 Martina Preisig1*
Martina Preisig1* Isabelle Häberling1
Isabelle Häberling1 Lukasz Smigielski1
Lukasz Smigielski1 Sophie Emery1Noemi Baumgartner2
Sophie Emery1Noemi Baumgartner2 Mona Albermann1Michael Strumberger3
Mona Albermann1Michael Strumberger3 Klaus Schmeck4Lars Wöckel5Suzanne Erb6Bruno Rhiner7Brigitte Contin-Waldvogel8
Klaus Schmeck4Lars Wöckel5Suzanne Erb6Bruno Rhiner7Brigitte Contin-Waldvogel8 Susanne Walitza1,9,10 for the Omega-3 study Team and
Susanne Walitza1,9,10 for the Omega-3 study Team and  Gregor Berger1
Gregor Berger1
- 1Clinic for Child and Adolescent Psychiatry and Psychotherapy, Psychiatric University Hospital Zurich, Zurich, Switzerland
- 2Outpatient Psychology Wil, Psychiatric Hospital St. Gallen Nord, Wil, Switzerland
- 3Outpatient Clinic, Psychiatric Services Lucerne, Lucerne, Switzerland
- 4Department of Clinical Research, University of Basel, Basel, Switzerland
- 5Center for Child and Adolescent Psychiatry and Psychotherapy, Clienia Littenheid AG, Littenheid, Switzerland
- 6Special Offers and Projects, Child and Adolescent Services St. Gallen, St. Gallen, Switzerland
- 7Child and Adolescent Psychiatry, Psychiatric Services Thurgau, Weinfelden, Switzerland
- 8Child and Adolescent Psychiatry, Psychiatric Services Baselland, Liestal, Switzerland
- 9Neuroscience Center Zurich, University of Zurich and ETH Zurich, Zurich, Switzerland
- 10Zurich Center for Integrative Human Physiology, University of Zurich, Zurich, Switzerland
Introduction: Adolescent suicidality is a significant public health issue. To develop effective interventions aimed at preventing suicide in this vulnerable population, it is essential to understand the complex interplay of health-related quality of life, depression and suicidal ideation.
Methods: For this purpose, we analyzed longitudinal data of 250 children and adolescents diagnosed with major depressive disorder (M = 15.7, SD = 1.6, range 8–18 years, 74% females). The main goal of the study was to examine whether the effect of health-related quality of life on individual trajectories of suicidal ideation is mediated by depression severity. A series of t-tests, Chi-squared-tests, Fisher’s exact tests and a mediation analysis including three robust linear mixed-effects models were conducted.
Results: Depressed adolescents with suicidal ideation reported lower health-related quality of life across physical, psychological, peer, and school domains compared to those without suicidal ideation, while no significant difference was observed in the family-related domain. Psychological well-being emerged as the sole domain of health-related quality of life with a direct influence on suicidal ideation. Notably, depression severity mediated the effect of physical, psychological, peer- and school-related quality of life on suicidal ideation.
Discussion: Our findings suggest that improving health-related quality of life reduces depressive symptoms, which in turn leads to lower suicidal ideation. This highlights the importance of including health-related quality of life in the clinical assessment of suicide risk as well as targeting health-related quality of life in therapeutic interventions. In the light of the results of this study, interventions should not only focus on classical clinical criteria of psychiatric diagnoses such as major depressive disorder, but also on broader, more resource-oriented constructs such as health-related quality of life to better mitigate the risk of suicide in this vulnerable population.
Clinical Trial Registration: www.ClinicalTrials.gov, identifier [NCT03167307].
1 Introduction
Suicidality poses a highly relevant public health concern, particularly in adolescents. In this population, suicide ranks as the fourth leading cause of death globally (1–3). Previous research has shown that health-related quality of life (HRQoL) is inversely associated with psychiatric symptoms including those typically observed in depression, such as suicidality (4–8). However, the intricate relationship between HRQoL, depression, and suicidal ideation in children and adolescents, particularly the mediating effects of depression on the impact of HRQoL on suicidal ideation, remains poorly understood.
HRQoL encompasses the physical, emotional, social, and psychological aspects of an individual's subjective well-being and functioning (9). It is often assessed across multiple dimensions such as physical well-being, psychological well-being, autonomy and parent relation, peers and social support, and school environment, reflecting the multidimensional nature of health (9). There are several advantages of HRQoL over traditional measures of mental health. HRQoL adds additional information to measures by also assessing differences in individuals with low symptomatology (10). As a continuous measure, HRQoL tends to provide greater differentiation between different levels of mental health than traditional categorical diagnostic criteria with strict cut-off values (11). Through its subjective, self-reported assessment and independency of specific diagnoses, HRQoL is comparable across different types of patients and is transdiagnostic in nature (11). While HRQoL and psychiatric symptoms are associated, they are not always linearly correlated (8, 10, 12). Treatment of depression generally improves HRQoL, however HRQoL tends to change more slowly than psychiatric symptoms and only up to half of the change in HRQoL can be explained by improvement in depression symptoms (8, 12). For the above-mentioned reasons, assessing and targeting HRQoL should be an important part of treating depression and HRQoL should be considered as an alternative primary outcome when testing for treatment efficacy in clinical trials (12).
In both general and adolescent populations, depressive symptoms and HRQoL are inversely related (10, 13–15). The relationship between suicidality and HRQoL has been increasingly studied in adult populations in the last decade (11, 16, 17). Researchers generally agree that lower HRQoL is associated with increased suicidal thoughts and behaviors as well as self-harm. A recent systematic review by Le et al. (16) shows that adolescents with non-suicidal self-harming behavior as well as those who attempted suicide have lower HRQoL than those without a history of these behaviors. However, no study to date has assessed the relationship between suicidal ideation and HRQoL in a sample of depressed adolescents (16). The mentioned systematic review also highlights the lack of longitudinal studies on HRQoL in depressed adolescents, especially those with major depressive disorder (MDD).
The mediating role of depression in the relationship between HRQoL and suicidal ideation remains even less explored. Understanding this effect is crucial for developing interventions aimed at improving HRQoL and reducing depressive symptoms, thereby mitigating the risk of suicide in the vulnerable population of children and adolescents. Numerous studies have highlighted the mediating role of depression in the relationship between various psychological factors and suicidal ideation (18–28). In adult populations and cross-sectional designs, depression has been found to mediate the relationship between emotional stability (28), impulsivity (18), psychological strain (27), gratitude (24) and suicidal ideation. In a population of 250 adult cancer patients in Nigeria, HRQoL was found to be indirectly associated with suicidal ideation through psychological distress, whereas no direct effect of HRQoL on suicidal ideation was found (19). In adolescent populations, depression has been identified as a mediator between parent-adolescent conflict (25) as well as school bullying (21) and suicidal ideation in cross-sectional studies. In pregnant female adolescents in Colombia, depression was found to mediate the effect of HRQOL measured by the Kidscreen-52 (9) on suicidal ideation (26). These studies suggest a mediating effect of depression between various psychological factors and suicidality, as well as between HRQoL itself and suicidality. To our knowledge, no study to date has assessed the relationship between HRQoL, depression and suicidal ideation with a focus on the mediating role of depression in a longitudinal, clinical sample of children and adolescents in the cultural context of European countries.
In the present study, we used a longitudinal dataset of 250 children and adolescents diagnosed with MDD from the longitudinal Omega-3 depression study (29) to test whether the effect of HRQoL on individual trajectories of suicidal ideation is mediated by depression severity. By examining data at three time points, we aimed to better understand the temporal dynamics and interactions between these three variables. Based on existing literature and the conceptual framework outlined above, our first hypothesis was that HRQoL is lower in depressed adolescents with suicidal ideation than in depressed adolescents without suicidal ideation. Our second hypothesis was that depression severity mediates the effect of HRQoL on suicidal ideation for each of the five domains of the KidScreen-27 (9). In line with the study by Soto-Chavarría et al. (26) and further studies outlined above, this hypothesis implies that lower HRQoL leads to higher levels of depression, which in turn increases the likelihood of suicidal ideation. By testing these hypotheses, we aimed to elucidate the pathways through which HRQoL influences suicidal thoughts, providing valuable insights for the development of effective mental health intervention and suicide prevention for children and adolescents.
2 Methods
The data used for this study stems from a phase III, 36-week multi-center double-blind placebo-controlled clinical trial investigating the effect of Omega-3 fatty acids on pediatric depression (29). The trial took place from 28th April 2017 to 24th March 2022. The clinical trial included an initial screening and a lead-in phase of seven to ten days, followed by assessments at five time points: baseline, and follow-ups at 6, 12, 24, and 36 weeks. It is important to note that not all measures were collected at each time point, therefore for the current study, longitudinal data could only be utilized from three time points: baseline, and around the 12- and 36-week follow-ups. The primary outcome of the clinical trial was change in depression severity as well as remission and recovery rates (29). The trial has been completed and cross-sectional studies based on its data have been published elsewhere (30–32). As per December 2024, manuscripts related to the primary outcome are undergoing the publication process. The clinical trial was registered at https://www.ClinicalTrials.gov (protocol number NCT03167307). The study was approved by the local ethics committees and was conducted according to the 1964 Declaration of Helsinki and its later amendments. Parents or legal guardians and adolescents aged over 14 years provided written informed consent, younger adolescents and children provided oral assent. The clinical trial was funded by the Swiss National Foundation (grant number 33IC30_166826). No industry funding was received for this study.
