 Alberto Alfonso Pimentel-Rentería1
Alberto Alfonso Pimentel-Rentería1 David Francisco Cantú de León2Eliseo Neftalí De la Cruz3David Suárez4Manuel Rodulfo Segura5José Gustavo Núñez6
David Francisco Cantú de León2Eliseo Neftalí De la Cruz3David Suárez4Manuel Rodulfo Segura5José Gustavo Núñez6 Livan Delgado-Roche7*
Livan Delgado-Roche7*- 1Hospital de Oncología, UMAE Centro Médico Nacional Siglo XXI, Instituto Mexicano del Seguro Social, Ciudad de México, Mexico
- 2Departamento de Investigación Clínica, Instituto Nacional de Cancerología, Ciudad de México, Mexico
- 3Hospital de Gineco-Obstetricia No. 3, UMAE Centro Médico Nacional La Raza, Instituto Mexicano del Seguro Social, Ciudad de México, Mexico
- 4Hospital de Especialidades No. 1, UMAE Centro Médico Nacional del Bajío, Instituto Mexicano del Seguro Social, León, Mexico
- 5Hospital de Especialidades, UMAE Centro Médico Nacional Ignacio García Téllez, Instituto Mexicano del Seguro Social, Mérida, Yucatán, Mexico
- 6Hospital de Especialidades, UMAE Centro Médico Nacional Manuel Ávila Camacho, Instituto Mexicano del Seguro Social, Puebla, Mexico
- 7Laboratorios Liomont, Ciudad de México, Mexico
Introduction: Safety of biosimilars is of major relevance for patients and medical community. The aim of this study was to evaluate the safety and tolerability of a bevacizumab biosimilar alongside standard chemotherapy in adult patients with cancer. In addition, the impact on patients’ quality-of-life was assessed.
Methods: This is an observational, multicenter, prospective, phase IV clinical study conducted from April 2022 to April 2024. Adult patients with metastatic cancer were enrolled after informed consent signing. Clinical history, adverse events, and quality of life data were recorded from source documents. Treatment regimens followed the Clinical Practice Guidelines and the Investigator criteria.
Results: Adult patients (n = 82) were included, 65.8% (n = 54) completed the full 6-cycle treatment, while 34.1% (n = 28) meet the criteria for early discontinuation including disease progression (18.3%), voluntary withdrawal or dropout (7.3%), treatment availability or brand switching (4.9%), and serious adverse events (3.7%). The incidence of adverse events was aligned with prior trials, with 97.5% (n = 80) of patients reporting at least one adverse event. The severity of adverse events was mild (86.7%, n = 873), while 11.2% (n = 113) were moderate and 2.1% (n = 22) severe. Five serious adverse events occurred in four patients. The average ECOG score at the end of treatment was similar to the basal score (p > 0.05).
Conclusions: The treatment with the bevacizumab biosimilar Effivia® was considered well tolerated with no additional safety concerns. The average quality-of-life remained stable during treatment. These findings contribute to the growing clinical evidence on the safe use of Effivia® in real-world settings.
1 Introduction
Bevacizumab, a recombinant humanized monoclonal antibody, represents a landmark development in oncology as the first angiogenesis inhibitor approved by the U.S. Food and Drug Administration (FDA) in 2004. Initially indicated for metastatic colorectal cancer, bevacizumab was developed following extensive research elucidating the role of vascular endothelial growth factor (VEGF) in tumor angiogenesis. VEGF is a pivotal mediator of neovascularization, a process critical for tumor growth and metastatic mechanisms. The approval of bevacizumab marked a paradigm shift in cancer therapy by offering a targeted approach to inhibit tumor vascularization and progression (Hurwitz et al., 2004).
Bevacizumab exerts its pharmacological action by binding VEGF-A, a predominant isoform of VEGF, with high affinity, thereby neutralizing its interaction with VEGF receptors (VEGFR-1 and VEGFR-2) expressed on endothelial cells. This inhibition disrupts downstream signaling pathways involved in endothelial cell proliferation, migration, and neovascular formation, effectively suppressing tumor angiogenesis (Ferrara et al., 2003). Additionally, bevacizumab reduces vascular permeability, contributing to decreased interstitial fluid pressure within tumors. With a terminal half-life of approximately 20 days, bevacizumab facilitates convenient dosing intervals, typically every 2 weeks to 3 weeks, when administered in combination with chemotherapy (Keating, 2014; Chitoran et al., 2025).
