Corrigendum: Efficacy and executive function of solution-focused brief therapy on adolescent depression
 Haisi Chen
Haisi Chen Mengmeng Zhou
Mengmeng Zhou Li Han1
Li Han1 Advaith Manoharasetty
Advaith Manoharasetty Hong Luo
Hong Luo- 1Affiliated Mental Health Center & Hangzhou Seventh People’s Hospital, Zhejiang University School of Medicine, Hangzhou, China
- 2Internal Medicine Department, Hangzhou Linping District Maternal and Child Care Hospital, Hangzhou, China
- 3Institute for International Education, Zhejiang Chinese Medical University, Hangzhou, China
Objective: To investigate the efficacy and impact on executive function of Solution-Focused Brief Therapy (SFBT) in treating Major Depressive Disorder (MDD) in adolescents.
Methods: A total of 129 adolescents diagnosed with MDD were enrolled in the study. Out of these, 28 adolescents were assigned to the SFBT group, while 25 were part of the Active Control group (AC group), receiving psychodynamic psychotherapy. Executive function, depressive and anxiety symptoms were assessed at baseline, at the time of the third intervention, the sixth intervention, and the 10th intervention.
Results: After the third intervention, the scores of the Patient Health Questionnaire-9 (PHQ-9) and Generalized Anxiety Disorder-7 (GAD-7) of the participants in the SFBT group decreased significantly, which had the cumulative effect at the 6th and 10th interventions. The verbal fluency task (VFT) performances of the SFBT group participants yielded significantly higher scores after the third intervention and remained increasing at the 6th and 10th interventions. The AC group steadily decreased after the intervention. Analysis of functional near-infrared spectroscopy (fNIRS) data revealed a progressive and significant increase in the average oxyhemoglobin (oxy-Hb) levels in the dorsolateral prefrontal cortex (DLPFC) in the SFBT group compared to the AC group after the 10th intervention.
Conclusions: SFBT might improve depressive and anxiety symptoms as well as executive function of adolescent depression.
Clinical trial registration: https://www.chictr.org.cn, identifier ChiCTR2300067909.
Introduction
According to the study, many adults with depression recall that their first depressive episode dates back to their teenage years (1). The diagnosis and treatment of Major Depressive Disorder (MDD) in adolescents are complicated by factors such as diminished self-awareness of depressive symptoms, heightened emotional volatility, and the subjective nature of clinical evaluations. Although antidepressants are the first-line treatment for depression, 50% of patients do not respond to early treatment, and it is difficult to predict the response to treatment at the onset (2). The prevalence of adolescent depression is 5.2~7.5%, and with higher prevalence among females than males (3). The latest survey report on the prevalence of mental illness in children and adolescents in China shows that the prevalence of depression in adolescents is as high as 3% (4). Numerous prevalence studies suggest that 8 to 20% adolescent depression is associated with poor relationships, academic failure, substance abuse, major depressive disorder, suicide, and other psychiatric disorders in adulthood, which predict an increased risk of lifelong dysfunction (5). However, current treatment options for adolescents suffered from depression remain limited.
According to the recommendations, psychotherapy is considered the first choice of initial treatment for adolescents with mild to moderate depression (6). Given guidelines recommend a combination of antidepressants and a recognized psychotherapy for moderate-to-severe adolescent depression. Most studies focused on Cognitive Behavioral Therapy or Interpersonal Therapy, but none of the studies have focused on Solution-Focused Brief Therapy (SFBT) as the treatment of adolescent depression (7). SFBT shifts the focus away from problem formation and problem resolution to participants’ future goals, strengths, and resiliency. In SFBT, a professional collaborates with the client to look for solutions to obtain goals and strongly stresses the client’s autonomy and competencies to achieve them (8). According to several meta-analyses and reviews, it has positive effects in a broad range of settings and problem areas (8–10). The latest and most extensive analysis, which includes five studies, centers on adult depression as a result (8). However, none of these investigations addressed depression in adolescents.
Functional near-infrared spectroscopy (fNIRS) is a real-time and non-invasive neuroimaging technique. Many studies have combined fNIRS and the verbal fluency task (VFT) to evaluate executive function, which refers to a series of neuropsychological abilities including maintaining attention, and flexibly changing goals and plans according to changing events (11). The prefrontal cortex is a key center for combining cognitive control and emotion regulation, which is closely associated with cognitive function and emotion regulation (12). Findings from several prior research efforts have indicated that patients with MDD exhibit reduced prefrontal cortex oxyhemoglobin (oxy-Hb) responses and suboptimal activation levels during cognitive challenges (13).
The present study was designed to remedy the relative lack of attention paid to the efficacy and executive function of SFBT on emotional regulation in adolescent depression. It was a preliminary exploration of efficacy and executive function of SFBT in clinical practice from the aspects of subjective scale evaluation and objective evaluation via near-infrared imaging spectrum.
Method
Participants
Consecutive outpatients with MDD were enrolled (N=129) from November 2021, underwent screening over a period of 12 months. To be eligible for this study, participants had to satisfy following inclusionary criteria (1): patients were aged 12–18 years (2); patients with DSM-IV clinical criteria for the major depressive episode using the Mini-International Neuropsychiatric Interview (MINI) by two psychiatrists who had at least 5 years of clinical experience. Important exclusion criteria were as follows (1): patients were diagnosed with mental retardation, psychosis, bipolar disorder, or obsessive–compulsive disorder, post traumatic stress disorder or eating disorders defined by DSM-IV; (2) The treatment history of electroconvulsive therapy or psychotherapy; (3) The presence of self-injury behavior or suicidal attempts during interview.
This study was registered at https://www.chictr.org.cn and the registration identification number was ChiCTR2300067909. The study was approved by the Institutional Review Board (IRB) of the Affiliated Hospital of Hangzhou Normal University (Hangzhou, China; 2022 (E2)-HS-076).
Treatments
The therapies
The study was non-randomized concurrent controlled trial (Non-R), for the consideration of various factors such as the patient’s condition, autonomous selectivity and flexible treatment time. Participants were allocated to either the SFBT group or the Active Control group (AC group), which received psychodynamic psychotherapy, according to their preference for the therapeutic approach. However, participants were kept unaware of the specific details of the psychological treatment they received, yet informed about the study’s general purpose and potential implications. For the SFBT group, subjects received solution-focused therapy a brief resource-oriented and goal-focused therapeutic approach, which helps clients change by constructing solutions (14). The technique includes the search for pre-session change, miracle and scaling questions, exploration of exceptions, use of a one-way mirror and consulting break, positive feedback and home assignments. The orientation was based on an approach developed by De Shazer and Berg (15).
