 Andrea Sangalli1*
Andrea Sangalli1* Valerio Pravettoni1
Valerio Pravettoni1 Mariarita Sciumè2
Mariarita Sciumè2 Dario Consonni3Silvio Sartorio4
Dario Consonni3Silvio Sartorio4 Nicola Montano1,5Federica Rivolta1
Nicola Montano1,5Federica Rivolta1
- 1General Medicine Unit, Department of Internal Medicine, Fondazione IRCCS Ca’ Granda, Ospedale Maggiore Policlinico, Milan, Italy
- 2Hematology Unit, Department of Internal Medicine, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Milan, Italy
- 3Occupational Health Unit, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Milan, Italy
- 4Allergy and Clinical Immunology Residency, University of Milan, Milan, Italy
- 5Department of Clinical Sciences and Community Health, University of Milan, Milan, Italy
Background: Patients with mastocytosis have a higher risk of anaphylactic reactions. This study aims to assess the prevalence and risk factors of anaphylaxis among patients diagnosed with Systemic Mastocytosis (SM), including pre-diagnostic Systemic Mastocytosis (pre-SM), a subgroup of patients often overlooked in current classifications.
Methods: A retrospective monocentric study was conducted at Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico in Milan, Italy. Patients aged ≥18 years diagnosed with SM or pre-SM between January 2009 and May 2025 were included. Demographic, clinical and laboratory data were analyzed using chi-squared test or Wilcoxon-Mann–Whitney and Kruskal–Wallis tests
Results: At the time of diagnosis, out of 162 patients (53% women), 29 (18%) experienced at least one episode of anaphylaxis. Hymenoptera venom was the main trigger (51.7%), followed by drugs (27.6%) and idiopathic cases (20.7%). Patients with anaphylaxis had 7% pre-SM, 48% BMM, 28% ISM, 0% SSM, 7% ASM, 10% SM-AHN, (p < 0.001). The prevalence of anaphylaxis in each subtype was as follows: 2/12 (17%) in pre-SM, 14/31 (45%) in BMM, 8/97 (8%) in ISM, 0/5 in SSM, 2/4 (50%) in ASM and 3/13 (23%) in SM-AHN, (p < 0.001). Hymenoptera venom–induced anaphylaxis occurred exclusively in indolent forms (pre-SM, BMM, and ISM) while drug-induced anaphylaxis was observed in both ISM and advanced SM subtypes. Idiopathic anaphylaxis was more evenly distributed across all SM subtypes, (p < 0.001). The presence of cutaneous lesions was associated with a lower risk of anaphylaxis: 10/114 (8.8%) vs. 19/48 (39.6%) without skin involvement (p < 0.001), with a confirmed protective effect in both ISM and pre-SM. Male sex was identified as an additional risk factor, (p = 0.03). A history of Hymenoptera sting was associated with a higher risk of Hymenoptera venom anaphylaxis: 15/113 (13%) vs. no reactions to the first sting in 47 patients, (p = 0.011).
Conclusion: Anaphylaxis is a relevant issue not only in acknowledged variants of SM, but also in pre-diagnostic forms. Idiopathic anaphylaxis may occur across different subtypes. Hymenoptera venom is the main trigger in indolent forms, whereas drug-induced reactions predominate in ISM and advanced SM, mainly through IgE-independent mechanisms. The risk of anaphylaxis is higher in pre-SM and ISM without cutaneous involvement, particularly in case of Hymenoptera venom sensitization. Our results highlight the need for allergological risk assessment and close monitoring especially in patients without skin lesions or with Hymenoptera venom sensitization.
Introduction
Mastocytosis comprises a heterogeneous group of rare clonal neoplasms characterized by the proliferation and accumulation of abnormal mast cells in one or more organ systems (1).
The latest World Health Organization (WHO) classification confirmed the established distinction between cutaneous mastocytosis (CM), systemic mastocytosis (SM), and the rare entity mast cell sarcoma (2).
CM is confined to the skin and predominantly affects pediatric patients, with a favorable prognosis and a significantly lower risk of anaphylaxis compared to SM (3).
SM is defined by the involvement of at least one internal organ, which may be accompanied by cutaneous lesions. The classification into subtypes is useful from a haematological perspective, especially regarding prognosis: non-advanced variants such as Bone Marrow Mastocytosis (BMM), Indolent SM (ISM) and Smoldering SM (SSM) have a higher survival rate compared to advanced forms such as Aggressive SM (ASM), SM with an Associated Hematopoietic Neoplasm (SM-AHN) and Mast Cell Leukemia (MCL) (4).
Patients who do not meet the diagnostic criteria for SM but fulfil one or two minor criteria of monoclonal origin are classified as having pre-diagnostic Systemic Mastocytosis (pre-SM) or monoclonal mast cell activation syndrome (MMCAS) depending on the presence or absence of mast cell activation symptoms (5, 6).
