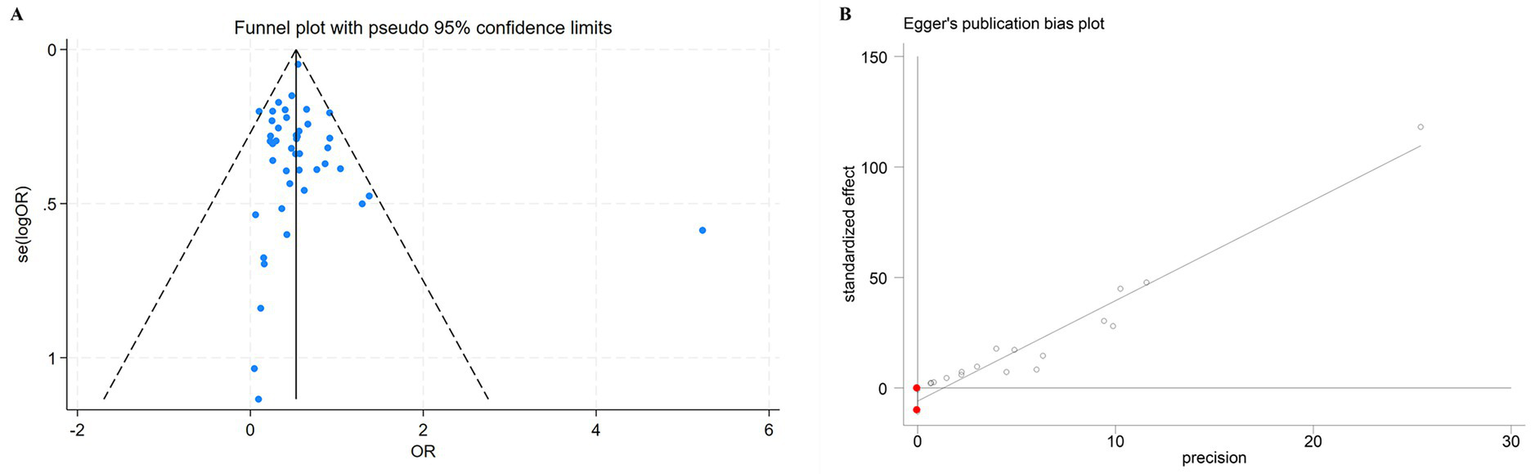
(A) Assessment of publication bias using funnel plots. Each dot represents one study. (B) Egger’s tests were used to verify the possibility of publication bias. The distance between the two red dots on the ordinate represents the 95% confidence interval.
3.8 Sensitivity analysis
Sensitivity analyses confirmed the robustness of the primary findings. Exclusion of 22 lower-quality studies (NOS < 7) yielded a pooled OR of 0.38 (95% CI: 0.29–0.49, p < 0.01) with reduced heterogeneity (I2 = 78.87%). Similarly, excluding 7 studies with sample sizes < 100 (OR: 0.43, 95% CI: 0.35–0.52) or 5 studies with unclear age stratification (“Not Applicable”; OR: 0.41, 95% CI: 0.33–0.52) did not alter the overall conclusion (Supplementary Figures 2–4).
4 Discussion
The current meta-analysis pooled data from 44 original studies published up to July 10th,2025, from 21 countries. The total number of IBD patients and controls were 14,100 and 291,352, respectively. Data synthesis using a random-effect model revealed a significant reduction in the odds of IBD among individuals infected with H. pylori (pooled OR: 0.43, 95%CI: 0.35–0.53, p < 0.01), particularly in CD (pooled OR: 0.36, 95% CI: 0.28–0.45, p < 0.01) and the Eastern population (pooled OR: 0.34, 95% CI: 0.28–0.40, p < 0.01). These results suggested a potential protective effect associated with the pathogen.
H. pylori was negatively associated with several atopic and inflammatory diseases, such as asthma and eczema (67, 68). Hypothesis was that the association may also exist in other Regulatory T cell (Treg)-associated autoimmune diseases. H. pylori’s immunomodulatory effect was modulated by Interleukin (IL)-18-producing, tolerogenic dendritic cells, which were able to induce T-cell conversion toward Foxp3 + Tregs and control the degree of inflammation (69). Recently, the cytotoxin-associated gene A (CagA), an important virulence factor of H. pylori typically associated with an increased risk of gastric cancer, was also found to have immunomodulatory effect. The meta-analysis by Tepler et al. found that serologic response to CagA was related to substantially lower odds of IBD and that individuals exposed to CagA-negative H.pylori were associated with similar odds of IBD to individuals without any exposure to the pathogen, supporting the hypothesis that CagA might be a key determinant in the protective association conferred by H. pylori (14).
