 Christine Elisabete Rubio Alem†
Christine Elisabete Rubio Alem† Bárbara Narciso Duarte†
Bárbara Narciso Duarte† Ana Elisa Ribeiro da Silva Cabello†Sandra Regina Campos Teixeira†Thiago Gaspar†Márcio Lopes de Souza†Cesar Cabello*†
Ana Elisa Ribeiro da Silva Cabello†Sandra Regina Campos Teixeira†Thiago Gaspar†Márcio Lopes de Souza†Cesar Cabello*†- Department of Obstetrics and Gynecology, Faculty of Medical Sciences, State University of Campinas (UNICAMP), FCM/UNICAMP, Campinas, São Paulo, Brazil
Introduction: Breast cancer is the most common malignant neoplasm among women in Brazil, excluding non-melanoma skin cancers, with a significant proportion of hereditary cases associated with pathogenic or likely pathogenic germline variants (PV/LPV) in various genes. The increased use of multigene panels to identify these PV/LPV has been recommended but highlights the challenge of detecting variants of uncertain significance (VUS), which complicate genetic counseling and clinical management.
Objective: To evaluate epidemiological and reproductive aspects, as well as the size of different germline multigene panels that may influence the proportion of VUS detections.
Materials and methods: A cross-sectional study was conducted with rigorous inclusion criteria, encompassing women with personal or family history relevant to hereditary breast cancer from November 2021 to October 2022 at the High-Risk Outpatient Clinic, of the Women's Hospital Prof. José Aristodemo Pinotti—CAISM, University of Campinas (UNICAMP). Selection was based on the NCCN 2022 criteria. Samples were analyzed using next-generation sequencing (NGS), focusing on 144 genes associated with hereditary syndromes. The following statistical tests were applied: Chi-Square, Fisher's Exact, Kruskal–Wallis, Bowker, McNemar, and Stepwise logistic regression. Significance level was set at p < 0.05.
Results: Among the 364 patients analyzed, 51 (14%) presented benign or likely benign results, while 313 (86%) showed alterations, including VUS and PV/LPV. The prevalence of VUS was high, particularly in the ATM gene. Univariate and multivariate logistic regression analyses detected no associations between the presence of VUS and reproductive or epidemiological variables. The 144-gene panel identified a higher number of VUS compared to the 20- or 23-gene panels: 56.3 vs. 23.9, and 31%, respectively (p < 0.001; p < 0.001).
Conclusion: The findings underscore the importance of panel size in the identification of PV/LPV vs. VUS. Most patients presented VUS, with the ATM gene being the most affected. None of the reproductive or epidemiological variables studied were associated with the presence of VUS across all groups. While the extended 144-gene panel significantly increased the detection of VUS compared to smaller panels (20–23 genes), it did not substantially improve the identification rate of PV/LPV, highlighting the need to improve genetic panels, especially for genetically diverse populations like the Brazilian population.
1 Introduction
Breast cancer is the most common malignant neoplasm among women, excluding non-melanoma skin cancers, both in Brazil and worldwide. In 2021, 18,134 deaths due to breast cancer were recorded in Brazil, with an estimated 73,630 new cases predicted for 2023–2025 (1). Additionally, in Brazil, breast cancer is often diagnosed at a younger age and in more advanced stages compared to populations from developed countries (2).
Between 10 and 36% of breast cancer cases are hereditary, with ~50% of hereditary breast cancers associated with pathogenic or likely pathogenic germline variants (PV/LPV) in high-penetrance genes, such as BRCA1 and BRCA2, which confer a lifetime relative risk of at least fourfold. Intermediate-penetrance genes, such as ATM, BARD1, PALB2, and CHEK2, present a relative risk of two to fourfold, leaving a considerable proportion of heritability unexplained by low-penetrance variants or single-nucleotide variant associations (3–5).
Multigene panels are increasingly used to manage breast cancer susceptibility in high-risk individuals suspected of hereditary breast cancer, yet evidence-based practical guidelines remain far from comprehensive. The advent of next-generation sequencing (NGS) technologies has made multigene panel testing more accessible (6, 7). Furthermore, multigene panel testing can identify up to 50% more individuals with genetic cancer susceptibility mutations compared to testing exclusively for BRCA1 and BRCA2 (8).
Another important point is that patients may benefit from appropriate screening, more targeted treatments, as well as genetic counseling for themselves and their family members. The identification of PV/LPV in these populations would allow for more effective primary, secondary, and tertiary prevention measures, with the potential to save lives. An important example is demonstrated by the study of Duarte et al. (4) conducted in a Brazilian high-risk population for breast cancer and users of the public healthcare system, which observed a change in behavior regarding the desire for risk-reducing mastectomy following genetic testing and counseling.