2.1 Participants
For the current analysis 250 participants aged 8–18 years were included (M = 15.70, SD = 1.60, range 8–18 years, 74% females; see Table 1 for sociodemographic and clinical information). Seven participants were excluded from the initial dataset as they did not complete measurement of HRQoL at any time point. Participants were recruited from seven in- and outpatient centers in four German-speaking cantons of Switzerland. Inclusion criteria were a) diagnosis of MDD according to the Diagnostic and Statistical Manual of Mental Disorders (95), assessed by the Kiddie-Schedule for Affective Disorders Schizophrenia Present and Lifetime (K-SADS) (33), and b) at least a moderate depression severity, defined by reaching a total score of ≥40 in the Children`s Depression Rating Scale revised (96). Exclusion criteria were lifetime diagnosis of schizophrenia, bipolar affective disorder or substance dependency, current eating disorder, mental retardation, developmental disorders (for example autism), clinically relevant somatic disorders and inability to follow study procedures (for example due to insufficient German language skills). Inclusion and exclusion criteria were assessed at screening. All participants received standard treatment of depression according to the German S3 Guidelines for the treatment of depression in children and adolescents (34).
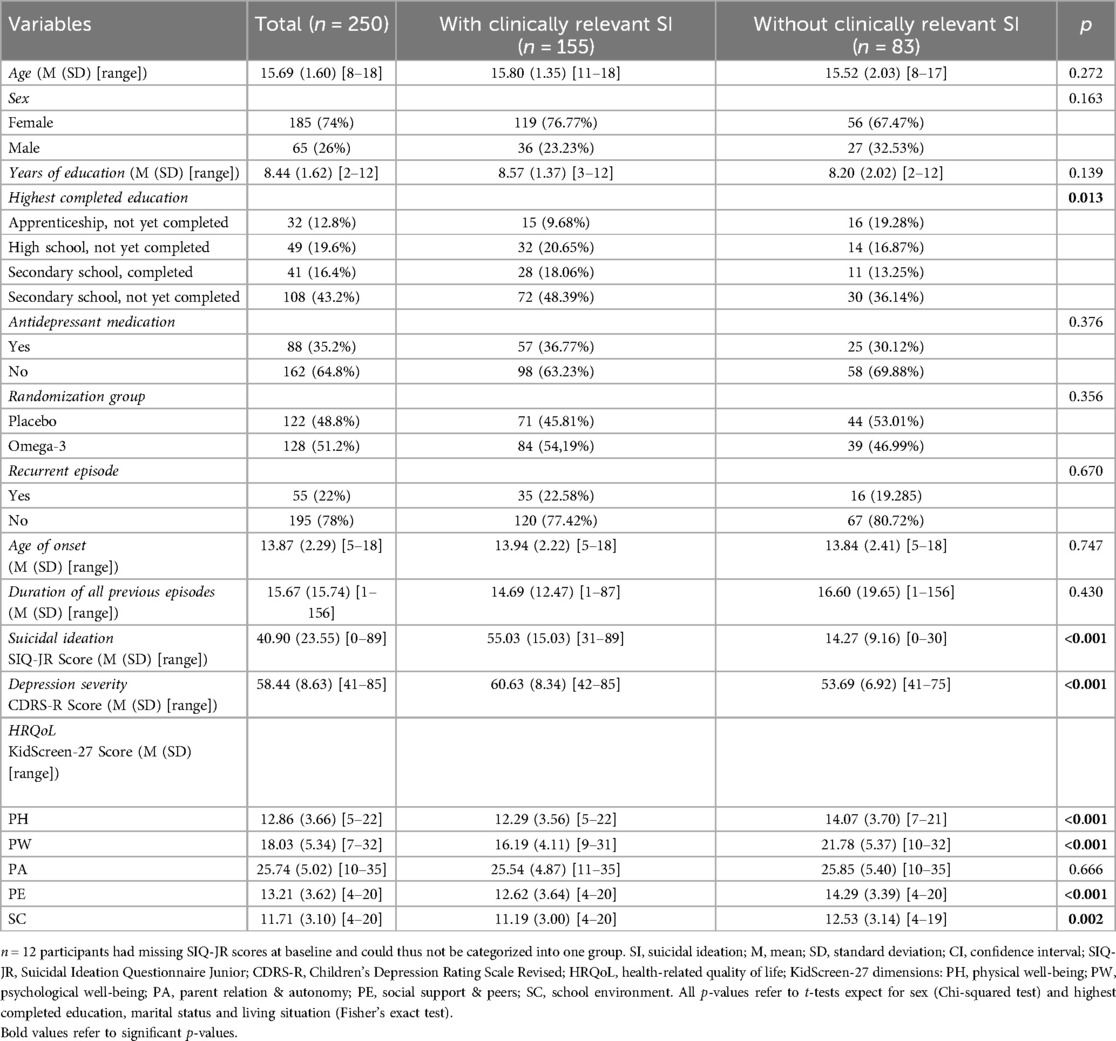
Table 1. Sociodemographic and clinical data for depressed adolescents with (n = 155) and without (n = 83) clinically relevant suicidal ideation (SI) at baseline.
2.2 Measures
Sociodemographic information as well as information on antidepressant medication were collected through patients’ medical records as well as through interviews at screening.
Perceived HRQoL was measured using the KidScreen-27 (9, 35). The KidScreen-27 consists of 27 items resulting in five dimensions of HRQoL: physical well-being (PH), psychological well-being (PW), autonomy and parent relation (PA), social support and peers (PE), and school environment (SC). There is a self-report and a parent-report version, each containing similarly phrased items rated on a 5-point Likert scale, asking to evaluate the frequency of a symptom occurring during the last week (35). For this study, only the self-reports and raw values were used in the analyses. All scales show good psychometric properties in various languages, including German (35).
Suicidal ideation was assessed by the Suicidal Ideation Questionnaire Junior (SIQ-JR) (36, 37), a 15-item self-report questionnaire. The instrument provides questions about the frequency of specific suicidal thoughts during the last month, which are rated on a 7-point Likert scale. Reynolds (37) proposed a cut-off value of ≥31 for clinically relevant suicidal thoughts, demanding further assessment from a healthcare professional. The SIQ-JR shows good psychometric properties, also for the German version (36–38).
Depression severity was assessed by the Children's Depression Rating Scale—Revised (CDRS-R) (39), a semi-structured clinical interview assessing 14 depression symptoms rated on a 5- or 7-point Likert scale by patients and parents in separate interviews. The interviewer provides a final score for each symptom. Three non-verbal symptoms are additionally rated solely by the interviewer. The ratings are added to a final score for depression severity; with scores of 0–39 indicating mild, 40–59 indicating moderate and ≥ 60 indicating severe symptom expression. Psychometric properties are good, also for the German version (40, 41).
2.3 Statistical analyses
All analyses were conducted in R version 4.3.3 (97). Prior to statistical testing, we assessed the number of missing observations and tested whether missing values were missing at random. At time point 2 and 3, 39 (15.18%) and 85 (33.07%) subjects had dropped out of the study, respectively. However, it is important to note, that some subjects skipped only single questionnaires or single items, resulting in an uneven number of missing values. Thus, we also explored the missing values per questionnaire or subscale of interest and per time point (see Supplementary Table A in the Supplementary Material). Missing data was missing completely at random according to Littlès MCAR test (χ2 = 820, df = 850, p = 0.763) (42), thus the missing data was omitted from the analyses.
To test our first hypothesis, that HRQoL is lower in depressed adolescents with suicidal ideation than in depressed adolescents without suicidal ideation, we compared the five domains of HRQoL as well as demographic and clinical information between depressed adolescents with clinically relevant suicidal ideation (≥31 in the SIQ-JR) and those without clinically relevant suicidal ideation (< 31 in the SIQ-JR) using either t-tests for independent samples (for continuous variables) or Chi-squared or Fisher's exact tests (for categorical variables). Fisher's exact tests were used instead of Chi-squared tests when the assumption of minimum expected frequencies of five was not met (43). The cut-off score of ≥31 for clinically relevant suicidal ideation in the SIQ-JR has been used in previous studies (44, 45).
