Abstract
Cutaneous vasculitis (CV) is an inflammatory skin-limited vascular disease affecting the dermal and/or hypodermal vessel wall. From the pathogenetic point of view, idiopathic forms are described as well as the induction from various triggers, such as drugs, infections, and vaccines. Following SARS-CoV-2 pandemic outbreak, cases of CV induced by both COVID-19 and COVID-19 vaccinations have been reported in literature. The aim of our work was to collect multiple cases available in the literature and analyze the frequency of the different forms of induced vasculitis, as well as their histological and immunopathological features. Although rare, CV induced by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and vaccines may provide interesting insights into the pathogenesis of these inflammatory processes that may in the future be useful to understand the mechanisms underlying cutaneous and systemic vasculitis.
Introduction
The term vasculitis encompasses a wide and heterogeneous group of disorders with shared histopathological findings. It is a pathological process characterized by an inflammatory process affecting the vessel wall, both arterial and venous, of different sizes and of any body area (1). Inside the vessel wall, there is an infiltrate, which can create discontinuity of the wall itself with red blood cells leaking. One of the most successful attempts at proper classification of such condition has been proposed by the 2012 Chapel Hill consensus cVonference nomenclature of vasculitides (CHCC 2012) (2), which divides them according to the diameter of the affected vessel: Large Vessel Vasculitis and Medium Vessel Vasculitis, which in the skin can cause necrosis and ulceration and livaedo reticularis; Small Vessel Vasculitis, manifesting with purpura and vesiculo-bullous lesions.
Since the skin is one of the most affected organs in vasculitides, in 2018, a Dermatological Addendum has been suggested to further help the clinician in dealing with such conditions, improving the definition of some forms of cutaneous vasculitis (CV) and adding other dermatological relevance (3). Accordingly, CV may be a cutaneous manifestation of systemic vasculitis or a skin-limited or skin-dominant variant of systemic vasculitis, but when affecting only the skin in the absence of any other systemic involvement, the term single-organ vasculitis (SOV) should be used.
CV is mainly a small-vessel vasculitis affecting dermal and/or hypodermal capillaries and venules, which usually show histopathologic findings consistent with leukocytoclastic vasculitis, characterized by fibrinoid necrosis of vessel wall, erythrocyte extravasation, and neutrophilic infiltrate with degeneration known as leukocytoclasis with nuclear dust (karyorrhexis) (4). The immune infiltration may be mainly lymphocytic in lesions that appeared more than 48 h before. Direct immunofluorescence (DIF) of lesional skin is helpful in the diagnosis of CV, with maximum efficacy for the diagnosis of IgA vasculitis and lupus vasculitis. It can aid in the accurate diagnosis even when the histological changes are minimal (5–7). However, DIF positivity is strongly influenced by the timing of the biopsy (8).
Even though in more than half cases of CV it is impossible to assess the disease-inducing or promoting factor, it is well-known that the most common triggering factors are related to immunopathogenic mechanisms secondary to infections or drug intake (9, 10). Therefore, it is not surprising that since the beginning of the COVID-19 pandemic and after the introduction and administration of COVID-19 vaccines on a global scale, cases of COVID-19-associated and vaccine-associated CV have been reported (11–13).
When involving the skin, clinical manifestations of the COVID-19 infection show a great range of signs and symptoms (14). Five major classes of cutaneous manifestations in the setting of COVID-19 infection have been proposed by Tan et al. (15), e.g., pseudo-chilblains lesions, urticarial rash, vesicular (varicella-like) eruption, maculo-papular rash, and vaso-occlusive lesions. Several cases of both new onset and flares of CV have also been linked to COVID-19 and SARS-CoV-2 vaccination. However, they are not included in the aforementioned classification due to their low frequency (12, 16, 17).
Similarly, many heterogeneous cutaneous reactions to COVID-19 vaccination have been reported and classified by Shakoei et al. into the following major categories: local site reactions, type 1 (immediate) hypersensitivity reactions, type 4 (delayed) hypersensitivity reactions, autoimmune-mediated reactions, functional angiopathies, and reactivation of other viral conditions (18). In this classification, CV are classified among the auto immune-mediated reactions. Most of the cases reported occurred after the administration of messenger ribonucleic acid (mRNA)-based vaccines (19). In the literature, vaccine-associated CVs have been more frequently reported than CVs secondary to the COVID-19 infection. The number of persons that received at least one dose of the vaccine worldwide is larger when compared to that of the persons who contracted the infection. However, it is known that the vaccine reproduces only a small degree of adverse effects provoked by the natural infection of the immune system. Therefore, more vaccine-associated CVs are diagnosed and reported due to the greater attention that has been given by patients to all the side effects related to the COVID-19 vaccine.
In this review, we analyze and compare the current and most recent literature on clinical and immunohistopathologic features of CV induced by systemic SARS-CoV-2 infection and CV secondary to the SARS-CoV-2 vaccine, focusing on the possible underlying pathogenetic mechanisms.
SARS-CoV-2 infection and cutaneous vasculitis
We collected clinicopathological features of a series of CV that occurred in association with the SARS-CoV-2 infection available in the literature (Table 1). Our search was restricted to cases with histological confirmation of leukocytoclastic vasculitis. Totally, 19 cases were included, mostly males (13/19) with variable age distribution ranging from 13 to 93 years with an average of 48.4 years. In three cases, the diagnosis was COVID-19-associated IgA vasculitis, while in five cases the patients had been diagnosed with COVID-19-associated urticarial vasculitis; finally, the other cases may be considered as cutaneous leukocytoclastic vasculitis associated with COVID-19, being not further classified according to the Dermatologic Addendum to the 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides (3). Regarding the clinical presentation, a comparison between the frequency of different types of lesions did not reveal feasible given the heterogeneity of their description. However, it is reasonable to consider palpable purpura as the main clinical manifestation, sometimes with necrotic features and hemorrhagic blistering. The most common sites affected were the lower limbs and trunk, as for the idiopathic forms of CV. The cases diagnosed with urticarial vasculitis showed slight clinical differences, since skin lesions were characterized by wheals or urticarial manifestations, associated with purpuric aspects. The edematous component of cutaneous lesions in COVID-19-associated urticarial vasculitis was appreciable at histological evaluation in 2 out of 5 cases, whose report mentioned dermal or endothelial swelling. The latency time between skin rash occurrence with SARS-CoV-2 infection is highly variable, ranging from concomitant signs appearing at the time of onset to more than 30 days after the first positive nasopharyngeal swab. The totality (3/3) of COVID-19-associated IgA vasculitis cases presented kidney involvement, but it is of interest that in two out of three cases, the direct immunofluorescence (DIF) performed on lesional skin resulted negative while positivity was seen in all three cases when performed on kidney biopsy. Although based on a few cases, our results are in accordance with Jedlowski et al., which published a case series of 10 subjects with COVID-19-associated systemic IgA vasculitis; in fact, authors found positive skin DIF in less than half of the series (40%) while kidney biopsies showed IgA deposition in all the cases. Moreover, it is of note that COVID-19-associated IgA vasculitis more commonly affects adults when compared to the classical form of IgA vasculitis in which 90% of cases occur in the pediatric population. In our series, one DIF resulted non-specifically positive for C3, while in nine cases, it was negative for all the reactants. No cases of cutaneous IgG/IgM vasculitis were diagnosed and in eight subjects DIF was not performed. Interestingly, three cases assessed the colocalization of SARS-CoV-2 in the vessel wall, finding positivity in 2/3 cases by the PCR technique. This may support the direct role of SARS-CoV-2 in the pathogenesis of cutaneous vasculitis and its tropism for a broad variety of human tissues.
