 Sixtus Aguree
Sixtus Aguree Maryam Zolnoori
Maryam Zolnoori Thea Patricia Atwood
Thea Patricia Atwood Arthur Owora
Arthur Owora- 1Department of Applied Health Science, School of Public Health, Indiana University Bloomington, Bloomington, IN, United States
- 2Columbia University Irving Medical Center, New York, NY, United States
- 3Department of Chemistry, Indiana University Bloomington, Bloomington, IN, United States
- 4Department of Pediatrics, School of Medicine, Indiana University, Indianapolis, IN, United States
Background and aims: There is growing evidence suggesting choline intake might have beneficial effects on cognitive function in the elderly. However, some studies report no relationship between choline intake and cognitive function or improvement in Alzheimer’s disease patients. This protocol is for a systematic review of choline intake and Alzheimer’s disease that aims to assess the comparative clinical effectiveness of choline supplementation on Alzheimer’s disease risk.
Methods and analysis: literature search will be performed in PubMed, MEDLINE, EMBASE, CINAHL, Scopus, Cochrane, and the Web of Science electronic databases from inception until October 2023. We will follow the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Studies will be included if they compared two different time points of choline biomarkers measures in men or women (65+) with Alzheimer’s Disease. The risk of bias in the included studies will be assessed within the Covidence data-management software.
Results: This review will summarize the clinical trial and quasi-experimental evidence of choline intake on Alzheimer’s disease risk for adults aged 65+. The results from all eligible studies included in the analysis will be presented in tables, text, and figures. A descriptive synthesis will present the characteristics of included studies (e.g., age, sex of participants, type, length of intervention and comparator, and outcome measures), critical appraisal results, and descriptions of the main findings.
Discussion: This systematic review will summarize the existing evidence on the association between Choline intake and AD and to make recommendations if appropriate. The results of this review will be considered with respect to whether there is enough evidence of benefit to merit a more definitive randomized controlled trial. The results will be disseminated through peer-reviewed journals population.
Conclusion: This protocol outlines the methodology for a systematic review of choline intake and AD. The resulting systematic review from this protocol will form an evidence-based foundation to advance nutrition care for individuals with AD or poor cognitive function.
Systematic review registration: http://www.crd.york.ac.uk/PROSPERO, identifier CRD42023395004.
1. Introduction
Alzheimer’s disease (AD) is a fatal neurodegenerative disorder characterized by cognitive decline, memory loss, behavioral changes, and other neurological symptoms (NIH, 2021). AD is the most common cause of dementia, accounting for 60% to 80% of cases (Alzheimer’s Association, 2023a). It is distinguished by anomalous protein deposits in the brain, such as beta-amyloid plaques and tau tangles (Alzheimer’s Association, 2023a). AD-related cognitive impairment in the US was estimated to affect 6.08 million Americans in 2017 and is projected to reach 15.0 million by 2,060 (Brookmeyer et al., 2018). Approximately 6.7 million American adults age 65+ are living with Alzheimer’s dementia in 2023, projected to reach 13.8 million by 2060 (Alzheimer’s Association, 2023a). AD is debilitating, affecting the patient’s quality of life and their families and creating a high financial burden on the healthcare system (Alzheimer’s Association, 2013, 2023a). Although the precise causes of Alzheimer’s disease are unknown, several risk factors have been identified, including aging and lifestyle factors such as diet (Smith et al., 2010; Alzheimer’s Association, 2013). Age is the strongest predictor or determinant of AD (Hebert et al., 2013)–AD is more common in the elderly over 65 (Alzheimer’s Association, 2011, 2023a; Hebert et al., 2013).
There are limited pharmacological interventions, such as Aducanumab for reduce amyloids levels and slight improvement in symptoms and Donepezil for treating memory and thinking difficulties in moderate-severe dementia (Cummings et al., 2021; Alzheimer’s Association, 2023b). These treatments are often accompanied by serious side effects, including amyloid-related imaging abnormalities, falls, and vomiting (Li et al., 2020). Due to these challenges, attention has turned to alternative approaches, specifically lifestyle modifications (Alzheimer’s Association, 2013; Martins et al., 2021). Of these, dietary supplements have become a primary focus, potentially holding promise in not just decelerating the progression from mild cognitive impairment to dementia but also delaying the advancement toward Alzheimer’s disease (Mosconi and McHugh, 2015; Gardener and Rainey-Smith, 2018; van den Brink et al., 2019). For instance, homocysteine-lowering B vitamins intakes are reported to protect against brain atrophy in the elderly, slowing down mental decline (Smith et al., 2010; Douaud et al., 2013; de Jager, 2014).
Another essential nutrient linked to regulating homocysteine level and brain function is choline. Choline is essential for maintaining the structural integrity of all cells, including brain cells (Hollenbeck, 2012) and studies have reported choline supplementation may benefit individuals with cognitive impairment or neurodegenerative diseases such as Alzheimer’s disease (Smith et al., 2010; Douaud et al., 2013; de Jager, 2014). One possible mechanism linking choline to improved neurocognition is its involvement in regulating one-carbon metabolism (Nurk et al., 2013), which is required for synthesizing phospholipids and other components of cell membranes essential for brain function. Choline is metabolized in the liver to generate a variety of metabolites, including betaine and phosphatidylcholine (Ueland et al., 2005). Betaine can donate a methyl group to homocysteine (an amino acid), generating S-adenosylmethionine (SAM), a critical methyl donor in one-carbon metabolism (Lu et al., 2001; Niculescu and Zeisel, 2002). SAM is an essential methyl donor in one-carbon metabolism and is involved in numerous cellular processes, including DNA and RNA methylation, which modulate gene expression, and neurotransmitter synthesis, which influences brain function (Lu et al., 2001; Bekdash, 2021).