The clinical presentation of mastocytosis is heterogeneous, ranging from symptoms due to cutaneous involvement to signs related to inappropriate mast cell mediator release (e.g., allergic reactions including anaphylaxis, osteopenia and osteoporosis). One hypothesis attributes the link between SM and anaphylaxis to the hyperactive state of mast cells carrying the activating D816V mutation, another one considers the increased number of potential effector cells as a factor increasing the risk of immediate-type allergic reactions (3). The risk of anaphylaxis is higher in ISM and BMM subtypes (7). Advanced forms of SM (advSM), characterized by extensive tissue infiltration, may manifest with organ dysfunction and often require cytoreductive therapy (1).
Considering the complexity of the disease, a multidisciplinary approach is essential, involving hematologists, allergists, dermatologists, endocrinologists, and gastroenterologists. Treatment options vary according to clinical presentation, ranging from symptomatic therapy (anti-mediators) and anaphylaxis prevention (e.g., emergency kit with epinephrine, patient education, venom immunotherapy when appropriate), to treatment of osteopenia or osteoporosis, and cytoreductive treatment (8).
Allergy evaluation is recommended as patients with SM have an approximately 100-fold increased risk of anaphylaxis compared to the general population. Given the rarity of the disease, the prevalence of anaphylactic reactions is estimated to range widely from 20% to 56%. The main cause of anaphylaxis is Hymenoptera venom (HV)—particularly wasp stings—followed by idiopathic anaphylaxis (with no identified cause) and lastly, drugs and foods (9).
Certain clonal mast cell disease (MCD) such as BMM, ISM and MMCAS are established risk factors for severe Hymenoptera sting–induced anaphylaxis. Hereditary alpha tryptasemia (HαT), a genetic trait characterized by increased copy numbers of TPSAB1 gene encoding alpha-tryptase and consequently by basal serum tryptase level above 8 μg/L, is also associated with severe Hymenoptera venom allergy (HVA), with the risk further increased in the presence of concomitant clonal MCD (10).
According to the 2022 WHO classification update, which recognized BMM as a distinct subtype (2), this monocentric study aimed to evaluate the prevalence of anaphylaxis in a group of patients with SM or pre-SM. Anaphylaxis triggers and possible risk or protective factors for anaphylaxis were analyzed across different SM subtypes, including emerging forms such as pre-SM, to stratify allergological risk.
Methods
A retrospective monocentric study group was conducted at the Allergology Clinic of the Foundation IRCCS Ca' Granda Ospedale Maggiore Policlinico in Milan, Italy, where patients with SM are managed by a multidisciplinary team including allergists, hematologists, dermatologists and endocrinologists.
Patients aged 18 years or older were included if diagnosed with SM according to latest WHO criteria (2) or pre-SM, defined as a clonal abnormal bone marrow mast cell infiltrate that does not meet full diagnostic criteria for SM. Markers of clonality are defined by the presence of KIT D816V mutation in bone marrow or in peripheral blood (digital or ASO-PCR, Sanger sequencing and next generation sequencing) and/or the aberrant expression of CD25/CD2 on mast cells on multiparameter flow cytometry.
Data were collected in a strictly pseudonymized manner using a case report form on the Research Electronic Data Capture (REDCap®) platform, which is validated in accordance with national regulations.
Clinical data were extracted from the electronic medical records of SM patients followed between January 2009 and May 2025, and included:
– Socio-demographic variables: sex, age at diagnosis,
– Anamnestic and laboratory data: SM subtypes by diagnostic criteria [presence of major and minor WHO criteria (2)], comorbid conditions (rhinitis, bronchial asthma, atopic dermatitis, food allergy), presence of cutaneous lesions, history of Hymenoptera stings, history of anaphylaxis at diagnosis and associated triggers identified through an allergological workup. HV allergy was confirmed by positive skin tests and/or serum IgE for venom extracts and for recombinant allergens (8) (ImmunoCAP system, Thermo Fisher Scientific®), food allergy by skin prick test (Lofarma® and Stallergenes®) and serum IgE for food and for recombinant allergens (ImmunoCAP system, Thermo Fisher Scientific®), drug allergy by serum specific IgE for beta-lactams (ImmunoCAP®, Thermo-Fisher), cutaneous tests (DAP, DIATER Laboratories®), basophil activation test (BAT) and drug provocation test. Idiopathic anaphylaxis was diagnosed if all potential triggers had been ruled out (3).
We calculated anaphylaxis prevalence and 95% confidence interval (CI). Associations between a history of anaphylaxis and clinical or laboratory variables were analyzed using the chi-squared tests.
