 Alexandra Lindsey Djomkam Zune1,2,3†
Alexandra Lindsey Djomkam Zune1,2,3† Charles Ochieng’ Olwal1,2,3†
Charles Ochieng’ Olwal1,2,3† Emmanuel Agbeli1
Emmanuel Agbeli1 Abdoulaye Baniré Diallo1
Abdoulaye Baniré Diallo1 Emmanuella Amoako1
Emmanuella Amoako1 Yaw Bediako1,2*
Yaw Bediako1,2* Lily Paemka1,2,3*
Lily Paemka1,2,3*- 1Yemaachi Biotech, Accra, Ghana
- 2West African Centre for Cell Biology of Infectious Pathogens (WACCBIP), University of Ghana, Accra, Ghana
- 3Department of Biochemistry, Cell and Molecular Biology, College of Basic and Applied Sciences, University of Ghana, Accra, Ghana
Variations in drug-metabolizing enzymes and transporters are associated with adverse drug reactions (ADRs). ADRs to cancer drugs can differ among populations owing to environmental and genetic differences. Due to limited resources and prohibitive costs associated with drug development, African countries rely on cancer drugs developed from non-African genetic backgrounds. Black Africans carry a high burden of ADRs partly because of the use of poorly optimized drugs. Black Africans are the least studied population despite being the most genetically diverse. There is a profound lack of pharmacogenetic studies in Black African populations, necessitating an urgent need for pharmacogenomic studies in Black African populations to optimize dosing and minimize ADRs. Using two common generic cancer drugs, capecitabine and cyclophosphamide, we leveraged the PharmGKB platform and several genomic databases to highlight the need for pharmacogenomic studies in Africa. Our computational approach identifies previously reported and unreported toxicity- and efficacy-associated variants that are overrepresented or underrepresented in Black Africans relative to other ethnicities. These findings suggest that capecitabine and cyclophosphamide may not work optimally and/or may predispose Black Africans to ADRs. This underscores the need for population-based drug screening and development to minimize ADRs and guarantee better treatment outcomes. Since Black Africans are currently underrepresented in genomic studies, African scientists could adopt our low-cost approach to evaluate the suitability of existing drugs for treating diseases. However, in the long term, African scientists must initiate large-scale genomic studies that will drive the discovery of African-tailored drugs and promote the implementation of precision medicine on the continent.
Introduction
Drug response is a complex, multifactorial phenomenon that can be attributed to demographic features, environmental factors, clinical backgrounds, and genetic makeup (Taylor et al., 2020). Given that genetics is the major determinant of drug response, the discipline of ‘pharmacogenomics’ emerged to study the genetic determinants influencing drug metabolism, efficacy and adverse drug reactions (ADRs) across individuals. Pharmacogenomics seeks to guide drug selection, dose selection, and/or prioritize patients for closer monitoring through stratification based on genetic variants. This approach could improve drug efficacy and/or safety. The advent of a patient-tailored approach to drug prescription and monitoring, termed ‘precision medicine,’ has improved patient care (Daly, 2017; Micaglio et al., 2021; van der Wouden et al., 2017) but has yet to be adopted in many low-income countries (LICs).
Differences in response to drugs among patients or populations are often attributed to variations in genes encoding drug-metabolizing enzymes. The most common type of genetic polymorphisms in metabolic enzymes is single nucleotide variants (SNVs), which result from variations in the nucleotide base at a single position in the gene encoding the enzyme (Lee, 2010). Variations in drug response are a major challenge in disease management worldwide. It has been estimated that 25%–50% of patients have an unfavorable response to various drugs (Spear et al., 2001). These variations may result in reduced drug efficacy and/or ADRs. Nearly 15% of all hospital admissions are associated with one or more ADRs (Bouvy et al., 2015; Giardina et al., 2018). Studies have indicated that certain races or ethnicities are more likely to experience ADRs compared to others. For instance, a systematic review reported that Asians, Black Africans and Caucasians are predisposed to anticoagulant-related adverse drug events (ADEs), diabetes agents-related ADEs and opioid-related ADEs, respectively (Baehr et al., 2015). Another study reported that Black Africans and Hispanic have a higher number of platin-associated pharmacogenomic variants associated with toxicity than Caucasians (Jordan et al., 2022). A systematic review by McDowell et al. (2006) reported that Black Africans are three times more likely to experience angioedema compared to non-Blacks when using angiotensin-converting enzyme inhibitors. McDowell and colleagues further noted a doubled risk of intracranial bleeding in Black Africans compared to non-Black people during thrombolytic therapy. The aforementioned reports highlight disparities among races/ethnicities, emphasizing the need for a deeper understanding of the factors underlying varied responses to medications.
Owing to the prohibitive costs and technology associated with drug development, many LICs rely on medications from high-income countries (HICs). However, due to inherent genetic differences among ethnicities, such drugs may be less efficacious or pose serious ADRs when administered to individuals in LICs where the drugs have not been optimized. This view is supported by previous reports, which demonstrated that warfarin dosage responses are largely influenced by ethnicity. For instance, the average daily warfarin doses differ, with individuals of African ancestry requiring the highest daily dose (5.7 mg) to achieve a stable therapeutic international normalized ratio, compared to 5.1 mg in Europeans, 4.4 mg in Latinos, and 3.4 mg in individuals of Asian ancestry (Kaye et al., 2017). Despite the existing evidence on the differences in drug responses across populations, pharmacogenomics remains in its infancy in LICs. This has contributed to severe drug reactions and deaths due to the administration of inappropriate drugs and/or dosage (Mosher et al., 2010; Pinheiro et al., 2016; Schneider et al., 2017; Wright et al., 2014). Among the 300-plus medications with FDA-labeled pharmacogenetic product information and the 100 small molecule-medications with clinical pharmacogenetics guidelines, a review by Radouani et al. (2020) reported that only a few have been studied in African populations. Moreover, despite the continent’s vastness and a population of over 1 billion people, encompassing a wide range of ethnically diverse populations, these drugs have only been investigated in 1–3 studies on average. This highlights a significant gap in knowledge and a pressing need to study drug metabolism and disposition in African populations to optimize dosing and minimize ADRs. This need becomes even more apparent in reviews that emphasize the differences in drug metabolizing enzymes across ethnicities. For example, Rajman et al. (2017) identified CYP alleles (CYP2B6*6, CYP2C8*2, CYP2D6*3, CYP2D6*17, CYP2D6*29, CYP3A5*6, and CYP3A5*7) of potential clinical relevance displaying a marked difference in distribution in Black Africans compared to Asian or Caucasian populations. Consequently, pharmacogenomic screening of Black African patients is crucial to determine their suitability for certain drugs.