Next, we used a mediation analysis to investigate the second hypothesis, whether the effect of HRQoL dimensions (PH, PW, PA, PE, SC) on suicidal ideation is mediated by depression severity. However, using the DHARMa package (46), we identified slight violations of the normality assumptions in our linear mixed-effects models. To address this, we employed robust linear mixed-effects models implemented in the “robustlmm” package (47), which are specifically designed to provide reliable parameter estimates in the presence of deviations from normality and other potential model misspecifications. These models are less sensitive to outliers and non-normal residuals, making them a robust alternative for our analyses. Subsequently, we customized the “mediation” package (48) to accommodate the use of robust linear mixed-effects models. In the approach applied by the “robustlmm” package (47), Satterthwaite degrees of freedom are employed to compute p-values, which accounts for the robustness of the linear mixed-effects models against potential violations of assumptions such as normality and heteroscedasticity (47, 49). The total effect model (M0) assessed the direct effect of HRQoL dimensions on suicidal ideation disregarding the effect of depression. The mediator model (M) assessed the effect of HRQoL dimensions on depression. The dependent variable model (Y) included the effect of HRQoL dimensions as well as depression on suicidal ideation. All three models included the covariates age, gender and randomization group (Omega-3 or Placebo) as well as a random intercept of subject and a random slope of time (baseline, approximately 12 weeks, and approximately 36 weeks), enabling examination of individual trajectories over time. To account for variations in the timing of follow-up assessments, we used the number of days since baseline as a more precise measure rather than relying on fixed 12- and 36-week intervals. However, given that this variable was on a considerably larger scale, we normalized it by dividing each value by its standard deviation. Models M and Y were used as input for mediation analysis. The indirect effect for each HRQoL dimension was computed as the product of the beta coefficient of the HRQoL dimension from the mediator model (M) and the beta coefficient of the mediator (depression) from the dependent variable model (Y). To compute 95% confidence intervals and p-values for the indirect effects, we performed a bootstrap resampling with 500 iterations. Each bootstrap sample involved randomly sampling participants with replacement, refitting the models, and calculating indirect effects. Prior to the mediation analysis, we confirmed a main effect of HRQoL dimensions in either model M0 or M, which is a premise for consecutive mediation analysis (50, 51). Figure 1 shows the proposed mediation relationship. A p-value of less than 0.05 was considered statistically significant across all analyses.
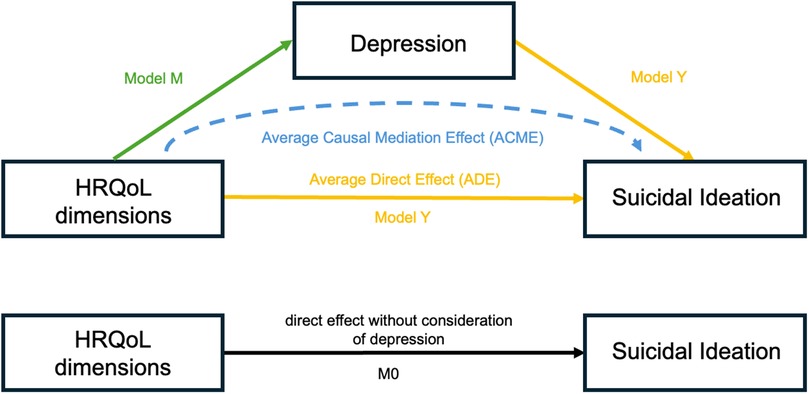
Figure 1. HRQoL, health-related quality of life. Model M0 shows the direct effect of HRQoL dimensions on suicidal ideation without consideration of depression. Model M reflects the effect of HRQoL dimensions on depression. Model Y shows the average direct effect (ADE) of HRQoL dimensions on suicidal ideation with consideration of depression. The indirect effect of HRQoL dimensions on suicidal ideation through the mediation of depression is the average causal mediation effect (ACME).
To explore potential bidirectional associations, we conducted additional exploratory analyses. Specifically, we computed mediation models applying the same statistical approach as described above, but with depression severity as the predictor and HRQoL dimensions as mediators.
3 Results
3.1 Descriptive statistics
Table 1 shows sociodemographic and clinical information for the depressed adolescents with and without clinically relevant suicidal ideation at baseline. Statistically significant group differences were found for suicidal ideation (t = −25.94, p < 0.001), depression severity (t = −6.86, p < 0.001), PH (t = 3.40, p = <0.001), PW (t = 8.11, p = <0.001), PE (t = 3.47, p = <0.001) and SC (t = 3.11, p = 0.002), indicating that adolescents with suicidal ideation have a higher depression severity, more suicidal ideation and lower values in PH, PW, PE and SC than adolescents without suicidal ideation. Further, the Fisher's exact test (p = 0.013) indicated a significant association between group (with vs. without suicidal ideation) and highest completed education.
3.2 Mediating effects of depression on suicidal ideation
To assess whether the effect of HRQoL dimensions on suicidal ideation is mediated by depression, we conducted a mediation analysis. The estimates of the three robust linear mixed effect models M0, M and Y can be found in Tables 2–4, respectively. For the total effect model M0 (Table 2), we found a statistically significant negative effect of PW (β = −1.89, p < 0.001) on suicidal ideation, suggesting that improvement of psychological well-being leads to reduced suicidal ideation. All other dimensions of HRQoL (PH, PA, PE, SC) as well as the covariates age, gender and randomization group did not reach statistical significance. Additionally, the model revealed a statistically significant negative effect of time (β = −3.20, p < 0.001) on suicidal ideation, indicating a decrease of suicidal ideation over time.
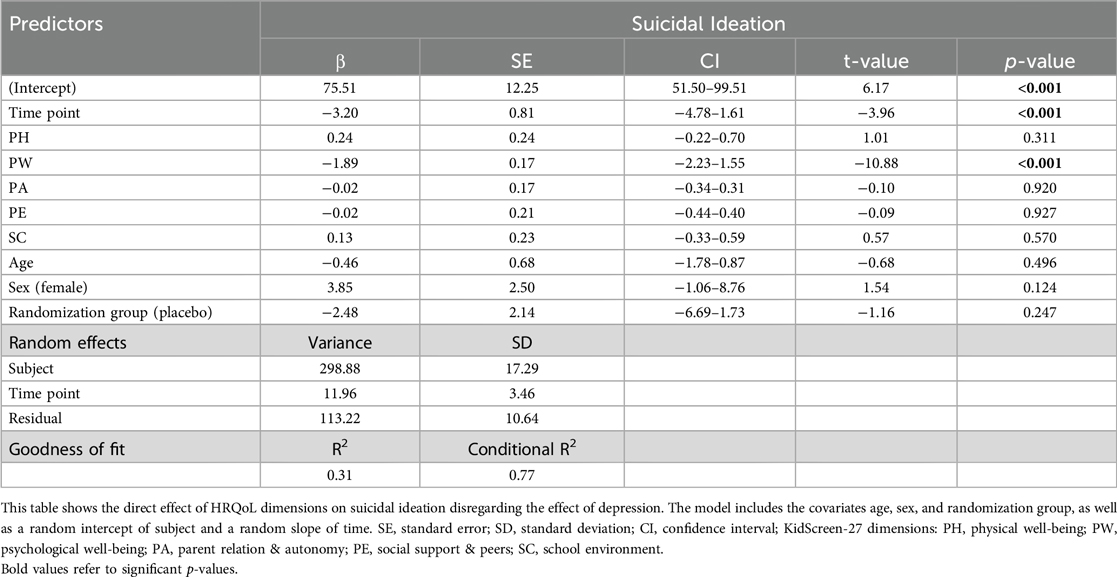
Table 2. Total effect model M0: robust linear mixed effect model showing the effect of HRQoL dimensions on suicidal ideation.
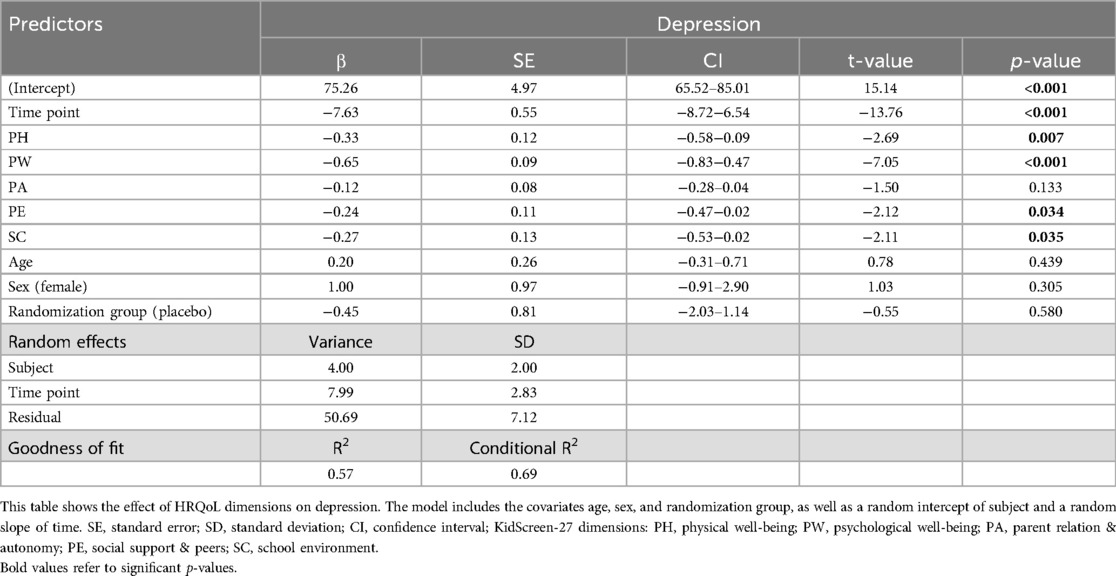
Table 3. Mediator model M: robust linear mixed effect model showing the effect of HRQoL dimensions on depression.
