 G. K. Scadding1*†
G. K. Scadding1*† D. M. Conti2,3,†
D. M. Conti2,3,† S. Scheire4,†
S. Scheire4,† V. Backer5,†
V. Backer5,† M. Blaiss6,†
M. Blaiss6,† L. O. Cardell7,8,†
L. O. Cardell7,8,† W. De Yun9,†A. K. Ellis10,†W. Fokkens11,†
W. De Yun9,†A. K. Ellis10,†W. Fokkens11,† A. T. Fox12,†
A. T. Fox12,† T. Gilbert Kruz13S. Halken14,†
T. Gilbert Kruz13S. Halken14,† P. W. Hellings2,15,16,†V. Hox17,†
P. W. Hellings2,15,16,†V. Hox17,† L. Kalogjera18
L. Kalogjera18 S. Lau19,†S. Marinho20,†
S. Lau19,†S. Marinho20,† M. McDonald21,†
M. McDonald21,† R. Mösges22,23
R. Mösges22,23 J. Mullol24,†S. Nasser25,†
J. Mullol24,†S. Nasser25,† R. Pawankar26,†
R. Pawankar26,† D. Price27,28,†D. Ryan29,†G. Scadding30P. Smith31,†M. Sosa Kostrábová13
D. Price27,28,†D. Ryan29,†G. Scadding30P. Smith31,†M. Sosa Kostrábová13 M. Vazquez-Ortiz32U. Wahn33
M. Vazquez-Ortiz32U. Wahn33 L. Zhang34,†
L. Zhang34,† P. Gevaert4,†
P. Gevaert4,†
- 1Royal National ENT Hospital and University College, London, United Kingdom
- 2Escuela de Doctorado UAM, Centro de Estudios de Posgrado, Universidad Autónoma de Madrid, Calle Francisco Tomás y Valiente, no. 2, Ciudad Universitaria de Cantoblanco, Madrid, Spain
- 3Allergy and Clinical Immunology Research Unit, Department of Microbiology and Immunology, KU Leuven, Leuven, Belgium
- 4Upper Airways Research Laboratory, Department of Head and Skin, Ghent University, Ghent, Belgium
- 5Department of Otorhinolaryngology, Head & Neck Surgery, and Audiology, Rigshospitalet, Copenhagen University, Copenhagen, Denmark
- 6Medical College of Georgia at Augusta University, Augusta, GA, United States
- 7Division of ENT Diseases, Department of Clinical Sciences, Intervention and Technology, Karolinska Institutet, Stockholm, Sweden
- 8Department of ENT Diseases, Karolinska University Hospital, Stockholm, Sweden
- 9Department of Otolaryngology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
- 10Division of Allergy & Immunology, Department of Medicine, Queen’s University, Kingston, ON, Canada
- 11Department of Otorhinolaryngology, Amsterdam University Medical Centres, Amsterdam, Netherlands
- 12Guy’s & St Thomas’ Hospitals NHS Foundation Trust, London, United Kingdom
- 13Patient Advisory Board, European Forum for Research and Education in Allergy and Airway Diseases, Brussels, Belgium
- 14Hans Christian Andersen Children’s Hospital, Odense University Hospital, Odense, Denmark
- 15Laboratory of Upper Airways Research, Department of Otorhinolaryngology, University of Ghent, Ghent, Belgium
- 16Clinical Department of Otorhinolaryngology, Head and Neck Surgery, University Hospitals Leuven, Leuven, Belgium
- 17Department of Otorhinolaryngology, Cliniques Universitaires Saint Luc, Brussels, Belgium
- 18Department of Otorhinolaryngology/Head and Neck Surgery, University Hospital Centre “Sestre milosrdnice”, Zagreb School of Medicine, Zagreb, Croatia
- 19Department of Pediatric Respiratory Medicine, Immunology and Critical Care Medicine, Charité Universitätsmedizin Berlin, Berlin, Germany
- 20Allergy Centre, Wythenshawe Hospital, Manchester University NHS Foundation Trust and The University of Manchester, Manchester, United Kingdom
- 21The Allergy Clinic, Johannesburg, South Africa
- 22ClinCompetence Cologne GmbH, Cologne, Germany
- 23Institute of Medical Statistics and Computational Biology, Faculty of Medicine, University of Cologne, Cologne, Germany
- 24Rhinology Unit & Smell Clínic, Department of Otorhinolaryngology, Hospital Clínic Barcelona, Universitat de Barcelona; FRCB-IDIBAPS; CIBERES, Barcelona, Catalonia, Spain
- 25Cambridge University Hospitals NHS Foundation Trust, Cambridge, United Kingdom
- 26Department of Pediatrics, Nippon Medical School, Bunkyo-ku, Tokyo, Japan
- 27Observational and Pragmatic Research Institute, Singapore, Singapore
- 28Centre of Academic Primary Care, Division of Applied Health Sciences, University of Aberdeen, Aberdeen, United Kingdom
- 29Usher Institute, University of Edinburgh, Edinburgh, Scotland
- 30Allergy Department, Royal Brompton Hospital, London, United Kingdom
- 31Griffth University, Southport, QLD, Australia
- 32Section of Inflammation, Repair and Development, National Heart and Lung Institute, Imperial College London, London, United Kingdom
- 33Charite University Medicine, Berlin, Germany
- 34Department of Otolaryngology Head and Neck Surgery and Department of Allergy, Beijing TongRen Hospital, Capital Medical University, Beijing, China
Allergic rhinitis (AR), the most prevalent immunological disease, affects approximately 400 million individuals globally and can significantly impact quality of life (QoL). Despite nearly 25 years of guidelines, AR remains largely under- diagnosed, suboptimally treated and poorly controlled. In the light of new knowledge and treatment options, there is a necessity to update or revise fundamental AR definitions to facilitate communication across diverse specialties engaged in its treatment and to improve patient care. The European Forum for Research and Education in Allergy and Airway Diseases (EUFOREA) convened a meeting of experts and patient representatives to deliberate the optimal methodology for measuring AR treatment responses and establishing novel treatment goals. This paper presents a consensus on revised AR definitions, including control, severe allergic rhinoconjunctivitis (SARC), refractory severe allergic rhinoconjunctivitis (R-SARC), remission, resolution, improvement, exacerbation, treatable traits (TTs), treat to target, relapse, progression, disease modification, and prevention.
Introduction
About 30% of the European population is affected by AR (1–3), an inflammatory disorder of the nasal lining that is caused by a reaction to various allergens. AR severity ranges from a minor nuisance to a condition which significantly reduces QoL, work and school attendance and performance (4–7). Furthermore, AR is a risk factor for a number of comorbidities, including allergic asthma (8–10). AR and asthma share a common pathology, based on Th2-inflammation, also relevant to other co-morbid conditions including chronic rhinosinusitis with nasal polyps (CRSwNP).
In light of evolving knowledge and treatment options, there is a growing necessity to (re)define fundamental terms across the diverse specialties engaged in AR management. These should facilitate communication between physicians and patients regarding therapeutic options and treatment goals (11, 12). In the same context, the chronic rhinosinusitis (CRS) expert panel members of the European Forum for Research and Education in Allergy and Airway disease (EUFOREA) has defined disease states in chronic rhinosinusitis, giving rise to the adoption of remission within the treatment goals of CRSwNP (13).
The AR and Its Impact on Asthma (ARIA) initiative is a non-governmental organisation that works in collaboration with the World Health Organization (WHO) to develop guidance on the management of patients with AR. ARIA has provided a useful classification for AR, stressed its frequent links with asthma, evaluated treatments according to Grading of Recommendations-Assessment, Development and Evaluation (GRADE) methodology and initiated mobile technology for disease monitoring (14–17). The most recent iteration of the ARIA document is devoid of a list of definitions, including one pertaining to resolution (15). EUFOREA is an international not-for-profit organisation with a mission of reducing the burden of chronic respiratory diseases by implementing optimal care in daily practice (11, 12). Optimal care implies a correct diagnosis and timely treatment, leading to improvement in QoL of individual patients and cost-savings for society. Following two consensus meetings on asthma in London (April 2023) and CRS in Brussels (June 2023) (13), EUFOREA is now focusing on AR with the objective of reaching a consensus on definitions for disease states and treatment targets. It is our intention that, following this academic exercise, those treating AR will be enabled to communicate more accurately with each other and with patients, allowing identification of areas that require further attention, approaches that warrant further consideration and the strengths and weaknesses of current approaches.
Methodology
A preliminary virtual meeting was convened to discuss the points and definitions that should be addressed until alignment was reached. The experts were given the opportunity to elaborate on the concepts in advance, thus allowing for a fluid discussion during the in-person debate.
