 Yuzhe Hua
Yuzhe Hua Yaxin Dai
Yaxin Dai Jingping Yi1
Jingping Yi1 Peng Li
Peng Li- 1Zhoushan Municipal Center for Disease Control and Prevention, Zhejiang, China
- 2Outpatient Department of The Second People's Hospital of Zhoushan, Zhejiang, China
Crew members aboard international voyage ships are susceptible to imported acute respiratory infections, leading to clusters of outbreaks that pose challenges to the health of crew members. The aim of the proposed study was to optimize a plan for the quarantine process and rescue measures in response to a coronavirus disease 2019 (COVID-19) outbreak at sea to provide policy guidance for the prevention and control of severe infectious diseases on international voyage ships. Here, we described the baseline characteristics of international voyage ships and crew members entering Zhoushan Port from 2020 to 2022 and analyzed the factors influencing the incidence rate of COVID-19 among crew members. There were 161 COVID-19 cases among cargo ships entering Zhoushan Port by sea, with an average incidence rate of 16.00% (95% CI: 13.73%–18.27%). The incidence rate of COVID-19 was significantly higher among crew members with replacement, long voyage, and those who stayed at multiple anchorages or stayed for a long time. The risk of COVID-19 infection for crew members staying at more than 4 anchorage was the highest, which was 2.667 (95% CI: 1.857–3.830) times that of crew members staying at less than 4 anchorage. We developed and refined the workflow for a public health assistance plan for outbreaks at sea on the basis of our experience with several COVID-19 outbreaks on international voyage ships. The workflow includes fundamental requirements, sampling and testing methods, personnel transfer procedures, medical waste disposal guidelines, and disinfection procedures for affected ships. Our public health assistance plan can be applied to other international voyage ships for which urgent public health assistance is needed during sudden infectious disease outbreaks.
1 Introduction
Since infection by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first recorded in humans in December 2019, this virus has caused many infections and deaths (Zhang et al., 2023). At present, coronavirus disease 2019 (COVID-19) is still a global pandemic that has had a significant impact on healthcare systems, economic development, and social stability worldwide (Yuan et al., 2023).
International voyage ships account for more than 80% of international trade and play an important role in economic and cultural exchanges (Cardoso et al., 2022). However, crew members aboard international voyage ships frequently interact with diverse populations, and these ships have relatively enclosed environments, with limited onboard medical facilities (Kak, 2015). This has created great challenges for international voyage ships, including SARS-CoV-2 infection at sea, crew replacement, and healthcare assistance. Recently, several COVID-19 outbreaks at sea have been reported worldwide (Maeda et al., 2021; Plucinski et al., 2021; Walker et al., 2021). Relevant public health assistance must be implemented to address these outbreaks at sea.
To address these health threats and minimize the interference of COVID-19 on maritime traffic, on the basis of our experience in the investigation and treatment of these COVID-19 outbreaks on international voyage ships, we developed and refined a plan for such outbreaks. Here, we describe the epidemiological characteristics of this COVID-19 outbreak and the rescue measures implemented for crew members at sea. Through this plan, we provide policy recommendations for the control and prevention of sudden severe infectious diseases on international voyage ships.
2 Materials and methods
2.1 Baseline information
During the period from 2020-2022, the Zhoushan Municipal Center for Disease Control and Prevention (Zhoushan CDC) received an online report of 161 COVID-19 cases, which were distributed on 45 cargo ships entering Zhoushan Port by sea.
Zhoushan has a coastline of over 2440 kilometers, making it the city with the longest island coastline in China. Zhoushan Port is an important node in the comprehensive transportation network of the Yangtze River Delta.
2.2 Data collection
Information on COVID-19 cases imported from the sea at Zhoushan Port, as well as data from international voyage ships docking at Zhoushan Port for humanitarian assistance, was collected from the “Infectious Disease Reporting Information Management System” (IDRIMS) and the “Public Health Emergency Information Management System” (PHEIMS). We used the VLOOKUP function to match these data with “ship name” as the keyword to obtain the epidemiological information of the crew members and the navigation information of the ships.
2.3 Study population
The inclusion criteria of the study population were as follows: ① crew members of international voyage ships entering Zhoushan port from 2020 to 2022; ② a clear history of SARS-CoV-2 exposure; and ③ cases were diagnosed as SARS-CoV-2 infection by laboratory tests. The exclusion criteria for the study population were as follows: ① crew members who did not enter Zhoushan port from 2020 to 2022; ② a ship type that was not a cargo ship; ③ no history or insufficient evidence of SARS-CoV-2 exposure; and ④ cases with negative results after repeated laboratory tests or suspected cases and clinically diagnosed cases without laboratory testing (Kordsmeyer et al., 2021).
