 Hélène Pluchart1,2,3*
Hélène Pluchart1,2,3* Sébastien Chanoine1,2,4
Sébastien Chanoine1,2,4 Denis Moro-Sibilot2,4,5
Denis Moro-Sibilot2,4,5 Christos Chouaid6,7Gil Frey8
Christos Chouaid6,7Gil Frey8 Julie Villa9
Julie Villa9 Bruno Degano2,5,10Matteo Giaj Levra4,5Pierrick Bedouch1,2,3
Bruno Degano2,5,10Matteo Giaj Levra4,5Pierrick Bedouch1,2,3 Anne-Claire Toffart2,4,5
Anne-Claire Toffart2,4,5- 1Pôle Pharmacie, Centre Hospitalier Universitaire Grenoble Alpes, La Tronche, France
- 2Université Grenoble Alpes, Grenoble, France
- 3Université Grenoble Alpes, CNRS, Grenoble INP, TIMC UMR5525, Grenoble, France
- 4Institut pour l’Avancée des Biosciences, UGA/INSERM U1209/CNRS 5309, Université Grenoble Alpes, La Tronche, France
- 5Service Hospitalier Universitaire de Pneumologie Physiologie, Centre Hospitalier Universitaire Grenoble Alpes, Grenoble, France
- 6Service de Pneumologie, Centre Hospitalier Intercommunal de Créteil, Créteil, France
- 7Inserm U955, UPEC, IMRB, équipe CEpiA, Créteil France
- 8Service de Chirurgie Thoracique, Vasculaire et Endocrinienne, Centre Hospitalier Universitaire Grenoble Alpes, Grenoble, France
- 9Service de Radiothérapie, Centre Hospitalier Universitaire Grenoble Alpes, Grenoble, France
- 10Laboratoire HP2, INSERM U1042, Université Grenoble Alpes, Grenoble, France
Most patients with lung cancer are smokers and are of advanced age. They are therefore at high risk of having age- and lifestyle-related comorbidities. These comorbidities are subject to treatment or even polypharmacy. There is growing evidence of a link between lung cancer, comorbidities and medications. The relationships between these entities are complex. The presence of comorbidities and their treatments influence the time of cancer diagnosis, as well as the diagnostic and treatment strategy. On the other hand, cancer treatment may have an impact on the patient’s comorbidities such as renal failure, pneumonitis or endocrinopathies. This review highlights how some comorbidities may have an impact on lung cancer presentation and may require treatment adjustments. Reciprocal influences between the treatment of comorbidities and anticancer therapy will also be discussed.
1 Background
Lung cancer is often diagnosed at an advanced stage of the disease (Jemal et al., 2010; Howlader et al., 2011), at a median age of 70 years (Noone et al., 2015). At this age, 65% of the general population has at least two comorbidities (Divo et al., 2014). The prevalence of comorbidities for lung cancer patients is higher than that of other cancer patients, approximately 50%–70% at diagnosis (Edwards et al., 2014a; Islam et al., 2015). However, little is known about lung cancer in elderly patients with comorbidities because they are excluded from most clinical trials (Hutchins et al., 1999).
On the one hand, comorbidities can have an impact on cancer survival (Islam et al., 2015; Leduc et al., 2017; Morishima et al., 2019) by influencing the therapeutic strategy. They could be responsible to an alteration of the general condition or a worse tolerance of anticancer treatments. In addition anticancer treatments can worsen or induce comorbidities (Laskin et al., 2012; Perazella, 2012; Haanen et al., 2017; McGowan et al., 2017; Hanania et al., 2019).
On the other hand, comorbidities generally imply the addition of medication to the symptomatic treatment intrinsically related to lung cancer. Such medication is likely to have consequences on drug-drug interactions or non-adherence or be responsible for adverse drug reactions (Scripture and Figg, 2006a; Popa et al., 2014a). Such multiple prescriptions can lead to polypharmacy (PP) (generally defined as a threshold of five medications) (Masnoon et al., 2017) and the administration of potentially inappropriate medications, which has been described for cancer patients, in particular, the elderly (Lees and Chan, 2011; LeBlanc et al., 2015; Nightingale et al., 2015).
This paradigm concerns all cancers, and we have chosen to focus on lung cancer. Very few data are available specifically on lung cancer. That is why we also presented publications (study or review) on all solid tumors. Although lung cancer population can be different from other cancer types, drug pharmacokinetics and pharmacodynamics are similar. Here, we propose a narrative review on the existing literature concerning the impact of both comorbidities and medication on lung cancer patients, as well as the consequences of anticancer treatments on comorbidities (Figure 1).
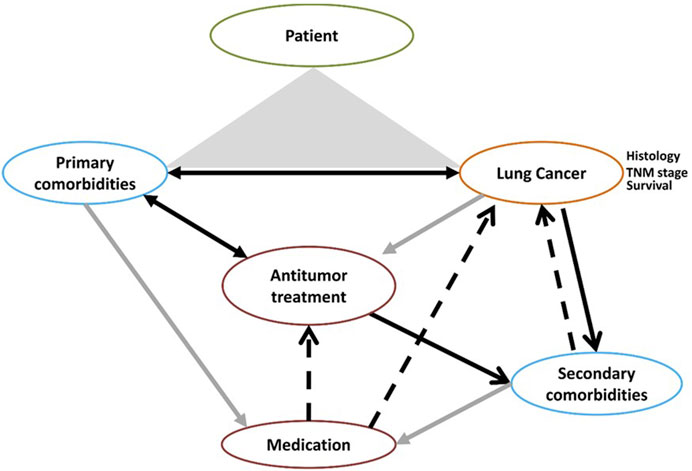
FIGURE 1. Lung, cancer, medication, and comobidities: an infernal trio.
2 Lung cancer and comorbidities
Comorbidity was first defined as the existence of any distinct additional clinical entity by Alvan Feinstein in 1970 (Feinstein, 1970). Comorbidity can be scored by several means. The most used in lung cancer is the Charlson Comorbidity Index (CCI), which assesses the impact of comorbidities (Charlson et al., 1987). There are several scores to describe the impact of comorbidities (Sarfati, 2012). More than half (50%–70%) of lung cancer patients have comorbidities at diagnosis (Edwards et al., 2014b; Islam et al., 2015). In 90% of cases (Barbone et al., 1997), lung cancer is associated with tobacco consumption, which can lead to lung injury, cardiovascular diseases, and diabetes mellitus (Chang, 2012; Goldkorn et al., 2014; Messner and Bernhard, 2014). Most lung cancer patients are over 65 years of age (Noone et al., 2015). Ageing can be associated with a decline in renal function and cardiovascular and metabolic disorders (Scheen, 2005; Halter et al., 2014; Mallappallil et al., 2014). The most frequent comorbidity of lung cancer patients is chronic obstructive pulmonary disease (COPD) (30%–50% of lung cancer patients), followed by diabetes (15%), congestive heart failure (12%), peripheral vascular disease (7%–8%), cerebrovascular disease (7%), and renal disease (from 2% to 6%) (Edwards et al., 2014b; Islam et al., 2015).
We first discuss the impact of comorbidities on lung cancer and the impact of lung cancer on comorbidities.
2.1 Impact of tobacco exposure and comorbidities on lung cancer features and treatments
Certain comorbidities taken separately are reported as independent poor prognostic factors for the survival of lung cancer patients (Leduc et al., 2017), such as COPD, tuberculosis, interstitial lung disease, cardiovascular diseases, and renal insufficiency (Table 1). Obesity is described as a favorable prognostic factor, within the framework of “obesity paradox” described in lung cancer (Li et al., 2016; Petrelli et al., 2021). While low body mass index is associated with lower survival, patients with obesity have improved survival.
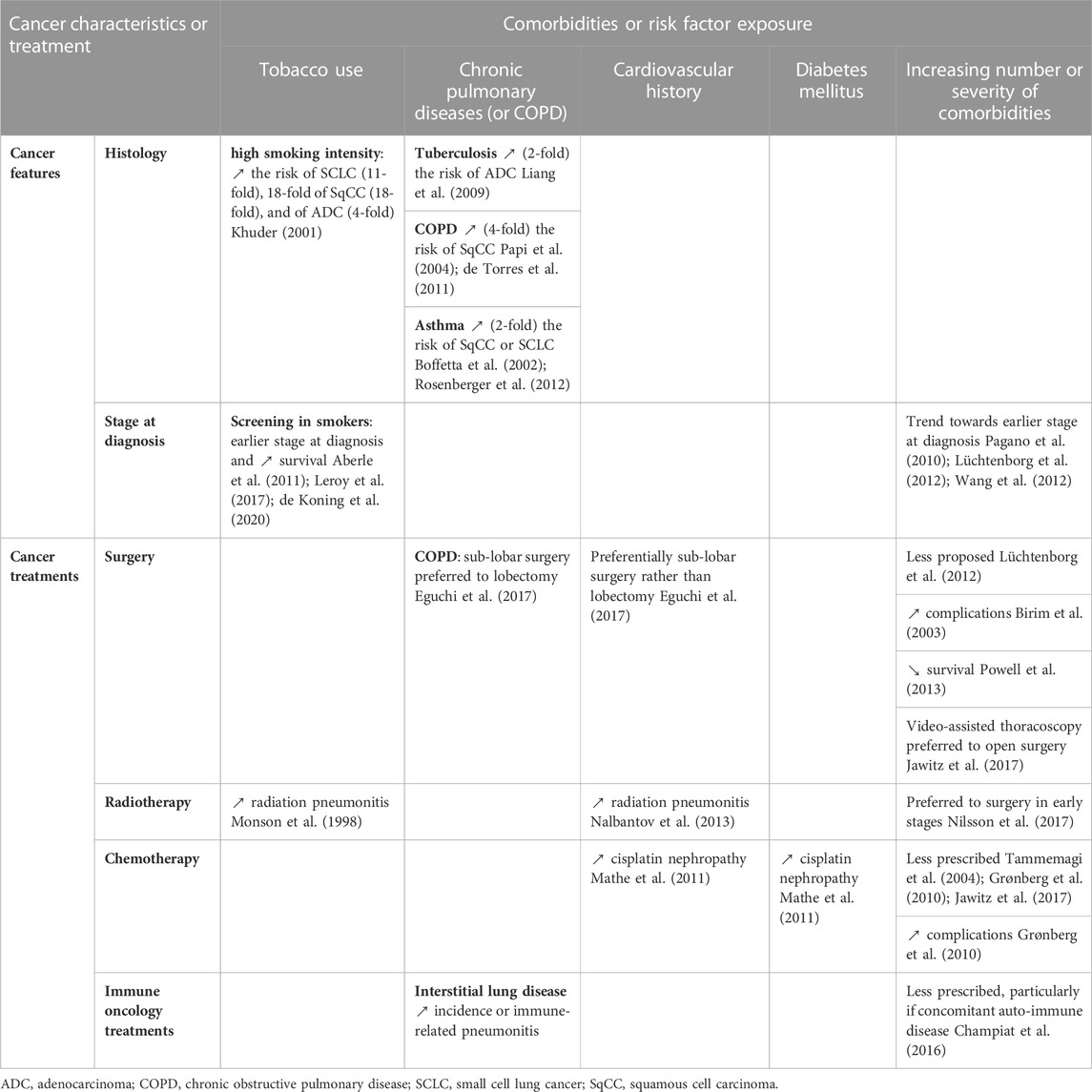
TABLE 1. Impact of tobacco exposure and comorbidities on lung cancer features and treatments.
