 Tomasz Gólczewski
Tomasz Gólczewski Anna M. Stecka
Anna M. Stecka Elżbieta M. Grabczak2
Elżbieta M. Grabczak2 Rafał Krenke
Rafał Krenke- 1Nalecz Institute of Biocybernetics and Biomedical Engineering, Polish Academy of Sciences, Warsaw, Poland
- 2Department of Internal Medicine, Pulmonary Diseases and Allergy, Medical University of Warsaw, Warsaw, Poland
Objectives: Although dyspnea is the most common symptom of pleural effusion (PE), its physiological basis has not yet been fully elucidated. The aim of this work is to investigate the cause of dyspnea before therapeutic thoracentesis (TT) by analyzing the lack of dyspnea relief after TT.
Methods: We retrospectively analyzed data gathered during TT. Among others, our database includes measurements of instantaneous pleural pressure (Ppl) in the ipsilateral hemithorax and airflow in the mouth (during TT), as well as arterial gas tensions (AGT) and dyspnea characterized quantitatively via the Modified Borg Scale (before and after TT). As the Borg scale is a subjective measure, the change in dyspnea (dB) was used in reliable quantitative analyses. Differences in various parameters and their changes between patients who reported dyspnea relief and the other patients (the YES and NO groups, respectively) were studied. Additionally, correlations between dB and these parameters (and their changes) were studied.
Results: Only the amplitude of Ppl changes related to breathing after TT was significantly different (higher) in group NO than in group YES (p < 0.003; the large effect size). dB correlated with this amplitude and the volume of withdrawn fluid (r = −0.51 and 0.51, respectively), but it correlated with neither changes in AGT nor minute ventilation.
Conclusion: The results suggest that the key mechanism of dyspnea in patients with malignant PE is related to reduced total lung compliance due to collapse of a lung part, leading to an increase in the work of breathing required to maintain adequate minute ventilation.
1 Introduction
Dyspnea is reported by approximately 50%–65% of patients with malignant pleural effusion (PE), compromising their quality of life and often being the primary reason for seeking emergency care (Antony et al., 2001; Piggott et al., 2023). Although various physiological mechanisms of dyspnea in patients with PE have been considered for decades, the key mechanism seems to remain unclear (Parshall et al., 2012; Thomas et al., 2015).
The accumulation of pleural fluid is associated with compression of the ipsilateral lung, which may result in increased ventilation‒perfusion mismatch and impaired gas exchange. However, neither low arterial O2 (PaO2) nor elevated CO2 (PaCO2) partial pressures can be responsible for dyspnea in patients with PE, as both may either decrease or increase after therapeutic thoracentesis (TT) despite dyspnea relief, and the changes in PaO2 and PaCO2 do not correlate (Karetzky et al., 1978; Brandstetter and Cohen, 1979; Agustí et al., 1997; Stecka et al., 2018; Muruganandan et al., 2020; Taylor et al., 2021; Zielinska-Krawczyk et al., 2022). Therefore, another cause of dyspnea in PE patients should be considered.
The hydrostatic pressure of the pleural fluid exerted on the ipsilateral hemidiaphragm may lead to flattening or even reversal, significantly impairing diaphragm function; likewise, a large volume of pleural fluid puts pressure on the chest wall (overstretching intercostal muscles) and mediastinum, resulting in its contralateral shift and changes in respiratory mechanics (Thomas et al., 2015; Skaarup et al., 2020). Recent studies have posited that dyspnea in PE may stem primarily from abnormal ipsilateral hemidiaphragm function. Consequently, the reduction in dyspnea following TT may be related to the restoration of the ipsilateral hemidiaphragm shape and function (Muruganandan et al., 2020; Skaarup et al., 2020; Muruganandan et al., 2023). This, however, has not been supported by a more recent study (Fjaellegaard et al., 2024). On the other hand, although dyspnea relief can be statistically correlated with improvement in the ipsilateral hemidiaphragm shape and function, these changes may not be causally linked, i.e., TT could influence both dyspnea and hemidiaphragm function independently. This could explain why dyspnea does not resolve in some patients despite the hemidiaphragm returning to its normal upward curve after TT (Muruganandan et al., 2020; Psallidas et al., 2017).
Given the difficulties in determining the physiological causes of dyspnea before TT, we propose a kind of reversal of the problem, i.e., investigation of the reasons for the lack of dyspnea relief after TT. We attempted to use our own database to study this problem. This database contains various data gathered during TT, including records of the pleural pressure (Ppl) enabling the determination of the amplitude of Ppl changes related to breathing (Ppl_ampl).
