 Denise Vianna Machado Ayres1
Denise Vianna Machado Ayres1 Sabrina Saemy Tome Uchiyama2
Sabrina Saemy Tome Uchiyama2 Andréa Oliveira Prates1
Andréa Oliveira Prates1 Rosana Aparecida Freitas Lopes1
Rosana Aparecida Freitas Lopes1 Antenor Bispo Santos Silva1Denise Rodrigues Tsukimoto1Rosimeire Alves Amorim1Taynah Souza Ribeiro1
Antenor Bispo Santos Silva1Denise Rodrigues Tsukimoto1Rosimeire Alves Amorim1Taynah Souza Ribeiro1 Artur Cesar Aquino Santos1
Artur Cesar Aquino Santos1 André Tadeu Sugawara1,2
André Tadeu Sugawara1,2 Marcos Montagnini3
Marcos Montagnini3 Linamara Rizzo Battistella1,2
Linamara Rizzo Battistella1,2 Marta Imamura1,2*
Marta Imamura1,2*- 1Instituto de Medicina Fisica e Reabilitacao, IMREA, Hospital das Clínicas HCFMUSP, Faculdade de Medicina FMUSP, Universidade de São Paulo, São Paulo, Brazil
- 2Departamento de Medicina Legal, Bioetica, Medicina do Trabalho e Medicina Fisica e Reabilitacao, Faculdade de Medicina da Universidade de São Paulo, FMUSP, São Paulo, Brazil
- 3Division of Geriatric and Palliative Medicine, University of Michigan, Ann Arbor, MI, United States
Background: Knee osteoarthritis (KOA) is the most common form of arthritis in adults and a leading cause of years lived with disability, representing a significant burden on healthcare worldwide.
Objective: Describe the structure and educational elements of the Knee-SCHOOL, a brief patient-centered multidisciplinary educational program for patients with KOA.
Design: Observational prospective study.
Setting: Academically affiliated rehabilitation outpatient center in Brazil.
Methods: The program consisted of three in-person educational sessions (4.5 hr each) for 55 community dwelling adults, aged ≥50 years, with primary KOA-related pain. Study measures included demographic data (age, sex, and educational level), pain duration (years), pain intensity (visual analogue scale), affected knee (right, left, or both knees), comorbidities (presence of hypertension, diabetes, and hypercholesterolemia), Body Mass Index (BMI), Bristol Stool Scale, Adapted Healthy Eating Index (AHEI), bioelectrical impedance, daytime sleepiness, and the impact of the KOA on pain, symptoms, activities of daily living, recreation, and quality of life. Participants attended educational sessions delivered by a multidisciplinary team (two physicians, two nurses, two physical therapists, one occupational therapist, one dietitian, one psychologist, one social worker, and one physical educator) addressing several aspects of KOA. They also participated in supervised exercise practice and a home exercise program.
Results: Fifty-five subjects completed the study. The mean age was 67.73 (± 7.73) years; most were females (70.9%), 92.7% had bilateral KOA, with mean pain duration of 12.41 (± 10.17) years. The mean BMI was 32.52 (± 5.99), 65.5% were obese, and 96.4% reported an inadequate diet. KOA had a more negative impact on sports, recreation and quality of life. Daytime sleepiness was uncommon. The mean pain intensity, measured with visual analogue scale, score reduced from 5.52 (± 2.11) at baseline to 4.04 (± 2.38) after the program (week 2). The effect size was 0.7 (95% CI 0.32 to 1.07). All participants received the program well, with no drop-out rates or reported adverse events.
Conclusion: The Knee-SCHOOL utilized a multidisciplinary educational approach and an exercise practice addressing multiple aspects of KOA pain. While more studies are needed to assess the longitudinal impact of the program, it was promising in managing pain.
Introduction
Knee osteoarthritis (KOA) is the most common type of arthritis in adults and a leading cause of years lived with disability (1). It also represents a significant financial burden on healthcare systems worldwide (1). The global prevalence of KOA was approximately 600 million in 2020 and is estimated to increase by almost 75% in 2050 (1). In addition to chronic pain and physical disability, patients with KOA frequently experience sleep problems (2, 3) and psychological symptoms, including depression and anxiety (4, 5). Population studies demonstrate a higher prevalence of KOA in women, older patients, and patients with obesity (6–8). In addition, there are increased cardiovascular risk factors in patients with KOA (9–12).
The overall management of KOA includes proper analgesia and improved function and quality of life. Pharmacological interventions for KOA-related pain include topical analgesics (such as diclofenac gel and capsaicin), oral analgesics (like non-steroidal anti-inflammatory drugs (NSAIDs), acetaminophen, paracetamol, and duloxetine), and intra-articular therapy (such as steroids and hyaluronic acid) (13). Non-pharmacological agents including complementary and integrative health interventions such as acupuncture (14), meditation and yoga (15), tai chi (16), and transcutaneous electrical nerve stimulation (17) improve pain and function in patients with KOA. Self-management is considered a mainstay approach for the management of osteoarthritis (OA) (18). It involves the patient actively managing the chronic condition. Self-management can be achieved through educational interventions focused on enhancing the understanding of the disease, pain management, establishing an exercise routine and activity pacing, weight loss, sleep, and other modifiable risk factors, including joint alignment and joint preservation (19–22).
Several studies demonstrated the benefits of patient education and exercise therapy in osteoarthritis-related pain (23–25). Hansson et al. (26) demonstrated that patient education is feasible and can improve self-perceived health and function in primary care patients with KOA. In addition, recent systematic reviews documented that patient education effectively reduces pain related to knee and hip OA (23), and combination therapy of exercise and education interventions improves physical activity and pain reduction in knee and hip OA (24, 25).
KOA represents a significant health system burden in Latin America (27). In Brazil, KOA has become a significant public health concern due to the growth of the aging population. It is estimated that 9.6% of Brazilians over 39 years of age suffer from KOA (28). Despite being one of the largest public health systems in the world (29), Brazil has historically lacked public health policies addressing the management of OA in the general population (30). In 2018, the Brazilian Ministry of Health launched a health systems research initiative focusing on interventions to improve the care of individuals with disabilities. Researchers from our institution, the Instituto de Medicina Física e Reabilitação (Instituto de Medicina Física e Reabilitação do Hospital das Clínicas da, Faculdade de Medicina da Universidade de São Paulo - IMREA HCFMUSP), successfully obtained grant funding under this governmental initiative to develop a clinical trial for studying interventions for KOA-related pain. The initial phase of this clinical trial involved implementing a multidisciplinary educational program for managing pain in a sample of community-dwelling adults with chronic pain related to KOA, the Knee- SCHOOL.