Table 1
| Case no | Age | Sex | Comorbid | Time to infection | Clinical presentation | Histology | DIF | SARS-CoV-2 in dermal vessels | Ref |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 93 | M | CKD | 8 days | purpuric macules and papules on legs, hands, and periumbilical area | Fibrin deposition, | Negative for IgG, IgA, IgM, C3 | N/A | Capoferri et al. (45) |
| PAD Hypertension | Obliteration of vessels | ||||||||
| Extravasated red blood cells | |||||||||
| 2 | 66 | M | T2DM Hypertension CAD | 15 days | Palpable purpuric papules with necrotic center | Fibrin extravasation in vascular structures | Negative for IgG, IgM, IgA, C3 | N/A | Bay et al. (46) |
| Inclusion bodies in endothelial cells | |||||||||
| Maculo-papular lesions on legs and forearms | |||||||||
| Perivascular neutrophil, lymphocyte infiltrate Leukocytoclasis in the dermis |
|||||||||
| 3 | 16 | F | None | N/A | Edematous, maculopapular erythematous rash on extremities, abdomen, back, thighs and face | Neutrophilic vasculitis | Negative for IgG, IgM, IgA, C3 | N/A | Gosnell et al. (47) |
| Karyorrhectic debris | |||||||||
| Focal degeneration of vessel wall | |||||||||
| Rare intraluminal fibrin deposits | |||||||||
| Micro-thrombi | |||||||||
| 4 | 13 | M | None | 28 days | Petechial and purpuric rash on both feet and ankles | Superficial epidermal necrosis | Negative for IgG, IgM, IgA, C3 | Positive (PCR) | Kumar et al. (48) |
| Small-vessel neutrophilic vasculitis | |||||||||
| 5 | 32 | F | Crohn disease | 14 days | Erythematous to violaceous macules and papules on lower extremities and dorsum of feet | Perivascular karyorrhectic material | Not performed | N/A | Nassani et al. (49) |
| Stromal edema and purpura | |||||||||
| Capillary ectasia | |||||||||
| Thrombotic vasculopathy | |||||||||
| 6 | 49 | M | None | 14 days | Palpable purpura on inferior limbs and abdomen | Hyperkeratosis | Not performed | N/A | Iraji et al. (50) |
| Moderate neutrophilic infiltration | |||||||||
| Extravasated red blood cells | |||||||||
| Lymphocytes around dermal vessels | |||||||||
| 7 | 70 | M | None | N/A | Palpable petechiae on dorsal feet, thighs, abdomen | Leukocytoclastic vasculitis | Positive for IgA | N/A | Jedlowski et al. (51) |
| Purpuric plaques | |||||||||
| 8 | 27 | M | None | N/A | Painful purpuric papules | Leukocytoclastic cutaneous vasculitis | Negative for IgG, IgM, IgA, C3 | N/A | Gouveia et al. (52) |
| Vesicobullous hemorrhagic lesions Necrotic lesions | Microthrombi | ||||||||
| 9 | 43 | M | Hypertension | N/A | Painful hemorrhagic bullae | Leukocytoclastic vessel vasculitis | Negative for IgG, IgM, IgA, C3 | N/A | Kösters et al. (53) |
| Necrotic lesions on trunk, arms, legs | Neutrophilic infiltration | ||||||||
| Eosinophils and histiocytes | |||||||||
| 10 | 29 | M | None | 28 days | Purple palpable papules | Heavy neutrophilic infiltrate in small vessel wall | Negative for IgG, IgA, IgM, C3 | Positive (PCR) | Camprodon Gómez et al. (54) |
| Necrotic lesions | |||||||||
| Serohaematic blisters on abdomen, buttocks, lower legs, feet | Leucocytoclasis | ||||||||
| Fibrinoid necrosis | |||||||||
| Extravasation of red blood cells | |||||||||
| 11 | 47 | M | Hypertension, impaired glucose tolerance | 18 days | Multiple, raised erythematous wheals, alone or in cluster, some with central purple Hyperpigmentation on head, trunk and upper arms | Orthokeratotic hyperkeratosis | Not performed | N/A | Skroza et al. (55) |
| Spongiosis | |||||||||
| Focal lymphocytic exocytosis | |||||||||
| Perivascular neutrophilic infiltration | |||||||||
| Vessel wall damage | |||||||||
| 12 | 64 | F | Hypertension, T2DM | Concomitant | Annular and polycyclic urticarial lesions with purpuric component on trunk and limbs | Dermal edema | Not performed | N/A | Nasiri et al. (56) |
| Leukocytoclastic vasculitis | |||||||||
| 13 | 59 | M | N/A | 35 days | Maculopapular purpuric exanthema on face, trunk, limbs | Perivascular neutrophilic infiltrate | Not performed | N/A | Caputo et al. (57) |
| Leucocytoclasis | |||||||||
| Red blood cell extravasation | |||||||||
| Fibrinoid necrosis of vessel walls | |||||||||
| 14 | N/A | F | N/A | N/A | Painful erythematous patches on trunk, hips | Red blood cell extravasation | Not performed | N/A | de Perosanz-Lobo et al. (58) |
| Purpura | Neutrophilic perivascular inflammation | ||||||||
| Karyorrhexis | |||||||||
| 15 | N/A | M | N/A | N/A | Erythematous and edematous plaques with a purpuric center | Perivascular neutrophilic inflammation | Not performed | N/A | de Perosanz-Lobo et al. (58) |
| Red blood cell extravasation | |||||||||
| Endothelial swelling | |||||||||
| Necrotic lesions | |||||||||
| Fibrin deposition | |||||||||
| 16 | 79 | F | N/A | 7 days | Purpuric macules and papules on legs | Fibrinoid necrosis of vessel walls | Positive for C3 | Negative (PCR) | Dominguez-Santas et al. (59) |
| Transmural infiltration by neutrophils | |||||||||
| Karyorrhexis | |||||||||
| Leukocytoclasia | |||||||||
| Red blood cell extravasation | |||||||||
| 17 | 83 | F | Hypertension | 30 days | Purpuric palpable papules and serohematic blisters on lower legs, feet, toes | Perivascular neutrophils | Not performed | Not performed | Mayor-Ibarguren et al. (60) |
| TIA | Fibrins in vessel wall of the dermis | ||||||||
| AF | Leukocytoclasia | ||||||||
| CKD | |||||||||
| 18 | 30 | M | No | Concomitant | Painful purpuric rash | Leukocytoclastic vasculitis | Negative for IgA, IgG, IgM, C3 | Not performed | Li et al. (61) |
| 19 | 22 | M | None | Concomitant | Palpable purpura with central vesicles on extremities, gluteal region, lower abdomen | Perivascular infiltrate of neutrophils, lymphocytes | Negative for IgG, IgM, IgA, C3 | Not performed | Sandhu et al. (62) |
| Red blood cell extravasation | |||||||||
| Fibrinoid necrosis of vessel wall |
Clinical, histological, and immunological findings in patients with COVID-19-associated CV.
CKD, chronic kidney disease; PAD, peripheral artery disease; T2DM, type 2 diabetes mellitus; CAD, coronary artery disease; TIA, transient ischaemic attack; AF, atrial fibrillation.
SARS-CoV-2 vaccination and cutaneous vasculitis
In the mini-series presented (Table 2), only patients with histological confirmation of leukocytoclastic vasculitis were included. Totally, 39 patients developed CV after the COVID-19 vaccine. Women were found to be more involved than men, counting 24 females vs. 15 males developing CV. The weighted average of the patients reported was of 53.2 years (range 22–94).