The active participation of internationally renowned specialists in the fields of primary care, ENT, paediatrics, pulmonology, allergology, and immunology facilitated the attainment of an agreement following a full day of discussion in the Royal Society of Medicine of UK in London in June 2024. A patient diagnosed with severe AR participated in the meeting and other patients from the EUFOREA Patient Advisory Board provided feedback on the draft manuscript. A preliminary draft of the consensus document was prepared and subsequently reviewed by a further group of experts, who also served as co-authors. Following the review process, the remaining points of contention were discussed and addressed in virtual web-based meetings until consensus was reached. In 2024, a revised draft was distributed for final review and approval by all contributing authors.
The following topics were included in the discussion: control, severe allergic rhinoconjunctivitis (SARC), refractory severe allergic rhinoconjunctivitis (R-SARC), remission, resolution, improvement, exacerbation, TTs, treat to target, relapse, progression, disease modification, and prevention.
Unmet needs in AR
Almost a quarter of a century has elapsed since the WHO first established a consensus on AR (14). The creation of the ARIA initiative paved the way for agreement on classifications, unification of diagnostic criteria, and determination of therapeutic measures. Nevertheless, despite the efforts of ARIA and EUFOREA in producing a substantial number of documents, guidelines and educational materials (1–3, 14, 15, 18), the reality is that AR remains a highly prevalent disease and many patients remain uncontrolled (5, 19–21).
Previous research has shown that multiple factors contribute to uncontrolled disease, including disease, patient, environmental, healthcare provider and treatment-related factors which also include the possibility of over-the-counter treatment without assessment or diagnosis of severity (20, 21). A recent observational study by Scheire et al. (5) examined rhinitis control in a real-world setting of Belgian pharmacy patients with persistent rhinitis, with a particular focus on the contribution of patient-related and treatment-related factors. This study revealed that treatment selection was suboptimal, with high usage of systemic corticosteroids and over-the-counter accessibility of nasal decongestants, capable of causing systemic adverse effects and rhinitis medicamentosa, respectively. Additionally, the authors identified that nasal spray technique and adherence to intranasal corticosteroids in real-life is poor with only 10% of patients administering medication correctly (Box 1). A further worry is the purchase of first-generation sedating antihistamines by the public who are unaware of the dangers these represent (22), especially for the treatment of AR symptoms in children in whom they reduce the ability to learn and increase the likelihood of epileptic seizures, among other side effects (23–25).
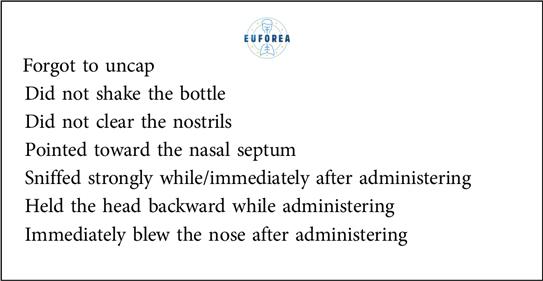
Box 1. Errors in nasal spray usage (data extracted from reference 5).
Patients suffering from AR often attempt to self-manage their disease, which can be advantageous from a superficial health economic perspective focused on short-term costs but potentially leads to incorrect treatment choices, inadequate response and increased adverse events (26). However, even among those seeking care from a physician, some patients remain uncontrolled despite optimal combination therapy with both intranasal corticosteroid plus intranasal antihistamine (19). The findings of these studies highlight the unmet need for both enhanced and comprehensive patient education (5, 27–29) and more effective AR treatments and preventive measures (19, 20, 30, 31).
Intranasal glucocorticoids (INCS) represent the preferred treatment option for a significant proportion of individuals with AR. However, there is a tendency for these medications to be employed in a suboptimal manner and subsequently discontinued (1–3, 5, 32). Factors influencing patients' adherence to INCS are illustrated in Table 1. Intentional causes represent the most common category. Disease control is frequently inadequate due to patients' reluctance to adhere to their medication regimens (33, 34). This illustrates the need for patient education as well as devices for administration that improve adherence.
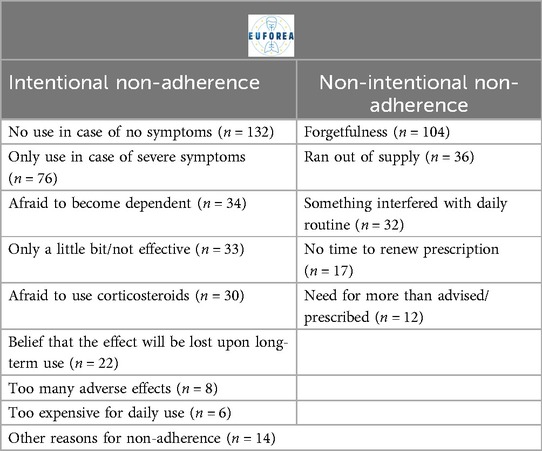
Table 1. Adherence to intranasal glucocorticoids (data extracted from reference 5).
The EUFOREA AR pocket guidelines (1–3) build on the foundations of ARIA (16) and the British Society for Allergy and Immunology (BSACI) guidelines (18) and present an updated algorithmic approach to the assessment and treatment of AR, at all levels within the health system, with separate diagrams for adults and for children (1–3).
Useful definitions of mild, moderate and severe AR have been previously proposed (35–37), together with those for allergic conjunctivitis (38). Although these represent a step forward, the authors believe that they do not address another problematic issue, which is represented by patients with severe disease, with a confirmed diagnosis after re-evaluation, who do not respond to guideline-directed treatments, even after associated comorbidities have been addressed. To address this gap, this group has agreed on two key concepts: a redefinition of severe allergic rhinoconjunctivitis (SARC) and the introduction of a new concept, refractory severe allergic rhinoconjunctivitis (R-SARC).While SARC refers to a condition characterized by allergic inflammation leading to persistent symptoms (>4 days per week for >4 consecutive weeks) which significantly impact QoL, including sleep, work, school or leisure activities, as exemplified by a visual analogue scale (VAS) score ≥70 mm for total nasal symptoms; R-SARC describes patients with ongoing SARC despite optimal guideline-informed pharmacological and non-pharmacological management. This addition is reflected in the algorithm shown in Figure 1.
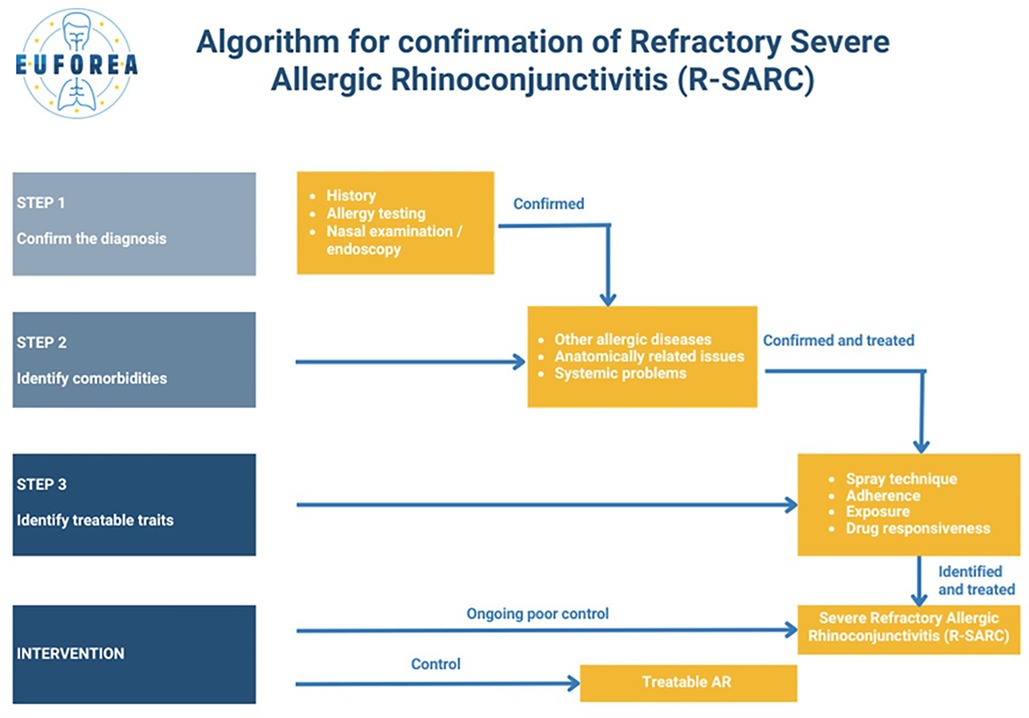
Figure 1. Algorithm for confirmation of refractory severe allergic rhinoconjunctivitis (R-SARC).
This milestone opens up a new spectrum of applications, not only in terms of a unified language and consideration of a new level of complexity, but also in terms of the associated therapeutic indications. Specialist treatment reduces AR severity (39).
To date, AIT has proven to be the only treatment capable of modifying disease progression in AR (40–43). Although its inclusion as a therapeutic option is generally accepted and included in guidelines (40–43), there are often barriers to its use, principally due to cost, lack of availability in certain countries, and lack of high-quality vaccine products for some allergens. This leaves a group of patients with severe disease without a therapeutic option. In addition, multiallergic patients are often unsuitable for AIT therapy.