As panels expand to identify more PV/LPV, evidence also suggests an increase in the detection of VUS, with a roughly linear relationship between the amount of DNA analyzed and the number of VUS identified (9). This trend is especially evident in understudied populations, such as those in Latin America. For instance, a recent Colombian study involving 769 high-risk individuals with solid tumors reported that while 26% carried pathogenic or likely pathogenic variants, 42% had one or more VUS, highlighting both the genetic heterogeneity of the region and the challenges associated with interpreting such findings (10). In addition to panel size, studies indicate that Hispanic, African American, and Asian populations exhibit higher rates of VUS compared to individuals of European ancestry (11).
VUS are genetic variants with unclear implications for gene function, posing challenges for clinical practice. It is uncertain whether they are clinically causal, potentially actionable, or benign (12). Interpreting these variants is a challenge for clinicians managing genetic counseling and cancer surveillance in families suspected of hereditary cancer syndromes, leading to confusion and anxiety among patients and professionals (13).
A frequently overlooked consequence of this approach is the identification of incidental findings, that is, PV/LPV in genes unrelated to the clinical phenotype that prompted the genetic testing (14). These findings can pose ethical, clinical, and psychological challenges for both healthcare professionals and patients, requiring appropriate genetic counseling to interpret and manage such information.
Therefore, it is essential to acknowledge incidental findings as a potential outcome of using expanded gene panels, which underscores the importance of careful gene selection and thorough pre-test discussions with patients regarding possible results and their implications (15).
In a country like Brazil, where access to genetic testing is significantly limited, our objective is to determine the ideal size of multigene panels for hereditary cancer to maximize the detection of PV/LPV while reducing the occurrence of VUS. This study aims to investigate this critical question.
2 Materials and methods
2.1 Study design and setting
This cross-sectional study was conducted at the Women's Hospital Prof. Dr. José Aristodemo Pinotti—CAISM, within the High-Risk Outpatient Clinic of the Department of Obstetrics and Gynecology, State University of Campinas (UNICAMP), from November 2021 to October 2022.
A convenience sample of 373 women at high risk for hereditary breast cancer was recruited. Inclusion criteria followed the 2022 NCCN guidelines and included: personal history of luminal or HER2-positive breast cancer diagnosed before age 45, with at least one first- or second-degree relative with breast, ovarian, and/or prostate cancer; personal history of triple-negative breast cancer diagnosed before age 60, with family history as above; individuals meeting NCCN high-risk criteria regardless of diagnosis; individuals without a personal cancer diagnosis but with a strong family history as defined.
Of 373 eligible participants, 364 were included in the final analysis after excluding 9 patients with cancer who were lost to follow-up. The analytic sample included 179 patients with cancer and 185 without cancer.
The study was approved by the Research Ethics Committee (CAAE: 54179621.1.0000.5404). All participants provided informed consent. Study procedures were explained in person, and participants signed two consent forms: one for the CAISM Biobank and one for the high-risk research project.
Participants completed a structured questionnaire (via REDCap platform), including sociodemographic variables (e.g., age, ethnicity), clinical history (e.g., BMI, comorbidities, gynecological and cancer history), and family cancer history (type and age at diagnosis).
2.2 Genetic testing and laboratory analysis
Blood samples (20 ml) were collected in EDTA tubes and processed at Eurofins Scientific Genome Center. Next-generation sequencing (NGS) was performed according to ACMG guidelines, including all coding and flanking intronic regions and CNV detection in 144 genes related to hereditary cancer syndromes. MLPA was applied as needed. Only PV, LPV, and VUS were reported. Benign (BV) and likely benign variants (LBV) were not included in the final analysis.
2.3 Return of results and genetic counseling
In a second phase, participants received their test results in person from trained members of the research team. Individualized genetic counseling and follow-up guidance were provided.
2.4 Panel construction and comparison strategy
Three gene panels were evaluated:
• 20-gene panel: based on our group's previous findings (4), including genes with identified PV/LPV.
• 23-gene panel: Based on Guindalini et al. (5), who analyzed 1,663 Brazilian patients using multigene testing.
• 144-gene panel: the full panel used in this study (4).
The 20-gene panel was derived from genes in which PV/LPV were detected in our current cohort, while the 23-gene panel was based on the study by Guindalini et al. (5), which identified clinically relevant variants in one of the largest Brazilian cohorts studied to date. Thus, the construction of both panels was based on real-world findings rather than purely theoretical or syndromic criteria.
The description of the genes included in each panel is provided in the Supplementary material.
2.5 Statistical analysis
Categorical variables were analyzed using Chi-square or Fisher's exact test (when expected values < 5). Numerical variables were assessed using Mann–Whitney or Kruskal–Wallis tests due to non-normal distribution. Associations with VUS were evaluated using univariate and multivariate logistic regression (stepwise selection), reporting odds ratios (OR) with 95% confidence intervals. Comparisons across panel sizes were performed using: Bowker's test for categorical variables with ≥3 categories and McNemar's test for binary comparisons within the same sample. Significance was set at p < 0.05. Analyses were conducted using SAS System for Windows, version 9.4 (SAS Institute Inc.) (16–22).
