 Abraham Alí-Munive1
Abraham Alí-Munive1 Josefina Zakzuk2,3*
Josefina Zakzuk2,3* Nelson J. Alvis-Zakzuk3,4
Nelson J. Alvis-Zakzuk3,4 Elizabeth García5,6Claudia Diaz Bossa7
Elizabeth García5,6Claudia Diaz Bossa7 Diana Jimena Cano Rosales8,9Fabio Bolívar8Alejandro Carreño10Paula Rodríguez-Ordoñez11Natalia Gómez-Ardila12Gabriel Patiño13Sergio Londoño11
Diana Jimena Cano Rosales8,9Fabio Bolívar8Alejandro Carreño10Paula Rodríguez-Ordoñez11Natalia Gómez-Ardila12Gabriel Patiño13Sergio Londoño11 Carlos A. Torres-Duque1
Carlos A. Torres-Duque1
- 1Asmaire ReXpira Program, Fundación Neumológica Colombiana, Bogotá, Colombia
- 2Institute for Immunological Research, University of Cartagena, Cartagena, Bolívar, Colombia
- 3ALZAK Research Group, ALZAK, Cartagena, Bolívar, Colombia
- 4Department of Health Sciences, Universidad de la Costa, Barranquilla, Colombia
- 5Allergy Unit, UNIMEQ-ORL, Bogotá, Colombia
- 6School of Medicine, Universidad de Los Andes, Bogotá, Colombia
- 7Research Department, NEUMOMED, Medellín, Antioquia, Colombia
- 8Asthma Program, Instituto Neumológico del Oriente, Bucaramanga, Colombia
- 9Department of Internal Medicine, Universidad Autónoma de Bucaramanga, Bucaramanga, Santander, Colombia
- 10Research Department, Centro de Alergología Alejandro Carreño, Barranquilla, Atlántico, Colombia
- 11Health Economics and Value Assessment, Sanofi, Bogotá, Colombia
- 12Medical Area, Sanofi, Bogotá, Colombia
- 13Market Access, Sanofi, Bogotá, Colombia
Background: Real-world effectiveness and safety of dupilumab for asthma treatment have been evaluated in USA and Europe, but research from Latin America is lacking. We aimed to describe the effectiveness of dupilumab in terms of changes in the annual rate of asthma exacerbations (AER) and their impact on lung function in Colombian patients.
Methods: Real-world, descriptive, and multi-centric (five clinical centers located in four different cities in Colombia) retrospective study that included patients aged ≥18 years with severe asthma, as defined by the GINA criteria. Data were collected from medical records of medical centers specialized in pulmonology or allergy care) spanning from 12 months before the prescription of dupilumab (baseline) to 25 months later. Follow-up data were categorized at various time points (2–4, 5–7, 8–10, 11–13, 14–18, and 19–25 months). Main outcomes were annual rates of asthma exacerbations (emergency visits or hospitalizations due to asthma), lung function measured through FEV1 and percent predicted FEV1 (FEV1pp), and Asthma Control Test (ACT) scores. Outcome rates were compared between baseline and follow-up data points. FeNO and absolute eosinophil counts throughout the observed period was also explored.
Results: A total of 98 patients were included. At baseline, the mean AER was 0.61 ± 1.45 per adult. Lower AER were observed after one (0.11 ± 0.54) or two-years (0.08 ± 0.20) of dupilumab treatment (p = 0.03). FEV1 measurements after one or two years of dupilumab treatment were significantly lower than baseline (p = 0.03). Mean change from baseline in FEV1 was 302.1 ± 481.97 ml (n = 19), 282.00 ± 231.99 ml (n = 10), and 248.18 ± 281.21 ml (n = 11) in the 2–4-, 11–13-, and 19–25-month follow-up periods, respectively. FEV1pp showed higher but not significant values from the 2–4-month period, with a median change of 12.5% (IQR: 0.3, 21.5). The proportion of patients with uncontrolled asthma (ACT ≤15) decreased from 68% at baseline to 19% and 20% at year-one and second year of treatment, respectively (p = 0.003). The proportion of patients reaching FeNO values below 25 ppb was lower after dupilumab treatment than in baseline (p < 0.0001). Of the total cohort (n = 99), 15 (15.2%) experienced an adverse event (AE). Three patients discontinued dupilumab permanently, and two discontinued dupilumab due to AEs.
Conclusions: Dupilumab is an effective and well-tolerated treatment for severe asthma in Colombia, resulting in reduced exacerbations and improved asthma control, lung function, and FeNO levels.
1 Introduction
Asthma remains one of the most prevalent chronic respiratory diseases worldwide, with a significant public health challenge, and persisting as a life-threatening condition (1, 2). While most individuals with asthma experience manageable symptoms, a subset, comprising approximately 5%–10%, faces severe manifestations, requiring high doses of inhaled corticosteroids (ICS) and long-acting beta-agonist (LABA), and episodically oral corticosteroids (OCS) (3, 4). This subset is classified as severe asthma (SA). SA is associated with a lower quality of life, greater risk of severe exacerbations and mortality, and increased healthcare costs (5, 6). According to the European Respiratory Society and the American Thoracic Society guidelines, SA is defined as “asthma which requires treatment with high-dose inhaled corticosteroids (ICS) plus a second controller medication and/or systemic corticosteroids to prevent it from becoming “uncontrolled” or which remains “uncontrolled” despite this therapy” (7). Conversely, GINA defines SA as a condition requiring high-intensity treatment to maintain good control, or a lack of good control despite high-intensity treatment (4).
Dupilumab, an antagonist of the alpha-chain interleukin (IL)-4 receptor, disrupts the IL-4 and IL-13 signaling pathways, key drivers of T helper 2 (Th2) inflammation observed in various allergic diseases, including asthma (8). The efficacy and safety of dupilumab for asthma treatment have been extensively evaluated in phase III randomized clinical trials (RCT) and subsequent analyses, yielding satisfactory results (9). This monoclonal antibody intervention significantly reduced asthma exacerbations and improved prebronchodilator forced expiratory volume in the first second (FEV1) in patients with uncontrolled moderate-to-severe asthma (9–12). However, there remains a gap in our understanding of the real-world (RW) effectiveness of dupilumab, particularly in populations not represented in RCTs, such as the Colombian population. RCTs provide robust evidence about the efficacy and safety of a treatment under ideal conditions, but they may not fully reflect responses in diverse populations. RW observational studies are crucial for providing complementary evidence on the practical efficacy and safety of interventions, addressing potential discrepancies between trial populations and RW patients. Most studies evaluating the effectiveness of dupilumab as a treatment option for SA have been done in Europe, US, and Japan (13–15). No studies in Latin-American populations have been published hitherto. In Colombia, where dupilumab has been utilized as an add-on therapy for SA since its approval in 2019, there is a lack of published data on its clinical effectiveness and local experience. Documenting and analyzing local experiences, has the potential to improve clinical practices and treatment guidelines for SA in Colombia and contribute to a more personalized and contextualized approach in the management of this chronic disease globally. Therefore, this study aimed to describe changes in asthma exacerbation, lung function, T2 inflammation biomarkers and other outcomes during a specific follow-up period in patients with SA treated with dupilumab in RW settings in Colombia.
