 Catarina Geraldes1,2,3,4,5*
Catarina Geraldes1,2,3,4,5* Adriana Roque1,6
Adriana Roque1,6 Ana Bela Sarmento-Ribeiro1,2,3,4,5
Ana Bela Sarmento-Ribeiro1,2,3,4,5 Manuel Neves7Alina Ionita8Rita Gerivaz9
Manuel Neves7Alina Ionita8Rita Gerivaz9 Ana Tomé9Sofia Afonso10,11
Ana Tomé9Sofia Afonso10,11 Maria Pedro Silveira12Patrícia Sousa12
Maria Pedro Silveira12Patrícia Sousa12 Rui Bergantim14,15,16Cristina João7,17
Rui Bergantim14,15,16Cristina João7,17- 1Serviço de Hematologia Clínica, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal
- 2Faculty of Medicine, University of Coimbra, Coimbra, Portugal
- 3Coimbra Institute for Clinical and Biomedical Research, Faculty of Medicine, University of Coimbra, Coimbra, Portugal
- 4Center for Innovative Biomedicine and Biotechnology (CIBB), University of Coimbra, Coimbra, Portugal
- 5Clinical Academic Center of Coimbra (CACC), Coimbra, Portugal
- 6Institute of Physiology, Faculty of Medicine, University of Coimbra, Coimbra, Portugal
- 7Hemato-Oncology Unit, Champalimaud Foundation, Lisboa, Portugal
- 8Hematology Department, Portuguese Institute of Oncology Francisco Gentil, Lisboa, Portugal
- 9Serviço de Hemato-oncologia, Hospital Garcia de Orta, Lisboa, Portugal
- 10Serviço de Hematologia Clínica, Centro Hospitalar Universitário Cova da Beira, Covilhã, Portugal
- 11Faculdade de Ciências da Saúde, Universidade da Beira Interior, Covilhã, Portugal
- 12Serviço de Imuno-Hemoterapia, Hospital Prof. Doutor Fernando Fonseca, EPE, Amadora, Portugal
- 13Haematology Department, Portuguese Oncology Institute of Coimbra, Coimbra, Portugal
- 14Serviço de Hematologia Clínica, Centro Hospitalar Universitário de São João (CHUSJ), Porto, Portugal
- 15Instituto de Investigação e Inovaçáo em Saúde, Universidade do Porto, Porto, Portugal
- 16Institute of Pathology and Molecular Immunology, Abel Salazar Institute of Biomedical Sciences, University of Porto, Porto, Portugal
- 17NOVA Medical School, Universidade Nova de Lisboa, Lisboa, Portugal
Multiple myeloma (MM) is a very heterogeneous disease with multiple symptoms and clinical manifestations. MM affects mainly elderly patients and is difficult to manage in the presence of comorbidities, polypharmacy, frailty and adverse events of disease-targeted drugs. The rapid changes in MM treatment resulting from constant innovations in this area, together with the introduction of numerous new drugs with distinct mechanisms of action and toxicity profiles, have led to an increased complexity in the therapeutic decision-making and patient management processes. The prolonged exposure to novel agents, sometimes in combination with conventional therapies, makes this management even more challenging. A careful balance between treatment efficacy and its tolerability should be considered for every patient. During treatment, a close monitoring of comorbidities, disease-related manifestations and treatment side effects is recommended, as well as a proactive approach, with reinforcement of information and patient awareness for the early recognition of adverse events, allowing prompt therapeutic adjustments. In this review, we discuss various issues that must be considered in the treatment of MM patients, while giving practical guidance for monitoring, prevention and management of myeloma-related manifestations and treatment-related toxicities.
Introduction
Multiple myeloma (MM) represents the second most frequent hematologic malignancy, with more than 176,000 new cases diagnosed worldwide and more than 50,000 in Europe in 2020 (1). It accounts for 1% of all cancers and approximately 10% of all hematologic malignancies.
In the last 2 decades, remarkable advances in the treatment of patients with MM have resulted in a significant improvement in prognosis, with increased overall survival (2), and have converted MM into a chronic disease in a considerable number of cases (3). New therapeutic agents with more selective targeted mechanisms of action and inducing less acute toxicity, when compared to classical cytotoxic agents, introduced the concept of continuous therapy and maintenance therapy. The current MM treatment paradigm includes combinations of antineoplastic drugs until disease progression, with patients continuously maintaining the same drug regimen for several years (4).
MM is a neoplasm that mostly affects elderly patients, with a median age at the time of diagnosis of 65 years (5). Consequently, many of these patients are frail,have age-related comorbidities at diagnosis or during the course of the disease, and are likely to experience polypharmacy (6). The most common comorbidities at diagnosis are cardiovascular disease (63-69%) (7), diabetes mellitus or other disorders of glucose metabolism (11-22% of patients with MM) (8), hypertensive, diabetic or atherosclerotic nephropathy(up to 15% of cases at presentation) (9, 10), neurological and cognitive changes, osteoarticular disease, poor bone marrow reserve and immunosenescence (5).
The patient population treated in real-life clinical practice differs from the patient population included in clinical trials, who are usually younger, with better performance status (PS) and without cardiovascular, renal or hepatic dysfunction (9). The available data on the efficacy and safety of new therapeutic agents are relatively scarce in subgroups of patients with specific comorbidities, and often fail to adequately capture long-term toxicities. The use of non-uniform criteria and definitions for frailty status and organ damage/dysfunction has implications for the quality and applicability of the scientific evidence, making it difficult to create clear recommendations that include the widest possible range of patient subgroups.
This increasing complexity poses challenges for the medical community treating these patients. The appropriate management of toxicities and comorbidities is essential to avoid treatment discontinuation or dose reduction, and the consequent compromise of treatment efficacy, as well as to optimize patients’ quality of life.
Below, we describe the adverse events, complications and comorbidities that are most frequently observed in patients with MM, during treatment with the new therapeutic combinations, as well as some recommendations for their approach.
Infections
Patients with MM are more susceptible to infections due to disease-related factors (suppression of cellular and humoral immunity, including hypogammaglobulinemia lymphocyte dysfunction, low CD4+ cell count and impaired function of natural killer cells), patient-related factors (old age, poor performance status, and comorbidities, including diabetes mellitus and renal dysfunction) and treatment-related factors (neutropenia) (11, 12) especially within the first year of diagnosis (11). Of note, patients with a high tumor burden (International Staging System II-III), marked elevation of serum lactate dehydrogenase, poor PS, low hemoglobin and renal dysfunction are at higher risk of early and severe infections (12). The incidence of severe infection in MM patients appears to be higher during the first months after diagnosis, so the use of risk scores may help to identify patients at higher risk of infection and who may therefore benefit from individualized prophylactic treatment. A recently published score identifies serum albumin ≤30 g/L, Eastern Cooperative Oncology Group performance status (ECOG PS)>1, male gender and non-IgA type MM, as variables associated with increased risk of severe infection in the first 4 months (13, 14). In this context, infections should be approached based on the individual risk of infection (Table 1).
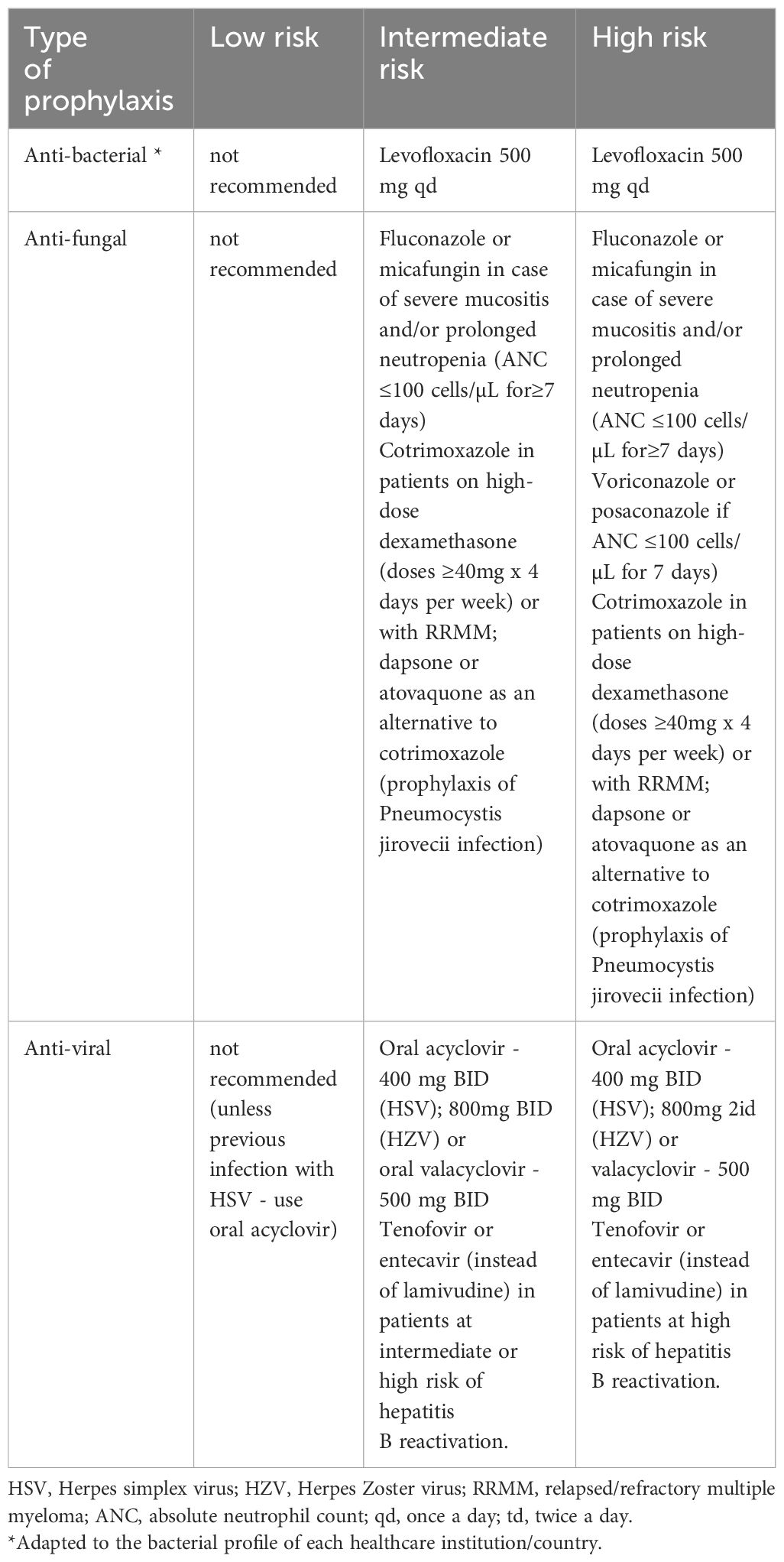
Table 1 Risk-adapted prophylaxis in patients with multiple myeloma.
The most frequent viral infections are respiratory, most often by herpes viruses (CMV, varicella zoster or herpes simplex) in patients treated with bortezomib or with monoclonal antibodies and without antiviral prophylaxis. Invasive fungal infections have an incidence of about 2.5% and the median time from diagnosis to presentation of invasive fungal infection is 35 months (15, 16). Bacterial infections are most often caused by coagulase-negative staphylococci (48%), Enterococcus faecalis (11%), and Escherichia coli (16%), among others, although bacterial strains are determined by the local epidemiology. In patients with IgG < 400 mg/dL and recurrent infections with encapsulated bacteria, or in those with proven specific antibody failure (PSAF), polyclonal immunoglobulin replacement (200-400 mg/kg IV every 3-4 weeks) may be considered (15). The International Myeloma Working Group (IMWG) recommends antibacterial, antifungal and antiviral prophylaxis (Table 1). These recommendations have a low level of evidence and are not based on randomized studies conducted specifically in MM patients. Prophylaxis with cotrimoxazole, as already proven in other studies, is a practice without consensus and based on the clinical practice of each hospital (17). Cotrimixazole was associated with a reduction in Pneumocystis jirovecii pneumonia-related mortality (14, 15). Levofloxacin prophylaxis, based on the phase 3 TEAMM randomized trial (18), is used in clinical practice irregularly, mainly due to the emergence of quinolone resistance. A systematic review of dysglycemic effect of fluoroquinolones showed that fluoroquinolones must be used with great caution among diabetic patients who have comorbidities and are receiving antidiabetics and/or steroids and that levofloxacin was associated with a very high level of hypoglycemic diabetic patients (19). In what concerns antifungal prophylaxis, previous studies showed a drug interaction between lenalidomide and itraconazole, which is a potent inhibitor of CYP3A4 and P-glycoprotein (P-gp) activity. P-gp is involved in the lenalidomide pharmacokinetics and drug-interactions. Because lenalidomide is scarcely metabolized by cytochrome P450s, the activity of drug-transporters such as P-gp may be a key determinant of lenalidomide pharmacokinetics. As previously reported, the AUC0–24 and Cmax for lenalidomide were markedly increased by itraconazole, though its elimination t1/2 was unaffected, suggesting that the drug interaction between lenalidomide and itraconazole occurs via P-gp during absorption from the small intestine. Lenalidomide exposure could contribute to its toxicity and careful monitoring of lenalidomide as well as creatinine clearance is recommended to avoid the risk of toxicity (20). Pomalidomide is partly metabolized by CYP1A2 and CYP3A4/5 and it is also a substrate for P-gp. Concomitant administration of pomalidomide with ketoconazole, a potent inhibitor of CYP3A4/5 and P-gp, demonstrated no clinically relevant effect on pomalidomide exposure (21).