Biologics, such as anti-IgE and anti-cytokine monoclonal antibodies, have recently been explored in the treatment of AR (44). Their potential role is particularly relevant in refractory severe AR with comorbidities (R-SARC) (45), where the use of systemic corticosteroids is frequent and often the only remaining treatment option (2, 3). In many cases of corticosteroid-dependent disease such as asthma or atopic dermatitis, alternatives like biologics have successfully reduced the need for systemic corticosteroids (10). Similarly, better treatment options are needed for this subset of R-SARC patients. The addition of biologics to other therapies has yielded promising outcomes, particularly in patients with severe disease and inadequate control (46, 47). Anti-IgE therapy has been extensively studied in AR; however, two decades ago, its cost-benefit ratio was considered unfavorable, although costs from systemic corticosteroid-related adverse events were ignored (48, 49). With the advent of biosimilars, which should reduce treatment costs, the incorporation of biologics should be considered as a viable option in R-SARC. The combination of AIT and anti-IgE (or other biologics) might allow treatment of patients otherwise deemed too high risk for AIT (typically because of severe/uncontrolled asthma) by reducing the risk of adverse reactions including asthma exacerbations and anaphylaxis. Moreover, the combination would be expected to give more rapid symptom control, giving time for the effects of AIT to be established. The outcomes of AIT are most optimal when used in young children (43). It is the more severely affected child with House dust mite—sensitive AR who is most likely to progress to asthma and other co- morbidities (8), thus such combined therapy in early life has the potential to prevent life-long problems. Research needs to be undertaken in this area. It is our hope that this document will serve as a foundation for the incorporation of biologics into further AR research and subsequently clinical practice.
Results
The following definitions were discussed and adopted:
Laying the foundations in AR: control, remission, and resolution
In the context of chronic diseases, including AR, control is typically the primary objective of treatment (50), given that cure is rarely achievable (50, 51).
While the recently introduced categories of uncontrolled disease have been referenced above under the acronyms SARC and R-SARC, this group proposes that control be defined as “the extent to which therapy goals are achieved, as determined by the patient and treating physician”. It is proposed that the VAS be used for this by the patient and the treating physician (48, 49, 52). The proposed limits are as follows: a score of less than or equal to 23 mm (for total symptom severity) would indicate that the patient is well-controlled, while a score greater than 23 mm but less than or equal to 50 mm would indicate that the patient is partially controlled (52, 53) (Figure 2).
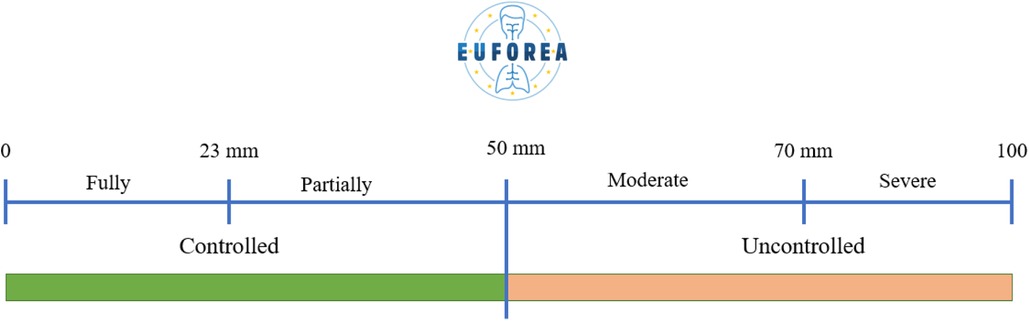
Figure 2. VAS scores and their interpretation.
In the context of AR, clinical remission is defined as “a state or period with low or no disease activity (on or off safe long-term treatment)”. In a state of remission, patients are free from exacerbations and have a VAS of less than 23 mm (54, 55). The expert board concurred that the definition of clinical remission should encompass not only patient-reported symptoms and control, but also physician-reported control (54, 55). Complete remission requires “normalisation or stabilisation of any underlying pathology in addition to symptomatic remission, as defined for asthma” occurring off therapy for a period of a year or more (56).
Resolution (or cure) can be defined as “a permanent return to a state of normal health, off treatment and without signs of active mucosal disease” (57, 58). We suggest that complete remission for a period of 5 years equates to resolution/cure.
The objective of treatment should be to achieve remission in all and resolution where possible. The available treatments targeting the underlying inflammation of AR and their possible disease-modifying effects must encourage clinicians to aim for more than mere control of the condition in their patients.
Improvement, exacerbation, and treatable traits
Although regression is the most commonly used term in the context of other airway diseases, such as CRSwNP (13), this group believes that it carries a negative connotation that is not helpful in the context of AR (59). It is our contention that the term improvement is the most accurate in this context.
An improvement of 23 mm in the VAS for total symptoms under therapy indicates effective treatment (60); moreover, an improvement of 30 mm has been consistently associated with improvements in QoL parameters (61). See therapeutic response below.
An exacerbation is “a sudden and pronounced intensification of existing symptoms (62), frequently precipitated by an increase in allergen exposure, environmental changes, or concurrent respiratory infections” (63). Such exacerbations can have a considerable impact on an individual's daily functioning and QoL, necessitating prompt and effective management (2, 3). It is of the utmost importance to identify and mitigate triggers through environmental controls and patient education in order to prevent exacerbations. In the management of severe exacerbations, pharmacological interventions may be required, including therapeutic escalation (2, 3). An understanding of the underlying mechanisms, including heightened inflammatory responses and airway hyperreactivity, is vital for the development of targeted strategies to predict, prevent and treat exacerbations. In the event of an exacerbation a step-up approach is typically employed, with rescue treatment often being administered (64). However, the expert board acknowledges the necessity of considering TTs prior to switching treatments.
TTs represent “specific phenotypic and endotypic characteristics that can be targeted to optimise patient management” (65). These traits include the type and severity of allergic response, environmental control, the presence of structural abnormalities (septal deviation, turbinate hypertrophy, or adenoid hypertrophy) or comorbid conditions such as asthma, common cold (including COVID-19)/acute rhinosinusitis, chronic rhinosinusitis with/without nasal polyps or mental health issues, and individual responsiveness to specific treatments. The identification of these traits through comprehensive clinical assessments and biomarker profiling enables a personalised approach to therapy, improving efficacy and reducing adverse effects (2, 3, 65–67). A typical TT fulfils three criteria: identifiable/measurable, clinically relevant, and treatable (68). A TTs strategy has already been implemented in other airway diseases such as CRSwNP and asthma (68, 69) with improvements in both QoL and response to biologics (68, 69).
Table 2 presents a list of TTs in patients with AR.
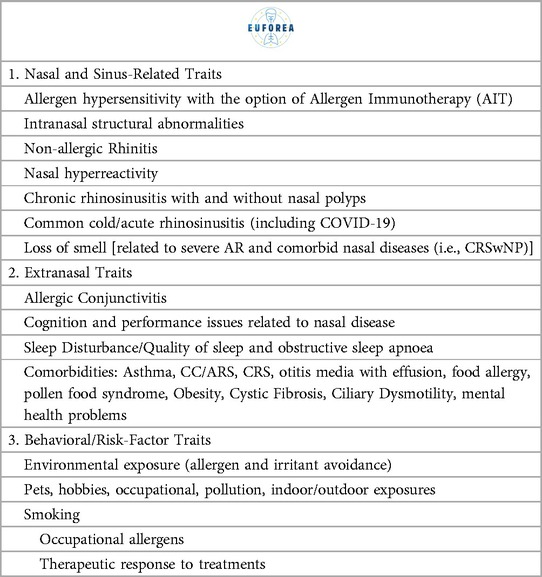
Table 2. Treatable traits in AR.
By defining, identifying and addressing these TTs, we aim to improve outcomes of care, including the reduction in oral corticosteroid and/or decongestant use (2, 3) and preventing their adverse effects (39).
Therapeutic response and treat to target
Therapy in AR is multifaceted, encompassing both pharmacological and non-pharmacological interventions and lifestyle (preventive) measures such as allergen avoidance and nasal douching (70, 71). When preventive measures fail, pharmacotherapy is recommended in addition to continued saline douching. The objective of these interventions is to mitigate symptoms and improve patient QoL, i.e., to achieve a good therapeutic response. First-line treatments typically comprise antihistamines and intranasal corticosteroids, either alone or in fixed (topical) combination, which have been demonstrated to be efficacious in the reduction of nasal congestion, rhinorrhoea and sneezing (70, 71) as well as in olfactory dysfunction which is a marker of severe AR (72) and adults (73).
