Abstract
The analysis of fetal heart rate variability has served as a scientific and diagnostic tool to quantify cardiac activity fluctuations, being good indicators of fetal well-being. Many mathematical analyses were proposed to evaluate fetal heart rate variability. We focused on non-linear analysis based on concepts of chaos, fractality, and complexity: entropies, compression, fractal analysis, and wavelets. These methods have been successfully applied in the signal processing phase and increase knowledge about cardiovascular dynamics in healthy and pathological fetuses. This review summarizes those methods and investigates how non-linear measures are related to each paper's research objectives. Of the 388 articles obtained in the PubMed/Medline database and of the 421 articles in the Web of Science database, 270 articles were included in the review after all exclusion criteria were applied. While approximate entropy is the most used method in classification papers, in signal processing, the most used non-linear method was Daubechies wavelets. The top five primary research objectives covered by the selected papers were detection of signal processing, hypoxia, maturation or gestational age, intrauterine growth restriction, and fetal distress. This review shows that non-linear indices can be used to assess numerous prenatal conditions. However, they are not yet applied in clinical practice due to some critical concerns. Some studies show that the combination of several linear and non-linear indices would be ideal for improving the analysis of the fetus's well-being. Future studies should narrow the research question so a meta-analysis could be performed, probing the indices' performance.
1. Introduction
Worldwide, it is estimated that the number of fetal deaths after week 20 of gestational age is around 2.6 million per year. Although the numbers have been decreasing in the past decades, the stillbirths' rate still ranges from about 1 in 250 births in developed countries and 1 per 33 in South Asia and Sub-Saharan Africa (data from 2009), according to Cousens et al. (1).
Cardiotocography (CTG) combines fetal heart rate (fHR) measurement, obtained through a uterine contraction monitoring probe and a Doppler ultrasound probe for fHR, recorded using an abdominal pressure transducer. In developed countries, clinical decisions during labor are firmly based on fHR monitoring (2, 3), being CTG the most used tool to assess fetal well-being since the early '60s according to Spencer (4). However, the information provided by CTG is limited since a complete electrocardiogram (ECG) signal of the fetus is not available. Moreover, the CTG is highly sensitive to both fetal and maternal movement. The use of an electrode placed on the fetus's scalp is more reliable as it retrieves fetal electrocardiogram, containing not only fHR but also other crucial clinical parameters (5, 6). On the other hand, this is an invasive method only possible during labor, after the beginning of cervical dilatation and the membranes' rupture, carrying with it risks of infection (7, 8). However, other methods for fetal monitoring are used such as fetal phonocardiography (9–11), fetal echocardiography (12, 13), and fetal magnetocardiography (14, 15). Each one of the methods has its own advantages and disadvantages. For more detail on this matter, see Jaros et al. (16) and Hoyer et al. (17).
Electronic fetal monitoring came with high expectations since it offered continuous monitoring, compared to the intermittent auscultation done until then. However, a meta-analysis of large multicenter studies did not prove any significant improvement. Also, electronic fetal monitoring became the main suspect for the increased rate of cesarean sections (18). These procedures result in a slight increase in poor outcomes in low-risk pregnancies. The cesarean sections also require a longer time to heal than a vaginal birth and present increased risks, including baby breathing problems, amniotic fluid embolism, and postpartum bleeding for the mother (19). Despite the importance of the fetus and mother well-being assessment, low concordance between physicians is still present, even among experienced obstetricians, resulting in a high rate of false-positives (2, 20, 21). In daily practice, fHR is subject to the clinician visual interpretation, even when following the guidelines provided by the International Federation of Obstetrics and Gynaecology (FIGO) (22, 23), which although being associated with high sensitivity but low specificity (24), might leads to a chance of more harmful than beneficial adherence to conventional guidelines (25).
The autonomic nervous system (ANS) is involved in the control of almost every organ system, and the beat-to-beat variation of fHR reflects the influence of the fetus' ANS and its components (sympathetic and parasympathetic) and, therefore, is an indicator of fetal well-being (8). A certain level of unpredictable fetal heart rate variability (fHRV) reflects sufficient capabilities of the organism in search of optimal behavior. Reduced fHRV is linked with limited capabilities and mental disorders (26). The linear modeling approaches quantify sympathetic and parasympathetic control mechanisms and their balance by measuring spectral low and high-frequency components. However, it has been shown that not all information carried by beat-to-beat variability can be explained by these components (27). For this matter, in the past couple of decades, and with the fast development of computation, new signal processing, and pattern recognition methodologies have been developed and applied to many different fields, including the analysis of fHRV using non-linear parameters (28, 29). These approaches can reveal relevant clinical information not exposed by temporal or frequency analysis (30).
Variability and complexity are different terms. While a complex system requires variability, the other way around is not guaranteed. For example, a set of random notes in music can be interpreted as having high complexity for its non-predictability, whereas a set of consecutive notes is highly predictable, and both have high variability. Thus, complexity signals, such as those produced by self-regulatory physiological systems, present temporal or spatial structures over a varied range of scales. Because of their non-linearity and non-stationarity, conventional indicators, such as the mean and the standard deviation, do not fulfill their purpose (31). In the end, complexity is a property of any system that quantifies the amount of structured information.
Chaffin et al. (32), in 1991, were the first to use non-linear analyzes in fHR. The authors applied fractal analysis (correlation dimension) to study 12 normal fetuses' well-being in labor. Later, in 1992, Pincus and Viscarello (33) found statistically significant results using approximate entropy (ApEn) when comparing a group of acidemic fetuses with non-acidemic ones. These results supported the hypothesis that regular fHR patterns are associated with acidemia. Datian and Xuemei (34), in 1996, introduced a new wavelet analysis method used to detect fetal electrocardiogram from the abdominal signal and compared to other methods in practice. Signorini et al. (35), in 2005, applied data compression (Lempel Ziv complexity) for the first time in the fHR analysis to improve the early detection of fetal distress conditions such as intrauterine growth restriction. The same authors, also in 2007 (36), used the Lempel Ziv complexity to successfully discriminate between severe intrauterine growth restriction (IUGR) (premature birth) and non-severe IUGR (term delivery) and normal fetuses. In the subsequent year, using a compressor-based clustering algorithm called normalized compression distance (NCD), Santos et al. (37) managed to clustered abnormal and suspicious tracks, regardless of the monitoring system used. Barquero-Pérez et al. (38) also used NCD for automatic detection of perinatal hypoxia.
The main contribution of this article is to provide a systematic review of articles that apply entropy, compression, fractal, and wavelet analysis to study the dynamics of fHR and analyze the research objectives of these articles. As far as we know, there is no systematic review for this purpose in the literature.
We begin by describing the methodology used, specifying the sources of information, the eligibility criteria, the study selection, data extraction, and quality assessment in section 2. Based on the systematic review results, we describe in detail the most commonly used non-linear methods to assess the dynamics of fetal heart rate and analyze how the study of the complexity of fHR has evolved over the years (section 3). In section 4, we describe the most frequent goals in research. We analyze the evolution of the non-linear methods' applications to these objectives and probe how the research objectives are related to non-linear methods. In section 5, we reflect on some open questions regarding the application of non-linear measurements to fHR dynamics. We finish this paper with the main conclusions in section 6.
2. Systematic Review Methods
This systematic review focused on original papers that include non-linear analysis, such as complexity measures, fractal approaches, and wavelets, of human fetal heart rate during ante and intrapartum. The online search was performed on Medline, through PubMed, and the Web of Science databases, searching all the papers published until the 4th of October 2020. The following terms were used as descriptors/Mesh: “non-linear dynamics,” “entropy,” “data compression,” “complexity,” “fractals,” “wavelets,” “fetal heart rate,” “foetal heart rate.” The queries used in each database can be found in Table 1. This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement (39). The review protocol was not registered prospectively.
Table 1
| Pubmed (https://www.ncbi.nlm.nih.gov/pubmed) |
| (“Nonlinear Dynamics”[Mesh] OR “Nonlinear Dynamics”[Title/Abstract] OR Nonlinear[Title/Abstract] OR “Entropy”[Mesh] OR Entropy[Title/Abstract] OR “Data Compression”[Mesh] OR “Data Compression”[Title/Abstract] OR Compression[Title/Abstract] OR complexity[Title/Abstract] OR “fractals”[MeSH Terms] OR fractals[Title/Abstract] OR “Wavelet Analysis”[Mesh] OR “Wavelet Analyses”[Title/Abstract] OR wavelet[Title/Abstract]) AND (“Heart Rate, Fetal”[Mesh] OR “Fetal Heart Rate”[Title/Abstract] OR “foetal heart rate”[Title/Abstract]) |
| Web of Science (https://www.webofknowledge.com) |
| (TS=(“Nonlinear Dynamics” OR nonlinear OR entropy OR Compression OR complexity OR fractal OR wavelet) OR TI=(“Nonlinear Dynamics” OR nonlinear OR entropy OR Compression OR complexity OR fractal OR wavelet)) AND (TI=(“Heart Rate, Fetal”) OR TI=(“Fetal Heart Rate”) OR TI=(“foetal heart rate”) OR TS=(“fetal heart rate”) OR TS=(“foetal heart rate”)) |
Online queries in Pubmed and Web of Science.
Inclusion criteria for selecting studies were the following: observational or experimental papers presenting complexity analysis of fetal heart rate; abstract found online; reported original research in peer-reviewed journals; at least one measure from the following was used in the analysis (entropy, compression, fractal, or wavelet). Papers using non-human fetal heart rate analysis, papers without an English version, reviews, case studies, dissertations, and thesis were excluded (see Figure 1).
Figure 1
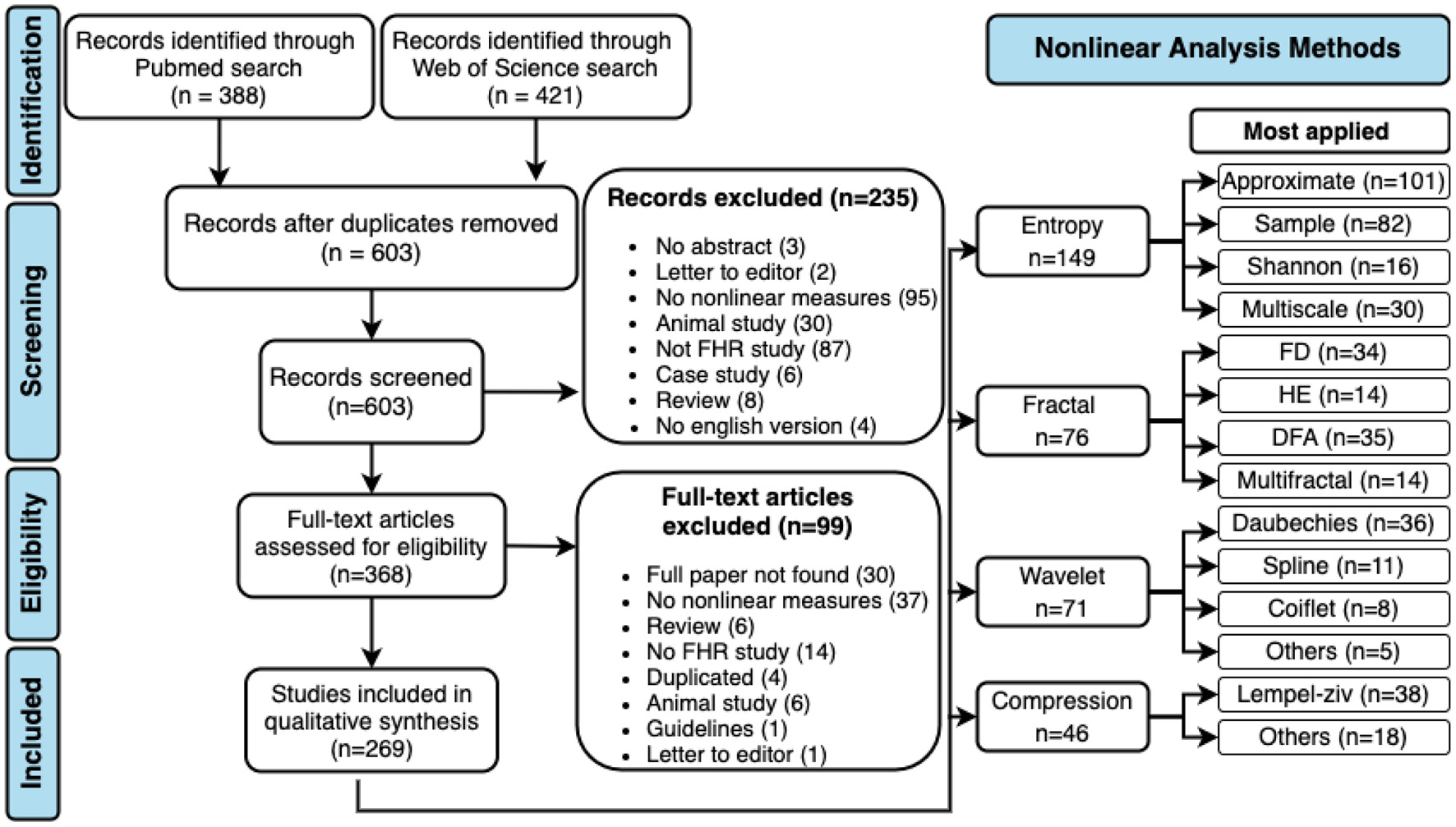
PRISMA flow diagram and non-linear methods most applied in fHR. DFA, detrended fluctuation analysis; FD, fractal dimension; HE, Hurst exponent.
All authors were involved in the selection of studies, data extraction, and quality assessment. Two authors independently assessed each title and abstract found in the databases. The full texts of potentially relevant studies have been retrieved and revised in depth. Disagreements between reviewers were resolved by consensus or by the decision of a third independent reviewer. For each article, the following data were collected: year of publication, study design, objective, sample size, measure(s) used to analyze fHR, and conclusions. Both reviewers made sure that all included papers met the criteria defined in the first stage.
A total of 603 abstracts were assessed, 368 of which retained for full-text screening. Two hundred and seventy papers were then included in the review after meeting all the criteria. Figure 1 contains the PRISMA flow diagram for study selection, including reasons for exclusion. The most used non-linear analysis measures to study the dynamics of fHR obtained in the systematic review are also represented in Figure 1.
3. Non-linear Methods
Although linear indices have been extensively used in fetal monitoring for the past decades, it is established that biological systems are more complex than they appear. Non-linear measures based on concepts of chaos, fractality, and complexity have gained space and demonstrated promising results in the analysis of fetal well-being and the prediction of pathologies. The application of non-linear measures to study the dynamics of fHR has increased over the years. The non-linear methods covered by this review are entropy, compression, fractal analysis, and wavelet analysis. The results show that entropy is the most applied measure in fetal heart rate, followed by fractal analysis, wavelet analysis, and the least applied is the compression (see Figures 1, 2). Although the application of entropy methods stands out, we can see that compression and wavelet analysis methods have been increasingly used in recent years (see Figure 2).
Figure 2
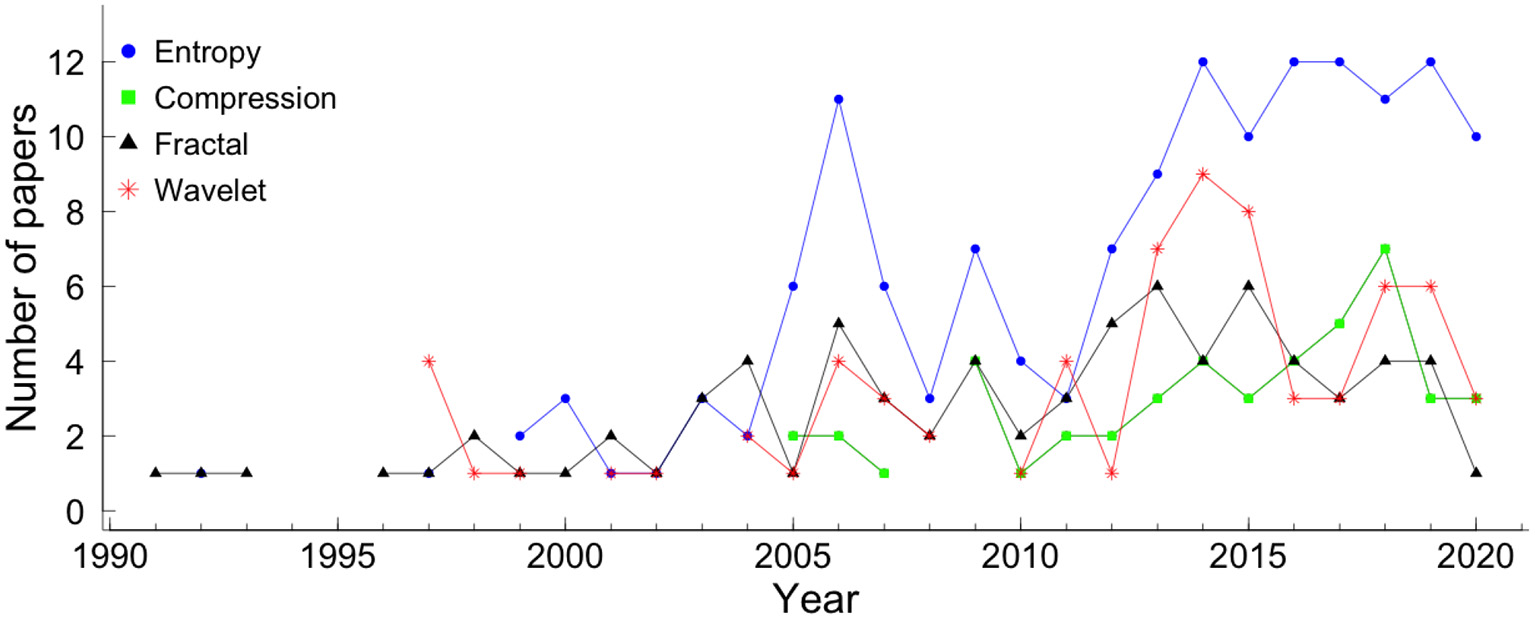
The number of papers, covered by the systematic review, that applied each method. The blue circle represents entropy, the green square represents compression, the black triangle represents fractal analysis, and the red star represents wavelet.
