 Aliénor Vienne-Jumeau
Aliénor Vienne-Jumeau Dominique Brémond-Gignac
Dominique Brémond-Gignac Matthieu P. Robert
Matthieu P. Robert- 1Department of Ophthalmology, Necker-Enfants Malades University Hospital, Assistance Publique - Hôpitaux de Paris (AP-HP), Paris, France
- 2Institut national de la santé et de la recherche médicale (INSERM), UMRS1138, Team 17, From Physiopathology of Ocular Diseases to Clinical Development, Sorbonne Paris Cité University, Centre de Recherche des Cordeliers, Paris, France
Background: Around one in forty patients are diagnosed with optic disc drusen (ODD) during their lifetime. Complications of these acellular deposits range from asymptomatic visual field deficits to artery occlusion and subsequent cecity. Still, the pathogenesis of their emergence remains controversial. In particular, it was suggested 50 years ago that a narrow disc and scleral canal is one factor leading to axoplasmic flow disturbance, which induces ODD formation. However, this hypothesis is still debated today. To evaluate the basis of this theory, we will conduct a systematic review and meta-analysis of studies evaluating the scleral canal size in patients with ODD and in healthy subjects.
Methods: We will search MEDLINE via PubMed, Cochrane, and EMBASE electronic databases to identify articles published before November 29, 2022 that measure the scleral canal size in patients with ODD and in healthy subjects. In addition, grey literature will be searched. The meta-analysis will include studies that include patients with a clinical or imaging diagnosis of ODD and healthy subjects. Additionally, we will perform a subgroup analysis to compare patients with buried ODD and patients with visible ODD. Extracted data from included studies will be presented descriptively, and effect sizes will be computed based on the recommendations from the Cochrane Collaboration handbook.
Discussion: The hypothesis that a narrow scleral canal is a risk factor of ODD has long been debated and this systematic review and meta-analysis should disentangle the different views. Understanding the underlying factors driving the development of ODD should help us focus on patients at risk and develop strategies to prevent advanced stages of the disease in these patients. Besides, focusing on patients with small scleral canals should help us derive associated factors and provide a better understanding of the pathology.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022375110.
1 Introduction
Optic disc drusen (ODD) are acellular deposits that are thought to result from axonal disintegration following axoplasmic flow disruption in the optic nerve head (1). The reported prevalence in adults varies from 0.2% (2) to around 2.0% (3, 4). Only 0.4% of children are thought to be affected. The diagnosis is often made incidentally in children with pseudo-papilloedema (5, 6) or in adults with visible drusen overlying the border of the disc. However, more than half of the patients have visual fields deficits (blind spot enlargement, field constriction) due to retinal nerve fiber layer atrophy (7) and a small number of patients with large ODD will develop dramatic complications, such as choroidal neovascularization, central artery occlusion or anterior ischemic neuropathy (8–12). Understanding underlying risk factors could allow clinicians to screen patients at risk and undertake a more specific follow-up to evaluate the evolution of the ODD and their consequences.
It has long been proposed that ODD are more likely to emerge in patients with a narrow scleral canal, as the latter is the location of increased axonal mechanical constraints. Several studies have been undertaken to test this hypothesis, but with diverging results (13–15). However, several factors – including the location of the ODD, the age of the patients, the instrument for measurement – are likely to influence the outcome. Therefore, the association between the presence of ODD and the size of the disc and scleral canal would be worth exploring in a systematic way.
The anterior opening of the optic nerve scleral canal is, by definition, the anatomic entrance to the scleral canal at the level of the sclera. It is mostly evaluated using either fundus pictures, where it corresponds to the limits of the disc, or optical coherence tomography (OCT). In most studies, measurements at the level of the Bruch’s membrane opening (BMO) are considered as proxies of the measurements at the level of the anterior opening of the optic nerve scleral canal (16, 17). Indeed, the BMO is well defined on OCT (14, 15, 18, 19) and seems to remain stable over time and conditions (17, 20). The high-resolution enhanced depth imaging spectral-domain OCT (EDI SD-OCT) and swept source OCT (SS-OCT), in particular, provide a greater penetration and a better characterization of deep structures, with less artefacts induced by the drusen themselves (21). EDI-SD-OCT with scan averaging is the ODD diagnostic modality recommended by the Optic Disc Drusen Studies Consortium (22). It has proven equivalent to SS-OCT in that regard (21).