Age at diagnosis and triptase levels were analyzed using Wilcoxon-Mann–Whitney and Kruskal–Wallis tests. Statistical analysis was performed using Stata 18 software (StataCorp, 2023).
The study received approval from the Ethics Committee of the Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico (5916_16.04.2025_P). It was conducted in accordance with the principles of Good Clinical Practice, the ethical guidelines of the Declaration of Helsinki, and current regulations on observational studies.
Results
Study group
The study group included 162 adult patients, comprising 86 women (53.1%) and 76 men (46.9%). The median/mean age at diagnosis was 49.5/50.8 years (range 22–86 years, SD 15.3).
Patients were classified into the following diagnostic subtypes: 12 (7.4%) pre-SM, 31 (19.1%) BMM, 97 (59.9%) ISM, 5 (3.1%) SSM, 4 (2.5%) ASM, and 13 (8.0%) SM-AHN.
Median and mean age were lower in patients with ASM and pre-SM, and was higher in patients with SM-AHN and SSM. Pre-SM, BMM and SSM were more frequently diagnosed in male patients, whereas ISM was more common in females.
The overall prevalence of atopy was 27.8%, with 37 of 162 patients (22.8%) affected by allergic rhinitis, 7 (4.3%) by allergic asthma, and 1 (0.6%) by atopic dermatitis. No significant differences were observed in the prevalence of allergic diseases among the different subtypes.
Cutaneous involvement due to mastocytosis was more frequently observed in ISM patients, but a prevalence above 60% was also seen in pre-SM, SSM, and ASM.
Mastocytosis diagnostic criteria showed a heterogeneous distribution across the different subtypes, except for the KIT D816V mutation, which was homogeneously expressed (Table 1).
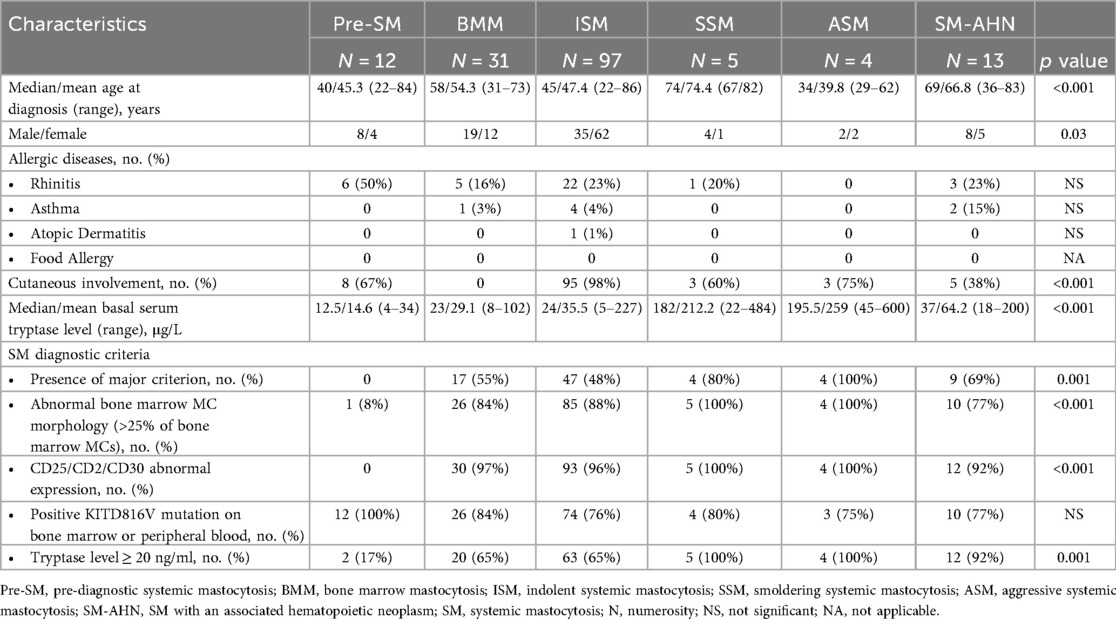
Table 1. Characteristics of the study group by subtype.
Anaphylaxis prevalence and triggers
At the initial evaluation, at least one episode of anaphylaxis was reported in 29 patients (17.9%), of whom 19 (65.5%) were male and 10 (34.5%) were female (p = 0.03).
The median/mean age at diagnosis was 58/52.7 years (range 29–78, SD 13.2) in the group with anaphylaxis and 49/50.3 (range 22–86, SD 15.7) in the group without anaphylaxis (p = 0.38).
The identified triggers of anaphylaxis included Hymenoptera venom in 15 of 29 cases (51.7%), drugs in 8 of 29 (27.6%), and idiopathic causes in 6 of 29 (20.7%).