In the following sections, the most applied non-linear methods are described. In our systematic review, other non-linear methods were found, such as, Poincaré plot (in 18 papers), symbolic dynamics (in 12 papers), phase rectified signal average (in 10 papers), Lyapunov exponents (in 6 papers), and recurrence plot analysis (in 6 papers). However, due to the reduced number of uses, they were not described in detail. For this review, we decided to describe only the measures most applied to fHR.
3.1. Entropy
According to Shannon (40), the information within a signal can be quantified with absolute precision as the amount of unexpected data in the message (defined as entropy). Entropy, a probabilistic complexity measure used to quantify a time series's irregularity, has been widely used in physiological signal analysis. The number of papers that applied each entropy measure per year is shown in Figure 2. The entropy measures that were applied to at least 15 articles were: Shannon entropy (SE), approximate entropy (ApEn), sample entropy (SampEn), and multiscale entropy (MSE).
From all 270 papers included in this review, 149 (55.2%) papers applied entropy: 16 (5.9%) show results with Shannon entropy (SE), 82 (30.4%) used SampEn, 101 (37.4%) used ApEn, and 30 (11.1%) used MSE (see Figure 1). Figure 3 shows the number of papers that applied measures of the entropy by year. ApEn is the most applied measure. However, in recent years the employment of SampEn and ApEn is similar.
Figure 3
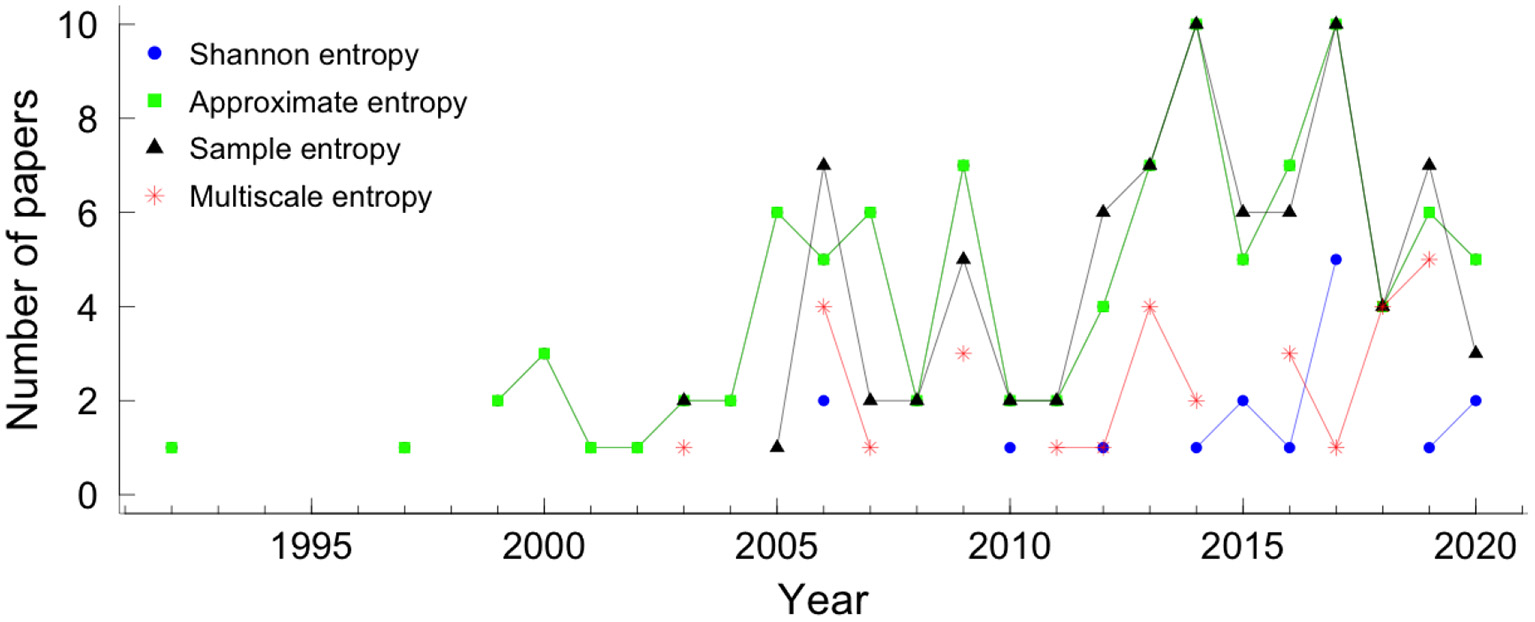
Entropies by year. The colors and symbols represent the different measures of entropy. The blue circle, green square, black triangle, and star red represented Shannon entropy, approximate entropy, sample entropy, and multiscale entropy, respectively.
In the literature, we found other entropy measures that appeared in less than 15 articles, such as, permutation entropy (41–45), Rnyi entropy (46–48), Kullback-Leibler entropy (41, 42, 49, 50), Kolmogorov-Sinai entropy (30), cross-sample entropy (51, 52), tone-entropy (53), bubble entropy (47), and compression entropy (46).
3.1.1. Shannon Entropy (SE)
In 1948, Shannon (40) proposed the concept of entropy (Shannon entropy - SE) to measure how the information within a signal can be quantified with absolute precision as the amount of unexpected data contained in the message. The Shannon entropy is obtained by:
where p(x(i)) represents the probability of the point x(i), of a time series X = (x1, x2, ..., xN).
Though SE was introduced back in 1948, and many new entropies appeared to overcome some of the SE limitations, some authors still applied it in the analysis of fHRV (46, 54).
3.1.2. Approximate Entropy (ApEn)
In 1991, Pincus et al. (55) developed a regularity statistic tool to quantify the amount of regularity and the unpredictability of fluctuations over time-series data. The ApEn is based on the assumption that healthy dynamic stability comes from specific networks' specific mechanisms and properties. When a vulnerable connection arises between systems or within one, it is the disease mechanism, which is characterized by an increase of regularity of the series (56).
Considering a time series X = (x1, x2, ..., xN), in order to calculate the ApEn the new series of a vector of length m (embedding dimension), Xm(i) = (xi, xi+1, xi+2, …, xi+m−1) are constructed for each i = 1, …, N − m + 1. For each vector Xm(i), the value , where r is referred as a tolerance value, is computed as:
Here, the distance between the vector Xm(i) and its neighbor Xm(j) is defined as:
Next, the average of the natural logarithm of is computed for all i:
Since in practice N is a finite number, the statistical estimate is computed as:
In the particular case of the ApEn, the most common value is m = 2. However, many algorithms were proposed to estimate the smallest sufficient embedding dimension, m. One of the most used methods is the “false nearest-neighbors” algorithm proposed by Kennel et al. (57). Though, the limitation of this method relies on the subjective definition of false neighbor (58). To overcome this limitation, Cao (58) proposed a new method.
For estimation of an appropriate time delay various approaches have been proposed. The most used two are the autocorrelation function and the average mutual information function (59). Pincus (60) and Pincus and Goldberger (61) recommends values between 10 and 25% of the standard deviation of the data, hence obtaining a scale-invariant measurement. The approach of choosing a fixed r value was also used with success (62, 63). However, the values of entropy in this case are usually highly correlated with the time series standard deviation. Lu et al. (64) showed that ApEn values varied significantly even within the defined range of r values and presented a new method for automatic selection of r that corresponds to the maximum ApEn value.
3.1.3. Sample Entropy (SampEn)
In 2000, Richman and Moorman (65) proposed the sample entropy (SampEn), with the same purpose as ApEn, to evaluate the randomness of biological time series, in particular, the HR time series. The main limitation of the ApEn is the dependence on the record length, i.e., the ApEn is lower for short records, and if one time series is higher than another, it should not remain higher for all conditions (65). In order to overcome the limitations, the authors proposed a new family of statistics, SampEn(m, r), which, with some differences, reducing bias specially in short data sets:
-
self-matches are not counted;
-
only the first N-vectors of length are considered;
-
the conditional probabilities are not estimated in a template manner.
To calculate the value of SampEn (65) the parameters m, and r defined for ApEn are needed. Considering A as the number of vector pairs of length m + 1 having d[Xm(i), Xm(j)] ≤ r, with i ≠ j and B as the total number of template matches of length m also with i ≠ j, the SampEn is defined by the equation:
This probability measure is computed directly as the logarithm of conditional probability and not from the logarithmic sums ratio, showing relative consistency in cases where ApEn does not (65).
3.1.4. Multiscale Entropy (MSE)
ApEn and SampEn have the disadvantage of outputting a single index concerning the time series's general behavior, thus not revealing its underlying dynamics. MSE has been widely employed in the biomedical signal analysis as it allows measuring signal properties at different time scales (66, 67).
Considering a time series X = {xi} of N points, it constructs consecutive coarse-grained time series , replacing τ non-overlapping points by their average. The MSE curve is created by computing the entropy for each of the scales and plotted vs. the scale. The information of the different time scales is clustered in the complexity index defined as the area under the MSE curve.
The estimation of the complexity methodology has to follow the multiscale application requirements, and SampEn was proposed using a tolerance r obtained from the original series and keeping it constant for all scales (67). Other authors were in favor of choosing an individual tolerance level r for each scale (68, 69). For example, the quadratic sample entropy permits a personalized estimation of r for each scale in short data (70).
The physiological interpretation of multiscale complexity is not always clear once, in a complex dynamic system, all scales might be affected by regulating influences (71). Low complexity scales indicate regular patterns with periodicity, but isolated ones would indicate one single frequency oscillation periodicity that usually is not present in complex systems. However, it is typical of the appearance of correlated neighboring scales (41, 67).
3.2. Compression
Dynamic systems theory was firstly linked with information theory by Kolmogorov (72), in 1958. Years later, “algorithm information theory” was then independently proposed by three different authors, Solomonoff (73), Kolmogorov (74) and Chaitin (75).
Let x be a finite length binary string, be a universal computer, l(x) denote the length of the string x and the output of the computer when presented with a program p. The Kolmogorov (or algorithmic) complexity (KC) of a string x with respect to a universal computer , , is defined as the shortest description length of x over all descriptions interpreted by computer . In different words, KC quantifies how “random” an individual object is in terms of the number of bits necessary to describe it. For a random string, the output of function will be the original string's length as any compression effort will end in information loss. The more reoccurring patterns, the less complex the signal is. Although this concept is objective, its applicability is limited to the fact that it is not computable. Compressors are a close upper-bounded approximation of the function. For over 30 years, data compression software has been developed for data storage and transmission efficiency purposes, and more recently, compression has been utilized in health research.
The innumerous compressors found in the literature can be divided into two big groups: lossless or lossy. The former group is composed of compressors in which, after being decompressed, all original information is restored. For the lossy group, this is not guaranteed, particularly for redundant information. The most applied compressors in health research belong to the first group.
The Lempel–Ziv algorithm was introduced, in 1976, by Lempel and Ziv (76) based on 'the concept of encoding future segments of the source output via maximum-length copying from a buffer containing the recent past output.' It was the starting point for different compressors such as the Lempel–Ziv–Markov chain algorithm, LZ77, LZ78, and gzip. The bzip2 was developed by Seward (77) and used the block sort algorithm giving speedy results.
In order to estimate the complexity of a physiological signal using compression, different approaches have been used, such as an increase/decrease coding system using a binary (30, 78, 79) or ternary alphabet (80, 81).
Compression also has been used for research purposes in a wide variety of fields such as literature (82), music (83), computer virus and internet (84) traffic, but only in 2004, it was first applied in HRV time series by Ferrario et al. (85). Here, compression demonstrated to differentiate healthy fetuses from unhealthy ones. In fact, the former group complexity calculated with LZ achieved similar results to random noise (meaning high complexity), while in the latter group, its complexity was lower, showing sinusoidal patterns. The applications of compression in health research range from event detection [such as epileptic seizure (86), the onset of ventricular tachycardia or fibrillation (87) and changes from sleep to waking state in-depth anesthesia (88)], characterizing neural spike trains (89), fHR biometric identification (90) or in DNA sequences studies (91). A distinct approach to applying compression on a time series uses the normalized compression distance (NCD) measure, a dissimilarity learning approach first used in fHR by Santos et al. (37).
From all 270 papers included in this review, 46 (17%) show results with compression. Its usage throughout recent years can be seen in Figure 4.
Figure 4
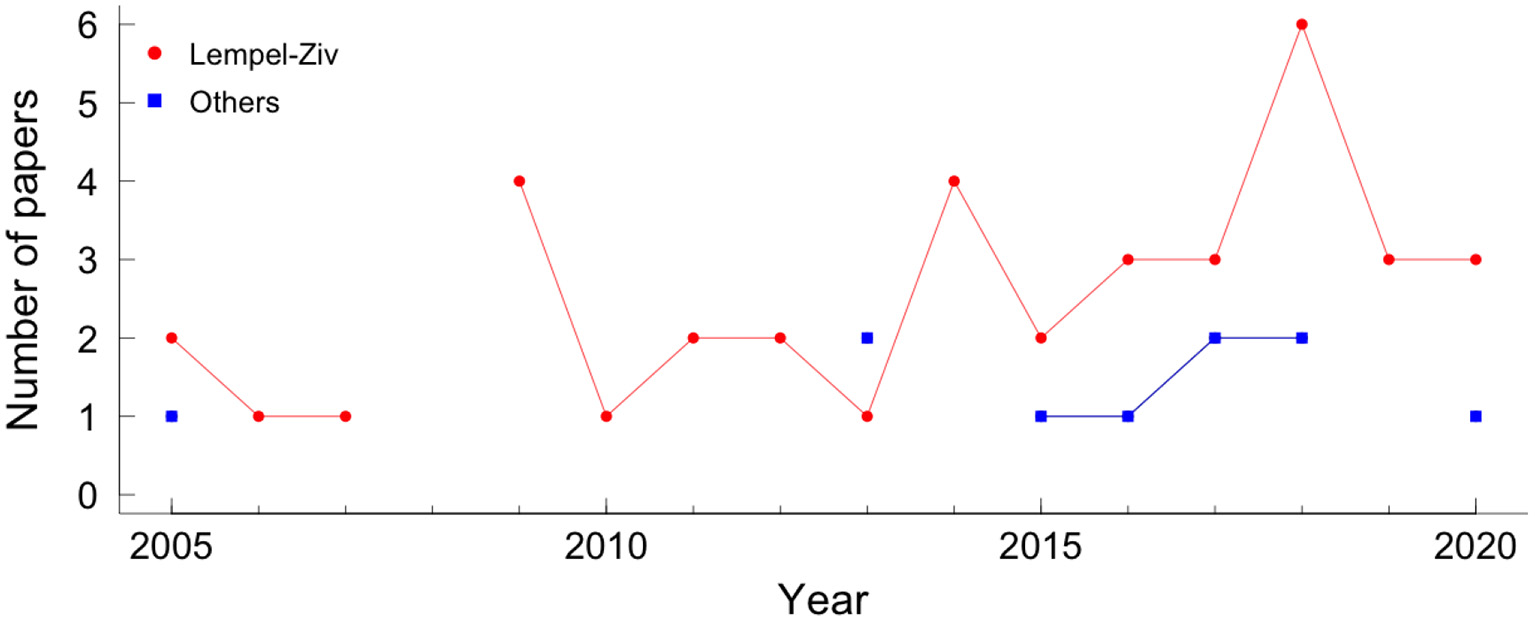
Papers using compression in fetal heart rate, by year. The red circle represents the Lempel-Ziv compressor and the blue square represents the other compressors.