The Clinical Pharmacogenetics Implementation Consortium (CPIC) has published more than 100 Level A gene–drug guidelines (Abdullah-Koolmees et al., 2021), with only a few addressing cancer drugs such as capecitabine, a DPYD-guided drug. However, in African settings, capecitabine is administered without genetic testing due to uncharacterized allele frequencies and limited infrastructure (Radouani et al., 2020). Cyclophosphamide, on the other hand, is a provisional Level D drug (i.e., no prescribing action recommended). Due to the low cost of cyclophosphamide and capecitabine, they are widely administered in sub-Saharan Africa to breast, colorectal and lymphoid cancer patients (Baissa et al., 2025; Ahmed et al., 2020; Herbst et al., 2018). Although some population-level differences in ADRs to capecitabine have been documented (Brazelton et al., 2022), the drugs are being used without substantial data on the likelihood of ADRs among Black Africans. To highlight the need for pharmacogenetic testing of drugs, particularly cancer drugs in genomically understudied populations, we compared the allele frequencies of variants associated with capecitabine and cyclophosphamide toxicity and efficacy across four populations. Our low-cost computational analysis uncovered some variants associated with toxicity or efficacy that are under- or over-represented in Black Africans relative to other ethnicities. These findings underscore the need for pharmacogenomic studies on both new and old drugs among Africans to guarantee their efficacy and limit ADRs. Furthermore, this innovative approach could also be extended to other drugs, broadening its applicability and impact.
Methods
Data acquisition
Data for this study were primarily mined from the PharmGKB platform (https://www.pharmgkb.org/), which curates pharmacogenetic data for clinicians and researchers. Using an automated Python script, we first pulled out SNVs associated with capecitabine (Supplementary Table S1) and cyclophosphamide (Supplementary Table S2) toxicity and efficacy. We then downloaded the allele frequencies of the SNVs from major multi-ethnic genomic studies on The National Center for Biotechnology Information (NCBI) as seen in Supplementary Tables S3 and S4). The CSV files downloaded were subsequently loaded into the R software for visualization. In brief, we filtered the PharmGKB datasets (Supplementary Tables S1 and S2) to obtain variants associated with capecitabine and cyclophosphamide toxicity or efficacy. We then annotated the allele frequencies of the toxicity- and efficacy-associated variants from six multi-ethnic studies (i.e., ExAC, gnomAD-Exomes, gnomAD-Genomes, 1,000 Genomes, HapMap, The PAGE Study) from NCBI (Supplementary Tables S3 and S4). Finally, the allele frequencies of the variants across four major ethnicities (i.e., Black Africans, Asians, Caucasians and Hispanics) were visualized as heatmaps and compared statistically. For capecitabine, 166 unique SNVs (i.e., 103 toxicity-associated; 63 efficacy-associated) were extracted. After filtering across the six studies, we identified 160 SNVs: 100 toxicity-associated and 60 efficacy-associated SNVs. All the 160 SNVs had allele frequency data for Black Africans. For cyclophosphamide, 189 unique SNVs (i.e., 147 for toxicity and 42 for efficacy) were retrieved; 180 SNVs remained after filtering across the six studies: 139 and 41 toxicity-associated and efficacy-associated SNVs, respectively. All the 180 SNVs had allele frequency data for Black Africans. The sample sizes of the populations across the six genomic studies are summarized in Table 1.
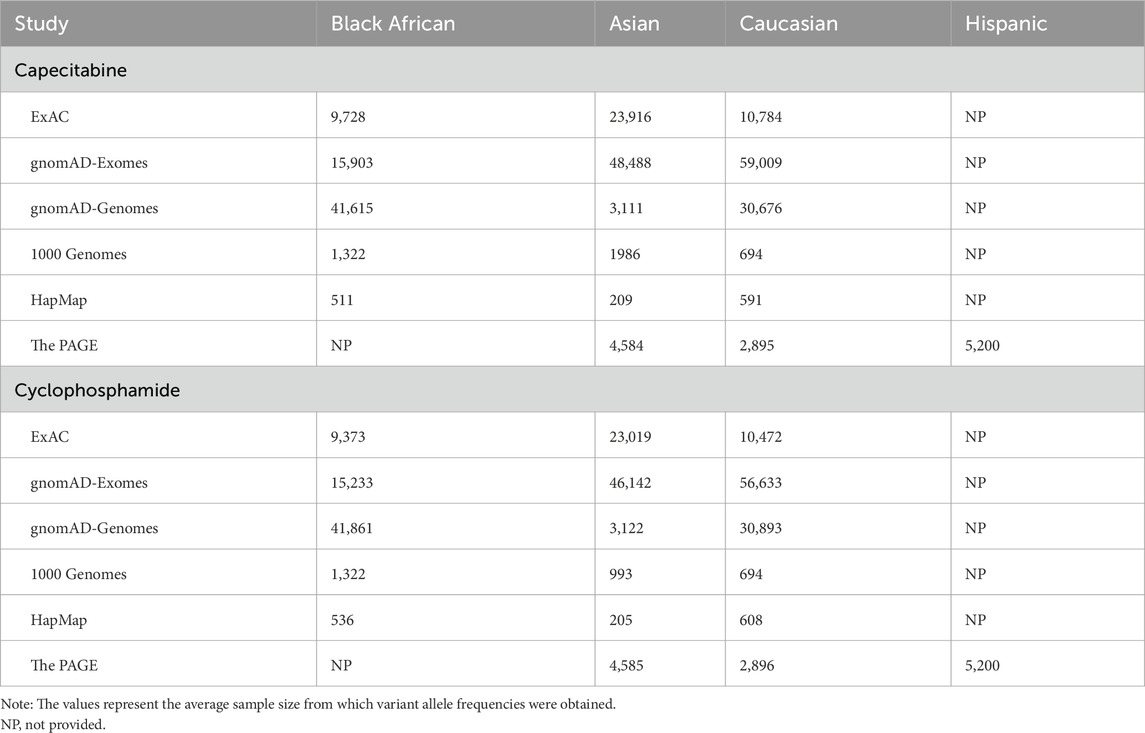
Table 1. Population sample sizes across genomic studies.