Hymenoptera venom–induced anaphylaxis occurred exclusively in indolent forms of SM (pre-SM, BMM, and ISM), drug-induced anaphylaxis was observed in both ISM and advanced SM subtypes, while idiopathic anaphylaxis showed a more homogeneous distribution across SM subtypes (Table 2).
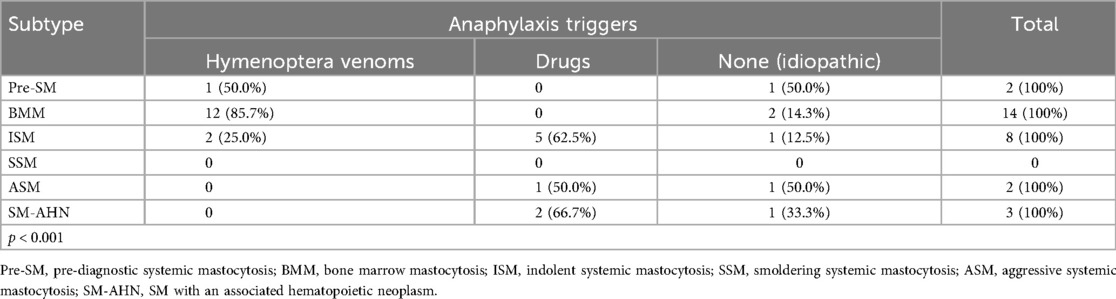
Table 2. Anaphylaxis triggers in systemic mastocytosis subtypes.
Wasp venom was the most frequent cause of HVA, accounting for 13 of 15 cases (87.7%). One patient (6.7%) experienced anaphylaxis due to bee venom, and another (6.7%) reacted to both wasp and bee venom. In one case (6.7%), the culprit insect could not be identified and standard diagnostic tests yielded negative results.
Involved drugs in 8 patients were acetylsalicylic acid (2), ibuprofen (1), ketorolac (1), amoxicillin (1), cephazolin as pre-anesthesia prophylaxis (1), intravenous iron preparation (1), intramuscular cyanocobalamin (1).
No association was found between the presence of specific allergic comorbidities and the occurrence of anaphylaxis.
Anaphylaxis and SM subtypes
Out of 29 cases of anaphylaxis 2 (6.9%) were registered in pre-SM, 14 (48.3%) in BMM, 8 (27.6%) in ISM, 0 (0%) in SSM, 2 (6.9%) in ASM, and 3 (10.3%) in SM-AHN (p < 0.001).
The prevalence of anaphylaxis was associated with subtype (p < 0.001, Table 3), with anaphylaxis around 50% in patients with BMM and ASM.
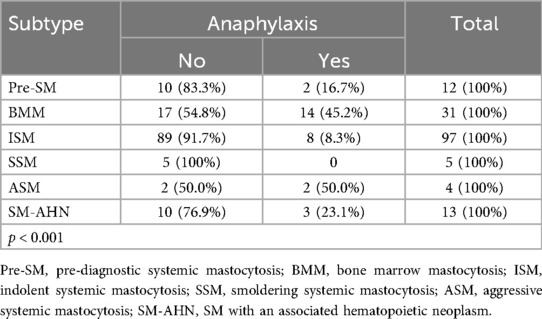
Table 3. Anaphylaxis prevalence in systemic mastocytosis subtypes.
The median/mean basal serum tryptase level was 25/43.5 μg/L (range: 4–484; SD: 61.0) in patients without anaphylaxis, compared to 26/57.4 μg/L (range: 6–600; SD: 111.2) in those with anaphylaxis (p = 0.97). No significant differences were found between the group with or without anaphylaxis with respect to comorbid atopic diseases or SM diagnostic criteria.
Anaphylaxis occurred in 10 of 114 patients (8.8%) with cutaneous lesions compared to 19 of 48 (39.6%) without skin involvement (p < 0.001).
Among ISM patients, 6 of 95 (6.3%) with cutaneous lesions experienced anaphylaxis vs. 2 of 2 (100%) without lesions (p < 0.001). In the pre-SM group, none of the 8 patients with skin lesions developed anaphylaxis, compared to 2 of 4 (50%) without lesions (p = 0.03). No significant association between cutaneous involvement and anaphylaxis was observed in patients with advSM (Table 4).
