Abstract
Background:
Anesthesiology research is growing at a rapid pace. It is essential to understand the scope and trends over time to identify gaps and future areas for growth. Systematic reviews and meta-analyses (SRMA) are summaries of the best available evidence to address a specific research question via a comprehensive literature search, in-depth analyses, and synthesis of results. High-quality SRMA are increasingly used and play an essential role in medical research.
Objective:
We aimed to explore the trends of SRMA in indexed anesthesia journals.
Methods:
SRMA published in indexed anesthesia journals from 2013 to 2023 were retrieved from the Web of Science database. Data were presented via descriptive statistics. We used CiteSpace 6.1.R6 to analyze countries, institutions, journals, authors, and keywords through visual maps to explore the research hotspots and trends. The journal’s Journal Citation Reports partition, impact factor, annual publications, journals H-index, and a number of highly-cited papers were calculated in the WoS database.
Results:
A total of 34 indexed anesthesia journals and 3,004 SRMA were included. The year 2021 was the year with the most SRMA (385/3,004). Out of the 3,004 SRMAs, 36 (0.03%) were highly cited papers, and 22 of the 36 highly cited papers focused on “pain management.” BRITISH JOURNAL OF ANAESTHESIA had the highest 5-year impact factor (9.6) in 2022 Journal Citation Reports, the most significant number of publications (268/3,004), the highest total number of citations (13,173/86,145), and the most significant number of SRMAs cited more than 100 (36/160). ANAESTHESIA achieved the highest impact factor in the 2022 Journal Citation Reports (10.7) and the highest average annual citations (58.82). PAIN had the highest number of highly cited papers (15/36). The United States of America was the most productive country, with 823/3,004 SRMAs. University Toronto had the highest number of publications (245/3,004). The most frequent of keywords was the topic “Pain Management” (1,622/29.1%).
Conclusion:
This present study would be valuable to practitioners, academics, researchers, and students in understanding the dynamics of progress in anesthesiology.
1 Introduction
Anesthesiology research is essential for understanding anesthesia and related fields of medicine (1). The number of articles published by an institution or country in indexed anesthesia journals indicate its contribution to creating new knowledge in anesthesiology (2, 3). However, the results of individual studies are often insufficient to provide confident answers, as their results are not consistently reproducible. A meta-analysis is a statistical method for combining the results of different studies on the same topic, and it may resolve conflicts among studies. A systematic review is a literature review focused on a single question that attempts to identify, evaluate, select, and synthesize all high-quality research evidence related to that question (4). High-quality systematic reviews and meta-analyses (SRMA) are increasingly used and play an essential role in medical research. The quality of meta-analyses published in indexed anesthesia journals was moderate to high, with statistically significant improvements over time (5).
In recent decades, the number of published SRMA has grown exponentially. According to PubMed, 435 SRMA were published in 1995 compared to 20,774 in 2017, representing a growth rate of approximately 4,676% (6). Such growth has increased overlap and redundancy among research topics, with only around 3% of SRMA estimated to be methodologically sound and non-redundant or to provide useful clinical information (7).
Bibliometric analyses offer one approach for identifying critical studies. They are a type of literature analysis comprising a collection of quantitative and statistical tools for evaluating the quality and impact of the literature associated with a certain topic or field (8). There has been an increasing number of bibliometric analyses in anesthesiology in recent years (5, 9, 10). These documents systematically revealed the productivity and collaborations of institutions, journals, and countries, making monitoring the development of a specific field possible. This present study would be valuable to practitioners, academics, researchers, and students in understanding the dynamics of progress in anesthesiology. Thus, we aimed to explore the trends of SRMA in indexed anesthesia journals from 2013 to 2023 according to bibliometric methods.
2 Methods
Journals related to anesthesiology were selected from the ‘anesthesiology’ category in 2022 Journal Citation Reports (JCR) established by the Institute for Scientific Information (ISI): https://jcr.clarivate.com/jcr/browse-journals. A total of 65 journals related to anesthesiology were selected. We included only the journals with an ISSN (print) number in the Science Citation Index Expanded (SCIE) of the WoS Core Collection. As a result, one journal without an ISSN (print) number and 30 non-SCIE journals were excluded from the study. WoS Core Collection (Clarivate Analytics) is a research platform that provides a substantial bibliographic database through the Science Citation Index Expanded (SCIE).
The Web of Science database was searched to retrieve SRMA publications in indexed anesthesia journals between 2013 and 2023. Data were presented via descriptive statistics. We used CiteSpace 6.1.R6 to analyze countries, institutions, journals, authors, and keywords through visual maps to explore the research hotspots and trends. The journal’s JCR partition, impact factor (IF), annual publications, journal H-index, and a number of highly-cited papers were calculated in the WoS database. We used CiteSpace 6.1.R6 to analyze keywords, and the type of each topic was manually coded through two authors.
A computerized literature search was conducted in the WoS database from January 1st, 2013, to December 31st, 2023. The titles of the 34 journals were used to perform searches in WoS, TS = (“meta analyses” OR “meta analyses” OR “systematic review”), language = “English,” type = “article or review,” search strategy in Supplementary 1.
3 Statistical analyses
Data were presented via descriptive statistics.
4 Results
4.1 Journals JCR partition and impact factor
Finally, 34 journals were included in this study, according to the 2022 JCR established by the ISI: Q1 (8;24.00%), Q2 (9;26.00%), Q3 (8;24.00%), Q4 (9;26.00%). The 34 included journals have IF and 5y-IF. The IF of the 34 journals in 2022 ranged from 0.4 to 10.7. Among these were 8 (24.00%) journals with an IF greater than 5. The top 10 journals with the highest IF: ANAESTHESIA: 10.7, BRIT J ANAESTH: 9.8, ANESTHESIOLOGY: 8.8, PAIN: 7.4, J CLIN ANESTH: 6.7, ANESTH. ANALG: 5.9, ANAESTH CRIT CARE PA: 5.5, REGION ANESTH PAIN M: 5.1, BEST PRAC RES-CL ANA: 4.8, CAN J ANEST: 4.2, as listed in Table 1.
