 Kajinth Manogarathaas1
Kajinth Manogarathaas1 Nicoline S. Arentoft1
Nicoline S. Arentoft1 Jens G. Hillingsø2
Jens G. Hillingsø2 Anne Marie R. Jensen1Annette D. Fialla3Gerda E. Villadsen4Peter Holland-Fischer5Shoaib Afzal6,7Børge G. Nordestgaard6,7Peter Brown8
Anne Marie R. Jensen1Annette D. Fialla3Gerda E. Villadsen4Peter Holland-Fischer5Shoaib Afzal6,7Børge G. Nordestgaard6,7Peter Brown8 Allan Rasmussen2
Allan Rasmussen2 Susanne D. Nielsen1,2,7*
Susanne D. Nielsen1,2,7*- 1Department of Infectious Diseases, Copenhagen University Hospital - Rigshospitalet, Copenhagen, Denmark
- 2Department of Surgery and Transplantation, Copenhagen University Hospital – Rigshospitalet, Copenhagen, Denmark
- 3Department of Gastroenterology, Odense University Hospital, Odense, Denmark
- 4Department of Hepatology and Gastroenterology, Aarhus University Hospital, Aarhus, Denmark
- 5Department of Gastroenterology, Aalborg University Hospital, Aalborg, Denmark
- 6The Copenhagen General Population Study, Department of Clinical Biochemistry, Copenhagen University Hospital - Herlev and Gentofte, Herlev, Denmark
- 7Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark
- 8Department of Hematology, Copenhagen University Hospital - Rigshospitalet, Copenhagen, Denmark
Hematological abnormalities are common in liver transplant recipients, but evidence beyond the first-year post-transplantation is scarce. We aimed to evaluate hematological abnormalities in liver transplant recipients beyond the first-year post-transplantation. We included 437 liver transplant recipients and 1,744 age- and sex-matched controls from the general population. Odds for cytopenias were assessed using logistic regression analyses adjusted for age, sex, ethnicity, hs-CRP, smoking, and alcohol use. Potential transplant-related risk factors were assessed in liver transplant recipients only. The median time since transplantation was 7.8 years, and 47% had autoimmune liver disease as the indication for transplantation. Compared to controls, liver transplant recipients had a higher prevalence of anemia (24.5% vs. 3.5%), neutropenia (2.1% vs. 0.1%), lymphocytopenia (18.4% vs. 1.5%), and thrombocytopenia (19.2% vs. 2.2%). Living with a transplanted liver was independently associated with higher odds of anemia (aOR, 7.84 [95% CI: 5.04 – 12.18], p<0.001), lymphocytopenia (aOR 16.69 [95% CI: 9.56 – 29.12], p<0.001), and thrombocytopenia (aOR 10.19 [95% CI: 6.07 – 17.13], p<0.001). No association was found between cytopenias, specific types of immunosuppressive treatments, or cirrhosis at transplantation. In conclusion, hematological abnormalities are common in liver transplant recipients, even several years post-transplantation, and increased attention towards cytopenia in this population is warranted.
Introduction
Hematological abnormalities are common among liver transplant recipients within the first-year post-transplantation (1–4), with anemia and thrombocytopenia being the most frequently reported cytopenias (3, 5–12). While cytopenias are highly prevalent in the early period post-transplantation, evidence beyond the first year is scarce. Post-transplant cytopenia can arise from various risk factors, including commonly used immunosuppressive medications like mycophenolate mofetil, tacrolimus, and prednisolone (13–18), as well as valganciclovir for CMV prophylaxis and sulfamethoxazole-trimethoprim for PCP prophylaxis (19–22). Additionally, factors such as increasing age, male sex, hypersplenism, impaired renal function affecting erythropoietin production, and infections may also contribute to cytopenia (6, 7, 23, 24).
One previous study found higher hemoglobin and thrombocyte counts 18 months post-transplantation compared to pre-transplantation levels in cirrhotic patients (25), but no studies have compared the prevalence of cytopenia in liver transplant recipients to that in the background population.
The objectives of this study were to determine the prevalence of anemia, neutropenia, lymphopenia, and thrombocytopenia in liver transplant recipients beyond the first-year post-transplantation compared to controls from the general population. Furthermore, we aimed to identify potential risk factors associated with cytopenias in liver transplant recipients. We hypothesized that the prevalence of cytopenia is higher in liver transplant recipients beyond the first-year post-transplantation than in the general population and that increasing age and treatment with immunosuppressive medications are risk factors for cytopenias, while increasing time since transplantation is associated with lower risk of cytopenias in liver transplant recipients.
Materials and methods
Study design and participants
The Danish Comorbidity in Liver Transplant Recipients (DACOLT) study is an ongoing prospective cohort study of liver transplant recipients that was initiated in 2021. The overall aim of the DACOLT study is to assess the burden of comorbidities in liver transplant recipients and the associated risk factors (26). All liver transplant recipients >20 years with residency in Denmark, who were able to give informed consent, were invited to participate in the study. The current study included all liver transplant recipients included in the DACOLT study before December 1st, 2023, who had at least one available measurement of hematology and were ≥1-year post-transplantation. Participants were followed at outpatient clinics at one of four regional hospitals in Denmark: Aalborg University Hospital, Aarhus University Hospital, Odense University Hospital, and Copenhagen University Hospital – Rigshospitalet. Controls were recruited from the Copenhagen General Population Study (CGPS), a prospective cohort study with >110.000 participants aged 20-100 years included from the general population in the greater Copenhagen area (27, 28).
Participants in both the DACOLT study and the CGPS completed a questionnaire regarding health and medication. Data from questionnaires included information on ethnicity, use of alcohol, and smoking habits, including current smoking status and cumulated smoking history, and educational level. Ethnicity was self-reported and defined according to grandparents’ country of origin. The response options were as follows: ‘Danish’, ‘Other Scandinavian’, ‘Other European’ or ‘Other Ethnicities’. If any grandparent had a different ethnicity, ‘Other Ethnicities’ was selected. Use of alcohol was categorized as one of the following: Never, monthly, weekly, or daily consumption of alcohol. Smoking status was defined as one of the following: Never, current, former, or unknown. Pack years was defined as number of years smoking 20 cigarettes per day.
Both the DACOLT study (H-20052199) and the CGPS (H-KF-01-144/01) received approval from the Ethics Committee of the Capital Region, Denmark. The DACOLT study has been registered at ClinicalTrials.gov (NCT04777032). All participants provided oral and written informed consent. The studies were conducted according to the Declaration of Helsinki.
Liver transplantation variables
Information regarding the use of immunosuppressive medication at time of inclusion in the DACOLT study was retrieved from medical records and the Shared Medication Record (FMK), a national health registry that contains all medical prescriptions authorized by healthcare professionals for citizens in Denmark (29). All liver transplant-related data, including the indication for transplantation and date of transplantation were acquired from review of the participants’ electronic medical records. Cirrhosis at the time of transplantation was defined according to the histological examination of the explant. Lack of energy was defined as “Yes” to the question “Have you felt lacking in energy or strength?”. Breathlessness was defined as “Yes” to the question “Do you get very breathless when walking uphill or climbing one flight of stairs?
Blood sample collection
Blood samples from liver transplant recipients in the DACOLT study and CGPS participants including measurements of hemoglobin, mean corpuscular volume (MCV), mean corpuscular hemoglobin concentration (MCHC), absolute neutrophil count (ANC), lymphocytes, thrombocyte count, and high-sensitivity C-reactive protein (hs-CRP) were analyzed as routine biochemistry.