Table 2
| Case no | Age | Sex | Vaccine type | Vaccine name | Exclusion of SARS-CoV-2 infection | Comorbid | Temporal relation to the vaccine | Clinical characteristics of CV reported | Systemic involvement | DIF | References |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 30 | M | Adenoviral vector-based | Johnson-Johnson | Negative nasopharyngeal RT-PCR swab | None | 17 days after the first dose | Painful hemorrhagic papules and vesicles on soles, shins, elbows | Mild proteinuria | Granular deposits of IgM, C3, and fibrin/fibrinogen in the walls of the dermal small vessels | Betetto L et al. (63) |
| Hypocomplementemia | |||||||||||
| Cryoglobulinemia | |||||||||||
| 2 | 45 | M | Inactivated vaccine | Sinopharm | Not mentioned | None | 2 days after the first dose | Papular lesions on upper and lower limbs | Pruritus | Not performed | Shakoei et al. (18) |
| 3 | 61 | F | Adenoviral vector-based | Oxford-AstraZeneca | Negative nasopharyngeal RT-PCR swab | Hypertension | 5 days after the first dose | Pruritic erythematous-purpuric macules involving the lower legs, feet, buttocks, axillae, abdomen | Myalgia | Not performed | Criado et al. (13) |
| Fatigue | |||||||||||
| 4 | 52 | M | m-RNA-based | Moderna | Not mentioned | Not mentioned | 11 days after the second dose | Erythematous, non-pruritic petechial rash on lower limbs | Not reported | Not performed | Gázquez Aguilera et al. (11) |
| 5 | 80 | M | m-RNA-based | BioNTech/ Pfizer | Negative serologic investigations | Psoriasis | 4 weeks after the second dose | Targetoid erythematous lesions | Fever | Negative for IgG, IgM, IgA, C3 | Wollina et al. (19) |
| Fatigue | |||||||||||
| General malaise | |||||||||||
| Necrotic lesions on legs Erythematous lesions on the soft palate | |||||||||||
| Hemochromatosis | |||||||||||
| Nodular goiter | |||||||||||
| Purpuric macules on fingers and palmar creases | |||||||||||
| Splinter hemorrhages on nails | |||||||||||
| 6 | 57 | F | Adenoviral vector-based | Oxford-AstraZeneca | Not mentioned | Fibrocystic mastopathy | 5 days after the second dose | Purpuric macules and papules on lower legs | Not reported | Linear and granular deposition of IgM within small vessels | Fiorillo et al. (64) |
| Hypertension | |||||||||||
| 7 | 51 | F | m-RNA-based | Moderna | No prior history of SARS-CoV2 infection | Sjögren syndrome Cryoglobulinemic vasculitis | 3 weeks after the second dose | Palpable purpura and ulcers Lower extremities pitting edema | Acute kidney injury | Not performed | Vornicu et al. (65) |
| Nephrotic syndrome | |||||||||||
| 8 | 59 | F | m-RNA-based | BioNTech/ Pfizer | No prior history of SARS-CoV2 infection | Sjögren syndrome Cryoglobulinemic vasculitis | 2 days after the first dose | Palpable purpura | Fatigue | Not performed | Vornicu et al. (65) |
| Small cutaneous malleolar ulcers | Fever | ||||||||||
| Myalgias | |||||||||||
| Acute kidney injury Nephritic syndrome | |||||||||||
| 9 | 55 | F | Adenoviral vector-based | Oxford-AstraZeneca | Negative RT-PCR | None | 5 days after the first dose | Palpable purpura on lower limbs | Fever | Negative | Sandhu et al. (66) |
| Myalgia | |||||||||||
| Wrist swelling | |||||||||||
| 10 | 48 | M | Adenoviral vector-based | Oxford-AstraZeneca | Negative RT-PCR | Hypertension | 2 days after the second dose | Palpable purpura on hands, forearms, gluteal region, lower limbs | Fever | Negative | Sandhu et al. (66) |
| Myalgia | |||||||||||
| 11 | 46 | F | m-RNA-based | BioNTech/ Pfizer | Not mentioned | Psoriasis | 2 days after the first dose (1st flare), 2 days after the second dose (2nd flare) | Exacerbation of palpable purpuric papules lower legs (first flare) | Not reported | Not performed | Cohen et al. (67) |
| PsA | |||||||||||
| Irritable bowel syndrome Leukocytoclastic vasculitis |
|||||||||||
| Palpable purpuric papules on the lower legs, feet, upper extremities, lower back, and abdomen (second flare) | |||||||||||
| 12 | 83 | F | m-RNA-based | BioNTech/ Pfizer | Not mentioned | None | 5 days after the second dose | Palpable purpura with erythema and edema on lower extremities | Elevated levels of C-reactive protein, elevated sedimentation rate, | Deposition of fibrinogen around superficial blood vessels | Larson et al. (68) |
| Rheumatoid factor | |||||||||||
| Hypocomplementemia | |||||||||||
| Cryoglobulinaemia | |||||||||||
| 13 | 57 | F | m-RNA-based | Not mentioned | Not mentioned | Epilepsy Bipolar disorder Depression | 7 days after the first dose | Erythematous confluent papules and plaques involving trunk, extremities | Not reported | Not performed | Bostan et al. (69) |
| 14 | 46 | F | Inactivated | Covaxin | Negative oro-nasopharyngeal RT-PCR swab | None | 5 days after the first dose | Palpable purpura on legs | Arthralgia | Not performed | Kar et al. (44) |
| Ankle swelling | |||||||||||
| Pitting edema on ankles | |||||||||||
| 15 | 47 | M | m-RNA-based | BioNTech/Pfizer | Not mentioned | Intermittent abdominal pain | 3 days after the first dose (first episode); 4 days after the second dose (flare) | Reddish spots in his ankles (first episode) | Elevated C-reactive protein | C3/C4 deposits | Gambichler et al. (70) |
| Proteinuria | |||||||||||
| Purpuric papules on legs, forearms (second episode) | Decreased glomerular filtration rate | ||||||||||
| 16 | 59 | F | m-RNA-based | Moderna | Not mentioned | Hypertension Hyperlipidemia | 1 day after the second dose | Violaceous petechiae on legs, pelvis, abdomen, upper limbs | Intermittent abdominal pain | Not performed | Ireifej et al. (71) |
| Elevated C-reactive protein | |||||||||||
| Prediabetes Obesity COVID-19 in April 2020 | |||||||||||
| 17 | 57 | F | Inactivated | Sinopharm | Not mentioned | None | 5 days after the second dose | Purpuric papules with central blistering | Fatigue | Not performed | Azzazi et al. (39) |
| Arthralgia | |||||||||||
| Necrotic lesions | |||||||||||
| Black eschars on legs | |||||||||||
| Palpable purpura on thighs, buttocks, abdomen, back, forearms | |||||||||||
| 18 | 94 | M | m-RNA-based | Moderna | Not mentioned | AF | 10 days after the second dose | Palpable purpura | Not reported | IgA immune deposits in the blood vessel walls | Grossman et al. (72) |
| Aortic valve replacement | |||||||||||
| Hypothyroidism | |||||||||||
| Anemia | |||||||||||