This systematic review and meta-analysis will thus aim at evaluating the mean difference of the scleral canal size at the level of the BMO between patients with ODD and healthy controls, with a secondary focus on patients with buried ODD versus patients with visible ODD.
Two main objectives will be evaluated:
● Mean difference of the scleral canal size at the level of the BMO using fundus pictures between patients with ODD and healthy controls.
● Mean difference of the scleral canal size at the level of the BMO using OCT (SD-EDI or SS) between patients with ODD and healthy controls.
Because we expect that patients with buried ODD and patients with visible ODD might differ, we will also undergo a subgroup analysis and compute the following outcomes:
● Mean difference of the scleral canal size at the level of the BMO using fundus pictures between patients with buried ODD and patients with visible ODD.
● Mean difference of the scleral canal size at the level of the BMO using OCT (SD-EDI or SS) between patients with buried ODD and patients with visible ODD.
2 Methods/design
The literature search and analysis will follow the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (23) (see Supplementary File 1) and Meta-analysis of Observational Studies in Epidemiology (MOOSE) (24) guidelines.
2.1 Search strategy
We will search MEDLINE via PubMed, Cochrane, and EMBASE electronic databases to identify articles published before November 29, 2022 that measure the mean difference of the scleral canal size at the level of the BMO between patients with ODD and healthy controls or between patients with buried ODD and patients with visible ODD. In addition, grey literature will be searched in Google Scholar, Greylit.org, World Health Organization Clinical Trials Search Portal, ClinicalTrials.gov and the European Union Clinical Trials Register. All reference lists and bibliographies of included studies will be reviewed for potentially relevant studies that could be missed by this literature search.
The search will involve the following MeSH keywords: optic AND (disk OR disc OR nerve) AND drusen AND (canal OR area OR size OR measure OR crowded OR small).
2.2 Inclusion criteria
Randomized controlled and non-randomized controlled trials, as well as observational studies will be eligible for inclusion. Inclusion criteria will be patients with a clinical or imaging (autofluorescence, B-scan ultrasound, OCT, CT scan) diagnosis of ODD.
2.3 Exclusion criteria
Articles with previously published data (review, meta-analysis, follow-up study) and case reports will be excluded. We will exclude articles of studies that do not include people with ODD, that do not quantify the size of the scleral canal, that do not have a control group (either HS for patients with ODD or visible ODD for patients with buried ODD) or that include only syndromic ODD (ODD associated to a known predisposing syndrome, such as Pseudoxanthoma Elasticum, Retinitis Pigmentosa, Usher syndrome, Down Syndrome, Alagille Syndrome, Noonan syndrome).
We will exclude from the meta-analysis (but include in the systematic review and the sensitivity analysis) studies relying on time-domain OCT (TD-OCT) or non-EDI SD OCT for performing the measurements of the scleral canal size at the level of the BMO. Likewise, for the second main objective and subgroup analysis (measurements based on OCT), only the studies relying on gold standards state-of-the-art OCT (EDI SD OCT or SS OCT) to exclude ODD and define normal optic nerve according to the Copenhagen Consortium (15) will be included. Articles that do not provide appropriate data for pooling the outcomes despite authors being contacted for missing material will also be excluded. Data (reported or obtained from one of the authors) will be considered sufficient in one of the three following situations: sample sizes, means and standard deviations for both groups considered; sample sizes, medians and all four quartiles for both groups considered; raw values for every patient for both groups considered.
2.4 Review process
Figure 1 is a PRISMA flow chart of the review process. Potentially eligible studies will be screened for eligibility by AVJ. We will import articles to Zotero, and all articles will be reviewed (title, abstract and main text when needed) to discard those that do not meet the criteria. Data of included papers will then be extracted and the studies will be assessed for risk of bias.