3.3. Fractal Analysis
Fractality indices quantify self-similarity and fractal- or multifractal-like behaviors. The heart rate fluctuates on different timescales and is similar to itself, which is a good premise for a fractal analysis approach (30).
Of all 270 papers included in this review, 28.1% applied fractal analysis. More specifically, 35 (13.0%) used detrended fluctuation analysis (DFA), 34 (12.6%) show results with fractal dimension (FD), 14 (5.2%) used Hurst exponent and 14 (5.2%) multifractal analysis (see Figure 1). Figure 5 shows the number of papers that applied measures of fractal analysis by year.
Figure 5

Papers using fractal analysis in fetal heart rate, by year. The blue circle represents the fractal dimension measure, the green square represents the detrended fluctuation analysis, the black triangle represents the Hurst exponent, the red star represents the multifractal analysis.
Fractal dimension, Hurst exponent, and DFA are described in sections 3.3.1–3.3.3, respectively. The multifractal analysis describes more complex signals than those fully characterized by a monofractal model but requires many local and theoretically infinite exponents to characterize their scaling properties completely. The multifractal detrended fluctuation analysis (MF-DFA), the most applied multifractal method in the papers covered by the systematic review, is described in section 3.3.4.
3.3.1. Fractal Dimension (FD)
A fractal dimension (FD) is a statistical index of how the detail in a pattern changes with the scale at which it is measured. The FD appears to provide a measure of how much space an object occupies between Euclidean dimensions. The higher the FD value, the more irregular the signal is and, therefore, the more self-similar the signal will be.
Of the various algorithms available to calculate the FD of a time series, the four most used are the algorithms proposed by Katz (92) and Higuchi (93, 94), the correlation dimension, and the box-counting dimension (95). More details on the FD calculation algorithms of a time series can found at Henriques et al. (96).
3.3.2. Hurst Exponent
Hurst exponent (HE) or Hurst coefficient is a dimensionless estimator used to evaluate the self-similarity and the long-range correlation properties of time series (97). There are many algorithms to estimate the HE parameter in the literature. The oldest is the so-called rescaled range analysis (R/S) popularized by Mandelbrot and Wallis (98, 99) and it is defined in terms of the asymptotic behavior of the rescaled range (a statistical measure of the variability of a time series). Alternative methods to estimate HE include detrended fluctuation analysis (100, 101), periodogram regression (102), aggregated variances (103), local Whittle's estimator (104), first return method (105), wavelet analysis (106), both in the time domain and frequency domain. Furthermore, there is a relation between HE and the FD, given by FD = E+1−HE, where E is the Euclidean dimension, which for time series is 1 obtaining their relationship FD = 2−HE (107). The HE may range between 0 and 1 and can indicate:
-
0 < HE < 0.5: time series has long-range anti-correlations;
-
HE = 0.5: there is no correlation in the time series;
-
0.5 < HE < 1: there are long-range correlations in the time series;
-
HE = 1: the time series is defined self-similar, i.e., it has a perfect correlation between increments.
3.3.3. Detrended Fluctuation Analysis (DFA)
Detrended fluctuation analysis (DFA) quantifies intrinsic fractal-like (short and long-range) correlation properties of dynamic systems (101). Two advantages of DFA over conventional methods (such as the HE method) are that this method allows the detection of intrinsic self-similarity embedded in a non-stationary time series and also avoids the detection of apparent self-similarity (108).
To execute the DFA algorithm the first step is to integrate the time series (of length N). The next step is to split the integrated time series into Nn windows of equal length n. Then, a least-squares line is fitted to the data, in each window of length n. The y-coordinate of the straight-line segments is given the name of yn(k). Then, the integrated time series is detrended, yn(k), in each window. The root mean square fluctuation of this integrated and detrended series is calculated by the following equation:
This algorithm is repeated for all time scales (box sizes) to characterize the relationship between F(n), the average fluctuation, and the box size, n. Normally, F(n) increases with the size of the window, according to F(n) ∝ nα. The α exponent can be viewed as an indicator of the “roughness” of the original time series: the higher the value of α, the smoother the time series:
-
if α ≃ 0.5, the time series represents uncorrelated randomness (white noise);
-
if α ≃ 1 (1/f-noise), the time series has long-range correlations and exhibits scale-invariant properties;
-
if α ≃ 1.5, the time series represents a random walk (Brownian motion).
Usually, the DFA method involves estimating a short-term fractal scaling exponent, α1, and a long-term scaling exponent, α2.
3.3.4. Multifractal Detrended Fluctuation Analysis (MF-DFA)
The multifractal DFA (MF-DFA) calculation (109, 110) is similar to the DFA since only two additional steps are taking into consideration. The fitting procedure in the MF-DFA can be linear, quadratic, cubic, or higher-order polynomials (MF-DFAm - the mth order of the MF-DFA) (101, 111, 112). By comparing the results obtained for different MF-DFA orders, it is possible to estimate the order of the polynomial segment trends in the time series (109, 112). The procedure must be repeated for various n time scales, as we are interested in how this q-dependent fluctuation function depends on the n time scale for different q values. The other additional step is a q dependent averaging procedure obtaining a generalized (multifractal) scaling exponent h(q). For q = 2, the standard DFA procedure is retrieved.
The main problem with the MF-DFA method is that all the steps are deeply dependent on the user's decisions. The Multiscale multifractal analysis (MMA) (71, 113) is a generalization of the MF-DFA method. The method creates a Hurst surface h(q,s), allowing a broader analysis of the fluctuation properties and more stable results. Also, all multifractal methods, including MMA, require a relatively long time series to analyze.
3.4. Wavelets Analysis
The first appearance of the term wavelet was in an annex to Haar thesis' (114). However, it is considered that the wavelet theory was developed in the late 1980s by Mallat (115), Daubechies and Bates (116, 117) to meet the needs for adaptive time-frequency analysis applied to signal processing, mathematics, physics, and engineering. Wavelets are functions that satisfy a series of mathematical parameters and are used in the representation of data or other functions. The term wavelet comes from the fluctuation around the axis, integrating to zero (the areas above the axis and below are the same). Wavelet algorithms process information at different scales (or resolutions). The decomposition of a function using wavelets is known as a transformed wavelet, and it has continuous and discrete variations. Due to the ability to decompose functions in frequency and time domains, wavelet functions are powerful tools for signal processing, widely used in data compression, noise elimination, separation of components in the signal, identification of singularities, and auto-similarity detection.
Let ψs, u(t), s, u ∈ ℜ, s > 0 be a family of functions defined as translations and re-scales of a single function ψ(t) ∈ L2(ℜ), L2(ℜ) denotes the space of square-integrable functions on ℜ (118),
where s is the scaling parameter and u the position parameter. The parameter u indicates that the function ψ(t) was translated on the t axis (translation parameter) by a distance equivalent to u. The parameter s causes a scale change, increasing (if s > 1) or decreasing (if s < 1) the wavelet formed by the function. The wavelet is defined as a mother wavelet ψ(t) [equivalent to ψ1, 0(t)], with a family of scale and time daughter wavelets . Therefore, daughter wavelets constitute a family of curves with a shape identical to that of the mother wavelet, displaced in time and scaled in amplitude. In the time domain, the wavelet transform measures the correlation between the f(t) signal and the daughter wavelets.
The wavelet ψs, u(t) has the following basic properties:
The wavelet ψs, u(t) has to meet the admissibility condition for the transformation to be invertible (116).
The term is a normalization factor that ensures that the energy of ψs, u(t) is independent of s and u, such that:
The continuous wavelet transform (CWT) of signal f(t) is defined as:
The CWT coefficients Wψf(s, u) can be obtained by continuously varying the scale parameter s and the position parameter u. For real discrete signals f(n), as is the case for the fHR signal, Wψf(s, u) can be calculated according to
If s is a continuous variable then Wψf(s, u) is called the continuous wavelet transform. However, if s = aj and where the integers j and n control the wavelet dilation and translation respectively; a is a specified fixed dilation step parameter set at a value greater than 1, and u0 is the location parameter which must be greater than zero then Wψf(s, u) = Wψf(j, u) is called the discrete wavelet transform (119). A useful property of the wavelet transform is that it can be viewed as the application of a filter bank (each filter corresponds to one scale) (120). Some authors, such as, Zhao et al. (121) and Papadimitriou et al. (122) apply different scale values, but, in practice, s = 2j and u0 = 1 are the most popular scale in fHR analysis (123–125).
There are a vast number of different mother wavelets, each suitable for different applications. In particular, several wavelet families have been proposed for fHR analysis. From all 270 papers included in this review, 26.3% applied wavelet analysis. The Daubechies (36 papers), spline (11 papers), symlets (11 papers), and coiflet (8 papers) wavelet families were the most applied in fHR analysis (see Figure 1). The application of wavelet analysis in fHR has intensified in the last 10 years, Figure 6.
Figure 6

The wavelet families most used in fHR analysis, by year. The colors and symbols represent the wavelet families. The black circle, blue triangle, purple diamond plus, green square, and star red represented Daubechies family, spline family, symlet family, coiflet family, and other families, respectively.
4. Results
There is no doubt of the importance of non-linear measures in fetal monitoring, as they enrich the signal description by providing new indicators for classification and diagnostic purposes. Numerous studies have documented the changes in fHRV during gestation, and fetal growth is associated with a drop in fetal heart rate and increased variability. As non-linear measures started being used, authors started to link their association with different physiological regulatory systems.
The history of non-linear methods reported to fHR summarizes 30 years. However, in the last 15 years, there has been a notable increase in their application to study fHR dynamics (see Figure 7). The main research objectives covered by this systematic review were signal processing (60 papers), hypoxia (56 papers), maturation or gestational age (53 papers), IUGR (44 papers), and fetal well-being or fetal distress (26) (see Figure 7 and Table 2). Also, in Figure 7, the evolution of papers' of the five most cited research objectives is presented per year.
Figure 7

The five most cited research objectives of the papers that applied non-linear methods in fHR, by year of publishing. The colors and symbols represent the different research objectives. The blue circle, cyan square, star red, green triangle, and black diamond plus represent maturation, hypoxia, intrauterine growth restriction, fetal distress, and signal processing, respectively.
Table 2
| Non-linear analysis | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Entropy | Comp | Fractal | Wavelet | O | T | |||||||||
| Objectives | ApEn | SampEn | SE | MSE | O | LZ | O | FD | HE | DFA | O | |||
| Healthy | ||||||||||||||
| Maturation | 19 | 12 | 4 | 13 | 11 | 7 | 1 | 3 | 12 | 4 | 3 | 14 | 53 | |
| Activity/behavior | 10 | 5 | 1 | 2 | 3 | 1 | 3 | 1 | 1 | 3 | 14 | |||
| Gender | 10 | 8 | 2 | 2 | 1 | 1 | 1 | 2 | 11 | |||||
| Presentation | 3 | 2 | 1 | 1 | 3 | |||||||||
| RM | 1 | 1 | ||||||||||||
| Labor | 3 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 3 | 6 | ||||
| Cesarean | 1 | 1 | 1 | 1 | 1 | 3 | 4 | |||||||
| Preterm | 2 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 3 | |||||
| Twins | 1 | 1 | 1 | 1 | 2 | |||||||||
| Nuchal cord | 1 | 1 | ||||||||||||
| FCTE | 1 | 1 | ||||||||||||
| Self-organization | 1 | 1 | 1 | |||||||||||
| Ethnic origins | 1 | 1 | ||||||||||||
| Pathologies | ||||||||||||||
| Hypoxia | 29 | 28 | 7 | 6 | 11 | 14 | 5 | 11 | 6 | 6 | 7 | 23 | 27 | 56 |
| IUGR | 26 | 13 | 2 | 6 | 3 | 15 | 2 | 1 | 7 | 1 | 2 | 16 | 44 | |
| Fetal distress | 13 | 7 | 2 | 3 | 4 | 3 | 1 | 4 | 3 | 1 | 2 | 3 | 12 | 26 |
| SIDS | 1 | 1 | 1 | |||||||||||
| Intrauterine demise | 1 | 1 | ||||||||||||
| PPA | 1 | 1 | 1 | 1 | 1 | |||||||||
| Anencephalus | 1 | 1 | 1 | |||||||||||
| Maternal | ||||||||||||||
| MP | 5 | 1 | 1 | 1 | 1 | 2 | 1 | 2 | 9 | |||||
| Hypnosis | 1 | 1 | 1 | 1 | ||||||||||
| Steroid treatment | 1 | 1 | ||||||||||||
| Uterine contraction | 2 | 2 | 1 | 1 | 4 | 4 | ||||||||
| Signals | ||||||||||||||
| MFCC | 1 | 3 | 4 | 1 | 1 | 4 | 7 | |||||||
| BI | 1 | 1 | 1 | 1 | ||||||||||
| FCEC | 1 | 1 | 1 | |||||||||||
| Signal Processing | 3 | 7 | 1 | 4 | 2 | 2 | 45 | 28 | 60 | |||||
| Signal acquisition | 1 | 1 | 1 | |||||||||||
| fHR baseline | 1 | 4 | 4 | |||||||||||
| Others | ||||||||||||||
| Expert annotation | 3 | 4 | 1 | 1 | 3 | 4 | 2 | 3 | 4 | 6 | ||||
| Patterns | 5 | 3 | 1 | 1 | 1 | 3 | 9 | |||||||
| Fractal value | 1 | 1 | 1 | |||||||||||
| Total | 101 | 82 | 16 | 30 | 38 | 38 | 8 | 34 | 14 | 15 | 15 | 71 | 112 | |
Research objectives and non-linear methods of the papers selected.
ApEn, approximate entropy; BI, biometric identification; CD, correlation dimension; Comp, Compressor; DFA, detrended fluctuation analysis; FCEC, fetal cardio-electrohysterographic coupling; FCTE, fetal cardiac timing events; FD, fractal dimension; HE, Hurst exponent; IUGR, intrauterine growth restriction; LZ, Lempel-ziv; MFCC, maternal-fetal cardiac coupling; MSE, multiscale entropy; MP, maternal pathologies; O, others; RM, Respiratory movement; PPA, partial placental abruption; SampEn, sample entropy; SE, Shannon entropy; SIDS, sudden infant death syndrome; T, total.
Hypoxia can be caused by prolonged or profound asphyxia, an oxygen deficiency due to a pathological change in either fetal or maternal components of the placenta, when there is an exchange of carbon dioxide and oxygen by the fetus during labor. This state leads to an accumulation of carbon dioxide leading to fetal acidemia, resulting in a lower pH in the fetal blood vessels. Early detection of which babies are at risk of acidemia is crucial, as it decreases the chance of a post-diagnosis of cerebral palsy, neonatal encephalopathy, or even death (126). To relate fHR with umbilical artery pH is, therefore, of extreme importance. However, the proper definition of fetal acidemia is still not established as different authors consider different pH cutoffs. Moreover, some authors also include in the definition the value of the base excess or base deficit (127). Some authors defined as “at risk of acidemia” when pH < 7.20 (33, 47, 128–136) or pH < 7.15 (30, 121, 137–143); others define when pH < 7.1 (43, 126, 144–146) or even when pH < 7.05 (38, 44, 48, 78, 147–165). Some studies used clinical experts to identify episodes of hypoxia and asphyxia, such as, (54, 166, 167). Another challenge relate to this pathology is to collect enough data for a proper acidemia analysis since prevalence of an acidemic fetus ranges from 0.6 to 3.5% (168, 169). From the 56 papers that aim to analyze of perinatal hypoxia or asphyxia 40 papers applied entropies, 19 applied compression measures, 23 applied fractal measures, and 23 papers applied wavelets analysis.
The development of non-invasive ultrasound techniques allowed a better estimation of gestational age and, therefore, the definition of a crucial fetal outcome: small for gestational age (SGA), which corresponds to fetuses having a weight lower than the 10th percentile adjusted to gestational age. Nevertheless, healthy babies can also be considered SGA, so it is still a challenge to decide whether the small dimensions are due to physiological or pathological conditions (170). Related to SGA fetus, one of the most common pathologies is IUGR. IUGR is a metabolic dysfunction inhibiting the fetus from achieving its average size. With a prevalence of 5−8% in the general population, it can complicate 10–15% of all pregnancies (171). IUGR is the second cause of perinatal mortality, after prematurity (172), and is still an important challenge for diagnosis and management (173). From the 44 papers that aim to study IUGR, 32 papers applied entropies, 15 applied compression measures, 11 fractal and only 2 papers used wavelets.