Immunotherapy, whether subcutaneous or sublingual, represents a disease-modifying approach that provides long-term relief and the potential for remission by inducing immunological tolerance (74–76). New therapies targeting specific immune pathways, such as biologics, show promise in cases where other treatments have failed, although further research is needed to fully elucidate their long-term benefits and safety profiles in AR (48, 49). Optimising therapeutic strategies through personalised medicine, considering patient-specific factors such as allergen sensitivity, comorbid conditions, and genetic predispositions, is pivotal in enhancing treatment outcomes. Several attempts have been made in the past decade within the ARIA and EUFOREA expert panels to define therapeutic response. In most consensus documents (2, 3, 14, 15, 34, 35), a therapeutic response using the following criteria has been proposed:
- Clinical/symptom score improvement represented by Rhinoconjunctivitis QoL Questionnaire (RQLQ) (77, 78), VAS, and Rhinitis Control Assessment Test (RCAT) (79). The established cut-off variation of 23 mm for VAS was associated with a cut-off variation of 0.5 for RQLQ. Sensitivity analysis with RQLQ and type VI secretion system scales confirmed the aptitude of the cut-off value (23 mm) to discriminate changes in symptoms and QoL (54, 55). A change of 3 points in the RCAT is significant (79).
- Improvement of Sleep quality/tiredness
- Decreased impact on Work/school attendance/performance
- Improvement in recreational activities
- Prevention of progression/improvement of comorbidities
- Reduction of on-demand/as needed pharmacotherapy
- Reduction in ≥1 level of severity (severe -> moderate -> mild) or ≥1 level of control (uncontrolled -> partially controlled -> controlled) could also be considered.
- Upper airway assessment by peak nasal inspiratory flow (PNIF), acoustic rhinometry or rhinomanometry (specialist tools)
- Rhinoscopy (specialist tool)
- A further possible measure is one of olfaction such as Sniffin Sticks (72) since smell loss is proportional to AR severity.
- Further work on such parameters in R-SARC is to be welcomed.
The treat to target approach to AR represents a paradigm shift towards personalised and goal-directed management (80, 81). This strategy focuses on achieving predefined clinical outcomes such as clinical remission (80, 81). By continuously monitoring patient response, including the use of mobile technology. and adjusting treatment accordingly, clinicians can better address the heterogeneity of patient outcomes in AR (80, 81). Mobile health applications can provide patients with daily management support: medication reminders, pollen count alerts and personalized advice based on symptom tracking. They empower patients to manage their condition more effectively, enhancing adherence and minimizing the impact of AR on daily activities.
Integration of artificial intelligence (AI) in these technologies offers more tailored management. AI can analyze data from a wide array of sources, including environmental monitoring systems and individual health trackers, to predict symptom flare-ups. In addition, AI-driven analytics can contribute to a better understanding of treatment responses and patient behaviours, leading to improved therapeutic strategies. Embracing these technologies in AR management promises to enhance individual patient care and aid in the broader goal of refining treatment protocols and improving outcomes (17, 82–83).
The treat to target approach often involves the integration of patient-reported outcome measures and objective assessments to precisely tailor interventions. Furthermore, advances in biomarkers and precision medicine are further refining the treat to target model, enabling more accurate prediction of therapeutic responses and fostering a more dynamic and responsive treatment landscape. The term treat to target is defined by this group as “any measure employed in the context of healthcare that is designed to facilitate control, whether that be the control of the patient's symptoms or the control of the pathologic process”.
Relapse, progression, and disease modification
A relapse in AR is “the recurrence of symptoms following a period of remission”. This can be triggered by renewed allergen exposure, seasonal changes, or lapses in treatment adherence (84). It is important to gain an understanding of the factors that contribute to relapse in order to develop effective strategies for maintaining long-term control.
Progression in AR involves the worsening of symptoms over time and the potential development of related comorbid conditions such as asthma, acute and chronic rhinosinusitis, and conjunctivitis (84, 85). This progression is often driven by persistent allergen exposure, ongoing inflammation, and genetic predisposition (84, 85). Early and effective intervention is crucial in altering the disease course and preventing complications. This group proposes to define progression as a development or worsening of AR symptoms and/or related comorbidities.
The objective of disease modification in AR is “to alter the natural course of the disease, thereby achieving sustained symptom relief and improved long-term outcomes”. This approach is primarily based on AIT (86), which has been demonstrated to induce long-lasting immunological tolerance and to reduce the progression of allergic symptoms, i.e., number of new sensitisations or the development of asthma (87, 88). By targeting the underlying immune mechanisms, such as IgE-mediated hypersensitivity and Th2-driven inflammation, AIT has the potential to significantly diminish the severity and frequency of allergic reactions (86–88). Furthermore, the development of novel biologic therapies that inhibit specific cytokines and immune pathways may represent a promising avenue for disease modification (86–88). Disease-modifying treatments are different from symptomatic treatments as they are able to address the pathogenesis of a disease, preventing progression or leading to a long-term reduction in symptoms even after discontinuation (86–88). Disease modification may be signalled by complete remission.
This group considers it appropriate to distinguish between the concept of disease modification in the clinical management of AR to that applied in research. While the former refers to changes induced by treatments or interventions targeting the underlying allergic cause, with effects that persist after treatment cessation the latter needs to be validated using biomarkers, such as IgG4.
Prevention
Prevention in AR involves ’strategies aimed at reducing the onset and progression of symptoms through a combination of environmental controls, pharmacologic interventions, and lifestyle modifications'.
There are three types of prevention: primary, secondary, and tertiary prevention that rely on recognition of the aetiology and triggers, early recognition of symptoms and a correct diagnosis/treatment. Primary prevention is intended to prevent disease development, secondary to limit disease progression, and tertiary to reduce associated symptoms and limit sequelae.
Primary prevention focuses on reducing disease incidence by changing causal or predisposing factors, e.g., in the workplace. It encompasses those patients who do not yet have AR but who are at risk of its development (89, 90).
Secondary prevention focuses on early disease detection to return a patient to full health and prevent persistent or extended disease. It refers to patients with early AR or already sensitised and describes measures to be taken to prevent AR from progressing in severity or developing comorbidities by means such as avoidance or reduction of exposure to allergens or irritants or by AIT (8, 43, 90, 91).
Tertiary prevention is defined by a reduction of the impact of ongoing disease and its complications in order to maximize QoL (89). In AR this refers to patients suffering from severe AR and describes measures to be taken to prevent the addition of comorbidities or sequelae (2, 3). This can be achieved by appropriate therapy according to the most recent guidelines (90–92). It is within this context that the incorporation of AIT or biologics into the therapeutic regimen becomes particularly pertinent (90–92).
Conclusion
This academic exercise sought to initiate improvement in the care and therapeutic management of patients suffering from AR, with a particular focus on those with severe or unresponsive forms of the disease by accurately defining disease states. The result is a list of foundational disease definitions, represented in Table 3.
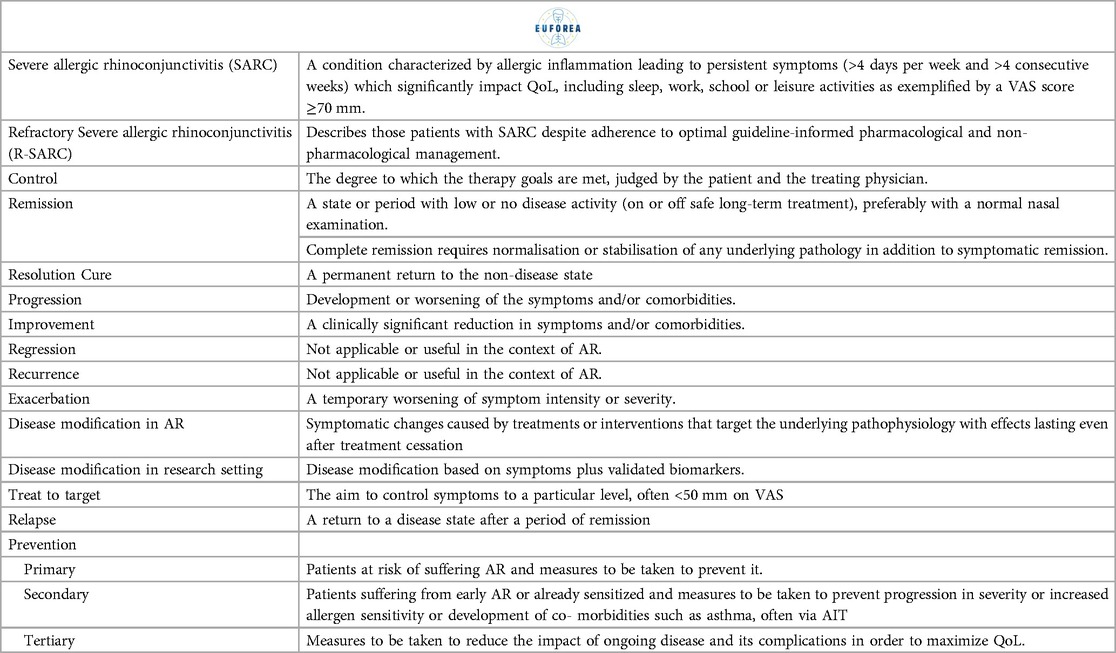
Table 3. Key definitions in AR agreed upon by EUFOREA expert panel members.