Table 1
| No | Journal name | Abbreviation | 2022 impact factor | 5 years impact factor | Journal citation reports partition |
|---|---|---|---|---|---|
| 1 | Anaesthesia | ANAESTHESIA | 10.7 | 8.4 | Q1 |
| 2 | British Journal of Anaesthesia | BRIT J ANAESTH | 9.8 | 9.6 | Q1 |
| 3 | Anesthesiology | ANESTHESIOLOGY | 8.8 | 8.4 | Q1 |
| 4 | Pain | PAIN | 7.4 | 7.7 | Q1 |
| 5 | Journal of Clinical Anesthesia | J CLIN ANESTH | 6.7 | 6.2 | Q1 |
| 6 | Anesthesia and Analgesia | ANESTH ANALG | 5.9 | 5.7 | Q1 |
| 7 | Anaesthesia Critical Care & Pain Medicine | ANAESTH CRIT CARE PA | 5.5 | 4.5 | Q1 |
| 8 | Regional Anesthesia and Pain Medicine | REGION ANESTH PAIN M | 5.1 | 5.7 | Q1 |
| 9 | Best Practice & Research-Clinical Anaesthesiology | BEST PRAC RES-CL ANA | 4.8 | 4.6 | Q2 |
| 10 | Canadian Journal of Anesthesia-Journal Canadien D Anesthesie | CAN J ANESTH | 4.2 | 4.2 | Q2 |
| 11 | Journal of Neurosurgical Anesthesiology | J NEUROSURG ANESTH | 3.7 | 2.9 | Q2 |
| 12 | European Journal of Anaesthesiology | EUR J ANAESTH | 3.6 | 4.4 | Q2 |
| 13 | European Journal of Pain | EUR J PAIN | 3.6 | 3.9 | Q2 |
| 14 | Minerva Anestesiologica | MINERVA ANESTESIOL | 3.2 | 2.9 | Q2 |
| 15 | Pain Medicine | PAIN MED | 3.1 | 3.4 | Q2 |
| 16 | Korean Journal of Anesthesiology | KOREAN J ANESTHESIOL | 2.9 | 4.8 | Q2 |
| 17 | Clinical Journal of Pain | CLIN J PAIN | 2.9 | 3.8 | Q2 |
| 18 | International Journal of Obstetric Anesthesia | INT J OBSTET ANESTH | 2.8 | 2.6 | Q3 |
| 19 | Journal of Anesthesia | J ANESTH | 2.8 | 2.5 | Q3 |
| 20 | Journal of Cardiothoracic and Vascular Anesthesia | J CARDIOTHOR VASC AN | 2.8 | 2.5 | Q3 |
| 21 | Perioperative Medicine | PERIOPER MED-LONDON | 2.6 | 3.2 | Q3 |
| 22 | Pain Practice | PAIN PRACT | 2.6 | 2.9 | Q3 |
| 23 | Current Opinion in Anesthesiology | CURR OPIN ANESTHESIO | 2.5 | 2.9 | Q3 |
| 24 | BMC Anesthesiology | BMC ANESTHESIOL | 2.2 | 2.6 | Q3 |
| 25 | Journal of Clinical Monitoring and Computing | J CLIN MONIT COMPUT | 2.2 | 2.1 | Q3 |
| 26 | Acta Anaesthesiologica Scandinavica | ACTA ANAESTH SCAND | 2.1 | 2.1 | Q4 |
| 27 | Pediatric Anesthesia | PEDIATR ANESTH | 1.7 | 2.3 | Q4 |
| 28 | Anaesthesia and Intensive Care | ANAESTH INTENS CARE | 1.5 | 1.9 | Q4 |
| 29 | Brazilian Journal of Anesthesiology | BRAZ J ANESTHESIOL | 1.3 | 1.3 | Q4 |
| 30 | Anaesthesiologie | ANAESTHESIOLOGIE | 1.1 | 1.1 | Q4 |
| 31 | Schmerz | SCHMERZ | 1 | 0.9 | Q4 |
| 32 | Revista Brasileira De Anestesiologia | REV BRAS ANESTESIOL | 1 | 1.1 | Q4 |
| 33 | Anasthesiologie & Intensivmedizin | ANASTH INTENSIVMED | 0.7 | 0.5 | Q4 |
| 34 | Anasthesiologie Intensivmedizin Notfallmedizin Schmerztherapie | ANASTH INTENSIV NOTF | 0.4 | 0.5 | Q4 |
Anesthesia journals.
The average 5y-IF of the 34 journals in 2022 ranged from 0.5 to 9.6. Among these were 7 (21.00%) journals with 5y-IF greater than 5. The top 10 journals with the highest average 5y-IF: BRIT J ANAESTH: 9.6, ANAESTHESIA: 8.4, ANESTHESIOLOGY: 8.4, PAIN: 7.7, J CLIN ANESTH: 6.2, ANESTH ANALG: 5.7, REGION ANESTH PAIN M: 5.7, KOREAN J ANESTHESIOL: 4.8, BEST PRAC RES-CL ANA: 4.6, ANAESTH CRIT CARE PA: 4.5, as listed in Table 1.
4.2 H-index of journals
The H-index of each journal ranged from 0 to 62. The top 10 journals with H-index SRMAs: BRIT J ANAESTH: 62, PAIN: 62, ANESTH ANALG: 48, ANAESTHESIA: 44, EUR J PAIN: 39, PAIN MED: 36, ANESTHESIOLOGY: 34, ACTA ANAESTH SCAND: 30, J CLIN ANESTH: 30, REGION ANESTH PAIN M: 29, CAN J ANESTH: 29, J CARDIOTHOR VASC AN: 29, as listed in Table 2.
Table 2
| Publications number | Journal citations | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | Journal | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | 2023 | Total | Total citations | Average/year | Citations ≥ 100 | H-index | Highly cited |
| 1 | ANAESTHESIA | 2 | 14 | 11 | 12 | 13 | 17 | 20 | 23 | 17 | 9 | 12 | 150/4.99% | 5,818 | 38.79 | 9 | 44 | 4/11.11% |
| 2 | BRIT J ANAESTH | 21 | 16 | 17 | 17 | 23 | 36 | 19 | 19 | 34 | 41 | 25 | 268/8.92% | 13,173 | 49.15 | 36 | 62 | 9/25.00% |
| 3 | ANESTHESIOLOGY | 9 | 4 | 8 | 8 | 9 | 1 | 4 | 4 | 8 | 4 | 2 | 61/2.03% | 3,588 | 58.82 | 14 | 34 | 1/2.78% |
| 4 | PAIN | 20 | 16 | 17 | 17 | 10 | 16 | 18 | 23 | 26 | 33 | 30 | 226/7.52% | 12,991 | 57.48 | 33 | 62 | 15/41.67% |
| 5 | J CLIN ANESTH | 2 | 3 | 3 | 19 | 21 | 20 | 16 | 28 | 28 | 19 | 15 | 174/5.79% | 3,223 | 18.52 | 1 | 30 | 1/2.78% |
| 6 | ANESTH ANALG | 12 | 13 | 15 | 23 | 31 | 29 | 26 | 18 | 16 | 16 | 20 | 219/7.29% | 8,034 | 36.68 | 15 | 48 | 2/5.56% |
| 7 | ANAESTH CRIT CARE PA | 0 | 0 | 0 | 1 | 2 | 2 | 4 | 6 | 8 | 6 | 7 | 36/1.20% | 439 | 12.19 | 0 | 12 | 0 |
| 8 | REGION ANESTH PAIN M | 2 | 1 | 3 | 9 | 7 | 5 | 8 | 13 | 14 | 11 | 7 | 80/2.66% | 2,305 | 28.81 | 3 | 29 | 0 |
| 9 | BEST PRAC RES-CL ANA | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 2 | 4/0.13% | 54 | 13.5 | 0 | 2 | 0 |