Furthermore, comorbidities could induce carcinogenesis, such as COPD (de Torres et al., 2011), infections (Kuper et al., 2000; Yu et al., 2011), diabetes mellitus (although still debated (Sciacca et al., 2013)) and obstructive sleep apnea through hypoxia (Gozal et al., 2015; Justeau et al., 2020). Several mechanisms have been proposed, mostly oxidative damage and chronic inflammation. Comorbidities can affect various lung cancer characteristics such as histology, stage at diagnosis, and anticancer treatment.
2.1.1 Impact of tobacco exposure and comorbidities on histology
COPD increases the frequency of squamous cell carcinoma by four fold (Papi et al., 2004; de Torres et al., 2011), whereas asthma increases the frequency of this histological subtype or of small-cell lung cancer (SCLC) by two fold (Boffetta et al., 2002; Rosenberger et al., 2012). The mechanism is still unclear but may involve an altered inflammatory response and fibrogenesis. Lung cancer patients who had prior tuberculosis show a higher frequency of adenocarcinoma (approximately two-fold higher) (Liang et al., 2009), probably also due to fibrosis and inflammation (Leduc et al., 2017).
Tobacco smoke has been shown to be strongly associated with SCLC and squamous cell carcinoma (proximal localization) (Khuder, 2001). The relationship between histology and the size of inhaled smoke particles was already described in 1989, supporting the hypothesis that the biggest particles settle on cells of the epidermal bronchi and the smallest in peripheral tissue near glandular cells (Yang et al., 1989). In addition, different molecular profiles have been described between smokers and never-smokers with non-small-cell lung cancer (NSCLC). Barlesi et al., 2016 reported that nearly 44% of patients who were never smokers had a mutation in the epidermal growth factor receptor (EGFR) gene (vs. 11% in the overall population). The carcinogens contained in tobacco smoke induce, instead, loss-of-function mutations in tumor suppressor genes, such as p53 (Couraud et al., 2012).
2.1.2 Impact of tobacco exposure and comorbidities on stage at diagnosis
Several studies have investigated how comorbidities affect the stage at diagnosis of lung cancer. However, most showed only a trend towards earlier stages for patients with more comorbidities (Pagano et al., 2010; Lüchtenborg et al., 2012; Wang et al., 2012). These findings may be due to bias related to higher level of medical monitoring in this population. For 402 patients with advanced NSCLC, a significantly higher proportion of stage IIIb than stage IV was observed at diagnosis for patients with severe comorbidities (Grønberg et al., 2010). Dalton et al. reported similar results, showing that a higher CCI correlated with an earlier stage at diagnosis (Dalton et al., 2015). However, these findings are still debated (Ahn et al., 2013; Sarfati et al., 2016).
Lung cancer screening of smokers or COPD patients with emphysema was investigated in the NELSON, NLST, and AIR trials (Aberle et al., 2011; Leroy et al., 2017; de Koning et al., 2020). These studies aimed to diagnose lung cancer at an early stage, when they are eligible for radical treatment that could improve patient survival. For example, lung cancer-specific mortality (primary outcome) was significantly lower in the screening group in the NELSON study (de Koning et al., 2020).
2.1.3 Impact of comorbidities on treatment strategy
2.1.3.1 Surgery
Studies clearly show that surgery is preferred for patients with no or few comorbidities (Cykert et al., 2010; Lüchtenborg et al., 2012). For example, in the Swedish Lung Cancer Data Base (Nilsson et al., 2017), surgery was performed less for patients in early stages of NSCLC with a CCI ≥3 than those without a comorbidity. In addition, the number of comorbidities has been shown to be associated with morbi-mortality for surgically treated NSCLC patients. A CCI score of 3–4 was predictive of major complications (Birim et al., 2003) and a CCI of 2–4 with higher 90-day mortality after surgery (Powell et al., 2013). In the European Respiratory Society and European Society of Thoracic Surgery guidelines, indications for surgery depend on the morbi-mortality risk, which takes into account comorbidities (Brunelli et al., 2009; Brunelli et al., 2013). Patients can be considered to have a low (<1%), moderate, or high (>10%) risk of mortality, depending on their respiratory and cardio-vascular status. The French Society of Thoracic and Cardio-Vascular Surgery developed a risk model to predict in-hospital mortality for patients undergoing lung surgery. The most frequent comorbidities were evaluated: COPD, arterial hypertension, smoking, heart disease, peripheral vascular disease, history of cancer, and diabetes mellitus (Falcoz et al., 2007). Having at least three comorbid conditions was associated with lower in-hospital survival. The revised cardiac risk index is a widely used tool for cardiac risk stratification before major lung resection (Brunel et al., 2010). It relies on four variables that were identified to be predictive risk factors of major cardiac morbidity (cerebrovascular disease, cardiac ischemia, renal disease, and pneumonectomy) and allows the selection of patients who need further cardiac testing. The burden of comorbidities also has an impact on the choice of surgical strategy. Patients with COPD, a history of cardiovascular disease, or a CCI ≥2 preferentially benefit from sub-lobar surgery rather than lobectomy (Eguchi et al., 2017). For patients with few comorbidities, lobectomy is preferentially offered over sub-lobar resection, because it is associated with higher overall survival (Boyer et al., 2017). Video-assisted thoracoscopic surgery is preferred to open surgery for patients with severe comorbidities (Jawitz et al., 2017).
2.1.3.2 Radiotherapy
In early stages, stereotactic radiotherapy is more likely to be proposed for patients with severe comorbidities (CCI ≥3) (Nilsson et al., 2017). The decision to attempt curative radiotherapy increases with the CCI. However, no impact of the CCI on survival after radiotherapy has been reported (Mellemgaard et al., 2015). Radiation-induced lung injury is a common complication of radiotherapy. In 1998, Monson et al. found that pre-existing comorbid lung disease increases the risk of radiation pneumonitis (Monson et al., 1998) and that tobacco consumption is responsible for more extensive lung injury. Cardiac comorbidity has been found to be associated with a higher risk of radiation-induced lung injury than for patients with no prior cardiac comorbidity (Nalbantov et al., 2013). However, the impact of these comorbidities on radiation-induced lung injury is also still debated (Dreyer et al., 2018).
2.1.3.3 Pharmacological treatment
In terms of chemotherapy-related toxicity, the choice of molecule should be very carefully made to not worsen patients‘ comorbidities. The number of comorbidities has an impact on pharmacological treatment (Lee et al., 2011) and chemotherapy in NSCLC is less prescribed as the number of comorbidities increases (Tammemagi et al., 2004; Grønberg et al., 2010; Jawitz et al., 2017). Patients with a high comorbidity score are more likely to have complications after chemotherapy. NSCLC patients with severe comorbidities have been shown to be more likely to have a higher frequency of thrombocytopenia, febrile neutropenia, or death after neutropenic infections than those without comorbidity (Grønberg et al., 2010). Another study which compared pemetrexed/carboplatin versus gemcitabine/carboplatin as first line therapy in stage IIIB/IV NSCLC patients reported that patients with comorbidities have a higher risk of developing grade 3 to 5 gastro-intestinal, cardiovascular, and infectious adverse events, rash, and nausea (Asmis et al., 2008). In addition, cardiovascular disease and diabetes increase the risk of cisplatin-induced nephropathy (Mathe et al., 2011).
Immune oncology treatments, such as immune-checkpoint inhibitors that target programmed cell death (PD)-1, PD-ligand (PD-L) 1, or cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) are routinely used in lung cancer. Given the protective role of PD-(L)1 signaling in immune tolerance (Riella et al., 2012), auto-immune diseases can appear or worsen with PD-(L)1 inhibitors. It is very important to identify the risk of dysimmunity before prescribing immune-checkpoint inhibitors (Champiat et al., 2016). Patients with auto-immune diseases have been excluded from phase 3 clinical trials testing immune oncology therapies. Therefore, prescribing this therapeutic class in the context of a pre-existing auto-immune disease can only be considered after multidisciplinary consultation. It has been reported that preexisting interstitial lung disease is associated with higher incidence of immune-related pneumonitis (Gomatou et al., 2020). The indication of immune-checkpoint inhibitors in these patients should be discussed in a multidisciplinary setting.
While some cytotoxic drugs prescriptions such as platin salts are capped if body surface area is superior to 2 square meters, the question of obesity impact on flat doses for immune oncology treatments arises. In obesity, blood volume increases but less than proportional with the change in body weight. Given that monoclonal antibodies distribute only in the blood plasma and extracellular fluids, for some of them, body weight does not have a significant impact on the volume of distribution. Based on pharmacokinetics, flat doses can be proposed in obese population (Hendrikx et al., 2017), as described in the updated ASCO guidelines (review of 6 studies that included overweight or obese patients with cancer) (Griggs et al., 2021). More interestingly, in some studies obese patients receiving PD-1 inhibitors show better survival than nonobese patients, this may due to increased PD-1 expression through leptin higher levels (Woodall et al., 2020).
2.2 Impact of lung cancer treatment on comorbidities
After lung cancer treatment, it is important to distinguish temporary side effects from lasting comorbidities (Table 2). This section will focus on the effect of lung cancer treatment in the exacerbation of pre-existing primary comorbidities or those that lead to irreversible secondary comorbidities.
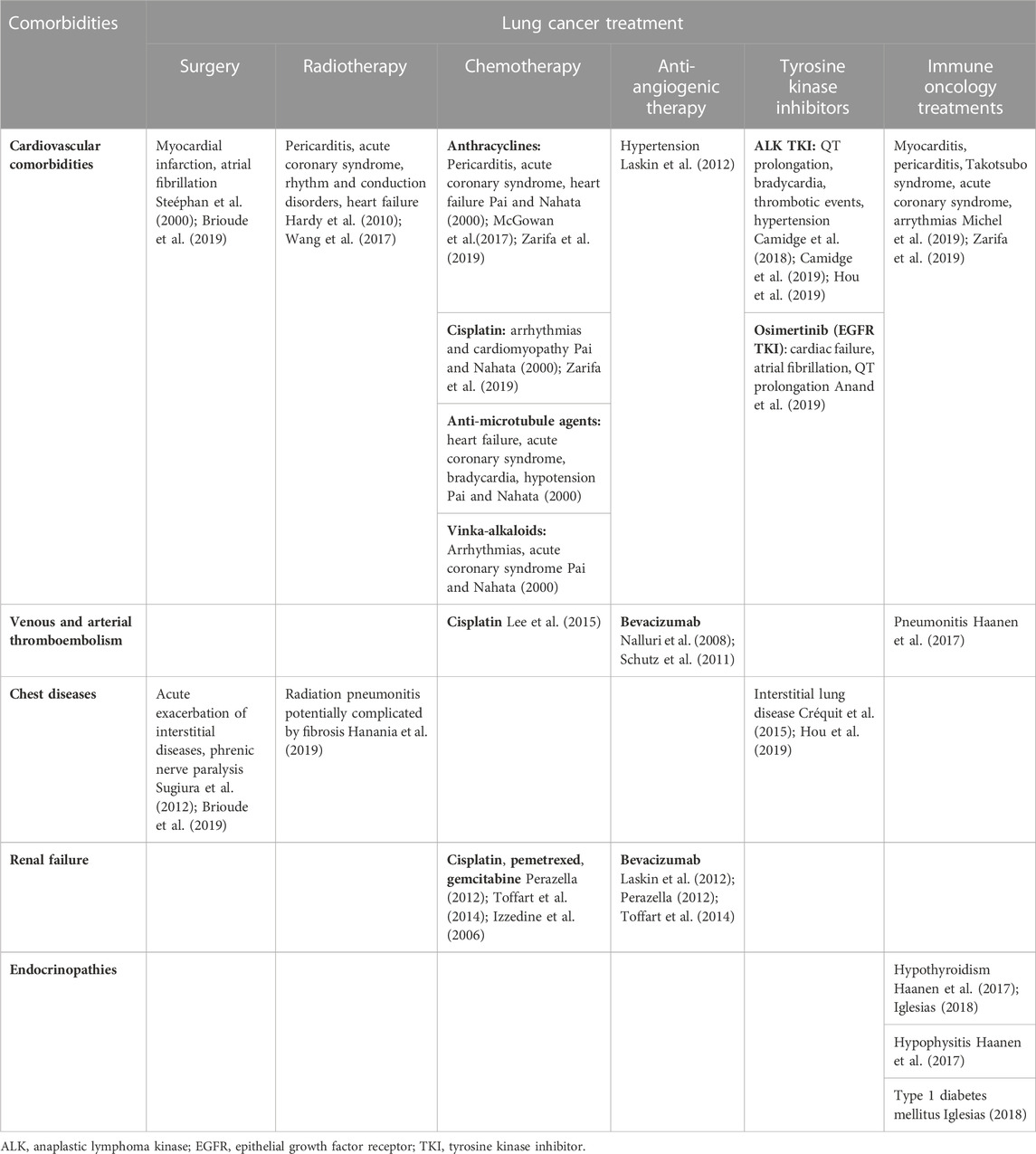
TABLE 2. Impact of lung cancer treatment on comorbidities.
