 Heather M. Wastler
Heather M. Wastler Daniel Núñez
Daniel Núñez- 1Department of Psychiatry and Behavioral Health, The Ohio State University, Columbus, OH, United States
- 2Faculty of Psychology, Universidad de Talca, Talca, Chile
- 3Millennium Nucleus to Improve the Mental Health of Adolescents and Youths (Imhay), Santiago, Chile
- 4Programa de Investigación Asociativa, Faculty of Psychology, Centro de Investigación en Ciencias Cognitivas, Universidad de Talca, Talca, Chile
Psychotic experiences are associated with increased risk for suicide. Despite this well-established finding, very little is known about factors that contribute to this relationship. The current study investigated the relationship between psychotic experiences, emotion regulation, and suicidal ideation among 1,590 Chilean adolescents in the general population. Participants completed self-report measures of psychotic experiences (Community Assessment of Psychic Experiences), emotion regulation (Emotion Regulation Questionnaire), depression (Patient Health Questionnaire-9), and suicidal ideation (Columbia Suicide Severity Rating Scale). Statistical analyses included Mann–Whitney U tests, point-biserial correlations, logistic regression, and moderation analyses. Results suggest that paranoid ideation, bizarre experiences, and perceptual abnormalities were moderately associated with suicidal ideation. Additionally, greater expressive suppression and cognitive reappraisal were associated with suicidal ideation. Results from the logistic regression indicate that paranoid ideation, perceptual abnormalities, and expressive suppression have the strongest relationship with suicidal ideation, even when controlling for depression and relevant demographic variables. Additionally, paranoid ideation interacted with expressive suppression to predict suicidal ideation, with expressive suppression having the strongest relationship with suicidal ideation when paranoid ideation was low to moderate. Taken together, these findings support the broader literature suggesting that emotion regulation might be a transdiagnostic risk factor for suicidal ideation. Additional longitudinal research is needed to examine whether expressive suppression and other maladaptive emotion regulation strategies serve as a mechanism for suicidal ideation both in the general population and among individuals with psychotic experiences.
Introduction
Psychotic disorders are serious mental illnesses that affect approximately 7.49/1,000 persons worldwide (1). There is growing recognition that psychosis exist on a continuum, ranging from subthreshold psychotic experiences to chronic mental health conditions such as schizophrenia spectrum disorders. Even among individuals who do not meet diagnostic criteria for a psychotic disorder, the presence of psychotic experiences is associated with significant distress (2, 3) and functional impairment (3). Importantly, approximately 7.5% of adolescents have psychotic experiences (3, 4), with such experiences increasing the risk of developing psychotic disorders and other mental health conditions later in life (2, 5–8). Additionally, psychotic experiences are associated with a number of co-occurring mental health difficulties, such as substance use (9, 10), depression (11, 12), anxiety (11, 12), greater emotional reactivity (13, 14), and trauma (15). There is also a growing body of literature demonstrating that psychotic experiences are associated with increased risk for suicide (16, 17). Specifically, recent meta-analyses have shown that psychotic experiences confer increased risk for suicidal ideation, suicide attempts, and suicide (16, 17). Interestingly, the strongest support has been for an association between positive symptoms (i.e., delusions and hallucinations) and suicide risk (16), with studies showing that specific psychotic experiences, such as persecutory ideation and perceptual abnormalities (PA) (18) might have the strongest association with suicide risk. Despite this growing body of literature, much less is known about factors that contribute to the relationship between psychotic experiences and suicide risk.
Outside of the psychosis literature, emotion regulation, the use of strategies to change the intensity, frequency, or perceived quality of emotion (19, 20), has been identified as a trans-diagnostic mechanism for suicide risk (21–24). Emotion regulation abnormalities are well documented among individuals with psychosis, with studies showing that individuals with schizophrenia spectrum disorders use greater maladaptive emotion regulation strategies (e.g., rumination, self-blaming, distraction, and suppression) and fewer adaptive strategies (e.g., reappraisal) than healthy controls (25, 26). Importantly, emotion regulation abnormalities exist across the psychosis continuum (27), occurring among adolescents with psychotic experiences (28, 29), individuals at clinical high-risk for psychosis (14, 30), and among individuals diagnosed with schizophrenia spectrum disorders (25, 26). Although few studies have explicitly examined how emotion regulation abnormalities can affect psychotic experiences, studies have shown that maladaptive emotion regulation strategies might maintain and exacerbate psychotic experiences (31). For instance, a recent study demonstrated that adaptive strategies such as cognitive reappraisal are used similarly among individuals with high/low psychotic experiences, whereas maladaptive strategies, such as expressive suppression, are more common among individuals with greater psychotic experiences (32). Further, another study demonstrated that individuals with psychotic disorders experience more difficulty regulating their emotions during the presence of psychotic experiences (33). Taken together, these findings suggest an important relationship between psychotic experiences and emotion regulation, highlighting the need for more research in this area (33).
Despite the well-established relationship between emotion regulation abnormalities and psychotic disorders, limited research has examined whether emotion regulation abnormalities contribute to suicidal risk in this population. This is a notable gap in the literature, as emotion regulation plays in important role across leading suicide theories (e.g., Escape Theory, Interpersonal Psychological Theory, Three Step Theory, Integrated Motivational-Volitional Model, and Fluid Vulnerability Theory) (34–38) and several theories even explicitly identify emotion regulation as a mechanism for suicidal thoughts and behaviors (23, 24, 39). The few studies that have examined emotion regulation and suicide risk in psychosis have found that emotion dysregulation (40) and coping beliefs (i.e., the perceived ability to regulation emotions) (41, 42) are associated with suicide risk among individuals with psychosis. Only one study to date has explicitly examined whether the use of maladaptive versus adaptive emotion regulation strategies contributes to the relationship between psychotic experiences and suicide risk (43). This study found that auditory hallucinations are associated with suicidal behavior and that lower reappraisal mediates this relationship; expressive suppression did not mediate the relationship between psychotic experiences and suicidal behavior. Taken together, these studies provide preliminary evidence that emotion regulation might influence the relationship between suicide risk and psychotic experiences. Notably, however, these studies were primarily based on high-income Western countries (e.g., Australia, United States, and England), which limits our understanding about factors that contribute to suicide among adolescents with psychotic experiences from developing countries (40, 41, 43). This is a significant gap in the literature as (1) psychotic experiences are more common in lower and middle income countries than high income countries (44); (2) suicide is a leading cause of death among adolescents worldwide (45); and (3) the consequences of specific emotion regulation strategies is culturally dependent (46). Thus, there is a great need for further research examining the relationship between psychotic experiences, emotion regulation, and suicidal ideation among adolescents from developing countries.