As it is shown in Figure 1A, the work done against elastic forces during one breath is approximately equal to 0.5⋅Ppl_ampl⋅VT. As the minute work, commonly called work of breathing (WOB), is equal to the work done in one breath multiplied by the respiratory rate (RR), the elastic WOB (WOBe) is equal to 0.5⋅Ppl_ampl⋅VT⋅RR. Since the minute ventilation is equal to VT⋅RR, we have:

Figure 1. Influence of pleural effusion on work of breathing – schematic diagrams. Bold red and blue curves – schematic nonlinear pressure-volume curves for the chest wall and lungs, respectively, characterizing their static, nonlinear compliances; V – the current volume of the chest cavity/lungs; FRC – functional residual capacity; VT – a fixed tidal volume; Ppl – pleural pressure, Ppl_FRC – Ppl at FRC; P – Patm-Ppl in the case of the chest wall and Ppl-Patm in the case of lungs, Ppl_ampl – the change in Ppl required to inspire VT; W – work done during one breath; VPE – the pleural fluid volume; CR and CL – volume-dependent compliance of the right and left lung, respectively; Ccollapsed – decrease in the (left) lung compliance caused by ‘elimination’ of a lung part due to its collapse. (A) To increase the lung volume by ΔV, respiratory muscles have to develop the pressure P1 that decreases Ppl to the value that corresponds to FRC+ΔV. According to the laws of physics, the work ΔW1 done by these muscles is equal to P1⋅ΔV. Further increase of V by next ΔV requires pressure P2 and the work ΔW2 is equal to P2⋅ΔV, etc. The total work done by the muscles to inspire VT is the sum of W1, W2, W3 … Wn, i.e., it is equal to the area of the grey triangle that is equal to 0.5⋅VT⋅Ppl_ampl. (B) Pleural fluid takes up space in the chest decreasing the chest cavity volume, which leads to a downward shift of the chest wall characteristics. Collapse of a lung part leads to compression of the lung characteristics. Although the above leads to a decrease in FRC, its value corresponds to smaller differential lung compliance. As a result, Ppl_ampl necessary for the required VT and WOB (grey triangle area) are greater than in the healthy respiratory system. (C) Pleural fluid withdrawal causes return of the chest wall characteristics to the original position; however, if the collapsed lung part is not recruited, the characteristics of the lungs does not change. FRC increases to the value for which this characteristics is much more horizontal, i.e., the differential compliance is smaller. As a result, Ppl_ampl necessary for the required VT and W are greater than before the fluid withdrawal. (D–F) present schematically contributions of individual lungs to the total lung compliance presented in (A), (B), (C), respectively. The magnitude of arrows indicates contributions of individual hemidiaphragms to W. (D) The pressure-volume curve for lungs illustrates the sum of volume-dependent CR and CL. (E) CL(B) is smaller than CL(A) by Ccollapsed due to collapse of a lung part; therefore, W must increase to maintain VT. (F) If the atelectatic part of the left lung is not recruited, the ventilated part must overexpand to take place of withdrawn pleural fluid; therefore, since CL is volume-dependent, CL(C) is smaller than CL(B). As a consequence, W is greater, not smaller, than before therapeutic thoracentesis.
Thus, if VE remains relatively stable, Ppl_ampl can be used to characterize WOBe. Consequently, this study is particularly focused on analyzing the relationship between dyspnea and WOBe.
2 Materials and methods
2.1 Patients
This study involved a retrospective analysis of data obtained from a comprehensive prospective project in which multiple physiological parameters were measured before, during, and after TT. This project received approval from the Institutional Review Board (KB 105/2012) and was registered on ClinicalTrials.gov (NCT02192138). Medical procedures were conducted at the Department of Internal Medicine, Pulmonary Diseases and Allergy of the Medical University of Warsaw.
The data used for analysis were obtained from patients with malignant PE referred to the hospital for TT. The inclusion criteria were as follows: (1) age between 18 and 85 years, (2) symptomatic pleural effusion occupying at least one-third of the hemithorax determined by posteroanterior chest radiogram, (3) the severity of symptoms (including dyspnea) warranting TT, (4) absence of contraindication for TT, and (5) signed consent to participate in the study. The following exclusion criteria were applied: (1) poor general health condition warranting non-extension of the procedure, (2) mechanical ventilation due to respiratory failure, and (3) unstable hemodynamic or respiratory status not related to pleural effusion.
2.2 Measurements and parameters
TT was performed with the patient in a sitting position. The pleural fluid was withdrawn intermittently, with 1-min breaks for measurement purposes.
Dyspnea was assessed just before and after TT via the Modified 10-point Borg Scale. Dyspnea relief associated with TT was quantified by the difference (ΔB) between the Borg Scores before (Bpre) and after TT (Bpost), i.e., ΔB = Bpre− Bpost. The instantaneous values of Ppl in the ipsilateral hemithorax (digital pleural manometer, IBBE, Poland) and airflow through the mouth (modified LungTest 1,000 spirometer, MES, Poland) were recorded and synchronized for further analyses. VE was calculated as the sum of tidal volumes during the period of the spirometric measurement divided by the duration of this period. The median value of Ppl_ampl after TT (Ppl_ampl post) was construed as an index of WOBe at the end of the procedure.
Arterial blood gases were measured 1 hour before and 1 hour after TT. Arterial blood samples were collected from the radial or ulnar artery of patients breathing ambient air. Blood samples were analyzed within 15 minutes after collection using the Blood Gas Analyzer ABL 800 FLEX (Medical ApS, Brønshøj, Denmark).
More details about patients and methods can be found in previous articles (e.g., Zielinska-Krawczyk et al., 2018; Zielinska-Krawczyk et al., 2022).
2.3 Data analyses
Since dyspnea is a subjective sensation and may be perceived and reported differently by each patient, the absolute value of dyspnea score might not be directly comparable between patients. The relative dyspnea index that are ΔB and ΔB/Bpre seem to be better parameters for objective quantitative analysis; therefore, they were compared with other parameters and their changes.
Since dyspnea relief after TT was observed in only some patients, we divided our patients into two groups: the YES group consisted of patients who reported dyspnea relief (i.e., ΔB>0) and the NO group consisted of the other patients (ΔB≤0). Then, we analyzed which of the following parameters (or their changes) differentiated these groups: PaO2, PaCO2, VE, the volume of withdrawn pleural fluid (Vw) and Ppl_ampl post.