The potential protective effect of H. pylori may also be related to the preservation of a healthy gut microbiome. H. pylori may alter gut microbiota and reduce dysbiosis linked to IBD, which typically shows less diversity and abundance than healthy individuals (70). This alteration also reduces the risk of pathogenic bacterial overgrowth and the subsequent immune response leading to chronic intestinal inflammation. However, a direct causal relationship between dysbiosis and IBD has not been definitively established in humans (71). A meta-analysis by Zhong et al. noted a higher recurrence rate of inflammatory bowel disease following Helicobacter pylori eradication, suggesting a potential link to gut microbiota dysbiosis (18).
To explore the sources of the substantial observed heterogeneity (I2 = 84.93%), subgroup analyses were performed based on pre-specified biological and methodological factors. The subgroup analysis stratified data according to 9 biological or methodological factors. Among these, IBD subtype, age stratification and source of control were associated with significant differences between the subgroups. The negative association between H. pylori and IBD was stronger in CD compared to UC and IBDU, and in the Eastern population compared to the Western population, corroborating previous studies (9, 16).
The differences in the disease subtypes could be explained by the immunologic profiles of the two conditions. The pathogenesis of IBD includes an inappropriate immune response generated by the genetically susceptible host to the intestinal microbiome (72, 73). Despite both being a mixed lymphocyte reaction involving Th1, Th2, Th9, Th17, and Treg, CD is characterized by a stronger Th1 response with IL-23/Th17 activation, in comparison to UC, which is predominantly a Th2-like response characterized by increased IL-13 and IL-5 (74, 75).
The difference in CagA expression between Western and Eastern H. pylori strains is possibly another explanation for the ethnic disparity in the result. Nearly 100% of the Eastern strain of H. pylori was found expressing CagA, compared to only 60–70% of the Western strain (76). Therefore, the Eastern population infected by H. pylori may develop a stronger immunomodulatory response with a CagA-positive strain.
Environmental and socioeconomic factors, such as diet and childhood environment, also contribute to the pathogenesis of IBD. The Western diet characterized by lower fiber and higher refined carbohydrates and processed meat is considered conducive to IBD (77). The incidence rates of IBD have been steadily rising in rapidly developing countries where changes in the structure of diet toward the Western style are happening (2). Epidemiological studies conducted on the first and second generations of immigrants from Asia, Latin America, Africa, and the Middle East to Canada found that second-generation immigrants shared a similar incidence rate of IBD with native Canadian children, which was much higher than that in their countries of origin (78).
The more pronounced negative association in younger populations (mean age ≤ 40 years; OR = 0.30) compared to older groups (OR = 0.53) may reflect age-dependent immune responsiveness. H. pylori infection typically occurs in childhood, and early-life exposure may induce long-term immunomodulatory effects (69) that are more effective in preventing the development of IBD, which often onset in early adulthood (14). In older individuals, cumulative environmental exposures, comorbidities, and age-related immune senescence may weaken the protective effect of H. pylori (79). Additionally, older populations may have a higher prevalence of prior H. pylori eradication therapy or spontaneous clearance, which could confound the association (80).
On a methodological level, several factors jointly contribute to the variation in effect sizes. Firstly, the diagnostic methods for defining H. pylori status were not uniform. Serology defines an “exposed” population that differs from those defined by tests for active infection, such as the urea breath test and histology. Secondly, the source of the control group significantly influenced the effect size, with studies using healthy controls demonstrating a stronger inverse association. This phenomenon is likely attributable to Berkson’s bias (81). Non-IBD patients presenting with gastrointestinal symptoms have an inherently higher prevalence of H. pylori infection than the general healthy population. Using this inflated baseline for comparison artificially diminishes the observed difference in infection rates between cases and controls. Thirdly, the effect sizes were similar regardless of whether IBD was defined by colonoscopy/biopsy or registry/medical records (p = 0.48). However, the subgroup using colonoscopy/biopsy was associated with a lower level of heterogeneity, suggesting that more stringent diagnostic criteria contribute to greater consistency in results. Finally, and most critically, many original studies failed to adequately control for or report key confounding variables, such as the use of 5-aminosalicylates commonly prescribed to IBD patients, a history of prior H. pylori eradication therapy, and disease activity at the time of testing. These factors could introduce bias and lead to inconsistencies between studies. Consequently, the pooled effect size presented in this meta-analysis should be interpreted as an overall estimate under the joint influence of these biological and methodological factors. The preceding subgroup analyses were instrumental in deconstructing this complexity and confirming the robustness of the core finding across various contexts.