Clinically, bevacizumab has been demonstrated to improve outcomes across multiple malignancies, including metastatic colorectal cancer, non-small cell lung cancer (NSCLC), ovarian cancer, renal cell carcinoma, glioblastoma, and cervical cancer (Sandler et al., 2006; Garcia et al., 2020). Numerous clinical trials have shown that adding bevacizumab to standard chemotherapy regimens significantly enhances progression-free survival and, in some instances, overall survival. However, its use has been associated with well-recognized adverse events, including hypertension, gastrointestinal perforation, bleeding, and thromboembolic events, thus requiring careful patient selection and monitoring during treatment (Wang et al., 2024).
The high cost of bevacizumab has presented a significant barrier to its accessibility, particularly in low-income countries, thereby driving the development and adoption of biosimilars (Lu et al. 2024). Biosimilars are biotech drugs that exhibit high similarity to the reference product in terms of structural, physicochemical, functional, and clinical characteristics, while offering reduced costs. The bevacizumab biosimilar Effivia® has undergone stringent analytical, preclinical, and clinical evaluations to establish equivalence to the reference product Avastin® (Trukhin et al., 2021; Schwabe et al., 2023; Zhao et al., 2023). Post-marketing studies and real-world evidence have further validated its comparable safety, efficacy, and pharmacological profiles across various indications (Zhao et al., 2023). In Latin America, including Mexico, observational studies evaluating the safety of bevacizumab biosimilars are of major relevance, supporting their incorporation into clinical practice, thereby enhancing access to effective and safe oncologic treatments and reducing economic burdens. The lack of post-marketing safety data on Effivia® in the Mexican population has been identified as a knowledge gap. Therefore, we conducted a multicenter observational study in Mexico to evaluate the safety and tolerability of the bevacizumab biosimilar Effivia® in adult cancer patients.
2 Materials and methods
2.1 Study design and population
The selection of the study design was based on the primary objective of the clinical study: to obtain safety and tolerability information regarding treatment with bevacizumab biosimilar (Effivia®) solution when used in combination with the standard chemotherapy in those indications approved in Mexico. This study was a multicenter, observational, phase IV, prospective, non-controlled study including patients of both sexes, aged 18 years and older; with diagnosis of metastatic colorectal cancer, locally recurrent or metastatic breast cancer, advanced, metastatic, or recurrent non-small cell lung cancer, metastatic and/or advanced renal cell carcinoma, epithelial ovarian cancer, fallopian tube cancer, primary peritoneal cancer, and cervical uterine cancer who were naïve to bevacizumab, were candidates for treatment with bevacizumab biosimilar (Effivia®), and who agreed to participate in the study by signing the informed consent. Patients were excluded if they meet the following criteria: recent history of severe bleeding or hemoptysis; risk factors for gastrointestinal bleeding or perforation; patients with ≥2 g of proteinuria in 24 h; major surgical procedures within 28 days prior to the start of treatment, or wounds with incomplete healing; pregnant or breastfeeding women; known hypersensitivity to any components of the drug, Chinese hamster ovary cell products, or other recombinant human or humanized antibodies.
A non-probabilistic sampling method was considered, aiming to include at least 5% of the total patients potentially exposed to bevacizumab biosimilar (Effivia®) from August 2022 to April 2024. Considering the stringent analytical, preclinical, and clinical evaluations to establish the equivalence of Effivia® to the reference product Avastin®, no active or placebo controls were included. There were no predetermined treatment protocols; instead, the dosing and scheduling of the bevacizumab and chemotherapy were determined based on the specific type of cancer, the local Clinical Practice Guidelines, and the Investigator criteria. The exposure time to the bevacizumab biosimilar (Effivia®) varied; however, a six-cycle regimen was suggested during the observational period. The study population received between one and six treatment cycles, administered every 2 weeks to 3 weeks. A specialized steering committee was formed, comprising external clinical experts and a patient advocate, to supervise the scientific advancement and integrity of the study.