If a patient reported insignificant dyspnea before TT, i.e., if Bpre≤2, he/she could not report significant ΔB regardless of the true degree of dyspnea relief. This might distort possible correlations between ΔB and other parameters or their changes; therefore, the main analyses were performed for patients who reported Bpre>2, however correlations were also calculated for all patients.
2.4 Statistical methods
Statistical analyses were performed via the Statistica 10 package (StatSoft Inc.). As some of the analyzed data had distributions different from the normal distribution, nonparametric statistical methods were used. Statistical significance was considered when p < 0.05. The Spearman correlation coefficient was used to estimate associations between the analyzed parameters. The difference in parameters between the NO and YES groups was assessed via the Mann–Whitney U test, and the Glass rank-biserial correlation (rg) was used to estimate the effect size; if rg > 0.45, then the effect size was interpreted as large.
3 Results
In general, data for 41 patients were analyzed; however, due to technical issues, arterial gasometry could not be done before or after TT in 14 patients. Table 1 presents the characteristics of the whole sample, and the YES and NO groups separately. Neither arterial blood gases (Figure 2B) nor VE nor their changes differed among these groups (Table 1). B pre and Vw were greater in the YES group; nevertheless, these differences were statistically insignificant. Moreover, although dispersion of PaO2 values was smaller in patients who reported not severe dyspnea before TT, neither the median values nor PaO2 changes were different (Figure 2A).

Table 1. Characteristics of the groups.
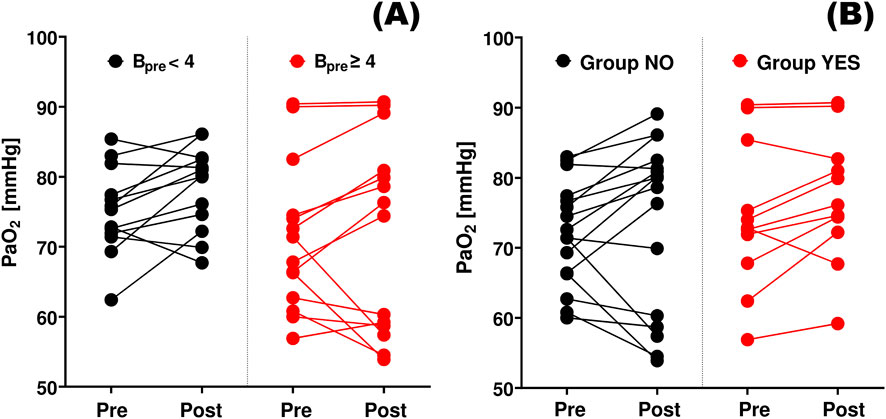
Figure 2. Changes in arterial oxygen tension. PaO2 pre and PaO2 post – the arterial oxygen tensions measured before (Pre) and after (Post) thoracentesis, respectively. (A) Bpre < 4: patients who reported no to moderate dyspnea before thoracentesis (Borg score <4); Bpre ≥ 4: patients with more severe dyspnea. (B) Group NO: patients who reported no dyspnea relief or worsening after therapeutic thoracentesis, Group YES – patients who reported dyspnea relief.
Ppl_ampl post was the only parameter that significantly differentiated these groups: it was much greater in the NO group than in the YES group (Table 1). The association between Ppl_ampl post and dyspnea is additionally confirmed by the statistically significant inverse correlation between Ppl_ampl post and ΔB (Table 2; Figure 3A) and the significant positive correlation between Ppl_ampl post and Bpost in patients reporting more considerable dyspnea before TT, i.e., in 33 patients with Bpre>2 (Table 3; Figure 3B).
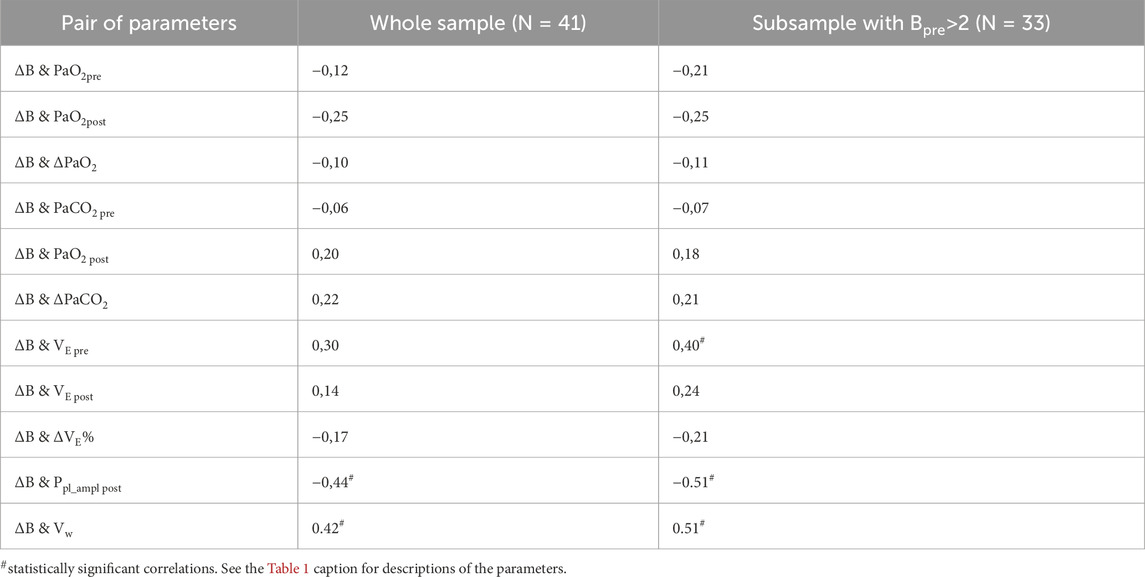
Table 2. Spearman’s correlations between changes in dyspnea (ΔB) and other parameters.
