 Kerri M. Gillespie
Kerri M. Gillespie Eva Kemps
Eva Kemps Melanie J. White
Melanie J. White Selena E. Bartlett
Selena E. Bartlett- 1Faculty of Health, School of Clinical Sciences, Queensland University of Technology, Kelvin Grove, QLD, Australia
- 2College of Education, Psychology and Social Work, Flinders University, Adelaide, SA, Australia
- 3Faculty of Health, School of Psychology and Counselling, Queensland University of Technology, Kelvin Grove, QLD, Australia
Introduction: Alcohol consumption is commonly considered to be a modifiable risk factor in cognitive decline. However, numerous studies have found an association between light to moderate consumption of alcohol and enhanced cognitive function. It has been proposed that this finding is due to the effects of socioeconomic status (SES) or other covariates on drinking behaviors. The present study aimed to investigate the effect of alcohol on cognition, and the impact of different socioeconomic indicators on this relationship.
Methods: An online, cross-sectional survey, including an assessment of five domains of cognitive function, was conducted in 123 healthy adults between 18 and 70 years of age. Secondary analysis of the 2018 National Health Survey was conducted to investigate drinking patterns, and their relationships to SES indicators, in the Australian population.
Results: Income and education showed dissimilar patterns of association with alcohol consumption. Enhancements in cognitive function were associated with light to moderate dose and frequency of alcohol consumption when unadjusted, or adjusted for SES using education level as an indicator. Benefits of light to moderate dose and frequency of consumption were not evident when using income as an indicator for SES. Inclusion of language spoken in the home as a covariate also resolved any association between moderate consumption and enhanced cognitive function.
Discussion: Findings suggest that associations between moderate alcohol consumption and cognition are an artifact of income, language proficiency, and culture. The use of income is more indicative of drinking behavior than education, and should be controlled for in studies of alcohol consumption behavior. Language spoken at home is also an important consideration as this factor is significantly associated with income, alcohol consumption, and cognitive test performance.
1 Introduction
Alcohol is considered a modifiable risk factor for cognitive decline. Excessive consumption can lead to changes in the brain similar to those seen in aging, with significant reductions in gray and white matter volume (Squeglia et al., 2014; Guerri and Pascual, 2019; Daviet et al., 2022). Large cohort, biobank, and brain imaging studies have found even light consumption associated with reductions in cortical volume and increased risk of dementia (Topiwala et al., 2017; Immonen et al., 2020; Daviet et al., 2022; Zheng et al., 2024). However, a large number of epidemiologic studies have identified an association between moderate, regular alcohol consumption and a decreased risk for cognitive decline and dementia (den Heijer et al., 2004; Almeida et al., 2014; Reas et al., 2016; Xu et al., 2017; Zhang et al., 2020; Akagi et al., 2022; Jeon et al., 2023).
Reasons for these conflicting findings have been proposed, but are still unclear. Stockwell et al. (2024) reviewed studies that associated lower mortality risk with low to moderate alcohol consumption and found they were more likely to rate alcohol consumption based on a short retrospective period (days or months); include older participants (aged over 55 years); include ex-drinkers in the non-drinking category; and control for smoking and socioeconomic status (SES). Smoking has been suggested as a mediator for alcohol use, and its complex relationship to alcohol and health may make it inappropriate to include as a covariate (Stockwell et al., 2024). Naimi et al. (2017) highlight the fact that those who stop drinking tend to have worse overall health, further biasing current non-drinkers toward ill health.
Socioeconomic status, and how it is measured, is another mechanism for potential bias (Towers et al., 2016; Gómez et al., 2021). Population survey data suggests that people with lower SES drink infrequently but in higher volumes than their higher SES counterparts [Centers for Disease Control and Prevention [CDC], 2012], while higher SES individuals frequently consume low or moderate amounts of alcohol (Casswell et al., 2003; Platt et al., 2010; Towers et al., 2016), biasing moderate drinkers toward improved health and cognition. A study of younger adults found drinking was positively associated with income, educational attainment, and health (Ng Fat and Shelton, 2012). Wine in particular has been associated with reduced cognitive risk (Neafsey and Collins, 2011; Xu et al., 2017), and is also associated with greater intelligence, more education, and higher SES (Mortensen et al., 2001). One proposed mechanism is via an improvement in cardiovascular health due to moderate alcohol intake (Ronksley et al., 2011). However, suggested cardioprotective effects of alcohol may also be an artifact of SES. Norström and Landberg (2023) identified that increased alcohol consumption led to increased ischemic heart disease mortality, but only in low SES groups.
A common indicator of SES is educational achievement or years of education, which may be a poor gauge of SES (Darin-Mattsson et al., 2017). Education has frequently shown a weaker association with health in later life than income (Darin-Mattsson et al., 2017). Tertiary education is becoming increasingly common, biasing older participants toward a lower education classification (Galobardes et al., 2006). Education and income also show different patterns of association with alcohol consumption. A population-based study in Japan (Murakami and Hashimoto, 2019) found low educational attainment was associated with greater risk of heavy drinking, while lower income was associated with a lower risk.
Cultural and linguistic background may also bias findings. The Australian Bureau of Statistics (ABS) (Australian Bureau of Statistics, 2011) found that citizens born in Australia who spoke a language other than English in the home had higher levels of education than those speaking mostly English. Individuals from a culturally and linguistically diverse (CALD) background are also less likely to drink alcohol (Australian Institute of Health and Welfare, 2024) and have lower incomes (Wang et al., 2023). Studies have also found significant impacts of language proficiency and multilingualism on cognitive test performance (Cormier et al., 2022; Pacifico et al., 2023). Despite the strong relationship between CALD membership, alcohol consumption, SES, and cognitive test outcomes, language spoken in the home and English language proficiency are rarely, if ever, controlled for in studies investigating the impacts of alcohol consumption on cognitive function.
The aim of this study was to examine the relationships between patterns of alcohol consumption and cognitive function, and investigate how these relationships are influenced by covariates. We therefore evaluated the impacts of alcohol dose and consumption frequency on neurocognitive domains. The differential effects of adjusting for covariates relating to education, income, and language was then investigated. Data from the 2018 National Health Survey were used to support these findings by investigating the relationships between these covariates in the Australian population.
2 Materials and methods
2.1 Study design and sample description
This cross-sectional study was reported in accordance with the Strengthening the Reporting of OBservational studies in Epidemiology (STROBE) reporting guidelines (Cuschieri, 2019). The study incorporated online, quantitative data collection to capture data for our “cognition study.” The recruitment period was between the 12th of June and 17th of November, 2023. Individuals were recruited if they were between 18 and 70 years of age, were able to read and write English, and had the use of a computer, laptop, or tablet that could access the internet. Individuals were not able to participate if they had a current or previous major psychiatric illness, substance use disorder, or eating disorder, or were experiencing a serious health condition or taking medications that influenced their thinking, diet, blood sugar levels, or weight. The study recruited 144 healthy adults from the community. Two of these were flagged as suspicious by the survey software (Qualtrics) and a further 14 were removed for failing to complete the cognitive assessment. Five participants not residing in Australia were removed to enable comparable analysis of income and socioeconomic status, leaving 123 participants in the final sample (see Table 1).