For the AC group, subjects received short-term psychodynamic psychotherapy, a brief, focal, transference-based therapeutic approach which helps patients by exploring and working through specific intra-psychic and interpersonal conflicts. Short-term psychodynamic psychotherapy is characterized by the exploration of a focus, which can be identified by both the therapist and the patient (16).
Ensure that all participants follow the same procedures and receive the same instructions, conducted at a separate physical location from the treatment sessions, regardless of their group assignment. The SFBT group and AC group received different intervention modalities, and the participants in the two groups remained consistent in the duration of a single intervention (40-60 minutes/session). But the interval between each intervention was not fixed, for it was decided by the therapist and patient discussion.
The therapists
The therapist in SFBT group had been trained for the method and received a qualification in solution-focused therapy provided by a local institute and had nearly 20 years of experience in solution-focused therapy without any training in psychodynamic psychotherapy. The therapist providing psychodynamic psychotherapy had received standard training in psychoanalytically orientated psychotherapy that was approved by one of the psychoanalytic or psychodynamic training institutes without any experience of solution-focused therapy.
In psychodynamic psychotherapies, the therapies were conducted in accordance with clinical practice, where the therapists might modify their interventions according to a patient’s needs within the framework of psychodynamic therapies. Accordingly, no adherence monitoring was organized and no manuals were used.
Measures
Clinical measurement
The measurements were carried out as ratings based on interviews and mental health questionnaires. such as the Patient Health Questionnaire-9 (PHQ-9) and Generalized Anxiety Disorder-7 (GAD-7). The assessments were completed at baseline examination and during follow-up at 3rd, 6th, 10th intervention.
The PHQ-9 (17) is a nine-item instrument that screens for the presence and severity of depression. It asks the patient about their experiences over the preceding 2 weeks. Scores range from 0 to 27. In general, a score ≥10 suggests depression.
GAD-7 (18) is a self-report instrument to assess the severity of anxiety in general. GAD-7 has seven items and scores range from 0 to 21. Greater scores indicate greater anxiety over the preceding 2 weeks.
The verbal fluency task (VFT) has been widely used to study executive capability in depression, which has been purported to be associated with cognitive impairment (19, 20). During the pre- and post-task baseline periods, the participants were asked to repeat counting from 1 to 5. During the task period, the participants were required to construct as many phrases as possible using three commonly used characters, such as “蓝” (blue), “大” (big), and “天” (sky). The three given characters changed every 20 s during the task period to reduce the time during which the subjects were silent (21).
NIRS measurement
The participants were seated comfortably in a quiet room, and hemoglobin concentrations were measured using a multi-channel near infrared optical imaging system (NirScan, Danyang Huichuang Medical Equipment Co., Ltd., China). The FPz channel was used (10/20 international system) as the center of the middle probe; a total of 19 single-distance (SD) probes (consisting of 7 sources and 7 detectors) with a fixed 3-cm inter-probe distance were placed to cover each subject’s bilateral prefrontal cortex. The integral value of oxy-Hb of the bilateral frontal lobe were used to characterize brain activation in adolescent depression.
Data processing and analysis
We used the NirSpark software package (HuiChuang, China) to analyze NIRS data. Data were preprocessed via the following steps. Motion artifacts were corrected by a moving SD and a cubic spline interpolation method. A bandpass filter with cut-off frequencies of 0.01–0.20 Hz was used to remove physiological noise (e.g., respiration, cardiac activity, and low-frequency signal drift). The modified Beer-Lambert law was used to convert optical densities into changes in oxy-Hb and deoxy-Hb concentrations. Oxy-Hb was used as the primary indicator in this analysis because it generally has a better signal-to-noise ratio than Deoxy-Hb (22). We used a 60-s task period of constructing phrases as the time window to analyze mean oxy-Hb changes. Linear fitting was applied to the data between these two baselines. The primary outcomes measured were the levels of depression and anxiety, alongside the average active oxy-Hb values of fNIRs during the VFT. The severity of depression was quantified by the PHQ-9 and anxiety symptoms were assessed by the GAD-7.
Statistical analysis
Statistical analyses were performed using SPSS Version 25.0. The NirSpark software package, GraphPad Prism 8, and Adobe Illustrator software were used to generate figures and graphs. Independent sample t-tests were used to investigate the differences between groups. A paired sample t-test or repeated-measures analysis of variance (ANOVA) was performed for standard distribution data. Data normality was tested via the Shapiro-Wilk test. The demographic and clinical data were compared by t-tests or chi-square tests. Student’s t-test was used to analyze differences in age and education level between the SFBT group and the AC group at baseline.
We used a two-way mixed ANOVA with different groups (SFBT group vs. AC group) as the between-subject factor and time (T0、T3、T6、T10) as the within-subject factor to analyze the effect of the SFBT therapy intervention on the oxy-Hb values. The two-way mixed ANOVA included a 4 (time point: T0、T3、T6、T10) × 2 (group: SFBT group and AC group) design.
Functional connectivity was analyzed by performing Spearman’s correlation between the time series of each channel-to-channel pair. A p-value less than 0.05 was considered statistically significant, and all p-values were two-tailed.
Results
A total of 129 adolescent depression who met the inclusion criteria were enrolled and underwent baseline measurements. 47 patients were excluded for the following reasons (1): they discontinued treatment for getting recovered (N=8); (2) they had to be hospitalized for suicidal attempt (N=2); (3) they refused to participate in the study (n = 37) (shown in Figure 1). Of the patients starting the therapy a total of 29 patients discontinued the treatment prematurely.