The current study sought to address this gap by examining the cross-sectional relationship between psychotic experiences, emotion regulation, and suicidal ideation among Chilean adolescents in the general population. The current study focuses specifically on adolescence, as suicide is a leading cause of death among adolescents worldwide (47). Additionally, we focus on Chilean adolescents, as prior research has shown that 52.5% of Chilean adolescents endorse bizarre experiences (BE) and 15.3% endorse perceptual anomalies in their lifetime, suggesting that psychotic experiences are common and relevant for this population (48). Based on prior studies, we hypothesized that greater psychotic experiences, specifically PA and paranoid ideation (PI) (18), would be associated with suicidal ideation. We also hypothesized that greater use of maladaptive emotion regulation strategies (i.e., expressive suppression) and decreased use of adaptive emotion regulation strategies (i.e., cognitive reappraisal) would be associated with suicidal ideation. Finally, we hypothesized that psychotic experiences would interact with emotion regulation to predict suicidal ideation, such that individuals with greater psychotic experiences and greater expressive suppression would have the highest rates of suicidal ideation.
Methods
Participants and procedures
Participants included 1,590 adolescents recruited from secondary public schools in Chile from April to September 2019. Participants were recruited from parents’ meetings, where they received information about the project before making a decision about their adolescent’s participation. Inclusion criteria were as follows: (1) ages 12–19 years and (2) written consent provided by both the adolescent and parent/legal guardian. Participants were only excluded if they were outside of the ages of 12–19 years. Participants then completed the self-report questionnaires administered by trained psychologists in a classroom setting. This study was approved by the Bioethics Committee of the University of Talca (02-2021).
Measures
Psychotic experiences
The Community Assessment of Psychic Experiences (CAPE-P15) (49) was used to assess psychotic experiences. The CAPE-P15 is a 15 items self-report measure that assesses BE (7 items), PA (3 items), and PI (5 items). Items were rated on a 1 (never) to 5 (very often) Likert scale (total scores ranging from 15 to 75), with higher scores indicating greater frequency of psychotic experiences. Cronbach’s alpha for the entire sample was 0.80 for PA, 0.82 for PI, and 0.85 for BE.
Suicidal ideation
The Columbia Suicide Severity Rating Scale (C-SSRS) (50) was used to assess suicidal ideation. Consistent with prior studies, items were adapted and administered in a self-report format (51). This self-report version included 7-items that assess suicidal ideation, suicide planning, and preparatory/suicidal behavior (51). Prior research has demonstrated that suicidal ideation and resolved planning/preparation are two distinct constructs (52–56) and that there are distinct risk factors for suicidal ideation and behavior (57, 58). Due to the higher prevalence of suicidal ideation, the current study focused only on suicidal ideation. Two items were used to assess suicidal ideation: (1) Have you wished you were dead or wished you could go to sleep and not wake up and (2) Have you actually had any thoughts of killing yourself? These items were used to create a binary variable for the presence of suicidal ideation.
Emotion regulation
The Emotion Regulation Questionnaire (ERQ) (59) was used to assess emotion regulation. The ERQ is a 10 item self-report measure that assesses the habitual use of cognitive reappraisal (i.e., reinterpreting an emotional event to change an emotion) and expressive suppression (i.e., concealing the outward expression of emotions). Items were rated on a 1 (strongly disagree) to 7 (strongly agree) Likert scale, with higher scores indicating greater use of each strategy. Cronbach’s alpha for the entire sample was 0.83 for cognitive reappraisal and 0.71 for expressive suppression.
Depressive symptoms
The Patient Health Questionnaire-9 (PHQ-9) (60) was used to assess depressive symptoms. The PHQ-9 is a 9-item self-report questionnaire with items rated on a 0 (not at all) to 3 (nearly every day) scale. Total scores range from 0 to 27 with scores 0–4 indicating no depressive symptoms, scores 5–9 indicating mild depressive symptoms, scores 10–14 indicating moderate depressive symptoms, scores 15–29 moderately severe depressive symptoms, and 20–27 indicating severe depressive symptoms. One PHQ-9 item assesses thoughts about wanting to be dead/thoughts of hurting oneself. To prevent criterion contamination, we calculated a total depression score excluding the suicidal ideation item of the PHQ-9. Cronbach’s alpha for the entire sample was 0.89.
Statistical analyses
First, we used descriptive statistics to examine the frequency of lifetime suicidal ideation in our sample. Variables of interest were not normally distributed. Therefore, Mann–Whitney U tests were used to examine whether individuals with and without suicidal ideation differed in psychotic experiences, emotion regulation, and depression. We then used point-biserial correlations to examine the relationship between suicidal ideation, depression, psychotic experiences, and emotion regulation. Multivariate logistic regression was used to determine which variables had the strongest relationship with suicidal ideation. Prior to conducting the logistic regression, we used Chi-square and point-biserial correlations to determine whether age and gender would be included in our model. Using a priori criteria (p < 0.10), we determined that both age and gender would be included as covariates. Logistic regression assumptions were also examined; 22 participants were identified as multivariate outliers and were therefore excluded from the analysis. We also conducted follow-up moderation analyses to examine the relationship between emotion regulation and suicidal ideation among individuals with psychotic experiences. Two separate logistic regression models were conducted with an interaction term for PI/expressive suppression in model 1 and PA/expressive suppression in model 2; multivariate outliers were excluded from each moderation analysis. Simple effects were used to probe significant interaction terms (61, 62).
Results
Participant characteristics and descriptive statistics
Our sample included 1,590 (751 females, 835 males, 4 with no sex reported) Chilean adolescents. The mean age was 15.26 ± 1.35. Lifetime suicidal ideation was present in 48.2% (n = 767) of the sample. Preparatory/suicidal behavior was present in only 2.8% (n = 45) of the total sample. Depressive symptoms (p < 0.001), PI (p < 0.001), BE (p < 0.001), and PA (p < 0.001) were greater among adolescents with suicidal ideation (Table 1). Additionally, adolescents with lifetime suicidal ideation endorsed greater habitual use of expressive suppression (p = 0.001) and cognitive reappraisal (p < 0.001) (Table 1).

Table 1. Depression, psychotic experiences, and emotion regulation among adolescents with and without suicidal ideation.
Correlation analysis
Point-biserial correlations between suicidal ideation, depression, psychotic experiences, and emotion regulation are displayed in Table 2. Suicidal ideation had a moderate association with depression (p < 0.001), PI (p < 0.001), BE (p < 0.001), PA (p < 0.001), and expressive suppression (p < 0.001). The relationship between suicidal ideation and cognitive reappraisal was significant, but small in magnitude.