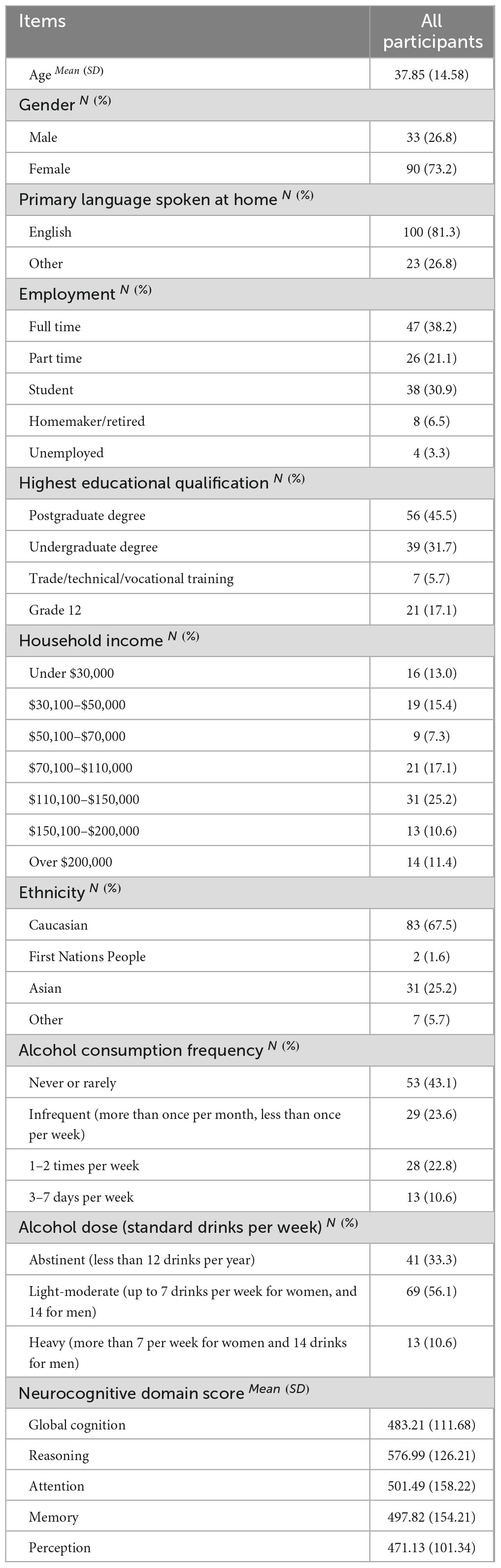
Table 1. Sample descriptives.
The National Health Survey (NHS) is a country-wide household-based health survey conducted every 3–6 years by the Australian Bureau of Statistics (Australian Bureau of Statistics, 2018). We conducted secondary analysis of weighted data from 16,370 adults included in the 2018 NHS.
2.2 Ethical statement
This study was approved by the Queensland University of Technology Human Research Ethics Committee (Ethics ID: 5872). All participants gave written, informed consent, before participating in online surveys.
2.3 Sample size calculation
A sample size calculation was conducted using G*Power software for linear multiple regression (fixed model, R2 deviation from zero). To detect a medium effect size (f2 = 0.15) with 80% power, alpha error probability of α = 0.05, and seven predictors, a minimum sample size of 103 was required.
2.4 Data collection
Participants in the cognition study were asked to complete all online assessments on the same day, on their home computer or other device. NHS data was collected by trained interviewers who surveyed the residents of 16,384 randomly chosen dwellings. Methods and survey composition is described in detail online (Australian Bureau of Statistics, 2018).
2.5 Measures
2.5.1 General cognitive assessment battery (GCAB) by Cognifit™
The Cognifit™ GCAB is a widely used and validated (Peretz et al., 2011; Yaneva et al., 2022), online cognitive assessment program that has demonstrated good internal consistency on each measure of cognitive function (α = 0.571 to α = 1) and test-retest reliability (0.696–0.998) (Cognifit, 2022). The online assessment lasts approximately 30 min. Raw data from 21 cognitive functions are age-adjusted by Cognifit and converted to five domains (reasoning, attention, memory, perception, and coordination) and a global score, scored from 0 to 800.
2.5.2 Alcohol consumption
Participants were asked to rate their frequency of alcohol consumption on a scale of “never or rarely”; “more than once a month but less than once a week”; “once or twice a week”; “most days”; or “every day.” Due to the small number of participants reporting daily consumption, “most days” and “every day” were collapsed. Participants were then asked how many standard drinks of alcohol they usually consumed on these occasions, and were given examples of what a standard drink of wine, beer, or spirits would be. Average amount consumed in one week was estimated from these responses, and the final dose variable was calculated based upon CDC guidelines (National Center for Health Statistics, 2018): Non-drinkers drank less than 12 drinks per year; light to moderate drinkers consumed at least one drink per month up to seven drinks per week for women and 14 for men; heavy drinkers consumed more than seven drinks per week for women and more than 14 for men. Alcohol data provided by the NHS calculated weekly consumption based upon the number of drinks consumed on the 3 days prior to the interview, together with the number of days alcohol was consumed that week. Number of days consuming 11 or more drinks in one sitting was used as a measure of binge drinking.
2.6 Demographic variables
A demographic survey incorporated variables such as highest level of education attained, income, main language spoken in the home, age, and sex. Data extracted from the NHS included age, sex, primary language spoken in the home, gross weekly personal income in deciles, frequency of alcohol consumption in the last 12 months, and estimated total weekly consumption of alcohol.
2.7 Statistical analysis
Survey data were analyzed using IBM SPSS version 29 and STATA Version 18. Normality was evaluated using the Shapiro-Wilk test. Descriptive data were analyzed using Means and standard deviations. For inferential analyses, significance was set at p ≤ 0.05. Chi square analyses determined relationships between categorical variables. General Linear Models (GLM) were conducted due to the high number of categorical predictor variables and the lack of normality observed in continuous variables. Each age-adjusted neurocognitive domain was included as an independent variable in separate GLM models. Smoking was not included as a potential covariate, as only two participants were current smokers and over 80% had never smoked. Model 1 was adjusted for gender only. Model 2 was adjusted for gender and education level. Model 3 was adjusted for gender, income, and primary language spoken in the home.
The National Health Survey data provides one person weight and 60 replicate weights. Jackknife weighting was conducted using these weighting variables in order to control for individual and sampling characteristics. Descriptive data and chi square analyses were then conducted and displayed using estimated population proportions.
3 Results
Score ranges for the neurocognitive domains are displayed in Figure 1. Mean scores are included in Table 1. Due to reported technical issues with manipulation of the mouse and touchscreen, and substantial variance in the final score, the neurocognitive domain of coordination was deemed unreliable and removed from the analysis.
