 Ashley van der Spek1
Ashley van der Spek1 Annemarie I. Luik2
Annemarie I. Luik2 Desana Kocevska3
Desana Kocevska3 Chunyu Liu4,5,6
Chunyu Liu4,5,6 Rutger W. W. Brouwer7
Rutger W. W. Brouwer7 Jeroen G. J. van Rooij8,9,10
Jeroen G. J. van Rooij8,9,10 Mirjam C. G. N. van den Hout7
Mirjam C. G. N. van den Hout7 Robert Kraaij1,8,9Albert Hofman1,11
Robert Kraaij1,8,9Albert Hofman1,11 André G. Uitterlinden1,8,9
André G. Uitterlinden1,8,9 Wilfred F. J. van IJcken7
Wilfred F. J. van IJcken7 Daniel J. Gottlieb12,13,14Henning Tiemeier1,15
Daniel J. Gottlieb12,13,14Henning Tiemeier1,15 Cornelia M. van Duijn1Najaf Amin1*
Cornelia M. van Duijn1Najaf Amin1*- 1Department of Epidemiology, Erasmus Medical Center, Rotterdam, Netherlands
- 2Sleep and Circadian Neuroscience Institute, Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, United Kingdom
- 3Department of Child and Adolescent Psychiatry, Erasmus Medical Center, Rotterdam, Netherlands
- 4Framingham Heart Study, National Heart, Lung, and Blood Institute, Framingham, MA, United States
- 5Population Sciences Branch, National Heart, Lung, and Blood Institute, Bethesda, MD, United States
- 6Department of Biostatistics, School of Public Health, Boston University, Boston, MA, United States
- 7Center for Biomics, Erasmus Medical Center, Rotterdam, Netherlands
- 8Department of Internal Medicine, Erasmus Medical Center, Rotterdam, Netherlands
- 9Netherlands Consortium for Healthy Ageing, Rotterdam, Netherlands
- 10Department of Neurology, Erasmus Medical Center, Rotterdam, Netherlands
- 11Department of Epidemiology, Harvard T. H. Chan School of Public Health, Boston, MA, United States
- 12VA Boston Healthcare System, Boston, MA, United States
- 13Departments of Medicine and Neurology, Brigham and Women's Hospital, Boston, MA, United States
- 14Division of Sleep Medicine, Harvard Medical School, Boston, MA, United States
- 15Department of Psychiatry, Erasmus Medical Center, Rotterdam, Netherlands
Obstructive sleep apnea (OSA) is a common sleep breathing disorder associated with an increased risk of cardiovascular and cerebrovascular diseases and mortality. Although OSA is fairly heritable (~40%), there have been only few studies looking into the genetics of OSA. In the present study, we aimed to identify genetic variants associated with symptoms of sleep apnea by performing a whole-exome sequence meta-analysis of symptoms of sleep apnea in 1,475 individuals of European descent. We identified 17 rare genetic variants with at least suggestive evidence of significance. Replication in an independent dataset confirmed the association of a rare genetic variant (rs2229918; minor allele frequency = 0.3%) with symptoms of sleep apnea (p-valuemeta = 6.98 × 10−9, βmeta = 0.99). Rs2229918 overlaps with the 3′ untranslated regions of ERCC1 and CD3EAP genes on chromosome 19q13. Both genes are expressed in tissues in the neck area, such as the tongue, muscles, cartilage and the trachea. Further, CD3EAP is localized in the nucleus and mitochondria and involved in the tumor necrosis factor-alpha/nuclear factor kappa B signaling pathway. Our results and biological functions of CD3EAP/ERCC1 genes suggest that the 19q13 locus is interesting for further OSA research.
Introduction
Sleep is a complex and essential biological process that has been conserved across diverse animal species throughout evolution (Rechtschaffen, 1998). Although normal healthy sleep highly varies within and between adults (Van Dongen et al., 2005; Knutson et al., 2007; Mezick et al., 2009), it has to consist of adequate duration, good quality, proper timing and regularity, and the absence of sleep disturbances or disorders (Consensus Conference Panel et al., 2015). Several large epidemiological studies have shown that short or disturbed sleep is associated with various cognitive (Pilcher and Huffcutt, 1996; Yaffe et al., 2014), psychiatric (Lovato and Gradisar, 2014; Peters van Neijenhof et al., 2016; Cosgrave et al., in press) and health consequences e.g., diabetes mellitus (Gottlieb et al., 2005; Yaggi et al., 2006), activation of pro-inflammatory pathways (Patel et al., 2009), and cardiovascular diseases (Hoevenaar-Blom et al., 2011). One of the most common causes of short and disturbed sleep is sleep apnea.
Sleep apnea is a highly prevalent (Peppard et al., 2013) sleep breathing disorder, with obstructive sleep apnea (OSA) as the most common type (Mehra et al., 2007). OSA affects up to 38% of the general adult population (Senaratna et al., 2016) and untreated OSA has been associated with severe health problems (Young et al., 2002a) such as hypertension (Peppard et al., 2000; Pedrosa et al., 2011), cardiovascular disease (Shamsuzzaman et al., 2003; Marin et al., 2005; Gottlieb et al., 2010), stroke (Yaggi et al., 2005), type 2 diabetes (Shaw et al., 2008; Aurora and Punjabi, 2013; Kendzerska et al., 2014), impaired cognitive function (Kim et al., 1997; Yaffe et al., 2011), depression (Peppard et al., 2006), and increased mortality (Marshall et al., 2008; Young et al., 2008; Punjabi et al., 2009). The main characteristic of OSA is the partial or complete obstruction of the upper airways during sleep, causing oxyhemoglobin desaturations and arousals from sleep. This leads to sleep fragmentation and decreased periods of slow wave and REM sleep (McNicholas, 2008; American Academy of Sleep Medicine, 2014). Consequently, the two most common signs and symptoms of OSA are snoring and excessive daytime sleepiness (Gottlieb et al., 1999) where the latter can result in personal and occupational problems, and an increased risk of traffic and work-related accidents (Young et al., 2002a; McNicholas, 2008; American Academy of Sleep Medicine, 2014).
OSA is a complex trait influenced by both environment and genetics (Redline et al., 1995; Redline and Tishler, 2000) with obesity, age, and sex as most important risk factors (Redline et al., 1994; Bixler et al., 2001; Young et al., 2002a,b, 2004; Peppard et al., 2013). About 40% of the variance in apneic activity can be explained by genetic factors (Redline et al., 1995). At least half of the genetic contribution to sleep apnea acts through mechanisms independent of obesity (Patel et al., 2008). Previous genetic studies have focused on several candidate genes for breathing disorders, where the most studied genes are the angiotensin-converting enzyme gene (ACE) (Lin et al., 2004; Bostrom et al., 2007; Patel et al., 2007); apolipoprotein, allele E4 (APOE ϵ4) (Kadotani et al., 2001; Gottlieb et al., 2004); serotonin receptors and transporters genes (5-HT2A, 5-HT2C, 5-HTT) (Sakai et al., 2005; Ylmaz et al., 2005; Bayazit et al., 2006; Larkin et al., 2010; Qin et al., 2014); adrenergic receptors (ADRB2/3) (Mills et al., 1995; Grote et al., 2000); and tumor necrosis factor (TNF) (Riha et al., 2005; Popko et al., 2008; Bhushan et al., 2009). However, the results of these studies have been inconsistent or have yet to be confirmed (Sleiman and Hakonarson, 2011). Using linkage analysis, a method to identify the chromosomal location of the disease influencing genes, two regions on chromosome 2p16 and 19q13 were found to be suggestively linked with OSA independent of obesity (Palmer et al., 2003). Genome wide association studies (GWASs) could provide more information on common variants involved in the pathogenesis of OSA. Until now only a few GWASs have been reported for OSA. Loci in GPR83 and C6ORF183/CCDC162P were found to be significantly associated with OSA (Cade et al., 2016), and a locus in the neuregulin-1 (NRG1) gene was suggestively implicated (Baik et al., 2015). Two other studies used customized or targeted genotyping arrays and identified loci in PPARGC1B (Kripke et al., 2015), PTGER3 (Patel et al., 2012), PLEK (Patel et al., 2012), and LPAR1 (Patel et al., 2012) to be associated with OSA. However, most of these findings were not replicated. Consequently, the genetic architecture of OSA remains largely unexplored.
In the present study we aimed to identify genetic variants associated with symptoms of sleep apnea, assessed using the Pittsburgh Sleep Quality Index (PSQI). We performed a GWAS using whole-exome sequence (WES) data of 1,475 individuals from two Dutch studies. Subsequently, we replicated our findings in an independent sample.
Materials and Methods
Study Populations
Discovery Cohorts
The discovery sample consists of participants from two cohorts including the Erasmus Rucphen Family (ERF) study and the Rotterdam Study (RS) from The Netherlands.