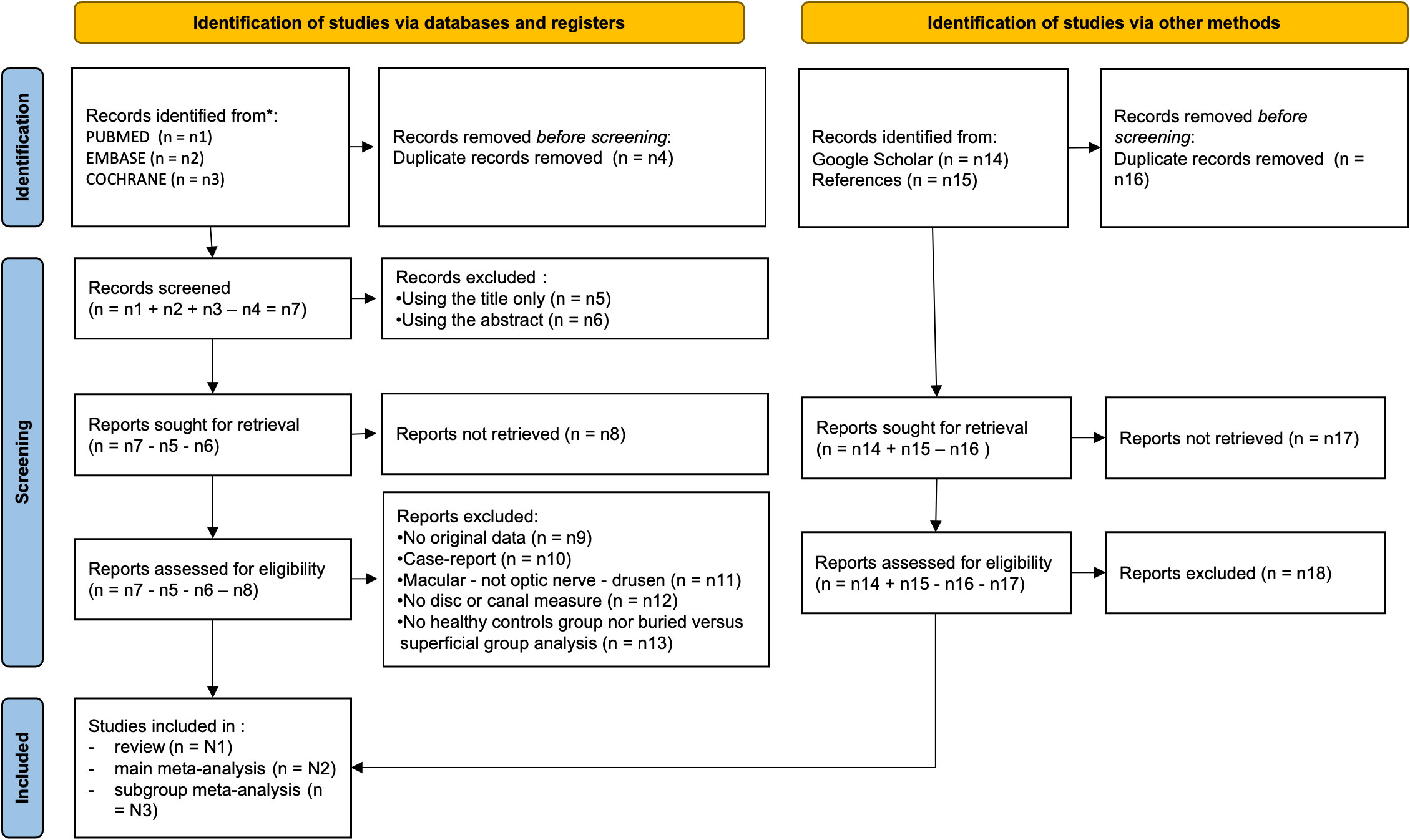
Figure 1 PRISMA flow chart of the review process.