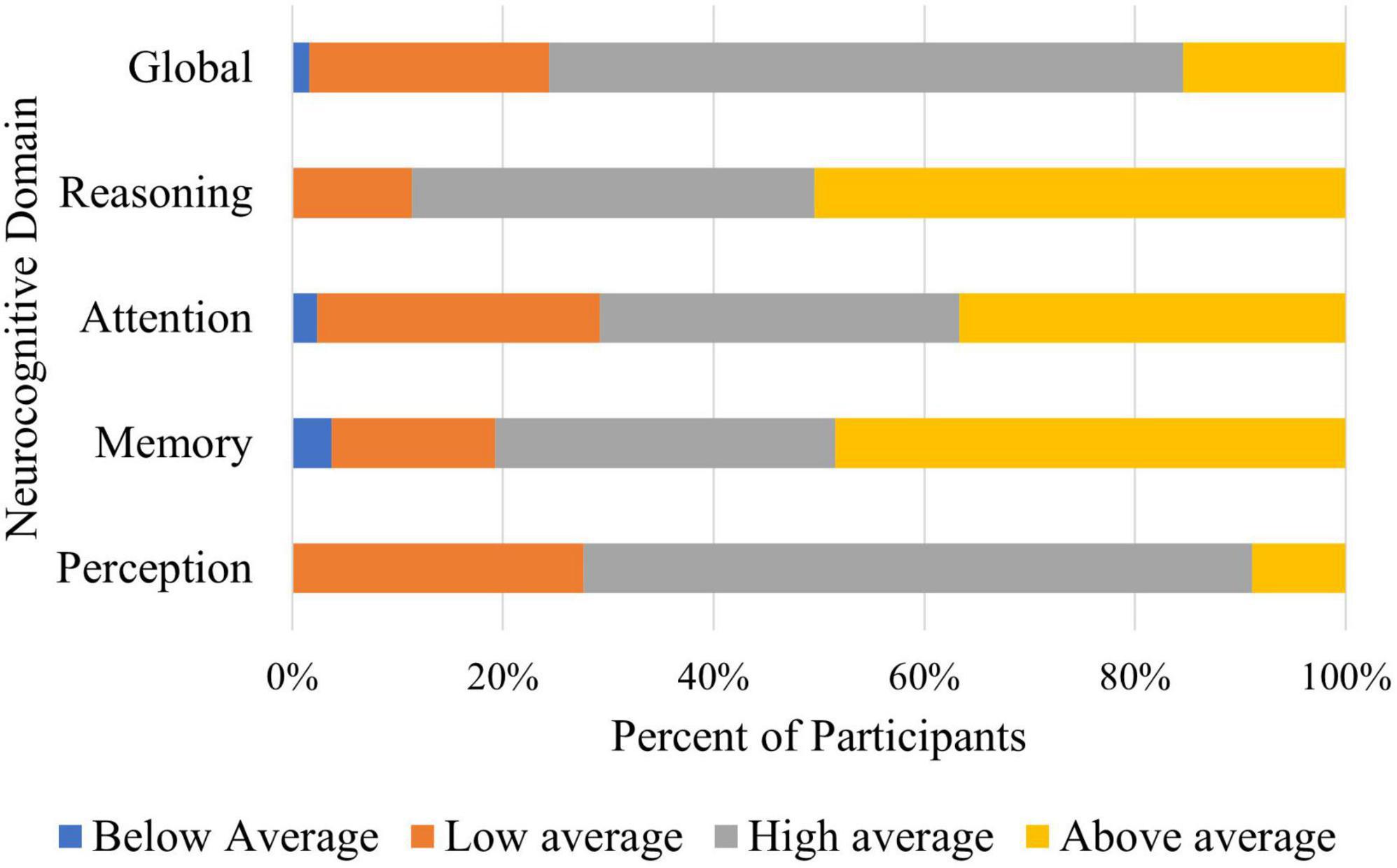
Figure 1. Neurocognitive domain scores. Percentage of participants within each category of cognitive functioning.
3.1 General linear models (GLM)
The impact of alcohol frequency and dose were investigated separately for their impact on neurocognitive domains. Model 1 controlled for gender, although results were similar when gender was not controlled for. Neither dose nor frequency of alcohol consumption were significantly related to Reasoning. Table 2 highlights the differences between different levels of dose and frequency on all other outcome variables when adjusted for gender; gender and education, and; gender, income and language. Figures 2, 3 are a visual representation of the Estimated Marginal Means. These graphs highlight the reduction in the difference between light and moderate drinkers and infrequent or non-drinkers, and show an increased impact of heavy consumption on cognition, when controlling for income and language. For the results of variables adjusted for income and language separately (see Supplementary Table 1). Reference categories were chosen to optimally highlight the relationships between variables.
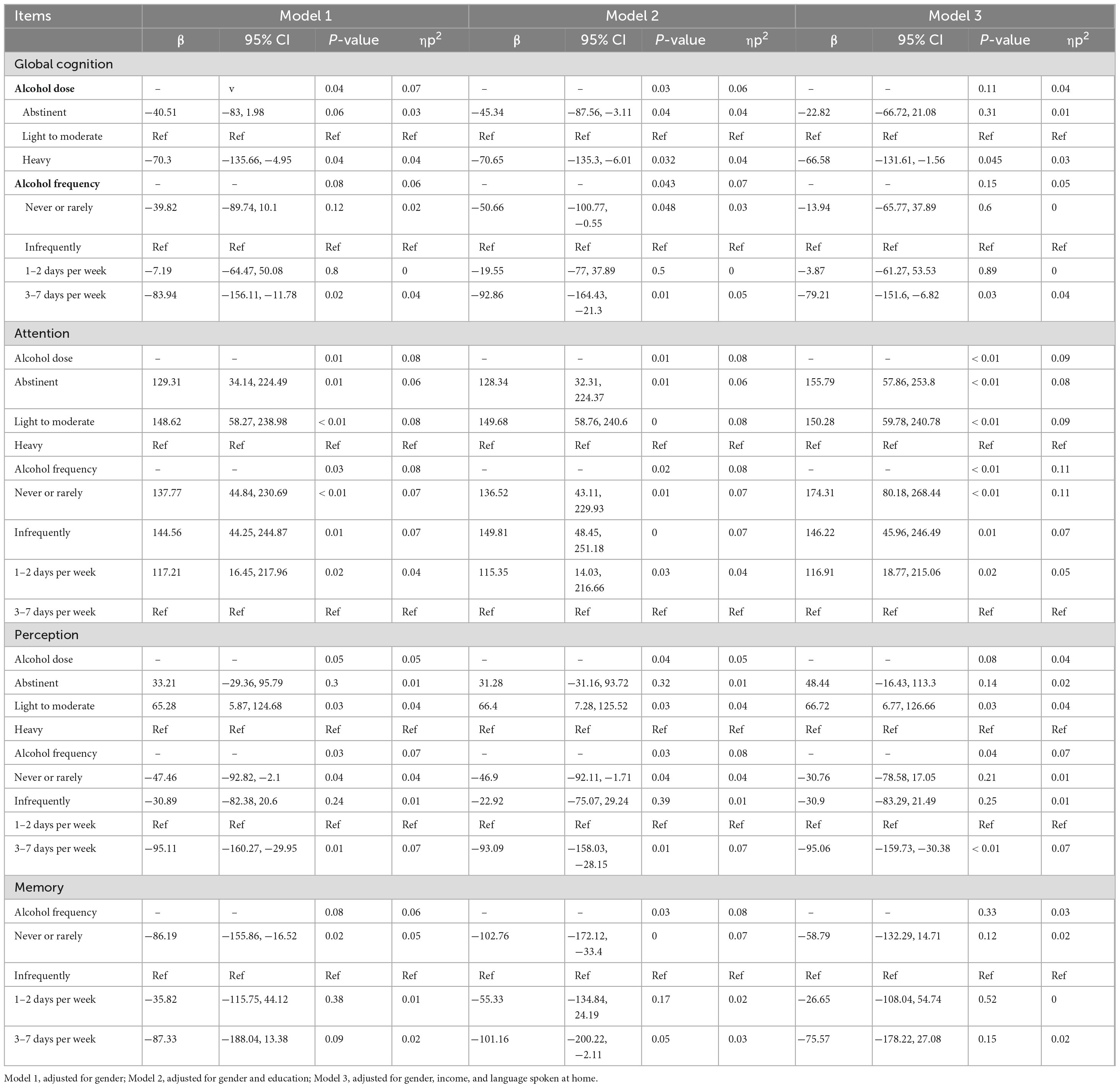
Table 2. General linear model (GLM) results for the relationship between alcohol consumption and neurocognitive domain scores adjusted for demographic covariates.