2.4 Definitions
A laboratory-diagnosed case was defined as a positive test result for SARS-CoV-2 infection confirmed by real-time fluorescence quantitative polymerase chain reaction (real-time PCR) at the Zhoushan CDC with or without signs and symptoms of COVID-19 in a crew member of international voyage ships (Guagliardo et al., 2023). The clinical signs and symptoms of COVID-19 recognized worldwide include fever, fatigue, cough, shortness of breath, sore throat, headache, and smell and taste disorders (Alharthy et al., 2021; Dao et al., 2021; Hu et al., 2021).
The incidence rate was defined as the incidence of SARS-CoV-2 infection among crew members of international voyage ships. The calculation method for the incidence rate was as follows: the total number of cases ÷ the total number of crew members × 100%.
Crew replacement was defined as when a crew member disembarked from the ship after completing handover procedures and another crew member embarked after completing identity verification and registration. The crew certificates and handover records of the new crew member must meet the requirements. Health certificates were also required during the COVID-19 epidemic.
Voyage time was defined as the actual time a ship moved at sea, excluding non-voyage time such as port loading, refueling, and maintenance.
Extreme value was defined as data that were outside the range of mean ± 2 standard deviations.
2.5 Measures
We took the following measures on the basis of our experience with the COVID-19 outbreaks on international voyage ships.
1. Establishment of a rescue system. Professional working groups on public health assistance were quickly set up, and the heads of the professional groups were responsible for arranging the composition and responsibilities of the staff. The local government has organized relevant departments to provide good guidance and supervision, such as customs, the CDC at all levels, and pest control operations (PCOs).
2. Monitoring of key personnel. The key personnel included sick crew members, staff who boarded the ship for rescue, and medical staff from designated hospitals. Given the need to maintain the ship’s power, sick crew members disembark in batches for medical assistance according to the severity of their illness. Crew members who tested negative for SARS-CoV-2 infection were isolated in the cabin or transferred to the centralized isolation point for 14 days of medical observation. The staff who participated in boarding and rescue implemented “7 + 7” management, that is, 7 days of centralized isolation observation and 7 days of home health monitoring. Medical staffs in designated hospitals live in designated places, and they are picked up in a point-to-point manner by special buses for commuting.
3. Environmental disinfection and sterilization. Three rounds of terminal disinfection of the ship involved in the epidemic were carried out. With the customs department as the main body, personnel of the provincial and municipal CDC provided guidance. Personnel of the PCO boarded the ship to carry out terminal disinfection work in the epidemic area of concern, involving the crew members’ living area, work area, engine room, and other places. All daily necessities on board were disposed of in accordance with medical waste and handled by environmental protection companies. After the ship was disinfected, environmental sampling was carried out. Environmental sampling of the tugboats involved in the rescue was also carried out.
2.6 Laboratory testing
In accordance with the Plan for the Prevention and Control of Pneumonia Caused by SARS-CoV-2 (Version 2) issued by the National Health Commission in 2020, oropharyngeal and nasopharyngeal swab samples from crew members were collected to detect SARS-CoV-2. Real-time PCR was used to determine whether SARS-CoV-2 infection was present. The work was conducted in a biosafety level 2 laboratory (BSL-2).
2.7 Statistical analysis
The mean was used to describe the age of the crew members. The rate was used to describe the incidence rate of COVID-19. The 95% confidence interval (95% CI) of incidence rate was estimated by normal approximation (Daly, 1998). The proportion was used to describe the proportion of a certain part of a population, expressed as the percentage (%) in the results. The median was used to define the threshold for level variables. The Wald chi-square test was used to evaluate whether there was a significant difference in crew replacement as well as whether there was a significant difference between different voyage times, different stay times at anchorages, and different anchorage numbers. The significance threshold was 0.05. All the statistical analyses were conducted using R software (R version 4.0.3). All the figures were drawn using WPS Office (version 12.1.0).
The work received ethical approval from the Ethics Committee of the Zhoushan CDC (approval number: Zs21-02). According to the “Ethical Review Measures for Biomedical Research Involving Human Beings” issued by the former National Health and Family Planning Commission in 2016, the ethics committee approved the exemption of subjects from signing informed consent forms.