2.5 Risk of bias appraisal
We will assess the quality of included studies through a domain-based quality assessment grid adapted from the National Institutes of Health quality assessment tool of case-control studies (25, 26). The assessment will be performed independently by two review authors (AVJ and MR), each blinded to the score given by the other. They will later discuss discrepancies until they reach consensus. If no consensus is reached, a third author (DBG) will arbitrate. Publication risk of bias will be characterized using Egger’s statistical test and visual inspection of the funnel plot, which represents the estimated effect size (horizontal axis) versus its standard error mean (vertical axis). Asymmetry of the inverted funnel shape favors publication bias.
2.6 Data extraction and analysis
2.6.1 Study review
Upon selecting articles for inclusion, all references will be imported in Microsoft® Excel (version 16.65) for data extraction. One assessor (AVJ) will extract and collate information. Another assessor (MR) will verify the extracted material from all included articles. The following data will be extracted (see Supplementary File 2):
- Study characteristics: authors, title, year of publication, inclusion and exclusion criteria, sample size;
- Population characteristics: percentage of buried versus visible drusen, age, spheric equivalent
- Outcome measure characteristics: type of the parameter, means and standard deviations (or median and interquartile range (IQR)), OCT type if appropriate, magnification correction formula if applied
- Statistical analysis: test for normality, test used, whether correction for multiple comparison was applied, confounding factors, parameter significance.
The data extraction tables will be pilot-tested and refined before extraction.
The means and standard deviations will be extracted when available. If the results are reported using medians and IQR, we will search the protocol – if available – and methods to determine whether the data was shewed or whether it was a preference of the authors and there had been no test of normality although the sample size was large enough to expect a Gaussian distribution. In case the choice is not explained and the sample size is above 50, we will suppose a normal distribution and apply the following transformation formulæ: and . In any other case, we will use the formulæ by Luo et al. (27) and Shi et al. (28):
where
and
where , and is the upper zth percentile of the standard normal distribution, and a is the minimum value, q1 the first quartile, q3 the third quartile and b the maximum value.
If neither one of those data is available, the raw data will be sought and retrieved. If none of this material is available, it will be requested from the corresponding author (he will be contacted up to three times via e-mail). If this latter cannot provide the information, the study will be excluded from the meta-analysis.
When data are not available in the main text, we will search Supplemental Materials for more detailed information. If data are only available by graphical representation, the assessors (AVJ and MR) will use Plot Digitizer to extract data from graphs: the final value will be the mean of these two extractions.
2.6.2 Strategy for data synthesis
Extracted data from included articles will be presented descriptively, and effect sizes will be computed based on the recommendations from the Cochrane Collaboration handbook. and Cochrane Review Manager v5.3.
Our preliminary search suggests that the mean diameter and the total area of the optic disc are two common parameters used to describe the optic disc size. Because the calculation of the mean diameter is more straightforward, we will report the mean diameter only. In cases where the mean diameter is not reported, we will transform the reported measure using the following formulas, which suppose that the optic disc can be approximated by a disc (29):
- The reported measure is the maximal and minimal diameters:
- The reported measure is the horizontal diameter:
- The reported measure is the total area: .
Extracted data will then be pooled to derive Hedge’s standardized mean difference. We will apply a fixed-effects model when the I2, the percentage of variation across studies due to heterogeneity rather than chance, was low to moderate (I2< 50%) (30, 31); otherwise, we will perform a random-effects model. The 95% confidence interval excluding the null value will be considered significant. The between-study variance, τ2, will be estimated using the Restricted Maximum-Likelihood formula (30).
We will use R v4.0.3 with the ‘Metafor’ package for the statistical analysis and the plots.
2.6.3 Sensitivity analysis
Two sensitivity analysis will be performed.
First, we will explore the impact of the hypothesis that the disc can be approximated by a disc. To that end, we will analyse only studies that computed the mean diameter.
Second, we will explore the impact of choosing only studies with recent state-of-the-art OCT modalities. To do so, we will add studies using TD-OCT and non-EDI SD OCT to the analysis.
In both cases, reporting will be done in a summary table.
The overall quality of the evidence for each outcome will be evaluated by using the GRADE criteria following the Cochrane Collaboration recommendations if enough RCTs and interventional studies are included (32).