Furthermore, choline is needed to produce acetylcholine, an important neurotransmitter for memory, mood, muscle control, and other brain and nervous system functions (National Academy of Sciences, 1998; Blusztajn et al., 2017). Loss of brain cell membrane function and intercellular communication is a hallmark of Alzheimer’s disease (Azam et al., 2021). Alzheimer’s disease patients are also reported to have decreased levels of the enzyme responsible for converting choline to acetylcholine in the brain (Higgins and Flicker, 2003) and phosphatidylcholine concentration (Whiley et al., 2014). As such, it has been suggested that consuming more phosphatidylcholines may slow the progression of Alzheimer’s disease (Higgins and Flicker, 2003). Phosphatidylcholine can serve as a phospholipid precursor; it may aid in maintaining the structural integrity of neurons, thereby promoting cognitive function in elderly/adults (Leermakers et al., 2015). Approximately 50 percent of the choline ingested in the United States is in the form of phosphatidylcholine (Sanders and Zeisel, 2007; Leermakers et al., 2015). Meat, poultry, fish, dairy products, and eggs are the principal dietary sources of choline in the United States, as they are particularly abundant in choline (Sanders and Zeisel, 2007; Chester et al., 2011; Hollenbeck, 2012; Leermakers et al., 2015).
Few observational studies have found an association between higher choline intakes and plasma concentrations and adult cognitive performance. In one observational study involving 2,195 adults aged 70–74 years in Norway, participants with plasma-free choline concentrations below 8.4 mcmol/L (20th percentile of concentrations in the study population) had poorer sensorimotor speed, perceptual speed, executive function, and global cognition than those with choline concentrations above 8.4 mcmol/L (Nurk et al., 2013). In another study involving 1,391 participants (aged 36–83) from the Framingham Offspring study, those with higher choline intake, as reported by food frequency questionnaires (between 1991–1995 and later 1998–2001), demonstrated enhanced verbal and visual memory (Poly et al., 2011).
Also, several small randomized intervention studies have demonstrated that choline supplements enhance adult cognitive performance (Buchman et al., 2001; Naber et al., 2015). Additional analysis of data (3,224 participants) from the Framingham Heart Study Offspring Cohort exams 5 to 9 revealed that a low choline intake was linked to a higher risk of developing dementia and Alzheimer’s disease (Yuan et al., 2022). These findings are consistent with observational studies showing that higher blood biomarkers of choline and betaine are associated with reduced risk of cognitive impairment in patients with acute ischemic stroke (Zhong et al., 2021). More compelling results linking Alzheimer’s disease and low choline intake, on the one hand, and the neuroprotective effect of supplementing choline in AD have been reported in animal models (Velazquez et al., 2019, 2020; Wang et al., 2019). Furthermore, recent studies reported an association between AD progression and low circulating choline levels in humans (Judd et al., 2023). In mice, dietary choline deficiency affected the function of the hippocampal network related to microtubules, regulation of the postsynaptic membrane, and the networks of proteins associated with mitochondrial function and inflammation (Dave et al., 2023). What is missing is evidence of choline’s effects compiled from pertinent studies. Some questions still remain unanswered, such as:(1) Based on the current body of research, to what extent do deficits contribute to an increased risk of Alzheimer’s disease? (2) To what degree are elevated choline levels (or blood choline concentrations) protective? (3) What is the minimum level of exposure necessary to experience a benefit? One review was conducted almost 10 years ago on the effect of choline and health across the life course. The review found that having higher blood metabolites of choline was associated with a lower risk of developing Alzheimer’s disease (Leermakers et al., 2015). But that review was not specific to Alzheimer’s disease, and there have since been additional studies on choline and Alzheimer’s disease in the elderly.
Systematic reviews are needed to elucidate the connection between choline consumption and Alzheimer’s disease and other forms of dementia. Therefore, we present a protocol of the methodology to undertake a systematic review, to evaluate population-based epidemiological associations between choline intake and Alzheimer’s disease in adults aged 65+ years.
2. Methods
2.1. Study registration
The protocol for this systematic review protocol has been registered with the Prospective Register of Systematic Reviews (PROSPERO) database (University of York, UK; http://www.crd.york.ac.uk/PROSPERO/: PROSPERO, registration number: CRD42023395004). The systematic review adheres to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRIMSA) guidelines (Liberati et al., 2009; Moher et al., 2009). Modifications to the protocol will subsequently be reported in PROSPERO.