Outcome definitions
All cytopenias were defined according to the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0 (30). Anemia was defined as low hemoglobin concentration (male: < 8.3 mmol/L; female: < 7.3 mmol/L) and classified as mild (male: 6.2 – 8.3 mmol/L; female: 6.2 – 7.3 mmol/L), moderate (4.9 – 6.1 mmol/L), and severe (< 4.9 mmol/L). MCV was classified as: microcytic (≤ 84 fL), normocytic (85 – 100 fL), and macrocytic (> 100 fL). MCHC was classified as: hypochromatic (≤ 19.6 mmol/L), normochromatic (19.7 – 22.2 mmol/L), and hyperchromatic (> 22.2 mmol/L). Neutropenia was defined as low neutrophil granulocytes < 1.5 x 109 cells/L and classified as mild (1.0 – 1.5 x 109 cells/L), moderate (0.5 – 0.9 x 109 cells/L), and severe (< 0.5 x 109 cells/L). Lymphocytopenia was defined as low lymphocytes < 1.0 x 109 cells/L) and classified as: mild (0.8 – 1.0 x 109 cells/L), moderate (0.5 – 0.79 x 109 cells/L), and severe (<0.5 x 109 cells/L). Thrombocytopenia was defined as low thrombocytes < 150 x 109 cells/L and classified as mild (100 – 150 x 109 cells/L), moderate (75 – 99 x 109 cells/L), and severe (< 75 x 109 cells/L).
Statistics
Liver transplant recipients were matched on sex and 1-year age intervals with controls, aiming for a matching ratio of 1:4. However, for two liver transplant recipients it was only possible to match with two controls. Descriptive statistics were used to assess differences between liver transplant recipients and controls. For continuous data, t-tests or the Wilcoxon rank sum test were performed for normally or non-normally distributed variables, respectively. Pearson’s chi-squared test was used for categorical variables.
The prevalence of cytopenias was compared between liver transplant recipients and controls using Pearson’s chi-squared test. The association between living with a transplanted liver and cytopenia was explored using logistic regression for each of the four dependent categorical variables: anemia, neutropenia, lymphocytopenia, and thrombocytopenia. The association between living with a transplanted liver and hemoglobin, neutrophile granulocytes, lymphocytes, and thrombocytes were assessed using linear regression analyses. In both the linear and logistic regression analyses, living with a transplanted liver was included as the independent variable in a base model adjusted for age and sex, and a fully adjusted model adjusted for age, sex, ethnicity, hs-CRP, smoking, and use of alcohol. To test the robustness of our findings of the association between living with a transplanted liver and cytopenias, we performed two stratified analyses: only comparing liver transplant recipients with cirrhosis at time of transplantation with controls and excluding liver transplant recipients with autoimmune liver disease as reason for transplantation. In exploratory analyses, we used logistic regression to investigate if anemia in liver transplant recipients was associated with more lack of energy and more breathlessness. In the combined cohort, potential risk factors for cytopenias were assessed using logistic regression both in univariate models and a model including all potential risk factors. The following risk factors were investigated: Liver transplantation, age, sex, ethnicity, hs-CRP, smoking, and alcohol.
Among liver transplant recipients, potential transplant-related risk factors for cytopenias were assessed using multiple logistic regression adjusted for age and sex with potential risk factors included in the model one at a time. The following possible risk factors were investigated: use of immunosuppressive medication (mycophenolate mofetil/azathioprine/none; tacrolimus/everolimus/cyclosporine/none; prednisolone, yes/no), cirrhosis at time of transplantation (yes/no), time since transplantation and indication for transplant (autoimmune liver disease, yes/no). To assess differences in the prevalence of anemia, neutropenia, lymphocytopenia and thrombocytopenia between liver transplant recipients with and without autoimmune liver disease, Pearson’s chi-square test was used. To investigate whether trough levels of tacrolimus were associated with the presence of cytopenias, we conducted logistic regression analyses with a base model and fully adjusted model.
A two-sided p-value < 0.05 was considered significant. The statistical analysis was conducted in R studio 2023.09.0 build 463 with R 4.3.2 for Windows 10 Enterprise.
Results
This study included 437 liver transplant recipients and 1744 controls. The median age for liver transplant recipients and controls was 55.4 and 55.3 years, respectively (Table 1). Both groups were predominantly males of Scandinavian descendent, but liver transplant recipients displayed a greater ethnic diversity than controls. Liver transplant recipients also had lower educational level than controls and were more likely to abstain from alcohol (Table 1).
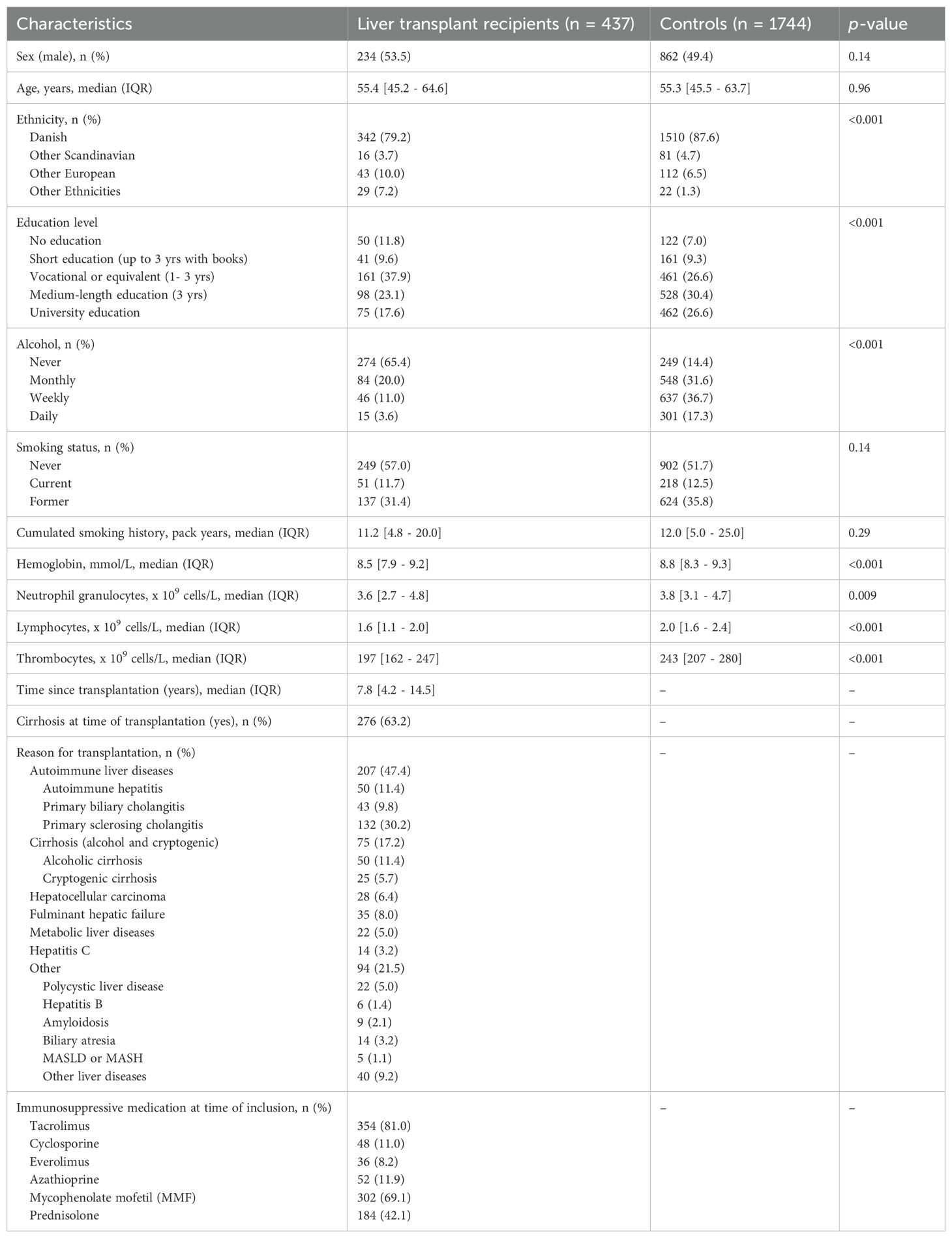
Table 1. Characteristics of liver transplant recipients and controls.
Median time since transplantation was 7.8 years [interquartile range (IQR), 4.2 – 14.5] (Table 1). At time of transplantation, 275 participants (62.9%) had cirrhosis, regardless of the underlying cause. Autoimmune liver disease was the most frequent indication for liver transplantation in 207 (47.4%) liver transplant recipients. Most liver transplant recipients were treated with tacrolimus and mycophenolate mofetil (81.0 and 69.1%, respectively), and 184 (42.1%) also received prednisolone at the time of inclusion in the study.