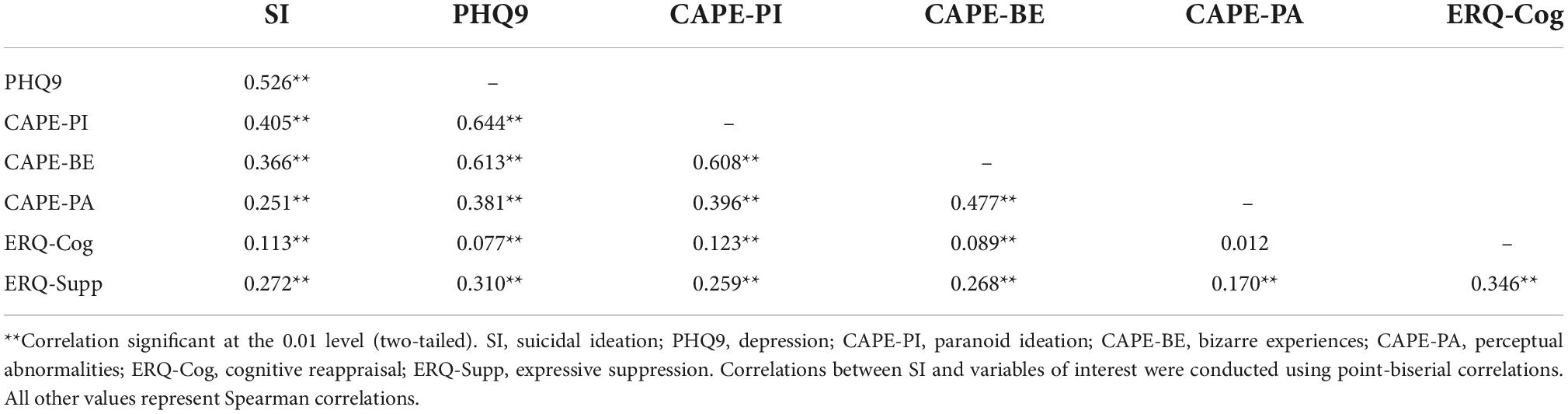
Table 2. Relationship between suicidal ideation, depression, psychotic experiences, and emotion regulation.
Logistic regression
Table 3 summarizes results from the logistic regression. The full model including all predictors was significant χ2(8) = 691.58, p < 0.001], correctly identifying 75.7% of cases and accounting for 35.7% (Cox and Snell R2) to 47.6% (Nagelkerke R2) of variance in lifetime suicidal ideation. Regarding demographic variables, older participants had greater odds of experiencing lifetime suicidal ideation and males had a lower odds of experiencing suicidal ideation relative to females. Depression (OR = 1.277, 95% CI = 1.226–1.330), PI (OR = 1.072, 95% CI = 1.019–1.128), and PA (OR = 1.118, 95% CI = 1.025–1.220) were associated with the presence of suicidal ideation. Additionally, greater use of expressive suppression (OR = 1.063, 95% CI = 1.035–1.092), but not cognitive reappraisal, was associated with suicidal ideation.
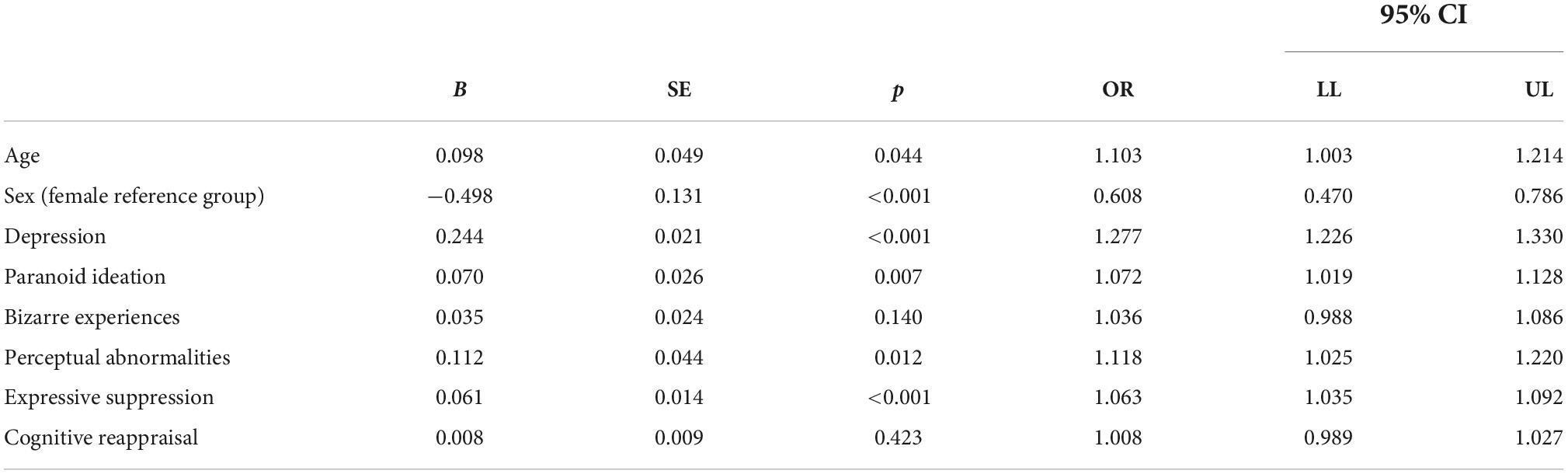
Table 3. Logistic regression examining the relationship between psychotic experiences, depression, emotion regulation, and suicidal ideation (n = 1,568).
Moderation analyses
Two separate moderation analyses were used to examine whether emotion regulation interacts with psychotic experiences to predict suicidal ideation. The first model examined the interaction between PI and expressive suppression when controlling for depression. Multivariate outliers were excluded from this analysis (n = 1,572). The overall model was significant χ2(4) = 670.75, p < 0.001], accounting for 34.7% (Cox and Snell R2) to 46.3% (Nagelkerke R2) of variance in lifetime suicidal ideation. Paranoid ideation significantly interacted with expressive suppression to predict suicidal ideation even when accounting for depressive symptoms (B = −0.009, SE = 0.004, p = 0.035, OR = 0.99, 95% CI = 0.98–0.99). Individuals with high levels of PI had the highest rates of expressive suppression and suicidal ideation (Figure 1). However, the relationship between expressive suppression and suicidal ideation was strongest when PI was low (B = 0.093, SE = 0.018, Z = 5.13, p < 0.001, 95% CI = 0.058–0.129) to moderate (B = 0.060, SE = 0.013, Z = 4.71, p < 0.001, 95% CI = 0.035–0.085). There was no relationship between expressive suppression and suicidal ideation when PI was high (B = 0.027, SE = 0.022, Z = 1.23, p = 0.22, 95% CI = −0.016 to 0.070).