2 Methods
2.1 Study design and population
This was a RW, descriptive, and multi-centric retrospective study involving five clinical centers located in four different cities in Colombia: Fundación Neumológica Colombiana and UNIMEQ ORL (Bogotá), Neumomed IPS (Medellín), Instituto Neumológico del Oriente (Bucaramanga), and Centro de Alergología Alejandro Carreño (Barranquilla). These medical centers are part of the private sector and receive mostly patients affiliated to the public health system of Colombia. These urban centers, representing different regions of the country (Andean, Pacific, and Caribbean), are characterized by diverse populations in terms of ethnicity and socioeconomic status. The majority of the population in these areas is covered by the national public health insurance system.
Eligible patients were identified from medical records at participating institutions between April 2019 and May 2023. We included patients aged 18 years or older receiving dupilumab, with a documented diagnosis of asthma (ICD-10: J45 or J46) in the medical record at least one year before the prescription of the biologic, receiving dupilumab therapy, and classified as having SA according to the GINA guidelines at least 1–2 months prior to initiating dupilumab (4).
Patient selection followed these criteria: (1) documentation of severe asthma and prescription of dupilumab; (2) confirmation of at least one additional medical control visit after the index date; (3) a final clinical control recorded at least six months after the index date; and (4) verification of a minimum of one year of baseline observation with a persistent diagnosis of asthma during that period.
We excluded patients with less than 6 months of observation after dupilumab prescription and/or with a co-diagnosis of chronic obstructive pulmonary disease (COPD) or other chronic respiratory diseases, such as bronchiectasis or tuberculosis, reported in the medical record at any time during the one-year observation period before dupilumab prescription. If, during the observation window, any center reported a patient who had discontinued dupilumab before completing six months of therapy for reasons unrelated to treatment failure, information on that case was retained for safety reporting, but clinical endpoints related to asthma control were not assessed.
2.2 Data collection and follow up definition
An electronic case report form (eCRF), developed in KoboToolbox, was used for data collection from medical records. Personal data were accessed once by designated research members; however, no data allowing patient identification were registered in the eCRF. Data consistency checks, outlier identification, and missing data handling were performed before analysis.
The day of dupilumab prescription was considered as the index date. This prescription date also represents the first time the patient receives the biologic. The baseline characteristics were assessed considering the 12-month period preceding the index date. All medical visits during dupilumab treatment were recorded with the same structured form. Clinical variables included: asthma control, lung function, healthcare resources utilization (HCRU) and medication prescriptions. Participating investigator physicians were invited to enter into the eCRF all clinical visits occurring after the initiation of the biologic therapy up to the latest permitted date. All recorded visits followed the same structured data capture format for entering outcomes and other reported variables of interest.
The follow-up period began on the index date and continued through the last available medical visit recorded for each patient. Follow-up duration varied across patients; however, the earliest possible date for entering the observation period was April 1, 2019, and the latest possible date for follow-up data was May 31, 2023.
2.3 Baseline characteristics
Demographic data collected at baseline included age, sex, socioeconomic stratum (Colombian classification from 1 to 6 based on dwelling characteristics and its surroundings), height, weight, department, working status, patient affiliation regime to social security (contributive/subsidized/special), educational level, and occupational status. The clinical variables analyzed included age at disease onset, comorbidities, and baseline pharmacotherapy, including biologic agents and immunotherapy. Asthma control metrics were evaluated using the Asthma Control Questionnaire-5 (ACQ-5) and Asthma Control Test (ACT). Quality of life was assessed using the Asthma Quality of Life Questionnaire (AQLQ). Other parameters included blood eosinophil count (BEC), fractional exhaled nitric oxide (FeNO) levels, pre-bronchodilator forced expiratory volume in one second (FEV1) values, and total immunoglobulin E (IgE) concentrations. Comorbidities were identified using ICD-10 codes documented in the medical records.
2.4 Outcomes
The main outcomes were asthma exacerbations, defined as an emergency room visit or hospitalization due to exacerbation, and lung function measured through FEV1 and the percent predicted FEV1 (FEV1pp).
The number of emergency room visits, and hospitalization and intensive care unit admissions due to asthma exacerbations are described as an information source for health care resource use (HCRU). Oral and inhaled corticosteroid use (dosage, frequency, and duration) were also described during the study period. Additionally, the study examined changes in asthma control using ACT scores. Presentation of common adverse events associated with dupilumab usage was reported.
Values of FeNO, total IgE values, BEC, and clinical asthma remission were explored when data were available. For FeNO, values below 25 ppb were interpreted as negative for airway inflammation. Clinical asthma remission was defined using three criteria for at least one year or in two follow-up time points separated by at least one year: 1) absence of exacerbations requiring oral corticosteroids or hospitalization, 2) an ACQ score ≤1.5 or an ACT score ≥20, and 3) an FEV1pp ≥80% or an improvement in FEV1 ≥ 100 ml.
2.5 Statistical analysis
Categorical variables were presented using absolute and relative frequency distributions. Numerical variables with a normal distribution were described using the mean and standard deviation (SD), while those not following a normal distribution were characterized using the median and interquartile range (IQR; first quartile—third quartile). Normality of the data was assessed using the Kolmogorov–Smirnov test.
Changes from baseline in lung function parameters, ACT and biologic markers (BEC and FeNO) were described at different follow-up time points (2–4, 5–7, 8–10, 11–13, 14–18, and 19–25 months) according to data availability for each patient. Due to structural characteristics of the Colombian healthcare system, delays in scheduling follow-up visits are common. Therefore, clinical assessments were grouped into standardized time-points (3, 6, 9, and 12 months), allowing a ± 1 month margin around each interval (e.g., the 3-month follow-up window included visits conducted between 2 and 4 months after treatment initiation). Post–12-month follow-up data were categorized into two descriptive intervals: 14–18 months and 19–25 months. In cases where temporary discontinuation of dupilumab longer than two months was detected, the analysis window was restricted to the date of the last prescription prior to interruption.