The dataset used in this study is publicly available at the State University of Campinas data repository (Reduc): https://redu.unicamp.br/.
3 Results
The percentage of patients with VUS was 62% in those without cancer and 51% in patients with a previous history of breast cancer (p = 0.801; Figure 1). Detailed information regarding the identified VUS can be found in Supplementary Material.
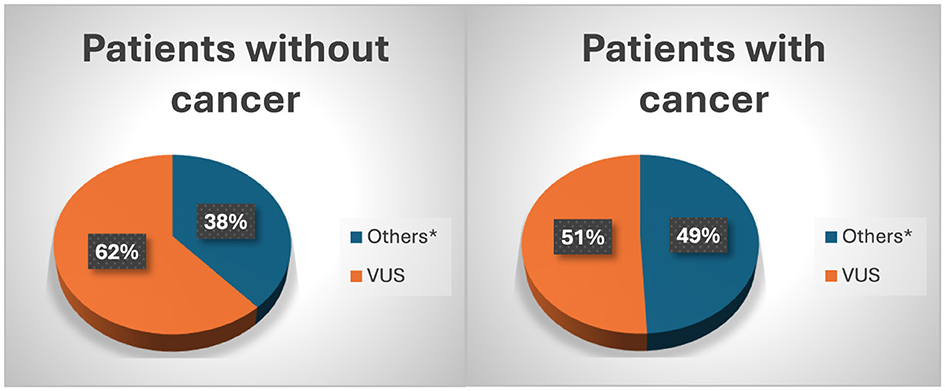
Figure 1. Distribution VUS in patients with or without breast cancer (4). *Others: PV/LPV/BV/LBV. Chi-square test: X2 = 8.78; df = 2; p = 0.801.
Regarding variant prevalence, we observed that both in the group of patients with cancer and in those without a cancer diagnosis, there was a higher frequency of PV and LPV in the BRCA1, BRCA2, TP53, PALB2, and MUTYH genes. In the analysis of VUS, the ATM gene exhibited the highest number of variants in both groups, with 12 variants identified in individuals without cancer and 10 in those with cancer, totaling 22 variants. Other genes with a high prevalence of VUS in both groups included FANCA (seven variants in patients without cancer and six in patients with cancer, totaling 13) and SLX4 (six variants in patients without cancer and seven in patients with cancer; Figure 2).
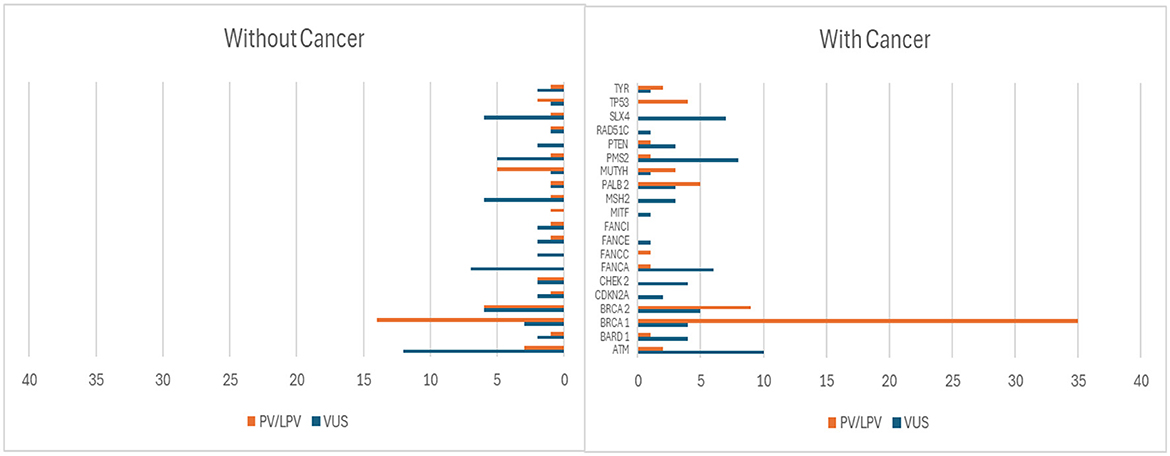
Figure 2. Distribution of PV/LPV and VUS in patients with and without breast cancer.
Regarding the presence of VUS, 27.19% did not show any variant. The number of VUS was similar in the groups with and without breast cancer, with one or more variants found in 73.51% of patients without cancer and 72.07% of patients with breast cancer (p = 0.688; Table 1).