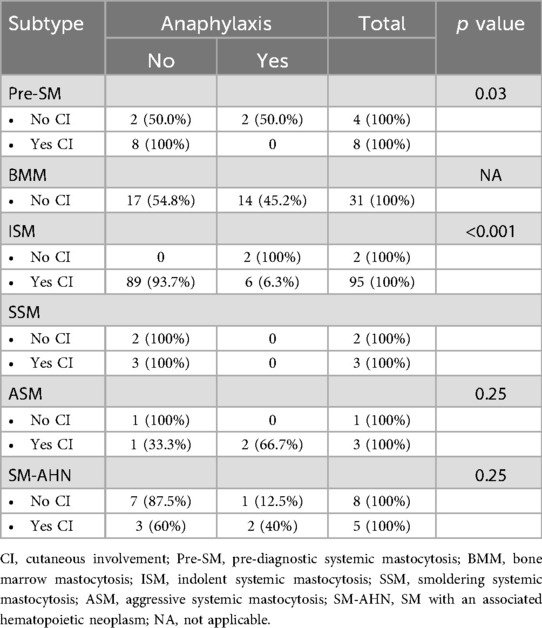
Table 4. Anaphylaxis prevalence in systemic mastocytosis subtypes according to cutaneous involvement.
Hymenoptera venom anaphylaxis and SM subtypes
HV anaphylaxis was more frequent in male patients (11 of 76; 14.5%) compared to females (4 of 86; 4.7%) (p = 0.031).
The median/mean age at diagnosis was 59/54.2 years (range: 33–67; SD: 11.0) in the anaphylaxis group and 49/50.4 years (range: 22–86; SD: 15.7) in the non-anaphylaxis group (p = 0.30).
Among those with HV anaphylaxis, 12 of 15 patients (80%) had BMM, 2 (13.3%) had ISM, and 1 (6.7%) had pre-SM.
Of the 113 patients with a documented history of a Hymenoptera sting, 15 (13.3%) developed anaphylaxis after a subsequent sting, compared to none of the 49 patients who had never been stung (p = 0.007).
Of the 162 patients, 132 underwent testing for HV sensitization. Among these, 13 of 43 sensitized individuals (30.2%) experienced HV anaphylaxis, vs. 2 of 89 (2.3%) who tested negative to standard diagnostic tests (p < 0.001).
The median/mean baseline serum tryptase level was 17/23.8 μg/L (range: 8–102; SD: 23.4) in the HV anaphylaxis group, compared to 26/48.3 μg/L (range: 4–600; SD: 75.3) in the non-HV anaphylaxis group (p = 0.03).
No differences in the prevalence of concomitant atopic diseases or SM diagnostic criteria were observed between groups.
HV anaphylaxis occurred in 2 of 114 patients (1.8%) with cutaneous lesions vs. 13 of 48 (27.1%) without skin involvement (p < 0.001).
Discussion
At the time of SM diagnosis, the overall prevalence of at least one episode of anaphylaxis was 17.9%, comparable to the 22% reported by a Spanish case series of the Red Espanola De Mastocitosis (REMA) group, which evaluated 163 adults with mastocytosis (11). Other studies have documented a higher prevalence of anaphylaxis in SM patients, ranging from 43% to 73% (12, 13). These discrepancies may stem from differences in patient selection—particularly in studies where many SMs were diagnosed following anaphylaxis—or from broader definitions of systemic reactions, including those limited to mucosal or cutaneous manifestations.
HV was identified as the main trigger of anaphylaxis (52%). Wasp venom was the most frequent cause. This finding confirms previous reports identifying Hymenoptera venom as the leading trigger of anaphylaxis in SM (11). The strong association between a history of Hymenoptera sting and HV anaphylaxis—confirmed by positive HV sensitization tests in most cases—supports an IgE-mediated mechanism.
Drugs represented the second most common trigger (28%), while 21% of anaphylaxis cases were idiopathic. No food-induced anaphylaxis was recorded. These results align with prior literature (3). One study reporting a higher frequency (24%) of food-related anaphylaxis attributed most reactions to alcohol ingestion, without evidence of food allergen sensitization, suggesting a nonspecific, mast cell–mediated activation mechanism (14).
Male sex remained a significant risk factor for anaphylaxis of all causes, consistent with the findings of the REMA group (11). We also observed a male predominance in HV anaphylaxis, although less pronounced than the strong correlation reported by Alvarez-Twose and colleagues in patients with ISM and HV reactions (15). As the author himself points out, it remains unclear whether male sex is an intrinsic predisposing factor or reflects increased occupational or recreational exposure to Hymenoptera stings (16).
The absence of a marked male predominance in all-cause anaphylaxis and the relatively low mean basal serum tryptase levels (<25 μg/L) in HV anaphylaxis support recent evidence indicating reduced sensitivity of the REMA score in detecting clonal MCD (10).
Atopic diseases had a prevalence of 28%, consistent with rates in the general population, and did not constitute a risk factor for anaphylaxis (11, 14).
A protective factor against anaphylaxis—both in ISM and pre-SM—was the presence of cutaneous involvement by the disease, even in patients with HV anaphylaxis. This observation corroborates findings from multiple case series (9, 14, 15).
