Abstract
Background:
Light chain (AL) amyloidosis stands as the most prevalent subtype of systemic amyloidosis, encompassing a group of rare diseases. Here, we evaluated the scientific landscape of AL amyloidosis to investigate research trends and identify hotspots within the field.
Methods:
Relevant studies on AL amyloidosis published over the past two decades were retrieved from the Web of Science Core Collection. The publications between 2005 and 2024 were subjected to bibliometric analyses, leveraging tools including CiteSpace, VOSviewer, RStudio and MS Excel to analyse and visualize the annual publication trend, co-occurrence patterns, collaborative networks among countries, organizations, and authors. Burst keywords and references were also examined to obtain the research history, and emerging hotspots.
Results:
The bibliometric analysis included 2,864 articles published between 2005 and 2024. The most productive journal is Amyloid-Journal of Protein Folding Disorders. The United States, along with several developed nations, emerges as a dominant force in international AL amyloidosis research. “AL amyloidosis” and “cardiac amyloidosis” were the primary hotspots over the past two decades, and “Biomarkers,” “Cardiac amyloidosis,” and “treatment” would be future trends.
Conclusion:
This bibliometric analysis examined the research developments in AL amyloidosis over the past two decades using bibliometric software. Recent research in this field primarily focuses on two main areas: clinical diagnosis and treatment of AL amyloidosis, as well as cardiac amyloidosis. Emphasis is placed on understanding the mechanisms underlying immunoglobulin light chain aggregation and deposition to mitigate organ involvement.
1 Introduction
Amyloidosis results from the extracellular deposition of amyloid, a fibril that self-assembles with highly ordered abnormal cross β-sheet conformation (1). There have been identified more than 60 proteins that are heterogeneous amyloidogenic and approximately more than 30 among them known to be associated with human disease (2). Immunoglobulin light chain (AL) amyloidosis or primary amyloidosis is the most frequent type of this rare group of diseases, with approximately 4,500 new cases diagnosed every year in the United States (3). It usually affects people from ages 50 to 80, with 64 years being the median age at diagnosis, and about two-thirds of the patients are male. AL amyloidosis is a clonal plasma cell disorder characterized by the systemic deposition of misfolded immunoglobulin light chains as insoluble fibrils or fragments in the extracellular space of various organs (4). The most common organ affected by AL amyloidosis is the heart, causing dysfunction and eventually death (5). Although significant advancements in the management and treatment of AL amyloidosis in the past 20 years, the disease remains fatal, especially in advanced patients (6). The molecular determinants of AL amyloidosis disease occurrence and development are still not fully clear (7).
Bibliometric analysis has recently emerged to be a popular and rigorous tool for investigating and analyzing large volumes of scientific literature (8). Using bibliometric analysis enables us to have a systematic and comprehensive understanding of the de facto structure in a particular field and capture emerging trends (9). Through measuring the scientific outputs of different scientific items, such as authors, keywords, journals, countries, and institutions, the results of the bibliometric method can be visualized in the form of figures and tables to get the research progress and identify the most contributed countries, authors, and institutions. As the most common form of systemic amyloidosis, it has entered a stage of rapid development, however, there is relatively few research in this field. To date, limited bibliometric studies have been conducted to describe the overall situation of AL amyloidosis. With the increasing number of literatures in this field, the bibliometric tool allows the researcher to identify the trends and status in research with an effective means.
In this study, we have conducted a comprehensive bibliometric analysis of AL amyloidosis during the period ranging from 2005 to 2024 using CiteSpace and VOSviewer, RStudio and MS Excel software. This review provides a systemic overview of the development trend and research outputs in the field of AL amyloidosis.
2 Materials and methods
2.1 Data sources
Web of Science Core Collection (WOSCC) serves as a key global data source for literature searches. The current bibliometric study was conducted by searching relevant publications from the WOSCC database, which covers documents published from Jan 1, 2005 to Apr 28, 2024. The search strategy used in the database was as follows:
The search terms were set to TS = (“AL amyloidos?s” OR “Primary amyloidos?s” OR “light chain amyloidos?s” OR “amyloid light chain” OR “amyloidogenic light chain” OR “light chain aggregation” OR “Immunoglobulin light chain amyloidos?s”). “?” is a wildcard representing “i” or “e.” Data were retrieved on the 28th of April 2024. A total of 4,980 records were retrieved. Among these, we focus on relevant articles and reviews that are limited to the English language. Thus, 2,116 meeting abstract, editorial material, book reviews, proceeding paper, letter, early access, retraction, book chapters, news item, and publication with expression of concern were excluded, resulting in 2,864 documents published from 2005 to 2024. The results were exported and checked for duplicates using CiteSpace (version 6.3.R1). After checking duplicates (0 duplicates found), a total number of 2,864 publications including 2,277 articles and 587 reviews were obtained for further analysis. The search strategy is presented in Figure 1.
Figure 1

Search strategy.
2.2 Data analysis
The present study employed CiteSpace (version 6.3.R1), VOSviewer (version 1.6.20), open-source Biblioshiny (R software, version 4.3.3), and MS Excel software for bibliometric analysis. CiteSpace is a web-based Java application for data analysis and visualization (10). The included documents were analyzed and visualized utilizing CiteSpace for keywords clusters, reference co-occurrence and top 25 keywords/references with bursts. The time-slicing specifications for CiteSpace were set to consider each year between 2005.01 and 2024.04 as a timestamp. VOSviewer is a software tool for creating and exploring maps based on network data (11). We used VOSviewer to explore keyword co-occurrence, author co-occurrence, country co-occurrence, and coupling analysis, including source journals and organizations. In addition, the bibiometrix (12)1 package of R software was used for the analysis of authors’ production over time, inter and intra collaboration of various countries. The Three-field plot analysis representing the author, country and source relationship was also conducted using Biblioshiny.
3 Results
3.1 Annual publications and growth trend
In the recent 20 years, a total of 2,864 articles in this field were published in the Web of Science. The volume of articles published in this field has generally shown a stable growth trend (Figure 2). The highest number of publications was published in 2020 (271/2,864, 9.462%).
Figure 2
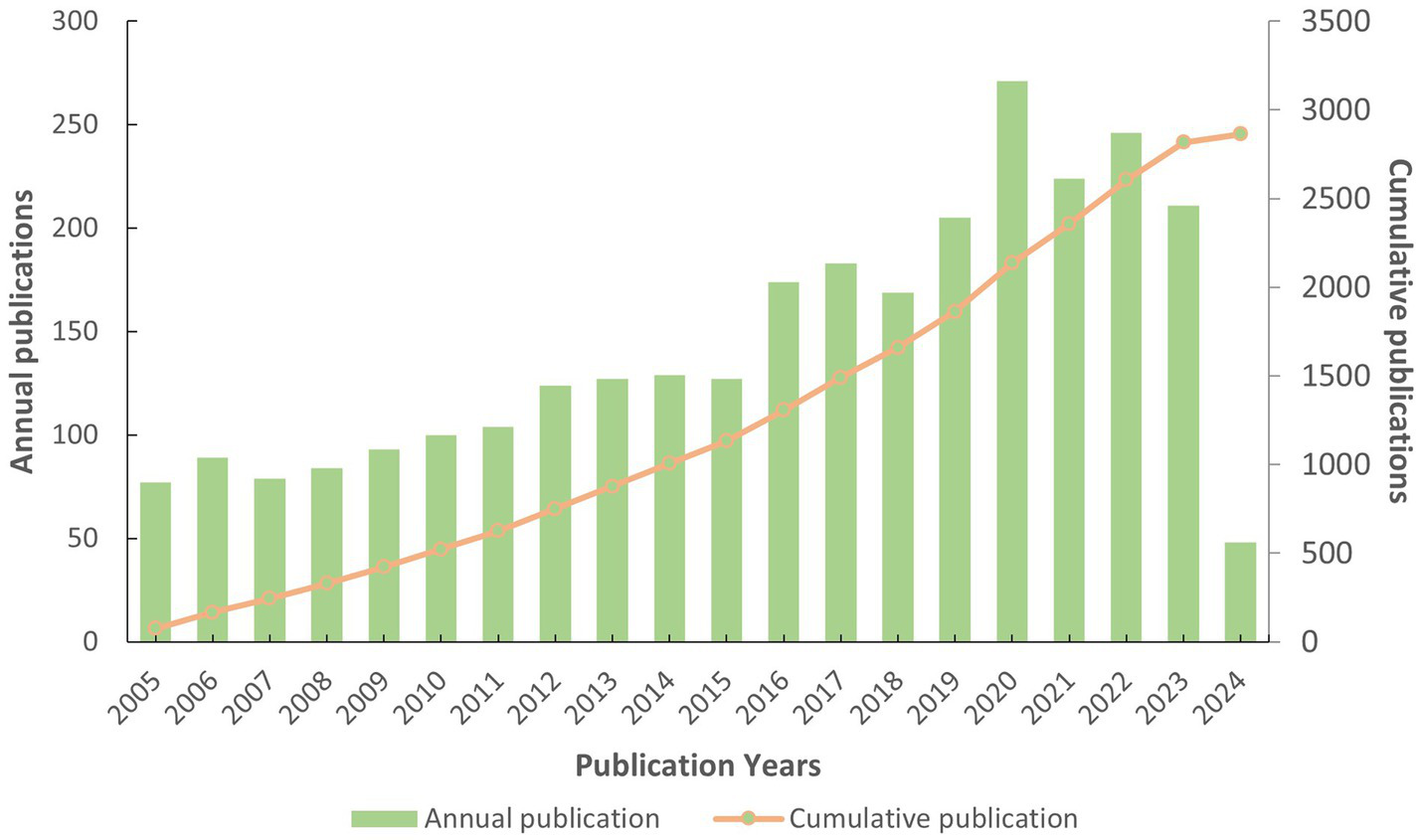
Yearly publication distribution and growth trend.
3.2 Leading countries/regions and their collaboration
The publication distribution of the top 20 countries/regions is shown in Figure 3. A total of 70 countries or regions have published articles in the AL amyloidosis field in the last 20 years. The United States (USA) has the highest number of publications (1,182 articles), followed by Italy with 395 articles, the United Kingdom (UK) with 278 articles, Germany with 266 articles, France with 215 articles, Japan with 214 articles, and China with 196 articles (Table 1). Among 70 countries, only 8 countries published more than 100 papers in the field. Additionally, the interconnection between countries is shown in Figure 4; Supplementary Figure S1. The size of the circle represents the number of articles published by the country. The shorter the distance between the two circles, the greater the cooperation between the two countries.