Prevalence of cytopenia in liver transplant recipients and controls
Liver transplant recipients had a lower hemoglobin concentration than controls (median IQR, 8.5 mmol/L [7.9 – 9.2] vs 8.8 mmol/L [8.3 – 9.3], p<0.001), and a higher prevalence of anemia. (24.5% vs 3.5%, p<0.001). However, no significant differences were found in the severity of anemia between liver transplant recipients and controls with anemia (Figure 1). Among participants with anemia, the prevalence of hypochromatic anemia was higher in liver transplant recipients than in controls (25.0% vs 8.2%, p=0.014), while the distribution of MCV was not significantly different between liver transplant recipients and controls. In logistic regression analysis adjusted for age and sex, anemia was associated with a borderline significant increase in odds of reporting lack of energy (OR 1.8 [95% CI: 0.97–3.33], p = 0.06). However, no significant association was found between anemia and breathlessness (OR 1.03 [95% CI: 0.60–1.77], p = 0.91).
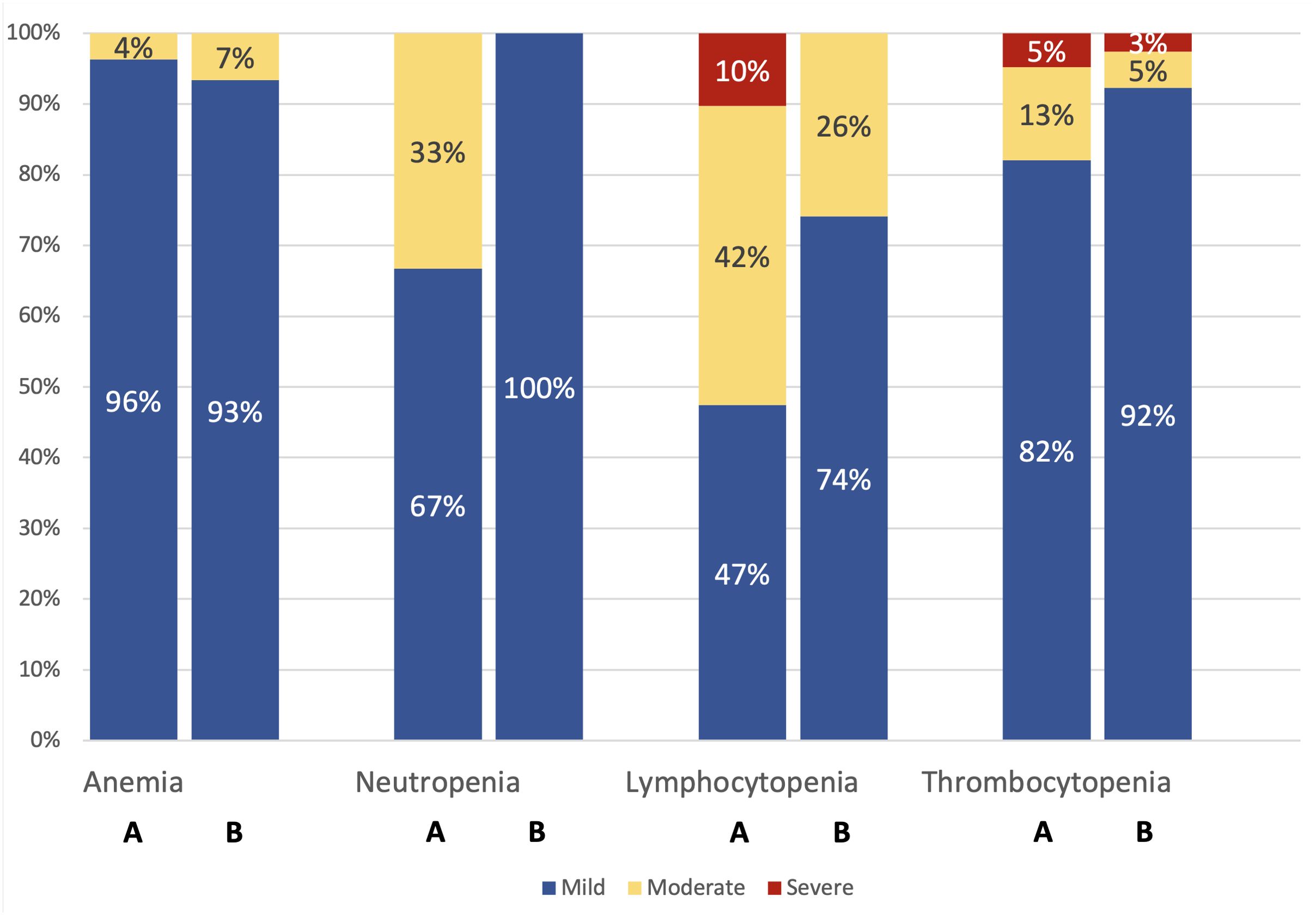
Figure 1. For each cytopenia (anemia, neutropenia, lymphocytopenia, and thrombocytopenia), bar A represents liver transplant recipients, and bar B represents controls. The severity of cytopenia, expressed as a percentage, was assessed only among participants with cytopenia. P-values for comparison between liver transplant recipients and controls: Anemia: p = 0.65; Neutropenia: p = 1.00; Lymphocytopenia: p = 0.03; Thrombocytopenia: p = 0.33.
The median neutrophil count was lower in liver transplant recipients (median IQR, 3.6 x 109 cells/L [2.7 – 4.8] vs 3.8 x 109 cells/L [3.1 – 4.7], p=0.009), with a higher prevalence of neutropenia (2.1% vs 0.1%, p<0.001). However, no significant differences were found in the severity of neutropenia between liver transplant recipients and controls with neutropenia (Figure 1).
The median lymphocytes count was lower in liver transplant recipients (median IQR, 1.6 x 109 cells/L [1.1 – 2.0] vs 2.0 [1.6 – 2.4], p<0.001), with a higher prevalence of lymphocytopenia. (18.4% vs 1.5%, p<0.001). Among those with lymphocytopenia, liver transplant recipients had more severe cases than controls (Figure 1).
The median thrombocyte count was lower in liver transplant recipients (median IQR, 197 x 109 cells/L [162 – 247] vs 243 x 109 cells/L [207 – 280], p<0.001), with a higher prevalence of thrombocytopenia (19.2% vs 2.2%, p<0.001). However, no significant differences were found in the severity of thrombocytopenia (Figure 1).
The prevalence of both single cytopenia and bicytopenia were higher in liver transplant recipients than in controls (Figure 2). While majority of both groups had no cytopenia, 32.8% of liver transplant recipients had a single cytopenia compared to 5.6% in controls (Table 2). Bicytopenia was present in 25 (5.9%) liver transplant recipients, while this was only the case for one of the controls (0.1%). Pancytopenia was only found in one liver transplant recipient.
