Abstract
Purpose:
What constitutes the optimal surgical plan for femoral neck fractures (FNFs) in elderly patients is controversial. The European quality of life 5-Dimension Questionnaire (EU-5Q) is an international scale used to measure the health-related quality of life (HRQoL) after surgery. We aim to verify the hip arthroplasty effect in elderly patients by analyzing HRQoL scores in the EU-5Q scale.
Methods:
We searched the EBSCO, Embase, PubMed, Ovid, Cochrane Library, and Web of Science databases using strict searching from established to 30 November 2022; used the Cochrane Library's Risk of Bias Assessment Tool and the Newcastle–Ottawa Scale to evaluate the literature; and used RevMan5.4.1 software to perform a meta-analysis. All the included studies used the EU-5Q scale to validate the overall outcomes for elderly hip arthroplasty.
Results:
The final included literature is composed of four RCTs, two cohort studies, three case–control trials, and three cross-sectional surveys. This study compared HRQoL scores measured by the EU-5Q scale, including 328 elderly patients with total hip arthroplasty (THA) and 323 elderly patients with hemiarthroplasty, which is statistically significant (OR = 0.05; 95% CI, 0.02~0.08; P = 0.002). The subgroups were as follows: unipolar vs. bipolar and cemented vs. uncemented hemiarthroplasty (OR = 0.06; 95% CI, 0.03~0.08; P < 0.001), follow-up time and age arthroplasty (OR = 0.16; 95% CI, 0.11~0.22; P < 0.001), molecular exercise and enhanced recovery after surgery (ERAS) (OR = 0.02; 95% CI,−0.03~0.07; P = 0.38), and analysis of hemiarthroplasty with cognitive dysfunction vs. the normal group (OR = 0.17; 95% CI, 0.08~0.26; P < 0.001). The outcome analysis was consistent with the included studies, and HRQoL of the EU-5Q scale is sensitive to surgical outcomes between THA and hemiarthroplasty.
Conclusion:
Surgeons still need to further evaluate and verify whether the hip arthroplasty surgical program or effect in elderly patients is optimal. Hemiarthroplasty operations in elderly patients have pointed toward a new direction for clinical treatment, and HRQoL scores measured by the EU-5Q can sensitively reflect the rehabilitation status after hip arthroplasty surgery. Moreover, the extensive correlation between surgical outcomes and perioperative neurocognitive function should be further investigated.
Introduction
The number of femoral neck fractures (FNFs) in the elderly population has been increasing drastically in the last few decades, and it will be 6.3 million by 2050 (1). The growing number of FNFs places a heavy burden on the health-related quality of life (HRQoL) of the global healthcare system (2). As the number of elderly patients with FNFs increases with the global aging trend, this study aims to analyze the differences in HRQoL scores between posterior femoral neck surgery in elderly patients, aiming to provide a basis for selecting optimal surgically effective nursing interventions. In order to improve the mobility and satisfaction of patients with FNFs, we should make great efforts in perioperative training and management (1, 3). In fact, the activity of daily living (ADL) and HRQoL, as well as mobility, pain, mortality, and neurocognitive function are more closely related to the surgical effect (4). The results of five RCTs of THA vs. hemiarthroplasty in elderly patients showed that postoperative dislocation of THA was higher than in the hemiarthroplasty group, and during the 1 and 2-year follow-up time, the incidence of THA reoperation was also higher, but the incidence of other complications such as pneumonia, hematoma, arrhythmia, congestive heart failure, deep vein thrombosis was lower than hemiarthroplasty (4). Consequently, we analyzed the applicable literature on HRQoL in elderly patients with THA and hemiarthroplasty, aiming to improve hip arthroplasty rehabilitation in elderly patients with FNFs.
The European quality of life 5-Dimension Questionnaire (EU-5Q) scale is responsive to the changes in HRQoL scores, including persons with cognitive impairment, and the EU-5Q has advantages in the setting items for postoperative follow-up (5, 6). It includes a visual analog pain assessment tool and an HRQoL assessment tool with five dimensions, namely, mobility, self-care, activities of daily living, pain or discomfort, and anxiety or depression (7). It is widely used and has been proven to have good reliability, validity, and sensitivity in a variety of populations (8).