ERF is a family-based study that includes inhabitants of a genetically isolated community in the Southwest of the Netherlands, ascertained as part of the Genetic Research in Isolated Population program. The ERF cohort includes ~3,000 living descendants of 22 founder couples, who had at least six children baptized in the community church. Individuals who were 18 years or older were invited to participate in the study. Data was collected between 2002 and 2005 (Pardo et al., 2005). The study was approved by the Medical Ethics Committee of the Erasmus Medical Center (EMC), Rotterdam, The Netherlands. All participants provided written informed consent and all investigations were carried out in accordance with the Declaration of Helsinki.
RS is a prospective cohort study ongoing since 1990, which aims to investigate determinants of disease occurrence and progression in the elderly (Hofman et al., 2015). Initially, the RS included 7,983 individuals of 55 years of age or over, living in the well-defined Ommoord district in Rotterdam, The Netherlands. All participants were examined at baseline by an at home interview and an extensive set of examinations in the research facility in Ommoord. The RS was approved by the Medical Ethics Committee of the EMC and by the Ministry of Health, Welfare and Sport of the Netherlands. All participants provided written informed consent to participate in the study. All investigations were carried out in accordance with the Declaration of Helsinki.
Study participants from ERF and RS were assessed for sleep phenotypes using a self-administered questionnaire including questions from the PSQI (Buysse et al., 1989). The PSQI has been specifically designed to measure sleep quality and sleep disturbances over a 1-month time interval. Symptoms of sleep apnea were assessed by asking the participants “How often did you or your partner notice long pauses between breaths while asleep?” Answers were provided on a categorical scale ranging from 1 to 4 (1. not during the past month; 2. less than once per week; 3. once or twice per week; 4. more than twice per week). Symptoms of sleep apnea were assessed in 1,366 ERF participants and 2,660 RS participants, where for the latter data of the fourth visit was used as it had the largest participation.
Replication Cohort
The replication sample included participants from the offspring cohort of the population-based prospective Framingham Heart Study (FHS) (Dawber et al., 1951). The offspring cohort was recruited between 1971 and 1975, including 5,124 offspring of the original FHS cohort and their spouses (Kannel et al., 1979). The study was approved by the Institutional Review Board for Human Research of the Boston University Medical Center, Boston, MA, USA. Each participant provided written informed consent.
FHS has collected sleep data using the Sleep Heart Health Study sleep habits questionnaire (Quan et al., 1997). Symptoms of sleep apnea scores were constructed as a combination of the following questions: “A. Are there times when you stop breathing during your sleep?” with answers “yes”, ”no”, “I don't know” and “B. If yes to question A: How often do you have times when you stop breathing during your sleep?”. Answers to question B were provided on a categorical scale ranging from 1 to 5 (1. Rarely, less than one night per week; 2. Sometimes, one or two nights per week; 3. Frequently, three to five nights per week; 4. always or almost always, six or seven nights per week; 5. I don't know). Individuals with answers “I don't know” were excluded, since this option is not available in the PSQI. The constructed symptoms of sleep apnea score had answers ranging from 1 to 4, matching the PSQI: 1. not during the past month (A2); 2. less than once per week (A1 and B1); 3. once or twice per week (A1 and B2); 4. more than twice per week (A1 and B3 or A1 and B4).
Sequencing and Quality Control
Discovery Cohorts
In ERF Genomic DNA was extracted from peripheral venous blood utilizing the salting out method (Miller et al., 1988). Exomes of 1,336 ERF participants were sequenced at the Erasmus Center for Biomics of the Cell Biology department of the EMC, The Netherlands, using the Agilent V4 capture kit on an Illumina HiSeq2000 sequencing machine with the TruSeq Version 3 protocol (Amin et al., 2016b). The sequence reads were aligned to the human genome build 19 (hg19) using Burrows Wheeler Aligner (BWA) (Li and Durbin, 2009) and the NARWHAL pipeline (Brouwer et al., 2012). Aligned reads were further processed using IndelRealigner, MarkDuplicates and TableRecalibration tools from the Genome Analysis Toolkit (GATK) (Mckenna et al., 2010), and Picard (http://broadinstitute.github.io/picard/). Genetic variants were called using the GATK UnifiedGenotyper tool. Individuals with low concordance to genotyping array or with a low call rate and low quality variants (Phred quality score <30, call rate <90%) and out of Hardy-Weinberg equilibrium (HWE) (p < 10−6), were removed. The final dataset for ERF included 528,617 single nucleotide variants (SNVs) in 1,308 individuals (Amin et al., 2016b) of whom 654 individual also had phenotype data on symptoms of sleep apnea available.
Exomes of 2,628 individuals from the RS population were sequenced at the Human Genotyping facility of the Internal Medicine department at the EMC, the Netherlands, to an average depth of 54x using the Nimblegen SeqCap EZ V2 capture kit on an Illumina Hiseq2000 sequencer using the TruSeq Version 3 protocol (Amin et al., 2016b). The sequenced reads were aligned to hg19 using BWA (Li and Durbin, 2009). Subsequently, the aligned reads were processed further using Picard's MarkDuplicates, SAMtools (Li et al., 2009), and GATK (Mckenna et al., 2010). Genetic variants were called using the Haplotypecaller from GATK. Samples with low concordance to genotyping array (<95%), low transition to transversion ratio (<2.3) and high heterozygote to homozygote ratio (>2.0) were removed and additionally SNVs with a low call rate (<90%) and out of HWE (p < 10−8) were also removed from the data. The final dataset included 600,806 SNVs in 2,356 individuals (Amin et al., 2016a) of whom 821 individuals also had phenotype data on symptoms of sleep apnea available.
For both ERF and RS, file handling and formatting was done using VCFtools (Danecek et al., 2011) and PLINK (Purcell et al., 2007) (http://pngu.mgh.harvard.edu/purcell/plink/). Annotation of the variants was performed using SeattleSeq Annotation 138 (http://snp.gs.washington.edu/SeattleSeqAnnotation138/).
Replication Cohort
In FHS exomes of 1,271 participants were sequenced using Illumina HiSeq2000 and 2500 platforms. DNA samples were constructed into Illumina paired-end pre-capture libraries according to the manufacturer's protocol. For exome capture, two, four or six pre-capture libraries were pooled together and hybridized to the HGSC VCRome 2.1 design (Bainbridge et al., 2011) (42 Mb, NimbleGen). After sequencing the HGSC Mercury analysis pipeline (https://www.hgsc.bcm.edu/content/mercury) and Illumina CASAVA software were used to perform sequencing analysis and to de-multiplex the pooled samples. Sequenced reads were aligned to Genome Reference Consortium Human Build 37 (GRCh37) using BWA (Li and Durbin, 2009) producing BAM files (Li et al., 2009). The aligned reads were recalibrated using GATK (Depristo et al., 2011) together with BAM sorting, duplicate read marking, and realignment near insertions or deletions. SNVs, insertions and deletions were called using Atlas2 (Challis et al., 2012). SNVs were excluded with low SNV posterior probability (<0.95), low variant read count (<3), variant read ratio <0.25 or >0.75, strand-bias of more than 99% variant reads in a single strand direction, or total coverage <10. Reference calls with <10 × coverage were also set to missing. Variants were excluded outside exon capture regions (VCRome 2.1), multi-allelic sites, monomorphic sites, missing rate >20%, mappability score <0.8, mean depth of coverage >500, or not fulfilling HWE (p < 5 × 10−6). Samples were excluded with missingness >20%, less than 6 SD from mean depth, more than 6 SD for singleton count, or outside of 6 SD for heterozygous to homozygous ratio or transition to transversion ratio. Variants were annotated using ANNOVAR (Wang et al., 2010) and dbNSFP v2.0 (https://sites.google.com/site/jpopgen/dbNSFP) according to the GRCh37 reference genome and National Center for Biotechnology Information RefSeq. The final dataset included 1,749,755 SNVs in 1,271 individuals of whom 472 individuals also had phenotype data on symptoms of sleep apnea available.
Statistical Analyses
Descriptive analysis was performed using IBM SPSS Statistics version 21 (IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp.). Study specific exome analyses and meta-analysis of the individual study data were performed using the seqMeta v1.5 library of the R software (http://cran.r-project.org/web/packages/seqMeta/). Single variant association analysis was performed by assuming an additive effect. In ERF and FHS a linear mixed effects model was used adjusting for familial relationships by including the kinship matrix. To account for population stratification in the RS, we tested the association of ten principal components with the phenotype. None of them was significantly associated with symptoms of sleep apnea and we did not include them in the analysis. The regression analysis was performed using the four categories of symptoms of sleep apnea score as a continuous trait, adjusting for the three main risk factors for OSA; age, sex and body mass index (BMI) (kg/m2). Meta-analysis was performed using a fixed effects model. Variants that were present in both discovery cohorts (ERF and RS, 115,526 variants) were tested for association, giving a Bonferroni corrected p-value threshold of 4.3 × 10−7. All variants that showed significant or suggestive (p < 1.0 × 10−6) association signals in the discovery samples, were tested for replication in FHS. Bonferroni correction was also applied to correct for multiple testing in the replication stage.