3 Discussion
Identifying the factors responsible for the emergence of ODD may help develop a better screening protocol and prevent dramatic complications through earlier diagnosis and care. We are not aware of any means to enlarge the scleral canal: therefore, it would not be a modifiable risk factor. Neither are we able to predict the impact of widening the scleral canal. However, should this study support the association between a narrow scleral canal and the presence of ODD, it would allow defining a better population for studies evaluating the impact of modifying other potential risk factors or introducing preventive treatments. In that regard, the potential interest of lowering the intra-ocular pressure is still pondered (33) and neuroprotective treatments are being developed, which might also prove useful to halt the progressive atrophy in patients with ODD (34–36).
Several observations support the hypothesis that a narrow scleral canal plays a central role in the formation of ODD. Genetic factors have been incriminated, which follow an irregular autosomal dominant pattern, and small optic discs have been observed in affected families (1). ODD are mainly found in caucasians, who have a smaller optic disc compared to African and Asian people (37, 38). ODD are more frequent in rod-cone dystrophies, and in particular in Usher syndrome, where scleral canals have been found smaller than in other dystrophies (39). In healthy subjects, the optic disc size correlates to the axial length (40). It is therefore interesting to note that the prevalence of ODD in nanophtalmos and posterior microphthalmos is higher than in the general population (41–43). In nanophtalmos, the presence of ODD correlates to the axial length (41). Pseudoxanthoma elasticum is another disease associated to the presence of ODD (44). If, to our knowledge, no direct link has been unveiled with the scleral canal size, it is remarkable that this pathology is characterized by ectopic mineralization in elastic fibers, and in particular in the Bruch’s membrane, which then becomes rigid. We can suppose that its opening turns out to be a zone of higher constraint for the nerve fibers.
Other hypotheses have been put forward: in particular, it has been proposed that ODD emerge from abnormal vasculature and branching, as higher frequencies of trifurcation and cilioretinal arteries have been observed in patients with ODD (45, 46). An abnormal permeability and a deficient blood barrier would induce chronic ischemia and calcium deposition, leading to ODD formation. Still, an association has been found between a small scleral canal and vascular anomalies in ODD patients (47), and it is possible that abnormal vessels are a consequence of the higher constraints induced pre- and post-natally by a narrow canal.
We acknowledge several limitations to this study. Although we will adhere to the PRISMA guidelines and methodology, it is not possible to completely account for the limitations of included studies. We expect moderate to high heterogeneity because of several variable factors, including patients’ age, measurement methods or magnification correction. However, these factors will be discussed in the narrative review, which will allow us to examine the results accordingly. A subgroup analysis taking into account the expected difference between buried ODD and visible ODD might help us explain part of the heterogeneity and the divergency observed in the literature. To limit the file drawer problem which results in publication bias, grey literature will be searched in addition to traditional databases of published literature.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
AV-J: Conceptualization, Writing – original draft, Writing – review & editing. DB-G: Conceptualization, Writing – review & editing. MR: Conceptualization, Writing – review & editing.
Funding
The authors declare financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author DB-G declared that they were an editorial board member of Frontiers at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fopht.2023.1256397/full#supplementary-material
Abbreviations
EDI, enhanced depth imaging; HS, Healthy subject; OCT, optical coherence tomography; ODD, Optic disc drusen; SD-OCT, spectral domain optical coherence tomography; SS-OCT, swept source optical coherence tomography; TD-OCT, time-domain optical coherence tomography.
