




- 1 Service d’Addictologie, Centre Hospitalier Sainte-Anne, Paris, France
- 2 Institut National de la Santé et de la Recherche Médicale, Laboratoire de Physiopathologie des Maladies Psychiatriques, Centre Psychiatrie et Neurosciences, Paris, France
- 3 Université Paris Descartes, Faculté de Médecine Paris Descartes, Service Hospitalo Universitaire, Centre Hospitalier Sainte-Anne, Paris, France
Objective: Some studies have found that high levels of impulsivity and sensation seeking, particularly disinhibition are associated with substance abuse in patients with schizophrenia, as in the general population. However, no study has assessed impulsivity and sensation seeking specifically in schizophrenia patients with alcohol abuse or dependence. Materials and methods: We compared impulsivity and sensation seeking in a group of schizophrenia patients (DSM-III-R criteria) with lifetime alcohol abuse or dependence (n = 34) and in a group without lifetime substance abuse or dependence (n = 66). The patients were assessed using the composite international diagnostic interview (CIDI) for DSM-III-R disorders, the positive and negative syndrome scale (PANSS), the Barratt impulsivity scale (BIS), the Zuckerman seeking sensation scale (SSS), and the physical anhedonia scale (PAS). Results: The mean scores for impulsivity and sensation seeking were higher in the group with lifetime alcohol abuse or dependence than in the group without substance abuse or dependence (BIS: 63.4 ± 18.7 vs 51.3 ± 14.2 respectively, ANOVA: F = 11.12, p = 0.001; SSS: 17.6 ± 5.9 vs 13.5 ± 6.7 respectively, ANOVA: F = 7.45, p = 0.008). There was no significant difference between the two groups on PAS score. Conclusion: Increased impulsivity or sensation seeking may be a link between schizophrenia and alcohol abuse or dependence.
Introduction
The high prevalence of alcohol use disorders (AUD, i.e. alcohol abuse or dependence) among patients with schizophrenia is now well established: in the Koskinen et al.’ meta-analysis of 60 studies, the median current rate of AUD was 9.4% and median of lifetime AUD prevalence 20.6% (Koskinen et al., 2009). The high comorbidity of AUD and schizophrenia may be related to male gender, younger persons (Cantor-Graae et al., 2001), availability of drugs (Dixon, 1999), increased vulnerability to the effects of alcohol in patients with schizophrenia (D’Souza et al., 2006; Krystal et al., 2006), or neurobiological factors (Chambers et al., 2001). The high prevalence of substance abuse in patients with schizophrenia has sometimes been interpreted as self-medication for negative symptoms, anhedonia, depression or neuroleptic side effects, but no convincing evidence supports this idea (Mueser et al., 1998; D’Souza et al., 2006).
In non-schizophrenic subjects, high levels of impulsivity (Evenden, 1999; Moeller et al., 2001; de Wit, 2009; Dick et al., 2010) and sensation seeking (Crawford et al., 2003; Dom et al., 2006a,b) have been found to be associated with AUD, but this has been little studied in patients with schizophrenia. We previously found that high levels of impulsivity and sensation seeking, particularly regarding the disinhibition dimension, were associated with substance abuse in patients with schizophrenia (Dervaux et al., 2001; Gut-Fayand et al., 2001). However, this was not specifically studied with regard to the different substances of abuse. Mueser et al. (1990) stressed the need to assess the abuse of specific classes of substances and analyze the data accordingly.
Liraud and Verdoux (2000) found that a lifetime history of alcohol misuse was independently associated with higher total scores on the sensation seeking scale (SSS), on the “experience-seeking” and “disinhibition” sub-scores of the SSS and on the ‘motor impulsivity’ subscale of the Barratt impulsivity scale (BIS) in subjects with psychotic and mood disorders. However, their study included a limited number of patients with schizophrenia (n = 24) and other non-affective psychotic disorders, delusional disorder, psychotic disorders (n = 21), and included few schizophrenia patients who engaged in alcohol abuse; they were not analyzed separately (Liraud and Verdoux, 2000).
To our knowledge, no study has assessed impulsivity and sensation seeking specifically in patients with schizophrenia and AUD. Our objective was to compare impulsivity, sensation seeking, and anhedonia in a sample of schizophrenia patients with and without lifetime alcohol abuse or dependence.