2.2.1 Impact of surgery on comorbidities
Resection of lung cancer can have a consequence on pre-existing comorbidity. Indeed, reduction of lung parenchyma and altered pulmonary function can provoke acute exacerbation of interstitial pneumonia or phrenic nerve paralysis, leading to long-term decreased pulmonary function (Sugiura et al., 2012). Cardiovascular complications in patients with and without risk factors are also frequent such as myocardial infarction, atrial fibrillation can require antiplatelets or anticoagulants prescription (Steéphan et al., 2000; Brioude et al., 2019). Principal risk factors identified for postoperative morbidity include decreased forced expiratory volume in one second, smoking, age and pre-existing cardiovascular disease (Myrdal et al., 2001; Alloubi et al., 2010; Lugg et al., 2015).
2.2.2 Impact of radiotherapy on comorbidities
In the 6 months following lung irradiation, irreversible radiation pneumonitis appears in up to 25% of cases, potentially complicated by fibrosis (1 year after) (Hanania et al., 2019). Glucocorticoids can be proposed for radiation pneumonitis, whereas patients with radiation pulmonary fibrosis should be given supportive care (Hanania et al., 2019).
Cardiac toxicity has also been described with radiotherapy: effusion, unstable angina, myocardial infarction, and arrhythmias (Wang et al., 2017). In addition, chemoradiation has been reported to be an independent risk factor of conduction disorders, cardiac dysfunction, and heart failure (Hardy et al., 2010).
2.2.3 Impact of oral targeted therapies on comorbidities
EGFR and anaplastic lymphoma kinase (ALK) tyrosine kinase inhibitors (TKIs), prescribed in stage IV NSCLC, are less responsible for chronic adverse events. The main adverse events of ALK TKIs are cardiovascular effects: QT prolongation (Camidge et al., 2019), bradycardia (Camidge et al., 2018), thrombotic events (Hou et al., 2019), or hypertension (Camidge et al., 2018). Osimertinib (EGFR TKI) can also induce cardiac failure, atrial fibrillation, and QT prolongation (Anand et al., 2019). A common toxicity of all TKIs is interstitial lung disease (Hou et al., 2019), which may be a hypersensitivity pneumonitis (Créquit et al., 2015).
2.2.4 Impact of chemotherapy, anti-angiogenic therapies and immune checkpoint inhibitors on comorbidities
These toxicities are not exclusive to lung cancer. They are summarized in Table 2 (references (Pai and Nahata, 2000; Nalluri et al., 2008; Schutz et al., 2011; Laskin et al., 2012; Perazella, 2012; Toffart et al., 2014; Izzedine et al., 2006; Lee et al., 2015; Haanen et al., 2017; McGowan et al., 2017; Iglesias, 2018; Michel et al., 2019; Zarifa et al., 2019)).
3 Lung cancer and comorbidity-related medication
3.1 Impact of comorbidity-related medications on lung cancer diagnosis
Performance of pulmonary diagnostic procedures (for example, bronchial biopsies, transthoracic needle biopsy) can lead to complications such as minimal or severe bleeding (Facciolongo et al., 2016). Concomitant use of antiplatelets or anticoagulant agents for cardiovascular comorbidities may increase this risk. The physician has to assess the risk of bleeding according to patient risk factor and adapt procedures and/or comorbidity-related medications to enable diagnosis to be carried out in safety. According to the level of procedure bleeding risk and the level of comorbidity severity, anticoagulants or antiplatelets are either stopped before the procedure or maintained according to guidelines, depending on diagnostic procedure (Veitch et al., 2016; Pathak et al., 2017).
3.2 Impact of comorbidity-related medications on lung cancer features
Comorbidities often lead to the prescription of medication, whereas support treatment is often proposed to counteract the side effects of anticancer treatment. This “prescribing cascade” increases the number of prescribed medications (Gurwitz, 2004). Consequently, lung cancer patients are at a high risk of iatrogenic drug problems, such as drug-drug interactions, adverse drug reactions, or nonadherence (Goh et al., 2018). Medication can include both prescribed drugs and over-the-counter medication, including complementary and alternative medicines (CAM) (Lees and Chan, 2011). Of note, there are discrepancies in the definition of PP (Bushardt et al., 2008). Several studies have defined PP as two to nine medications (Shah and Hajjar, 2012; Turner et al., 2016), whereas others in the geriatric oncology population have used the threshold of five to six (Gnjidic et al., 2012; Nightingale et al., 2015; Sharma et al., 2016). Medication and PP in elderly cancer patients has been widely described in many studies (Lees and Chan, 2011; Maggiore et al., 2014; LeBlanc et al., 2015; Alkan et al., 2016; Lund et al., 2018). Nightingale et al. (Nightingale et al., 2015) reported a mean number of medications of 9, a prevalence of PP of 41%, and excessive PP of 43% (defined as more than 10 medications) in elderly cancer patients.
In the following section, we focus on the impact of medications for comorbidities in lung cancer and anticancer treatment, although some of data are not well described in the literature and were deduced from hypotheses based on physiopathology (Figure 2).
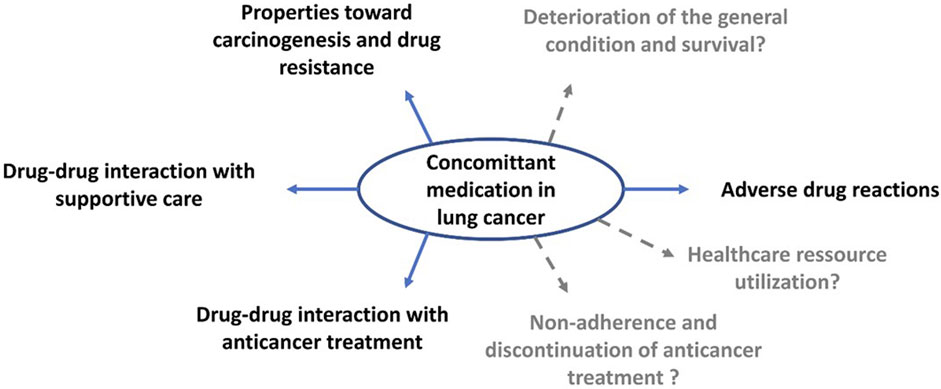
FIGURE 2. Consequences of concomitant medications in lung cancer patients.
3.2.1 Impact of comorbidity-related medications on cancer history
Certain molecules used for the treatment of comorbidities have shown properties towards carcinogenesis or drug resistance.
It appears that AMP-activated kinase, a metformin target, is associated with the tumor suppressor TET2 (Wu et al., 2018). In a recent meta-analysis, metformin showed a possible positive effect in advanced NSCLC, both on overall and progression-free survival (Zhang et al., 2018). The tendency of a favorable effect of statins in cancer has also been described (Han et al., 2011; Nielsen et al., 2012; Cardwell et al., 2015; Lin et al., 2016), although the results have not been consistent between studies (Seckl et al., 2017). There are several possible explanations for such an effect of statins (mevalonate pathway or the inhibition of cholesterol synthesis). Decreased activity of cyclin D1, cyclin-dependent kinase, and metallopeptidase 9 (involved in angiogenesis) by simvastatin would arrest the cell cycle and reduce metastatic potential (Yu et al., 2013). Even more surprisingly, simvastatin appears to reverse the resistance of tumors harboring the T790 M mutation of the EGFR in NSCLC cell lines (Hwang et al., 2014).
Non-steroidal anti-inflammatory drugs may play a positive role in carcinogenesis, the induction of apoptosis, and angiogenesis (Gurpinar et al., 2014). For many years, the literature has suggested that aspirin may have a protective role against cancer, more specifically in colorectal cancer (Garcia-Albeniz and Chan, 2011) and even lung cancer (Muscat et al., 2003).
Lung cancer resistance is caused by various mechanisms (Shanker et al., 2010), such as P-glycoprotein (P-gp), a protein highly expressed in multi-drug resistant lung cancer cells (Cole et al., 1992). P-gp is a drug efflux pump and can decrease antitumor drug concentrations. Verapamil, a calcium channel blocker that inhibits P-gp, may improve the survival of patients being treated with chemotherapy (Millward et al., 1993).
3.2.2 Impact of comorbidity-related medications on drug-drug interactions with anticancer treatment
PP is a risk factor for drug-drug interactions, which can have consequences on the patient, the cancer treatment, and the lung cancer prognosis. Given the narrow therapeutic index of cytotoxic antitumor treatment, it can lead to higher toxicity or therapeutic failure. Drug-drug interactions with antitumor treatment can be pharmacokinetic or involve pharmacodynamic interactions (Scripture and Figg, 2006b). PP, lung cancer diagnosis, and inpatient status are associated with severe drug-drug interactions (Alkan et al., 2016). Potential drug-drug interactions are common among cancer patients and most often involve medications related to comorbid conditions (Riechelmann et al., 2007).
A drug-drug interaction with concomitant medication was detected as a potential problem in 32% of cases in a study of 112 cancer patients, of whom 103 were taking medication for a comorbidity, with a mean number of five medications (Puts et al., 2009). A larger study also reported a frequency of 35% of severe drug-drug interactions among patients (32% of PP), which required considering modification of their therapy or avoidance of the combination. Such potential drug-drug interactions have often been identified with chemotherapy, 14% with a potentially severe impact (Popa et al., 2014b). In a large cohort of 7237 lung cancer patients with stage I/II disease, the most frequent and serious potential drug-drug interactions observed were warfarin associated with etoposide (14%) or gemcitabine (15%). Among the 302 patients treated with cisplatin, 34 (11%) had a concomitant furosemide prescription, which is considered to be a serious potential drug-drug interaction (Lund et al., 2018).
It is well established that TKIs can interact with treatments affecting cytochrome P450 (Song et al., 2011) or with antiacids (Duong and Leung, 2011). A recent review focused on the cardiovascular system and detailed all drug-drug interactions involving cancer treatment and cardiovascular drugs (Akbulut and Urun, 2020). Drug-drug interactions can occur between TKIs and drugs that prolong the QT interval, calcium-channel blockers, diuretics, and anticoagulants. Absorption of the EFGR TKI can be influenced by acid-reducing agents (with a reduced area under the curve) (Peters et al., 2014). A study recently reported that 507 NSCLC patients being concomitantly treated with erlotinib and acid-suppression drugs showed significantly lower progression-free and overall survival (Chu et al., 2015). The same results were found with the concomitant use of erlotinib (Sharma et al., 2019) or gefitinib (Fang et al., 2019) and proton-pump inhibitors, with decreased overall survival. TKIs can be also be involved in metabolism-based interactions through cytochrome P450 activity (Peters et al., 2014).