Figure 3
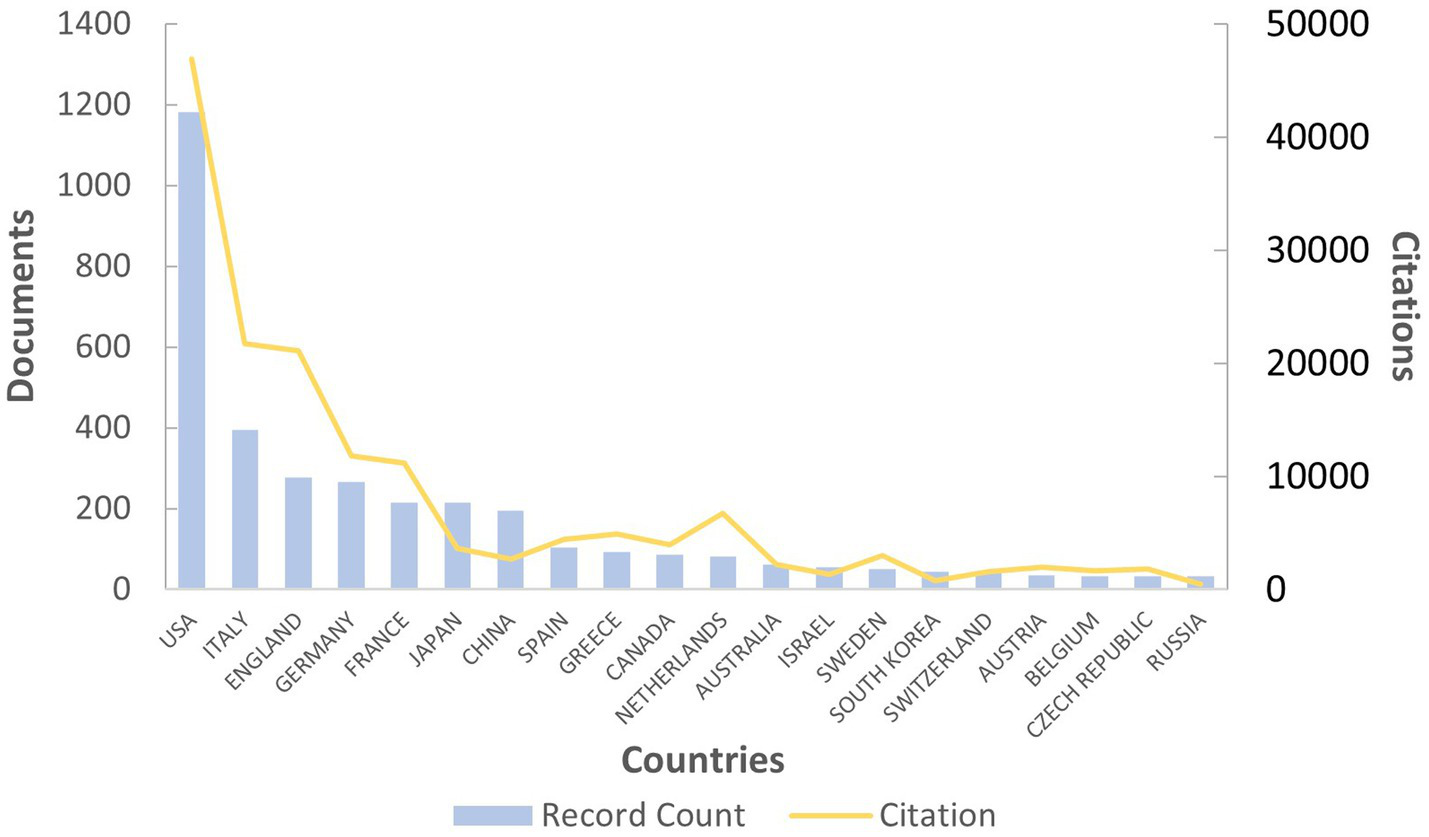
Top 20 countries with the highest number of papers and their citation trend.
Table 1
| Country | Documents | Citations | Average citation | Total link strength |
|---|---|---|---|---|
| USA | 1,182 | 46,900 | 39.68 | 34,766 |
| Italy | 395 | 21,718 | 54.98 | 21,431 |
| UK | 278 | 21,114 | 75.95 | 17,640 |
| Germany | 266 | 11,770 | 44.25 | 11,823 |
| France | 215 | 11,141 | 51.82 | 9,200 |
| Japan | 214 | 3,627 | 16.95 | 4,267 |
| China | 196 | 2,666 | 13.60 | 5,154 |
| Spain | 103 | 4,400 | 42.72 | 4,261 |
| Greece | 92 | 4,903 | 53.29 | 6,270 |
| Canada | 87 | 3,967 | 45.60 | 4,314 |
| Netherlands | 81 | 6,690 | 82.59 | 4,680 |
| Australia | 61 | 2,198 | 36.03 | 2,794 |
| Israel | 56 | 1,336 | 23.86 | 2,176 |
| Sweden | 50 | 3,002 | 60.04 | 1,525 |
| South Korea | 43 | 757 | 17.60 | 1,562 |
| Switzerland | 43 | 1,578 | 36.70 | 1,186 |
| Austria | 35 | 1,993 | 56.94 | 1,076 |
| Belgium | 32 | 1,654 | 51.69 | 1,619 |
| Czech Republic | 32 | 1,810 | 56.56 | 1,294 |
| Russia | 32 | 455 | 14.22 | 411 |
Top 20 countries with a minimum of 5 published in the field of AL amyloidosis (61 countries found out of 98).
Figure 4
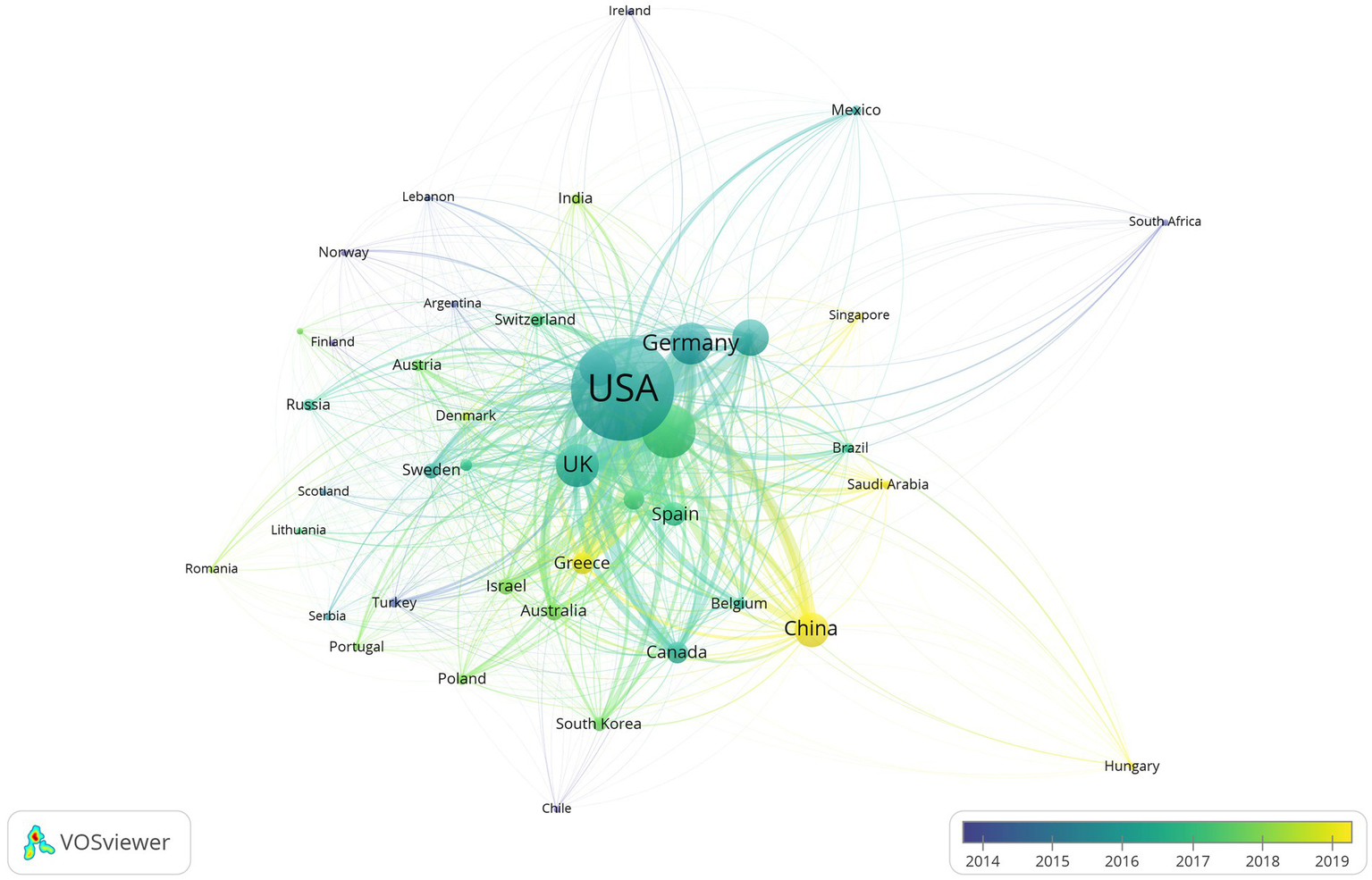
Network visualization of collaboration across countries chronologically in the field of AL amyloidosis.
Moreover, the total link strength (TLS) can measure the collaboration across countries. The TLS analysis revealed that the USA had the highest collaborative research with a TLS of 34,766 for all 1,182 articles, Italian researchers ranked second with a TLS of 21,431, followed by the UK with a TLS of 17,640 (Table 1). Results also revealed that publications of the USA had the maximum number of citations (46,900 citations, with an average citation per document of 39.68), followed by Italy with 21,718 citations (average of 54.98), UK with 21,114 citations (average of 75.95) and Germany with 11,770 citations (average of 44.25). Figure 5 displays the intra and inter-collaboration of various countries to publish articles in the field of AL amyloid by analyzing single country publications (SCPs) and multiple country publications (MCPs). MCP represents collaboration among different countries, while SCP indicates the production of a single country. Countries were selected based on the corresponding author’s country. The USA and UK had the highest number of MCPs as compared to other countries, followed by Italy and Germany. The USA and Italy also had the first and 2nd highest number of SCPs, respectively (Figure 5).