In recent years, research on functional reporting and outcome variables of elderly hip arthroplasty surgery has become more and more popular, for example, the enhanced recovery after surgery (ERAS) protocols, which involved surgeons, nurses, dietitians, etc., are designed to facilitate the speed of recovery, decrease the patients cost, improve the medical quality, etc. (9). Then, there are many imaging and functional outcome assessment methods and indicators for the prognosis, but there are few articles about the HRQoL evaluation of EU-5Q for elderly hip arthroplasty. The future of medical science is not only to treat diseases but also to pay more attention to the patient's overall health (10). The EU-5Q questionnaire is an international evaluation tool to effectively evaluate the surgery outcome. It provides the best treatment plan and nursing measures for elderly patients with FNFs by performing the positive reflection of the surgical effect measured by the EU-5Q scale. It uses the HRQoL score of elderly hip arthroplasty as the outcome index. First, it reflects the comparison of THA and hemiarthroplasty surgery. Second, it reflects that the EU-5Q scale can effectively measure the HRQoL status after hip arthroplasty in elderly patients. Moreover, in future research, from the comparison of the HRQoL scores, we can find out the health deficiencies of these elderly patients, which is convenient for clinical symptomatic treatment and nursing.
Materials and methods
Inclusion and exclusion criteria
Inclusion criteria: (1) age ≥ 60 years; (2) no ethnic and geographical restrictions; (3) HRQoL score measured by EU-5Q is the outcome evaluation indicator; (4) RCT, case–control trials, high-quality original literature of cohort studies and cross-sectional survey.
Exclusion criteria: (1) animal experiments, uncontrolled trials, case reports, and reviews; (2) the inclusion and exclusion criteria for the study were not clear or reasonable; (3) the full text could not be obtained or the original data were incomplete.
Search strategy
We searched online medical databases, including Ebsco, Embase, PubMed, Ovid, Cochrane Library, and Web of Science databases. We built a study library through screening clinical trials and original data research that met the inclusion and exclusion criteria. The databases were established until 30 November 2022. We used the following keywords: geriatric, elderly, femoral neck fractures, hip, joint replacement, total hip replacement, hemi-hip replacement, femoral head replacement, total hip arthroplasty, hemiarthroplasty, health-related quality of life, quality of life, nursing outcomes, surgical outcomes, etc. We used MeSH Terms in the four databases EBSCO, PubMed, Cochrane Library and Web of Science. All searches used the PICO principle under evidence-based nursing. This method used a broad search strategy: (elderly AND femoral neck fracture* AND (“total hip arthroplasty” OR hemiarthroplasty) AND “health related quality of life”). We performed a snowball search of the included studies according to the PRISMA guidelines and the screening studies process is shown in Figure 1.
Figure 1

PRISMA flow diagram of screening studies process.
Study selection
We got 178 pieces of literature. This was achieved by screening the article title and abstract and through full-text reading. Finally, 12 articles fit the theme. There were four RCTs, three cross-sectional studies, two cohort studies, and three case–control trials.
Characteristics of the included studies
The baseline data of the 12 included studies are shown in Table 1. They include four comparisons of HRQoL in elderly patients after THA and hemiarthroplasty surgery (11, 13, 17, 18), and the others were on the assessment of HRQoL after hemiarthroplasty in elderly patients with different interventions (1–4, 12, 14–16). We analyzed two of the four RCT studies to compare the scores of HRQoL between elderly patients with THA and patients with hemiarthroplasty (Figure 4) (11, 13). The other two RCT studies are about the outcomes of hemiarthroplasty under different interventions, and we created subgroups to analyze the HRQoL scores (Figure 5A) (2, 12). A subgroup of cross-sectional surveys is shown in Figure 5B (3, 18), a subgroup of case–control trials is shown in Figure 5C (1, 14), and a subgroup of cohort studies is shown in Figure 5D (15, 16).
Table 1
| Author Year | Country | Study type | Patients number | Survey | Follow-up | Intervention | Case and control |
|---|---|---|---|---|---|---|---|
| Hedbeck et al. (11) | Sweden | RCT | 120 | / | 1, 2, 4years | / | THA vs. Hemiarthroplasty |
| Hedbeck et al. (12) | Sweden | RCT | 120 | / | 4, 12months | / | Unipolar Hemiarthroplasty vs. Bipolar Hemiarthroplasty |
| Sköldenberg et al. (13) | Sweden | RCT | 120 | / | 3months, 1, 2, 4years | / | THA vs. Hemiarthroplasty |
| Solarino et al. (1) | Italy | CC | 118 | January 2016 to June 2017 | 1, 3, 6months, 1, 2years | Molecular neck | Senior orthopedic surgeons vs. Orthopedic residents |
| Tian et al. (14) | China | CC | 92 | July to December, 2018 | 1, 3months | ERAS | Hemiarthroplasty |
| Wang et al. (4) | China | CC | 226 | 2015 to 2019 | 24~78months | / | THA vs. Hemiarthroplasty with neuromuscular imbalance |
| Chammout et al. (15) | Sweden | CS | 98 | / | 3months, 1year | / | Primary Hemiarthroplasty with cognitive dysfunction |
| Sebastian et al. (16) | Sweden | CS | 188 | February 2012 to July 2014 |
1year | / | Hemiarthroplasty vs. cognitive impairment Hemiarthroplasty |
| Pass et al. (3) | Germany | CSS | 4662 | 2016 to 2018 | 7, 120days | / | THA vs. Hemiarthroplasty |
| Gjertsen et al. (17) | Norway | CSS | 10325 | 2005 to 2012 | 4, 12months | / | THA vs. Hemiarthroplasty |
| Leonardsson et al. (18) | Sweden | CSS | 5902 | August 15 to October 25, 2010 | 7~24months | / | THA vs. Hemiarthroplasty |
| Fernandez et al. (2) | England | RCT | 1225 | / | 4months | / | Cemented vs. uncemented Hemiarthroplasty |
Baseline data and quality evaluation of the 12 included articles.