In recent years, question of gut and lung microbiome role as driver of immune checkpoint inhibitors efficacy has been raised. Because antibiotics and antiacids can unbalance gut microbiome, some papers suggested their negative role during immune checkpoint inhibitors treatment (Carbone et al., 2019). However, these data are based mostly on retrospective study and should be addressed on prospective studies focused on this hypothesis. For example, a study in 2022 using a shotgun-metagenomics-based microbiome profiling in a large cohort of patients with advanced NSCLC demonstrated that intestinal Akkermansia muciniphila can predicts increased objective response to immune checkpoint inhibitors treatments (Derosa et al., 2022).
3.2.3 Impact of the use of CAM on efficacy of anticancer treatment
The use of CAM has probably been underestimated in all studies, but 30%–50% of patients with lung cancer probably use them (Wyatt et al., 1999; Micke et al., 2010), which is a higher proportion than for other cancer patients (Johnson et al., 2018). CAM must be thoroughly researched by the oncologist before (and during) the prescription of any treatment, particularly for TKIs. The use of CAM could lead either to side-effects or decrease activity of the antitumor treatment (Berretta et al., 2017). For example, a pharmacokinetic drug-drug interaction was reported between crizotinib and ginger in a NSCLC patient, leading to higher plasma concentrations of crizotinib (via inhibition of the cytochrome P450 3A4 isoform, which metabolizes crizotinib), associated with hepatic cytolysis and discontinuation of the treatment (Revol et al., 2020).
3.2.4 Impact of comorbidity-related medications on adverse drug reactions
Concomitant medication is a risk factor for adverse drug reactions (Hanlon et al., 2006). Most studies have estimated a risk of adverse drug reactions, for which the search is inherent in the process of the pharmaceutical analysis of prescriptions. Taking five or more drugs and an age of over 76 years have been identified as potential factors associated with moderate/severe potential drug related problems (defined as drug interactions, additive toxicity, contraindications) (Puts et al., 2009; Goh et al., 2018). In 244 patients receiving chemotherapy taking a mean of 12 medications (Popa et al., 2014b), the risk of severe non-hematological toxicity was almost doubled for each additional potential drug-drug interaction and tripled for each additional potential drug-drug interaction involving chemotherapeutics. No association between potential drug-drug interaction and hematological toxicity was found. Goh et al., 2018 also reported that PP leading to drug problems was frequent in elderly cancer patients receiving chemotherapy. Another study did not report any association between chemotherapy related toxicity and a higher number of medications (Maggiore et al., 2014). Interestingly, high concomitant medication does not predict adverse radiotherapy outcomes (Nieder et al., 2017).
CAM can lead to antitumor treatment adverse events through pharmacodynamic interactions (Revol et al., 2020), as discussed in Section 1.3.
3.2.5 Impact of comorbidity-related medications on adherence and continuation of anticancer treatments
It is commonly accepted that concomitant medication increases the rate of non-adherence (Gray et al., 2001; Mansur et al., 2009). There is much less data available for lung cancer patients than for breast cancer patients and oral therapy (He et al., 2015) and they do not report non-adherence. In 62 patients treated with erlotinib taking a mean of five co-medications (range from 1 to 13), no association was reported between incorrect intake of erlotinib under fasting conditions and the number of drugs (Timmers et al., 2015). Similarly, Sud et al., 2015 did not identify any association between PP (defined as ≥ 6 medications) and toxicity-related discontinuation of chemotherapy.
3.2.6 Impact of comorbidity-related medications on utilization of healthcare resources
As medications can affect cancer and patient characteristics, they may lead to more utilization of healthcare resources. Taking a large number of medications has been shown to be associated with an increased risk of hospitalizations or emergency room visits (Sud et al., 2015; Hong et al., 2019). Among 298 unplanned admissions of cancer patients, 11% were considered to be associated with an adverse drug reaction and 2% with a drug-drug interaction (Miranda et al., 2011). The most common drug-drug interactions involved warfarin, captopril, and anti-inflammatory agents, and the most frequent adverse drug reaction was neutropenic fever post-chemotherapy. Having a prescription of two or more psychotropic medication classes for at least 90 days in the first year after cancer diagnosis was reported to be associated with a higher number of outpatient visits, office visits, hospitalizations, and longer length of stay (Pamoukdjian et al., 2017). However, these results are controversial (Maggiore et al., 2014).
3.2.7 Impact of comorbidity-related medications on general condition and survival
Medication can be associated with frailty (poor ECOG-performance status) or disability, which can have consequences on the administration and tolerance of antitumor treatment. In a cohort of 290 cancer patients, multiple medication was a risk factor of disability (Pamoukdjian et al., 2017). This finding was supported by another study in which multiple medication was associated with pre-frailty or frailty and poor physical function (Turner et al., 2014). A cut-off between 6 and 9 medications was proposed for predicting the risk of frailty (Williams et al., 2015; Turner et al., 2016).
A recent meta-analysis of 47 studies (not focused on cancer patients) showed a significant association between PP and death. This association increased with the number of medications (Leelakanok et al., 2017). In 289 cancer patients receiving palliative radiotherapy, neither PP nor the use of corticosteroids or opioid analgesics independently influenced overall survival (Nieder et al., 2017). Although potential drug-drug interactions were significantly associated with lower overall survival in breast cancer, this was not true for NSCLC. CAM use without anticancer treatment was independently associated with the risk of death in cancer patients (Johnson et al., 2018).
3.3 Impact of lung cancer features on comorbidity-related medications
Although the impact of comorbidity-related medications on lung cancer is described in the literature, there are no data on the impact of lung cancer on concomitant medications. This raises the question of whether the treatment needs to be simplified to avoid known and unknown drug-drug interactions to improve therapeutic adhesion with respect to the clinical benefit when the predicted survival is short. Medication should be re-evaluated on a case-by-case basis according to the type of tumor, its treatment, and the prognosis of the patient. These issues need to be addressed in large-scale studies.
4 Conclusion
Lung cancer is the cancer associated with the most comorbidities. These comorbidities and their related medications should be considered in lung cancer management, particularly in the choice of anticancer treatment. There are close relationships between these three entities. They are all intertwined and dependent on each other in lung cancer. Although several observational studies have been carried out, the impact of comorbidity-related medications on the care of cancer patients is less known. Further studies should assess the impact of both medications and comorbidities on lung cancer management and the prognosis of patients. There is a true need in the era of personalized medicine to better understand the impact of comorbidities on cancer and which drugs need to be avoided to optimize patient care.
Author contributions
HP and A-CT participated in the bibliographical research and drafted the manuscript. All authors reviewed the manuscript and revised it critically before submission. All authors have seen and approved the final version of the manuscript. They agreed to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgments
The authors thank Alex Edelman and Associates for providing language help and writing assistance.
Conflict of interest
HP, SC, PB, GF, JV, and BD have nothing to disclose. A-CT received consulting fees and non-financial support from Astra Zeneca, BMS, MSD, Novartis, Boehringer Ingelheim, Roche, Pfizer. DMS received grants or contracts from any entity from Roche, Astra Zeneca, BMS, Boehringer Ingelheim, Abbvie, Pfizer; received consulting fees from Roche, Astra Zeneca, BMS, MSD, Lilly, Takeda, Boehringer Ingelheim, Abbvie, Becton Dickinson, Pfizer, Novartis; received non-financial support from Roche, Astra Zeneca, BMS, MSD, Lilly, Takeda, Boehringer Ingelheim and Pfizer. CC received grants or contracts from any entity, consulting fees and non-financial support from Astra Zeneca, Boehringer Ingelheim, GSK, Roche, Sanofi Aventis, BMS, MSD, Lilly, Novartis, Pfizer, Takeda, Bayer, Amgen. MGL received grants or contracts from any entity from Astra Zeneca, BMS; received consulting fees from Astra Zeneca, BMS, MSD; received non financial support from MSD, Takeda.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ALK, Anaplastic lymphoma kinase; CAM, Complementary and alternative medicines; CCI, Charlson comorbidity index; COPD, Chronic obstructive pulmonary disease; CTLA-4, Cytotoxic T-lymphocyte-associated protein 4; EGFR, Epidermal growth factor receptor; NSCLC, Non-small cell lung cancer; PD-1, Programmed cell death 1; PD-L1, Programmed death-ligand 1; PP, Polypharmacy; SCLC, Small-cell lung cancer; TKI, Tyrosine kinase inhibitor.