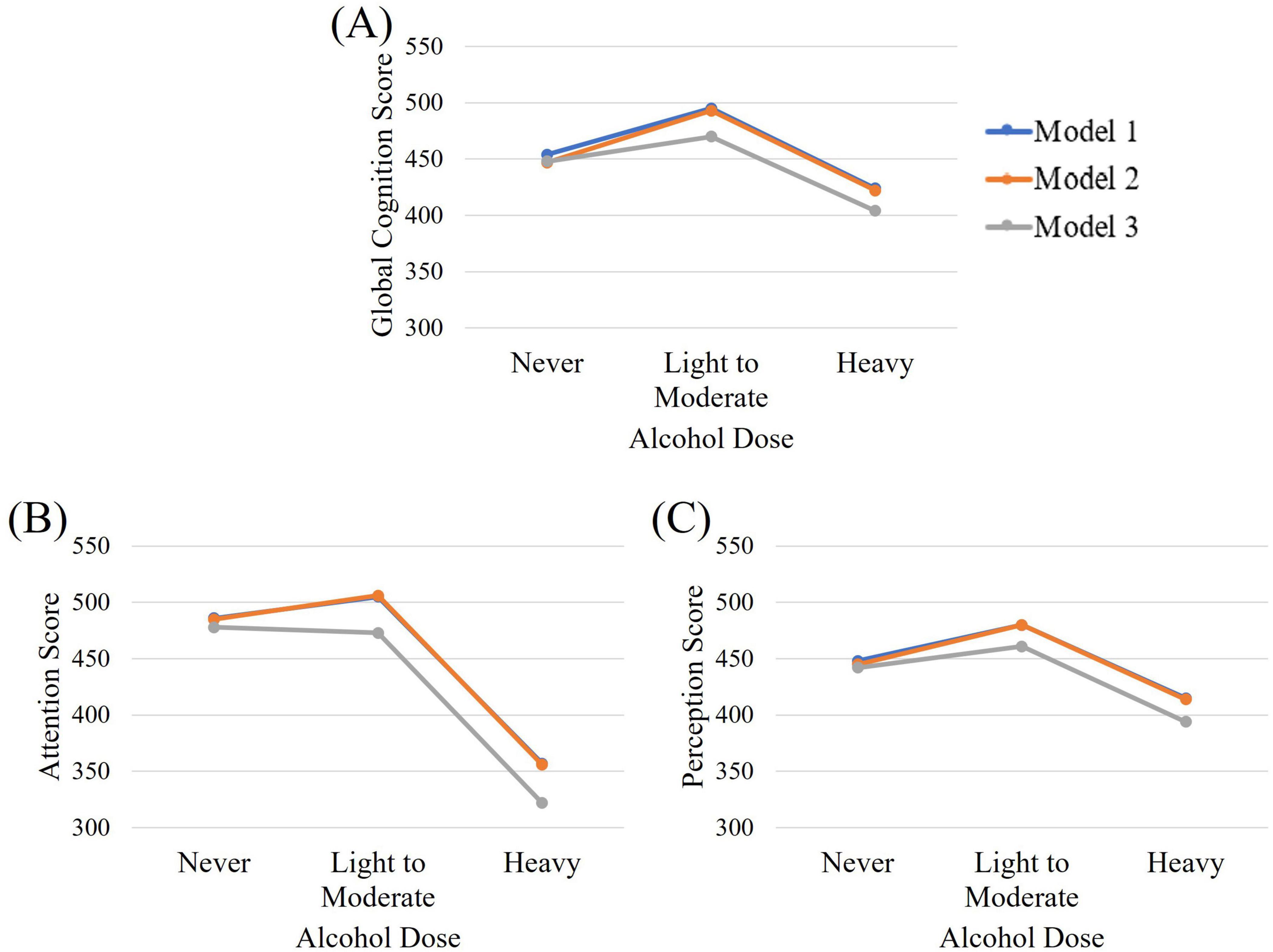
Figure 2. Estimated marginal means for (A) global cognition, (B) attention, and (C) perception across alcohol dose groups when controlling for gender (Model 1), gender and education (Model 2), and gender, income, and language (Model 3).
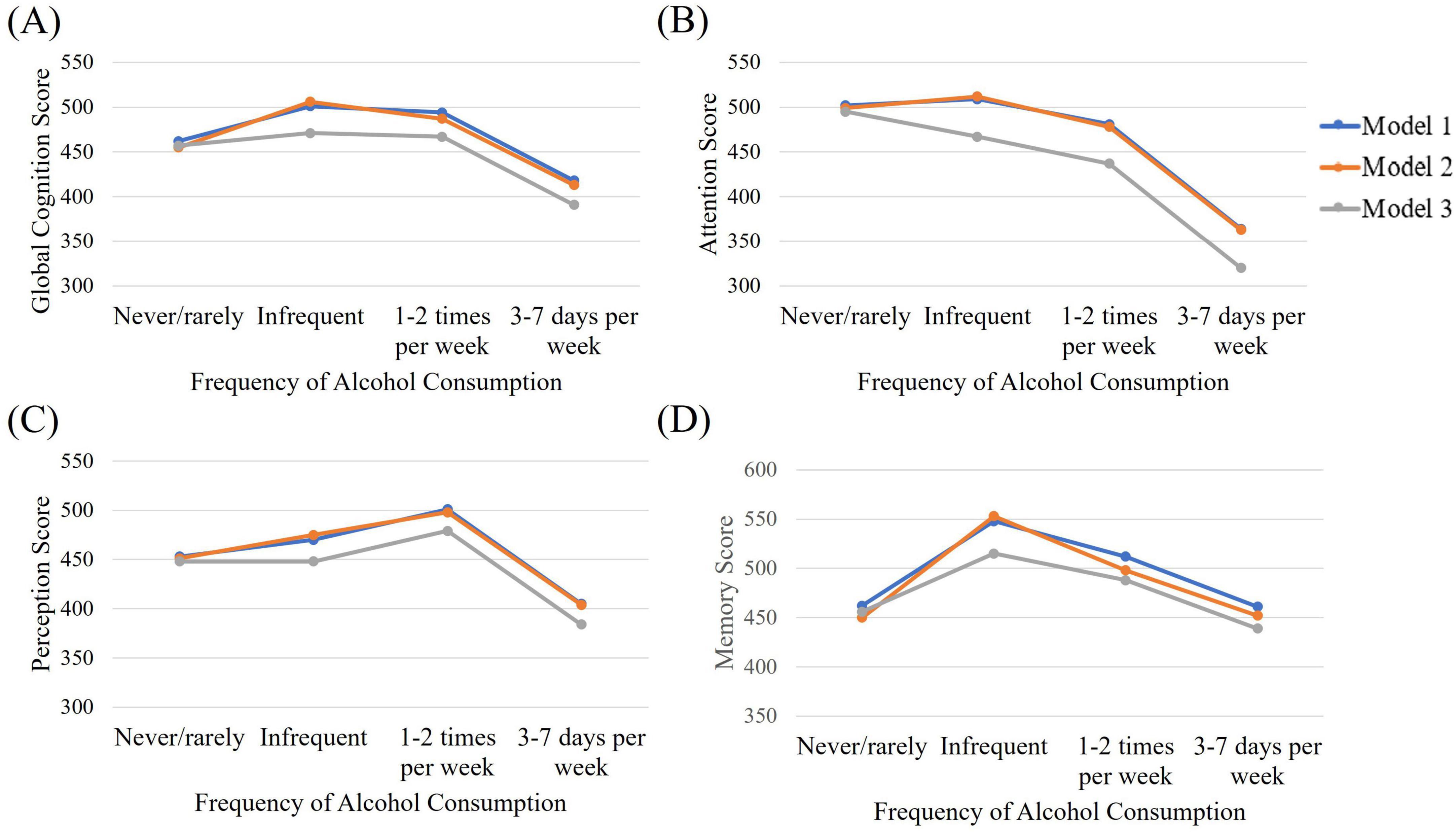
Figure 3. Estimated marginal means for (A) global cognition, (B) attention, (C) perception, and (D) memory across alcohol frequency of consumption groups when controlling for gender (Model 1), gender and education (Model 2), and gender, income, and language (Model 3).
3.2 Global cognition
A significant benefit of moderate drinking over heavy drinking is observed in Model 1. When this relationship is adjusted for education level, the superiority of light to moderate consumption over heavy consumption is increased and a benefit over no drinking appears. The benefit of moderate consumption over no drinking disappears when we adjust for income and language. Alcohol frequency of 3–7 days per week was significantly worse than drinking 1–2 times per week (β = −76.75, p = 0.04, 95% CI = −149.23, −4.27) or infrequent drinking (see Table 2) in Model 1. When education was included in the model, infrequent drinking was also superior to drinking never or rarely. When adjusting for income and language spoken in the home, infrequent and moderate drinking were only superior to heavy drinking, although the model itself was no longer significant.