References
1. Spencer WH. Drusen of the optic disk and aberrant axoplasmic transport. The XXXIV Edward Jackson memorial lecture. Am J Ophthalmol (1978) 85(1):1–12. doi: 10.1016/S0002-9394(14)76658-9
2. You QS, Xu L, Wang YX, Jonas JB. Prevalence of optic disc drusen in an adult Chinese population: The Beijing Eye Study. Acta Ophthalmol (2009) 87(2):227–8. doi: 10.1111/j.1755-3768.2008.01211.x
3. Auw-Haedrich C, Staubach F, Witschel H. Optic disk drusen. Surv Ophthalmol (2002) 47(6):515–32. doi: 10.1016/S0039-6257(02)00357-0
4. Skougaard M, Heegaard S, Malmqvist L, Hamann S. Prevalence and histopathological signatures of optic disc drusen based on microscopy of 1713 enucleated eyes. Acta Ophthalmol (2020) 98(2):195–200. doi: 10.1111/aos.14180
5. Rebolleda G, Muñoz-Negrete FJ. The role of OCT in the differential diagnosis between buried optic nerve drusen and papilloedema. Arch Soc Esp Oftalmol. (2016) 91(9):431–8. doi: 10.1016/j.oftal.2016.02.022
6. Mezad-Koursh D, Klein A, Rosenblatt A, Teper Roth S, Neudorfer M, Loewenstein A, et al. Peripapillary hyperreflective ovoid mass-like structures-a novel entity as frequent cause of pseudopapilloedema in children. Eye (Lond) (2020) 35(4):1228–34. doi: 10.1038/s41433-020-1067-x
7. Nana Wandji B, Dugauquier A, Ehongo A. Visual field defects and retinal nerve fiber layer damage in buried optic disc drusen: A new insight. Int J Ophthalmol (2022) 15(10):1641–9. doi: 10.18240/ijo.2022.10.12
8. Cennamo G, Montorio D, Giunta P, Tranfa F. Optical coherence tomography angiography in nonarteritic anterior ischemic optic neuropathy due to optic nerve head drusen. Neurol Sci (2020) 41(11):3349–51. doi: 10.1007/s10072-020-04493-4
9. Law DZ, Yang FPL, Teoh SCB. Case report of optic disc drusen with simultaneous peripapillary subretinal hemorrhage and central retinal vein occlusion. Case Rep Ophthalmol Med (2014) 2014:156178. doi: 10.1155/2014/156178
10. Douglas VP, Douglas KAA, Miller JB, Cestari DM. Juxtapapillary choroidal neovascular membrane as a complication of optic disc drusen: Multimodal imaging with swept source-optical coherence tomography and optical coherence tomography angiography. J Neuroophthalmol. (2022) 42(1):e430–3. doi: 10.1097/WNO.0000000000001227
11. Rothenbuehler SP, Maloca PM, Belmouhand M, Hamann S, Larsen M. Branch retinal vein occlusion precipitated by compression between a major retinal artery and underlying optic disc drusen. Acta Ophthalmol (2021) 99(8):931–3. doi: 10.1111/aos.14840
12. Obuchowska I, Ustymowicz A. Blood flow disturbances in the central retinal artery in patients with bilateral optic disc drusen. Sci Rep (2020) 10(1):11111. doi: 10.1038/s41598-020-68090-3
13. Floyd MS, Katz BJ, Digre KB. Measurement of the scleral canal using optical coherence tomography in patients with optic nerve drusen. Am J Ophthalmol (2005) 139(4):664–9. doi: 10.1016/j.ajo.2004.11.041
14. Thompson AC, Bhatti MT, El-Dairi MA. Bruch’s membrane opening on optical coherence tomography in pediatric papilledema and pseudopapilledema. J AAPOS. (2018) 22(1):38–43.e3. doi: 10.1016/j.jaapos.2017.09.003
15. Malmqvist L, Li XQ, Eckmann CL, Skovgaard AM, Olsen EM, Larsen M, et al. Optic disc drusen in children: The copenhagen child cohort 2000 eye study. J Neuroophthalmol. (2018) 38(2):140–6. doi: 10.1097/WNO.0000000000000567