To obtain representative information on asthma control for each treatment year, we identified a single follow-up visit per patient corresponding to the end of the first year (T1 = 11–13 months) and the second year (T2 = 18–24 months) of treatment. These time points were selected to summarize the cumulative impact of dupilumab over each annual period. AER and mean FEV1 and FEV1 pp parameters were assessed at baseline, T1 and T2. AER represents the cumulative number of ER or hospitalization events recorded in each medical control during the first and second year of follow-up. Annualized rates were calculated as a ratio between the number of events and the number of months of follow-up and multiplied by 12. Comparisons of continuous variables across the three time points (baseline, T1, and T2) were performed using the Kruskal–Wallis test, due to the non-parametric distribution of the data. For categorical variables, such as the proportion of patients experiencing exacerbations, the chi-squared test was used. All statistical tests were two-sided, and a p-value < 0.05 was considered statistically significant. Statistical analyses were performed using R software (version 4.4.0 “Angel Food Cake”; R Foundation for Statistical Computing, Vienna, Austria).
3 Results
3.1 Baseline clinical and sociodemographic characteristics
Ninety-eight SA cases met the eligibility criteria for this study, including 6 or more months of using dupilumab. Table 1 shows descriptive sociodemographic features of the included cohort is (n = 98). The mean body mass index was 27.7 ± 5.0; 34 (39.5%) were overweight, and 23 (26.7%) were obese. The most common comorbidities were rhinosinusitis with nasal polyps (62.2%, n = 61) and allergic rhinitis (41.8%, n = 41). OCS were prescribed for disease control in 23.5% (n = 23) of patients. The mean treatment duration with dupilumab was 14.4 ± 7.1 months (Supplementary Table S1).
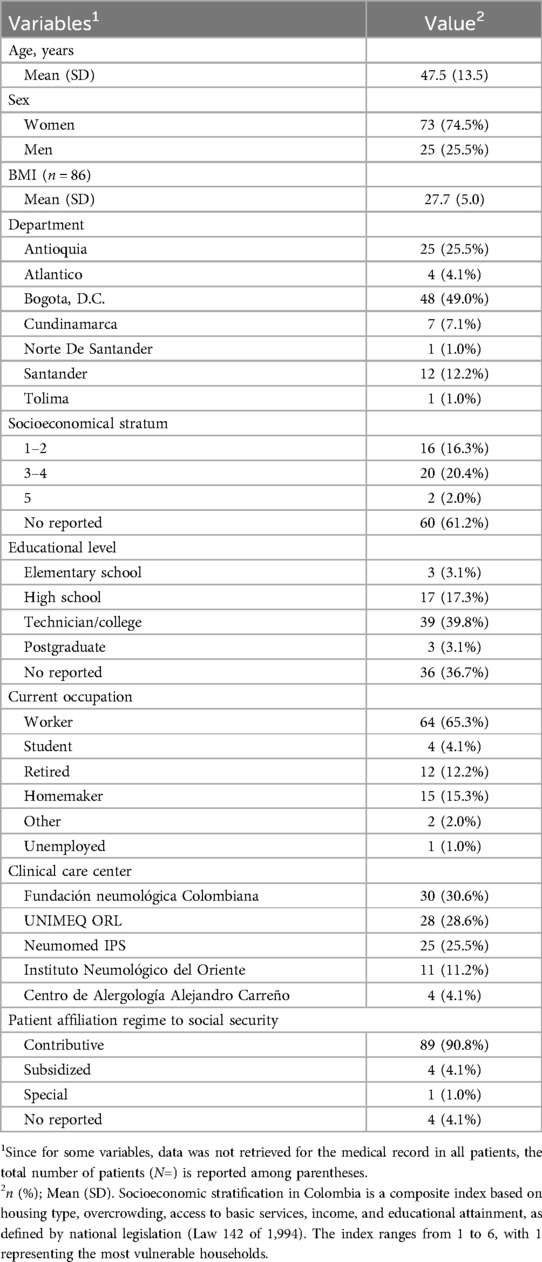
Table 1. Sociodemographic characteristics of the cohort (N = 98).
The clinical characteristics of patients are presented in Table 2. Twenty-four patients (24.5%) experienced at least one episode of severe exacerbation in the last year (Table 2); among this subgroup, the average number of exacerbations was 2.5 ± SD 1.98. Most patients (69.3%, n = 52) had uncontrolled asthma (ACT ≤15). Furthermore, pulmonary function tests indicate a mean FEV1 of 1,782.5 ± 740.6 ml and a median FeNO of 47.0 (IQR: 20.5, 96.0) ppb, while IgE levels median of 183.5 (IQR: 52.0, 685.0) IU/ml and BEC of 350.0 (IQR: 165.0, 635.0) cells/µl.
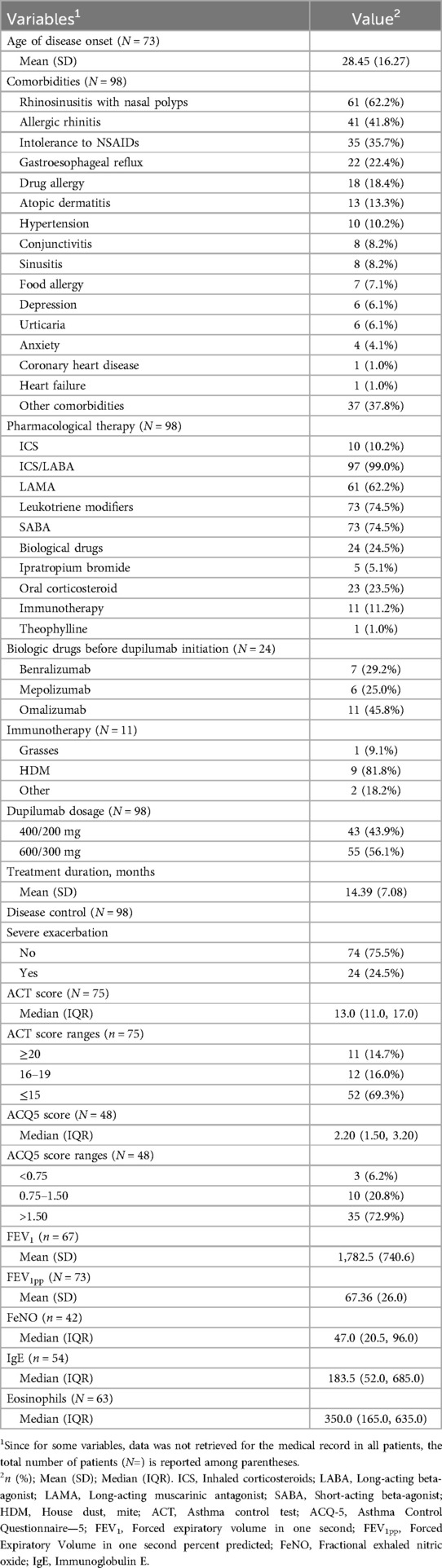
Table 2. Baseline clinical characteristics.