Data analysis, visualization and code availability
Bioinformatics analyses were performed primarily using ggplot2 v3.5.2, ComplexHeatmap v2.25.0 packages anchored in R version 4.5.0 (R Development Core Team, Vienna, Austria) and RStudio v2025.5.0.496. Using the Wilcoxon test from the ggsignif package v0.6.4, we statistically compared the allele frequencies of Black Africans versus Asians, Caucasians or Hispanics. A p-value <0.05 was considered significant. Python codes used to extract datasets for the study are available at https://gitfront.io/r/Agbeli/3XCD8Hd3zMGr/precision-medicine/. No custom R codes were used in this study.
Results
Several SNVs associated with capecitabine and cyclophosphamide toxicity are overrepresented in Black Africans
Our initial assessment focused on identifying SNVs associated with capecitabine or cyclophosphamide toxicity in Black Africans, and to compare these findings with other ethnicities. To achieve this, we retrieved variants associated with the toxicity and efficacy of the two drugs curated in PharmGKB (Supplementary Tables S1 and S2; https://www.pharmgkb.org/). From the PharmGKB database, we pulled datasets providing the allele frequencies of variants across ethnicities obtained from major studies including gnomAD, 1000Genomes and ExAC (Supplementary Tables S3 and S4). Our analyses identified several SNVs associated with capecitabine toxicity that are either overrepresented or underrepresented in Black Africans relative to Asians, Caucasians or Hispanics (Figure 1A). Statistical comparisons uncovered certain variants (i.e., XRCC1-rs25487, ERCC1-rs11615, ABCB1-rs1128503, SLC22A7-rs2270860, CDA-rs1048977, DPYD-rs1801265) associated with capecitabine toxicity that were significantly overrepresented in Black Africans compared to the other three ethnicities (Figure 2A). Concerning cyclophosphamide, our analysis also identified several SNVs associated with toxicity that were either overrepresented or underrepresented in Black Africans relative to Asians, Caucasians or Hispanics (Figure 1B). A statistical comparison of the allele frequencies of the variants across ethnicities showed that 10 variants (i.e., ALDH1A1-rs3764435, RAB27A-rs4261468, ABCC1-rs35596, CYP1B1-rs1056836, ABCC1-rs903880, DDX20-rs197388, ERCC1-rs11615, ABCB1-rs2032582, ABCB1-rs1045642, ALDH1A1-rs63319) associated with toxicity were significantly overrepresented in Black Africans compared to the other ethnicities (Figure 2B). Taken together, these findings suggest that Black Africans have a higher predisposition to adverse events associated with capecitabine and/or cyclophosphamide compared to other ethnicities.
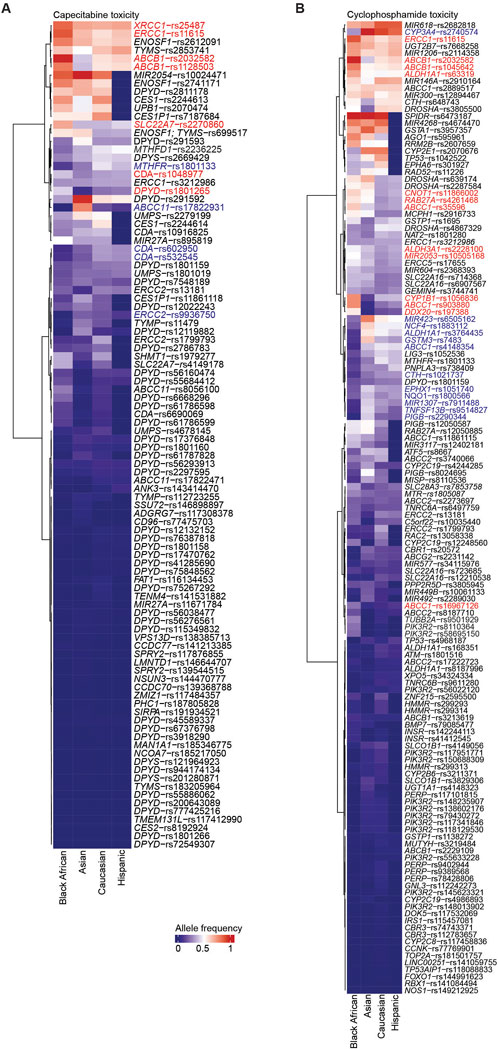
Figure 1. SNVs associated with capecitabine and cyclophosphamide toxicity across ethnicities. Heatmap summarizing the allele frequencies of SNVs associated with capecitabine (A) and cyclophosphamide (B) toxicity across four ethnicities. The values on the heatmap are the median allele frequencies for six genomic studies (i.e., ExAC, gnomAD-Exomes, gnomAD-Genomes, 1,000 Genomes, HapMap, The PAGE Study). The SNVs overrepresented and underrepresented are highlighted in red and blue, respectively. Only variants with allele frequencies across the four populations are highlighted.