| 10 | CAN J ANESTH | 4 | 10 | 9 | 6 | 5 | 12 | 15 | 15 | 13 | 10 | 19 | 118/3.93% | 2,323 | 19.69 | 2 | 29 | 0 |
| 11 | J NEUROSURG ANESTH | 1 | 1 | 1 | 2 | 2 | 2 | 2 | 1 | 5 | 6 | 7 | 30/1.00% | 514 | 17.13 | 0 | 13 | 0 |
| 12 | EUR J ANAESTH | 2 | 3 | 5 | 9 | 5 | 9 | 4 | 13 | 15 | 13 | 8 | 86/2.86% | 2,302 | 26.77 | 3 | 24 | 2/5.56% |
| 13 | EUR J PAIN | 8 | 8 | 6 | 13 | 11 | 10 | 15 | 28 | 21 | 21 | 11 | 152/5.06% | 5,532 | 36.39 | 16 | 39 | 0 |
| 14 | MINERVA ANESTESIOL | 8 | 10 | 11 | 12 | 14 | 11 | 12 | 12 | 12 | 13 | 16 | 131/4.36% | 2,182 | 16.66 | 2 | 27 | 0 |
| 15 | PAIN MED | 10 | 19 | 7 | 10 | 10 | 10 | 21 | 49 | 50 | 32 | 9 | 227/7.56% | 4,464 | 19.67 | 6 | 36 | 0 |
| 16 | KOREAN J ANESTHESIOL | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 8 | 7 | 3 | 19/0.63% | 183 | 9.63 | 1 | 6 | 0 |
| 17 | CLIN J PAIN | 11 | 8 | 8 | 14 | 15 | 22 | 18 | 15 | 18 | 14 | 17 | 160/5.33% | 4,575 | 28.59 | 8 | 37 | 1/2.78% |
| 18 | INT J OBSTET ANESTH | 3 | 0 | 3 | 2 | 2 | 2 | 7 | 6 | 2 | 3 | 3 | 33/1.10% | 551 | 16.7 | 0 | 16 | 0 |
| 19 | J ANESTH | 2 | 7 | 4 | 4 | 6 | 2 | 3 | 6 | 11 | 8 | 10 | 63/2.10% | 834 | 13.24 | 0 | 16 | 0 |
| 20 | J CARDIOTHOR VASC AN | 8 | 11 | 8 | 11 | 13 | 15 | 9 | 12 | 14 | 16 | 18 | 135/4.49% | 2,734 | 20.25 | 2 | 29 | 0 |
| 21 | PERIOPER MED-LONDON | 0 | 0 | 0 | 0 | 2 | 5 | 2 | 6 | 9 | 2 | 7 | 33/1.10% | 336 | 10.18 | 0 | 10 | 0 |
| 22 | PAIN PRACT | 4 | 11 | 5 | 10 | 10 | 12 | 9 | 14 | 11 | 10 | 18 | 114/3.79% | 2,405 | 21.1 | 3 | 27 | 0 |
| 23 | CURR OPIN ANESTHESIO | 3 | 1 | 1 | 3 | 8 | 2 | 8 | 2 | 2 | 6 | 8 | 44/1.46% | 478 | 10.86 | 0 | 12 | 0 |
| 24 | BMC ANESTHESIOL | 1 | 5 | 8 | 6 | 7 | 12 | 14 | 26 | 13 | 10 | 29 | 131/4.36% | 1,794 | 13.69 | 0 | 23 | 0 |
| 25 | J CLIN MONIT COMPUT | 0 | 0 | 0 | 3 | 5 | 1 | 0 | 5 | 2 | 4 | 6 | 26/0.87% | 430 | 16.54 | 0 | 11 | 0 |
| 26 | ACTA ANAESTH SCAND | 6 | 12 | 11 | 9 | 7 | 14 | 27 | 17 | 18 | 18 | 25 | 164/5.46% | 2,820 | 17.2 | 4 | 30 | 1/2.78% |
| 27 | PEDIATR ANESTH | 3 | 9 | 8 | 7 | 4 | 4 | 4 | 8 | 7 | 6 | 8 | 68/2.26% | 1,374 | 20.21 | 2 | 23 | 0 |
| 28 | ANAESTH INTENS CARE | 1 | 0 | 3 | 3 | 3 | 2 | 0 | 2 | 1 | 0 | 0 | 15/0.50% | 265 | 17.67 | 0 | 7 | 0 |
| 29 | BRAZ J ANESTHESIOL | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 6 | 13 | 20/0.67% | 69 | 3.45 | 0 | 4 | 0 |
| 30 | ANAESTHESIOLOGIE | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1/0.03% | 1 | 1 | 0 | 1 | 0 |
| 31 | SCHMERZ | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 3/0.10% | 130 | 43.33 | 0 | 2 | 0 |
| 32 | REV BRAS ANESTESIOL | 2 | 0 | 3 | 3 | 4 | 0 | 0 | 0 | 0 | 0 | 0 | 12/0.40% | 224 | 18.67 | 0 | 10 | 0 |
| 33 | ANASTH INTENSIVMED | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1/0.03% | 0 | 0 | 0 | 0 | 0 |
| 34 | ANASTH INTENSIV NOTF | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Total | 145 | 182 | 175 | 235 | 249 | 273 | 286 | 372 | 385 | 347 | 355 | 3,004 | 86,145 | 732.56 | 160 | 755 | 36 | |
Publications number, journal citations and H-index, and highly cited papers.
4.3 Country
The 3,004 SRMAs were published across 89 different countries, and the total number of SRMAs published by each country ranged from 1 to 823. The top 10 countries with the highest number of SRMAs: the United States (USA) (823/3, 004; 27.40%), Canada (513/3, 004; 15.35%), United Kingdom (461/3, 004; 15.35%), China (445/3, 004; 15.15%), Australia (310/3, 004; 10.32%), Denmark (247/3, 004; 8.22%), Germany (214/3, 004; 7.12%), Italy (210/3, 004; 6.99%), Netherlands (204/3, 004; 6.79%), Switzerland (141/3, 004; 4.69%), as listed in Supplementary 2.
4.4 Institutions
The 3,004 SRMAs were published across 465 different institutions, and the total number of SRMAs published by each institution ranged from 2 to 245. The top 10 institutions with the highest number of SRMAs: University (Univ) Toronto (Canada, 245), Univ Copenhagen (Denmark, 92), McMaster Univ (Canada, 87), Univ Ottawa (Canada, 85), Copenhagen Univ Hosp (Denmark, 68), Stanford Univ (USA, 68), Univ Sydney (Australia, 68), Monash Univ (Australia, 65), Univ Washington (USA, 59), Kings Coll London (United Kingdom, 57). The 10 institutions were from 5 different countries: Canada (3, 30%), Denmark (2, 20%), USA (2, 20%), Australia (2, 20%), United Kingdom (1, 10%), as listed in Supplementary 3.
4.5 Total number of publications
A total of 3,004 SRMAs were published in 34 selected journals from 2013 to 2023 worldwide. Of these, 2,398 were “Review SRMAs” and 606 were “SRMAs,” with an annual range from 145 to 385. 2013: 145/4.83%, 2014: 182/6.06%, 2015: 175/5.83%, 2016: 235/7.82%, 2017: 249/8.29%, 2018: 273/9.09%, 2019: 286/9.52%, 2020: 272/12.38%, 2021: 385/12.82%, 2022: 347/11.55%, 2023: 355/11.82%, as listed in Table 2 and show in Figure 1.
Figure 1

The annual number of systematic reviews and meta-analyses articles in indexed anesthesia journals.