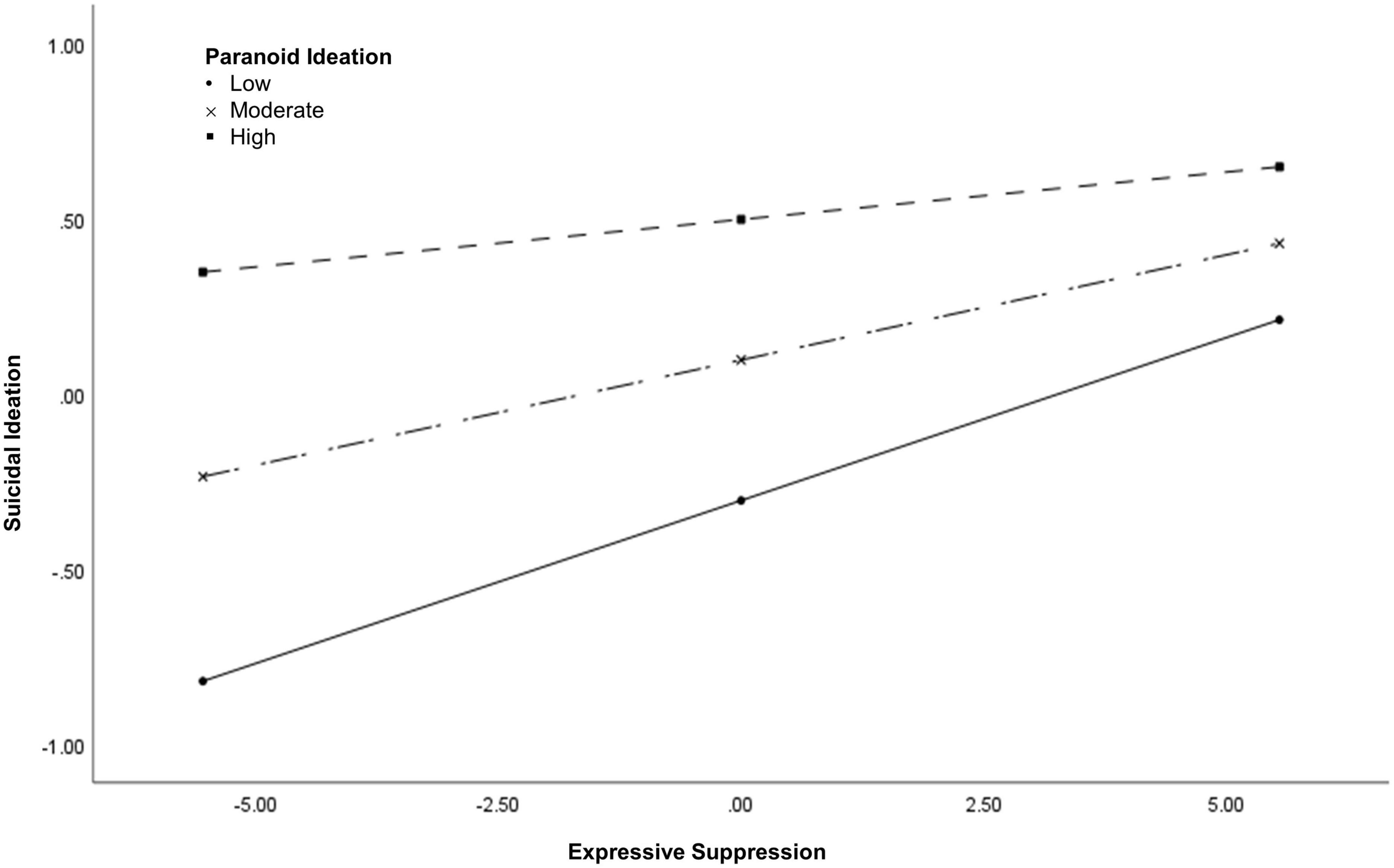
Figure 1. The interaction between paranoid ideation and expressive suppression.
The second model examined the interaction between PA and expressive suppression when controlling for depression. Multivariate outliers were excluded from this analysis (n = 1,575). The overall model was significant χ2(4) = 652.98, p < 0.001], accounting for 33.9% (Cox and Snell R2) to 45.3% (Nagelkerke R2) of variance in lifetime suicidal ideation. Perceptual abnormalities did not interact with expressive suppression to predict suicidal ideation (B = −0.005, SE = 0.008, p = 0.506, OR = 0.995, 95% CI = 0.98−1.01). Rather, PA (B = 0.149, SE = 0.041, p < 0.001, OR = 1.161, 95% CI = 1.072–1.258) and expressive suppression (B = 0.060, SE = 0.012, p < 0.001, OR = 1.061, 95% CI = 1.036–1.087) were independently associated with suicidal ideation.
Discussion
The present study examined the relationship between psychotic experiences, emotion regulation, and suicidal ideation among adolescents in Chile. Nearly half of our sample endorsed lifetime suicidal ideation, suggesting that suicide risk is a major concern for this population. Though these rates of suicidal ideation are high, they are consistent with the broader literature demonstrating that approximately 66% of individuals at clinical high-risk for psychosis experience suicidal ideation (63). The current study also found that adolescents with suicidal ideation had higher rates of psychotic experiences and the presence of suicidal ideation was significantly associated with PI, BE, and PA. These findings are consistent with the broader literature (16, 17), suggesting that psychotic experiences, even among individuals who do not meet diagnostic criteria for a schizophrenia spectrum disorder, are associated with increased risk for suicide. Further research is needed to determine the mechanisms by which psychotic experiences confer increased risk for suicide.