The effect of an antepartum vs. intrapartum analysis on the complexity indices and the differences in the signal acquisition methods are important to correctly evaluate and assess fetus well-being (174, 175). Throughout pregnancy, the fetus interacts with its environment, as the mother sets the framework for the state and development of the fetus (176). In a study where the mother's breathing was controlled, Van Leeuwen et al. (176) found that the presence or absence of interaction between mother and fetus cardiac activity might be due to maternal respiration. Also, the fetal cardiac system seems to have the capability to adjust its activation rate when responding to external stimuli. Spyridou et al. (177) studied the effect of smoking in fHR and found differences with several linear and non-linear parameters (such as, mutual information, MSE, and compression). In particular, it was shown less complexity for fetus exposed, enhancing its danger. From the 26 papers that aim to study fetal well-being or fetal distress 17 papers applied entropies, 4 applied compression measures, 7 fractal, and only 3 papers used wavelets.
When assessing fHRV, it is essential to control any factor which might confound its interpretation. Some of the most studied factors are the baby's maturation reflected in gestational age, behavioral state, and maternal condition (178). From the 53 papers that aim to study maturation or gestational age 38 papers applied entropies, 7 applied compression measures, 18 fractal and only 3 papers used wavelets. First trimester observations during pregnancy have shown a low intraindividual variation of the fHR, compared to variation between different fetuses (179). Later in pregnancy, Arduini also found this high intraindividual consistency concerning fetal behavioral states' characteristics, particularly fHR, in 2 consecutive days (180). In fact, an association between individual differences in prenatal heart rate and HRV and postnatal neural development has been reported (181). Besides these factors, Gonçalves et al. (131) and Spyridou et al. (182) noted that gender also has an effect on fHR analysis and should be considered, while Tagliaferri et al. (183) found differences on both linear and non-linear indices between different ethnic groups. Gender was also shown to influence maternal heart rate (MHR) (52). Even when twins are considered, sex differences were found both by linear and non-linear indices (184). Fetal presentation at birth has also been studied (185, 186). Reports are stating that breech fetuses have worse neurological outcomes compared to cephalic presentation ones (187, 188). Furthermore, in a study by Choi and Hoh (189), non-linear dynamic indices were able to differentiate normal pregnancies from ones with partial placental abruption with high accuracy, while linear indices were not.
The evaluation of neonatal behavior has shown more success in predicting neurodevelopment disability than neurological examination (190). Therefore, the same approach was adopted for fetal well-being assessment. These fetal behavioral states were introduced back in 1982 in studies combining the assessment of fetal body and eye movements (191). They include calm or non-eye movement sleep state (1F), active or rapid eye movement sleep state (2F), calm wakefulness state (3F), and active wakefulness state (4F). The importance of these definitions in understanding fetal physiology, interpretation of fHR monitoring, and diagnosis of pathological conditions is described with more detail elsewhere (192). There are associations between fetal behavioral states and fHR patterns. 1F is related to a stable baseline with absent or sporadic and short-lasting accelerations; 2F is associated with a stable baseline and frequent accelerations, and it is the most frequent state. 3F is rare and is usually very short in time. It also has a stable baseline but with wide variability and no accelerations. 4F shows repetitive and long-lasting accelerations with eventual returns to the baseline (193).
This field's interest is not only focused on fHR tracings classification. Features like frequency and amplitude traditionally characterize physiological signals. However, these parameters do not provide us with an insight into the regulatory processes underlying the signal dynamics, thus requiring a further extraction of more appropriate features, which has become a difficult task. These difficulties lie in the lack of a priori information on which process belongs to each component (i.e., fetal, maternal, or environmental) and the lack of knowledge on how each component behave (194). Much effort has been put into the signal acquisition and processing models because the extracted features' usability highly relies on the preprocessing steps' quality, such as artifacts removal, interpolation method, segmentation, and detrending signal (30).
In 2013, an open challenge was created, the Physionet Challenge (195), in order to promote the development of advanced signal processing techniques. Many different approaches were suggested, such as wavelet de-denoising, subspace decomposition and reconstruction, adaptive filtering and averaging, matched filtering, and entropy. Most of them followed these four steps: signal processing, maternal heartbeat detection, maternal heartbeat cancelation, fetal heartbeat detection. More information can be found in Di Maria et al. (196). These non-linear methodologies have been studied and applied to retrieve signal with the best quality possible, dismissing as much noise as possible. The preprocessing is even more important when adopting low-cost systems for signal extraction, as is the case of the fetal phonocardiography, which has a poor signal-to-noise ratio (11). From the 60 papers that aim to study signal processing 7 papers applied entropies, 1 applied compression measures, 7 fractal, and 45 papers used wavelets.
Table 2 presents the number of articles that applied each non-linear method for each research objective. Entropy, compression, and fractal measures are most used in classification papers, mainly when applied to analyze the variability of fHR in hypoxia, IUGR, and fetal distress. However, these measures are still underused in studies whose research objective is signal processing. On the other hand, wavelet analysis is most used when the research objective is signal processing (43 papers) or hypoxia (25 papers).
5. Discussion
The number of articles probing the use of non-linear measures to assess the fHR signals analysis has been growing in the past decade. Non-linear analysis has been successfully applied in the study of fetal heart rate with several research objectives, such as fetal maturation or gestational age (197–199), fetal gender (182, 200), labor stages (201, 202), cesarean section (51, 203), preterm birth (80, 204), impact of nuchal cord on antenatal (205), fHR baseline (206), behavioral state (207, 208), IUGR (209–213), hypoxia (128, 137, 214, 215), fetal distress (216–218), maternal pathologies (219, 220), and signal processing (198, 221–224). Therefore, it is important that the scientific community is aware of the non-linear methods used depending on the research objective. Additionally, they are not yet used in clinical practice due to some critical concerns that need to be further discussed.
Systems, such as, Omniview SisPorto (225), OxSys (226), NST-Expert, which later became CAFE (227) already automatically deal with CTG assessment. All the fHR processing and analysis in these systems are based on morphological features defined by FIGO guidelines. In some, the CTG is complemented with the ST-analysis method. It has been shown that it slightly improves labor outcomes, but its use is not always possible since it requires an invasive measurement (228). However, none of these systems still integrates non-linear indices, so they can and should be optimized.
When analyzing fHR time series automated, there are two main aspects to contemplate: the signal properties and quality and the clinical characteristics that might influence the measures used. Accordingly, we found that the most studied research objectives in fHR are signal processing, hypoxia, and maturation. Furthermore, the results show that entropy is the most applied measure in fetal heart rate, followed by fractal analysis, wavelet analysis, and the least applied is compression. Although the application of entropy methods stands out, we can see that compression and wavelet analysis methods have been increasingly used in recent years. Also, highlighting the fact that entropy is the oldest method, and that is it has been extensively studied and refined when applied to much different time series (229). On the other hand, wavelets are widely used in signal processing (124, 222) dealing with the signal itself, handling problems such as noise (230) and frequency.
Routinely, the fetal heart rate monitors acquire the beat-to-beat intervals in milliseconds either from Doppler or electrocardiographic signals and then convert them to provide a sequence of instantaneous heart rates in beats per minute (bpm). However, when data is exported, it is sampled, implying an interpolation of signals (132). The sampling rate does not seem to affect many linear parameters, but differences were found when non-linear indices were considered (175). Caution must be taken when defining reference values for irregularity indices, such as entropy, as they depend on the sampling frequency, as shown in (175), where 2 vs. 4 Hz sampling was compared. It is most important not to compare computerized systems for heart rate frequency analysis that use different sampling rates (225, 231).
Several linear methods have been studied as a forecaster of fetal well-being by measuring the interaction between the fetal sympathetic and parasympathetic nervous systems and its effects on fetal cardiovascular activity (232). As the parasympathetic nervous system is more responsible for variations in short-term variability (STV), which usually assesses the beat-to-beat differences, it might be reduced in central nervous system hypoxia/ acidosis. If hypoxia is sustained and increases in severity, it leads to the loss of long-term variability (LTV) (233), resulting in a global decrease of sympathetic and parasympathetic activity. On the other hand, it has been shown that fetal hypoxia's early effects increased short and long-term variability (234). Notwithstanding, many studies verify the weakness of STV and LTV indices in identifying fetal pathologies (235). Furthermore, with fetus maturity throughout pregnancy, an increase in fetal autonomic nervous system activity and the sympathovagal balance is expected. Moreover, motor and neurological delay, as well as damage in specific brain areas with cognitive effects, also affect the STV (236). The IUGR showed a reduction in both components of the autonomic nervous system activity, which modulates heartbeat intervals receiving inputs from the heart, the lungs, and the blood vessels (204, 209, 237).
The indices presented in this review are closely related to fetal heart variability. For instance, in (199) the authors showed that the complexity indices correlate highly with abnormal STV. In (143) the authors also report correlations between the complexity indices ranging from 0.53 to 0.78. Therefore, many studies found a reduction of complexity in the fHR signal associated with hypoxia/ acidosis. However, these indices were not always able to identify fHR from IUGR fetuses (237). Contrastingly, the fractal indices are measures of long-range correlations and long-term memory of time series, therefore, applied mainly in maturation studies.
Furthermore, many of the fetal heart rate analysis methods rely upon stationarity properties like mean, variance, and correlation structure. However, it is known that these fHR properties vary in time through events like uterine contractions. One way to counter this is to select small temporal windows where this property holds. Usually, an interval of 10–20 min is considered the minimum time window to perform the analysis for tracing classification and clinical decision (231, 238). In addition, many of the described measures are parametric measures. The choice of the ideal parameter is far from established in most cases. This heterogeneity limits the possible comparison between the results of different studies. In fact, in various papers, the choice of parameters is neither discussed nor even fully described.
Factors like fetus maturation, behavioral states, and maternal conditions are critical for a good assessment of the fetus and fully understanding their influence in the fHRV is no easy task. Incorporating such variables in predictive models for fetal evaluation will elucidate the importance of individual fHRV and increase its accuracy (178). Maternal psychological conditions such as stress and anxiety influence fHR and maternal hormones transferred via placenta or changes in the oxygen and nutrition supply for the fetus (239, 240). As seen in some results, gender is also a factor that should be taken into consideration. Even when twins are considered, sex differences were found both by linear and non-linear indices (184). Although Park et al. (185) found no significant differences between fetuses with different fetal presentation using spectral and complexity measures such as Lempel-Ziv complexity, ApEn, SampEn, and CD. Gonçalves et al. (186) found differences not only using linear indices but also with non-linear and spectral ones. This example of contrasting results reflects the difficulty and complexity of the fetal assessment. In this case, and according to the authors, the discrepancy might have resulted from different inclusion criteria, conditions for fHR recording, the occurrence of maternal fasting, time interval between acquisition and delivery, and equipment used. Moreover, an interesting study comparing uterine contraction influence on fHRV features between acidemic and non-acidemic fetuses suggested that separating contractions from rest periods improves fHRV analysis in detecting asphyxia during labor (151).
Having as a premise that humans are a result of self-organization and adaptation process and that ontogenetic development reflects phylogenetic development and indices of developmental biology may be helpful in fetal maturation assessment. Many studies addressed here found HRV changes, such as variability increase and pattern formation (204). These universal developmental features deliver appropriate measures of fetal maturation. Therefore, it seems only natural that these self-organization and adaptation features might better understand and identify developmental disorders (241). In fact, attention-deficit hyperactivity disorders in teenage boys were associated with antenatal maternal anxiety (242), which might influence fetal humoral development and autonomic control reproduced in heart rate patterns. This phenomenon, resulting from adverse influences on the fetus explained by epigenetic mechanisms, is called “fetal programming.” Therefore, early identification of fetal developmental disorders is essential as they may not be wholly compensated for later postnatal therapies (243). Many different approaches to fHR processing and analysis have been studied. They range from simple feature extraction methods to more sophisticated classification programs and joining research centers from different countries for joint projects, as the Digi-Newb project (244). Usage of continuous non-invasive evaluation, such as the usage of wearables, have been discussed (27, 245) and will contribute to the patient's care improvement since it will improve data gathering, reducing costs of fetal monitoring. Insurgent approaches are opening new windows on the continuous monitoring of fetal development. A single index cannot retrieve all the information from pathophysiological processes in the fetus's development, so approaches considering both linear and non-linear measures, through multivariate analysis, can improve the assessment of both fetal and maternal well-being.
In (35, 246), time, spectral and complexity indices were used as parameters to discriminate fetuses who were or not in a distressed state. Ferrario et al. (247) conclude that compression quantifies the rate of new patterns arising as the signal evolves, whereas entropy quantifies the recurrence of repetitive patterns. This idea of complementary of different indices is also supported in other papers (130, 145, 167, 247). It seems only logical for such a complex/chaotic system to be evaluated using a multiparameteric approach through advanced classification techniques capable of discriminating fetuses in distress in non-linear regions of a multidimensional space (30). With this approach, Signorini (248) was able to classify IUGR fetuses with accuracy, sensitivity, and specificity above 90%.
Mapping from feature space captured from the fHR signal to the space of decision or diagnosis, many machine learning, and deep learning techniques has been applied. Some examples are: support vector machines (38, 150, 152, 249, 250), conventional methods like k-nearest neighbors (250, 251), a hybrid approach using grammatical evolution (146, 252), artificial neural networks (134), and random forests (49, 253, 254). Cömert and Kocamaz (166) introduced a novel software for comprehensive CTG signals analysis, named CTG Open Access Software (CTG-OAS). This software embeds machine learning tools, such as preprocessing, feature extraction, feature selection, and classification. Fergus et al. (51) demonstrated, using deep learning tools, that machine learning significantly improves the efficiency of detecting cesarean section and vaginal deliveries, compared with the usual visual assessment. In this paper, impressive results were achieved, with both sensitivity and specificity over 90%. One problem of comparing these classification approaches is the apriori definition of the classes. For example, as said before, the definition of acidemia based on the umbilical cord artery's pH varies greatly between studies. Karvelis et al. (255) proposed a classification approach based on weighted voting of clinical annotations. These weights are estimated by using a latent class model with three or four latent classes. Moreover, as these learning techniques depend on the signal and the linear and non-linear measures computed, all the previously referred concerns must be contemplated meticulously. Therefore, the machine and deep learning techniques are particularly resourceful when the measures are thoroughly probed and understood. In this systematic review were found several other articles with machine learning and deep learning techniques. However, the description of these techniques is not the focus of this paper. Future work that analyzes in detail the machine learning and deep learning techniques that apply measures based on fHR dynamics should be considered.
The non-linear methods described in this review are entropy (Shannon, approximate, sample, and multiscale), compression, fractal analysis (fractal dimension, Hurst exponent, detrended fluctuation analysis, and multifractal detrended fluctuation analysis), and wavelet analysis. Other non-linear methods were found in our review, such as Poincaré plot (217), symbolic dynamics (256), phase rectified signal average (210, 211, 257, 258), Lyapunov exponents (259), and recurrence plot analysis (137). In the recent years, Phase Rectified Signal Averaging and derived parameters have been largely applied in fHR analysis to face the problem of accelerations and deceleration which are characteristic of the fHR signal.
Due to the high heterogeneity of study designs, data acquisition methods, aims of the studies, signal processing techniques, and measures (and parameters) used, no meta-analysis was possible to be performed.
This systematic review confirmed the importance of non-linear fetal monitoring measures to analyze the fetus' well-being and pathologies' prediction. The methods probed successfully diagnose pathologies, and new techniques are being proposed and explored to improve that prediction. However, the contradictory results of some of the findings due to the characteristic of the signal, or the sensibility of the measures to some clinical factors, such as fetus sex and gestational age, revealed that the use of these findings in clinical practice is far from reality. These results inhibit the reach for a gold standard or the creation of a decision support system. This review determined the significance of creating several small meta-analyses that might focus on a specific research aim. Additionally, a sizeable multicentric study that can assess the multitude of perspectives involved in the fHR signal analysis is imperative.