Recommendations for vaccinations in MM patients have been published by the European Myeloma Network, the CDC (Center of Disease Control), IDSA (Infectious Disease Society of America) and NCCN (National Comprehensive Cancer Network) (Table 2) (15, 22).
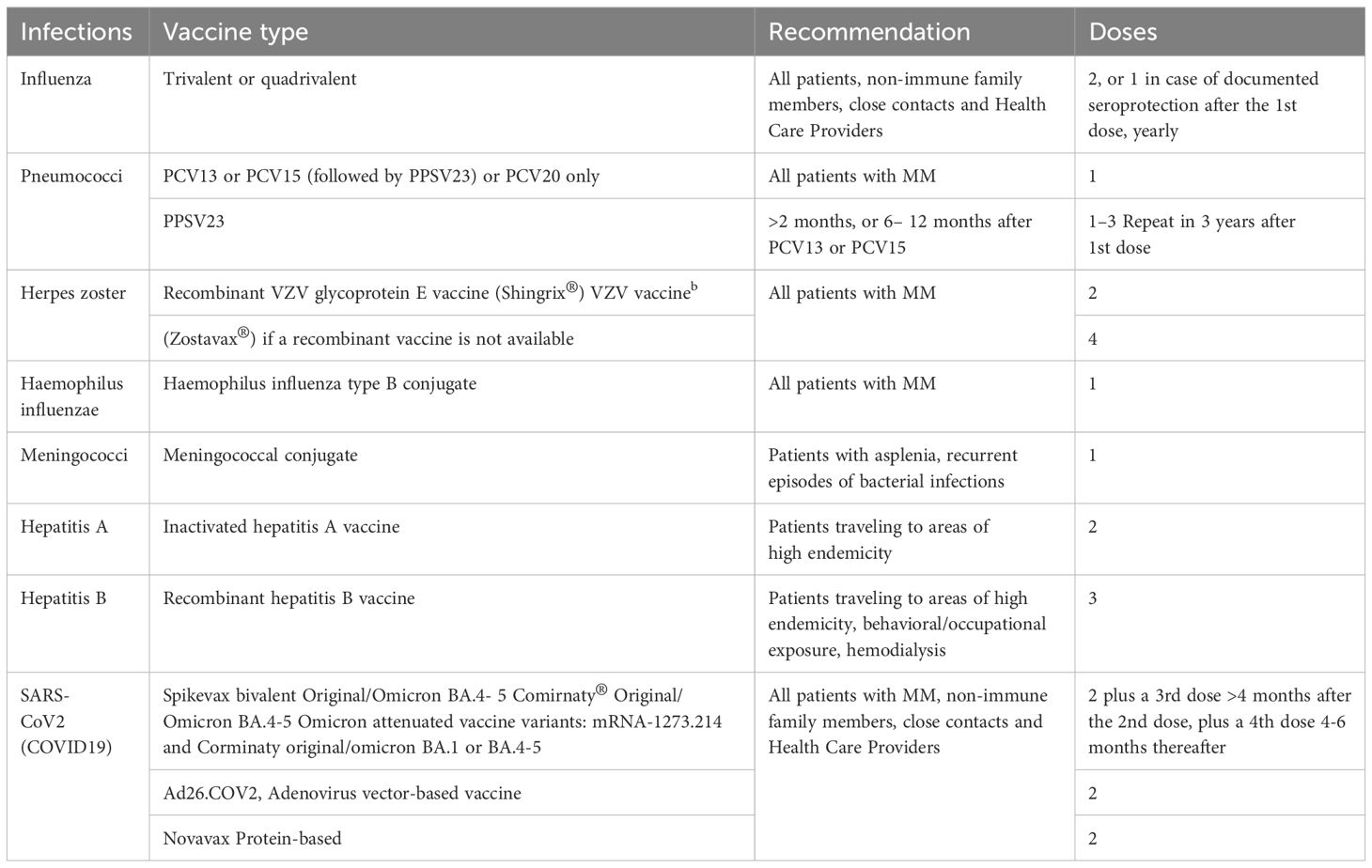
Table 2 Recommendations for vaccination in multiple myeloma patients .
Kidney injury
Kidney injury is one of the most frequent complications in MM patients, and establishing the cause is essential to the treatment approach (10). The initial evaluation should include the determination of serum urea, creatinine, electrolytes and serum free light chain (sFLC) levels, as well as urine protein electrophoresis and 24-hour urine free light chain levels. Additionally, monitoring and characterization of proteinuria is mandatory in the assessment of response to therapy and progression of MM (22, 23).
Selective proteinuria of light chains is suggestive of light chain nephropathy (LCN) and is considered not to require histological characterization, whereas non-selective proteinuria or albuminuria point to alternative causes of kidney damage (23). Renal biopsy (RB) is recommended in situations without a clear etiology, such as non-selective proteinuria, albuminuria without a prior cause or disproportionate to it, or in cases with unexplained kidney injury and sFLC < 500 mg/L. In suspected cases of AL amyloidosis, abdominal fat fine needle aspiration and bone marrow biopsy for amyloid screening should be considered, thus avoiding RB (23). While the risk associated with RB, in patients with MM overlaps that of the general population, there is an increased risk of hemorrhagic complications in patients with suspected AL amyloidosis. In these cases, minimally invasive techniques should be preferred (24).
LCN constitutes a hematological emergency, and its approach should include renal supportive measures, high-dose corticosteroid therapy, and therapy directed at the neoplastic clone (24).
Supportive measures encompass the removal of the precipitating factors of nephropathy, with vigorous hydration (2 L/m2/day) with particular attention to the fluid balance, especially in patients with reduced urine output and cardiac disease. Diuretics should be avoided, except in situations of fluid overload. The use of bicarbonate to achieve a urinary pH of 7 is controversial and should be avoided in hypercalcemia, due to the risk of calcium phosphate precipitation in the renal tubules (24).
Other key measures include discontinuation of angiotensin-converting enzyme inhibitors and of non-steroidal anti-inflammatory drugs, and the treatment of concomitant infections with non-nephrotoxic antibiotics (23, 24).
Hypercalcemia should be corrected urgently, with hydration and bisphosphonates, with dose-adjustment to creatinine clearance (CrCl). High-dose dexamethasone - with anti-inflammatory, catabolic and anti-neoplastic effects - should be started early, at a dose of 40 mg/day (20 mg in patients ≥75 years-old), 4 days on and 4 days off during the first month, and thereafter according to the prescribed protocol (23). In anuric patients, fluid-challenge may be attempted, with particular attention to signs of fluid overload; however, the initiation of dialysis should not be delayed in patients with severe renal failure (25).
In patients requiring dialysis, the use of high cut-off filters remains controversial, and no benefit in terms of survival or hemodialysis independence has been demonstrated in a meta-analysis of the 2 controlled studies available to date (26–28).
Therapy targeting the neoplastic clone should be initiated as soon as possible. In the absence of clear guidelines for this subgroup of patients, recommendations favor a first-line triplet regimen based on bortezomib and high-dose corticosteroid therapy (if appropriate to the patient’s frailty score), due to its efficacy, rapid onset of response, and pharmacokinetics that are independent of CrCl. According to published recommendations, bortezomib should be started on a twice-weekly basis, in association with high-dose dexamethasone (23). In patients undergoing dialysis, bortezomib should be administered preferably after dialysis. Cyclophosphamide does not require dose adjustment and the VCD regimen is recommended by the IMWG (23).
The pharmacokinetics and efficacy of carfilzomib are not influenced by renal dysfunction, making this drug a valid option at doses of 56 mg/m² (29). Ixazomib can also be used in this context, with a dose adjustment to 3 mg in cases of patients with CrCl <30 mL/min (30).
Thalidomide does not require renal dose adjustment, while lenalidomide doses should be adjusted according to CrCl. Although effective, it may be associated with increased toxicity, mainly hematological and infectious (23, 31, 32). Pomalidomide does not require renal dose adjustment and can be used in patients on hemodialysis, with comparable efficacy in patients with and without renal dysfunction and with an acceptable toxicity profile (32).
The rapid anti-neoplastic activity of anti-CD38 monoclonal antibodies allows for the potential reversibility of renal injury, and renal response rates of up to 70% have been reported with isatuximab (32).
Autologous hematopoietic stem cell transplantation (ASCT) is not universally recommended, but may be an option in selected patients. Although possible even in patients undergoing dialysis, transplant-related mortality is higher in patients with renal dysfunction (4% vs 1%) and should be considered with particular care. In these patients, melphalan dose adjustment is mandatory (100 to 140 mg/m2), but its efficacy seems to be preserved (23).
The selection of the therapeutic regimen in RRMM patients with renal dysfunction continues to be guided by frailty, and exposure and response to previous therapies (23, 29).
With the development of increasingly effective therapies and the increased survival of MM patients, kidney transplantation has become an option to consider in patients with dialysis-dependence and adequate response to therapy. Data from the American registry of kidney transplantation (National Kidney Registry) show equivalent transplanted organ lifespans in MM patients and in the general population. Survival remains lower in patients undergoing kidney transplantation due to MM, compared to other causes of renal failure, but this difference is not evident in patients over 50 years of age (33).
Neurological manifestations
The presence of peripheral neuropathy (PN) in a MM patient should raise the suspicion of associated amyloidosis (34). Although the incidence of PN varies between authors, it is estimated that up to 20% of patients with MM may present with PN at diagnosis, and up to 75% develop this complication during therapy (35).
Treatment-induced peripheral neuropathy (TIPN) is one of the most frequent complications (35–37) with implications for the management of therapeutic protocols, patient quality of life and future therapeutic options (36).The most frequently involved drugs are thalidomide and bortezomib (38, 39). TIPN presents as a distal, symmetrical sensory polyneuropathy with associated neuropathic pain (36, 37), which occurs spontaneously or after physical stimuli, such as touch, or thermal stimuli, such as cold or heat. There may be motor involvement, usually associated with severe sensory changes, as well as autonomic symptoms such as orthostatic hypotension, bradycardia, constipation, urinary incontinence or erectile dysfunction (36, 37, 40).
Close surveillance is fundamental for the early diagnosis of TIPN, and the patient should be alerted to the main symptoms related to TIPN; the involvement of the whole patient-care team is important in monitoring its progression.
In the assessment of the patient, the use of scales based on clinical evaluation and neurophysiological studies - such as the ICT-NCN and the Total Neuropathy Score (TNS) - are important (36).
Treatment includes correction of all potentially reversible additional causes of PN and control of comorbidities [e.g. vitamin B12 deficiency, alcoholism, chronic kidney disease or diabetes mellitus (36)], as well as early dose adjustments, to limit the consequences of neurological damage and prevent irreversible changes.
Dose adjustments should be made according to the recommendations defined for each drug, and are based on the grades established by the NCI-CTC. The IMWG recommends a different schema for bortezomib, with a switch to weekly treatment in Grade 1 TIPN, and definitive discontinuation if Grade 2 or higher and with pain (35). Thalidomide should be dose-reduced by 50% if Grade 1 TIPN, and suspended if Grade 2, with resumption with a dose reduction of 50% if there is an improvement in the PN to Grade 1 (35), always taking into account the risk-benefit ratio. The duration of thalidomide therapy should not exceed 6-12 months (35, 41) Currently, the use of other active treatments against the neoplastic clone, such as other PIs (ixazomib) and monoclonal antibodies, facilitate the management of these patients.
Duloxetine has been shown to reduce pain associated with TIPN, although MM patients were not included in duloxetine clinical trials (42, 43). The use of gabapentin or pregabalin, by analogy to the benefits seen with these drugs in neuropathic pain associated with other pathologies such as diabetes mellitus, trigeminal neuralgia or post-herpetic neuralgia, is widespread (37, 44). There seems to be no advantage with pharmacological prophylaxis, and there is no solid evidence of the benefit of adjunctive practices, such as exercise, acupuncture, cryotherapy, compressive therapy or transcutaneous electrical neurostimulation (TENS). Similarly, no benefit has been demonstrated with the use of vitamins either (44).
Assessment by a neurologist and referral to a chronic pain specialist may be necessary (35).
Cardiovascular involvement
The presence of cardiovascular (CV) risk factors or comorbidities at the time of MM diagnosis is frequent (45, 46) in elderly patients, and can be considered to fall into 3 categories:
- not directly related to MM nor to the targeted therapy, such as advanced age, diabetes mellitus, dyslipidemia, obesity, or previous cardiovascular disease
- directly related to MM, such as cardiac AL amyloidosis, hyperviscosity, high output heart failure, arteriovenous shunts, anemia, and renal dysfunction
- resulting from MM treatment-related toxicity, including through anthracyclines, corticosteroids, alkylating agents, IMIDs and PIs, often in combination regimens (47).