4.6 Total number of publications per journal
The total number of SRMAs published by each journal from 2013 to 2023 ranges from 0 to 268. The top 10 journals with the highest number of publications: BRIT J ANAESTH: 268/8.92%, PAIN MED: 227/7.56%, PAIN: 226/7.52%, ANESTH ANALG: 219/7.29%, J CLIN ANESTH: 174/5.79%, ACTA ANAESTH SCAND:164/5.46%, CLIN J PAIN: 160/5.33%, EUR J PAIN:152/5.06%, ANAESTHESIA: 150/4.99%, J CARDIOTHOR VASC AN: 135/4.49%, as listed in Table 2 and Figure 2.
Figure 2
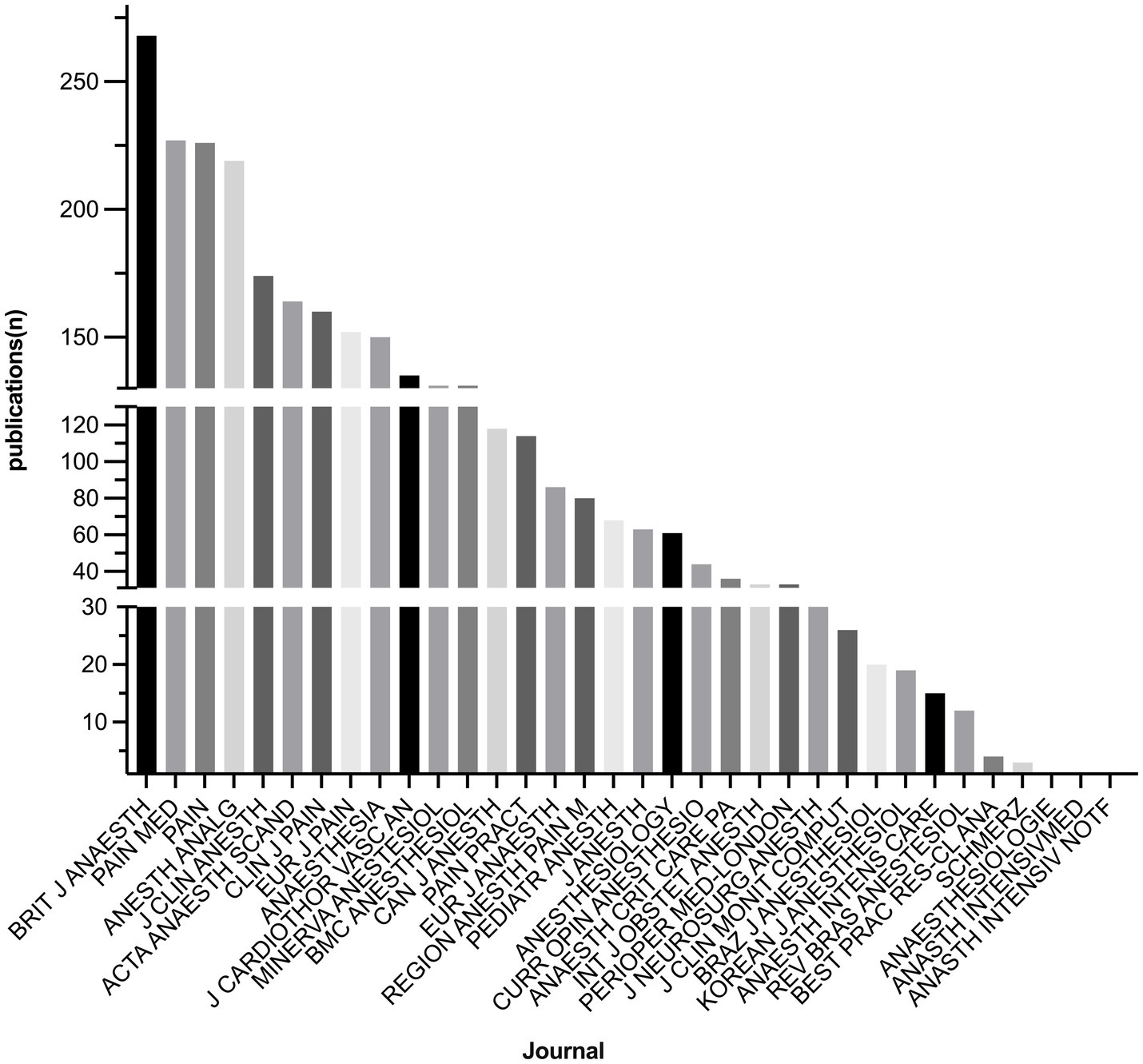
Publications of SRMAs per journal.
4.7 Citations
4.7.1 Total citations
The total citations of the 3,004 SRMA from 2013 to 2023 were 86,145. The range of total citations for each journal was from 0 to 13,713. The top 10 journals with the highest number of total citations: BRIT J ANAESTH: 13,173/15.29%, PAIN: 12,991/15.08%, ANESTH ANALG: 8,034/9.33%, ANAESTHESIA: 5,818/6.75%, EUR J PAIN: 5,532/6.42%, CLIN J PAIN: 4,575/5.31%, PAIN MED: 4,464/5.18%, ANESTHESIOLOGY: 3,588/4.17%, J CLIN ANESTH: 3,223/3.74%, ACTA ANAESTH SCAND: 2,820/3.27%, as listed in Table 2.
4.7.2 Average citations per year
Each journal’s average citations per year was from 0 to 58.82. The top 10 journals with the highest number of average citations per year: ANESTHESIOLOGY: 58.82, PAIN: 57.48, BRIT J ANAESTH: 49.15, SCHMERZ: 43.33, ANAESTHESIA: 38.79, ANESTH ANALG: 36.68, EUR J PAIN: 36.39, REGION ANESTH PAIN M: 28.81, CLIN J PAIN: 28.59, EUR J ANAESTH: 26.77, as listed in Table 2.
4.7.3 Citations of more than 100 SRMAs
Out of the 34 journals, 18 of them contained a total of 160 SRMAs that received more than 100 citations each. The top 10 journals with SRMAs with more than 100 citations: BRIT J ANAESTH: 36/22.50%, PAIN: 33/20.63%, EUR J PAIN: 16/10.00%, ANESTH ANALG: 15/9.38%, ANESTHESIOLOGY: 14/8.75%, ANAESTHESIA: 9/5.63%, CLIN J PAIN: 8/5.00%, PAIN MED: 6/3.75%, ACTA ANAESTH SCAND: 4/2.50%, REGION ANESTH PAIN M: 3/1.88%, EUR J ANAESTH: 3/1.88%, PAIN PRACT: 3/1.88%, as listed in Table 2.
4.8 Highly cited papers
Among the 3,004 SRMAs, 36 (0.03%) of them were highly cited papers: PAIN: 15/41.67%, BRIT J ANAESTH: 9/25.00%, ANAESTHESIA 4/11.11%, ANESTH ANALG: 2/5.56%, EUR J ANAESTH: 2/5.56%, ANESTHESIOLOGY: 1/2.78%, J CLIN ANESTH: 1/2.78%, CLIN J PAIN: 1/2.78%, ACTA ANAESTH SCAND: 1/2.78%, as listed in Supplementary 4.