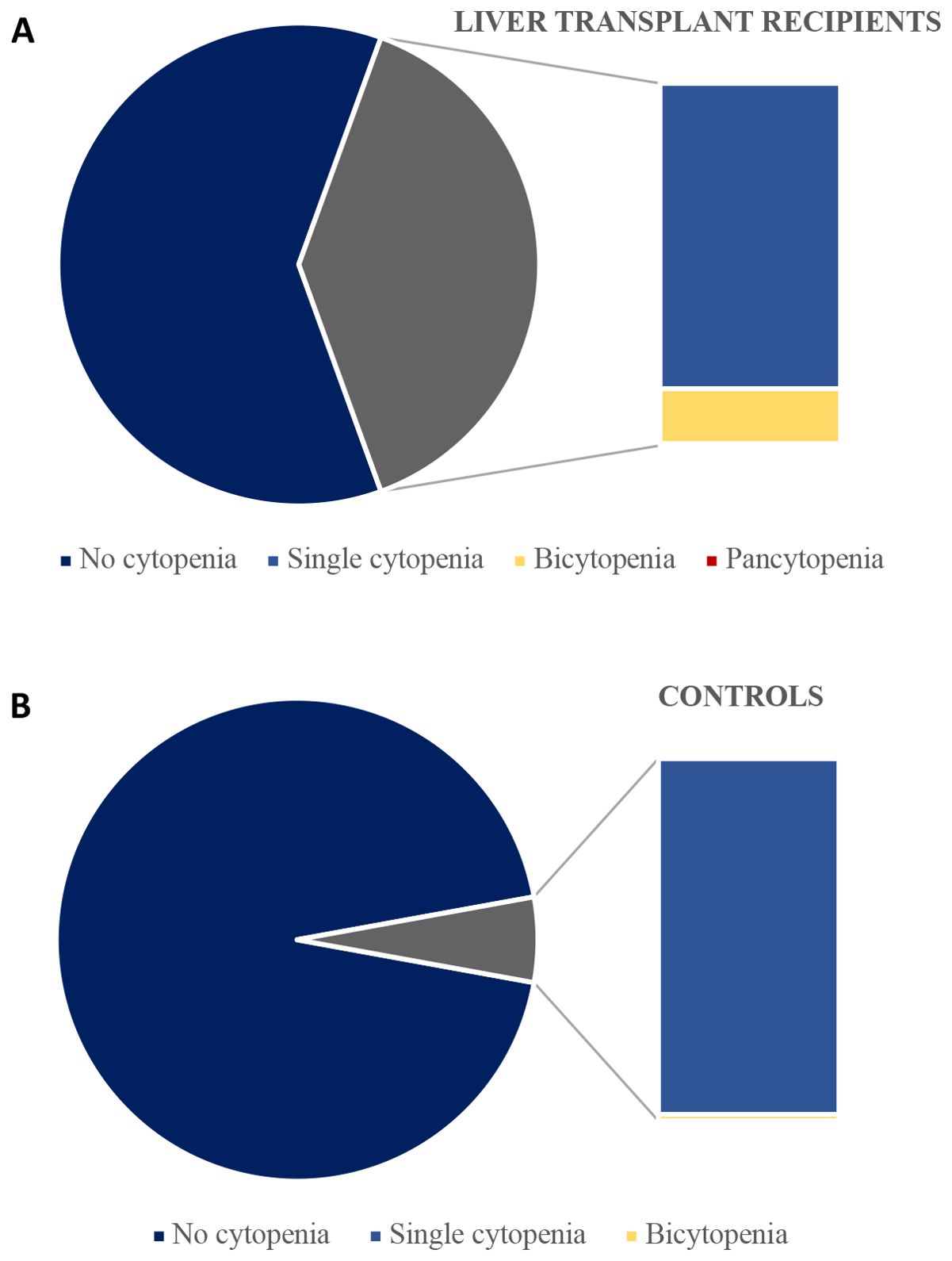
Figure 2. Prevalence of single-, bi- and pancytopenia among liver transplant recipients (A) and controls with complete data (B).
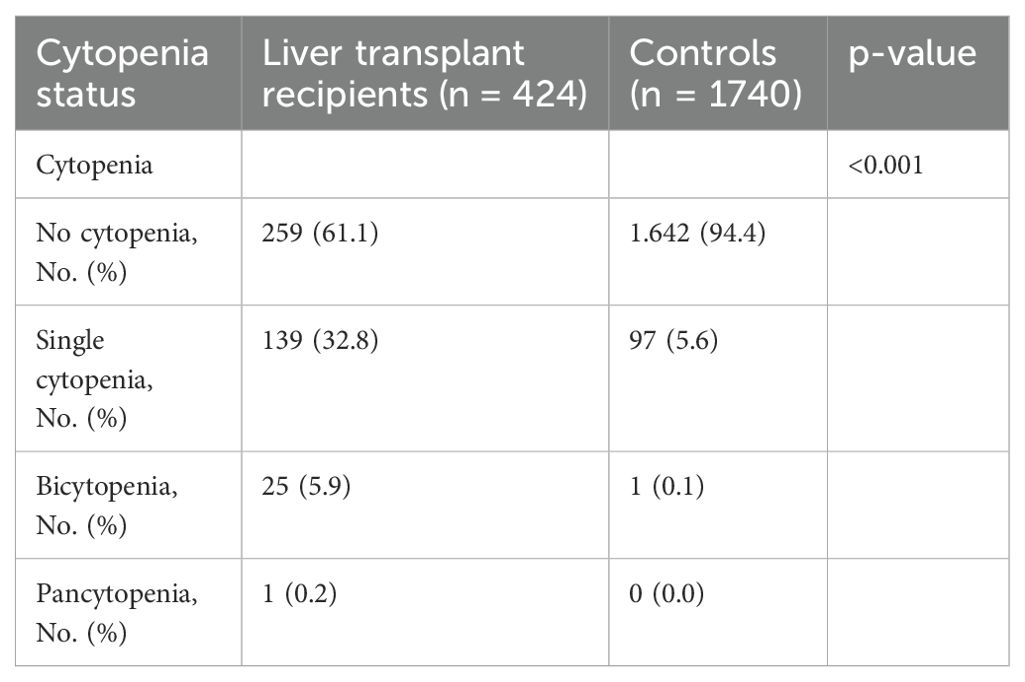
Table 2. Prevalence of single-, bi- and pancytopenia among liver transplant recipients and controls with complete data.
Risk factors associated with cytopenia in liver transplant recipients and controls
Living with a transplanted liver was associated with higher odds of anemia, lymphocytopenia, and thrombocytopenia both in the base model and after adjustment for age, sex, ethnicity, hs-CRP, smoking, and alcohol (adjusted odds ratio (aOR), 7.84 [95% confidence interval (CI): 5.04 – 12.18], p<0.001 for anemia, aOR 16.69 [95% CI: 9.56 – 29.12], p<0.001 for lymphocytopenia), and aOR 10.19 [95% CI: 6.07 – 17.13], p<0.001 for thrombocytopenia, Table 3). Living with a transplanted liver was associated with neutropenia in the base model adjusted for age and sex (OR 37.71 [4.76 – 298.50], p<0.001, Table 3). Adjusted analyses for neutropenia were not feasible as only one of the controls had neutropenia. These findings were further supported by our linear regression analyses among liver transplant recipients (Table 4).
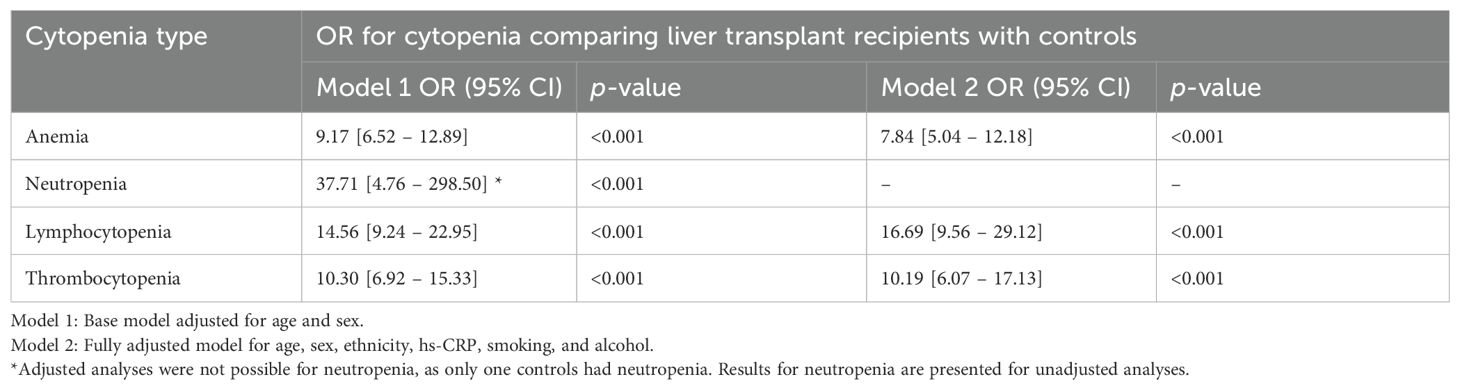
Table 3. Odds ratios for cytopenia comparing liver transplant recipients with controls.