Figure 1
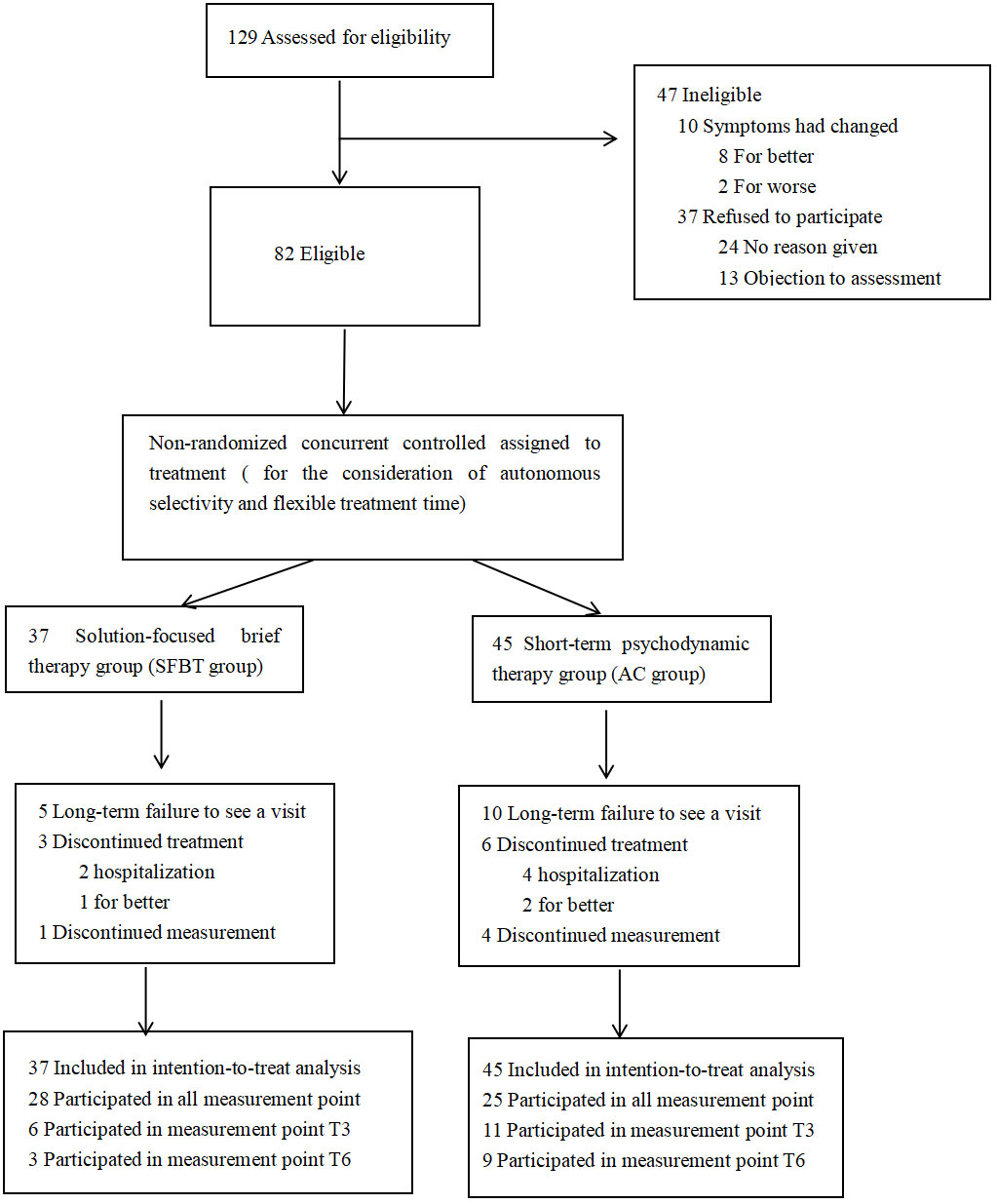
Figure 1 Number of patients assessed for eligibility, assigned to study group, and who completed the protocol.
The remaining 82 participants underwent long-term follow-up. Among the 37 participants who enrolled in the SFBT group, 28 of them completed the full 10-session intervention program and provided comprehensive post-test data at T3, T6, and T10. In the AC group, which initially had 45 participants, 25 persisted through to the final intervention and also provided complete post-test data at the same three time points. As shown in Figure 1.
Demographic and clinical characteristics
The demographic characteristics of participants in each group are presented in Table 1. The SFBT group included 9 males and 19 females (mean age = 15.11 years; SD = 1.42). The AC group included 5 males and 20 females (mean age = 14.80 years; SD = 1.41). Both groups showed no difference in age, gender or education (P > 0.05). No statistically significant differences among treatment groups were found with respect to medication at baseline. As shown in Table 1.
Table 1
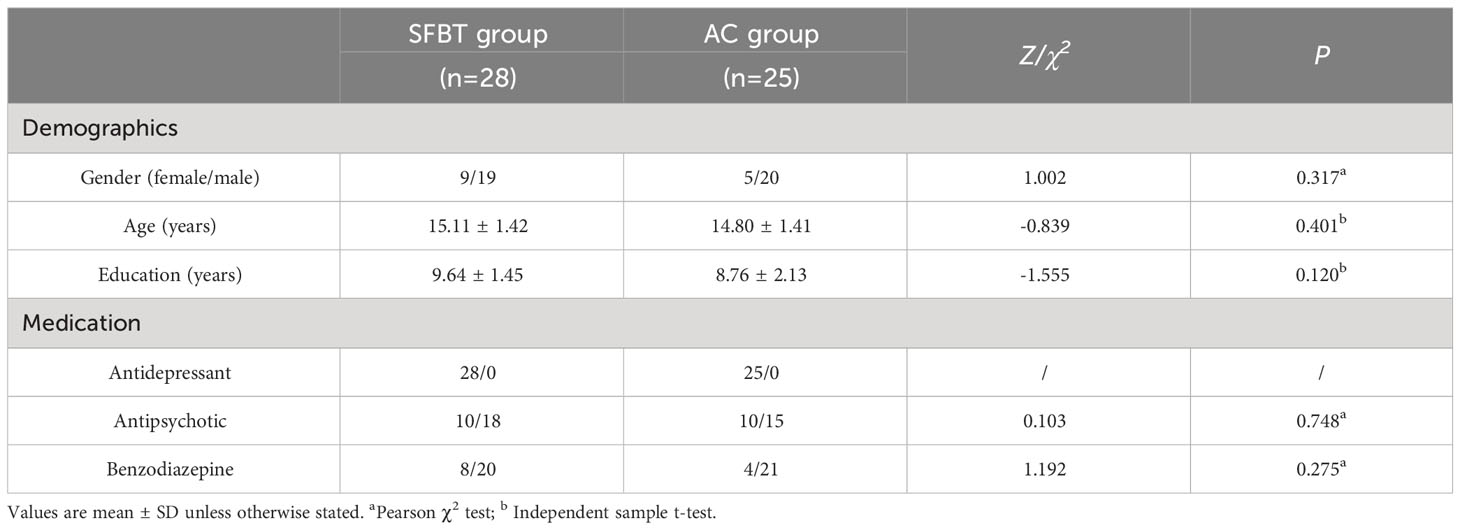
Table 1 Demographic data of the SFBT group and AC group (mean ± SD).
Clinical data and VFT task performance of participants before and after therapy
Clinical data
The results showed that the main effect of time point was significant [F (3,49)=9.865, P<0.001,η2 = 0.377], meaning that PHQ-9 scores decreased after therapy in all participants (see Table 2). The main effect of Group was not significant [F (1, 51)=2.293, P=0.136]. The interaction between Group and Time point was significant [F (3, 49)=2.969, P=0.056, η2 = 0.142]. Simple effect analysis revealed that the PHQ-9 scores in both two groups were significantly reduced at T3, T6, T10 assessment compared with the T0 point (P < 0.05). The simple effect analysis also showed no significant difference in PHQ-9 scores between the two groups at T0, T3, and T10. However, at T6, the SFBT group had significantly lower PHQ-9 scores than the AC group (P=0.006).