In our study, anaphylaxis was frequently observed in recognized forms of SM, except for SSM, and also occurred in pre-SM. Notably, 17% of patients with pre-SM experienced anaphylaxis, triggered by HV or of idiopathic origin. As early as 2007, a subset of patients initially diagnosed with idiopathic anaphylaxis were found to harbor aberrant mast cells with clonal markers (17). Consequently, some authors proposed applying similar clinical management for pre-diagnostic forms as for SM, including anaphylaxis prevention, anti-mediator therapy, assessment for bone disease, and close monitoring for potential disease progression (5, 18). Our findings suggest that pre-SM warrants recognition in the current classification of SM, which remains absent in both the latest 2022 WHO and International Consensus Classification (ICC) updates (2, 19).
Although the elevated risk of anaphylaxis in ISM and BMM is well established (7), our data indicate that this risk is not negligible in advanced subtypes either, though it may present with distinct characteristics.
HV-induced anaphylaxis was exclusively observed in indolent forms—most frequently in BMM, followed by ISM and pre-SM. The CEREMAST study group reported an even higher rate of HV-induced anaphylaxis in patients with bone marrow clonal mast cells who did not meet SM or mast cell activation syndrome (MCAS) diagnostic criteria, emphasizing the need for tailored monitoring and management (20). One hypothesis to explain the higher prevalence of HVA in non-advSM is the increased susceptibility to IgE-mediated reactions in the context of a relatively low mast cell burden.
In contrast, drug-induced anaphylaxis occurred in both ISM and advSM, particularly in response to non-steroidal anti-inflammatory drugs (NSAIDs; 4/8, 50%) and beta-lactams (BLs; 2/8, 25%). The remaining cases involved intravenous iron and subcutaneous cyanocobalamin. Most of these reactions were likely due to IgE-independent mechanisms, leading to direct mast cell degranulation (21, 22). Interestingly, the ECNM registry identified a higher incidence of drug-induced hypersensitivity in advSM. The most frequent triggers were NSAIDs and BLs, with elevated serum tryptase levels identified as a significant risk factor for drug reactions. As previously hypothesized by the authors of the ECNM registry (23), the greater likelihood of drug-induced anaphylaxis in advanced forms may result from increased medication exposure in patients with aggressive hematologic diseases, and from the potential direct mast cell activation, especially in a context where cytoreductive therapies are frequently used.
Idiopathic anaphylaxis occurs across all SM subtypes without a specific distribution pattern (3).
It is clear that mastocytosis is not a homogeneous disorder, therefore, its subtypes require precise characterization and individualized risk stratification (24).
A particularly underrecognized subtype is pre-SM, which is associated with an increased risk of severe allergic reactions, bone involvement, and mast cell–mediated symptoms (25, 26). As such, pre-SM should be evaluated and monitored similarly to other non-advanced forms of SM, in order to prevent complications, such as anaphylaxis and osteoporosis (24, 27).
A strenght of the study is the recruitment of patients by a multidisciplinary team made up of haematologist, allergist, dermatologist, endocrinologist and gastroenterologist which allowed us to have a heterogeneous population of patients affected by systemic mastocytosis. The retrospective design of the study allowed the inclusion of a relatively large number of patients with SM and pre-SM, which is essential to study a rare disease. The analysis succeeded in identifying subgroups of patients with specific clinical characteristics associated with a higher risk of anaphylaxis, aiding in patient risk stratification and guiding personalized care.
Nonetheless, the study has several limitations inherent to its observational nature. First, the reliance on medical records may have led to incomplete data, potentially affecting the identification of anaphylaxis cases. Second, the lack of a temporal relationship in some records precluded definitive attribution of anaphylaxis to mastocytosis. Third, the rarity of mastocytosis and a single Centre recruitment limited the sample size, which may impact statistical power and generalizability of the findings. Lastly, in the absence of genetic testing, it was not possible to search for HαT, a genetic trait known to increase the risk of severe anaphylaxis when associated with SM and IgE-mediated allergy (1).
Conclusions
Pre-SM and recognized SM are associated with a higher risk of anaphylaxis compared with the general population. Idiopathic anaphylaxis can occur across most subtypes, while specific triggers exhibit peculiar characteristics: Hymenoptera venom is mainly implicated in IgE-mediated anaphylaxis in indolent forms, whereas drug-induced anaphylaxis is more frequent in advSM subtypes, predominantly through IgE-independent mechanisms.
Patients sensitized to Hymenoptera venom or lacking skin lesions need a close allergological monitoring. In fact, the presence of cutaneous lesions is a protective factor in non-advanced forms, while sensitization to Hymenoptera venom is a significant risk factor and should be a central focus of allergological management.