The secondary objectives of the study were as follows: to determine the frequency of identified risks associated with bevacizumab; to evaluate the tolerability of bevacizumab biosimilar treatment, defined as the time elapsed from the first administration of the drug to its discontinuation due to unacceptable toxicity; to assess the effect of bevacizumab biosimilar treatment on patients’ functional status using the Eastern Cooperative Oncology Group (ECOG) score before and after completing the treatment regimen according to standard clinical practice.
This study was conducted in strict compliance with the ICH E6 (R2) and NOM-012-SSA3-2012 guidelines, the Declaration of Helsinki, the General Health Law Regulation, which establishes the criteria for conducting health research projects involving human subjects, and the guidelines set forth by the National Commission of Bioethics. Prior to participating in the study, all subjects received a comprehensive explanation of the potential risks, anticipated benefits, and their rights as research subjects. Patient data were anonymized and securely handled according to the local regulations and laws, ensuring the protection of participants’ rights and privacy. This information was reviewed and approved by the Institutional Ethics Committees of Instituto Mexicano del Seguro Social (IMSS) with the reference number R-2022-785-008 and the Institutional Ethics Committees of Instituto Nacional de Cancerología with reference number INCAN/CEI/905/21. All patients provided written informed consent before any study procedures started. Finally, the clinical study was registered in a public database [NCT 06313268 (ClinicalTrials.gov)].
2.2 Data collection
Patient data, including safety and quality of life variables, were evaluated using standard procedures from routine clinical practice. Adverse events (AE) or significant risks associated with treatment with bevacizumab biosimilar (Effivia®) were also monitored and assessed accordingly. The patients’ functional status was assessed using the ECOG scale, which has been validated by the World Health Organization (WHO) and adopted by the Clinical Practice Guidelines in Mexico to indirectly evaluate the quality of life in oncology patients.
Data collection was conducted prospectively from source documents during visits and/or chemotherapy/bevacizumab infusion sessions. Special emphasis was placed on the quality and traceability of data, from collection to processing and storage in compliance with ICH (E6R2) Good Clinical Practice guidelines.
Reporting, analysis, and classification of adverse events were carried out in accordance with the current NOM-220-SSA1-2016 and pharmacovigilance guidelines. AEs of interest included but were not limited to the following: severe hemorrhagic events, venous and arterial thromboembolic events (including deep vein thrombosis and pulmonary embolism, cardiac ischemia, myocardial infarction, cerebrovascular accident, transient ischemic attack, thrombotic microangiopathy, and peripheral arterial ischemia), gastrointestinal perforation, postoperative wound-bleeding or -healing complications, new or worsening hypertension requiring medication, symptomatic congestive heart failure, pulmonary hypertension, reversible posterior leukoencephalopathy syndrome (RPLS), and osteonecrosis in children (population not included in this study).
2.3 Statistical analysis
Demographic and baseline variables, including vital signs and clinical laboratory values, were analyzed by descriptive statistics. Data were analyzed in aggregate (pooled across cancer types) because there were not enough patients in each subgroup to allow for meaningful comparisons by indication or regimen. The safety analysis includes data from all enrolled patients, regardless of protocol adherence. The ECOG score was determined at baseline and at the end of treatment, including patients who completed the six treatment cycles. However, a complementary analysis of ECOG was carried out using data from patients who experienced early termination or discontinuation (when data were available). Comparisons between baseline and the last evaluable point were performed using Student’s t-test for paired samples. A p-value < 0.05 was considered a statistically significant difference.
3 Results
In the present study, 82 patients were enrolled after informed consent was obtained and eligibility criteria were confirmed. A total of 65.8% (n = 54) of patients completed the full six-cycle treatment regimen, while 34.1% (n = 28) discontinued treatment early due to one of the criteria established in the protocol. Of these, 18.3% discontinued bevacizumab biosimilar Effivia® treatment due to disease progression, 7.3% due to voluntary withdrawal or loss to follow-up, 4.9% for other reasons (primarily the availability of treatment at institutions or switching to other commercial brands of bevacizumab), and 3.7% discontinued due to serious adverse events or a risk outweighing the benefit. No patients were withdrawn from the study prematurely due to the unacceptable toxicity of the biosimilar drug. Subject allocation is illustrated in Figure 1 in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines, which provide standards for the reporting of clinical trials. Of note, a patient diagnosed with hepatocarcinoma was enrolled as per the Investigator criteria. This indication is not approved in Mexico; however, the investigator deemed that the benefit of treatment with bevacizumab biosimilar Effivia® solution outweighed the potential risks. This deviation from the selection criteria was classified as a major deviation and was promptly reported to the ethics committees. Demographic characteristics, baseline variables, and type of cancer are depicted in Table 1. The mean age was 58.3 years, and 45.1% of the patients were men. The average dosage was 500.52 ± 241.21 mg in the total population observed. The cancer type dosages were as follows: colorectal cancer (406.54 ± 125.51 mg), cervical uterine cancer (958.50 ± 250.72 mg), ovarian cancer (843.89 ± 185.40 mg), and others, including endometrial, breast, and hepatic carcinoma (743.33 ± 388.12 mg).