Being a multifactorial disease, the study of IBD benefits from a large pooled sample size and the inclusion of recent studies. This is the 13th meta-analysis focusing on H. pylori and IBD, and the 9th specifically analyzing the association between H. pylori infection and IBD onset (9–19). Luther et al. (12), in their 2010 study of 5,903 subjects, first reported a statistically significant association between H. pylori and IBD (RR: 0.64, 95%CI:0.54–0.75). This finding was later confirmed by Wu et al. (16)(RR: 0.48, 95%CI:0.43–0.54) and Rokkas et al. (19) (RR: 0.62, 95%CI:0.55–0.71) in 2015. Castaño-Rodríguez et al. (9) not only further validated this negative association (P-OR: 0.43, 95%CI:0.36–0.50), but also verified its robustness across different ethnicities, age groups, and detection methods of H pylori. Recently, Shirzad-Aski et al. conducted a study with the largest pooled sample size (13,549 individuals from 58 studies up to June 2018), which yielded similar results (13). However, in that meta-analysis, two studies conducted by Sonnenberg et al. using the same electronic database with another two in an overlapping time frame were included, raising concerns about data redundancy (50). These studies were excluded in this meta-analysis (22, 23). Compared to the 2020 study by Shirzad-Aski, the current meta-analysis included some of the latest original researches up to July 10th, 2025. Only published resources were sought, and statistical results from conference proceedings, comments, letters, and editorials were excluded for greater statistical robustness. With a stricter inclusion and exclusion criteria and statistical rigor, the current meta-analysis offers a reliable update and extension of the preceding works.
Despite the strengths of this meta-analysis stemming from the comprehensive literature search, rigorous methodological approach, and large sample size, there are still limitations to consider. First, the high heterogeneity among the included studies, which was not effectively addressed by any subgroup analyses, may have introduced bias. Second, in pursuit of statistical robustness, the current meta-analysis sought only published data in peer-reviewed publications, which inevitably lowered the scale of the total sample size. Third, our literature search was restricted to English-language publications. While this ensured accuracy in data handling, it may have introduced language bias by excluding relevant studies published in other languages, particularly from Eastern regions. This could potentially affect the generalizability of our findings. However, the consistent negative association observed specifically within the Eastern subgroup, derived from a substantial number of English-language studies conducted in those regions, suggests that the core finding remains robust. Moreover, most observational studies not containing sufficient background data during their publication had limited further exploration of heterogeneity sources. These missing data included but were not limited to: the exact timing of pylori testing in relation to the diagnosis of IBD, the history of H. pylori eradication, the extent and severity of IBD according to the Montreal Classification, and the detailed medication history. However, it should be acknowledged that since the investigation on the relationship between H. pylori and IBD has spanned nearly 3 decades and the concepts and therapeutic techniques have been constantly evolving, setting too high a bar for certain previous studies is unreasonable. Hopefully, future studies will document or control for these factors, helping elucidate the true nature of the relationship between H. pylori infection and IBD. Besides, despite being statistically insignificant, the effect of publication bias should not be neglected. Finally, although this meta-analysis confirms a negative association between H. pylori infection and IBD, as with all epidemiological studies, this association does not necessarily imply causality and should be interpreted cautiously.
In conclusion, this meta-analysis demonstrates a significant negative association between H. pylori infection and IBD, particularly in patients with Crohn’s disease, younger populations and Eastern populations. This specific pattern of association—most pronounced in a condition dominated by Th1/Th17 immune responses (CD) and among populations with a high prevalence of CagA-positive strains—suggests that H. pylori, particularly CagA-positive strains, may play a potential protective role, likely mediated through immunomodulatory mechanisms. However, it is crucial to emphasize that this finding is based on observational evidence and cannot establish causality. Current clinical guidelines recommending H. pylori eradication for gastric health remain largely applicable. The decision to eradicate H. pylori in patients with IBD should be individualized, based on a comprehensive assessment of factors such as gastric cancer risk, symptomatology, and disease activity. Therefore, the management of H. pylori infection in this population should shift from a routine eradication approach toward a more prudent and individualized strategy.
Statements
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
YB: Formal analysis, Funding acquisition, Writing – original draft, Investigation, Conceptualization, Data curation, Software. LZ: Supervision, Data curation, Writing – review & editing, Visualization, Formal analysis. SZ: Software, Writing – original draft. YS: Writing – review & editing, Methodology. JZ: Validation, Conceptualization, Writing – review & editing, Formal analysis.
Funding
The author(s) declared that financial support was received for this work and/or its publication. This study was supported by the key project of Chun’an county medical and health science and technology plan (2024CAYY002).
Conflict of interest
The author(s) declared that this work was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declared that Generative AI was not used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2026.1757356/full#supplementary-material
SUPPLEMENTARY TABLE 1Search Syntax of the Databases.