Materials and Methods
All consecutive patients over 18 years with DSM-III-R criteria for schizophrenia or schizoaffective disorder treated in a psychiatric department in south suburbs of Paris during 2 years, were enrolled in the study. Inclusion criteria for participation in the study were age 18 years or older and willingness to provide consent to participate in the study.
The method is described elsewhere (Dervaux et al., 2006). Briefly, all subjects were assessed by a senior psychiatrist (Alain Dervaux) using the composite international diagnostic interview (CIDI) for DSM-III-R diagnoses of abuse or dependence on alcohol, cannabis, amphetamines, sedatives, opioids, cocaine, hallucinogens, phencyclidine, and inhalants (Robins et al., 1988). Current psychotic symptomatology was assessed using the positive and negative syndrome scale (PANSS) (Kay et al., 1987). Impulsivity was assessed using the BIS 10 (Patton et al., 1995), a 34-item self-report (scores from 0 to 136). The BIS includes three component subscales found in the French translation (Baylé et al., 2000): (1) motor impulsivity (2) cognitive impulsivity (3) non-planning. Sensation seeking was assessed using the SSS form V by Zuckerman (SSS, Zuckerman, 1978), a 40-item self-report (scores from 0 to 40). The SSS includes four components found in the French translation (Carton et al., 1990): (1) disinhibition (2) thrill and adventure seeking (3) experience seeking (4) boredom susceptibility. Anhedonia was assessed using the Chapman physical anhedonia scale (PAS, Chapman et al., 1976), a 61-item self-report (scores from 0 to 61). The data obtained during the interview were supplemented by information from relatives, clinicians, and medical records. Patients were evaluated shortly before they were discharged, when their condition had stabilized. The study was approved by the local Ethical committee and all subjects provided their informed consent.
Impulsivity, sensation seeking and anhedonia were compared in a group of schizophrenia patients with lifetime alcohol abuse or dependence, and in a group without lifetime AUD. The quantitative variables were studied using analyses of covariance (ANCOVA) adjusted on the basis of age and gender, since these variables could be confounding factors. All the tests were two-tailed, with alpha-risk set at 0.05.
Results
One hundred and fifteen patients with schizophrenia (n = 106) or schizoaffective disorder (n = 9) according to DSM-III-R criteria were included in the study. Since 15 patients with cannabis, stimulant, sedative, or opiate abuse or dependence were excluded, the study finally included 100 subjects including a first group of schizophrenia patients with lifetime AUD (n = 34, alcohol abuse: n = 4; alcohol dependence: n = 30) and a second group without any lifetime psychoactive substance abuse (n = 66). Twenty-four (20.9%) patients presented AUD within the 6 months prior to the assessment.
Sociodemographic Characteristics of Schizophrenia Patients with or without Lifetime AUD
Among patients with AUD, 85.3% were male (n = 29) compared to 62.1% in the other group (n = 41) (χ2= 5.73, df = 1, p = 0.02). The patients with AUD had a higher mean number of hospitalizations (mean = 7.3, SD = 10.6 vs mean = 4.4, SD = 4.3, ANCOVA F = 5.39, df = 1.96 p = 0.02).
There were no significant differences between the two groups for age (patients with AUD: mean age = 34.1 years, SD = 7.7, patients without substance abuse: mean age = 37.0, SD = 12.7, ANOVA F = 1.95, df = 1.98 p = 0.16), marital status (never married: patients with AUD: 73.5%, subjects without substance abuse: 68.2% of the subjects, χ2= 0.31, df = 1, p = 0.58), level of education (completed high school: patients with AUD: 40.0%, patients without substance abuse: 49.2%, χ2= 0.70, df = 1, p = 0.40), mean age of first psychiatric treatment (patients with AUD: mean = 23.7 years SD = 5.7%, patients without substance abuse: mean = 25.2, SD = 8.3, ANCOVA F = 0.08, df = 1.97 p = 0.77), mean scores on the PANSS (patients with AUD: mean = 79.6, SD = 10.2%, patients without substance abuse: mean = 79.7, SD = 14.4, ANCOVA F = 0.03, df = 1.97 p = 0.86).