2.2. Search strategy and selection criteria
A specific search strategy will be developed by the principal investigators and reviewed by a Health Science Liberian with expertise in systematic review and meta-analysis. The initial search will be developed on PubMed-MEDLINE using varied Medical Subject Headings (MeSH) and free-text terms and then translated into electronic databases. The search will include combinations of keywords related to choline, Alzheimer’s disease or dementia, and aging in the article titles, abstracts, and keywords such as “Alzheimer’s disease,” “AD,” “dementia,” “cognitive function,” “cognitive impairment,” “cognitive decline,” “choline,” or “dimethylglycine” or “trimethylamine N-oxide” or “TMAO” or “Citicoline” or “cytidine 5’-diphosphocholine,” phosphatidylcholine.” The Boolean operators (“AND” and “OR”) will be applied to each term in every set. A comprehensive literature search will be performed on PubMed, Web of Sciences, PsycINFO, EMBASE, SCOPUS, and the Cochrane Library databases to identify relevant studies published between the inception of each database and October 2023. The queries will be re-run just before the final analyses, and additional studies will be retrieved for inclusion. Combinations of choline, Alzheimer’s disease or dementia, and aging-related keywords will be included in article titles, abstracts, and keywords. The search strategy for MEDLINE is displayed in Table 1, for example. The final report will detail the complete search strategy in an appendix. To obtain a more exhaustive retrieval, a manual search of the reference lists of each eligible study will be performed. All considered studies will be imported into reference management software (EndNote software, version 20, Clarivate), and duplicate publications will be deleted.
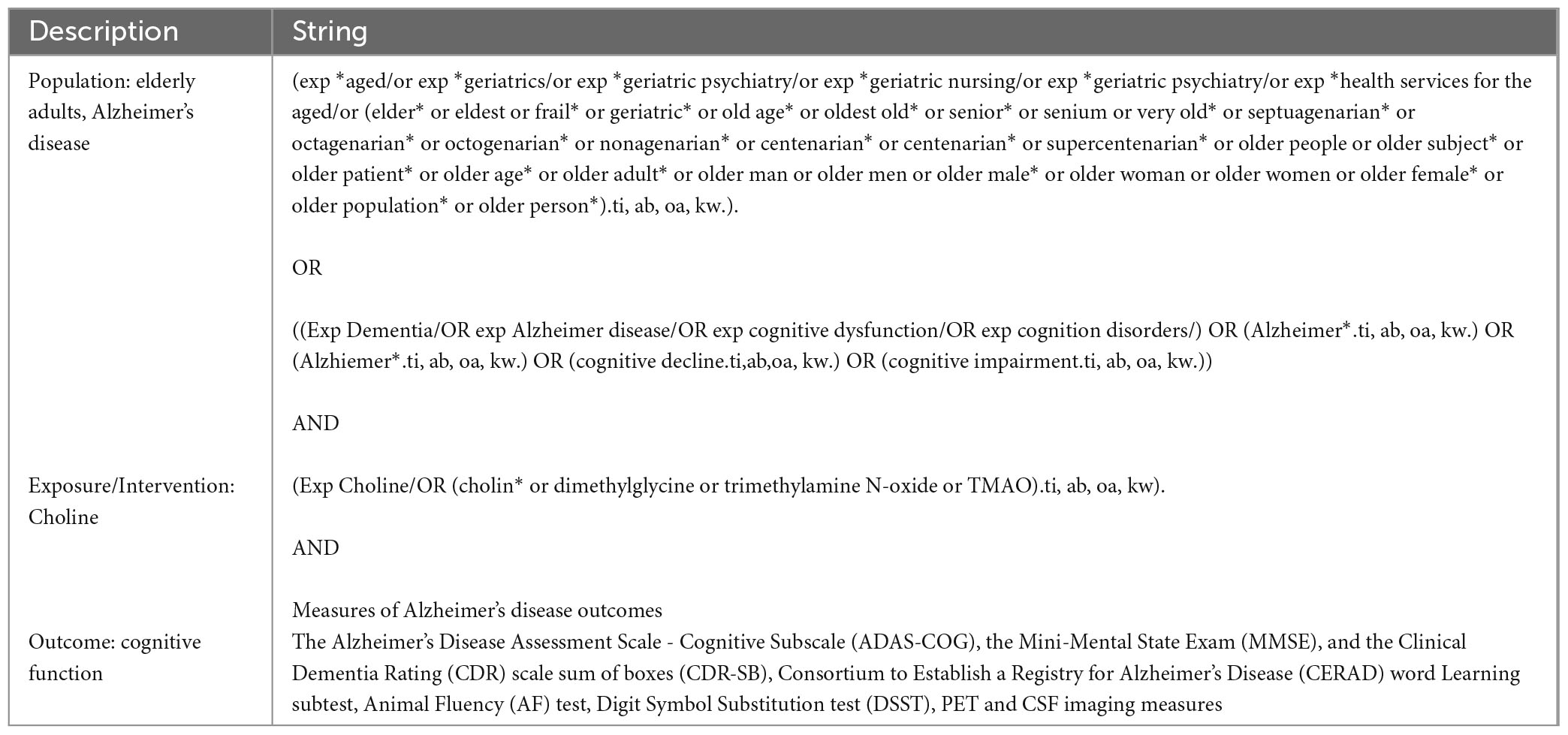
Table 1. Sample search strategy in MEDLINE.