Figure 5
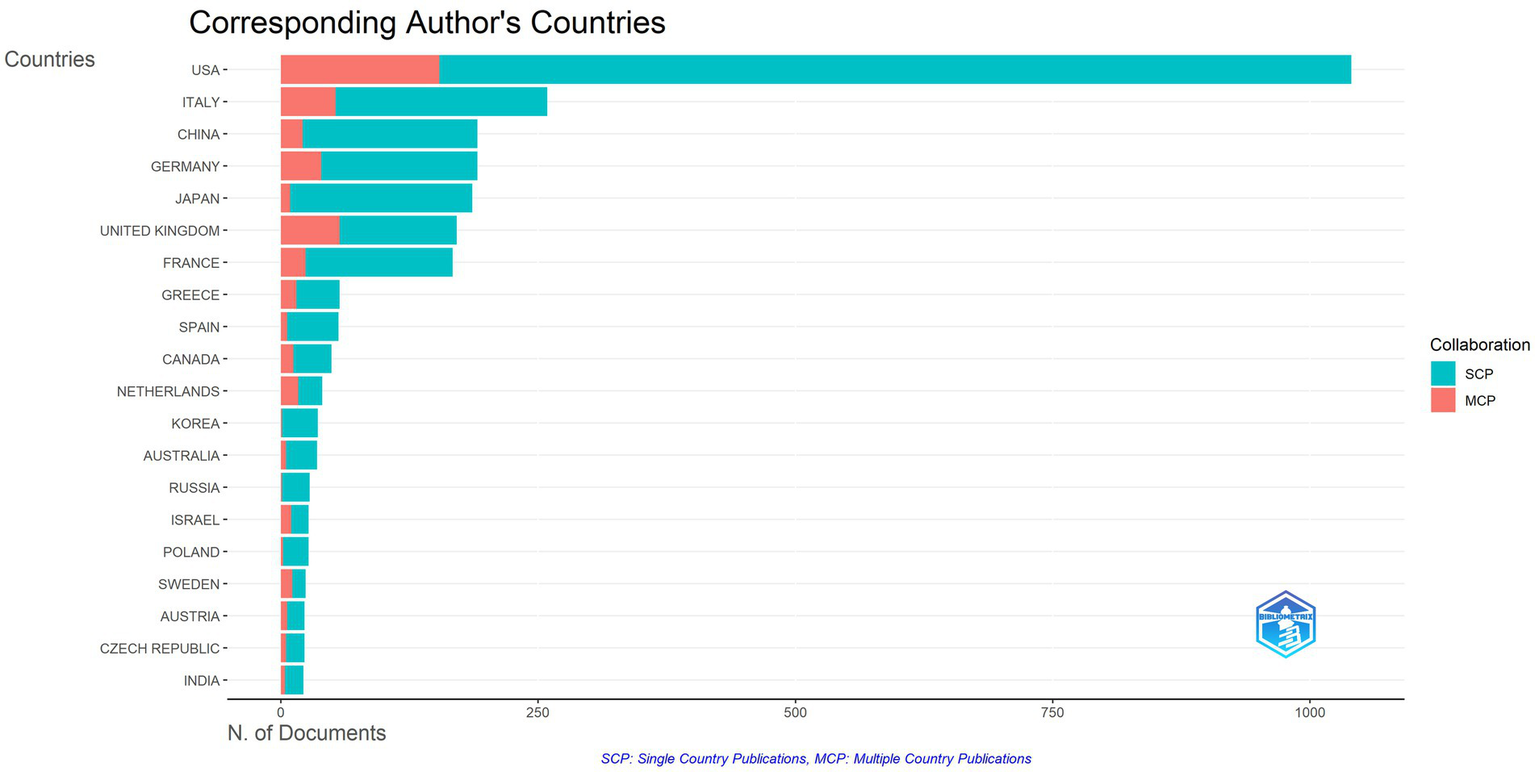
Inter and intra collaboration of various countries.
3.3 Publication distribution of organization
The organization with a minimum of 5 publications in the field of AL amyloidosis were analyzed using VOSviewer. A total of 2,896 institutions have participated in the studies of AL amyloidosis in the past 20 years, and 285 of them published more than 5 pieces of literature. The top five organizations with the highest number of publications were Mayo Clinic (394), University of Pavia (190), Boston University (175), University College London (153), and Fdn IRCCS Policlin San Matteo (69). The top 20 organizations with the highest number of published documents and citations are shown in Table 2, and the institute’s cooperation network map is displayed in Figure 6; Supplementary Figure S2.
Table 2
| Organizaiton | Country | Documents | Citations | Average citation |
|---|---|---|---|---|
| Mayo Clinic | The United States | 394 | 21,820 | 55.38 |
| University of Pavia | Italy | 190 | 12,540 | 66 |
| Boston University | The United States | 175 | 11,270 | 64.4 |
| University College London | The United Kingdom | 153 | 12,438 | 81.29 |
| Fdn IRCCS Policlin San Matteo | Italy | 69 | 3,542 | 51.33 |
| Heidelberg University | Germany | 63 | 3,729 | 59.19 |
| Boston Medical Center | The United States | 62 | 3,252 | 52.45 |
| Memorial Sloan Kettering Cancer Center | The United States | 57 | 3,553 | 62.33 |
| Tufts Medical Center | The United States | 56 | 3,264 | 58.29 |
| Columbia University in the City of New York | The United States | 55 | 4,536 | 82.47 |
| National and Kapodistrian University of Athens | Greece | 46 | 699 | 15.20 |
| Stanford University | The United States | 45 | 1,383 | 30.73 |
| Harvard Medical School | The United States | 40 | 1,017 | 25.43 |
| Brigham and Women’s Hospital | The United States | 38 | 3,965 | 104.34 |
| Medical College of Wisconsin | The United States | 37 | 762 | 20.59 |
| Shinshu University | Japan | 37 | 705 | 19.05 |
| The University of Tennessee | The United States | 32 | 1983 | 61.97 |
| Cleveland Clinic | The United States | 29 | 1,464 | 50.48 |
| University of Athens | Greece | 29 | 3,068 | 105.79 |
| Kumamoto University | Japan | 28 | 905 | 32.32 |
Top 20 institutes with a minimum of 5 published in the field of AL amyloidosis (285 countries found out of 2,896).
Figure 6
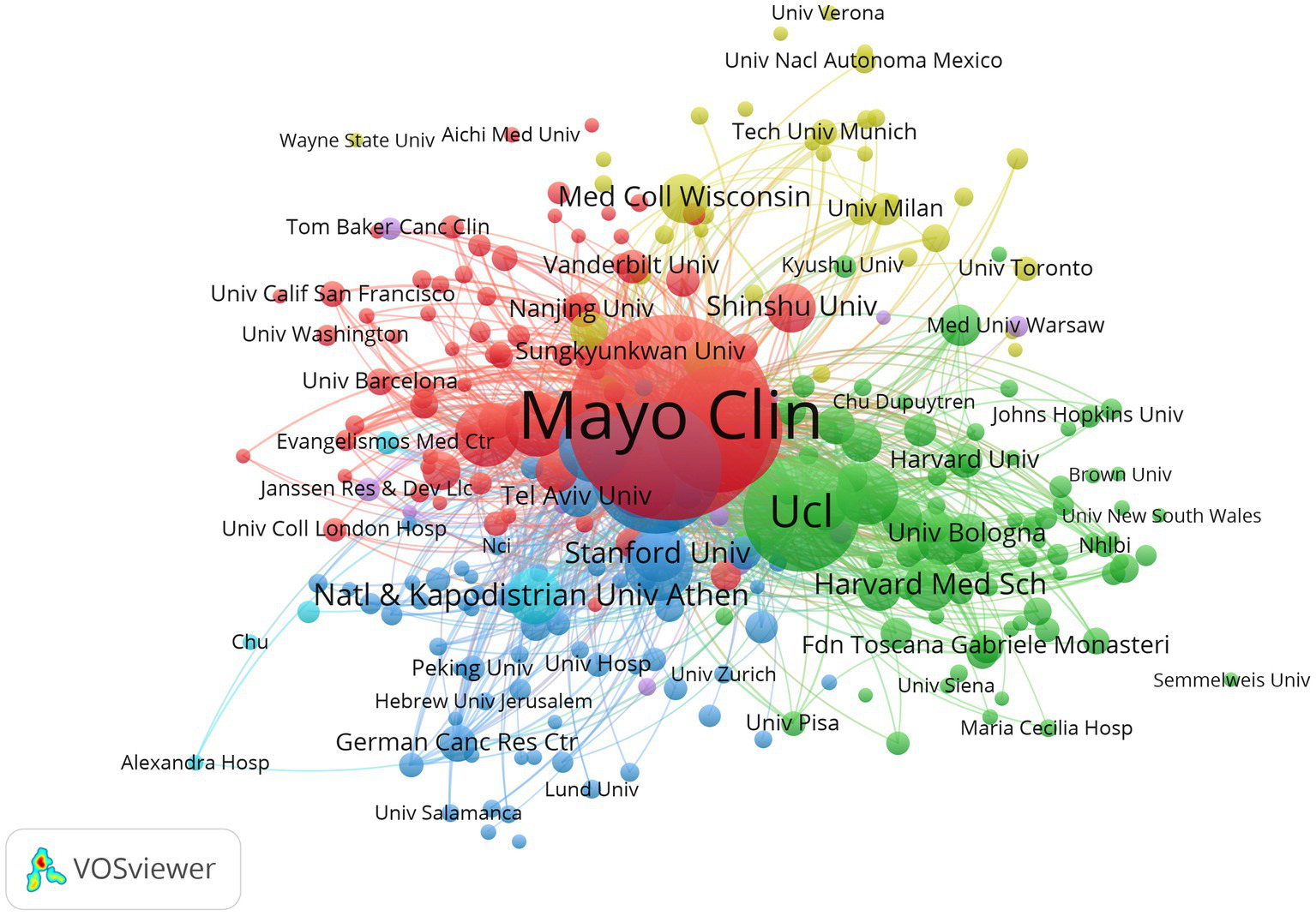
Organizations cooperation network map of relevant literature.
3.4 Most productive authors and co-author relationship
Among 12,366 authors, 44 leading authors published more than 30 publications in the field of AL amyloidosis. The top 20 productive authors were shown in Supplementary Figure S3A, while the top 20 cited ones were displayed in Supplementary Figure S3B. According to the total number of publications, Dispenzieri A. (199), Gertz M. A. (165), and Merlini G. (135) were the top 3 most productive authors, respectively. In terms of the metrics of citations received, Dispenzieri A. (10,529), Merlini G. (9,080), and Hawkins P. N. (9,035) were the top 3 most productive authors, respectively (Table 3). H-index and G-index were used to characterize the scientific output of a researcher. The top 20 authors are all high impact with H-indexes over 30. Notably, Dispenzieri A. has the highest H-index of 65, and Merlini G. has the highest G-index of 117 (Supplementary Figures S3C,D). Analysis of the author’s cooperation network map is displayed in Figure 7A and Supplementary Figure S4. Moreover, the author’s production over time was analyzed to investigate the spatial and temporal progress of AL amyloidosis research. Figure 7B shows the contribution of the top 20 authors over different years. The size of the dots represents the number of articles, and the color of the dots (light to dark) represents the total citations (TC) per year.