Table 2
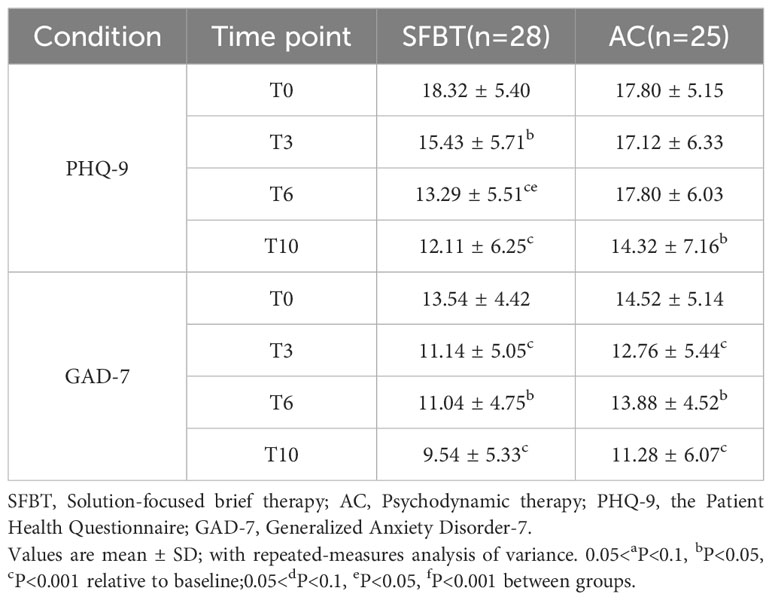
Table 2 Clinical data of SFBT group and controls (mean ± SD).
The GAD-7 was employed to assess the severity of anxiety in the SFBT group and AC group. The results showed that the main effect of time point was significant [F (3,49)=11.148, P<0.001,η2 = 0.406], meaning that GAD-7 scores decreased after therapy in all participants (refer to Table 2). The main effect of Group was not significant [F (1, 51)=2.618, P=0.112]. The interaction between Group and Time point was not significant [F (3, 49)=0.589, P=0.625].
Additional post hoc analyses found that the GAD-7 scores of T3, T6 and T10 were significantly lower than that of T0 (P<0.05). The GAD-7 scores of T10 showed a marginal significant lower than the score at T3 (P=0.061), and was significantly lower than the scores at T6 (P=0.002). No significant differences were found in the GAD-7 scores between the other time points (P>0.1). As shown in Table 2.
VFT task performance
During the VFT task, the number of words generated by the SFBT and AC groups are summarized in Table 3. The results showed that the main effect of Group was significant [F (1,51) = 8.752, P = 0.005, η2 = 0.146], meaning that the performances on the VFT task in the SFBT group were higher than those in the AC group. The main effect of Time point was not significant [F (3,49) = 0.143, P = 0.934]. The interaction between Group and Time point was significant [F (3,49) = 4.473, P = 0.005, η2 = 0.081]. There was no significant difference in the performances on the VFT task at T0 (P=0.980), while the SFBT group were significantly higher than those in the AC group in the time of T3, T6 and T10 (P<0.05). As shown in Table 3.
Table 3
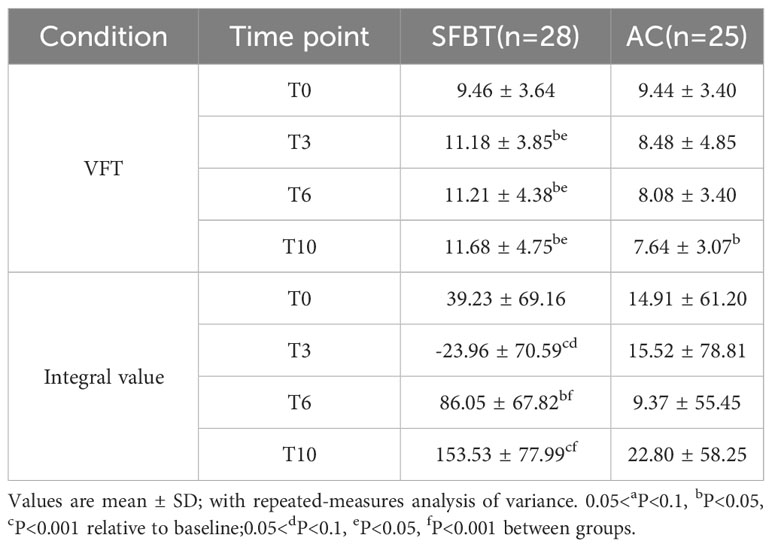
Table 3 VFT task performance and the mean integral value of oxy-Hb of the frontal lobe area during VFT (mean ± SD).
The integral value of oxy-Hb in the frontal lobe
The results showed that the main effect of Time point was significant [F (1,51)=12.559, P=0.001,η2 = 0.198] and the interaction between Group and Time point was significant [F (3, 49)=1.960, P<0.001, η2 = 0.494]. The integral value of oxy-Hb at T10 was significantly higher than that at T0, T3, T6 (P<0.05) in SFBT group. While there was no significant difference in the integral value of oxy-Hb in AC group at the time point of T0, T3, T6 and T10 (P>0.1). As shown in Table 3.
Figure 2 demonstrates the integral value of oxy-Hb in the frontal lobe of the SFBT group and AC group during the task of VFT. It can be seen that there was no significant difference in the integral value of oxy-Hb between the SFBT group and the AC group at baseline. However, the SFBT group exhibited a marginally significant lower integral value of oxy-Hb compared to the AC group (P=0.060). At T6 and T10, the integral value of oxy-Hb in the SFBT group was significantly higher than that in the AC group (P<0.001).