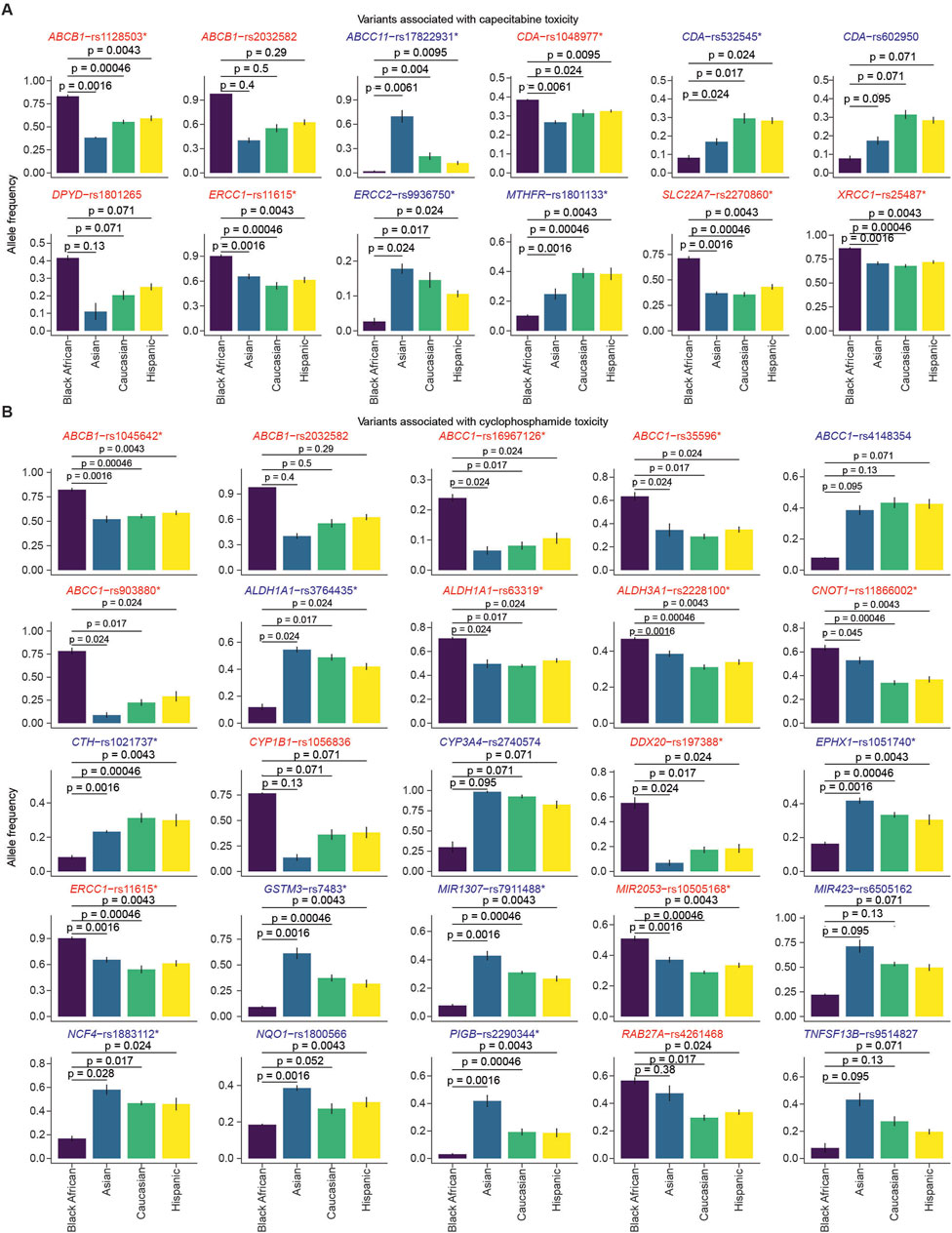
Figure 2. Comparison of allele frequencies of variants associated with capecitabine and cyclophosphamide toxicity across ethnicities. The bar plots show the minor-allele frequencies of SNVs associated with capecitabine (A) and cyclophosphamide (B) toxicity across four ethnic groups (Black African, Asian, Caucasian, Hispanic). Statistical comparison between Black Africans versus each of the three ethnicities was performed using the Wilcoxon test. SNVs that had significantly higher or lower allele frequencies compared to all the other ethnicities are marked with asterisks. The bars represent the mean allele frequencies from the six studies (i.e., ExAC, gnomAD-Exomes, gnomAD-Genomes, 1,000 Genomes, HapMap, The PAGE Study), with error bars indicating the standard error. The SNVs overrepresented and underrepresented are highlighted in red and blue, respectively.
Variants associated with capecitabine and cyclophosphamide efficacy are underrepresented in Black Africans
We next sought to identify SNVs associated with capecitabine or cyclophosphamide efficacy in Black Africans, comparing them to other ethnicities using the same analysis described for toxicity. We identified SNVs associated with capecitabine efficacy that are either overrepresented or underrepresented in Black Africans compared to Asians, Caucasians or Hispanics (Figure 3A). Additionally, statistical comparisons identified four variants (i.e., SLC19A1-rs1051266, SMARCAD1-rs11722476, RRM1-rs9937, AREG-rs11942466) associated with capecitabine efficacy that were significantly underrepresented in Black Africans compared to Asians, Caucasians or Hispanics (Figure 4A).