Emotion regulation has repeatedly been identified as a trans-diagnostic mechanism for suicidal thoughts and behaviors (21–24). The current study found that adolescents with suicidal ideation report greater habitual use of both adaptive and maladaptive emotion regulation strategies compared to adolescents without suicidal ideation. Similarly, suicidal ideation was associated with greater use of both cognitive reappraisal and expressive suppression in the entire sample, though the association between cognitive reappraisal and suicidal ideation was small in magnitude. Our finding that adolescents with suicidal ideation have increased use of cognitive reappraisal is somewhat surprising given prior research demonstrating that decreased use of adaptive emotion regulation strategies is associated with suicidal ideation among adults (64). Our results indicate that adolescents with suicidal ideation engage in greater overall efforts to regulate their emotions, rather than only using maladaptive emotion regulation strategies. These inconsistent findings might be attributable to differences in emotion regulation among adolescents versus adults (65, 66) and/or across cultures (46). Additionally, it is possible that adolescents with suicidal ideation engage in more emotion regulation because they experience higher levels of negative affect (67) and/or because their emotion regulation efforts are unsuccessful, thereby warranting increased use of various strategies. Furthermore, the relationship between reappraisal and suicidal ideation might differ depending on the severity of these thoughts; for instance, adolescents with lower severity suicidal ideation might use reappraisal more often than those with higher severity suicidal ideation. Despite these somewhat surprising findings, results from the overall logistic regression model suggest that cognitive reappraisal is no longer associated with suicidal ideation when including psychotic experiences, expressive suppression, depression, and demographic variables in the model. In other words, expressive suppression has a stronger relationship with suicidal ideation than cognitive reappraisal. Although these findings provide preliminary support for the notion that some emotion regulation strategies have a stronger relationship with suicide risk than others, further research is needed to examine other emotion regulation strategies, such as distraction, rumination, emotion suppression, seeking social support, physiological intervention, acceptance (19, 20).
Given the well-established finding that emotion regulation abnormalities exist across the psychosis continuum (14, 25–30), the current study also examined whether psychotic experiences interact with emotion regulation to predict suicidal ideation. Results demonstrate that PI, but not PA, interact with expressive suppression to predict suicidal ideation. Consistent with our hypotheses, individuals with high levels of PI had the highest rates of expressive suppression and suicidal ideation. However, the relationship between expressive suppression and suicidal ideation was actually strongest when PI was low to moderate; additionally, there was no relationship between expressive suppression and suicidal ideation when PI was high. Importantly, expressive suppression involves concealing the outward expression of negative emotions. In the general population, expressive suppression is associated with a wealth of negative consequences, including high blood pressure (68), poor social relationships (68), and suicidal ideation (64). However, for individuals with PI, concealing the outward expression of negative emotions toward others might actually be adaptive, protecting against the negative impact paranoia has on social relationships (69–71). Further, the negative consequences of expressive suppression might be dependent on the specific emotion that an individual is concealing. For instance, concealing the outward expression of paranoia might be adaptive for individuals with psychotic experiences, whereas concealing other emotions such as sadness, anxiety, and anger might lead to negative consequences similar to what is observed in the general population (68). This notion is consistent with broader emotion regulation theories, suggesting that the distinction between adaptive and maladaptive strategies is context dependent and that flexible implementation of various strategies might be key for successful emotion regulation (19, 72). Additional research is needed to determine whether specific emotion regulation strategies are adaptive versus maladaptive within the context of psychotic experiences.
Emotion regulation is widely regarded as a transdiagnostic process, with emotion regulation difficulties presenting across a range of mental health disorders (73, 74). Our findings further support emotion regulation as a transdiagnostic risk factor for suicide as we found that (1) PA and expressive suppression were independently associated with suicidal ideation and (2) that the relationship between expressive suppression and suicidal ideation was strongest when PI was low to moderate. In other words, expressive suppression was not a psychosis specific risk factor for suicidal ideation. Nonetheless, we found that individuals with psychotic experiences engaged in high levels of expressive suppression, which might contribute to the high rates of suicidal ideation in this population. Future longitudinal research is needed to determine whether emotion regulation is a mechanism for suicide risk both in the general population and among individuals with psychotic experiences.
Notable strengths of the current study include (1) our large representative sample, (2) our focus on psychotic experiences among Chilean adolescents, expanding our understanding about suicidal ideation among adolescents from developing countries, and (3) our dimensional approach to assessing psychotic experiences. The current study was limited in the following ways. First, this study involved a cross-sectional design, which precludes our ability to make inferences about the causal nature and direction of the relationship between emotion regulation, psychotic experiences, and suicidal ideation. For instance, it is possible that the relationship between emotion regulation and suicidal ideation is bidirectional, as difficulty regulating negative emotions might lead to suicidal ideation and individuals might engage in emotion regulation strategies to manage suicidal ideation. Research that utilizes ecological momentary assessment would shed light into the temporal patterns associated with emotion regulation and suicidal ideation among individuals with psychosis. Second, the current study focused only on suicidal ideation as an outcome, limiting our understanding about the relationship between psychotic experiences, emotion regulation, and suicidal behavior. Leading suicide theories propose distinct mechanisms for suicidal ideation and suicidal behavior (23, 35, 75). Thus, additional research is needed to examine the relationship between psychotic experiences, emotion regulation, and suicidal behavior. Third, although we recruited from the general population, our sample was limited to adolescents with a relatively narrow age range, limiting the generalizability of our findings. As the onset of psychotic disorders often occurs during late adolescents through young adulthood, additional research that includes young adults is warranted. Finally, the current study did not examine distress associated with psychotic experiences. There is some debate about whether the association between psychotic experiences and suicidal ideation is attributable to third variables such as psychological distress (17). Additional research is needed to determine whether distress influences the relationship between psychotic experiences, emotion regulation, and suicidal ideation.
Conclusion
In summary, the current study found that psychotic experiences and emotion regulation were associated with suicidal ideation among Chilean adolescents. We found that PI, PA, and expressive suppression had the strongest relationship with suicidal ideation, even when accounting for depression and demographic variables. Although PI and expressive suppression interacted to predict suicidal ideation, results from the simple effects suggested that expressive suppression had a stronger relationship with suicidal ideation among individuals with low to moderate PI. Taken together, these findings suggest that expressive suppression is likely a transdiagnostic risk factor for suicidal ideation and that individuals with psychotic experiences might experience higher rates of suicidal ideation because they engage in greater expressive suppression. Additionally, longitudinal research is needed to further examine whether expressive suppression and other maladaptive emotion regulation strategies (i.e., distraction, emotion suppression, and rumination) serve as a mechanism for suicidal ideation both in the general population and among individuals with psychotic experiences.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Bioethics Committee of the University of Talca. Written informed consent to participate in this study was provided by the participants or their legal guardian/next of kin.
Author contributions
DN and HW designed the study. HW conducted the literature search, statistical analyses, and prepared the manuscript. DN provided consultation for statistical analyses and critically revised the manuscript for intellectual content. Both authors contributed to the article and approved the submitted version.