3 Results
3.1 Basic information
3.1.1 Ships information
Among the international voyage ships entering Zhoushan Port by sea, 45 crew members were infected with SARS-CoV-2. The main sources of ship registration were 17 countries and regions. Among them, Panama had the largest number of ships, accounting for 24%, followed by Marshall Islands nationality (16%), Russian nationality (13%), Liberian nationality (11%), and Singaporean nationality (7%). Please refer to Appendix Table 1 for specific details. These ships passed through 54 countries and regions before arriving at Zhoushan Port, mainly Singapore, Japan, the Philippines, Russia, South Korea, Indonesia, India, and Australia. Among them, the port in Singapore was one of the busiest Asian ports, with 15 ships remaining at the anchorage for a total of 43 days. Next, the port in Japan had 9 ships staying at the anchorage for a total of 60 days. The longest stay in the anchorage of a Russian port was 121 days, with a total of 7 ships. Please refer to Appendix Table 2 for specific details.
3.1.2 Crew members’ information
There were 161 COVID-19 cases among international voyage ships entering Zhoushan Port by sea, with an average incidence rate of 16.00% (95% CI: 13.73%–18.27%). Among them, the incidence rate of ships in Hong Kong was the highest (60.0%), followed by the incidence rate of ships in Bangladesh, which was 37.5%. The incidence rates of Liberian ships, Panamanian ships and Bahamas ships were 29.5%, 28.1% and 21.1%, respectively. See Appendix Table 3 for specific details. According to Table 1, the sex of the sick crew members was mainly male (99.4%), which was related to the occupation of the crew members. The age of the sick crew members ranged from 18–67 years, with an average age of 37.5 years. The 31–40 year age group had the highest number of sick crew members, accounting for 40.0% of all crew members. In terms of race, 65.8% were Asian, and 34.2% were white. Among the sick crew members, 64.60% had been replaced. The incidence rate of COVID-19 was significantly higher among crew members with replacement, those who sailed for more than 38 days, those who stayed at anchorage for more than 15 days, and those who stayed at more than 4 anchorages. The risk of COVID-19 infection for crew members staying at more than 4 anchorage was the highest, which was 2.667 (95% CI: 1.857–3.830) times that of crew members staying at less than 4 anchorage.

Table 1. Demographic characteristic of sick crew members on international voyage ships entering Zhoushan Port by sea.
3.1.3 Sensitivity analysis
We conducted sensitivity analysis after excluding extreme values of voyage time. Similarly, the incidence rate of COVID-19 was higher among the crew members with replacement, long voyage, and those who stayed at multiple anchorages or stayed for a long time. In addition to Crew replacement, the risk of COVID-19 infection among crew members with long voyage and those who stayed at multiple anchorages or stayed for a long time had increased. See Appendix Table 4 for specific details.
3.2 Public health assistance plan
3.2.1 Organizational management
To implement the public health assistance plan, the following professional working groups were established: a comprehensive coordination group, an epidemiological investigation group, a sampling and testing group, a personnel transport group, an environmental disinfection group, and a logistics support group. Point leaders were appointed at specific places, including infected ships, transport ships, wharfs, and designated hospitals, where there was a risk of spreading the virus to supervise the implementation of personnel transfer and epidemic control at each point.
3.2.2 Material preparation
Professionals were responsible for the procurement, management, storage, and distribution of epidemic prevention materials. Protective equipment included protective clothing, medical masks, medical hats, goggles, gloves, rubber shoes, waterproof shoe covers, waterproof aprons, etc., which met the requirements of WS/T 697-2020. Disinfection materials include chlorine-containing disinfectants, compound quaternary ammonium salts, ethanol, etc., which meet the requirements of GB/T 36758.
3.2.3 Sampling
On the basis of the risk assessment, the samplers wore secondary protective equipment and collected samples from the crew members in accordance with the Plan for the Prevention and Control of Pneumonia Caused by SARS-CoV-2 (Version 2) issued by the National Health Commission in 2020. Two upper respiratory tract samples, oropharyngeal swabs and nasopharyngeal swabs, which were placed in the same sample tube, were taken from each individual. The decision to collect additional samples was made on the basis of the results of the risk assessment. The samples were collected and sent to two departments with testing qualifications for parallel testing.