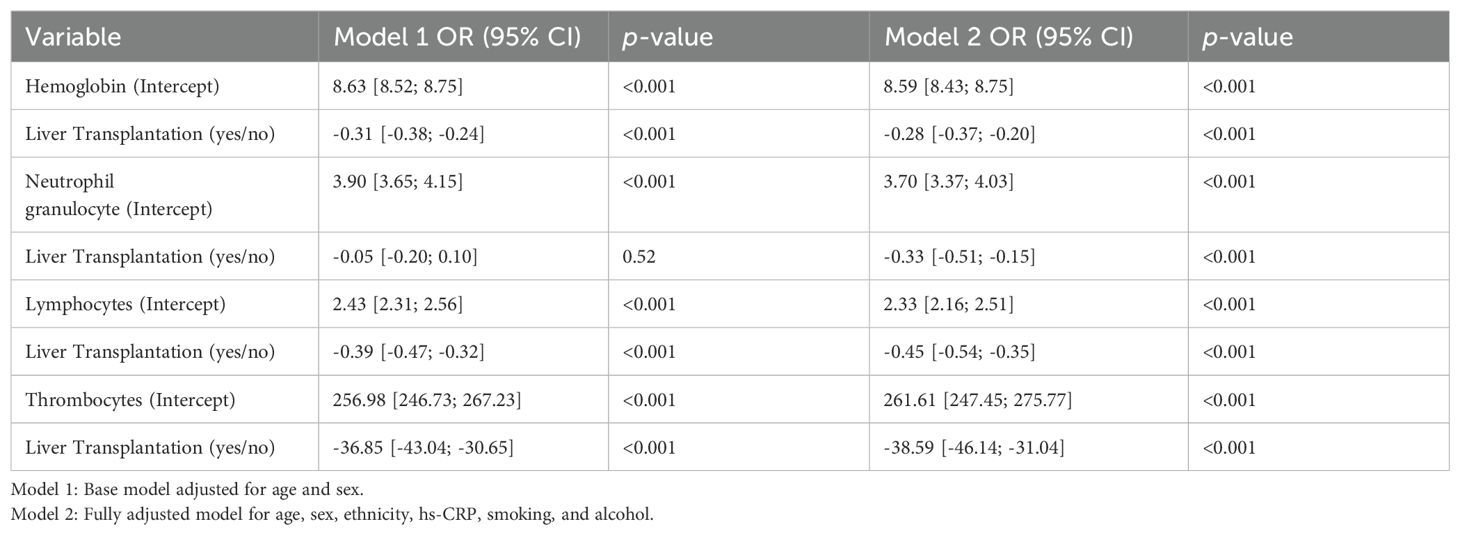
Table 4. Linear regression analysis of hemoglobin, neutrophile granulocytes, lymphocytes, and thrombocytes in liver transplant recipients.
Increasing age was associated with higher odds for anemia and lymphocytopenia in both univariate models and the fully adjusted model with potential risk factors (Supplementary Table 1). Male sex was associated with higher odds for anemia and thrombocytopenia in univariate analysis, however only remained significant for anemia in the fully adjusted model. Higher hs-CRP was associated with higher odds for lymphocytopenia in both univariate analyses and the fully adjusted model (Supplementary Table 1). No other factors were found to be significantly associated with cytopenias.
Liver transplantation related risk factors associated with cytopenias
No significant associations were found between specific types of immunosuppressive medication and cytopenia in analyses only including liver transplant recipients (Table 5). A shorter time since transplantation was associated with higher odds of anemia (OR 2.49 [95% CI: 1.56 – 3.99], p<0.001) and neutropenia (OR 4.48 [95% CI: 1.09 – 18.36], p<0.04) for participants between 1 – 5 years post-transplantation compared to >5 years post-transplantation in the base model after adjustment for age and sex and remained significant for anemia after full adjustment. No significant associations were found between cytopenias and the reason for transplantation or presence of cirrhosis at the time of transplantation. As a sensitivity analyses, we assessed the prevalence of cytopenias among liver transplant recipients with cirrhosis at time of transplantation compared to controls. Cytopenias were significantly more prevalent across all categories in liver transplant recipients. Anemia was observed in 26.5% of liver transplant recipients with cirrhosis at the time of transplantation compared to 3.5% of controls (p < 0.001), neutropenia in 2.2% versus 0.1% (p < 0.001), lymphocytopenia in 19.7% versus 1.5% (p < 0.001), and thrombocytopenia in 20.7% versus 2.2% (p < 0.001). The association between living with a transplanted liver and cytopenias remained consistent in analyses limited to patients with cirrhosis and in those excluding autoimmune liver disease as the indication for transplantation (Supplementary Tables 3, 4).
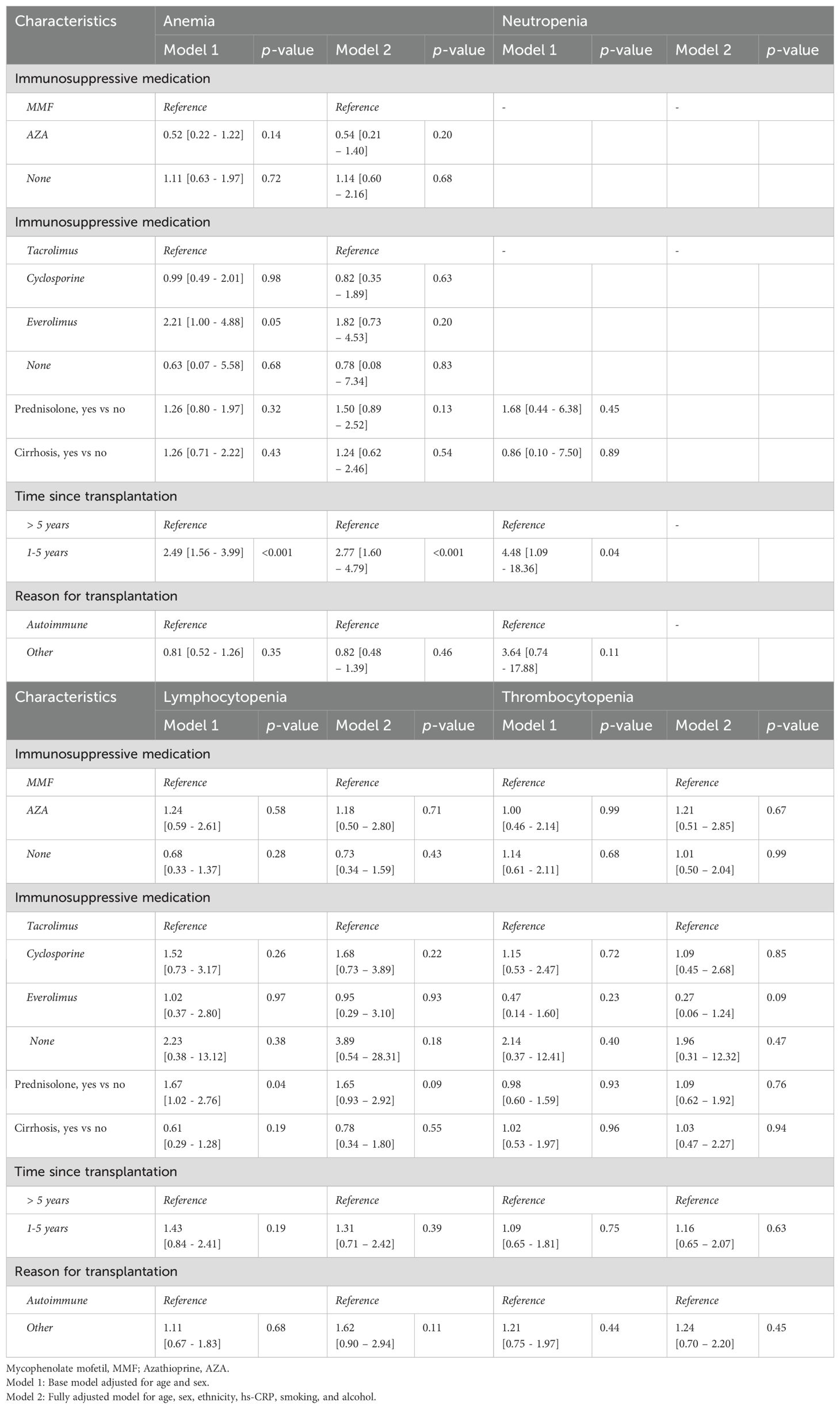
Table 5. Transplant-related risk factors for cytopenia in liver transplant recipients.