3.3 Attention
Heavy alcohol consumption showed significantly lower scores for attention than did abstinent or moderate consumption, no matter which model was used. The same pattern was seen for frequency of alcohol consumption.
3.4 Perception
The relationship between alcohol dose and perception is not significant in Models 1 or 3. Only when adjusting for education and gender does a benefit of moderate consumption become evident. When investigating frequency of consumption, heavy or rare drinking shows worse performance than drinking 1–2 times per week. This pattern is maintained when correcting for education. Model 2 also shows a benefit of infrequent consumption over drinking 3–7 days per week (β = 70.17, p = 0.04, 95% CI = 5.2, 135.14). When adjusting for income and language, the benefit of weekly consumption over infrequent or rare consumption was no longer present.
3.5 Memory
No relationship was seen between alcohol dose and memory. The relationship between alcohol frequency and memory are not significant in models 1 and 3. When adjusting for gender and education, infrequent consumption had better scores than never or rarely drinking, or drinking 3–7 days per week.
3.6 Patterns of alcohol consumption
Figure 4 highlights the different patterns of alcohol consumption associated with educational attainment and income. This relationship was only significant for income and alcohol consumption frequency. However, for Chi square analyses to be conducted, income had to be collapsed to above and below $110,000 due to cell sizes smaller than five. Participants who spoke a language other than English in the home had similar educational attainment to those who spoke English. However, their income was significantly lower, and their alcohol consumption was significantly less in terms of dose and frequency (see Figure 5). Participants who spoke a language other than English at home also had significantly lower scores on all neurocognitive domains, despite similar educational attainment. For Chi square analyses described in Figure 5, alcohol dose and consumption were dichotomized into abstinent and other, and never or rarely drink and all other frequencies of consumption due to small cell sizes.
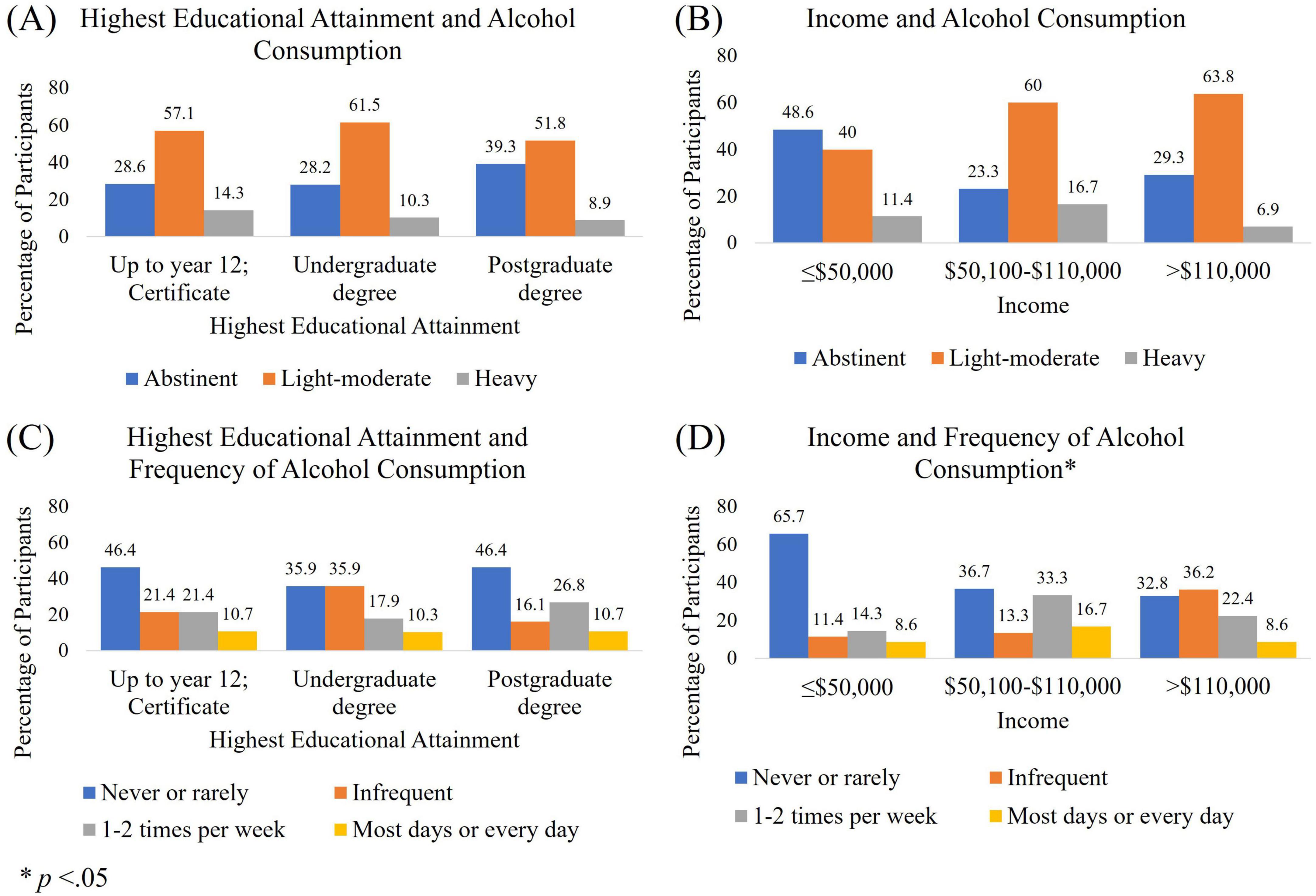
Figure 4. Patterns of alcohol consumption per week. Alcohol per week by (A) educational attainment and (B) income. Frequency of alcohol consumption dose per week by (C) educational attainment and (D) income.
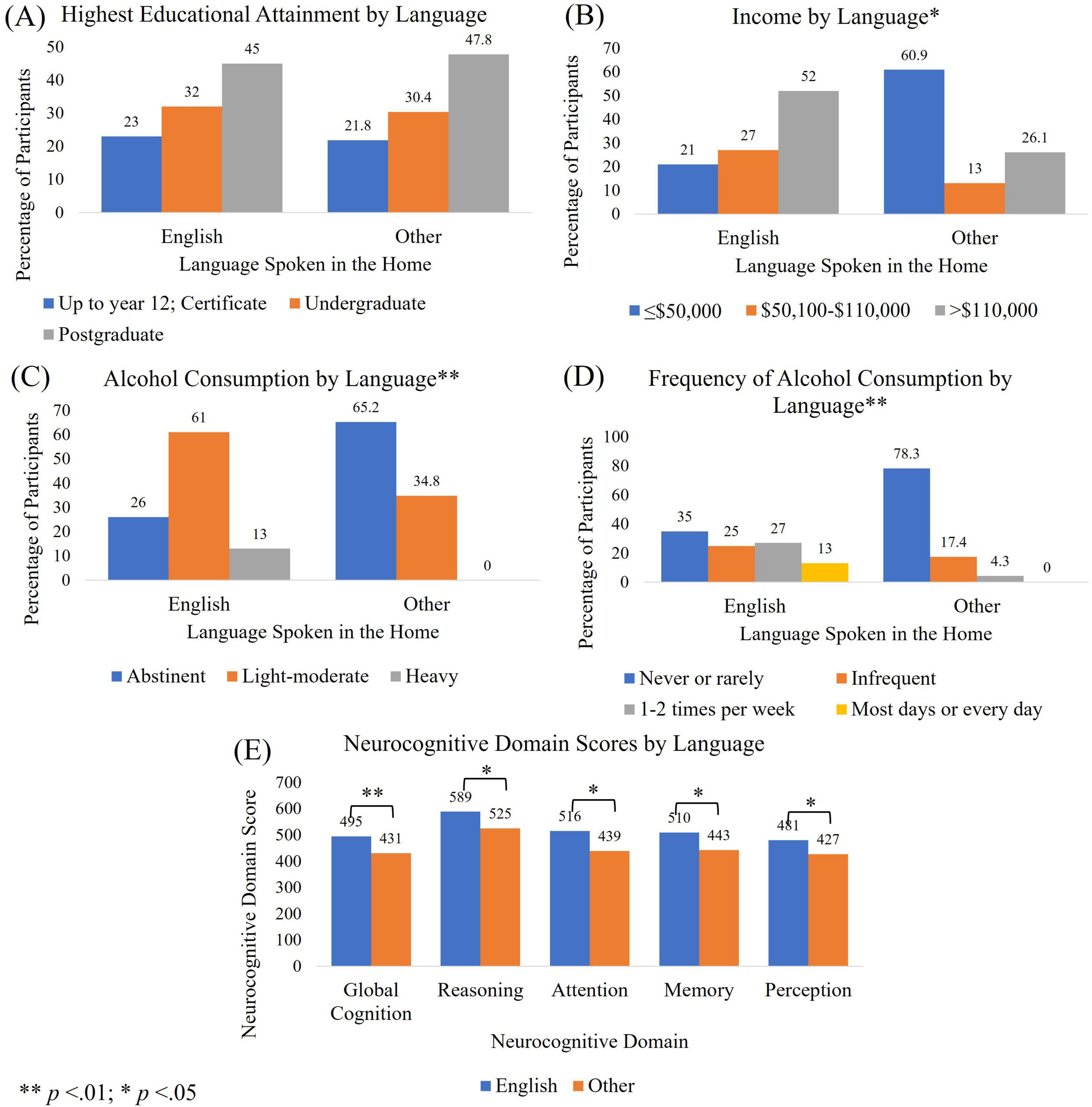
Figure 5. Participant characteristics by language. Differences between individuals speaking English or a language other than English in the home for (A) educational attainment; (B) income; (C) alcohol consumption dose per week; (D) frequency of alcohol consumption, and; (E) neurocognitive domain scores.