3.2.4 Personnel transfer
The transport of infected persons was divided into two situations on the basis of the number of infected persons (Figure 1):
1. The number of crew members who tested positive for SARS-CoV-2 infection was relatively small. If crew members who tested negative for SARS-CoV-2 infection could still maintain the ship’s power according to the postsetting requirements, all crew members who tested positive for SARS-CoV-2 infection were transferred at one time. Port supervisors took the transfer ship to the anchorage and supervised crew members who tested positive for SARS-CoV-2 infection, recommending that they take secondary protection measures. The personal belongings of crew members were disinfected. Supervisors maintained a certain distance from crew members who tested positive for SARS-CoV-2 infection and were not in the same enclosed space as infected individuals. Individuals who tested positive for SARS-CoV-2 infection maintained a distance of more than 1 meter from each other and disembarked to transfer ships in sequence. After arriving at the dock, the supervisor guided the crew members who tested positive for SARS-CoV-2 infection to walk to the negative pressure ambulance along the designated route. During the whole process, supervisors were not allowed direct physical contact with crew members who tested positive for SARS-CoV-2 infection. In the process of land personnel transfer, rush hours, congested roads, and crowded areas were as common as possible. After the ambulance arrives at the designated hospital, the medical staff on duty guided the crew members who tested positive for SARS-CoV-2 infection to enter the isolation ward via the designated route. Crew members who tested negative for SARS-CoV-2 were isolated in a single room on the ship. Daily health monitoring was needed.
2. Many crew members tested positive for SARS-CoV-2 infection. In this situation, crew members who tested positive for SARS-CoV-2 infection could not maintain the ship’s power according to the postsetting requirements. To maintain the safety of ships at sea, it was necessary to disembark them in batches for rescue. Crew members were transferred in batches; that is, some of the crew members were transferred first, and the necessary crew members were left behind to maintain the ship’s power. After the shipping company called for a full shift of crew members, the remaining crew members who tested positive for SARS-CoV-2 infection were transferred for treatment. In addition, new crew members were organized to board and change shifts. All crew members who tested positive for SARS-CoV-2 infection were subjected to risk assessment and disembarked in batches according to the severity of their illness, importance of their position, and age until new crew members replaced them. If the number of remaining crew members was not enough to maintain the ship’s power, the local government arranged enough tugs to guard the ship and turn on the main lighting on the ship at night. Crew members who tested negative for SARS-CoV-2 infection were generally transferred after crew members who tested positive for SARS-CoV-2 infection were transferred. The crew members could be transferred one hour after the point, and the transfer ship was disinfected. The transfer process was similar to that when the number of crew members who tested positive for SARS-CoV-2 infections was small.