Funding
DN was supported by Fondo de Innovación y Competitividad (FIC_40.001.103-0), ANID – Millennium Science Initiative Program (NCS17_035), and Programa de Investigación Asociativa (PIA) en Ciencias Cognitivas, Facultad de Psicología, Universidad de Talca (RU-158-2019). HW reported a grant from the American Foundation for Suicide Prevention during the conduct of the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Author disclaimer
The content of this manuscript is solely the responsibility of the authors and does not necessarily represent the official views of the American Foundation for Suicide Prevention.
References
1. Moreno-Küstner B, Martín C, Pastor L. Prevalence of psychotic disorders and its association with methodological issues. A systematic review and meta-analyses. PLoS One. (2018) 13:e0195687. doi: 10.1371/journal.pone.0195687
2. Collip D, Wigman JTW, Myin-Germeys I, Jacobs N, Derom C, Thiery E, et al. From epidemiology to daily life: linking daily life stress reactivity to persistence of psychotic experiences in a Longitudinal General Population Study. PLoS One. (2013) 8:e62688. doi: 10.1371/journal.pone.0062688
3. Kelleher I, Wigman JTW, Harley M, O’Hanlon E, Coughlan H, Rawdon C, et al. Psychotic experiences in the population: association with functioning and mental distress. Schizophr Res. (2015) 165:9–14. doi: 10.1016/j.schres.2015.03.020
4. Ronald A, Sieradzka D, Cardno AG, Haworth CMA, McGuire P, Freeman D. Characterization of psychotic experiences in adolescence using the specific psychotic experiences questionnaire: findings from a study of 5000 16-year-old twins. Schizophr Bull. (2014) 40:868–77. doi: 10.1093/schbul/sbt106
5. Cannon TD, Cadenhead K, Cornblatt B, Woods SW, Addington J, Walker E, et al. Prediction of psychosis in youth at high clinical risk: a multisite Longitudinal Study in North America. Arch Gen Psychiatry. (2008) 65:28. doi: 10.1001/archgenpsychiatry.2007.3
6. Lenzenweger MF. Schizotypy 17 years on: psychotic symptoms in midlife. J Abnorm Psychol. (2021) 130:399–412. doi: 10.1037/abn0000680
7. Kaymaz N, Drukker M, Lieb R, Wittchen HU, Werbeloff N, Weiser M, et al. Do subthreshold psychotic experiences predict clinical outcomes in unselected non-help-seeking population-based samples? A systematic review and meta-analysis, enriched with new results. Psychol Med. (2012) 42:2239–53. doi: 10.1017/S0033291711002911
8. Michel C, Ruhrmann S, Schimmelmann BG, Klosterkötter J, Schultze-Lutter F. Course of clinical high-risk states for psychosis beyond conversion. Eur Arch Psychiatry Clin Neurosci. (2018) 268:39–48. doi: 10.1007/s00406-016-0764-8
9. Mackie CJ, Castellanos-Ryan N, Conrod PJ. Developmental trajectories of psychotic-like experiences across adolescence: impact of victimization and substance use. Psychol Med. (2011) 41:47–58. doi: 10.1017/S0033291710000449
10. Stefanis NC, Delespaul P, Henquet C, Bakoula C, Stefanis CN, Van Os J. Early adolescent cannabis exposure and positive and negative dimensions of psychosis. Addiction. (2004) 99:1333–41. doi: 10.1111/j.1360-0443.2004.00806.x
11. Sun M, Hu X, Zhang W, Guo R, Hu A, Mwansisya TE, et al. Psychotic-like experiences and associated socio-demographic factors among adolescents in China. Schizophr Res. (2015) 166:49–54. doi: 10.1016/j.schres.2015.05.031
12. Wigman JTW, van Nierop M, Vollebergh WAM, Lieb R, Beesdo-Baum K, Wittchen HU, et al. Evidence that psychotic symptoms are prevalent in disorders of anxiety and depression, impacting on illness onset, risk, and severity–implications for diagnosis and ultra-high risk research. Schizophr Bull. (2012) 38:247–57. doi: 10.1093/schbul/sbr196
13. Kline E, Thompson E, Bussell K, Pitts SC, Reeves G, Schiffman J. Psychosis-like experiences and distress among adolescents using mental health services. Schizophr Res. (2014) 152:498–502. doi: 10.1016/j.schres.2013.12.012
14. Vines L, Bridgwater M, Bachman P, Hayes R, Catalano S, Jalbrzikowski M. Elevated emotion reactivity and emotion regulation in individuals at clinical high risk for developing psychosis and those diagnosed with a psychotic disorder. Early Interv Psychiatry. (2021) 16:724–735. doi: 10.1111/eip.13212
15. McGrath JJ, Saha S, Lim CCW, Aguilar-Gaxiola S, Alonso J, Andrade LH, et al. Trauma and psychotic experiences: transnational data from the World Mental Health Survey. Br J Psychiatry. (2017) 211:373–80. doi: 10.1192/bjp.bp.117.205955
16. Huang X, Fox KR, Ribeiro JD, Franklin JC. Psychosis as a risk factor for suicidal thoughts and behaviors: a meta-analysis of longitudinal studies. Psychol Med. (2018) 48:765–76. doi: 10.1017/S0033291717002136
17. Honings S, Drukker M, Groen R, van Os J. Psychotic experiences and risk of self-injurious behaviour in the general population: a systematic review and meta-analysis. Psychol Med. (2016) 46:237–51. doi: 10.1017/S0033291715001841
18. Núñez D, Fresno A, van Borkulo CD, Courtet P, Arias V, Garrido V, et al. Examining relationships between psychotic experiences and suicidal ideation in adolescents using a network approach. Schizophr Res. (2018) 201:54–61. doi: 10.1016/j.schres.2018.05.020
19. Gross JJ. Emotion regulation: current status and future prospects. Psychol Inq. (2015) 26:1–26. doi: 10.1254/fpj.151.21
21. Anestis MD, Bagge CL, Tull MT, Joiner TE. Clarifying the role of emotion dysregulation in the interpersonal-psychological theory of suicidal behavior in an undergraduate sample. J Psychiatr Res. (2011) 45:603–11. doi: 10.1016/j.jpsychires.2010.10.013
22. Bryan CJ, Wood DS, May A, Peterson AL, Wertenberger E, Rudd MD. Mechanisms of action contributing to reductions in suicide attempts following brief cognitive behavioral therapy for military personnel: a test of the interpersonal-psychological theory of suicide. Arch Suicide Res. (2018) 22:241–53. doi: 10.1080/13811118.2017.1319313
23. Klonsky ED, Saffer BY, Bryan CJ. Ideation-to-action theories of suicide: a conceptual and empirical update. Curr Opin Psychol. (2018) 22:38–43. doi: 10.1016/j.copsyc.2017.07.020