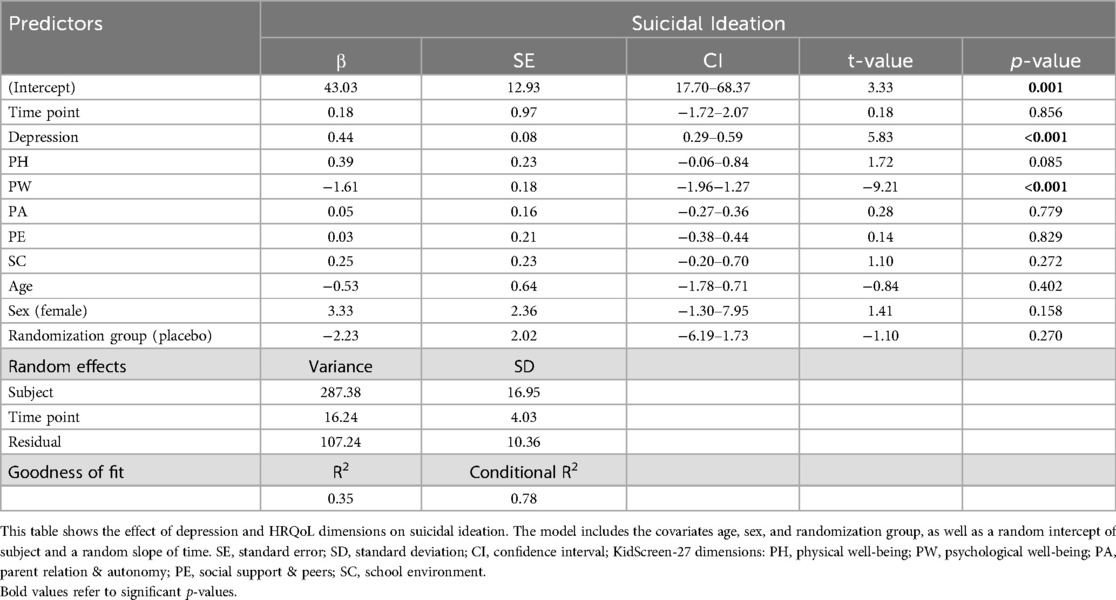
Table 4. Dependent Variable model Y: robust linear mixed effect model showing the effect of HRQoL dimensions and depression on suicidal ideation.
For the mediator model M (Table 3), we found statistically significant negative effects for PH (β = −0.33, p = 0.007), PW (β = −0.65, p < 0.001), PE (β = −0.24, p = 0.034) and SC (β = −0.27, p = 0.035) on depression, indicating that an improvement in these dimensions of HRQoL is associated with lower depression severity. PA as well as the covariates age, gender and randomization group did not yield statistically significant effects. Additionally, the model showed a statistically significant negative effect of time (β = −7.63, p < 0.001) on depression, indicating a decrease of depression over time.
For the dependent variable model Y (Table 4), we found a statistically significant negative effect for PW (β = −1.61, p < 0.001) on suicidal ideation, indicating that increased psychological well-being is associated with lower suicidal ideation when taking depression severity into consideration (average direct effect; ADE). The model also showed a statistically significant positive effect of depression (β = 0.44, p < 0.001) on suicidal ideation, suggesting that increased depression is associated with increased suicidal ideation. The other dimensions of HRQoL (PH, PA, PE, SC) as well as time and the covariates age, gender and randomization group did not reach statistical significance.
For all three models M0, M and Y we observed a substantial variation in the baseline levels of suicidal ideation among subjects, as indicated by the random intercept (SD = 17.29, 2.00 and 16.95 for models M0, M and Y, respectively), and a considerable variability in the rate of change over time of suicidal ideation across subjects, as indicated by the random slope (SD = 3.46, 2.83 and 4.03 for models M0, M and Y, respectively).
Finally, we computed the average causal mediation effect (ACME) of HRQoL dimensions on suicidal ideation. This procedure yielded a statistically significant ACME of PH (β = −0.15, p < 0.001), PW (β = −0.29, p < 0.001), PE (β = −0.11, p = 0.004) and SC (β = −0.12, p = 0.008) on suicidal ideation, suggesting that depression severity mediates the effect of these dimensions of HRQoL on suicidal ideation. The effect of PA did not reach statistical significance. The results of the mediation analysis are summarized in Figure 2.
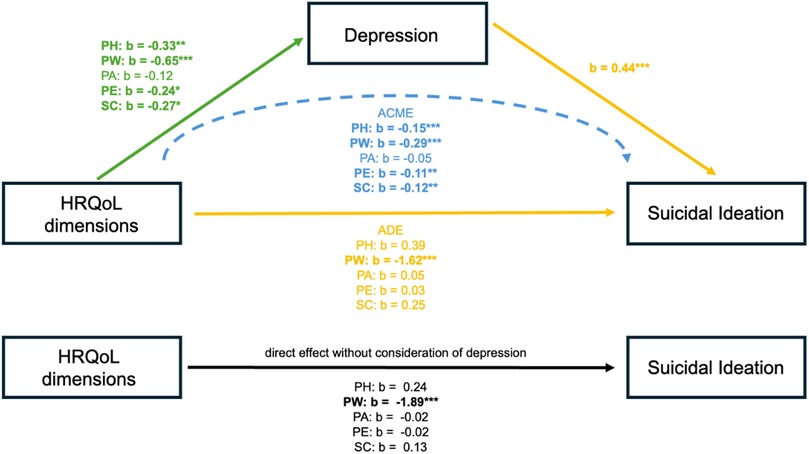
Figure 2. HRQoL, health-related quality of life; KidsScreen-27 dimensions: PH, physical well-being; PW, psychological well-being; PA, parent relation & autonomy; PE, social support & peers; SC, school environment; ADE, average direct effect; ACME, average causal mediation effect; ***p < 0.001; **p < 0.01; *p < 0.05.
The additional exploratory analyses indicate that the HRQoL dimensions PH (ACME: β = 0.08, p < 0.001), PW (ACME: β = 0.42, p < 0.001), PA (ACME: β = 0.03, p = 0.028), PE (ACME: β = 0.05, p < 0.001), and SC (ACME: β = 0.05, p < 0.001) serve as mediators in the relationship between depression severity and suicidal ideation. See Supplementary Figures A–E in the Supplementary Material for the results of these additional exploratory analyses.
4 Discussion
In this study, we investigated the relationship of health-related quality of life (HRQoL), suicidal ideation and depression utilizing longitudinal data of 250 children and adolescents diagnosed with MDD. At baseline, we found that depressed adolescents with suicidal ideation showed significantly higher depression severity and lower HRQoL in four out of five dimensions—physical well-being (PH), psychological well-being (PW), social support and peers (PE), and school environment (SC)—compared to those without suicidal ideation. Our mediation analysis revealed that the relationship between HRQoL dimensions and suicidal ideation was mediated by depression severity. While only the PW dimension showed a statistically significant direct effect on suicidal ideation, the mediation analysis indicated that PH, PW, PE, and SC had significant indirect effects, meaning their impact on suicidal ideation was mediated through depression severity. These findings highlight the importance of addressing both HRQoL and depression in interventions targeting suicidality in adolescents with MDD.
4.1 Differences in depression severity and health-related quality of life at baseline
At baseline, the observed group differences between adolescents with and without suicidal ideation emphasize the substantial impact of suicidal ideation on both depression severity and various dimensions of HRQoL. These findings are consistent with existing literature indicating a robust association between suicidal ideation and increased depression severity in both general and adolescents populations (52, 53). Additionally, we observed significant group differences in HRQoL dimensions (PH, PW, PE and SC), indicating that adolescents with suicidal ideation have lower HRQoL in these domains than those without suicidal ideation. This is in line with previous research demonstrating an inverse relationship between HRQoL and suicidality as well as self-harm in both adult and adolescent populations (11, 16, 54, 55).
4.2 Longitudinal changes in depression severity and suicidal ideation
The analysis of longitudinal data indicated a decline in both depression severity and suicidal ideation over time, consistent with the fact that participants were receiving standard treatment for depression. This aligns with the German S3 Guidelines for the treatment of depression in children and adolescents, indicating that therapeutic interventions, such as cognitive-behavioral therapy, medication, or a combination of both, can lead to significant reductions of depressive symptoms and suicidal ideation over time (34). However, there was a substantial variability in baseline levels of suicidal ideation and depression across participants, as well as in the rates of change over time, which indicates that individual trajectories differ considerably, highlighting the need for personalized approaches to treatment. These findings align with existing longitudinal studies, which have shown that depression and suicidal ideation often improve with appropriate interventions, but that the degree and speed of recovery can vary (56, 57). Overall, the observed decrease in depression and suicidal ideation over time highlight the effectiveness of standard treatments in alleviating these issues, while also emphasizing the importance of monitoring individual progress and adjusting interventions as needed to ensure long-term recovery.
4.3 The mediating role of depression severity in the relationship between health-related quality of life and suicidal ideation
The longitudinal analysis of HRQoL dimensions revealed that only psychological well-being had a direct impact on suicidal ideation. This is in line with previous research, such as the prospective study with 573 young individuals by Russell et al. (58), which demonstrated an association between mental well-being and later self-harming thoughts and behaviors, likely mediated by feelings of defeat and entrapment. Similarly, Morey et al. (59) showed that lower levels of mental well-being were associated with self-harming behavior in a cross-sectional sample of 2’000 adolescents. However, in our analysis, psychological well-being influenced suicidal ideation both directly and indirectly through its effect on depression severity. This finding is unsurprising, as psychological well-being is closely linked to depression, with psychological well-being influencing subsequent depression and vice versa in a population of adolescents (60). Other studies have identified similar mediating effects for depression severity or related constructs. For instance, Chukwuemeka et al. (19) demonstrated that psychological distress mediated the effect of HRQoL on suicidal ideation in adult cancer patients in Nigeria.