| 19 | 76 | M | m-RNA-based | BioNTech/ Pfizer | Not mentioned | Liver cirrhosis | 12 days after the second dose | Pruritic purpuric macules on hands, feet, legs, thighs, abdomen | Bloody diarrhea | Not performed | Mücke et al. (73) |
| Heart failure | |||||||||||
| Previous gastroesophageal junction cancer and prostate cancer | |||||||||||
| 20 | 65 | M | m-RNA-based | BioNTech/ Pfizer | Not mentioned | T2DM | 2 days after the third dose | Purpuric palpable lesions on legs | Not reported | Not performed | Dicks et al. (74) |
| Hypertension | |||||||||||
| 21 | 50 | M | m-RNA-based | BioNTech/ Pfizer | Not mentioned | None | 2 days after the second dose | Rash on the legs | Not reported | IgA-dominant immune deposits in the blood vessel walls | Mohamed et al. (75) |
| 22 | 40 | F | m-RNA-based | BioNTech/ Pfizer | Not mentioned | Hashimoto's thyroiditis | 20 days after second dose | Purpuric rash on gluteal region | Headache | Not performed | Hines et al. (76) |
| 23 | 57 | M | Adenoviral vector-based | Oxford-AstraZeneca | Not mentioned | Hypertension | 14 days after the first dose | Purpura on lower limbs, abdomen, trunk, head | Not reported | Not performed | Cavalli G et al. (77) |
| 24 | 57 | F | Adenoviral vector-based | Oxford-AstraZeneca | Not mentioned | Hypertension | 5 days after the first dose | Palpable purpura on buttocks, legs, arms | Not reported | Negative for IgG, IgM, IgA, C3 | Guzmán-Pérez et al. (78) |
| Hypothyroidism | |||||||||||
| 25 | 77 | F | Adenoviral vector-based | Oxford-AstraZeneca | Not mentioned | None | 10 days after the first dose | Palpable indurated purpuric papules | Not reported | Negative for IgG, IgM, IgA, C3 | Shahrigharahkoshan et al. (79) |
| Erythematous plaques and bullae on lower limbs, hands. Purpuric lesions on soft palate, tongue |
|||||||||||
| 26 | 68 | F | Adenoviral vector-based | Oxford-AstraZeneca | Not mentioned | None | 7 days after the first dose | Erythematous to purpuric non-blanching macules on lower extremities | Not reported | Not performed | Jin et al. (80) |
| 27 | 60 | F | Adenoviral vector-based | Oxford-AstraZeneca | Not mentioned | Chronic liver disease | 11 days after the second dose | Painful purpuric lesions on lower limbs | Not reported | IgA and IgM deposits on the walls of postcapillary vessels | Fritzen et al. (81) |
| Portal hypertension | |||||||||||
| Polycythemia vera | |||||||||||
| Hypothyroidism | |||||||||||
| T2DM | |||||||||||
| 28 | 76 | F | Adenoviral vector-based | Oxford-AstraZeneca | Not mentioned | None | 7 days after the first dose | Maculopapular rash on lower extremities | Hematuria | Not performed | Sirufo MM et al. (43) |
| Arthralgia | |||||||||||
| 29 | 46 | F | Inactivated | Covaxin | Negative oropharyngeal RT-PCR swab | None | 5 days after the first dose | Purpuric papules on legs | Arthralgia | Not performed | Kar et al. (44) |
| Ankle swelling | |||||||||||
| 30 | 31 | F | Inactivated | Covaxin | Negative oropharyngeal RT-PCR swab | None | 4 days after the second dose | Palpable purpura on left leg | Not reported | Not performed | Kharkar et al. (82) |
| Pitting edema | |||||||||||
| 31 | 77 | M | Adenoviral vector-based | Sinovac | Negative nasopharyngeal RT-PCR swab | None | 2 weeks after the third dose | Palpable violaceous patches | Gastrointestinal involvement (abdominal pain, stool tests on occult blood-positive) | Negative for IgG, IgM, IgA, C3 | Oskay et al. (83) |
| Bullous hemorrhagic lesions on lower limbs, hands | |||||||||||
| 32 | 33 | M | Adenoviral vector-based | Not mentioned | Mildly symptomatic COVID-19 three months before | None | 3 days after the first dose | Violaceous eruption | Not reported | IgA deposition within small vessel walls | Bostan et al. (84) |
| Erythematous macules | |||||||||||
| Palpable papules on legs, forearms | |||||||||||
| 33 | 91 | F | m-RNA-based | BioNTech/Pfizer | No evidence of acute SARS-CoV-2 infection | Dementia Hypertension T2DM | 4 days after the third dose | Palpable purpuric lesions on lower limbs | Not reported | Not performed | Carrillo-Garcia et al. (37) |
| 34 | 38 | M | m-RNA-based | BioNTech/Pfizer | Not mentioned | None | 4 days before the first dose | Purpuric-erythematous macules, papules, and plaques on lower limbs | Arthralgia | Not performed | Altun et al. (36) |
| 35 | 52 | M | m-RNA-based | Moderna | Not mentioned | Not mentioned | 11 days after the second dose | Erythematous, non-pruritic rash on legs | Not reported | Not performed | Gázquez Aguilera et al. (11) |
| Petechiae on lower limbs | |||||||||||
| 36 | 42 | F | m-RNA-based | BioNTech/Pfizer | Not mentioned | Hypertension Obesity |
4 days after injection (dose number non-specified) | Cutaneous eruption on lower limbs, gluteal area | Not reported | Not evaluable | Erler et al. (85) |
| 37 | 22 | F | m-RNA-based | BioNTech/Pfizer | Not mentioned | None | 7 days after the second dose | Small, red, raised, itchy lesions on legs. Purpuric lesions on lower limbs | Not reported | Not performed | Ripalta Colia et al. (38) |
| 38 | 23 | F | Inactivated | Sinovac | Not mentioned | None | 36 h after first dose | Non-blanchable erythematous plaques with purpura on extremities | None | C3 and fibrinogen deposition around blood vessel walls | Bencharattanapet al. (86) |
| 39 | 26 | F | Inactivated | Sinovac | Not mentioned | None | 4 h after first dose | Non-blanchable purpuric purpura on extremities | None | IgM, C3, and IgA deposition | Bencharattanaphakhi et al. (86) |
Clinical, histological, and immunological findings in patients with COVID-19-vaccine associated CV.
CKD, chronic kidney disease; PAD, peripheral artery disease; T2DM, type 2 diabetes mellitus; CAD, coronary artery disease; TIA, transient ischaemic attack; AF, atrial fibrillation.
Clinically, purpuric papules or maculae in the lower extremities were the most commonly reported skin manifestation (Figure 1). DIF was not reported in 21 cases (53.8%) and in 5 cases (12.8%) it was negative. Features were heterogeneous in the remaining 13 cases, with 5 cases (12.8%) of IgA vasculitis and 3 cases (7.7%) of vasculitis with C3 deposition, and some isolated cases of IgM vasculitis with fibrinogen deposit.
Figure 1
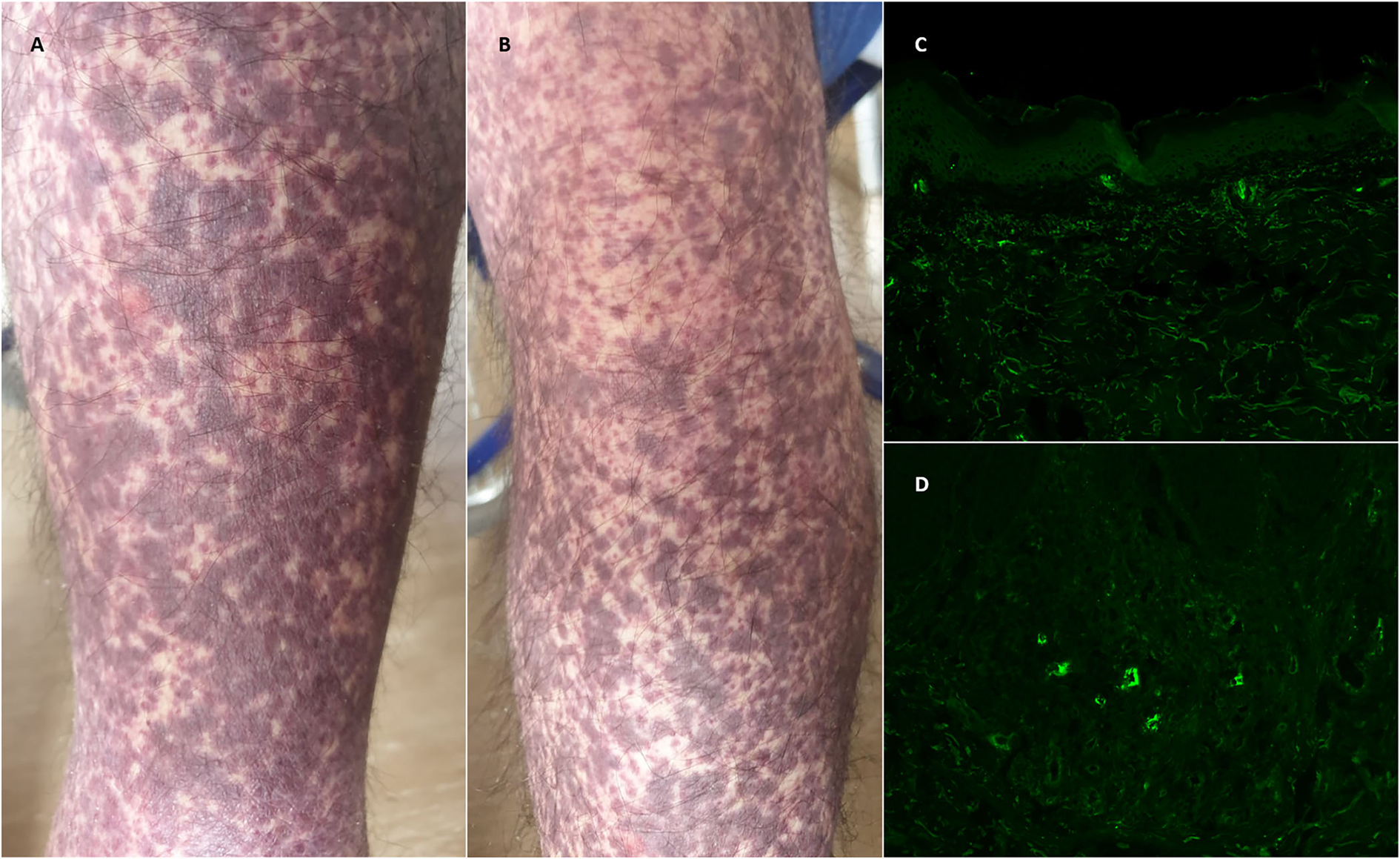
(A,B) Purpuric maculae and papules in the lower extremities in a patient with a recent anamnesis of COVID-19 vaccination. (C,D) Direct immunofluorescence performed on lesional skin, with evidence of perivascular deposition of C3. (c: 10% magnification, d: 20% magnification).