SUPPLEMENTARY IMAGE 1Association between Hp infection and IBD stratified by subgroup.
SUPPLEMENTARY IMAGE 2Results of sensitivity analyses, excluded lower-quality studies.
SUPPLEMENTARY IMAGE 3Results of sensitivity analyses excluded studies with a sample size smaller than 100.
SUPPLEMENTARY IMAGE 4Results of sensitivity analyses excluded studies with unclear age stratification.
References
1.
Guan Q . A comprehensive review and update on the pathogenesis of inflammatory bowel disease. J Immunol Res. (2019) 2019:7247238. doi: 10.1155/2019/7247238,
2.
Wang R Li Z Liu S Zhang D . Global, regional and national burden of inflammatory bowel disease in 204 countries and territories from 1990 to 2019: a systematic analysis based on the global burden of disease study 2019. BMJ Open. (2023) 13:e065186. doi: 10.1136/bmjopen-2022-065186,
3.
Lewis JD Parlett LE Jonsson Funk ML Brensinger C Pate V Wu Q et al . Incidence, prevalence, and racial and ethnic distribution of inflammatory bowel disease in the United States. Gastroenterology. (2023) 165:1197–1205.e2. doi: 10.1053/j.gastro.2023.07.003,
4.
Kusters JG van Vliet AH Kuipers EJ . Pathogenesis of Helicobacter pylori infection. Clin Microbiol Rev. (2006) 19:449–90. doi: 10.1128/CMR.00054-05,
5.
Sugano K Tack J Kuipers EJ Graham DY el-Omar EM Miura S et al . Kyoto global consensus report on Helicobacter pylori gastritis. Gut. (2015) 64:1353–67. doi: 10.1136/gutjnl-2015-309252,
6.
Ormand JE Talley NJ Shorter RG . Prevalence of Helicobacter pylori in specific forms of gastritis. Further evidence supporting a pathogenic role for H. pylori in chronic nonspecific gastritis. Dig Dis Sci. (1991) 36:142–5.
7.
El-Omar E Penman I Cruikshank G Dover S Banerjee S Williams C et al . Low prevalence of Helicobacter pylori in inflammatory bowel disease: association with sulphasalazine. Gut. (1994) 35:1385–8.
8.
Graca-Pakulska K Błogowski W Zawada I Deskur A Dąbkowski K Urasińska E et al . Endoscopic findings in the upper gastrointestinal tract in patients with Crohn's disease are common, highly specific, and associated with chronic gastritis. Sci Rep. (2023) 13:703. doi: 10.1038/s41598-022-21630-5,
9.
Castaño-Rodríguez N Kaakoush NO Lee WS Mitchell HM . Dual role of Helicobacter and Campylobacter species in IBD: a systematic review and meta-analysis. Gut. (2017) 66:235–49. doi: 10.1136/gutjnl-2015-310545,
10.
Imawana RA Smith DR Goodson ML . The relationship between inflammatory bowel disease and Helicobacter pylori across east Asian, European and Mediterranean countries: a meta-analysis. Ann Gastroenterol. (2020) 33:485–94. doi: 10.20524/aog.2020.0507,
11.
Kong G Liu Z Lu Y Li M Guo H . The association between Helicobacter pylori infection and inflammatory bowel disease in children: a systematic review with meta-analysis. Medicine (Baltimore). (2023) 102:e34882. doi: 10.1097/MD.0000000000034882,
12.
Luther J Dave M Higgins PD Kao JY . Association between Helicobacter pylori infection and inflammatory bowel disease: a meta-analysis and systematic review of the literature. Inflamm Bowel Dis. (2010) 16:1077–84. doi: 10.1002/ibd.21116,
13.
Shirzad-Aski H Besharat S Kienesberger S Sohrabi A Roshandel G Amiriani T et al . Association between Helicobacter pylori colonization and inflammatory bowel disease: a systematic review and Meta-analysis. J Clin Gastroenterol. (2021) 55:380–92. doi: 10.1097/MCG.0000000000001415,
14.
Tepler A Narula N Peek RM Jr Patel A Edelson C Colombel JF et al . Systematic review with meta-analysis: association between Helicobacter pylori CagA seropositivity and odds of inflammatory bowel disease. Aliment Pharmacol Ther. (2019) 50:121–31. doi: 10.1111/apt.15306,
15.
Wang WL Xu XJ . Correlation between Helicobacter pylori infection and Crohn's disease: a meta-analysis. Eur Rev Med Pharmacol Sci. (2019) 23:10509–16. doi: 10.26355/eurrev_201912_19691,
16.