Assessment of cardiovascular risk prior to the initiation of therapy
The recommendations published by the European Society for Medical Oncology (ESMO) and the European Society of Cardiology (ESC) (48, 49) regarding the management of treatment-related cardiac events indicate that an assessment of the potential risk for cardiotoxicity and of pre-existing CV risk factors - such as obesity, smoking, diabetes mellitus, hypercholesterolemia, and personal or family history of CV disease (50)- should be performed before treatment initiation, and patient education and healthy lifestyle changes should be encouraged.
Cardiac function should be assessed by objective examination, electrocardiography (ECG) and echocardiography (51) including left ventricular ejection fraction (LVEF), cardiac morphology and valvular function assessment. The basal determination of brain natriuretic peptide (BNP) and its precursor (NT-proBNP) can also be used, but there is a low specificity in MM patients (51). Some authors indicate that blood pressure (in dorsal decubitus and orthostatism) should be assessed on D1 of each treatment cycle (51). Patients treated with carfilzomib have an increased risk of cardiac toxicity after 75 years of age and if one of the following risk factors is present: heart failure with or without reduction of LVEF, coronary heart disease, valvular pathology, cardiomyopathy, uncontrolled arrhythmia or previous anthracycline therapy. Patients who are smokers, obese or sedentary are also at increased risk of cardiac adverse events (52).
Up to 30% of MM patients may have cardiac involvement by AL amyloidosis deposits, that probably will increase with improving longevity in MM. This involvement can be asymptomatic but confers dismal prognosis often constituting major morbidity. In patients with abnormal BNP/NT-proBNP values or suggestive alterations in echocardiography, a cardiac magnetic resonance should be performed (53).
Cardiovascular risk monitoring and management during therapy
During treatment, patients and physicians should be aware of possible signs and symptoms of CV origin. Symptoms of dyspnea, chest pain, edema or fatigue should be investigated to ascertain whether they are being caused by cardiac dysfunction. Monitoring of cardiac function during treatment using echocardiography and ECG is also recommended. If a significant decline in LVEF is observed (>10% below the lower limit of normal), initiation of targeted treatment for left ventricular dysfunction with angiotensin-converting enzyme inhibitors and beta-blockers should be considered (48). The decision to continue or discontinue treatment must be made individually, taking into account the context of each patient, their relative risk, overall CV status and also the probability of cardiac effects of the prescribed drugs (51). In the case of treatment with carfilzomib, the recommendations of the European Myeloma Network (EMN) for grade 3 (or higher) cardiac adverse events are to suspend the drug and administer fluids. If deemed appropriate, carfilzomib therapy can be restarted at a lower dose level, based on an individualized risk-benefit assessment. A sub-analysis of the ENDEAVOR study suggests that the reduction in LVEF related to bortezomib or carfilzomib is in most cases reversible (54). When therapy is restarted, follow-up should be considered with regular echocardiography (52) and clinical evaluation, whenever possible in a cardio-oncology consultation.
Prevention remains crucial to improve patient care in this setting. Cardioprotective drugs can be given in addition to specific thromboprophylaxis whenever necessary. There are a small number of studies suggesting that angiotensin-converting enzyme inhibitors such as enalapril, angiotensin receptor blockers such as candesartan, and selected beta-blockers such as carvedilol and nebivolol, may be the preferred agents to reduce the risk of cardiotoxicity, in addition to mineralocorticoid receptor antagonists such as spironolactone (55).
Hemostatic abnormalities
Thrombotic Complications
The incidence of venous thromboembolism (VTE) in patients with MM is approximately 9 times higher than in the general population, with about 8-12 cases per 1,000 patient-years; the risk of arterial thrombosis is also increased. VTE is a leading cause of death in cancer patients and, in the case of MM patients, the presence of VTE in the first year after diagnosis is associated with a three-fold increase in the risk of death, compared to patients without VTE (56). In addition to the increased risk induced by the neoplasm, some drugs (e.g. IMIDs) specifically increase the risk of thromboembolism. Several scores have been published to stratify the risk of VTE (and the consequent indication for prophylaxis) in patients with MM (IMWG, SAVED, IMPEDE VTE); however, none has demonstrated a satisfactory discriminatory power, and this remains an unmet need (56–58).
Increased D-dimer and PAI-1 levels have been associated with an increased risk of VTE in MM patients. However, elevation of D-dimer above the normal upper limit was nearly universal with no consensus on a clear cut-off point at which it becomes predictive. Data about fibrinogen, FVIII, alpha-2-antiplasmin and Protein C and S found no significant relation with VTE risk and markedly conflicting results were observed to date. Also, the toxic effect of anti-myeloma therapies on the endothelium and contribution to thrombosis has been widely described (59, 60).
VTE therapy in patients with MM should be carried out according to international guidelines (61, 62). Before initiation of therapy with IMIDs, risk factors for VTE should be assessed (Table 2). The guidelines published by the IMWG (2008), still widely used today, advocate for the use of acetylsalicylic acid (ASA) 75-325 mg od in patients with 0 to 1 risk factors, and low molecular weight heparin (enoxaparin 40 mg od, or equivalent) or warfarin for a target INR of 2.0-3.0, in patients with 2 or more risk factors (63)(Table 3) and all those receiving high dose dexamethasone (≥480 mg per month), concomitant doxorubicin or multidrug regimens (excluding bortezomib).
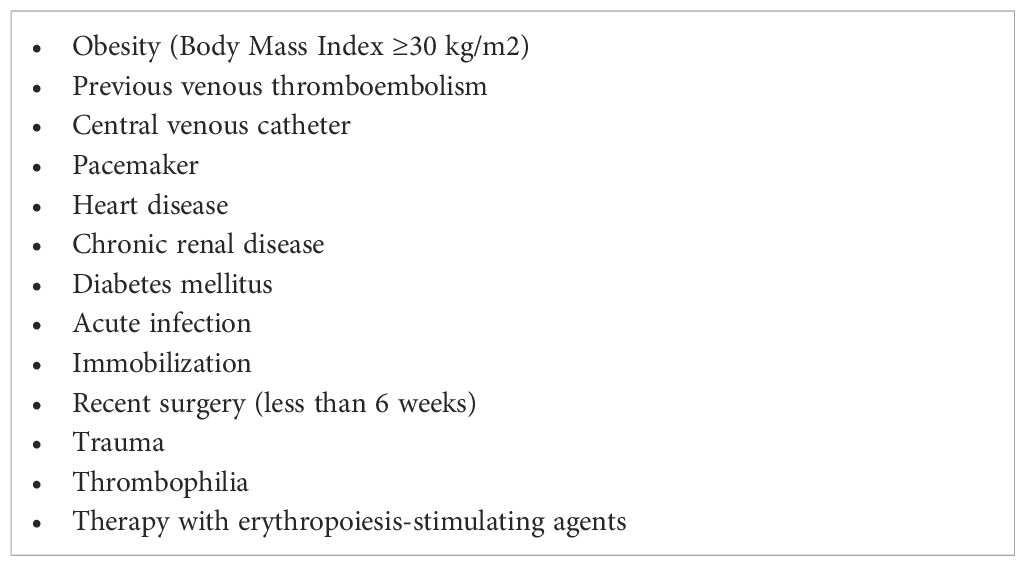
Table 3 Risk factors for venous thrombosis in patients with multiple myeloma.
The guidelines recently published by the American Society of Hematology (ASH), recommend the use of low-dose ASA, low and fixed-dose vitamin K antagonists (1.25 mg daily) or low molecular weight heparin (LMWH) in patients receiving regimens including IMIDs (61). Despite its superior efficacy, especially in high-risk patients, the use of subcutaneous (SC) therapy with LMWH for prolonged periods becomes a less comfortable option in the long term due to the route of administration (61).
The evidence for the direct oral anticoagulants (DOACs) in VTE prophylaxis in MM and cancer, in general, is still limited (with some studies demonstrating efficacy at the cost of an increased risk of bleeding, and with most trials including <5% of MM patients). Several trials with DOAC are ongoing, and many authors already advocate their use, based on their safety profile and convenient administration (64–67).
According to ASH recommendations, therapy with LMWH or with DOACs (apixaban and rivaroxaban) is indicated in the first 5-10 days after a thrombotic event. In patients with severe renal impairment (CrCl <30 mL/min), non-fractionated heparin should be considered, although from a practical point of view, this option is less feasible. Over the subsequent 3 to 6 months, therapy with a DOAC (apixaban, edoxaban, or rivaroxaban), LMWH or, as a last resort, warfarin, is recommended. In patients with CrCl <30 mL/min, warfarin is the preferred option for prolonged therapy. For patients with recurrent VTE despite LMWH at a therapeutic dose, recommendations suggest increasing the dose to supra-therapeutic levels or maintains a therapeutic dose (61). In patients with active cancer and VTE, long term maintenance of anticoagulation at a therapeutic dose is suggested. The choice of NOACs over vitamin K antagonists is also recommended in the guidelines of other scientific societies (61, 62).
Thrombocytopenia is a frequent constraint in VTE prophylaxis. Prophylaxis should be maintained, with close monitoring, in patients with platelet counts of 50 to 100 x 109/L,and discontinued in the majority of patients with platelet counts <50 x 109/L, particularly after 6 months of therapy with IMIDs (where the risk of thrombosis is lower); maintained could be indicated in high-risk patients, always weighing thrombotic and bleeding risks (68).
Hemorrhagic complications
Hemorrhage is rarely associated with MM at diagnosis, being mostly prevalent in progressive disease, particularly in association with hyperviscosity syndrome, thrombocytopenia, renal failure or infection (68, 69).
Abnormal screening coagulation test results, including prothrombin time (PT), activated partial thromboplastin time (APTT), and thrombin time (TT), are commonly encountered in patients with plasma cell neoplasms and are not typically associated with clinically significant bleeding (69).
In patients on antithrombotic prophylaxis and IMIDs, the incidence of major bleeding is higher in patients with a previous history of bleeding, renal disease or advanced age (70).
The use of ASA in combination with corticosteroids (particularly dexamethasone) is associated with an increased risk of bleeding, especially gastrointestinal hemorrhage, so caution is advised in patients with previous episodes of ulcerative peptic disease, or other causes of digestive bleeding (61).
Bone disease
Bone disease, in particular lytic lesions, result from the neoplastic proliferation of plasma cells and alterations in the bone remodeling mechanisms, leading to bone pain. The management of bone pain in MM is mostly palliative but essential for the patient’s quality of life. It includes antiresorptive therapy (e.g. bisphosphonates), to prevent new lesions, radiotherapy, surgery, corticosteroids and analgesia (71).
Intravenous antiresorptive therapy with bisphosphonates should be administered in MM patients under chemotherapy, regardless of the existence of bone disease, although its benefit in patients without bone disease staged by MRI or PET has not been unequivocally demonstrated (71).
Zoledronate or pamidronate, at 28-day intervals, should be given for at least 12 to 24 months in patients with a complete response or a very good partial response, and until disease progression in the case of partial response or stable disease (71). Patients should be monitored for renal function and electrolyte imbalance – particularly of calcium and phosphorus -, and 600 mg of calcium and 400 IU of vitamin D supplements should be given daily.
Osteonecrosis of the jaw (the exposure of jaw bone without healing after 2 months of therapy) is a complication described in 5-10% of patients on bisphosphonate therapy, with an incidence of 1% per year (68). Risk factors include dental procedures, local infections or concomitant corticosteroid therapy. Dental evaluation is recommended before bisphosphonate therapy is started, with dental extractions or other more invasive procedures performed, if necessary. If there is an episode of osteonecrosis, there is no contraindication to restarting bisphosphonates after healing (68).
Radiotherapy is an excellent tool to consider for the relief of bone pain, particularly in acute pain occurring in the context of vertebral collapse. A single dose of 8 Gy is recommended (68). Higher doses, up to 30 Gy, fractionated over 2 weeks, are associated with better pain control and should be considered when there is an associated soft tissue component or pathological fracture with spinal cord compression (72).
Vertebroplasty and kyphoplasty are alternatives to control pain associated with vertebral collapse. These techniques consist of the percutaneous injection of bone cement to stabilize the vertebral body, and should ideally be performed as soon as possible after vertebral collapse. Both techniques carry a low risk of extravasation of bone cement, with the possibility of neurological compromise or thromboembolism (71, 73). These techniques are equally effective as surgery in treating pain, with very low infectious risk (74). If vertebral collapse with spinal cord compression occurs, this must be approached as a medical emergency, due to the risk of irreversible neurological lesions.
Chronic and acute pain
Chronic pain is one of the most frequent symptoms in MM patients, in relation either to bone disease or to peripheral neuropathy. The WHO establishes a 3-step algorithm in pain management, taking into account the pain score reported by the patient:
- Scores 1-4: do not require opioid use. Paracetamol (up to 3 g/day, oral or IV) should be preferred. Non-steroidal anti-inflammatory drugs should be used with caution due to their renal, gastrointestinal and hematological side effects.
- Scores 5-6: weak opioids associated with non-opioids, such as tramadol (up to 400 mg/day, per os, SC, IM or IV) and paracetamol, may be used.
- Scores 7-10: strong opioids are mandatory. Morphine (oral, SC or IV, including continuous infusion) is a good option given its efficacy, safety profile, versatility, and low cost. Fentanyl is about 100 times more potent than morphine and, although it can be given IV, it is primarily given transdermal in chronic pain, and via the transmucosal or sublingual route in acute pain (75).