EUFOREA suggests this glossary may serve as a guide to establish a foundation for improved care for patients with AR.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
GS: Conceptualization, Supervision, Writing – original draft, Writing – review & editing. DC: Conceptualization, Methodology, Supervision, Writing – original draft, Writing – review & editing. SS: Conceptualization, Methodology, Resources, Writing – original draft. VB: Conceptualization, Methodology, Supervision, Writing – review & editing. MB: Conceptualization, Methodology, Supervision, Writing – review & editing. LC: Conceptualization, Methodology, Supervision, Writing – review & editing. DW: Conceptualization, Methodology, Supervision, Writing – review & editing. AE: Conceptualization, Investigation, Methodology, Supervision, Writing – review & editing. WF: Conceptualization, Investigation, Methodology, Writing – review & editing. AF: Conceptualization, Investigation, Methodology, Writing – review & editing. TG: Conceptualization, Supervision, Validation, Visualization, Writing – review & editing. SH: Conceptualization, Supervision, Validation, Writing – review & editing. PH: Conceptualization, Supervision, Validation, Writing – review & editing. VH: Conceptualization, Supervision, Validation, Writing – review & editing. LK: Conceptualization, Investigation, Methodology, Writing – review & editing. SL: Conceptualization, Investigation, Supervision, Writing – review & editing. SM: Conceptualization, Methodology, Supervision, Writing – review & editing. MM: Conceptualization, Methodology, Supervision, Writing – review & editing. RM: Conceptualization, Supervision, Validation, Writing – review & editing. JM: Conceptualization, Investigation, Supervision, Writing – review & editing. SN: Conceptualization, Investigation, Methodology, Writing – review & editing. RP: Conceptualization, Resources, Supervision, Writing – review & editing. DP: Conceptualization, Resources, Supervision, Writing – review & editing. DR: Conceptualization, Resources, Supervision, Writing – review & editing. GS: Conceptualization, Resources, Supervision, Writing – review & editing. PS: Conceptualization, Resources, Supervision, Writing – review & editing. MK: Conceptualization, Investigation, Resources, Writing – review & editing. MV: Conceptualization, Resources, Supervision, Writing – review & editing. UW: Conceptualization, Resources, Supervision, Writing – review & editing. LZ: Conceptualization, Resources, Supervision, Writing – review & editing. PG: Conceptualization, Investigation, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. EUFOREA received an unrestricted grant by Lilly for the organization of the physical consensus meeting.
Acknowledgments
To the EUFOREA management team for their kind help in making this consensus meeting possible.
Conflict of interest
GKS: Honoraria for articles, speaker and advisory boards: ALK, Bayer, Chiesi, GlaxoSmithKline, Haleon, Noucor, Sanofi- Regeneron, and Viatris. Chair of BSACI rhinitis guidelines, Scientific Chief Editor, Rhinology Section of Frontiers in Allergy, Vice President and AR lead for EUFOREA, and Chair/ member Data Monitoring Committees on SLIT for ALK. DMC: Serves as Academic Manager at the European Forum for Research and Education in Allergy and Airway Diseases (EUFOREA) and as Review Editor at Frontiers in Allergy, Rhinology Section. SS: Serves as the Patient Education Manager at the European Forum for Research and Education in Allergy and Airway Diseases (EUFOREA). VB: Has received research grants, participated in advisory boards, and developed pharmaceutical studies for GSK, AstraZeneca, Sanofi, Regeneron, Novartis, MSD, Pharmaxis, ALK Abello, Birk NPC, Chiesi and Menarini. MB: Consultation and Advisory Boards: GSK, TerSera Pharma. Bryn Pharma, Soundhealth, Prollergy, and ALK. Speakers Bureau: AstraZeneca, Sanofi, Regeneron, and ALK. AKE: has participated in advisory boards for Abbvie, ALK-Abelló, AstraZeneca, Bausch Health, Circassia Ltd, laxoSmithKline, LEO Pharma, Johnson & Johnson, Merck, Miravo, Mylan, Novartis, Pediapharm and Pfizer, has been a speaker for ALK, Aralez, AstraZeneca, Bausch Health, Boehringer-Ingelheim, CACME, Meda, Medexus, Mylan, Merck, Novartis, Pfizer, The ACADEMY, and Takeda. Her institution has received research grants from AstraZeneca, Bayer, LLC, Circassia Ltd, Green Cross Pharmaceuticals, GlaxoSmithKline, Sun Pharma, Merck, Novartis, Pfizer, Regeneron and Sanofi. She has also served as an independent consultant to Allergy Therapeutics, Bayer, LLC, Ora Inc., and Regeneron in the past. WF: The department of Otorhino. SN: speaker and advisory boards for ALK and Astra Zeneca.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AIT, allergen immunotherapy; AR, allergic rhinitis; ARIA, allergic rhinitis and its impact on asthma; BSACI, British society for allergy and immunology; CRSwNP, chronic rhinosinusitis with masal polyps; EUFOREA, European forum for research and education in allergy and airway diseases; GRADE, grading of recommendations-assessment, development and evaluation; QoL, quality of life; RCAT, rhinitis control assessment test; RQLQ, rhinoconjunctivitis quality of life questionnaire; R-SARC, severe refractory allergic rhinoconjunctivitis; SARC, severe allergic rhinoconjunctivitis; TT, treatable traits; VAS, visual analogue scale; WHO, world health organization.
References
1. Scadding G, Bousquet J, Bachert C, Fokkens WJ, Hellings PW, Prokopakis E, et al. Rhinology future trends: 2017 EUFOREA debate on allergic rhinitis. Rhinol J. (2019) 57(1):49–56. doi: 10.4193/Rhin18.076
2. Scadding GK, Smith PK, Blaiss M, Roberts G, Hellings PW, Gevaert P, et al. Allergic rhinitis in childhood and the new EUFOREA algorithm. Front Allergy. (2021) 2:706589. doi: 10.3389/falgy.2021.706589
3. Hellings PW, Scadding G, Bachert C, Bjermer L, Canonica GW, Cardell LO, et al. Effect of the tongue-in-groove technique on the smile form. Rhinol J. (2020) 58(6):626–28. doi: 10.4193/Rhin20.246
4. Hellings PW, Akdis CA, Bachert C, Bousquet J, Pugin B, Adriaensen G, et al. EUFOREA rhinology research forum 2016: report of the brainstorming sessions on needs and priorities in rhinitis and rhinosinusitis. Rhinol J. (2017) 55(3):202–10. doi: 10.4193/Rhin17.028
5. Scheire S, Germonpré S, Mehuys E, Van Tongelen I, De Sutter A, Steurbaut S, et al. Rhinitis control and medication use in a real-world sample of patients with persistent rhinitis or rhinosinusitis: a community pharmacy study. J Allergy Clin Immunol Pract. (2024) 12(7):1865–1876.e6. doi: 10.1016/j.jaip.2024.04.031
6. Klimek L, Mullol J, Ellis AK, Izquierdo-Domínguez A, Hagemann J, Casper I, et al. Current management of allergic rhinitis. J Allergy Clin Immunol Pract. (2024) 12(6):1399–412. doi: 10.1016/j.jaip.2024.03.023
7. Bousquet J, Schünemann HJ, Sousa-Pinto B, Zuberbier T, Togias A, Samolinski B, et al. Concepts for the development of person-centred, digitally-enabled, artificial intelligence-assisted ARIA care pathways (ARIA 2024). J Allergy Clin Immunol Pract: (2024) 12(24):2648–68. doi: 10.1016/j.jaip.2024.06.040
8. Scadding GK, McDonald M, Backer V, Scadding G, Bernal-Sprekelsen M, Conti DM, et al. Pre-asthma: a useful concept for prevention and disease-modification? a EUFOREA paper. part 1—allergic asthma. Front Allergy. (2024) 4:1291185. doi: 10.3389/falgy.2023.1291185