Out of the 36 highly cited papers, 22 focused on “pain management.” Out of the 22 papers focused on “pain management,” 5 were focused on chronic pain, 8 were focused on perioperative pain, one of which was specifically about perioperative pain in children. Additionally, 2 papers focused on neuropathic pain, 2 focused on conditioned pain, and 2 focused on physical, psychological, and self-management interventions for pain. There was a paper on instruments used for measuring non-specific low back pain, a study that examined the reliability of divergent published trial data in spinal pain, and another paper that looked into the prevalence of pain symptoms of musculoskeletal origin following coronavirus (COVID) infection, as listed in Supplementary 4.
4.9 Keywords
The 5,581 keywords were categorized into 6 topics, and each topic’s keyword frequency and percentage were: Pain Management (1,622/29.1%), Surgical Procedures (970/17.4%), Anesthesia Techniques (902/16.2%), Perioperative Management (889/15.9%), Anesthetic Agents (626/11.2%), Anesthesia Complications (572/10.2%), as shown in Figure 3A and listed in Table 3.
Figure 3

(A) Each topic’s keyword frequency and percentage. (B) Number of SRMAs per topic.
Table 3
| Topic | Frequency/percentage |
|---|---|
| Anesthesia Techniques | 902/16.2% |
| regional anesthesia | 199 |
| general anesthesia | 175 |
| nerve block | 105 |
| neuraxial anesthesia | 81 |
| lumboabdominal nerve block | 67 |
| upper limbs block | 42 |
| lower limbs block | 39 |
| thoracic nerve block | 29 |
| Anesthesia Management | 889/15.9% |
| airway management and mechanical ventilation | 278 |
| patient safety | 237 |
| organ perfusion | 175 |
| fluid therapy | 82 |
| recovery | 81 |
| patient blood management | 36 |
| Anesthesia Complications | 572/10.2% |
| complication | 249 |
| postoperative cognitive dysfunction | 168 |
| acute kidney injury | 66 |
| postoperative nausea and vomiting | 47 |
| acute lung injury | 27 |
| hoarseness | 8 |
| cerebrospinal injury | 7 |
| Surgical Procedures | 970/17.4% |
| surgery | 352 |
| cardiac surgery | 263 |
| abdominal surgery | 98 |
| orthopedic surgery | 97 |
| obstetric operation (cesarean section) | 85 |
| breast surgery | 42 |
| thoracic surgery | 20 |
| urologic surgery (prostatectomy) | 8 |
| thrombectomy | 3 |
| gynecological surgery (hysterectomy) | 2 |
| Anesthetics | 626/11.2% |
| opioids | 169 |
| local anesthetics | 97 |
| propofol | 86 |
| volatile anesthetics | 84 |
| corticosteroid | 62 |
| midazolam | 28 |
| nonsteroidal anti-inflammatory drugs | 23 |
| clonidine | 20 |
| nitrous oxide | 17 |
| ketamine | 11 |
| pregabalin | 9 |
| ondansetron | 5 |
| tramadol | 4 |
| magnesium sulfate | 3 |
| gabapentin | 3 |
| epsilon aminocaproic acid | 3 |
| amitriptyline | 2 |
| Pain or Pain Management | 1622/29.1% |
| pain management | 423 |
| chronic pain | 303 |
| postoperative pain | 229 |
| low back pain | 196 |
| acute pain | 179 |
| neuropathic pain | 104 |
| musculoskeletal pain | 40 |
| knee osteoarthritis | 35 |
| back pain | 30 |
| osteoarthritis | 21 |
| neck pain | 15 |
| cancer pain | 11 |
| headache | 9 |
| rheumatoid arthritis | 9 |
| shoulder pain | 7 |
| phantom limb pain | 3 |
| hyperalgesia | 3 |
Keywords classification.
Number of SRMAs per topic was as follows: “Pain Management” had 1,143 SRMAs, “Surgical Procedures” had 931 SRMAs, “Anesthetic Agents” had 823 SRMAs, “Anesthesia Techniques” had 707 SRMAs, “Perioperative Management” had 595 SRMAs, “Anesthesia Complications” had 853 SRMAs, as shown in Figure 3B.
5 Discussion
The present study comprehensively analyzed SRMA in indexed anesthesia journals from 2013 to 2023, including their JCR partition, IF, H-index, total/annual number of publications, citations, institutions, and countries that published the most literature. Furthermore, they helped researchers or clinicians to master the research trends precisely and quickly, thereby aiding in conducting further studies.
The BRIT J ANAESTH had the highest 5-year impact factor (9.6), the greatest number of publications (268/3,004), the highest total number of citations (13,173/86,145), and the greatest number of SRMAs cited more than 100 (36/160). The ANAESTHESIA achieved the highest IF in the 2022 JCR (IF 10.7) and the highest average yearly citations (58.82). The PAIN had the highest number of highly cited papers (15/36). The United States was the most productive country, with 823/3,004 SRMAs. The University of Toronto (Canada) had the highest number of publications (245/3,004).
This study includes publications only in English since it is the international language of science (11). ISI and WoS databases mainly include English journals, which makes it difficult for journals in other languages to attain high impact (12). Dogan and Karaca reviewed anesthesia-related publications that were indexed in the WOS between 2009 and 2018; the USA produced more than one-fourth (28.9%) of the literature, with 89.7% of the documents published in English (13).
According to the 2022 JCR, 34 anesthesia journals were included in our study, while only 18 anesthesia journals were listed in the 2007 JCR (2). The number of anesthesia-related journals has nearly doubled in the past 15 years. The IF of the 18 journals ranged from 0.28 to 4.6 in the 2007 JCR, with none having an IF greater than 5. However, the average 5y-IF of the 34 anesthesia journals in 2022 JCR ranged from 0.5 to 9.6. Among these were 7 (21.00%) journals with an IF greater than 5.
The IF is a metric that calculates the average number of citations received by SRMAs published in a journal. If the IF of a journal is 5, it means that, on average, each SRMA published in the journal receives five citations within the first 2 years. In 2008, the Thomson Institute for Scientific Information introduced the 5y-IF, besides the conventional 2-year IF (2y-IF). The 5y-IF might provide a more accurate representation of a journal’s quality over the last 10 years. The IF was created to evaluate a journal’s quality, not individual SRMAs’ quality (14). However, authors and readers should be aware of several caveats (9, 15, 16): IF is an average, a few highly cited SRMAs can easily skew it. IF is calculated over a two-year window and does not consider later spikes in citations to an SRMA. Several communities benefit from reading SRMAs even if they do not write or cite them. A journal with a low IF may still contain valuable content that impacts readers. IF varies depending on the type of SRMA. Review SRMAs are often cited more frequently, resulting in journals that publish them having higher IF. The IF only considers citations from a limited number of indexed journals and does not consider citations from non-indexed journals.