24. Linehan M. Cognitive-Behavioral Treatment of Borderline Personality Disorder. New York: NY: Guilford Press (1993).
25. Ludwig L, Werner D, Lincoln TM. The relevance of cognitive emotion regulation to psychotic symptoms – A systematic review and meta-analysis. Clin Psychol Rev. (2019) 72:101746. doi: 10.1016/j.cpr.2019.101746
26. O’Driscoll C, Laing J, Mason O. Cognitive emotion regulation strategies, alexithymia and dissociation in schizophrenia, a review and meta-analysis. Clin Psychol Rev. (2014) 34:482–95. doi: 10.1016/j.cpr.2014.07.002
27. Chapman HC, Visser KF, Mittal VA, Gibb BE, Coles ME, Strauss GP. Emotion regulation across the psychosis continuum. Dev Psychopathol. (2020) 32:219–27. doi: 10.1017/S0954579418001682
28. Prochwicz K, Kłosowska J, Sznajder D. The role of expressive suppression in hallucinatory-like and delusion-like experiences. Findings in a non-clinical sample. Compr Psychiatry. (2018) 82:121–7. doi: 10.1016/j.comppsych.2018.02.001
29. Gong J, Luo Y, He Y, Zhou L, Zhao L, Liu J. Epidemiology of psychotic-like experiences by subtypes and their relationship with emotional regulation and affective lability among Chinese college students. Schizophr Res. (2022) 244:39–45. doi: 10.1016/j.schres.2022.02.037
30. Kimhy D, Gill KE, Brucato G, Vakhrusheva J, Arndt L, Gross JJ, et al. The impact of emotion awareness and regulation on social functioning in individuals at clinical high risk for psychosis. Psychol Med. (2016) 46:2907–18. doi: 10.1017/S0033291716000490
31. Liu J, Chua JJ, Chong SA, Subramaniam M, Mahendran R. The impact of emotion dysregulation on positive and negative symptoms in schizophrenia spectrum disorders: a systematic review. J Clin Psychol. (2020) 76:612–24. doi: 10.1002/jclp.22915
32. Langer ÁI, Wardenaar K, Wigman JTW, Ulloa JL, Núñez D. A latent profile analysis of psychotic experiences, non-psychotic symptoms, suicidal ideation and underlying mechanisms in a sample of adolescents from the general population. Front Psychiatry. (2022) 13:926556. doi: 10.3389/fpsyt.2022.926556
33. Strauss GP, Zamani Esfahlani F, Visser KF, Dickinson EK, Gruber J, Sayama H. Mathematically modeling emotion regulation abnormalities during psychotic experiences in schizophrenia. Clin Psychol Sci. (2019) 7:216–33. doi: 10.1177/2167702618810233
34. Baumeister RE. Suicide as escape from self. Psychol Rev. (1990) 97:90–113. doi: 10.1037/0033-295X.97.1.90
35. Klonsky ED, May AM. The three-step theory (3ST): a new theory of suicide rooted in the “ideation-to-action” framework. Int J Cogn Ther. (2015) 8:114–29. doi: 10.1521/ijct.2015.8.2.114
37. O’Connor RC. The integrated motivational-volitional model of suicidal behavior. Crisis. (2011) 32:295–8. doi: 10.1027/0227-5910/a000120
38. Rudd MD. Fluid vulnerability theory: a cognitive approach to understanding the process of acute and chronic risk. In: Ellis TE editor. Cognition and Suicide: Theory, Research, and Therapy. Washington, DC: American Psychological Association (2006). doi: 10.1037/11377-016
39. Bryan CJ, Rozek DC. Suicide prevention in the military: a mechanistic perspective. Curr Opin Psychol. (2018) 22:27–32. doi: 10.1016/j.copsyc.2017.07.022
40. Grattan RE, Tryon VL, Carter CS, Niendam TA. Suicide behavior is associated with childhood emotion dysregulation but not trait impulsivity in first episode psychosis. Psychiatry Res. (2020) 294:113517. doi: 10.1016/j.psychres.2020.113517
41. Johnson J, Gooding PA, Wood AM, Taylor PJ, Pratt D, Tarrier N. Resilience to suicidal ideation in psychosis: positive self-appraisals buffer the impact of hopelessness. Behav Res Ther. (2010) 48:883–9. doi: 10.1016/j.brat.2010.05.013
42. Chang WC, Chen ESM, Hui CLM, Chan SKW, Lee EHM, Chen EYH. The relationships of suicidal ideation with symptoms, neurocognitive function, and psychological factors in patients with first-episode psychosis. Schizophr Res. (2014) 157:12–8. doi: 10.1016/j.schres.2014.06.009
43. Hielscher E, DeVylder J, Hasking P, Connell M, Martin G, Scott JG. Mediators of the association between psychotic experiences and future non-suicidal self-injury and suicide attempts: results from a three-wave, prospective adolescent cohort study. Eur Child Adolesc Psychiatry. (2021) 30:1351–65. doi: 10.1007/s00787-020-01593-6
44. Wüsten C, Schlier B, Jaya ES. Genetic risk and outcome of psychosis (GROUP) Investigators, Alizadeh BZ, Bartels-Velthuis AA, et al. Psychotic experiences and related distress: a cross-national comparison and network analysis based on 7141 participants from 13 countries. Schizophr Bull. (2018) 44:1185–94. doi: 10.1093/schbul/sby087
45. Wasserman D, Cheng Q, Jiang GX. Global suicide rates among young people aged 15-19. World Psychiatry. (2005) 7:114–20.