Most of the reported cases (n = 19, 48.7%) were associated with mRNA vaccines; particularly, 13 patients underwent BNT162b2 [BioNTech/Pfizer] vaccines and five patients underwent mRNA-1273 [Moderna] vaccines. In one case, the commercial name of the vaccine was not reported. Eleven cases (28.2%) of CV were associated with adenoviral vector-based vaccines, of whom 10 were with ChAdOx1 nCoV-19 [Oxford-AstraZeneca] and one was with Ad26.Cov2.S [Johnson & Johnson].
Among the nine cases (23.1%) associated with inactivated vaccines, only one was not named, three cases were found after the administration of both Covaxin and Sinovac, and two cases after Sinopharm administration.
Nineteen patients (48.7%) developed CV after the first dose of the vaccine, while 16 (41%) after the second dose; only 3 (7.7%) cases were reported to occur after the third dose of the vaccine injection. In one case (2.6%), the dose number was non-specified.
Discussion
Our review reported the main aspects of both CVs induced by COVID-19 infection and vaccines. Only leukocytoclastic vasculitis was included, and DIF pattern was also analyzed. Unfortunately, in many of the reported cases, DIF was not conducted, while some cases were negative. Its evaluation is extremely important in defining the type of CV and DIF positivity may raise the suspicion of systemic disease, providing useful prognostic information where histology alone cannot. Therefore, DIF should be always performed especially on early lesions because immune deposits may disappear in lesions that occurred more than 48 h before.
To date, the exact pathogenetic mechanisms underlying COVID-19-associated CV have not been fully understood. Since its outbreak in 2019, COVID-19 had spread all over the world causing a global pandemic affecting more than 500 million people and at least 6 million deaths (20). The enveloped RNA virus called Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) is the etiologic agent, which primarily affects the respiratory tract leading to general symptoms like fever, fatigue, anosmia, and dysgeusia, while respiratory symptoms are variable in severity ranging from cough and rhinorrhea to dyspnea, pneumonia, or acute respiratory distress syndrome. However, evidence about the involvement of other organs and systems is increasing; in fact, knowledge about the neurological, gastrointestinal, and ocular manifestations of SARS-CoV-2 infection is deepening (21, 22). Similarly, cutaneous signs of COVID-19 are continuously reported and attempts at classifications are already available in the literature, together with the first prevalence estimations in which dermatologic manifestations would place between 1.8 and 20.4% of the COVID-19 patients (23, 24). In particular, several works identified clusters of skin manifestations that are suggestive of skin vascular damage, namely chilblain-like lesions, acral ischemia, acral vasculitis, livedo reticularis, livedo racemosa, purpuric “vasculitic” rash, or petechial eruptions (25–27). While a definitive nomenclature is justifiably actually lacking, considering the novelty of these entities, it is well known that SARS-CoV-2 features a markable tropism for endothelial cells. The first hypothesis of vascular damage provoked by the novel coronavirus was provided from autoptic studies showing platelet-fibrin thrombi in lung blood vessels in patients who died of severe COVID-19 (28), advancing the evidence of coagulopathy as a main pathogenetic mechanism of single- or multiorgan damage induced by SARS-CoV-2. Indeed, the term “immunothrombosis” is now used to refer to the typical pattern of lung damage resulting from massive viral-induced inflammation, which leads to the activation of the endothelium and triggers intravascular coagulation. Similar mechanisms may be responsible for skin manifestations reflecting vascular dysfunction or true vasculitis, since it was demonstrated that ACE2 is expressed in the skin basal cell layer, dermal vessels endothelium, eccrine glands, and subcutaneous fat tissue and act as a receptor for SARS-CoV-2 Spike protein binding (29). Viral uptake precludes the ACE2-dependent protective action of angiotensin 1–7 and results in oxidative stress, inflammatory cytokine production, and vasoconstriction (30, 31). Endotheliitis following virus internalization enhances endothelial injury, thrombogenesis, and immune recruitment, while the cytokine storm typical of severe cases may additionally boost the same mechanism in multiple anatomical districts (32). Moreover, sustained activation of the complement system causes microvascular injury and a procoagulant state triggered by the deposition of complement component C4d and colocalization of SARS-CoV-2 Spike protein in dermal vessels (33). All these mechanisms contribute to the inflammatory dermal microenvironment, which may be the subject of the innate and adaptive immune cell recruitment leading to the extension of inflammatory process toward the vessel wall, causing vasculitis. Another proposed pathogenetic mechanism may involve an autoimmune response targeting vessel wall components following a break of tolerance or molecular mimicry with SARS-CoV-2 proteins (34). Furthermore, CV was described in the context of Kawasaki-like syndrome, a generalized inflammatory disease affecting mainly infants for which the term “multisystem inflammatory syndrome in children (MIS-C) has been coined. However, the specificity of skin vasculitis in the setting of MIS-C still remains unclear, also due to the less frequency of skin biopsies performed in children.
All vaccines authorized for use by the U.S. Food and Drug Administration (FDA) and the European Agency for the Evaluation of Medicinal Products (EMEA) have been thoroughly studied and found to be safe and effective in preventing severe COVID-19 cases (35). However, as globally millions of people have now been vaccinated, with increasing frequency, vaccination-related diseases have been observed (36), including CV.
Almost all the available COVID-19 vaccines have been associated with CV, e.g., mRNA vaccines (Pfizer BioNTech), mRNA-1273 (Moderna), adenoviral vector-based vaccines (ChAdOx1 nCoV-19; Oxford-AstraZeneca), and inactivated vaccines (Covaxin, Sinovac). Correlations between vaccination and the subsequent appearance of several types of vasculitis have been also described in the literature with vaccines against influenza, hepatitis B, serogroup B meningococcus, hepatitis A, Human Papilloma Virus (HPV) and with Bacillus of Calmette-Guérin (BCG) (37).
An important criterion guiding the assessment of causality is the temporal relationship between immunization and the side event: for drug- and vaccine-induced vasculitis it is considered to be in the range of 1–6 weeks (38). Most of the cases were self-limiting skin forms without systemic involvement, solved spontaneously or after systemic treatment.
The link between vasculitis and vaccination from a pathogenetic point of view is not clear but may involve an immune complex and antibodies deposition in the blood vessel walls (39). Recently, cytoplasmatic granular positivity for SARS-CoV-2 Spike protein was found in some skin specimens of infection-related CV (40). The vaccine proteins are structurally analogous to the wild viral antigens and could induce a pro-inflammatory cascade similar to that caused by the viral protein. Thus, vaccine antigens may activate B/T cells and cause antibody formation with subsequent immune complex deposition in small-caliber vessels. Along with this, Baiu et al. demonstrated the role of Th1 response and suggested that interferon-gamma is critically required for the initiation of vascular inflammation (41). Then, the whole-virion inactivated SARS-CoV-2 vaccine induces primarily a Th1-biased response, which could lead to the induction of an inflammatory response in the vessel wall (42). An open issue for patients who developed such adverse events following COVID-19 vaccination is whether the booster dose should be administered or not. In fact, repeating the administration could potentially cause more severe immunologic reactions (43). However, cutaneous small-vessel vasculitis secondary to infections, drugs, and vaccines is reported to have a less protracted course when compared to primary vasculitis. Therefore, this should not be a deterrent to the use of the COVID-19 vaccine, which is the most effective weapon to curb the pandemic (44).
Conclusion
Although rarely, CV has been reported in both SARS-CoV-2 -infected and SARS-CoV-2-vaccinated patients. In many cases, these were self-limiting skin forms without systemic involvement, solved spontaneously or after systemic treatment. Studies on this topic are however important to better understand the pathogenetic mechanisms underlying their origin.