In contrast, the other HRQoL dimensions (PH, PA, PE, and SC) did not exhibit a direct effect on suicidal ideation. However, depression severity mediated the impact of PH, PE, and SC on suicidal ideation. This is consistent with a substantial body of literature regarding the association between physical activity, depression and suicidality. Numerous recent systematic reviews and meta-analyses in adult populations indicate a significant association between physical activity and reduced depressive symptoms (61–63). For example, Pearce et al. (62) found that adults meeting the recommended physical activity guidelines (2.5 h of walking per week or equivalent) had a 25% reduced risk of depression. Sibold et al. (64) revealed that students engaging in physical activity four to five days per week were less likely to exhibit suicidal ideation than students engaging in physical activity on only one or no day a week. Further, several studies support our finding that depressed adolescents with suicidal ideation report lower physical well-being compared to those without suicidal ideation. For instance, Gyori et al. (54) observed lower physical HRQoL in adolescents engaging in self-harming behavior, while Li et al. (5) found lower physical HRQoL in students with depression compared to their peers without depression. Those associations can be attributed to several neurophysiological, psychological and social mechanisms, including neuroendocrine and inflammatory responses, as well as improved body image, all of which are directly related to higher physical well-being (62, 63). Other studies, such as those by Algorta et al. (65) and Fairweather-Schmidt et al. (11), reported no significant effects of physical well-being on suicidal ideation, and in some cases, young adults with suicidal ideation exhibited better physical HRQoL than those without. These discrepancies may stem from methodological differences and the lack of consensus on the dimensions of HRQoL and their operationalization.
Our findings further suggest that peer relationships influence suicidal ideation indirectly by affecting depression severity, aligning with literature highlighting the protective role of social support for various psychological outcomes. Social support is an established protective factor against depression (66) and suicidality (67, 68). However, some studies have reported contradictory findings, indicating no significant association (69) or a relationship only for support from family members, rather than peers (70, 71). Wan et al. (72) found depressive symptoms to mediate between perceived social support and suicidal ideation in an adolescent population in China. Additionally, negative peer interactions, such as bullying, can exacerbate depression and increase the risk of suicidal ideation. Gómez-Tabares (21) showed that depression mediated the link between bullying and suicidal behavior. Bullying, which is often assessed in a school environment, has been consistently linked to both depressive symptoms (73, 74) as well as suicidality (75–77), suggesting that the social environment at school plays a critical role in influencing both depression and suicidal ideation. Other aspects of school environment in varying cultural contexts are also associated with suicidal ideation, including school safety and the availability of illegal drugs, as demonstrated in the study by Pfledderer et al. (78) in the USA, and stressful psychosocial school environment, measured by effort-reward imbalance, in a Chinese population experiencing suicidal ideation (79).
Unexpectedly, our analysis did not reveal any significant group differences in the parent relation and autonomy dimension of HRQoL (PA) between depressed adolescents with and without suicidal ideation at baseline, nor did PA significantly contribute to the mediation models. This suggests that there is no effect of PA on suicidal ideation or depression severity and consequently depression severity also does not mediate the effect of PA on suicidal ideation. This result is contrary to our hypotheses and existing literature such as Low (25), who found that depression mediated the effect of parent-adolescent conflict on suicidal ideation. Based on previous literature we would have expected the family and peer domains of HRQoL to be especially relevant in this age group. Several studies show the importance of family factors for suicidality and self-harm, such as quality of interaction with parents (80), perceived family support (98), family dysfunction and absent parents (81). In the systematic review by Le et al. (16) several studies emphasize the importance of family domains of HRQoL in this population. Four studies reported a significant negative association of family related HRQoL with self-harm (54, 55) and suicidal attempt (65, 82). Three studies showed a negative association between family-related HRQoL and suicidal ideation (83–85). Gyori et al. (54) even found the only direct association between HRQoL and self-harm for the family area, which seems to highlight the importance of the family for self-harm.
A possible explanation for our findings might be the developmental shift during adolescence, where peer relationships become more essential than family relationships for social support (86–88). The study by Zullig (55) supports this hypothesis, finding only a weak although significant association between deliberate self-harm and family satisfaction, but the strongest association for satisfaction with friendships in a sample of college students. Another potential explanation could relate to the methodology used to assess the PA dimension in the KidScreen-27 questionnaire (9). The PA dimension includes broad and somewhat vague items that assess not only parent relationships but also autonomy, with questions like ‘Have you had enough time for yourself?’ or ‘Have you been able to do the things you want to do in your free time?’. These items may be influenced by external factors unrelated to the family, such as academic stress. Moreover, the items addressing parent relationships are quite general and do not capture specific family conflicts, which might explain the divergence from findings like those of Low (25). In contrast, other HRQoL dimensions, such as PE, include more precise items about social support. Additionally, the PA dimension appears to be more stable over time, as family relationships tend to be relatively constant during adolescence, making it harder to detect significant changes or effects. This stability aligns with research suggesting that family relationships are less volatile than peer relationships in early adolescence, where friendships are more likely to change frequently (87).
4.4 Strengths and limitations
A key strength of the current study is its longitudinal design combined with a large sample size. Furthermore, we employed robust linear mixed-effects models to analyze the data, which are well-suited for longitudinal analyses when not all assumptions for standard linear mixed-effects models are met. However, this approach did not permit the examination of reciprocal relationships. This is significant, as previous studies have demonstrated that HRQoL mediates the relationship between internalizing psychopathology and suicidal ideation in adolescent clinical samples (89). This is in line with the findings of our additional exploratory analyses, showing that HRQoL dimensions mediate the relationship between depression severity and suicidal ideation. The study of Gyori et al. (54) used network modelling to test the association between HRQoL dimensions and non-suicidal self-harm in 202 adolescents. The authors found that, contrary to their initial hypothesis, mental disorders mediated the effect between HRQoL dimensions and non-suicidal self-harm behavior and not the reverse. More recent studies, such as that by Soto-Chavarría et al. (26), also support this proposed relationship. Their findings indicate that depression mediates the association between HRQoL and suicidal ideation in pregnant female adolescents. Our additional exploratory analyses indicate that both depression and HRQoL dimensions may act as mediators. This suggests that depression might deteriorate HRQoL and thereby indirectly increase suicidal ideation. On the other hand, impaired HRQoL may lead to depressive symptoms, which in turn increase suicidal ideation.
Further bidirectional effects between the examined variables are plausible. For instance, prior research suggests that suicidal ideation may lead to lower HRQoL (11, 90). Similarly, while depression is commonly assessed as precursor to suicidality, reverse effects cannot be ruled out (91). Depression severity may also influence participants’ answers in the KidScreen-27, as the dimension regarding psychological well-being includes items assessing mood, listlessness, and self-esteem, which are typical symptoms of depression (9, 35, 39). Structural equation modeling would be a valuable approach to examine such potential bidirectional associations. However, the current sample size was insufficient for these complex analyses, increasing the risk of poor model fit and convergence problems (92). Therefore, further studies employing even larger samples and a longitudinal design, utilizing advanced statistical methods such as cross-lagged panel models, may be necessary to more thoroughly investigate potential reciprocal relationships between HRQoL, depression and suicidality.
Furthermore, there was a substantial amount of missing data at follow-up, which may affect the reliability and validity of the findings due to attrition bias. Attrition bias arises when participants who drop out differ systematically from the remaining study sample (93). In our study, individuals with more severe symptoms may have been more likely to discontinue participation—potentially due to low motivation, a common feature of severe depression—which could have led to an underestimation of symptom severity at follow-up (94). Therefore, our results regarding the longitudinal decline of depression severity and suicidal ideation should be interpreted with caution.
Additionally, the generalizability of the results is limited, as the study focused on a specific clinical sample of depressed adolescents. Future studies should be conducted in more heterogeneous samples, as HRQoL may be more effective in distinguishing individuals with lower symptomatology (10). Moreover, future research should not only examine suicidal ideation but also suicidal behaviors, exploring the distinct impact of HRQoL on both. Further investigations into the individual effects of different HRQoL dimensions are also warranted.
4.5 Conclusion and practical implications
In conclusion, this study provides insight into the complex relationship of HRQoL, depression and suicidal ideation in a clinical sample of adolescents. Our findings show that while psychological well-being had a direct effect on suicidal ideation, other HRQoL dimensions, such as physical well-being, social support and peers, and school environment, influenced suicidal ideation indirectly through depression severity. Clinically, these findings support the use of HRQoL assessments as a tool for identifying suicide risk and emphasize the need for resource-oriented therapeutic approaches. Rather than focusing solely on diagnostic criteria, interventions should target HRQoL domains to extend support beyond therapy, improving outcomes in real-life settings like schools. By addressing broader aspects of adolescents’ well-being, such interventions can potentially reduce depression and prevent suicide in this vulnerable population more effectively.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Kantonale Ethikkommission Zürich (Lead-Ethic Commission), Ethikkommission Ostschweiz, Ethikkommission Nordwest- und Zentralschweiz, number: 2016-02116. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
MP: Conceptualization, Methodology, Formal analysis, Writing – original draft, Visualization. IH: Conceptualization, Investigation, Methodology, Project administration, Supervision, Writing – review & editing. LS: Methodology, Supervision, Validation, Writing – review & editing. SE: Investigation, Writing – review & editing. NB: Investigation, Writing – review & editing. MA: Investigation, Writing – review & editing. MS: Investigation, Writing – review & editing. KS: Investigation, Writing – review & editing. LW: Investigation, Writing – review & editing. SE: Investigation, Writing – review & editing. BR: Investigation, Writing – review & editing. BC-W: Investigation, Writing – review & editing. SW: Funding acquisition, Investigation, Resources, Writing – review & editing. GB: Investigation, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The study was mainly funded by the Swiss National Science Foundation. Grant number 33IC30_166826.