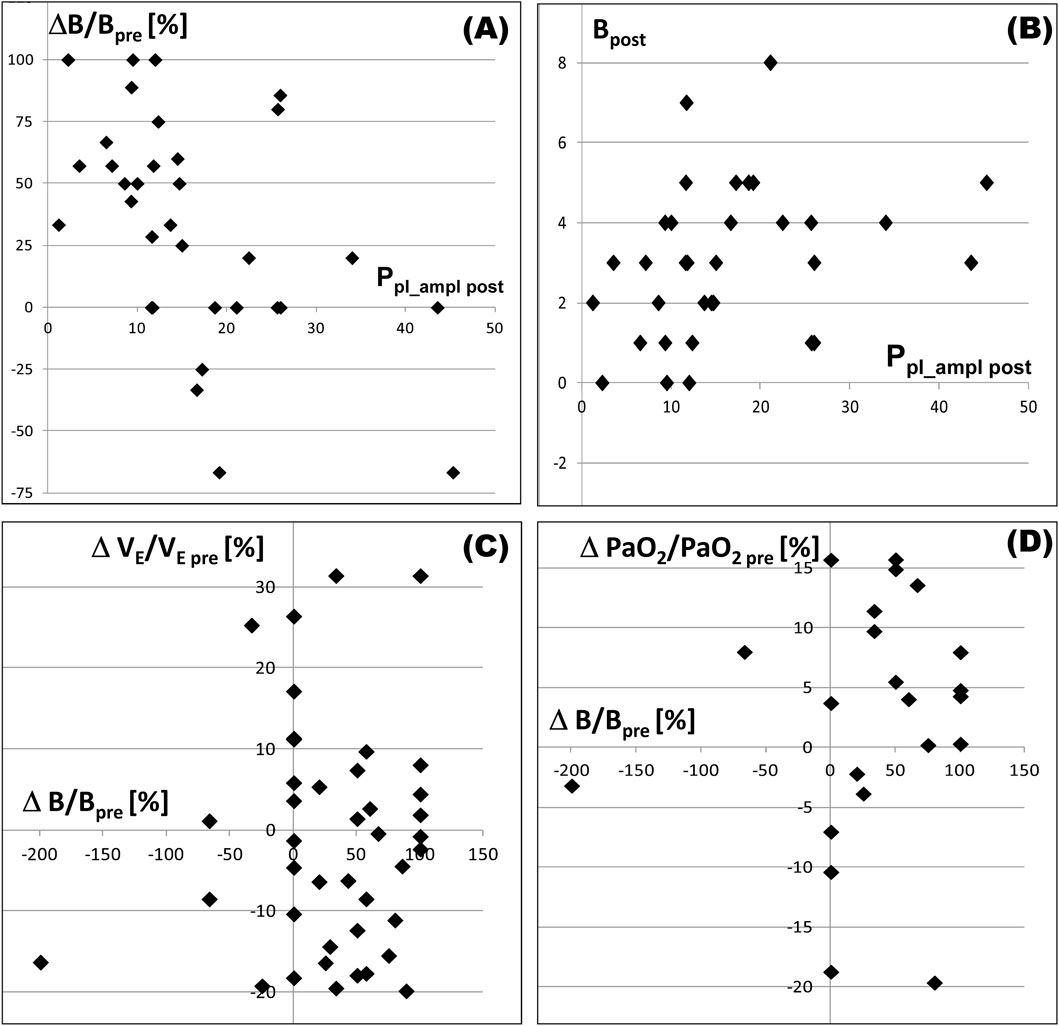
Figure 3. Relationships between selected parameters in patients with Bpre>2. Subscripts “pre”and “post”indicate the value of a parameter before and after pleural fluid withdrawal, respectively; Ppl_ampl post – the amplitude of pleural pressure changes related to breathing (after the fluid withdrawal); (B) Borg score characterizing dyspnea reported by a patient; ΔB/Bpre – relative dyspnea relief, i.e., the decrease in B (=Bpre-Bpost) caused by pleural fluid withdrawal expressed as percentage of Bpre; ΔVE/VE pre – relative minute ventilation (VE) increase (=VE post-VE pre) expressed as percentage of VE pre; ΔPaO2/PaO2 pre – PaO2 increase expressed as percentage of PaO2 pre. (A) there is an inverse correlation between dyspnea relief and the amplitude; (B), there is a positive correlation between dyspnea after pleural fluid withdrawal and the amplitude; (C,D) – dyspnea relief is associated with neither changes in VE nor in PaO2.