RCT, randomized controlled trial; CC, case control trial; CS, cohort study; CSS, cross-sectional study; THA, total hip arthroplasty; ERAS, enhanced recovery after surgery.
Data extraction and evaluation of evidence
Two researchers independently evaluated the included 12 articles, and they discussed or asked a third senior professional expert to give a suggestion when there was any doubt about the quality evaluation. Data from the included literature were organized and entered into the software RevMan 5.4.1 by two independent researchers.
The cross-sectional survey was evaluated using the American Health Care Quality and Research Institutions Evaluation Tool, the quality of case–control and cohort studies was evaluated by the Newcastle–Ottawa evaluation tool, and the quality evaluation of RCTs was performed by the risk of bias assessment tool from the Cochrane Library.
Outcome measures
The health-related quality of life (HRQoL) scale is assessed using the EU-5Q scale, and this includes five dimensions, namely, mobility, self-care ability, daily activities (such as work, study, housework, and leisure activities), pain or discomfort, and anxiety or depression. The data that we collected included dichotomous variables from the five EU-5Q dimensions as well as continuous variables for the mean and standard deviation of HRQoL and interquartile range for the overall patient population. We aggregated and analyzed different types of variables separately. Furthermore, it also extracted monitoring data on nursing outcomes and rehabilitation effects, and the EU-5Q scale includes both physiological structure and functional testing evaluation. Items can also effectively assess the mental health status of elderly patients, which is helpful for us to identify the problem and then treat it symptomatically. The HRQoL scores of patients after 1 month of prognosis were significantly higher than pre-operation, but they began to decline at 12 months after operation (11, 12, 16). Therefore, more problems are reported after intertrochanteric fractures than basal-type fractures and intracapsular femoral fractures, it is a key issue for surgeons to carefully consider the choice of prosthesis type (17).
Statistical analysis
The Mantel–Haenszel model and odds ratios (ORs) with 95% confidence intervals (95% CIs) for outcomes were used to compare dichotomous variables. Mean and standard deviation were used for analysis when the units of continuous variables were consistent. A P < 0.05 was considered statistically significant. Statistical heterogeneity between trials was evaluated using the I2 test. Heterogeneity was considered when I2 > 50% and P ≤ 0.100. Then, the source of heterogeneity was analyzed, and the random effects model was used for meta-analysis. When I2 ≤ 50% and P > 0.100, there was no heterogeneity, and the fixed effects model was used for meta-analysis. The aforementioned statistical values were calculated using the statistical method provided by the RevMan 5.4.1 software.
Risk of bias in the included studies
Random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, and selective reporting were evaluated as the study bias according to the Cochrane Handbook of Systematic Review (19). A risk-of-bias graph and risk-of-bias summary generated by RevMan 5.4.1 software are shown in Figures 2, 3, respectively.
Figure 2

Risk of bias graph of included studies.
Figure 3

Risk of bias summary of included studies.
Meta-analysis outcomes
Scores of EU-5Q between hip arthroplasty
There are two types of RCT literature on the comparison of HRQoL assessment after THA and hemiarthroplasty in elderly patients. The HRQoL scores of THA are higher than hemiarthroplasty. THA is the preferred surgical method for elderly patients with FNFs, its mobility and self-care ability, as well as psychological status are better than hemiarthroplasty surgery. The outcomes are shown in Figure 4, which is consistent with the result of another case–control study comparing THA and hemiarthroplasty (4).