We found no statistically significant associations between tacrolimus trough levels and anemia, thrombocytopenia, and any type of cytopenia (Supplementary Table 5). In contrast, a borderline significant association with higher OR for lymphocytopenia was seen when tacrolimus trough levels increased (aOR 6.94 [95% CI: 0.71–67.62], p = 0.10). Furthermore, no significant differences were found in the prevalence of anemia, neutropenia, lymphocytopenia, and thrombocytopenia between liver transplant recipients with and without autoimmune liver disease (Table 6).
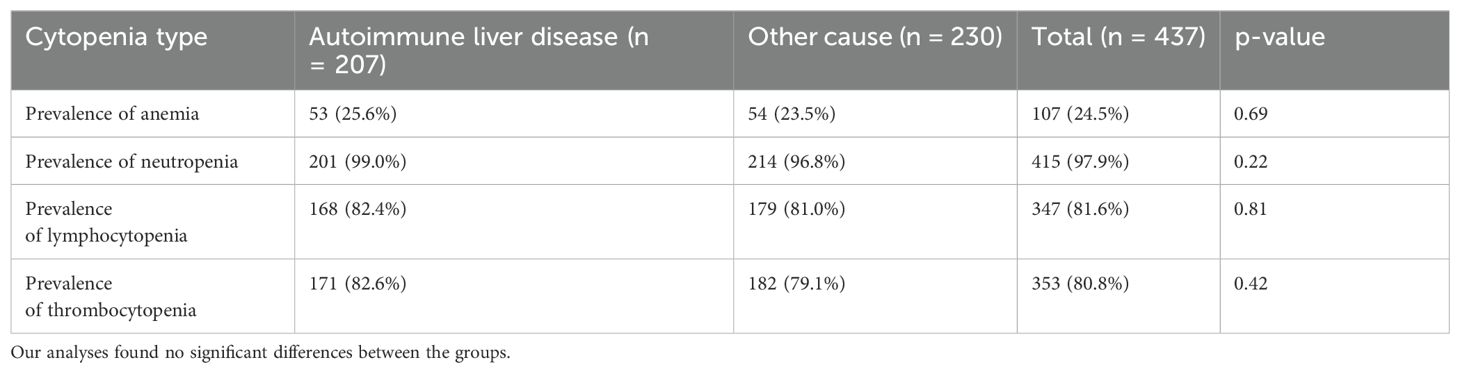
Table 6. Prevalence of anemia, neutropenia, lymphocytopenia and thrombocytopenia in patients with and without autoimmune liver disease.
Discussion
We found that living with a transplanted liver was independently associated with higher odds of anemia, lymphocytopenia and thrombocytopenia compared to controls from the general population. Male sex and shorter time since transplantation was associated with higher odds for anemia, while higher age was associated with anemia and lymphocytopenia, and higher levels of hs-CRP were associated with lymphocytopenia. No association was found between cytopenias and specific types of immunosuppressive treatments or cirrhosis at the time of transplantation.
The prevalence of anemia was higher in liver transplant recipients than controls and living with a transplanted liver was an independent risk factor for anemia. Furthermore, we found that male sex and shorter time since transplantation were associated with an increased risk of anemia. These results were consistent with other studies, in which even higher prevalence of anemia was observed one- and two-years post-transplantation, respectively (3, 23). However, the lack of consensus definition for anemia poses a challenge in comparing our results to existing literature. The severity of anemia was most commonly mild in both liver transplant recipients and controls with anemia with a similar distribution of anemia severity in the two groups. However, liver transplant recipients had more cases of hypochromatic anemia compared to controls. This finding is consistent with data from a prior study (3), which additionally found no significant impact of late onset of anemia on mortality or graft failure three years post-transplantation. The larger proportion of hypochromatic anemia may indicate iron deficiency that may, in part, be explained by underlying factors such as hemolysis, inflammation, malabsorption, or impaired utilization of iron post-transplantation (23, 31). Although, other causes of anemia such as bone marrow dysfunction cannot be ruled out. However, existing evidence has already identified hemoglobin levels as an independent risk factor for cardiovascular events, ischemic stroke and long-term mortality in patients with acute myocardial infarction (32–35). Overall identifying risk factors such as male sex and shorter time since transplantation to be associated with an increased risk of anemia may aid physicians on who to prioritize to proactively monitor at-risk patients with early intervention if necessary. While anemia in the general population is associated with impaired cognitive function, fatigue, cardiovascular strain, and higher mortality (30), anemia in liver transplant recipients may present additional challenges such as graft dysfunction and mortality (3). Due to the cross-sectional design of the study, clinical implications are difficult to assess. However, there was a borderline significant association between anemia and breathlessness. Further studies of the clinical presentation and clinical consequences of anemia in liver transplant recipients are warranted.
We found a prevalence of neutropenia of 2.1% in liver transplant recipients that were more than one-year post-transplantation. In contrast, previous studies have reported the prevalence of neutropenia ranging from 24% to 31% within the first-year post-transplantation (21, 36). The low prevalence of neutropenia among both liver transplant recipients and controls in our study precluded fully adjusted analyses of potential risk factors. However, neutropenia was still twenty times more prevalent among liver transplant recipients than controls. This increased prevalence of neutropenia may partly be explained by the use of immunosuppressive medications, due to bone marrow suppression and inhibition the production of neutrophil precursors (6). Existing evidence found an increased risk of infections, hematological malignancies, and mortality in neutropenic patients, with greater severity being associated with worse outcomes (37, 38).
Liver transplant recipients also had a higher prevalence of lymphocytopenia and more severe cases than controls, and living with a transplanted liver, higher hs-CRP levels and older age were independent risk factors for lymphocytopenia. Surprisingly, the specific types of immunosuppressive medications and prednisolone use were not associated with lymphocytopenia in our study, possibly due to confounding by indications. In our study, more than one in six liver transplant recipients had lymphocytopenia and among those with lymphocytopenia 10% had severe lymphocytopenia. Lymphocytopenia has been associated with increased susceptibility to infections (39–42) and worse cumulative survival in liver transplant recipients (43). While one study found lymphopenia to be associated with a 1.4-fold increased risk of infections and a 1.7-fold increased risk of mortality from infection in the general population (39). However, further studies are needed to assess the potential long-term impact of lymphocytopenia on morbidity and mortality in liver transplant recipients.
Liver transplant recipients had lower thrombocyte counts than controls and living with a transplanted liver was independently associated with higher odds of thrombocytopenia in our study. Older age and male sex were associated with higher odds of thrombocytopenia. Among liver transplant recipients, transplant-related risk factors such as specific types of immunosuppressive medications and cirrhosis at time of transplantation were not associated with thrombocytopenia. A previous study with serial measurement of thrombocytes found that the prevalence of thrombocytopenia declined from 54% one-year post-transplantation to 25% three-years post-transplantation (10), we found an even lower prevalence of thrombocytopenia (19.2%) among liver transplant recipients a median of 7.8 years after transplantation. However, we found no significant association between being 1–5 years post-transplantation compared to beyond 5 years post-transplantation and thrombocytopenia suggesting the effect of thrombocytopenia wanes before the fifth-year post-transplantation. Several factors may contribute to thrombocytopenia in liver transplant recipients, including reduced thrombocyte lifespan and reduced thrombocyte production. This could be due to a reduced release of the growth factor, thrombopoietin, which under normal circumstances is secreted from the liver. Finally, factors such as hypersplenism may also contribute to the development of thrombocytopenia. Although most cases of thrombocytopenia were either mild or moderate in our study, lower thrombocyte counts may still be associated with a higher risk of bleeding and infections (6, 44). Studies investigating serum levels of thrombopoietin, or the thrombocyte function may provide additional information about the pathogenesis.
Autoimmune liver disease was the most common cause of transplantation in the DACOLT cohort which is typical for Scandinavian populations. To address generalizability, we conducted two stratified analyses where we only included liver transplant recipients with cirrhosis at time of transplantation and excluded liver transplant recipients with autoimmune liver disease. Our results were consistent, indicating generalizability across different causes of liver transplantation.