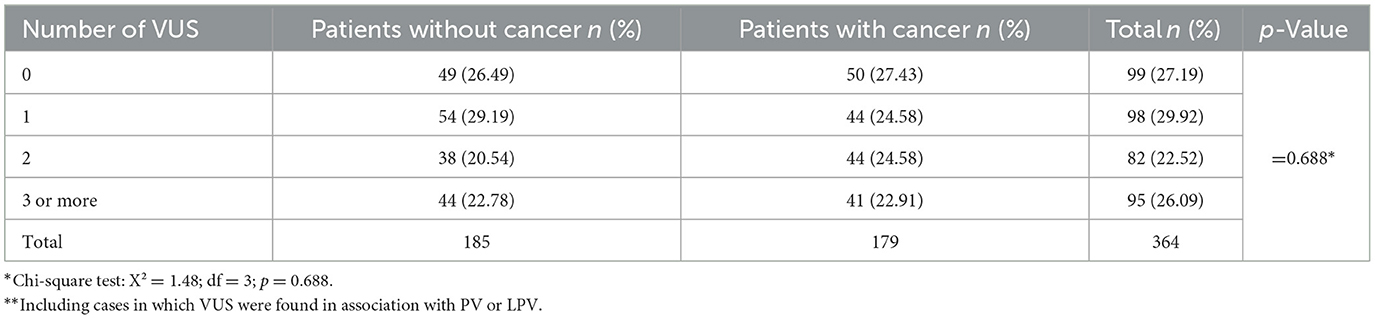
Table 1. Distribution of VUS** in patients with and without breast cancer.
According to the results of the univariate and multivariate logistic regression analyses (using the stepwise variable selection criterion) to study the factors associated with the genetic test results of BV/LBV vs. VUS, no variable was selected as significantly associated with the test result showing VUS. For this analysis, we included 205 cases with VUS and 51 with BV/LBV (Table 2).
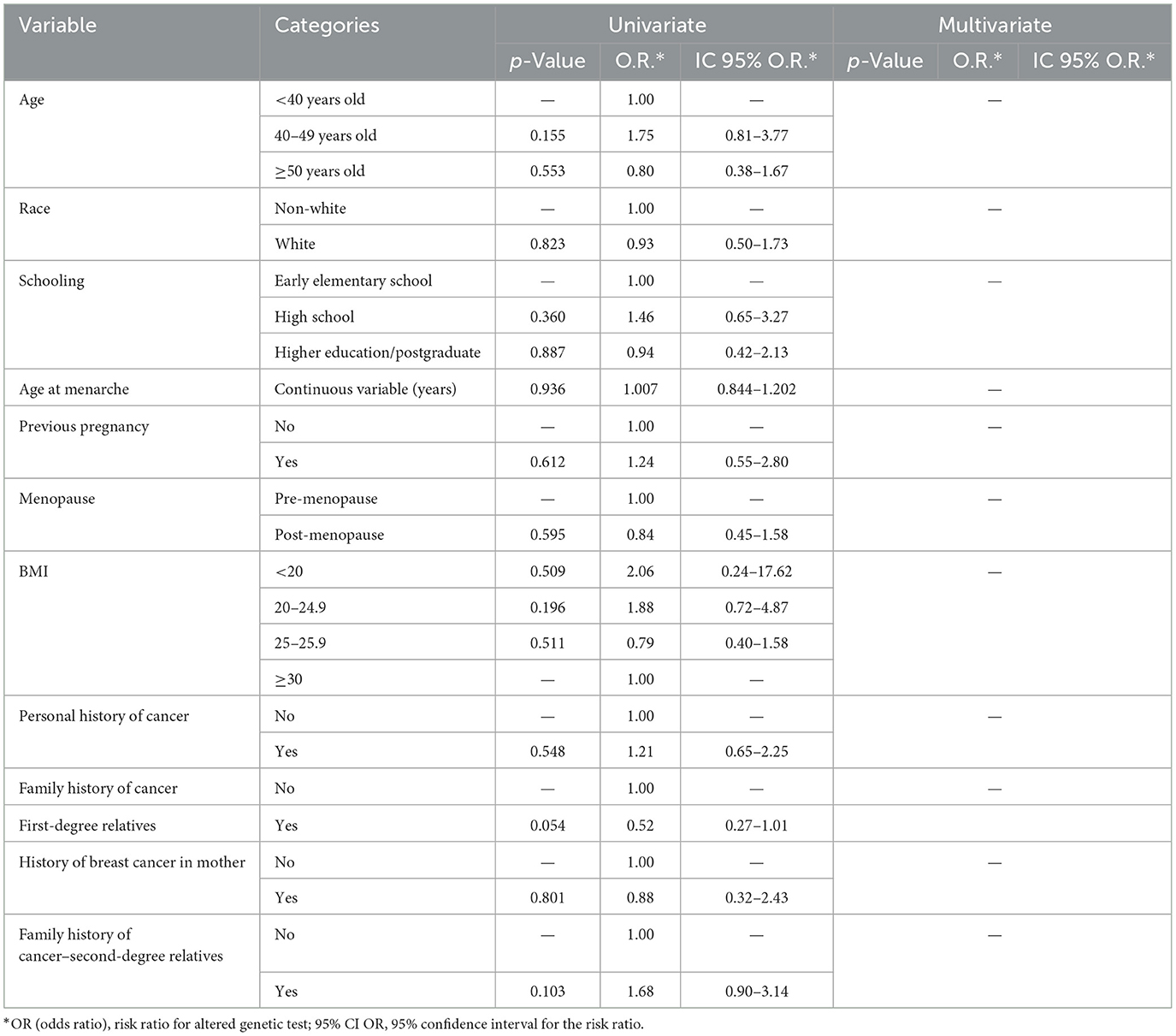
Table 2. Univariate and multivariate analysis of the presence of VUS according to clinical characteristics (n = 256)*.