The goal of this paper is to describe the structure and educational elements of the Knee-SCHOOL. We also explore the impact of this program on reducing pain in patients with KOA.
Materials and methods
This is a descriptive and observational prospective study of a multidisciplinary educational program for community-dwelling adults with KOA. The study is part of a major Randomized Clinical Trial (RCT) conducted at IMREA HCFMUSP, a teaching hospital of the University of São Paulo School of Medicine and approved by the Institution Review Board (CAAE: 0875619.8.000.0068). IMREA is accredited by the Commission on Accreditation of Rehabilitation Facilities (CARF) and fully integrated into the public health system, providing tertiary care in an academic setting.
Study participants were recruited from the institution’s patient registry and the community. In addition, patients referred to IMREA for pain related to KOA were screened to participate in the study. Study investigators assessed eligibility for the study by reviewing medical records, radiologic data, and by patient interviews.
The inclusion criteria included patients older than 50 years and with moderate to severe pain related to KOA for at least 3 months duration who met the American College of Rheumatology (31) and the Kellgren-Lawrence radiographic grading criteria (32) for primary KOA.
The exclusion criteria included patients with severe psychological or psychiatric diseases, fibromyalgia, systemic inflammatory rheumatic diseases and neoplasia. Patients with other forms of KOA (e.g., post-traumatic, inflammatory and hemosiderosis arthritis) were excluded from the study. Participation was voluntary and all patients provided informed consent before enrollment.
Study measures included demographic (age, sex, and educational level), pain duration and intensity, affected knee (right, left, or both knees), comorbidities, and Body Mass Index and other nutritional measures, daytime sleepiness, and the patient’s rating of the KOA on five domains: pain, symptoms, activities of daily living, sports/recreation activities, and quality of life. Frequency of attendance was captured and recorded as patient participation.
Pain intensity was assessed using a 10-cm visual analogue scale (VAS) at the beginning and end of the program. The participants were instructed to mark their perceived pain intensity on the scale (zero: no pain, 10: the worst possible pain).
The Knee injury and osteoarthritis outcome score (KOOS) (33) was used to evaluate patient’s opinion about their knee and associated problems. It is a self-administered questionnaire that evaluates five outcomes related to KOA: pain, symptoms, and activities of daily living, sports /recreational activities, and quality of life. The scoring is based on a 0 to 100 scale, where zero represents severe knee problems and 100 indicates no knee issues.
The nutritional measures included information on Body Mass Index (BMI), bowel habits based on the Bristol scale (34), Adapted Healthy Eating Index (AHEI), bioelectrical impedance, and comorbidities (diabetes, hypertension, and hyperlipidemia).
The nutritional status was classified based on the BMI cut-off points adopted by the Pan American Health Organization (PAHO) for the SABE Study: ≤23 kg/m2 = underweight; >23.0 and < 28.0 kg/m2 = normal weight; ≥28.0 and < 30.0 kg/m2 = overweight; ≥30.0 kg/m2 = obesity (35).
The Bristol Stool Scale is a tool used to assess the shape and consistency of stool; the scale categorizes stool into seven types based on shape and consistency (34). Stool shape and consistency is categorized as: Type 1: Separate small lumps, Type 2: Sausage-shaped with irregular surface. Type 3: Sausage-shaped with smooth surface. Type 4: Smooth sausage or cylinder. Type 5: Ball or oval-shaped. Type 6: Flaky or fragmented. Type 7: Liquid or completely unformed. Types 3 and 4 are considered normal.
The Avanturi nutritional analysis software program was used to calculate the 24-hour food record (Santana RI. Avanturi: nutritional assessment software, version 4.0. Rio de Janeiro, 2009). Eating habits were calculated using the adapted Brazilian version of the Healthy Eating Index (36). This index evaluates 12 components, including food groups such as cereals, fruits, vegetables, legumes, meats, dairy products, oils and fats, sweets and sugars, as well as nutrients (total fat, saturated fat, and cholesterol) and food variety. Diets scoring below 71 points on the AHEI are classified as poor quality, while those between 71 and 100 need improvement, and above 100 are considered good quality (36). Poor quality and need improvement categories were considered as inadequate diets.
A bioelectrical impedance test was also performed using the InBody 370S device (Ottoboni, Rio de Janeiro, Brazil). BMI, fat percentage, and skeletal muscle mass index (SMI) were calculated as body composition measures.
The Epworth Sleepiness Scale (ESS) (37) was used to evaluate the degree of daytime sleepiness. It is a self-administered questionnaire that assesses the probability of falling asleep in eight everyday situations. The scoring for each item varies from 0 (no chance of napping) to 3 (great probability of napping). The total score is based on a scale of 0 to 24. A score of ≥11 was defined to indicate daytime sleepiness.
Program structure
The Knee-SCHOOL consisted of three face-to-face educational sessions of 4.5 hr each over two consecutive weeks. Each session was limited to ten participants. The sessions included presentations by the members of the multidisciplinary research team, including two Physical Medicine and Rehabilitation physicians, two nursing professionals, two dietitians, two physiotherapists, one occupational therapist, one psychologist, one social worker, and one physical educator. The sessions also included supervised exercise practice; all participants received a prescription for home exercises. Table 1 describes the educational content of each session.