Results
Descriptive statistics of the study populations are presented in Table 1. The mean age in RS was 75 years ( = 27.4 kg/m2), where the mean age in ERF was 46 years ( = 26.7 kg/m2) and 59 years in FHS ( = 27.5 kg/m2). The prevalence of symptoms of sleep apnea was higher in the ERF population, where 16.8% of the participants reported to have experienced apneas during the last month, compared to 11.6 and 6.6% of the RS and FHS participants, respectively (Table 2).
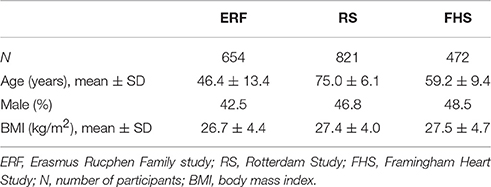
Table 1. Descriptive statistics of the study populations.
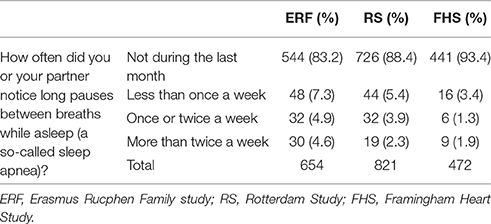
Table 2. Answers to the sleep apnea question for the discovery and replication populations.
The exome-wide association results and the distribution of the test statistic (λ = 1.02) are illustrated in Figures 1, 2 respectively. Significant associations of symptoms of sleep apnea were observed with six rare variants [minor allele frequency (MAF) <1%] (located in ACE, AIFM3, LIPJ, MUC2, AP2A2, SH3BP1) (Table 3). Suggestive associations of symptoms of sleep apnea were observed with 11 rare variants (located in KANK2, LCN6, TRAF3, PLEK, HIF1A, SLC45A3, ERCC1/CD3EAP, MRGPRE, GRAMD4, TYW5, CST5) (Table 3). Of all 17 variants, only seven were polymorphic in the replication sample and could be tested for association (Table 4). Of the six significantly associated variants, two could be tested for association with symptoms of sleep apnea in the FHS (located in MUC2 and SH3BP1).
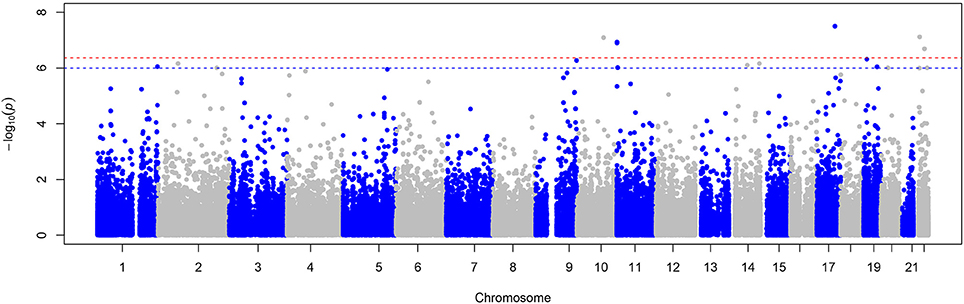
Figure 1. Manhattan plot of the meta-analysis of symptoms of sleep apnea. This plot shows −log10 transformed p-values (y-axis) for all SNPs present in the meta-analysis according to their position on each chromosome (x-axis). The red dashed line represents the Bonferroni corrected p-value threshold for significance (p < 4.3 × 10−7) and the blue dashed line indicates the threshold for suggestive associations (p < 1.0 × 10−6).
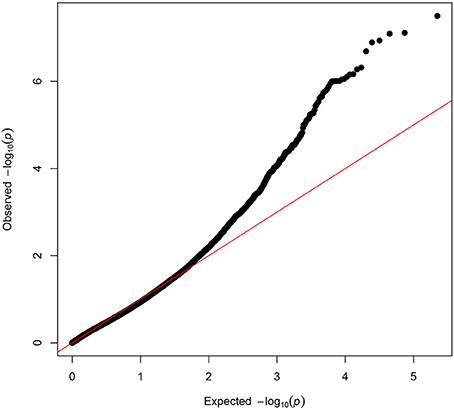
Figure 2. Quantile-Quantile plot of the meta-analysis of symptoms of sleep apnea. The QQ-plot shows the observed p-values plotted on the y-axis against the expected values of the test statistics on the x-axis (X2-distribution). The red line shows the distribution under the null hypothesis.
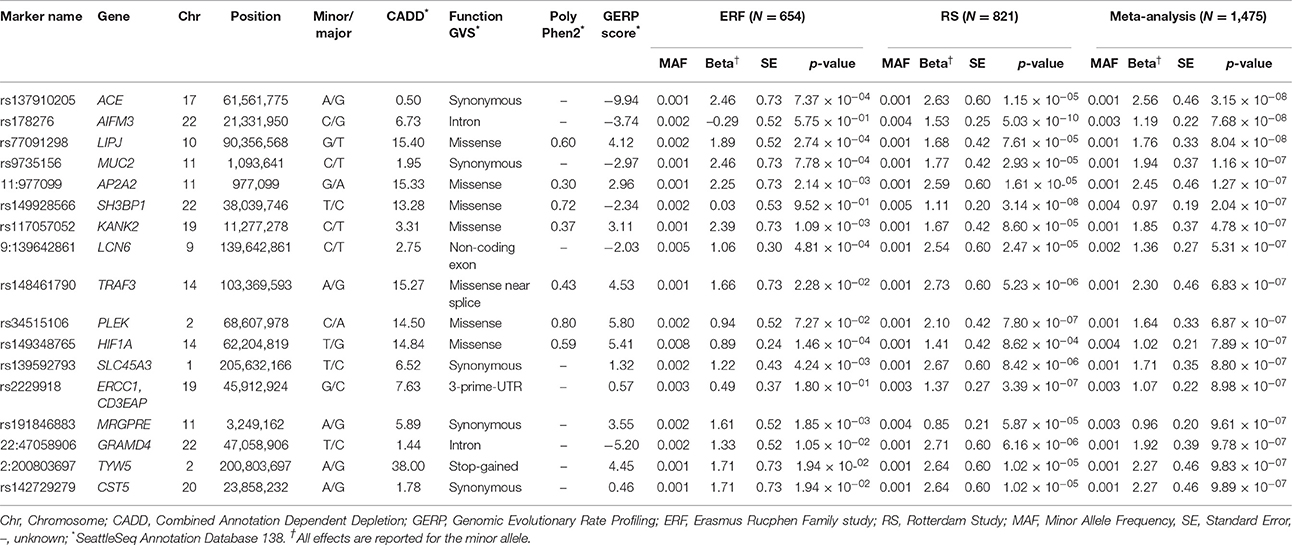
Table 3. Meta-analysis association results, filtered on p < 1.0 × 10−6.
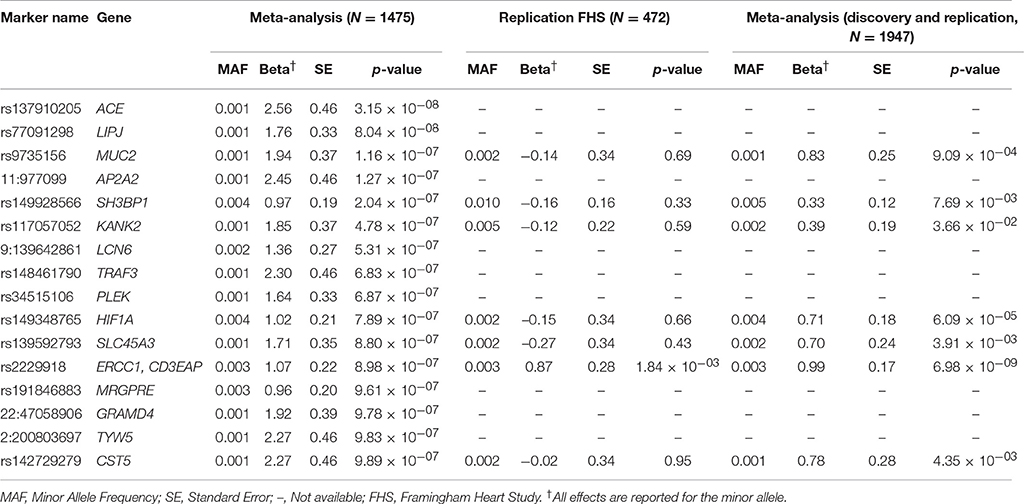
Table 4. Replication results, filtered on p < 1.0 × 10−6.