Figure 4
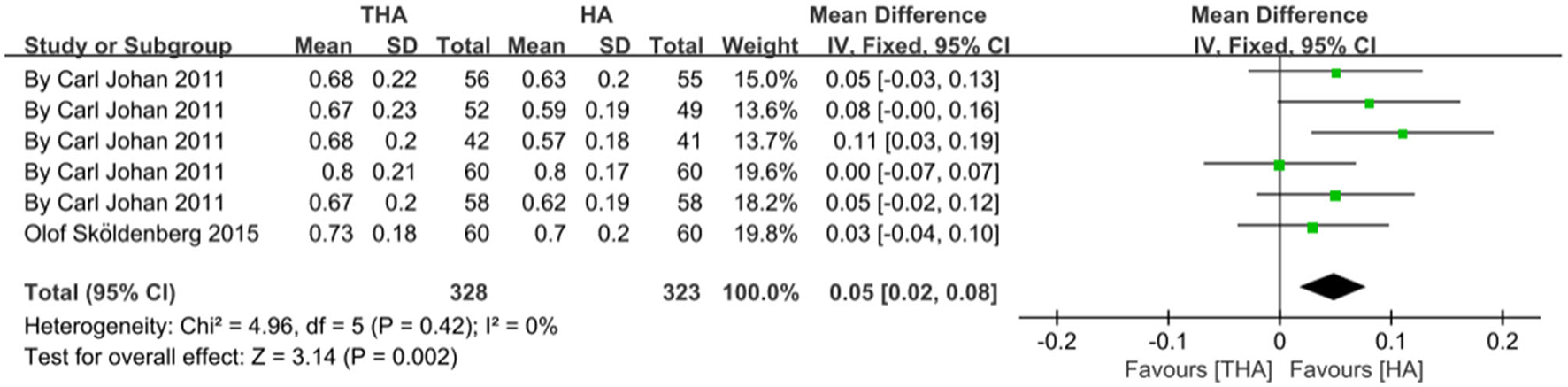
Forest plot depicting the relationship of health-related quality of life between THA and HA.
Scores of EU-5Q under hemiarthroplasty
The EU-5Q scores improved the HRQoL of hemiarthroplasty surgery in elderly patients, such as ERAS concept, neurocognitive, and different prosthesis-type interventions. As shown in Figure 5, we performed a meta-integration by literature study type and performed a subgroup analysis under different interventions. Hedbeck published an RCT of a unipolar/bipolar femoral head and Fernandez published an RCT of cemented/uncemented prostheses in elderly patients (2, 11). After integrating these two studies, we found that the HRQoL score after interventions was significantly superior to the control group (P < 0.01). Figure 5A shows the OR value is 0.06, 95% CI [0.03, 0.08]. This demonstrates that the EU-5Q scale could assess differences in HRQoL (12, 20). The pass has performed a retrospective analysis from the Geriatric Trauma Center Registry, there was no statistically significant difference in HRQoL scores between 1 week and 3 months after surgery, but clinical scores increased with time, and it is certain that the 3-month HRQoL average level was >1 week (Figure 5B) (3). Similarly, Tian performed the concept of ERAS on elderly patients with hemiarthroplasty. After 1 and 3 months of follow-up times, the HRQoL scores increased, but the difference between the two time periods was not statistically significant (Figure 5C) (14). However, in Chammout's prospective cohort study, there were statistically significant differences (P = 0.02) in HRQoL scores at 3 and 12 months after surgery (Figure 5D) (15). As shown in Figure 5B, Leonardsson followed 14 months of THA and hemiarthroplasty surgery for displaced FNFs in different age groups in elderly patients, and HRQoL scores were statistically significant (P < 0.001) (18). In a word, the HRQoL score after hip arthroplasty for elderly patients with FNFs should have shown rapid recovery in the first 6 months or first year, during which time the incidence of complications is higher (21).
Figure 5

(A–D) Forest plot depicting.
Publication bias
Solarino evaluated HRQoL in the elderly after 2 years, and the outcomes were not statistically significant, possibly owing to their telephone interview methods. The online telephone method perhaps neglected some important indicators, especially the patient's neurocognitive status motoring self-control and the ability to cooperate in physiotherapy treatment (1). The HRQoL scores of the observation group were dominant, and the results were statistically different. Results from both cohort studies and RCT studies were statistically significant. The bias published in this meta-analysis can be ignored. Moreover, the differences in HRQoL scores after intervention need to be verified in a multi-center, large-sample RCT that can refer to this research design (2).
Discussion
Studies have shown that the postoperative outcomes of elderly patients with hip arthroplasty are affected by a variety of factors, the physical quality of patients, and rehabilitation nursing measures are positively correlated with the prognosis of patients (22). They assessed prognosis status by the EU-5Q (22).
Influencing factors of medical level
The development of the medical level has promoted the improvement of medical quality. Analyzing these studies is the key to improving the hip arthroplasty quality of elderly patients and is also an important part of patients' surgical expectations. Although HRQoL in THA has obvious advantages, it still has obvious defects, which are worthy of further in-depth discussion and scientific and reasonable clinical research in the future (23, 24). Perhaps it is inconclusive about the best surgical method for elderly patients with FNFs. This is an effective surgical program that needs to consider comprehensively the patients' basic physical conditions (comorbidity index, frailty index, etc.) to choose the optimal treatment and nursing measures. Modular surgical training residents can help them efficiently restore femoral offset and balance damaged soft tissue, reducing the incidence of postoperative abductor imbalance, hip pain, and acetabular wear (1). Its dislocation rate of THA is higher than hemiarthroplasty and internal fixation; however, there is still controversy about the dislocation rate of THA in elderly patients (25, 26). Although unstable elderly patients with FNFs are mostly treated with THA surgery, internal fixation, hemiarthroplasty surgery are recommended for stable FNFs (27).