With the evolution of the infection and with the finding of less aggressive SARS-CoV-2 variants, it will be necessary to follow the patients who will develop a CV, to better define their characteristics, and possibly understand which variants are more associated with the development of CV. Moreover, the epidemiological trend of COVID-19 infection and the need to protect especially the fragile population made it necessary to start a vaccination campaign with a fourth additional dose. Therefore, careful monitoring of these patients is essential to identify the presence of CV and to make a correct diagnosis, based not only on histological examination but also on DIF, essential to better define the characteristics of SARS-CoV-2 and vaccine-related CV.
Statements
Author contributions
AV, CHS, and MC contributed to conception and design of the study. EM organized the database of cases collected. AC, EM, VR, and AV wrote the first draft of the manuscript. LQ and CA wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1.
Caproni M Verdelli A . An update on the nomenclature for cutaneous vasculitis. Curr Opin Rheumatol. (2019) 31:46–52. 10.1097/BOR.0000000000000563
2.
Jennette JC Falk RJ Bacon PA Basu N Cid MC Ferrario F et al . 2012 revised international chapel hill consensus conference nomenclature of vasculitides. Arthritis Rheum. (2013) 65:1–11. 10.1002/art.37715
3.
Sunderkötter CH Zelger B Chen KR Requena L Piette W Carlson JA et al . Nomenclature of cutaneous vasculitis: dermatologic addendum to the 2012 revised international chapel hill consensus conference nomenclature of vasculitides. Arthritis Rheumatol. (2018) 70:171–84. 10.1002/art.40375
4.
Filosa A Verdelli A Bianchi B Del Bianco E Bugatti L Filosa G et al . Cutaneous vasculitidis: histology and immunofluorescence. G Ital Dermatol Venereol. (2015) 150:183–91.
5.
Morita TCAB Criado PR Criado RFJ Trés GFS Sotto MN . Update on vasculitis: overview and relevant dermatological aspects for the clinical and histopathological diagnosis - Part II. An Bras Dermatol. (2020) 95:493–507. 10.1016/j.abd.2020.04.004
6.
Morita TCAB Trés GFS Criado RFJ Sotto MN Criado PR . Update on vasculitis: an overview and dermatological clues for clinical and histopathological diagnosis - part I. An Bras Dermatol. (2020) 95:355–71. 10.1016/j.abd.2020.01.003
7.
Lath K Chatterjee D Saikia UN Saikia B Minz R De D et al . Role of direct immunofluorescence in cutaneous small-vessel vasculitis: experience from a tertiary center. Am J Dermatopathol. (2018) 40:661–6. 10.1097/DAD.0000000000001170
8.
Nandeesh BN Tirumalae R . Direct immunofluorescence in cutaneous vasculitis: experience from a referral hospital in India. Indian J Dermatol. (2013) 58:22–5. 10.4103/0019-5154.105280
9.
Micheletti RG Werth VP . Small vessel vasculitis of the skin. Rheum Dis Clin North Am. (2015) 41:21–32. 10.1016/j.rdc.2014.09.006
10.
Antiga E Verdelli A Bonciani D Bonciolini V Quintarelli L Volpi W et al . Drug-induced cutaneous vasculitides. G Ital Dermatol Venereol. (2015) 150:203–10.
11.
Gázquez Aguilera EM Rodríguez García M Cantón Yebra MT . Cutaneous vasculitis due to COVID-19 vaccination. Med Clin. (2022) 158:493–4. 10.1016/j.medcle.2021.09.019
12.
Valero C Baldivieso-Achá JP Uriarte M Vicente-Rabaneda EF Castañeda S García-Vicuña R . Vasculitis flare after COVID-19: report of two cases in patients with preexistent controlled IgA vasculitis and review of the literature. Rheumatol Int. (2022) 42:5153. 10.1007/s00296-022-05153-w
13.
Criado PR Giordani LP Yoshimoto TA Vieira IC Landman G Pincelli TP . Vasculitis in the setting of COVID-19: From the disease to the vaccine. report of a case of cutaneous vasculitis after immunization. Dermatol Ther. (2022) 35:15367. 10.1111/dth.15367
14.
Pendlebury GA Oro P Haynes W Merideth D Bartling S Bongiorno MA . The impact of COVID-19 pandemic on dermatological conditions: a novel, comprehensive review. Dermatopathology (Basel). (2022) 9:212–43. 10.3390/dermatopathology9030027
15.
Tan SW Tam YC Oh CC . Skin manifestations of COVID-19: a worldwide review. JAAD Int. (2021) 2:119–33. 10.1016/j.jdin.2020.12.003
16.
Ehrenfeld M Tincani A Andreoli L Cattalini M Greenbaum A Kanduc D et al . Covid-19 and autoimmunity. Autoimmun Rev. (2020) 19:102597. 10.1016/j.autrev.2020.102597
17.
Dotan A Muller S Kanduc D David P Halpert G Shoenfeld Y . The SARS-CoV-2 as an instrumental trigger of autoimmunity. Autoimmun Rev. (2021) 20:15651. 10.1016/j.autrev.2021.102792
18.
shakoei S Kalantari Y Nasimi M Toutounchi NM Ansari MS Razavi Z et al . Cutaneous manifestations following COVID-19 vaccination: a report of 25 cases. Dermatol Ther. (2022) 35:15651. 10.1111/dth.15651
19.
Wollina U Schönlebe J Kodim A Hansel G . Severe leukocytoclastic vasculitis after. covid-19 vaccination - cause or coincidence? Case report and literature review. Georgian Med News [Internet]. (2022) 324:134–9.
20.
WHO Coronavirus (COVID-19) Dashboard . WHO Coronavirus (COVID-19) Dashboard With Vaccination Data. (2022). Available online at: https://covid19.who.int/ (accessed July 20, 1985).
21.
Luo X Lv M Zhang X Estill J Yang B Lei R et al . Clinical manifestations of COVID-19: an overview of 102 systematic reviews with evidence mapping. J Evid Based Med. (2022) 13:12. 10.1111/jebm.12483
22.
Purja S Oh S Kim E . A systematic review on neurological aspects of COVID-19: exploring the relationship between COVID-19-related olfactory dysfunction and neuroinvasion. Front Neurol. (2022) 13:164. 10.3389/fneur.2022.887164
23.
Guan WJ Ni ZY Hu Y Liang WH Ou C Quan H et al . Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. (2020) 382:1708–20. 10.1056/NEJMoa2002032
24.
Recalcati S . Cutaneous manifestations in COVID-19: a first perspective. J Eur Acad Dermatol Venereol. (2020) 34:e212–3. 10.1111/jdv.16387
25.
Farajzadeh S Khalili M Dehghani S Babaie S Fattah M Abtahi-Naeini B . Top 10 acral skin manifestations associated with COVID-19: a scoping review. Dermatol Ther. (2021) 34:15157. 10.1111/dth.15157
26.
Genovese G Moltrasio C Berti E Marzano AV . Skin manifestations associated with COVID-19: current knowledge and future perspectives. Dermatology. (2021) 237:1–12. 10.1159/000512932
27.
Galván Casas C Català A Carretero Hernández G Rodríguez-Jiménez P Fernández-Nieto D Rodríguez-Villa Lario A et al . Classification of the cutaneous manifestations of COVID-19: a rapid prospective nationwide consensus study in Spain with 375 cases. Br J Dermatol. (2020) 183:71–7. 10.1111/bjd.19163
28.
Carsana L Sonzogni A Nasr A Rossi RS Pellegrinelli A Zerbi P et al . Pulmonary post-mortem findings in a series of COVID-19 cases from northern Italy: a two-centre descriptive study. Lancet Infect Dis. (2020) 20:1135–40. 10.1016/S1473-3099(20)30434-5
29.
Li MY Li L Zhang Y Wang XS . Expression of the SARS-CoV-2 cell receptor gene ACE2 in a wide variety of human tissues. Infect Dis Poverty. (2020) 9:62. 10.1186/s40249-020-00662-x
30.
Gencer S Lacy M Atzler D Van Der Vorst EPC Döring Y Weber C . Immunoinflammatory, Thrombohaemostatic, and Cardiovascular Mechanisms in COVID-19. Thromb Haemost. (2020) 120:1629–41. 10.1055/s-0040-1718735
31.