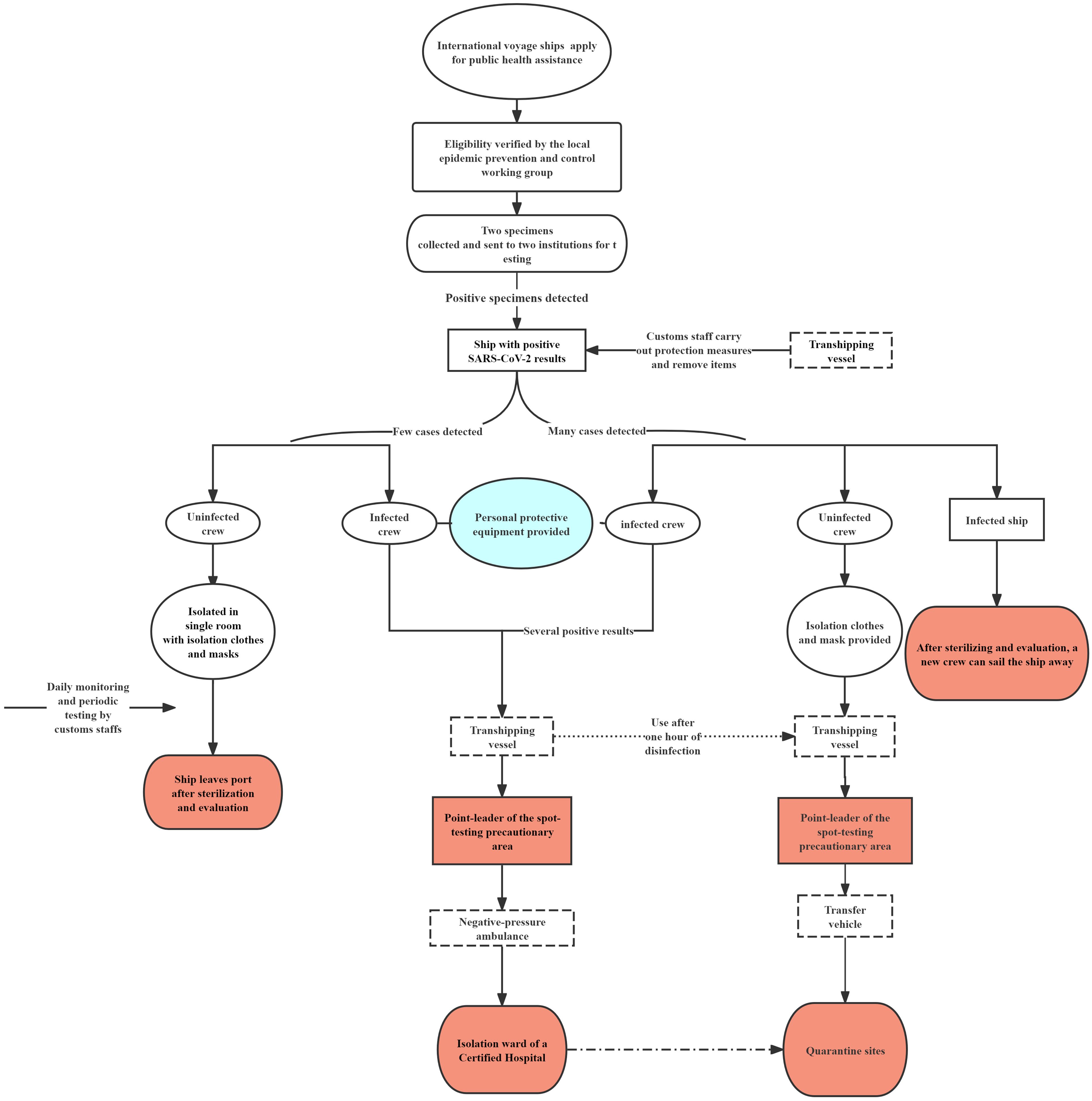
Figure 1. Public health assistance for the coronavirus disease 2019 (COVID-19) outbreak on international voyage ships.
4 Discussion
After the outbreak of COVID-19, it was necessary not only to protect the health of crew members to avoid further spread of the illness but also to maintain the power of the ship. These conditions required us to formulate a public health assistance plan for outbreaks of infectious diseases on these international voyage ships. We have developed and refined a plan for an outbreak of acute respiratory infectious diseases, which can provide policy recommendations for the control and prevention of sudden severe infectious diseases on international voyage ships.
Because of the enclosed or semienclosed environment and poor ventilation of international voyage ships, the rapid spread of infectious diseases easily occurs (Phares and Ortega, 2014). Among the international voyage ships entering Zhoushan Port by sea, the average incidence rate of crew members was 16.00% (95% CI: 13.73%–18.27%). The previous COVID-19 outbreaks involving international voyage ships were mainly concentrated on cruise ships, although a few were naval ships and cargo ships. On the Diamond Princess cruise ship and the Grand Princess cruise ship, the incidence rate of COVID-19 was 19.20% and 16.60%, respectively (Moriarty et al., 2020). The USS Theodore Roosevelt (TR) naval ship had an incidence rate of COVID-19 of 18.02% (Alvarado et al., 2020). These reports are consistent with our research findings. The incidence rate of crew members on long voyage was significantly higher than that of crew members on short voyage. This may indicate that prolonged exposure to a closed environment is beneficial for the spread of SARS-CoV-2 in populations as well as the need to improve ventilation and avoid air recirculation during ship navigation (Morawska and Cao, 2020). However, it seems that renovating the ventilation system onboard a ship is not easy (Cardoso et al., 2022). The incidence rate of crew members on ships with crew replacement was significantly higher than that of crew members without crew replacement, which indicates that the threat of SARS CoV-2 can result from shared exposure to infections with people carrying the pathogen, contact with food or water contaminated with the pathogen, etc (Kak, 2015). This finding suggests that we must complete personal health monitoring before the crew members are replaced and at least carry out personal protection before the crew members board the ship even if they are infected with SARS-CoV-2. However, if there is a lack of possibility for crew replacement due to travel restrictions, the working hours of the crew may be greatly extended, which poses challenges to the crew themselves (Kordsmeyer et al., 2021). Our research showed that the crew members who stayed at multiple anchorages or stayed at anchorages for a long time have a higher incidence rate of COVID-19, which may be due to the higher risk of virus exposure.