2.3. Inclusion criteria
All AD-related studies meeting the following criteria will be included as eligible articles: (1) original research studies (observational, cross-sectional, case-control, longitudinal, and interventional designs with a control group); (2) human investigations conducted on older adults or the elderly (age 65 and older); (3) studies describing the consumption of dietary choline or choline supplement, or measuring blood biomarkers of choline or dietary or supplemental choline; (4) studies that provided information on the methodologies used to assess AD, dementia, and other cognition-related health outcomes such as cognitive impairment and cognitive decline; (5) reported risk estimates (relative risk or hazard ratios (HRs) and corresponding 95% confidence intervals (CIs) for dementia or AD, or provided enough information to calculate effect size; (6) reported dementia or AD incidence at follow-up, if longitudinal; and (7) studies written in English with entire available texts. The following criteria will be applied to exclude studies:(1) reviews and book chapters or secondary-research evidence such as meta-analysis; (2) non-individual studies such as ecological methods; (3) overlapping studies (the study with the smaller sample size); and (4) studies with incomplete data (in which relative risk or hazard ratios for dementia were not reported or the study was only published as an abstract).
All participants will be included in such investigations, regardless of age, gender, nationality, or inpatient or outpatient status.
2.4. Outcome measures
We will assess the association between choline and AD using data from RCTs, quasi-experimental studies, and observational. We have identified the preferred cognitive outcomes as changes in memory, executive functions, language and communication, judgment and insight, orientation, and spatial cognition. The outcome measure metrics will be measures of association (RR, ORs, regression coefficients, etc.) from these studies. The National Institute on Aging-Alzheimer’s Association (NIA-AA) (Albert et al., 2011; Jack et al., 2011; McKhann et al., 2011; Sperling et al., 2011) and the International Working Group (IWG) (Dubois et al., 2007, 2010, 2014) proposed diagnostic criteria for AD will be used. To be clear, we will consider AD to include both the underlying disease process (pathophysiological, e.g., Aβ amyloidosis) and the various clinical stages of the illness (Sperling et al., 2011). Studies should specifically include AD or ADRD patient population to be considered.
Advancements in neuroimaging [amyloid positron emission tomography (PET)] and cerebrospinal fluid (CSF) assays biomarkers allow for studying the preclinical state of Alzheimer’s pathology (AP) (Dubois et al., 2016) to detect evidence of Alzheimer’s disease in vivo (Pontecorvo and Mintun, 2011; Bateman et al., 2012; Johnson et al., 2013; Dubois et al., 2016). These advances have been incorporated into the new NIA-AA and IWG criteria for defining AD. Because NIA-AA and IWG are relatively new revision to National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) criteria which has been in existence for about four decades McKhann et al. (1984), we expect most available studies to be based on NINCDS-ADRDA. Thus, studies where clinical diagnosis of AD was based on the NINCDS-ADRDA criteria will be accepted. The NINCDS-ADRDA approach involves evaluating cognitive and functional impairments through clinical assessments while ruling out other potential causes of dementia.
Thus, we would consider studies suitable for inclusion if they have reported a measurable impact of choline on cognitive function, such as improvement in cognitive assessment tests (e.g., performance-based assessments of cognitive functions such as the Alzheimer’s Disease Assessment Scale - Cognitive Subscale (ADAS-COG), the Mini-Mental State Exam (MMSE), and the Clinical Dementia Rating (CDR) scale sum of boxes (CDR-SB), Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) word Learning subtest, Animal Fluency (AF) test, Digit Symbol Substitution test (DSST), PET and CSF imaging measures, or other AD biomarkers. Conversely, studies focusing solely on the impact of choline on sleep will be excluded from our review since they do not align with our defined outcomes. Cognitive assessment based on self-report will also be excluded as they have been shown to be unreliable.
2.5. Data collection and analysis
Pre-designed, standardized data extraction forms will be created to record pertinent information from each included study. Data extraction will be performed using Covidence software1 (Babineau, 2014; Covidence, 2020). All citations identified by our search strategy will be imported into Covidence systematic review software, where duplicates will automatically remove. Two reviewers will independently screen the studies for titles and abstracts against the inclusion and exclusion criteria. A third reviewer will solve conflicts and discrepancies that emerged during the two screening stages. The reference lists of eligible studies will also be screened to identify additional studies that might have been missed.
The data to be extracted from the eligible articles are the first author’s name, year of publication, the country where the study was conducted, study design, method of randomization, exposure or intervention details (which can include assessment method, distribution in the study population, and dosage when describing choline supplements), control group details, sample size, patient demographics, including age and sex, criteria used to diagnose AD, all outcome measures, follow-up duration, dietary intervention protocol, main results, distribution of results, statistical methods, and adjustment.
A final collation of data will be imported into STATA for statistical review and analysis. Each final article will be subjected to a quality and risk of bias assessment within Covidence. The Covidence software has a built-in Cochrane risk of bias assessment tool. We will use the Cochrane risk-of-bias tool for randomized trials (RoB 2) to assess the risk of bias in randomized trials and the ROBINS-I tool to assess non-randomized studies of interventions included in the study (Sterne et al., 2016, 2019). The GRADE (grading of recommendation, assessment, development, and evaluation) assessment will then be conducted to evaluate the included studies. The GRADE assessment determines the quality of evidence by considering factors such as study design, risk of biases, precision, consistency, directness, and other reported aspects. The evidence is then classified as very low, low, moderate, or high.