We conducted a comparison between 20-gene, 23-gene, and 144-gene panels, as described in Section 2.
The analysis revealed differences among the panel sizes evaluated. When comparing the 20-gene panel to the 23-gene panel, a higher frequency of PV/LPV was observed in the 20-gene panel, whereas the 23-gene panel showed a higher frequency of VUS. In the comparison between the 20-gene and 144-gene panels, the 20-gene panel demonstrated a higher frequency (BV/LBV), while the 144-gene panel exhibited a significantly higher frequency of VUS. Finally, comparing the 23-gene and 144-gene panels, the 23-gene panel showed a higher frequency of BV/LBV, whereas the 144-gene panel had higher frequencies of both VUS and PV/LPV (Table 3).
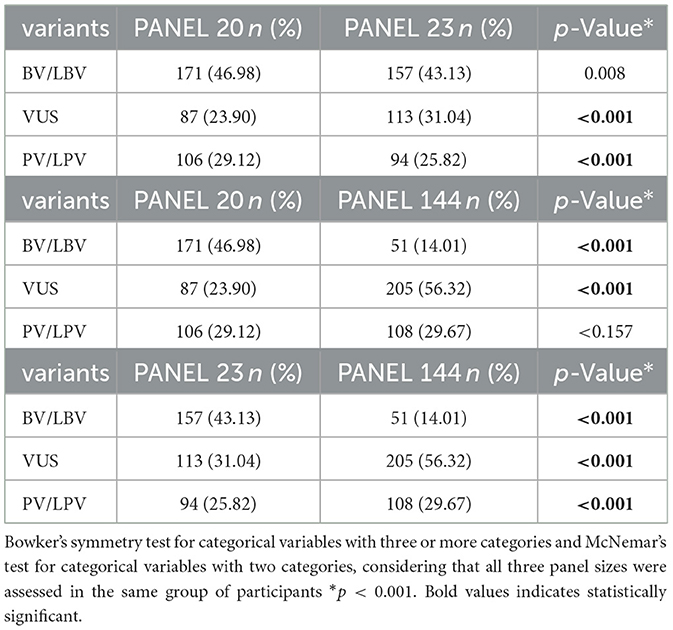
Table 3. Comparison between the sizes of the 20, 23, and 144 gene panels and the presence of BV, LBV, VUS, LPV, and PV.
It is important to emphasize that the slight difference in the number of PV/LPV cases between the two panels 20 × 144-gene (106 for the 20-gene panel vs. 108 for the 144-gene panel) can be explained by the fact that the 20-gene panel includes only a selected subset of genes in which PV/LPV were most frequently observed. Although all individuals in the cohort were analyzed using the 144-gene panel, only variants identified in the 20 selected genes were considered in the analysis of the smaller panel. Consequently, two PV/LPV cases found in genes outside this 20-gene subset are not counted in the 20-gene panel results, leading to the observed discrepancy.
4 Discussion
Our study investigated important aspects related to the prevalence of VUS in patients with and without breast cancer, selected based on high risk for hereditary factors in a Brazilian public health population.
Some previously presented data from our group observed a higher prevalence of PV and LPV in the genes BRCA1, BRCA2, TP53, PALB2, in both the breast cancer and non-breast cancer groups, which reflects the pattern found in other studies that identify these genes as highly relevant in the context of hereditary breast cancer predisposition (4, 5).
PV/LPV in the BRCA1 and BRCA2 genes remain the most studied and are widely associated with hereditary breast and ovarian cancer. The cumulative risk of developing breast cancer for carriers of variants in BRCA1 is between 55 and 72%, while for BRCA2, this risk ranges from 45 to 69% (23).
A high number of VUS was observed, particularly in the ATM gene, followed by FANCA and SLX4. Variants in the ATM gene are of special interest because ATM plays a crucial role in DNA repair, and its deleterious variants can increase the risk of breast cancer, although with lower penetrance compared to BRCA1 and BRCA2 (24).