6. Conclusions
Non-linear measures based on the concepts of chaos, fractality, and complexity gained space in the analysis of fetal heart rate. Good results were achieved in signal processing, in the analysis of fetal well-being, and in diagnosing and predicting pathologies. This systematic review of the non-linear methods (entropy, data compression, fractal analysis, and wavelet analysis) applied to fetal heart rate dynamics includes 270 papers. The application of non-linear methods in the fHR analysis is around 30 years old. However, its application has significantly increased in the last 15 years. This review's main contributions are a detailed description of the non-linear methods most applied in the fHR papers and a discussion of the research objectives. Signal processing, hypoxia, and maturation lead the research objectives of papers that use non-linear analysis in fHR. We found that entropy has been the most used method in classification analysis. Despite, in signal processing, the most used method is wavelet analysis. Machine learning and deep learning techniques should also be analyzed with results in the study of fHR dynamics using linear and non-linear measures. The multitude of conditioning involved in the analysis and classification of the fHR, from the signal characteristics to the effect of some clinical factors in the measures, limits the use of the non-linear measures in clinical practice and difficult the creation of a decision support system. Future studies should focus on a research question and perform a meta-analysis, probing the indices' performance.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Statements
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author contributions
JM-S, LA, CC-S, and AT conducted the preliminary literature review by establishing the search method and keywords. MR, JM-S, and AT determined the eligibility, summarized the findings from each study, and compiled them in tables. LC, CC-S, and TH analyzed the disagreements between reviewers. MR, JM-S, LC, AT, and TH writing and editing of the manuscript. CC-S, LA, AT, and TH supervision. All authors revised the paper critically for important intellectual content, made substantial contributions to the conception and design of the article, and agreed to the published version of the manuscript.
Acknowledgments
The authors acknowledge professor Luís Azevedo for helping to build the queries for the systematic review. MR acknowledges Fundação para a Ciência e a Tecnologia (FCT) under scholarship SFRH/BD/138302/2018. The authors also acknowledge FCT, within CINTESIS, R&D Unit (reference UIDB/4255/2020).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1.
Cousens S Blencowe H Stanton C Chou D Ahmed S Steinhardt L et al . National, regional, and worldwide estimates of stillbirth rates in 2009 with trends since 1995: a systematic analysis. Lancet. (2011) 377:1319–30. 10.1016/S0140-6736(10)62310-0
2.
Ayres-de Campos D Bernardes J Costa-Pereira A Pereira-Leite L . Inconsistencies in classification by experts of cardiotocograms and subsequent clinical decision. BJOG Int J Obstetr Gynaecol. (1999) 106:1307–10. 10.1111/j.1471-0528.1999.tb08187.x
3.
Bernardes J Ayres-de Campos D . The persistent challenge of foetal heart rate monitoring. Curr Opin Obstetr Gynecol. (2010) 22:104–9. 10.1097/GCO.0b013e328337233c
4.
Spencer J . Role of cardiotocography. Brit J Hospital Med. (1992) 48:115–8.
5.
Martinek R Kahankova R Jezewski J Jaros R Mohylova J Fajkus M et al . Comparative effectiveness of ICA and PCA in extraction of fetal ECG from abdominal signals: toward non-invasive fetal monitoring. Front Physiol. (2018) 9:648. 10.3389/fphys.2018.00648
6.
Sameni R Clifford GD . A review of fetal ECG signal processing; issues and promising directions. Open Pac Electrophysiol Therapy J. (2010) 3:4. 10.2174/1876536X01003010004
7.
Bartlett M Murray A Dunlop W . Is fetal heart rate monitoring sufficiently sensitive to detect changes during labour?J Biomed Eng. (1992) 14:431–4. 10.1016/0141-5425(92)90090-8
8.
Parer JT . Handbook of Fetal Heart Rate Monitoring. Philadelphia, PA: Saunders (1997).
9.
Kovács F Horváth C Balogh ÁT Hosszú G . Fetal phonocardiography-past and future possibilities. Comput Methods Prog Biomed. (2011) 104:19–25. 10.1016/j.cmpb.2010.10.006
10.
Adithya PC Sankar R Moreno WA Hart S . Trends in fetal monitoring through phonocardiography: challenges and future directions. Biomed Signal Process Control. (2017) 33:289–305. 10.1016/j.bspc.2016.11.007
11.
Chourasia VS Tiwari AK . Fetal heart rate variability analysis from phonocardiographic recordings. J Mech Med Biol. (2011) 11:1315–31. 10.1142/S0219519411004174
12.
Persico N Moratalla J Lombardi C Zidere V Allan L Nicolaides K . Fetal echocardiography at 11-13 weeks by transabdominal high-frequency ultrasound. Ultrasound Obstetr Gynecol. (2011) 37:296–301. 10.1002/uog.8934
13.
Zhang D Zhang Y Ren W Sun F Guo Y Sun W et al . Prenatal diagnosis of fetal interrupted aortic arch type A by two-dimensional echocardiography and four-dimensional echocardiography with B-flow imaging and spatiotemporal image correlation. Echocardiography. (2016) 33:90–8. 10.1111/echo.12996
14.
Quartero H Stinstra J Golbach E Meijboom E Peters M . Clinical implications of fetal magnetocardiography. Ultrasound Obstetr Gynecol. (2002) 20:142–53. 10.1046/j.1469-0705.2002.00754.x
15.
Grimm B Haueisen J Huotilainen M Lange S Leeuwen PV Menendez T et al . Recommended standards for fetal magnetocardiography. Pac Clin Electrophysiol. (2003) 26:2121–6. 10.1046/j.1460-9592.2003.00330.x
16.
Jaros R Martinek R Kahankova R . Non-adaptive methods for fetal ECG signal processing: a review and appraisal. Sensors. (2018) 18:3648. 10.3390/s18113648
17.
Hoyer D Zebrowski J Cysarz D Gonçalves H Pytlik A Amorim-Costa C et al . Monitoring fetal maturation-objectives, techniques and indices of autonomic function. Physiol Measure. (2017) 38:R61. 10.1088/1361-6579/aa5fca
18.
Steer PJ . Has electronic fetal heart rate monitoring made a difference? In: Seminars in Fetal and Neonatal Medicine. Philadelphia, PA: Elsevier (2008). p. 2–7. 10.1016/j.siny.2007.09.005
19.
Caughey AB Cahill AG Guise JM Rouse DJ of Obstetricians AC Gynecologists . Safe prevention of the primary cesarean delivery. Am J Obstetr Gynecol. (2014) 210:179–93. 10.1016/j.ajog.2014.01.026
20.
Bernardes J Costa-Pereira A Ayres-de Campos D Van Geijn H Pereira-Leite L . Evaluation of interobserver agreement of cardiotocograms. Int J Gynecol Obstetr. (1997) 57:33–7. 10.1016/S0020-7292(97)02846-4
21.
Donker DK van Geijn HP Hasman A . Interobserver variation in the assessment of fetal heart rate recordings. Eur J Obstetr Gynecol Reproduct Biol. (1993) 52:21–8. 10.1016/0028-2243(93)90220-7
22.
Huch A Huch R Rooth G . Guidelines for blood sampling and measurement of pH and blood gas values in obstetrics: based upon a workshop held in Zurich, Switzerland, March 19, 1993 by an Ad Hoc Committee. Eur J Obstetr Gynecol Reproduct Biol. (1994) 54:165–75. 10.1016/0028-2243(94)90277-1
23.
Ayres-de Campos D Spong CY Chandraharan E . FIGO consensus guidelines on intrapartum fetal monitoring: cardiotocography. Int J Gynecol Obstetr. (2015) 131:13–24. 10.1016/j.ijgo.2015.06.020
24.
Schiermeier S Pildner von Steinburg S Thieme A Reinhard J Daumer M Scholz M et al . Sensitivity and specificity of intrapartum computerised FIGO criteria for cardiotocography and fetal scalp pH during labour: multicentre, observational study. BJOG Int J Obstetr Gynaecol. (2008) 115:1557–63. 10.1111/j.1471-0528.2008.01857.x
25.
Plsek PE Greenhalgh T . The challenge of complexity in health care. BMJ. (2001) 323:625–8. 10.1136/bmj.323.7313.625
26.
Rotmensch S Liberati M Vishne T Celentano C Ben-Rafael Z Bellati U . The effect of betamethasone and dexamethasone on fetal heart rate patterns and biophysical activities, a prospective randomized trial. Acta Obstetr Gynecol Scand. (1999) 78:493–500. 10.1034/j.1600-0412.1999.780604.x
27.
Signorini MG Fanelli A Magenes G . Monitoring fetal heart rate during pregnancy: contributions from advanced signal processing and wearable technology. Comput Math Methods Med. (2014) 2014: 707581. 10.1155/2014/707581
28.
Nunes I Ayres-de Campos D Figueiredo C Bernardes J . An overview of central fetal monitoring systems in labour. J Perinatal Med. (2013) 41:93–9. 10.1515/jpm-2012-0067
29.
Wilson T Holt T Greenhalgh T . Complexity and clinical care. BMJ. (2001) 323:685–8. 10.1136/bmj.323.7314.685
30.
Chudáček V Spilka J Huptych M Georgoulas G Jankŭ P P Koucký M et al . Automatic classification of intrapartal fetal heart-rate recordings- can it compete with experts? In: International Conference on Information Technology in Bio Medical Informatics. Berlin: Springer (2010) p. 57–66. 10.1007/978-3-642-15020-3_5
31.
Schnettler WT Goldberger AL Ralston SJ Costa M . Complexity analysis of fetal heart rate preceding intrauterine demise. Eur J Obstetr Gynecol Reproduct Biol. (2016) 203:286–90. 10.1016/j.ejogrb.2016.06.025
32.
Chaffin DG Goldberg CC Reed KL . The dimension of chaos in the fetal heart rate. Am J Obstetr Gynecol. (1991) 165:1425–9. 10.1016/S0002-9378(12)90778-4
33.
Pincus SM Viscarello RR . Approximate entropy: a regularity measure for fetal heart rate analysis. Obstet Gynecol. (1992) 79:249–55.
34.
Datian Y Xuemei O . Application of wavelet analysis in detection of fetal ECG. In: Proceedings of 18th Annual International Conference of the IEEE Engineering in Medicine and Biology Society. Amsterdam: IEEE (1996). p. 1043–4.
35.
Signorini MG Ferrario M Pedrinazzi L Magenes G . Analysis of echographic and heart rate time and frequency domain parameters for the antepartum fetal surveillance. In: Computers in Cardiology. Lyon: IEEE (2005). p. 679–82. 10.1109/CIC.2005.1588193
36.
Ferrario M Signorini MG Magenes G . Comparison between fetal heart rate standard parameters and complexity indexes for the identification of severe intrauterine growth restriction. Methods Inform Med. (2007) 46:186–90. 10.1055/s-0038-1625404
37.
Santos CC Bernardes J Vitányi PM Antunes L . Clustering fetal heart rate tracings by compression. In: 19th IEEE Symposium on Computer-Based Medical Systems (CBMS'06). Salt Lake City, UT: IEEE (2006). p. 685–90.
38.
Barquero-Pérez Ó Santiago-Mozos R Lillo-Castellano JM Garcia-Viruete B Goya-Esteban R Caamano AJ et al . Fetal heart rate analysis for automatic detection of perinatal hypoxia using normalized compression distance and machine learning. Front Physiol. (2017) 8:113. 10.3389/fphys.2017.00113
39.
Liberati A Altman DG Tetzlaff J Mulrow C Gøtzsche PC Ioannidis JP et al . The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. (2009) 62:e1–34. 10.1016/j.jclinepi.2009.06.006
40.
Shannon CE . A mathematical theory of communication. Bell Syst Tech J. (1948) 27:379–423. 10.1002/j.1538-7305.1948.tb01338.x
41.
Hoyer D Nowack S Bauer S Tetschke F Ludwig S Moraru L et al . Fetal development assessed by heart rate patterns-time scales of complex autonomic control. Comput Biol Med. (2012) 42:335–41. 10.1016/j.compbiomed.2011.05.003
42.
Frank B Pompe B Schneider U Hoyer D . Permutation entropy improves fetal behavioural state classification based on heart rate analysis from biomagnetic recordings in near term fetuses. Med Biol Eng Comput. (2006) 44:179. 10.1007/s11517-005-0015-z
43.
Fulcher B Georgieva A Redman C . Highly comparative fetal heart rate analysis. In: Annual International Conference of the IEEE Engineering in Medicine and Biology-Proceedings. San Diego, CA (2012). 3135–8. 10.1109/EMBC.2012.6346629
44.
Barquero-Pérez Ó Goya-Esteban R Caamano A Martin-Caballero C Rojo-Álvarez JL . Fetal heart rate complexity measures to detect hypoxia. In: 2015 Computing in Cardiology Conference (CinC). IEEE (2015). p. 133–6. 10.1109/CIC.2015.7408604
45.
Schneider U Frank B Fiedler A Kaehler C Hoyer D Liehr M et al . Human fetal heart rate variability-characteristics of autonomic regulation in the third trimester of gestation. J Perinatal Med. (2008) 36:433–41. 10.1515/JPM.2008.059
46.
Khandoker AH Marzbanrad F Voss A Schulz S Kimura Y Endo M et al . Analysis of maternal-fetal heart rate coupling directions with partial directed coherence. Biomed Signal Process Control. (2016) 30:25–30. 10.1016/j.bspc.2016.06.010
47.
Manis G Sassi R . Relation between fetal HRV and value of umbilical cord artery pH in labor, a study with entropy measures. In: 2017 IEEE 30th International Symposium on Computer-Based Medical Systems (CBMS). IEEE (2017). p. 272–7. 10.1109/CBMS.2017.139
48.
Granero-Belinchon C Roux SG Abry P Doret M Garnier NB . Information theory to probe intrapartum fetal heart rate dynamics. Entropy. (2017) 19:640. 10.3390/e19120640
49.
Tetschke F Schneider U Schleussner E Witte OW Hoyer D . Assessment of fetal maturation age by heart rate variability measures using random forest methodology. Comput Biol Med. (2016) 70:157–62. 10.1016/j.compbiomed.2016.01.020
50.
Schneider U Fiedler A Schröder B Jaekel S Stacke A Hoyer D et al . The effect of antenatal steroid treatment on fetal autonomic heart rate regulation revealed by fetal magnetocardiography (fMCG). Early Hum Dev. (2010) 86:319–25. 10.1016/j.earlhumdev.2010.05.018
51.
Fergus P Hussain A Al-Jumeily D Huang DS Bouguila N . Classification of caesarean section and normal vaginal deliveries using foetal heart rate signals and advanced machine learning algorithms. Biomed Eng Online. (2017) 16:89. 10.1186/s12938-017-0378-z
52.
Gonçalves H Fernandes D Pinto P Ayres-de Campos D Bernardes J . Simultaneous monitoring of maternal and fetal heart rate variability during labor in relation with fetal gender. Dev Psychobiol. (2017) 59:832–39. 10.1002/dev.21554
53.
Khandoker A Karmakar C Kimura Y Endo M Oshio S Palaniswami M . Tone entropy analysis of foetal heart rate variability. Entropy. (2015) 17:1042–53. 10.3390/e17031042
54.
Hopkins P Outram N Lofgren N Ifeachor EC Rosén KG . A comparative study of fetal heart rate variability analysis techniques. In: 2006 International Conference of the IEEE Engineering in Medicine and Biology Society. IEEE (2006). p. 1784–7. 10.1109/IEMBS.2006.260258
55.
Pincus SM Gladstone IM Ehrenkranz RA . A regularity statistic for medical data analysis. J Clin Monitor. (1991) 7:335–45. 10.1007/BF01619355
56.
Buchman TG . The community of the self. Nature. (2002) 420:246–51. 10.1038/nature01260
57.
Kennel MB Brown R Abarbanel HDI . Determining embedding dimension for phase-space reconstruction using a geometrical construction. Phys RevA. (1992) 45:3403. 10.1103/PhysRevA.45.3403
58.
Cao L . Practical method for determining the minimum embedding dimension of a scalar time series. Phys D Nonlinear Phenomena. (1997) 110:43–50. 10.1016/S0167-2789(97)00118-8
59.
Fraser AM Swinney HL . Independent coordinates for strange attractors from mutual information. Phys Rev A. (1986) 33:1134. 10.1103/PhysRevA.33.1134
60.
Pincus SM . Approximate entropy as a measure of system complexity. Proc Natl Acad Sci USA. (1991) 88:2297–301. 10.1073/pnas.88.6.2297
61.
Pincus SM Goldberger AL . Physiological time-series analysis: what does regularity quantify?Am J Physiol. (1994) 266:H1643. 10.1152/ajpheart.1994.266.4.H1643
62.
Marques de Sá JP . Characterization of fetal heart rate using approximate entropy. In: Computers in Cardiology. Lyon: IEEE (2005). p. 671–3. 10.1109/CIC.2005.1588190
63.
Magalhaes F Marques de Sá J Bernardes J Ayres-de Campos D . Characterization of fetal heart rate irregularity using approximate entropy and wavelet filtering. In: 2006 Computers in Cardiology. Valencia: IEEE (2006). p. 933–6.