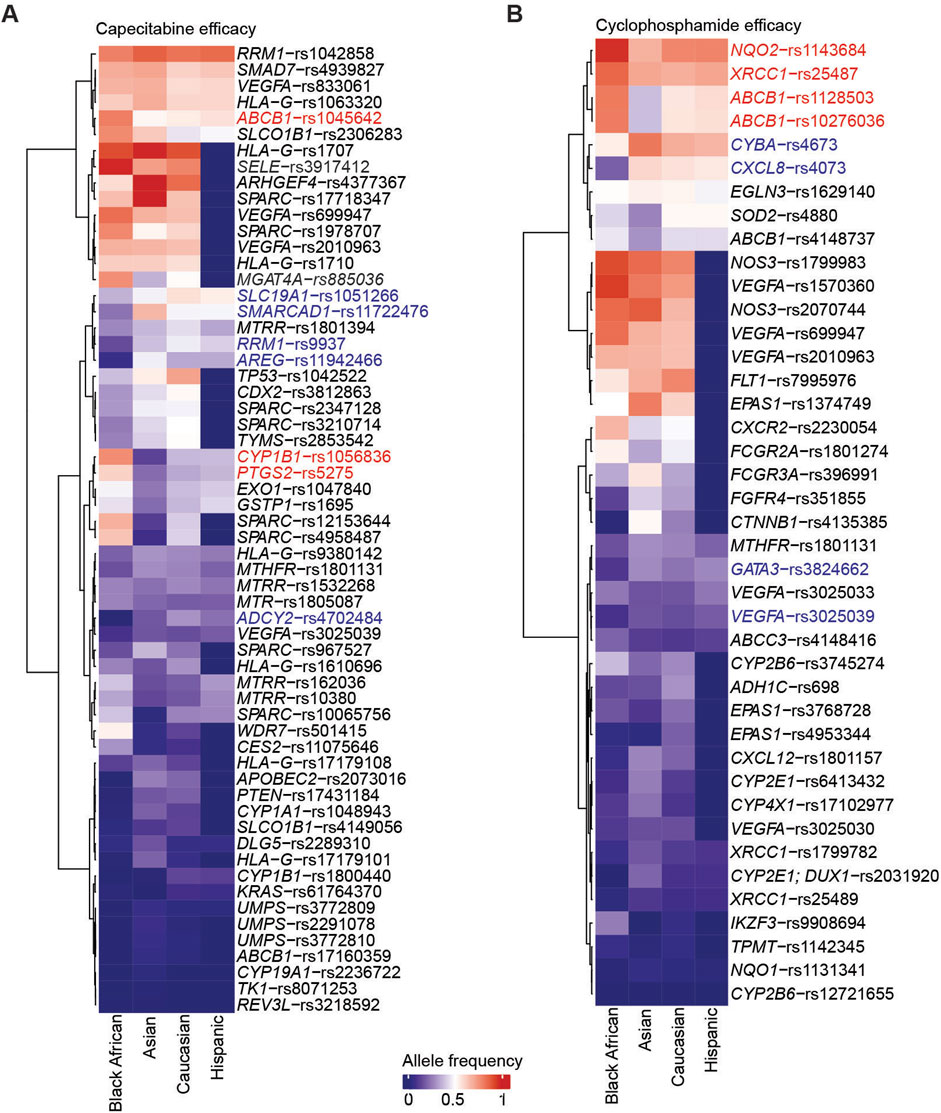
Figure 3. SNVs associated with capecitabine and cyclophosphamide efficacy across ethnicities. Heatmap summarizing the allele frequencies of SNVs associated with capecitabine (A) and cyclophosphamide (B) efficacy across four ethnicities. The values on the heatmap are the median allele frequencies for six genomic studies. The SNVs overrepresented and underrepresented are highlighted in red and blue, respectively. Only variants with allele frequencies across the four populations are highlighted.
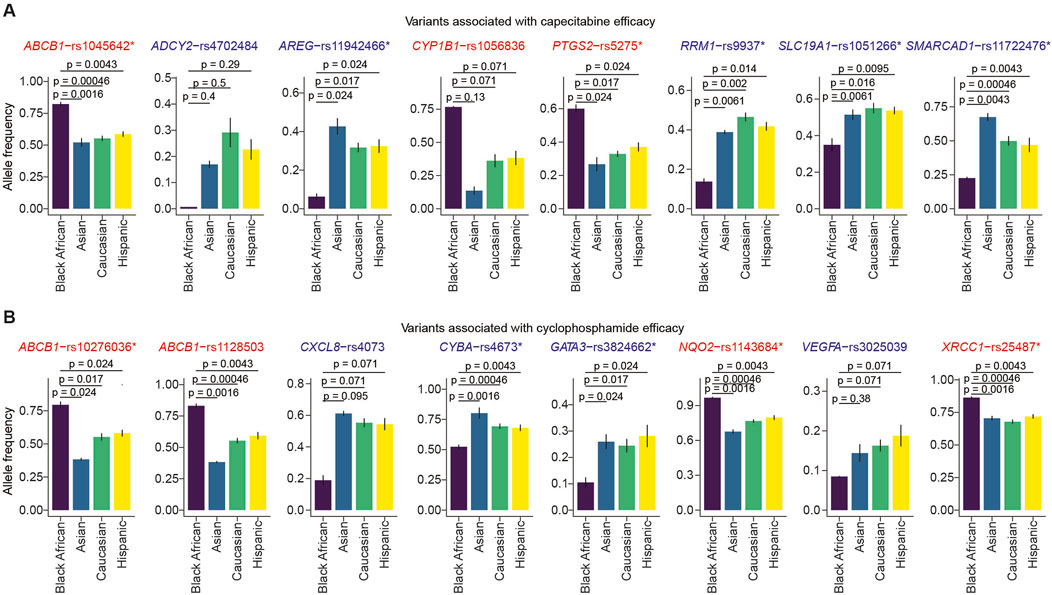
Figure 4. Comparison of allele frequencies of variants associated with capecitabine and cyclophosphamide efficacy across ethnicities. The bar plots show the minor-allele frequencies of SNVs associated with capecitabine (A) and cyclophosphamide (B) efficacy across four ethnic groups (Black African, Asian, Caucasian, Hispanic). Statistical comparison between Black Africans versus each of the three ethnicities was performed using the Wilcoxon test. SNVs with significantly higher or lower allele frequencies compared to the other ethnicities are marked with asterisks. The bars represent the mean allele frequencies from six genomic studies, while error bars depict the standard error. The SNVs overrepresented and underrepresented are highlighted in red and blue, respectively.
