 María Olimpia Paz Alvarenga1
María Olimpia Paz Alvarenga1 Deborah Ribeiro Frazão1
Deborah Ribeiro Frazão1 Isabella Gomes de Matos1Leonardo Oliveira Bittencourt1
Isabella Gomes de Matos1Leonardo Oliveira Bittencourt1 Nathália Carolina Fernandes Fagundes2
Nathália Carolina Fernandes Fagundes2 Cassiano Kuchenbecker Rösing3
Cassiano Kuchenbecker Rösing3 Lucianne Cople Maia4
Lucianne Cople Maia4 Rafael Rodrigues Lima1*
Rafael Rodrigues Lima1*- 1Laboratory of Functional and Structural Biology, Institute of Biological Sciences, Federal University of Pará, Belém, Brazil
- 2Faculty of Medicine and Dentistry, School of Dentistry, University of Alberta, Edmonton, AB, Canada
- 3Department of Periodontology, School of Dentistry, Federal University of Rio Grande Do Sul (UFRGS), Porto Alegre, Brazil
- 4Department of Pediatric Dentistry and Orthodontics, School of Dentistry, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil
Background: Neurodegenerative diseases are a group of progressive disorders that affect the central nervous system (CNS) such as Alzheimer, Parkinson, and multiple sclerosis. Inflammation plays a critical role in the onset and progression of these injuries. Periodontitis is considered an inflammatory disease caused by oral biofilms around the tooth-supporting tissues, leading to a systemic and chronic inflammatory condition. Thus, this systematic review aimed to search for evidence in the association between neurodegenerative disorders and periodontitis.
Methods: This systematic review was registered at International Prospective Register of Systematic Reviews (PROSPERO) under the code CRD 42016038327. The search strategy was performed in three electronic databases and one gray literature source—PubMed, Scopus, Web of Science, and OpenGrey, based on the PECO acronym: observational studies in humans (P) in which a neurodegenerative disease was present (E) or absent (C) to observe an association with periodontitis (O). The Fowkes and Fulton checklist was used to critically appraise the methodological quality and the risk of bias of individual studies. The quality of evidence was assessed by the Grading of Recommendations Assessment, Development and Evaluation (GRADE).
Results: From 534 articles found, 12 were included, of which eight were case–control, three were cross-sectional, and one was a cohort, giving a total of 3,460 participants. All the included studies reported an association between some neurodegenerative diseases and periodontitis and presented a low risk of bias. According to the GRADE approach, the level of evidence of probing pocket depth was considered very low due to the significant heterogeneity across the studies' upgrading imprecision and inconsistency.
Conclusions: Although all the included studies in this review reported an association between neurodegenerative diseases and periodontitis, the level of evidence was classified to be very low, which suggests a cautious interpretation of the results.
Introduction
Neurodegenerative disease is a broad expression for a group of disorders that damage the central nervous system (CNS), characterized by the progressive loss of neuronal structure and function. These diseases are incurable and lead to a progressive decline or even the complete loss of sensory, motor, and cognitive functions (Hussain et al., 2018). According to the World Health Organization (WHO), neurodegenerative disorders affect up to 1 billion people worldwide, and the proportion is growing with the aging of the world population; they lead to the death of about 6.8 million people per year, equivalent to 12% of all deaths in the world (Feigin et al., 2020).
Among the different types of neurodegenerative diseases, Alzheimer's disease (AD), Huntington's disease, Parkinson's disease (PD), and multiple sclerosis are the most frequently occurring (Hussain et al., 2018). These disorders damage the CNS and trigger rapid microglial activation, the main component of neuroinflammation. Activated microglia produce and secrete inflammatory mediators, such as eicosanoids, cytokines, chemokines, reactive free radicals, and proteases. Although a well-regulated inflammatory process is beneficial for injured CNS tissue, an excessive inflammatory response can be a source of additional injury and may affect the chronic progression of these diseases (Gao and Hong, 2008).
Some inflammatory diseases, such as periodontitis, might represent a factor that can contribute to CNS damage. Periodontitis is a multifactorial chronic inflammatory disease that affects the supporting tissues around the teeth such as gum, cementum, periodontal ligament, and alveolar bone triggered by dysbiotic biofilms that can lead to a systemic inflammatory (Papapanou et al., 2018). Periodontal disease is one of the most frequent causes of tooth loss, leading to alterations in the masticatory and aesthetic functions and, finally, impairing the quality of life of individuals (Papapanou et al., 2018). It is highly prevalent in adults affecting about 20–50% of the global population (Nazir, 2017). It can lead to a systemic inflammatory state through mechanisms that include the spread of pro-inflammatory cytokines and/or bacteria located in the oral cavity (Hajishengallis, 2015). Persistent systemic inflammation/infection can cause neuroinflammation in the brain (Perry et al., 2003).
Considering this possible interaction, the present study aims to systematically review the evidence supporting the association between the presence of some neurodegenerative disease and periodontitis.
Methods
Protocol and Registration
This review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Moher et al., 2009). It was registered under number CRD: 42016038327 in the International Prospective Register of Systematic Reviews (PROSPERO) (http://www.crd.york.ac.uk).
Search Strategy
The search strategy was performed on four electronic databases, PubMed, Scopus, Web of Science, and The Cochrane Library, and a gray literature source, OpenGrey. Both MeSH and entry terms were adapted adequately according to each database's syntax rule, as shown in Supplementary Table 1, using the operator's Booleans (OR, AND) to combine searches. The articles found in more than one database were considered only once. No restrictions were placed on publication date or language. We performed a manual search of the reference lists of the included studies to find additional articles and an alert on each database platform to detect articles on the topic published until December 2020.
Selection and Eligibility Criteria
Studies were selected based on the PECO acronym, including observational studies in humans (P, population) in which a neurodegenerative disease was present (E, exposure) or absent (C, comparison) to observe an association between this and periodontitis (O, outcome). The aim was to answer the focused question: Is there any association between neurodegenerative disease and periodontitis in adult patients?
All titles, abstracts, and full-text reading of the articles were independently analyzed by two reviewers (MA and IM) who imported all relevant citations into a bibliographic reference manager (EndNote®, version X7, Thomson Reuters, Philadelphia, USA). In case of disagreement between the examiners, a third reviewer (RL) was involved. Studies that included patients without a diagnostic of neurodegenerative disease, groups with gingivitis only, case reports, descriptive studies, review articles, opinion articles, technical articles, guidelines, animal and in vitro studies were excluded.
Data Extraction and Risk of Bias Assessment
The following data were extracted from the articles: authors and year; study design; characteristics of the sample (size, age, location, and study group); evaluation method (clinical and laboratory parameters); statistical analysis; results (study group, control group); and the outcome. Data were extracted and tabulated independently by two reviewers (MA and LB).