Wu XW Ji HZ Yang MF Wu L Wang FY . Helicobacter pylori infection and inflammatory bowel disease in Asians: a meta-analysis. World J Gastroenterol. (2015) 21:4750–6. doi: 10.3748/wjg.v21.i15.4750,
17.
Yu Q Zhang S Li L Xiong L Chao K Zhong B et al . Enterohepatic Helicobacter species as a potential causative factor in inflammatory bowel disease: a Meta-analysis. Medicine (Baltimore). (2015) 94:e1773. doi: 10.1097/MD.0000000000001773,
18.
Zhong Y Zhang Z Lin Y Wu L . The relationship between Helicobacter pylori and inflammatory bowel disease. Arch Iran Med. (2021) 24:317–25. doi: 10.34172/aim.2021.44,
19.
Rokkas T Gisbert JP Niv Y O'Morain C . The association between Helicobacter pylori infection and inflammatory bowel disease based on meta-analysis. United European Gastroenterol J. (2015) 3:539–50. doi: 10.1177/2050640615580889,
20.
Page MJ McKenzie JE Bossuyt PM . The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
21.
Higgins JP Thompson SG Deeks JJ Altman DG . Measuring inconsistency in meta-analyses. BMJ. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557,
22.
Sonnenberg A Genta RM . Inverse association between Helicobacter pylori gastritis and microscopic colitis. Inflamm Bowel Dis. (2016) 22:182–6. doi: 10.1097/MIB.0000000000000595,
23.
Sonnenberg A Melton SD Genta RM . Frequent occurrence of gastritis and Duodenitis in patients with inflammatory bowel disease. Inflamm Bowel Dis. (2011) 17:39–44. doi: 10.1002/ibd.21356,
24.
Ando T Watanabe O Ishiguro K Maeda O Ishikawa D Minami M et al . Relationships between Helicobacter pylori infection status, endoscopic, histopathological findings, and cytokine production in the duodenum of Crohn's disease patients. J Gastroenterol Hepatol. (2008) 23:S193–7. doi: 10.1111/j.1440-1746.2008.05438.x
25.
Basset C Holton J Bazeos A Vaira D Bloom S . Are Helicobacter species and enterotoxigenic Bacteroides fragilis involved in inflammatory bowel disease?Dig Dis Sci. (2004) 49:1425–32. doi: 10.1023/b:ddas.0000042241.13489.88,
26.
D'Incà R Sturniolo G Cassaro M di Pace C Longo G Callegari I et al . Prevalence of upper gastrointestinal lesions and Helicobacter pylori infection in Crohn's disease. Dig Dis Sci. (1998) 43:988–92.
27.
Magalhães-Costa MH Reis BR Chagas VL Nunes T Souza HS Zaltman C . Focal enhanced gastritis and macrophage microaggregates in the gastric mucosa: potential role in the differential diagnosis between Crohn's disease and ulcerative colitis. Arq Gastroenterol. (2014) 51:276–82. doi: 10.1590/S0004-28032014000400003,
28.
Ding ZH Xu XP Wang TR Liang X Ran ZH Lu H . The prevalence of Helicobacter pylori infection in inflammatory bowel disease in China: a case-control study. PLoS One. (2021) 16:e0248427. doi: 10.1371/journal.pone.0248427,
29.
Duggan AE Usmani I Neal KR Logan RF . Appendicectomy, childhood hygiene, Helicobacter pylori status, and risk of inflammatory bowel disease: a case control study. Gut. (1998) 43:494–8.
30.
Farkas K Chan H Rutka M Szepes Z Nagy F Tiszlavicz L et al . Gastroduodenal involvement in asymptomatic Crohn's disease patients in two areas of emerging disease: Asia and Eastern Europe. J Crohns Colitis. (2016) 10:1401–6. doi: 10.1093/ecco-jcc/jjw113,
31.
Feeney MA Murphy F Clegg AJ Trebble TM Sharer NM Snook JA . A case-control study of childhood environmental risk factors for the development of inflammatory bowel disease. Eur J Gastroenterol Hepatol. (2002) 14:529–34. doi: 10.1097/00042737-200205000-00010,
32.
Garza-Gonzalez E Perez-Perez GI Mendoza-Ibarra SI Flores-Gutiérrez JP Bosques-Padilla FJ . Genetic risk factors for inflammatory bowel disease in a north-eastern Mexican population. Int J Immunogenet. (2010) 37:355–9. doi: 10.1111/j.1744-313X.2010.00932.x,
33.
Halme L Rautelin H Leidenius M Kosunen TU . Inverse correlation between Helicobacter pylori infection and inflammatory bowel disease. J Clin Pathol. (1996) 49:65–7.
34.