Impulsivity, Sensation Seeking and Anhedonia in Schizophrenia Patients with or without Lifetime AUD
The mean total scores for BIS and SSS were higher in the group with AUD compared to the group with cannabis use without AUD (Table 1). All mean scores on the BIS and SSS subscales were higher in the group with AUD than in the group without AUD, except the SSS experience-seeking subscale (Table 1). In contrast, there was no significant difference between the two groups for physical anhedonia scale mean score (Table 1).
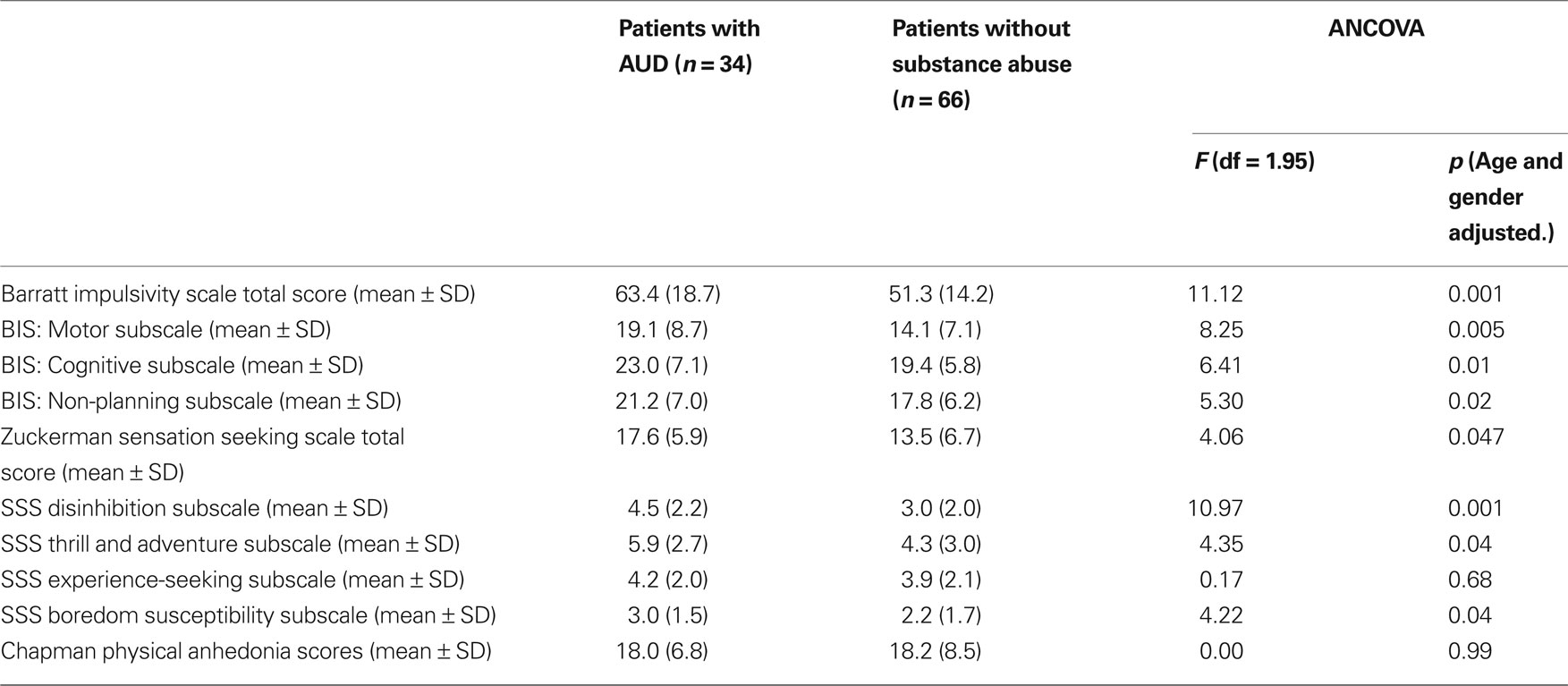
Table 1. Impulsivity and sensation seeking score ratings in schizophrenia patients with lifetime AUD (alcohol abuse or dependence) or without substance abuse.