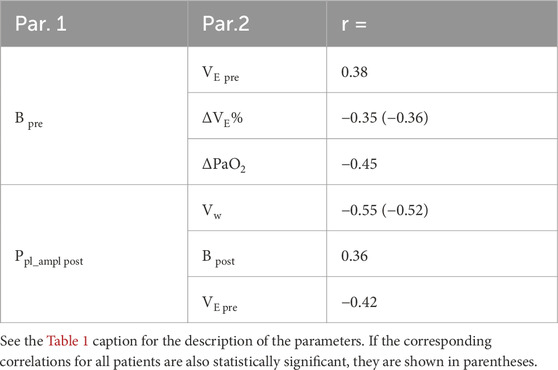
Table 3. Other statistically significant Spearman’s correlations for the Bpre>2 subsample.
Although the minute ventilation (both VE pre, VE post and ΔVE) did not differ significantly between the YES and NO groups (Table 1), VE pre was statistically significantly correlated with ΔB (Table 2) and B pre (Table 3) in the subsample Bpre>2. Table 3 shows other statistically significant correlations.
4 Discussion
There are a number of underlying causes of dyspnea, including various cardiovascular, neuromuscular or respiratory disorders, pain, psychiatric disorders and others (Coccia et al., 2016; Beaudry et al., 2022; Ritter et al., 2024). Some of them may also be present in patients with PE. Nevertheless, since pleural fluid withdrawal usually alleviates dyspnea (the high correlation between ΔB and Vw, Table 2), the presence of this fluid should be suspected as the main cause in patients with PE not related to congestive heart failure (dyspnea does not correlate with the pleural fluid volume in patients with cardiac-related PE (Wijayaratne et al., 2024)); however, this explains only the reason for dyspnea but does not explain its pathophysiological mechanism, i.e., the direct cause.
Changes of PaO2 and PaCO2 during TT appeared to be not associated with changes in dyspnea (Table 2); moreover, these changes were insignificant and could be both positive and negative (Table 1), even in the group YES (Figure 2B), which agrees with results of in silico studies (Gólczewski et al., 2025). If low PaO2 pre was indeed a significant cause of considerable dyspnea before TT, more significant dyspnea relief (i.e., greater ΔB) after TT should be associated with more significant improvement of PaO2 (i.e., greater ΔPaO2) giving a significant positive correlation, which was not observed (Table 2; Figure 3D). Additionally, the higher the level of dyspnea was before TT, the less significant the PaO2 improvement was observed (inverse correlation between Bpre and ΔPaO2, Table 3), whereas if low PaO2 would be the reason for dyspnea, one could expect more significant improvement in patients with higher Bpre. Thus, our results confirm previous suggestions that low PaO2 and/or elevated PaCO2 are not directly responsible for dyspnea in patients with PE not related to cardiovascular diseases.
In our patients with considerable dyspnea at baseline (i.e., Bpre>2), VE pre demonstrated a statistically significant positive correlation with both Bpre (Table 3) and ΔB (Table 2). This might suggest that increased VE could be perceived by patients as dyspnea. However, if increased VE were indeed a substantial cause of dyspnea, relief of dyspnea would be associated with a decrease in VE. In, fact, changes in VE were generally small and not associated with ΔB (Figure 3C). Furthermore, they could be both positive and negative, even in the group YES (Table 1). Additionally, ΔVE% exhibited a negative correlation with Bpre (Table 3). The above proves that more intensive ventilation could not be a substantial cause of the feeling of dyspnea in our patients.
Thus, the observed correlations (Table 2 and 3) between B pre and ΔB on the one hand, and VE pre, ΔVE% and ΔPaO2 on the other hand were likely related to secondary associations only.
Ppl_ampl post was the only parameter that was significantly different between the YES and NO groups (Table 1) and was correlated with dyspnea change (ΔB in Table 2) as well as with dyspnea after TT (Bpost in Table 3). The observed inverse correlation between ΔB and Ppl_ampl post (Table 2) suggests that the more intensive the work of the respiratory muscles was after TT, the smaller the relief of dyspnea was reported. Moreover, high or even very high Ppl_ampl post in patients in the group NO suggests that inspiratory muscles worked very effectively in these patients. This phenomenon is most likely related to the ipsilateral hemidiaphragm, as it is the main inspiratory muscle producing Ppl changes in this cavity (Figure 1F). Thus, on the one hand, patients from this group reported either no dyspnea relief (10 patients) or even dyspnea increase (5 patients); on the other hand, the respiratory muscles worked very effectively since they could produce such a high Ppl_ampl post. This seems to confirm the most recent results reported by Fjaellegaard et al. (Fjaellegaard et al., 2024) that neither the normal shape nor movement of the diaphragm after TT is associated with potential dyspnea relief, as it has been suggested lately by other authors (Muruganandan et al., 2020; Skaarup et al., 2020; Muruganandan et al., 2023).
In general, WOBe depends directly on Ppl_ampl according to the fundamental equation WOBe = 0.5⋅Ppl_ampl⋅VE. Thus, regardless of which respiratory muscles are responsible for such high Ppl_ampl post in patients in the group NO, these patients may report dyspnea due to high WOBe. In the YES group, WOBe was significantly lower after TT, and those patients reported dyspnea relief. The association between post-TT dyspnea and post-TT WOBe seems to be additionally confirmed by the correlation between Bpost and Ppl_ampl post (Table 3). Note, however, that although this correlation is statistically significant, it is not very high. This may suggest that either other factors could also contribute to dyspnea or subjective feeling of increased WOBe was different in individual patients or both.