The citations to an article are highly related to the quality of the article and the novelty of the findings. Importantly, citation counts are influenced by various factors (17). Some factors like structured abstracts (18) and study design (19) may reflect the reporting quality and strength of evidence. On the other hand, visibility and accessibility may be affected by factors such as open access (20) and title length (21). The relationship between citation counts and quality must be considered carefully due to citation bias, the preferential to cite statistically significant results that may inflate efficacy expectations (22). Certain studies may be cited more often if published in high-reputation journals despite similar quality to those in lesser-known journals. As this was a bibliometric study, we did not review the quality and reporting of meta-analyses, and these considerations have been addressed elsewhere (23). It is important to note that citation counts can be useful in measuring the level of interest in anesthesia-related research within the research community. However, it is essential to understand that these metrics may not accurately reflect the clinical effectiveness of these modalities or the practicality of implementing new guidelines in clinical practice.
In the present study, the annual number of SRMA increased from 2013 to 2021. The minimum number of SRMAs recorded was 145 in 2013, with a peak of 385 in 2021. The number of articles published in a particular medical field measures its productivity (24). Publications share knowledge and new findings and increase an author’s recognition within the medical community. It may enable more accessible access to research funding for future studies (25). The number of original articles published by a country or institution indicates their contribution to creating new knowledge in anesthesia. The strength of this metric lies in its intrinsic validity, as opposed to surrogates such as the number of academic staff and independent grant funding, which can be affected by factors such as cost-effectiveness (2, 26). Studies found that high-income countries, particularly the USA, produced most global anesthesia publications analyzed in highly cited journals (2, 27). From 2000 to 2009, middle-income countries, particularly Turkey, China, and India, published more articles than a decade earlier (9, 14). A decline in the original research published by the USA (28), the United Kingdom (26), and Canada (4) in anesthesia journals was observed between 1997 and 2008.
Anesthesia is a broad topic, and many anesthesia-related articles have been published in non-anesthesiology field journals (9, 28). Various reasons explain the significant decline in surgical research in high-income countries. One of the reasons is the increased pressure to generate funds through clinical practice. Additionally, there are increasingly stringent institutional review board requirements, making obtaining informed consent and eligibility for research difficult. Another reason is the lack of governmental and private funding (4, 28). The shortage of anesthesiologists worldwide has also impacted research activities. The demands of clinical duties have reduced the time available for research activities (4, 28). According to a survey conducted by the Society of Academic Anesthesiology Chairs/Association of Anesthesiology Program Directors in August 2000, 91.5% of academic departments required additional anesthesiologists, while 66.5% of necessary departments additional coverage by certified registered nurse anesthetists. Academic positions in anesthesiology have remained unfilled, and those practicing at academic centers are forced to spend more time performing clinical duties. Consequently, they have less time to devote to teaching and research activities (4, 28).
In the present study, Canadian institutions accounted for 30% of the top 10 institutions with the highest number of articles, with the University of Toronto having the highest number of publications, listed in Supplementary 3. Our results are consistent with the research of Tsui et al.; from 2000 to 2004, the University of Toronto had the highest number of publications (4). Total Canadian anesthesia publications remained constant from 2000 to 2004. The number of randomized controlled trials (RCTs) conducted seems to be decreasing, whereas the number of case reports and reviews published has remained constant over the past 5 years. The University of Toronto had the highest number of publications in this five-year time frame. These universities conducted primarily RCTs, whereas smaller Canadian universities mainly published case reports, reviews, and cohort studies (4). The University of Toronto has the largest Canadian anesthesia residency program in the number of teaching staff, hospital facilities, and patient volume. Such resources offer an unequaled opportunity for University of Toronto anesthesia residents and staff to provide a supportive environment for learning and inquiry in all aspects of anesthesia. The University of Toronto is the leader of Canadian anesthesia departments in terms of research productivity (4).
Previous reports confirm a decline in anesthesia publications, particularly original articles and RCTs from high-income countries (4, 26, 28). In the present study, from 2013 to 2023, high-income countries, particularly the USA, produced the most significant number of SRMA in indexed anesthesia journals. The USA had the highest number of SRMA (823/3,004; 27.40%), followed by Canada (513/3,004; 15.35%), and United Kingdom (461/3,004; 15.35%) 461, as listed in Supplementary 2.
RCTs are the most reliable study design to answer a specific clinical question, making them a cornerstone of evidence-based medicine. Performing RCTs with a large sample size is a challenge for researchers in reaching reliable statistical outcomes (29). Systematic reviews and meta-analyses allow combining data from individual RCTs to reach more robust and reliable conclusions regarding a clinical question. SRMA is a statistical method that provides objective and quantitative estimates on a specific topic. Understanding how to conduct a meta-analysis is useful for clinicians in making clinical decisions (30). Furthermore, compared to RCTs, meta-analyses do not require additional funding, ethics committee approval, qualifications, consent signing, or sample collection/testing. The results of meta-analyses can serve as academic achievements for authors, aiding in the advancement of their careers, obtaining financial support to conduct RCTS, and saving resources (manpower and money).
In the present study, keywords related to anesthetic agents were mainly traditional anesthetics, such as opioids, local anesthetics, propofol, and volatile anesthetics. Some newer anesthetics, such as ciprofol correlated SRMA, did not appear in the 34 indexed anesthesia journals between 2013 and 2023, while ciprofol (31, 32) correlated meta-analyses appeared in indexed anesthesia journals in 2024. In the topic of surgical procedures, there were almost no operations related to large arteries, such as the aorta, pulmonary artery, or vena cava surgery.
Among the 3,004 SRMAs, 36 (0.03%) SRMAs were highly cited papers; out of the 36 highly cited papers, 22 focused on “pain management.” Opioids are administered peri-operatively for postoperative analgesia and intra-operatively to control sympathetic responses to surgical stimuli, frequently as a surrogate for presumed pain (33). As there is strong evidence that opioid-inclusive anesthesia does not reduce postoperative pain but is associated with more postoperative nausea and vomiting when compared with opioid-free anesthesia, it suggested that anesthetists should reconsider their intra-operative opioid choices on a case-by-case basis (33).
It remains unclear whether the risks of opioid use outweigh the potential benefits in the long-term management of chronic pain (34–36). Concerns about inappropriate opioid use have grown as the incidence and prevalence of long-term opioid prescribing for chronic pain have increased. Chronic pain patients prescribed opioids is a vexing problem that is compounded by complex clinical presentations that often include mental health and persistent pain problems (34, 36).
Neuropathic pain is widely recognized as one of the most difficult pain syndromes to manage, and outcomes often are unsatisfactory (37, 38). This is partly because the contribution of neuropathy to pain presenting in primary care may be unrecognized (39), and there is evidence of suboptimal drug use in the treatment of neuropathic pain (40). Epidemiological research in this area can be problematic, and the reasons for this are multifactorial: the lack of agreed, valid case definitions that truly reflect the condition under consideration and that are feasible to apply in population-based studies; heterogeneous studies of variable quality, using different means of case ascertainment; and inclusion or exclusion of cases in which pain is not a primary presenting complaint (39).
In this study, multiple factors are related to the research results. The selection criteria for journals impact the scope and nature of the research data. We selected journals from the “Anesthesiology” category in the 2022 JCR and further screened for those with an ISSN (print) number and included them in the Science Citation Index Expanded (SCIE) of the WoS Core Collection. This ensured the standardization of the data source, but it may have excluded some valuable journals that were not included. The data retrieval was sourced from the Web of Science database, which may have missed relevant literature in other important databases. Moreover, the search keyword “anesthesia” was limited to standard American English vocabulary, potentially overlooking related studies using different expressions. At the same time, the citation situation of the literature is affected by various factors, such as article structure, research design, open-access status, and title length. These factors were not deeply explored in this study but can influence the influence of journals and articles measured by citation counts, thus affecting the research results.