Table 3
| Author name | Documents | Citations | Average citation | Total link strength |
|---|---|---|---|---|
| Dispenzieri A. | 199 | 10,529 | 52.9095 | 17,441 |
| Gertz M. A. | 165 | 8,953 | 54.2606 | 18,772 |
| Merlini G. | 135 | 9,080 | 67.2593 | 17,576 |
| Palladini G. | 119 | 6,618 | 55.6134 | 16,487 |
| Leung N. | 110 | 5,484 | 49.8545 | 10,077 |
| Sanchorawala V. | 101 | 3,509 | 34.7426 | 7,874 |
| Lacy M. Q. | 91 | 4,325 | 47.5275 | 10,036 |
| Hawkins P. N. | 86 | 9,035 | 105.0581 | 8,178 |
| Dingli D. | 80 | 3,303 | 41.2875 | 8,828 |
| Rajkumar S. V. | 80 | 4,263 | 53.2875 | 8,271 |
| Wechalekar A. D. | 79 | 5,587 | 70.7215 | 7,670 |
| Buadi F. K. | 78 | 3,324 | 42.6154 | 9,027 |
| Hegenbart U. | 78 | 4,343 | 55.6795 | 8,024 |
| Hayman S. R. | 74 | 3,809 | 51.473 | 8,568 |
| Gillmore J. D. | 73 | 6,118 | 83.8082 | 5,512 |
| Kumar S. K. | 72 | 2,725 | 37.8472 | 8,078 |
| Kyle R. A. | 71 | 4,649 | 65.4789 | 7,365 |
| Kapoor P. | 69 | 1,874 | 27.1594 | 6,774 |
| Milani P. | 68 | 2,900 | 42.6471 | 9,228 |
| Kastritis E. | 59 | 2,831 | 47.9831 | 6,703 |
Leading authors in the field of AL amyloidosis.
Figure 7
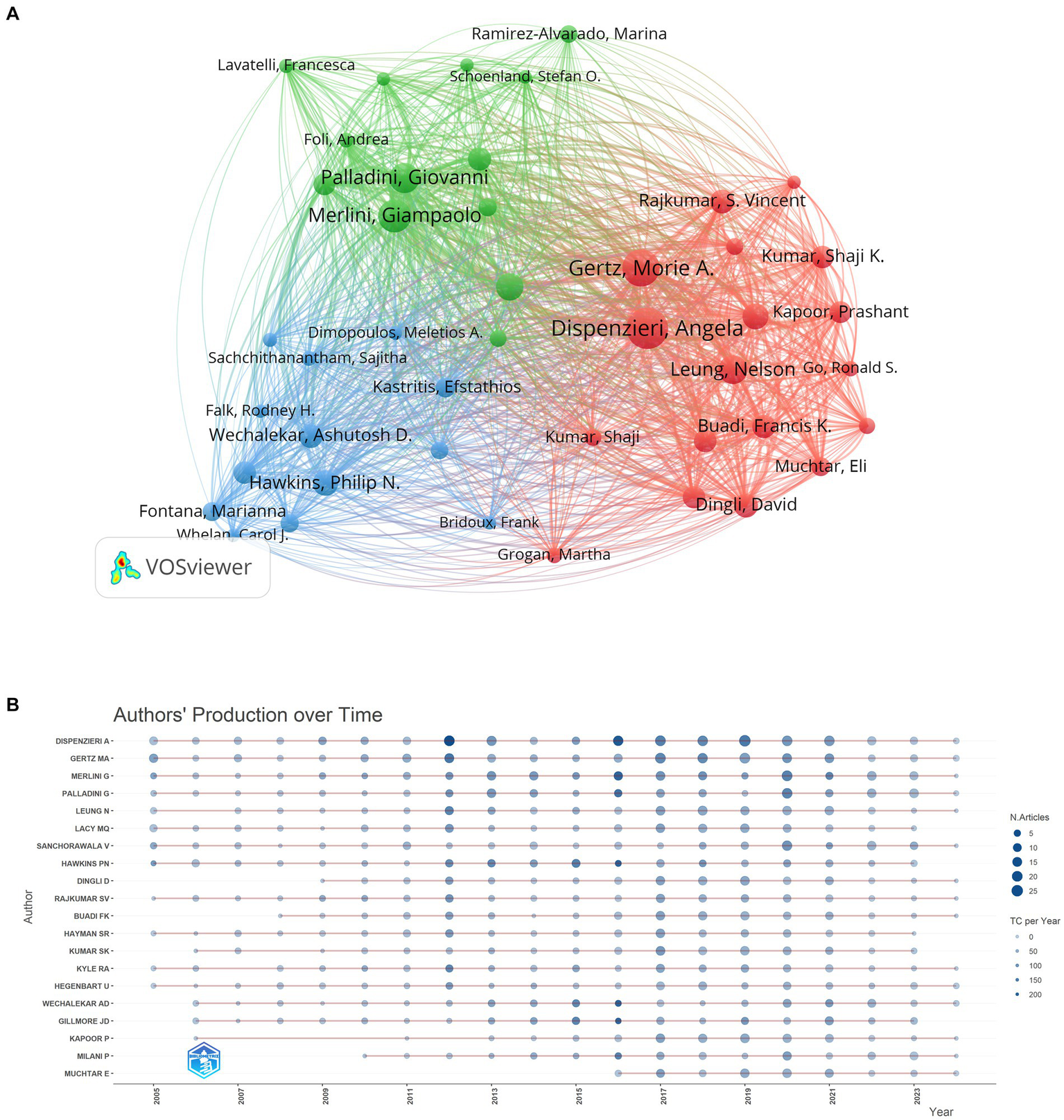
Author visual analysis. (A) Network visualization of collaborative research among authors. (B) Top 20 authors over different years.
3.5 Primary academic journals
All the articles related to AL amyloidosis were published in 733 journals, among which 63 journals with a minimum number of 10 articles were selected for analysis (Figure 8; Supplementary Figure S5). Table 4 provides a list of the top 20 most productive journals that have published research articles in the field of AL amyloidosis. A total of 152 publications ranked the journal Amyloid-Journal of Protein Folding Disorders at the top position, followed by Blood (95), American Journal of Hematology (57), and British Journal of Haematology (48) (Supplementary Figure S6A). Among them, Blood (IF = 20.3) is the most cited journal with citations of 9,384. The journals’ production over time of top five most productive journals were shown in Supplementary Figure S6B.
Figure 8
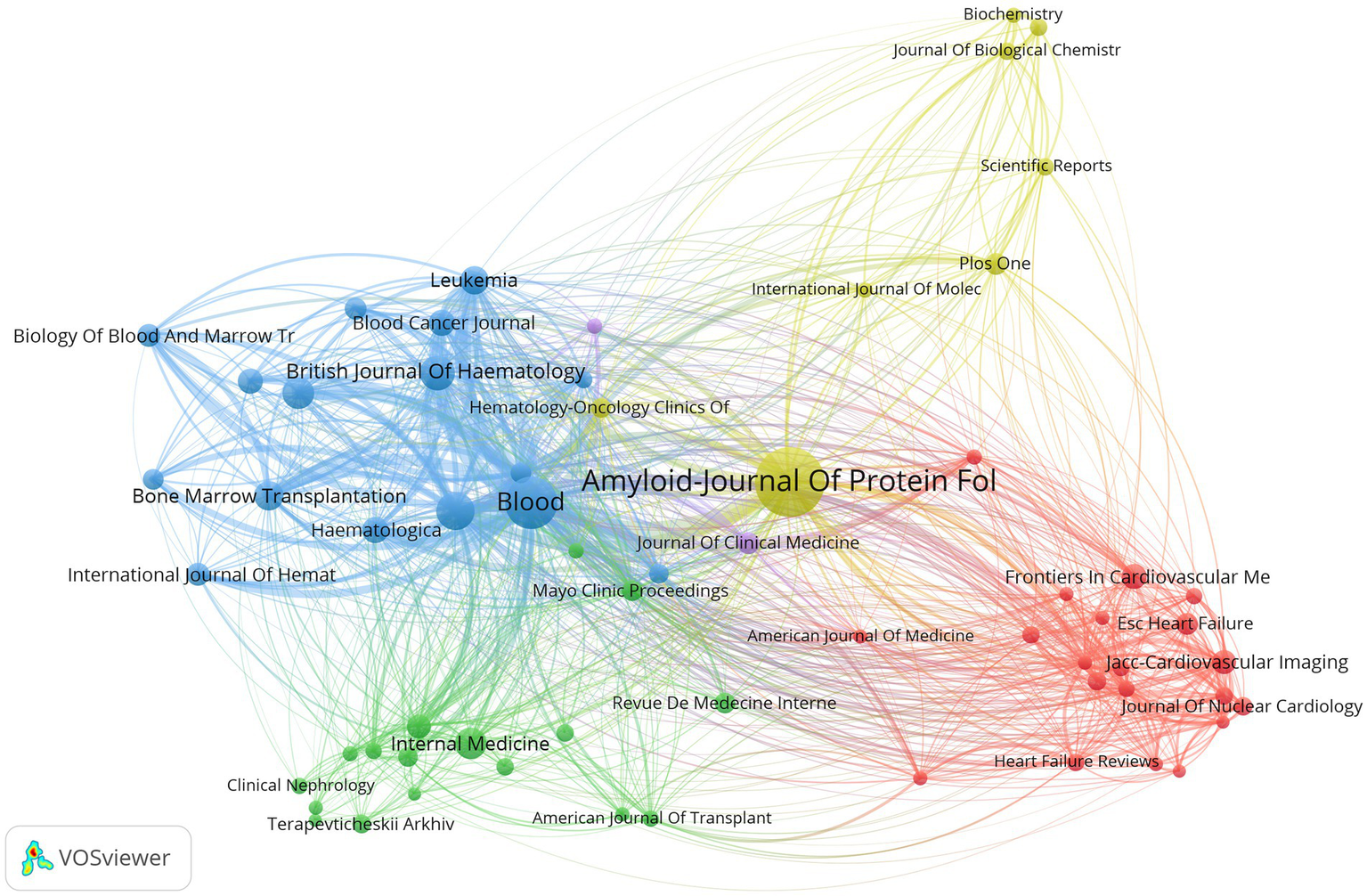
Primary journals visual analysis.