9. Scadding GK, Gray C, Conti DM, McDonald M, Backer V, Scadding G, et al. Pre-asthma: a useful concept? a EUFOREA paper. part 2—late onset eosinophilic asthma. Front Allergy. (2024) 5:1404735. doi: 10.3389/falgy.2024.1404735
10. Diamant Z, Jesenak M, Hanania NA, Heaney LG, Djukanovic R, Ryan D, et al. EUFOREA pocket guide on the diagnosis and management of asthma: an educational and practical tool for general practitioners, non-respiratory physicians, paramedics and patients. Respir Med. (2023) 218:107361. doi: 10.1016/j.rmed.2023.107361
11. Hellings PW, Lau S, Scadding GK, Bjermer L, Backer V, Chaker AM, et al. EUFOREA summit in Brussels (2023): inspiring the future of allergy & respiratory care. Front Allergy. (2023) 4:1236977. doi: 10.3389/falgy.2023.1236977
12. Conti DM, Vibeke B, Kirsten B, Leif B, Adam C, Stephanie D, et al. EUFOREUM Berlin 2023: optimizing care for type 2 inflammatory diseases from clinic to AI: a pediatric focus. Pediatr Allergy Immunol. (2024) 35:e14183. doi: 10.1111/pai.14183
13. Fokkens WJ, De Corso E, Backer V, Bernal-Sprekelsen M, Bjermer L, von Buchwald C, et al. EPOS2020/EUFOREA expert opinion on defining disease states and therapeutic goals in CRSwNP. Rhinol J. (2024) 62(3):287–98. doi: 10.4193/Rhin23.415
14. Bousquet J, Van Cauwenberge P, Khaltaev N, Aria Workshop Group, World Health Organization. Allergic rhinitis and its impact on asthma. J Allergy Clin Immunol. (2001) 108(5 Suppl):S147–334. doi: 10.1067/mai.2001.118891
15. Bousquet J, Toumi M, Sousa-Pinto B, Anto JM, Bedbrook A, Czarlewski W, et al. The allergic rhinitis and its impact on asthma (ARIA) approach of value-added medicines: as-needed treatment in allergic rhinitis. J Allergy Clin Immunol Pract. (2022) 10(11):2878–88. doi: 10.1016/j.jaip.2022.07.020
16. Bousquet J, Schünemann HJ, Togias A, Bachert C, Erhola M, Hellings PW, et al. Next-generation allergic rhinitis and its impact on asthma (ARIA) guidelines for allergic rhinitis based on grading of recommendations assessment, development and evaluation (GRADE) and real-world evidence. J Allergy Clin Immunol. (2020) 145(1):70–80.e3. doi: 10.1016/j.jaci.2019.06.049 Erratum in: J Allergy Clin Immunol. 2022 Jun;149(6):2180. doi: 10.1016/j.jaci.2022.04.016.31627910
17. Bousquet J, Devillier P, Arnavielhe S, Bedbrook A, Alexis-Alexandre G, van Eerd M, et al. Treatment of allergic rhinitis using mobile technology with real-world data: the MASK observational pilot study. Allergy. (2018) 73(9):1763–74. doi: 10.1111/all.13406
18. Scadding GK, Kariyawasam HH, Scadding G, Mirakian R, Buckley RJ, Dixon T, et al. BSACI guideline for the diagnosis and management of allergic and non-allergic rhinitis (revised edition 2017; first edition 2007). Clin Exp Allergy. (2017) 47(7):856–89. doi: 10.1111/cea.12953
19. Price DB, Scadding G, Bachert C, Saleh H, Nasser S, Carter V, et al. UK prescribing practices as proxy markers of unmet need in allergic rhinitis: a retrospective observational study. NPJ Prim Care Resp Med. (2016) 26:16033. doi: 10.1038/npjpcrm.2016.33
20. Bousquet J, Bachert C, Canonica GW, Casale TB, Cruz AA, Lockey RJ, et al. Unmet needs in severe chronic upper airway disease (SCUAD). J Allergy Clin Immunol. (2009) 124(3):428–33. doi: 10.1016/j.jaci.2009.06.027
21. Van Bulck P, Cools L, Soumya MS, Nyembue DT, Kabobo P, Zhang L, et al. A multicenter real-life study on the multiple reasons for uncontrolled allergic rhinitis. Int Forum Allergy Rhinol. (2021) 11(10):1452–60. doi: 10.1002/alr.22808
22. Church MK, Church DS. Pharmacology of antihistamines. Indian J Dermatol. (2013) 58(3):219–24. doi: 10.4103/0019-5154.110832
23. Kim JH, Cha HR, Ha EK, Kwak JH, Kim H, Shin J, et al. Association between first-generation antihistamine use in children and cardiac arrhythmia and ischemic heart disease: a case-crossover study. Pharmaceuticals. (2023) 16(8):1073. doi: 10.3390/ph16081073
24. Fitzsimons R, van der Poel LA, Thornhill W, du Toit G, Shah N, Brough HA. Antihistamine use in children. Arch Dis Child Educ Pract Ed. (2015) 100(3):122–31. doi: 10.1136/archdischild-2013-304446
25. Casale TB, Blaiss MS, Gelfand E, Gilmore T, Harvey PD, Hindmarch I, et al. First do no harm: managing antihistamine impairment in patients with allergic rhinitis. J Allergy Clin Immunol. (2003) 111(5):S835–42. doi: 10.1067/mai.2003.1550
26. Bridgeman MB. Overcoming barriers to intranasal corticosteroid use in patients with uncontrolled allergic rhinitis. Integr Pharm Res Pract. (2017) 6:109–19. doi: 10.2147/IPRP.S129544
27. Pugin B, Deneyer L, Bachert C, Alobid I, Bousquet J, De Carlo G, et al. Patient advisory board for chronic rhinosinusitis—a EUFOREA initiative. Rhinol J. (2019) 57(5):331–5. doi: 10.4193/Rhin19.012
28. De Prins L, Raap U, Mueller T, Schmid-Grendelmeier P, Haase CH, Backer V, et al. White paper on European patient needs and suggestions on chronic type 2 inflammation of airways and skin by EUFOREA. Front Allergy. (2022) 3:889221. doi: 10.3389/falgy.2022.889221
29. Claeys N, Teeling MT, Legrand P, Poppe M, Verschueren P, De Prins L, et al. Patients unmet needs in chronic rhinosinusitis with nasal polyps care: a patient advisory board statement of EUFOREA. Front Allergy. (2021) 2:761388. doi: 10.3389/falgy.2021.761388
30. Scadding GK. Inadequate rhinitis control in real life-what to do? J Allergy Clin Immunol Pract. (2024) 12(7):1877–8. doi: 10.1016/j.jaip.2024.05.009
31. Vieira RJ, Azevedo LF, Pereira AM, Nogueira-Leite D, Rocha Gonçalves FN, Larenas-Linnemann DE, et al. Impact of allergic rhinitis control on work productivity and costs: a real-world data MASK-air study. J Allergy Clin Immunol Pract. (2024) 12(11):3107–15. doi: 10.1016/j.jaip.2024.07.026
32. Larenas-Linnemann DES, Domthong P, Di Francesco RC, González-Pérez R, Verma M. General practitioner and patient perspectives on intranasal corticosteroids for allergic rhinitis: treatment duration and obstacles to adherence, findings from a recent survey. World Allergy Organ J. (2024) 17(7):100925. doi: 10.1016/j.waojou.2024.100925
33. Hellings PW, Borrelli D, Pietikainen S, Agache I, Akdis C, Bachert C, et al. European summit on the prevention and self-management of chronic respiratory diseases: report of the European union parliament summit (29 march 2017). Clin Transl Allergy. (2017) 7:49. doi: 10.1186/s13601-017-0186-3
34. Hellings PW, Fokkens WJ, Bachert C, Akdis CA, Bieber T, Agache I, et al. Positioning the principles of precision medicine in care pathways for allergic rhinitis and chronic rhinosinusitis—a EUFOREA-ARIA-EPOS-AIRWAYS ICP statement. Allergy. (2017) 72(9):1297–305. doi: 10.1111/all.13162
35. Valero A, Ferrer M, Baró E, Sastre J, Navarro AM, Martí-Guadaño E, et al. Discrimination between moderate and severe disease may be used in patients with either treated or untreated allergic rhinitis. Allergy. (2010) 65(12):1609–13. doi: 10.1111/j.1398-9995.2010.02410.x
36. Montoro J, Del Cuvillo A, Mullol J, Molina X, Bartra J, Dávila I, et al. Validation of the modified allergic rhinitis and its impact on asthma (ARIA) severity classification in allergic rhinitis children: the PEDRIAL study. Allergy. (2012) 67(11):1437–42. doi: 10.1111/all.12011
37. Del Cuvillo A, Santos V, Montoro J, Bartra J, Davila I, Ferrer M, et al. Allergic rhinitis severity can be assessed using a visual analogue scale in mild, moderate and severe. Rhinol J. (2017) 55(1):34–8. doi: 10.4193/Rhin16.025