References
Aberle, D. R., Adams, A. M., Berg, C. D., Black, W. C., Clapp, J. D., Fagerstrom, R. M., et al. (2011). Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 365 (5), 395–409. doi:10.1056/NEJMoa1102873
Ahn, D., Mehta, N., Yorio, J. T., Xie, Y., Yan, J., and Gerber, D. E. (2013). Influence of medical comorbidities on the presentation and outcomes of stage I-iii non–small-cell lung cancer. Clin. Lung Cancer 14 (6), 644–650. doi:10.1016/j.cllc.2013.06.009
Akbulut, M., and Urun, Y. (2020). Onco-cardiology: Drug-drug interactions of antineoplastic and cardiovascular drugs. Crit. Rev. Oncology/Hematology 145, 102822. doi:10.1016/j.critrevonc.2019.102822
Alkan, A., Yaşar, A., Karcı, E., Köksoy, E. B., Ürün, M., Şenler, F. Ç., et al. (2016). Severe drug interactions and potentially inappropriate medication usage in elderly cancer patients. Support. Care Cancer 25, 229–236. doi:10.1007/s00520-016-3409-6
Alloubi, I., Jougon, J., Delcambre, F., Baste, J. M., and Velly, J. F. (2010). Early complications after pneumonectomy: Retrospective study of 168 patients. Interact. Cardiovasc. Thorac. Surg. 11 (2), 162–165. doi:10.1510/icvts.2010.232595
Anand, K., Ensor, J., Trachtenberg, B., and Bernicker, E. H. (2019). Osimertinib-induced cardiotoxicity: A retrospective review of the fda adverse events reporting system (faers). JACC CardioOncology. 1 (2), 172–178. doi:10.1016/j.jaccao.2019.10.006
Asmis, T. R., Ding, K., Seymour, L., Shepherd, F. A., Leighl, N. B., Winton, T. L., et al. (2008). Age and comorbidity as independent prognostic factors in the treatment of non–small-cell lung cancer: A review of national cancer institute of Canada clinical trials group trials. J. Clin. Oncol. 26 (1), 54–59. doi:10.1200/JCO.2007.12.8322
Barbone, F., Bovenzi, M., Cavallieri, F., and Stanta, G. (1997). Cigarette smoking and histologic type of lung cancer in men. Chest 112 (6), 1474–1479. doi:10.1378/chest.112.6.1474
Barlesi, F., Mazieres, J., Merlio, J. P., Debieuvre, D., Mosser, J., Lena, H., et al. (2016). Routine molecular profiling of patients with advanced non-small-cell lung cancer: Results of a 1-year nationwide programme of the French cooperative thoracic intergroup (IFCT). Lancet 387 (10026), 1415–1426. doi:10.1016/S0140-6736(16)00004-0
Berretta, M., Pepa, C. D., Tralongo, P., Fulvi, A., Martellotta, F., Lleshi, A., et al. (2017). Use of Complementary and Alternative Medicine (CAM) in cancer patients: An Italian multicenter survey. Oncotarget 8 (15), 24401–24414. doi:10.18632/oncotarget.14224
Birim, O., Maat, APWM, Kappetein, A. P., van Meerbeeck, J. P., Damhuis, R. a. M., and Bogers, AJJC (2003). Validation of the Charlson comorbidity index in patients with operated primary non-small cell lung cancer. Eur. J. Cardiothorac. Surg. 23 (1), 30–34. doi:10.1016/s1010-7940(02)00721-2
Boffetta, P., Ye, W., Boman, G., and Nyrén, O. (2002). Lung cancer risk in a population-based cohort of patients hospitalized for asthma in Sweden. Eur. Respir. J. 19 (1), 127–133. doi:10.1183/09031936.02.00245802
Boyer, M. J., Williams, C. D., Harpole, D. H., Onaitis, M. W., Kelley, M. J., and Salama, J. K. (2017). Improved survival of stage I non–small cell lung cancer: A va central cancer registry analysis. J. Thorac. Oncol. 12 (12), 1814–1823. doi:10.1016/j.jtho.2017.09.1952
Brioude, G., Gust, L., Thomas, P. A., and D’Journo, X. B. (2019). Postoperative complications after major lung resection. Rev. Des. Mal. Respir. 36 (6), 720–737. doi:10.1016/j.rmr.2018.09.004
Brunelli, A., Varela, G., Salati, M., Jimenez, M. F., Pompili, C., Novoa, N., et al. (2010). Recalibration of the revised cardiac risk index in lung resection candidates. Ann. Thorac. Surg. 90 (1), 199–203. doi:10.1016/j.athoracsur.2010.03.042
Brunelli, A., Charloux, A., Bolliger, C. T., Rocco, G., Sculier, J. P., Varela, G., et al. (2009). ERS/ESTS clinical guidelines on fitness for radical therapy in lung cancer patients (surgery and chemo-radiotherapy). Eur. Respir. J. 34 (1), 17–41. doi:10.1183/09031936.00184308
Brunelli, A., Kim, A. W., Berger, K. I., and Addrizzo-Harris, D. J. (2013). Physiologic evaluation of the patient with lung cancer being considered for resectional surgery: Diagnosis and management of lung cancer, 3rd ed: American college of chest physicians evidence-based clinical practice guidelines. Chest 143 (5), e166S–e190S. doi:10.1378/chest.12-2395
Bushardt, R., Massey, E. B., Simpson, T. W., Ariail, J. C., and Simpson, K. N. (2008). Polypharmacy: Misleading, but manageable. CIA 3, 383–389. doi:10.2147/cia.s2468
Camidge, D. R., Dziadziuszko, R., Peters, S., Mok, T., Noe, J., Nowicka, M., et al. (2019). Updated efficacy and safety data and impact of the EML4-ALK fusion variant on the efficacy of alectinib in untreated ALK-positive advanced non–small cell lung cancer in the global phase III ALEX study. J. Thorac. Oncol. 14 (7), 1233–1243. doi:10.1016/j.jtho.2019.03.007
Camidge, D. R., Kim, H. R., Ahn, M. J., Yang, J. C. H., Han, J. Y., Lee, J. S., et al. (2018). Brigatinib versus crizotinib in ALK -positive non–small-cell lung cancer. N. Engl. J. Med. 379 (21), 2027–2039. doi:10.1056/NEJMoa1810171
Carbone, C., Piro, G., Di Noia, V., D’Argento, E., Vita, E., Ferrara, M. G., et al. (2019). Lung and gut microbiota as potential hidden driver of immunotherapy efficacy in lung cancer. Mediat. Inflamm. 2019, 1–10. doi:10.1155/2019/7652014
Cardwell, C. R., Mc Menamin Ú, , Hughes, C. M., and Murray, L. J. (2015). Statin use and survival from lung cancer: A population-based cohort study. Cancer Epidemiol. Biomarkers Prev. 24 (5), 833–841. doi:10.1158/1055-9965.EPI-15-0052
Champiat, S., Lambotte, O., Barreau, E., Belkhir, R., Berdelou, A., Carbonnel, F., et al. (2016). Management of immune checkpoint blockade dysimmune toxicities: A collaborative position paper. Ann. Oncol. 27 (4), 559–574. doi:10.1093/annonc/mdv623
Chang, S. A. (2012). Smoking and type 2 diabetes mellitus. Diabetes & Metabolism J. 36 (6), 399–403. doi:10.4093/dmj.2012.36.6.399
Charlson, M. E., Pompei, P., Ales, K. L., and MacKenzie, C. R. (1987). A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 40 (5), 373–383. doi:10.1016/0021-9681(87)90171-8
Chu, M. P., Ghosh, S., Chambers, C. R., Basappa, N., Butts, C. A., Chu, Q., et al. (2015). Gastric acid suppression is associated with decreased erlotinib efficacy in non–small-cell lung cancer. Clin. Lung Cancer 16 (1), 33–39. doi:10.1016/j.cllc.2014.07.005
Cole, S. P., Bhardwaj, G., Gerlach, J. H., Mackie, J. E., Grant, C. E., Almquist, K. C., et al. (1992). Overexpression of a transporter gene in a multidrug-resistant human lung cancer cell line. Science 258 (5088), 1650–1654. doi:10.1126/science.1360704
Couraud, S., Zalcman, G., Milleron, B., Morin, F., and Souquet, P. J. (2012). Lung cancer in never smokers – a review. Eur. J. Cancer 48 (9), 1299–1311. doi:10.1016/j.ejca.2012.03.007
Créquit, P., Wislez, M., Fleury Feith, J., Rozensztajn, N., Jabot, L., Friard, S., et al. (2015). Crizotinib associated with ground-glass opacity predominant pattern interstitial lung disease: A retrospective observational cohort study with a systematic literature review. J. Thorac. Oncol. 10 (8), 1148–1155. doi:10.1097/JTO.0000000000000577
Cykert, S., Dilworth-Anderson, P., Monroe, M. H., Walker, P., McGuire, F. R., Corbie-Smith, G., et al. (2010). Factors associated with decisions to undergo surgery among patients with newly diagnosed early-stage lung cancer. JAMA 303 (23), 2368–2376. doi:10.1001/jama.2010.793
Dalton, S. O., Steding-Jessen, M., Jakobsen, E., Mellemgaard, A., Østerlind, K., Schüz, J., et al. (2015). Socioeconomic position and survival after lung cancer: Influence of stage, treatment and comorbidity among Danish patients with lung cancer diagnosed in 2004-2010. Acta Oncol. 54 (5), 797–804. doi:10.3109/0284186X.2014.1001037
de Koning, H. J., van der Aalst, C. M., de Jong, P. A., Scholten, E. T., Nackaerts, K., Heuvelmans, M. A., et al. (2020). Reduced lung-cancer mortality with volume CT screening in a randomized trial. N. Engl. J. Med. 382 (6), 503–513. doi:10.1056/NEJMoa1911793
de Torres, J. P., Marín, J. M., Casanova, C., Cote, C., Carrizo, S., Cordoba-Lanus, E., et al. (2011). Lung cancer in patients with chronic obstructive pulmonary disease- incidence and predicting factors. Am. J. Respir. Crit. Care Med. 184 (8), 913–919. doi:10.1164/rccm.201103-0430OC
Derosa, L., Routy, B., Thomas, A. M., Iebba, V., Zalcman, G., Friard, S., et al. (2022). Intestinal Akkermansia muciniphila predicts clinical response to PD-1 blockade in patients with advanced non-small-cell lung cancer. Nat. Med. 28 (2), 315–324. doi:10.1038/s41591-021-01655-5
Divo, M. J., Martinez, C. H., and Mannino, D. M. (2014). Ageing and the epidemiology of multimorbidity. Eur. Respir. J. 44 (4), 1055–1068. doi:10.1183/09031936.00059814
Dreyer, J., Bremer, M., and Henkenberens, C. (2018). Comorbidity indexing for prediction of the clinical outcome after stereotactic body radiation therapy in non-small cell lung cancer. Radiat. Oncol. 13 (1), 213. doi:10.1186/s13014-018-1156-1
Duong, S., and Leung, M. (2011). Should the concomitant use of erlotinib and acid-reducing agents be avoided? The drug interaction between erlotinib and acid-reducing agents. J. Oncol. Pharm. Pract. 17 (4), 448–452. doi:10.1177/1078155210381794
Edwards, B. K., Noone, A. M., Mariotto, A. B., Simard, E. P., Boscoe, F. P., Henley, S. J., et al. (2014a). Annual Report to the Nation on the status of cancer, 1975-2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. Cancer 120 (9), 1290–1314. doi:10.1002/cncr.28509
Edwards, B. K., Noone, A. M., Mariotto, A. B., Simard, E. P., Boscoe, F. P., Henley, S. J., et al. (2014b). Annual Report to the Nation on the status of cancer, 1975-2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. Cancer 120 (9), 1290–1314. doi:10.1002/cncr.28509
Eguchi, T., Bains, S., Lee, M. C., Tan, K. S., Hristov, B., Buitrago, D. H., et al. (2017). Impact of increasing age on cause-specific mortality and morbidity in patients with stage I non–small-cell lung cancer: A competing risks analysis. JCO 35 (3), 281–290. doi:10.1200/JCO.2016.69.0834