Conflict of interest
SW has received royalities from Thieme Hogrefe, Kohlhammer, Springer, and Beltz in the last 5 years. SW has received lecture honoraria from Opopharma in the last 5 years. Her work was supported in the last 5 years by the Swiss National Science Foundation (SNF), diff. EU FP7s, HSM Hochspezialisierte Medizin of the Kanton Zurich, Switzerland, Bfarm Germany, ZInEP, Hartmann Müller Stiftung, Olga Mayenfisch, and Gertrud Thalmann Fonds. KS has received royalities from Springer, Hogrefe, and Schattauer in the last five years. Since 2014, KS received no honoraria from pharmaceutical or other industrial companies. His work was supported in the last five years by the Swiss National Science Foundation (SNF), Swiss Ministry of Justice, University of St. Gallen, Botnar Foundation, and Gertrud Thalmann Fonds. GB was supported by the Swiss National Science Foundation, the Stanley Foundation, the Gertrud Thalmann Fonds, and the Ebnet Foundation and has received lecture honoraria from Lundbeck, Opopharma, Antistress AG (Burgerstein) in the last 5 years.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frcha.2025.1567387/full#supplementary-material
References
1. Berger G, Pauli D, Blaser M, Häberling I, Kaess M, Walitza S. Editorial - Jugendsuizidalität stabil hoch. Psychiatrie und Neurologie. (2021) 2:1–3. doi: 10.5167/uzh-203183
2. Groholt B, Ekeberg Ø, Haldorsen T. Adolescent suicide attempters: what predicts future suicidal acts? Suicide Life Threat Behav. (2006) 36(6):638–50. doi: 10.1521/suli.2006.36.6.638
3. WHO. Suicide. Geneva: World Health Organization (2021). Available online at: https://www.who.int/news-room/factsheets/detail/suicide
4. Akosile CO, Mgbeojedo UG, Maruf FA, Okoye EC, Umeonwuka IC, Ogunniyi A. Depression, functional disability and quality of life among Nigerian older adults: prevalences and relationships. Arch Gerontol Geriatr. (2018) 74:39–43. doi: 10.1016/j.archger.2017.08.011
5. Li YX, Lu YH, Wen XS, Chen DD, Tao SJ, Xu XL, et al. Correlation between current situation of self-injury and suicide behaviors and relevant health behaviors among adolescents. Fudan Univ J Med Sci. (2020) 47(3):327–33. doi: 10.3969/j.issn.1672-8467.2020.03.004
6. Papakostas GI, Petersen T, Mahal Y, Mischoulon D, Nierenberg AA, Fava M. Quality of life assessments in major depressive disorder: a review of the literature. Gen Hosp Psychiatry. (2004) 26(1):13–7. doi: 10.1016/j.genhosppsych.2003.07.004
7. Sivertsen H, Bjorklof GH, Engedal K, Selbaek G, Helvik AS. Depression and quality of life in older persons: a review. Dement Geriatr Cogn Disord. (2015) 40(5-6):311–39. doi: 10.1159/000437299
8. Trivedi MH, Rush AJ, Wisniewski SR, Warden D, McKinney W, Downing M, et al. Factors associated with health-related quality of life among outpatients with major depressive disorder: a STAR* D report. J Clin Psychiatry. (2006) 67(2):185–95. doi: 10.4088/jcp.v67n0203
9. Ravens-Sieberer U, Herdman M, Devine J, Otto C, Bullinger M, Rose M, et al. The European KIDSCREEN approach to measure quality of life and well-being in children: development, current application, and future advances. Qual Life Res. (2014) 23(3):791–803. doi: 10.1007/s11136-013-0428-3
10. Huebner ES, Valois RF, Suldo SM, Smith LC, McKnight CG, Seligson JL, et al. Perceived quality of life: a neglected component of adolescent health assessment and intervention. J Adolesc Health. (2004) 34(4):270–8. doi: 10.1016/j.jadohealth.2003.07.007
11. Fairweather-Schmidt A, Batterham P, Butterworth P, Nada-Raja S. The impact of suicidality on health-related quality of life: a latent growth curve analysis of community-based data. J Affect Disord. (2016) 203:14–21. doi: 10.1016/j.jad.2016.05.067
12. IsHak WW, Greenberg JM, Balayan K, Kapitanski N, Jeffrey J, Fathy H, et al. Quality of life: the ultimate outcome measure of interventions in major depressive disorder. Harv Rev Psychiatry. (2011) 19(5):229–39. doi: 10.3109/10673229.2011.614099
13. Freire T, Ferreira G. Health-related quality of life of adolescents: relations with positive and negative psychological dimensions. Int J Adolesc Youth. (2016) 23(1):11–24. doi: 10.1080/02673843.2016.1262268
14. Gomez-Delgado G, Almaraz-Vega E, Ramirez-Mireles JE, Gutierrez-Paredes ME, Padilla-Galindo MDR. Health-Related quality of life and depressive symptomatology in high school students during the lockdown period due to SARS-CoV-2. Int J Environ Res Public Health. (2022) 19:14. doi: 10.3390/ijerph19148780
15. Jenkins PE, Ducker I, Gooding R, James M, Rutter-Eley E. Anxiety and depression in a sample of UK college students: a study of prevalence, comorbidity, and quality of life. J Am Coll Health. (2021) 69(8):813–9. doi: 10.1080/07448481.2019.1709474
16. Le N, Belay YB, Le LK, Pirkis J, Mihalopoulos C. Health-related quality of life in children, adolescents and young adults with self-harm or suicidality: a systematic review. Aust N Z J Psychiatry. (2023) 57(7):952–65. doi: 10.1177/00048674231165477
17. Vilugrón Aravena F, Molina T, Gras Pérez ME, Font-Mayolas S. Conducta suicida, consumo de sustancias psicoactivas y calidad de vida en adolescentes chilenos. Revista Médica de Chile. (2022) 150(8):1036–45. doi: 10.4067/s0034-98872022000801036
18. Chen X, Li S. Serial mediation of the relationship between impulsivity and suicidal ideation by depression and hopelessness in depressed patients. BMC Public Health. (2023) 23:1. doi: 10.1186/s12889-023-16378-0
19. Chukwuemeka NA, Yinka Akintunde T, Uzoigwe FE, Okeke M, Tassang A, Oloji Isangha S. Indirect effects of health-related quality of life on suicidal ideation through psychological distress among cancer patients. J Health Psychol. (2024) 29(10):1061–73. doi: 10.1177/13591053231225306
20. Fu J, Chen X, Dai Z, Huang Y, Xiao W, Wang H, et al. HIV-related stigma, depression and suicidal ideation among HIV-positive MSM in China: a moderated mediation model. BMC Public Health. (2023) 23(1):1–12. doi: 10.1186/s12889-023-17047-y
21. Gómez-Tabares AS. Depression as a mediator between bullying and suicidal behavior in children and adolescents. Behav Psychol. (2021) 29(2):259–81. doi: 10.51668/bp.8321203n
22. Hwang MG, Kim EJ. The effect of subjective quality of life and self-esteem on suicide ideation among the older adults: focused on the mediating effect of depression. Korean Gerontol Soc. (2008) 28(4):865–85. doi: 10.15300/jcw.2024.88.1.31
23. Lee KS, Lennie TA, Wu JR, Biddle MJ, Moser DK. Depressive symptoms, health-related quality of life, and cardiac event-free survival in patients with heart failure: a mediation analysis. Qual Life Res. (2014) 23:1869–76. doi: 10.1007/s11136-014-0636-5
24. Lin C-C. The effects of gratitude on suicidal ideation among late adolescence: a mediational chain. Curr Psychol. (2021) 40(5):2242–50. doi: 10.1007/s12144-019-0159-x
25. Low YTA. Family conflicts, anxiety and depressive symptoms, and suicidal ideation of Chinese adolescents in Hong Kong. Appl Res Qual Life. (2021) 16(6):2457–73. doi: 10.1007/s11482-021-09925-7
26. Soto-Chavarría E, Hidalgo-Rasmussen C, Nieto L. Quality of life, depressive symptoms, suicidal behavior and social support among pregnant adolescents in Mexico. Clin Med Insights Psychiatry. (2023) 14:1–10. doi: 10.1177/11795573231204015
27. Sun G, Zhao J, Tian S, Zhang L, Jia C. Psychological strain and suicidal ideation in athletes: the multiple mediating effects of hopelessness and depression. Int J Environ Res Public Health. (2020) 17:21. doi: 10.3390/ijerph17218087
28. Vidal-Arenas V, Bravo AJ, Ortet-Walker J, Ortet G, Mezquita L, Ibáñez MI, et al. Neuroticism, rumination, depression and suicidal ideation: a moderated serial mediation model across four countries. Int J Clin Health Psychol. (2022) 22:3. doi: 10.1016/j.ijchp.2022.100325
29. Haberling I, Berger G, Schmeck K, Held U, Walitza S. Omega-3 fatty acids as a treatment for pediatric depression. A phase III, 36 weeks, multi-center, double-blind, placebo-controlled randomized superiority study. Front Psychiatry. (2019) 10:1–16. doi: 10.3389/fpsyt.2019.00863
30. Albermann M, Emery S, Baumgartner N, Strumberger M, Erb S, Wockel L, et al. Executive functions and borderline personality features in adolescents with major depressive disorder. Front Hum Neurosci. (2023) 17:1–15. doi: 10.3389/fnhum.2023.957753
31. Baumgartner N, Haberling I, Emery S, Strumberger M, Nalani K, Erb S, et al. When parents and children disagree: informant discrepancies in reports of depressive symptoms in clinical interviews. J Affect Disord. (2020) 272:223–30. doi: 10.1016/j.jad.2020.04.008
32. Emery S, Haberling I, Berger G, Baumgartner N, Strumberger M, Albermann M, et al. Verbal memory performance in depressed children and adolescents: associations with EPA but not DHA and depression severity. Nutrients. (2020) 12(12):1–25. doi: 10.3390/nu12123630
33. Kaufman J, Birmaher B, Brent D, Rao U, Ryan N. Diagnostic Interview: Kiddie-SADS-present and Lifetime Version (K-SADS-PL). Pittsburgh: University of Pittsburgh (1996).