The checklist developed by Fowkes and Fulton (1991) was used for critical appraisal of the methodological quality and risk of bias of individual studies. This checklist has domains related to study and sample design; control group characteristics; quality of measures and results; integrity; and distorted influences. For each criterion, a sign was assigned (++) in case of major problems in the study or (+) in case of minor issues, to assess whether the methods are adequate to produce consistent and valid information, as well as whether the results offered the expected effects that might infer conclusions. In areas where the question did not apply to the type of study, NA was assigned (not applicable). No problem has been designated by the sign (0). The evaluation for each domain was standardized by the examiners, as described in Supplementary Table 2. After assessment of each field, the studies were analyzed to determine the value of the study through three summary questions: “Are the results erroneously biased in a certain direction?”; “Are there any serious confounding or other distorting influences?”; and “Is it likely that the results occurred by chance?”. These items were assigned “yes” and “no” answers. If the answer is no, in the three questions, the article is considered reliable, with a low risk of bias.
Level of Evidence (Grading of Recommendations Assessment, Development, and Evaluation)
The quality of evidence was rated using the GRADE approach (Movsisyan et al., 2016). A narrative assessment was chosen according to the types of studies selected by eligibility. According to the GRADE parameters, when observational studies are considered, a “low” rating is initially given. Then, assessments within the magnitude of the effect, dose–response relationship in development, and counteracting plausible residual bias or confounding may be used to upgrade the initial “low” rating. However, if there are serious or very serious issues related to the risk of bias, inconsistency, indirectness, imprecision, and publication bias, the level of evidence declines to “very low.” Thus, the certainty of evidence can be categorized into 1 of 4 ratings—high, moderate, low, and very low—reflecting the extent to which the review authors are confident that an estimate of the effect for a specific outcome is correct (Movsisyan, 2018).
Results
Study Selection
We identified 534 articles in the databases and the gray literature source accessed using our search strategy. After the duplicates were removed automatically and manually, 385 citations were screened by title and abstract, and 284 were excluded because they did not meet our eligibility criteria. In this phase, 101 citations were analyzed for potential eligibility, but only 20 studies remained for full-text reading from which eight articles were excluded because they did not meet the inclusion criteria (Supplementary Table 3). Finally, 12 studies were considered for qualitative analysis. All the selection phases are described in a flow diagram in Figure 1.
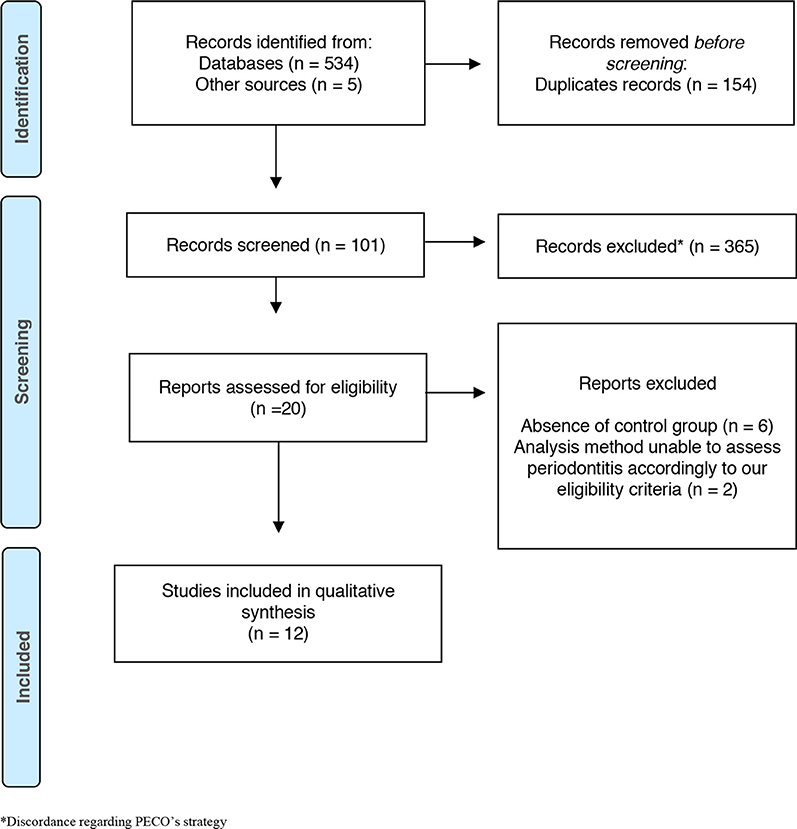
Figure 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of the different phases for exclusion and inclusion of the studies. *Discordance PECO's strategy.
Characteristics of the Included Studies
All of the included articles were observational studies: two cross-sectional, eight case–control, and two retrospective cohorts. The age range comprises 40–90 years and was considered a confounding factor and controlled in all the analyses. All studies evaluated the association between neurodegenerative disease and clinical and/or laboratory parameters of periodontitis, as described in Table 1.
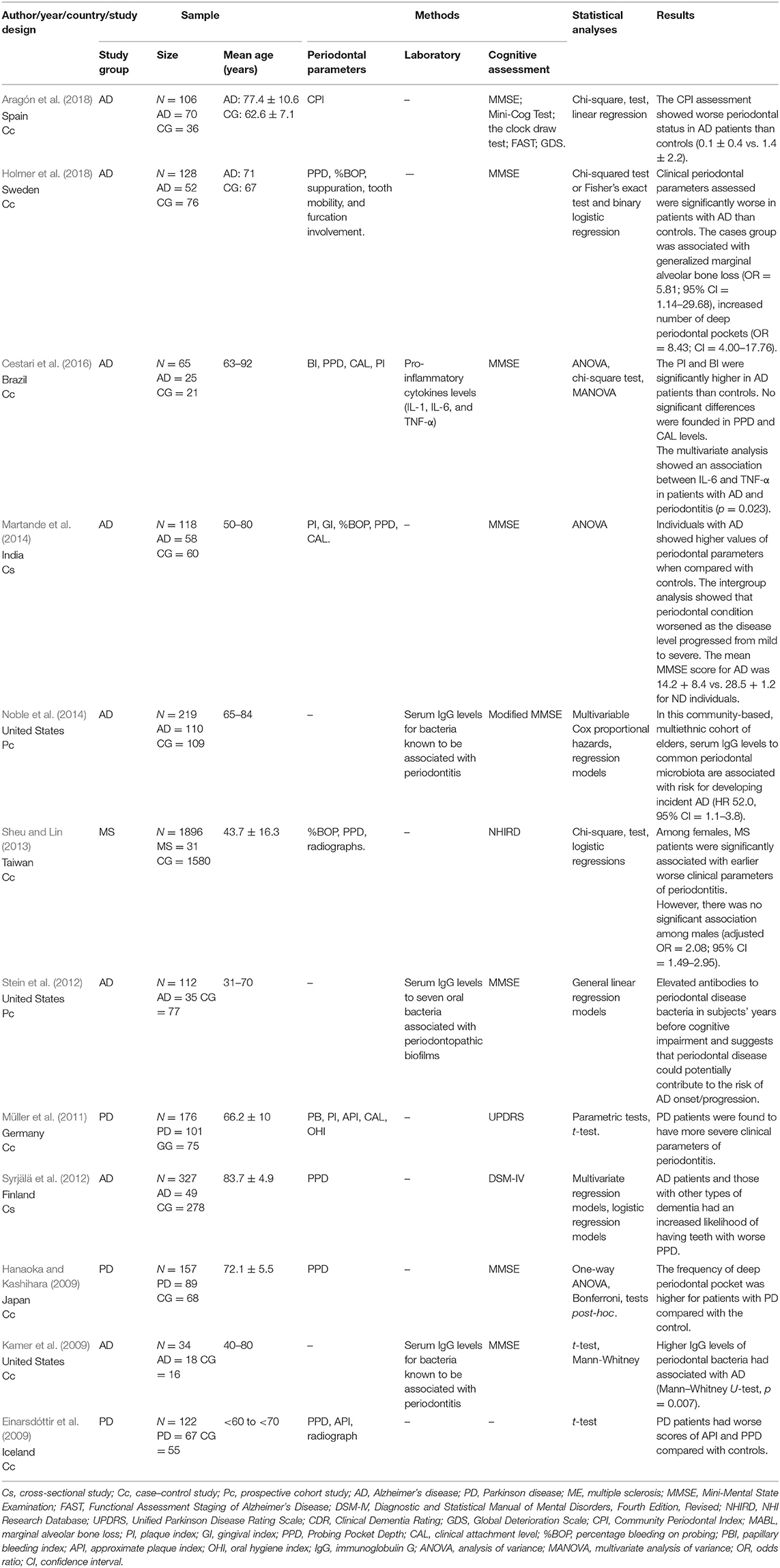
Table 1. Characteristics of the included studies.