64.
Lu S Chen X Kanters JK Solomon IC Chon KH . Automatic selection of the threshold value for approximate entropy. IEEE Trans Biomed Eng. (2008) 55:1966–72. 10.1109/TBME.2008.919870
65.
Richman JS Moorman JR . Physiological time-series analysis using approximate entropy and sample entropy. Am J Physiol Heart Circ Physiol. (2000) 278:H2039–49. 10.1152/ajpheart.2000.278.6.H2039
66.
Costa M Goldberger A Peng CK . Multiscale entropy to distinguish physiologic and synthetic RR time series. In: Computers in Cardiology. Memphis, TN: IEEE (2002). p. 137–40.
67.
Costa M Goldberger AL Peng CK . Multiscale entropy analysis of biological signals. Phys Rev E. (2005) 71:021906. 10.1103/PhysRevE.71.021906
68.
Valencia JF Porta A Vallverdu M Claria F Baranowski R Orlowska-Baranowska E et al . Refined multiscale entropy: application to 24-h holter recordings of heart period variability in healthy and aortic stenosis subjects. IEEE Trans Biomed Eng. (2009) 56:2202–13. 10.1109/TBME.2009.2021986
69.
Nikulin VV Brismar T . Comment on “Multiscale entropy analysis of complex physiologic time series”. Phys Rev Lett. (2004) 92:089803. 10.1103/PhysRevLett.92.089803
70.
Lake DE Moorman JR . Accurate estimation of entropy in very short physiological time series: the problem of atrial fibrillation detection in implanted ventricular devices. Am J Physiol Heart Circ Physiol. (2011) 300:H319–25. 10.1152/ajpheart.00561.2010
71.
Gierałtowski J Hoyer D Tetschke F Nowack S Schneider U Zebrowski J . Development of multiscale complexity and multifractality of fetal heart rate variability. Auton Neurosci. (2013) 178:29–36. 10.1016/j.autneu.2013.01.009
72.
Kolmogorov AN . A new metric invariant of transient dynamical systems and automorphisms in Lebesgue spaces. In: Doklady Akademii Nauk. Moscow: Russian Academy of Sciences (1958). p. 861–4.
73.
Solomonoff RJ . A formal theory of inductive inference. Part II. Inform Control. (1964) 7:224–54. 10.1016/S0019-9958(64)90131-7
74.
Kolmogorov AN . Three approaches to the definition of the concept “quantity of information”. Problemy Peredachi Informatsii. (1965) 1:3–11.
75.
Chaitin GJ . On the length of programs for computing finite binary sequences: statistical considerations. J ACM. (1969) 16:145–59. 10.1145/321495.321506
76.
Lempel A Ziv J . On the complexity of finite sequences. IEEE Trans Inform Theory. (1976) 22:75–81. 10.1109/TIT.1976.1055501
77.
Seward J . bzip2. (1996). Available online at: http://wwwmuraroademoncouk/
78.
Spilka J Chudáček V Koucký M Lhotská L Huptych M Jankŭ P et al . Using nonlinear features for fetal heart rate classification. Biomed Signal Process Control. (2012) 7:350–7. 10.1016/j.bspc.2011.06.008
79.
Yang ACC Hseu SS Yien HW Goldberger AL Peng CK . Linguistic analysis of the human heartbeat using frequency and rank order statistics. Phys Rev Lett. (2003) 90:108103. 10.1103/PhysRevLett.90.108103
80.
Ferrario M Signorini MG Magenes G . Complexity analysis of the fetal heart rate variability: early identification of severe intrauterine growth-restricted fetuses. Med Biol Eng Comput. (2009) 47:911–9. 10.1007/s11517-009-0502-8
81.
Magenes G Bellazzi R Fanelli A Signorini MG . Multivariate analysis based on linear and non-linear FHR parameters for the identification of IUGR fetuses. In: 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society. Chicago, IL: IEEE (2014). p. 1868–71. 10.1109/EMBC.2014.6943974
82.
Cilibrasi R Vitányi PM . Clustering by compression. IEEE Trans Inform Theory. (2005) 51:1523–45. 10.1109/TIT.2005.844059
83.
Cilibrasi R Vitányi P Wolf Rd . Algorithmic clustering of music based on string compression. Comput Music J. (2004). 28:49–67. 10.1162/0148926042728449
84.
Wehner S . Analyzing worms and network traffic using compression. J Comput Security. (2007) 15:303–20. 10.3233/JCS-2007-15301
85.
Ferrario M Signorini MG Cerutti S . Complexity analysis of 24 hours heart rate variability time series. In: The 26th Annual International Conference of the IEEE Engineering in Medicine and Biology Society. San Francisco, CA: IEEE (2004). p. 3956–9.
86.
Radhakrishnan N Gangadhar B . Estimating regularity in epileptic seizure time-series data. IEEE Eng Med Biol Mag. (1998) 17:89–94. 10.1109/51.677174
87.
Zhang XS Zhu YS Thakor NV Wang ZZ . Detecting ventricular tachycardia and fibrillation by complexity measure. IEEE Trans Biomed Eng. (1999) 46:548–55. 10.1109/10.759055
88.
Zhang XS Roy RJ Jensen EW . EEG complexity as a measure of depth of anesthesia for patients. IEEE Trans Biomed Eng. (2001) 48:1424–33. 10.1109/10.966601
89.
Szczepański J Amigó JM Wajnryb E Sanchez-Vives M . Application of Lempel-Ziv complexity to the analysis of neural discharges. Network Comput Neural Syst. (2003) 14:335–50. 10.1088/0954-898X_14_2_309
90.
Castro L Teixeira A Brás S Santos M Costa-Santos C . Towards FHR biometric identification: a comparison between compression and entropy based approaches. In: 2018 IEEE 31st International Symposium on Computer-Based Medical Systems (CBMS). Karlstad: IEEE (2018). p. 440–1. 10.1109/CBMS.2018.00085
91.
Orlov YL Potapov VN . Complexity: an internet resource for analysis of DNA sequence complexity. Nucleic Acids Res. (2004) 32:W628–33. 10.1093/nar/gkh466
92.
Katz MJ . Fractals and the analysis of waveforms. Comput Biol Med. (1988) 18:145–56. 10.1016/0010-4825(88)90041-8
93.
Higuchi T . Approach to an irregular time series on the basis of the fractal theory. Phys D Nonlinear Phenomena. (1988) 31:277–83. 10.1016/0167-2789(88)90081-4
94.
Higuchi T . Relationship between the fractal dimension and the power law index for a time series: a numerical investigation. Phys D Nonlinear Phenomena. (1990) 46:254–64. 10.1016/0167-2789(90)90039-R
95.
Barabási AL . Fractal Concepts in Surface Growth. Cambridge, UK: Cambridge University Press (1995).
96.
Henriques T Ribeiro M Teixeira A Castro L Antunes L Costa-Santos C . Nonlinear methods most applied to heart-rate time series: a review. Entropy. (2020) 22:309. 10.3390/e22030309
97.
Hurst HE . Long-term storage capacity of reservoirs. Trans Am Soc Eng. (1951) 116:770–808. 10.1061/TACEAT.0006518
98.
Mandelbrot BB Wallis JR . Noah, Joseph, and operational hydrology. Water Resour Res. (1968) 4:909–18. 10.1029/WR004i005p00909
99.
Mandelbrot BB Wallis JR . Robustness of the rescaled range R/S in the measurement of noncyclic long run statistical dependence. Water Resour Res. (1969) 5:967–88. 10.1029/WR005i005p00967
100.
Moreira J da Silva JKL Kamphorst SO . On the fractal dimension of self-affine profiles. J Phys A Math Gen. (1994) 27:8079. 10.1088/0305-4470/27/24/018
101.
Peng CK Buldyrev SV Havlin S Simons M Stanley HE Goldberger AL . Mosaic organization of DNA nucleotides. Phys Rev E. (1994) 49:1685. 10.1103/PhysRevE.49.1685
102.
Geweke J Porter-Hudak S . The estimation and application of long memory time series models. J Time Ser Anal. (1983) 4:221–38. 10.1111/j.1467-9892.1983.tb00371.x
103.
Beran J . Statistics for Long-Memory Processes. vol. 61. Boca Raton, FL: CRC Press (1994).
104.
Robinson PM et al . Gaussian semiparametric estimation of long range dependence. Ann Stat. (1995) 23:1630–61. 10.1214/aos/1176324317
105.
Hansen A Engøy T Måløy KJ . Measuring Hurst exponents with the first return method. Fractals. (1994) 2:527–33. 10.1142/S0218348X94000740
106.
Abry P Gonçalvés P Flandrin P . Wavelets, spectrum analysis and 1/f processes. In: AntoniadisAOppenheimG editors, Wavelets and Statistics Lecture Notes in Statistics, vol 103. New York, NY: Springer (1995). p. 15–29. 10.1007/978-1-4612-2544-7_2
107.
Schepers HE Van Beek JH Bassingthwaighte JB . Four methods to estimate the fractal dimension from self-affine signals (medical application). In: Antoniadis A, Oppenheim G, editors. IEEE Engineering in Medicine and Biology Magazine. New York, NY: Springer (1992). 11:57–64. 10.1109/51.139038
108.
Peng CK Havlin S Hausdorff JM Mietus JE Stanley HE Goldberger AL . Fractal mechanisms and heart rate dynamics: long-range correlations and their breakdown with disease. J Electrocardiol. (1995) 28:59–65. 10.1016/S0022-0736(95)80017-4
109.
Kantelhardt JW Koscielny-Bunde E Rego HHA Havlin S Bunde A . Detecting long-range correlations with detrended fluctuation analysis. Phys A Stat Mech Appl. (2001) 295:441–54. 10.1016/S0378-4371(01)00144-3
110.
Kantelhardt JW Zschiegner SA Koscielny-Bunde E Havlin S Bunde A Stanley HE . Multifractal detrended fluctuation analysis of nonstationary time series. Phys A Stat Mech Appl. (2002) 316:87–114. 10.1016/S0378-4371(02)01383-3
111.
Ossadnik S Buldyrev SV Goldberger AL Havlin S Mantegna RN Peng CK et al . Correlation approach to identify coding regions in DNA sequences. Biophys J. (1994) 67:64–70. 10.1016/S0006-3495(94)80455-2
112.
Bunde A Havlin S Kantelhardt JW Penzel T Peter JH Voigt K . Correlated and uncorrelated regions in heart-rate fluctuations during sleep. Phys Rev Lett. (2000) 85:3736. 10.1103/PhysRevLett.85.3736
113.
Gierałtowski J Zebrowski J Baranowski R . Multiscale multifractal analysis of heart rate variability recordings with a large number of occurrences of arrhythmia. Phys Rev E. (2012) 85:021915. 10.1103/PhysRevE.85.021915
114.
Haar A . Zur Theorie der Orthogonalen Funktionensysteme. Georg-August-Universitat, Gottingen (1909). 10.1007/BF01456326
115.
Mallat SG . A theory for multiresolution signal decomposition: the wavelet representation. IEEE Trans Pattern Anal Mach Intell. (1989) 11:674–93. 10.1109/34.192463
116.
Daubechies I . The wavelet transform, time-frequency localization and signal analysis. IEEE Trans Inform Theory. (1990) 36:961–1005. 10.1109/18.57199
117.
Daubechies I Bates BJ . Ten Lectures on Wavelets. Philadelphia, PA: Acoustical Society of America (1993). 10.1137/1.9781611970104
118.
Mallat S . A Wavelet Tour of Signal Processing. Los Angeles, CA: Elsevier (1999). 10.1016/B978-012466606-1/50008-8
119.
Desai K Jadhav SD Sankhe MS . A comparison and quantification of fetal heart rate variability using Doppler ultrasound and direct electrocardiography acquisition techniques. In: 2013 International Conference on Advances in Technology and Engineering (ICATE). Mumbai: IEEE (2013). p. 1–8. 10.1109/ICAdTE.2013.6524738
120.
Gilles J . Empirical wavelet transform. IEEE Trans Signal Process. (2013) 61:3999–4010. 10.1109/TSP.2013.2265222
121.
Zhao Z Deng Y Zhang Y Zhang Y Zhang X Shao L . DeepFHR: intelligent prediction of fetal Acidemia using fetal heart rate signals based on convolutional neural network. BMC Med Inform Decis Mak. (2019) 19:286. 10.1186/s12911-019-1007-5
122.
Papadimitriou S Papadopoulos V Gatzounas D Tzigounis V Bezerianos A . The performance and reliability of wavelet denoising for Doppler ultrasound fetal heart rate signal preprocessing. Stud Health Technol Inform. (1997) 43:561–5.
123.
Barnova K Martinek R Jaros R Kahankova R . Hybrid methods based on empirical mode decomposition for non-invasive fetal heart rate monitoring. IEEE Access. (2020) 8:51200–18. 10.1109/ACCESS.2020.2980254
124.
Meddour C Kedir-Talha M . New method exploiting a hybrid techniques for fetal cardiac signal extraction. Biomed Eng Appl Basis Commun. (2019) 31:1950027. 10.4015/S1016237219500273
125.
Jaros R Martinek R Kahankova R Koziorek J . Novel hybrid extraction systems for fetal heart rate variability monitoring based on non-invasive fetal electrocardiogram. IEEE Access. (2019) 7:131758–131784. 10.1109/ACCESS.2019.2933717
126.
Georgoulas G Stylios C Groumpos P . Feature extraction and classification of fetal heart rate using wavelet analysis and support vector machines. Int J Artif Intell Tools. (2006) 15:411–32. 10.1142/S0218213006002746
127.
Elliott C Warrick PA Graham E Hamilton EF . Graded classification of fetal heart rate tracings: association with neonatal metabolic acidosis and neurologic morbidity. Am J Obstetr Gynecol. (2010) 202:258. 10.1016/j.ajog.2009.06.026
128.
Cömert Z Şengür A Budak Ü Kocamaz AF . Prediction of intrapartum fetal hypoxia considering feature selection algorithms and machine learning models. Health Inform Sci Syst. (2019) 7:1–9. 10.1007/s13755-019-0079-z
129.
Cömert Z Kocamaz AF . Open-access software for analysis of fetal heart rate signals. Biomed Signal Process Control. (2018) 45:98–108. 10.1016/j.bspc.2018.05.016
130.
Monteiro-Santos J Gonçalves H Bernardes J Antunes L Nozari M Costa-Santos C . Entropy and compression capture different complexity features: the case of fetal heart rate. Entropy. (2017) 19:688. 10.3390/e19120688
131.
Gonçalves H Ayres-de Campos D Bernardes J . The effect of gender, gestational age and behavioral states on fetal heart rate variability. In: 2014 8th Conference of the European Study Group on Cardiovascular Oscillations (ESGCO). IEEE (2014). p. 19–20. 10.1109/ESGCO.2014.6847498
132.
Gonçalves H Costa A Ayres-de Campos D Costa-Santos C Rocha AP Bernardes J . Comparison of real beat-to-beat signals with commercially available 4 Hz sampling on the evaluation of foetal heart rate variability. Med Biol Eng Comput. (2013) 51:665–76. 10.1007/s11517-013-1036-7
133.
Bernardes J Gonçalves H Ayres-de Campos D Rocha AP . Sex differences in linear and complex fetal heart rate dynamics of normal and acidemic fetuses in the minutes preceding delivery. J Perinatal Med. (2009) 37:168–76. 10.1515/JPM.2009.024
134.
Salamalekis E Thomopoulos P Giannaris D Salloum I Vasios G Prentza A et al . Computerised intrapartum diagnosis of fetal hypoxia based on fetal heart rate monitoring and fetal pulse oximetry recordings utilising wavelet analysis and neural networks. BJOG Int J Obstetr Gynaecol. (2002) 109:1137–42. 10.1111/j.1471-0528.2002.01388.x
135.
Vasios G Prentza A Blana D Salamalekis E Thomopoulos P Giannaris D et al . Classification of fetal heart rate tracings based on wavelet-transformand self-organizing-map neural networks. In: 2001 Conference Proceedings of the 23rd Annual International Conference of the IEEE Engineering in Medicine and Biology Society. Istanbul: IEEE (2001). p. 1633–6.
136.
Kimura Y Okamura K Watanabe T Yaegashi N Uehara S Yajima A . Time-frequency analysis of fetal heartbeat fluctuation using wavelet transform. Am J Physiol Heart Circ Physiol. (1998) 275:H1993–9. 10.1152/ajpheart.1998.275.6.H1993
137.