Discussion
Our results indicate that in a group of patients with schizophrenia, mean scores on the BIS and SSS are higher in patients with lifetime AUD (alcohol abuse or dependence) than in patients without AUD. The results of the present study are consistent with those of our previous studies assessing impulsivity and sensation seeking in two independent samples of schizophrenia patients with substance abuse disorders, including alcohol, cannabis, opiates, and cocaine use disorders (Dervaux et al., 2001; Gut-Fayand et al., 2001) and with previous studies in alcohol or drug abusing patients with severe mental illness, including affective disorders (Liraud and Verdoux, 2000; Bizzarri et al., 2009). However, the previous studies did not examine AUD specifically in patients with schizophrenia.
Our results are also consistent with studies which found higher impulsivity and sensation seeking scores in non-schizophrenic patients with AUD (Dick et al., 2010) or other drug use disorders (Pedersen, 1991; Luthar et al., 1992; Kosten et al., 1994; Scourfield et al., 1996), compared to subjects without substance use disorders.
Since the present study was cross-sectional, it is not possible to determine the causal relationship between impulsivity or sensation seeking and AUD. The developmental studies referred to earlier suggest that impulsive tendencies lead to alcohol use (Dom et al., 2006b). Moreover, in our previous study in schizophrenia patients, we found higher BIS scores in the “past substance abuse or dependence” sub-group, suggesting that impulsivity is not induced by alcohol or drugs. Nevertheless, we cannot exclude impulsivity or sensation seeking reflecting the behavioral consequences of alcohol use (Lawrence et al., 2009). Finally, higher impulsivity and sensation seeking could be linked to a third factor. A prospective longitudinal follow-up of a cohort of young subjects, studying the occurrence of impulsivity, sensation seeking, substance abuse, and/or schizophrenia, would be more reliable but hardly feasible.
As suggested by Liraud and Verdoux (2000), impulsivity or sensation seeking may favor substance use disorders in a non-specific way. These personality dimensions are linked to substance abuse in several psychiatric disorders (Moeller et al., 2001). For instance, BIS scores were also found to be increased in patients with bipolar disorder and substance abuse (Swann et al., 2004).
In line with previous studies, the absence of any link between physical anhedonia scores and cannabis use or AUD does not support the self-medication hypothesis of alcohol abuse in schizophrenia (Mueser et al., 1998; Dervaux et al., 2001; D’Souza et al., 2009).
There are some limitations to our study. First, the patients included are not necessarily representative of all patients with schizophrenia, although the exhaustive recruitment limits the selection bias. Secondly, as in any retrospective study, the prevalence of lifetime alcohol abuse may have been under-estimated. Denial or under-estimation of substance abuse is common in patients with schizophrenia. However, certain authors have stressed that structured interviews are more sensitive for the diagnosis of lifetime substance abuse in patients with schizophrenia than toxicology tests (Albanese et al., 1994). In addition, Hides et al. (2006) found that self-reports of substance use showed good reliability with drug screens in a subsample of a cohort of patients with recent-onset psychosis (Cohen’s kappa = 0.90). Finally, the limited size of this sub-group does not permit a definitive conclusion to be reached.
Conclusions
Increased impulsivity or sensation seeking may be a link between schizophrenia and alcohol abuse or dependence. However, the role of impulsivity or sensation seeking may not be specific to AUD. Further studies will be needed to fully understand the relationship, particularly the addition of risk factors, between alcohol abuse or dependence and schizophrenia.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Albanese, M. J., Bartel, R. L., Bruno, R. F., Morgenbesser, M. W., and Schatzberg, A. F. (1994). Comparison of measures used to determine substance abuse in an inpatient psychiatric population. Am. J. Psychiatry 151, 1077–1078.
Baylé, F. J., Bourdel, M. C., Caci, H., Gorwood, P., Chignon, J. M., Adés, J., and Lôo, H. (2000). Factor analysis of french translation of the Barratt impulsivity scale (BIS-10). Can. J. Psychiatry 45, 156–165.
Bizzarri, J. V., Rucci, P., Sbrana, A., Miniati, M., Raimondi, F., Ravani, L., Massei, G. J., Milani, F., Milianti, M., Massei, G., Gonnelli, C., and Cassano, G. B. (2009). Substance use in severe mental illness: self-medication and vulnerability factors. Psychiatry Res. 165, 88–95.