16. Amini N, Miraftabi A, Henry S, Chung N, Nowroozizadeh S, Caprioli J, et al. The relationship of the clinical disc margin and bruch’s membrane opening in normal and glaucoma subjects. Invest Ophthalmol Vis Sci (2016) 57(3):1468–75. doi: 10.1167/iovs.15-18382
17. Chauhan BC, Burgoyne CF. From clinical examination of the optic disc to clinical assessment of the optic nerve head: A paradigm change. Am J Ophthalmol (2013) 156(2):218–227.e2. doi: 10.1016/j.ajo.2013.04.016
18. Bellezza AJ, Rintalan CJ, Thompson HW, Downs JC, Hart RT, Burgoyne CF. Anterior scleral canal geometry in pressurised (IOP 10) and non-pressurised (IOP 0) normal monkey eyes. Br J Ophthalmol (2003) 87(10):1284–90. doi: 10.1136/bjo.87.10.1284
19. Schuman JS, Wollstein G, Farra T, Hertzmark E, Aydin A, Fujimoto JG, et al. Comparison of optic nerve head measurements obtained by optical coherence tomography and confocal scanning laser ophthalmoscopy. Am J Ophthalmol (2003) 135(4):504–12. doi: 10.1016/S0002-9394(02)02093-7
20. Belghith A, Bowd C, Medeiros FA, Hammel N, Yang Z, Weinreb RN, et al. Does the location of bruch’s membrane opening change over time? Longitudinal analysis using San Diego automated layer segmentation algorithm (SALSA). Invest Ophthalmol Vis Sci (2016) 57(2):675–82. doi: 10.1167/iovs.15-17671
21. Waldstein SM, Faatz H, Szimacsek M, Glodan AM, Podkowinski D, Montuoro A, et al. Comparison of penetration depth in choroidal imaging using swept source vs spectral domain optical coherence tomography. Eye. (2015) 29(3):409–15. doi: 10.1038/eye.2014.319
22. Malmqvist L, Bursztyn L, Costello F, Digre K, Fraser JA, Fraser C, et al. The optic disc drusen studies consortium recommendations for diagnosis of optic disc drusen using optical coherence tomography. J Neuroophthalmol. (2018) 38(3):299–307. doi: 10.1097/WNO.0000000000000585
23. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. (2009) 62(10):1006–12. doi: 10.1016/j.jclinepi.2009.06.005
24. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. (2000) 283(15):2008–12. doi: 10.1001/jama.283.15.2008
25. Ma LL, Wang YY, Yang ZH, Huang D, Weng H, Zeng XT. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: what are they and which is better? Military Med Res (2020) 7(1):7. doi: 10.1186/s40779-020-00238-8
26. Study quality assessment tools | NHLBI, NIH . Available at: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools.
27. Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res (2018) 27(6):1785–805. doi: 10.1177/0962280216669183
28. Shi J, Luo D, Weng H, Zeng XT, Lin L, Chu H, et al. Optimally estimating the sample standard deviation from the five-number summary. Res Synth Methods (2020) 11(5):641–54. doi: 10.1002/jrsm.1429
29. Jonas JB, Gusek GC, Guggenmoos-Holzmann I, Naumann GOH. Size of the optic nerve scleral canal and comparison with intravital determination of optic disc dimensions. Graefe’s Arch Clin Exp Ophthalmol (1988) 226(3):213–5. doi: 10.1007/BF02181183
30. Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Introduction to meta-analysis. Chichester, UK: John Wiley & Sons, Ltd (2009). doi: 10.1002/9780470743386
31. Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327(7414):557–60. doi: 10.1136/bmj.327.7414.557
32. Ryan R, Hill S. How to GRADE the quality of the evidence. Cochrane Consumers and Communication Group (2016). Available at: http://cccrg.cochrane.org/author-resources. Version 3.0 December 2016.