Facciolongo, N., Patelli, M., Gasparini, S., Lazzari Agli, L., Salio, M., Simonassi, C., et al. (2016). Incidence of complications in bronchoscopy. Multicentre prospective study of 20,986 bronchoscopies. Monaldi Arch. Chest Dis. 71 (1), 8–14. doi:10.4081/monaldi.2009.370
Falcoz, P. E., Conti, M., Brouchet, L., Chocron, S., Puyraveau, M., Mercier, M., et al. (2007). The Thoracic Surgery Scoring System (Thoracoscore): Risk model for in-hospital death in 15,183 patients requiring thoracic surgery. J. Thorac. Cardiovasc. Surg. 133 (2), 325–332. doi:10.1016/j.jtcvs.2006.09.020
Fang, Y. H., Yang, Y. H., Hsieh, M. J., Hung, M. S., and Lin, Y. C. (2019). Concurrent proton-pump inhibitors increase risk of death for lung cancer patients receiving 1st-line gefitinib treatment - a nationwide population-based study. Cancer Manag. Res. 11, 8539–8546. doi:10.2147/CMAR.S222278
Feinstein, A. R. (1970). The pre-therapeutic classification of co-morbidity in chronic disease. J. Chronic Dis. 23 (7), 455–468. doi:10.1016/0021-9681(70)90054-8
Garcia-Albeniz, X., and Chan, A. T. (2011). Aspirin for the prevention of colorectal cancer. Best. Pract. Res. Clin. Gastroenterol. 25 (4–5), 461–472. doi:10.1016/j.bpg.2011.10.015
Gnjidic, D., Hilmer, S. N., Blyth, F. M., Naganathan, V., Waite, L., Seibel, M. J., et al. (2012). Polypharmacy cutoff and outcomes: Five or more medicines were used to identify community-dwelling older men at risk of different adverse outcomes. J. Clin. Epidemiol. 65 (9), 989–995. doi:10.1016/j.jclinepi.2012.02.018
Goh, I., Lai, O., and Chew, L. (2018). Prevalence and risk of polypharmacy among elderly cancer patients receiving chemotherapy in ambulatory oncology setting. Curr. Oncol. Rep. 20 (5), 38. doi:10.1007/s11912-018-0686-x
Goldkorn, T., Filosto, S., and Chung, S. (2014). Lung injury and lung cancer caused by cigarette smoke-induced oxidative stress: Molecular mechanisms and therapeutic opportunities involving the ceramide-generating machinery and epidermal growth factor receptor. Antioxidants Redox Signal. 21 (15), 2149–2174. doi:10.1089/ars.2013.5469
Gomatou, G., Tzilas, V., Kotteas, E., Syrigos, K., and Bouros, D. (2020). Immune checkpoint inhibitor-related pneumonitis. Respiration 99 (11), 932–942. doi:10.1159/000509941
Gozal, D., Farré, R., and Nieto, F. J. (2015). Putative links between sleep apnea and cancer: From hypotheses to evolving evidence. Chest 148 (5), 1140–1147. doi:10.1378/chest.15-0634
Gray, S. L., Mahoney, J. E., and Blough, D. K. (2001). Medication adherence in elderly patients receiving home health services following hospital discharge. Ann. Pharmacother. 35 (5), 539–545. doi:10.1345/aph.10295
Griggs, J. J., Bohlke, K., Balaban, E. P., Dignam, J. J., Hall, E. T., Harvey, R. D., et al. (2021). Appropriate systemic therapy dosing for obese adult patients with cancer: ASCO guideline update. JCO 21, 00471. doi:10.1200/JCO.21.00471
Grønberg, B. H., Sundstrøm, S., Kaasa, S., Bremnes, R. M., Fløtten, Ø., Amundsen, T., et al. (2010). Influence of comorbidity on survival, toxicity and health-related quality of life in patients with advanced non-small-cell lung cancer receiving platinum-doublet chemotherapy. Eur. J. Cancer 46 (12), 2225–2234. doi:10.1016/j.ejca.2010.04.009
Gurpinar, E., Grizzle, W. E., and Piazza, G. A. (2014). NSAIDs inhibit tumorigenesis, but how? Clin. Cancer Res. 20 (5), 1104–1113. doi:10.1158/1078-0432.CCR-13-1573
Gurwitz, J. H. (2004). Polypharmacy: A new paradigm for quality drug therapy in the elderly? Arch. Intern Med. 164 (18), 1957–1959. doi:10.1001/archinte.164.18.1957
Haanen, JBAG, Carbonnel, F., Robert, C., Kerr, K. M., Peters, S., Larkin, J., et al. (2017). Management of toxicities from immunotherapy: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 28, iv119–42. doi:10.1093/annonc/mdx225
Halter, J. B., Musi, N., McFarland Horne, F., Crandall, J. P., Goldberg, A., Harkless, L., et al. (2014). Diabetes and cardiovascular disease in older adults: Current status and future directions. Diabetes 63 (8), 2578–2589. doi:10.2337/db14-0020
Han, J. Y., Lee, S. H., Yoo, N. J., Hyung, L. S., Moon, Y. J., Yun, T., et al. (2011). A randomized phase II study of gefitinib plus simvastatin versus gefitinib alone in previously treated patients with advanced non-small cell lung cancer. Clin. Cancer Res. 17 (6), 1553–1560. doi:10.1158/1078-0432.CCR-10-2525
Hanania, A. N., Mainwaring, W., Ghebre, Y. T., Hanania, N. A., and Ludwig, M. (2019). Radiation-induced lung injury: Assessment and management. Chest 156 (1), 150–162. doi:10.1016/j.chest.2019.03.033
Hanlon, J. T., Pieper, C. F., Hajjar, E. R., Sloane, R. J., Lindblad, C. I., Ruby, C. M., et al. (2006). Incidence and predictors of all and preventable adverse drug reactions in frail elderly persons after hospital stay. J. Gerontol. A Biol. Sci. Med. Sci. 61 (5), 511–515. doi:10.1093/gerona/61.5.511
Hardy, D., Liu, C. C., Cormier, J. N., Xia, R., and Du, X. L. (2010). Cardiac toxicity in association with chemotherapy and radiation therapy in a large cohort of older patients with non-small-cell lung cancer. Ann. Oncol. 21 (9), 1825–1833. doi:10.1093/annonc/mdq042
He, W., Fang, F., Varnum, C., Eriksson, M., Hall, P., and Czene, K. (2015). Predictors of discontinuation of adjuvant hormone therapy in patients with breast cancer. J. Clin. Oncol. 33 (20), 2262–2269. doi:10.1200/JCO.2014.59.3673
Hendrikx, JJMA, Haanen, JBAG, Voest, E. E., Schellens, J. H. M., Huitema, A. D. R., and Beijnen, J. H. (2017). Fixed dosing of monoclonal antibodies in oncology. Oncologist 22 (10), 1212–1221. doi:10.1634/theoncologist.2017-0167
Hong, S., Lee, J. H., Chun, E. K., Kim, K., Kim, J. W., Kim, S. H., et al. (2019). Polypharmacy, inappropriate medication use, and drug interactions in older Korean patients with cancer receiving first-line palliative chemotherapy. Oncol. 25, e502–e511. theoncologist.2019-0085. doi:10.1634/theoncologist.2019-0085
Hou, H., Sun, D., Liu, K., Jiang, M., Liu, D., Zhu, J., et al. (2019). The safety and serious adverse events of approved ALK inhibitors in malignancies: A meta-analysis. CMAR 11, 4109–4118. doi:10.2147/CMAR.S190098
Howlader, N., Noone, A. M., Krapcho, M., Garshell, J., Miller, D., Altekruse, S. F., et al. (2011). SEER cancer statistics review. Natl. Cancer Inst. Available at: https://seer.cancer.gov/archive/csr/1975_2011/.
Hutchins, L. F., Unger, J. M., Crowley, J. J., Coltman, C. A., and Albain, K. S. (1999). Underrepresentation of patients 65 years of age or older in cancer-treatment trials. N. Engl. J. Med. 341 (27), 2061–2067. doi:10.1056/NEJM199912303412706
Hwang, K. E., Kwon, S. J., Kim, Y. S., Park, D. S., Kim, B. R., Yoon, K. H., et al. (2014). Effect of simvastatin on the resistance to EGFR tyrosine kinase inhibitors in a non-small cell lung cancer with the T790M mutation of EGFR. Exp. Cell Res. 323 (2), 288–296. doi:10.1016/j.yexcr.2014.02.026
Iglesias, P. (2018). Cancer immunotherapy-induced endocrinopathies: Clinical behavior and therapeutic approach. Eur. J. Intern. Med. 47, 6–13. doi:10.1016/j.ejim.2017.08.019
Islam, K. M. M., Jiang, X., Anggondowati, T., Lin, G., and Ganti, A. K. (2015). Comorbidity and survival in lung cancer patients. Cancer Epidemiol. Biomarkers Prev. 24 (7), 1079–1085. doi:10.1158/1055-9965.EPI-15-0036
Izzedine, H., Isnard-Bagnis, C., Launay-Vacher, V., Mercadal, L., Tostivint, I., Rixe, O., et al. (2006). Gemcitabine-induced thrombotic microangiopathy: A systematic review. Nephrol. Dial. Transplant. 21 (11), 3038–3045. doi:10.1093/ndt/gfl507
Jawitz, O. K., Wang, Z., Boffa, D. J., Detterbeck, F. C., Blasberg, J. D., and Kim, A. W. (2017). The differential impact of preoperative comorbidity on perioperative outcomes following thoracoscopic and open lobectomies. Eur. J. Cardiothorac. Surg. 51 (1), 169–174. doi:10.1093/ejcts/ezw239
Jemal, A., Siegel, R., Xu, J., and Ward, E. (2010). Cancer statistics. CA Cancer J. Clin. 60 (5), 277–300. doi:10.3322/caac.20073
Johnson, S. B., Park, H. S., Gross, C. P., and Yu, J. B. (2018). Use of alternative medicine for cancer and its impact on survival. JNCI J. Natl. Cancer Inst. 110 (1), 121–124. doi:10.1093/jnci/djx145
Justeau, G., Gervès-Pinquié, C., Le Vaillant, M., Trzepizur, W., Meslier, N., Goupil, F., et al. (2020). Association between nocturnal hypoxemia and cancer incidence in patients investigated for OSA: Data from a large multicenter French cohort. Chest 158 (6), 2610–2620. doi:10.1016/j.chest.2020.06.055
Khuder, S. A. (2001). Effect of cigarette smoking on major histological types of lung cancer: A meta-analysis. Lung Cancer 31 (2–3), 139–148. doi:10.1016/s0169-5002(00)00181-1
Kuper, H., Adami, H. O., and Trichopoulos, D. (2000). Infections as a major preventable cause of human cancer. J. Intern Med. 248 (3), 171–183. doi:10.1046/j.1365-2796.2000.00742.x
Laskin, J., Crinò, L., Felip, E., Franke, F., Gorbunova, V., Groen, H., et al. (2012). Safety and efficacy of first-line bevacizumab plus chemotherapy in elderly patients with advanced or recurrent nonsquamous non-small cell lung cancer: Safety of avastin in lung trial (MO19390). J. Thorac. Oncol. 7 (1), 203–211. doi:10.1097/JTO.0b013e3182370e02
LeBlanc, T. W., McNeil, M. J., Kamal, A. H., Currow, D. C., and Abernethy, A. P. (2015). Polypharmacy in patients with advanced cancer and the role of medication discontinuation. Lancet Oncol. 16 (7), e333–e341. doi:10.1016/S1470-2045(15)00080-7
Leduc, C., Antoni, D., Charloux, A., Falcoz, P. E., and Quoix, E. (2017). Comorbidities in the management of patients with lung cancer. Eur. Respir. J. 49 (3), 1601721. doi:10.1183/13993003.01721-2016
Lee, L., Cheung, W. Y., Atkinson, E., and Krzyzanowska, M. K. (2011). Impact of comorbidity on chemotherapy use and outcomes in solid tumors: A systematic review. J. Clin. Oncol. 29 (1), 106–117. doi:10.1200/JCO.2010.31.3049
Lee, Y. G., Lee, E., Kim, I., Lee, K. W., Kim, T. M., Lee, S. H., et al. (2015). Cisplatin-based chemotherapy is a strong risk factor for thromboembolic events in small-cell lung cancer. Cancer Res. Treat. 47 (4), 670–675. doi:10.4143/crt.2014.045
Leelakanok, N., Holcombe, A. L., Lund, B. C., Gu, X., and Schweizer, M. L. (2017). Association between polypharmacy and death: A systematic review and meta-analysis. J. Am. Pharm. Assoc. 57 (6), 729–738. doi:10.1016/j.japh.2017.06.002