Meining A Bayerdörffer E Bastlein E Bastlein E Raudis N Thiede C et al . Focal inflammatory infiltrations in gastric biopsy specimens are suggestive of Crohn's disease. Crohn's Dis Study Group, Germany Scand J Gastroenterol. (1997) 32:813–8.
35.
Oberhuber G Püspök A Oesterreicher C Novacek G Zauner C Burghuber M et al . Focally enhanced gastritis: a frequent type of gastritis in patients with Crohn's disease. Gastroenterology. (1997) 112:698–706. doi: 10.1053/gast.1997.v112.pm9041230,
36.
Wagtmans MJ Witte AM Taylor DR Biemond I Veenendaal RA Verspaget HW et al . Low seroprevalence of Helicobacter pylori antibodies in historical sera of patients with Crohn's disease. Scand J Gastroenterol. (1997) 32:712–8. doi: 10.3109/00365529708996523,
37.
Parente F Cucino C Bollani S Imbesi V Maconi G Bonetto S et al . Focal gastric inflammatory infiltrates in inflammatory bowel diseases: prevalence, immunohistochemical characteristics, and diagnostic role. Am J Gastroenterol. (2000) 95:705–11. doi: 10.1111/j.1572-0241.2000.01851.x,
38.
Pearce CB Duncan HD Timmis L Green JR . Assessment of the prevalence of infection with Helicobacter pylori in patients with inflammatory bowel disease. Eur J Gastroenterol Hepatol. (2000) 12:439–43.
39.
Matsumura M Matsui T Hatakeyama S Matake H Uno H Sakurai T et al . Prevalence of Helicobacter pylori infection and correlation between severity of upper gastrointestinal lesions and H. pylori infection in Japanese patients with Crohn's disease. J Gastroenterol. (2001) 36:740–7. doi: 10.1007/s005350170015
40.
Väre PO Heikius B Silvennoinen JA Karttunen R Niemelä SE Lehtola JK et al . Seroprevalence of Helicobacter pylori infection in inflammatory bowel disease: is Helicobacter pylori infection a protective factor?Scand J Gastroenterol. (2001) 36:1295–300. doi: 10.1080/003655201317097155,
41.
Piodi LP Bardella M Rocchia C Cesana BM Baldassarri A Quatrini M . Possible protective effect of 5-aminosalicylic acid on Helicobacter pylori infection in patients with inflammatory bowel disease. J Clin Gastroenterol. (2003) 36:22–5. doi: 10.1097/00004836-200301000-00008,
42.
Prónai L Schandl L Orosz Z Magyar P Tulassay Z . Lower prevalence of Helicobacter pylori infection in patients with inflammatory bowel disease but not with chronic obstructive pulmonary disease - antibiotic use in the history does not play a significant role. Helicobacter. (2004) 9:278–83. doi: 10.1111/j.1083-4389.2004.00223.x,
43.
Moriyama T Matsumoto T Jo Y Yada S Hirahashi M Yao T et al . Mucosal proinflammatory cytokine and chemokine expression of gastroduodenal lesions in Crohn's disease. Aliment Pharmacol Ther. (2005) 21:85–91. doi: 10.1111/j.1365-2036.2005.02480.x
44.
Oliveira AG Rocha GA Rocha AM Sanna Md Moura SB Dani R et al . Isolation of Helicobacter pylori from the intestinal mucosa of patients with Crohn's disease. Helicobacter. (2006) 11:2–9. doi: 10.1111/j.0083-8703.2006.00368.x
45.
Ando T Watanabe O Nobata K Ishiguro K Maeda O Ishikawa D et al . Immunological status of the stomach in inflammatory bowel disease - comparison between ulcerative colitis and Crohn's disease. Digestion. (2008) 77:145–9. doi: 10.1159/000140973,
46.
Laharie D Asencio C Asselineau J Bulois P Bourreille A Moreau J et al . Association between entero-hepatic Helicobacter species and Crohn's disease: a prospective cross-sectional study. Aliment Pharmacol Ther. (2009) 30:283–93. doi: 10.1111/j.1365-2036.2009.04034.x,
47.
Lidar M Langevitz P Barzilai O Ram M Porat-Katz BS Bizzaro N et al . Infectious serologies and autoantibodies in inflammatory bowel disease: insinuations at a true pathogenic role. Ann N Y Acad Sci. (2009) 1173:640–8. doi: 10.1111/j.1749-6632.2009.04673.x,
48.
Song MJ Park DI Hwang SJ Kim ER Kim YH Jang BI et al . The prevalence of Helicobacter pylori infection in Korean patients with inflammatory bowel disease, a multicenter study. Korean J Gastroenterol. (2009) 53:341–7. doi: 10.4166/kjg.2009.53.6.341,
49.