Furthermore, we found no significant differences in cytopenia prevalence between recipients with autoimmune liver disease and those transplanted for other reasons, suggesting that the increased risk is not related to a specific indication for transplantation, but rather a general consequence of living with a transplanted liver.
Our study had limitations: First, recall bias cannot be excluded, as some information was collected from questionnaires, albeit this bias would be present in both liver transplant recipients and controls. Second, the absence of certain parameters in the blood samples resulted in an incomplete classification of anemia. Third, we were unable to assess if any cytopenia was symptomatic. Fourth, the cross-sectional study design limits our ability to assess whether any of the cytopenias were present prior to transplantation. Fifth, the lack of kidney function in our analyses limited our ability to explore its impact, which could have helped to better understand the underlying mechanisms. Furthermore, the cross-sectional design of the study limits our ability to establish causality and to determine clinical consequences of the finding. However, our study also had several strengths: First, the large population in the DACOLT and CGPS and the use of identical standard operating procedures in both studies allow for consistency and comparability in data collection and analysis. Second, we addressed all cytopenias according to the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0 to ensure a standardized approach for future studies. Finally, through the Shared Medication Record (FMK) and extensive journal entries, we have complete and thorough dataset of transplant-related variables in our cohort to eliminate potential selection and recall bias.
In conclusion, liver transplant recipients had a higher prevalence of cytopenias compared to the general population and living with a transplanted liver was independently associated with anemia, thrombocytopenia, and lymphocytopenia. Among liver transplant recipients, no association was found between cytopenias and specific types of immunosuppressive medication or cirrhosis at the time of transplantation. While our study revealed that almost 39% of liver transplant recipients experienced hematological abnormalities, additional research is needed to evaluate the clinical significance of cytopenia and the effectiveness of preventive measures in this patient population.
Data availability statement
The datasets presented in this article are not readily available because this study has the potential to determine prevalence, incidence and risk factors for development of comorbidity in liver transplant recipients and may be used to develop guidelines on screening, monitoring and long-term treatment of liver transplant recipients and thereby improve survival. Use of data will be confined to the study group, but potential collaborators or request for data can be submitted toZGFjb2x0LnJpZ3Nob3NwaXRhbGV0QHJlZ2lvbmguZGs=. Requests to access the datasets should be directed to DACOLT, ZGFjb2x0LnJpZ3Nob3NwaXRhbGV0QHJlZ2lvbmguZGs=.
Ethics statement
The studies involving humans were approved by the Ethics Committee of the Capital Region, Denmark (the DACOLT study (H-20052199) and the CGPS (H-KF-01-144/01)). The DACOLT study has been registered at ClinicalTrials.gov (NCT04777032). The studies were conducted according to the Declaration of Helsinki. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
KM: Writing – original draft, Writing – review & editing, Conceptualization. NA: Writing – review & editing, Conceptualization. JH: Conceptualization, Writing – review & editing. AJ: Conceptualization, Writing – review & editing. AF: Conceptualization, Writing – review & editing. GV: Conceptualization, Writing – review & editing. PH-F: Conceptualization, Writing – review & editing. SA: Conceptualization, Writing – review & editing. BN: Conceptualization, Writing – review & editing. PB: Conceptualization, Writing – review & editing. AR: Conceptualization, Writing – review & editing. SN: Conceptualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study received financial support from Kirsten and Freddy Johansens Foundation, SvendAndersen Foundation, Independent Research Foundation Denmark, Rigshospitalet’s Research Foundation.
Acknowledgments
The authors thank all the study participants.
Conflict of interest
PB has served on advisory boards for Roche, Gilead, Abbvie, and SERB. NA has received a PhD stipend from the Odense University Hospital Rigshospitalet’s Research Fund.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgstr.2025.1543618/full#supplementary-material
References
1. Takahashi K, Nagai S, Safwan M, Liang C, and Ohkohchi N. Thrombocytopenia after liver transplantation: Should we care? World J Gastroenterol. (2018) 24:1386–97. doi: 10.3748/wjg.v24.i13.1386
2. Takahashi K, Nagai S, Putchakayala KG, Safwan M, Li AY, Kane WJ, et al. Prognostic impact of postoperative low platelet count after liver transplantation. Clin Transplant. (2017) 31. doi: 10.1111/ctr.12891
3. Berger T, Reisler I, Shochat T, Raanani P, Nesher E, Mor E, et al. Post-liver transplantation anemia and its correlation with mortality and graft failure. Dig Dis Sci. (2020) 65:3040–51. doi: 10.1007/s10620-019-06021-7
4. Terrault NA, Francoz C, Berenguer M, Charlton M, and Heimbach J. Liver transplantation 2023: status report, current and future challenges. Clin Gastroenterol Hepatology. (2023) 21:2150–66. doi: 10.1016/j.cgh.2023.04.005
5. Guitard J, Ribes D, Kamar N, Muscari F, Lavayssière L, Suc B, et al. Predictive factors for anemia six and twelve months after orthotopic liver transplantation. Transplantation. (2006) 81:1525–31. doi: 10.1097/01.tp.0000209602.54351.a6
6. Barry M, Chandra S, and Hymes KB. Cytopenias in transplant patients. In: Principles and practice of transplant infectious diseases. Springer New York, New York, NY (2019). p. 199–207. doi: 10.1007/978-1-4939-9034-4_10
7. Maheshwari A, Mishra R, and Thuluvath PJ. Post-liver-transplant anemia: etiology and management. Liver Transpl. (2004) 10:165–73. doi: 10.1002/lt.20031
8. Stanca CM, Fiel MI, Aledort L, Cohen E, del Rio Martin J, and Schiano TD. Factors associated with persistent thrombocytopenia after liver transplantation. Transplant Proc. (2010) 42:1769–73. doi: 10.1016/j.transproceed.2010.02.075
9. Chatzipetrou MA, Tsaroucha AK, Weppler D, Pappas PA, Kenyon NS, Nery JR, et al. THROMBOCYTOPENIA AFTER LIVER TRANSPLANTATION. Transplantation. (1999) 67:702–6. doi: 10.1097/00007890-199903150-00010
10. Sutedja DS, Wai CT, Teoh KF, Lee HL, Dacosta M, Kaur M, et al. Persistent thrombocytopenia in liver transplant patients. In: Transplantation Proceedings. Elsevier Science Inc. (2004). p. 2331–3. doi: 10.1016/j.transproceed.2004.07.001
11. Richards EM, Alexander GJM, Calne RY, and Baglin TP. Thrombocytopenia following liver transplantation is associated with platelet consumption and thrombin generation. Br J Haematol. (1997) 98:315–21. doi: 10.1046/j.1365-2141.1997.2363056.x
12. Pamecha V, Mahansaria SS, Kumar S, Bharathy KGS, Sasturkar SV, Sinha PK, et al. Association of thrombocytopenia with outcome following adult living donor liver transplantation. Transpl Int. (2016) 29:1126–35. doi: 10.1111/tri.12819
13. Adport® - information til sundhedsfaglige - Medicin.dk. Available online at: https://pro.medicin.dk/Medicin/Praeparater/6208a060 (Accessed December 7, 2023).
14. Prednisolon “DAK” - information til sundhedsfaglige - Medicin.dk. Available online at: https://pro.medicin.dk/Medicin/Praeparater/56a060 (Accessed December 7, 2023).
15. Cellcept® - information til sundhedsfaglige - Medicin.dk. Available online at: https://pro.medicin.dk/Medicin/Praeparater/1903 (Accessed December 7, 2023).
16. Brum S, Nolasco F, Sousa J, Ferreira A, Possante M, Pinto JR, et al. Leukopenia in kidney transplant patients with the association of valganciclovir and mycophenolate mofetil. Transplant Proc. (2008) 40:752–4. doi: 10.1016/j.transproceed.2008.02.048
17. Abbas F, El Kossi M, Shaheen IS, Sharma A, and Halawa A. Drug-induced myelosuppression in kidney transplant patients. Exp Clin Transplantation. (2021) 19:999–1013. doi: 10.6002/ect.2020.0100
18. Khalil MAM, Khalil MAU, Khan TFT, and Tan J. Drug-induced hematological cytopenia in kidney transplantation and the challenges it poses for kidney transplant physicians. J Transplant. (2018) 2018:1–22. doi: 10.1155/2018/9429265
19. Valganciclovir “Accord” - information til sundhedsfaglige - Medicin.dk . Available online at: https://pro.medicin.dk/Medicin/Praeparater/8586a060 (Accessed December 7, 2023).