Figure 2
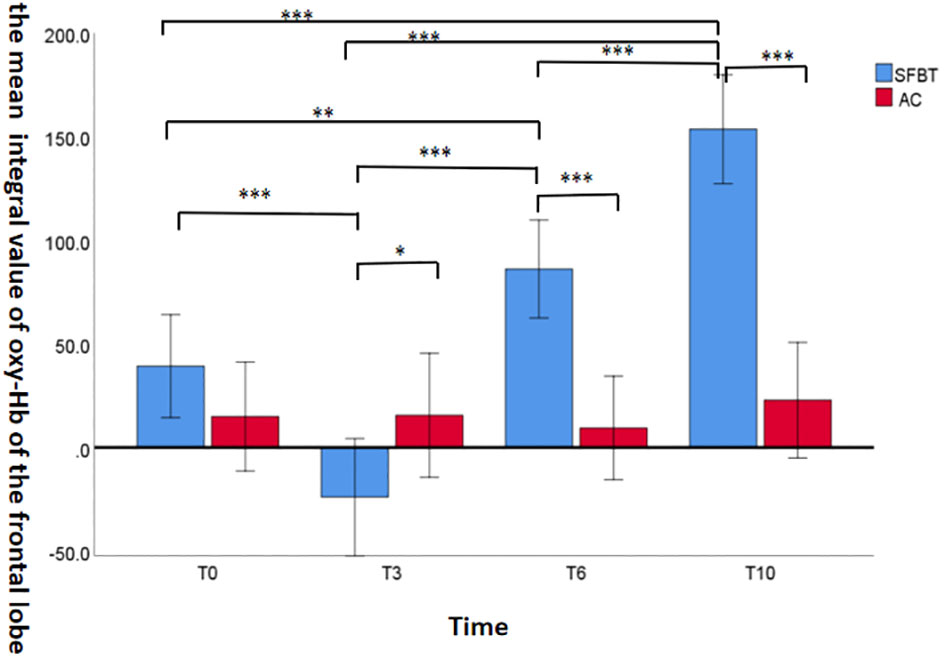
Figure 2 The mean integral value of oxy-Hb of the frontal lobe area during the performance of the task of VFT across the groups. (*P<0.1, **P<0.05, ***P<0.001).
The main effect of time point of fNIRS data analysis
The results showed that the main effect of Time point was significant in channel 17 [F (3,49) = 3.687, P = 0.013, η2 = 0.067]. Additional post hoc analyses found that the mean active Oxy-Hb values at T10 was significantly higher than that at T3 (P=0.004), and was marginal significantly higher than those at T0 and T6 (P=0.056, P=0.062). As shown in Table 4.
Table 4
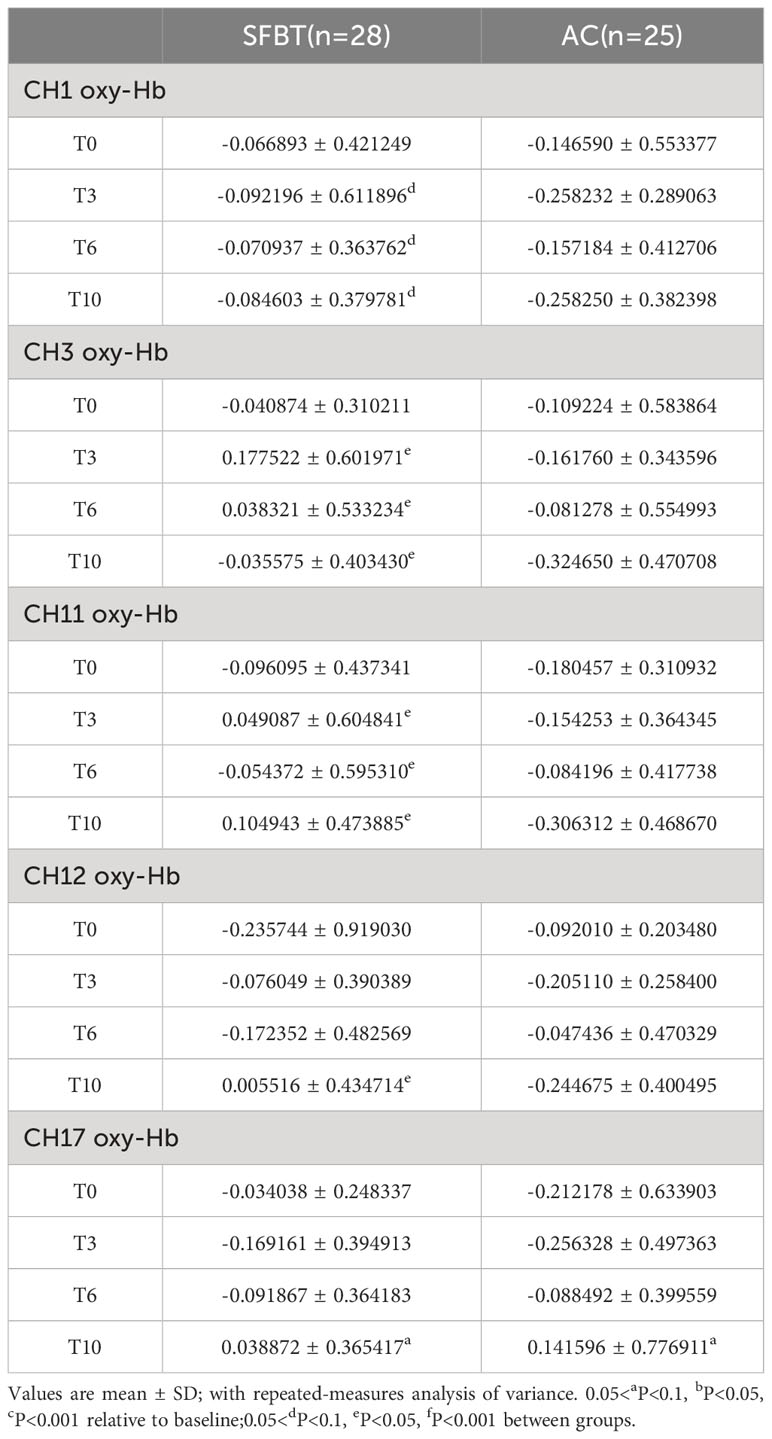
Table 4 The mean oxy-Hb changes in the five channels across the groups.(mean ± SD).
The main effect of group
The results showed that the main effect of Group was significant in channel 3 [F (1,51) = 8.116, P = 0.006, η2 = 0.137], channel 11 [F (1,51) = 6.849, P = 0.012, η2 = 0.118], indicating that the mean active oxy-Hb values in the SFBT group were higher than those in the AC group. Channel 1 showed a marginal significant change [F (1,51) = 3.705, P = 0.060, η2 = 0.068].
The interaction between group and time point
The interaction between Group and Time point showed that Channel 12 showed a marginal significant change [F (3,49) = 2.459, P = 0.074, η2 = 0.131]. The mean active oxy-Hb values in participants are shown in Figure 3.