A significant association of symptoms of sleep apnea with rs2229918, located on chromosome 19q13 in the overlapping 3′-untranslated region (UTR) of the ERRC1 and CD3EAP genes (Figure 3), was observed in the replication sample (p = 1.84 × 10−3). Moreover, both the frequency (MAFFHS = 0.3%) and the effect size of the minor allele (G; βFHS = 0.87) were consistent with that of the discovery cohorts (MAF = 0.3%, β = 1.07) suggesting that each copy of the minor allele (G) can result in a shift to a higher category in self-reported apnea symptoms (PSQI). Meta-analysing the discovery and replication cohorts yielded an increased significance of the association of rs2229918 with symptoms of sleep apnea (p = 6.98 × 10−9, β = 0.99).
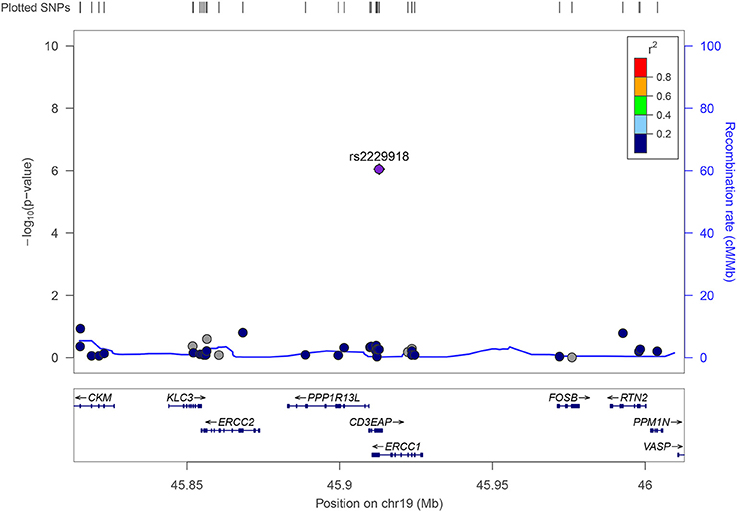
Figure 3. Regional association plot for rs2229918. Rs2229918 is located in purple. The dots show the variants tested in this region on chromosome 19. The −log10 transformed p-values are plotted on the y-axis and the genes and positions of the variants (Mb) in this region are depicted on the x-axis.
Discussion
This study aimed at identifying genetic variants associated with symptoms of sleep apnea by performing a meta-analysis of WES data. We identified a rare genetic variant (MAF = 0.3%), rs2229918, located in the shared 3′-UTR region of the ERCC1 and CD3EAP genes with a large effect on symptoms of sleep apnea. We show significant replication of rs2229918 in an independent sample.
The CD3EAP gene is located in antisense orientation to ERCC1 where the 3′-UTRs of both genes overlap. This type of 3′-UTR overlap is conserved in mice and yeast suggesting an important biological function (OMIM #107325). 3′-UTRs can be highly enriched for regulatory elements such as binding sites for regulatory proteins and microRNAs and therefore are most likely involved in post-transcriptional regulation (Xie et al., 2005). ERCC1 encodes Excision Repair Cross-Complementation Group 1, a protein functioning in the nucleotide excision repair pathway and needed for the repair of DNA lesions but also involved in recombinational DNA repair and the repair of inter-strand crosslinks (Stelzer et al., 2016). Mutations in ERCC1 have been linked to cerebro-oculo-facio-skeletal syndrome 4, a severe autosomal recessive disorder characterized by growth retardation, dysmorphic facial features, arthrogryposis, and neurologic abnormalities (OMIM #610758). CD3EAP is a component of RNA polymerase I which synthesizes ribosomal RNA precursors and is involved in poly(A) RNA binding and DNA-directed RNA polymerase activity (Stelzer et al., 2016). CD3EAP is localized in the nucleus and mitochondria and has two isoforms, isoform 1 is involved in UBTF-activated (Upstream Binding Transcription Factor, RNA Polymerase 1) transcription, while isoform 2 is a component of preformed T-cell receptor complex. CD3EAP is involved in multiple pathways including rRNA expression and RNA Polymerase 1 transcription related pathways; RNA polymerase I promotor escape and transcription; gene expression; and the TNF-alpha/NF-kB signaling pathway (Stelzer et al., 2016). Previous genetic studies have associated NF-kB-dependent genes, especially TNF-α, with OSA (Riha et al., 2005; Ryan et al., 2006; Popko et al., 2008; Bhushan et al., 2009). Moreover, NF-kB is thought to play a key role in mediation of the inflammatory and cardiovascular consequences of OSA (Ryan et al., 2005; Garvey et al., 2009). GeneNetwork (Fehrmann et al., 2015) (http://129.125.135.180:8080/GeneNetwork/) shows that both ERCC1 and CD3EAP are expressed in tissues that may be related to obstruction of the upper airway or diseases of tissues/organs associated with OSA, such as muscle cells, cartilage, trachea, salivary glands, heart and heart ventricles, glucagon secreting cells, the neck and the tongue. This further supports that ERCC1 and CD3EAP are interesting candidate genes for symptoms of sleep apnea.
Rs2229918 is located on chromosome 19q13, a previously identified region with suggestive evidence for linkage to OSA in European-Americans, independently of BMI (Palmer et al., 2003). Although APOE, a known candidate gene for OSA, is also located in this region, it did not show association with OSA in the present study. A previous study fine-mapped the APOE region and concluded that APOE does not explain the linkage signal, suggesting that APOE is not the causative locus (Larkin et al., 2006). Although the linkage analysis performed by Palmer et al. (2003) was redone by adding additional family members and families, the chromosome 19 region was not confirmed. However, this could be due to the genetic or disease heterogeneity (Larkin et al., 2008).
Additionally, there were six rare variants (MAF < 0.4%) that surpassed the Bonferroni corrected p-value threshold, of which three (located in ACE, LIPJ and AP2A2) were monomorphic in the FHS and could not be tested for replication. Our top finding, rs137910205, a synonymous variant, is located in the ACE (angiotensin converting enzyme) gene, one of the most studied genes for OSA. Previous studies found an association between the ACE insertion/deletion polymorphism and an increased risk of hypertension in OSA patients (Lin et al., 2004; Bostrom et al., 2007), although results are conflicting (Patel et al., 2007). Further, plasma activity of ACE has been found to be increased in untreated OSA patients (Barcelo et al., 2001). Both carriers of rs137910205 (1 in each cohort) reported the highest score for symptoms of sleep apnea, i.e. these individuals have experienced pauses in breathing at least twice per week. The second variant is the missense variant, rs77091298, located in the LIPJ (Lipase Family Member J) gene. GeneNetwork showed that LIPJ is expressed in the nasopharynx, neck, and muscle cells, all highly relevant tissues in the pathogenesis of OSA (Fehrmann et al., 2015). The third variant that could not be tested for replication, 11:977099, has not been identified before. The variant is located in the AP2A2 gene (Adaptor Related Protein Complex 2 Alpha 2 Subunit), which is related to lipid binding (Stelzer et al., 2016). However, we caution against the interpretation of statistics when the number of carriers of the genetic variants is less than five. Larger sample sizes are needed to further investigate the possible association of these rare genetic variants with OSA.
This study has some limitations regarding the study design. We have used questionnaire data for the assessment of symptoms of sleep apnea, which could introduce bias (Fedson et al., 2012). Although reports of breathing pauses more than twice per week are highly predictive of polysomnographic sleep apnea, self- or partner-reported breathing pauses have low sensitivity (Young et al., 2002b). Individuals with sleep apnea who experience predominantly hypopneas (shallow breathing) rather than apneas may be less likely to be identified with questionnaire data, as these individuals and their partners may be less likely to recognize these events. Another limitation of using questionnaire data is that the discrimination between OSA, central sleep apnea and mixed sleep apnea is not possible. Although the prevalence of central sleep apnea is generally much lower than OSA in particular in general population samples (Donovan and Kapur, 2016). Another limitation is that our findings might not be generalizable to other populations as all studies used in this analysis are predominantly European or European American populations. Previous studies have shown a difference in prevalence of sleep apnea between populations, where young African Americans may be at increased risk for sleep apnea (Redline et al., 1997) and had a higher apnea-hypopnea index relative to European Americans with OSA/hypopnea syndrome (Pranathiageswaran et al., 2013). The frequency of the rs2229918 minor allele (G), based on the 1000 Genomes data, also differs across populations (https://www.ncbi.nlm.nih.gov/variation/tools/1000genomes/). Lastly, sleep apnea is a complex and heterogeneous disease influenced by many risk factors such as obesity, age, gender (Redline et al., 1994; Bixler et al., 2001; Young et al., 2002b,a, 2004; Peppard et al., 2013), craniofacial and upper airway abnormalities (Mayer et al., 1996; White, 2005), race (Redline et al., 1997; Li et al., 2000), alcohol intake (Young et al., 2002a), smoking (Wetter et al., 1994), and reduced nasal patency due to congestion and respiratory allergies (Young et al., 1997). Despite this phenotypic complexity, we have identified and replicated a rare variant associated with symptoms of sleep apnea. However, we have only used one replication sample and additional studies should further investigate the association of rs2229918 with sleep apnea using objective measurements.