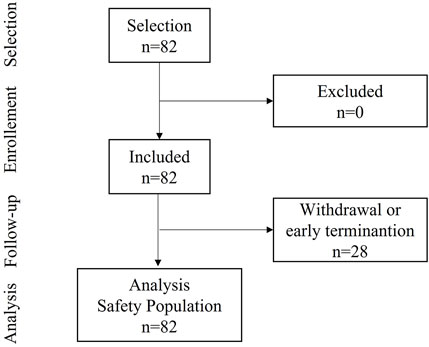
Figure 1. Consolidated Standards of Reporting Trials (CONSORT) flow diagram.
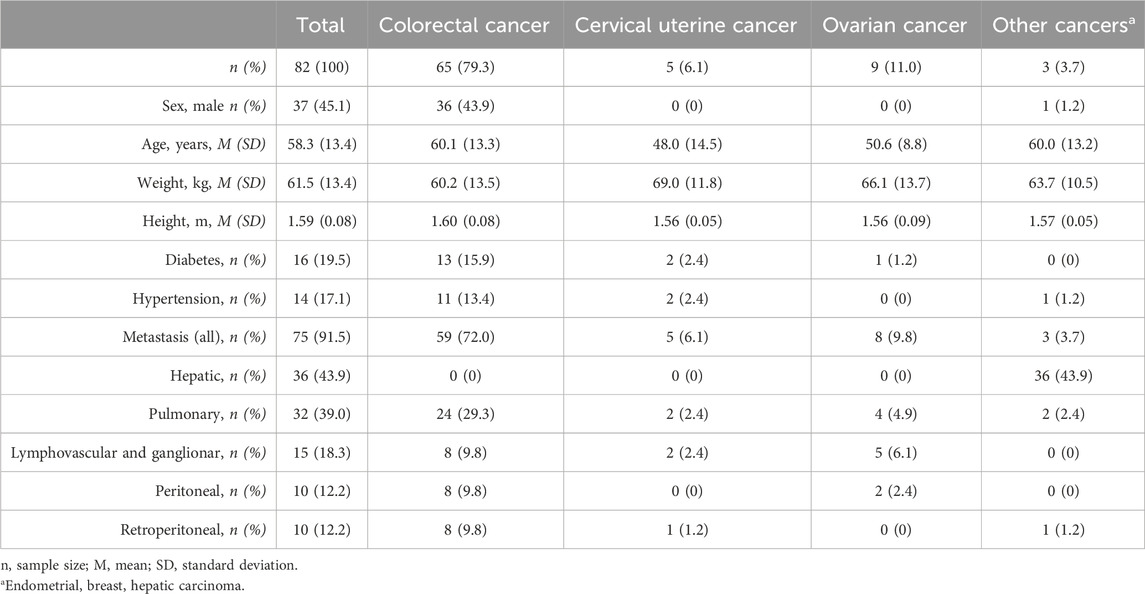
Table 1. Summary of demographic characteristics, baseline variables, and type of cancer in the study population.
Of the study population (n = 82), 80 patients (97.5%) reported at least one adverse event (AE). Based on the study analysis, 873 AEs (86.7%) were considered mild, 113 AEs (11.2%) were moderate, and 22 AEs (2.1%) were severe. Only five serious AEs were reported in 4/82 patients (see Table 2). During the study, three deaths were reported, two of them attributed to serious AEs comprising hemorrhagic stroke and intestinal obstruction with septic shock.