Figure 3
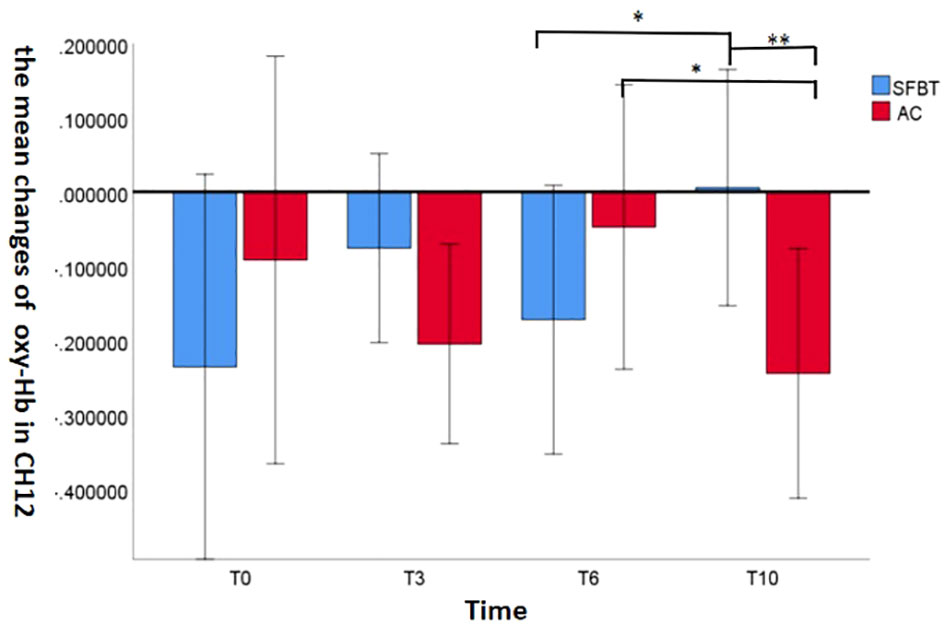
Figure 3 The mean Oxy-Hb changes in the channel 12 across the groups. (*P<0.1, **P<0.05, ***P<0.001).
Simple effect analyses revealed that the mean active oxy-Hb value in channel 12 in SFBT group was significantly increased at the T10 assessment compared with the T6 (P = 0.082). While the mean active oxy-Hb value in channel 12 in the AC group was significant decreased at the T10 assessment compared with the T6 (P = 0.069). According to the simple effect analysis of treatment time, the results demonstrated that the mean active oxy-Hb value in the SFBT group was significantly higher than that in the AC group at the T10 (P = 0.035), but no significant change was found at the T0, T3, T6 between the groups (P>0.1).
Discussion
Our finding showed that SFBT produced a faster symptom reduction than psychodynamic therapy during the entire 10 times of treatment and has not been reported previously. The score of PHQ-9 in the SFBT group significantly decreased at T3 compared to the baseline and showed a stable decline pattern at T6 and T10. Meanwhile the score of PHQ-9 in the AC group decreased only after the 10th intervention and no significant difference was found at T3 and T6. The results confirmed the clinical expectation of greater beneficial effects from short-term SFBT treatment. A quasi-experimental study undertaken to explore the effectiveness of psychoanalysis, long-term and short-term psychotherapy during a 5-year follow-up supported that short-term therapies as SFBT were more effective than psychoanalysis during the first year, whereas the long-term therapy was more effective after 3 years of follow-up (23). In addition, a pilot study revealed that the solution-focused questions in SFBT were overall more effective, providing the same benefits as the problem-focused condition while also increasing positive affect and participants’ understanding of the nature of the problem, suggesting that coaches aim for solution-focused theme in work to build self-efficacy (24).
To the best of our knowledge, this study is the first to use fNIRS to investigate the efficacy and executive function of SFBT on oxy-Hb changes in adolescent depression. Our results showed that the mean active oxy-Hb values of channels 3, 11 and 12 (mainly consisted of dorsolateral prefrontal cortical regions) gradually and significantly increased in the SFBT group compared to the AC group after 10th therapy sessions. These results indicated that SFBT is more effective in improving brain function in adolescent depression than psychodynamic therapy within a brief period. The most relevant cortex is the dorsolateral prefrontal cortex (DLPFC). Recent neuroimaging studies on adolescent depression offered evidence of specific functional abnormalities in the DLPFC. Xie et al. demonstrated that the neuropsychopathological factor mainly encompassed prefrontal cortical circuits, such as the superior medial frontal, salience and frontoparietal networks, and delayed development of the prefrontal cortex that further led to poor executive function (25). Some researchers found that adolescent depression had hypofunction in the DLPFC and the frontotemporal cortex during the VFT, which made it difficult for the patients to make plans and decisions and to susceptible to affective disorders (26–29). Consistent to previous findings, researchers found that emotion regulation and cognitive control were improved by activating the left DLPFC in MDD patients (30). It should be noted that the mean active oxy-Hb values of channels 1, 3, 11, 12 and 17 were not significantly increased than those at the baseline in both two groups in our study. Possible explanations for these findings may include the absence of long-term follow-up, which may indicate a need for additional therapy sessions, considering that most depressive episodes last for at least a few months. Besides, the SFBT mean integral value of oxy-Hb in T3 was negative in the study. Possible explanations may be motion artifacts and physiological factors such as blood pressure, heart rate, and respiratory rate can affect the oxy-Hb levels and lead to a negative integral value (31).
This study found that the number of words in the VFT task of the SFBT group was gradually significantly increased after the third intervention. However, the AC group exhibited a gradual decline in VFT task performance, which was opposite to the trend observed in the SFBT group. Thus, these findings suggested that a performance improvement in cognitive capacity accompanied with SFBT therapy. The neural signatures of anxiety and depressive symptoms within the prefrontal cortex (PFC) were found to be similar when using fNIRS, had less cortex activation during the tasks compared to healthy controls (HCs) particularly in the medial subregions, indicating a potential shared neural basis for these symptoms during late adolescence (32, 33). Zhang et al. found that MDD patients had considerably decreased PFC activation and were associated with reduced rise in oxy-Hb in prefrontal regions when undertaking cognitive tasks relative to controls (34). Tseng et al. showed that there was a negative correlation between state anxiety and the right lateralization index in the ventrolateral prefrontal cortex (VLPFC) in fNRIS during the period of n-back working memory task (35). However, the results about the clinical correlations between cognition and depression symptom severity were still remains controversial as several studies suggested that a correlation existed, while others did not (36, 37). The difference between these results may be related to the inconsistency in the patient characteristics between studies or the letters used and different time settings in the VFT (38).
Limitations
There were several limitations to the current study. First, our study used non-randomized design but we tried to clearly report the study design, methods, and any limitations in details based on Transparent Reporting of Evaluations with Non-randomized Designs (TREND) statement. Employing a single-blind design, participants were kept unaware of the specific details of the psychological treatment they received, yet informed about the study’s general purpose and potential implications. All participants adhered to standardized procedures, conducted in a dedicated location separate from treatment sessions, to control for procedural variances.