To conclude, this first meta-analysis of symptoms of sleep apnea using WES data identified a rare genetic variant, rs2229918 (MAF 0.3%), located in the 3′-UTR of ERCC1 and CD3EAP, associated with symptoms of sleep apnea. Both genes are interesting candidate genes for (symptoms of) sleep apnea based on their function and expression in tissues relevant for the pathogenesis of the disease. However, the involvement of rs2229918 in OSA pathology should be further examined in larger datasets with more objective measurements.
Author Contributions
AvdS, CvD, and NA contributed to the conceptualization and design of this work; AvdS and CL were involved in the analysis of the data; AvdS, AL, DK, DG, HT, CvD, and NA were involved in interpretation of the results; AvdS and NA were involved in writing and revising the manuscript; AL, DK, RB, JvR, MvdH, RK, AH, AU, WvI, HT, and CvD were involved in data collection/preparation; AL, DK, CL, RB, JvR, MvdH, RK, AH, AU, WvI, DG, HT, and CvD contributed to the interpretation of the data, read and approved the final manuscript.
Funding
The ERF study as a part of EUROSPAN (European Special Populations Research Network) was supported by European Commission FP6 STRP grant number 018947 (LSHG-CT-2006-01947) and also received funding from the European Community's Seventh Framework Programme (FP7/2007-2013)/grant agreement HEALTH-F4-2007-201413 by the European Commission under the programme “Quality of Life and Management of the Living Resources” of 5th Framework Programme (no. QLG2-CT-2002-01254). High-throughput analysis of the ERF data was supported by joint grant from Netherlands Organization for Scientific Research and the Russian Foundation for Basic Research (NWO-RFBR 047.017.043). Exome sequencing analysis in ERF was supported by the ZonMw grant (project 91111025).
The generation and management of the exome sequencing data for the RS was executed by the Human Genotyping Facility of the Genetic Laboratory of the Department of Internal Medicine, EMC, The Netherlands. The Exome Sequencing data set was funded by the Netherlands Genomics Initiative (NGI)/Netherlands Organization for Scientific Research (NWO) sponsored Netherlands Consortium for Healthy Aging (NCHA; project nr. 050-060-810), by the Genetic Laboratory of the Department of Internal Medicine, Erasmus MC, and by a Complementation Project of the Biobanking and Biomolecular Research Infrastructure Netherlands (BBMRI-NL; www.bbmri.nl; project number CP2010-41). The RS is funded by EMC and Erasmus University, Rotterdam, Netherlands Organization for the Health Research and Development (ZonMw), the Research Institute for Diseases in the Elderly (RIDE), the Ministry of Education, Culture and Science, the Ministry for Health, Welfare and Sports, the European Commission (DG XII), and the Municipality of Rotterdam.
The Framingham Heart Study is conducted and supported by the National Heart, Lung, and Blood Institute (NHLBI) in collaboration with Boston University (Contract No. N01-HC-25195 and HHSN268201500001I). SHARe Illumina genotyping was provided under an agreement between Illumina and Boston University. A portion of this research was conducted using the Linux Cluster for Genetic Analysis (LinGA-II) funded by the Robert Dawson Evans Endowment of the Department of Medicine at Boston University School of Medicine and Boston Medical Center. Funding support for the Framingham Sleep Heart Health Study was provided by NIH/NHLBI grant U01 HL 53941.
Conflict of Interest Statement
NA reports grants from Netherlands Brain Foundation, outside the submitted work. DG reports grants from NIH, during the conduct of the study; personal fees from VIVUS, Inc., outside the submitted work. RK reports grants from Netherlands Genomics Initiative (NGI), grants from Biobanking and Biomolecular Research Infrastructure Netherlands (BBMRI-NL), during the conduct of the study. AL reports grants and non-financial support from Big Health Ltd., outside the submitted work. HT reports grants from Netherlands Organization for Health Research and Development, during the conduct of the study.
The other authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
Erasmus Rucphen Family study: We are grateful to all study participants and their relatives, general practitioners and neurologists for their contributions and to P. Veraart for her help in genealogy, J. Vergeer for the supervision of the laboratory work and P. Snijders for his help in data collection.
Rotterdam Study: We thank Pascal Arp, Mila Jhamai, JvR, Marijn Verkerk, and RK, for their help in creating the RS-Exome Sequencing database. The authors are grateful to the study participants, the staff from the Rotterdam Study and the participating general practitioners and pharmacists.
Abbreviations
BMI, body mass index; BWA, Burrows Wheeler Aligner; EMC, Erasmus Medical Center; ERF, Erasmus Rucphen Family; FHS, Framingham Heart Study; GATK, Genome Analysis Toolkit; GRCh37, Genome Reference Consortium Human Build 37; GWAS, genome wide association study; Hg19, human genome build 19; HWE, Hardy-Weinberg equilibrium; MAF, minor allele frequency; OSA, obstructive sleep apnea; PSQI, Pittsburgh Sleep Quality Index; RS, Rotterdam Study; SNV, single nucleotide variant; UBTF, upstream binding transcription factor; UTR, untranslated region; WES, whole-exome sequence.
References
American Academy of Sleep Medicine (2014). International Classification of Sleep Disorders. Darien, IL: American Academy of Sleep Medicine.
Amin, N., Belonogova, N. M., Jovanova, O., Brouwer, R. W., Van Rooij, J. G., Van Den Hout, M. C., et al. (2016a). Nonsynonymous variation in NKPD1 Increases depressive symptoms in the european populations. Biol. Psychiatry 81, 702–707. doi: 10.1016/j.biopsych.2016.08.008
Amin, N., Jovanova, O., Adams, H. H., Dehghan, A., Kavousi, M., Vernooij, M. W., et al. (2016b). Exome-sequencing in a large population-based study reveals a rare Asn396Ser variant in the LIPG gene associated with depressive symptoms. Mol. Psychiatry 22, 537–543. doi: 10.1038/mp.2016.101
Aurora, R. N., and Punjabi, N. M. (2013). Obstructive sleep apnoea and type 2 diabetes mellitus: a bidirectional association. Lancet Respir. Med. 1, 329–338. doi: 10.1016/S2213-2600(13)70039-0
Baik, I., Seo, H. S., Yoon, D., Kim, S. H., and Shin, C. (2015). Associations of sleep apnea, NRG1 polymorphisms, alcohol consumption, and cerebral white matter hyperintensities: analysis with genome-wide association data. Sleep 38, 1137–1143. doi: 10.5665/sleep.4830
Bainbridge, M. N., Wang, M., Wu, Y., Newsham, I., Muzny, D. M., Jefferies, J. L., et al. (2011). Targeted enrichment beyond the consensus coding DNA sequence exome reveals exons with higher variant densities. Genome Biol. 12:R68. doi: 10.1186/gb-2011-12-7-r68
Barcelo, A., Elorza, M. A., Barbe, F., Santos, C., Mayoralas, L. R., and Agusti, A. G. (2001). Angiotensin converting enzyme in patients with sleep apnoea syndrome: plasma activity and gene polymorphisms. Eur. Respir. J. 17, 728–732. doi: 10.1183/09031936.01.17407280
Bayazit, Y. A., Yilmaz, M., Ciftci, T., Erdal, E., Kokturk, O., Gokdogan, T., et al. (2006). Association of the−1438G/A polymorphism of the 5-HT2A receptor gene with obstructive sleep apnea syndrome. ORL J. Otorhinolaryngol. Relat. Spec. 68, 123–128. doi: 10.1159/000091216
Bhushan, B., Guleria, R., Misra, A., Luthra, K., and Vikram, N. K. (2009). TNF-alpha gene polymorphism and TNF-alpha levels in obese Asian Indians with obstructive sleep apnea. Respir. Med. 103, 386–392. doi: 10.1016/j.rmed.2008.10.001
Bixler, E. O., Vgontzas, A. N., Lin, H. M., Ten Have, T., Rein, J., Vela-Bueno, A., et al. (2001). Prevalence of sleep-disordered breathing in women: effects of gender. Am. J. Respir. Crit. Care Med. 163, 608–613. doi: 10.1164/ajrccm.163.3.9911064
Bostrom, K. B., Hedner, J., Melander, O., Grote, L., Gullberg, B., Rastam, L., et al. (2007). Interaction between the angiotensin-converting enzyme gene insertion/deletion polymorphism and obstructive sleep apnoea as a mechanism for hypertension. J. Hypertens. 25, 779–783. doi: 10.1097/HJH.0b013e328017f6d5
Brouwer, R. W., Van Den Hout, M. C., Grosveld, F. G., and Van Ijcken, W. F. (2012). NARWHAL, a primary analysis pipeline for NGS data. Bioinformatics 28, 284–285. doi: 10.1093/bioinformatics/btr613
Buysse, D. J., Reynolds, C. F. III., Monk, T. H., Berman, S. R., and Kupfer, D. J. (1989). The pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 28, 193–213. doi: 10.1016/0165-1781(89)90047-4
Cade, B. E., Chen, H., Stilp, A. M., Gleason, K. J., Sofer, T., Ancoli-Israel, S., et al. (2016). Genetic associations with obstructive sleep apnea traits in Hispanic/Latino Americans. Am. J. Respir. Crit. Care Med. 194, 886–897. doi: 10.1164/rccm.201512-2431OC
Challis, D., Yu, J., Evani, U. S., Jackson, A. R., Paithankar, S., Coarfa, C., et al. (2012). An integrative variant analysis suite for whole exome next-generation sequencing data. BMC Bioinformatics 13:8. doi: 10.1186/1471-2105-13-8
Consensus Conference Panel, Watson, N. F., Badr, M. S., Belenky, G., Bliwise, D. L., Buxton, O. M., et al. (2015). Recommended amount of sleep for a healthy adult: a joint consensus statement of the american academy of sleep medicine and sleep research society. J. Clin. Sleep Med. 11, 591–592. doi: 10.5665/sleep.4716
Cosgrave, J., Haines, R., van Heugten-van der Kloet, D., Purple, R., Porcheret, K., Foster, R., et al. (in press). The interaction between subclinical psychotic experiences, insomnia objective measures of sleep. Schizophr. Res.. doi: 10.1016/j.schres.2017.06.058. [Epub ahead of print].