Wang found that THA was associated with better functional outcomes, quality of life, and lower pain intensities, despite longer operation times and higher intraoperative blood loss (4). This is consistent with the findings of Yu et al. (25) and Hopley et al. (26). The evaluation of HRQoL in elderly patients with FNFs is associated with the outcome of THA and hemiarthroplasty operation. Younger orthopedic residents should gain more experience working with elderly patients with FNFs under supervision from senior orthopedic surgeons to acquire proficient skills for hip arthroplasty operations (1). Simultaneously, orthopedic nurses need continuing education about hip arthroplasty perioperative management. The first thing that orthopedic surgeons think about is the surgical effect of THA and hemiarthroplasty, such as the functional recovery benefits and pain alleviation after the surgery (28). THA surgery has obvious advantages in terms of prognosis. What constitutes the optimal surgical program for elderly FNFs has been controversial (23). We do not dismiss that hemiarthroplasty is generally recognized by physicians and patients, and we have thus integrated studies on HRQoL with hemiarthroplasty in elderly patients with FNFs and found favorable and unfavorable factors affecting patients' recovery. One study of a 4-year follow-up between THA and hemiarthroplasty showed significant differences in HRQoL scores, measured by EU-5Q, with THA superior to hemiarthroplasty after 48 months (P < 0.039) (11). The findings demonstrated that rapid rehabilitation interventions, modular training of residents, and choice of prosthesis type all contribute to improving HRQoL scores after hemiarthroplasty in elderly patients, both in medical education and in future clinical practice. The improvement of the management concept is effective for elderly surgical rehabilitation.
Influencing factors from patients
As we age, various physiological functions of the human body decline, and this is closely related to the rehabilitation effect (18). However, HRQoL scores of elderly patients with hip arthroplasty are statistically different with age, and there is a clinically significant difference in the prognosis after 1 year of follow-up. Therefore, age is an independent risk factor affecting the surgical effect. Moreover, the most important thing is that clinicians should not only use age as an important reference for performing surgical programs but also need to consider physiological factors (29). There are significant statistical differences in the HRQoL scores, such as drawing the line between 70 and 80 years (17). The funnel plot shows the heterogeneity of retrospective case–control trials of neuromuscular imbalances, suggesting that elderly THA with neuromuscular disease were also reported to be superior to a hemiarthroplasty, they were superior to patient rehabilitation in reasons of EU-5Q evaluation, hemiarthroplasty is a safe and available treatment option for elderly patients with FNFs, but its clinical outcomes are a little poor (risk of dislocation and prosthetic fracture), and it is urgent to explore the optimal rehabilitation care plan for such disorders (23). As is well known, age was an important factor influencing the recovery of HRQoL after hip arthroplasty with FNFs in elderly patients, mobility recovery becomes slower and slower with aging. Supplementally, the ERAS nursing intervention improved HRQoL scores after hemiarthroplasty surgery in elderly patients with FNFs. In the perioperative nursing process, we can integrate systematic nursing routines or emergency plans to improve the elderly hip arthroplasty quality.
Neurocognitive function during the perioperative period is highly related to surgery outcomes, surgeons should take into account the elderly patients' cognitive function whose risk factors may refer to neurocognitive complications, such as perioperative neurocognitive disorders (30, 31). Thus, further study is needed on the subject of the correlation between elderly cognitive function and perioperative medical quality; for example, there was a study indicating that neuropsychiatric disease occurred subsequently after cobalt and chromium metallosis following metal-on-metal implant failure (32). It is recommended to carry out future follow-up trials of more than half a year can identify the main clinical factors that affect the recovery of HRQoL (15).
Rehabilitation factors
The success of hip arthroplasty in elderly patients is the first key link with patients' rehabilitation. Postoperative rehabilitation and nursing measures are the most important factors. Moreover, HRQoL scores after hip arthroplasty for elderly patients with FNFs have accelerated recovery in the first 6 months (21), and the dislocation rate is 2.7 times higher in the first year of follow-up time (24). For elderly patients with hip arthroplasty, it is relatively difficult to implement postoperative nursing interventions and promote the rehabilitation process due to the existence of objective factors such as hearing loss, poor understanding ability, and poor compliance (33). The medical staff needs more patience, carefulness, love, and responsibility to provide medical services for elderly patients with hip arthroplasty. Preoperative preparation, intraoperative care, and postoperative observation are the three most critical stages for elderly patients with hip arthroplasty.