The findings of this study can provide valuable insights for anesthesiology practitioners and clinicians. By leveraging the journal indicators from this study, they can strategically select high-impact journals for publication, enhancing their academic influence. Additionally, the high-frequency keywords and highly cited paper topics identified in this research can serve as a guide for future studies, helping researchers to stay at the forefront of academic trends. This study offers a comprehensive overview of the current status and hotspots in anesthesiology research and can help students make topic selection and literature review more targeted and efficient. Moreover, recognizing the limitations of this study can foster critical thinking, which is essential for conducting independent research in the future.
As the finding of the current study, the high-cited papers on pain management can directly benefit patient care. For instance, studies on different types of pain like chronic pain, peri-operative pain, and neuropathic pain offer evidence-based strategies for pain assessment and treatment. The research on using virtual reality to reduce pain and anxiety in pediatric patients during medical procedures can be directly applied in pediatric care settings. By implementing these findings, healthcare providers can improve the quality of pain management for patients, enhancing their overall experience and recovery. The study’s findings on anesthetic agents can inform clinical anesthesiologists. Although most of the research is currently on traditional anesthetics, with the emergence of new agents, the research direction may change. Clinicians can stay updated on these trends to make more informed decisions about anesthetic choices.
6 Limitations
Although the selected journals belong to the JCR anesthesiology category, some cover disciplines beyond anesthesiology and perioperative medicine. On the other hand, some general medicine journals may also publish a few SRMAs related to anesthesiology research. However, it is worth noting that many journals in the field of anesthesiology solely focus on pain research, which can result in a distorted assessment of the anesthesia literature. Despite this, the 34 journals included in these analyses are the indexed international journals dedicated to anesthesiology research. The study only analyzes the WoS database, which could exclude important SRMAs not indexed by WoS. However, WoS claims to provide quality literature. Another limitation was the keyword ‘Anesthesia’ which was used in the search query and was restricted to standard American (US English) vocabulary. Authors who primarily produce reviews and meta-analyses may not be equally prolific in conducting other types of studies, such as RCTs. The impact of self-citations—both by authors and journals—should be considered when evaluating the IF. A series of reviews authored by the same individual, particularly an opinion leader in a specific research area, could skew the results of a purely descriptive statistical analysis. During the analysis process, the keyword classification and topic coding were manually completed by two authors, which may introduce certain subjectivity.
7 Conclusion
The current study demonstrated that PAIN had the highest number of highly-cited papers. The United States was the most productive country. University of Toronto had the highest number of publications. The most frequent of keywords was the topic “Pain Management.” This present study would be valuable to practitioners, academics, researchers, and students in understanding the dynamics of progress in anesthesiology.
Statements
Author contributions
Z-yZ: Data curation, Methodology, Software, Writing – original draft. X-jH: Data curation, Methodology, Writing – original draft. J-rS: Methodology, Writing – original draft. Y-tY: Methodology, Data curation, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by Talent Cultivation Program of Fuwai Yunnan Hospital, Chinese Academy of Medical Sciences. (No. 2024RCT-QN003), the Yunnan Provincial Clinical Medicine Research Special Program (No. 202405AJ310003), and the Technology Research and Device Development Project for Innovative Diagnosis and Treatment of Structural Heart Disease in the Southwest Plateau Region (No. 202302AA310045).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1523630/full#supplementary-material
SUPPLEMENTARY 1Search strategy of the Web of Science.
SUPPLEMENTARY 2The top 10 countries with the highest number of publications.
SUPPLEMENTARY 3The top 10 institutions with the highest number of publications.
SUPPLEMENTARY 4Highly cited papers.
References
1.
Nishino T . Research in anesthesia and the future of our specialty. J Anesth. (2002) 16:185–6. doi: 10.1007/s005400200021
2.
Bould MD Boet S Riem N Kasanda C Sossou A Bruppacher HR . National representation in the anaesthesia literature: a bibliometric analysis of highly cited anaesthesia journals. Anaesthesia. (2010) 65:799–804. doi: 10.1111/j.1365-2044.2010.06424.x
3.
Lee YH . An overview of meta-analysis for clinicians. Korean J Intern Med. (2018) 33:277–83. doi: 10.3904/kjim.2016.195
4.
Tsui BC Li LX Ma V Wagner AM Finucane BT . Declining randomized clinical trials from Canadian anesthesia departments?Can J Anaesth. (2006) 53:226–35. doi: 10.1007/bf03022207
5.
Hall AM Lee S Zurakowski D . Quality assessment of Meta-analyses published in leading anesthesiology journals from 2005 to 2014. Anesth Analg. (2017) 124:2063–7. doi: 10.1213/ane.0000000000002074
6.
Niforatos JD Weaver M Johansen ME . Assessment of publication trends of systematic reviews and randomized clinical trials, 1995 to 2017. JAMA Intern Med. (2019) 179:1593–4. doi: 10.1001/jamainternmed.2019.3013
7.
Siontis KC Ioannidis JPA . Replication, duplication, and waste in a quarter million systematic reviews and Meta-analyses. Circ Cardiovasc Qual Outcomes. (2018) 11:e005212. doi: 10.1161/circoutcomes.118.005212
8.
Choudhri AF Siddiqui A Khan NR Cohen HL . Understanding bibliometric parameters and analysis. Radiographics. (2015) 35:736–46. doi: 10.1148/rg.2015140036
9.
Li Z Qiu LX Wu FX Yang LQ Sun YM Yu WF . Scientific publications in anesthesiology journals from East Asia: a 10-year survey of the literature. J Anesth. (2011) 25:257–62. doi: 10.1007/s00540-010-1073-4
10.
Swaminathan M Phillips-Bute BG Grichnik KP . A bibliometric analysis of global clinical research by anesthesia departments. Anesth Analg. (2007) 105:1741–6. doi: 10.1213/01.ane.0000286149.57763.e7
11.
Maher J . English as an international language of medicine. Med Educ. (1987) 21:283–4. doi: 10.1111/j.1365-2923.1987.tb00363.x
12.
van Leeuwen TN Moed HF Tijssen RJW Visser MS van Raan AFJ . Language biases in the coverage of the science citation index and its consequences for international comparisons of national research performance. Scientometrics. (2001) 51:335–46. doi: 10.1023/a:1010549719484
13.
Doğan G Karaca O . A bibliometric analysis of the field of anesthesia during 2009-2018. Braz J Anesthesiol. (2020) 70:140–52. doi: 10.1016/j.bjan.2020.02.003
14.
Li Z Shi J Liao Z Wu FX Yang LQ Yu WF . Scientific publications in anesthesiology journals from mainland China, Taiwan, and Hong Kong: a 10-year survey of the literature. Anesth Analg. (2010) 110:918–21. doi: 10.1213/ANE.0b013e3181c793ee
15.