3.7 Australian national health survey—2018
Data from the National Health Survey 2018 was used to further investigate the relationships between drinking patterns and socioeconomic and demographic variables. When investigating alcohol consumption across income and education groups, we observed an even more pronounced difference in patterns of drinking (see Supplementary Figure 1). Higher income respondents were more likely to drink heavily and frequently than low income, but those with higher educational qualifications had similar drinking patterns to other non-school qualifications. Those with certificate training had the highest rates of daily or almost daily drinking. We also investigated the relationship between income and binge drinking, which has often been associated with poorer cognitive and physical health outcomes. A U-shaped curve was observed with middle-quintile income earners binge drinking more frequently than those at the lower or higher ends of the income spectrum. Binge drinking is also more associated with lower educational attainment. Language spoken in the home had a similar pattern to the data found in the cross-sectional survey data (see Supplementary Figure 2). Those who spoke a language other than English in the home were more likely to have attained a bachelor or postgraduate qualification, were more likely to be in the lowest two income quintiles, and consumed alcohol less frequently and in smaller doses.
4 Discussion
The present study aimed to evaluate the relationship between alcohol consumption and cognition, investigating the differential influence of potential confounders: education; income; and language. Heavy and frequent alcohol consumption was associated with poorer performance on attention, perception, and global cognition. When including education as a separate covariate, results were more likely to indicate a benefit of light to moderate alcohol consumption, or of moderately frequent consumption over abstinence or heavy drinking. A difference between drinking frequencies on memory scores was only significant when education was controlled for. Benefits of moderate consumption were not observed when adjusted for income and language. An assessment of drinking patterns associated with education and income clarify the potential reasons for these differences. Findings from both the cognition study and NHS data show that higher income is associated with higher rates of alcohol consumption. However, individuals with higher educational qualifications have similar drinking and abstinence rates to those with the lowest levels of educational attainment. This could be due to the differences in job opportunities and average income observed in different disciplines of postgraduate study. Findings could also be influenced by the number of highly paid positions in trades that do not require university qualifications.
The findings from the current study indicate little difference between abstinence and moderate drinking in terms of cognitive outcomes. However, several human neuroimaging studies have identified a linear relationship, with greater alcohol consumption associated with smaller volume across a range of brain regions (Karoly et al., 2024). This reduction in cortical thickness was observed even with low and moderate alcohol consumption. Findings from animal models have identified both protective and detrimental impacts of low-moderate consumption. Studies of neuronal cultures found that low ethanol concentrations prevented neurodegeneration due to β-amyloid and other neuroinflammatory proteins (Collins et al., 2010; Muñoz et al., 2015). This could potentially explain the reduction in dementia risk observed in some human studies. On the other hand, a study of Sprague-Dawley rats consuming moderate amounts of alcohol found a reduction in the number of cells produced in the dentate gyrus of the hippocampus, despite no significant reductions in behavioral tests of motor skills or learning (Anderson et al., 2012). Similarly, human cognitive testing may fail to identify early or minimal neurological impairment caused by alcohol consumption.
Individuals from lower SES experience disproportionate levels of alcohol-related harm (Katikireddi et al., 2017), greater mortality risk (Stringhini et al., 2017), and accelerated rates of cognitive decline (Steptoe and Zaninotto, 2020) compared to their more affluent counterparts. The fact that lower SES groups also have the highest rates of abstinence could bias study findings in favor of any amount of alcohol consumption over abstinence. Data from the NHS supports previous research suggesting that impairments observed in those from lower SES who consume less frequent, and less weekly doses of alcohol, may be due to infrequent episodes of “binge” drinking (Probst et al., 2020). Previous studies have also found long-term binge drinking associated with impaired memory, learning, and planning (Hendriks et al., 2020). It is unclear how infrequent, heavy episodes of drinking are captured in studies that reflect only daily or weekly drinking habits.
Language was also strongly associated with drinking behaviors, SES, and cognitive test performance. Despite holding higher educational qualifications, individuals who spoke a language other than English at home were more likely to score worse on all cognitive domains, creating additional bias in favor of alcohol consumption if not controlled for. Past research has also identified potential enhancements in cognitive performance (specifically processing speed) in those who are bi- or multi-lingual (Pacifico et al., 2023), suggesting that English proficiency may be a better predictor of cognitive test performance than primary language spoken. However, the relationship between language proficiency, alcohol consumption and SES must be investigated further. Conducting neurocognitive testing in participants’ first language may help to overcome this confounding and produce more reliable results.
Previous studies have identified sex-specific deficits in cognitive functions associated with alcohol consumption (Hone et al., 2020; Salvador et al., 2022). However, the current study found that gender had little influence on the relationship between alcohol consumption and cognitive outcomes. This may be due to the small number of male participants in the sample. It could also be due to other socio-economic or lifestyle factors that could not be adequately explored due to the limited sample size.
5 Strengths and limitations
The study utilized an adequately powered cross-sectional survey and a large population-based dataset to test the hypotheses. Findings from the survey were supported by the relationships identified in NHS data, indicating the generalizability of the results. Limitations of the study included the small number of questions regarding alcohol consumption and the lack of questions investigating past drinking behaviors. However, an investigation of past drinking behaviors was frequently omitted from studies that identified links between moderate alcohol consumption and enhanced cognitive function, making our paper comparable in methodology to the papers our findings challenged; enabling us to replicate and then test their findings. The sample contained a large number of highly educated participants, and few heavy or frequent drinkers. The findings also rely on participant recall. Recall bias is commonly seen in alcohol questionnaires, particularly in sporadic drinkers, with underestimation of consumption also common (Gmel and Daeppen, 2007; Gilligan et al., 2019). While the study was adequately powered for the included analyses, a larger sample may have allowed for a larger proportion of male participants and a more diverse sample in terms of socio-economic and cultural backgrounds that would have enabled additional investigation relating to the influences of these factors.