34. Härter M, Schorr S, Schneider F. S3-Leitlinie/Nationale Versorgungsleitlinie Unipolare Depression. Berlin Heidelberg: Springer (2017). doi: 10.1007/978-3-662-52906-5
35. Europe, T. K. G. The KIDSCREEN Questionnaires. Quality of Life Questionnaires for Children and Adolescents. Lengerich: Pabst Science Publishers (2006).
36. Nock MK, Holmberg EB, Photos VI, Michel BD. Self-Injurious thoughts and behaviors interview: development, reliability, and validity in an adolescent sample. Psychol Assess. (2007) 19(3):309–17. doi: 10.1037/1040-3590.19.3.309
37. Reynolds WM. SIQ, Suicidal ideation questionnaire: Professional manual: Psychological Assessment Resources (1988).
38. Fischer G, Ameis N, Parzer P, Plener PL, Groschwitz R, Vonderlin E, et al. The German version of the self-injurious thoughts and behaviors interview (SITBI-G): a tool to assess non-suicidal self-injury and suicidal behavior disorder. BMC Psychiatry. (2014) 14:1–8. doi: 10.1186/s12888-014-0265-0
39. Poznanski E, Mokros H. Children’s Depression Rating Scale-Revised (Vol. 12). Los Angeles, CA, USA: WPS (1996).
40. Keller F, Grieb J, Ernst M, Spröber N, Fegert JM, Kölch M. Children’s depression rating scale–revised (CDRS-R). entwicklung einer deutschen version und psychometrische gütekriterien in einer klinischen stichprobe. Z Kinder Jugendpsychiatr Psychother. (2011) 39(3):179–85. doi: 10.1024/1422-4917/a000090
41. Mayes TL, Bernstein IH, Haley CL, Kennard BD, Emslie GJ. Psychometric properties of the children’s depression rating scale–revised in adolescents. J Child Adolesc Psychopharmacol. (2010) 20(6):513–6. doi: 10.1089/cap.2010.0063
42. Little RJ. A test of missing completely at random for multivariate data with missing values. J Am Stat Assoc. (1988) 83(404):1198–202. doi: 10.1080/01621459.1988.10478722
43. Kim H-Y. Statistical notes for clinical researchers: chi-squared test and fisher’s exact test. Restor Dent Endod. (2017) 42(2):152. doi: 10.5395/rde.2017.42.2.152
44. Davis JM. Suicidal ideation questionnaire. J Psychoeduc Assess. (1992) 10(3):298–301. doi: 10.1177/073428299201000311
45. van der Spek N, Dekker W, Peen J, Santens T, Cuijpers P, Bosmans G, et al. Attachment-based family therapy for adolescents and young adults with suicide ideation and depression: an open trial. Crisis. (2023) 45(1):48–56. doi: 10.1027/0227-5910/a000916
46. Hartig F. DHARMA: Residual Diagnostics for Hierarchical (multi-level/mixed) Regression Models. R Package Version 0.4. 6. Vienna: CRAN The Comprehensive R Archive Network. (2022). doi: 10.32614/cran.package.dharma
47. Koller M. Robust linear mixed-effects models: an R package for handling outliers and non-normal data in longitudinal studies. J Stat Softw. (2023) 85(4):1–26. doi: 10.18637/jss.v075.i06
48. Tingley D, Yamamoto T, Hirose K, Keele L, Imai K. Mediation: R package for causal mediation analysis. J Stat Softw. (2014) 59:1–38. doi: 10.18637/jss.v059.i05
49. Alnosaier W. Comparisons of the satterthwaite approaches for fixed effects in linear mixed models. Int J Stat Probab. (2024) 13:1. doi: 10.5539/ijsp.v13n1p22
50. Baron RM, Kenny DA. The moderator–mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. (1986) 51(6):1173–82. doi: 10.1037//0022-3514.51.6.1173
51. Shrout PE, Bolger N. Mediation in experimental and nonexperimental studies: new procedures and recommendations. Psychol Methods. (2002) 7(4):422. doi: 10.1037//1082-989x.7.4.422
52. Gijzen MW, Rasing SP, Creemers DH, Smit F, Engels RC, De Beurs D. Suicide ideation as a symptom of adolescent depression. A network analysis. J Affect Disord. (2021) 278:68–77. doi: 10.1016/j.jad.2020.09.029
53. Wiebenga JX, Dickhoff J, Mérelle SY, Eikelenboom M, Heering HD, Gilissen R, et al. Prevalence, course, and determinants of suicide ideation and attempts in patients with a depressive and/or anxiety disorder: a review of NESDA findings. J Affect Disord. (2021) 283:267–77. doi: 10.1016/j.jad.2021.01.053
54. Gyori D, Farkas BF, Horvath LO, Komaromy D, Meszaros G, Szentivanyi D, et al. The association of nonsuicidal self-injury with quality of life and mental disorders in clinical adolescents-A network approach. Int J Environ Res Public Health. (2021) 18:4. doi: 10.3390/ijerph18041840
55. Zullig KJ. The association between deliberate self-harm and college student subjective quality of life. Am J Health Behav. (2016) 40(2):231–9. doi: 10.5993/ajhb.40.2.8
56. Cuijpers P, Karyotaki E, Ciharova M, Miguel C, Noma H, Stikkelbroek Y, et al. The effects of psychological treatments of depression in children and adolescents on response, reliable change, and deterioration: a systematic review and meta-analysis. Eur Child Adolesc Psychiatry. (2023) 32(1):177–92. doi: 10.1007/s00787-021-01884-6
57. Cuijpers P, Stringaris A, Wolpert M. Treatment outcomes for depression: challenges and opportunities. Lancet Psychiatry. (2020) 7(11):925–7. doi: 10.1016/s2215-0366(20)30036-5
58. Russell K, Rasmussen S, Hunter SC. Does mental well-being protect against self-harm thoughts and behaviors during adolescence? A six-month prospective investigation. Int J Environ Res Public Health. (2020) 17(18):1–18. doi: 10.3390/ijerph17186771
59. Morey Y, Mellon D, Dailami N, Verne J, Tapp A. Adolescent self-harm in the community: an update on prevalence using a self-report survey of adolescents aged 13–18 in England. J Public Health. (2017) 39(1):58–64. doi: 10.1093/pubmed/fdw010
60. Zadow C, Houghton S, Hunter SC, Rosenberg M, Wood L. Associations between positive mental wellbeing and depressive symptoms in Australian adolescents. Educ Dev Psychol. (2017) 34(2):95–105. doi: 10.1017/edp.2017.6
61. Gianfredi V, Blandi L, Cacitti S, Minelli M, Signorelli C, Amerio A, et al. Depression and objectively measured physical activity: a systematic review and meta-analysis. Int J Environ Res Public Health. (2020) 17(10):3738. doi: 10.3390/ijerph17103738
62. Pearce M, Garcia L, Abbas A, Strain T, Schuch FB, Golubic R, et al. Association between physical activity and risk of depression: a systematic review and meta-analysis. JAMA Psychiatry. (2022) 79(6):550–9. doi: 10.1001/jamapsychiatry.2022.0609
63. Singh B, Olds T, Curtis R, Dumuid D, Virgara R, Watson A, et al. Effectiveness of physical activity interventions for improving depression, anxiety and distress: an overview of systematic reviews. Br J Sports Med. (2023) 57(18):1203–9. doi: 10.1136/bjsports-2022-106195
64. Sibold J, Edwards E, Murray-Close D, Hudziak JJ. Physical activity, sadness, and suicidality in bullied US adolescents. J Am Acad Child Adolesc Psychiatry. (2015) 54(10):808–15. doi: 10.1016/j.jaac.2015.06.019
65. Algorta GP, Youngstrom EA, Frazier TW, Freeman AJ, Youngstrom JK, Findling RL. Suicidality in pediatric bipolar disorder: predictor or outcome of family processes and mixed mood presentation? Bipolar Disord. (2011) 13(1):76–86. doi: 10.1111/j.1399-5618.2010.00886.x
66. Çavuşoğlu H, Sağlam H. Examining the perceived social support and psychological symptoms among adolescents with leukemia. J Spec Pediatr Nurs. (2015) 20(1):76–85. doi: 10.1111/jspn.12101
67. King CA, Merchant CR. Social and interpersonal factors relating to adolescent suicidality: a review of the literature. Arch Suicide Res. (2008) 12(3):181–96. doi: 10.1080/13811110802101203