Unfortunately, WOBe before TT cannot be assessed on the basis of Ppl_ampl measured in the ipsilateral hemithorax because the ipsilateral hemidiaphragm has an insignificant contribution to respiration before TT (Figure 3B), and WOBe is mostly done by the contralateral hemidiaphragm; in particular, Ppl_ampl in the ipsilateral hemithorax may have negative values when the ipsilateral hemidiaphragm is inverted (which would yield a ridiculous result, i.e., a ‘negative WOBe’). Nevertheless, WOBe before pleural fluid withdrawal can be assessed on the basis of the laws of physics since, in general:
where Ctot is the total respiratory system compliance. Thus, since neither VE (Table 1) nor the median RR (Zielinska-Krawczyk et al., 2018) changes significantly during TT, changes in Ctot are responsible for changes in WOBe. Before TT, the pleural fluid causes collapse of a part of the ipsilateral lung or even the whole ipsilateral lung is not ventilated; this means that Ctot is reduced proportionally. According to the above formula, WOBe is increased to the same extent. Moreover, lung compliance is nonlinear. Therefore, the same VT ventilated smaller amount of lungs requires an additional increase of WOBe (Figure 1C).
The pleural fluid compresses both the lungs and bronchi; therefore, the total WOB = WOBe + WOBr (where WOBr is the resistive work) is additionally increased by raised work against bronchi resistance. Moreover, under physiological conditions, ribcage elastance helps inspiration, whereas additional effort is required if the thoracic cavity is expanded by PE over the volume for which the trans-wall pressure is positive at the FRC. Thus, WOB has to be increased before TT, and patients can interpret this increase as dyspnea regardless of the other possible causes.
For reasons discussed above, before TT, WOB must be increased at least owing to the collapse of a part of the lungs (Figures 1B,E), thoracic cavity expansion and narrowed bronchi. After TT, the collapsed parts can be either recruited or not. If these parts are recruited, then Ctot increases to the normal value (Figures 1A,D). In consequence, Ppl_ampl = VT/Ctot can be small, the required WOBe decreases and dyspnea is reduced as in the group YES. However, if these parts remain collapsed after TT, Ctot is still small, and thus (Figures 1C,F).
a. WOBe cannot decrease and dyspnea remains,
b. Ppl_ampl in the contralateral hemithorax has to be high because of the small Ctot,
c. as the ipsilateral hemidiaphragm is curved upward at least as much as the contralateral hemidiaphragm, high Ppl_ampl in the ipsilateral hemithorax, similar to Ppl_ampl in the contralateral hemithorax, may be generated,
d. lung compliance nonlinearity may cause an increase in WOBe (Figure 1C) leading to dyspnea increase, not relief.
The above can explain the lack of dyspnea relief and intriguing dyspnea increase after TT in the group NO if dyspnea in those patients before TT has been caused just by increased WOBe.
Concluding, either dyspnea is reduced (ΔB is large) because the WOBe and Ppl_ampl post are small after TT (the YES group in Table 1) or WOBe is still large, dyspnea persists (ΔB≤0) and Ppl_ampl post is high (the NO group). Certainly, some collapsed parts can be recruited, and the others remain collapsed; thus, both ΔB and Ppl_ampl can be moderate. As the result, a negative correlation between ΔB and Ppl_ampl post (Table 2) and a positive correlation between Ppl_ampl post and Bpost (Table 3) are observed.
It should be noted that if the mediastinum is very compliant, Ppl need not be very low despite high Ppl_ampl post (Gólczewski et al., 2025). Indeed, in such a case, a lack of collapsed lung part recruitment requires high Ppl_ampl post to maintain VE at a necessary level, whereas the space in the ipsilateral hemithorax that has been occupied by pleural fluid may be partly filled with the contralateral lung, which protects against excessive Ppl fall and seemingly suggests an expandable lung. This may partly explain the lack of differences in post-TT dyspnea relief between patients with expandable and non-expandable lung (Petersen et al., 2024). Thus, not only Ppl but also Ppl_ampl should be monitored during TT, at least to differentiate expandable and non-expandable lungs.
Although not very high, the statistically significant positive correlation between Bpre and VE pre in the subsample Bpre>2 (Table 3) seems to confirm that WOBe is responsible for dyspnea in PE, as the greater the VE pre value is, the greater the WOBe. It is not clear, however, why changes in dyspnea, i.e., ΔB, are not associated with ΔVE (Table 2), whereas ΔVE is inversely correlated with Bpre (Table 3). Notably, no correlations between VE and arterial gas tensions were found. The relatively high inverse correlation between Ppl_ampl post and VE pre (Table 3) has not yet been explained.
4.1 Study limitation
The main limitation is related to the fact that neither Ppl_ampl in the contralateral hemithorax nor WOBe is precisely known, particularly before TT; therefore, we have had to rely on laws of physics in the interpretation of results. The fact that a study is retrospective is usually considered a limitation. In our case, however, even a prospective study would not supply better data related directly to WOBe because additional measurements in patients in such poor condition would be impossible for ethical reasons. Thus, the only true limitation related to the retrospective character of this study is that TT was terminated both because of symptoms (such as too intensive cough, for example,) and when there was no more fluid or when Ppl excessively fell or Ppl_ampl increased too much (hence the inverse correlation between Ppl_ampl post and Vw in Table 3), which means some lack of sample uniformity. Certainly, the feeling of dyspnea might also be affected by other factors, such as pain, stress or fear, in patients with serious comorbidities undergoing interventional procedure; however, these factors have not been precisely recorded and, therefore, their influence cannot be analyzed here. Nevertheless, the association between WOB and dyspnea was so strong that the influence of the other causes was insufficient to destroy the correlation between Ppl_ampl post and dyspnea (both Bpost and ΔB).