6 Conclusion
Our findings support previous assertions that income may provide a superior measure of SES than education. This is evidenced by the fact that education and income are associated with substantially different patterns of alcohol consumption. The relationships between income and education, and other lifestyle factors (such as exercise, nutrition, smoking, or occupation), should also be investigated to further explore the suitability of these variables as indicators of SES in health research. The study also identified detrimental impacts of heavy and/or frequent drinking on cognitive function, with little evidence for any benefit of moderate consumption over abstinence when income and language are controlled for. The study highlights a number of common study characteristics that may bias outcomes toward showing a beneficial impact of moderate drinking behaviors on cognitive function. Future research investigating lifestyle factors and cognitive function should include additional measures of SES to ensure they are appropriately controlling for confounding factors. Research that fails to account for the influence of accurate SES measures may unintentionally lead to an increase in damaging drinking behaviors and alcohol-related injury and disease. Understanding the true impact of alcohol on physical and cognitive health is crucial for developing guidelines and public health policy for safe alcohol consumption.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors upon reasonable request.
Ethics statement
The studies involving humans were approved by the Queensland University of Technology Human Research Ethics Committee (Ethics ID: 5872). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
KG: Conceptualization, Formal Analysis, Investigation, Methodology, Visualization, Writing – original draft. EK: Methodology, Supervision, Writing – review and editing. MW: Methodology, Supervision, Writing – review and editing. SB: Methodology, Supervision, Writing – review and editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. SB is partially funded by contributions from the Children’s Hospital Research Foundation, and EK is partially funded by the Australian Research Council’s Discovery Project funding scheme (project number DP180100545).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnagi.2025.1569069/full#supplementary-material
References
Akagi, Y., Kabayama, M., Gondo, Y., Masui, Y., Yasumoto, S., Klinpudtan, N., et al. (2022). Alcohol drinking patterns have a positive association with cognitive function among older people: A cross-sectional study. BMC Geriatr. 22:158. doi: 10.1186/s12877-022-02852-8
Almeida, O. P., Hankey, G. J., Yeap, B. B., Golledge, J., and Flicker, L. (2014). Alcohol consumption and cognitive impairment in older men: A mendelian randomization study. Neurology 82, 1038–1044. doi: 10.1212/wnl.0000000000000255
Anderson, M. L., Nokia, M. S., Govindaraju, K. P., and Shors, T. J. (2012). Moderate drinking? Alcohol consumption significantly decreases neurogenesis in the adult hippocampus. Neuroscience 224, 202–209. doi: 10.1016/j.neuroscience.2012.08.018
Australian Bureau of Statistics (2011). Perspectives on education and training: Social inclusion, 2009. Canberra, ACT: Australian Bureau of Statistics.
Australian Bureau of Statistics (2018). National health Survey: First results. Canberra, ACT: Australian Bureau of Statistics.
Australian Institute of Health and Welfare (2024). Alcohol, tobacco & other drugs in Australia. Bruce, ACT: Australian Institute of Health and Welfare.
Casswell, S., Pledger, M., and Hooper, R. (2003). Socioeconomic status and drinking patterns in young adults. Addiction 98, 601–610. doi: 10.1046/j.1360-0443.2003.00331.x
Centers for Disease Control and Prevention [CDC] (2012). Vital signs: Binge drinking prevalence, frequency, and intensity among adults - United States, 2010. MMWR Morb. Mortal Wkly Rep. 61, 14–19.
Collins, M. A., Neafsey, E. J., Wang, K., Achille, N. J., Mitchell, R. M., and Sivaswamy, S. (2010). Moderate ethanol preconditioning of rat brain cultures engenders neuroprotection against dementia-inducing neuroinflammatory proteins: Possible signaling mechanisms. Mol. Neurobiol. 41, 420–425. doi: 10.1007/s12035-010-8138-0
Cormier, D. C., Bulut, O., Mcgrew, K. S., and Kennedy, K. (2022). Linguistic influences on cognitive test performance: Examinee characteristics are more important than test characteristics. J. Intell. 10:8. doi: 10.3390/jintelligence10010008
Cuschieri, S. (2019). The strobe guidelines. Saudi J. Anaesth. 13, S31–S34. doi: 10.4103/sja.SJA_543_18
Darin-Mattsson, A., Fors, S., and Kåreholt, I. (2017). Different indicators of socioeconomic status and their relative importance as determinants of health in old age. Int. J. Equity Health 16:173. doi: 10.1186/s12939-017-0670-3
Daviet, R., Aydogan, G., Jagannathan, K., Spilka, N., Koellinger, P. D., Kranzler, H. R., et al. (2022). Associations between alcohol consumption and gray and white matter volumes in the UK Biobank. Nat. Commun. 13:1175. doi: 10.1038/s41467-022-28735-5
den Heijer, T., Vermeer, S. E., Van Dijk, E. J., Prins, N. D., Koudstaal, P. J., Van Duijn, C. M., et al. (2004). Alcohol intake in relation to brain magnetic resonance imaging findings in older persons without dementia. Am. J. Clin. Nutr. 80, 992–997. doi: 10.1093/ajcn/80.4.992
Galobardes, B., Shaw, M., Lawlor, D. A., Lynch, J. W., and Davey Smith, G. (2006). Indicators of socioeconomic position (part 1). JECH 60:7. doi: 10.1136/jech.2004.023531
Gilligan, C., Anderson, K. G., Ladd, B. O., Yong, Y. M., and David, M. (2019). Inaccuracies in survey reporting of alcohol consumption. BMC Public Health 19:1639. doi: 10.1186/s12889-019-7987-3
Gmel, G., and Daeppen, J. B. (2007). Recall bias for seven-day recall measurement of alcohol consumption among emergency department patients: Implications for case-crossover designs. J. Stud. Alcohol Drugs 68, 303–310. doi: 10.15288/jsad.2007.68.303
Gómez, G., Kovalskys, I., Leme, A. C. B., Quesada, D., Rigotti, A., Cortés Sanabria, L. Y., et al. (2021). Socioeconomic status impact on diet quality and body mass index in eight latin american countries: ELANS study results. Nutrients 13:2404. doi: 10.3390/nu13072404
Guerri, C., and Pascual, M. (2019). “Chapter nine - role of neuroinflammation in ethanol neurotoxicity,” in Advances in neurotoxicology, eds M. Aschner and L. G. Costa (Cambridge, MA: Academic Press), 259–294.
Hendriks, H., Van De Rest, O., Snippe, A., Kieboom, J., and Hogenelst, K. (2020). Alcohol consumption, drinking patterns, and cognitive performance in young adults: A cross-sectional and longitudinal analysis. Nutrients 12:200. doi: 10.3390/nu12010200
Hone, L. S. E., Scofield, J. E., Bartholow, B. D., and Geary, D. C. (2020). Frequency of recent binge drinking is associated with sex-specific cognitive deficits: Evidence for condition-dependent trait expression in humans. Evol. Psychol. 18:1474704920954445. doi: 10.1177/1474704920954445
Immonen, S., Launes, J., Järvinen, I., Virta, M., Vanninen, R., Schiavone, N., et al. (2020). Moderate alcohol use is associated with decreased brain volume in early middle age in both sexes. Sci. Rep. 10:13998. doi: 10.1038/s41598-020-70910-5
Jeon, K. H., Han, K., Jeong, S.-M., Park, J., Yoo, J. E., Yoo, J., et al. (2023). Changes in alcohol consumption and risk of dementia in a nationwide cohort in South Korea. JAMA Netw. Open 6:e2254771. doi: 10.1001/jamanetworkopen.2022.54771
Karoly, H. C., Kirk-Provencher, K. T., Schacht, J. P., and Gowin, J. L. (2024). Alcohol and brain structure across the lifespan: A systematic review of large-scale neuroimaging studies. Addict. Biol. 29:e13439. doi: 10.1111/adb.13439
Katikireddi, S. V., Whitley, E., Lewsey, J., Gray, L., and Leyland, A. H. (2017). Socioeconomic status as an effect modifier of alcohol consumption and harm: Analysis of linked cohort data. Lancet Public Health 2:e267. doi: 10.1016/S2468-2667(17)30078-6
Mortensen, E. L., Jensen, H. H., Sanders, S. A., and Reinisch, J. M. (2001). Better psychological functioning and higher social status may largely explain the apparent health benefits of wine: A study of wine and beer drinking in young Danish adults. Arch. Int. Med. 161, 1844–1848. doi: 10.1001/archinte.161.15.1844
Muñoz, G., Urrutia, J. C., Burgos, C. F., Silva, V., Aguilar, F., Sama, M., et al. (2015). Low concentrations of ethanol protect against synaptotoxicity induced by Aβ in hippocampal neurons. Neurobiol. Aging 36, 845–856. doi: 10.1016/j.neurobiolaging.2014.10.017
Murakami, K., and Hashimoto, H. (2019). Associations of education and income with heavy drinking and problem drinking among men: Evidence from a population-based study in Japan. BMC Public Health 19:420. doi: 10.1186/s12889-019-6790-5
Naimi, T. S., Stockwell, T., Zhao, J., Xuan, Z., Dangardt, F., Saitz, R., et al. (2017). Selection biases in observational studies affect associations between ‘moderate’ alcohol consumption and mortality. Addiction 112, 207–214. doi: 10.1111/add.13451
National Center for Health Statistics (2018). National health interview survey: Glossary - alcohol. Hyattsville, MD: National Center for Health Statistics.