The findings support the need for personalized allergological workup, as anaphylaxis risk varies significantly based on disease subtype and cutaneous involvement.
Future studies should aim to investigate the prevalence of HαT in different SM subtypes to refine allergological risk stratification.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Comitato Etico Territoriale Lombardia 3, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
AS: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. VP: Writing – review & editing. MS: Writing – review & editing. DC: Formal analysis, Writing – review & editing. SS: Writing – review & editing. NM: Supervision, Writing – review & editing. FR: Conceptualization, Methodology, Project administration, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was partially funded by Italian Ministry of Health, Current research IRCCS.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Valent P, Akin C, Sperr WR, Horny HP, Arock M, Metcalfe DD, et al. New insights into the pathogenesis of mastocytosis: emerging concepts in diagnosis and therapy. Annu Rev Pathol. (2023) 18:361–86. doi: 10.1146/annurev-pathmechdis-031521-042618
2. Khoury JD, Solary E, Abla O, Akkari Y, Alaggio R, Apperley JF, et al. The 5th edition of the world health organization classification of haematolymphoid tumours: myeloid and histiocytic/dendritic neoplasms. Leukemia. (2022) 36(7):1703–19. doi: 10.1038/s41375-022-01613-1
3. Schuch A, Brockow K. Mastocytosis and anaphylaxis. Immunol Allergy Clin North Am. (2017) 37(1):153–64. doi: 10.1016/j.iac.2016.08.017
4. Valent P, Sotlar K, Horny HP, Arock M, Akin C. World health organization classification and diagnosis of mastocytosis: update 2023 and future perspectives. Immunol Allergy Clin North Am. (2023) 43(4):627–49. doi: 10.1016/j.iac.2023.04.011
5. Beyens M, Elst J, van der Poorten ML, Van Gasse A, Toscano A, Verlinden A, et al. Mastocytosis and related entities: a practical roadmap. Acta Clin Belg. (2023) 78(4):325–35. doi: 10.1080/17843286.2022.2137631
6. Pardanani A. Systemic mastocytosis in adults: 2023 update on diagnosis, risk stratification and management. Am J Hematol. (2023) 98(7):1097–116. doi: 10.1002/ajh.26962
7. Li JY, Ryder CB, Zhang H, Cockey SG, Hyjek E, Moscinski LC, et al. Review and updates on systemic mastocytosis and related entities. Cancers. (2023) 15(23):5626. doi: 10.3390/cancers152356268
8. Zanotti R, Tanasi I, Crosera L, Bonifacio M, Schena D, Orsolini G, et al. Systemic mastocytosis: multidisciplinary approach. Mediterr J Hematol Infect Dis. (2021) 13(1):e2021068. doi: 10.4084/MJHID.2021.068
9. Gülen T, Ljung C, Nilsson G, Akin C. Risk factor analysis of anaphylactic reactions in patients with systemic mastocytosis. J Allergy Clin Immunol Pract. (2017) 5(5):1248–55. doi: 10.1016/j.jaip.2017.02.008
10. Korošec P, Sturm GJ, Lyons JJ, Marolt TP, Svetina M, Košnik M, et al. High burden of clonal mast cell disorders and hereditary α-tryptasemia in patients who need hymenoptera venom immunotherapy. Allergy. (2024) 79(9):2458–69. doi: 10.1111/all.16084
11. González de Olano D, de la Hoz Caballer B, Núñez López R, Sánchez Muñoz L, Cuevas Agustín M, Diéguez MC, et al. Prevalence of allergy and anaphylactic symptoms in 210 adult and pediatric patients with mastocytosis in Spain: a study of the Spanish network on mastocytosis (REMA). Clin Exp Allergy. (2007) 37(10):1547–55. doi: 10.1111/j.1365-2222.2007.02804.x
12. Gülen T, Hägglund H, Dahlén B, Nilsson G. High prevalence of anaphylaxis in patients with systemic mastocytosis—a single-centre experience. Clin Exp Allergy. (2014) 44(1):121–9. doi: 10.1111/cea.12225
13. Górska A, Niedoszytko M, Lange M, Chełmińska M, Nedoszytko B, Wasąg B, et al. Risk factors for anaphylaxis in patients with mastocytosis. Pol Arch Med Wewn. (2015) 125(1-2):46–53. doi: 10.20452/pamw.2644
14. Brockow K, Jofer C, Behrendt H, Ring J. Anaphylaxis in patients with mastocytosis: a study on history, clinical features and risk factors in 120 patients. Allergy. (2008) 63(2):226–32. doi: 10.1111/j.1398-9995.2007.01569.x