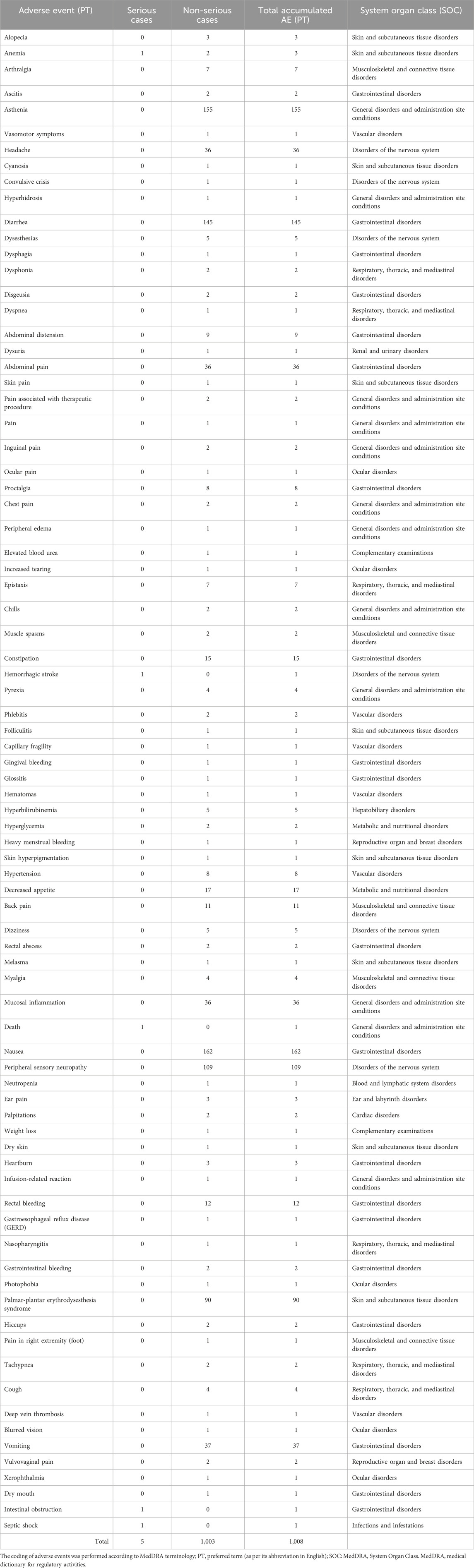
Table 2. Summary of adverse events (n = 82).
Figure 2 shows the analysis of the ECOG score, including 54 patients who completed all six treatment cycles. As shown, the average ECOG score at baseline was 0.9074 ± 0.4863, without statistical differences at the end of treatment (p > 0.05).
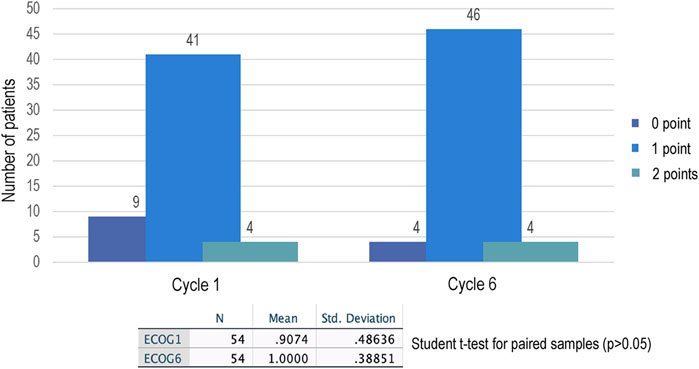
Figure 2. ECOG score in patients who completed six treatment cycles with Effivia®. The values 0, 1, and 2 correspond to the ECOG classification assigned by the investigator. p-values <0.05 represent significant differences.
Many patients showed abnormal vital sign ranges, consistent with their current pathology or personal medical history and reported comorbidities (see Table 3).