Regarding the number of VUS, our study found similar numbers in both the breast cancer and non-breast cancer groups, with one or more variants found in 73.51% of the non-cancer patients and 72.07% of the cancer patients, with no statistically significant difference between the groups.
Several studies have reported higher rates of VUS among racial and ethnic minority populations, largely due to their underrepresentation in genomic reference databases. A study investigating genetic testing patterns and clinical outcomes of patients stratified by race/ethnicity found higher VUS rates in minorities compared to non-white, non-Hispanic people (25). Herzog et al. (26) observed a VUS prevalence of around 30% in Latin American women tested for hereditary breast cancer, a value lower than that found in our study, but still higher than in European populations.
The study by Caswell-Jin et al. (11) evaluated genetic testing results and clinical information from 1,483 patients at Stanford University, highlighting that the greater genetic heterogeneity in mixed populations, such as the Brazilian one, increases the number of VUS identified, due to the underrepresentation of these populations in genomic databases used to interpret these variants.
The findings of our study corroborate those previously reported by Guindalini et al. who evaluated 1,663 Brazilian breast cancer patients using multigene panels ranging from 20 to 38 genes. In that cohort, the overall rate of VUS was 46.1%, increasing progressively with the number of genes analyzed up to 11.6 times higher compared to testing restricted to BRCA1/2 genes alone. Both the study by Guindalini et al. (5) and the present investigation emphasize that the high prevalence of VUS poses a significant challenge in clinical practice, particularly in countries with substantial genetic heterogeneity, such as Brazil.
In our study, personal history of cancer, race and other variables were not significantly associated with the presence of VUS in either the univariate or multivariate analyses.
When comparing different panels, we observed a significant increase in the VUS rate with the panel size. The rate of VUS increases with the addition of genes of moderate and low penetrance, and in some cases, a panel test may show several VUS in different genes (27), which frequently occurs in extended panels like ours.
The standard medical treatment recommendation for a VUS is to treat the individual based on their personal and family medical history, rather than the potential implications of the VUS. This can be a difficult concept for a patient seeking an explanation for cancer in their family. There is also the possibility of incorrect actions if a VUS is misinterpreted as deleterious and medical intervention is taken based on that interpretation (6).
As new evidence becomes available, VUS can be reclassified. Current data suggest that 10–15% of reclassified VUS will be updated to LPV/PV, and the remainder to LBV/BV (28).
Another important factor is the identification of genetic variants that are not directly related to the patient's clinical presentation, known as incidental findings, which have become an increasingly relevant issue. One example is the detection of alterations in genes such as RAD50, which were initially included in breast cancer screening panels, but over time have come to be considered as not significantly associated with increased risk for the disease. This highlights the interpretive challenges involved in such cases (3).
An opinion article published in 2023 emphasizes the importance of directing investments to eliminate VUS, as their frequency is one of the main challenges in precision genomic medicine. It is believed that by 2030, most, if not all, VUS cases will be resolved due to advances in variant classification methodologies, the development of more effective computational tools to predict the effects of variants, ensuring comprehensive genomic coverage, as well as collaborative initiatives for data sharing and a larger number of sequenced samples (29).
Moreover, strategies include the creation of more effective genetic panels, reducing the frequency of VUS reporting, studies aimed at improving counseling and education, as well as the creation of uniform policies, which will require the formation of a consensus (30). Thus, our results reinforce the need to develop smaller panels based on observations from national studies like ours. We believe that studies like these should be replicated around the world, considering the genetic differences of populations.
5 Study limitations and strengths
This study has several limitations that should be taken into account when interpreting the results. First, the relatively small sample size may have reduced the statistical power of our analyses, making it difficult to detect associations of smaller magnitude between clinical and genetic variables. Second, recruitment by convenience from a single clinical center may have introduced selection bias, limiting the generalizability of our findings to other populations or epidemiological contexts. In addition, functional validation of VUS was not performed, which constrains the biological and clinical interpretation of these mutations in the context of hereditary cancer predisposition. Finally, potential reclassification of variants after data collection—due to updates in genomic databases and new cohort studies—poses an additional challenge, since changes in pathogenicity status could alter the observed frequencies of VUS, BV/LBV, and PV/LPV.
Despite these limitations, our study offers important strengths. It represents the first Brazilian investigation to analyze VUS in a cohort composed exclusively of public health system patients, thereby providing greater epidemiological and operational relevance. Moreover, it was conducted in a country with high rates of breast cancer among young women—a population for whom molecular testing is critically important for early detection and clinical management. Lastly, by focusing on a real-world public health setting, our findings are directly applicable to routine practice and can inform the development of genomic screening strategies and genetic counseling tailored tão the Brazilian context.