5 Conclusion
Respiratory chemoreceptors seem to control breathing effectively in patients with malignant PE since arterial blood gases do not change significantly; therefore, changes in dyspnea after pleural fluid withdrawal can be associated with neither blood gas tensions nor VE changes. Our results suggest that dyspnea in PE not associated with congestive heart failure can be related to a decrease in total lung compliance (due to the collapse of a part or the whole ipsilateral lung). This decrease forces a proportional increase in WOBe to maintain the ventilation and arterial gas tensions required by respiratory chemoreceptors. The strong association between dyspnea changes and Ppl_ampl post (statistical significance, large effect size) confirms that if pleural fluid withdrawal leads to recruitment of the collapsed parts, then both WOBe and dyspnea decrease; otherwise, WOBe and dyspnea do not change or can even increase owing to the nonlinearity of lung compliance. Thus, although there can be various other causes of dyspnea in an individual patient with PE, an increase in WOB should also be taken into account. Based on the analyses presented here, we recommend pleural manometry during TT, which will enable to adjust the fluid removal rate to the observed value of Ppl_ampl.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving humans were approved by the Institutional Review Board Medical University of Warsaw (KB 105/2012). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
TG: Conceptualization, Formal analysis, Investigation, Writing – original draft. AS: Formal analysis, Data curation, Writing – original draft. EG: Data curation, Project administration, Writing – review and editing. MZ-K: Data curation, Writing – review and editing. RK: Data curation, Supervision, Writing – review and editing.
Funding
The author(s) declared that financial support was received for this work and/or its publication. This study was supported by the National Science Center, Poland (grant N 2019/35/B/NZ5/02531) and Nalecz Institute of Biocybernetics and Biomedical Engineering, Polish Academy of Sciences.
Acknowledgements
The authors thank Marcin Michnikowski and Katarzyna Faber for their assistance during therapeutic thoracentesis.
Conflict of interest
The author(s) declared that this work was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declared that generative AI was used in the creation of this manuscript. Generative AI tools were used exclusively for language editing and improving the clarity of the text.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2025.1664237/full#supplementary-material
Abbreviations
PE, pleural effusion; TT, therapeutic thoracentesis; Ppl, pleural pressure; AGT, arterial gas tensions; dB, ΔB, change in dyspnea, difference between the Borg Scores before and after therapeutic thoracentesis; PaO2, arterial oxygen partial pressure; PaCO2, arterial carbon dioxide partial pressure; Ppl_ampl, amplitude of pleural pressure changes related to breathing; Ppl_ampl post, Ppl_ampl after therapeutic thoracentesis; VE, minute ventilation; WOB, work of breathing (from the point of view of physics it is actually power, not work); WOBe, work of breathing which is required to overcome elastic forces; WOBr, work of breathing which is required to is the resistive work; RR, respiratory rate; VT, tidal volume; Bpre, the Borg Scores before therapeutic thoracentesis; Bpost, the Borg Scores after therapeutic thoracentesis; Vw, the volume of withdrawn pleural fluid; rg, the Glass rank-biserial correlation.
References
Agustí A. G., Cardús J., Roca J., Grau J. M., Xaubet A., Rodriguez-Roisin R. (1997). Ventilation-perfusion mismatch in patients with pleural effusion: effects of thoracentesis. Am. J. Respir. Crit. Care Med. 156, 1205–1209. doi:10.1164/ajrccm.156.4.9612113
Antony V. B., Loddenkemper R., Astoul P., Boutin C., Goldstraw P., Hott J., et al. (2001). Management of malignant pleural effusions. Eur. Respir. J. 18 (2), 402–419. doi:10.1183/09031936.01.00225601
Beaudry R. I., Brotto A. R., Varughese R. A., de Waal S., Fuhr D. P., Damant R. W., et al. (2022). Persistent dyspnea after COVID-19 is not related to cardiopulmonary impairment; a cross-sectional study of persistently dyspneic COVID-19, non-dyspneic COVID-19 and controls. Front. Physiol. 13, 917886. doi:10.3389/fphys.2022.917886
Brandstetter R. D., Cohen R. P. (1979). Hypoxemia after thoracentesis: a predictable and treatable condition. JAMA 242, 1060–1061. doi:10.1001/jama.1979.03300100038019
Coccia C. B., Palkowski G. H., Schweitzer B., Motsohi T., Ntusi N. A. (2016). Dyspnoea: pathophysiology and a clinical approach. S. Afr. Med. J. 106 (1), 32–36. doi:10.7196/samj.2016.v106i1.10324
Fjaellegaard K., Koefod Petersen J., Alstrup G., Skaarup S., Frost Clementsen P., Laursen C. B., et al. (2024). Ultrasound in predicting improvement in dyspnoea after therapeutic thoracentesis in patients with recurrent unilateral pleural effusion. Eur. Clin. Respir. J. 11 (1), 2337446. doi:10.1080/20018525.2024.2337446