Table 4
| Sources/Journals | Publisher | Documents | Citations | Average citation | Impact factor (2023) |
|---|---|---|---|---|---|
| Amyloid-Journal of Protein Folding Disorders | Taylor & Francis | 152 | 2,567 | 16.89 | 5.5 |
| Blood | American Society of Hematology | 95 | 9,384 | 98.78 | 20.3 |
| American Journal of Hematology | Wiley | 57 | 2,673 | 46.89 | 12.8 |
| British Journal of Haematology | Wiley | 48 | 1,207 | 25.15 | 6.5 |
| Clinical Lymphoma Myeloma & Leukemia | Elsevier | 41 | 397 | 9.68 | 2.7 |
| Internal Medicine | Japanese Society of Internal Medicine | 40 | 251 | 6.28 | 1.2 |
| Bone Marrow Transplantation | Springer | 37 | 1,147 | 31 | 4.8 |
| Leukemia | Springer | 35 | 2,707 | 77.34 | 11.4 |
| Blood Cancer Journal | Springer | 31 | 721 | 23.26 | 12.8 |
| Haematologica | Ferrata Storti Foundation | 31 | 1,447 | 46.68 | 10.1 |
| European Journal of Haematology | Wiley | 29 | 366 | 12.62 | 3.1 |
| Frontiers in Cardiovascular Medicine | Frontiers | 28 | 116 | 4.14 | 3.6 |
| JACC-Cardiovascular Imaging | Elsevier | 27 | 2,630 | 97.41 | 14 |
| Nephrology Dialysis Transplantation | Oxford University Press | 26 | 673 | 25.88 | 6.1 |
| Biology of Blood and Marrow Transplantation | Elsevier | 25 | 405 | 16.20 | 4.3 |
| International Journal of Hematology | Springer | 24 | 152 | 6.33 | 2.1 |
| ESC Heart Failure | Wiley | 23 | 244 | 10.61 | 3.8 |
| Journal of Clinical Medicine | MDPI | 23 | 57 | 2.48 | 3.9 |
| Leukemia & Lymphoma | Informa Healthcare | 22 | 332 | 15.09 | 2.6 |
| PLoS One | Public Library of Science | 22 | 496 | 22.55 | 3.7 |
Top 20 journals with the highest number of publications.
3.6 Documents co-citation and references burst analysis
We selected articles with a minimum of 100 citations for analysis. Among the 39,672 documents, 77 articles meet the threshold (Figure 9A). The article Gertz (2005), American Journal of Hematology (13) has received the highest number of 695 citations. The 2nd and 3rd highest number of citations were received by papers authored by Kumar (2012), Journal of Clinical Oncology (14) and Dispenzieri (2004), Journal of Clinical Oncology (15) with 494 and 492 citations, respectively. Reference co-occurrence analysis generated a visual network map, which contains 233 nodes, 378 connected lines, and 9 main clusters (Figure 9B). The log-likelihood ratio (LLR) was used to characterize the nature of a cluster by CiteSpace, and then noun phrases were extracted from the keywords in the cluster. Log-likelihood ratio (LLR) clustered the cited literature into 9 groups, with the first three clusters’ labels named (#0) AL amyloidosis, (#1) high-dose melphalan, and (#2) cardiac amyloidosis, respectively. The weighted mean silhouette was 0.9231, which indicates the structure of the clustering has good stability and credibility. The modularity Q is 0.6932, which indicates that the clustering of the network is reasonable. The top 25 references with the strongest citation bursts are displayed in Figure 9C, which shows the first citation bursts occurred in 2005 (16). The blue bars represent the timeline, and the red bars represent the start and end years of the burst duration. An article entitled “New Criteria for Response to Treatment in Immunoglobulin Light Chain Amyloidosis Based on Free Light Chain Measurement and Cardiac Biomarkers: Impact on Survival Outcomes” authored by Palladini G. and colleagues published in Journal of Clinical Oncology (Q1, IF: 45.3) in 2012 (17) was the strongest citation burst with a strength value of 73.33 during a period of 4 years until 2017.
Figure 9
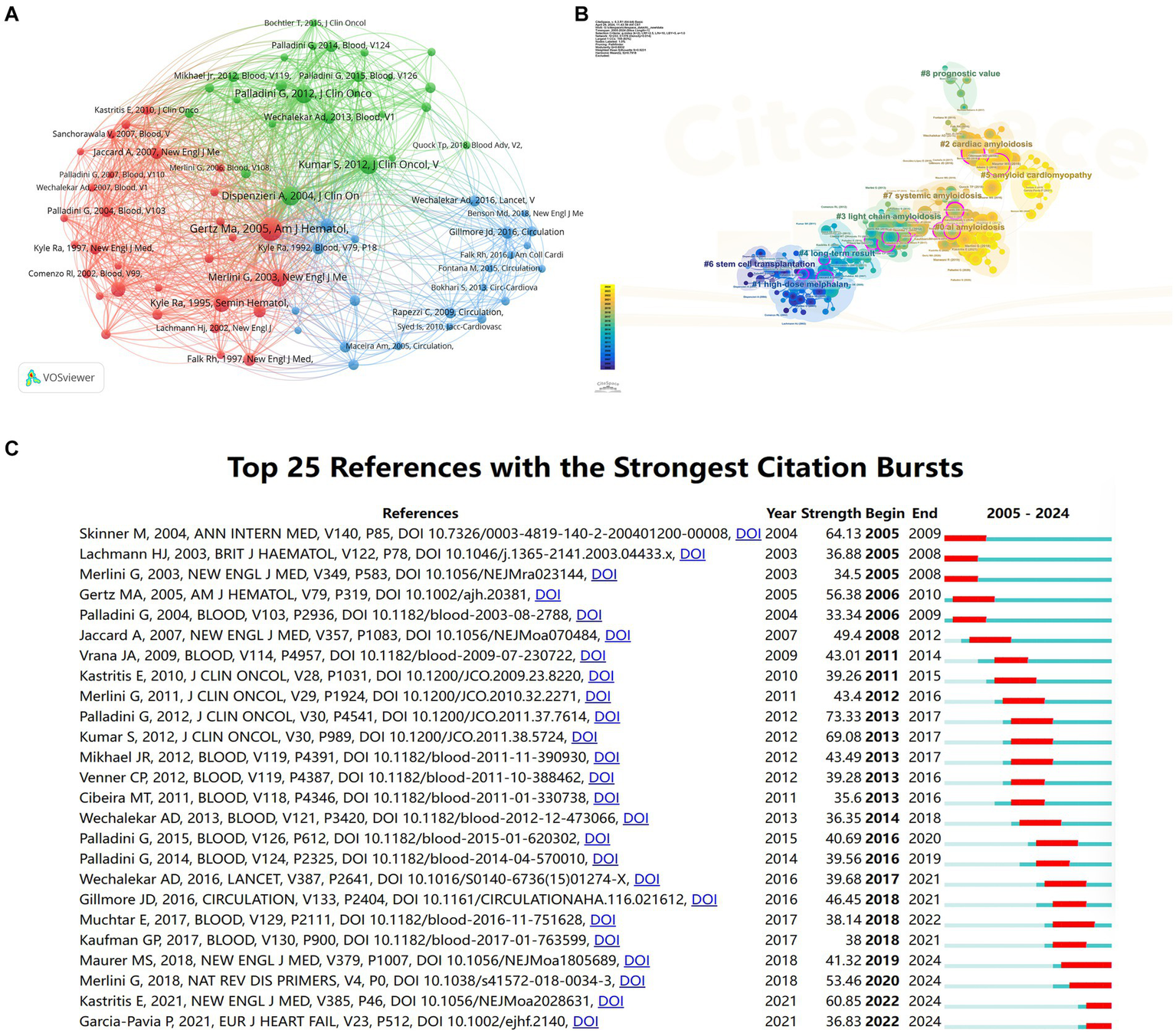
Visual analyses of AL amyloidosis documents and relevant cited references. (A) Analysis of documents citation. (B) Analysis of references clusters. (C) The top 25 references that had the most significant bursts of citations.
3.7 Analysis of burst words, keyword clusters and co-occurrence network
A total of 6,147 keywords were obtained, while keywords with a minimum of 20 occurrences were taken into consideration. Keywords co-occurrence analysis revealed a total of 216 keywords had a minimum of 20 occurrences. Among them, the term “AL amyloidosis” had the highest frequency with 1,048 occurrences, followed by “Light-Chain Amyloidosis” with 715 occurrences, and “Amyloidosis” with 701 occurrences (Figure 10A; Supplementary Figure S7). The keyword clustering analysis was conducted in CiteSpace. Results showed the hotspots in the field of AL amyloidosis. As shown in Figure 10B, keywords were grouped into seven clusters, (#0) AL amyloidosis, (#1) cardiac amyloidosis, (#2) autologous stem cell transplantation, (#3) light-chain cardiac amyloidosis, (#4) monoclonal gammopathy, (#5) supportive care, and (#6) renal diseases, respectively. The timeline of keywords further elucidated the temporal characteristics and evolution trend of the core terms (Figure 10C). Additionally, the top 25 keywords with the strongest citation bursts based on citation burst values were identified, including primary systemic amyloidosis, stem cell transplantation, prednisone, features, melphalan, primary amyloidosis, nephrotic syndrome, high dose dexamethasone, colchicine, therapy, chemotherapy, aa amyloidosis, proteins, combination, localized amyloidosis, diagnosed AL amyloidosis, outcome, natural history, transthyretin amyloidosis, impact, recommendations, light-chain amyloidosis, cardiac amyloidosis and biomarkers (Figure 10D).