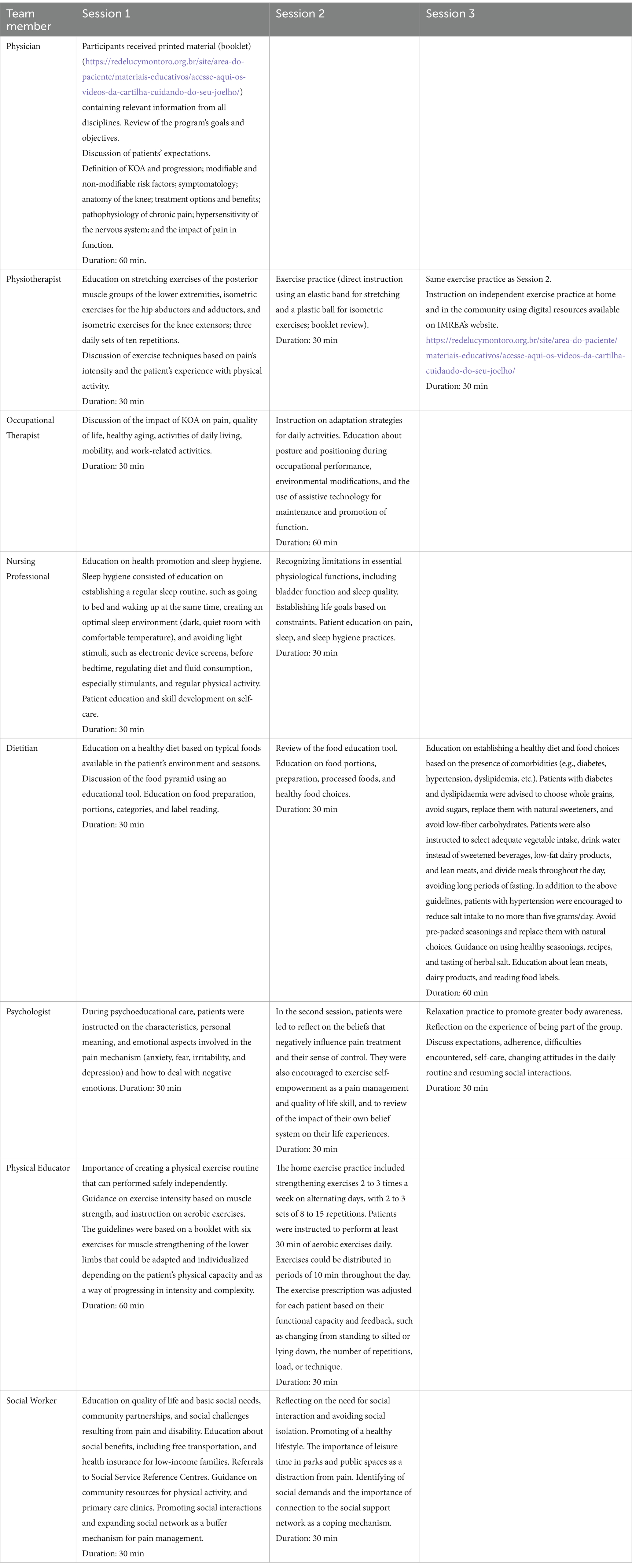
Table 1. Educational content of the Knee-SCHOOL.
In addition to attending the educational sessions, participants received printed materials containing the educational content from each discipline, exercise instruction, and links to educational videos on the IMREA website.1 The use of the content on the IMREA website was strongly emphasized for the home exercise program.
Each educational session began with an interactive discussion about the session objectives, patients’ goals and expectations, feedback on their exercise routine, and general questions. The research team met weekly to review the program logistics and discuss each patient’s needs. Elements of the program, such as exercise prescription and dietary plans, were individualized based on the patient’s feedback, physical limitations, exercise tolerance, and comorbidities. Patients were instructed to complete their exercise prescription for at least 30 min daily, however, no log was required from the participants. The study social workers assisted in identifying local facilities for the daily exercise routine if desired by the patient. We have not monitored analgesic medication use, however, patients were instructed to maintain their prescribed or over-the-counter analgesic regimen.
Statistical analysis
The baseline characteristics were described as means and standard deviations for continuous variables and percentages for categorical variables. Pain intensity was assessed for each knee (R and L) with the VAS at baseline (Session 1) and at the completion of the program (Session 3). The mean pain level for each knee was tested for normality with the Shapiro–Wilk test. Comparisons before and after the intervention were conducted using the Student’s T-test for dependent samples and the Welch approximation for different variances. For the VAS, a significance of 0.05 was established, and the Cohen’s d effect size was calculated for significant differences. All statistical analyses were conducted with STATA14®.
Results
We recruited 176 participants and 55 were enrolled in the study. The study was conducted from February 2022 through July 2023. All fifty-five subjects completed the Knee-SCHOOL program. Six (10.91%) patients attended one of the sessions online due to the inability to attend the class in person. No adverse events were reported.
Table 2 outlines the characteristics of the participants. The mean age was 67.73 (± 7.73) years; most were females (70.9%), and fifty-one (92.7%) had bilateral KOA. The mean BMI was 32.52 (± 5.99), 65.5% were obese (>30 kg/m2), and 96.4% reported an inadequate diet. Most participants had normal bowel function. According to the KOOS, KOA had a more negative impact on sports and recreation and quality of life. Daytime sleepiness, measured by the EES, was uncommon among participants.
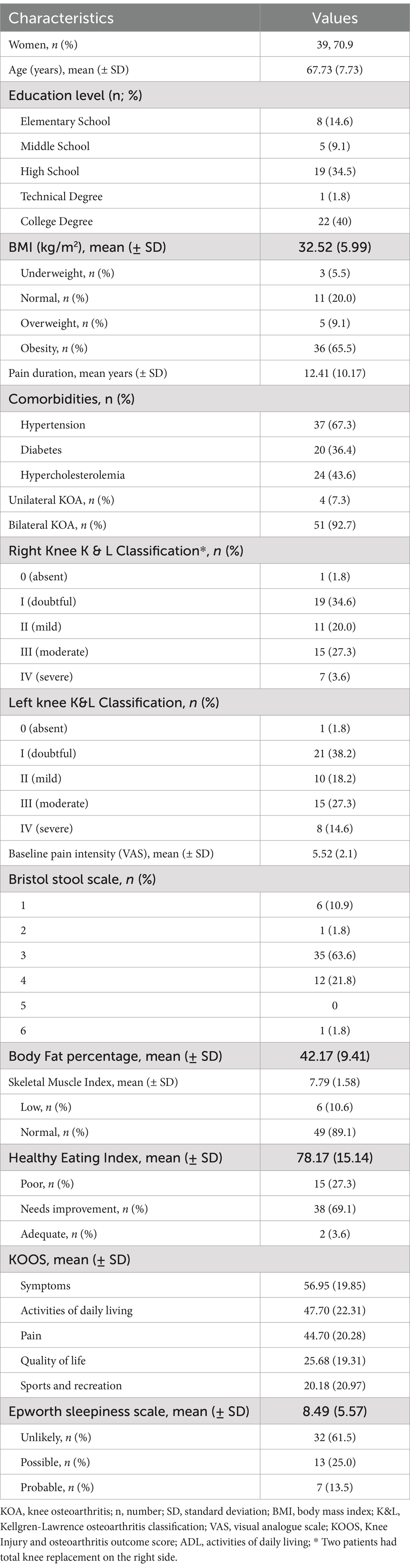
Table 2. Baseline characteristics of study participants (n = 55).