Statistical analysis will be performed using STATA software 17.0 (Stata Corporation, College Station, TX, USA) with the contributed “metan” (Harris et al., 2008), “metabias” (Harbord et al., 2009), and “confunnel” (Palmer et al., 2008; Peters et al., 2008) packages. Study heterogeneity will be assessed using I2 estimations. The I2 estimation is a statistical measure representing the percentage of variation across studies due to heterogeneity rather than chance. Using Cochrane review group criteria, study heterogeneity (Higgins et al., 2003) will be divided into three levels: low heterogeneity (I2 < 25%), moderate heterogeneity (I2 25–50%), and high heterogeneity (I2 > 50%). Cochran Q statistics will be conducted to evaluate the heterogeneity between studies, where P < 0.10 will be regarded as statistically significant. A P > 0.10 in the Q test and I2 < 50% will indicate no heterogeneity. A formal meta-analysis will be conducted if deemed suitable based on the quantity and quality of eligible studies. We will use a fixed effects model if no statistical heterogeneity is detected; otherwise, a random effects model will be used. RR, ORs, and regression coefficients will be considered measures of effect size for eligible studies. We will use forest plots to depict the results graphically. Publication bias will be evaluated by the funnel plot and Begg’s test. Visually symmetrical distribution of data points (p > 0.05) will be considered as indicating no (low) publication bias. We will perform a leave-one-out analysis to assess the influence of each study. This sensitivity analysis evaluates each study’s influence on the overall pooled effect size by omitting one study at a time to examine the stability of the results. Subgroup analyses will consider age (<80 vs. >80), duration of intervention, study design (RCT vs. observational), and differences between men and women. A 2-tailed P < 0.05 will be considered statistically significant.
We will perform a narrative synthesis if there is a high heterogeneity (I2 > 50%) study, such as in study designs, exposure, outcome measures, and analytical methods that makes it inappropriate to statistically combine all the included studies in a meta-analysis. A formal narrative synthesis on quantitative studies will be undertaken according to the reporting guideline of the synthesis without meta-analysis (SWiM) (Campbell et al., 2020). The included studies will be grouped by study designs and ordered by publication years. Vote-counting methods based on directions of effect and P-values will be applied. Quality assessments on studies included will be considered when interpreting findings.
3. Discussion
This will be the first systematic evaluating of the effect of choline intake on AD. There is evidence that choline consumption might help improve cognitive performance or delay cognitive deterioration in the elderly, but a systematic review on this topic is currently lacking. The proposed systematic review will strengthen the evidence base on what is known regarding associations between choline intake and AD by identifying, evaluating, and synthesizing the findings of existing clinical and observational studies on this topic. We will conduct a structured literature search using the Medline, EMBASE, and Cochrane CENTRAL databases from inception to October 2023. Then formal inclusion and exclusion criteria will be applied to the review articles found via these searchers to obtain eligible studies for further evaluation. From the eligible articles, we will perform data extraction, validity assessment, and meta-analyses if appropriate. Appropriateness for meta-analysis will be based on the total number of eligible studies meeting quality control checks. If heterogeneity (e.g., I2 = 50%) is detected, subgroup/sensitivity analysis may be used to explore the possible sources. If meta-analysis is not feasible based on the quality studies, narrative reviews will be performed.
Our report will be divided into two sections. The first section will delve into patients suffering from MCI, including pathophysiological conditions such as Aβ amyloidosis and symptomatic and amnestic cases. The second section will focus on individuals who have been diagnosed with Alzheimer’s disease, with a particular emphasis on the clinical stage of the condition. The implications of this systematic review extend beyond the immediate research community. If our study suggests a potential benefit of choline in combating the effects of AD, it could catalyze the initiation of a larger, more definitive randomized controlled trial. This could potentially bring us closer to an effective dietary strategy for mitigating the impact of AD, a leading cause of functional impairment in the elderly population, thus having profound implications for public health and healthcare policy.
Data availability statement
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
This study is exempt from ethics approval or consent procedures as it does not include identifiable human data.
Author contributions
SA: conceptualization, methodology (search strategy for English databases, analysis tools), investigation, data curation, project administration, writing—original draft, and writing—review and editing. MZ: methodology (search strategy for English databases, analysis tools), investigation, data curation, and writing—review and editing. TA: methodology, validation, and writing—review and editing. AO: conceptualization, methodology, validation, supervision, and writing—review and editing. All authors contributed to the article and approved the final version.
Funding
This study was partly funded by internal funds from the Indiana University School of Public Health, Bloomington, Indiana, USA.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
Albert, M. S., Albert, M. S., Knopman, D. S., McKhann, G. M., Sperling, R. A., Carrillo, M. C., et al. (2011). The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 7, 270–279. doi: 10.1016/j.jalz.2011.03.008
Alzheimer’s Association (2011). 2011 Alzheimer’s disease facts and figures. Alzheimers Dement. 7, 208–244. doi: 10.1016/j.jalz.2011.02.004
Alzheimer’s Association (2013). 2013 Alzheimer’s disease facts and figures. Alzheimers Dement. 9, 208–245. doi: 10.1016/j.jalz.2013.02.003
Alzheimer’s Association (2023a). 2023 Alzheimer’s disease facts and figures. Alzheimers Dement. 19, 1598–1695. doi: 10.1002/alz.13016
Alzheimer’s Association (2023b). 2023 Alzheimer’s Association webpage. Available online at: https://www.alz.org/alzheimers-dementia/treatments/medications-for-memory (accessed June 10, 2023).