3.2 Exacerbations
The AERs were significantly lower after dupilumab treatment compared to baseline (p = 0.03). Compared to baseline AER (0.61 ± 1.45 per adult), a reduction of 82.0% and 86.9% in T1 and T2 AERs were observed, respectively (Figure 1 and Supplementary Table S2). ICU admissions were registered for five patients (5.1%) at baseline. After dupilumab, only one ICU admission occurred within the first year of initiating.
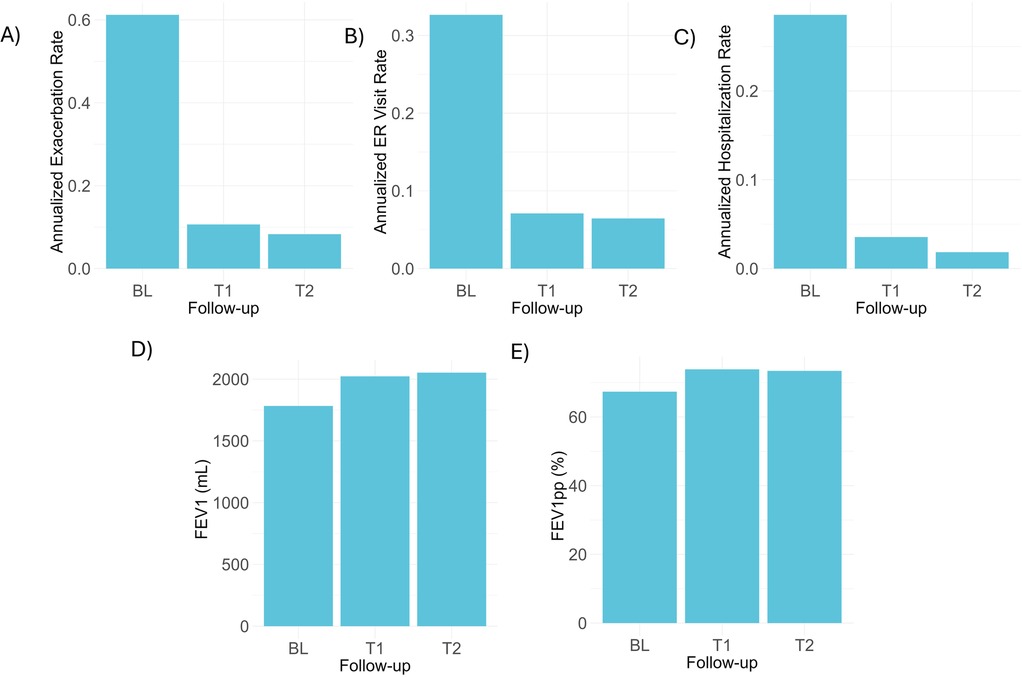
Figure 1. Frequency of exacerbations and lung function before and after dupilumab treatment. Annualized exacerbation (A), emergency room visit (B), and hospitalization rates (C) at baseline and during the first (T1) or second year (T2) of treatment with dupilumab. Mean FEV1 and FEV1pp values are also presented before and after treatment with the biologic. BL, baseline; ER, emergency room; FEV1, forced expiratory volume in one second, FEV1pp, forced expiratory volume in one second percent predicted.
3.3 Lung function
As shown in Figure 1, mean FEV1 values were higher at one-year (2,022.5 ± 766.4 ml) and second year (2,052.3 ± 759.6 ml) of follow-up after treatment with dupilumab, compared to baseline (1,782.5 ± 740.5 ml) reaching statistical significance (p = 0.03). Higher FEV1 values were observed from the 2–4-month time-point and median changes were greater than 200 ml in most follow-up controls (Table 3 and Figure 2). Mean FEV1pp was 67.4% at baseline, and 73.9% at T1 and 73.4% at T2 (p = 0.14). Changes in FEV1pp showed improvement from the 2 to 4-month period, with a median change of 12.5% (IQR: 0.3, 21.5) (Table 3).
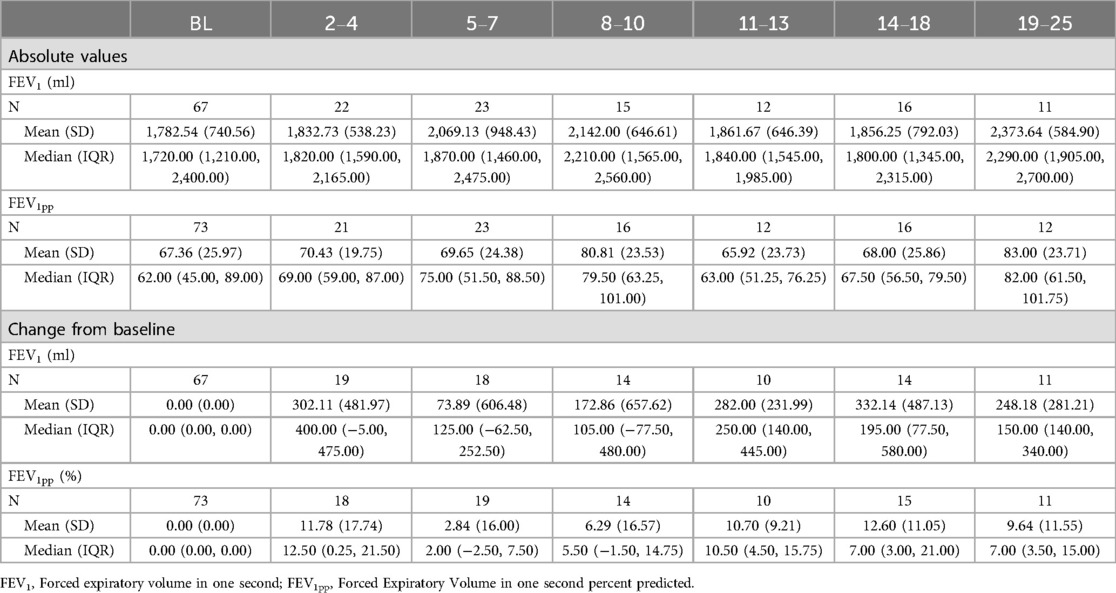
Table 3. Measured values and changes from baseline in FEV1 and percent predicted FEV1 (FEV1pp) at baseline and follow-up time point.