Enhanced recovery after surgery (ERAS) nursing speeds up the rehabilitation process, shortens the hospital stay time, reduces hospitalization cost, improves patient satisfaction, and increases the operation rate within 48 h. In addition, the HRQoL score shows a statistically significant difference, and the EU-5Q scale is a promoting factor for the prognosis (14). The utility scores on the EU-5Q questionnaire in the THA group, bipolar hemiarthroplasty group, cemented group, and senior surgeons group would be modestly but significantly better than the control group in these included studies. The THA surgery plan, type of bipolar prosthesis, type cemented, and highly qualified surgeons are protective factors for elderly FNFs surgery. All of the above provides a scientific basis for the FNFs treatment. Neuromuscular imbalance (stroke, Parkinson's disease, etc.) and cognitive impairment are impediments to FNFs surgery in elderly patients, and patients have poor postoperative HRQoL scores, but hemiarthroplasty surgery can be considered a safer option. In view of the low OR value between the THA and hemiarthroplasty groups, in addition to the EU-5Q questionnaire, the five dimensions of the scale can be evaluated separately, both of which can sensitively prove the advantage of surgical outcome variables (17).
Conclusion
In this study, although there is more prior evidence about THA surgery, hemiarthroplasty also has good functional rehabilitation. Consequently, this points to new directions for the treatment and nursing of elderly femoral neck fractures with cognitive or mobility impairment. In the future, the correlation between surgical treatment outcomes and preoperative and postoperative neurocognitive degradation in elderly patients with FNFs should be further investigated.
The findings demonstrated that hip arthroplasty intervention should be implemented in 6 months because there is a significant statistical difference in the HRQoL score during this period. Moreover, it is effective for rapid elderly surgical rehabilitation including modular training of residents, prosthesis type, and improvement of management concept.
Limitation
The influence of the patient's neurocognitive status in physiotherapy treatment should be deepened. Most important of all, the study of the correlation between surgical treatment outcomes and preoperative and postoperative neurocognitive degradation in elderly patients should be further investigated. Moreover, elderly people with obesity after hip surgery, the mood variables, the society supporting system, etc. all should be associated with exploring its effects after surgery, and the beneficial measurement questionnaire can support effective interventions for elderly patients with hip arthroplasty.
Statements
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
RL conceived and designed the framework of the article. YS and XR searched and screened the literature, evaluated the quality of the included articles, completed the manuscript with the help of RL, and consulted YW and LH when there was doubt. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the 2020 Undergraduate Teaching Reform Research and Practice Project of Henan University Reform and Practice of Innovative Talent Training Mode for Elderly Nursing Professionals No. (HDXJJG2020-09) and Research and Practice Project of Higher Education Teaching Reform in Henan Province “Research on the reform and practice of the training model of innovative elderly nursing professionals” No. (2021SJGLX333).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1.
Solarino G Moretti L Vicenti G Bizzoca D Piazzolla A Moretti B . Hip hemiarthroplasty with modular neck: Is it useful in residents' learning curve? A prospective clinical trial. Hip Int. (2020) 30:30–6. 10.1177/1120700020964988
2.
Fernandez MA Achten J Parsons N Griffin XL Png M-E Gould J et al . Cemented or uncemented hemiarthroplasty for intracapsular hip fracture. N Engl J Med. (2022) 386:521–30. 10.1056/NEJMoa2108337
3.
Pass B Nowak L Eschbach D Volland R Knauf T Knobe M et al . Differences of hemiarthroplasty and total hip replacement in orthogeriatric treated elderly patients: a retrospective analysis of the registry for geriatric trauma dgu(®). Eur J Trauma Emerg Surg. (2022) 48:1841–50. 10.1007/s00068-020-01559-y
4.
Wang Y Deng X Wang Z Zhu Y Chen W Zhang Y . Total hip arthroplasty or hemiarthroplasty for femoral neck fractures in elderly patients with neuromuscular imbalance. Aging Clin Exp Res. (2021). 10.1007/s40520-021-01976-y
5.
van Hout B Janssen MF Feng Y-S Kohlmann T Busschbach J Golicki D et al . Interim scoring for the eq-5d-5l: mapping the eq-5d-5l to eq-5d-3l value sets. Value Health. (2012) 15:708–15. 10.1016/j.jval.2012.02.008
6.
Parsons N Griffin XL Achten J Costa ML . Outcome assessment after hip fracture: is eq-5d the answer?Bone Joint Res. (2014) 3:69–75. 10.1302/2046-3758.33.2000250
7.