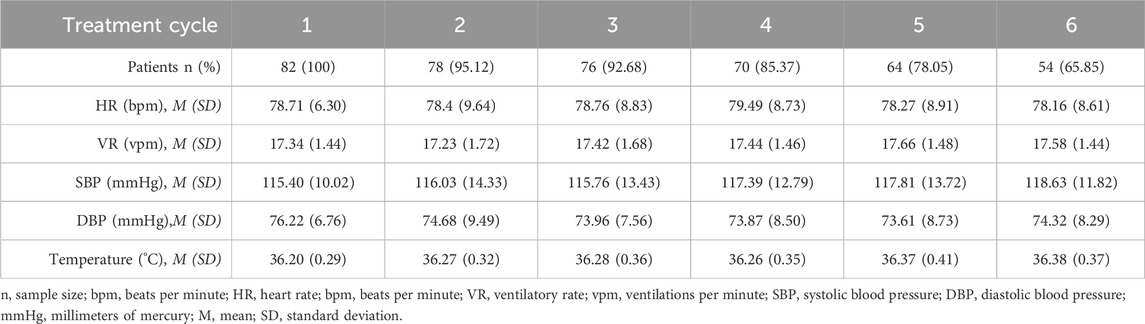
Table 3. Summary of vital signs in the study population.
4 Discussion
The safety profile of bevacizumab has been extensively characterized for both the reference drug (Avastin®) and the biosimilar Effivia®. In metastatic colorectal cancer, a meta-analysis of six randomized controlled clinical trials, involving 3,385 patients, showed that hypertension (RR 2.98, 95% CI, 2.32–3.84), gastrointestinal perforations (RR 5.04, 95% CI, 1.72–14.79), and bleeding (RR 2.07, 95% CI, 1.19–3.62) significantly increased in patients receiving bevacizumab (Galfrascoli et al., 2011). Another meta-analysis, which included 15 randomized controlled trials with a total of 6,937 patients, found that treatment with bevacizumab had a slightly higher risk of any serious adverse event (pooled RR 1.07, 95% CI, 1.02–1.12) than other treatments or placebo. The combined risk difference was 5% (95% CI: 2%–9%), with a number needed to harm (NNH) of 20 treated patients. The analyses indicated a significantly higher risk for bevacizumab, which was associated with a three-fold increase in the risk of hypertension [pooled RR 3.06 (95% CI 2.45–3.83)], a two-fold increase in the risk of gastrointestinal bleeding/perforation, and a lower risk of neutropenia [pooled RR 0.75 (95% CI 0.26–2.19)] (Dai et al., 2013). The results from these analyses and the accumulated evidence suggest that the benefits of bevacizumab treatment outweigh the risks, supporting its use in this indication (Lauro et al., 2014).
Two major cohort studies have focused on evaluating the safety of bevacizumab: the SAiL (Safety of Avastin in Lung) and ARIES (Avastin Registry: Investigation of Effectiveness and Safety) trials. SAiL was a phase IV trial involving 2,212 patients, assessing the safety of bevacizumab in first-line treatment at doses of 7.5 mg/kg and 15 mg/kg in combination with standard chemotherapy for up to six cycles, followed by bevacizumab until disease progression or unacceptable toxicity. Significant adverse events (grade 3 or higher) were infrequent: bleeding occurred in 80 cases (4%), pulmonary hemorrhage in 15 cases (1%), hypertension in 125 cases (6%), proteinuria in 67 cases (3%), and venous thromboembolism in 172 cases (8%) (Barlesi et al., 2013).
In contrast, the ARIES trial was conducted in 1,518 patients with non-small cell lung cancer, treated with first-line standard chemotherapy in combination with bevacizumab. In the studied population, hypertension was observed in 3.8% of cases, while bleeding (>grade 3) occurred in 1.9% of cases (gastrointestinal bleeding in 1.1%, pulmonary hemorrhage in 0.7%, and CNS hemorrhage in 0.1%) (Lynch et al., 2014). Here, we included a broad range of indications, which increases the generalizability of the safety outcomes. However, the study did not include enough patients to analyze safety by cancer type or chemotherapy protocol, which is an area for future research.
Although a high incidence of adverse events (97.5%) was observed in the present study, most of these events were “expected” and mild (86.7%). This is in accordance with the known safety profile for bevacizumab. The low proportion of severe AEs suggests that while bevacizumab carries some risk, these risks are largely manageable. The reported serious adverse events (4.8%) remain within the expected safety data for bevacizumab treatment schemes. Two fatalities were attributed to serious AEs: one due to hemorrhagic cerebrovascular accident and another due to intestinal obstruction with septic shock. These outcomes, while serious, are consistent with known risks associated with anti-angiogenic therapy such as bevacizumab, which has been linked to complications like gastrointestinal perforations, bleeding, and thromboembolism in prior studies.