Danecek, P., Auton, A., Abecasis, G., Albers, C. A., Banks, E., Depristo, M. A., et al. (2011). The variant call format and VCFtools. Bioinformatics 27, 2156–2158. doi: 10.1093/bioinformatics/btr330
Dawber, T. R., Meadors, G. F., and Moore, F. E. Jr. (1951). Epidemiological approaches to heart disease: the Framingham Study. Am. J. Public Health Nations. Health 41, 279–281. doi: 10.2105/AJPH.41.3.279
Depristo, M. A., Banks, E., Poplin, R., Garimella, K. V., Maguire, J. R., Hartl, C., et al. (2011). A framework for variation discovery and genotyping using next-generation DNA sequencing data. Nat. Genet. 43, 491–498. doi: 10.1038/ng.806
Donovan, L. M., and Kapur, V. K. (2016). Prevalence and characteristics of central compared to obstructive sleep apnea: analyses from the sleep heart health study cohort. Sleep 39, 1353–1359. doi: 10.5665/sleep.5962
Fedson, A. C., Pack, A. I., and Gislason, T. (2012). Frequently used sleep questionnaires in epidemiological and genetic research for obstructive sleep apnea: a review. Sleep Med. Rev. 16, 529–537. doi: 10.1016/j.smrv.2011.12.002
Fehrmann, R. S., Karjalainen, J. M., Krajewska, M., Westra, H. J., Maloney, D., Simeonov, A., et al. (2015). Gene expression analysis identifies global gene dosage sensitivity in cancer. Nat. Genet. 47, 115–125. doi: 10.1038/ng.3173
Garvey, J. F., Taylor, C. T., and Mcnicholas, W. T. (2009). Cardiovascular disease in obstructive sleep apnoea syndrome: the role of intermittent hypoxia and inflammation. Eur. Respir. J. 33, 1195–1205. doi: 10.1183/09031936.00111208
Gottlieb, D. J., Destefano, A. L., Foley, D. J., Mignot, E., Redline, S., Givelber, R. J., et al. (2004). APOE epsilon4 is associated with obstructive sleep apnea/hypopnea: the Sleep Heart Health Study. Neurology 63, 664–668. doi: 10.1212/01.WNL.0000134671.99649.32
Gottlieb, D. J., Punjabi, N. M., Newman, A. B., Resnick, H. E., Redline, S., Baldwin, C. M., et al. (2005). Association of sleep time with diabetes mellitus and impaired glucose tolerance. Arch. Intern. Med. 165, 863–867. doi: 10.1001/archinte.165.8.863
Gottlieb, D. J., Whitney, C. W., Bonekat, W. H., Iber, C., James, G. D., Lebowitz, M., et al. (1999). Relation of sleepiness to respiratory disturbance index: the Sleep Heart Health Study. Am. J. Respir. Crit. Care Med. 159, 502–507. doi: 10.1164/ajrccm.159.2.9804051
Gottlieb, D. J., Yenokyan, G., Newman, A. B., O'connor, G. T., Punjabi, N. M., Quan, S. F., et al. (2010). Prospective study of obstructive sleep apnea and incident coronary heart disease and heart failure: the sleep heart health study. Circulation 122, 352–360. doi: 10.1161/CIRCULATIONAHA.109.901801
Grote, L., Kraiczi, H., and Hedner, J. (2000). Reduced alpha- and beta(2)-adrenergic vascular response in patients with obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 162, 1480–1487. doi: 10.1164/ajrccm.162.4.9912028
Hoevenaar-Blom, M. P., Spijkerman, A. M., Kromhout, D., Van Den Berg, J. F., and Verschuren, W. M. (2011). Sleep duration and sleep quality in relation to 12-year cardiovascular disease incidence: the MORGEN study. Sleep 34, 1487–1492. doi: 10.5665/sleep.1382
Hofman, A., Brusselle, G. G., Darwish Murad, S., Van Duijn, C. M., Franco, O. H., Goedegebure, A., et al. (2015). The Rotterdam Study: 2016 objectives and design update. Eur. J. Epidemiol. 30, 661–708. doi: 10.1007/s10654-015-0082-x
Kadotani, H., Kadotani, T., Young, T., Peppard, P. E., Finn, L., Colrain, I. M., et al. (2001). Association between apolipoprotein E epsilon4 and sleep-disordered breathing in adults. JAMA 285, 2888–2890. doi: 10.1001/jama.285.22.2888
Kannel, W. B., Feinleib, M., Mcnamara, P. M., Garrison, R. J., and Castelli, W. P. (1979). An investigation of coronary heart disease in families. The Framingham offspring study. Am. J. Epidemiol. 110, 281–290. doi: 10.1093/oxfordjournals.aje.a112813
Kendzerska, T., Gershon, A. S., Hawker, G., Tomlinson, G., and Leung, R. S. (2014). Obstructive sleep apnea and incident diabetes. A historical cohort study. Am. J. Respir. Crit. Care Med. 190, 218–225. doi: 10.1164/rccm.201312-2209OC
Kim, H. C., Young, T., Matthews, C. G., Weber, S. M., Woodward, A. R., and Palta, M. (1997). Sleep-disordered breathing and neuropsychological deficits. A population-based study. Am. J. Respir. Crit. Care Med. 156, 1813–1819. doi: 10.1164/ajrccm.156.6.9610026
Knutson, K. L., Rathouz, P. J., Yan, L. L., Liu, K., and Lauderdale, D. S. (2007). Intra-individual daily and yearly variability in actigraphically recorded sleep measures: the CARDIA study. Sleep 30, 793–796. doi: 10.1093/sleep/30.6.793
Kripke, D. F., Kline, L. E., Nievergelt, C. M., Murray, S. S., Shadan, F. F., Dawson, A., et al. (2015). Genetic variants associated with sleep disorders. Sleep Med. 16, 217–224. doi: 10.1016/j.sleep.2014.11.003
Larkin, E. K., Patel, S. R., Elston, R. C., Gray-Mcguire, C., Zhu, X., and Redline, S. (2008). Using linkage analysis to identify quantitative trait loci for sleep apnea in relationship to body mass index. Ann. Hum. Genet. 72, 762–773. doi: 10.1111/j.1469-1809.2008.00472.x
Larkin, E. K., Patel, S. R., Goodloe, R. J., Li, Y., Zhu, X., Gray-Mcguire, C., et al. (2010). A candidate gene study of obstructive sleep apnea in European Americans and African Americans. Am. J. Respir. Crit. Care Med. 182, 947–953. doi: 10.1164/rccm.201002-0192OC
Larkin, E. K., Patel, S. R., Redline, S., Mignot, E., Elston, R. C., and Hallmayer, J. (2006). Apolipoprotein, E., and obstructive sleep apnea: evaluating whether a candidate gene explains a linkage peak. Genet. Epidemiol. 30, 101–110. doi: 10.1002/gepi.20127
Li, H., and Durbin, R. (2009). Fast and accurate short read alignment with Burrows-Wheeler transform. Bioinformatics 25, 1754–1760. doi: 10.1093/bioinformatics/btp324
Li, H., Handsaker, B., Wysoker, A., Fennell, T., Ruan, J., Homer, N., et al. (2009). The sequence alignment/map format and SAMtools. Bioinformatics 25, 2078–2079. doi: 10.1093/bioinformatics/btp352
Li, K. K., Kushida, C., Powell, N. B., Riley, R. W., and Guilleminault, C. (2000). Obstructive sleep apnea syndrome: a comparison between Far-East Asian and white men. Laryngoscope 110, 1689–1693. doi: 10.1097/00005537-200010000-00022
Lin, L., Finn, L., Zhang, J., Young, T., and Mignot, E. (2004). Angiotensin-converting enzyme, sleep-disordered breathing, and hypertension. Am. J. Respir. Crit. Care Med. 170, 1349–1353. doi: 10.1164/rccm.200405-616OC