Out of the 12 studies, eight involved patients diagnosed with AD. The cognitive status was assessed through validated instruments, most of them using the scores of the Mini-Mental State Examination (MMSE), modified (Noble et al., 2014) or not (Kamer et al., 2009; Stein et al., 2012; Martande et al., 2014; Cestari et al., 2016; Aragón et al., 2018; Holmer et al., 2018). In one study, besides the MMSE, they used a Mini-Cog Test, the clock draw test, the Functional Assessment Staging of Alzheimer's Disease (FAST), the Clinical Dementia Rating (CDR), and the Global Deterioration Scale (GDS) (Aragón et al., 2018). One study used the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) (Syrjälä et al., 2012).
PD patients were evaluated in three studies (Einarsdóttir et al., 2009; Hanaoka and Kashihara, 2009; Müller et al., 2011); one of them assessed the global cognitive function using the MMSE (Hanaoka and Kashihara, 2009); another used the scores of the Unified Parkinson Disease Rating Scale (UPDRS) (Müller et al., 2011); and in the last study, the instrument used is unclear (Einarsdóttir et al., 2009).
Only one included a study that evaluated patients diagnosed with multiple sclerosis. In this study, the authors assessed cognition status through the NHI Research Database (NHIRD) (Sheu and Lin, 2013).
All the studies that met eligibility criteria assessed periodontitis through at least one validated clinical parameter of periodontitis, such as clinical attachment loss (CAL) or probing depth (PPD >3 mm), bleeding on probing (BOP% >25%) of evaluated sites, and/or >30% of radiographic bone loss. Another criterion that was considered in some studies was the Community Periodontal Index (CPI) score 3 (PPD of 3.5–5.5 mm) and score 4 (PPD >5.5 mm) (Einarsdóttir et al., 2009; Hanaoka and Kashihara, 2009; Müller et al., 2011; Syrjälä et al., 2012; Sheu and Lin, 2013; Martande et al., 2014; Cestari et al., 2016; Aragón et al., 2018; Holmer et al., 2018). One study also evaluated pro-inflammatory cytokine levels (IL-1, IL-6, and TNF-α) (Cestari et al., 2016). Three studies assessed serum immunoglobulin G (Bos et al., 2015) levels of bacteria associated with periodontopathic biofilms (Kamer et al., 2009; Stein et al., 2012; Noble et al., 2014).
Risk of Bias Assessment
In the individual assessment for risk of bias, we found minor problems in some domains. In the item sampling method, six studies have minor issues since they performed convenience samples, unspecified sampling method, invited patients, and consecutive selection. Only one study (Holmer et al., 2018) reported the calculation of sample size. Two studies (Kamer et al., 2009; Cestari et al., 2016) presented a major problem in this domain, not describing the sample size calculation and having a sample size smaller than 50. For matching/randomization, one article presented a major problem due to the absence of matching groups (Einarsdóttir et al., 2009). Only one study highlighted blinding both among evaluators and in the research subjects (Martande et al., 2014). Each study assessment is shown in Table 2.
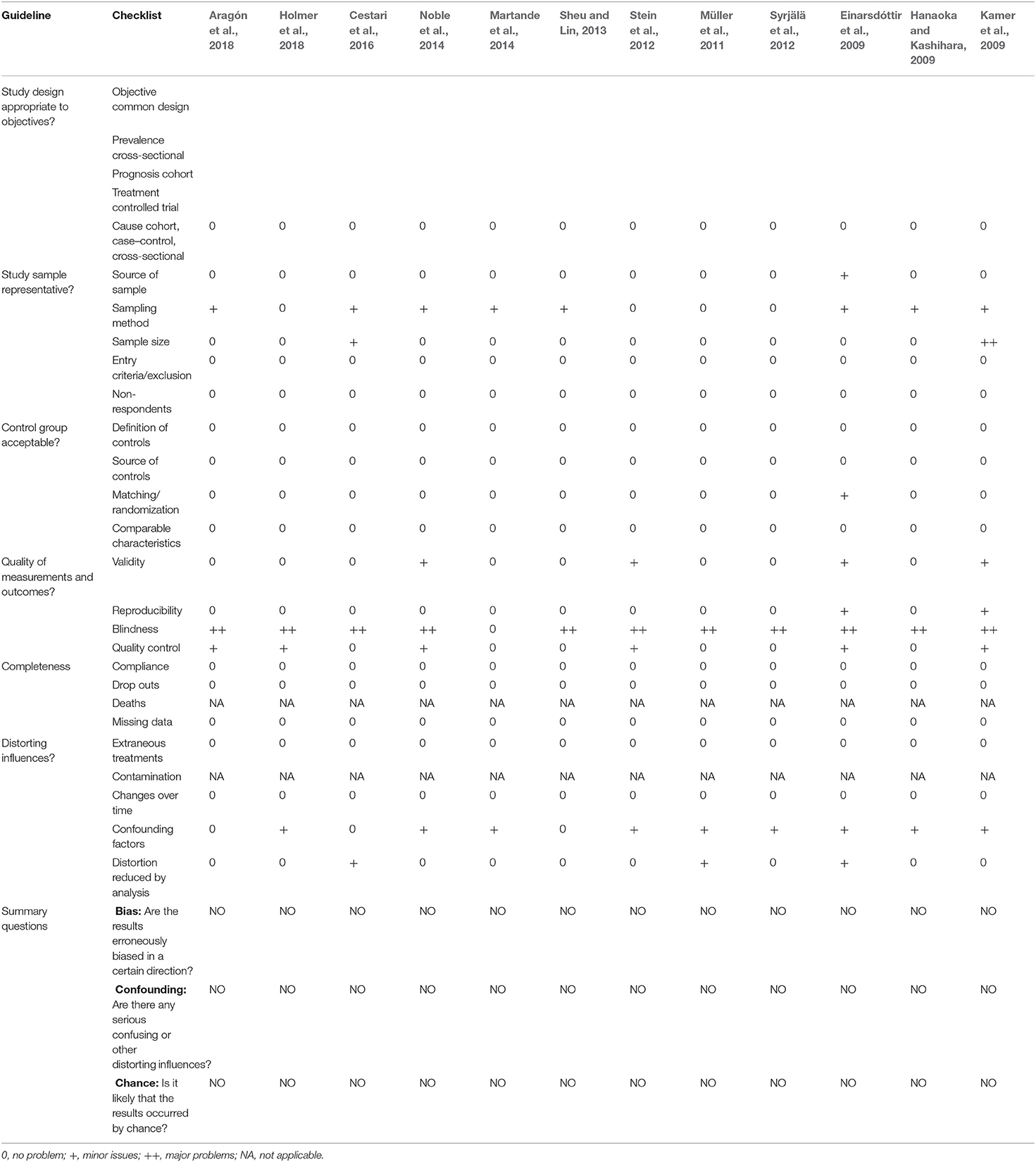
Table 2. Risk of bias assessment of the included studies.