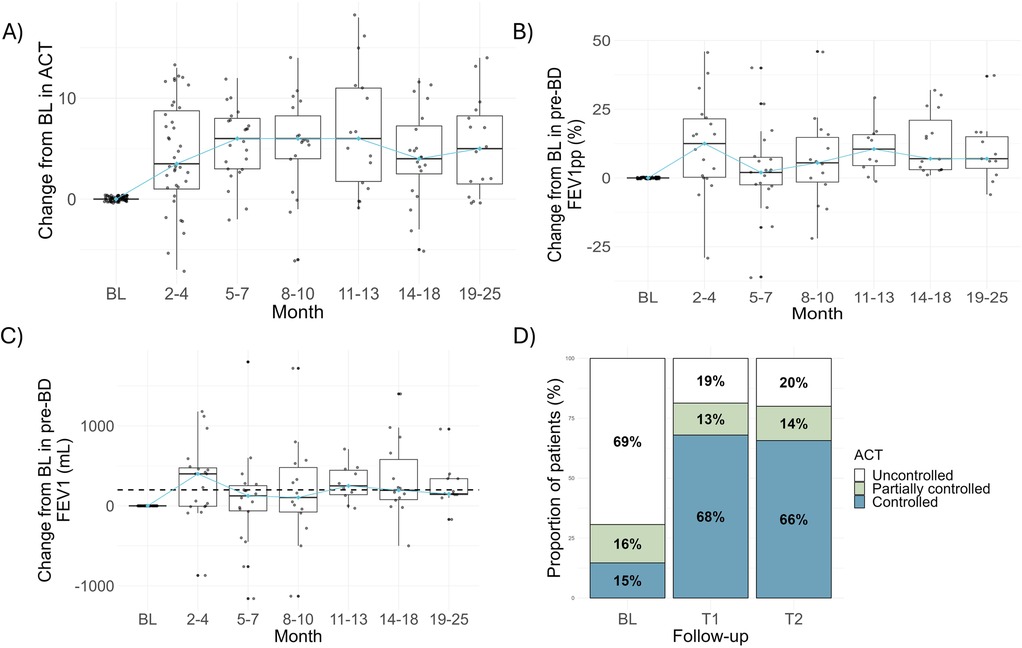
Figure 2. Changes from baseline in lung function and asthma control during two years of treatment with dupilumab. Changes in baseline in FEV1 (A) and FEV1pp (B) before bronchodilator at different time-points during dupilumab treatment are shown. (C) Changes in the Asthma Control Test are presented. (D) Based on ACT, relative frequencies of controlled, partially controlled and uncontrolled asthma were calculated at baseline, one (T1) or second year (T2) of treatment. Dashed line in A was set at 200 mL to highlight patients with improvements over this value. Blue line in all box plots is connecting median values. BL, baseline; FEV1, forced expiratory volume in one second; FEV1pp, forced expiratory volume in one second percent predicted.
3.4 Oral corticosteroid prescriptions
OCS prescriptions decreased from 20.4% (n = 20 out of 98 patients) at baseline to 2.5% (n = 1 out of 40 patients) at the 8–10 months period (Supplementary Table S3). In subsequent periods, while the percentages fluctuate, they consistently remain lower than those reported at baseline. The use of ICS/LABA medications remained unchanged throughout the analyzed periods, with minimal meaningful changes (Supplementary Table S3).
3.5 Asthma control
At baseline, 68% of patients had uncontrolled asthma. After dupilumab, lower rates of uncontrolled asthma were observed at year-one (19%) and second year of treatment (20%), respectively (chi2 = 47.14, p < 0.0001). Positive changes in ACT values were observed from 2 to 4 months (Supplementary Table S4 and Figure 2).
3.6 Feno
A decline of FeNO was observed beginning at the 2–4 months period, showing a reduction of 45.73% [Means: 63.57 (SD 56.69) ppb at BL and 34.50 (23.76) ppb at 2–4 months]. This trend persisted, with mean FeNO levels consistently remaining below 25 ppb after the 5–7 months period (Supplementary Table S5 and Figure 3). To allow for the maximum number of FeNO data points after dupilumab therapy, the last FeNO measurement available for each patient was identified and proportions of patients below the threshold to consider airway inflammation were compared with baseline. Among a total of 47 follow-up data points, 35 patients had FeNO values below 25 ppb (74.5%), which is significantly higher compared to baseline (15 out of 43, 34.9%; chi2 = 12.69, p = 0.0004).
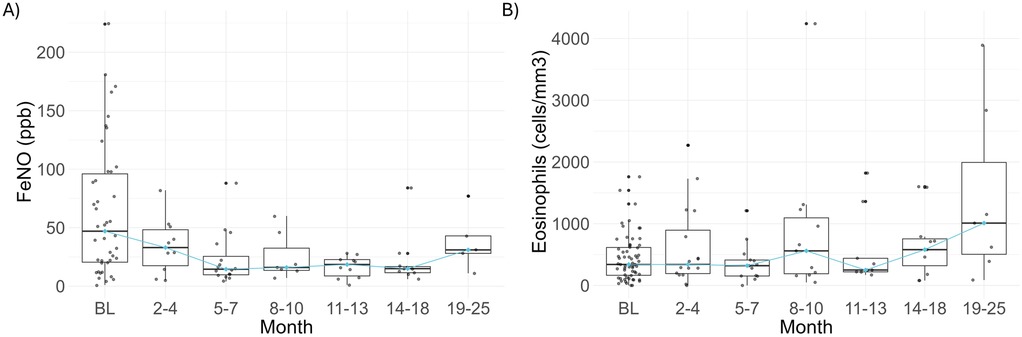
Figure 3. Assessment of type 2 inflammation markers during dupilumab treatment. (A) FeNO and (B) absolute eosinophil blood counts are shown at baseline and after dupilumab treatment. Blue line in all box plots is connecting median values. BL, baseline; FeNO, fractional exhaled nitric oxide.
3.7 Blood eosinophil count (BEC)
Median BEC at baseline was 350.0 (IQR: 165.0–635.0) cells/µl; 48 (76.2%) and 37(58.7%) out of 63 (58.7%) patients had counts >150 and >300 cells/µl, respectively. Similar median values were observed during dupilumab treatment, except at 14–18 and 19–25-months periods with median values of 580.00 (IQR: 320–755) and 1,010 (IQR: 505–1,993) cells/µl, respectively (Supplementary Table S5 and Figure 3). Ten patients had BEC above 1,500 cells/µl during dupilumab treatment; however, for none of them eosinophilia was symptomatic. Baseline BEC was available for 7 out of 10 cases (Supplementary Table S6), observing that during dupilumab administration all of them had greater BEC than baseline.