Lovato, N., and Gradisar, M. (2014). A meta-analysis and model of the relationship between sleep and depression in adolescents: recommendations for future research and clinical practice. Sleep Med. Rev. 18, 521–529. doi: 10.1016/j.smrv.2014.03.006
Marin, J. M., Carrizo, S. J., Vicente, E., and Agusti, A. G. (2005). Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 365, 1046–1053. doi: 10.1016/S0140-6736(05)74229-X
Marshall, N. S., Wong, K. K. H., Liu, P. Y., Cullen, S. R. J., Knuiman, M. W., and Grunstein, R. R. (2008). Sleep apnea as an independent risk factor for all-cause mortality: the Busselton health study. Sleep 31, 1079–1085. doi: 10.5665/sleep/31.8.1079
Mayer, P., Pepin, J. L., Bettega, G., Veale, D., Ferretti, G., Deschaux, C., et al. (1996). Relationship between body mass index, age and upper airway measurements in snorers and sleep apnoea patients. Eur. Respir. J. 9, 1801–1809. doi: 10.1183/09031936.96.09091801
Mckenna, A., Hanna, M., Banks, E., Sivachenko, A., Cibulskis, K., Kernytsky, A., et al. (2010). The Genome Analysis Toolkit: a MapReduce framework for analyzing next-generation DNA sequencing data. Genome Res. 20, 1297–1303. doi: 10.1101/gr.107524.110
McNicholas, W. T. (2008). Diagnosis of obstructive sleep apnea in adults. Proc. Am. Thorac. Soc. 5, 154–160. doi: 10.1513/pats.200708-118MG
Mehra, R., Stone, K. L., Blackwell, T., Ancoli Israel, S., Dam, T. T., Stefanick, M. L., et al. (2007). Prevalence and correlates of sleep-disordered breathing in older men: osteoporotic fractures in men sleep study. J. Am. Geriatr. Soc. 55, 1356–1364. doi: 10.1111/j.1532-5415.2007.01290.x
Mezick, E. J., Matthews, K. A., Hall, M., Kamarck, T. W., Buysse, D. J., Owens, J. F., et al. (2009). Intra-individual variability in sleep duration and fragmentation: associations with stress. Psychoneuroendocrinology 34, 1346–1354. doi: 10.1016/j.psyneuen.2009.04.005
Miller, S. A., Dykes, D. D., and Polesky, H. F. (1988). A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res. 16, 1215–1215. doi: 10.1093/nar/16.3.1215
Mills, P. J., Dimsdale, J. E., Coy, T. V., Ancoli-Israel, S., Clausen, J. L., and Nelesen, R. A. (1995). Beta 2-adrenergic receptor characteristics in sleep apnea patients. Sleep 18, 39–42. doi: 10.1093/sleep/18.1.39
Palmer, L. J., Buxbaum, S. G., Larkin, E., Patel, S. R., Elston, R. C., Tishler, P. V., et al. (2003). A whole-genome scan for obstructive sleep apnea and obesity. Am. J. Hum. Genet. 72, 340–350. doi: 10.1086/346064
Pardo, L. M., Mackay, I., Oostra, B., Van Duijn, C. M., and Aulchenko, Y. S. (2005). The effect of genetic drift in a young genetically isolated population. Ann. Hum. Genet. 69, 288–295. doi: 10.1046/J.1469-1809.2005.00162.x
Patel, S. R., Goodloe, R., De, G., Kowgier, M., Weng, J., Buxbaum, S. G., et al. (2012). Association of genetic loci with sleep apnea in European Americans and African-Americans: the Candidate Gene Association Resource (CARe). PLoS ONE 7:e48836. doi: 10.1371/journal.pone.0048836
Patel, S. R., Larkin, E. K., Mignot, E., Lin, L., and Redline, S. (2007). The association of angiotensin converting enzyme (ACE) polymorphisms with sleep apnea and hypertension. Sleep 30, 531–533. doi: 10.1093/sleep/30.4.531
Patel, S. R., Larkin, E. K., and Redline, S. (2008). Shared genetic basis for obstructive sleep apnea and adiposity measures. Int. J. Obes. 32, 795–800. doi: 10.1038/sj.ijo.0803803
Patel, S. R., Zhu, X., Storfer-Isser, A., Mehra, R., Jenny, N. S., Tracy, R., et al. (2009). Sleep duration and biomarkers of inflammation. Sleep 32, 200–204. doi: 10.1093/sleep/32.2.200
Pedrosa, R. P., Drager, L. F., Gonzaga, C. C., Sousa, M. G., De Paula, L. K., Amaro, A. C., et al. (2011). Obstructive sleep apnea: the most common secondary cause of hypertension associated with resistant hypertension. Hypertension 58, 811–817. doi: 10.1161/HYPERTENSIONAHA.111.179788
Peppard, P. E., Szklo-Coxe, M., Hla, K. M., and Young, T. (2006). Longitudinal association of sleep-related breathing disorder and depression. Arch. Intern. Med. 166, 1709–1715. doi: 10.1001/archinte.166.16.1709
Peppard, P. E., Young, T., Barnet, J. H., Palta, M., Hagen, E. W., and Hla, K. M. (2013). Increased prevalence of sleep-disordered breathing in adults. Am. J. Epidemiol. 177, 1006–1014. doi: 10.1093/aje/kws342
Peppard, P. E., Young, T., Palta, M., and Skatrud, J. (2000). Prospective study of the association between sleep-disordered breathing and hypertension. N. Engl. J. Med. 342, 1378–1384. doi: 10.1056/NEJM200005113421901
Peters van Neijenhof, R. J. G., van Duijn, E., Comijs, H. C., van den Berg, J. F., de Waal, M. W. M., Oude Voshaar, R. C., et al. (2016). Correlates of sleep disturbances in depressed older persons: the Netherlands study of depression in older persons (NESDO). Aging Ment. Health doi: 10.1080/13607863.2016.1247421. [Epub ahead of print].
Pilcher, J. J., and Huffcutt, A. I. (1996). Effects of sleep deprivation on performance: a meta-analysis. Sleep 19, 318–326. doi: 10.1093/sleep/19.4.318
Popko, K., Gorska, E., Potapinska, O., Wasik, M., Stoklosa, A., Plywaczewski, R., et al. (2008). Frequency of distribution of inflammatory cytokines IL-1, IL-6 and TNF-alpha gene polymorphism in patients with obstructive sleep apnea. J. Physiol. Pharmacol. 59(Suppl. 6), 607–614.
Pranathiageswaran, S., Badr, M. S., Severson, R., and Rowley, J. A. (2013). The influence of race on the severity of sleep disordered breathing. J. Clin. Sleep Med. 9, 303–309. doi: 10.5664/jcsm.2572
Punjabi, N. M., Caffo, B. S., Goodwin, J. L., Gottlieb, D. J., Newman, A. B., O'connor, G. T., et al. (2009). Sleep-disordered breathing and mortality: a prospective cohort study. PLoS Med. 6:e1000132. doi: 10.1371/journal.pmed.1000132
Purcell, S., Neale, B., Todd-Brown, K., Thomas, L., Ferreira, M. A., Bender, D., et al. (2007). PLINK: a tool set for whole-genome association and population-based linkage analyses. Am. J. Hum. Genet. 81, 559–575. doi: 10.1086/519795
Qin, B., Sun, Z., Liang, Y., Yang, Z., and Zhong, R. (2014). The association of 5-HT2A, 5-HTT, and LEPR polymorphisms with obstructive sleep apnea syndrome: a systematic review and meta-analysis. PLoS ONE 9:e95856. doi: 10.1371/journal.pone.0095856
Quan, S. F., Howard, B. V., Iber, C., Kiley, J. P., Nieto, F. J., O'connor, G. T., et al. (1997). The sleep heart health study: design, rationale, and methods. Sleep 20, 1077–1085.