68. Kleiman EM, Law KC, Anestis MD. Do theories of suicide play well together? Integrating components of the hopelessness and interpersonal psychological theories of suicide. Compr Psychiatry. (2014) 55(3):431–8. doi: 10.1016/j.comppsych.2013.10.015
69. Hetrick SE, Parker AG, Robinson J, Hall N, Vance A. Predicting suicidal risk in a cohort of depressed children and adolescents. Crisis. (2012) 33(1):13–20. doi: 10.1027/0227-5910/a000095
70. Czyz EK, Liu Z, King CA. Social connectedness and one-year trajectories among suicidal adolescents following psychiatric hospitalization. J Clin Child Adolesc Psychol. (2012) 41(2):214–26. doi: 10.1080/15374416.2012.651998
71. Gariepy G, Honkaniemi H, Quesnel-Vallee A. Social support and protection from depression: systematic review of current findings in western countries. Br J Psychiatry. (2016) 209(4):284–93. doi: 10.1192/bjp.bp.115.169094
72. Wan L-p, Yang X-f, Liu B-p, Zhang Y-y, Liu X-c, Jia C-x, et al. Depressive symptoms as a mediator between perceived social support and suicidal ideation among Chinese adolescents. J Affect Disord. (2022) 302:234–40. doi: 10.1016/j.jad.2022.01.061
73. Lutrick K, Clark R, Nuño VL, Bauman S, Carvajal S. Latinx bullying and depression in children and youth: a systematic review. Syst Rev. (2020) 9:1–10. doi: 10.1186/s13643-020-01383-w
74. Ye Z, Wu D, He X, Ma Q, Peng J, Mao G, et al. Meta-analysis of the relationship between bullying and depressive symptoms in children and adolescents. BMC Psychiatry. (2023) 23(1):215. doi: 10.1186/s12888-023-04681-4
75. Limbana T, Khan F, Eskander N, Emamy M, Jahan N. The association of bullying and suicidality: does it affect the pediatric population? Cureus. (2020) 12(8):1–9. doi: 10.7759/cureus.9691
76. Quintero-Jurado J, Moratto-Vásquez N, Caicedo-Velasquez B, Cárdenas-Zuluaga N, Espelage DL. Association between school bullying, suicidal ideation, and eating disorders among school-aged children from Antioquia, Colombia. Trends Psychol. (2022) 30(1):58–72. doi: 10.1007/s43076-021-00101-2
77. Serafini G, Aguglia A, Amerio A, Canepa G, Adavastro G, Conigliaro C, et al. The relationship between bullying victimization and perpetration and non-suicidal self-injury: a systematic review. Child Psychiatry Hum Dev. (2023) 54(1):154–75. doi: 10.1007/s10578-021-01231-5
78. Pfledderer CD, Burns RD, Brusseau TA. School environment, physical activity, and sleep as predictors of suicidal ideation in adolescents: evidence from a national survey. J Adolesc. (2019) 74:83–90. doi: 10.1016/j.adolescence.2019.05.008
79. Shang L, Li J, Li Y, Wang T, Siegrist J. Stressful psychosocial school environment and suicidal ideation in Chinese adolescents. Soc Psychiatry Psychiatr Epidemiol. (2014) 49:205–10. doi: 10.1007/s00127-013-0728-5
80. Klemera E, Brooks FM, Chester KL, Magnusson J, Spencer N. Self-harm in adolescence: protective health assets in the family, school and community. Int J Public Health. (2017) 62:631–8. doi: 10.1007/s00038-016-0900-2
81. Valdivia M, Silva D, Sanhueza F, Cova F, Melipillán R. Prevalencia de intento de suicidio adolescente y factores de riesgo asociados en una comuna rural de la provincia de concepción. Revista Médica de Chile. (2015) 143(3):320–8. doi: 10.4067/s0034-98872015000300006
82. Thatcher WG, Reininger BM, Drane JW. Using path analysis to examine adolescent suicide attempts, life satisfaction, and health risk behavior. J School Health. (2002) 72(2):71–7. doi: 10.1111/j.1746-1561.2002.tb06518.x
83. Lai Kwok SY, Shek DT. Personal and family correlates of suicidal ideation among Chinese adolescents in Hong Kong. Soc Indic Res. (2010) 95:407–19. doi: 10.1007/s11205-009-9528-4
84. Luo J-M, Liu E-Z, Yang H-D, Du C-Z, Xia L-J, Zhang Z-C, et al. Prevalence and factors associated with suicidal ideation in medical students with migraine. Front Psychiatry. (2021) 12:1–8. doi: 10.3389/fpsyt.2021.683342
85. Wang W, Zhou DD, Ai M, Chen XR, Lv Z, Huang Y, et al. Internet addiction and poor quality of life are significantly associated with suicidal ideation of senior high school students in Chongqing, China. PeerJ. (2019) 7:e7357. doi: 10.7717/peerj.7357
86. Bodenmann G. Lehrbuch klinische paar–und familienpsychologie. Hogrefe AG. (2016) 2:77–181. doi: 10.1024/85620-000
87. Brown BB, Larson J. Peer relationships in adolescence. Handbook Adolesc Psychol. (2009) 2(Pt I):74–104. doi: 10.1002/9780470479193.adlpsy002004
88. Valkenburg PM, Sumter SR, Peter J. Gender differences in online and offline self-disclosure in pre-adolescence and adolescence. Br J Dev Psychol. (2011) 29(2):253–69. doi: 10.1348/2044-835x.002001
89. Balazs J, Miklosi M, Halasz J, Horvath LO, Szentivanyi D, Vida P. Suicidal risk, psychopathology, and quality of life in a clinical population of adolescents. Front Psychiatry. (2018) 9:1–8. doi: 10.3389/fpsyt.2018.00017
90. Narita K, Yonemoto N, Kawashima Y, Takai M, Matsuo M, Hirayasu Y, et al. Changes in health-related quality of life in patients admitted to emergency departments for attempted suicide: findings from a large longitudinal study. J Affect Disord. (2024) 347:262–8. doi: 10.1016/j.jad.2023.11.036
91. Ribeiro JD, Huang X, Fox KR, Franklin JC. Depression and hopelessness as risk factors for suicide ideation, attempts and death: meta-analysis of longitudinal studies. Br J Psychiatry. (2018) 212(5):279–86. doi: 10.1192/bjp.2018.27
92. Deng L, Yang M, Marcoulides KM. Structural equation modeling with many variables: a systematic review of issues and developments. Front Psychol. (2018) 9:580. doi: 10.3389/fpsyg.2018.00580
93. Nunan D, Aronson J, Bankhead C. Catalogue of bias: attrition bias. BMJ Evid Based Med. (2018) 23(1):21–2. doi: 10.1136/ebmed-2017-110883
94. Graca BD, Hall LR, Sanchez K, Bennett MM, Powers MB, Warren AM. The risks of attrition bias in longitudinal surveys of the impact of COVID-19. Proc (Bayl Univ Med Cent). (2023) 36(2):161–4. doi: 10.1080/08998280.2022.2139541
95. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association (1994). doi: 10.1017/s0033291700035765
96. Poznanski E, Mokros H. Children's Depression Rating Scale – Revised. Vol 12. Los Angeles, CA: WPS Western Psychological Services (1996). doi: 10.1037/t55280-000
97. R Core Team. R: A language and environment for statistical computing. Vienna: R Foundation for Statistical Computing (2020). Available online at: https://www.R-project.org/V
Keywords: health-related quality of life, HRQoL, suicidality, suicidal ideation, depression, children, adolescents
Citation: Preisig M, Häberling I, Smigielski L, Emery S, Baumgartner N, Albermann M, Strumberger M, Schmeck K, Wöckel L, Erb S, Rhiner B, Contin-Waldvogel B, Walitza S and Berger G (2025) The mediating role of depression in the association between health-related quality of life and suicidal ideation in adolescents: findings from a longitudinal study. Front. Child Adolesc. Psychiatry 4:1567387. doi: 10.3389/frcha.2025.1567387
Received: 27 January 2025; Accepted: 25 July 2025;
Published: 14 August 2025.
Edited by:
Tiziana Pisano, Azienda Ospedaliera Universitaria Meyer IRCCS—Firenze, ItalyReviewed by:
Barbara Remberk, Institute of Psychiatry and Neurology (IPiN), PolandChengchen Zhang, Shanghai Children’s Medical Center, China
Copyright: © 2025 Preisig, Häberling, Smigielski, Emery, Baumgartner, Albermann, Strumberger, Schmeck, Wöckel, Erb, Rhiner, Contin-Waldvogel, Walitza and Berger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martina Preisig, bWFydGluYS5wcmVpc2lnQHB1a3poLmNo