Azam, S., Haque, M. E., Balakrishnan, R., Kim, I. S., and Choi, D. K. (2021). The ageing brain: Molecular and cellular basis of neurodegeneration. Front. Cell Dev. Biol. 9:683459. doi: 10.3389/fcell.2021.683459
Babineau, J. (2014). Product review: Covidence (Systematic Review Software). J. Can. Health Libr. Assoc. 35, 68–71. doi: 10.5596/c14-016
Bateman, R. J., Xiong, C., Benzinger, T. L., Fagan, A. M., Goate, A., Fox, N. C., et al. (2012). Clinical and biomarker changes in dominantly inherited Alzheimer’s disease. N. Engl. J. Med. 367, 795–804. doi: 10.1056/NEJMoa1202753
Bekdash, R. A. (2021). Early life nutrition and mental health: The role of DNA methylation. Nutrients 13:3111. doi: 10.3390/nu13093111
Blusztajn, J. K., Slack, B. E., and Mellott, T. J. (2017). Neuroprotective actions of dietary choline. Nutrients 9:815. doi: 10.3390/nu9080815
Brookmeyer, R., Abdalla, N., Kawas, C. H., and Corrada, M. M. (2018). Forecasting the prevalence of preclinical and clinical Alzheimer’s disease in the United States. Alzheimers Dement. 14, 121–129. doi: 10.1016/j.jalz.2017.10.009
Buchman, A. L., Sohel, M., Brown, M., Jenden, D. J., Ahn, C., Roch, M., et al. (2001). Verbal and visual memory improve after choline supplementation in long-term total parenteral nutrition: A pilot study. JPEN J Parenter. Enteral Nutr. 25, 30–35. doi: 10.1177/014860710102500130
Campbell, M., McKenzie, J. E., Sowden, A., Katikireddi, S. V., Brennan, S. E., Ellis, S., et al. (2020). Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ 368:l6890. doi: 10.1136/bmj.l6890
Chester, D. N., Goldman, J. D., Ahuja, J. K., and Moshfegh, A. J. (2011). Dietary intakes of choline: What we eat in America, NHANES 2007-2008. Food Surveys Research Group dietary data brief No. 9. October 2011. Available online at: http://ars.usda.gov/Services/docs.htm?docid=19476 (accessed March 31, 2023).
Covidence (2020). Covidence: Better systematic review management. Available online at: https://www.covidence.org/home (accessed March 10, 2023).
Cummings, J., Aisen, P., Lemere, C., Atri, A., Sabbagh, M., and Salloway, S. (2021). Aducanumab produced a clinically meaningful benefit in association with amyloid lowering. Alzheimers Res. Ther. 13:98. doi: 10.1186/s13195-021-00838-z
Dave, N., Judd, J. M., Decker, A., Winslow, W., Sarette, P., Villarreal Espinosa, O., et al. (2023). Dietary choline intake is necessary to prevent systems-wide organ pathology and reduce Alzheimer’s disease hallmarks. Aging Cell 22:e13775. doi: 10.1111/acel.13775
de Jager, C. A. (2014). Critical levels of brain atrophy associated with homocysteine and cognitive decline. Neurobiol. Aging 35, S35–S39. doi: 10.1016/j.neurobiolaging.2014.03.040
Douaud, G., Refsum, H., de Jager, C. A., Jacoby, R., Nichols, T. E., Smith, S. M., et al. (2013). Preventing Alzheimer’s disease-related gray matter atrophy by B-vitamin treatment. Proc. Natl. Acad. Sci. U.S.A. 110, 9523–9528. doi: 10.1073/pnas.1301816110
Dubois, B., Feldman, H. H., Jacova, C., Cummings, J. L., Dekosky, S. T., Barberger-Gateau, P., et al. (2010). Revising the definition of Alzheimer’s disease: A new lexicon. Lancet Neurol. 9, 1118–1127. doi: 10.1016/S1474-4422(10)70223-4
Dubois, B., Feldman, H. H., Jacova, C., Dekosky, S. T., Barberger-Gateau, P., Cummings, J., et al. (2007). Research criteria for the diagnosis of Alzheimer’s disease: Revising the NINCDS-ADRDA criteria. Lancet Neurol. 6, 734–746. doi: 10.1016/S1474-4422(07)70178-3
Dubois, B., Feldman, H. H., Jacova, C., Hampel, H., Molinuevo, J. L., Blennow, K., et al. (2014). Advancing research diagnostic criteria for Alzheimer’s disease: The IWG-2 criteria. Lancet Neurol. 13, 614–629. doi: 10.1016/S1474-4422(14)70090-0
Dubois, B., Hampel, H., Feldman, H. H., Scheltens, P., Aisen, P., Andrieu, S., et al. (2016). Preclinical Alzheimer’s disease: Definition, natural history, and diagnostic criteria. Alzheimers Dement. 12, 292–323. doi: 10.1016/j.jalz.2016.02.002
Gardener, S. L., and Rainey-Smith, S. R. (2018). The role of nutrition in cognitive function and brain ageing in the elderly. Curr. Nutr. Rep. 7, 139–149. doi: 10.1007/s13668-018-0229-y
Harbord, R. M., Harris, R. J., and Sterne, J. A. C. (2009). Updated tests for small-study effects in meta-analyses. Stata J. 9, 197–210. doi: 10.1177/1536867X0900900202
Harris, R. J., Deeks, J. J., Altman, D. G., Bradburn, M. J., Harbord, R. M., and Sterne, J. A. C. (2008). metan: Fixed- and random-effects meta-analysis. Stata J. 8, 3–28. doi: 10.1177/1536867X0800800102
Hebert, L. E., Weuve, J., Scherr, P. A., and Evans, D. A. (2013). Alzheimer disease in the United States (2010–2050) estimated using the 2010 census. Neurology 80, 1778–1783. doi: 10.1212/WNL.0b013e31828726f5
Higgins, J. P., and Flicker, L. (2003). Lecithin for dementia and cognitive impairment. Cochrane Database Syst. Rev. 2003:Cd001015.