Repeating the analysis for cyclophosphamide, we identified SNVs associated with toxicity that were overrepresented or underrepresented in Black Africans relative to Asians, Caucasians or Hispanics (Figure 3B). Statistical comparisons of variant allele frequencies across ethnicities revealed that GATA3-rs3824662 and VEGFA-rs3025039 were significantly underrepresented in Black Africans compared to the other three ethnicities (Figure 4B). Taken together, these findings suggest that capecitabine and/or cyclophosphamide may be less efficacious in Black Africans as certain variants associated with efficacy seem to be underrepresented in this population.
Discussion
Due to Africa’s high genetic diversity and overdependence on drugs from developed countries, individuals of African ancestry are more susceptible to ADR-related challenges. In this brief research report, we present several variants associated with the toxicity or efficacy of two cancer drugs (i.e., capecitabine and cyclophosphamide) commonly administered in African countries (Kizub et al., 2022).
The present study demonstrated that allele frequencies of SNVs associated with capecitabine or cyclophosphamide toxicity vary across ethnicities, predicting differences in ADRs among patients from these ethnic backgrounds. Notably, our bioinformatics analysis indicated that XRCC1-rs25487, ERCC1-rs11615, ABCB1-rs1128503, SLC22A7-rs2270860, CDA-rs1048977 and DPYD-rs1801265, which confer toxicity to capecitabine, are overrepresented in Black Africans. Similarly, we found ALDH1A1-rs3764435, RAB27A-rs4261468, ABCC1-rs35596, CYP1B1-rs1056836, ABCC1-rs903880, DDX20-rs197388, ERCC1-rs11615, ABCB1-rs2032582, ABCB1-rs1045642 and ALDH1A1-rs63319, which are known to confer toxicity to cyclophosphamide to be overrepresented in Black Africans. A previous study conducted in Spain confirmed the link between some of these SNVs (i.e., CDA rs1048977 and SLC22A7 rs2270860) with severe capecitabine toxicity (Pellicer et al., 2017). Another study conducted in Spain also linked ABCB1-rs1128503, rs2032582, and rs1045642 with a high risk of grade >2 diarrhea and overall toxicity upon capecitabine administration for colorectal cancer (Garc et al., 2015). A North American study reported that ABCC1-rs903880, ALDH1A1-rs3764435 and ALDH1A1-rs63319 are associated with severe hematological toxicity after administration of doxorubicin and cyclophosphamide (Yao et al., 2014). Regarding efficacy, several SNVs associated with efficacy to capecitabine (i.e., SLC19A1-rs1051266, SMARCAD1-rs11722476, RRM1-rs9937, AREG-rs11942466) and cyclophosphamide (i.e., GATA3-rs3824662, VEGFA-rs3025039) were underrepresented in Black Africans compared to other ethnicities. The present findings are consistent with previous studies conducted on other drugs. For example, a study associated SLC19A1-rs1051266 with methotrexate efficacy (Eektimmerman et al., 2020). Notably, many of the SNVs identified in our study have not been reported in pharmacogenetic studies. Further investigation is needed to elucidate the impact of these unknown variants on toxicity or efficacy. The SNVs highlighted in this study could serve as potential pharmacogenomic markers for increased ADRs or reduced efficacy.
In the present study, we identified several toxicity-associated (Figures 1, 2) and efficacy-associated (Figures 3, 4) SNVs that are underrepresented and overrepresented in Black Africans. These findings indicate that Black Africans carry certain variants that may reduce toxicity or increase efficacy to capecitabine and/or cyclophosphamide, suggesting a differential response to these drugs among Black Africans. Thus, the blanket administration of these drugs in this population could have serious ramifications. Taken together, our findings underscore the need for pharmacogenetic testing of these variants in Black African patients prior to the administration of specific drugs to avoid severe ADRs and ensure optimal therapeutic benefit.
Due to the substantial resources and extended duration required to conduct pharmacogenomic studies and generate African-tailored drugs, the African continent will continue to depend on drugs developed from genomic studies conducted in other populations. However, as demonstrated in this study, the dependence on such drugs is likely to pose serious health challenges since Black Africans are more genetically diverse and are more likely to carry more variants, including those that predispose them to ADRs. This calls for policymakers and researchers in these genomically underrepresented settings to evaluate the suitability of cancer drugs from the HICs. In this study, we propose an approach for identifying variants that may confer toxicity or efficacy to a drug of interest before its administration to a patient. Our approach could be utilized to identify candidate variants for inclusion in pharmacogenetic screening in low-resource settings. This will ensure that efficacious and less toxic drugs are administered, resulting in better cancer management and reduced ADRs.
In this study, we aimed to highlight the need for pharmacogenetic testing of cancer drugs in genomically understudied populations, such as Africa, by identifying candidate variants unique to Africans for inclusion in pharmacogenetic screening. However, we recognize that this approach may not have an immediate impact on cancer management. Our analysis identified several toxicity- and efficacy-associated variants that had similar allele frequencies across the four populations, indicating an opportunity to utilize existing pharmacogenetic data. Since drug metabolism or pharmacokinetics involve conserved molecular pathways across humans, Africans could benefit from the similarities in allele frequencies of certain variants and adopt pharmacogenetic screening protocols based on guidelines established in HICs. For example, cancer drugs with actionable drug-gene pairs (e.g., CYP2D6-tamoxifen, DPYD-fluoroucil, DPYD-tegafur, UGT1A1-irinotecan, DPYD-capecitabine) could be considered. Rather than focusing on the differential allele frequencies in variants of these genes, Africa could target variants with similar allele frequencies across populations for pharmacogenetic screening before administering drugs like tamoxifen, tegafur, capecitabine, among others. This approach could provide immediate benefits for Africans as they await large-scale genomic studies that will inform the development of African-tailored therapies.