However, all articles are liable to be reproduced, describing all methods used in their work and including qualified and calibrated evaluators to reduce bias. There was no sample loss in any of the included studies and nor refusal to participate—it was assumed because the sample size remained the same from beginning to end. Data were collected in the same period, and confounding factors were adjusted without interfering with the results. Despite that some domains presented minor and major problems, these issues did not influence the overall judgment; hence, we judged them to be low risk of bias.
Level of Evidence (Grading of Recommendations Assessment, Development, and Evaluation)
In the narrative of the certainty of evidence using the GRADE tool, the clinical parameter of probing pocket depth was used. The index was divided by the association with PD and AD, which was further separated for case–control and cross-sectional studies. The certainty of the evidence was considered very low for all analyses due to their inconsistency because the methods of analysis were different, making it challenging to gather the evidence. The PPD for AD in cross-sectional studies had a serious imprecision because the separation of the exposed group and the control group was performed in different ways in the two studies, hindering the accuracy of the evidence, as shown in Table 3.
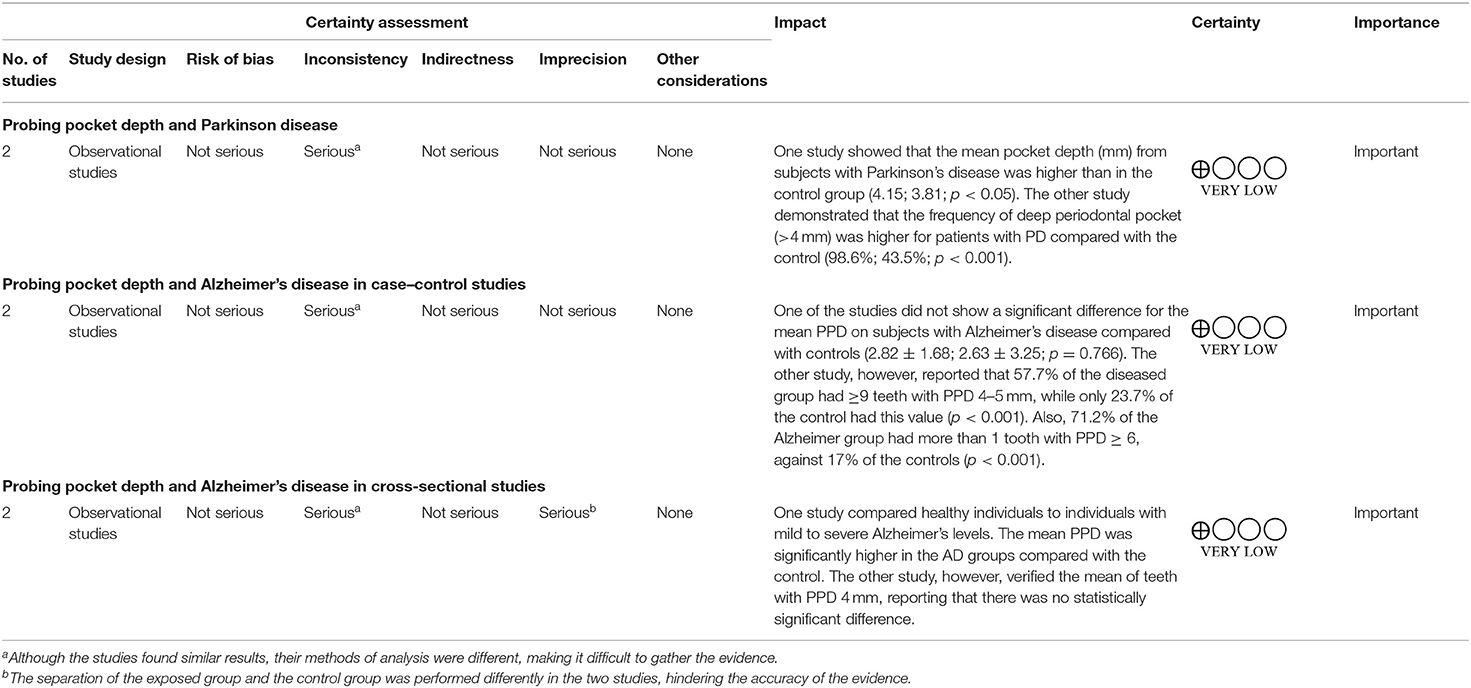
Table 3. Level of evidence by Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.
Discussion
The present systematic review summarized the evidence supporting the association between periodontitis and neurodegenerative diseases, especially AD and PD. The selection of studies to be included was performed after rigid criteria. All studies presented a low risk of bias and reported an association between neurodegenerative disease and periodontitis. The articles showed that the groups with the two concomitant diseases had higher inflammatory markers levels, IgG levels of periodontal bacteria, and/or clinical parameters of periodontitis compared with the isolated conditions. However, the heterogeneity of the studies taken together hindered the accuracy of the evidence and also made impossible the merging of data. In this sense, the present systematic review sticks to a qualitative analysis of the literature.
Periodontitis is an inflammatory disease triggered by dysbiotic biofilms and the most severe form of periodontal disease (Saini et al., 2011). It is diagnosed using clinical and radiographic evaluation of periodontal parameters, such as clinical attachment loss, probing depth, bleeding on probing, and/or radiographic bone loss (Armitage, 1999; Papapanou et al., 2018). In worse cases, the radiographic analysis shows an extensive loss of the bone supporting the compromised teeth (Page and Kornman, 1997). The dental biofilm is primarily composed of several gram-negative bacteria; the most relevant is Porphyromonas gingivalis, which stimulates the immuno-inflammatory response of the organism (Gaur and Agnihotri, 2015), followed by Prevotella intermedia, Fusobacterium nucleatum, Tannerella forsythia, and Treponema denticola (Bartova et al., 2014; Papapanou et al., 2018). The importance of specific bacteria is continuously subject to controversy since the understanding of the dysbiosis that occurs in periodontal tissues goes beyond the particular infection.