46. Ford BQ, Mauss IB. Culture and emotion regulation. Curr Opin Psychol. (2015) 3:1–5. doi: 10.1016/j.copsyc.2014.12.004
47. Mokdad AH, Forouzanfar MH, Daoud F, Mokdad AA, El Bcheraoui C, Moradi-Lakeh M, et al. Global burden of diseases, injuries, and risk factors for young people’s health during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. (2016) 387:2383–401. doi: 10.1016/S0140-6736(16)00648-6
48. Núñez D, Monjes P, Campos S, Wigman JTW. Evidence for specific associations between depressive symptoms, psychotic experiences, and suicidal ideation in chilean adolescents from the general population. Front Psychiatry. (2021) 11:552343. doi: 10.3389/fpsyt.2020.552343
49. Capra C, Kavanagh DJ, Hides L, Scott JG. Current CAPE-15: a measure of recent psychotic-like experiences and associated distress: a measure of recent PLEs. Early Interv Psychiatry. (2017) 11:411–7. doi: 10.1111/eip.12245
50. Posner K, Brown GK, Stanley B, Brent DA, Yershova KV, Oquendo MA, et al. The Columbia–Suicide severity rating scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. (2011) 168:1266–77. doi: 10.1176/appi.ajp.2011.10111704
51. Núñez D, Arias V, Méndez-Bustos P, Fresno A. Is a brief self-report version of the Columbia severity scale useful for screening suicidal ideation in Chilean adolescents? Compr Psychiatry. (2019) 88:39–48. doi: 10.1016/j.comppsych.2018.11.002
52. Baertschi M, Costanza A, Canuto A, Weber K. The dimensionality of suicidal ideation and its clinical implications. Int J Methods Psychiatr Res. (2019) 28:e1755. doi: 10.1002/mpr.1755
53. Holden RR, Mendonca JD, Mazmanian D. Relation of response set to observed suicide intent. Can J Behav Sci Rev Can Sci Comport. (1985) 17:359–68. doi: 10.1016/j.pscychresns.2018.11.007
54. Holden RR, DeLisle MM. Factor analysis of the beck scale for suicide ideation with female suicide attempters. Assessment. (2005) 12:231–8. doi: 10.1177/1073191105274925
55. Joiner T, Rudd D, Rajab H. The modified scale for suicidal ideation: factors of suicidality and their relation to clinical and diagnostic variables. J Abnorm Psychol. (1997) 106:260–5. doi: 10.1037/0021-843X.106.2.260
56. Steer RA, Rissmiller DJ, Ranieri WF, Beck AT. Dimensions of suicidal ideation in psychiatric inpatients. Behav Res Ther. (1993) 31:229–36. doi: 10.1016/0005-7967(93)90090-H
57. Franklin JC, Ribeiro JD, Fox KR, Bentley KH, Kleiman EM, Huang X, et al. Risk factors for suicidal thoughts and behaviors: a meta-analysis of 50 years of research. Psychol Bull. (2017) 143:187–232.
58. Cassidy RM, Yang F, Kapczinski F, Passos IC. Risk factors for suicidality in patients with schizophrenia: a systematic review, meta-analysis, and meta-regression of 96 studies. Schizophr Bull. (2018) 44:787–97. doi: 10.1093/schbul/sbx131
59. Gross JJ, John OP. Individual differences in two emotion regulation processes: implications for affect, relationships, and well-being. J Pers Soc Psychol. (2003) 85:348–62. doi: 10.1037/0022-3514.85.2.348
60. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
61. Bauer DJ, Curran PJ. Probing interactions in fixed and multilevel regression: inferential and graphical techniques. Multivar Behav Res. (2005) 40:373–400. doi: 10.1207/s15327906mbr4003_5
62. Rogosa D. Comparing nonparallel regression lines. Psychol Bull. (1980) 88:307–21. doi: 10.1037/0033-2909.88.2.307
63. Taylor PJ, Hutton P, Wood L. Are people at risk of psychosis also at risk of suicide and self-harm? A systematic review and meta-analysis. Psychol Med. (2015) 45:911–26. doi: 10.1017/S0033291714002074
64. Forkmann T, Scherer A, Böcker M, Pawelzik M, Gauggel S, Glaesmer H. The relation of cognitive reappraisal and expressive suppression to suicidal ideation and suicidal desire. Suicide Life Threat Behav. (2014) 44:524–36. doi: 10.1111/sltb.12076
65. McRae K, Gross JJ, Weber J, Robertson ER, Sokol-Hessner P, Ray RD, et al. The development of emotion regulation: an fMRI study of cognitive reappraisal in children, adolescents and young adults. Soc Cogn Affect Neurosci. (2012) 7:11–22. doi: 10.1093/scan/nsr093
66. Tottenham N, Hare TA, Casey BJ. Behavioral assessment of emotion discrimination, emotion regulation, and cognitive control in childhood, adolescence, and adulthood. Front Psychol. (2011) 2:39. doi: 10.3389/fpsyg.2011.00039
67. Rojas SM, Leen-Feldner EW, Blumenthal H, Lewis SF, Feldner MT. Risk for suicide among treatment seeking adolescents: the role of positive and negative affect intensity. Cogn Ther Res. (2015) 39:100–9. doi: 10.1007/s10608-014-9650-8
68. Butler EA, Egloff B, Wlhelm FH, Smith NC, Erickson EA, Gross JJ. The social consequences of expressive suppression. Emotion. (2003) 3:48–67. doi: 10.1037/1528-3542.3.1.48
69. Pinkham AE, Harvey PD, Penn DL. Paranoid individuals with schizophrenia show greater social cognitive bias and worse social functioning than non-paranoid individuals with schizophrenia. Schizophr Res Cogn. (2016) 3:33–8. doi: 10.1016/j.scog.2015.11.002
70. Fan L, Bass E, Klein H, Springfield C, Pinkham A. A preliminary investigation of paranoia variability and its association with social functioning. Schizophr Res Cogn. (2022) 29:100258.
71. Hajdúk M, Klein HS, Harvey PD, Penn DL, Pinkham AE. Paranoia and interpersonal functioning across the continuum from healthy to pathological - Network analysis. Br J Clin Psychol. (2019) 58:19–34. doi: 10.1111/bjc.12199
72. Aldao A. The future of emotion regulation research: capturing context. Perspect Psychol Sci. (2013) 8:155–72.
73. Beauchaine TP, Cicchetti D. Emotion dysregulation and emerging psychopathology: a transdiagnostic, transdisciplinary perspective. Dev Psychopathol. (2019) 31:799–804. doi: 10.1017/S0954579419000671
74. Cludius B, Mennin D, Ehring T. Emotion regulation as a transdiagnostic process. Emotion. (2020) 20:37–42.
Keywords: psychotic experiences, psychosis proneness, suicide risk, adolescence, developing countries
Citation: Wastler HM and Núñez D (2022) Psychotic experiences, emotion regulation, and suicidal ideation among Chilean adolescents in the general population. Front. Psychiatry 13:983250. doi: 10.3389/fpsyt.2022.983250
Received: 30 June 2022; Accepted: 24 October 2022;
Published: 16 November 2022.
Edited by:
Sahar Obeid, Holy Spirit University of Kaslik, LebanonReviewed by:
Clara Rahme, Psychiatric Hospital of the Cross, LebanonDorota Frydecka, Wrocław Medical University, Poland
Copyright © 2022 Wastler and Núñez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniel Núñez, dnunez@utalca.cl