Bhandari M Einhorn TA Guyatt G Schemitsch EH Zura RD Sprague S et al . Total hip arthroplasty or hemiarthroplasty for hip fracture. N Engl J Med. (2019) 381:2199–208. 10.1056/NEJMoa1906190
8.
Parsons N Griffin XL Achten J Chesser TJ Lamb SE Costa ML . Modelling and estimation of health-related quality of life after hip fracture: a re-analysis of data from a prospective cohort study. Bone Joint Res. (2018) 7:1–5. 10.1302/2046-3758.71.BJR-2017-0199
9.
Pujic B Kendrisic M Shotwell M Shi Y Baysinger CL . A survey of enhanced recovery after surgery protocols for cesarean delivery in serbia. Front Med. (2018) 5:100. 10.3389/fmed.2018.00100
10.
Kumar P Sen RK Aggarwal S Jindal K Rajnish RK . Assessment and reliability of the world health organisation quality of life (WHO QOL-BREF) questionnaire in total hip replacement patients. J Clin Orthop Trauma. (2020) 11:S756–S59. 10.1016/j.jcot.2020.07.020
11.
Hedbeck CJ Enocson A Lapidus G Blomfeldt R Törnkvist H Ponzer S et al . Comparison of bipolar hemiarthroplasty with total hip arthroplasty for displaced femoral neck fractures: a concise four-year follow-up of a randomized trial. J Bone Joint Surg Am. (2011) 93:445–50. 10.2106/JBJS.J.00474
12.
Hedbeck CJ Blomfeldt R Lapidus G Törnkvist H Ponzer S Tidermark J . Unipolar hemiarthroplasty versus bipolar hemiarthroplasty in the most elderly patients with displaced femoral neck fractures: a randomised, controlled trial. Int Orthop. (2011) 35:1703–11. 10.1007/s00264-011-1213-y
13.
Sköldenberg O Chammout G Mukka S Muren O Nåsell H Hedbeck CJ et al . Hope-trial: hemiarthroplasty compared to total hip arthroplasty for displaced femoral neck fractures in the elderly-elderly, a randomized controlled trial. BMC Musculoskelet Disord. (2015) 16:3. 10.1186/s12891-015-0763-3
14.
Tian ZZ Pang D Liu HN Zhou L Zheng YY . Effect of enhanced recovery after surgery for elderly patients with hemiarthroplasty for the treatment of femoral neck fracture. Zhonghua Yi Xue Za Zhi. (2020) 100:2903–07. 10.3760/cma.j.cn112137-20200308-00647
15.
Chammout G Kelly-Pettersson P Hedbeck CJ Bodén H Stark A Mukka S et al . Primary hemiarthroplasty for the elderly patient with cognitive dysfunction and a displaced femoral neck fracture: a prospective, observational cohort study. Aging Clin Exp Res. (2021) 33:1275–83. 10.1007/s40520-020-01651-8
16.
Mukka S Knutsson B Krupic F Sayed-Noor AS . The influence of cognitive status on outcome and walking ability after hemiarthroplasty for femoral neck fracture: a prospective cohort study. Eur J Orthop Surg Traumatol. (2017) 27:653–58. 10.1007/s00590-016-1873-9
17.
Gjertsen JE Baste V Fevang JM Furnes O Engesaeter LB . Quality of life following hip fractures: results from the norwegian hip fracture register. BMC Musculoskelet Disord. (2016) 17:265. 10.1186/s12891-016-1111-y
18.
Leonardsson O Rolfson O Hommel A Garellick G Akesson K Rogmark C . Patient-reported outcome after displaced femoral neck fracture a national survey of 4467 patients. J Bone Joint Surg. (2013) 95:1693–99. 10.2106/JBJS.L.00836
19.
Higgins JPT, Jacqueline, C, Miranda, C, Tianjing, L, Matthew, P, Welch, V, . Cochrane Handbook for Systematic Reviews of Interventions, Version 6.3.0. The Cochrane Collaboration (2022). Available online at: https://training.cochrane.org/handbook/current
20.
Beauchamp-Chalifour P Pelet S Belhumeur V Angers-Goulet M Bédard L Belzile EL . Should we use bipolar hemiarthroplasty in patients ≥70 years old with a femoral neck fracture? A review of literature and meta-analysis of randomized controlled trials. J Arthroplasty. (2022) 37:601–08. 10.1016/j.arth.2021.12.004
21.
Liu Y Chen X Zhang P Jiang B . Comparing total hip arthroplasty and hemiarthroplasty for the treatment of displaced femoral neck fracture in the active elderly over 75 years old: A systematic review and meta-analysis of randomized control trials. J Orthop Surg Res. (2020) 15:215. 10.1186/s13018-020-01725-3
22.