20. Sulfametoxazol med trimetoprim “SAD”, komb. - information til sundhedsfaglige - Medicin.dk. Available online at: https://pro.medicin.dk/Medicin/Praeparater/3151a060 (Accessed December 7, 2023).
21. Alraddadi B, Nierenberg NE, Price LL, Chow JKL, Poutsiaka DD, Rohrer RJ, et al. Characteristics and outcomes of neutropenia after orthotopic liver transplantation. Liver Transpl. (2016) 22:217–25. doi: 10.1002/lt.24332
22. Smith EP. Hematologic Disorders after Solid Organ Transplantation . Available online at: http://ashpublications.org/hematology/article-pdf/2010/1/281/1492296/bep00110000281.pdf (Accessed December 16, 2023).
23. Hegland NØ, Rezahosseini O, Pedersen CR, Møller DL, Bugge TB, Wareham NE, et al. Anemia in liver transplant recipients: prevalence, severity, risk factors, and survival. APMIS. (2023) 132(3):152-160. doi: 10.1111/apm.13364
24. Eyraud D, Granger B, Ionescu C, Fratéa S, Darnat S, Vaillant JC, et al. Thrombocytopenia, splenomegaly, and portal blood flow in patients who have undergone liver transplantation for cirrhosis. Liver Transplantation. (2012) 18:340–6. doi: 10.1002/lt.22456
25. Ishigami M, Ishizu Y, Onishi Y, Kamei H, Kiuchi T, Itoh A, et al. Long-term dynamics of hematological data and spleen volume in cirrhotic patients after liver transplantation-various dynamics depending on etiology. Springerplus. (2013) 2:1–9. doi: 10.1186/2193-1801-2-374
26. Thomsen MT, Høgh J, Knudsen AD, Jensen AMR, Gelpi M, Villadsen GE, et al. The Danish comorbidity in liver transplant recipients study (DACOLT): a non-interventional prospective observational cohort study. BMC Gastroenterol. (2021) 21:145. doi: 10.1186/s12876-021-01733-5
27. Bergholdt HKM, Bathum L, Kvetny J, Rasmussen DB, Moldow B, Hoeg T, et al. Study design, participation and characteristics of the danish general suburban population study. Dan Med J. (2013) 60:A4693–3.
28. Mortensen MB, Afzal S, Nordestgaard BG, and Falk E. The high-density lipoprotein-adjusted SCORE model worsens SCORE-based risk classification in a contemporary population of 30 824 Europeans: the Copenhagen General Population Study. Available online at: https://academic.oup.com/eurheartj/article/36/36/2446/2398213 (Accessed September 27, 2023).
29. Sundhedsdatastyrelsen. FMK for sundhedsprofessionelle . Available online at: https://sundhedsdatastyrelsen.dk/da/registre-og-services/om-faelles-medicinkort (Accessed September 26, 2023).
30. U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES. Common Terminology Criteria for Adverse Events (CTCAE) (2017). Available online at: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.pdf (Accessed September 28, 2023).
32. Houghton DE, Koh I, Ellis A, Key NS, Douce DR, Howard G, et al. Hemoglobin levels and coronary heart disease risk by age, race, and sex in the reasons for geographic and racial differences in stroke study (REGARDS). Am J Hematol. (2020) 95:258–66. doi: 10.1002/ajh.25703
33. Colombo MG, Kirchberger I, Amann U, Heier M, Thilo C, Kuch B, et al. Association between admission anemia and long-term mortality in patients with acute myocardial infarction: results from the MONICA/KORA myocardial infarction registry. BMC Cardiovasc Disord. (2018) 18:50. doi: 10.1186/s12872-018-0785-5
34. Sarnak MJ, Tighiouart H, Manjunath G, MacLeod B, Griffith J, Salem D, et al. Anemia as a risk factor for cardiovascular disease in the atherosclerosis risk in communities (aric) study. J Am Coll Cardiol. (2002) 40:27–33. doi: 10.1016/s0735-1097(02)01938-1
35. Heo J, Youk TM, and Seo KD. Anemia is a risk factor for the development of ischemic stroke and post-stroke mortality. J Clin Med. (2021) 10:2556. doi: 10.3390/jcm10122556
36. Mavrakanas TA, Fournier MA, Clairoux S, Amiel JA, Tremblay ME, Vinh DC, et al. Neutropenia in kidney and liver transplant recipients: Risk factors and outcomes. Clin Transplant. (2017) 31. doi: 10.1111/ctr.13058
37. Boxer LA. How to approach neutropenia . Available online at: http://ashpublications.org/hematology/article-pdf/2012/1/174/1501776/bep00112000174.pdf (Accessed January 24, 2024).
38. Andersen CL, Tesfa D, Siersma VD, Sandholdt H, Hasselbalch H, Bjerrum OW, et al. Prevalence and clinical significance of neutropenia discovered in routine complete blood cell counts: a longitudinal study. J Intern Med. (2016) 279:566–75. doi: 10.1111/joim.12467
39. Warny M, Helby J, Nordestgaard BG, Birgens H, and Bojesen SE. Lymphopenia and risk of infection and infection-related death in 98,344 individuals from a prospective Danish population-based study. PloS Med. (2018) 15. doi: 10.1371/journal.pmed.1002685
40. Elçioğlu Z, Errington L, Metes B, Sendama W, Powell J, Simpson A, et al. Pooled prevalence of lymphopenia in all-cause hospitalisations and association with infection: a systematic review and meta-analysis. BMC Infect Dis. (2023) 23. doi: 10.1186/s12879-023-08845-1
41. Chang CJ, Chen LY, Liu LK, Lin MH, Peng LN, and Chen LK. Lymphopenia and poor performance status as major predictors for infections among residents in long-term care facilities (LTCFs): a prospective cohort study. Arch Gerontol Geriatr. (2014) 58:440–5. doi: 10.1016/j.archger.2013.12.001
42. Merayo-Chalico J, Gómez-Martín D, Piñeirúa-Menéndez A, Santana-De Anda K, and Alcocer-Varela J. Lymphopenia as risk factor for development of severe infections in patients with systemic lupus erythematosus: a case-control study. QJM. (2013) 106:451–7. doi: 10.1093/qjmed/hct046
43. Nagai S, Mangus RS, Anderson E, Ekser B, Kubal CA, Burch T, et al. Post-transplant persistent lymphopenia is a strong predictor of late survival in isolated intestine and multivisceral transplantation. Transplant Int. (2015) 28:1195–204. doi: 10.1111/tri.12620
Keywords: cytopenia, anemia, neutropenia, lymphocytopenia, thrombocytopenia, liver transplantation, LTX, liver transplant receipients
Citation: Manogarathaas K, Arentoft NS, Hillingsø JG, Jensen AMR, Fialla AD, Villadsen GE, Holland-Fischer P, Afzal S, Nordestgaard BG, Brown P, Rasmussen A and Nielsen SD (2025) Living with a transplanted liver is associated with cytopenias: a nationwide cohort study. Front. Gastroenterol. 4:1543618. doi: 10.3389/fgstr.2025.1543618
Received: 11 December 2024; Accepted: 03 July 2025;
Published: 06 August 2025.
Edited by:
Palash Mandal, Charotar University of Science and Technology, IndiaReviewed by:
Yongbing Qian, Shanghai Jiao Tong University, ChinaAmol Rangnekar, MedStar Georgetown Transplant Institute, United States
Copyright © 2025 Manogarathaas, Arentoft, Hillingsø, Jensen, Fialla, Villadsen, Holland-Fischer, Afzal, Nordestgaard, Brown, Rasmussen and Nielsen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susanne D. Nielsen, c2RuQGRhZGxuZXQuZGs=