Zhao Z Zhang Y Comert Z Deng Y . Computer-aided diagnosis system of fetal hypoxia incorporating recurrence plot with convolutional neural network. Front Physiol. (2019) 10:255. 10.3389/fphys.2019.00255
138.
Zhao Z Zhang Y Deng Y . A comprehensive feature analysis of the fetal heart rate signal for the intelligent assessment of fetal state. J Clin Med. (2018) 7:223. 10.3390/jcm7080223
139.
Cömert Z Kocamaz AF Subha V . Prognostic model based on image-based time-frequency features and genetic algorithm for fetal hypoxia assessment. Comput Biol Med. (2018) 99:85–97. 10.1016/j.compbiomed.2018.06.003
140.
Arican M Cömer Z Kocamaz AF Polat K . Analysis of fetal heart rate signal based on neighborhood-based variance compression method. In: 2018 International Conference on Artificial Intelligence and Data Processing (IDAP). Malatya: IEEE (2018). p. 1–6. 10.1109/IDAP.2018.8620898
141.
Gonçalves H Pinto P Silva M Ayres-de Campos D Bernardes J . Toward the improvement in fetal monitoring during labor with the inclusion of maternal heart rate analysis. Med Biol Eng Comput. (2016) 54:691–9. 10.1007/s11517-015-1359-7
142.
Pasarica A Rotariu C Bozomitu RG Eva OD . Dynamic of couplings between fetal heart rate and uterine contractions. In: 2015 International Symposium on Signals, Circuits and Systems (ISSCS). Iasi: IEEE (2015). p. 1–4. 10.1109/ISSCS.2015.7203968
143.
Chudáček V Spilka J Jankŭ P Koucký M Lhotská L Huptych M . Automatic evaluation of intrapartum fetal heart rate recordings: a comprehensive analysis of useful features. Physiol Measure. (2011) 32:1347. 10.1088/0967-3334/32/8/022
144.
Gonçalves H Rocha AP Ayres-de Campos D Bernardes J . Frequency domain and entropy analysis of fetal heart rate: appealing tools for fetal surveillance and pharmacodynamic assessment of drugs. Cardiovasc Haematol Disord Drug Targets. (2008) 8:91–8. 10.2174/187152908784533720
145.
Henriques T Gonçalves H Antunes L Matias M Bernardes J Costa-Santos C . Entropy and compression: two measures of complexity. J Eval Clin Pract. (2013) 19:1101–6. 10.1111/jep.12068
146.
Gavrilis D Tsoulos I . Classification of fetal heart rate using grammatical evolution. In: IEEE Workshop on Signal Processing Systems Design and Implementation. (2005). IEEE (2005). p. 425–9.
147.
Fuentealba P Illanes A Ortmeier F . Cardiotocographic signal feature extraction through ceemdan and time-varying autoregressive spectral-based analysis for fetal welfare assessment. IEEE Access. (2019) 7:159754–72. 10.1109/ACCESS.2019.2950798
148.
Granero-Belinchon C Roux SG Garnier NB Abry P Doret M . Mutual information for intrapartum fetal heart rate analysis. In: 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC). Jeju: IEEE (2017). p. 2014–7. 10.1109/EMBC.2017.8037247
149.
Georgoulas G Karvelis P Spilka J Chudáček V Stylios CD Lhotska L . Investigating pH based evaluation of fetal heart rate (FHR) recordings. Health Technol. (2017) 7:241–54. 10.1007/s12553-017-0201-7
150.
Stylios CD Georgoulas G Karvelis P Spilka J Chudáček V Lhotska L . Least squares support vector machines for FHR classification and assessing the pH based categorization. In: XIV Mediterranean Conference on Medical and Biological Engineering and Computing. Paphos: Springer (2016). p. 1211–5. 10.1007/978-3-319-32703-7_234
151.
Warmerdam G Vullings R Van Laar JO Bergmans J Schmitt L Oei S et al . Using uterine activity to improve fetal heart rate variability analysis for detection of asphyxia during labor. Physiol Measure. (2016) 37:387. 10.1088/0967-3334/37/3/387
152.
Spilka J Frecon J Leonarduzzi R Pustelnik N Abry P Doret M . Intrapartum fetal heart rate classification from trajectory in sparse SVM feature space. In: 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC). Milan: IEEE (2015). p. 2335–8. 10.1109/EMBC.2015.7318861
153.
Spilka J Abry P Goncalves P Doret M . Impacts of first and second labour stages on Hurst parameter based intrapartum fetal heart rate analysis. In: Computing in Cardiology. Cambridge, MA: IEEE (2014). p. 777–780.
154.
Doret M Spilka J Chudáček V Gonçalves P Abry P . Fractal analysis and Hurst parameter for intrapartum fetal heart rate variability analysis: a versatile alternative to frequency bands and LF/HF ratio. PLoS ONE. (2015) 10:e0136661. 10.1371/journal.pone.0136661
155.
Leonarduzzi R Spilka J Wendt H Jaffard S Torres ME Abry P et al . p-leader based classification of first stage intrapartum fetal HRV. In: VI Latin American Congress on Biomedical Engineering CLAIB. Paraná: Springer (2015). p. 504–7. 10.1007/978-3-319-13117-7_129
156.
Chudáček V Andén J Mallat S Abry P Doret M . Scattering transform for intrapartum fetal heart rate variability fractal analysis: a case-control study. IEEE Trans Biomed Eng. (2013) 61:1100–8. 10.1109/TBME.2013.2294324
157.
Abry P Roux SG Chudáček V Borgnat P Gonçalves P Doret M . Hurst exponent and intrapartum fetal heart rate: impact of decelerations. In: Proceedings of the 26th IEEE International Symposium on Computer-Based Medical Systems.Porto: IEEE (2013) p. 131–6. 10.1109/CBMS.2013.6627777
158.
Spilka J Roux SG Garnier NB Abry P Gonçalves P Doret M . Nearestneighbor based wavelet entropy rate measures for intrapartum fetal heart rate variability. In: 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society. Chicago, IL: IEEE (2014). p. 2813–6. 10.1109/EMBC.2014.6944208
159.
Costa MD Schnettler WT Amorim-Costa C Bernardes J Costa A Goldberger AL et al . Complexity-loss in fetal heart rate dynamics during labor as a potential biomarker of acidemia. Early Hum Dev. (2014) 90:67–71. 10.1016/j.earlhumdev.2013.10.002
160.
Santiago-Mozos R Garcia-Vizuete B Lillo-Castellano JM Rojo-Alvarez JL Martin-Caballero C . On the early detection of perinatal hypoxia with information-theory based methods. In: Computing in Cardiology. Zaragoza: IEEE (2013). p. 425–8.
161.
Doret M Helgason H Abry P Goncalves P Gharib C Gaucherand P . Multifractal analysis of fetal heart rate variability in fetuses with and without severe acidosis during labor. Am J Perinatol. (2011) 28:259–66. 10.1055/s-0030-1268713
162.
Abry P Helgason H Gonçalves P Pereira E Gaucherand P Doret M . Multifractal analysis of ECG for intrapartum diagnosis of fetal asphyxia. In: 2010 IEEE International Conference on Acoustics, Speech and Signal Processing. Dallas, TX: IEEE (2010). p. 566–9. 10.1109/ICASSP.2010.5495583
163.
Spilka J Chudáček V Koucký M Lhotská L . Assessment of non- linear features for intrapartal fetal heart rate classification. In: 2009 9th International Conference on Information Technology and Applications in Biomedicine. Larnaka: IEEE (2009). p. 1–4. 10.1109/ITAB.2009.5394442
164.
Gonçalves H Rocha AP Ayres-de Campos D Bernardes J . Linear and nonlinear fetal heart rate analysis of normal and acidemic fetuses in the minutes preceding delivery. Med Biol Eng Comput. (2006) 44:847. 10.1007/s11517-006-0105-6
165.
Salamalekis E Siristatidis C Vasios G Saloum J Giannaris D Chrelias C et al . Fetal pulse oximetry and wavelet analysis of the fetal heart rate in the evaluation of abnormal cardiotocography tracings. J Obstetr Gynaecol Res. (2006) 32:135–139. 10.1111/j.1447-0756.2006.00377.x
166.
Cömert Z Kocamaz AF . A novel software for comprehensive analysis of cardiotocography signals “CTG-OAS”. In: 2017 International Artificial Intelligence and Data Processing Symposium (IDAP). Malatya: IEEE (2017). p. 1–6. 10.1109/IDAP.2017.8090210
167.
Chudáček V Spilka J Lhotská L Jankŭ P Koucký M Huptych M et al . Assessment of features for automatic CTG analysis based on expert annotation. In: 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society. Boston, MA: IEEE (2011). p. 6051–4.
168.
d'Aloja E Müller M Paribello F Demontis R Faa A . Neonatal asphyxia and forensic medicine. J Maternal Fetal Neonatal Med. (2009) 22:54–6. 10.1080/14767050903198397
169.
Heintz E Brodtkorb TH Nelson N Levin LÅ . The long-term cost-effectiveness of fetal monitoring during labour: a comparison of cardiotocography complemented with ST analysis versus cardiotocography alone. BJOG Int J Obstetr Gynaecol. (2008) 115:1676–87. 10.1111/j.1471-0528.2008.01935.x
170.
Malcus P . Antenatal fetal surveillance. Curr Opin Obstetr Gynecol. (2004) 16:123–8. 10.1097/00001703-200404000-00005
171.
Florio P Marinoni E Di Iorio R Bashir M Ciotti S Sacchi R et al . Urinary S100B protein concentrations are increased in intrauterine growth-retarded newborns. Pediatrics. (2006) 118:e747–54. 10.1542/peds.2005-2875
172.
Zeitlin J El Ayoubi M Jarreau PH Draper ES Blondel B Künzel W et al . Impact of fetal growth restriction on mortality and morbidity in a very preterm birth cohort. J Pediatr. (2010) 157:733–9. 10.1016/j.jpeds.2010.05.002
173.
Figueras F Gardosi J . Intrauterine growth restriction: new concepts in antenatal surveillance, diagnosis, and management. Am J Obstetr Gynecol. (2011) 204:288–300. 10.1016/j.ajog.2010.08.055
174.
Fukushima T Flores CA Hon EH Davidson EC Jr . Limitations of autocorrelation in fetal heart rate monitoring. Am J Obstetr Gynecol. (1985) 153:685–92. 10.1016/S0002-9378(85)80261-1
175.
Gonçalves H Rocha AP Ayres-de Campos D Bernardes J . Internal versus external intrapartum foetal heart rate monitoring: the effect on linear and nonlinear parameters. Physiol Measure. (2006) 27:307. 10.1088/0967-3334/27/3/008
176.
Van Leeuwen P Geue D Thiel M Cysarz D Lange S Romano MC et al . Influence of paced maternal breathing on fetal-maternal heart rate coordination. Proc Natl Acad Sci USA. (2009) 106:13661–6. 10.1073/pnas.0901049106
177.
Spyridou K Chouvarda I Hadjileontiadis L Maglaveras N . The effect of cigarette smoking on fetal heart rate tracing during pregnancy. J Perinatal Med. (2017) 45:403–11. 10.1515/jpm-2015-0275
178.
Van Leeuwen P Cysarz D Edelhäuser F Grönemeyer D . Heart rate variability in the individual fetus. Auton Neurosci. (2013) 178:24–8. 10.1016/j.autneu.2013.01.005
179.
Montenegro N Ramos C Matias A Barros H . Variation of embryonic/fetal heart rate at 6-13 weeks' gestation. Ultrasound Obstetr Gynecol. (1998) 11:274–6. 10.1046/j.1469-0705.1998.11040274.x
180.
Arduini D Rizzo G Caforio L Boccolini MR Romanini C Mancuso S . Behavioural state transitions in healthy and growth retarded fetuses. Early Hum Dev. (1989) 19:155–65. 10.1016/0378-3782(89)90076-5
181.
DiPietro JA Bornstein MH Hahn CS Costigan K Achy-Brou A . Fetal heart rate and variability: stability and prediction to developmental outcomes in early childhood. Child Dev. (2007) 78:1788–98. 10.1111/j.1467-8624.2007.01099.x
182.
Spyridou K Chouvarda I Hadjileontiadis L Maglaveras N . Linear and nonlinear features of fetal heart rate on the assessment of fetal development in the course of pregnancy and the impact of fetal gender. Physiol Measure. (2018) 39:015007. 10.1088/1361-6579/aa9e3c
183.
Tagliaferri S Esposito FG Fagioli R Di Cresce M Sacchi L Signorini MG et al . Ethnic analogies and differences in fetal heart rate variability signal: a retrospective study. J Obstetr Gynaecol Res. (2017) 43:281–290. 10.1111/jog.13213
184.
Tendais I Figueiredo B Gonçalves H Bernardes J Ayres-de Campos D Montenegro N . Sex differences in the fetal heart rate variability indices of twins. J Perinatal Med. (2015) 43:221–5. 10.1515/jpm-2014-0031
185.
Park YS Ryu KY Shim SS Hoh JK Park MI . Comparison of fetal heart rate patterns using nonlinear dynamics in breech versus cephalic presentation at term. Early Hum Dev. (2013) 89:101–6. 10.1016/j.earlhumdev.2012.08.006
186.
Gonçalves H Ayres-de Campos D Bernardes J . Fetal behavioral dynamics in cephalic versus breech presentations. Dev Psychobiol. (2014) 56:1595–600. 10.1002/dev.21242
187.
Takashima T Koyanagi T Horimoto N Satoh S Nakano H . Breech presentation: is there a difference in eye movement patterns compared with cephalic presentation in the human fetus at term?Am J Obstetr Gynecol. (1995) 172:851–5. 10.1016/0002-9378(95)90010-1
188.
Kean L Suwanrath C Gargari S Sahota D James D . A comparison of fetal behaviour in breech and cephalic presentations at term. BJOG Int J Obstetr Gynaecol. (1999) 106:1209–13. 10.1111/j.1471-0528.1999.tb08150.x
189.
Choi WY Hoh JK . Nonlinear analysis of fetal heart rate dynamics in fetuses compromised by asymptomatic partial placental abruption. Placenta. (2015) 36:1474–9. 10.1016/j.placenta.2015.10.002
190.
Moraes ER Murta Jr LO Baffa O Wakai RT Comani S . Linear and nonlinear measures of fetal heart rate patterns evaluated on very short fetal magnetocardiograms. Physiol Measure. (2012) 33:1563. 10.1088/0967-3334/33/10/1563
191.
Nijhuis J Prechtl H Martin CB Jr Bots R . Are there behavioural states in the human fetus?Early Hum Dev. (1982) 6:177–95. 10.1016/0378-3782(82)90106-2
192.
Nijhuis IJ ten Hof J . Development of fetal heart rate and behavior: indirect measures to assess the fetal nervous system. Eur J Obstetr Gynecol. (1999) 1:1–2. 10.1016/S0301-2115(99)00143-8
193.
Swartjes J Van Geijn H Mantel R Van Woerden E Schoemaker H . Coincidence of behavioural state parameters in the human fetus at three gestational ages. Early Hum Dev. (1990) 23:75–83. 10.1016/0378-3782(90)90130-B
194.
Jiménez-González A James C . On the interpretation of the independent components underlying the abdominal phonogram: a study of their physiological relevance. Physiol Measure. (2012) 33:297. 10.1088/0967-3334/33/2/297
195.
Silva I Behar J Sameni R Zhu T Oster J Clifford GD et al . Noninvasive fetal ECG: the PhysioNet/computing in cardiology challenge. In: Computing in Cardiology. Zaragoza: IEEE (2013). p. 149–52.
196.
Di Maria C Liu C Zheng D Murray A Langley P . Extracting fetal heart beats from maternal abdominal recordings: selection of the optimal principal components. Physiol Measure. (2014) 35:1649. 10.1088/0967-3334/35/8/1649
197.
Alnuaimi S Jimaa S Kimura Y Apostolidis GK Hadjileontiadis LJ Khandoker AH . Fetal cardiac timing events estimation from Doppler ultrasound signals using swarm decomposition. Front Physiol. (2019) 10:789. 10.3389/fphys.2019.00789
198.
Lin C Yeh CH Wang CY Shi W Serafico BMF Wang CH et al . Robust fetal heart beat detection via R-peak intervals distribution. IEEE Trans Biomed Eng. (2019) 66:3310–9. 10.1109/TBME.2019.2904014
199.
Monteiro-Santos J Henriques T Nunes I Amorim-Costa C Bernardes J Costa-Santos C . Complexity of cardiotocographic signals as a predictor of labor. Entropy. (2020) 22:104. 10.3390/e22010104
200.