In summary, we performed computational analysis using multi-ethnic genomic data integrated with variants associated with capecitabine and cyclophosphamide toxicity and efficacy. Our analysis identified variants with differing allele frequencies in Black Africans compared to other populations, some of which may predispose Black Africans to capecitabine and cyclophosphamide-associated ADRs. Additionally, we identified several variants with similar allele frequencies across the four populations. Variants with unique allele frequencies in Africans could be prioritized for pharmacogenetic testing in this population. For immediate impact and to address the growing burden of cancers, African countries could also focus on pharmacogenetic screening of variants with similar allele frequencies, leveraging well-established guidelines from HICs. Both strategies will ensure that African cancer patients receive less toxic and more efficacious drugs. Even though our conclusions may be limited by the imbalanced sample sizes across populations, our study provides a low-budget approach through which many of the drugs developed in non-Africans could be screened for use, not only in Black Africans but also in other LICs, to identify possible markers for drug toxicity and efficacy. However, in the long term, it is imperative to conduct large-scale pharmacogenomic studies among Black populations to address the existing knowledge gap and pave the way for African-tailored cancer therapies and drive the advancement of personalized treatments for cancer and other terminal diseases.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
AD: Formal Analysis, Investigation, Methodology, Software, Visualization, Writing – original draft. CO: Formal Analysis, Investigation, Methodology, Software, Visualization, Writing – original draft. EAg: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Writing – review and editing. AB: Writing – review and editing. EAm: Writing – review and editing. YB: Conceptualization, Project administration, Resources, Supervision, Writing – review and editing. LP: Conceptualization, Investigation, Methodology, Project administration, Supervision, Writing – review and editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
Authors AD, CO, EAg, AB, EAm, YB, and LP were employed by company Yemaachi Biotech.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fbinf.2025.1555637/full#supplementary-material
References
Abdullah-Koolmees, H., van Keulen, A. M., Nijenhuis, M., and Deneer, V. H. M. (2021). Pharmacogenetics guidelines: overview and comparison of the DPWG, CPIC, CPNDS, and RNPGx guidelines. Front. Pharmacol. 11, 595219. doi:10.3389/fphar.2020.595219
Ahmed, J. H., Makonnen, E., Bisaso, R. K., Mukonzo, J. K., Fotoohi, A., Aseffa, A., et al. (2020). Population pharmacokinetic, pharmacogenetic, and pharmacodynamic analysis of cyclophosphamide in Ethiopian breast cancer patients. Front. Pharmacol. 11, 406. doi:10.3389/fphar.2020.00406
Baehr, A., Peña, J. C., and Hu, D. J. (2015). Racial and ethnic disparities in adverse drug events: a systematic review of the literature. J. Racial Ethn. Health Disparities 2 (4), 527–536. doi:10.1007/s40615-015-0101-3
Baissa, O. T., Ben-Shushan, T., and Paltiel, O. (2025). Lymphoma in Sub-Saharan Africa: a scoping review of the epidemiology, treatment challenges, and patient pathways. Cancer Causes Control 36 (3), 199–230. doi:10.1007/s10552-024-01922-z
Bouvy, J. C., De Bruin, M. L., and Koopmanschap, M. A. (2015). Epidemiology of adverse drug reactions in Europe: a review of recent observational studies. Drug Saf. 38 (5), 437–453. doi:10.1007/s40264-015-0281-0
Brazelton, A., Yande, S., Pope, R., Johnson, M. L., Musher, B., and Trivedi, M. V. (2022). Racial and ethnic differences in capecitabine toxicity in patients with gastrointestinal tract cancers. Ann. Gastroenterol. 35 (2), 182–186. doi:10.20524/aog.2022.0688
Daly, A. K. (2017). Pharmacogenetics: a general review on progress to date. Br. Med. Bull. 124 (1), 65–79. doi:10.1093/bmb/ldx035
Eektimmerman, F., Swen, J. J., Madhar, M. B., Allaart, C. F., and Guchelaar, H. J. (2020). Predictive genetic biomarkers for the efficacy of methotrexate in rheumatoid arthritis: a systematic review. Pharmacogenomics J. 20 (2), 159–168. doi:10.1038/s41397-019-0098-9
García-González, X., Cortejoso, L., García, M. I., García-Alfonso, P., Robles, L., Grávalos, C., et al. (2015). Variants in CDA and ABCB1 are predictors of capecitabine-related adverse reactions in colorectal cancer. Oncotarget 6 (8), 6422–6430. doi:10.18632/oncotarget.3289
Giardina, C., Cutroneo, P. M., Mocciaro, E., Russo, G. T., Mandraffino, G., Basile, G., et al. (2018). Adverse drug reactions in hospitalized patients: results of the FORWARD (facilitation of reporting in hospital ward) study. Front. Pharmacol. 9, 350. doi:10.3389/fphar.2018.00350
Herbst, C. lee, Miot, J. K., Moch, S. L., and Ruff, P. (2018). Access to colorectal cancer (CRC) chemotherapy and the associated costs in a South African public healthcare patient cohort. J. Cancer Policy 15, 18–24. doi:10.1016/j.jcpo.2017.11.005