All the included studies in this review assessed periodontal status by clinical or laboratory parameters in subjects with a neurodegenerative disease (i.e., AD, PD, or multiple sclerosis). Nine studies assessed periodontitis by clinical parameters such as CPI, CAL, BOP, and PPD (Einarsdóttir et al., 2009; Hanaoka and Kashihara, 2009; Müller et al., 2011; Syrjälä et al., 2012; Sheu and Lin, 2013; Martande et al., 2014; Cestari et al., 2016; Aragón et al., 2018; Holmer et al., 2018). Three studies only assessed the serum IgG levels of the oral bacteria associated with periodontopathic biofilms (Kamer et al., 2009; Stein et al., 2012; Noble et al., 2014); one study evaluated periodontitis by clinical parameters and also assessed pro-inflammatory cytokines levels (IL-1, IL-6, and TNF-α) in serum (Cestari et al., 2016). The immune-inflammatory response triggered by periodontal pathogens turns the individual more susceptible to several systemic diseases (Friedewald et al., 2009; Hanes and Krishna, 2010; Otomo-Corgel et al., 2012; Tonetti et al., 2013; Ferreira et al., 2017; Martelli et al., 2017; Syahputra et al., 2018) including dementia (National Academies of Sciences, 2017) and neurodegenerative diseases (Webster et al., 2008; Kamer et al., 2009).
Neurodegenerative disease is a broad term for some illnesses that progressively affect the function of neurons in the human brain such as multiple sclerosis, PD, and AD (Bertram et al., 2005). These conditions are incurable and result in progressive degeneration and/or death of neurons, triggering ataxias and dementias (Bredesen et al., 2006). It has been advocated that periodontitis is associated with neurodegenerative diseases by two pathways: the most studied relates to the fact that the mediators of inflammation are present in the blood circulation, generating a constant inflammatory status (Teixeira et al., 2017); another possibility is related to gram-negative bacteria involved, e.g., P. gingivalis could directly induce damage (Dominy et al., 2019).
Gram-negative bacteria present lipopolysaccharides (LPSs), B-lymphocyte activators. P. gingivalis presents a cysteine protease called gingipain. This protease is divided into molecules of CD14, a receptor for the LPS enzyme, which allows bacteria to suppress the immune reaction against LPS (Bainbridge and Darveau, 2001). The rupture of the periodontal pocket is an easy access route for periodontal bacteria in the systemic circulation (Curtis, 2014). As a result, pro-inflammatory cytokines that are located in this area are taken to the systemic circulation, making periodontitis no longer a local inflammation and can be considered as “low-grade systemic inflammation;” increasing the inflammatory pool in the brain by two different pathways, by systemic circulation and by neural pathways; compromising the blood–brain barrier (BBB); and having facilitated access to the brain (D'aiuto et al., 2005). The constant exchange of solutes from the fluids of soft tissues and the blood plasma allows the systemic circulation of inflammatory-related molecules, which can trespass the BBB (D'aiuto et al., 2005).
The neural pathway might be conditioned to both the pathophysiology of the neurodegenerative diseases and the increase of systemic pro-inflammatory cytokines. Microglial cells are the predominant immune cells of the brain, and preclinical evidence also suggests the association between systemic inflammation and microglial activation, which can play a detrimental role in the progression of neurodegenerative due to the neurotoxicity mediated by oxidative stress and inflammation, leading to neuronal death (Holmes, 2013; Hoogland et al., 2015). The microglia can be stimulated not only by its neural microenvironment but by systemic stimuli as well (Perry and Teeling, 2013). Some evidence has shown the involvement of toll-like receptor activation (Bilbo et al., 2010) via pathogen-associated molecular patterns, complement 1q, and adenosine triphosphate release from astrocytes, producing TNF-α, Il-1β, and Il-6 (Hoogland et al., 2015; Tang and Le, 2016). In this way, as previously reviewed by Teixeira et al. (2017), the cross talk between neurodegenerative diseases and periodontitis underlies the priming of the microglia, i.e., the phenotype switch, in which the cell adopts a pro-inflammatory profile, aggravating the neuroinflammation.
Out of the 12 included studies, eight evaluated the possible association between periodontitis and AD (Kamer et al., 2009; Stein et al., 2012; Syrjälä et al., 2012; Martande et al., 2014; Noble et al., 2014; Cestari et al., 2016; Aragón et al., 2018; Holmer et al., 2018). Patients with AD present cognitive and behavioral damage (Hill et al., 2014), consistent neuroinflammation with infection, microglial activation, inflammasome activation, complement activation, and altered cytokine profiles (Dominy et al., 2019). Infections or systemic peripheral inflammation has been associated with the onset and progression of cognitive decline (Cunningham and Hennessy, 2015). The expression of TNF-α is considered an essential inflammatory cytokine to regulate the cascade of cellular events that occur during the neuroinflammatory response (Gurav, 2014). This inflammatory marker is up-regulated in AD and used as a diagnostic for this disease (Kamer et al., 2009; Ding et al., 2019). In one of our included studies, the multivariate analysis showed an association between IL-6 and TNF-α in patients with AD and periodontitis (Cestari et al., 2016). The concentration of IL-6 was negatively correlated with the MMSE, meaning that subjects with low scores in the cognitive test had high serum IL-6 levels. On the other hand, TNF-α concentration was positively correlated with PPD and CAL, showing that patients with worse periodontal conditions had more elevated TNF-α levels in serum. This finding suggests that immune-inflammatory mechanisms of periodontitis may underlie its role in the onset, progression, or aggravation of AD (Cestari et al., 2016). Previous studies have reported higher levels of inflammatory molecules in the brain in the presence of periodontitis (Kamer et al., 2009), playing an essential role in neuroinflammation and a potential risk factor for the incidence and progression of AD (Wu and Nakanishi, 2014).
Another pathway in the association between periodontitis and AD is related to periodontitis's main pathogenic bacteria (Underly et al., 2016; Dominy et al., 2019). P. gingivalis was identified in the brain of AD patients; the bacteria levels were positively correlated with the pathology of tau and ubiquitin (Dominy et al., 2019), classical biological markers of this disease (Underly et al., 2016). Out of the eight studies evaluating this association, three evaluated the serum IgG levels for bacteria associated with periodontitis. They detected higher levels of antibodies in patients diagnosed with the two concomitant diseases (Kamer et al., 2009; Stein et al., 2012; Noble et al., 2014). In the five remaining studies, the authors reported worse scores in at least one clinical parameter of periodontitis in patients with AD (Syrjälä et al., 2012; Martande et al., 2014; Cestari et al., 2016; Aragón et al., 2018; Holmer et al., 2018), and the intergroup analysis in one of them showed that periodontal condition worsened as the disease level presented higher severity (Martande et al., 2014).
PD is another neurodegenerative disease associated with periodontitis. This disease is related to movement disorders, degeneration of dopaminergic neurons, and the presence of cytoplasmic inclusion bodies—known as Lewy bodies (Matsui and Takahashi, 2018). PD is the second most common progressive neurodegenerative disease after AD (Kaur et al., 2016). Similar to the mechanism in AD, the bacteremia and systemic translocation triggered by the gram-negative bacteria present in periodontitis (Ebersole and Cappelli, 2000) might initiate and progress PD (Kaur et al., 2016). The rupture of the BBB allows the entry of macrophages and pro-inflammatory mediators, turning inactive microglia into active ones. When activated, they can produce several inflammatory mediators, such as TNF-α, Il-1β, Il-6, iNOS, and reactive oxygen species (ROS), triggering necrosis and, finally, apoptosis of dopaminergic neurons in the CNS, marking the onset and/or progression of PD. Three of the 12 studies included evaluated this association and detected patients with PD having more severe clinical parameters of periodontitis (Einarsdóttir et al., 2009; Hanaoka and Kashihara, 2009; Müller et al., 2011).