Patients with pain scores greater than 5 or who, after analgesic therapy, do not show a score reduction of at least 2 points, should be referred to pain medicine teams (68).
The most common adverse effects of opioids include constipation, nausea and vomiting, pruritus, urinary retention, respiratory failure, and tolerance and hyperalgesia (with these latter two situations requiring referral to pain medicine specialists). Concomitant prescription of antiemetics and laxatives is advised (68, 75).
Given the mixed etiology of pain in MM patients, a multimodal approach is the most appropriate. In this regard, the concomitant use of calcium channel blockers such as gabapentin or pregabalin, as well as antidepressants such as duloxetine or amitriptyline should be considered (76).
Metabolic disorders
Hyperglycemia
Diabetes is a frequent comorbidity of MM, with an estimated 11-22% of MM patients presenting with diabetes or other disorders of glucose metabolism (8). It is recommended that MM patients be screened for diabetes (by fasting blood glucose and, ideally, HbA1c levels) before initiation of corticosteroid therapy, particularly if they have additional risk factors such as age, obesity, a family history of diabetes or a personal history of gestational diabetes (8, 77).
Patients previously on oral antidiabetics who maintain adequate glycemic control should maintain their usual therapy. However, most patients will need to initiate insulin therapy, and those previously on insulin will likely need to increase basal and pre-prandial insulin doses 2- to 3-fold (8, 77). On the other hand, it should be noted that patients with MM often present with anorexia and nausea/vomiting, which can lead to hypoglycemic events, particularly when medicated with high-risk oral antidiabetics, such as sulfonylureas, or high doses of basal insulin; basal therapy adjustments are recommended, particularly by changing sulfonylureas to metformin and/or glinides, as well as avoiding mixed insulins and favoring rescue with rapid insulin according to pre-prandial glycemic levels (8, 77). Reductions in the dose of corticosteroids must be accompanied by a reduction in insulin doses, to minimize the risk of hypoglycemia (77).
In addition to hyperglycemia, diabetes mellitus is associated with multiple organ dysfunctions - neuropathy, nephropathy, retinopathy and cardiovascular changes - which may also be induced by MM itself, worsening their severity and potentially confounding an adequate diagnosis and a timely correction (8).
Electrolyte imbalances: hyper- and hypocalcemia
The mainstay of therapy for hypercalcemia is intravenous hydration (0.9% sodium chloride, 35 mL/kg/day in young patients, and 15-20 mL/kg/day in elderly patients with renal, hepatic or cardiac dysfunction), bone disease-modifying agents, calcitonin, corticosteroids and, in particularly severe and refractory cases, hemodialysis. Diuretics should be delayed until adequate hydration has been ensured, and calcium and vitamin D supplements should be discontinued (64, 72, 78).
Prevention of bone resorption with targeted therapies (namely bisphosphonates) is essential to restore the homeostasis of calcium metabolism, with an onset of action about 2-4 days after administration (79). Among the bisphosphonates, zoledronic acid has been shown to be superior in the rate of normalization, time to resolution and duration of hypercalcemia control, compared with pamidronate (80). Zoledronic acid is administered in a single dose of 4 mg (in 100 mL of 0.9% sodium chloride or 5% glucose, infused over 15-30 minutes) in patients with a corrected serum calcium ≥ 12 mg/dL, whereas the maximum daily dose of pamidronate is 90 mg (diluted in 500 mL of 0.9% sodium chloride or 5% glucose, given in a 2-4 hour infusion, at a maximum rate 1 mg/min), once every 4 weeks. A supplementary dose may be given in the absence of reversal of hypercalcemia after 3-7 days (81).
Dose adjustment of bisphosphonates is necessary in renal dysfunction (Table 3) (72, 79), and bisphosphonates are formally contraindicated in severe renal dysfunction (CrCl <30 mL/min); however, in the case of severe hypercalcemia in which the benefits outweigh the risks, the lowest dose should be given, with a prolonged infusion time. In the case of moderate renal impairment, the dose should be adjusted according to Table 4 (82).
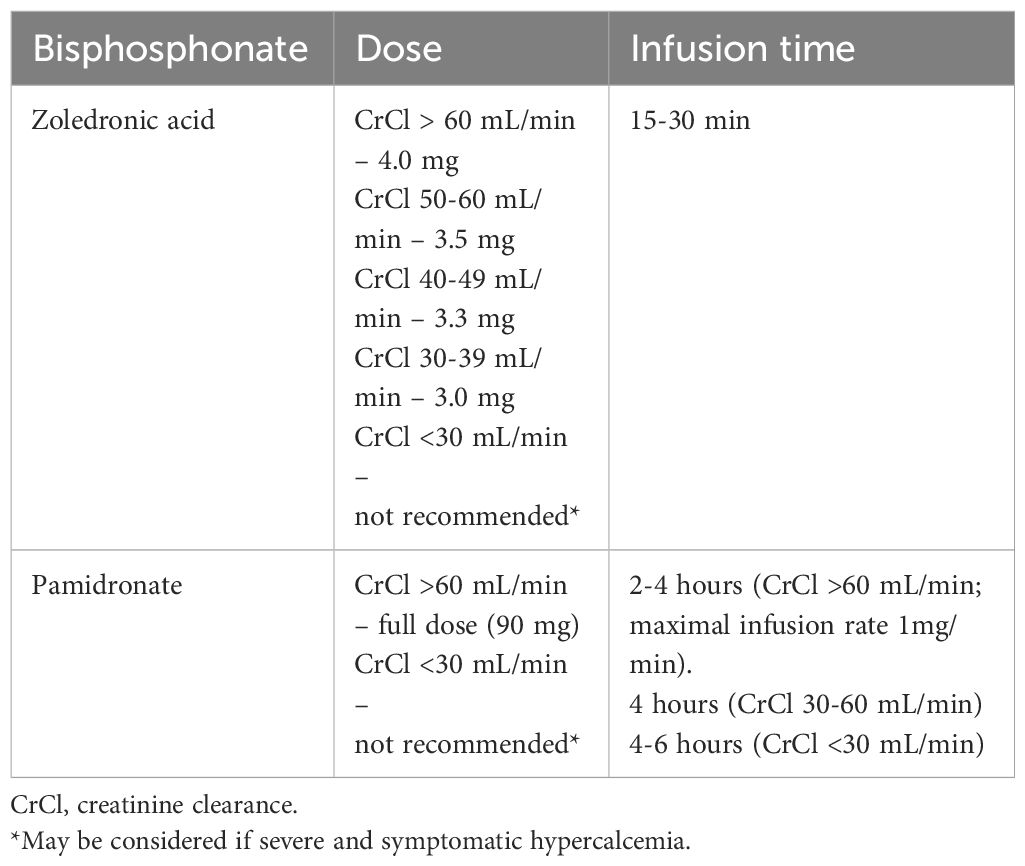
Table 4 Dose and infusion time of bisphosphonates according to renal function.
Denosumab, a humanized monoclonal antibody directed to the RANK ligand (receptor activator of nuclear factor Kappa B) may be considered in the management of hypercalcemia that is refractory to bisphosphonates, as well as in patients with severe renal dysfunction, as it is not excreted by the kidneys (79). Denosumab has been shown to be associated with a greater reduction in serum calcium levels when compared with zoledronic acid (83). The recommended dose in hypercalcemia is a single administration of 120 mg, sc, in patients with serum calcium levels >12.5 mg/dL (79).
Calcitonin can be administered at a dose of 4-8 IU/kg, sc, every 6-12 hours, with a faster onset of action than bisphosphonates (within the first 4-6 hours after administration). However, its effect is limited in time (24-48 hours) due to the risk of tachyphylaxis (64, 84).
Although MM is classically associated with hypercalcemia, hypocalcemia may be present, mostly as a consequence of hypercalcemia therapy or bone disease. It is almost always asymptomatic; symptoms (such as paresthesia, cramps and rarely cardiac dysfunction) usually are only present with severe hypocalcemia (serum calcium levels <7 mg/dL) (64, 82).
Treatment-induced hypocalcemia is more frequently seen in patients on denosumab therapy (17%) than in those on zoledronic acid (12%) (83). In patients with renal dysfunction, denosumab dose adjustments should be considered due to the increased risk of hypocalcemia (85).
Tumor lysis syndrome
MM is associated with a low incidence of tumor lysis syndrome (TLS); patients at higher risk are those with baseline hyperuricemia, renal dysfunction, volume depletion or high tumor burden. In the current therapeutic scenario, bortezomib and carfilzomib are the drugs most frequently associated with this complication. Prophylaxis of TLS is recommended with reinforcement of oral hydration and allopurinol (100-300 mg/day) (64, 86, 87). Anti-myeloma monoclonal antibodies (daratumumab, isatuximab, elotuzumab) and the antibody-drug conjugate belantamab mafodotin have been shown to induce TLS (88), as has CAR-T cell therapy (89).
In patients with ongoing TLS or severe hyperuricemia, administration of rasburicase (0.2mg/kg/day, in 50 mL of 0.9% sodium chloride, infused over 30 minutes) is recommended (64, 86).
Neuropsychiatric symptoms
Corticosteroids are associated with a wide spectrum of clinical manifestations - ranging from sleep and mood disturbances, including insomnia, irritability, depression and euphoria, to cognitive impairment, psychosis and delirium -, in about 60% of patients. Although existing research suggests that there is a dose-dependent relationship between steroids and neuropsychiatric symptoms, with increased cases reported at higher doses, even very low doses can lead to symptoms (90, 91).
Corticosteroid-induced neuropsychiatric symptoms have a variable chronological relationship to the initiation of therapy, ranging from hours from the first administration, to late manifestations and even after the terminus of therapy. However, most manifestations occur early after the start of therapy (days) (90).
Among the corticosteroids, those with a long duration of action (such as dexamethasone) are associated with a higher incidence of symptoms, and evidence suggests that non-continuous regimens may have less severe symptoms (90).
The hyperviscosity syndrome (present in 2-6% of patients with MM) also manifests itself with non-specific neurological symptoms that range from the - headache, dizziness, tinnitus, difficulty concentrating, sleepiness or hypoacusis to ataxia, convulsions, and even coma, in addition, to an increased risk of stroke (92).
In the presence of persistent unexplained psychiatric and neuropsychiatric symptoms, particularly in patients who have previously undergone multiple lines of therapy, it is important not only to perform central nervous system (CNS) imaging (with CT and/or MRI) but also a cerebral spinal fluid analyses to exclude CNS involvement by MM (present in <1% of patients and usually in progressive disease) or infection (bacterial, viral or fungal meningitis, or more rarely infection by the JC virus) (64, 93).
Ocular disorders
Ocular manifestations due to the direct invasion of ocular structures by MM are rare, and may be present in heavily pretreated patients and with uncontrolled systemic disease. Therapy focuses on systemic treatment, targeted radiotherapy and, in specific cases, decompressive surgery (93, 94).
Hyperviscosity syndrome can present with visual manifestations, such as blurred vision or diplopia. Ophthalmoscopic examination of the fundus can reveal characteristic findings of hyperviscosity, such as the presence of dilated and tortuous retinal veins, flame-shaped hemorrhages, edema of the papilla, and retinal exudates. Although uncommon, there may be central retinal vein occlusion and retinal detachment (92).Once the diagnosis is established (or if suspicion is high), emergent therapy with plasma exchange is imperative. Initial exchange of 1.5 plasma volumes in the first session and 1 volume in subsequent sessions is recommended. Replacement fluids should be 5% albumin and fresh frozen plasma, to reduce the risk of coagulopathy. Although there is no evidence regarding the ideal number of sessions, daily sessions for three days with frequent reassessment and simultaneous initiation of MM-targeted therapy are recommended.
It Is estimated that about 12% of MM patients experience ocular adverse effects of treatment, with the most common being keratopathy/keratitis, xerophthalmia and blurred vision. In most cases, there is a resolution with topical therapy (95).
In addition, some of the drugs used in MM treatment have specific ocular toxicity. Glaucoma and cataracts are the main adverse effects of corticosteroids. In the case of glaucoma, therapeutic protocols with lower doses of corticosteroids should be considered (96). Patients at high risk for cataracts (namely those with a previous history of glaucoma) and/or those with reduced visual acuity should be observed by the ophthalmologist (97).
Corneal epithelium changes (keratopathy) were found in patients treated with belantamab mafodotin, an antibody-drug conjugate targeting the B-cell maturation antigen (BCMA), in the DREAMM-2 study, where it led to the majority of dose adjustments, treatment delays and discontinuations. Patient education is key to minimizing and preventing complications associated with belantamab mafodotin. To minimize the risk of ocular toxicity, it is imperative that patients see an eye specialist for baseline assessment prior to starting treatment and prior to each subsequent dose, to monitor for worsening eye symptoms (dry eyes, blurred vision, deteriorating visual acuity, and corneal ulceration). To help reduce the incidence of ocular events, patients should be educated on the use of preservative-free ophthalmic lubricants at least four times daily starting prior to the first treatment and continuing to the end of treatment. Since patients with preexisting corneal disease are at higher risk of developing keratopathy, contact lens use discontinuation is recommended while on therapy (98).