Cantor-Graae, E., Nordström, L. G., and McNeil, T. F. (2001). Substance abuse in schizophrenia: a review of the literature and a study of correlates in Sweden. Schizophr. Res. 48, 69–82.
Carton, S., Lacour, C., Jouvent, R., and Widlöcher, D. (1990). Le concept de recherche de sensations: traduction et validation de l’échelle de Zuckerman. Psychiatr. Psychobiol. 5, 39–44.
Chambers, R. A., Krystal, J. H., and Self, D. W. (2001). A neurological basis for substance abuse comorbidity in schizophrenia. Biol. Psychiatry 50, 71–83.
Chapman, L. J., Chapman, J. P., and Raulin, M. L. (1976). Scales for physical and social anhedonia. J. Abnorm. Psychol. 4, 374–382.
Crawford, A. M., Pentz, M. A., Chou, C. P., and Li, C. Dwyer, J. H. (2003). Parallel developmental trajectories of sensation seeking and regular substance use in adolescents. Psychol. Addict. Behav. 17, 179–192.
de Wit, H. (2009). Impulsivity as a determinant and consequence of drug use: a review of underlying processes. Addict. Biol. 14, 22–31.
Dervaux, A., Baylé, F. J., Laqueille, X., Bourdel, M. C., Le Borgne, M. H., Olié, J. P., and Krebs, M. O. (2001). Is substance abuse in schizophrenia related to impulsivity, sensation seeking or anhedonia? Am. J. Psychiatry 158, 492–494.
Dervaux, A., Baylé, F. J., Laqueille, X., Bourdel, M. C., Leborgne, M., Olié, J. P., and Krebs, M. O. (2006). Validity of the CAGE questionnaire in schizophrenic patients with alcohol abuse and dependence. Schizophr. Res. 81, 151–155.
Dick, D. M., Smith, G., Olausson, P., Mitchell, S. H., Leeman, R. F., O’Malley, S. S., and Sher, K. (2010). Understanding the construct of impulsivity and its relationship to alcohol use disorders. Addict. Biol. 15, 217–226.
Dixon, L. (1999). Dual diagnosis of substance abuse in schizophrenia: prevalence and impact on outcomes. Schizophr. Res. 35, S93–S100.
Dom, G., Hulstijn, W., and Sabbe, B. (2006a). Differences in impulsivity and sensation seeking between early- and late-onset alcoholics. Addict. Behav. 31, 298–308.
Dom, G., D’Haene, P., Hulstijn, W., and Sabbe, B. (2006b). Impulsivity in abstinent early- and late-onset alcoholics: differences in self-report measures and a discounting task. Addiction 101, 50–59.
D’Souza, D. C., Gil, R. B., Madonick, S., Perry, E. B., Forselius-Bielen, K., Braley, G., Donahue, L., Tellioglu, T., Zimolo, Z., Gueorguieva, R., and Krystal, J. H. (2006). Enhanced sensitivity to the euphoric effects of alcohol in schizophrenia. Neuropsychopharmacology 31, 2767–2775.
D’Souza, D. C., Sewell, R. A., and Ranganathan, M. (2009). Cannabis and psychosis/schizophrenia: human studies. Eur. Arch. Psychiatry Clin. Neurosci. 259, 413–431.
Gut-Fayand, A., Dervaux, A., Olié, J. P., Lôo, H., Poirier, M. F., and Krebs, M. O. (2001). Substance abuse and suicidality in schizophrenia: a common risk factor linked to impulsivity. Psychiatry Res. 102, 65–72.
Hides, L., Dawe, S., Kavanagh, D. J., and Young, R. M. (2006). Psychotic symptom and cannabis relapse in recent-onset psychosis. Prospective study. Br. J. Psychiatry 189, 137–143.
Kay, S. R., Fiszbein, A., and Opler, L. A. (1987). The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 13, 261–276.
Koskinen, J., Löhönen, J., Koponen, H., Isohanni, M., and Miettunen, J. (2009). Prevalence of alcohol use disorders in schizophrenia – a systematic review and meta-analysis. Acta Psychiatr. Scand. 120, 85–96.