3.8 Clinical asthma remission
Only one individual had data from two follow-up time points separated by a year, which enabled the assessment of clinical remission status. Although this individual was in clinical remission, the absence of similar data for the remaining patients made it difficult to determine the proportion of patients who achieved clinical remission within the entire cohort.
3.9 Safety
Besides the number of patients within the analyzed cohort used to report clinical outcomes related with asthma control, we considered an additional case to describe the presentation of adverse effects: a patient who discontinued dupilumab at 2 months due to AE; she was 59-years old woman who experienced headache, nervousness, and tremor and discontinued dupilumab. Headache was the most common AE (4.0%, n = 4 of 99 patients) followed by conjunctivitis (3.0%, n = 3), and sinusitis (3.0%, n = 3) (Table 4). Additionally, among the other reported adverse events (Supplementary Table S7), gastrointestinal symptoms (3.0%, n = 3), arthralgias (2.0%, n = 2), and blurred vision (2.0%, n = 2) were the most reported.
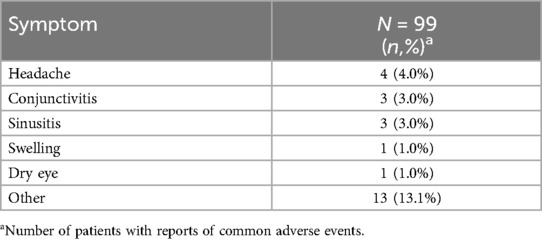
Table 4. Reported adverse events per person.
3.10 Temporary discontinuation and complete withdrawal
Twenty patients (20.4%) had temporary discontinuation of dupilumab (mean time: 2.2 months) and some had more than one treatment suspension for a total of 23 events (Supplementary Table S8). Most suspensions (65.2%, n = 15) were due to delays in drug administration by the Health Insurance Provider (Supplementary Table S9).
Three (3.1%) patients completely withdrew from the medication after 6 months of usage (with an average duration of 6.3 months for those on dupilumab). The reason for complete withdrawal was not recorded in the medical record in one patient, while two patients withdrew due to adverse events: one experienced gastrointestinal symptom, while the other experienced both gastrointestinal symptoms and a lack of efficacy, leading to a switch to benralizumab.
4 Discussion
In this RW study, we documented clinical improvement after dupilumab use in patients with SA treated in different centers in Colombia. We observed significant reductions in the occurrence of severe exacerbations that led to HCRU, and in the proportion of uncontrolled asthma symptoms as reported by ACT. Also, the FeNO decline supported a marked reduction in the inflammatory airway process in most treated patients. In general, the biologic was well-tolerated, observing that adverse events were reported in a similar rate to those reported in pivotal clinical trials (10–12). Although, high BEC was observed in some patients, this was not associated with clinical symptoms that could raise concerns about dupilumab safety.
Exacerbation reduction is an important criterion to assess the effectiveness of an asthma intervention. In this cohort, a reduced severe AER was observed after dupilumab initiation. AER changed from 0.6 to 0.1 and 0.08 in the first and second year of treatment, respectively. This reduction rate of approximately 80%, was notably higher than that reported in other real-world studies from the US (14) and Japan (13), where the reduction was close to 40%, as well as that reported in RCTs (9). A higher reduction in exacerbation rates was published by Caminati et al. in an Italian cohort, wherein the exacerbation numbers decreased from 2.6 to 0.1 at 12 months of therapy (15). Our cohort is more similar to the one described in that study in terms of the number of patients with nasal polyps co-morbidity (15). Prescription of OCS for asthma control was also reduced in this cohort after dupilumab initiation coinciding with other real-word reports (13, 16) and clinical studies (17). The sparing effect on OCS use may have beneficial effects on patients due to well-known adverse events associated with them (18).
Eosinophilia has been reported as an adverse event associated with the use of dupilumab, with cases ranging from asymptomatic to severe (19). Hypereosinophilia at any moment during dupilumab treatment was observed in ∼10% of patients, although this rate varies compared to other studies. However, it is noteworthy that no cases were associated with symptoms. Notably, none of these cases were symptomatic. However, there is a safety concern due to instances of conjunctivitis and gastroenteritis potentially linked to eosinophilia. One proposed mechanism for the increase in eosinophils is that dupilumab's inhibition of the IL-4/IL-13 pathway reduces eosinophil infiltration into inflamed tissue, thereby potentially increasing circulating eosinophils (20). Follow-up studies, such as TRAVERSE, suggest that this hypereosinophilia may be transient. In the TRAVERSE study, which observed patients for 96 weeks, the rise in eosinophils declined over time, with no cases observed after two years. In our cohort, most cases of elevated eosinophil absolute counts (BEC >1,500 cells/ul) were observed during the 22–24-month follow-up period. In contrast, other studies have observed high BEC levels within the first three months, whereas in our study, the median BEC at that time point was similar to baseline levels. Unfortunately, BEC data were unavailable at all time points or at baseline, limiting our ability to draw definitive conclusions about BEC patterns in the Colombian population. Thus, this area warrants further exploration, because other environmental exposures, such as helminth infections, may affect blood eosinophils (12). This observation regarding hypereosinophilia, although seen in a small percentage of patients without associated clinical symptoms, underscores the importance of monitoring eosinophil levels during dupilumab treatment.
FeNO has been proposed as a reliable biomarker to evaluate the impact of biologics on airway inflammation. In this RWE, we observed that 74.5% of patients achieved reduction of FeNO below 25 ppb. This agrees with preliminary publications for the VESTIGE trials that reported an achievement of FeNO normalization in 66% of patients with dupilumab compared with 10% of patients receiving placebo. This improvement in airway inflammation was also evidenced by measuring mucus plugging and airway volume through structural studies (21).
Notably, despite delays or temporary discontinuation in the administration of dupilumab, primarily because of health system-related access difficulties, a favorable clinical response to this biologic was observed, as evidenced by both direct medical and patient-reported outcomes. These findings underscore the importance of RW data, which can be highly valuable in clinical decision-making, particularly in underdeveloped countries, where clinical scenarios may differ significantly from the controlled administration of medication observed in RCTs. Local data can also optimize the cost-effectiveness modeling of health interventions for SA (22). For instance, in Colombia, two studies comparing biologics as interventions for SA used RCTs to assess efficacy (22, 23). Our data can enhance the accuracy and applicability of modeling studies in this context.