Higgins, J. P., Thompson, S. G., Deeks, J. J., and Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ 327, 557–560. doi: 10.1136/bmj.327.7414.557
Hollenbeck, C. B. (2012). An introduction to the nutrition and metabolism of choline. Cent. Nerv. Syst. Agents Med. Chem. 12, 100–113. doi: 10.2174/187152412800792689
Jack, C. R. Jr., Albert, M. S., Knopman, D. S., McKhann, G. M., Sperling, R. A., Carrillo, M. C., et al. (2011). Introduction to the recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 7, 257–262. doi: 10.1016/j.jalz.2011.03.004
Johnson, K. A., Sperling, R. A., Gidicsin, C. M., Carmasin, J. S., Maye, J. E., Coleman, R. E., et al. (2013). Florbetapir (F18-AV-45) PET to assess amyloid burden in Alzheimer’s disease dementia, mild cognitive impairment, and normal aging. Alzheimers Dement. 9(5 Suppl), S72–S83. doi: 10.1016/j.jalz.2012.10.007
Judd, J. M., Jasbi, P., Winslow, W., Serrano, G. E., Beach, T. G., Klein-Seetharaman, J., et al. (2023). Inflammation and the pathological progression of Alzheimer’s disease are associated with low circulating choline levels. Acta Neuropathol. doi: 10.1007/s00401-023-02616-7 [Epub ahead of print].
Leermakers, E. T., Moreira, E. M., Kiefte-de Jong, J. C., Darweesh, S. K., Visser, T., Voortman, T., et al. (2015). Effects of choline on health across the life course: A systematic review. Nutr. Rev. 73, 500–522. doi: 10.1093/nutrit/nuv010
Li, H. C., Luo, K. X., Wang, J. S., and Wang, Q. X. (2020). Extrapyramidal side effect of donepezil hydrochloride in an elderly patient: A case report. Medicine 99:e19443. doi: 10.1097/MD.0000000000019443
Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., Ioannidis, J. P., et al. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 6:e1000100. doi: 10.1371/journal.pmed.1000100
Lu, S. C., Alvarez, L., Huang, Z. Z., Chen, L., An, W., Corrales, F. J., et al. (2001). Methionine adenosyltransferase 1A knockout mice are predisposed to liver injury and exhibit increased expression of genes involved in proliferation. Proc. Natl. Acad. Sci. U.S.A. 98, 5560–5565. doi: 10.1073/pnas.091016398
Martins, L. B., Malheiros Silveira, A. L., and Teixeira, A. L. (2021). The link between nutrition and Alzheimer’s disease: From prevention to treatment. Neurodegener. Dis. Manag. 11, 155–166. doi: 10.2217/nmt-2020-0023
McKhann, G. M., Knopman, D. S., Chertkow, H., Hyman, B. T., Jack, C. R. Jr., Kawas, C. H., et al. (2011). The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 7, 263–269. doi: 10.1016/j.jalz.2011.03.005
McKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D., and Stadlan, E. (1984). Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA work group under the auspices of department of health and human services task force on Alzheimer’s disease. Neurology 34, 939–944. doi: 10.1212/wnl.34.7.939
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., and Prisma Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 6:e1000097. doi: 10.1371/journal.pmed.1000097
Mosconi, L., and McHugh, P. F. (2015). Let food be thy medicine: Diet, nutrition, and biomarkers’ risk of Alzheimer’s disease. Curr. Nutr. Rep. 4, 126–135. doi: 10.1007/s13668-014-0111-5
Naber, M., Hommel, B., and Colzato, L. S. (2015). Improved human visuomotor performance and pupil constriction after choline supplementation in a placebo-controlled double-blind study. Sci. Rep. 5:13188. doi: 10.1038/srep13188
National Academy of Sciences (1998). The National Academies Collection: Reports funded by National Institutes of Health, in Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B(6), Folate, Vitamin B(12), Pantothenic Acid, Biotin, and Choline. Washington, DC: National Academies Press.
Niculescu, M. D., and Zeisel, S. H. (2002). Diet, methyl donors and DNA methylation: Interactions between dietary folate, methionine and choline. J. Nutr. 132(8 Suppl), 2333s–2335s. doi: 10.1093/jn/132.8.2333S
NIH (2021). What Is Alzheimer’s Disease? NIH National Institute on Aging website. Available online at: https://www.nia.nih.gov/health/what-alzheimers-disease (accessed May 30, 2023).