Zhang S Zhong B Chao K . Role of Helicobacter species in Chinese patients with inflammatory bowel disease. J Clin Microbiol. (2011) 49:1987–9. doi: 10.1128/JCM.02630-10,
50.
Sonnenberg A Genta RM . Low prevalence of Helicobacter pylori infection among patients with inflammatory bowel disease. Aliment Pharmacol Ther. (2012) 35:469–76. doi: 10.1111/j.1365-2036.2011.04969.x,
51.
Xiang Z Chen YP Ye YF Ma KF Chen SH Zheng L et al . Helicobacter pylori and Crohn's disease: a retrospective single-center study from China. World J Gastroenterol. (2013) 19:4576–81. doi: 10.3748/wjg.v19.i28.4576,
52.
Ostrowski J Kulecka M Zawada I Żeber-Lubecka N Paziewska A Graca-Pakulska K . The gastric microbiota in patients with Crohn's disease; a preliminary study. Sci Rep. (2021) 11:17866. doi: 10.1038/s41598-021-97261-z,
53.
Alotaibi AD Al-Abdulwahab AA Ismail MH . Prevalence of H. pylori in inflammatory bowel disease patients and its association with severity. BMC Gastroenterol. (2025) 25:892. doi: 10.1186/s12876-025-03892-1
54.
Sonnenberg A Turner KO Genta RM . Decreased risk for microscopic colitis and inflammatory bowel disease among patients with reflux disease. Color Dis. (2018) 20:813–20. doi: 10.1111/codi.14114,
55.
Rosania R Von Arnim U Link A Rajilic-Stojanovic M Franck C Canbay A et al . Helicobacter pylori eradication therapy is not associated with the onset of inflammatory bowel diseases. A case-control study. J Gastrointestin Liver Dis. (2018) 27:119–25. doi: 10.15403/jgld.2014.1121.272.hpy,
56.
Lorenzo MV Agel FM Mengual ES-V . Eradication of Helicobacter pylori in patients with inflammatory bowel disease for prevention of recurrences - impact on the natural history of the disease. Eurasian J Med Oncol. (2019). 3:59–65. doi: 10.14744/ejmo.2018.0058
57.
Ali I Abdo Q Al-Hihi S . Association between ulcerative colitis and Helicobacter pylori infection: a case-control study. Heliyon. (2022) 8:e08930. doi: 10.1016/j.heliyon.2022.e08930
58.
Jin X Chen YP Chen SH Xiang Z . Association between Helicobacter Pylori infection and ulcerative colitis--a case control study from China. Int J Med Sci. (2013) 10:1479–84. doi: 10.7150/ijms.6934,
59.
Thomson JM Hansen R Berry SH Hope ME Murray GI Mukhopadhya I et al . Enterohepatic helicobacter in ulcerative colitis: potential pathogenic entities?PLoS One. (2011) 6:e17184. doi: 10.1371/journal.pone.0017184,
60.
Oliveira AG das Graças Pimenta Sanna M Rocha GA Rocha AM Santos A Dani R et al . Helicobacter species in the intestinal mucosa of patients with ulcerative colitis. J Clin Microbiol. (2004) 42:384–6. doi: 10.1128/JCM.42.1.384-386.2004
61.
Parente F Molteni P Bollani S Maconi G Vago L Duca PG et al . Prevalence of Helicobacter pylori infection and related upper gastrointestinal lesions in patients with inflammatory bowel diseases. A cross-sectional study with matching. Scand J Gastroenterol. (1997) 32:1140–6. doi: 10.3109/00365529709002994
62.
Mansour L El-Kalla F Kobtan A Abd-Elsalam S Yousef M Soliman S et al . Helicobacter pylori may be an initiating factor in newly diagnosed ulcerative colitis patients: a pilot study. World J Clin Cases. (2018) 6:641–9. doi: 10.12998/wjcc.v6.i13.641,
63.
Cheul Ho Hong DIP Choi WH Park JH Kim HJ Cho YK . The clinical usefulness of focally enhanced gastritis in Korean patients with Crohn’s disease. Korean J Gastroenterol. (2009). 53:23–8.
64.
Koskela RM Niemelä SE Lehtola JK Bloigu RS Karttunen TJ . Gastroduodenal mucosa in microscopic colitis. Scand J Gastroenterol. (2011) 46:567–76. doi: 10.3109/00365521.2011.551889,
65.
Ram M Barzilai O Shapira Y Anaya JM Tincani A Stojanovich L et al . Helicobacter pylori serology in autoimmune diseases - fact or fiction?Clin Chem Lab Med. (2013) 51:1075–82. doi: 10.1515/cclm-2012-0477,
66.