Ferrario CM Jessup J Chappell MC Averill DB Brosnihan KB Tallant EA et al . Effect of angiotensin-converting enzyme inhibition and angiotensin II receptor blockers on cardiac angiotensin-converting enzyme 2. Circulation. (2005) 111:2605–10. 10.1161/CIRCULATIONAHA.104.510461
32.
Varga Z Flammer AJ Steiger P Haberecker M Andermatt R Zinkernagel AS et al . Endothelial cell infection and endotheliitis in COVID-19. Lancet. (2020) 395:1417–8. 10.1016/S0140-6736(20)30937-5
33.
Magro C Mulvey JJ Berlin D Nuovo G Salvatore S Harp J et al . Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: a report of five cases. Transl Res. (2020) 220:1–13. 10.1016/j.trsl.2020.04.007
34.
Kaya G Kaya A Saurat JH . Clinical and histopathological features and potential pathological mechanisms of skin lesions in COVID-19: review of the literature. Dermatopathology (Basel). (2020) 7:3–16. 10.3390/dermatopathology7010002
35.
Shakoor MT Birkenbach MP Lynch M . ANCA-associated vasculitis following pfizer-BioNTech COVID-19 vaccine. Am J Kidney Dis. (2021) 78:611–3. 10.1053/j.ajkd.2021.06.016
36.
Altun E Kuzucular E . Leukocytoclastic vasculitis after COVID-19 vaccination. Dermatol Ther. (2022) 35:1527. 10.1111/dth.15279
37.
Carrillo-Garcia P Sánchez-Osorio L Gómez-Pavón J . Leukocytoclastic vasculitis in possible relation to the BNT162b2 mRNA COVID-19 vaccine. J Am Geriatr Soc. (2022) 70:971–3. 10.1111/jgs.17675
38.
Colia R Rotondo C Corrado A Cantatore FP . Cutaneous vasculitis after severe acute respiratory syndrome coronavirus 2 vaccine. Rheumatol Adv Pract. (2021) 5:50. 10.1093/rap/rkab050
39.
Azzazi Y Abdelkader HA Khedr H El-Komy MHM . Extensive cutaneous leukocytoclastic vasculitis after Sinopharm vaccine: Case report and review of the literature. J Cutan Pathol. (2022) 49:14235. 10.1111/cup.14235
40.
Santonja C Heras F Núñez L Requena L . COVID-19 chilblain-like lesion: immunohistochemical demonstration of SARS-CoV-2 spike protein in blood vessel endothelium and sweat gland epithelium in a polymerase chain reaction-negative patient. Br J Dermatol. (2020) 183:778–80. 10.1111/bjd.19338
41.
Baiu DC Sandor M Hart M . CD4+ T cells sensitized by vascular smooth muscle induce vasculitis, and interferon gamma is critical for the initiation of vascular pathology. Am J Pathol. (2010) 177:3215–23. 10.2353/ajpath.2010.090985
42.
Dash S Behera B Sethy M Mishra J Garg S . COVID-19 vaccine-induced urticarial vasculitis. Dermatol Ther. (2021) 34:15093. 10.1111/dth.15093
43.
Sirufo MM Raggiunti M Magnanimi LM Ginaldi L De Martinis M . Henoch-Schönlein Purpura Following the first dose of cOVID-19 viral vector vaccine: a case report. Vaccines (Basel). (2021) 9:1078. 10.3390/vaccines9101078
44.
Kar BR Singh BSTP Mohapatra L Agrawal I . Cutaneous small-vessel vasculitis following COVID-19 vaccine. J Cosmet Dermatol. (2021) 20:3382–3. 10.1111/jocd.14452
45.
Capoferri G Daikeler T Mühleisen B Trendelenburg M Müller S . Cutaneous leukocytoclastic vasculitis secondary to COVID-19 infection leading to extensive skin necrosis. Clin Dermatol. (2022). 10.1016/j.clindermatol.2022.02.013. [Epub ahead of print].
46.
Yildirim Bay E Moustafa E Semiz Y Gündogdu O Oguz Topal I Yalçin Ö . Leukocytoclastic vasculitis secondary to COVID-19 infection presenting with inclusion bodies: a histopathological correlation. J Cosmet Dermatol. (2022) 21:27–9. 10.1111/jocd.14637
47.
Gosnell HL Grider DJ . Urticarial vasculitis: a potential signpost for multisystem inflammatory syndrome in children. J Cutan Pathol. (2022) 49:163–6. 10.1111/cup.14134
48.
Kumar G Pillai S Norwick P Bukulmez H . Leucocytoclastic vasculitis secondary to COVID-19 infection in a young child. BMJ Case Rep. (2021) 14:1–4. 10.1136/bcr-2021-242192
49.
Nassani N Sweiss N Berry JT Calhoun C Polick A Trivedi I . Leukocytoclastic Vasculitis in Cutaneous Crohn Disease in the Setting of COVID-19. Inflamm Bowel Dis. (2021) 27:E74–5. 10.1093/ibd/izab045
50.
Iraji F ., Galehdari H, Siadat AH, Bokaei Jazi S. Cutaneous leukocytoclastic vasculitis secondary to COVID-19 infection: a case report. (2021) 9:830–4. 10.1002/ccr3.3596
51.
Jedlowski PM Jedlowski MF . Coronavirus disease 2019-associated immunoglobulin A vasculitis/Henoch–Schönlein purpura: a case report and review. J Dermatol. (2022) 49:190–6. 10.1111/1346-8138.16211
52.
Gouveia PA da C Cipriano IC de Melo MAZ da Silva HTA Amorim MA de O de Sá Leitão CC et al . Exuberant bullous vasculitis associated with SARS-CoV-2 infection. IDCases. (2021) 23:e01047. 10.1016/j.idcr.2021.e01047
53.
Kösters K Schwarzer S Labuhn A Rübben A Yang S Hessler F et al . Cutaneous vasculitis in a patient with COVID-19. Open Forum Infect Dis. (2020) 7:474. 10.1093/ofid/ofaa474
54.
Gómez MC González-Cruz C Ferrer B Barberá MJ . Leucocytoclastic vasculitis in a patient with COVID-19 with positive SARS-CoV-2 PCR in skin biopsy. BMJ Case Rep. (2020) 13:238039. 10.1136/bcr-2020-238039
55.
Skroza N Bernardini N Balduzzi V Mambrin A Marchesiello A Michelini S et al . A late-onset widespread skin rash in a previous COVID-19-infected patient: viral or multidrug effect?J Eur Acad Dermatol Venereol. (2020) 34:e438–9. 10.1111/jdv.16633
56.
Nasiri S Dadkhahfar S Abasifar H Mortazavi N Gheisari M . Urticarial vasculitis in a COVID-19 recovered patient. Int J Dermatol. (2020) 59:1285–6. 10.1111/ijd.15112
57.
Caputo V Schroeder J Rongioletti F A . generalized purpuric eruption with histopathologic features of leucocytoclastic vasculitis in a patient severely ill with COVID-19. J Eur Acad Dermatol Venereol. (2020) 34:e579–81. 10.1111/jdv.16737
58.
de Perosanz-Lobo D Fernandez-Nieto D Burgos-Blasco P Selda-Enriquez G Carretero I Moreno C et al . Urticarial vasculitis in COVID-19 infection: a vasculopathy-related symptom?J Eur Acad Dermatol Venereol. (2020) 34:e566–8. 10.1111/jdv.16713
59.
Dominguez-Santas M Diaz-Guimaraens B Garcia Abellas P Moreno-Garcia del Real C Burgos-Blasco P Suarez-Valle A . Cutaneous small-vessel vasculitis associated with novel 2019 coronavirus SARS-CoV-2 infection (COVID-19). J Eur Acad Dermatol Venereol. (2020) 34:e536–7. 10.1111/jdv.16663
60.
Mayor-Ibarguren A Feito-Rodriguez M Quintana Castanedo L Ruiz-Bravo E Montero Vega D Herranz-Pinto P . Cutaneous small vessel vasculitis secondary to COVID-19 infection: a case report. J Eur Acad Dermatol Venereol. (2020) 34:e541–2. 10.1111/jdv.16670
61.