As the cornerstone of infectious disease control and prevention, quarantine ensures early detection of cases by restricting the movement of individuals who may have been exposed to pathogens or infected individuals or by separating these individuals from others (WHO, 2022). Quarantine includes movement restrictions on the ships and travel restrictions on the personnel (Moriarty et al., 2020). Restrictions on the movement of ships, whether isolated on board or on land, can effectively prevent further spread of the virus (Hatzianastasiou et al., 2021). However, Yamahata et al. argue that land isolation is not feasible due to transportation issues and a lack of land isolation facilities (Yamahata and Shibata, 2020). Cruise ships are suitable for mass population isolation because of their well-equipped accommodation spaces (Anan et al., 2020; Moriarty et al., 2020; Codreanu et al., 2021a). In addition, the quarantine policy should include close contacts, suspected cases, and other individuals involved in the outbreak. It should be isolated according to the region, and isolated as much as possible in a single compartment (Zhang et al., 2022). We rescued the sick crew members in batches and transferred them to the isolation ward of the hospital for treatment. We isolated crew members who tested negative for SARS-CoV-2 infection in the cabin to maintain the ship’s power to the greatest extent possible. If the ship’s power could not be maintained, they were transferred to a centralized isolation point by land transportation, which is consistent with the conclusions of a study by Anan et al (Anan et al., 2020). We required supervisors to maintain a certain social distance from sick crew members, which has been proven to be an effective preventive measure (Payne et al., 2020). Other effective prevention and control measures include personal protection, antiviral treatment, specific vaccination, and cleaning and disinfection (Kak, 2015; Moriarty et al., 2020). In addition, personal hygiene habits, such as following sneezing and coughing etiquette and washing hands with running water and alcohol-based hand sanitizers, are particularly important (Kordsmeyer et al., 2021). Currently, quarantine is utilized in conjunction with other measures to control COVID-19 outbreaks on cruise ships and cargo ships (Codreanu et al., 2021a; Codreanu et al., 2021b). When COVID-19 breaks out, the ship’s medical resources may be overwhelmed. To allocate medical resources, patients can be classified and sent to the corresponding hospital on the basis of their health status and PCR results (Anan et al., 2020). This task requires guidance and operation from a professional medical team, similar to the method we use to transport patients.
At present, Zhoushan Port has been reopened, and the maintenance and business of international voyage ships in the port has resumed, but the risk of the outbreak of acute infectious diseases such as COVID-19 continues to exist. The outbreak of COVID-19 has had a major impact on human health and international trade at sea. Therefore, effective prevention and control measures, including efficient public health assistance, must be taken. Our public health plan showed great advantages for controlling the COVID-19 outbreak on this international voyage ship. First, we transferred the ship according to the severity of the crew members’ illness so that the power of the ship could be maintained. Second, we adopted strict and effective closed-loop management measures, including strict personal protection and disinfection measures, to avoid the spillover of the virus during the transit process. Third, we established a relatively complete maritime rescue system, and the rescue efficiency was effectively improved through the mutual efforts of multiple departments. The limitation of this study is that the complete vaccination status of crew members was not collected, which makes it impossible to conduct research on the protective effects of vaccines. Vaccination may reduce the incidence rate of COVID-19, which may be a confounding factor that contributes to underestimation of the incidence rate of COVID-19. In addition, our public health assistance plan was summarized from real-life cases, and an evaluation of its effectiveness is lacking.
In conclusion, during an outbreak of COVID-19 at sea, we demonstrated the feasibility and safety of a plan through risk assessment and implementation of corresponding public health rescue procedures, including basic requirements, sampling and testing, personnel transport, medical waste disposal, and disinfection of the involved ship. This plan can be implemented for other international voyage ships for which public health assistance for sudden severe respiratory diseases is needed. Next, we will implement a scientific evaluation system to verify the effectiveness of the public health assistance plan. In addition, we will conduct research on public health rescue measures for other infectious diseases (such as infectious diarrhea) on international voyage ships to improve the public health rescue system for ship-related infectious diseases.