Sayar R Shokri Shirvani J Hajian-Tilaki K Vosough Z Ranaei M . The negative association between inflammatory bowel disease and Helicobacter pylori seropositivity. Caspian J Intern Med. (2019) 10:217–22. doi: 10.22088/cjim.10.2.217,
67.
Chen Y Blaser MJ . Helicobacter pylori colonization is inversely associated with childhood asthma. J Infect Dis. (2008) 198:553–60. doi: 10.1086/590158,
68.
Wjst M . Does Helicobacter pylori protect against asthma and allergy?Gut. (2008) 57:1178–9. doi: 10.1136/gut.2007.133462
69.
Arnold IC Hitzler I Müller A . The immunomodulatory properties of Helicobacter pylori confer protection against allergic and chronic inflammatory disorders. Front Cell Infect Microbiol. (2012) 2:10. doi: 10.3389/fcimb.2012.00010,
70.
Bai X Jiang L Ruan G Liu T Yang H . Helicobacter pylori may participate in the development of inflammatory bowel disease by modulating the intestinal microbiota. Chin Med J. (2022) 135:634–8. doi: 10.1097/CM9.0000000000002008,
71.
Ni J Wu GD Albenberg L Tomov VT . Gut microbiota and IBD: causation or correlation?Nat Rev Gastroenterol Hepatol. (2017) 14:573–84. doi: 10.1038/nrgastro.2017.88,
72.
Abraham C Cho JH . Inflammatory bowel disease. N Engl J Med. (2009) 361:2066–78. doi: 10.1056/NEJMra0804647,
73.
Podolsky DK . Inflammatory bowel disease. N Engl J Med. (2002) 347:417–29. doi: 10.1056/nejmra020831,
74.
Sakuraba A Sato T Kamada N Kitazume M Sugita A Hibi T . Th1/Th17 immune response is induced by mesenteric lymph node dendritic cells in Crohn's disease. Gastroenterology. (2009) 137:1736–45. doi: 10.1053/j.gastro.2009.07.049,
75.
Strober W Fuss IJ . Proinflammatory cytokines in the pathogenesis of inflammatory bowel diseases. Gastroenterology. (2011) 140:1756–67. doi: 10.1053/j.gastro.2011.02.016,
76.
Wroblewski LE Peek RM Jr Wilson KT . Helicobacter pylori and gastric cancer: factors that modulate disease risk. Clin Microbiol Rev. (2010) 23:713–39. doi: 10.1128/CMR.00011-10,
77.
Haskey N Gibson DL . An examination of diet for the maintenance of remission in inflammatory bowel disease. Nutrients. (2017) 9:259. doi: 10.3390/nu9030259,
78.
Benchimol EI Manuel DG Mack DR Nguyen GC Gommerman JL . Asthma, type 1 and type 2 diabetes mellitus, and inflammatory bowel disease amongst south Asian immigrants to Canada and their children: a population-based cohort study. PLoS One. (2015) 10:e0123599. doi: 10.1371/journal.pone.0123599,
79.
Franceschi C Campisi J . Chronic inflammation (inflammaging) and its potential contribution to age-associated diseases. J Gerontol A Biol Sci Med Sci. (2014) 69:S4–9. doi: 10.1093/gerona/glu057
80.
Malfertheiner P Megraud F Rokkas T Gisbert JP Liou JM Schulz C et al . Management of Helicobacter pylori infection: the Maastricht VI/Florence consensus report. Gut. (2022) 71:1724–62. doi: 10.1136/gutjnl-2022-327745
81.
Schwartzbaum J Ahlbom A Feychting M . Berkson's bias reviewed. Eur J Epidemiol. (2003) 18:1109–12. doi: 10.1023/b:ejep.0000006552.89605.c8
Summary
Keywords
Crohn disease, Helicobacter pylori , inflammatory bowel diseases, negative association, ulcerative colitis
Citation
Bi Y, Zhou L, Zhou S, Sun Y and Zhang J (2026) To eradicate or not? Helicobacter pylori in patients with inflammatory bowel disease: an updated systematic review and meta-analysis. Front. Med. 13:1757356. doi: 10.3389/fmed.2026.1757356
Received
30 November 2025
Revised
08 January 2026
Accepted
15 January 2026
Published
03 February 2026
Volume
13 - 2026
Edited by
Iain Brownlee, Northumbria University, United Kingdom
Reviewed by
Vali Musazadeh, Iran University of Medical Sciences, Iran
Vijay K. Verma, University of Delhi, India
Updates
Copyright
© 2026 Bi, Zhou, Zhou, Sun and Zhang.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jun Zhang, zhangjun1@hmc.edu.cn
†These authors have contributed equally to this work
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.