Multiple sclerosis is not yet fully understood, but multiple infections are crucial in the development of the disease; thus, it has also been associated with bacteremia present in periodontitis (Sheu and Lin, 2013). This neurodegenerative disease is an inflammatory condition characterized by demyelination and axonal degeneration. Multiple sclerosis is considered an autoimmune-mediated disease, resulting from several interactions between environmental factors and genetic predisposition (Sheu and Lin, 2013; Bos et al., 2015). These interactions cause an autoimmune response, which in turn causes inflammation in the myelin sheath that surrounds the axons of the CNS (Sheu and Lin, 2013). This disease caused more burden in women than in men (Feigin et al., 2020). One study in our review evaluated this association and conducted further analysis on the odds ratio for earlier worse clinical parameters of periodontitis by sex and detected higher odds in female patients only (Sheu and Lin, 2013); this finding might be related to gender differences in immune responses to chronic infection.
Regarding the methodological quality and risk of bias of individual studies, the checklist developed by Fowkes and Fulton was used (Fowkes and Fulton, 1991), which evaluates the articles according to sample design, control group characteristics, quality of measures and results, integrity, and confounding factors. The main problems were related to the sampling method, sample calculation, and the definition of the control group. Despite that, all included articles were disposed to reproducibility, because they had careful evaluators and calibration to reduce bias.
However, even though they had a low risk of bias, the certainty of the evidence for all analyzed parameters was considered as very low according to the GRADE approach. For this systematic review, it was possible only to gather sufficient information about probing pocket depth for the analysis of the level of evidence. Even though the outcomes presented serious problems related to inconsistency and imprecision because there is high heterogeneity across the included studies, the forms of analysis of the results were different from each study. Also, the separation of the exposed group and the control group was performed differently, hindering the accuracy of the evidence.
Limitations
The main limitation of performing this systematic review was the impossibility of merging data to perform a quantitative analysis. The studies present high heterogeneity due to the variations in the assessment of periodontitis and neurodegenerative across them. Also, it should be highlighted that no cohort study was retrieved regarding the association between periodontal disease and neurodegenerative diseases; therefore, causality cannot be claimed. On the other hand, associations found that inadequately performed studies allow hypotheses to be raised regarding risk. Such approaches can be further studied both to establish a risk factor and to look for common risk factors between both diseases that should be commonly targeted. Also, a bidirectional interference could be considered since the potentially impaired dexterity of arms and fingers in PD, for example, may interfere in oral hygiene care (Vanbellingen et al., 2011).
Conclusions
All the included studies reported higher levels of inflammatory markers, IgG levels of periodontal bacteria, and/or clinical parameters of periodontitis with the two concomitant diseases (some neurodegenerative disease and periodontitis), compared with the diseases isolated (summarized in Figure 2). Despite that we found some minor problems in domains in the qualitative analysis, all the studies have consistent and valid information and were judged to be at low risk of bias. However, when we analyzed the body of the evidence, some problems regarding the imprecision and inconsistency hindered the accuracy of the evidence, alerting us to interpret cautiously the results.
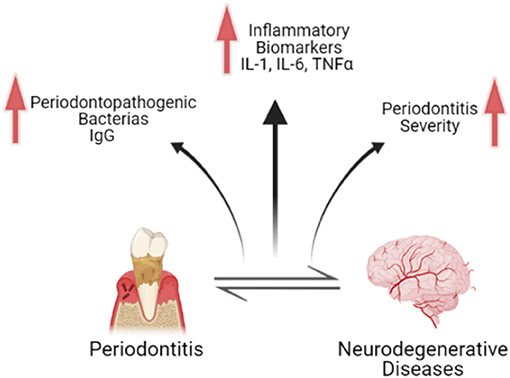
Figure 2. Schematic figure representing the main findings regarding the association between periodontitis and neurodegenerative diseases. The bidirectional relationship between both conditions is associated with the increase of inflammatory biomarkers, increase in immunoglobulins G related to periodontopathogenic bacteria, and increase in periodontitis severity. Schematic figure created with biorender.com.
More longitudinal studies and multicenter trials with larger sample sizes should be conducted to assess whether periodontitis could be a risk factor for the onset and/or progression of neurodegenerative diseases, impacting the quality of life in elderly people. At the moment, it can be concluded that there is an association between neurodegenerative diseases and periodontitis, but causality cannot be claimed.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Materials, further inquiries can be directed to the corresponding author.
Author Contributions
MA drafted the paper with input from all authors. NF and LM designed the study. MA, IM, and LB performed the searches and data extraction. MA and DF performed and interpreted the qualitative analysis. RL and CR revised the manuscript critically for important intellectual content and final approval of the version to be published.