Data availability statement
The datasets presented in this article cannot be publicly shared due to privacy restrictions. Requests to access the datasets should be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Ethics Committee of the Zhoushan Center for Disease Control and Prevention. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because According to the “Ethical Review Measures for Biomedical Research Involving Human Beings” issued by the former National Health and Family Planning Commission in 2016, the ethics committee approved the exemption of subjects from signing informed consent forms. Written informed consent was not obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article because According to the “Ethical Review Measures for Biomedical Research Involving Human Beings” issued by the former National Health and Family Planning Commission in 2016, the ethics committee approved the exemption of subjects from signing informed consent forms.
Author contributions
YH: Conceptualization, Methodology, Writing – original draft. YD: Investigation, Writing – original draft, Software. JY: Data curation, Writing – original draft. WW: Data curation, Writing – original draft. PL: Visualization, Writing – original draft. KL: Visualization, Writing – original draft. WC: Supervision, Writing – review & editing. AT: Funding acquisition, Project administration, Resources, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The work was supported by Basic Welfare Research Project of Zhejiang Province (No.LGF22H260024) and Medical Science and Technology Project of Zhejiang Province (No.2022RC082).
Acknowledgments
In this study, we would like to express our gratitude to the laboratory of Zhoushan Municipal Center for Disease Control and Prevention for their support, as well as other authors who provided assistance in the research work.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be constructed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmars.2025.1566150/full#supplementary-material
References
Alharthy A., Aletreby W., Faqihi F., Balhamar A., Alaklobi F., Alanezi K., et al. (2021). Clinical characteristics and predictors of 28-day mortality in 352 critically ill patients with COVID-19: a retrospective study. J. Epidemiol. Glob. Health 11, 98–104. doi: 10.2991/jegh.k.200928.001
Alvarado G. R., Pierson B. C., Teemer E. S., Gama H. J., Cole R. D., Jang S. S. (2020). Symptom characterization and outcomes of sailors in isolation after a COVID-19 outbreak on a US aircraft carrier. JAMA Netw. Open 3, e2020981. doi: 10.1001/jamanetworkopen.2020.20981
Anan H., Kondo H., Takeuchi I., Nakamori T., Ikeda Y., Akasaka O., et al. (2020). Medical transport for 769 COVID-19 patients on a cruise ship by Japan disaster medical assistance team. Disaster Med. Public Health Prep. 14, e47–e50. doi: 10.1017/dmp.2020.187
Cardoso C. W., Souza M., Teles A., Argibay H. D., Reis O. B. D., Pereira F. M., et al. (2022). COVID-19 outbreaks among crew members in non-cruise vessels anchoring in Salvador, Brazil, 2021. Mem. Inst. Oswaldo Cruz. 117, e220114. doi: 10.1590/0074-02760220114
Codreanu T. A., Ngeh S., Trewin A., Armstrong P. K. (2021a). Successful control of an onboard COVID-19 outbreak using the cruise ship as a quarantine facility, Western Australia, Australia. Emerg. Infect. Dis. 27, 1279–1287. doi: 10.3201/eid2705.204142
Codreanu T. A., Pingault N., O’Loughlin E., Armstrong P. K., Scalley B. (2021b). The healthy crew, clean vessel, and set departure date triad: successful control of outbreaks of COVID-19 on board four cargo vessels. Prehosp Disaster Med. 36, 611–620. doi: 10.1017/S1049023X21000686
Daly L. E. (1998). Confidence limits made easy: interval estimation using a substitution method. Am. J. Epidemiol. 147, 783–790. doi: 10.1093/oxfordjournals.aje.a009523
Dao T. L., Hoang V. T., Gautret P. (2021). Recurrence of SARS-CoV-2 viral RNA in recovered COVID-19 patients: a narrative review. Eur. J. Clin. Microbiol. Infect. Dis. 40, 13–25. doi: 10.1007/s10096-020-04088-z