Second, the relatively small percentage of patients included in the follow-up examination may have caused a bias. In fact, a comparison between the 53 patients analyzed in this study and the remaining 76 patients that were not included showed a significant difference in the sex ratio. Future research should aim to address this limitation by recruiting a more balanced sample or exploring the role of gender by regressing sex ratio or gender-sensitive statistical analyses, which would provide a more comprehensive understanding of the effects being studied across different genders.
Third, the study did not control the medications taken by participants, and thus, the potential influence of drugs on the findings cannot be ruled out. No clear evidence demonstrated effects of these drugs on the NIRS signals. In some brain regions, however, diazepam equivalent doses were related to NIRS signals in a cross-sectional analysis. In the future, it is therefore necessary to elucidate the influence of medication on NIRS signals in more detail. Furthermore, we should take into account pre-disease IQ, cognitive reserve, and the prevalence of cognitive impairment. In future research, we will further improve these shortcomings.
Conclusions
Altogether, our results support that SFBT can improve depressive and anxiety symptoms as well as executive function of adolescent depression. Further studies will expand the sample size and have a longer follow-up to explore the mechanism of brain regulation.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study was approved by the Institutional Review Board (IRB) of the Affiliated Hospital of Hangzhou Normal University (Hangzhou, China; 2022 (E2)-HS-076). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
HC, MZ and ZY conceptualized the study and funding proposal, as well as drafted the manuscript. HL, LH and AM revised the manuscript and provided expert consultation on the design of the study. HC and MZ analyzed the data. All authors contributed to the article and approved the submitted version.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was supported by the Project for Hangzhou Medical Disciplines of Excellence & Key Project for Hangzhou Medical Disciplines (202004A11).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Nikolakaros G, Vahlberg T, Sillanmäki L, Sourander A. Recurrent depression in childhood and adolescence and low childhood socioeconomic status predict low cardiorespiratory fitness in early adulthood. J Affect Disord. (2020) 266:782–92. doi: 10.1016/j.jad.2019.11.029
2. Zhou X, Teng T, Zhang Y, Del Giovane C, Furukawa TA, Weisz JR, et al. Comparative efficacy and acceptability of antidepressants, psychotherapies, and their combination for acute treatment of children and adolescents with depressive disorder: a systematic review and network meta-analysis. Lancet Psychiatry. (2020) 7(1):581–601. doi: 10.1016/S2215-0366(20)30137-1
3. Friedrich MJ. Depression is the leading cause of disability around the world. JAMA. (2017) 317:1517. doi: 10.1001/jama.2017.3826
4. Li F, Cui Y, Li Y, Guo L, Ke X, Liu J, et al. Prevalence of mental disorders in school children and adolescents in China: diagnostic data from detailed clinical assessments of 17,524 individuals. J Child Psychol Psychiatry. (2022) 63(1):34–46. doi: 10.1111/jcpp.13445
5. Cui X, Bray S, Bryant DM, Glover GH, Reiss AL. A quantitative comparison of NIRS and fMRI across multiple cognitive tasks. Neuroimage. (2011) 54:2808–21. doi: 10.1016/j.neuroimage.2010.10.069
6. Yan M, Chen L, Yang M, Zhang L, Niu M, Wu F, et al. Evidence mapping of clinical practice guidelines recommendations and quality for depression in children and adolescents. Eur Child Adolesc Psychiatry. (2023) 32(11):2091–108. doi: 10.1007/s00787-022-01958-z
7. Kramer J, Conijn B, Oijevaar P, Riper H. Effectiveness of a web-based solution-focused brief chat treatment for depressed adolescents and young adults: randomized controlled trial. J Med Internet Res. (2014) 16:e141. doi: 10.2196/jmir.3261
8. Gingerich WJ, Peterson LT. Effectiveness of solution-focused brief therapy: A systematic qualitative review of controlled outcome studies. Res Soc Work Pract. (2013) 23:266–83. doi: 10.1177/1049731512470859
9. Gingerich WJ, Eisengart S. Solution-focused brief therapy: a review of the outcome research. Fam Process. (2000) 39:477–98. doi: 10.1111/j.1545-5300.2000.39408.x
10. Kim JS. Examining the effectiveness of solution-focused brief therapy: A meta-analysis. Res Soc Work Pract. (2008) 18:107–16. doi: 10.1177/1049731507307807
11. Ozga JE, Povroznik JM, Engler-Chiurazzi EB, Vonder Haar C. Executive (dys)function after traumatic brain injury: special considerations for behavioral pharmacology. Behav Pharmacol. (2018) 29:617–37. doi: 10.1097/FBP.0000000000000430
12. Johnson SL, Elliott MV, Carver CS. Impulsive responses to positive and negative emotions: parallel neurocognitive correlates and their implications. Biol Psychiatry. (2020) 87:338–49. doi: 10.1016/j.biopsych.2019.08.018
13. Takizawa R, Fukuda M, Kawasaki S, Kasai K, Mimura M, Pu S, et al. Neuroimaging-aided differential diagnosis of the depressive state [published correction appears in Neuroimage. 2015 Apr 1;109:530]. Neuroimage. (2014) 85 Pt 1:498–507. doi: 10.1016/j.neuroimage.2013.05.126
14. Lambert MJ, Okiishi JC, Finch AE, Johnson LD. Outcome assessment: From conceptualization to implementation. Prof Psychology: Res Pract. (1998) 29:63–70. doi: 10.1037/0735-7028.29.1.63
15. De Shazer S, Berg IK, Lipchik E, Nunnally E, Molnar A, Gingerich W, et al. Brief therapy: focused solution development. Fam Process. (1986) 25(2):207–21. doi: 10.1111/j.1545-5300.1986.00207.x
16. Sifneos PE. Short-term dynamic psychotherapy for patients with physical symptomatology. Psychother Psychosom. (1984) 42:48–51. doi: 10.1159/000287823
17. Levis B, Benedetti A, Thombs BD. DEPRESsion Screening Data (DEPRESSD) Collaboration. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: individual participant data meta-analysis [published correction appears in BMJ. 2019 Apr 12;365:l1781]. BMJ. (2019) 365:l1476. doi: 10.1136/bmj.l1476
18. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