This study has limitations that should be noted. First, dupilumab was approved in Colombia in 2019, and the observation window overlaps with the period when COVID-19 pandemic lockdowns affected medical follow-up for patients. Additionally, SARS-CoV-2 infection could have influenced lung function. The regularity of medical visits and controls, as well as attendance for lab tests, could also have been negatively impacted by the pandemic. Second, the use of OCS was not considered as part of the criteria to define severe exacerbations due to concerns about patients self-administering OCS regardless of the severity, as well as the lack of reporting in medical records. Since most studies use this criterion to define severe exacerbations, AER could be underestimated in this cohort. Additionally, although the observed reduction in AER after one and two years of treatment could theoretically be subject to attrition bias—if patients with more frequent exacerbations discontinued treatment or follow-up—this risk is likely minimal in our cohort. Only 3 out of 98 patients (3.1%) dropped out during the study period, suggesting that the impact of patient attrition on outcome estimates is limited. Although we attempted to retrieve as much data as possible from clinical records, missing data at various time points limited the ability to perform repeated measures analyses. As a result, we opted for independent group comparisons based on rates at baseline and follow-up time points. Also, it should be noted that no sample size estimation was performed to ensure the robustness of these comparisons. This study did not include data from claims databases that register all prescriptions for a patient as reported for other studies, but only those from the specialized consultation service if reported in the medical record. However, an advantage is that different clinical and biological criteria, used in real practice, could also be analyzed, and support an improvement in asthma symptoms and disease control. This study highlights the importance of generating local data to optimize cost-effectiveness models for health interventions in the treatment of severe asthma in developing countries. Additionally, it can provide a stronger basis for clinical decision-making and health policy formulation.
In conclusion, dupilumab is an effective and well-tolerated treatment for severe asthma in Colombia, showing substantial reductions in severe exacerbations and improvements in asthma control and FeNO values. Ongoing research and long-term follow-up studies are essential to further validate these findings and explore the underlying mechanisms of eosinophilia in treated patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Fundación Neumológica Colombiana. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
AA-M: Conceptualization, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. JZ: Conceptualization, Formal analysis, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing. NA-Z: Funding acquisition, Project administration, Writing – original draft, Writing – review & editing. EG: Investigation, Writing – original draft, Writing – review & editing. CD: Investigation, Writing – original draft, Writing – review & editing. DC: Investigation, Writing – original draft, Writing – review & editing. FB: Investigation, Writing – original draft, Writing – review & editing. AC: Investigation, Writing – original draft, Writing – review & editing. PR-O: Conceptualization, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. NG-A: Conceptualization, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. GP: Supervision, Visualization, Writing – original draft, Writing – review & editing. SL: Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing. CT-D: Conceptualization, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research has been funded by Sanofi Colombia.
Acknowledgments
To Ana Lozano, for kindly checking structure of scripts for data analysis
Conflict of interest
AAl-M reports lecture fees from GSK, AstraZeneca and Sanofi (outside the submitted work), Grants from AstraZeneca (outside the submitted work) and support for attending meetings and/or travel from Boehringer Ingelheim (outside the submitted work). EG reports consulting and lecture fees from Novartis, Sanofi, Faes farma-Glaxo and Abbvie (outside the submitted work) and support for attending meetings and/or travel from Novartis, Sanofi and Faes farma-Glaxo (outside the submitted work). CD-B reports lecture fees and support for attending meetings and/or travel from GSK, Megalabs, AstraZeneca, Axon Pharma, Boehringer Ingelheim and Sanofi (outside the submitted work). Also, she had participated in data safety monitoring board or advisory board from GSK, Valentech and Sanofi. DC serves as an advisory board member at Asoneumocito and Colegio Medico de Santander. Also, she reports support for attending meetings and/or travel at 17 congress ALAT. AC reports consulting fees from Glaxo Smith Kline and Support for attending meetings and/or travel from Takeda (outside the submitted work). CT-D serves as an advisory board member at AstraZeneca and GlaxoSmithKline. He reports lecture fees from AstraZeneca, Boehringer-Ingelheim, Glaxo Smith Kline, Novartis and Sanofi-Aventis (outside the submitted work); payment for expert testimony from AstraZeneca, and Glaxo Smith Kline; support for attending meetings and/or travel from AstraZeneca and Sanofi. NA-Z is an employee of ALZAK Consulting & Research, a center that has developed research projects in conjunction with GSK, Sanofi, MSD, Merck, Abbvie, Bayer, Biopas and received fees for developing this project. JZ received fees from ALZAK to participate in this study. The authors from Fundación Neumológica Colombiana, UNIMEQ-ORL, NEUMOMED, Instituto Neumológico del Oriente; Centro de Alergología Alejandro Carreño and ALZAK reported receiving fees for this research from Sanofi. PR-O, NG-A, GP and SL are employees of Sanofi de Colombia and may hold shares and/or stock options in the company.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/falgy.2025.1564033/full#supplementary-material
References
1. Cao Y, Chen S, Chen X, Zou W, Liu Z, Wu Y, et al. Global trends in the incidence and mortality of asthma from 1990 to 2019: an age-period-cohort analysis using the global burden of disease study 2019. Front Public Health. (2022) 10:1036674. doi: 10.3389/fpubh.2022.1036674
2. GBD. 2016 DALYs and HALE collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Lond Engl. (2017) 390(10100):1260–344. doi: 10.1016/S0140-6736(17)32130-X
3. Hekking PPW, Wener RR, Amelink M, Zwinderman AH, Bouvy ML, Bel EH. The prevalence of severe refractory asthma. J Allergy Clin Immunol. (2015) 135(4):896–902. doi: 10.1016/j.jaci.2014.08.042
4. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. (2023). Available online at: www.ginasthma.org (updated July 2023).