Guagliardo S. A. J., Quilter L. A. S., Uehara A., White S. B., Talarico S., Tong S., et al. (2023). COVID-19 on the Nile: a cross-sectional investigation of COVID-19 among Nile River cruise travellers returning to the United States, February-March 2020. J. Travel Med. 30. doi: 10.1093/jtm/taac153
Hatzianastasiou S., Mouchtouri V. A., Pavli A., Tseroni M., Sapounas S., Vasileiou C., et al. (2021). COVID-19 outbreak on a passenger ship and assessment of response measures, Greece, 2020. Emerg. Infect. Dis. 27, 1927–1930. doi: 10.3201/eid2707.210398
Hu B., Guo H., Zhou P., Shi Z. L. (2021). Characteristics of SARS-coV-2 and COVID-19. Nat. Rev. Microbiol. 19, 141–154. doi: 10.1038/s41579-020-00459-7
Kak V. (2015). Infections on cruise ships. Microbiol. Spectr. 3. doi: 10.1128/microbiolspec.IOL5-0007-2015
Kordsmeyer A. C., Mojtahedzadeh N., Heidrich J., Militzer K., von Münster T., Belz L., et al. (2021). Systematic review on outbreaks of SARS-coV-2 on cruise, navy and cargo ships. Int. J. Environ. Res. Public Health 18, 5195. doi: 10.3390/ijerph18105195
Maeda H., Sando E., Toizumi M., Arima Y., Shimada T., Tanaka T., et al. (2021). Epidemiology of coronavirus disease outbreak among crewmembers on cruise ship, Nagasaki City, Japan, April 2020. Emerg. Infect. Dis. 27, 2251–2260. doi: 10.3201/eid2709.204596
Morawska L., Cao J. (2020). Airborne transmission of SARS-CoV-2: The world should face the reality. Environ. Int. 139, 105730. doi: 10.1016/j.envint.2020.105730
Moriarty L. F., Plucinski M. M., Marston B. J., Kurbatova E. V., Knust B., Murray E. L., et al. (2020). Public health responses to COVID-19 outbreaks on cruise ships - worldwide, February-March 2020. MMWR Morb. Mortal Wkly Rep. 69, 347–352. doi: 10.15585/mmwr.mm6912e3
Payne D. C., Smith-Jeffcoat S. E., Nowak G., Chukwuma U., Geibe J. R., Hawkins R. J., et al. (2020). SARS-coV-2 infections and serologic responses from a sample of U.S. Navy service members - USS theodore roosevelt, April 2020. MMWR Morb. Mortal Wkly Rep. 69, 714–721. doi: 10.15585/mmwr.mm6923e4
Phares C. R., Ortega L. (2014). Crossing borders: one world, global health. Clin. Infect. Dis. 58, iv–iv. doi: 10.1093/cid/cit762
Plucinski M. M., Wallace M., Uehara A., Kurbatova E. V., Tobolowsky F. A., Schneider Z. D., et al. (2021). Coronavirus disease 2019 (COVID-19) in Americans aboard the diamond princess cruise ship. Clin. Infect. Dis. 72, e448–ee57. doi: 10.1093/cid/ciaa1180
Walker L. J., Codreanu T. A., Armstrong P. K., Goodwin S., Trewin A., Spencer E., et al. (2021). SARS-CoV-2 infections among Australian passengers on the Diamond Princess cruise ship: A retrospective cohort study. PloS One 16, e0255401. doi: 10.1371/journal.pone.0255401
WHO (2022). Contact tracing and quarantine in the context of COVID-19: interim guidance. Available online at: https://www.who.int/publications/i/item/WHO-2019-nCoV-Contact_tracing_and_quarantine-2022.1 (Accessed November 13, 2024).
Yamahata Y., Shibata A. (2020). Preparation for quarantine on the cruise ship diamond princess in Japan due to COVID-19. JMIR Public Health Surveill. 6, e18821. doi: 10.2196/18821
Yuan Y., Jiao B., Qu L., Yang D., Liu R. (2023). The development of COVID-19 treatment. Front. Immunol. 14, 1125246. doi: 10.3389/fimmu.2023.1125246
Zhang H. P., Sun Y. L., Wang Y. F., Yazici D., Azkur D., Ogulur I., et al. (2023). Recent developments in the immunopathology of COVID-19. Allergy 78, 369–388. doi: 10.1111/all.15593
Keywords: international voyage ship, Zhoushan port, COVID-19, cross-sectional survey, public health assistance
Citation: Hua Y, Dai Y, Yi J, Wu W, Li P, Li K, Chen W and Tang A (2025) A cross-sectional survey of international voyage ships entering Zhoushan Port by sea, Zhoushan, 2020-2022. Front. Mar. Sci. 12:1566150. doi: 10.3389/fmars.2025.1566150
Received: 24 January 2025; Accepted: 09 April 2025;
Published: 30 April 2025.
Edited by:
Yen-Chiang Chang, Dalian Maritime University, ChinaCopyright © 2025 Hua, Dai, Yi, Wu, Li, Li, Chen and Tang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: An Tang, dGFuZ2FuenNjZGNAMTI2LmNvbQ==
†These authors share first authorship