Funding
This research was funded by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brazil (CAPES)—Finance Code 001 and PROCAD Amazônia (23038.005350/2018-78). The APC was funded by Pró-Reitoria de Pesquisa e Pós-graduação from Federal University of Pará (PROPESP-UFPA).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnagi.2021.651437/full#supplementary-material
References
Aragón, F., Zea-Sevilla, M., Montero, J., Sancho, P., Corral, R., Tejedor, C., et al. (2018). Oral health in Alzheimer's disease: a multicenter case-control study. Clin. Oral Investig. 22, 3061–3070. doi: 10.1007/s00784-018-2396-z
Armitage, G. C. (1999). Development of a classification system for periodontal diseases and conditions. Ann. Periodontol. 4, 1–6. doi: 10.1902/annals.1999.4.1.1
Bainbridge, B. W., and Darveau, R. P. (2001). Porphyromonas gingivalis lipopolysaccharide: an unusual pattern recognition receptor ligand for the innate host defense system. Acta Odontol. Scand. 59, 131–138. doi: 10.1080/000163501750266710
Bartova, J., Sommerova, P., Lyuya-Mi, Y., Mysak, J., Prochazkova, J., Duskova, J., et al. (2014). Periodontitis as a risk factor of atherosclerosis. J. Immunol. Res. 2014:636893. doi: 10.1155/2014/636893
Bertram, L., Hiltunen, M., Parkinson, M., Ingelsson, M., Lange, C., Ramasamy, K., et al. (2005). Family-based association between Alzheimer's disease and variants in UBQLN1. N. Engl. J. Med. 352, 884–894. doi: 10.1056/NEJMoa042765
Bilbo, S. D., Wieseler, J. L., Barrientos, R. M., Tsang, V., Watkins, L. R., and Maier, S. F. (2010). Neonatal bacterial infection alters fever to live and simulated infections in adulthood. Psychoneuroendocrinology 35, 369–381. doi: 10.1016/j.psyneuen.2009.07.014
Bos, S. D., Page, C. M., Andreassen, B. K., Elboudwarej, E., Gustavsen, M. W., Briggs, F., et al. (2015). Genome-wide DNA methylation profiles indicate CD8+ T cell hypermethylation in multiple sclerosis. PLoS ONE 10:e0117403. doi: 10.1371/journal.pone.0117403
Bredesen, D. E., Rao, R. V., and Mehlen, P. (2006). Cell death in the nervous system. Nature 443, 796–802. doi: 10.1038/nature05293
Cestari, J. A. F., Fabri, G. M. C., Kalil, J., Nitrini, R., Jacob-Filho, W., and J. T. T. (2016). Oral infections and cytokine levels in patients with Alzheimer's disease and mild cognitive impairment compared with controls. J. Alzheimer Dis. 52, 1479–1485. doi: 10.3233/JAD-160212
Cunningham, C., and Hennessy, E. (2015). Co-morbidity and systemic inflammation as drivers of cognitive decline: new experimental models adopting a broader paradigm in dementia research. Alzheimer Res. Ther. 7, 1–13. doi: 10.1186/s13195-015-0117-2
Curtis, M. (2014). Periodontal microbiology—the lid's off the box again. J. Dental Res. 93, 840–842. doi: 10.1177/0022034514542469
D'aiuto, F., Nibali, L., Parkar, M., Suvan, J., and Tonetti, M. (2005). Short-term effects of intensive periodontal therapy on serum inflammatory markers and cholesterol. J. Dental Res. 84, 269–273. doi: 10.1177/154405910508400312
Ding, Y., Sohn, J. H., Kawczynski, M. G., Trivedi, H., Harnish, R., Jenkins, N. W., et al. (2019). A deep learning model to predict a diagnosis of Alzheimer disease by using 18F-FDG PET of the brain. Radiology 290, 456–464. doi: 10.1148/radiol.2018180958
Dominy, S. S., Lynch, C., Ermini, F., Benedyk, M., Marczyk, A., Konradi, A., et al. (2019). Porphyromonas gingivalis in alzheimer's disease brains: evidence for disease causation and treatment with small-molecule inhibitors. Sci. Adv. 5:eaau3333. doi: 10.1126/sciadv.aau3333
Ebersole, J. L., and Cappelli, D. (2000). Acute-phase reactants in infections and inflammatory diseases. Periodontology 2000 23, 19–49. doi: 10.1034/j.1600-0757.2000.2230103.x
Einarsdóttir, E. R., Gunnsteinsdóttir, H., Hallsdóttir, M. H., Sveinsson, S., Jónsdóttir, S. R., Olafsson, V. G., et al. (2009). Dental health of patients with Parkinson's disease in Iceland. Special Care Dentistry 29, 123–127. doi: 10.1111/j.1754-4505.2009.00075.x
Feigin, V. L., Vos, T., Nichols, E., Owolabi, M. O., Carroll, W. M., Dichgans, M., et al. (2020). The global burden of neurological disorders: translating evidence into policy. Lancet Neurol. 19, 255–265. doi: 10.1016/S1474-4422(19)30411-9
Ferreira, M., Dias-Pereira, A., Branco-de-Almeida, L., Martins, C., and Paiva, S. (2017). Impact of periodontal disease on quality of life: a systematic review. J. Periodontal Res. 52, 651–665. doi: 10.1111/jre.12436
Fowkes, F., and Fulton, P. (1991). Critical appraisal of published research: introductory guidelines. Br. Med. J. 302:1136. doi: 10.1136/bmj.302.6785.1136
Friedewald, V. E., Kornman, K. S., Beck, J. D., Genco, R., Goldfine, A., Libby, P., et al. (2009). The American Journal of Cardiology and Journal of Periodontology editors' consensus: periodontitis and atherosclerotic cardiovascular disease. J. Periodontol. 80, 1021–1032. doi: 10.1902/jop.2009.097001
Gao, H.-M., and Hong, J.-S. (2008). Why neurodegenerative diseases are progressive: uncontrolled inflammation drives disease progression. Trends Immunol. 29, 357–365. doi: 10.1016/j.it.2008.05.002
Gaur, S., and Agnihotri, R. (2015). A lzheimer's disease and chronic periodontitis: is there an association? Geriatrics Gerontol Int. 15, 391–404. doi: 10.1111/ggi.12425
Hajishengallis, G. (2015). Periodontitis: from microbial immune subversion to systemic inflammation. Nat. Rev. Immunol. 15, 30–44. doi: 10.1038/nri3785
Hanaoka, A., and Kashihara, K. (2009). Increased frequencies of caries, periodontal disease and tooth loss in patients with Parkinson's disease. J. Clin. Neurosci. 16, 1279–1282. doi: 10.1016/j.jocn.2008.12.027
Hanes, P. J., and Krishna, R. (2010). Characteristics of inflammation common to both diabetes and periodontitis: are predictive diagnosis and targeted preventive measures possible? EPMA J. 1, 101–116. doi: 10.1007/s13167-010-0016-3
Hill, J. M., Clement, C., Pogue, A. I., Bhattacharjee, S., Zhao, Y., and Lukiw, W. J. (2014). Pathogenic microbes, the microbiome, and Alzheimer's disease (AD). Front. Aging Neurosci. 6:127.
Holmer, J., Eriksdotter, M., Schultzberg, M., Pussinen, P. J., and Buhlin, K. (2018). Association between periodontitis and risk of Alzheimer′ s disease, mild cognitive impairment and subjective cognitive decline: a case–control study. J. Clin. Periodontol. 45, 1287–1298. doi: 10.1111/jcpe.13016
Holmes, C. (2013). Review: systemic inflammation and Alzheimer's disease. Neuropathol. Appl. Neurobiol. 39, 51–68. doi: 10.1111/j.1365-2990.2012.01307.x
Hoogland, I. C. M., Houbolt, C., van Westerloo, D. J., van Gool, W. A., and van de Beek, D. (2015). Systemic inflammation and microglial activation: systematic review of animal experiments. J. Neuroinflamm. 12:114. doi: 10.1186/s12974-015-0332-6
Hussain, R., Zubair, H., Pursell, S., and Shahab, M. (2018). Neurodegenerative diseases: regenerative mechanisms and novel therapeutic approaches. Brain Sci. 8:177. doi: 10.3390/brainsci8090177
Kamer, A. R., Craig, R. G., Pirraglia, E., Dasanayake, A. P., Norman, R. G., Boylan, R. J., et al. (2009). TNF-α and antibodies to periodontal bacteria discriminate between Alzheimer's disease patients and normal subjects. J. Neuroimmunol. 216, 92–97. doi: 10.1016/j.jneuroim.2009.08.013
Kaur, T., Uppoor, A., and Naik, D. (2016). Parkinson's disease and periodontitis–the missing link? A review. Gerodontology 33, 434–438. doi: 10.1111/ger.12188
Martande, S. S., Pradeep, A., Singh, S. P., Kumari, M., Suke, D. K., Raju, A. P., et al. (2014). Periodontal health condition in patients with Alzheimer's disease. Am. J. Alzheimer Dis. Other Dement. 29, 498–502. doi: 10.1177/1533317514549650
Martelli, M. L., Brandi, M. L., Martelli, M., Nobili, P., Medico, E., and Martelli, F. (2017). Periodontal disease and women's health. Curr. Med. Res. Opin. 33, 1005–1015. doi: 10.1080/03007995.2017.1297928
Matsui, H., and Takahashi, R. (2018). Parkinson's disease pathogenesis from the viewpoint of small fish models. J. Neural Transmission 125, 25–33. doi: 10.1007/s00702-017-1772-1
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., and PRISMA Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6:e1000097. doi: 10.1371/journal.pmed.1000097
Movsisyan, A., Melendez-Torres, G. J., and Montgomery, P. (2016). Users identified challenges in applying GRADE to complex interventions and suggested an extension to GRADE. J. Clin. Epidemiol. 70, 191–199. doi: 10.1016/j.jclinepi.2015.09.010
Movsisyan, A. (2018). Applying GRADE in Systematic Reviews of Complex Interventions: Challenges and Considerations for a New Guidance. Oxford: University of Oxford.