Lees, J., and Chan, A. (2011). Polypharmacy in elderly patients with cancer: Clinical implications and management. Lancet Oncol. 12 (13), 1249–1257. doi:10.1016/S1470-2045(11)70040-7
Leroy, S., Benzaquen, J., Mazzetta, A., Marchand-Adam, S., Padovani, B., Israel-Biet, D., et al. (2017). Circulating tumour cells as a potential screening tool for lung cancer (the AIR study): Protocol of a prospective multicentre cohort study in France. BMJ Open 7 (12), e018884. doi:10.1136/bmjopen-2017-018884
Li, S., Wang, Z., Huang, J., Fan, J., Du, H., Liu, L., et al. (2016). Systematic review of prognostic roles of body mass index for patients undergoing lung cancer surgery: Does the ‘obesity paradox’ really exist? Eur. J. Cardiothorac. Surg., ezw386. doi:10.1093/ejcts/ezw386
Liang, H. Y., Li, X. L., Yu, X. S., Guan, P., Yin, Z. H., He, Q. C., et al. (2009). Facts and fiction of the relationship between preexisting tuberculosis and lung cancer risk: A systematic review. Int. J. Cancer 125 (12), 2936–2944. doi:10.1002/ijc.24636
Lin, J. J., Ezer, N., Sigel, K., Mhango, G., and Wisnivesky, J. P. (2016). The effect of statins on survival in patients with stage IV lung cancer. Lung Cancer 99, 137–142. doi:10.1016/j.lungcan.2016.07.006
Lüchtenborg, M., Jakobsen, E., Krasnik, M., Linklater, K. M., Mellemgaard, A., and Møller, H. (2012). The effect of comorbidity on stage-specific survival in resected non-small cell lung cancer patients. Eur. J. Cancer 48 (18), 3386–3395. doi:10.1016/j.ejca.2012.06.012
Lugg, S. T., Agostini, P. J., Tikka, T., Kerr, A., Adamas, K., Bishay, E., et al. (2015). Long-term impact of developing a postoperative pulmonary complications after lung surgery. Thorax. 71 (2), 171–176. doi:10.1136/thoraxjnl-2015-207697
Lund, J. L., Sanoff, H. K., Peacock Hinton, S., Muss, H. B., Pate, V., and Stürmer, T. (2018). Potential medication-related problems in older breast, colon, and lung cancer patients in the United States. Cancer Epidemiol. Biomarkers Prev. 27 (1), 41–49. doi:10.1158/1055-9965.EPI-17-0523
Maggiore, R. J., Dale, W., Gross, C. P., Feng, T., Tew, W. P., Mohile, S. G., et al. (2014). Polypharmacy and potentially inappropriate medication use in older adults with cancer undergoing chemotherapy: Effect on chemotherapy-related toxicity and hospitalization during treatment. J. Am. Geriatrics Soc. 62 (8), 1505–1512. doi:10.1111/jgs.12942
Mallappallil, M., Friedman, E. A., Delano, B. G., McFarlane, S. I., and Salifu, M. O. (2014). Chronic kidney disease in the elderly: Evaluation and management. Clin. Pract. (Lond) 11 (5), 525–535. doi:10.2217/cpr.14.46
Mansur, N., Weiss, A., and Beloosesky, Y. (2009). Is there an association between inappropriate prescription drug use and adherence in discharged elderly patients? Ann. Pharmacother. 43 (2), 177–184. doi:10.1345/aph.1L461
Masnoon, N., Shakib, S., Kalisch-Ellett, L., and Caughey, G. E. (2017). What is polypharmacy? A systematic review of definitions. BMC Geriatr. 17 (1), 230. doi:10.1186/s12877-017-0621-2
Mathe, C., Bohacs, A., Duffek, L., Lukacsovits, J., Komlosi, Z. I., Szondy, K., et al. (2011). Cisplatin nephrotoxicity aggravated by cardiovascular disease and diabetes in lung cancer patients. Eur. Respir. J. 37 (4), 888–894. doi:10.1183/09031936.00055110
McGowan, J. V., Chung, R., Maulik, A., Piotrowska, I., Walker, J. M., and Yellon, D. M. (2017). Anthracycline chemotherapy and cardiotoxicity. Cardiovasc Drugs Ther. 31 (1), 63–75. doi:10.1007/s10557-016-6711-0
Mellemgaard, A., Lüchtenborg, M., Iachina, M., Jakobsen, E., Green, A., Krasnik, M., et al. (2015). Role of comorbidity on survival after radiotherapy and chemotherapy for nonsurgically treated lung cancer. J. Thorac. Oncol. 10 (2), 272–279. doi:10.1097/JTO.0000000000000416
Messner, B., and Bernhard, D. (2014). Smoking and cardiovascular disease: Mechanisms of endothelial dysfunction and early atherogenesis. Arteriosclerosis, Thrombosis, Vasc. Biol. 34 (3), 509–515. doi:10.1161/ATVBAHA.113.300156
Michel, L., Rassaf, T., and Totzeck, M. (2019). Cardiotoxicity from immune checkpoint inhibitors. Int. J. Cardiol. Heart Vasc. 25, 100420. doi:10.1016/j.ijcha.2019.100420
Micke, O., Buntzel, J., Kisters, K., Schafer, U., Micke, P., and Mucke, R. (2010). Complementary and alternative medicine in lung cancer patients: A neglected phenomenon? Front. Radiat. Ther. Oncol. 42, 198–205. doi:10.1159/000262477
Millward, M., Cantwell, B., Munro, N., Robinson, A., Corris, P., and Harris, A. (1993). Oral verapamil with chemotherapy for advanced non-small cell lung cancer: A randomised study. Br. J. Cancer 67 (5), 1031–1035. doi:10.1038/bjc.1993.189
Miranda, V., Fede, A., Nobuo, M., Ayres, V., Giglio, A., Miranda, M., et al. (2011). Adverse drug reactions and drug interactions as causes of hospital admission in oncology. J. Pain Symptom Manag. 42 (3), 342–353. doi:10.1016/j.jpainsymman.2010.11.014
Monson, J. M., Stark, P., Reilly, J. J., Sugarbaker, D. J., Strauss, G. M., Swanson, S. J., et al. (1998). Clinical radiation pneumonitis and radiographic changes after thoracic radiation therapy for lung carcinoma. Cancer 82 (5), 842–850. doi:10.1002/(sici)1097-0142(19980301)82:5<842:aid-cncr7>3.0.co;2-l
Morishima, T., Matsumoto, Y., Koeda, N., Shimada, H., Maruhama, T., Matsuki, D., et al. (2019). Impact of comorbidities on survival in gastric, colorectal, and lung cancer patients. J. Epidemiol. 29 (3), 110–115. doi:10.2188/jea.JE20170241
Muscat, J. E., Chen, S. Q., Richie, J. P., Altorki, N. K., Citron, M., Olson, S., et al. (2003). Risk of lung carcinoma among users of nonsteroidal antiinflammatory drugs. Cancer 97 (7), 1732–1736. doi:10.1002/cncr.11242
Myrdal, G., Gustafsson, G., Lambe, M., Hörte, L. G., and Ståhle, E. (2001). Outcome after lung cancer surgery. Factors predicting early mortality and major morbidity. Eur. J. Cardio-Thoracic Surg. 20 (4), 694–699. doi:10.1016/s1010-7940(01)00875-2
Nalbantov, G., Kietselaer, B., Vandecasteele, K., Oberije, C., Berbee, M., Troost, E., et al. (2013). Cardiac comorbidity is an independent risk factor for radiation-induced lung toxicity in lung cancer patients. Radiotherapy Oncol. 109 (1), 100–106. doi:10.1016/j.radonc.2013.08.035
Nalluri, S. R., Chu, D., Keresztes, R., Zhu, X., and Wu, S. (2008). Risk of venous thromboembolism with the angiogenesis inhibitor bevacizumab in cancer patients: A meta-analysis. JAMA 300 (19), 2277–2285. doi:10.1001/jama.2008.656
Nieder, C., MannsăKer, B., Pawinski, A., and Haukland1, E. (2017). Polypharmacy in older patients ≥70 Years receiving palliative radiotherapy. Anticancer Res. 37 (2), 795–799. doi:10.21873/anticanres.11379
Nielsen, S. F., Nordestgaard, B. G., and Bojesen, S. E. (2012). Statin use and reduced cancer-related mortality. N. Engl. J. Med. 367 (19), 1792–1802. doi:10.1056/NEJMoa1201735
Nightingale, G., Hajjar, E., Swartz, K., Andrel-Sendecki, J., and Chapman, A. (2015). Evaluation of a pharmacist-led medication assessment used to identify prevalence of and associations with polypharmacy and potentially inappropriate medication use among ambulatory senior adults with cancer. J. Clin. Oncol. 33 (13), 1453–1459. doi:10.1200/JCO.2014.58.7550
Nilsson, J., Berglund, A., Bergström, S., Bergqvist, M., and Lambe, M. (2017). The role of comorbidity in the management and prognosis in nonsmall cell lung cancer: A population-based study. Acta Oncol. 56 (7), 949–956. doi:10.1080/0284186X.2017.1324213
Noone, A. M., Howlader, N., Krapcho, M., Miller, D., Brest, A., Yu, M., et al. (2015). SEER cancer statistics review. Natl. Cancer Inst. Available at: https://seer.cancer.gov/csr/1975_2015/sections.html.
Pagano, E., Filippini, C., Di Cuonzo, D., Ruffini, E., Zanetti, R., Rosso, S., et al. (2010). Factors affecting pattern of care and survival in a population-based cohort of non-small-cell lung cancer incident cases. Cancer Epidemiol. 34 (4), 483–489. doi:10.1016/j.canep.2010.04.002
Pai, V. B., and Nahata, M. C. (2000). Cardiotoxicity of chemotherapeutic agents: Incidence, treatment and prevention. Drug Saf. 22 (4), 263–302. doi:10.2165/00002018-200022040-00002
Pamoukdjian, F., Aparicio, T., Zelek, L., Boubaya, M., Caillet, P., François, V., et al. (2017). Impaired mobility, depressed mood, cognitive impairment and polypharmacy are independently associated with disability in older cancer outpatients: The prospective Physical Frailty in Elderly Cancer patients (PF-EC) cohort study. J. Geriatric Oncol. 8 (3), 190–195. doi:10.1016/j.jgo.2017.02.003
Papi, A., Casoni, G., Caramori, G., Guzzinati, I., Boschetto, P., Ravenna, F., et al. (2004). COPD increases the risk of squamous histological subtype in smokers who develop non-small cell lung carcinoma. Thorax 59 (8), 679–681. doi:10.1136/thx.2003.018291
Pathak, V., Allender, J. E., and Grant, M. W. (2017). Management of anticoagulant and antiplatelet therapy in patients undergoing interventional pulmonary procedures. Eur. Respir. Rev. 26 (145), 170020. doi:10.1183/16000617.0020-2017
Perazella, M. A. (2012). Onco-nephrology: Renal toxicities of chemotherapeutic agents. Clin. J. Am. Soc. Nephrol. 7 (10), 1713–1721. doi:10.2215/CJN.02780312
Peters, S., Zimmermann, S., and Adjei, A. A. (2014). Oral epidermal growth factor receptor tyrosine kinase inhibitors for the treatment of non-small cell lung cancer: Comparative pharmacokinetics and drug–drug interactions. Cancer Treat. Rev. 40 (8), 917–926. doi:10.1016/j.ctrv.2014.06.010
Petrelli, F., Cortellini, A., Indini, A., Tomasello, G., Ghidini, M., Nigro, O., et al. (2021). Association of obesity with survival outcomes in patients with cancer: A systematic review and meta-analysis. JAMA Netw. Open 4 (3), e213520. doi:10.1001/jamanetworkopen.2021.3520
Popa, M. A., Wallace, K. J., Brunello, A., Extermann, M., and Balducci, L. (2014a). Potential drug interactions and chemotoxicity in older patients with cancer receiving chemotherapy. J. Geriatric Oncol. 5 (3), 307–314. doi:10.1016/j.jgo.2014.04.002
Popa, M. A., Wallace, K. J., Brunello, A., Extermann, M., and Balducci, L. (2014b). Potential drug interactions and chemotoxicity in older patients with cancer receiving chemotherapy. J. Geriatric Oncol. 5 (3), 307–314. doi:10.1016/j.jgo.2014.04.002