It is noteworthy that only four patients had an ECOG score = 2, while the rest were rated by the investigator with an ECOG score = 0 or 1. During treatment with Effivia® solution, the average patient performance was not affected, as suggested by the ECOG score of 1 at the end of the study. These results suggest that, under the conditions of this study, the bevacizumab biosimilar Effivia® contributes to maintaining patient autonomy in performing daily activities and supports their quality of life.
These findings indicate that treatment with Effivia® solution in combination with standard chemotherapy, administered every 2 weeks or 3 weeks for six cycles, is a safe and well-tolerated therapeutic alternative. Based on these results, no specific monitoring strategies or patient selection criteria for Effivia® are anticipated. It is important to note that not assessing the safety and tolerability of Effivia® beyond six cycles in patients who required a second six-cycle treatment represents a study limitation. These findings contribute to the growing evidence on the safety and tolerability of Effivia® in real-world settings, giving oncologists and payers confidence that the biosimilar is a safe option.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: NCT 06313268 ClinicalTrials.gov.
Ethics statement
The study was approved by the Institutional Ethics Committees of Instituto Mexicano del Seguro Social (IMSS) and the Institutional Ethics Committees of Instituto Nacional de Cancerología. The study was conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AP-R: formal analysis, investigation, resources, and writing – review and editing. DC: formal analysis, investigation, resources, and writing – review and editing. ED: formal analysis, investigation, resources, and writing – review and editing. DS: investigation, resources, supervision, and writing – review and editing. MS: investigation, resources, supervision, and writing – review and editing. JN: investigation, resources, supervision, and writing – review and editing. LD-R: conceptualization, formal analysis, investigation, methodology, project administration, supervision, writing – original draft, and writing – review and editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authros wants to acknowledge the support of the CRO Servicios Especializados en Ensayos Clínicos, México.
Conflict of interest
Author LD-R was employed by Laboratorios Liomont.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Barlesi, F., Scherpereel, A., Gorbunova, V., Gervais, R., Vikström, A., Chouaid, C., et al. (2014). Maintenance bevacizumab-pemetrexed after first-line cisplatin-pemetrexed-bevacizumab for advanced nonsquamous nonsmall-cell lung cancer: updated survival analysis of the AVAPERL (MO22089) randomized phase III trial. Ann. Oncol. 25 (5), 1044–1052. doi:10.1093/annonc/mdu098
Chitoran, E., Rotaru, V., Stefan, D. C., Gullo, G., and Simion, L. (2025). Blocking tumoral angiogenesis VEGF/VEGFR pathway: bevacizumab-20 years of therapeutic success and controversy. Cancers (Basel). 17 (7), 1126. doi:10.3390/cancers17071126
Dai, F., Shu, L., Bian, Y., Wang, Z., Yang, Z., Chu, W., et al. (2013). Safety of bevacizumab in treating metastatic colorectal cancer: a systematic review and meta-analysis of all randomized clinical trials. Clin. Drug Investig. 33 (11), 779–788. doi:10.1007/s40261-013-0125-6
Ferrara, N., Gerber, H. P., and LeCouter, J. (2003). The biology of VEGF and its receptors. Nat. Med. 9 (6), 669–676. doi:10.1038/nm0603-669
Galfrascoli, E., Piva, S., Cinquini, M., Rossi, A., La Verde, N., Bramati, A., et al. (2011). Risk/benefit profile of bevacizumab in metastatic colon cancer: a systematic review and meta-analysis. Dig. Liver Dis. 43 (4), 286–294. doi:10.1016/j.dld.2010.10.010
Garcia, J., Hurwitz, H. I., Sandler, A. B., Miles, D., Coleman, R. L., Deurloo, R., et al. (2020). Bevacizumab (Avastin) in cancer treatment: a review of 15 years of clinical experience and future outlook. Cancer Treat. Rev. 86, 102017. doi:10.1016/j.ctrv.2020.102017
Hurwitz, H., Fehrenbacher, L., Novotny, W., Cartwright, T., Hainsworth, J., Heim, W., et al. (2004). Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N. Engl. J. Med. 350 (23), 2335–2342. doi:10.1056/NEJMoa032691
Keating, G. M. (2014). Bevacizumab: a review of its use in advanced cancer. Drugs. 74 (16), 1891–1925. doi:10.1007/s40265-014-0302-9
Lauro, S., Onesti, C. E., Righini, R., and Marchetti, P. (2014). The use of bevacizumab in non-small cell lung cancer: an update. Anticancer Res.;34(4):1537–1545. https://pubmed.ncbi.nlm.nih.gov/24692680/.