Figure 10
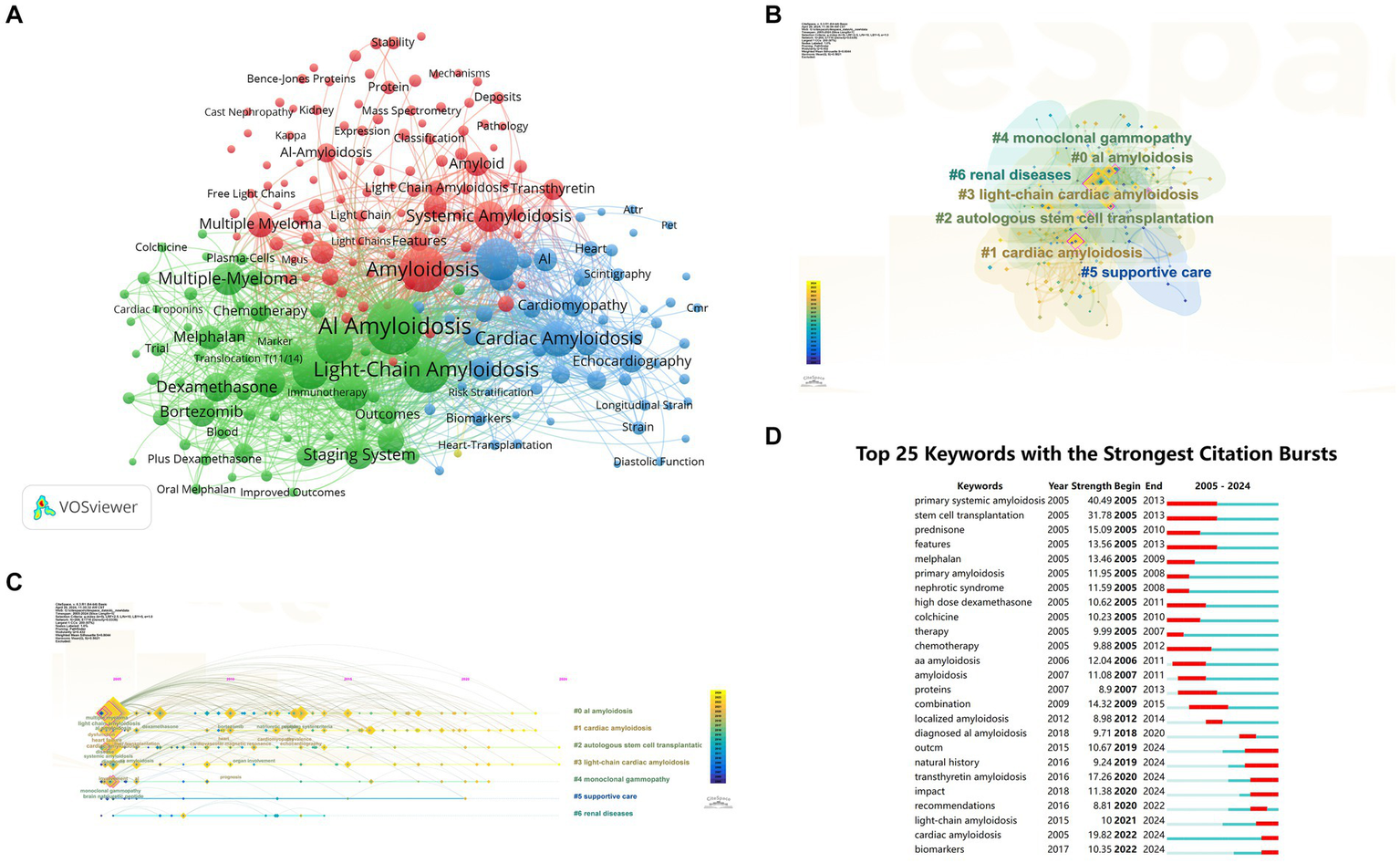
Analyses of keywords. (A) Visual analysis of keywords co-occurrence. (B) Cluster view of co-citation of keywords. (C) A timeline view of the co-citation of keywords. (D) The 25 most cited keywords.
3.8 Three-field plot analysis representing keywords-sources-countries
The three-field plot displayed the relationship between keywords, sources and countries (Figure 11). The lines and boxes demonstrate the association between the three variables. The height of the boxes and the thickness of the connecting lines show the strength of the association between variables (18). The result highlights “AL amyloidosis” as the most prevalent keyword connected strongly with the source Amyloid-journal of protein folding disorders. Moreover, the source Amyloid-journal of protein folding disorders had highly strength of association with the keywords “AL amyloid,” “light-chain amyloidosis,” “survival,” and “primary systemic amyloidosis” and countries like the USA, France and Italy.
Figure 11

The three-field plot analysis representing keywords (left), sources (middle), and countries (right).
4 Discussion
4.1 Basic information
This bibliometric study was conducted to identify the status of global scientific output, the hotpots, frontiers, and future trends of AL amyloidosis between January 1, 2005 and April 28, 2024. Software including CiteSpace, VOSviewer, and R were applied to analyze and visualize the countries/regions, authors, organizations, and sources of documents published over the past 20 years. A total number of 4,980 publications was retrieved from the WOSCC database. According to the screening criteria, 2,864 papers (including 2,277 articles and 587 reviews) met the threshold, which were written by 12,366 authors from 2,896 institutions in 70 countries/regions, published in 733 journals with 39,672 co-cited references.
A steady increasing trend in the number of international publications indicates that this field is a promising field, which continues to attract the attention of international researchers. Overall, the United States and some developed countries dominate the international research in the AL amyloidosis field. The United States had the highest number of documents, citations and total link strength, followed by Italy, the United Kingdom, Germany, and France, which implies that The United States dominates the core of the field and has formed academic cooperation networks with many European countries. There are 12 American organizations among the top 20. It is necessary for the above-mentioned countries to take an active lead in establishing worldwide academic cooperation networks. Some Asian countries like Japan, China, South Korea, Saudi Arabia and Singapore, as shown in Table 1 and Figure 4, have started paying attention to this field in recent years as well. From 2015 to 2023, the number of publications in this field increased significantly, and to date, 48 papers have been published in 2024, indicating that AL amyloidosis has been attracted increasingly attention in recent few years and is undergoing a rapid developmental stage.
4.2 Hotspots and frontiers
Keyword frequency analysis, co-occurrence network mapping, and cluster analysis serve as valuable tools for identifying the research themes and hotspots in AL amyloidosis over the past two decades, providing crucial guidance for researchers. In Figure 10A, keywords are grouped into 3 clusters, delineating the pathological mechanisms of light chain amyloid protein formation (red), clinical diagnosis and treatment strategies for AL amyloidosis (green), and cardiac-related amyloidosis (blue). Burst keywords and references highlight prominent research directions. Among the top 25 burst keywords and references in CiteSpace software, it reflects that the researchers focus on the clinical efficacy of treatment on AL amyloidosis and the diagnosis in cardiac amyloidosis. We will further elaborate on the following 3 research directions.
4.2.1 Biomarkers
Appropriate biomarkers play a crucial role in the early diagnosis and prognostic assessment of AL amyloidosis due to its non-specific presentation, which leads to delayed diagnosis, and increased mortality rates (19). However, a significant challenge persists in identifying a sensitive and specific biomarker that encompasses all aspects of disease, including cardiac damage, renal failure, monoclonal plasma cell burden, and toxic free immunoglobulin light chains circulation (19).
Given the significant prognostic implications of cardiac involvement and its association with early mortality, biomarkers indicative of cardiac injury and dysfunction have emerged as powerful prognostic indicators over time. The Mayo 2004 staging system, an early benchmark, incorporates three biomarkers: N-terminal pro-brain natriuretic peptide (NT-proBNP), brain natriuretic peptide (BNP), and cardiac troponin T (cTnT) (15). Subsequent refinements, such as the Mayo 2012 system, introduced additional parameters like the difference between involved and uninvolved free light chain concentration (dFLC), recognizing the significance of FLC levels in reflecting the underlying clonal disease burden (14). Although the combination of cTnT and NT-proBNP offers an objective and reproducible risk assessment tool, their reliability may be compromised in the presence of renal dysfunction and other confounding factors, such as fluid overload and atrial arrythmias (20). Hence, their reliability in such contexts is therefore questioned. The current staging system incorporates estimated glomerular filtration rate (eGFR) and proteinuria for prognostic evaluation of renal involvement, serving as endpoints in clinical trials (21). However, neither marker is sufficiently specific nor sensitive, nor do they directly reflect renal cell injury. Even though creatinine, eGFR, and proteinuria are established biomarkers, they are subject to influences such as hydration status, diuretic use, fluctuations in weight, and comorbidities, necessitating ongoing efforts to identify more sensitive biomarkers (19).
In addition to the abovementioned biomarkers, other parameters including cardiac troponin I (cTnI) (22), high-sensitivity cardiac troponin(hs-cTnT) (23), ejection fraction (EF) (24), left ventricle longitudinal function (25), left ventricle septum thickness (15), systolic blood pressure (26), uric acid (27), albumin-to creatinine ratio (28), albumin (21), and proteinuria (21) have also been explored as indicators in patients with AL amyloidosis in recent years.
Tumor-related biomarkers were screened based on the characteristics of the underlying clonal disorder, the burden and qualities of the clonal plasma or other B-cells, and the secreted amyloidogenic FLCs. They have emerged as indicators predominantly associated with long-term prognostic outcomes, in contrast to organ-function-related markers which tend to predict short-term outcomes. Furthermore, they hold significant value in various clinical aspects including response assessment, patient surveillance, and tailoring of treatment. In this respect, quantity of serum FLC (29), bone marrow plasma cell burden (30), abnormality in cytogenetics of the plasma cell clone (31) and immunoparesis (32) serves as adverse factors in AL amyloidosis prognosis.
Novel biomarkers have emerged as potential tools for refining risk stratification and predicting outcomes in the AL amyloidosis population. These include D-dimer (33), von Willebrand factor (vWF) (34), red cell distribution width (RDW) (35), soluble suppression of tumorigenicity 2 (sST2) (36), osteopontin (37), flow-mediated dilatation (FMD) (38), myocardial contraction fraction (39), left ventricle longitudinal axis strain (39), extracellular volume (ECV) (40), growth differentiation factor-15 (GDF-15) (41), soluble urokinase-type plasminogen receptor (suPAR) (42), and galectin-3 (Gal-3) (43). However, their clinical utility remains to be verified. Given the complexity and heterogeneity of the disease, it is unlikely that a single biomarker will adequately reflect prognostic value such as survival, risk of dialysis, and treatment response. With the advent of new diagnostics and therapeutics, there is potential for the discovery of additional biomarkers. On one hand, there is a need to conduct largescale epidemiological surveys and multicenter clinical trials to obtain detailed and complete patient information. On the other hand, with the era of big data, artificial intelligence should be used to in biomarker discovery.
4.2.2 Cardiac amyloidosis
Cardiac amyloidosis is characterized by the extracellular deposition of misfolded proteins known as amyloid fibrils within the myocardium, typically exhibiting Congo red positive staining and green birefringence when viewed under cross polarized light microscopy. Among the 9 amyloidogenic proteins accumulating in the myocardium to cause significant cardiac disease, the most prevalent are monoclonal immunoglobulin light chain (AL amyloidosis) and transthyretin (ATTR) (44). AL cardiac amyloidosis often eludes timely diagnosis or is misdiagnosed due to its non-specific clinical manifestations and relative rarity (45). Differential diagnosis challenges may arise, such as distinguishing between cardiac amyloidosis, hypertrophic cardiomyopathy, or heart failure. The identification of individuals with pre-symptomatic AL amyloidosis prior to the onset of significant organ involvement may allow for facilitating more efficacious therapeutic interventions, resulting in improved response rates and survival.
The diagnosis of cardiac amyloidosis involves two distinct phases: (i) the suspicious phase, and (ii) the definitive diagnosis phase. During the suspicious phase, extracardiac signs and symptoms like polyneuropathy, dysautonomia, skin bruising, macroglossia, renal insufficiency and proteinuria, in conjunction with cardiac indications such as hypotension or normotensive (in previously hypertensive patients), pseudoinfarct pattern, low or decreased QRS voltage to degree of left ventricular thickness, atrio-ventricular conduction disease, disproportionally elevated NT-proBNP to degree of heart failure, persistent elevation in troponin levels, granular sparkling of the myocardium, increased right ventricular wall thickness, increased valve thickness, pericardial effusion, and reduced longitudinal strain with apical sparing pattern, should raise suspicion for cardiac amyloidosis. Both invasive and non-invasive diagnostic modalities are available for cardiac amyloidosis, whereas non-invasive criteria are primarily applicable to transthyretin amyloidosis (ATTR), such as Grade 2 or 3 cardiac uptake at diphosphonate Scintigraphy combining with typical echocardiographic/cardiac magnetic resonance (CMR) findings and negative serum free light chains together with negative serum and urine immunofixation (46, 47). The presence of Congo red-positive deposits on biopsy remains the gold standard for the diagnosis of amyloidosis. Subsequently, accurate typing of the amyloid is critical to guide specific treatment strategies. Mass spectrometry stands as the gold standard for determining the amyloid type (48).