Powell, H. A., Tata, L. J., Baldwin, D. R., Stanley, R. A., Khakwani, A., and Hubbard, R. B. (2013). Early mortality after surgical resection for lung cancer: An analysis of the English national lung cancer audit. Thorax 68 (9), 826–834. doi:10.1136/thoraxjnl-2012-203123
Puts, M. T. E., Costa-Lima, B., Monette, J., Girre, V., Wolfson, C., Batist, G., et al. (2009). Medication problems in older, newly diagnosed cancer patients in Canada: How common are they? A prospective pilot study. Drugs Aging 26 (6), 519–536. doi:10.2165/00002512-200926060-00008
Revol, B., Gautier-Veyret, E., Arrivé, C., Fouilhé Sam-Laï, N., McLeer-Florin, A., Pluchart, H., et al. (2020). Pharmacokinetic herb-drug interaction between ginger and crizotinib. Br. J. Clin. Pharmacol. 86 (9), 1892–1893. doi:10.1111/bcp.13862
Riechelmann, R. P., Tannock, I. F., Wang, L., Saad, E. D., Taback, N. A., and Krzyzanowska, M. K. (2007). Potential drug interactions and duplicate prescriptions among cancer patients. JNCI J. Natl. Cancer Inst. 99 (8), 592–600. doi:10.1093/jnci/djk130
Riella, L. V., Paterson, A. M., Sharpe, A. H., and Chandraker, A. (2012). Role of the PD-1 pathway in the immune response: PD-1 in alloimmunity. Am. J. Transplant. 12 (10), 2575–2587. doi:10.1111/j.1600-6143.2012.04224.x
Rosenberger, A., Bickeböller, H., McCormack, V., Brenner, D. R., Duell, E. J., Tjønneland, A., et al. (2012). Asthma and lung cancer risk: A systematic investigation by the international lung cancer consortium. Carcinogenesis 33 (3), 587–597. doi:10.1093/carcin/bgr307
Sarfati, D., Koczwara, B., and Jackson, C. (2016). The impact of comorbidity on cancer and its treatment: Cancer and Comorbidity. CA A Cancer J. Clin. 66 (4), 337–350. doi:10.3322/caac.21342
Sarfati, D. (2012). Review of methods used to measure comorbidity in cancer populations: No gold standard exists. J. Clin. Epidemiol. 65 (9), 924–933. doi:10.1016/j.jclinepi.2012.02.017
Scheen, A. J. (2005). Diabetes mellitus in the elderly: Insulin resistance and/or impaired insulin secretion? Diabetes Metab. 31 (2), 5S27–5S34. doi:10.1016/s1262-3636(05)73649-1
Schutz, F. A. B., Je, Y., Azzi, G. R., Nguyen, P. L., and Choueiri, T. K. (2011). Bevacizumab increases the risk of arterial ischemia: A large study in cancer patients with a focus on different subgroup outcomes. Ann. Oncol. 22 (6), 1404–1412. doi:10.1093/annonc/mdq587
Sciacca, L., Vigneri, R., Tumminia, A., Frasca, F., Squatrito, S., Frittitta, L., et al. (2013). Clinical and molecular mechanisms favoring cancer initiation and progression in diabetic patients. Nutr. Metabolism Cardiovasc. Dis. 23 (9), 808–815. doi:10.1016/j.numecd.2013.05.006
Scripture, C. D., and Figg, W. D. (2006a). Drug interactions in cancer therapy. Nat. Rev. Cancer 6 (7), 546–558. doi:10.1038/nrc1887
Scripture, C. D., and Figg, W. D. (2006b). Drug interactions in cancer therapy. Nat. Rev. Cancer 6 (7), 546–558. doi:10.1038/nrc1887
Seckl, M. J., Ottensmeier, C. H., Cullen, M., Schmid, P., Ngai, Y., Muthukumar, D., et al. (2017). Multicenter, phase III, randomized, double-blind, placebo-controlled trial of pravastatin added to first-line standard chemotherapy in small-cell lung cancer (LUNGSTAR). J. Clin. Oncol. 35 (14), 1506–1514. doi:10.1200/JCO.2016.69.7391
Shah, B. M., and Hajjar, E. R. (2012). Polypharmacy, adverse drug reactions, and geriatric syndromes. Clin. Geriatr. Med. 28 (2), 173–186. doi:10.1016/j.cger.2012.01.002
Shanker, M., Willcutts, D., Roth, J. A., and Ramesh, R. (2010). Drug resistance in lung cancer. Lung Cancer (Auckl) 1, 23–36.
Sharma, M., Holmes, H. M., Mehta, H. B., Chen, H., Aparasu, R. R., Shih, Y. T., et al. (2019). The concomitant use of tyrosine kinase inhibitors and proton pump inhibitors: Prevalence, predictors, and impact on survival and discontinuation of therapy in older adults with cancer. Cancer 125 (7), 1155–1162. doi:10.1002/cncr.31917
Sharma, M., Loh, K. P., Nightingale, G., Mohile, S. G., and Holmes, H. M. (2016). Polypharmacy and potentially inappropriate medication use in geriatric oncology. J. Geriatric Oncol. 7 (5), 346–353. doi:10.1016/j.jgo.2016.07.010
Song, X., Varker, H., Eichelbaum, M., Stopfer, P., Shahidi, M., Wilson, K., et al. (2011). Treatment of lung cancer patients and concomitant use of drugs interacting with cytochrome P450 isoenzymes. Lung Cancer 74 (1), 103–111. doi:10.1016/j.lungcan.2011.01.016
Steéphan, F., Boucheseiche, S., Hollande, J., Flahault, A., Cheffi, A., Bazelly, B., et al. (2000). Pulmonary complications following lung resection: A comprehensive analysis of incidence and possible risk factors. Chest 118 (5), 1263–1270. doi:10.1378/chest.118.5.1263
Sud, S., Lai, P., Zhang, T., Clemons, M., and Wheatley-Price, P. (2015). Chemotherapy in the oldest old: The feasibility of delivering cytotoxic therapy to patients 80years old and older. J. Geriatric Oncol. 6 (5), 395–400. doi:10.1016/j.jgo.2015.07.002
Sugiura, H., Takeda, A., Hoshi, T., Kawabata, Y., Sayama, K., Jinzaki, M., et al. (2012). Acute exacerbation of usual interstitial pneumonia after resection of lung cancer. Ann. Thorac. Surg. 93 (3), 937–943. doi:10.1016/j.athoracsur.2011.12.010
Tammemagi, C. M., Neslund-Dudas, C., Simoff, M., and Kvale, P. (2004). In lung cancer patients, age, race-ethnicity, gender and smoking predict adverse comorbidity, which in turn predicts treatment and survival. J. Clin. Epidemiol. 57 (6), 597–609. doi:10.1016/j.jclinepi.2003.11.002
Timmers, L., Boons, CCLM, Moes-ten Hove, J., Smit, E. F., van de Ven, P. M., Aerts, J. G., et al. (2015). Adherence, exposure and patients’ experiences with the use of erlotinib in non-small cell lung cancer. J. Cancer Res. Clin. Oncol. 141 (8), 1481–1491. doi:10.1007/s00432-015-1935-0
Toffart, A. C., Belaiche, S., Moro-Sibilot, D., Couraud, S., and Sakhri, L. (2014). Impact of lung cancer treatments on renal function. Rev. Mal. Respir. 31 (10), 1003–1012. doi:10.1016/j.rmr.2014.03.008
Turner, J. P., Jamsen, K. M., Shakib, S., Singhal, N., Prowse, R., and Bell, J. S. (2016). Polypharmacy cut-points in older people with cancer: How many medications are too many? Support Care Cancer 24 (4), 1831–1840. doi:10.1007/s00520-015-2970-8
Turner, J. P., Shakib, S., Singhal, N., Hogan-Doran, J., Prowse, R., Johns, S., et al. (2014). Prevalence and factors associated with polypharmacy in older people with cancer. Support. Care Cancer 22 (7), 1727–1734. doi:10.1007/s00520-014-2171-x
Veitch, A. M., Vanbiervliet, G., Gershlick, A. H., Boustiere, C., Baglin, T. P., Smith, L. A., et al. (2016). Endoscopy in patients on antiplatelet or anticoagulant therapy, including direct oral anticoagulants: British society of gastroenterology (BSG) and European society of gastrointestinal endoscopy (ESGE) guidelines. Gut 65 (3), 374–389. doi:10.1136/gutjnl-2015-311110
Wang, K., Eblan, M. J., Deal, A. M., Lipner, M., Zagar, T. M., Wang, Y., et al. (2017). Cardiac toxicity after radiotherapy for stage III non–small-cell lung cancer: Pooled analysis of dose-escalation trials delivering 70 to 90 gy. JCO 35 (13), 1387–1394. doi:10.1200/JCO.2016.70.0229
Wang, S., Wong, M. L., Hamilton, N., Davoren, J. B., Jahan, T. M., and Walter, L. C. (2012). Impact of age and comorbidity on non-small-cell lung cancer treatment in older veterans. J. Clin. Oncol. 30 (13), 1447–1455. doi:10.1200/JCO.2011.39.5269
Williams, G. R., Deal, A. M., Nyrop, K. A., Pergolotti, M., Guerard, E. J., Jolly, T. A., et al. (2015). Geriatric assessment as an aide to understanding falls in older adults with cancer. Support Care Cancer 23 (8), 2273–2280. doi:10.1007/s00520-014-2598-0
Woodall, M. J., Neumann, S., Campbell, K., Pattison, S. T., and Young, S. L. (2020). The effects of obesity on anti-cancer immunity and cancer immunotherapy. Cancers 12 (5), 1230. doi:10.3390/cancers12051230
Wu, D., Hu, D., Chen, H., Shi, G., Fetahu, I. S., Wu, F., et al. (2018). Glucose-regulated phosphorylation of TET2 by AMPK reveals a pathway linking diabetes to cancer. Nature 559 (7715), 637–641. doi:10.1038/s41586-018-0350-5
Wyatt, G. K., Friedman, L. L., Given, C. W., Given, B. A., and Beckrow, K. C. (1999). Complementary therapy use among older cancer patients. Cancer Pract. 7 (3), 136–144. doi:10.1046/j.1523-5394.1999.07305.x
Yang, C. P., Gallagher, R. P., Weiss, N. S., Band, P. R., Thomas, D. B., and Russell, D. A. (1989). Differences in incidence rates of cancers of the respiratory tract by anatomic subsite and histologic type: An etiologic implication. J. Natl. Cancer Inst. 81 (23), 1828–1831. doi:10.1093/jnci/81.23.1828
Yu, X., Pan, Y., Ma, H., and Li, W. (2013). Simvastatin inhibits proliferation and induces apoptosis in human lung cancer cells. Oncol. Res. 20 (8), 351–357. doi:10.3727/096504013X13657689382897
Yu, Y. H., Liao, C. C., Hsu, W. H., Chen, H. J., Liao, W. C., Muo, C. H., et al. (2011). Increased lung cancer risk among patients with pulmonary tuberculosis: A population cohort study. J. Thorac. Oncol. 6 (1), 32–37. doi:10.1097/JTO.0b013e3181fb4fcc
Zarifa, A., Albittar, A., Kim, P. Y., Hassan, S., Palaskas, N., Iliescu, C., et al. (2019). Cardiac toxicities of anticancer treatments: Chemotherapy, targeted therapy and immunotherapy. Curr. Opin. Cardiol. 34 (4), 441–450. doi:10.1097/HCO.0000000000000641
Keywords: comorbidities, lung cancer, survival, polypharmacy, drug-drug interaction
Citation: Pluchart H, Chanoine S, Moro-Sibilot D, Chouaid C, Frey G, Villa J, Degano B, Giaj Levra M, Bedouch P and Toffart A-C (2024) Lung cancer, comorbidities, and medication: the infernal trio. Front. Pharmacol. 14:1016976. doi: 10.3389/fphar.2023.1016976
Received: 11 August 2022; Accepted: 25 September 2023;
Published: 21 February 2024.
Edited by:
Yi Guo, University of Florida, United StatesReviewed by:
Rutugandha Paranjpe, Boston Scientific, United StatesBrian A. Wall, Rutgers, The State University of New Jersey, United States
Copyright © 2024 Pluchart, Chanoine, Moro-Sibilot, Chouaid, Frey, Villa, Degano, Giaj Levra, Bedouch and Toffart. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hélène Pluchart, helene.pluchart@sfr.fr