Müller, T., Palluch, R., and Jackowski, J. (2011). Caries and periodontal disease in patients with Parkinson's disease. Special Care Dentistry 31, 178–181. doi: 10.1111/j.1754-4505.2011.00205.x
National Academies of Sciences and Medicine, E. (2017). Preventing Cognitive Decline and Dementia: A Way Forward. Washington, DC: National Academies Press.
Nazir, M. A. (2017). Prevalence of periodontal disease, its association with systemic diseases and prevention. Int. J. Health Sci. 11:72.
Noble, J. M., Scarmeas, N., Celenti, R. S., Elkind, M. S., Wright, C. B., Schupf, N., et al. (2014). Serum IgG antibody levels to periodontal microbiota are associated with incident Alzheimer disease. PLoS ONE 9:e114959. doi: 10.1371/journal.pone.0114959
Otomo-Corgel, J., Pucher, J. J., Rethman, M. P., and Reynolds, M. A. (2012). State of the science: chronic periodontitis and systemic health. J. Evid. Based Dental Prac. 12, 20–28. doi: 10.1016/S1532-3382(12)70006-4
Page, R. C., and Kornman, K. S. (1997). The pathogenesis of human periodontitis: an introduction. Periodontology 2000 14, 9–11. doi: 10.1111/j.1600-0757.1997.tb00189.x
Papapanou, P. N., Sanz, M., Buduneli, N., Dietrich, T., Feres, M., Fine, D. H., et al. (2018). Periodontitis: consensus report of workgroup 2 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J. Periodontol. 89, S173–S182. doi: 10.1002/JPER.17-0721
Perry, E., McKeith, I., and Ballard, C. (2003). Butyrylcholinesterase and progression of cognitive deficits in dementia with Lewy bodies. Neurology 60, 1852–1853. doi: 10.1212/01.WNL.0000068336.84399.9E
Perry, V. H., and Teeling, J. (2013). Microglia and macrophages of the central nervous system: the contribution of microglia priming and systemic inflammation to chronic neurodegeneration. Semin. Immunopathol. 35, 601–612. doi: 10.1007/s00281-013-0382-8
Saini, R., Saini, S., and Sugandha, R. (2011). Periodontal disease: the sixth complication of diabetes. Journal of family and community medicine. 18, 31. doi: 10.4103/1319-1683.78636
Sheu, J. J., and Lin, H. C. (2013). Association between multiple sclerosis and chronic periodontitis: a population-based pilot study. Eur. J Neurol. 20, 1053–1059. doi: 10.1111/ene.12103
Stein, P. S., Steffen, M. J., Smith, C., Jicha, G., and Ebersole, J. L. E. (2012). Serum antibodies to periodontal pathogens are a risk factor for Alzheimer's disease. Alzheimer Dement. 8, 196–203. doi: 10.1016/j.jalz.2011.04.006
Syahputra, A., Pasaribu, K., and Pulungan, D. (2018). “The difference of superoxide dismutase levels in patient's saliva with gingivitis associated with dental plaque only before and after scaling at periodontics installation, Faculty of Dentistry USU,” in International Dental Conference of Sumatera Utara 2017 (IDCSU 2017) (Medan: Atlantis Press).
Syrjälä, A. M. H., Ylöstalo, P., Ruoppi, P., Komulainen, K., Hartikainen, S., Sulkava, R., et al. (2012). Dementia and oral health among subjects aged 75 years or older. Gerodontology 29, 36–42. doi: 10.1111/j.1741-2358.2010.00396.x
Tang, Y., and Le, W. (2016). Differential roles of M1 and M2 microglia in neurodegenerative diseases. Mol. Neurobiol. 53, 1181–1194. doi: 10.1007/s12035-014-9070-5
Teixeira, F. B., Saito, M. T., Matheus, F. C., Prediger, R. D., Yamada, E. S., Maia, C. S., et al. (2017). Periodontitis and Alzheimer's disease: a possible comorbidity between oral chronic inflammatory condition and neuroinflammation. Front. Aging Neurosci. 9:327. doi: 10.3389/fnagi.2017.00327
Tonetti, M. S., Van Dyke, T. E., and Working Group 1 of the Joint EFP/AAP Workshop (2013). Periodontitis and atherosclerotic cardiovascular disease: consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Periodontol. 84, S24–S29. doi: 10.1902/jop.2013.1340019
Underly, R., Song, M.-S., Dunbar, G. L., and Weaver, C. L. (2016). Expression of Alzheimer-type neurofibrillary epitopes in primary rat cortical neurons following infection with Enterococcus faecalis. Front. Aging Neurosci. 7:259. doi: 10.3389/fnagi.2015.00259
Vanbellingen, T., Kersten, B., Bellion, M., Temperli, P., Baronti, F., Müri, R., et al. (2011). Impaired finger dexterity in Parkinson's disease is associated with praxis function. Brain Cogn. 77, 48–52. doi: 10.1016/j.bandc.2011.06.003
Webster, J. A., Myers, A. J., Pearson, J. V., Craig, D. W., Hu-Lince, D., Coon, K. D., et al. (2008). Sorl1 as an Alzheimer's disease predisposition gene? Neurodegener. Dis. 5, 60–64. doi: 10.1159/000110789
Keywords: neurodegenerative diseases, Alzheimer's disease, Parkinson's disease, periodontitis, systematic review
Citation: Alvarenga MOP, Frazão DR, Matos IGd, Bittencourt LO, Fagundes NCF, Rösing CK, Maia LC and Lima RR (2021) Is There Any Association Between Neurodegenerative Diseases and Periodontitis? A Systematic Review. Front. Aging Neurosci. 13:651437. doi: 10.3389/fnagi.2021.651437
Received: 09 January 2021; Accepted: 18 February 2021;
Published: 24 May 2021.
Edited by:
Xinglong Wang, University of Nebraska Medical Center, United StatesReviewed by:
Xiaojia Ren, University of Nebraska Medical Center, United StatesGraziela De Luca Canto, Federal University of Santa Catarina, Brazil
Copyright © 2021 Alvarenga, Frazão, Matos, Bittencourt, Fagundes, Rösing, Maia and Lima. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rafael Rodrigues Lima, cmFmYWxpbWFAdWZwYS5icg==