The Shapiro–Wilk test demonstrated that the pain intensity at baseline and at completion of the study was parametric (p > 0.05) regardless of the side, and the variances were similar along the pain measures. Therefore, the comparisons were conducted with paired Student T-tests without corrections. The mean pain level decreased from 5.52 (± 2.11) at baseline (Session 1) to 4.04 (± 2.38) at completion of the study (Session 3), a mean reduction of 1.48 points (± 2.37). This reduction was statistically significant (p = 0.0001) with Cohen’s d effect sizes of 0.70 (CI95% 0.32 to 1.07) (Figure 1).
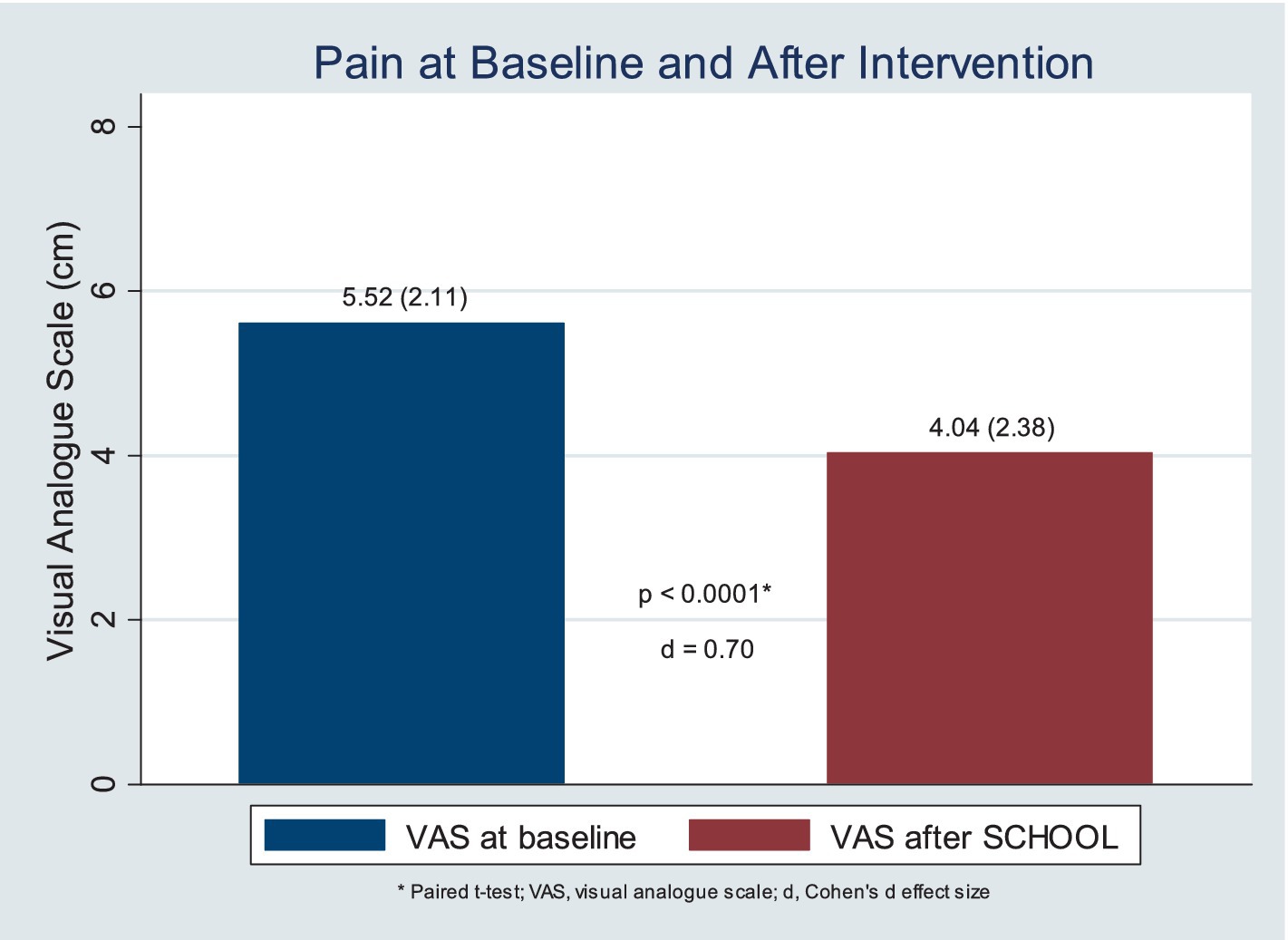
Figure 1. Pain reduction after the Knee-SCHOOL, per visual analogue scale.
Discussion
The Knee-SCHOOL is unique because it incorporates a comprehensive face-to-face educational component customized to each patient, and it can be completed in less than 2 weeks. The program covers disease understanding, treatment options, self-management strategies, and coping mechanisms. Additionally, it provides education on physical activity, lifestyle changes, sleep hygiene, nutritional health, and the psychosocial aspects of pain. It includes an exercise plan tailored to the patient’s physical abilities and tolerance. Moreover, it uses booklets and web-based resources to reinforce the educational content covered during the in-person sessions and the home exercise practice (see footnote 1).
Existing self-management programs for KOA often only cover patient education and physical exercise (19–25). The Knee-SCHOOL, however, provides a more comprehensive approach by addressing additional elements, such as nutritional health, sleep hygiene, and psychosocial factors. It is grounded on a solid multidisciplinary team, so all those elements can be adequately addressed.