While several staging systems in cardiac amyloidosis have been put forward to facilitate prognosis, there are limited data on how to assess progression (47). This field requires urgent efforts from clinician and researchers. Treatment of cardiac amyloidosis involves supportive care, and specific treatment, such as targeting the production of amyloid precursor protein or the aggregation of amyloid fibrils. Tafamidis has shown efficacy in a randomized trial in patients with wild-type transthyretin and variant transthyretin amyloidosis with cardiomyopathy (49).
4.2.3 Treatment
In the mid-1990s, high-dose melphalan and autologous stem cell transplantation (HDM/SCT) demonstrated positive survival outcomes, and make it a crucial standard of care for early-diagnosed patients (50). Subsequently, in the mid-2000s, oral melphalan with dexamethasone became the standard of care for non-transplant-eligible patients (51). Bortezomib came into view as a third-generation treatment option. The marked excess of misfolded toxic light chains in AL renders plasma cells more sensitive to proteasome inhibition in AL compared to multiple myeloma (52). The combination of bortezomib-dexamethasone with cyclophosphamide (VCD) has shown very good partial responses in more than half of all patients, and complete responses in a quarter of patients (53). However, the recognized cardiac toxicity of proteasome inhibitors raises concerns about their contribution to early deaths in AL. Daratumumab, a high-affinity human IgGκ1 monoclonal antibody targeting CD38, is an antigen ubiquitously expressed all plasma cells, causing cell death by multiple pathways (6). Thus, it reduces the concentration of monoclonal immunoglobulin light chain quickly. Daratumumab has shown efficacy in relapsed AL amyloidosis and is being investigated for in front-line treatment. Clinical trials combining daratumumab with ixazomib, pomalidomide, bortezomib, and dexamethasone are currently underway. However, the limitation of daratumumab lies in its increased risk of infections (54), necessitating large-scale randomized experiments to validate its impact. Despite advancements in therapeutic method leading to gradual improvements in survival rates, little progress has been made in treating advanced patients, and addressing the actual deposits remains challenging (54). New therapies, such as anti-CD38 antibody isatuximab, chimeric antigen receptor T cells, bispecific T-cell engager antibodies, and antibody-drug conjugates, are emerging. Future researches should focus on the drug efficacy through international collaborative clinical trials. Combination anti-plasm cell therapy with above-mentioned new therapies will offer a more complete approach to cure this disease, however, the most reasonable joint scheme, the optimal administration sequence and the safety are directions that need to be explored (55). Additionally, while keywords such as “aggregation,” “fibril formation” and “protein aggregation” experienced a burst in interest 5 years ago, continued attention to basic and translational research on the aggregation and deposition mechanisms of immunoglobulin light chain is warranted, as the underlying mechanisms can provide a theoretical basis for clinical application and new drug development. In a word, the treatment of AL amyloidosis requires comprehensive concept in the future, which still calls for continuous basic and translational research.
5 Advantages and limitations
The current bibliometric investigation offers comprehensive analyses of scholarly outputs in the realm of AL amyloidosis spanning the period from 2005 to 2024, including publication volumes and growth patterns, primary sources, leading authors, collaborative networks, as well as bursts of keywords and references. We simultaneously employed three bibliometric tools, namely CiteSpace, VOSviewer and Biblioshiny package, improving the credibility and robustness of our findings. It is inevitable to acknowledge a limitation of our study, namely, the restriction of our literature research to the WOSCC database. Consequently, despite this database is widely recognized for its comprehensiveness and reliability, its coverage may not encompass all relevant publications on AL amyloidosis. There exists the possibility of overlooking valuable insights and perspectives offered by studies not included in our analysis.
6 Conclusion
This bibliometric analysis examined the research developments in AL amyloidosis over the past two decades using bibliometric software. A total of 2,864 relevant documents were retrieved from the Web of Science Core Collection. Research activity in the field of AL amyloidosis has exhibited a steady increase, with countries such as the United States and various European nations leading in achievements, consistent with the organizations and authors in the field. Notably, publications are predominantly found in journals specializing in amyloid research and hematology. The journal with the highest publication volume is Amyloid-Journal of Protein Folding Disorders. Recent research in this field primarily focuses on two main areas: clinical diagnosis and treatment of AL amyloidosis, as well as cardiac amyloidosis. Emphasis is placed on understanding the mechanisms underlying immunoglobulin light chain aggregation and deposition to mitigate organ involvement.
Statements
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Author contributions
XL: Data curation, Methodology, Software, Visualization, Writing – original draft. JW: Data curation, Methodology, Software, Visualization, Writing – review & editing. YL: Writing – review & editing. WS: Writing – review & editing. XZ: Writing – review & editing. SL: Conceptualization, Funding acquisition, Project administration, Supervision, Writing – review & editing. BC: Conceptualization, Funding acquisition, Project administration, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was financially supported by the Major Program of National Natural Science Foundation of China (No. 82293650/82293651), Postdoctoral Fund of Hebei Medical University (No. 30705010059) and Hebei Province Medical Science Research Project (No. 20240885).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1441032/full#supplementary-material
Footnotes
References
1.
Wechalekar AD Gillmore JD Hawkins PN . Systemic amyloidosis. Lancet. (2016) 387:2641–54. doi: 10.1016/S0140-6736(15)01274-X
2.
Baker KR . Light chain amyloidosis: epidemiology, staging, and prognostication. Methodist Debakey Cardiovasc J. (2022) 18:27–35. doi: 10.14797/mdcvj.1070
3.
Gertz MA Dispenzieri A . Systemic amyloidosis recognition, prognosis, and therapy: a systematic review. JAMA. (2020) 324:79–89. doi: 10.1001/jama.2020.5493
4.
Pick M Lebel E Elgavish S Benyamini H Nevo Y Hertz R et al . Amyloidogenic light chains impair plasma cell survival. Haematologica. (2023) 108:3359–71. doi: 10.3324/haematol.2022.282484
5.
Merlini G Dispenzieri A Sanchorawala V Schönland SO Palladini G Hawkins PN et al . Systemic immunoglobulin light chain amyloidosis. Nat Rev Dis Primers. (2018) 4:38. doi: 10.1038/s41572-018-0034-3
6.
Wechalekar AD Sanchorawala V . Daratumumab in AL amyloidosis. Blood. (2022) 140:2317–22. doi: 10.1182/blood.2021014613
7.
Misra P Ramirez-Alvarado M . Early events in light chain aggregation at physiological pH reveal new insights on assembly, stability, and aggregate dissociation. Amyloid. (2021) 28:113–24. doi: 10.1080/13506129.2021.1877129
8.
Donthu N Kumar S Mukherjee D Pandey N Lim WM . How to conduct a bibliometric analysis: an overview and guidelines. J Bus Res. (2021) 133:285–96. doi: 10.1016/j.jbusres.2021.04.070
9.
Ninkov A Frank JR Maggio LA . Bibliometrics: methods for studying academic publishing. Perspect Med Educ. (2022) 11:173–6. doi: 10.1007/s40037-021-00695-4
10.
Chen C . Searching for intellectual turning points: progressive knowledge domain visualization. Proc Natl Acad Sci USA. (2004) 101:5303–10. doi: 10.1073/pnas.0307513100
11.
van Eck NJ Waltman L . Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics. (2010) 84:523–38. doi: 10.1007/s11192-009-0146-3
12.
Arruda H Silva ER Lessa M Proenca DJ Bartholo R . VOSviewer and bibliometrix. J Med Libr Assoc. (2022) 110:392–5. doi: 10.5195/jmla.2022.1434
13.
Gertz MA Comenzo R Falk RH Fermand JP Hazenberg BP Hawkins PN et al . Definition of organ involvement and treatment response in immunoglobulin light chain amyloidosis (AL): a consensus opinion from the 10th international symposium on amyloid and amyloidosis, tours, France, 18–22 April 2004. Am J Hematol. (2005) 79:319–28. doi: 10.1002/ajh.20381
14.
Kumar S Dispenzieri A Lacy MQ Hayman SR Buadi FK Colby C et al . Revised prognostic staging system for light chain amyloidosis incorporating cardiac biomarkers and serum free light chain measurements. J Clin Oncol. (2012) 30:989–95. doi: 10.1200/JCO.2011.38.5724
15.
Dispenzieri A Gertz MA Kyle RA Lacy MQ Burritt MF Therneau TM et al . Serum cardiac troponins and n-terminal pro-brain natriuretic peptide: a staging system for primary systemic amyloidosis. J Clin Oncol. (2004) 22:3751–7. doi: 10.1200/JCO.2004.03.029
16.
Skinner M Sanchorawala V Seldin DC Dember LM Falk RH Berk JL et al . High-dose melphalan and autologous stem-cell transplantation in patients with al amyloidosis: an 8-year study. Ann Intern Med. (2004) 140:85–93. doi: 10.7326/0003-4819-140-2-200401200-00008
17.
Palladini G Dispenzieri A Gertz MA Kumar S Wechalekar A Hawkins PN et al . New criteria for response to treatment in immunoglobulin light chain amyloidosis based on free light chain measurement and cardiac biomarkers: impact on survival outcomes. J Clin Oncol. (2012) 30:4541–9. doi: 10.1200/JCO.2011.37.7614
18.
Stasi A Mir T Pellegrino A Wani AK Shukla S . Forty years of research and development on forensic genetics: a bibliometric analysis. Forensic Sci Int Genet. (2023) 63:102826. doi: 10.1016/j.fsigen.2023.102826
19.
Fotiou D Theodorakakou F Kastritis E . Biomarkers in al amyloidosis. Int J Mol Sci. (2021) 22:10916. doi: 10.3390/ijms222010916
20.
Kristensen SL Jhund PS Mogensen UM Rorth R Abraham WT Desai A et al . Prognostic value of N-terminal pro-B-type natriuretic peptide levels in heart failure patients with and without atrial fibrillation. Circ Heart Fail. (2017) 10:e004409. doi: 10.1161/CIRCHEARTFAILURE.117.004409
21.
Palladini G Hegenbart U Milani P Kimmich C Foli A Ho AD et al . A staging system for renal outcome and early markers of renal response to chemotherapy in al amyloidosis. Blood. (2014) 124:2325–32. doi: 10.1182/blood-2014-04-570010
22.
Dispenzieri A Kyle RA Gertz MA Therneau TM Miller WL Chandrasekaran K et al . Survival in patients with primary systemic amyloidosis and raised serum cardiac troponins. Lancet. (2003) 361:1787–9. doi: 10.1016/S0140-6736(03)13396-X
23.