33. Falardeau JM, Pineles SL, Van Stavern GP, Lee AG. Should patients with optic disc drusen be treated with intraocular pressure-lowering medications? J Neuroophthalmol (2020) 40(4):538–43. doi: 10.1097/WNO.0000000000000929
34. Pardue MT, Allen RS. Neuroprotective strategies for retinal disease. Prog Retinal Eye Res (2018) 65:50–76. doi: 10.1016/j.preteyeres.2018.02.002
35. Fernández-Vega B, Nicieza J, Álvarez-Barrios A, Álvarez L, García M, Fernández-Vega C, et al. The use of vitamins and coenzyme Q10 for the treatment of vascular occlusion diseases affecting the retina. Nutrients. (2020) 12(3):723. doi: 10.3390/nu12030723
36. Boatright JH, Nickerson JM, Moring AG, Pardue MT. Bile acids in treatment of ocular disease. J Ocul Biol Dis Infor. (2009) 2(3):149–59. doi: 10.1007/s12177-009-9030-x
37. Seider MI, Lee RY, Wang D, Pekmezci M, Porco TC, Lin SC. Optic disk size variability between African, Asian, white, Hispanic, and Filipino Americans using Heidelberg retinal tomography. J Glaucoma. (2009) 18(8):595–600. doi: 10.1097/IJG.0b013e3181996f05
38. Hoyt WF, Pont ME. Pseudopapilledema: Anomalous elevation of optic disk. Pitafalls in diagnosis and management. JAMA. (1962) 181:191–6. doi: 10.1001/jama.1962.03050290013003
39. Serpen JY, Prasov L, Zein WM, Cukras CA, Cunningham D, Murphy EC, et al. Clinical features of optic disc drusen in an ophthalmic genetics cohort. J Ophthalmol (2020) 2020:5082706. doi: 10.1155/2020/5082706
40. Oliveira C, Harizman N, Girkin CA, Xie A, Tello C, Liebmann JM, et al. Axial length and optic disc size in normal eyes. Br J Ophthalmol (2007) 91(1):37–9. doi: 10.1136/bjo.2006.102061
41. Mansour AM, Stewart MW, Yassine SW, Mehanna CJZ, Casella AMB, Hamam RN, et al. Unmeasurable small size superficial and deep foveal avascular zone in nanophthalmos: The Collaborative Nanophthalmos OCTA Study. Br J Ophthalmol (2019) 103(8):1173–8. doi: 10.1136/bjophthalmol-2018-312781
42. Raval N, Zhang C, Yao WJ, Lin J. Posterior segment abnormalities in posterior microphthalmos. Am J Ophthalmol Case Rep (2020) 20. doi: 10.1016/j.ajoc.2020.100915
43. Ren X, Gao Y, Lin Y, Fu X, Xiao L, Wang X, et al. A novel mutation in the membrane frizzled-related protein gene for posterior microphthalmia, non-pigmented retinitis pigmentosa, optic nerve drusen, and retinoschisis in a consanguineous family. Front Med (2022) 9. doi: 10.3389/fmed.2022.835621
44. Pipelart V, Leroux B, Leruez S, Henni S, Navasiolava N, Martin L, et al. A study of optic nerve head drusen in 38 pseudoxanthoma elasticum (PXE) patients (64 eyes). Location of optic nerve head drusen in PXE. J Fr Ophtalmol. (2019) 42(3):262–8. doi: 10.1016/j.jfo.2018.08.007
45. Pilat AV, Proudlock FA, McLean RJ, Lawden MC, Gottlob I. Morphology of retinal vessels in patients with optic nerve head drusen and optic disc edema. Invest Ophthalmol Vis Sci (2014) 55(6):3484–90. doi: 10.1167/iovs.14-13903
46. Antcliff RJ, Spalton DJ. Are optic disc drusen inherited? Ophthalmology (1999) 106(7):1278–81. doi: 10.1016/S0161-6420(99)00708-3
Keywords: optic nerve head drusen, optic disc drusen, scleral canal, Bruch’s membrane opening, disc size, crowded disc
Citation: Vienne-Jumeau A, Brémond-Gignac D and Robert MP (2023) Optic disc drusen and scleral canal size – protocol for a systematic review and meta-analysis. Front. Ophthalmol. 3:1256397. doi: 10.3389/fopht.2023.1256397
Received: 10 July 2023; Accepted: 15 September 2023;
Published: 05 October 2023.
Edited by:
Andrew Lee, Houston Methodist Hospital, United StatesReviewed by:
Huban Atilla, Ankara University, TürkiyeFabienne C. Fierz, University Hospital Zürich, Switzerland
Copyright © 2023 Vienne-Jumeau, Brémond-Gignac and Robert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aliénor Vienne-Jumeau, YWxpZW5vci52aWVubmUtanVtZWF1QGhvdG1haWwuY29t