Physical exercise is a core component in any self-management program for KOA. Exercise programs are safe and effective for pain and strength improvement in KOA (19–25, 38). The Knee-SCHOOL strongly emphasizes the importance of physical activity, and each patient receives an individualized prescription containing stretching and strengthening exercises based on their physical ability. Patients unable to perform exercises in a standing position are taught exercises that can be performed on a chair or lying down. A walking routine is also integrated into the program. The physical therapists and physical educator supervise each patient individually to ensure they learn their exercise routine correctly. In addition, patients are encouraged to access the exercise videos on the IMREA website for their home exercise program.
KOA significantly affects a person’s daily life, causing difficulties in performing activities of daily living (ADL) (39), limited mobility, and reduced participation in work-related activities. Individuals with KOA attribute their difficulty in performing daily activities to symptoms such as pain and limitations in performing essential tasks. In our program, Occupational Therapists assess ADL performance, teach adaptation strategies, and use assistive technology to maintain and promote functionality.
The Knee-SCHOOL prioritizes nutritional health and uses various measures to assess nutritional status. Most participants were found to be overweight or obese, which is consistent with findings in other studies (40). BMI is linked to the severity of pain and should be routinely assessed in pain management educational programs (41). In addition to BMI, our program includes a more in-depth assessment of the patient’s body composition. Some patients were identified as having a low skeletal mass index. We also discovered that a significant number of individuals had unhealthy eating habits, systemic hypertension, and dyslipidemia.
We provide general nutritional education and personalized dietary plans to address these findings. Poor diet is associated with an inflammatory status that can exacerbate symptoms of KOA (42, 43). Proper education on food quality, quantity, meal intervals, and eating habits is also essential to the Knee-SCHOOL (44). Compared to other studies (45, 46), the nutrition education component in our program was much more comprehensive and personalized.
Nursing professionals provided education on the basic physiological functions of the body and other aspects of health education, including an assessment of sleep and education on sleep hygiene. Despite evidence linking sleep duration, restlessness, and sleep quality to KOA (2, 3), sleep is often overlooked in exiting self-management programs for KOA (19, 21, 23–25). We found only two KOA educational programs (45, 47) addressing sleep hygiene, and none included a formal assessment of daytime sleepiness. Restful sleep improves the body’s inflammatory response (48) and can reduce pain and stiffness in KOA, improving quality of life (49). Conversely, lack of sleep or poor-quality sleep can worsen pain perception and affect mood, creating a harmful cycle of insomnia and chronic pain (49). In our study, some participants reported possible or probable excessive daytime sleepiness, and one patient was later diagnosed with sleep apnea. It is essential to routinely assess sleep dysfunction in any self-management program for OA, provide proper education on sleep hygiene, and ensure that patients with more severe symptoms are appropriately evaluated for sleep disorders.
Some educational programs for OA include community resources education (50). Our team social worker provided education on community resources for exercise practice, social benefits, and the importance of having a solid network and social activities, as chronic pain usually causes social isolation and sedentarism.
Another significant component of the Knee-SCHOOL is the education on the psychological aspects of chronic pain. Strong emphasis was given to teaching patients to recognize and reconstruct negative thoughts and behaviors associated with chronic pain, as pain evokes brain modifications (nociplasticity) as an unconscious and involuntary learning process. Such thoughts and behaviors negatively affect patients and their family members (51). Educating and promoting experiences addressing negative ruminations can enhance social support and positive outcomes (52). During the Knee-SCHOOL, patients also received instruction on self-guided relaxation to increase body awareness and relaxation and to improve self-efficacy. Promoting social interactions in the community and within the group was another crucial element, as group-based interventions effectively manage chronic pain (53). The Psychologist promoted group discussions and interactions so participants could share their experiences with the program and reflect on the difficulties and challenges of changing attitudes and behaviors in daily life. Group members supported each other and shared their experiences on solutions to similar challenges.
The multidisciplinary team’s awareness of the importance of lifestyle modifications may play a role in empowering patients to make behavioral changes. Group-based educational intervention allows individuals to develop tools for self-management, enabling them to manage their conditions more effectively (54). Information does not guarantee adherence or modification to different programs (55). What sets the Knee-SCHOOL apart is its focus on lifestyle awareness through a patient-centered multidisciplinary team that includes peer participation from individuals with KOA, facilitating the exchange of information, experiences, and practical strategies. A meta-analysis suggests that strategies aimed at motivating or changing behaviour can enhance adherence to exercise (56), whereas coping counselling and exercise recommendations through audio/video or text message encouragement alone did not significantly improve adherence (56, 57).
All participants received the program well, with no drop-out rates or reported adverse events. Based on the preliminary findings on pain, the Knee-SCHOOL is being considered as the initial step in the treatment plan of patients referred to our institution for KOA-related pain. Also, we observed a reduction in pain level in the short-term, with a Cohen d effect size of 0.7, even though this result should be seen with caution, as no control group was included in this analysis.
Some of the study’s limitations include a small sample size, the absence of a control group, and the lack of measurement of pain beyond the program duration. Additionally, our study does not capture changes in quality of life, functional status, nutritional health, and sleep status following the completion of the program. The Knee-SCHOOL is the initial intervention of a large clinical trial involving other therapies for KOA-related pain. Upon the trial’s completion, data on the long-term effects of the Knee-SCHOOL and the different interventions on pain and additional outcomes will be reported. We have not controlled for analgesic medication use; however, patients reported no changes to the analgesic medication used during the study. Moreover, the Knee-SCHOOL also uses a robust multidisciplinary approach, which may limit its reproducibility in less resourced settings.
Conclusion
The Knee-SCHOOL employed a comprehensive and team-based educational approach to address pain’s physical, functional, nutritional, and psychological aspects. The program used a patient-centered approach and emphasized collaboration among the healthcare team as a crucial element. It showed promising results in managing KOA-related pain, however future research is also needed to evaluate the long-term impact of Knee-SCHOOL on pain and other outcomes, as well as its applicability in different environments and cultures.
Data availability statement
The data presented in this article is available upon request. Please submit an inquiry to Dr. Marta Imamura on the following email address: bWFydGEuaW1hbXVyYUBmbS51c3AuYnI=.