15. Alvarez-Twose I, Zanotti R, González-de-Olano D, Bonadonna P, Vega A, Matito A, et al. Nonaggressive systemic mastocytosis (SM) without skin lesions associated with insect-induced anaphylaxis shows unique features versus other indolent SM. J Allergy Clin Immunol. (2014) 133(2):520–8. doi: 10.1016/j.jaci.2013.06.020
16. Alvarez-Twose I, Matito A. Mastocytosis presenting as insect anaphylaxis: gender differences and natural history. Curr Opin Allergy Clin Immunol. (2019) 19(5):468–74. doi: 10.1097/ACI.0000000000000567
17. Akin C, Scott LM, Kocabas CN, Kushnir-Sukhov N, Brittain E, Noel P, et al. Demonstration of an aberrant mast-cell population with clonal markers in a subset of patients with “idiopathic” anaphylaxis. Blood. (2007) 110(7):2331–3. doi: 10.1182/blood-2006-06-028100
18. Castells M, Butterfield J. Mast cell activation syndrome and mastocytosis: initial treatment options and long-term management. J Allergy Clin Immunol Pract. (2019) 7(4):1097–106. doi: 10.1016/j.jaip.2019.02.002
19. Arber DA, Orazi A, Hasserjian RP, Borowitz MJ, Calvo KR, Kvasnicka HM, et al. International consensus classification of myeloid neoplasms and acute leukemias: integrating morphologic, clinical, and genomic data. Blood. (2022) 140(11):1200–28. doi: 10.1182/blood.2022015850
20. Ballul T, Sabato V, Valent P, Hermine O, Lortholary O, Rossignol J, et al. Characterization of patients with clonal mast cells in the bone marrow with clinical significance not otherwise specified. EClinicalMedicine. (2025) 80:103043. doi: 10.1016/j.eclinm.2024.103043
21. Rama TA, Morgado JM, Henriques A, Escribano L, Alvarez-Twose I, Sanchez-Muñoz L, et al. Mastocytosis presenting with mast cell-mediator release-associated symptoms elicited by cyclo oxygenase inhibitors: prevalence, clinical, and laboratory features. Clin Transl Allergy. (2022) 12(3):e12132. doi: 10.1002/clt2.12132
22. Caimmi S, Crisafulli G, Franceschini F, Liotti L, Bianchi A, Bottau P, et al. Hypersensitivity to intravenous iron preparations. Children. (2022) 9(10):1473. doi: 10.3390/children9101473
23. Niedoszytko M, Gorska A, Brockow K, Bonadonna P, Lange M, Kluin-Nelemans H, et al. Prevalence of hypersensitivity reactions in various forms of mastocytosis: a pilot study of 2485 adult patients with mastocytosis collected in the ECNM registry. Allergy. (2024) 79(9):2470–81. doi: 10.1111/all.16132
24. Sciumè M, Serpenti F, Zanotti R, Bonadonna P, Tanasi I, Crosera L, et al. Comparison between indolent systemic mastocytosis and clonal mast cell disease not meeting WHO diagnostic criteria: a nationwide multicenter retrospective analysis. Hematol Oncol. (2024) 42(3):e3277. doi: 10.1002/hon.3277
25. Pardanani A, Chen D, Abdelrahman RA, Reichard KK, Zblewski D, Wood AJ, et al. Clonal mast cell disease not meeting WHO criteria for diagnosis of mastocytosis: clinicopathologic features and comparison with indolent mastocytosis. Leukemia. (2013) 27(10):2091–4. doi: 10.1038/leu.2013.227
26. Grifoni FI, Sciumè M, Ceparano G, Lavezzari M, Galassi G, Pravettoni V, et al. Demystifying the diagnostic criteria of indolent systemic mastocytosis. Hematol Oncol. (2022) 40(1):122–4. doi: 10.1002/hon.2920
Keywords: anaphylaxis, anaphylaxis risk factors, hymenoptera venom allergy, mast cell disease, pre-diagnostic systemic mastocytosis, systemic mastocytosis
Citation: Sangalli A, Pravettoni V, Sciumè M, Consonni D, Sartorio S, Montano N and Rivolta F (2025) Pre-diagnostic and non-advanced systemic mastocytosis without cutaneous involvement have an increased risk of anaphylaxis. Front. Allergy 6:1681051. doi: 10.3389/falgy.2025.1681051
Received: 6 August 2025; Accepted: 18 September 2025;
Published: 17 October 2025.
Edited by:
Simon Blank, Technical University of Munich and Helmholtz Center Munich, GermanyReviewed by:
Seyed Ali Aghapour, Golestan University of Medical Sciences, IranSimona Percic, National Institute of Public Health, Slovenia
Copyright: © 2025 Sangalli, Pravettoni, Sciumè, Consonni, Sartorio, Montano and Rivolta. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrea Sangalli, YW5kcmVhLnNhbmdhbGxpQHBvbGljbGluaWNvLm1pLml0