Rechtschaffen, A. (1998). Current perspectives on the function of sleep. Perspect. Biol. Med. 41, 359–390. doi: 10.1353/pbm.1998.0051
Redline, S., Kump, K., Tishler, P. V., Browner, I., and Ferrette, V. (1994). Gender differences in sleep disordered breathing in a community-based sample. Am. J. Respir. Crit. Care Med. 149, 722–726. doi: 10.1164/ajrccm.149.3.8118642
Redline, S., and Tishler, P. V. (2000). The genetics of sleep apnea. Sleep Med. Rev. 4, 583–602. doi: 10.1053/smrv.2000.0120
Redline, S., Tishler, P. V., Hans, M. G., Tosteson, T. D., Strohl, K. P., and Spry, K. (1997). Racial differences in sleep-disordered breathing in African-Americans and Caucasians. Am. J. Respir. Crit. Care Med. 155, 186–192. doi: 10.1164/ajrccm.155.1.9001310
Redline, S., Tishler, P. V., Tosteson, T. D., Williamson, J., Kump, K., Browner, I., et al. (1995). The familial aggregation of obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 151, 682–687. doi: 10.1164/ajrccm/151.3_Pt_1.682
Riha, R. L., Brander, P., Vennelle, M., Mcardle, N., Kerr, S. M., Anderson, N. H., et al. (2005). Tumour necrosis factor-alpha (-308) gene polymorphism in obstructive sleep apnoea-hypopnoea syndrome. Eur. Respir. J. 26, 673–678. doi: 10.1183/09031936.05.00130804
Ryan, S., Taylor, C. T., and Mcnicholas, W. T. (2005). Selective activation of inflammatory pathways by intermittent hypoxia in obstructive sleep apnea syndrome. Circulation 112, 2660–2667. doi: 10.1161/CIRCULATIONAHA.105.556746
Ryan, S., Taylor, C. T., and Mcnicholas, W. T. (2006). Predictors of elevated nuclear factor-kappaB-dependent genes in obstructive sleep apnea syndrome. Am. J. Respir. Crit. Care Med. 174, 824–830. doi: 10.1164/rccm.200601-066OC
Sakai, K., Takada, T., Nakayama, H., Kubota, Y., Nakamata, M., Satoh, M., et al. (2005). Serotonin-2A and 2C receptor gene polymorphisms in Japanese patients with obstructive sleep apnea. Intern. Med. 44, 928–933. doi: 10.2169/internalmedicine.44.928
Senaratna, C. V., Perret, J. L., Lodge, C. J., Lowe, A. J., Campbell, B. E., Matheson, M. C., et al. (2016). Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 34, 70–81. doi: 10.1016/j.smrv.2016.07.002
Shamsuzzaman, A. S., Gersh, B. J., and Somers, V. K. (2003). Obstructive sleep apnea: implications for cardiac and vascular disease. JAMA 290, 1906–1914. doi: 10.1001/jama.290.14.1906
Shaw, J. E., Punjabi, N. M., Wilding, J. P., Alberti, K. G., and Zimmet, P. Z. (2008). Sleep-disordered breathing and type 2 diabetes: a report from the International Diabetes Federation Taskforce on Epidemiology and Prevention. Diabetes Res. Clin. Pract. 81, 2–12. doi: 10.1016/j.diabres.2008.04.025
Sleiman, P., and Hakonarson, H. (2011). Genetic underpinnings of obstructive sleep apnea: are we making progress? Sleep 34, 1449–1452. doi: 10.5665/sleep.1366
Stelzer, G., Rosen, N., Plaschkes, I., Zimmerman, S., Twik, M., Fishilevich, S., et al. (2016). The genecards suite: from gene data mining to disease genome sequence analyses. Curr. Protoc. Bioinformatics 54, 1 30 31-31 30 33. doi: 10.1002/cpbi.5
Van Dongen, H. P., Vitellaro, K. M., and Dinges, D. F. (2005). Individual differences in adult human sleep and wakefulness: leitmotif for a research agenda. Sleep 28, 479–496. doi: 10.1093/sleep/28.4.479
Wang, K., Li, M., and Hakonarson, H. (2010). ANNOVAR: functional annotation of genetic variants from high-throughput sequencing data. Nucleic Acids Res. 38:e164. doi: 10.1093/nar/gkq603
Wetter, D. W., Young, T. B., Bidwell, T. R., Badr, M. S., and Palta, M. (1994). Smoking as a risk factor for sleep-disordered breathing. Arch. Intern. Med. 154, 2219–2224. doi: 10.1001/archinte.1994.00420190121014
White, D. P. (2005). Pathogenesis of obstructive and central sleep apnea. Am. J. Respir. Crit. Care Med. 172, 1363–1370. doi: 10.1164/rccm.200412-1631SO
Xie, X., Lu, J., Kulbokas, E. J., Golub, T. R., Mootha, V., Lindblad-Toh, K., et al. (2005). Systematic discovery of regulatory motifs in human promoters and 3′ UTRs by comparison of several mammals. Nature 434, 338–345. doi: 10.1038/nature03441
Yaffe, K., Falvey, C. M., and Hoang, T. (2014). Connections between sleep and cognition in older adults. Lancet Neurol. 13, 1017–1028. doi: 10.1016/S1474-4422(14)70172-3
Yaffe, K., Laffan, A. M., Harrison, S. L., Redline, S., Spira, A. P., Ensrud, K. E., et al. (2011). Sleep-disordered breathing, hypoxia, and risk of mild cognitive impairment and dementia in older women. JAMA 306, 613–619. doi: 10.1001/jama.2011.1115
Yaggi, H. K., Araujo, A. B., and Mckinlay, J. B. (2006). Sleep duration as a risk factor for the development of type 2 diabetes. Diabetes Care 29, 657–661. doi: 10.2337/diacare.29.03.06.dc05-0879
Yaggi, H. K., Concato, J., Kernan, W. N., Lichtman, J. H., Brass, L. M., and Mohsenin, V. (2005). Obstructive sleep apnea as a risk factor for stroke and death. N. Engl. J. Med. 353, 2034–2041. doi: 10.1056/NEJMoa043104
Ylmaz, M., Bayazit, Y. A., Ciftci, T. U., Erdal, M. E., Urhan, M., Kokturk, O., et al. (2005). Association of serotonin transporter gene polymorphism with obstructive sleep apnea syndrome. Laryngoscope 115, 832–836. doi: 10.1097/01.MLG.0000157334.88700.E6
Young, T., Finn, L., and Kim, H. (1997). Nasal obstruction as a risk factor for sleep-disordered breathing. The University of Wisconsin Sleep and Respiratory Research Group. J. Allergy Clin. Immunol. 99, S757–S762. doi: 10.1016/S0091-6749(97)70124-6
Young, T., Finn, L., Peppard, P. E., Szklo-Coxe, M., Austin, D., Nieto, F. J., et al. (2008). Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep 31, 1071–1078. doi: 10.5665/sleep/31.8.1071
Young, T., Peppard, P. E., and Gottlieb, D. J. (2002a). Epidemiology of obstructive sleep apnea: a population health perspective. Am. J. Respir. Crit. Care Med. 165, 1217–1239. doi: 10.1164/rccm.2109080
Young, T., Shahar, E., Nieto, F. J., Redline, S., Newman, A. B., Gottlieb, D. J., et al. (2002b). Predictors of sleep-disordered breathing in community-dwelling adults: the sleep heart health study. Arch. Intern. Med. 162, 893–900. doi: 10.1001/archinte.162.8.893
Keywords: sleep apnea syndromes, sleep, genetics, exome, sequence analysis, ERCC1, CD3EAP
Citation: van der Spek A, Luik AI, Kocevska D, Liu C, Brouwer RWW, van Rooij JGJ, van den Hout MCGN, Kraaij R, Hofman A, Uitterlinden AG, van IJcken WFJ, Gottlieb DJ, Tiemeier H, van Duijn CM and Amin N (2017) Exome-Wide Meta-Analysis Identifies Rare 3′-UTR Variant in ERCC1/CD3EAP Associated with Symptoms of Sleep Apnea. Front. Genet. 8:151. doi: 10.3389/fgene.2017.00151
Received: 26 July 2017; Accepted: 28 September 2017;
Published: 18 October 2017.
Edited by:
Jill Barnholtz-Sloan, Case Western Reserve University, United StatesReviewed by:
Jimmy Thomas Efird, East Carolina University, United StatesDiddahally Govindaraju, Albert Einstein College of Medicine, United States
Copyright © 2017 van der Spek, Luik, Kocevska, Liu, Brouwer, van Rooij, van den Hout, Kraaij, Hofman, Uitterlinden, van IJcken, Gottlieb, Tiemeier, van Duijn and Amin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Najaf Amin, bi5hbWluQGVyYXNtdXNtYy5ubA==