Ethics statement
The studies involving humans were approved by Comissão de Ética para Análise de Projetos de Pesquisa do HCFMUSP. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
DA: Conceptualization, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. SU: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. AP: Investigation, Methodology, Writing – original draft, Writing – review & editing. RL: Investigation, Methodology, Writing – original draft, Writing – review & editing. ASi: Investigation, Writing – original draft, Writing – review & editing. DT: Investigation, Methodology, Writing – review & editing. RA: Investigation, Writing – original draft. TR: Investigation, Writing – review & editing. ASa: Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. ASu: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. MM: Conceptualization, Methodology, Validation, Visualization, Writing – review & editing. LB: Conceptualization, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – review & editing, Funding acquisition, Resources. MI: Conceptualization, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by a grant from the Brazilian Ministry of Health (PRONAS; NUP: 25000.014364/2018-35).
Acknowledgments
Patients or the public were not involved in the design, conduct, reporting, or dissemination plans of our research.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^https://redelucymontoro.org.br/site/area-do-paciente/materiais-educativos/acesse-aqui-os-videos-da-cartilha-cuidando-do-seu-joelho/
References
1. GBD 2021 Osteoarthritis Collaborators. Global, regional, and national burden of osteoarthritis, 1990-2020 and projections to 2050: a systematic analysis for the global burden of disease study 2021. Lancet Rheumatol. (2023) 5:e508–22. doi: 10.1016/S2665-9913(23)00163-7
2. Cho, Y, Jung, B, Lee, YJ, Kim, MR, Kim, EJ, Sung, WS, et al. Association between sleep duration and osteoarthritis and their prevalence in Koreans: a cross-sectional study. PLoS One. (2020) 15:e0230481. doi: 10.1371/journal.pone.0230481
3. Lapane, KL, Shridharmurthy, D, Harkey, MS, Driban, JB, Dubé, CE, and Liu, SH. The relationship between restless sleep and symptoms of the knee: data from the osteoarthritis initiative. Clin Rheumatol. (2021) 40:2167–75. doi: 10.1007/s10067-020-05531-4
4. Aqeel, M, Rehna, T, and Sarfraz, R. The association among perception of osteoarthritis with adverse pain anxiety, symptoms of depression, positive and negative affects in patients with knee osteoarthritis: a cross sectional study. J Pak Med Assoc. (2021) 71:645–50. doi: 10.47391/JPMA.862
5. Poon, CL, Cheong, P, Tan, JW, Thumboo, J, Woon, EL, Clark, RA, et al. Associations of the modified STarT back tool and hospital anxiety and depression scale (HADS) with gait speed and knee pain in knee osteoarthritis: a retrospective cohort study. Disabil Rehabil. (2022) 44:4452–8. doi: 10.1080/09638288.2021.1883750
6. Reyes, C, Leyland, KM, Peat, G, Cooper, C, Arden, NK, and Prieto-Alhambra, D. Association between overweight and obesity and risk of clinically diagnosed knee, hip, and hand osteoarthritis: a population-based cohort study. Arthritis Rheumatol. (2016) 68:1869–75. doi: 10.1002/art.39707
7. Pacca, DM, de-Campos, GC, Zorzi, AR, Chaim, EA, and de-Miranda, JB. Prevalence of joint pain and osteoarthritis in obese Brazilian population. Arq Bras Cir Dig. (2018) 31:e1344. doi: 10.1590/0102-672020180001e1344
8. Go, DJ, Kim, DH, Guermazi, A, Crema, MD, Hunter, DJ, Hwang, HS, et al. Metabolic obesity and the risk of knee osteoarthritis progression in elderly community residents: a 3-year longitudinal cohort study. Int J Rheum Dis. (2022) 25:192–200. doi: 10.1111/1756-185X.14255
9. Hawker, GA, Croxford, R, Bierman, AS, Harvey, PJ, Ravi, B, Stanaitis, I, et al. All-cause mortality and serious cardiovascular events in people with hip and knee osteoarthritis: a population-based cohort study. PLoS One. (2014) 9:e91286. doi: 10.1371/journal.pone.0091286
10. Hall, AJ, Stubbs, B, Mamas, MA, Myint, PK, and Smith, TO. Association between osteoarthritis and cardiovascular disease: systematic review and meta-analysis. Eur J Prev Cardiol. (2016) 23:938–46. doi: 10.1177/2047487315610663
11. Wang, H, Bai, J, He, B, Hu, X, and Liu, D. Osteoarthritis and the risk of cardiovascular disease: a meta-analysis of observational studies. Sci Rep. (2016) 6:39672. doi: 10.1038/srep39672
12. Park, D, Park, YM, Ko, SH, Choi, YH, Min, DU, Ahn, JH, et al. Association between knee osteoarthritis and the risk of cardiovascular disease and the synergistic adverse effects of lack of exercise. Sci Rep. (2023) 13:2777. doi: 10.1038/s41598-023-29581-1
13. Jang, S, Lee, K, and Ju, JH. Recent updates of diagnosis, pathophysiology, and treatment on osteoarthritis of the knee. Int J Mol Sci. (2021) 22:2619. doi: 10.3390/ijms22052619
14. Li, S, Xie, P, Liang, Z, Huang, W, Huang, Z, Ou, J, et al. Efficacy comparison of five different acupuncture methods on pain, stiffness, and function in osteoarthritis of the knee: a network meta-analysis. Evid Based Complement Alternat Med. (2018) 2018:1638904. doi: 10.1155/2018/1638904
15. Park, J, McCaffrey, R, Newman, D, Liehr, P, and Ouslander, JG. A pilot randomized controlled trial of the effects of chair yoga on pain and physical function among community-dwelling older adults with lower extremity osteoarthritis. J Am Geriatr Soc. (2017) 65:592–7. doi: 10.1111/jgs.14717
16. Wang, C, Schmid, CH, Iversen, MD, Harvey, WF, Fielding, RA, Driban, JB, et al. Comparative effectiveness of tai chi versus physical therapy for knee osteoarthritis: a randomized trial. Ann Intern Med. (2016) 165:77–86. doi: 10.7326/M15-2143
17. Wu, Y, Zhu, F, Chen, W, and Zhang, M. Effects of transcutaneous electrical nerve stimulation (TENS) in people with knee osteoarthritis: a systematic review and meta-analysis. Clin Rehabil. (2022) 36:472–85. doi: 10.1177/02692155211065636
18. Ahmad, MA, Yusof, A, Hamid, MSA, Zulkifli Amin, FH, Kamsan, SS, Ag Daud, DM, et al. Effects of self-management program as adjunctive to usual rehabilitation exercise on pain and functional outcomes in knee osteoarthritis: a randomized controlled trial. J Res Health Sci. (2023) 23:e00569. doi: 10.34172/jrhs.2023.104
19. Rausch Osthoff, AK, Niedermann, K, Braun, J, Adams, J, Brodin, N, Dagfinrud, H, et al. 2018 EULAR recommendations for physical activity in people with inflammatory arthritis and osteoarthritis. Ann Rheum Dis. (2018) 77:1251–60. doi: 10.1136/annrheumdis-2018-213585
20. Bannuru, RR, Osani, MC, Vaysbrot, EE, Arden, NK, Bennell, K, Bierma-Zeinstra, SMA, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr Cartil. (2019) 27:1578–89. doi: 10.1016/j.joca.2019.06.011
21. World Health Organization. Package of interventions for rehabilitation. Module 2. Musculoskeletal conditions. Geneva: World Health Organization (2023).