Cutaneous lesions
Exanthema is one of the most common non-hematological adverse effects of IMIDs and PIs (although less frequent and less severe with the latter), and may present different features including morbilliform, dermatitis-like, acneiform or urticarial exanthema. Mild to moderate cases of exanthema associated with PI therapy or IMIDs can be treated with topical corticosteroids and oral antihistamines, while in severe cases discontinuation of the drug and the use of systemic corticosteroids are recommended. There is usually good tolerance to the reintroduction of the drug (particularly lenalidomide) within 1-2 weeks of resolution, and desensitization protocols can be performed in patients with recurrence of symptoms (99–102).
Gastrointestinal manifestations
Gastrointestinal tract symptoms are very frequent in patients with MM (103, 104). Constipation is a complaint often associated with opioid analgesics but also with thalidomide and 5-HT3 receptor antagonists (used in the prevention or treatment of emesis) (68). Dietary measures and laxatives are useful in these situations (68, 105). Diarrhea is also a symptom frequently associated with bortezomib and ixazomib (in up to 45% of patients) (106) and occurs on the day of administration or the following day (107). Therapy is symptomatic; in severe cases, dose reduction or even suspension of these drugs may be necessary (106).Lenalidomide-associated diarrhea is also of note, as it is frequent with prolonged use (occurring in about 30% of patients) (105, 108). It appears several months after the start of treatment (108) and seems to be related to bile acid malabsorption (109). Reduced dietary fat intake and the use of bile acid chelators such as cholestyramine are recommended (109). General measures in any patient with diarrhea include proper hydration, a low-fiber diet, and the consumption of frequent, lighter meals. Loperamide and electrolyte replacement therapy may also be used (105).
Several treatment protocols include a prolonged use of corticosteroids, which can lead to an increased risk of gastrointestinal bleeding and colonic perforation (110, 111). Therefore, prophylactic proton pump inhibitors should be prescribed concomitantly with these drugs.
Taking into account that gastrointestinal symptoms are very frequent and non-specific and that, although they may be related to the disease, to treatment toxicity, or to other causes such as infections, neoplasms and AL amyloidosis (112), careful investigation is recommended, with evaluation by a gastroenterologist whenever necessary.
Second primary malignancies
The risk of second primary malignancies (SPM) in MM is low and is partially related to the increased survival of these patients (113), and no particular oncological screening program has been defined within this context. The development of SPM is multipronged, including treatment-related factors (such as alkylating agents or lenalidomide), MM-related factors (with an increased risk of acute myeloid leukemia in IgG and IgA gammopathies), patient-related factors (genetic polymorphisms, advanced age, male gender, or previous neoplasms), as well as environmental and behavioral factors (114).
Combined exposure to drugs such as lenalidomide and oral melphalan appears to be the main factor associated with a substantially increased risk of hematological SPM (acute myeloid leukemia and myelodysplastic syndrome) (113, 115). Some studies also evidence an increased risk (although lower) of SPM in patients treated with lenalidomide on a maintenance regimen (113). However, this risk is largely outweighed by the favorable impact of maintenance therapy on patient survival.
The most frequent SPM include cutaneous neoplasms (basal cell or spinal cell carcinoma) (114), solid neoplasms, mainly urinary tract tumors (partly explained by the renal excretion of lenalidomide) (113) and hematological neoplasms. An increased incidence of SPM has not been observed with the association of lenalidomide and dexamethasone, or with the various associations with bortezomib (melphalan, dexamethasone, or thalidomide) (113).
Thus, the therapeutic decision process in MM should not influenced by the risk of SPM, since the risk of death from MM is substantially higher than the risk of death from a SPM. However, and because of the above, treatment regimens including associations of lenalidomide with melphalan should be avoided. Furthermore, close and timely monitoring of more susceptible organs or systems is fundamental to the early diagnosis of a SPM.
Teratogenic risk
Due to the low incidence of MM in young adults, the available data regarding the safety of anti-myeloma drugs during pregnancy are very limited. First-generation alkylating drugs and PIs, such as bortezomib, are among the drugs most often used in the treatment of MM, and have been associated with a risk of intrauterine death and fetal malformations in animal studies. For this reason, the FDA classifies these drugs in category D of pharmacological risk in pregnancy (116, 117). Corticosteroids are the group of drugs with the best safety profile when used during pregnancy, especially after the first trimester (category C pharmacological risk in pregnancy, according to the FDA (118, 119). Data on the use of monoclonal antibodies and subsequent-generation PIs in pregnant women are insufficient, so their use is not recommended during pregnancy or in women of childbearing potential who do not use contraception (116, 119) during treatment. IMIDs are contraindicated during pregnancy because of their well-established teratogenic risk (113, 119).
Toxicities associated with autologous stem cell transplant
In the era of innovative drugs, significant progress has been achieved in the treatment of multiple myeloma. However, for young and eligible patients, high-dose chemotherapy with melphalan followed by autologous stem cell transplant (ASCT) continues to stand as the gold standard. This approach boasts a remarkably low transplant-related mortality rate, ranging from 1% to 2%, despite the rapid evolution of treatment modalities (120, 121).
Over the past few decades, advancements in hematopoietic stem cell mobilization have given rise to the creation of regimens that are both less toxic and more effective. Notably, there are now chemo-free protocols, such as the combination of G-CSF plus plerixafor, which eliminate the concerns associated with neutropenia and the potential risk of febrile neutropenia (122).
Hematological toxicity is an anticipated side effect that impacts every multiple myeloma (MM) patient undergoing autologous stem cell transplant (ASCT), albeit with varying degrees of severity. Following the myeloablative effect induced by melphalan and occurring prior to engraftment, typically around Day 12 post-transplant, patients experience profound neutropenia and lymphopenia, along with varying levels of anemia and thrombocytopenia (121). During this period, febrile neutropenia is highly prevalent, affecting approximately half of patients, particularly those with severe oral and gastrointestinal mucositis, reaching grades 3-4 in 30 per cent of cases (123).
Non-pharmacological interventions for oral and gastrointestinal mucositis, as well as nausea/vomiting, such as cryotherapy and modified diets, respectively, can prove beneficial in alleviating patients’ distress and reducing the severity of symptoms (121, 124, 125).
Prophylaxis for HSV/VZV using acyclovir, for Pneumocystis jirovecii with trimethoprim-sulfamethoxazole, and antifungal with fluconazole should ideally be administered until Day 100 post-transplant (123, 126).
A delay in the recovery of lymphocyte count and function, which can extend up to 2 years for CD4+T cells, contributes to an elevated risk of infections beyond Day 100 post-transplant. This heightened susceptibility is primarily attributed to encapsulated bacteria, viruses, Aspergillus spp., and Pneumocystis jiroveci. The myeloablative conditioning regimen results in the loss of immunological memory, necessitating patients to essentially repeat the entire vaccination plan (123, 126).
High-dose melphalan conditioning does not appear to elevate the risk of secondary neoplasms. The 10-year incidence rates for secondary myelodysplasia and acute myeloid leukemia stand at 4% and 2%, respectively (121, 127).
Toxicities associated with T-cell engaging therapies
In recent years, immunotherapy has made significant strides in the field of multiple myeloma, particularly with the introduction of T-cell engaging therapies, including bispecific T-cell engagers (BiTEs) and chimeric antigen receptor (CAR)-T cells. Currently, both the FDA and EMA have granted approval for BiTEs such as teclistamab (anti-BCMA/CD3), talquetamab (anti-GPRC5D), and elranatamab (anti-BCMA/CD3), as well as anti-BCMA CAR-T cells, namely ciltacabtagene autoleucel and idecabtagene vicleucel (128, 129).
However, these therapies brought along additional toxicities, requiring the adoption of an entirely new approach (130, 131).
Cytokine release syndrome (CRS)
The cytokine release syndrome (CRS) is a multisystemic syndrome observed in both BiTEs (72-56%; <1% grade≥3) and CAR-T therapies (84-95%; 4-5% grade≥3). It arises from T-cell activation and proliferation, resulting in systemic inflammation (131).
In patients receiving BiTEs, CRS typically manifests during step-up doses and the initial full dose. Conversely, in CAR-T cell therapy, it generally occurs 1-14 days post-infusion with varying durations (131, 132).
CRS is characterized by fever accompanied by hemodynamic instability and/or hypoxemia, with severity graded according to the American Society for Transplantation and Cellular Therapy consensus criteria (Hayden et al., 2022). A high level of suspicion is crucial for an appropriate approach, emphasizing the importance of early diagnosis and therapy. Management of CRS is contingent on its severity, incorporating supportive therapy (IV fluid hydration, vasopressor support, supplemental oxygen/mechanical ventilation, and antibiotics). Additionally, tocilizumab (IL-6 receptor antagonist), corticosteroids, and, in refractory cases, siltuximab (anti-IL-6) or anakinra (anti-IL1-R) are used (131–133).
Immune effector cell-associated neurotoxicity syndrome (ICANS)
The immune effector cell-associated neurotoxicity syndrome (ICANS) encompasses a range of neurological symptoms, often emerging within the initial days following CAR-T infusion (18-17%; 2-3% grade≥3) or during the administration of the first BiTEs doses (3-6%; 0-1% grade≥3). Despite ongoing research, the precise cause of ICANS remains incompletely understood, with various studies proposing that its pathophysiology revolves around the release of cytokines and subsequent inflammation in the central nervous system (131, 132).
Manifestations of ICANS span from mild symptoms like tremors, somnolence, or dysgraphia to more severe conditions such as aphasia, apraxia, seizures, or even coma. Monitoring and grading involve the systematic use of the 10-point Immune Effector Cell Encephalopathy (ICE) scale (132). A comprehensive diagnostic approach, including consultation with a neurologist, electroencephalogram, and MRI evaluation, is crucial. Treatment is centered on a symptomatic approach utilizing antiseizure drugs, corticosteroids, and, in severe cases, siltuximab or anakinra (131–133).
Delayed neurotoxicity, primarily observed in CAR-T cell therapy (affecting 12% of patients), may present as cranial nerve palsies, neuropathy, or parkinsonism. Treatment is based on corticosteroids and intravenous immunoglobulin (131, 132).
Infectious complications
One of the most prevalent complications involves opportunistic infections, primarily stemming from neutropenia, lymphopenia, and B-cell aplasia, leading to hypogammaglobulinemia. As a result, prophylaxis is necessary until immune reconstitution (132). Consensus guidelines advocate for acyclovir/valacyclovir to prevent HSC/VZV reactivation, trimethoprim-sulfamethoxazole for Pneumocystis jirovecii (in CAR-T cells: recommended for 12-18 months post-infusion, at least until CD4 count exceeds >200/μL; in BiTEs: during treatment and up to 1 month post-treatment discontinuation), and antifungal prophylaxis with fluconazole during periods of prolonged severe neutropenia or extended steroid therapy (131, 134).
Following CAR-T cell therapy (preceded by lymphodepletion), neutropenia and lymphopenia are common, impacting approximately 10-20% and 40-50% of patients, respectively, within 3 months post-infusion. Bacterial and respiratory viral infections dominate in the first month, transitioning to a prevalence of viral infections thereafter (132, 134). Particularly in T-cell engaging therapies targeting BCMA, hypogammaglobulinemia stands out as a key risk factor for infections. Therefore, the replacement of immunoglobulins is recommended for cases with gammaglobulin levels <4 g/L, particularly when associated with serious, recurrent, or chronic infections (131, 132, 134).
Other toxicities
Hematological toxicity represents a frequent adverse event associated with T-cell engaging therapies, particularly CAR-T cells. The incidence and severity of this toxicity tend to escalate in patients experiencing complications such as CRS, ICANS, or immune effector cell-associated hemophagocytic lymphohistiocytosis-like syndrome (IEC-HS)/macrophage activation syndrome (MAS). In such cases, cytopenias can be profound and prolonged, heightening the vulnerability to infections. The management of this toxicity aligns with established approaches for other drugs, involving interventions like transfusions and growth factor support, primarily with G-CSF. However, a small subset of refractory patients may necessitate more advanced measures, such as autologous hematopoietic stem cell boost or allogeneic hematopoietic cell transplantation (130–132, 135).
Certain agents exhibit distinct and common adverse events, as observed with talquetamab, which is known to frequently induce skin and nail-related events, along with dysgeusia (131).
Conclusions
Despite the increased efficacy and survival with new treatment options, patients with MM continue to present with a high burden of symptoms, resulting not only from the disease but also from treatment toxicities, even in periods of disease remission and off treatment. These symptoms and adverse events have a profound impact on their quality of life, namely due to sequelae of bone destruction, reduced physical capacity and loss of muscle mass, frequently associated with chronic pain, therapeutic toxicities and worsening of comorbidities. Thus, personalization of treatment in MM patients is critical to ensure effective long-term disease control and should be based on individual patient factors such as age, general condition, comorbidities, and side effects of previous treatments. Rapid and appropriate intervention on treatment-related adverse events and on worsening of comorbidities should be based on scientific evidence, consensus recommendations, clinical experience, and is of extreme importance for patients and their families, impacting the prognosis and quality of life of those who suffer daily with MM.