Kosten, T. A., Ball, S. A., and Rounsaville, B. J. (1994). A sibling study of sensation seeking and opiate addiction. J. Nerv. Ment. Dis. 182, 284–289.
Krystal, J. H., D’Souza, D. C., Gallinat, J., Driesen, N., Abi-Dargham, A., Petrakis, I., Heinz, A., and Pearlson, G. (2006). The vulnerability to alcohol and substance abuse in individuals diagnosed with schizophrenia. Neurotox Res. 10, 235–252.
Lawrence, A. J., Luty, J., Bogdan, N. A., Sahakian, B. J., and Clark, L. (2009). Impulsivity and response inhibition in alcohol dependence and problem gambling. Psychopharmacology (Berl.) 207, 163–172.
Liraud, F., and Verdoux, H. (2000). Which temperamental characteristics are associated with substance use in subjects with psychotic and mood disorders? Psychiatry Res. 93, 63–72.
Luthar, S. S., Anton, S. F., Merikangas, K. R., and Rounsaville, B. J. (1992). Vulnerability to drug abuse among opioid addicts’ siblings: individual, familial, and peer influences. Compr. Psychiatry 33, 190–196.
Moeller, F. G., Barratt, E. S., Dougherty, D. M., Schmitz, J. M., and Swann, A. C. (2001). Psychiatric aspects of impulsivity. Am. J. Psychiatry 158, 1783–1793.
Mueser, K. T., and Drake, R. E., Wallach, MA. (1998). Dual diagnosis: a review of etiological theories. Addict. Behav. 23, 717–734.
Mueser, K. T., Yarnold, P. R., Levinson, D. F., Singh, H., Bellack, A. S., Kee, K., Morrison, R. L., and Yadalam, K. G. (1990). Prevalence of substance abuse in schizophrenia: demographic and clinical correlates. Schizophr. Bull. 16, 31–56.
Patton, J. H., Stanford, M. S., and Barratt, E. S. (1995). Factor structure of the Barratt impulsiveness scale. J. Clin. Psychol. 51, 768–774.
Pedersen, W. (1991). Mental health, sensation seeking and drug use patterns: a longitudinal study. Br. J. Addict. 86, 195–204.
Robins, L. N., Wing, J., Wittchen, H. U., Helzer, J. E., Babor, T. F., and Burke, J. D. Farmer, A., Jablenski, A., Pickens, R., Regier, D. A., Sartorius, N., Towle, L. H. (1988). The composite international diagnostic interview: an epidemiologic instrument suitable for use in conjunction with different diagnostic systems and in different cultures. Arch. Gen. Psychiatry 45, 1069–1077.
Scourfield, J., Stevens, D. E., and Merikangas, R. (1996). Substance abuse, comorbidity, and sensation seeking: gender differences. Compr. Psychiatry 37, 384–392.
Keywords: schizophrenia, alcohol, dependence, abuse, impulsivity, sensation seeking, anhedonia
Citation: Dervaux A, Laqueille X, Bourdel M-C, Olié J-P and Krebs M-O (2010) Impulsivity and sensation seeking in alcohol abusing patients with schizophrenia. Front. Psychiatry 1:135. doi: 10.3389/fpsyt.2010.00135
Received: 17 May 2010;
Paper pending published: 01 June 2010;
Accepted: 01 September 2010;
Published online: 17 September 2010.
Edited by:
Pinhas N. Dannon, Tel Aviv University, IsraelReviewed by:
Pinhas N. Dannon, Tel Aviv University, IsraelSally Gainsbury, University of Sydney, Australia
Copyright: © 2010 Dervaux, Laqueille, Bourdel, Olié and Krebs. This is an open-access article subject to an exclusive license agreement between the authors and the Frontiers Research Foundation, which permits unrestricted use, distribution, and reproduction in any medium, provided the original authors and source are credited.
*Correspondence: Alain Dervaux, Service d’Addictologie, Centre Hospitalier Sainte-Anne, 1 Rue Cabanis, 75014 Paris, France. e-mail:YS5kZXJ2YXV4QGNoLXNhaW50ZS1hbm5lLmZy