Neafsey, E. J., and Collins, M. A. (2011). Moderate alcohol consumption and cognitive risk. Neuropsychiatr. Dis. Treat 7, 465–484. doi: 10.2147/ndt.S23159
Ng Fat, L., and Shelton, N. (2012). Associations between self-reported illness and non-drinking in young adults. Addiction 107, 1612–1620. doi: 10.1111/j.1360-0443.2012.03878.x
Norström, T., and Landberg, J. (2023). The association between population drinking and ischemic heart disease mortality in educational groups. Alcohol Alcohol 58, 385–392. doi: 10.1093/alcalc/agad033
Pacifico, D., Sabatini, S., Fiordelli, M., Annoni, A. M., Frei, A., Puhan, M., et al. (2023). Associations of multilingualism and language proficiency with cognitive functioning: Epidemiological evidence from the SwissDEM study in community dwelling older adults and long-term care residents. BMC Geriatr. 23:629. doi: 10.1186/s12877-023-04311-4
Peretz, C., Korczyn, A. D., Shatil, E., Aharonson, V., Birnboim, S., and Giladi, N. (2011). Computer-based, personalized cognitive training versus classical computer games: A randomized double-blind prospective trial of cognitive stimulation. Neuroepidemiology 36, 91–99. doi: 10.1159/000323950
Platt, A., Sloan, F. A., and Costanzo, P. (2010). Alcohol-consumption trajectories and associated characteristics among adults older than age 50. J. Stud. Alcohol Drugs 71, 169–179. doi: 10.15288/jsad.2010.71.169
Probst, C., Kilian, C., Sanchez, S., Lange, S., and Rehm, J. (2020). The role of alcohol use and drinking patterns in socioeconomic inequalities in mortality: A systematic review. Lancet Public Health 5, e324–e332. doi: 10.1016/S2468-2667(20)30052-9
Reas, E. T., Laughlin, G. A., Kritz-Silverstein, D., Barrett-Connor, E., and Mcevoy, L. K. (2016). Moderate, regular alcohol consumption is associated with higher cognitive function in older community-dwelling adults. J. Prev. Alzheimers Dis. 3, 105–113. doi: 10.14283/jpad.2016.89
Ronksley, P. E., Brien, S. E., Turner, B. J., Mukamal, K. J., and Ghali, W. A. (2011). Association of alcohol consumption with selected cardiovascular disease outcomes: A systematic review and meta-analysis. BMJ 342:d671. doi: 10.1136/bmj.d671
Salvador, L., Giatti, L., Viana, M. C., Suemoto, C. K., Duncan, B. B., Molina, M. D. C. B., et al. (2022). Sex differences in the association between alcohol intake and cognitive decline over 4 years in a middle-aged cohort: The Brazilian longitudinal study of adult health. Eur. J. Neurol. 29, 1903–1912. doi: 10.1111/ene.15315
Squeglia, L. M., Jacobus, J., and Tapert, S. F. (2014). The effect of alcohol use on human adolescent brain structures and systems. Handb. Clin. Neurol. 125, 501–510. doi: 10.1016/b978-0-444-62619-6.00028-8
Steptoe, A., and Zaninotto, P. (2020). Lower socioeconomic status and the acceleration of aging: An outcome-wide analysis. Proc. Natl. Acad. Sci. U. S. A. 117, 14911–14917. doi: 10.1073/pnas.1915741117
Stockwell, T., Zhao, J., Clay, J., Levesque, C., Sanger, N., Sherk, A., et al. (2024). Why do only some cohort studies find health benefits from low-volume alcohol use? a systematic review and meta-analysis of study characteristics that may bias mortality risk estimates. J. Stud. Alcohol Drugs 85, 441–452. doi: 10.15288/jsad.23-00283
Stringhini, S., Carmeli, C., Jokela, M., Avendaño, M., Muennig, P., Guida, F., et al. (2017). Socioeconomic status and the 25 × 25 risk factors as determinants of premature mortality: A multicohort study and meta-analysis of 1⋅7 million men and women. Lancet 389, 1229–1237. doi: 10.1016/s0140-6736(16)32380-7
Topiwala, A., Allan, C. L., Valkanova, V., Zsoldos, E., Filippini, N., Sexton, C., et al. (2017). Moderate alcohol consumption as risk factor for adverse brain outcomes and cognitive decline: Longitudinal cohort study. BMJ 357:j2353. doi: 10.1136/bmj.j2353
Towers, A., Philipp, M., Dulin, P., and Allen, J. (2016). The “Health Benefits” of moderate drinking in older adults may be better explained by socioeconomic status. J. Gerontol. B Psychol. Sci. Soc. Sci. 73, 649–654. doi: 10.1093/geronb/gbw152
Wang, S., Sun, Q. C., Martin, C., Cai, W., Liu, Y., Duckham, M., et al. (2023). Tracking the settlement patterns of Culturally and Linguistically Diverse (CALD) populations in Australia: A census-based study from 2001 to 2021. Cities 141:104482. doi: 10.1016/j.cities.2023.104482
Xu, W., Wang, H., Wan, Y., Tan, C., Li, J., Tan, L., et al. (2017). Alcohol consumption and dementia risk: A dose–response meta-analysis of prospective studies. Eur. J. Epidemiol. 32, 31–42. doi: 10.1007/s10654-017-0225-3
Yaneva, A., Massaldjieva, R., and Mateva, N. (2022). Initial adaptation of the general cognitive assessment battery by cognifit™ for bulgarian older adults. Exp. Aging Res. 48, 336–350. doi: 10.1080/0361073x.2021.1981096
Zhang, R., Shen, L., Miles, T., Shen, Y., Cordero, J., Qi, Y., et al. (2020). Association of low to moderate alcohol drinking with cognitive functions from middle to older age among US adults. JAMA Netw. Open 3:e207922. doi: 10.1001/jamanetworkopen.2020.7922
Keywords: cognition, alcohol, socioeconomic status, income, language
Citation: Gillespie KM, Kemps E, White MJ and Bartlett SE (2025) Moderate alcohol consumption does not protect cognitive function when controlling for income and cultural factors. Front. Aging Neurosci. 17:1569069. doi: 10.3389/fnagi.2025.1569069
Received: 31 January 2025; Accepted: 25 April 2025;
Published: 26 May 2025.
Edited by:
Jun Wang, Texas A&M University, United StatesCopyright © 2025 Gillespie, Kemps, White and Bartlett. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kerri M. Gillespie, a2VycmkuZ2lsbGVzcGllQHF1dC5lZHUuYXU=