Author contributions
CG: Conceptualization, Methodology, Supervision, Writing – original draft, Writing – review & editing. AR: Methodology, Writing – original draft, Writing – review & editing. ABSR: Methodology, Writing – review & editing. MN: Methodology, Writing – original draft, Writing – review & editing. AI: Methodology, Writing – original draft, Writing – review & editing. RG: Methodology, Writing – original draft, Writing – review & editing. AT: Methodology, Writing – original draft, Writing – review & editing. SA: Methodology, Writing – original draft, Writing – review & editing. MS: Methodology, Writing – original draft, Writing – review & editing. PS: Writing – review & editing. RB: Conceptualization, Methodology, Supervision, Writing – original draft, Writing – review & editing. CJ: Conceptualization, Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. International Agency for Research on Cancer (IARC). Portugal - global cancer observatory. Globocan (2020).
2. Anderson KC. Progress and paradigms in multiple myeloma. Clin Cancer Res an Off J Am Assoc Cancer Res (2016) 22:5419–27. doi: 10.1158/1078-0432.CCR-16-0625
3. D’Agostino M, Bertamini L, Oliva S, Boccadoro M, Gay F. Pursuing a curative approach in multiple myeloma: A review of new therapeutic strategies. Cancers (Basel) (2019) 11:2015. doi: 10.3390/cancers11122015
4. Ludwig H, Zojer N. Fixed duration vs continuous therapy in multiple myeloma. Hematol Am Soc Hematol Educ Progr (2017) 2017:212–22. doi: 10.1182/asheducation-2017.1.212
5. Kumar SK, Rajkumar V, Kyle RA, van Duin M, Sonneveld P, Mateos M-V, et al. Multiple myeloma. Nat Rev Dis Prim (2017) 3:17046. doi: 10.1038/nrdp.2017.46
6. Rajkumar SV. Multiple myeloma: 2022 update on diagnosis, risk stratification, and management. Am J Hematol (2022) 97:1086–107. doi: 10.1002/ajh.26590
7. Kistler KD, Kalman J, Sahni G, Murphy B, Werther W, Rajangam K, et al. Incidence and risk of cardiac events in patients with previously treated multiple myeloma versus matched patients without multiple myeloma: An observational, retrospective, cohort study. Clin Lymphoma Myeloma Leuk (2017) 17:89–96.e3. doi: 10.1016/j.clml.2016.11.009
8. Issa ZA, Zantout MS, Azar ST. Multiple myeloma and diabetes. ISRN Endocrinol (2011) 2011:1–6. doi: 10.5402/2011/815013
9. Hungria VTM, Lee HC, Abonour R, Rifkin RM, Terpos E, Leleu X, et al. Real-world (RW) multiple myeloma (MM) patients (Pts) remain under-represented in clinical trials based on standard laboratory parameters and baseline characteristics: Analysis of over 3,000 pts from the insight MM global, prospective, observational study. Blood (2019) 134:1887. doi: 10.1182/blood-2019-125749
10. Nasr SH, Valeri AM, Sethi S, Fidler ME, Cornell LD, Gertz MA, et al. Clinicopathologic correlations in multiple myeloma: a case series of 190 patients with kidney biopsies. Am J Kidney Dis Off J Natl Kidney Found (2012) 59:786–94. doi: 10.1053/j.ajkd.2011.12.028
11. Blimark C, Holmberg E, Mellqvist U-H, Landgren O, Björkholm M, Hultcrantz M, et al. Multiple myeloma and infections: a population-based study on 9253 multiple myeloma patients. Haematologica (2015) 100:107–13. doi: 10.3324/haematol.2014.107714
12. Mikulski D, Robak P, Ryżewska W, Stańczak K, Kościelny K, Góra-Tybor J, et al. Risk factors of infection in Relapsed/Refractory multiple myeloma patients treated with lenalidomide and dexamethasone (Rd) regimen: Real-life results of a large single-center study. J Clin Med (2022) 11:5908. doi: 10.3390/jcm11195908
13. Encinas C, Hernandez-Rivas J-Á, Oriol A, Rosiñol L, Blanchard M-J, Bellón J-M, et al. A simple score to predict early severe infections in patients with newly diagnosed multiple myeloma. Blood Cancer J (2022) 12:68. doi: 10.1038/s41408-022-00652-2
14. Raje NS, Anaissie E, Kumar SK, Lonial S, Martin T, Gertz MA, et al. Consensus guidelines and recommendations for infection prevention in multiple myeloma: a report from the international myeloma working group. Lancet Haematol (2022) 9:e143–61. doi: 10.1016/S2352-3026(21)00283-0
15. Ludwig H, Kumar S. Prevention of infections including vaccination strategies in multiple myeloma. Am J Hematol (2023) 98 Suppl 2:S46–62. doi: 10.1002/ajh.26766
16. Teh BW, Teng JC, Urbancic K, Grigg A, Harrison SJ, Worth LJ, et al. Invasive fungal infections in patients with multiple myeloma: a multi-center study in the era of novel myeloma therapies. Haematologica (2015) 100:e28–31. doi: 10.3324/haematol.2014.114025
17. Wolfe RM, Beekmann SE, Polgreen PM, Winthrop KL, Peacock JEJ. Practice patterns of pneumocystis pneumonia prophylaxis in connective tissue diseases: A survey of infectious disease physicians. Open Forum Infect Dis (2019) 6:ofz315. doi: 10.1093/ofid/ofz315
18. Drayson MT, Bowcock S, Planche T, Iqbal G, Pratt G, Yong K, et al. Levofloxacin prophylaxis in patients with newly diagnosed myeloma (TEAMM): a multicentre, double-blind, placebo-controlled, randomised, phase 3 trial. Lancet Oncol (2019) 20:1760–72. doi: 10.1016/S1470-2045(19)30506-6
19. Althaqafi A, Ali M, Alzahrani Y, Ming LC, Hussain Z. How safe are fluoroquinolones for diabetic patients? a systematic review of dysglycemic and neuropathic effects of fluoroquinolones. Ther Clin Risk Manag (2021) 17:1083–90. doi: 10.2147/TCRM.S284171
20. Takahashi N, Miura M, Kameoka Y, Abumiya M, Sawada K. Drug interaction between lenalidomide and itraconazole. Am J Hematol (2012) 87:338–9. doi: 10.1002/ajh.22260
21. Azanza JR, Mensa J, Barberán J, Vázquez L, Pérez de Oteyza J, Kwon M, et al. Recommendations on the use of azole antifungals in hematology-oncology patients. Rev Esp Quimioter Publ Of La Soc Esp Quimioter (2023) 36:236–58. doi: 10.37201/req/013.2023
22. Ludwig H, Boccadoro M, Moreau P, San-Miguel J, Cavo M, Pawlyn C, et al. Recommendations for vaccination in multiple myeloma: a consensus of the european myeloma network. Leukemia (2021) 35:31–44. doi: 10.1038/s41375-020-01016-0
23. Dimopoulos MA, Sonneveld P, Leung N, Merlini G, Ludwig H, Kastritis E, et al. International myeloma working group recommendations for the diagnosis and management of myeloma-related renal impairment. J Clin Oncol Off J Am Soc Clin Oncol (2016) 34:1544–57. doi: 10.1200/JCO.2015.65.0044
24. Bridoux F, Leung N, Belmouaz M, Royal V, Ronco P, Nasr SH, et al. Management of acute kidney injury in symptomatic multiple myeloma. Kidney Int (2021) 99:570–80. doi: 10.1016/j.kint.2020.11.010
25. Dimopoulos MA, Roussou M, Gavriatopoulou M, Fotiou D, Ziogas DC, Migkou M, et al. Outcomes of newly diagnosed myeloma patients requiring dialysis: renal recovery, importance of rapid response and survival benefit. Blood Cancer J (2017) 7:e571. doi: 10.1038/bcj.2017.49
26. Tarragón B, Ye N, Gallagher M, Sen S, Portolés JM, Wang AY. Effect of high cut-off dialysis for acute kidney injury secondary to cast nephropathy in patients with multiple myeloma: a systematic review and meta-analysis. Clin Kidney J (2021) 14:1894–900. doi: 10.1093/ckj/sfaa220
27. Cook M, Hutchison C, Fifer L GJ. High cut-off haemodialysis (HCO-HD) does not improve outcomes in myeloma cast nephropathy: results of european trial of free light chain removal extended haemodialysis in cast nephropathy (EULITE). Haematologica (2016) p 101(s1):80. P270.
28. Bridoux F, Pegourie B, Augeul-Meunier K, Royer B, Joly B, Lamy T, et al. Treatment of myeloma cast nephropathy (MCN): A randomized trial comparing intensive haemodialysis (HD) with high cut-off (HCO) or standard high-flux dialyzer in patients receiving a bortezomib-based regimen (the MYRE study, by the intergroupe francophone. Blood (2016) 128:978. doi: 10.1182/blood.V128.22.978.978
29. Dimopoulos MA, Roussou M, Gkotzamanidou M, Nikitas N, Psimenou E, Mparmparoussi D, et al. The role of novel agents on the reversibility of renal impairment in newly diagnosed symptomatic patients with multiple myeloma. Leukemia (2013) 27:423–9. doi: 10.1038/leu.2012.182
30. Gupta N, Hanley MJ, Harvey RD, Badros A, Lipe B, Kukreti V, et al. A pharmacokinetics and safety phase 1/1b study of oral ixazomib in patients with multiple myeloma and severe renal impairment or end-stage renal disease requiring haemodialysis. Br J Haematol (2016) 174:748–59. doi: 10.1111/bjh.14125
31. Ailawadhi S, Lee HC, Omel J, Toomey K, Hardin JW, Gasparetto C, et al. Impact of lenalidomide-bortezomib-dexamethasone (RVd) induction on patients with newly diagnosed multiple myeloma and renal impairment: Results from the connect MM registry. J Clin Oncol (2020) 38:8518. doi: 10.1200/JCO.2020.38.15_suppl.8518
32. Bozic B, Rutner J, Zheng C, Ruckser R, Selimi F, Racz K, et al. Advances in the treatment of relapsed and refractory multiple myeloma in patients with renal insufficiency: Novel agents, immunotherapies and beyond. Cancers (Basel) (2021) 13:5036. doi: 10.3390/cancers13205036
33. Dykes K, Desale S, Javaid B, Miatlovich K, Kessler C. A new reality for multiple myeloma renal failure: US data report on kidney transplant outcomes. Clin Lymphoma Myeloma Leuk (2022) 22:e314–20. doi: 10.1016/j.clml.2021.11.002
34. Dispenzieri A, Kyle RA. Neurological aspects of multiple myeloma and related disorders. Best Pract Res Clin Haematol (2005) 18:673–88. doi: 10.1016/j.beha.2005.01.024
35. Richardson PG, Delforge M, Beksac M, Wen P, Jongen JL, Sezer O, et al. Management of treatment-emergent peripheral neuropathy in multiple myeloma. Leukemia (2012) 26:595–608. doi: 10.1038/leu.2011.346
36. Grammatico S, Cesini L, Petrucci MT. Managing treatment-related peripheral neuropathy in patients with multiple myeloma. Blood Lymphat Cancer (2016) 6:37–47. doi: 10.2147/BLCTT.S91251
37. Delforge M, Bladé J, Dimopoulos MA, Facon T, Kropff M, Ludwig H, et al. Treatment-related peripheral neuropathy in multiple myeloma: the challenge continues. Lancet Oncol (2010) 11:1086–95. doi: 10.1016/S1470-2045(10)70068-1
38. Mohty B, El-Cheikh J, Yakoub-Agha I, Moreau P, Harousseau J-L, Mohty M. Peripheral neuropathy and new treatments for multiple myeloma: background and practical recommendations. Haematologica (2010) 95:311–9. doi: 10.3324/haematol.2009.012674
39. Qureshi A, Tariq MJ, Shah Z, Abu Zar M, Aslam S, Rafae A, et al. Evidence-based supportive care in multiple myeloma. J Community Hosp Intern Med Perspect (2020) 10:313–7. doi: 10.1080/20009666.2020.1771124
40. Fokkema C, Moreau P, van der Holt B, Lambert J, Van Duin M, Wester R, et al. Treatment emergent peripheral neuropathy in the CASSIOPEIA trial. Haematologica (2022) 107:1726–30. doi: 10.3324/haematol.2021.280567
41. Moore DC, Ringley JT, Nix D, Muslimani A. Impact of body mass index on the incidence of bortezomib-induced peripheral neuropathy in patients with newly diagnosed multiple myeloma. Clin Lymphoma Myeloma Leuk (2020) 20:168–73. doi: 10.1016/j.clml.2019.08.012
42. Smith EML, Pang H, Cirrincione C, Fleishman S, Paskett ED, Ahles T, et al. Effect of duloxetine on pain, function, and quality of life among patients with chemotherapy-induced painful peripheral neuropathy: a randomized clinical trial. JAMA (2013) 309:1359–67. doi: 10.1001/jama.2013.2813
43. Farshchian N, Alavi A, Heydarheydari S, Moradian N. Comparative study of the effects of venlafaxine and duloxetine on chemotherapy-induced peripheral neuropathy. Cancer Chemother Pharmacol (2018) 82:787–93. doi: 10.1007/s00280-018-3664-y