Lu, B., Dvorani, E., Nguyen, L., Beca, J. M., Mercer, R. E., Adamic, A., et al. (2024) Cost-effectiveness analysis of bevacizumab biosimilars versus originator bevacizumab for metastatic colorectal cancer: a comparative study using real-world data. Value Health. 27 (12), 1689–1697. doi:10.1016/j.jval.2024.07.018
Lynch, T. J., Spigel, D. R., Brahmer, J., Fischbach, N., Garst, J., Jahanzeb, M., et al. (2014). Safety and effectiveness of bevacizumab-containing treatment for non-small-cell lung cancer: final results of the ARIES observational cohort study. J. Thorac. Oncol. 9 (9), 1332–1339. doi:10.1097/JTO.0000000000000257
Sandler, A., Gray, R., Perry, M. C., Brahmer, J., Schiller, J. H., Dowlati, A., et al. (2006). Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. N. Engl. J. Med. 355 (24), 2542–2550. doi:10.1056/NEJMoa061884
Schwabe, C., Cole, A., Espigares-Correa, A., Beydon, M. E., Florez-Igual, A., and Queiruga-Parada, J. (2023). A randomized, double-blind, single-dose study to assess bioequivalence of MB02 biosimilar after manufacturing iteration and reference bevacizumab. Pharmacol. Res. Perspect. 11 (2), e01070. doi:10.1002/prp2.1070
Trukhin, D., Poddubskaya, E., Andric, Z., Makharadze, T., Bellala, R. S., Charoentum, C., et al. (2021). Efficacy, safety and immunogenicity of MB02 (bevacizumab biosimilar) versus reference bevacizumab in advanced non-small cell lung cancer: a randomized, double-blind, phase III study (stella). BioDrugs 35 (4), 429–444. doi:10.1007/s40259-021-00483-w
Wang, L., Fei, Y., Qu, H., Zhang, H., Wang, Y., Wu, Z., and Fan, G. (2024). Five years of safety profile of bevacizumab: an analysis of real-world pharmacovigilance and randomized clinical trials. J. Pharm. Health Care Sci. 10, 1. doi:10.1186/s40780-023-00314-w
Zhao, Z., Zhao, L., Xia, G., Lu, J., Shen, B., Zhou, G., et al. (2023). Efficacy and safety of bevacizumab biosimilar compared with reference bevacizumab in locally advanced and advanced non-small cell lung cancer patients: a retrospective study. Front. Oncol. 12, 1036906. doi:10.3389/fonc.2022.1036906
Keywords: bevacizumab, biosimilar, metastatic cancer, safety, pharmacovigilance
Citation: Pimentel-Rentería AA, Cantú de León DF, De la Cruz EN, Suárez D, Segura MR, Núñez JG and Delgado-Roche L (2025) Safety and tolerability of a bevacizumab biosimilar (Effivia®) in adult Mexican patients with cancer: a multicenter, observational, prospective clinical study. Front. Drug Discov. 5:1591991. doi: 10.3389/fddsv.2025.1591991
Received: 19 March 2025; Accepted: 21 April 2025;
Published: 30 May 2025.
Edited by:
Yusuf Tutar, University of Health Sciences, TürkiyeReviewed by:
Aaron Zefrin Fernandis, MSD International GmBH, SingaporeMahmut Demirbilek, Biruni University Hospital, Türkiye
Copyright © 2025 Pimentel-Rentería, Cantú de León, De la Cruz, Suárez, Segura, Núñez and Delgado-Roche. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Livan Delgado-Roche, bGRlbGdhZG9AbGlvbW9udC5jb20ubXg=