Gólczewski T., Stecka A. M., Grabczak E. M., Michnikowski M., Zielińska-Krawczyk M., Krenke R. (2025). Hemidiaphragm work in large pleural effusion and its insignificant impact on blood gases: a new insight based on in silico study. Front. Physiol. 16, 1539781. doi:10.3389/fphys.2025.1539781
Karetzky M. S., Kothari G. A., Fourre J. A., Khan A. U. (1978). Effect of thoracentesis on arterial oxygen tension. Respiration 36 (2), 96–103. doi:10.1159/000193932
Muruganandan S., Azzopardi M., Thomas R., Fitzgerald D. B., Kuok Y. J., Cheah H. M., et al. (2020). The pleural effusion and symptom evaluation (PLEASE) study of breathlessness in patients with a symptomatic pleural effusion. Eur. Respir. J. 55 (5), 1900980. doi:10.1183/13993003.00980-2019
Muruganandan S., Mishra E., Singh B. (2023). Breathlessness with pleural effusion: what do we know? Semin. Respir. Crit. Care Med. 44 (4), 502–508. doi:10.1055/s-0043-1769098
Parshall M. B., Schwartzstein R. M., Adams L., Banzett R. B., Manning H. L., Bourbeau J., et al. (2012). An official American thoracic society statement: update on the mechanisms, assessment, and management of dyspnea. Am. J. Respir. Crit. Care Med. 185 (4), 435–452. doi:10.1164/rccm.201111-2042ST
Petersen J. K., Fjaellegaard K., Rasmussen D. B., Alstrup G., Høegholm A., Sidhu J. S., et al. (2024). Patient-reported outcome measures in patients with and without non-expandable lung secondary to malignant pleural Effusion—A single-centre observational study. Diagn. (Basel) 14 (11), 1176. doi:10.3390/diagnostics14111176
Piggott L. M., Hayes C., Greene J., Fitzgerald D. B. (2023). Malignant pleural disease. Breathe (Sheff) 19 (4), 230145. doi:10.1183/20734735.0145-2023
Psallidas I., Yousuf A., Talwar A., Hallifax R. J., Mishra E. K., Corcoran J. P., et al. (2017). Assessment of patient-reported outcome measures in pleural interventions. BMJ Open Respir. Res. 4 (1), e000171. doi:10.1136/bmjresp-2016-000171
Ritter O., Noureddine S., Laurent L., Roux P., Westeel V., Barnig C. (2024). Unraveling persistent dyspnea after mild COVID: insights from a case series on hyperventilation provocation tests. Front. Physiol. 15, 1394642. doi:10.3389/fphys.2024.1394642
Skaarup S. H., Lonni S., Quadri F., Valsecchi A., Ceruti P., Marchetti G. (2020). Ultrasound evaluation of hemidiaphragm function following thoracentesis: a study on mechanisms of dyspnea related to pleural effusion. J. Bronchology Interv. Pulmonol. 27 (3), 172–178. doi:10.1097/LBR.0000000000000627
Stecka A. M., Gólczewski T., Grabczak E. M., Zieliński K., Michnikowski M., Zielińska-Krawczyk M., et al. (2018). The use of a virtual patient to follow changes in arterial blood gases associated with therapeutic thoracentesis. Int. J. Artif. Organs 41 (11), 690–697. doi:10.1177/0391398818793354
Taylor T. M., Radchenko C., Sanchez T. M., Shepherd R. W., Kang L., Shojaee S. (2021). The Impact of thoracentesis on postprocedure pulse oximetry. J. Bronchology Interv. Pulmonol. 28 (3), 192–200. doi:10.1097/LBR.0000000000000747
Thomas R., Jenkins S., Eastwood P. R., Lee Y. C., Singh B. (2015). Physiology of breathlessness associated with pleural effusions. Curr. Opin. Pulm. Med. 21 (4), 338–345. doi:10.1097/MCP.0000000000000174
Wijayaratne T., Yousuf A., Panchal R. (2024). Cardiac related pleural effusions: a narrative review. J. Thorac. Dis. 16 (2), 1674–1686. doi:10.21037/jtd-23-1731
Zielinska-Krawczyk M., Grabczak E. M., Michnikowski M., Zielinski K., Korczynski P., Stecka A., et al. (2018). Patterns of pleural pressure amplitude and respiratory rate changes during therapeutic thoracentesis. BMC Pulm. Med. 18 (1), 36. doi:10.1186/s12890-018-0595-7
Zielinska-Krawczyk M., Stecka A. M., Grabczak E. M., Michnikowski M., Zieliński K., Korczynski P., et al. (2022). Impact of therapeutic thoracentesis and pleural pressure changes on breathing pattern, dyspnea, lung function, and arterial blood gases. Pol. Arch. Intern. Med. 132 (4), 16185. doi:10.20452/pamw.16185
Keywords: dyspnea, pleural effusion, pleural manometry, thoracentesis, work of breathing
Citation: Gólczewski T, Stecka AM, Grabczak EM, Zielińska-Krawczyk M and Krenke R (2025) Increased work of breathing and its relationship to dyspnea in malignant pleural effusion. Front. Physiol. 16:1664237. doi: 10.3389/fphys.2025.1664237
Received: 14 July 2025; Accepted: 09 December 2025;
Published: 19 December 2025.
Edited by:
Alexander V. Glushkov, Odessa National Polytechnic University, UkraineReviewed by:
Rohin Banerji, Boston University, United StatesDalia Anas Ibrahim, Zagazig University, Egypt
Copyright © 2025 Gólczewski, Stecka, Grabczak, Zielińska-Krawczyk and Krenke. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anna M. Stecka, YXN0ZWNrYUBpYmliLndhdy5wbA==