Palladini G Barassi A Klersy C Pacciolla R Milani P Sarais G et al . The combination of high-sensitivity cardiac troponin T (hs-cTnT) at presentation and changes in N-terminal natriuretic peptide type B (NT-proBNP) after chemotherapy best predicts survival in AL amyloidosis. Blood. (2010) 116:3426–30. doi: 10.1182/blood-2010-05-286567
24.
Kristen AV Giannitsis E Lehrke S Hegenbart U Konstandin M Lindenmaier D et al . Assessment of disease severity and outcome in patients with systemic light-chain amyloidosis by the high-sensitivity troponin t assay. Blood. (2010) 116:2455–61. doi: 10.1182/blood-2010-02-267708
25.
Buss SJ Emami M Mereles D Korosoglou G Kristen AV Voss A et al . Longitudinal left ventricular function for prediction of survival in systemic light-chain amyloidosis: incremental value compared with clinical and biochemical markers. J Am Coll Cardiol. (2012) 60:1067–76. doi: 10.1016/j.jacc.2012.04.043
26.
Palladini G Campana C Klersy C Balduini A Vadacca G Perfetti V et al . Serum n-terminal pro-brain natriuretic peptide is a sensitive marker of myocardial dysfunction in al amyloidosis. Circulation. (2003) 107:2440–5. doi: 10.1161/01.CIR.0000068314.02595.B2
27.
Kumar S Dispenzieri A Lacy MQ Hayman SR Leung N Zeldenrust SR et al . Serum uric acid: novel prognostic factor in primary systemic amyloidosis. Mayo Clin Proc. (2008) 83:297–303. doi: 10.4065/83.3.297
28.
Palladini G Milani P Basset M Russo F Lavatelli F Nuvolone M et al . Urinary albumin to creatinine ratio in diagnosis and risk stratification of renal al amyloidosis. Amyloid. (2017) 24:68–9. doi: 10.1080/13506129.2017.1293644
29.
Milani P Basset M Russo F Foli A Merlini G Palladini G . Patients with light-chain amyloidosis and low free light-chain burden have distinct clinical features and outcome. Blood. (2017) 130:625–31. doi: 10.1182/blood-2017-02-767467
30.
Muchtar E Gertz MA Kourelis TV Sidana S Go RS Lacy MQ et al . Bone marrow plasma cells 20% or greater discriminate presentation, response, and survival in al amyloidosis. Leukemia. (2020) 34:1135–43. doi: 10.1038/s41375-019-0655-x
31.
Bochtler T Hegenbart U Kunz C Benner A Seckinger A Dietrich S et al . Gain of chromosome 1q21 is an independent adverse prognostic factor in light chain amyloidosis patients treated with melphalan/dexamethasone. Amyloid. (2014) 21:9–17. doi: 10.3109/13506129.2013.854766
32.
Sachchithanantham S Berlanga O Alvi A Mahmood SA Lachmann HJ Gillmore JD et al . Immunoparesis defined by heavy + light chain suppression is a novel marker of long-term outcomes in cardiac al amyloidosis. Br J Haematol. (2017) 179:575–85. doi: 10.1111/bjh.14908
33.
Sidana S Muchtar E Sidiqi MH Jevremovic D Dispenzieri A Gonsalves W et al . Impact of minimal residual negativity using next generation flow cytometry on outcomes in light chain amyloidosis. Am J Hematol. (2020) 95:497–502. doi: 10.1002/ajh.25746
34.
Pudusseri A Sanchorawala V Sloan JM Bever KM Doros G Kataria S et al . Prevalence and prognostic value of D-dimer elevation in patients with al amyloidosis. Am J Hematol. (2019) 94:1098–103. doi: 10.1002/ajh.25576
35.
Jaiswal S Fontanillas P Flannick J Manning A Grauman PV Mar BG et al . Age-related clonal hematopoiesis associated with adverse outcomes. N Engl J Med. (2014) 371:2488–98. doi: 10.1056/NEJMoa1408617
36.
Dispenzieri A Gertz MA Saenger A Kumar SK Lacy MQ Buadi FK et al . Soluble suppression of tumorigenicity 2 (sST2), but not galactin-3, adds to prognostication in patients with systemic AL amyloidosis independent of NT-proBNP and troponin T. Am J Hematol. (2015) 90:524–8. doi: 10.1002/ajh.24001
37.
Waller AH Sanchez-Ross M Kaluski E Klapholz M . Osteopontin in cardiovascular disease: a potential therapeutic target. Cardiol Rev. (2010) 18:125–31. doi: 10.1097/CRD.0b013e3181cfb646
38.
Park KH Han SJ Kim HS Jo SH Kim SA Park WJ . Endothelial function and cardiovascular autonomic activity in neurally mediated syncope. Cardiology. (2016) 134:65–71. doi: 10.1159/000443519
39.
Arenja N Andre F Riffel JH Siepen F Hegenbart U Schonland S et al . Prognostic value of novel imaging parameters derived from standard cardiovascular magnetic resonance in high risk patients with systemic light chain amyloidosis. J Cardiovasc Magn Reson. (2019) 21:53. doi: 10.1186/s12968-019-0564-1
40.
Lin L Li X Feng J Shen KN Tian Z Sun J et al . The prognostic value of T1 mapping and late gadolinium enhancement cardiovascular magnetic resonance imaging in patients with light chain amyloidosis. J Cardiovasc Magn Reson. (2018) 20:2. doi: 10.1186/s12968-017-0419-6
41.
Kastritis E Papassotiriou I Merlini G Milani P Terpos E Basset M et al . Growth differentiation factor-15 is a new biomarker for survival and renal outcomes in light chain amyloidosis. Blood. (2018) 131:1568–75. doi: 10.1182/blood-2017-12-819904
42.
Hayek SS Koh KH Grams ME Wei C Ko Y Li J et al . A tripartite complex of suPAR, APOL1 risk variants and αvβ3 integrin on podocytes mediates chronic kidney disease. Nat Med. (2017) 23:945–53. doi: 10.1038/nm.4362
43.
Li T Huang X Wang Q Zhao L Ren G Chen W et al . A risk stratification for systemic immunoglobulin light-chain amyloidosis with renal involvement. Br J Haematol. (2019) 187:459–69. doi: 10.1111/bjh.16112
44.
Benson MD Buxbaum JN Eisenberg DS Merlini G Saraiva M Sekijima Y et al . Amyloid nomenclature 2018: recommendations by the International Society of Amyloidosis (ISA) nomenclature committee. Amyloid. (2018) 25:215–9. doi: 10.1080/13506129.2018.1549825
45.
Kittleson MM Maurer MS Ambardekar AV Bullock-Palmer RP Chang PP Eisen HJ et al . Cardiac amyloidosis: evolving diagnosis and management: a scientific statement from the American heart association. Circulation. (2020) 142:e7–e22. doi: 10.1161/CIR.0000000000000792
46.
Gillmore JD Maurer MS Falk RH Merlini G Damy T Dispenzieri A et al . Nonbiopsy diagnosis of cardiac transthyretin amyloidosis. Circulation. (2016) 133:2404–12. doi: 10.1161/CIRCULATIONAHA.116.021612
47.
Garcia-Pavia P Rapezzi C Adler Y Arad M Basso C Brucato A et al . Diagnosis and treatment of cardiac amyloidosis. A position statement of the European society of cardiology working group on myocardial and pericardial diseases. Eur J Heart Fail. (2021) 23:512–26. doi: 10.1002/ejhf.2140
48.
Maleszewski JJ . Cardiac amyloidosis: pathology, nomenclature, and typing. Cardiovasc Pathol. (2015) 24:343–50. doi: 10.1016/j.carpath.2015.07.008
49.
Rapezzi C Elliott P Damy T Nativi-Nicolau J Berk JL Velazquez EJ et al . Efficacy of tafamidis in patients with hereditary and wild-type transthyretin amyloid cardiomyopathy: further analyses from ATTR-ACT. JACC Heart Fail. (2021) 9:115–23. doi: 10.1016/j.jchf.2020.09.011
50.
Comenzo RL Vosburgh E Simms RW Bergethon P Sarnacki D Finn K et al . Dose-intensive melphalan with blood stem cell support for the treatment of AL amyloidosis: one-year follow-up in five patients. Blood. (1996) 88:2801–6. doi: 10.1182/blood.V88.7.2801.bloodjournal8872801
51.
Kyle RA Gertz MA Greipp PR Witzig TE Lust JA Lacy MQ et al . A trial of three regimens for primary amyloidosis: colchicine alone, melphalan and prednisone, and melphalan, prednisone, and colchicine. N Engl J Med. (1997) 336:1202–7. doi: 10.1056/NEJM199704243361702
52.
Oliva L Orfanelli U Resnati M Raimondi A Orsi A Milan E et al . The amyloidogenic light chain is a stressor that sensitizes plasma cells to proteasome inhibitor toxicity. Blood. (2017) 129:2132–42. doi: 10.1182/blood-2016-08-730978
53.
Palladini G Sachchithanantham S Milani P Gillmore J Foli A Lachmann H et al . A European collaborative study of cyclophosphamide, bortezomib, and dexamethasone in upfront treatment of systemic al amyloidosis. Blood. (2015) 126:612–5. doi: 10.1182/blood-2015-01-620302
54.
Kastritis E Palladini G Minnema MC Wechalekar AD Jaccard A Lee HC et al . Daratumumab-based treatment for immunoglobulin light-chain amyloidosis. N Engl J Med. (2021) 385:46–58. doi: 10.1056/NEJMoa2028631
55.
Wang J Li J Zhong L . Current status and prospect of anti-amyloid fibril therapy in AL amyloidosis. Blood Rev. (2024) 66:101207. doi: 10.1016/j.blre.2024.101207
Summary
Keywords
AL amyloidosis, light chain amyloidosis, bibliometrics, research trend, Web of Science
Citation
Liu X, Wang J, Li Y, Shi W, Zhang X, Li S and Cong B (2024) A bibliometric analysis of light chain amyloidosis from 2005 to 2024: research trends and hot spots. Front. Med. 11:1441032. doi: 10.3389/fmed.2024.1441032
Received
30 May 2024
Accepted
10 July 2024
Published
30 July 2024
Volume
11 - 2024
Edited by
Ahmet Emre Eskazan, Istanbul University-Cerrahpasa, Türkiye
Reviewed by
Ayse Salihoglu, Istanbul University Cerrahpasa, Türkiye
Zuzana Chyra, University of Ostrava, Czechia
Updates
Copyright
© 2024 Liu, Wang, Li, Shi, Zhang, Li and Cong.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shujin Li, shujinli@hebmu.edu.cnBin Cong, cong6406@hebmu.edu.cn
†These authors have contributed equally to this work and share first authorship
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.