Kim KN Park YS Hoh JK . Sex-related differences in the development of fetal heart rate dynamics. Early Hum Dev. (2016) 93:47–55. 10.1016/j.earlhumdev.2015.12.005
201.
Montalvo-Jaramillo CI Pliego-Carrillo AC Pena-Castillo MÁ Echeverria JC Becerril-Villanueva E Pavón L et al . Comparison of fetal heart rate variability by symbolic dynamics at the third trimester of pregnancy and low-risk parturition. Heliyon. (2020) 6:e03485. 10.1016/j.heliyon.2020.e03485
202.
Lim J Kwon JY Song J Choi H Shin JC Park IY . Quantitative comparison of entropy analysis of fetal heart rate variability related to the different stages of labor. Early Hum Dev. (2014) 90:81–85. 10.1016/j.earlhumdev.2013.12.007
203.
Saleem S Naqvi SS Manzoor T Saeed A Mirza J et al . A strategy for classification of “vaginal vs. cesarean section” delivery: bivariate empirical mode decomposition of cardiotocographic recordings. Front Physiol. (2019) 10:246. 10.3389/fphys.2019.00246
204.
Gonçalves H Amorim-Costa C Ayres-de Campos D Bernardes J . Evolution of linear and nonlinear fetal heart rate indices throughout pregnancy in appropriate, small for gestational age and preterm fetuses: a cohort study. Comput Methods Prog Biomed. (2018) 153:191–9. 10.1016/j.cmpb.2017.10.015
205.
Tagliaferri S Esposito FG Esposito G Saccone G Signorini MG Magenes G et al . Impact of nuchal cord on antenatal and intrapartum foetal heart rate surveillance and perinatal outcome. J Obstetr Gynaecol. (2020) 40:316–23. 10.1080/01443615.2019.1621816
206.
Boudet S de l'Aulnoit AH Demailly R Peyrodie L Beuscart R de l'Aulnoit DH . Fetal heart rate baseline computation with a weighted median filter. Comput Biol Med. (2019) 114:103468. 10.1016/j.compbiomed.2019.103468
207.
Magenes G Signorini MG Arduini D Cerutti S . Fetal heart rate variability due to vibroacoustic stimulation: linear and nonlinear contribution. Methods Inform Med. (2004) 43:47–51. 10.1055/s-0038-1633833
208.
Annunziata ML Scala M Giuliano N Tagliaferri S Imperato OCM Esposito FG et al . Fetal vibroacoustic stimulation in computerized cardiotocographic analysis: the role of short-term variability and approximate entropy. J Pregnancy. (2012) 2012:814987. 10.1155/2012/814987
209.
Signorini MG Magenes G Cerutti S Arduini D . Linear and nonlinear parameters for the analysis of fetal heart rate signal from cardiotocographic recordings. IEEE Trans Biomed Eng. (2003) 50:365–74. 10.1109/TBME.2003.808824
210.
Signorini MG Pini N Malovini A Bellazzi R Magenes G . Dataset on linear and non-linear indices for discriminating healthy and IUGR fetuses. Data Brief . (2020) 29:105164. 10.1016/j.dib.2020.105164
211.
Chen K Zhao Y Li S Chen L Wang N Zhang K et al . Multiscale coupling of uterine electromyography and fetal heart rate as a novel indicator of fetal neural development. Front Neurol. (2019) 10:760. 10.3389/fneur.2019.00760
212.
Esposito FG Tagliaferri S Giudicepietro A Giuliano N Maruotti GM Saccone G et al . Fetal heart rate monitoring and neonatal outcome in a population of early-and late-onset intrauterine growth restriction. J Obstetr Gynaecol Res. (2019) 45:1343–351. 10.1111/jog.13981
213.
Fuentealba P Illanes A Ortmeier F . Independent analysis of decelerations and resting periods through CEEMDAN and spectral-based feature extraction improves cardiotocographic assessment. Appl Sci. (2019) 9:5421. 10.3390/app9245421
214.
Fuentealba P Illanes A Ortmeier F . Cardiotocograph data classification improvement by using empirical mode decomposition. In: 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC). Berlin: IEEE (2019). p. 5646–9. 10.1109/EMBC.2019.8856673
215.
Frasch MG Herry CL Niu Y Giussani DA . First evidence that intrinsic fetal heart rate variability exists and is affected by hypoxic pregnancy. J Physiol. (2020) 598:249–63. 10.1113/JP278773
216.
Khandoker AH Schulz S Al-Angari HM Voss A Kimura Y . Alterations in maternal-fetal heart rate coupling strength and directions in abnormal fetuses. Front Physiol. (2019) 10:482. 10.3389/fphys.2019.00482
217.
Marques JAL Cortez PC Madeiro JP de Albuquerque VHC Fong SJ Schlindwein FS . Nonlinear characterization and complexity analysis of cardiotocographic examinations using entropy measures. J Supercomput. (2020) 76:1305–20. 10.1007/s11227-018-2570-8
218.
Keenan E Udhayakumar RK Karmakar CK Brownfoot FC Palaniswami M . Entropy profiling for detection of fetal arrhythmias in short length fetal heart rate recordings. In: 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC). Montreal, QC: IEEE (2020). p. 621–4. 10.1109/EMBC44109.2020.9175892
219.
Hoyer D Schmidt A Gustafson KM Lobmaier SM Lakhno I van Leeuwen P et al . Heart rate variability categories of fluctuation amplitude and complexity: diagnostic markers of fetal development and its disturbances. Physiol Measure. (2019) 40:064002. 10.1088/1361-6579/ab205f
220.
Park YS Hoh JK . Complex and irregular heart rate dynamics in fetuses compromised by maternal anemia as a high-risk pregnancy. J Perinatal Med. (2015) 43:741–748. 10.1515/jpm-2014-0104
221.
Alshebly Y Nafea M . Isolation of fetal ECG signals from abdominal ECG using wavelet analysis. IRBM. (2020) 41:252–60. 10.1016/j.irbm.2019.12.002
222.
John RG Ramachandran K . Extraction of foetal ECG from abdominal ECG by nonlinear transformation and estimations. Comput Methods Prog Biomed. (2019) 175:193–204. 10.1016/j.cmpb.2019.04.022
223.
Al-Sheikh B Salman MS Eleyan A Alboon S . Non-invasive fetal ECG extraction using discrete wavelet transform recursive inverse adaptive algorithm. Technol Health Care. (2019) 28:507–20. 10.3233/THC-191948
224.
Yuan L Yuan Y Zhou Z Bai Y Wu S . A fetal ECG monitoring system based on the android smartphone. Sensors. (2019) 19:446. 10.3390/s19030446
225.
Ayres-de Campos D Bernardes J Garrido A Marques de Sa J Pereira-Leite L . SisPorto 2.0: a program for automated analysis of cardiotocograms.J Maternal Fetal Med. (2000) 9:311–8. 10.1002/1520-6661(200009/10)9:5<311::AID-MFM12>3.0.CO;2-9
226.
Georgieva A Payne SJ Moulden M Redman CW . Artificial neural networks applied to fetal monitoring in labour. Neural Comput Appl. (2013) 22:85–93. 10.1007/s00521-011-0743-y
227.
Guijarro-Berdinas B Alonso-Betanzos A Fontenla-Romero O . Intelligent analysis and pattern recognition in cardiotocographic signals using a tightly coupled hybrid system. Artif Intell. (2002) 136:1–27. 10.1016/S0004-3702(01)00163-1
228.
Amer-Wåhlin I Maršál K . ST analysis of fetal electrocardiography in labor. In: Seminars in Fetal and Neonatal Medicine. Philadelphia, PA: WB Saunders (2011). p. 29–35. 10.1016/j.siny.2010.09.004
229.
Ribeiro M Henriques T Castro L Souto A Antunes L Costa-Santos C et al . The entropy universe. Entropy. (2021) 23:222. 10.3390/e23020222
230.
Tomassini S Strazza A Sbrollini A Marcantoni I Morettini M Fioretti S et al . Wavelet filtering of fetal phonocardiography: a comparative analysis. Math Biosci Eng. (2019) 16:6034–46. 10.3934/mbe.2019302
231.
Dawes G Moulden M Redman C . Criteria for the design of fetal heart rate analysis systems. Int J biomed Comput. (1990) 25:287–94. 10.1016/0020-7101(90)90032-P
232.
Maulik D Saini V Zigrossi S . Clinical significance of short-term variability computed from heart-rate waveforms. J Perinatal Med. (1983) 11:243–8. 10.1515/jpme.1983.11.5.243
233.
Modanlou HD Freeman RK Braly P . A simple method of fetal and neonatal heart rate beat-to-beat variability quantitation: Preliminary report. Am J Obstetr Gynecol. (1977) 127:861–8. 10.1016/0002-9378(77)90119-3
234.
Druzen M Ikenoye T Murata Y . A possible mechanism for the increase in FHR variability following hypoxemia. In: Presented before the 26th Annual Meeting of the Society for Gynecologic Investigation. San Diego, CA (1979).
235.
Ferrario M Signorini MG Magenes G Cerutti S . Comparison of entropy-based regularity estimators: application to the fetal heart rate signal for the identification of fetal distress. IEEE Trans Biomed Eng. (2006) 53:119–25. 10.1109/TBME.2005.859809
236.
Baschat A . Neurodevelopment following fetal growth restriction and its relationship with antepartum parameters of placental dysfunction. Ultrasound Obstetr Gynecol. (2011) 37:501–14. 10.1002/uog.9008
237.
Tagliaferri S Fanelli A Esposito G Esposito FG Magenes G Signorini MG et al . Evaluation of the acceleration and deceleration phase-rectified slope to detect and improve IUGR clinical management. Comput Math Methods Med. (2015) 2015:236896. 10.1155/2015/236896
238.
Bernardes J Moura C Marques de Sa JP Leite LP . The Porto system for automated cardiotocographic signal analysis. J Perinatal Med. (1991) 19:61–5. 10.1515/jpme.1991.19.1-2.61
239.
Ivanov PC Ma QD Bartsch RP . Maternal-fetal heartbeat phase synchronization. Proc Natl Acad Sci USA. (2009) 106:13641–2. 10.1073/pnas.0906987106
240.
Kinsella MT Monk C . Impact of maternal stress, depression & anxiety on fetal neurobehavioral development. Clin Obstetr Gynecol. (2009) 52:425. 10.1097/GRF.0b013e3181b52df1
241.
Hoyer D Nowack S Bauer S Tetschke F Rudolph A Wallwitz U et al . Fetal development of complex autonomic control evaluated from multiscale heart rate patterns. Am J Physiol Regulat Integr Comp Physiol. (2013) 304:R383–92. 10.1152/ajpregu.00120.2012
242.
Van den Bergh BR Mennes M Stevens V van der Meere J Börger N Stiers P et al . ADHD deficit as measured in adolescent boys with a continuous performance task is related to antenatal maternal anxiety. Pediatr Res. (2006) 59:78–82. 10.1203/01.pdr.0000191143.75673.52
243.
Barker DJ . In utero programming of chronic disease. Clin Sci. (1998) 95:115–28. 10.1042/cs0950115
244.
Värri A Kallonen A Helander E Ledesma A Pladys P . The Digi-NewB project for preterm infant sepsis risk and maturity analysis. Finnish J eHealth eWelfare. (2018) 10:330–3. 10.23996/fjhw.69152
245.
Signorini MG Ferrario M Cerutti S Magenes G . Advances in monitoring cardiovascular signals. Contribution of nonlinear signal processing. In: 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society. Boston, MA: IEEE (2011). p. 6568–71. 10.1109/IEMBS.2011.6091620
246.
Magenes G Signorini MG Ferrario M Lunghi F . 2CTG2: A new system for the antepartum analysis of fetal heart rate. In: 11th Mediterranean Conference on Medical and Biomedical Engineering and Computing. Ljubljana: Springer (2007). p. 781–4. 10.1007/978-3-540-73044-6_203
247.
Ferrario M Signorini MG Magenes G . New indexes from the Fetal Heart Rate analysis for the identification of severe intra uterine growth restricted fetuses. In: 2006 International Conference of the IEEE Engineering in Medicine and Biology Society. New York, NY: IEEE (2006). p. 1458–61. 10.1109/IEMBS.2006.259274
248.
Signorini MG Magenes G . Reliable nonlinear indices for fetal heart rate variability signal analysis. In: 2014 8th Conference of the European Study Group on Cardiovascular Oscillations (ESGCO). Trento: IEEE (2014). p. 213–4. 10.1109/ESGCO.2014.6847595
249.
Lunghi F Magenes G Pedrinazzi L Signorini MG . Detection of fetal distress though a support vector machine based on fetal heart rate parameters. In: Computers in Cardiology. Lyon: IEEE (2005). p. 247–50. 10.1109/CIC.2005.1588083
250.
Delgado JA Altuve M Homsi MN . Haar wavelet transform and principal component analysis for fetal QRS classification from abdominal maternal ECG recordings. In: 2015 20th Symposium on Signal Processing, Images and Computer Vision (STSIVA). Bogota: IEEE (2015). p. 1–6. 10.1109/STSIVA.2015.7330451
251.
Lu YS Wei Sy Liu Xl . Nonlinear FHR baseline estimation using empirical mode decomposition and kohonen neural network. In: 2012 IEEE Biomedical Circuits and Systems Conference (BioCAS). Hsinchu: IEEE (2012). p. 368–71. 10.1109/ICoSP.2012.6491896
252.
Georgoulas G Gavrilis D Tsoulos IG Stylios C Bernardes J Groumpos PP . Novel approach for fetal heart rate classification introducing grammatical evolution. Biomed Signal Process Control. (2007) 2:69–79. 10.1016/j.bspc.2007.05.003
253.
Inbarani HH Banu PN Azar AT . Feature selection using swarm-based relative reduct technique for fetal heart rate. Neural Comput Appl. (2014) 25:793–806. 10.1007/s00521-014-1552-x
254.
Spilka J Georgoulas G Karvelis P Chudáček V Stylios CD Lhotská L . Discriminating normal from "abnormal" pregnancy cases using an automated FHR evaluation method. In: Hellenic Conference on Artificial Intelligence. Cham: Springer (2014). p. 521–31. 10.1007/978-3-319-07064-3_45
255.
Karvelis P Spilka J Georgoulas G Chudáček V Stylios CD Lhotská L . Combining latent class analysis labeling with multiclass approach for fetal heart rate categorization. Physiol Measure. (2015) 36:1001. 10.1088/0967-3334/36/5/1001
256.
Khandoker AH Al-Angari HM Voss A Schulz S Kimura Y . Quantification of maternal-fetal cardiac couplings in normal and abnormal pregnancies applying high resolution joint symbolic dynamics. Math Biosci Eng. (2020) 17:802–13. 10.3934/mbe.2020042
257.
Montero-Nava JE Pliego-Carrillo AC Ledesma-Ramirez CI Pena-Castillo MÁ Echeverria JC Pacheco-López G et al . Analysis of the fetal cardio-electrohysterographic coupling at the third trimester of gestation in healthy women by Bivariate Phase-Rectified Signal Averaging. PLoS ONE. (2020) 15:e0236123. 10.1371/journal.pone.0236123
258.
Signorini MG Pini N Malovini A Bellazzi R Magenes G . Integrating machine learning techniques and physiology based heart rate features for antepartum fetal monitoring. Comput Methods Prog Biomed. (2020) 185:105015. 10.1016/j.cmpb.2019.105015
259.
Lee SK Park YS Cha KJ . Recovery of signal loss adopting the residual bootstrap method in fetal heart rate dynamics. Biomed Eng. (2019) 64:157–61. 10.1515/bmt-2017-0203
Summary
Keywords
fetal heart rate, non-linear methods, entropy, data compression, fractal analysis, wavelet analysis, systematic review
Citation
Ribeiro M, Monteiro-Santos J, Castro L, Antunes L, Costa-Santos C, Teixeira A and Henriques TS (2021) Non-linear Methods Predominant in Fetal Heart Rate Analysis: A Systematic Review. Front. Med. 8:661226. doi: 10.3389/fmed.2021.661226
Received
30 January 2021
Accepted
04 November 2021
Published
30 November 2021
Volume
8 - 2021
Edited by
Patrice Abry, École Normale Supérieure de Lyon, Université de Lyon, France
Reviewed by
Maria G. Signorini, Politecnico di Milano, Italy; Giovanni Magenes, University of Pavia, Italy
Updates
Copyright
© 2021 Ribeiro, Monteiro-Santos, Castro, Antunes, Costa-Santos, Teixeira and Henriques.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Ribeiro maria.r.ribeiro@inesctec.pt
†These authors share last authorship
This article was submitted to Obstetrics and Gynecology, a section of the journal Frontiers in Medicine
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.