Blom AW Hunt LP Matharu GS Reed MR Whitehouse MR . The effect of surgical approach in total hip replacement on outcomes: An analysis of 723,904 elective operations from the national joint registry for england, wales, northern ireland and the isle of man. BMC Med. (2020) 18:242. 10.1186/s12916-020-01672-0
23.
Metcalfe D Judge A Perry DC Gabbe B Zogg C Costa ML . Total hip arthroplasty versus hemiarthroplasty for independently mobile older adults with intracapsular hip fractures. BMC Musculoskelet Disord. (2019) 20:4. 10.1186/s12891-019-2590-4
24.
Blanco JF da Casa C Fidalgo H García-Iglesias MA González-García L Burón-Álvarez I et al . Effect of hip hemiarthroplasty dislocation on mortality after hip fracture surgery. Rev Esp Cir Ortop Traumatol. (2023) 67:6. 10.1016/j.recot.2022.08.006
25.
Yu L Wang Y Chen J . Total hip arthroplasty versus hemiarthroplasty for displaced femoral neck fractures: Meta-analysis of randomized trials. Clin Orthop Relat Res. (2012) 470:2235–43. 10.1007/s11999-012-2293-8
26.
Hopley C Stengel D Ekkernkamp A Wich M . Primary total hip arthroplasty versus hemiarthroplasty for displaced intracapsular hip fractures in older patients: systematic review. BMJ. (2010) 340:c2332. 10.1136/bmj.c2332
27.
Afaq S Hara NN Schemitsch EH Bzovsky S Sprague S Poolman RW et al . Arthroplasty versus internal fixation for the treatment of undisplaced femoral neck fractures: a retrospective cohort study. J Orthop Trauma. (2020) 34:S9. 10.1097/BOT.0000000000001940
28.
Valcarenghi J Martinov S Chahidi E Jennart H Bui Quoc E Dimanche MC et al . Hip fractures re-operation compared with death at two year in elderly patients: Lowest risk of revision with dual mobility total hip arthroplasty than with bipolar hemiarthroplasty or internal fixation of garden i and ii. Int Orthop. (2022) 46:1945–53. 10.1007/s00264-022-05479-x
29.
Ayers DC Yousef M Zheng H Yang W Franklin PD . Do patient outcomes vary by patient age following primary total hip arthroplasty?J Arthroplasty. (2022) 37:S510–S16. 10.1016/j.arth.2022.03.032
30.
Wang R Gao R Xie X Chen H Zhao Q Zhang X et al . Perioperative platelet count in peripheral blood is associated with the early stage of pnd after major orthopedic surgery: a prospective observational study. BMC Geriatr. (2022) 22:200. 10.1186/s12877-022-02899-7
31.
Edusei E Kim KY Anoushiravani AA Yu S Steiger D Slover JD . Prevalence of neurocognitive dysfunction and its effects on postoperative outcomes in total joint arthroplasty. J Arthroplasty. (2018) 33:350–54. 10.1016/j.arth.2017.09.008
32.
Green B Griffiths E Almond S . Neuropsychiatric symptoms following metal-on-metal implant failure with cobalt and chromium toxicity. BMC Psychiatry. (2017) 17:33. 10.1186/s12888-016-1174-1
33.
Zhong M Liu D Tang H Zheng Y Bai Y Liang Q et al . Impacts of the perioperative fast track surgery concept on the physical and psychological rehabilitation of total hip arthroplasty: a prospective cohort study of 348 patients. Medicine. (2021) 100:e26869. 10.1097/MD.0000000000026869
Summary
Keywords
elderly, femoral neck fracture, hemiarthroplasty, total hip arthroplasty, the health-related quality of life, EU-5Q, perioperative nursing
Citation
Su Y, Li R, Ren X, Wang Y, Bai X, Zhang Y, Han L, Wang Y and Liang R (2023) The health-related quality of life for hemiarthroplasty and total hip arthroplasty in the elderly: A meta-analysis. Front. Med. 10:1022584. doi: 10.3389/fmed.2023.1022584
Received
12 December 2022
Accepted
30 January 2023
Published
24 February 2023
Volume
10 - 2023
Edited by
Vahid Rashedi, University of Social Welfare and Rehabilitation Sciences, Iran
Reviewed by
Giuseppe Basile, IRCCS Istituto Ortopedico Galeazzi, Italy; Marjan Haghi, University of Social Welfare and Rehabilitation Sciences, Iran; Radu-Dan Necula, Universitatea Transilvania din Braşov, Romania
Updates
Copyright
© 2023 Su, Li, Ren, Wang, Bai, Zhang, Han, Wang and Liang.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ruiling Li ✉ kflrl66@163.com
This article was submitted to Geriatric Medicine, a section of the journal Frontiers in Medicine
†ORCID: Ruiling Li orcid.org/0000-0002-7262-7414
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.