6 Conclusions
With the use of an extended 144-gene panel, most women presented diagnoses VUS (78.53% of the overall population and 56.31% with exclusively VUS). The ATM gene showed the highest number of VUS in patients with or without a personal history of breast cancer.
No association was found between any of the epidemiological variables studied and the presence of VUS.
The extended 144-gene panel increased the number of VUS detected with respect to the smaller panels (20–23 genes).
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Comite De Ètica em Pesquisa https://plataformabrasil.saude.gov.br/ CAAE: 54179621.1.0000.5404. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
CA: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. BD: Investigation, Writing – review & editing. AC: Data curation, Investigation, Project administration, Writing – review & editing. ST: Investigation, Writing – review & editing. TG: Investigation, Writing – review & editing. MS: Investigation, Writing – review & editing. CC: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was funded by internal resources from the University of Campinas (Universidade Estadual de Campinas -UNICAMP).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Instituto Nacional de Câncer (INCA). Available online at: https://www.gov.br/inca/pt-br/assuntos/cancer/numeros/ (Accessed 2022).
2. Simon SD, Bines J, Werutsky G, Nunes JS, Pacheco FC, Segalla JG, et al. Characteristics and prognosis of stage I-III breast cancer subtypes in Brazil: the AMAZONA retrospective cohort study. Breast. (2019) 44:113–9. doi: 10.1016/j.breast.2019.01.008
3. Sapkota Y. Germline DNA variations in breast cancer predisposition and prognosis: a systematic review of the literature. Cytogenet Genome Res. (2014) 144:77–91. doi: 10.1159/000369045
4. Duarte BN, Alem CER, da Silva Cabello AER, Teixeira SRC, Cabello C. Risk-reducing surgeries for breast cancer in Brazilian patients undergoing multigene germline panel: impact of results on decision making. Breast Cancer Res Treat. (2024). doi: 10.1007/s10549-024-07476-7
5. Guindalini RSC, Viana DV, Kitajima J, Rocha VM, López RVM, Zheng Y, et al. Detection of germline variants in Brazilian breast cancer patients using multigene panel testing. Sci Rep. (2022) 12:4190. doi: 10.1038/s41598-022-07383-1
6. Stanislaw C, Xue Y, Wilcox WR. Genetic evaluation and testing for hereditary forms of cancer in the era of next-generation sequencing. Cancer Biol Med. (2016) 13:55–67. doi: 10.20892/j.issn.2095-3941.2016.0002
7. Robson ME, Bradbury AR, Arun B, Domchek SM, Ford JM, Hampel HL, et al. American society of clinical oncology policy statement update: genetic and genomic testing for cancer susceptibility. J Clin Oncol. (2015) 33:3660–7. doi: 10.1200/JCO.2015.63.0996
8. Desmond A, Kurian AW, Gabree M, Mills MA, Anderson MJ, Kobayashi Y, et al. Clinical actionability of multigene panel testing for hereditary breast and ovarian cancer risk assessment. JAMA Oncol. (2015) 1:943–51. doi: 10.1001/jamaoncol.2015.2690
9. van Marcke C, Collard A, Vikkula M, Duhoux FP. Prevalence of pathogenic variants and variants of unknown significance in patients at high risk of breast cancer: a systematic review and meta-analysis of gene-panel data. Crit Rev Oncol Hematol. (2018) 132:138–44. doi: 10.1016/j.critrevonc.2018.09.009
10. Sanabria-Salas MC, Rivera-Herrera AL, Manotas MC, Guevara G, GF3mez AM, Medina V, et al. Building a hereditary cancer program in Colombia: analysis of germline pathogenic and likely pathogenic variants spectrum in a high-risk cohort. Eur J Hum Genet. (2025) 33:913–29. doi: 10.1038/s41431-025-01807-y
11. Caswell-Jin JL, Gupta T, Hall E, Petrovchich IM, Mills MA, Kingham KE, et al. Racial/ethnic differences in multiple-gene sequencing results for hereditary cancer risk. Genet Med. (2018) 20:234–9. doi: 10.1038/gim.2017.96
12. Clift K, Macklin S, Halverson C, McCormick JB, Abu Dabrh AM, Hines S. Patients' views on variants of uncertain significance across indications. J Community Genet. (2020) 11:139–45. doi: 10.1007/s12687-019-00434-7
13. Bittar CM, Vieira IA, Sabato CS, Andreis TF, Alemar B, Artigalás O, et al. TP53 variants of uncertain significance: increasing challenges in variant interpretation and genetic counseling. Fam Cancer. (2019) 18:451–6. doi: 10.1007/s10689-019-00140-w
14. Kalia SS, Adelman K, Bale SJ, Chung WK, Eng C, Evans JP, et al. Recommendations for reporting of secondary findings in clinical exome and genome sequencing, 2016 update (ACMG SF v2.0): a policy statement of the American college of medical genetics and genomics. Genet Med. (2017) 19:249–55. doi: 10.1038/gim.2017.17
15. van El CG, Cornel MC, Borry P, Hastings RJ, Fellmann F, Hodgson SV, et al. Whole-genome sequencing in health care. Recommendations of the European society of human genetics. Eur J Hum Genet. (2013) 21 Suppl 1:S1–5.