44. Loprinzi CL, Lacchetti C, Bleeker J, Cavaletti G, Chauhan C, Hertz DL, et al. Prevention and management of chemotherapy-induced peripheral neuropathy in survivors of adult cancers: ASCO guideline update. J Clin Oncol Off J Am Soc Clin Oncol (2020) 38:3325–48. doi: 10.1200/JCO.20.01399
45. Palumbo A, Bringhen S, Ludwig H, Dimopoulos MA, Bladé J, Mateos MV, et al. Personalized therapy in multiple myeloma according to patient age and vulnerability: a report of the european myeloma network (EMN). Blood (2011) 118:4519–29. doi: 10.1182/blood-2011-06-358812
46. Kistler KD, Rajangam K, Faich G, Lanes S. Cardiac event rates in patients with newly diagnosed and relapsed multiple myeloma in US clinical practice. Blood (2012) 120:2916. doi: 10.1182/blood.V120.21.2916.2916
47. Bringhen S, Milan A, Ferri C, Wäsch R, Gay F, Larocca A, et al. Cardiovascular adverse events in modern myeloma therapy - incidence and risks. a review from the european myeloma network (EMN) and italian society of arterial hypertension (SIIA). Haematologica (2018) 103:1422–32. doi: 10.3324/haematol.2018.191288
48. Zamorano JL, Lancellotti P, Rodriguez Muñoz D, Aboyans V, Asteggiano R, Galderisi M, et al. 2016 ESC position paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC committee for practice guidelines: The task force for cancer treatments and cardiovascular toxicity of the european society of cardiology (ES. Eur J Heart Fail (2017) 19:9–42. doi: 10.1002/ejhf.654
49. Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, et al. 2016 European guidelines on cardiovascular disease prevention in clinical practice: The sixth joint task force of the european society of cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representat. Eur Heart J (2016) 37:2315–81. doi: 10.1093/eurheartj/ehw106
50. Curigliano G, Cardinale D, Suter T, Plataniotis G, de Azambuja E, Sandri MT, et al. Cardiovascular toxicity induced by chemotherapy, targeted agents and radiotherapy: ESMO clinical practice guidelines. Ann Oncol Off J Eur Soc Med Oncol (2012) 23(Suppl 7):vii155–66. doi: 10.1093/annonc/mds293
51. Bovelli D, Plataniotis G, Roila F. Cardiotoxicity of chemotherapeutic agents and radiotherapy-related heart disease: ESMO clinical practice guidelines. Ann Oncol Off J Eur Soc Med Oncol (2010) 21(Suppl 5):v277–82. doi: 10.1093/annonc/mdq200
52. Ludwig H, Delforge M, Facon T, Einsele H, Gay F, Moreau P, et al. Prevention and management of adverse events of novel agents in multiple myeloma: a consensus of the european myeloma network. Leukemia (2018) 32:1542–60. doi: 10.1038/s41375-018-0040-1
53. Bhatti S, Watts E, Syed F, Vallurupalli S, Pandey T, Jambekar K, et al. Clinical and prognostic utility of cardiovascular magnetic resonance imaging in myeloma patients with suspected cardiac amyloidosis. Eur Hear J - Cardiovasc Imaging (2016) 17:970–7. doi: 10.1093/ehjci/jew101
54. Chari A, Aggarwal SK, Mezzi K, Wang K, Kim C, Zhu S, et al. Cardiac events in real-world multiple myeloma patients treated with carfilzomib: A retrospective claims database analysis. Blood (2016) 128:3319. doi: 10.1182/blood.V128.22.3319.3319
55. El-Cheikh J, Moukalled N, Malard F, Bazarbachi A, Mohty M. Cardiac toxicities in multiple myeloma: an updated and a deeper look into the effect of different medications and novel therapies. Blood Cancer J (2023) 13:83. doi: 10.1038/s41408-023-00849-z
56. Baljevic M, Sborov DW, Lim MY, Hillengass J, Martin T, Castillo JJ, et al. Optimizing thromboembolism prophylaxis for the contemporary age of multiple myeloma. JNCCN J Natl Compr Cancer Netw (2022) 20:91–5. doi: 10.6004/jnccn.2021.7112
57. Sanfilippo KM, Luo S, Wang TF, Fiala M, Schoen M, Wildes TM, et al. Predicting venous thromboembolism in multiple myeloma: development and validation of the IMPEDE VTE score. Am J Hematol (2019) 94:1176–84. doi: 10.1002/ajh.25603
58. Lapietra G, Serrao A, Fazio F, Petrucci MT, Chistolini A. Venous thromboembolism prophylaxis in patients with multiple myeloma: where are we and where are we going? J Thromb Thrombolysis (2021) 52:584–9. doi: 10.1007/s11239-020-02354-7
59. Samuelson Bannow BT, Konkle BA. Laboratory biomarkers for venous thromboembolism risk in patients with hematologic malignancies: A review. Thromb Res (2018) 163:138–45. doi: 10.1016/j.thromres.2018.01.037
60. Comerford C, Glavey S, Quinn J, O’Sullivan JM. The role of VWF/FVIII in thrombosis and cancer progression in multiple myeloma and other hematological malignancies. J Thromb Haemost (2022) 20:1766–77. doi: 10.1111/jth.15773
61. Lyman GH, Carrier M, Ay C, Di NM, Hicks LK, Khorana AA, et al. American society of hematology 2021 guidelines for management of venous thromboembolism: Prevention and treatment in patients with cancer. Blood Adv (2021) 5:927–74. doi: 10.1182/bloodadvances.2020003442
62. Streiff MB, Abutalib SA, Farge D, Murphy M, Connors JM, Piazza G. Update on guidelines for the management of cancer-associated thrombosis. Oncologist (2021) 26:e24–40. doi: 10.1002/onco.13596
63. Palumbo A, Rajkumar SV, Dimopoulos MA, Richardson PG, San Miguel J, Barlogie B, et al. Prevention of thalidomide- and lenalidomide-associated thrombosis in myeloma. Leukemia (2008) 22:414–23. doi: 10.1038/sj.leu.2405062
64. LeBlanc R, Bergstrom DJ, Côté J, Kotb R, Louzada ML, Sutherland HJ. Management of myeloma manifestations and complications: The cornerstone of supportive care: Recommendation of the canadian myeloma research group (formerly myeloma canada research network) consensus guideline consortium. Clin Lymphoma Myeloma Leuk (2022) 22:e41–56. doi: 10.1016/j.clml.2021.07.028
65. Fotiou D, Gavriatopoulou M, Terpos E. Multiple myeloma and thrombosis: Prophylaxis and risk prediction tools. Cancers (Basel) (2020) 12:191. doi: 10.3390/cancers12010191
66. Cornell RF, Goldhaber SZ, Engelhardt BG, Moslehi J, Jagasia M, Patton D, et al. Apixaban for primary prevention of venous thromboembolism in patients with multiple myeloma receiving immunomodulatory therapy. Front Oncol (2019) 9:45. doi: 10.3389/fonc.2019.00045
67. Piedra KM, Hassoun H, Buie LW, Devlin SM, Flynn J, Hultcrantz M, et al. VTE rates and safety analysis of newly diagnosed multiple myeloma patients receiving carfilzomib-Lenalidomide-Dexamethasone (KRD) with or without rivaroxaban prophylaxis. Blood (2019) 134:1835–5. doi: 10.1182/blood-2019-124403
68. Snowden JA, Ahmedzai SH, Ashcroft J, D’Sa S, Littlewood T, Low E, et al. Guidelines for supportive care in multiple myeloma 2011. Br J Haematol (2011) 154:76–103. doi: 10.1111/j.1365-2141.2011.08574.x
69. Eby C. Pathogenesis and management of bleeding and thrombosis in plasma cell dyscrasias. Br J Haematol (2009) 145:151–63. doi: 10.1111/j.1365-2141.2008.07577.x
70. Li A, Warnick G, Libby E, Garcia D, Lyman G. No bleeding risk assessment model for older multiple myeloma patients on immunomodulatory drugs (IMIDs). Res Pr Thromb Haemost (2020) 4(Suppl 1).
71. Terpos E, Zamagni E, Lentzsch S, Drake MT, García-Sanz R, Abildgaard N, et al. Treatment of multiple myeloma-related bone disease: recommendations from the bone working group of the international myeloma working group. Lancet Oncol (2021) 22:e119–30. doi: 10.1016/S1470-2045(20)30559-3
72. Mirrakhimov AE. Hypercalcemia of malignancy: An update on pathogenesis and management. N Am J Med Sci (2015) 7:483–93. doi: 10.4103/1947-2714.170600
73. Ninan PJ, Sivaramakrishnan R, Sm B. Pain relief associated with radiotherapy for symptomatic vertebral lesions in multiple myeloma- a retrospective analysis. Galore Int J Heal Sci Res (2020) 5:601. doi: 10.3389/fonc.2019.00601
74. Kyriakou C, Molloy S, Vrionis F, Alberico R, Bastian L, Zonder JA, et al. The role of cement augmentation with percutaneous vertebroplasty and balloon kyphoplasty for the treatment of vertebral compression fractures in multiple myeloma: a consensus statement from the international myeloma working group (IMWG). Blood Cancer J (2019) 9:27. doi: 10.1038/s41408-019-0187-7
75. Niscola P, Scaramucci L, Romani C, Giovannini M, Maurillo L, del Poeta G, et al. Opioids in pain management of blood-related malignancies. Ann Hematol (2006) 85:489–501. doi: 10.1007/s00277-005-0062-4
76. Davies MP, Fingas S, Chantry A. Mechanisms and treatment of bone pain in multiple myeloma. Curr Opin Support Palliat Care (2019) 13:408–16. doi: 10.1097/SPC.0000000000000467
77. Aberer F, Hochfellner DA, Sourij H, Mader JK. A practical guide for the management of steroid induced hyperglycaemia in the hospital. J Clin Med (2021) 10:2154. doi: 10.3390/jcm10102154
78. Walsh J, Gittoes N, Selby P. Emergency management of acute hypercalcaemia in adult patients. Endocr Connect (2016) 5:G9–11. doi: 10.1530/EC-16-0055
79. Terpos E, Ntanasis-Stathopoulos I. Controversies in the use of new bone-modifying therapies in multiple myeloma. Br J Haematol (2021) 193:1034–43. doi: 10.1111/bjh.17256
80. Major P, Lortholary A, Hon J, Abdi E, Mills G, Menssen HD, et al. Zoledronic acid is superior to pamidronate in the treatment of hypercalcemia of malignancy: a pooled analysis of two randomized, controlled clinical trials. J Clin Oncol Off J Am Soc Clin Oncol (2001) 19:558–67. doi: 10.1200/JCO.2001.19.2.558
81. Terpos E, Kleber M, Engelhardt M, Zweegman S, Gay F, Kastritis E, et al. European myeloma network guidelines for the management of multiple myeloma-related complications. Haematologica (2015) 100:1254–66. doi: 10.3324/haematol.2014.117176
82. Terpos E, Sezer O, Croucher PI, García-Sanz R, Boccadoro M, San Miguel J, et al. The use of bisphosphonates in multiple myeloma: Recommendations of an expert panel on behalf of the european myeloma network. Ann Oncol (2009) 20:1303–17. doi: 10.1093/annonc/mdn796
83. Raje N, Terpos E, Willenbacher W, Shimizu K, García-Sanz R, Durie B, et al. Denosumab versus zoledronic acid in bone disease treatment of newly diagnosed multiple myeloma: an international, double-blind, double-dummy, randomised, controlled, phase 3 study. Lancet Oncol (2018) 19:370–81. doi: 10.1016/S1470-2045(18)30072-X
84. Goldner W. Cancer-related hypercalcemia. J Oncol Pract (2016) 12:426–32. doi: 10.1200/JOP.2016.011155
85. Cicci JD, Buie L, Bates J, Van Deventer H. Denosumab for the management of hypercalcemia of malignancy in patients with multiple myeloma and renal dysfunction. Clin Lymphoma Myeloma Leuk (2014) 14:e207–11. doi: 10.1016/j.clml.2014.07.005
86. Cairo MS, Coiffier B, Reiter A, Younes A. Recommendations for the evaluation of risk and prophylaxis of tumour lysis syndrome (TLS) in adults and children with malignant diseases: An expert TLS panel consensus. Br J Haematol (2010) 149:578–86. doi: 10.1111/j.1365-2141.2010.08143.x
87. Howard SC, Trifilio S, Gregory TK, Baxter N, McBride A. Tumor lysis syndrome in the era of novel and targeted agents in patients with hematologic malignancies: a systematic review. Ann Hematol (2016) 95:563–73. doi: 10.1007/s00277-015-2585-7
88. Trudel S, McCurdy A, Fu M, Sutherland HJ, Louzada ML, Chu MP, et al. Belantamab mafodotin in combination with pomalidomide and dexamethasone demonstrates durable responses in triple class Exposed/Refractory multiple myeloma. Blood (2022) 140:7306–7. doi: 10.1182/blood-2022-160445
89. Zhang Q, Zu C, Jing R, Feng Y, Zhang Y, Zhang M, et al. Incidence, clinical characteristics and prognosis of tumor lysis syndrome following b-cell maturation antigen-targeted chimeric antigen receptor-t cell therapy in relapsed/refractory multiple myeloma. Front Immunol (2023) 14:1125357. doi: 10.3389/fimmu.2023.1125357