38. Sánchez-Hernández MC, Navarro AM, Colás C, Del Cuvillo A, Sastre J, Mullol J, et al. Validation of the DECA criteria for allergic conjunctivitis severity and control. Clin Transl Allergy. (2020) 10:43. doi: 10.1186/s13601-020-00349-4
39. Mullol J, Bartra J, del Cuvillo A, Izquierdo I, Muñoz-Cano R, Valero A. Specialist-based treatment reduces the severity of allergic rhinitis. Clin Exp Allergy. (2013) 43(7):723–9. doi: 10.1111/cea.12081
40. Hellings PW, Pugin B, Mariën G, Bachert C, Breynaert C, Bullens DM, et al. Stepwise approach towards adoption of allergen immunotherapy for allergic rhinitis and asthma patients in daily practice in Belgium: a BelSACI-Abeforcal-EUFOREA statement. Clin Transl Allergy. (2019) 9:1. doi: 10.1186/s13601-019-0243-1
41. Cingi C, Gevaert P, Mösges R, Rondon C, Hox V, Rudenko M, et al. Multi-morbidities of allergic rhinitis in adults: European academy of allergy and clinical immunology task force report. Clin Transl Allergy. (2017) 7:17. doi: 10.1186/s13601-017-0153-z
42. Shaaban R, Zureik M, Soussan D, Neukirch C, Heinrich J, Sunyer J, et al. Rhinitis and onset of asthma: a longitudinal population-based study. Lancet. (2008) 372(9643):1049–57. doi: 10.1016/S0140-6736(08)61446-4
43. Hamelmann E, Hammerby E, Scharling KS, Pedersen M, Okkels A, Schmitt J. Quantifying the benefits of early sublingual allergen immunotherapy tablet initiation in children. Allergy. (2024) 79(4):1018–27. doi: 10.1111/all.15985
44. Atanasio A, Orengo JM, Sleeman MA, Stahl N. Biologics as novel therapeutics for the treatment of allergy: challenges and opportunities. Front Allergy. (2022) 3:1019255. doi: 10.3389/falgy.2022.1019255
45. Gevaert P, Wong K, Millette LA, Carr TF. The role of IgE in upper and lower airway disease: more than just allergy!. Clin Rev Allergy Immunol. (2022) 62(1):200–15. doi: 10.1007/s12016-021-08901-1
46. Weinstein SF, Katial R, Jayawardena S, Pirozzi G, Staudinger H, Eckert L, et al. Efficacy and safety of dupilumab in perennial allergic rhinitis and comorbid asthma. J Allergy Clin Immunol. (2018) 142(1):171–177.e1. doi: 10.1016/j.jaci.2017.11.051
47. Okubo K, Okano M, Sato N, Tamaki Y, Suzuki H, Uddin A, et al. Add-on omalizumab for inadequately controlled severe pollinosis despite standard-of-care: a randomized study. J Allergy Clin Immunol Pract. (2020) 8(9):3130–3140.e2. doi: 10.1016/j.jaip.2020.04.068
48. Bayar Muluk N, Cingi C. Biologics in allergic rhinitis. Eur Rev Med Pharmacol Sci. (2023) 27(5 Suppl):43–52. doi: 10.26355/eurrev_202310_34069
49. Geng B, Dilley M, Anterasian C. Biologic therapies for allergic rhinitis and nasal polyposis. Curr Allergy Asthma Rep. (2021) 21(6):36. doi: 10.1007/s11882-021-01013-y
50. Sharma K, Akre S, Chakole S, Wanjari MB. Allergic rhinitis and treatment modalities: a review of literature. Cureus. (2022) 14(8):e28501. doi: 10.7759/cureus.28501
51. Hoyte FCL, Nelson HS. Recent advances in allergic rhinitis. F1000Research. (2018) 7:1333. doi: 10.12688/f1000research.15367.1
52. Klimek L, Bergmann KC, Biedermann T, Bousquet J, Hellings P, Jung K, et al. Visual analogue scales (VAS): measuring instruments for the documentation of symptoms and therapy monitoring in cases of allergic rhinitis in everyday health care: position paper of the German society of allergology (AeDA) and the German society of allergy and clinical immunology (DGAKI), ENT section, in collaboration with the working group on clinical immunology, allergology and environmental medicine of the German society of otorhinolaryngology, head and neck surgery (DGHNOKHC). Allergo J Int. (2017) 26(1):16–24. doi: 10.1007/s40629-016-0006-7
53. Caimmi D, Baiz N, Tanno LK, Demoly P, Arnavielhe S, Murray R, et al. Validation of the MASK-rhinitis visual analogue scale on smartphone screens to assess allergic rhinitis control. Clin Exp Allergy. (2017) 47(12):1526–33. doi: 10.1111/cea.13025
54. Larenas-Linnemann DE, Mayorga-Butrón JL, Maza-Solano J, Emelyanov AV, Dolci RL, Miyake MM, et al. Global expert views on the diagnosis, classification and pharmacotherapy of allergic rhinitis in clinical practice using a modified Delphi panel technique. World Allergy Organ J. (2023) 16(7):100800. doi: 10.1016/j.waojou.2023.100800
55. Heldin J, Malinovschi A, Johannessen A, Alving K, Holm M, Franklin KA, et al. Clinical remission of asthma and allergic rhinitis—in a longitudinal population study. J Asthma Allergy. (2022) 15:1569–78. doi: 10.2147/JAA.S378584
56. Thomas D, McDonald VM, Pavord ID, Gibson PG. Asthma remission: what is it and how can it be achieved? Eur Respir J. (2022) 60(5):2102583. doi: 10.1183/13993003.02583-2021
57. Wise SK, Lin SY, Toskala E, Orlandi RR, Akdis CA, Alt JA, et al. International consensus statement on allergy and rhinology: allergic rhinitis. Int Forum Allergy Rhinol. (2018) 8(2):108–352. doi: 10.1002/alr.22073
58. Wise SK, Damask C, Roland LT, Ebert C, Levy JM, Lin S, et al. International consensus statement on allergy and rhinology: allergic rhinitis—2023. Int Forum Allergy Rhinol. (2023) 13(4):293–859. doi: 10.1002/alr.23090
59. Gani F, Lombardi C, Barrocu L, Landi M, Ridolo E, Bugiani M, et al. The control of allergic rhinitis in real life: a multicenter cross-sectional Italian study. Clin Mol Allergy. (2018) 16:4. doi: 10.1186/s12948-018-0082-y
60. Demoly P, Bousquet PJ, Mesbah K, Bousquet J, Devillier P. Visual analogue scale in patients treated for allergic rhinitis: an observational prospective study in primary care: asthma and rhinitis. Clin Exp Allergy. (2013) 43(8):881–8. doi: 10.1111/cea.12121
61. Bousquet PJ, Combescure C, Klossek JM, Daurès JP, Bousquet J. Change in visual analog scale score in a pragmatic randomized cluster trial of allergic rhinitis. J Allergy Clin Immunol. (2009) 123(6):1349–54. doi: 10.1016/j.jaci.2009.02.033
62. Iordache A, Balica NC, Horhat ID, Morar R, Tischer AA, Milcu AI, et al. A review regarding the connections between allergic rhinitis and asthma—epidemiology, diagnosis and treatment. Curr Health Sci J. (2023) 49(1):5–18. doi: 10.12865/CHSJ.49.01.5
63. Miao P, Jiang Y, Jian Y, Shi J, Liu Y, Piewngam P, et al. Exacerbation of allergic rhinitis by the commensal bacterium streptococcus salivarius. Nat Microbiol. (2023) 8(2):218–30. doi: 10.1038/s41564-022-01301-x
64. Li CH, Sayeau K, Ellis AK. Air pollution and allergic rhinitis: role in symptom exacerbation and strategies for management. J Asthma Allergy. (2020) 13:285–92. doi: 10.2147/JAA.S237758
65. Yii ACA, Tay TR, Choo XN, Koh MSY, Tee AKH, Wang DY. Precision medicine in united airways disease: a “treatable traits” approach. Allergy. (2018) 73(10):1964–78. doi: 10.1111/all.13496
66. Chung KF, Adcock IM. Precision medicine for the discovery of treatable mechanisms in severe asthma. Allergy. (2019) 74(9):1649–59. doi: 10.1111/all.13771
67. Lin T, Pham J, Denton E, Lee J, Hore-Lacy F, Sverrild A, et al. Trait profiles in difficult-to-treat asthma: clinical impact and response to systematic assessment. Allergy. (2023) 78(9):2418–27. doi: 10.1111/all.15719
68. McDonald VM, Gibson PG. Treatable traits in asthma: moving beyond diagnostic labels. Med J Aust. (2022) 216(7):331–3. doi: 10.5694/mja2.51464
69. McDonald VM, Gibson PG. Treatable traits in asthma and COPD. Arch Bronconeumol. (2022) 58(8):583–5. doi: 10.1016/j.arbres.2021.07.003
70. Wang J, Zhou Y, Zhang H, Hu L, Liu J, Wang L, et al. Pathogenesis of allergic diseases and implications for therapeutic interventions. Sig Transduct Target Ther. (2023) 8:138. doi: 10.1038/s41392-023-01344-4