19. Fusar-Poli P, Howes OD, Allen P, Broome M, Valli I, Asselin MC, et al. Abnormal prefrontal activation directly related to pre-synaptic striatal dopamine dysfunction in people at clinical high risk for psychosis. Mol Psychiatry. (2011) 16(1):67–75. doi: 10.1038/mp.2009.108
20. He X, Bassett DS, Chaitanya G, Sperling MR, Kozlowski L, Tracy JI. Disrupted dynamic network reconfiguration of the language system in temporal lobe epilepsy. Brain. (2018) 141:1375–89. doi: 10.1093/brain/awy042
21. Quan W, Wu T, Li Z, Wang Y, Dong W, Lv B. Reduced prefrontal activation during a verbal fluency task in Chinese-speaking patients with schizophrenia as measured by near-infrared spectroscopy. Prog Neuropsychopharmacol Biol Psychiatry. (2015) 58:51–8. doi: 10.1016/j.pnpbp.2014.12.005
22. Strangman G, Culver JP, Thompson JH, Boas DA. A quantitative comparison of simultaneous BOLD fMRI and NIRS recordings during functional brain activation. Neuroimage. (2002) 17:719–31. doi: 10.1006/nimg.2002.1227
23. Knekt P, Lindfors O, Laaksonen MA, Renlund C, Haaramo P, Härkänen T, et al. Quasi-experimental study on the effectiveness of psychoanalysis, long-term and short-term psychotherapy on psychiatric symptoms, work ability and functional capacity during a 5-year follow-up. J Affect Disord. (2011) 132(1-2):37–47. doi: 10.1016/j.jad.2011.01.014
24. Solms L, Koen J, van Vianen AEM, Theeboom T, Beersma B, de Pagter APJ, et al. Simply effective? The differential effects of solution-focused and problem-focused coaching questions in a self-coaching writing exercise. Front Psychol. (2022) 13:895439. doi: 10.3389/fpsyg.2022.895439
25. Xie C, Xiang S, Shen C, Peng X, Kang J, Li Y, et al. A shared neural basis underlying psychiatric comorbidity [published correction appears in Nat Med. 2023 Sep;29(9):2375]. Nat Med. (2023) 29(5):1232–42. doi: 10.1038/s41591-023-02317-4
26. Akashi H, Tsujii N, Mikawa W, Adachi T, Kirime E, Shirakawa O. Prefrontal cortex activation is associated with a discrepancy between self- and observer-rated depression severities of major depressive disorder: a multichannel near-infrared spectroscopy study. J Affect Disord. (2015) 174:165–72. doi: 10.1016/j.jad.2014.11.020
27. Hirano J, Takamiya A, Yamagata B, Hotta S, Miyasaka Y, Pu S, et al. Frontal and temporal cortical functional recovery after electroconvulsive therapy for depression: A longitudinal functional near-infrared spectroscopy study. J Psychiatr Res. (2017) 91:26–35. doi: 10.1016/j.jpsychires.2017.02.018
28. Liu X, Cheng F, Hu S, Wang B, Hu C, Zhu Z, et al. Cortical activation and functional connectivity during the verbal fluency task for adolescent-onset depression: A multi-channel NIRS study. J Psychiatr Res. (2022) 147:254–61. doi: 10.1016/j.jpsychires.2022.01.040
29. Huang J, Zhang J, Zhang T, Wang P, Zheng Z. Increased prefrontal activation during verbal fluency task after repetitive transcranial magnetic stimulation treatment in depression: A functional near-infrared spectroscopy study. Front Psychiatry. (2022) 13:876136. doi: 10.3389/fpsyt.2022.876136
30. Brunoni AR, Vanderhasselt MA. Working memory improvement with non-invasive brain stimulation of the dorsolateral prefrontal cortex: a systematic review and meta-analysis. Brain Cogn. (2014) 86:1–9. doi: 10.1016/j.bandc.2014.01.008
31. Huppert TJ, Diamond SG, Franceschini MA, Boas DA. HomER: a review of time-series analysis methods for near-infrared spectroscopy of the brain. Appl Opt. (2009) 48:D280–98. doi: 10.1364/ao.48.00d280
32. Papasideris M, Ayaz H, Hall PA. Medial prefrontal brain activity correlates with emerging symptoms of anxiety and depression in late adolescence: A fNIRS study. Dev Psychobiol. (2021) 63:e22199. doi: 10.1002/dev.22199
33. Lang X, Wen D, Li Q, Yin Q, Wang M, Xu Y. fNIRS evaluation of frontal and temporal cortex activation by verbal fluency task and high-level cognition task for detecting anxiety and depression. Front Psychiatry. (2021) 12:690121. doi: 10.3389/fpsyt.2021.690121
34. Zhang H, Dong W, Dang W, Quan W, Tian J, Chen R, et al. Near-infrared spectroscopy for examination of prefrontal activation during cognitive tasks in patients with major depressive disorder: a meta-analysis of observational studies. Psychiatry Clin Neurosci. (2015) 69(1):22–33. doi: 10.1111/pcn.12209
35. Tseng YL, Lu CF, Wu SM, Shimada S, Huang T, Lu GY. A functional near-infrared spectroscopy study of state anxiety and auditory working memory load. Front Hum Neurosci. (2018) 12:313. doi: 10.3389/fnhum.2018.00313
36. Fu L, Xiang D, Xiao J, Yao L, Wang Y, Xiao L, et al. Reduced prefrontal activation during the tower of london and verbal fluency task in patients with bipolar depression: A multi-channel NIRS study. Front Psychiatry. (2018) 9:214. doi: 10.3389/fpsyt.2018.00214
37. Satomura Y, Sakakibara E, Takizawa R, Koike S, Nishimura Y, Sakurada H, et al. Severity-dependent and -independent brain regions of major depressive disorder: A long-term longitudinal near-infrared spectroscopy study. J Affect Disord. (2019) 243:249–54. doi: 10.1016/j.jad.2018.09.029
38. Noda T, Yoshida S, Matsuda T, Okamoto N, Sakamoto K, Koseki S, et al. Frontal and right temporal activations correlate negatively with depression severity during verbal fluency task: a multi-channel near-infrared spectroscopy study. J Psychiatr Res. (2012) 46(7):905–12. doi: 10.1016/j.jpsychires.2012.04.001
Keywords: Solution-Focused Brief therapy, psychodynamic psychotherapy, adolescent, Major depressive disorder, Functional near-infrared spectroscopy
Citation: Chen H, Zhou M, Han L, Manoharasetty A, Yu Z and Luo H (2024) Efficacy and executive function of solution-focused brief therapy on adolescent depression. Front. Psychiatry 15:1246986. doi: 10.3389/fpsyt.2024.1246986
Received: 26 June 2023; Accepted: 21 February 2024;
Published: 08 March 2024.
Edited by:
Ting Li, Chinese Academy of Medical Sciences and Peking Union Medical College, ChinaReviewed by:
Chenyang Gao, Peking Union Medical College Hospital (CAMS), ChinaWu Jeong Hwang, Seoul National University, Republic of Korea
Copyright © 2024 Chen, Zhou, Han, Manoharasetty, Yu and Luo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hong Luo, luohong@vip.126.com; Zhenghe Yu, yuzhcoo@sina.com
†These authors share first authorship