90. Dubovsky AN, Arvikar S, Stern TA, Axelrod L. The neuropsychiatric complications of glucocorticoid use: Steroid psychosis revisited. Psychosomatics (2012) 53:103–15. doi: 10.1016/j.psym.2011.12.007
91. Jasani R, Deacon JW, Sertich A. Corticosteroid-induced mania after previous tolerance of higher doses. Cureus (2021) 13:e17719. doi: 10.7759/cureus.17719
92. Mehta J, Singhal S. Hyperviscosity syndrome in plasma cell dyscrasias. Semin Thromb Hemost (2003) 29:467–71. doi: 10.1055/s-2003-44554
93. Jurczyszyn A, Grzasko N, Gozzetti A, Czepiel J, Cerase A, Hungria V, et al. Central nervous system involvement by multiple myeloma: A multi-institutional retrospective study of 172 patients in daily clinical practice. Am J Hematol (2016) 91:575–80. doi: 10.1002/ajh.24351
94. Chin KJ, Kempin S, Milman T, Finger PT. Ocular manifestations of multiple myeloma: Three cases and a review of the literature. Optometry (2011) 82:224–30. doi: 10.1016/j.optm.2010.10.009
95. Wang F, Sansbury L, Ferrante S, Maiese EM, Willson J, Chen CC, et al. Incidence of corneal adverse events in patients with multiple myeloma and their clinical and economic impact: A real-world retrospective cohort study. J Med Econ (2022) 25:182–92. doi: 10.1080/13696998.2022.2029088
96. Phulke S, Kaushik S, Kaur S, Pandav SS. Steroid-induced glaucoma: An avoidable irreversible blindness. J Curr Glaucoma Pract (2017) 11:67–72. doi: 10.5005/jp-journals-10028-1226
97. James ER. The etiology of steroid cataract. J Ocul Pharmacol Ther (2007) 23:403–20. doi: 10.1089/jop.2006.0067
98. Lu R, Morphey A, Diaz F, Chen J, Razmandi A, Richards T. Management of ocular toxicity in patients receiving belantamab mafodotin. J Adv Pract Oncol (2023) 14:300–6. doi: 10.6004/jadpro.2023.14.4.4
99. Nardone B, Wu S, Garden BC, West DP, Reich LM, Lacouture ME. Risk of rash associated with lenalidomide in cancer patients: A systematic review of the literature and meta-analysis. Clin Lymphoma Myeloma Leuk (2013) 13:424–9. doi: 10.1016/j.clml.2013.03.006
100. Delforge M, Ludwig H. How i manage the toxicities of myeloma drugs. Blood (2017) 129:2359–67. doi: 10.1182/blood-2017-01-725705
101. Sviggum HP, Davis MDP, Rajkumar SV, Dispenzieri A. Dermatologic adverse effects of lenalidomide therapy for amyloidosis and multiple myeloma. Arch Dermatol (2006) 142:1298–302. doi: 10.1001/archderm.142.10.1298
102. Miceli TS, Gonsalves WI BF. Supportive care in multiple myeloma: Current practices and advances. Cancer Treat Res Commun (2021) 29:100476. doi: 10.1016/j.ctarc.2021.100476
103. Ramsenthaler C, Kane P, Gao W, Siegert RJ, Edmonds PM, Schey SA, et al. Prevalence of symptoms in patients with multiple myeloma: a systematic review and meta-analysis. Eur J Haematol (2016) 97:416–29. doi: 10.1111/ejh.12790
104. He J, Duenas A, Collacott H, Lam A, Gries KS, Carson R, et al. Patient perceptions regarding multiple myeloma and its treatment: Qualitative evidence from interviews with patients in the united kingdom, france, and germany. Patient (2021) 14:613–23. doi: 10.1007/s40271-021-00501-7
105. Smith LC, Bertolotti P, Curran K, Jenkins B. Gastrointestinal side effects associated with novel therapies in patients with multiple myeloma: consensus statement of the IMF nurse leadership board. Clin J Oncol Nurs (2008) 12:37–52. doi: 10.1188/08.CJON.S1.37-51
106. Stansborough RL, Gibson RJ. Proteasome inhibitor-induced gastrointestinal toxicity. Curr Opin Support Palliat Care (2017) 11:133–7. doi: 10.1097/SPC.0000000000000266
107. Hall KH. Management of gastrointestinal toxicities from ixazomib: Tips to curb nausea, vomiting, diarrhea, and constipation. Oncol (Williston Park) (2019) 33:89–90.
108. Faiman B, Sidana S, Elson P, Bruening K, Duong HK, Dean RM, et al. Lenalidomide related diarrhea correlates with survival in multiple myeloma. Blood (2013) 122:5397. doi: 10.1182/blood.V122.21.5397.5397
109. Pawlyn C, Khan MS, Muls A, Sriskandarajah P, Kaiser MF, Davies FE, et al. Lenalidomide-induced diarrhea in patients with myeloma is caused by bile acid malabsorption that responds to treatment. Blood (2014) 124:2467–8. doi: 10.1182/blood-2014-06-583302
110. Vaxman I, Al Saleh AS, Kumar S, Nitin M, Dispenzieri A, Buadi F, et al. Colon perforation in multiple myeloma patients - a complication of high-dose steroid treatment. Cancer Med (2020) 9:8895–901. doi: 10.1002/cam4.3507
111. Narum S, Westergren T, Klemp M. Corticosteroids and risk of gastrointestinal bleeding: a systematic review and meta-analysis. BMJ Open (2014) 4:e004587. doi: 10.1136/bmjopen-2013-004587
112. Arasaradnam RP, Brown S, Forbes A, Fox MR, Hungin P, Kelman L, et al. Guidelines for the investigation of chronic diarrhoea in adults: British society of gastroenterology, 3rd edition. Gut (2018) 67:1380–99. doi: 10.1136/gutjnl-2017-315909
113. Musto P, Anderson KC, Attal M, Richardson PG, Badros A, Hou J, et al. Second primary malignancies in multiple myeloma: an overview and IMWG consensus. Ann Oncol Off J Eur Soc Med Oncol (2018) 29:1074. doi: 10.1093/annonc/mdx160
114. Thomas A, Mailankody S, Korde N, Kristinsson SY, Turesson I, Landgren O. Second malignancies after multiple myeloma: from 1960s to 2010s. Blood (2012) 119:2731–7. doi: 10.1182/blood-2011-12-381426
115. European Medicines Agency. Summary of product characteristics - revlimid (n.d). Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/revlimid (Accessed July 31, 2023).
116. Magen H, Simchen MJ, Erman S, Avigdor A. Diagnosis and management of multiple myeloma during pregnancy: case report, review of the literature, and an update on current treatments. Ther Adv Hematol. (2022) 13:20406207211066172. doi: 10.1177/20406207211066173
117. FDA Pregnancy Categories. (n.d). Available at: https://www.drugs.com/pregnancy/ (Accessed July 31, 2023).
118. Dexamethasone Pregnancy and Breastfeeding Warnings. (n.d). Available at: https://www.drugs.com/pregnancy/dexamethasone.html (Accessed July 31, 2023).
119. Jurczyszyn A, Olszewska-Szopa M, Vesole AS, Vesole DH, Siegel DS, Richardson PG, et al. Multiple myeloma in pregnancy–a review of the literature and a case series. Clin Lymphoma Myeloma Leuk. (2016) 16:e39–45. doi: 10.1016/j.clml.2015.11.020
120. Gertz MA. Is there still a role for stem cell transplantation in multiple myeloma? Hematol Oncol Clin North Am (2023) 38:407–20. doi: 10.1016/j.hoc.2023.12.005
121. Harousseau J-L, Moreau P. Autologous hematopoietic stem-cell transplantation for multiple myeloma. N Engl J Med (2009) 360:2645–54. doi: 10.1056/NEJMct0805626
122. Arora S, Majhail NS, Liu H. Hematopoietic progenitor cell mobilization for autologous stem cell transplantation in multiple myeloma in contemporary era. Clin Lymphoma Myeloma Leuk (2019) 19:200–5. doi: 10.1016/j.clml.2018.12.010
123. Christopeit M, Schmidt-Hieber M, Sprute R, Buchheidt D, Hentrich M, Karthaus M, et al. Prophylaxis, diagnosis and therapy of infections in patients undergoing high-dose chemotherapy and autologous haematopoietic stem cell transplantation. 2020 update of the recommendations of the infectious diseases working party (AGIHO) of the german society of hematology and medical oncology (DGHO). Ann Hematol (2021) 100:321–36. doi: 10.1007/s00277-020-04297-8
124. Marchesi F, Tendas A, Giannarelli D, Viggiani C, Gumenyuk S, Renzi D, et al. Cryotherapy reduces oral mucositis and febrile episodes in myeloma patients treated with high-dose melphalan and autologous stem cell transplant: a prospective, randomized study. Bone Marrow Transplant (2017) 52:154–6. doi: 10.1038/bmt.2016.207
125. Tendas A, Marchesi F, Mengarelli A, Annibali O, Tomarchio V, Saltarelli D, et al. Prevention of chemotherapy-induced nausea and vomiting after high-dose melphalan and stem cell transplantation: review of the evidence and suggestions. Support Care Cancer Off J Multinatl Assoc Support Care Cancer (2019) 27:793–803. doi: 10.1007/s00520-018-4594-2
126. Jahan D, Peile E, Sheikh MA, Islam S, Parasnath S, Sharma P, et al. Is it time to reconsider prophylactic antimicrobial use for hematopoietic stem cell transplantation? a narrative review of antimicrobials in stem cell transplantation. Expert Rev Anti Infect Ther (2021) 19:1259–80. doi: 10.1080/14787210.2021.1902304
127. Barlogie B, Tricot G, Haessler J, van Rhee F, Cottler-Fox M, Anaissie E, et al. Cytogenetically defined myelodysplasia after melphalan-based autotransplantation for multiple myeloma linked to poor hematopoietic stem-cell mobilization: the arkansas experience in more than 3,000 patients treated since 1989. Blood (2008) 111:94–100. doi: 10.1182/blood-2007-06-097444
128. Firestone RS, Mailankody S. Current use of CAR t cells to treat multiple myeloma. Hematol Am Soc Hematol Educ Progr (2023) 2023:340–7. doi: 10.1182/hematology.2023000434
129. Cipkar C, Chen C, Trudel S. Antibodies and bispecifics for multiple myeloma: effective effector therapy. Hematol Am Soc Hematol Educ Progr (2022) 2022:163–72. doi: 10.1182/hematology.2022000334
130. Rejeski K, Subklewe M, Locke FL. Recognizing, defining, and managing CAR-t hematologic toxicities. Hematol Am Soc Hematol Educ Progr (2023) 2023:198–208. doi: 10.1182/hematology.2023000472
131. Liang EC, Sidana S. Managing side effects: guidance for use of immunotherapies in multiple myeloma. Hematol Am Soc Hematol Educ Progr (2023) 2023:348–56. doi: 10.1182/hematology.2023000435
132. Hayden PJ, Roddie C, Bader P, Basak GW, Bonig H, Bonini C, et al. Management of adults and children receiving CAR t-cell therapy: 2021 best practice recommendations of the european society for blood and marrow transplantation (EBMT) and the joint accreditation committee of ISCT and EBMT (JACIE) and the european haematology association (EHA). Ann Oncol Off J Eur Soc Med Oncol (2022) 33:259–75. doi: 10.1016/j.annonc.2021.12.003
133. Khanam R, Faiman B, Batool S, Najmuddin MM, Usman R, Kuriakose K, et al. Management of adverse reactions for BCMA-directed therapy in relapsed multiple myeloma: A focused review. J Clin Med (2023) 12:5539. doi: 10.3390/jcm12175539
134. Kampouri E, Little JS, Rejeski K, Manuel O, Hammond SP, Hill JA. Infections after chimeric antigen receptor (CAR)-t-cell therapy for hematologic malignancies. Transpl Infect Dis an Off J Transplant Soc (2023) 25(Suppl 1):e14157. doi: 10.1111/tid.14157
Keywords: delivery of health care, cancer management, anticancer drug toxicities, multiple myeloma, real life practical considerations, myeloma-related manifestations
Citation: Geraldes C, Roque A, Sarmento-Ribeiro AB, Neves M, Ionita A, Gerivaz R, Tomé A, Afonso S, Silveira MP, Sousa P, Bergantim R and João C (2024) Practical management of disease-related manifestations and drug toxicities in patients with multiple myeloma. Front. Oncol. 14:1282300. doi: 10.3389/fonc.2024.1282300
Received: 23 August 2023; Accepted: 07 February 2024;
Published: 22 March 2024.
Edited by:
Carlo Finelli, Sant’Orsola-Malpighi Polyclinic, ItalyReviewed by:
Hussain Alizadeh, University of Pécs, HungaryJakub Krejcik, Odense University Hospital, Denmark
Copyright © 2024 Geraldes, Roque, Sarmento-Ribeiro, Neves, Ionita, Gerivaz, Tomé, Afonso, Silveira, Sousa, Bergantim and João. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Catarina Geraldes, 7495@chuc.min-saude.pt