Jordan, I. K., Sharma, S., Nagar, S. D., and Mariño-Ramírez, L. (2022). The apportionment of pharmacogenomic variation: race, ethnicity, and adverse drug reactions. Med. Res. Arch. 10 (9). doi:10.18103/mra.v10i9.2986
Kaye, J. B., Schultz, L. E., Steiner, H. E., Kittles, R. A., Cavallari, L. H., and Karnes, J. H. (2017). Warfarin pharmacogenomics in diverse populations. Pharmacother. J. Hum. Pharmacol. Drug Ther. 37 (9), 1150–1163. doi:10.1002/phar.1982
Kizub, D. A., Naik, S., Abogan, A. A., Pain, D., Sammut, S., Shulman, L. N., et al. (2022). Access to and affordability of World Health Organization essential medicines for cancer in Sub-Saharan Africa: examples from Kenya, Rwanda, and Uganda. Oncol. 27 (11), 958–970. doi:10.1093/oncolo/oyac143
Lee, N. H. (2010). Pharmacogenetics of drug metabolizing enzymes and transporters: effects on pharmacokinetics and pharmacodynamics of anticancer agents. Anticancer Agents Med. Chem. 10 (8), 583–592. doi:10.2174/187152010794474019
McDowell, S. E., Coleman, J. J., and Ferner, R. E. (2006). Systematic review and meta-analysis of ethnic differences in risks of adverse reactions to drugs used in cardiovascular medicine. BMJ 332 (7551), 1177–1181. doi:10.1136/bmj.38803.528113.55
Micaglio, E., Locati, E. T., Monasky, M. M., Romani, F., Heilbron, F., and Pappone, C. (2021). Role of pharmacogenetics in adverse drug reactions: an update towards personalized medicine. Front. Pharmacol. 12, 651720. doi:10.3389/fphar.2021.651720
Mosher, C. E., DuHamel, K. N., Egert, J., and Smith, M. Y. (2010). Self-efficacy for coping with cancer in a multiethnic sample of breast cancer patients: associations with barriers to pain management and distress. Clin. J. Pain 26 (3), 227–234. doi:10.1097/ajp.0b013e3181bed0e3
Pellicer, M., García-González, X., García, M. I., Robles, L., Grávalos, C., García-Alfonso, P., et al. (2017). Identification of new SNPs associated with severe toxicity to capecitabine. Pharmacol. Res. 120, 133–137. doi:10.1016/j.phrs.2017.03.021
Pinheiro, L. C., Samuel, C. A., Reeder-Hayes, K. E., Wheeler, S. B., Olshan, A. F., and Reeve, B. B. (2016). Understanding racial differences in health-related quality of life in a population-based cohort of breast cancer survivors. Breast Cancer Res. Treat. 159 (3), 535–543. doi:10.1007/s10549-016-3965-y
Radouani, F., Zass, L., Hamdi, Y., Rocha, J., Sallam, R., Abdelhak, S., et al. (2020). A review of clinical pharmacogenetics studies in African populations. Pers. Med. 17 (2), 155–170. doi:10.2217/pme-2019-0110
Rajman, I., Knapp, L., Morgan, T., and Masimirembwa, C. (2017). African genetic diversity: implications for cytochrome P450-mediated drug metabolism and drug development. EBioMedicine 17, 67–74. doi:10.1016/j.ebiom.2017.02.017
Schneider, B. P., Shen, F., Jiang, G., O’Neill, A., Radovich, M., Li, L., et al. (2017). Impact of genetic ancestry on outcomes in ECOG-ACRIN-5103. JCO Precis. Oncols. 1, 1–9. doi:10.1200/PO.17.00059
Spear, B. B., Heath-Chiozzi, M., and Huff, J. (2001). Clinical application of pharmacogenetics. Trends Mol. Med. 7 (5), 201–204. doi:10.1016/s1471-4914(01)01986-4
Taylor, C., Crosby, I., Yip, V., Maguire, P., Pirmohamed, M., and Turner, R. M. (2020). A review of the important role of CYP2D6 in pharmacogenomics. Genes 11 (11), 1295. doi:10.3390/genes11111295
van der Wouden, C. H., Cambon-Thomsen, A., Cecchin, E., Cheung, K. C., Dávila-Fajardo, C. L., Deneer, V. H., et al. (2017). Implementing pharmacogenomics in Europe: design and implementation strategy of the ubiquitous pharmacogenomics consortium. Clin. Pharmacol. Ther. 101 (3), 341–358. doi:10.1002/cpt.602
Wright, J. L., Takita, C., Reis, I. M., Zhao, W., Lee, E., and Hu, J. J. (2014). Racial variations in radiation-induced skin toxicity severity: data from a prospective cohort receiving postmastectomy radiation. Int. J. Radiat. Oncol. Biol. Phys. 90 (2), 335–343. doi:10.1016/j.ijrobp.2014.06.042
Yao, S., Sucheston, L. E., Zhao, H., Barlow, W. E., Zirpoli, G., Liu, S., et al. (2014). Germline genetic variants in ABCB1, ABCC1, and ALDH1A1 and risk of hematological and gastrointestinal toxicities in a SWOG phase III trial S0221 for breast cancer. Pharmacogenomics J. 14 (3), 241–247. doi:10.1038/tpj.2013.32
Keywords: precision medicine, capecitabine, cyclophosphamide, pharmacogenomics, drug metabolizing enzymes
Citation: Djomkam Zune AL, Olwal CO, Agbeli E, Diallo AB, Amoako E, Bediako Y and Paemka L (2025) Precision medicine on a budget in Africa: using existing genetic data to mitigate adverse drug reactions to conventional cancer drugs. Front. Bioinform. 5:1555637. doi: 10.3389/fbinf.2025.1555637
Received: 05 January 2025; Accepted: 23 July 2025;
Published: 14 August 2025.
Edited by:
Fernanda Rodrigues-Soares, Universidade Federal do Triângulo Mineiro, BrazilReviewed by:
Martha Sosa-Macías, National Polytechnic Institute (IPN), MexicoTracey Hurrell, Council for Scientific and Industrial Research (CSIR), South Africa
Copyright © 2025 Djomkam Zune, Olwal, Agbeli, Diallo, Amoako, Bediako and Paemka. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lily Paemka, bGlseUB5ZW1hYWNoaS5jb20=; Yaw Bediako, eWF3QHllbWFhY2hpLmNvbQ==
†These authors have contributed equally to this work