Yaxley KL To MS . The 100 top-cited meta-analyses of diagnostic accuracy in radiology journals: a bibliometric analysis. Insights Imaging. (2020) 11:123. doi: 10.1186/s13244-020-00936-w
16.
Smart P . Is the impact factor the only game in town?Ann R Coll Surg Engl. (2015) 97:405–8. doi: 10.1308/rcsann.2015.0028
17.
McHugh UM Yentis SM . An analysis of citations of publications in anaesthesia journals. Anaesthesia. (2020) 75:648–53. doi: 10.1111/anae.14933
18.
Lokker C McKibbon KA McKinlay RJ Wilczynski NL Haynes RB . Prediction of citation counts for clinical articles at two years using data available within three weeks of publication: retrospective cohort study. BMJ. (2008) 336:655–7. doi: 10.1136/bmj.39482.526713.BE
19.
Patsopoulos NA Analatos AA Ioannidis JP . Relative citation impact of various study designs in the health sciences. JAMA. (2005) 293:2362–6. doi: 10.1001/jama.293.19.2362
20.
Davis PM Lewenstein BV Simon DH Booth JG Connolly MJ . Open access publishing, article downloads, and citations: randomised controlled trial. BMJ. (2008) 337:a568. doi: 10.1136/bmj.a568
21.
Letchford A Moat HS Preis T . The advantage of short paper titles. R Soc Open Sci. (2015) 2:150266. doi: 10.1098/rsos.150266
22.
Jannot AS Agoritsas T Gayet-Ageron A Perneger TV . Citation bias favoring statistically significant studies was present in medical research. J Clin Epidemiol. (2013) 66:296–301. doi: 10.1016/j.jclinepi.2012.09.015
23.
Fleuren LM Klausch TLT Zwager CL Schoonmade LJ Guo T Roggeveen LF et al . Machine learning for the prediction of sepsis: a systematic review and meta-analysis of diagnostic test accuracy. Intensive Care Med. (2020) 46:383–400. doi: 10.1007/s00134-019-05872-y
24.
Stossel TP Stossel SC . Declining American representation in leading clinical-research journals. N Engl J Med. (1990) 322:739–42. doi: 10.1056/nejm199003153221106
25.
Kumararatne M . A piece of my mind. Why publish?JAMA. (1997) 277:957. doi: 10.1001/jama.277.12.957
26.
Feneck RO Natarajan N Sebastian R Naughton C . Decline in research publications from the United Kingdom in anaesthesia journals from 1997 to 2006. Anaesthesia. (2008) 63:270–5. doi: 10.1111/j.1365-2044.2008.05475.x
27.
Figueredo E Sánchez Perales G Muñoz Blanco F . International publishing in anaesthesia - how do different countries contribute?Acta Anaesthesiol Scand. (2003) 47:378–82. doi: 10.1034/j.1399-6576.2003.00105.x
28.
Szokol JW Murphy GS Avram MJ Nitsun M Wynnychenko TM Vender JS . Declining proportion of publications by American authors in major anesthesiology journals. Anesth Analg. (2003) 96:513–7. doi: 10.1097/00000539-200302000-00039
29.
Alkhutari AS Al-Moraissi EA Galvão EL Christidis N Falci SGM . Top 100 cited systematic reviews and meta-analyses in the major journals of oral and maxillofacial surgery: a bibliometric analysis. Oral Maxillofac Surg. (2022) 26:343–56. doi: 10.1007/s10006-021-00981-9
30.
Murad MH Montori VM Ioannidis JP Jaeschke R Devereaux PJ Prasad K et al . How to read a systematic review and meta-analysis and apply the results to patient care: users' guides to the medical literature. JAMA. (2014) 312:171–9. doi: 10.1001/jama.2014.5559
31.
Akhtar SMM Fareed A Ali M Khan MS Ali A Mumtaz M et al . Efficacy and safety of Ciprofol compared with Propofol during general anesthesia induction: a systematic review and meta-analysis of randomized controlled trials (RCT). J Clin Anesth. (2024) 94:111425. doi: 10.1016/j.jclinane.2024.111425
32.
Ainiwaer D Jiang W . Efficacy and safety of ciprofol versus propofol for anesthesia induction in adult patients received elective surgeries: a meta-analysis. BMC Anesthesiol. (2024) 24:93. doi: 10.1186/s12871-024-02479-9
33.
Frauenknecht J Kirkham KR Jacot-Guillarmod A Albrecht E . Analgesic impact of intra-operative opioids vs. opioid-free anaesthesia: a systematic review and meta-analysis. Anaesthesia. (2019) 74:651–62. doi: 10.1111/anae.14582
34.
Fletcher D Martinez V . Opioid-induced hyperalgesia in patients after surgery: a systematic review and a meta-analysis. Br J Anaesth. (2014) 112:991–1004. doi: 10.1093/bja/aeu137
35.
Banta-Green CJ Merrill JO Doyle SR Boudreau DM Calsyn DA . Opioid use behaviors, mental health and pain--development of a typology of chronic pain patients. Drug Alcohol Depend. (2009) 104:34–42. doi: 10.1016/j.drugalcdep.2009.03.021
36.
Sullivan MD Edlund MJ Zhang L Unützer J Wells KB . Association between mental health disorders, problem drug use, and regular prescription opioid use. Arch Intern Med. (2006) 166:2087–93. doi: 10.1001/archinte.166.19.2087
37.
Van Hecke O Austin SK Khan RA Smith BH Torrance N . Neuropathic pain in the general population: a systematic review of epidemiological studies. Pain. (2014) 155:654–62. doi: 10.1016/j.pain.2013.11.013
38.
Balanaser M Carley M Baron R Finnerup NB Moore RA Rowbotham MC et al . Combination pharmacotherapy for the treatment of neuropathic pain in adults: systematic review and meta-analysis. Pain. (2023) 164:230–51. doi: 10.1097/j.pain.0000000000002688
39.
Dieleman JP Kerklaan J Huygen F Bouma PAD Sturkenboom M . Incidence rates and treatment of neuropathic pain conditions in the general population. Pain. (2008) 137:681–8. doi: 10.1016/j.pain.2008.03.002
40.
Dworkin RH Panarites CJ Armstrong EP Malone DC Pham SV . Is treatment of postherpetic neuralgia in the community consistent with evidence-based recommendations?Pain. (2012) 153:869–75. doi: 10.1016/j.pain.2012.01.015
Summary
Keywords
anesthesia journal, systematic review, meta-analysis, bibliometrics, citation
Citation
Zou Z-y, Huang X-j, Song J-r and Yao Y-t (2025) Publications of systematic review and meta-analysis in the indexed anesthesia journals: a 10-year bibliometric analysis. Front. Med. 12:1523630. doi: 10.3389/fmed.2025.1523630
Received
06 November 2024
Accepted
11 April 2025
Published
07 May 2025
Volume
12 - 2025
Edited by
J. Douglas Thornton, University of Houston, United States
Reviewed by
Mirko Filippetti, University of Verona, Italy
Somchai Amornyotin, Mahidol University, Thailand
Updates
Copyright
© 2025 Zou, Huang, Song and Yao.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yun-tai Yao, yuntaiyao@126.com
†These authors have contributed equally to this work
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.