22. Krishnamurthy, A, Lang, AE, Pangarkar, S, Edison, J, Cody, J, and Sall, J. Synopsis of the 2020 US Department of veterans affairs/US Department of defense clinical practice guideline: the non-surgical Management of hip and Knee Osteoarthritis. Mayo Clin Proc. (2021) 96:2435–47. doi: 10.1016/j.mayocp.2021.03.017
23. Sinatti, P, Sánchez Romero, EA, Martínez-Pozas, O, and Villafañe, JH. Effects of patient education on pain and function and its impact on conservative treatment in elderly patients with pain related to hip and knee osteoarthritis: a systematic review. Int J Environ Res Public Health. (2022) 19:6194. doi: 10.3390/ijerph19106194
24. Sasaki, R, Honda, Y, Oga, S, Fukushima, T, Tanaka, N, Kajiwara, Y, et al. Effect of exercise and/or educational interventions on physical activity and pain in patients with hip/knee osteoarthritis: a systematic review with meta-analysis. PLoS One. (2022) 17:e0275591. doi: 10.1371/journal.pone.0275591
25. Lesmond, I, Calvache-Mateo, A, Heredia-Ciuró, A, Martín-Núñez, J, Navas-Otero, A, López-López, L, et al. Neurophysiological pain education for patients with symptomatic knee osteoarthritis: a systematic review and meta-analysis. Patient Educ Couns. (2024) 120:108128. doi: 10.1016/j.pec.2023.108128
26. Hansson, EE, Jönsson-Lundgren, M, Ronnheden, AM, Sörensson, E, Bjärnung, A, and Dahlberg, LE. Effect of an education programme for patients with osteoarthritis in primary care - a randomized controlled trial. BMC Musculoskelet Disord. (2010) 11:1–7. doi: 10.1186/1471-2474-11-244
27. de Andrade, DC, Saaibi, D, Sarría, N, Vainstein, N, Ruiz, LC, and Espinosa, R. Assessing the burden of osteoarthritis in Latin America: a rapid evidence assessment. Clin Rheumatol. (2022) 41:1285–92. doi: 10.1007/s10067-022-06063-9
28. Miguel, RCC, Machado, LA, Costa-Silva, L, Telles, RW, and Barreto, SM. Performance of distinct knee osteoarthritis classification criteria in the ELSA-Brasil musculoskeletal study. Clin Rheumatol. (2019) 38:793–802. doi: 10.1007/s10067-018-4347-0
29. Demo, MLO, Orth, LC, and Marcon, CEM. Brazil’s health-care system. Lancet. (2019) 394:1992. doi: 10.1016/S0140-6736(19)32630-3
30. Burgos-Vargas, R, Cardiel, MH, Loyola-Sánchez, A, De Abreu, MM, Pons-Estel, BA, Rossignol, M, et al. Characterization of knee osteoarthritis in Latin America. A comparative analysis of clinical and health care utilization in Argentina, Brazil, and Mexico. Reumatol Clin. (2014) 10:152–9. doi: 10.1016/j.reuma.2013.07.013
31. Altman, R, Asch, E, Bloch, D, Bole, G, Borenstein, D, Brandt, K, et al. Development of criteria for the classification and reporting of osteoarthritis: classification of osteoarthritis of the knee. Arthritis Rheum. (1986) 29:1039–49. doi: 10.1002/art.1780290816
32. Kellgren, JH, and Lawrence, JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. (1957) 16:494–502. doi: 10.1136/ard.16.4.494
33. Roos, EM, and Toksvig-Larsen, S. Knee injury and osteoarthritis outcome score (KOOS) - validation and comparison to the WOMAC in total knee replacement. Health Qual Life Outcomes. (2003) 1:17. doi: 10.1186/1477-7525-1-17
34. Martinez, AP, and Azevedo, GR. The Bristol stool form scale: its translation to Portuguese, cultural adaptation and validation. Rev Lat Am Enfermagem. (2012) 20:583–9. doi: 10.1590/s0104-11692012000300021
35. Organizacion Panamericana de la Salud and Division de Promocion y Proteccion de la Salud (HPP). Encuesta multicentrica salud bienestar y envejecimiento (SABE) en America Latina: informe preliminar. Washington, DC: Organización Panamericana de la Salud (2001).