5. Hossny E, Caraballo L, Casale T, El-Gamal Y, Rosenwasser L. Severe asthma and quality of life. World Allergy Organ J. (2017) 10(1):28. doi: 10.1186/s40413-017-0159-y
6. Flórez-Tanus Á, Parra D, Zakzuk J, Caraballo L, Alvis-Guzmán N. Health care costs and resource utilization for different asthma severity stages in Colombia: a claims data analysis. World Allergy Organ J. (2018) 11(1):26. doi: 10.1186/s40413-018-0205-4
7. Chung KF, Wenzel SE, Brozek JL, Bush A, Castro M, Sterk PJ, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. (2014) 43(2):343–73. doi: 10.1183/09031936.00202013
8. Izuhara K, Arima K, Yasunaga S. IL-4 and IL-13: their pathological roles in allergic diseases and their potential in developing new therapies. Curr Drug Targets Inflamm Allergy. (2002) 1(3):263–9. doi: 10.2174/1568010023344661
9. Zayed Y, Kheiri B, Banifadel M, Hicks M, Aburahma A, Hamid K, et al. Dupilumab safety and efficacy in uncontrolled asthma: a systematic review and meta-analysis of randomized clinical trials. J Asthma Off J Assoc Care Asthma. (2019) 56(10):1110–9. doi: 10.1080/02770903.2018.1520865
10. Castro M, Corren J, Pavord ID, Maspero J, Wenzel S, Rabe KF, et al. Dupilumab efficacy and safety in moderate-to-severe uncontrolled asthma. N Engl J Med. (2018) 378(26):2486–96. doi: 10.1056/NEJMoa1804092
11. Busse WW, Maspero JF, Rabe KF, Papi A, Wenzel SE, Ford LB, et al. Liberty asthma QUEST: phase 3 randomized, double-blind, placebo-controlled, parallel-group study to evaluate dupilumab efficacy/safety in patients with uncontrolled, moderate-to-severe asthma. Adv Ther. (2018) 35(5):737–48. doi: 10.1007/s12325-018-0710-1
12. Wechsler ME, Ford LB, Maspero JF, Pavord ID, Papi A, Bourdin A, et al. Long-term safety and efficacy of dupilumab in patients with moderate-to-severe asthma (TRAVERSE): an open-label extension study. Lancet Respir Med. (2022) 10(1):11–25. doi: 10.1016/S2213-2600(21)00322-2
13. Kimura Y, Suzukawa M, Inoue N, Imai S, Akazawa M, Matsui H. Real-world benefits of biologics for asthma: exacerbation events and systemic corticosteroid use. World Allergy Organ J. (2021) 14(11):100600. doi: 10.1016/j.waojou.2021.100600
14. Al-Shaikhly T, Norris MR, Dennis EH, Liu G, Craig TJ. Comparative impact of asthma biologics: a nationwide US claim-based analysis. J Allergy Clin Immunol Pract. (2024) 12(6):1558–67. doi: 10.1016/j.jaip.2024.02.029
15. Caminati M, Maule M, Benoni R, Bagnasco D, Beghè B, Braido F, et al. Dupilumab efficacy on asthma functional, inflammatory, and patient-reported outcomes across different disease phenotypes and severity: a real-life perspective. Biomedicines. (2024) 12(2):390. doi: 10.3390/biomedicines12020390
16. Blaiss M, Bleecker ER, Jacob-Nara J, Nair R, Duh MS, Wang Z, et al. Real-world effectiveness of dupilumab in patients with asthma: findings from the US ADVANTAGE study. Ann Allergy Asthma Immunol Off Publ Am Coll Allergy Asthma Immunol. (2024) 132(4):463–468.e1. doi: 10.1016/j.anai.2023.11.006
17. Rabe KF, Nair P, Brusselle G, Maspero JF, Castro M, Sher L, et al. Efficacy and safety of dupilumab in glucocorticoid-dependent severe asthma. N Engl J Med. (2018) 378(26):2475–85. doi: 10.1056/NEJMoa1804093
18. Bleecker ER, Menzies-Gow AN, Price DB, Bourdin A, Sweet S, Martin AL, et al. Systematic literature review of systemic corticosteroid use for asthma management. Am J Respir Crit Care Med. (2020) 201(3):276–93. doi: 10.1164/rccm.201904-0903SO
19. Eger K, Pet L, Weersink EJM, Bel EH. Complications of switching from anti-IL-5 or anti-IL-5R to dupilumab in corticosteroid-dependent severe asthma. J Allergy Clin Immunol Pract. (2021) 9(7):2913–5. doi: 10.1016/j.jaip.2021.02.042
20. Allinne J, Scott G, Birchard D, Asrat S, Nagashima K, Le Floc’h A, et al. Broader Impact of IL-4Rα Blockade Than IL-5 Blockade on Mediators of Type 2 Inflammation and Lung Pathology in a House Dust Mite-Induced Asthma Mouse Model. En: C93 Mechanisms of Airway Inflammation in Asthma and COPD. New York, NY: American Thoracic Society (2019). p. A5555–A5555. (American Thoracic Society International Conference Abstracts). Available online at: https://www.atsjournals.org/doi/abs/10.1164/ajrccm-conference.2019.199.1_MeetingAbstracts.A5555 (accessed June 10, 2024).
21. Castro M, Papi A, Porsbjerg C, Lugogo N, Brightling C, González-Barcala FJ, et al. Evaluating the effect of dupilumab on type 2 airway inflammation and mucus plugging in patients with uncontrolled moderate-to-severe asthma: the VESTIGE trial. J Allergy Clin Immunol. (2024) 153(2):AB368. doi: 10.1016/j.jaci.2023.11.879
22. Ali A, García E, Torres-Duque CA, Rey D, Botero L, Saenz S, et al. Cost-effectiveness analysis of dupilumab versus omalizumab, mepolizumab, and benralizumab added to the standard of care in adults with severe asthma in Colombia. Expert Rev Pharmacoecon Outcomes Res. (2024) 24(3):361–74. doi: 10.1080/14737167.2023.2282668
Keywords: asthma, dupilumab, treatment outcome, Colombia, effectiveness
Citation: Alí-Munive A, Zakzuk J, Alvis-Zakzuk NJ, García E, Diaz Bossa C, Cano Rosales DJ, Bolívar F, Carreño A, Rodríguez-Ordoñez P, Gómez-Ardila N, Patiño G, Londoño S and Torres-Duque CA (2025) Real world evidence of dupilumab effectiveness in a Colombian cohort of patients diagnosed with severe asthma. Front. Allergy 6:1564033. doi: 10.3389/falgy.2025.1564033
Received: 20 January 2025; Accepted: 9 April 2025;
Published: 13 May 2025.
Edited by:
Igor Kaidashev, Poltava State Medical University, UkraineReviewed by:
Matteo Monzio Compagnoni, University of Milano-Bicocca, ItalySergii Zaikov, Shupyk National Medical Academy of Postgraduate Education, Ukraine
Copyright: © 2025 Alí-Munive, Zakzuk, Alvis-Zakzuk, García, Diaz Bossa, Cano Rosales, Bolívar, Carreño, Rodríguez-Ordoñez, Gómez-Ardila, Patiño, Londoño and Torres-Duque. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Josefina Zakzuk, anpha3p1a3NAdW5pY2FydGFnZW5hLmVkdS5jbw==