Li NL Papini AB Shao T Girard L . Immunoglobulin-A vasculitis with renal involvement in a patient with COVID-19: a case report and review of acute kidney injury related to SARS-CoV-2. Can J Kidney Health Dis. (2021) 8:1684. 10.1177/2054358121991684
62.
Sandhu S Chand S Bhatnagar A Dabas R Bhat S Kumar H et al . Possible Association Between IgA Vasculitis and COVID-19. Dermatol Ther. (2021) 34:e14551. 10.1111/dth.14551
63.
Ðordević Betetto L Luzar B Pipan Tkalec Ž Ponorac S . Cutaneous leukocytoclastic vasculitis following COVID-19 vaccination with Ad26.COV2.S vaccine: a case report and literature review. Acta Dermatovenerologica Alpina Pannonica et Adriatica. (2022) 31:83–7. 10.15570/actaapa.2022.12
64.
Fiorillo G Pancetti S Cortese A Toso F Manara S Costanzo A et al . Leukocytoclastic vasculitis (cutaneous small-vessel vasculitis) after COVID-19 vaccination. J Autoimmun. (2022) 127:102783. 10.1016/j.jaut.2021.102783
65.
Vornicu A Berechet A Fră?ilă G Obrişcă B Jurcut C Ismail G . Relapse of cryoglobulinemic vasculitis with new-onset severe renal involvement in two patients following mRNA COVID-19 vaccination: a case report. Medicine [Internet]. (2022) 101:e29431. 10.1097/MD.0000000000029431
66.
Sandhu S Bhatnagar A Kumar H Dixit PK Paliwal G Suhag DK et al . Leukocytoclastic vasculitis as a cutaneous manifestation of ChAdOx1 nCoV-19 corona virus vaccine (recombinant). Dermatol Ther. (2021) 34:15142. 10.1111/dth.15141
67.
Cohen SR Prussick L Kahn JS Gao DX Radfar A Rosmarin D . Leukocytoclastic vasculitis flare following the COVID-19 vaccine. Int J Dermatol [Internet]. (2021) 60:1032–3. 10.1111/ijd.15623
68.
Larson V Seidenberg R Caplan A Brinster NK Meehan SA Kim RH . Clinical and histopathological spectrum of delayed adverse cutaneous reactions following COVID-19 vaccination. J Cutan Pathol [Internet]. (2022) 49:34–41. 10.1111/cup.14104
69.
Bostan E Zaid F Akdogan N Gokoz O . Possible case of mRNA COVID-19 vaccine-induced small-vessel vasculitis. J Cosmet Dermatol [Internet]. (2022) 21:51–3. 10.1111/jocd.14568
70.
Gambichler T Abu Rached N Scholl L Behle B Mansour R Nick M et al . Reproducible leukocytoclastic vasculitis following severe acute respiratory syndrome coronavirus 2 vaccination. J Dermatol [Internet]. (2022) 49:145–6. 10.1111/1346-8138.16282
71.
Ireifej B Weingarten M Dhamrah U Weingarten M Hadi S . Leukocytoclastic Vasculitic Rash Following Second Dose of Moderna COVID-19 Vaccine. J Investig Med High Impact Case Rep. (2022) 10:6283. 10.1177/23247096211066283
72.
Grossman ME Appel G Little AJ Ko CJ . Post-COVID-19 vaccination IgA vasculitis in an adult. J Cutan Pathol [Internet]. (2022) 49:385–7. 10.1111/cup.14168
73.
Mücke VT Knop V Mücke MM Ochsendorf F Zeuzem S . First description of immune complex vasculitis after COVID-19 vaccination with BNT162b2: a case report. BMC Infect Dis. (2021) 21:958. 10.1186/s12879-021-06655-x
74.
Dicks AB Gray BH . Images in vascular medicine: leukocytoclastic vasculitis after COVID-19 vaccine booster. Vasc Med [Internet]. (2022) 27:100–1. 10.1177/1358863X211055507
75.
Mohamed MMB Wickman TJ Fogo AB Velez JCQ De . Novo immunoglobulin a vasculitis following exposure to SARS-CoV-2 immunization. Ochsner J [Internet]. (2021) 21:395–401. 10.31486/toj.21.0083
76.
Hines AM Murphy N Mullin C Barillas J Barrientos JC . Henoch-Schönlein purpura presenting post COVID-19 vaccination. Vaccine [Internet]. (2021) 39:4571–2. 10.1016/j.vaccine.2021.06.079
77.
Cavalli G Colafrancesco S de Luca G Rizzo N Priori R Conti F et al . Cutaneous vasculitis following COVID-19 vaccination. Lancet Rheumatol. (2021) 3:e743–4. 10.1016/S2665-9913(21)00309-X
78.
Guzmán-Pérez L Puerta-Peña M Falkenhain-López D Montero-Menárguez J Gutiérrez-Collar C Rodríguez-Peralto JL et al . Small-vessel vasculitis following Oxford-AstraZeneca vaccination against SARS-CoV-2. J Eur Acad Dermatol Venereol. (2021) 35:e741–3. 10.1111/jdv.17547
79.
Shahrigharahkoshan S Gagnon LP Mathieu S . Cutaneous leukocytoclastic vasculitis induction following ChAdOx1 nCoV-19 vaccine. Cureus. (2021) 13:19005. 10.7759/cureus.19005
80.
Jin WJ Ahn SW Jang SH Hong SM Seol JE Kim H . Leukocytoclastic vasculitis after coronavirus disease 2019 vaccination. J Dermatol. (2022) 49:e34–5. 10.1111/1346-8138.16212
81.
Fritzen M Funchal GDG Luiz MO Durigon GS . Leukocytoclastic vasculitis after exposure to COVID-19 vaccine. An Bras Dermatol. (2022) 97:118–21. 10.1016/j.abd.2021.09.003
82.
Kharkar V Vishwanath T Mahajan S Joshi R Gole P . Asymmetrical cutaneous vasculitis following COVID-19 vaccination with unusual eosinophil preponderance. Clin Exp Dermatol. (2021) 46:1596–7. 10.1111/ced.14797
83.
Oskay T Isik M . Leukocytoclastic vasculitis after the third dose of CoronaVac vaccination. Clin Rheumatol. (2022) 41:1931–3. 10.1007/s10067-021-05993-0
84.
Bostan E Gulseren D Gokoz O . New-onset leukocytoclastic vasculitis after COVID-19 vaccine. Int J Dermatol. (2021) 60:1305–6. 10.1111/ijd.15777
85.
Erler A Fiedler J Koch A Heldmann F Schütz A . Leukocytoclastic vasculitis after vaccination with a SARS-CoV-2 vaccine. Arthritis Rheumatol [Internet]. (2021) 73:2188. 10.1002/art.41910
86.
Bencharattanaphakhi R Rerknimitr P . Sinovac COVID-19 vaccine-induced cutaneous leukocytoclastic vasculitis. JAAD Case Rep. (2021) 18:1–3. 10.1016/j.jdcr.2021.10.002
Summary
Keywords
vasculitis, cutaneous vasculitis, COVID-19, leukocytoclastic vasculitis, IgA vasculitis, urticarial vasculitis, COVID-19 vaccines, vaccine-induced vasculitis
Citation
Corrà A, Verdelli A, Mariotti EB, Ruffo di Calabria V, Quintarelli L, Aimo C, Sunderkötter CH and Caproni M (2022) Cutaneous vasculitis: Lessons from COVID-19 and COVID-19 vaccination. Front. Med. 9:1013846. doi: 10.3389/fmed.2022.1013846
Received
07 August 2022
Accepted
28 October 2022
Published
09 December 2022
Volume
9 - 2022
Edited by
Giusto Trevisan, University of Trieste, Italy
Reviewed by
Sebastiano Recalcati, Alessandro Manzoni Hospital, Italy
Updates
Copyright
© 2022 Corrà, Verdelli, Mariotti, Ruffo di Calabria, Quintarelli, Aimo, Sunderkötter and Caproni.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marzia Caproni marzia.caproni@unifi.it; alberto.corra@unifi.it
†These authors have contributed equally to this work and share first authorship
This article was submitted to Dermatology, a section of the journal Frontiers in Medicine
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.