36. Mota, JF, Rinaldi, AEM, Pereira, AF, Maestá, N, Scarpin, MM, and Burini, RC. Adaptação do índice de alimentação saudável ao guia alimentar da população brasileira. Brazil J Nutr. (2008) 21:545–52. doi: 10.1590/S1415-52732008000500007
37. Johns, MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. (1991) 14:540–5. doi: 10.1093/sleep/14.6.540
38. Raposo, F, Ramos, M, and Cruz, AL. Effects of exercise on knee osteoarthritis: a systematic review. Musculoskeletal Care. (2021) 19:399–435. doi: 10.1002/msc.1538
39. Murphy, SL, Strasburg, DM, Lyden, AK, Smith, DM, Koliba, JF, Dadabhoy, DP, et al. Effects of activity strategy training on pain and physical activity in older adults with knee or hip osteoarthritis: a pilot study. Arthritis Rheum. (2008) 59:1480–7. doi: 10.1002/art.24105
40. Souza, IFDS, Oliveira Neta, RS, Gazzola, JM, and Souza, MC. Elderly with knee osteoarthritis should perform nutritional assessment: integrative literature review. Einstein. (2017) 15:226–32. doi: 10.1590/S1679-45082017RW3834
41. Basem, JI, White, RS, Chen, SA, Mauer, E, Steinkamp, ML, Inturrisi, CE, et al. The effect of obesity on pain severity and pain interference. Pain Manag. (2021) 11:571–81. doi: 10.2217/pmt-2020-0089
42. Ricker, MA, and Haas, WC. Anti-inflammatory diet in clinical practice: a review. Nutr Clin Pract. (2017) 32:318–25. doi: 10.1177/0884533617700353
43. Cooper, I, Brukner, P, Devlin, BL, Reddy, AJ, Fulton, M, Kemp, JL, et al. An anti-inflammatory diet intervention for knee osteoarthritis: a feasibility study. BMC Musculoskelet Disord. (2022) 23:47. doi: 10.1186/s12891-022-05003-7
44. Ministério da Saúde. Guia alimentar para a população brasileira / Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Básica – 2 ed, 1reimpr. Brasília: Ministério da Saúde (2014).
45. Allen, KD, Oddone, EZ, Coffman, CJ, Datta, SK, Juntilla, KA, Lindquist, JH, et al. Telephone-based self-management of osteoarthritis: a randomized trial. Ann Intern Med. (2010) 153:570–9. doi: 10.7326/0003-4819-153-9-201011020-00006
46. Vincent, KR, and Vincent, HK. Concentric and eccentric resistance training comparison on physical function and functional pain outcomes in knee osteoarthritis: a randomized controlled trial. Am J Phys Med Rehabil. (2020) 99:932–40. doi: 10.1097/PHM.0000000000001450
47. Murphy, SL, Janevic, MR, Lee, P, and Williams, DA. Occupational therapist-delivered cognitive-behavioral therapy for knee osteoarthritis: a randomized pilot study. Am J Occup Ther. (2018) 72:7205205040p1–9. doi: 10.5014/ajot.2018.027870
48. Irwin, MR. Sleep and inflammation: partners in sickness and in health. Nat Rev Immunol. (2019) 19:702–15. doi: 10.1038/s41577-019-0190-z
49. Finan, PH, Goodin, BR, and Smith, MT. The association of sleep and pain: an update and a path forward. J Pain. (2013) 14:1539–52. doi: 10.1016/j.jpain.2013.08.007
50. Hinman, RS, Campbell, PK, Lawford, BJ, Briggs, AM, Gale, J, Bills, C, et al. Does telephone-delivered exercise advice and support by physiotherapists improve pain and/or function in people with knee osteoarthritis? Telecare randomised controlled trial. Br J Sports Med. (2020) 54:790–7. doi: 10.1136/bjsports-2019-101183
51. Li, J, Qin, Y, Zhong, Z, Meng, L, Huang, L, and Li, B. Pain experience reduces social avoidance to others in pain: a c-Fos-based functional connectivity network study in mice. Cereb Cortex. (2024) 34:bhae207. doi: 10.1093/cercor/bhae207
52. Borowski, SK, and Rose, AJ. Co-rumination between friends: considering the roles of outcome expectations, relationship provisions, and perceptions of problems. Child Dev. (2024) 95:1063–75. doi: 10.1111/cdev.14054
53. Franqueiro, AR, Yoon, J, Crago, MA, Curiel, M, and Wilson, JM. The interconnection between social support and emotional distress among individuals with chronic pain: a narrative review. Psychol Res Behav Manag. (2023) 16:4389–99. doi: 10.2147/PRBM.S410606
54. Lavender, EC, Anderson, AM, Dusabe-Richards, E, Antcliff, D, Kingsbury, SR, Conaghan, PG, et al. Understanding peer mentorship in supporting self-management of hip and knee osteoarthritis: a qualitative study of mentees’ perspectives. Musculoskeletal Care. (2022) 20:180–91. doi: 10.1002/msc.1580
55. Egerton, T, Lawford, BJ, Campbell, PK, Plinsinga, ML, Spiers, L, Mackenzie, DA, et al. Expert-moderated peer-to-peer online support Group for People with Knee Osteoarthritis: mixed methods randomized controlled pilot and feasibility study. JMIR Form Res. (2022) 6:e32627. doi: 10.2196/32627
56. Nicolson, PJA, Bennell, KL, Dobson, FL, Van Ginckel, A, Holden, MA, and Hinman, RS. Interventions to increase adherence to therapeutic exercise in older adults with low back pain and/or hip/knee osteoarthritis: a systematic review and meta-analysis. Br J Sports Med. (2017) 51:791–9. doi: 10.1136/bjsports-2016-096458
Keywords: knee osteoarthritis, education, rehabilitation, pain, self-management
Citation: Ayres DVM, Uchiyama SST, Prates AO, Lopes RAF, Silva ABS, Tsukimoto DR, Amorim RA, Ribeiro TS, Santos ACA, Sugawara AT, Montagnini M, Battistella LR and Imamura M (2025) The Knee-SCHOOL: a brief patient-centered multidisciplinary educational program for knee osteoarthritis. Front. Med. 11:1497774. doi: 10.3389/fmed.2024.1497774
Edited by:
Kate Thompson, Leeds Beckett University, United KingdomReviewed by:
Lisa H. Antoine, University of Alabama at Birmingham, United StatesDaniela Poenaru, Carol Davila University of Medicine and Pharmacy, Romania
Copyright © 2025 Ayres, Uchiyama, Prates, Lopes, Silva, Tsukimoto, Amorim, Ribeiro, Santos, Sugawara, Montagnini, Battistella and Imamura. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marta Imamura, bWFydGEuaW1hbXVyYUBmbS51c3AuYnI=