Nurk, E., Refsum, H., Bjelland, I., Drevon, C. A., Tell, G. S., Ueland, P. M., et al. (2013). Plasma free choline, betaine and cognitive performance: The Hordaland Health Study. B.r J. Nutr. 109, 511–519. doi: 10.1017/S0007114512001249
Palmer, T. M., Sutton, A. J., Peters, J. L., and Moreno, S. G. (2008). Contour-enhanced funnel plots for meta-analysis. Stata J. 8, 242–254. doi: 10.1177/1536867X0800800206
Peters, J. L., Sutton, A. J., Jones, D. R., Abrams, K. R., and Rushton, L. (2008). Contour-enhanced meta-analysis funnel plots help distinguish publication bias from other causes of asymmetry. J. Clin. Epidemiol. 61, 991–996. doi: 10.1016/j.jclinepi.2007.11.010
Poly, C., Massaro, J. M., Seshadri, S., Wolf, P. A., Cho, E., Krall, E., et al. (2011). The relation of dietary choline to cognitive performance and white-matter hyperintensity in the Framingham Offspring Cohort. Am. J. Clin. Nutr. 94, 1584–1591. doi: 10.3945/ajcn.110.008938
Pontecorvo, M. J., and Mintun, M. A. (2011). PET amyloid imaging as a tool for early diagnosis and identifying patients at risk for progression to Alzheimer’s disease. Alzheimers Res. Ther. 3:11. doi: 10.1186/alzrt70
Sanders, L. M., and Zeisel, S. H. (2007). Choline: Dietary requirements and role in brain development. Nutr. Today 42, 181–186. doi: 10.1097/01.NT.0000286155.55343.fa
Smith, A. D., Smith, S. M., de Jager, C. A., Whitbread, P., Johnston, C., Agacinski, G., et al. (2010). Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment: A randomized controlled trial. PLoS One 5:e12244. doi: 10.1371/journal.pone.0012244
Sperling, R. A., Aisen, P. S., Beckett, L. A., Bennett, D. A., Craft, S., Fagan, A. M., et al. (2011). Toward defining the preclinical stages of Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 7, 280–292. doi: 10.1016/j.jalz.2011.03.003
Sterne, J. A. C., Savović, J., Page, M. J., Elbers, R. G., Blencowe, N. S., Boutron, I., et al. (2019). RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 366:l4898. doi: 10.1136/bmj.l4898
Sterne, J. A., Hernán, M. A., Reeves, B. C., Savović, J., Berkman, N. D., Viswanathan, M., et al. (2016). ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355:i4919. doi: 10.1136/bmj.i4919
Ueland, P. M., Holm, P. I., and Hustad, S. (2005). Betaine: A key modulator of one-carbon metabolism and homocysteine status. Clin. Chem. Lab. Med. 43, 1069–1075. doi: 10.1515/CCLM.2005.187
van den Brink, A. C., Brouwer-Brolsma, E. M., Berendsen, A. A. M., and van de Rest, O. (2019). The Mediterranean, dietary approaches to stop hypertension (DASH), and Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diets Are Associated with Less Cognitive Decline and a Lower Risk of Alzheimer’s Disease-A Review. Adv. Nutr. 10, 1040–1065. doi: 10.1093/advances/nmz054
Velazquez, R., Ferreira, E., Knowles, S., Fux, C., Rodin, A., Winslow, W., et al. (2019). Lifelong choline supplementation ameliorates Alzheimer’s disease pathology and associated cognitive deficits by attenuating microglia activation. Aging Cell 18:e13037. doi: 10.1111/acel.13037
Velazquez, R., Ferreira, E., Winslow, W., Dave, N., Piras, I. S., Naymik, M., et al. (2020). Maternal choline supplementation ameliorates Alzheimer’s disease pathology by reducing brain homocysteine levels across multiple generations. Mol. Psychiatry 25, 2620–2629. doi: 10.1038/s41380-018-0322-z
Wang, Y., Guan, X., Chen, X., Cai, Y., Ma, Y., Ma, J., et al. (2019). Choline supplementation ameliorates behavioral deficits and Alzheimer’s disease-like pathology in transgenic APP/PS1 mice. Mol. Nutr. Food Res. 63:1801407. doi: 10.1002/mnfr.201801407
Whiley, L., Sen, A., Heaton, J., Proitsi, P., García-Gómez, D., Leung, R., et al. (2014). Evidence of altered phosphatidylcholine metabolism in Alzheimer’s disease. Neurobiol. Aging 35, 271–278. doi: 10.1016/j.neurobiolaging.2013.08.001
Yuan, J., Liu, X., Liu, C., Ang, A. F., Massaro, J., Devine, S. A., et al. (2022). Is dietary choline intake related to dementia and Alzheimer’s disease risks? Results from the Framingham Heart Study. Am. J. Clin. Nutr. 116, 1201–1207. doi: 10.1093/ajcn/nqac193
Keywords: one-carbon metabolism, dementia, nutrition and cognition, aging, geriatrics, nutrition and brain, acetylcholine
Citation: Aguree S, Zolnoori M, Atwood TP and Owora A (2023) Association between choline supplementation and Alzheimer’s disease risk: a systematic review protocol. Front. Aging Neurosci. 15:1242853. doi: 10.3389/fnagi.2023.1242853
Received: 19 June 2023; Accepted: 15 August 2023;
Published: 28 August 2023.
Edited by:
Matthew G. Pontifex, University of East Anglia, United KingdomReviewed by:
Omonigho Michael Bubu, New York University, United StatesRamon Velazquez, Arizona State University, United States
Copyright © 2023 Aguree, Zolnoori, Atwood and Owora. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sixtus Aguree, c2FndXJlZUBpdS5lZHU=