71. Kang J, Lee G, Son M, Kim Y, Heo N, Lee D. Effects and safety of intranasal phototherapy for allergic rhinitis: study protocol for a single-center, randomized, parallel (acupuncture-controlled), open-label, investigator-initiated, pilot study. Medicine. (2020) 99(30):e21183. doi: 10.1097/MD.0000000000021183
72. Mariño-Sanchez F, Valls-Mateus M, Haag O, Alobid I, Bousquet J, Mullol J. Smell loss is associated with severe and uncontrolled disease in children and adolescents with persistent allergic rhinitis. J Allergy Clin Immunol Pract. (2018) 6(5):1752–1755.e3. doi: 10.1016/j.jaip.2017.12.031
73. Guilemany JM, Angrill J, Alobid I, Centellas S, Pujols L, Bartra J, et al. United airways again: high prevalence of rhinosinusitis and nasal polyps in bronchiectasis. Allergy. (2009) 64(5):790–7. doi: 10.1111/j.1398-9995.2008.01892.x
74. Drazdauskaitė G, Layhadi JA, Shamji MH. Mechanisms of allergen immunotherapy in allergic rhinitis. Curr Allergy Asthma Rep. (2021) 21(1):2. doi: 10.1007/s11882-020-00977-7
75. Arshad H, Lack G, Durham SR, Penagos M, Larenas-Linnemann D, Halken S. Prevention is better than cure: impact of allergen immunotherapy on the progression of airway disease. J Allergy Clin Immunol Pract. (2024) 12(1):45–56. doi: 10.1016/j.jaip.2023.10.013
76. Durham SR, Shamji MH. Allergen immunotherapy: past, present and future. Nat Rev Immunol. (2023) 23(5):317–28. doi: 10.1038/s41577-022-00786-1
77. Juniper EF, Guyatt GH. Development and testing of a new measure of health status for clinical trials in rhinoconjunctivitis. Clin Exp Allergy. (1991) 21(1):77–83. doi: 10.1111/j.1365-2222.1991.tb00807.x
78. Juniper EF, Guyatt GH, Griffith LE, Ferrie PJ. Interpretation of rhinoconjunctivitis quality of life questionnaire data. J Allergy Clin Immunol. (1996) 98(4):843–5. doi: 10.1016/S0091-6749(96)70135-5
79. Meltzer EO, Schatz M, Nathan R, Garris C, Stanford RH, Kosinski M. Reliability, validity, and responsiveness of the rhinitis control assessment test in patients with rhinitis. J Allergy Clin Immunol. (2013) 131(2):379–86. doi: 10.1016/j.jaci.2012.10.022
80. Klimek L, Casper I, Bergmann KC, et al. Therapy of allergic rhinitis in routine care: evidence-based benefit assessment of freely combined use of various active ingredients. Allergo J Int. (2020) 29:129–38. doi: 10.1007/s40629-020-00133-7
81. Abdullah B, Abdul Latiff AH, Manuel AM, Mohamed Jamli F, Dalip Singh HS, Ismail IH, et al. Pharmacological management of allergic rhinitis: a consensus statement from the Malaysian society of allergy and immunology. J Asthma Allergy. (2022) 15:983–1003. doi: 10.2147/JAA.S374346
82. Ryan D, Price D, Musgrave SD, Malhotra S, Lee AJ, Ayansina D, et al. Clinical and cost effectiveness of mobile phone supported self monitoring of asthma: multicentre randomised controlled trial. Br Med J. (2012) 344:e1756. doi: 10.1136/bmj.e1756
83. Smolinska S, Popescu FD, Izquierdo E, Antolín-Amérigo D, Price OJ, Alvarez-Perea A, et al. Telemedicine with special focus on allergic diseases and asthma-Status 2022: an EAACI position paper. Allergy. (2024) 79(4):777–92. doi: 10.1111/all.15964
84. Liva GA, Karatzanis AD, Prokopakis EP. Review of rhinitis: classification, types, pathophysiology. J Clin Med. (2021) 10(14):3183. doi: 10.3390/jcm10143183
85. Nur Husna SM, Tan HT, Md Shukri N, Mohd Ashari NS, Wong KK. Allergic rhinitis: a clinical and pathophysiological overview. Front Med (Lausanne). (2022) 9:874114. doi: 10.3389/fmed.2022.874114
86. Fritzsching B, Contoli M, Porsbjerg C, Buchs S, Larsen JR, Elliott L, et al. Long-term real-world effectiveness of allergy immunotherapy in patients with allergic rhinitis and asthma: results from the REACT study, a retrospective cohort study. Lancet Reg Health Eur. (2022) 13:100275. doi: 10.1016/j.lanepe.2021.100275
87. Bousquet J, Pham-Thi N, Bedbrook A, Agache I, Annesi-Maesano I, et al. Next-generation care pathways for allergic rhinitis and asthma multimorbidity: a model for multimorbid non-communicable diseases-meeting report (part 2). J Thorac Dis. (2019) 11(9):4072–84. doi: 10.21037/jtd.2019.09.38
88. Pfaar O, Bousquet J, Durham SR, Kleine-Tebbe J, Larché M, Roberts G, et al. One hundred and ten years of allergen immunotherapy: a journey from empiric observation to evidence. Allergy. (2022) 77(2):454–68. doi: 10.1111/all.15023
89. Brożek JL, Bousquet J, Agache I, Agarwal A, Bachert C, Bosnic-Anticevich S, et al. Allergic rhinitis and its impact on asthma (ARIA) guidelines-2016 revision. J Allergy Clin Immunol. (2017) 140(4):950–8. doi: 10.1016/j.jaci.2017.03.050
90. Krzych-Fałta E, Lisiecka-Biełanowicz M, Furmańczyk K, Dziewa-Dawidczyk D, Stróżek J, Wojas O, et al. Prevention of perennial allergic rhinitis in the conception of coordinated healthcare in Poland. Arch Med Sci. (2021) 18(6):1475–87. doi: 10.5114/aoms/110155
91. Grabenhenrich LB, Keil T, Reich A, Gough H, Beschorner J, Hoffmann U, et al. Prediction and prevention of allergic rhinitis: a birth cohort study of 20 years. J Allergy Clin Immunol. (2015) 136(4):932–40.e12. doi: 10.1016/j.jaci.2015.03.040
Keywords: allergic rhinitis, quality of life, definitions, severe allergic rhinoconjunctivitis (SARC), refractory severe allergic rhinoconjunctivitis (R-SARC), biologics, allergen immunotherapy (AIT), control
Citation: Scadding GK, Conti DM, Scheire S, Backer V, Blaiss M, Cardell LO, De Yun W, Ellis AK, Fokkens W, Fox AT, Gilbert Kruz T, Halken S, Hellings PW, Hox V, Kalogjera L, Lau S, Marinho S, McDonald M, Mösges R, Mullol J, Nasser S, Pawankar R, Price D, Ryan D, Scadding G, Smith P, Sosa Kostrábová M, Vazquez-Ortiz M, Wahn U, Zhang L and Gevaert P (2025) EUFOREA meeting on defining disease states in allergic rhinitis: towards a unified language in AR. Front. Allergy 5:1531788. doi: 10.3389/falgy.2024.1531788
Received: 20 November 2024; Accepted: 30 December 2024;
Published: 3 February 2025.
Edited by:
Iordanis Konstantinidis, Aristotle University of Thessaloniki, GreeceReviewed by:
Kachorn Seresirikachorn, Chulalongkorn University, ThailandVicky Kritikos, Woolcock Institute of Medical Research, Australia
Copyright: © 2025 Scadding, Conti, Scheire, Backer, Blaiss, Cardell, De Yun, Ellis, Fokkens, Fox, Gilbert Kruz, Halken, Hellings, Hox, Kalogjera, Lau, Marinho, McDonald, Mösges, Mullol, Nasser, Pawankar, Price, Ryan, Scadding, Smith, Sosa Kostrábová, Vazquez-Ortiz, Wahn, Zhang and Gevaert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: G. K. Scadding, Zy5zY2FkZGluZ0B1Y2wuYWMudWs=
†ORCID:
G. K. Scadding
orcid.org/0000-0002-0732-9728
D. M. Conti
orcid.org/0000-0002-8896-495X
S. Scheire
orcid.org/0000-0001-9623-4458
V. Backer
orcid.org/0000-0002-7806-7219
M. Blaiss
orcid.org/0000-0002-0733-9408
L. O. Cardell
orcid.org/0000-0003-0538-9580
W. De Yun
orcid.org/0000-0002-0909-2963
A. K. Ellis
orcid.org/0000-0002-0725-2353
W. Fokkens
orcid.org/0000-0003-4852-229X
A. T. Fox
orcid.org/0000-0002-3533-9798
S. Halken
orcid.org/0000-0003-0161-8278
P. W. Hellings
orcid.org/0000-0001-6898-688X
V. Hox
orcid.org/0000-0003-2390-294X
S. Lau
orcid.org/0000-0002-5189-4265
S. Marinho
orcid.org/0000-0003-3069-6187
M. McDonald
orcid.org/0000-0002-5348-3849
J. Mullol
orcid.org/0000-0003-3463-5007
S. Nasser
orcid.org/0000-0002-9924-4616
R. Pawankar
orcid.org/0000-0002-3091-7237
D. Price
orcid.org/0000-0002-9728-9992
D. Ryan
orcid.org/0000-0002-4115-7376
P. Smith
orcid.org/0000-0002-2629-8963
L. Zhang
orcid.org/0000-0002-0910-9884
P. Gevaert
orcid.org/0000-0002-1629-8468