16. National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology. Genetic/Familial High Risk Assessment: Breast and Ovarian [Internet] (2022). Available online at: https://www.nccn.org/professionals/physician_gls/pdf/genetics_bop.pdf
18. Fletcher RH, Fletcher SW. Epidemiologia Clínica: Elementos Essenciais. 4th ed. Porto Alegre: Artmed (2006).
19. Fleiss JL, Levin B, Paik MC. Statistical Methods for Rates and Proportions. 3rd ed. Hoboken: John Wiley & Sons (2003). doi: 10.1002/0471445428
20. Hosmer DW, Lemeshow SL. Applied Logistic Regression. New York: John Wiley & Sons (1989). doi: 10.2307/2531779
21. Siegel S, Castellan NJ Jr. Estatística Não-Paramétrica para Ciências do Comportamento. 2rd ed. Porto Alegre: Artmed (2006).
22. Tabachnick BG, Fidell LS. Using Multivariate Statistics. 4th ed. Boston: Allyn and Bacon (2001).
23. Kuchenbaecker KB, Hopper JL, Barnes DR, Phillips KA, Mooij TM, Roos-Blom MJ, et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA. (2017) 317:2402–16. doi: 10.1001/jama.2017.7112
24. Teive HA, Moro A, Moscovich M, Arruda WO, Munhoz RP, Raskin S, et al. Ataxia-telangiectasia - a historical review and a proposal for a new designation: ATM syndrome. J Neurol Sci. (2015) 355:3–6. doi: 10.1016/j.jns.2015.05.022
25. Chapman-Davis E, Zhou ZN, Fields JC, Frey MK, Jordan B, Sapra KJ, et al. Racial and ethnic disparities in genetic testing at a hereditary breast and ovarian cancer center. J Gen Intern Med. (2021) 36:35–42. doi: 10.1007/s11606-020-06064-x
26. Herzog JS, Chavarri-Guerra Y, Castillo D, Abugattas J, Villarreal-Garza C, Sand S, et al. Genetic epidemiology of BRCA1- and BRCA2-associated cancer across Latin America. NPJ Breast Cancer. (2021) 7:107. doi: 10.1038/s41523-021-00317-6
27. Tung N, Battelli C, Allen B, Kaldate R, Bhatnagar S, Bowles K, et al. Frequency of mutations in individuals with breast cancer referred for BRCA1 and BRCA2 testing using next-generation sequencing with a 25-gene panel. Cancer. (2015) 121:25–33. doi: 10.1002/cncr.29010
28. Shirts BH, Pritchard CC, Walsh T. Family-specific variants and the limits of human genetics. Trends Mol Med. (2016) 22:925–34. doi: 10.1016/j.molmed.2016.09.007
29. Fowler DM, Rehm HL. Will variants of uncertain significance still exist in 2030? Am J Hum Genet. (2024) 111:5–10. doi: 10.1016/j.ajhg.2023.11.005
Keywords: high risk, germline mutations, genetic testing, breast cancer, variants of uncertain significance (VUS)
Citation: Alem CER, Duarte BN, Cabello AERdS, Teixeira SRC, Gaspar T, de Souza ML and Cabello C (2025) Impact of germline panel size on hereditary cancer: findings of variants of uncertain significance in the Brazilian public health population selected for high hereditary cancer risk. Front. Cancer Control Soc. 3:1549584. doi: 10.3389/fcacs.2025.1549584
Received: 16 January 2025; Accepted: 25 August 2025;
Published: 12 September 2025.
Edited by:
Luis G. Carvajal-Carmona, University of California, Davis, United StatesReviewed by:
Danilo Ceschin, University Institute of Biomedical Sciences of Córdoba (IUCBC), ArgentinaMaria Carolina Sanabria Salas, University Health Network (UHN), Canada
Copyright © 2025 Alem, Duarte, Cabello, Teixeira, Gaspar, de Souza and Cabello. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cesar Cabello, Y2FiZWxsb0B1bmljYW1wLmJy
†ORCID: Christine Elisabete Rubio Alem orcid.org/0009-0001-7766-1013
Bárbara Narciso Duarte orcid.org/0000-0003-0261-1676
Ana Elisa Ribeiro da Silva Cabello orcid.org/0000-0001-6575-432X
Sandra Regina Campos Teixeira orcid.org/0000-0002-2143-3214
Thiago Gaspar orcid.org/0000-0001-9079-3718
Márcio Lopes de Souza orcid.org/0009-0004-4437-5653
Cesar Cabello orcid.org/0000-0002-7180-460X