 Jinguo Liu
Jinguo Liu Jing Xu2
Jing Xu2- 1Department of Endoscopy Center, Sir Run Run Shaw Hospital, Zhejiang University, Hangzhou, China
- 2Department of Pathology, Sir Run Run Shaw Hospital, Zhejiang University, Hangzhou, China
- 3Department of Surgery, Huangshi Traditional Chinese Medicine Hospital, Hubei Chinese Medical University, Huangshi, China
Endoscopic full-thickness resection (EFTR) is an effective, economical, and minimally invasive technique for submucosal tumors (SMTs). However, technical complexity and prolonged operative time remain significant limitations. This study introduces a refined EFTR strategy termed “single traction combined with pre-clamping” in a cohort of 10 patients. The proposed technique demonstrates reduced procedural duration, technical difficulty, and intraoperative risks compared to the conventional approach.
Introduction
Endoscopic full-thickness resection (EFTR) has emerged as a therapeutic cornerstone for SMTs originating from the muscularis propria layer (1, 2). Despite its efficacy, post-resection wound closure remains technically demanding (3, 4), with serosal surface bleeding and inadvertent tumor displacement into the abdominal cavity posing critical challenges. To address these limitations, we present an innovative EFTR protocol integrating single traction with pre-clamping.
Case description
Ten patients (3 males, 7 females; mean age 61.7 years) with SMTs (gastric fundus: 8, gastric body: 1, duodenal bulb: (1) underwent EFTR using the novel technique (Table 1). Illustrative Case: A 57-year-old female with a gastric fundus SMT (Figure 1A) underwent EFTR after obtaining informed consent. Key procedural steps included: (1) Full-thickness incision to expose the tumor (Figure 1B). (2) Traction using the dental floss anchored with a titanium clip (Figure 1C). (3) Pre-clamping with three titanium clips (Figure 1D, Supplementary Video 1). (4) En bloc tumor resection with complete wound closure (Figure 1E). The operative time from full-thickness incision to wound closure took about
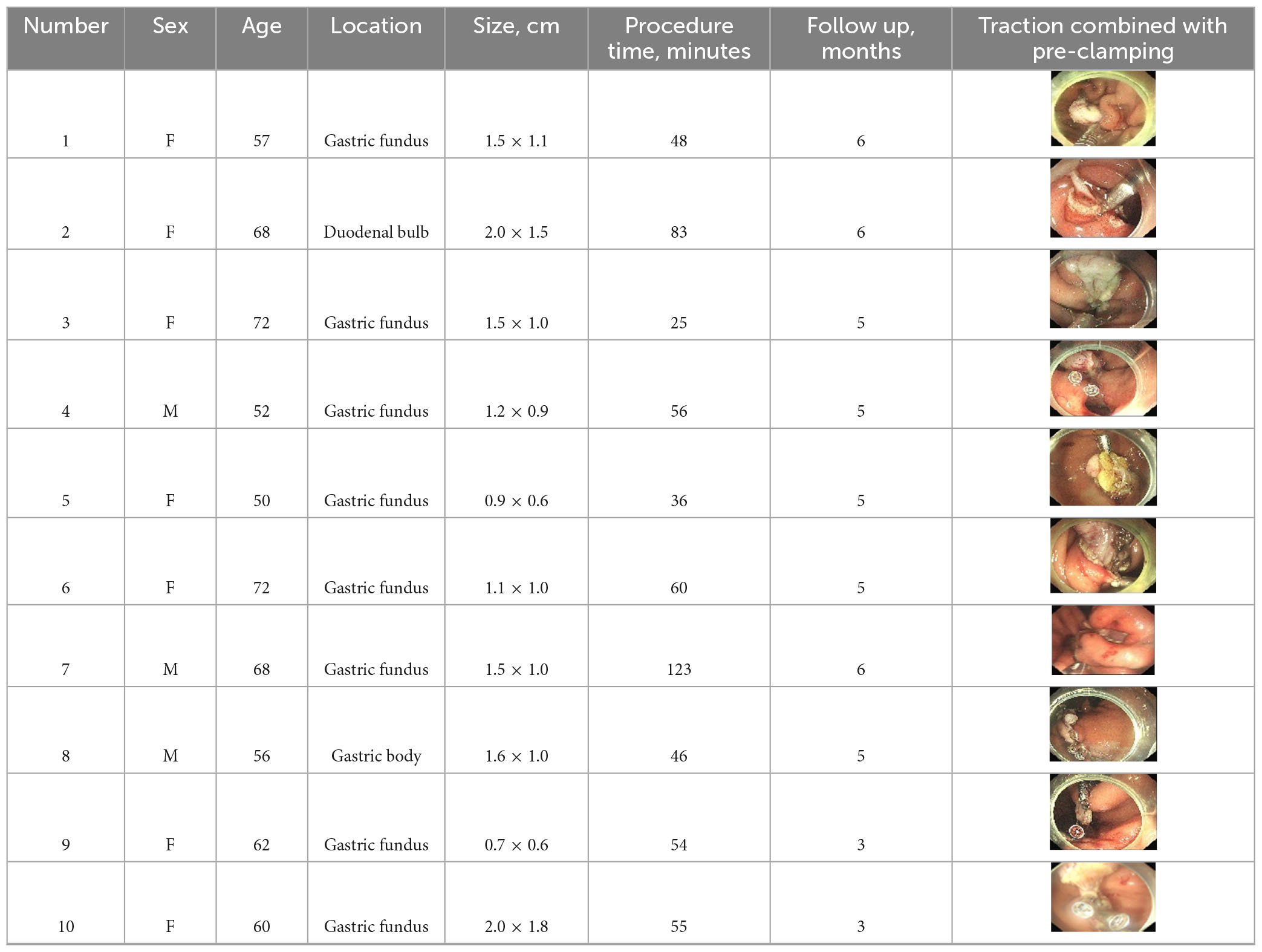
Table 1. Characteristics of ten patients undergoing EFTR with the “single traction combined with pre-clamping” technique.
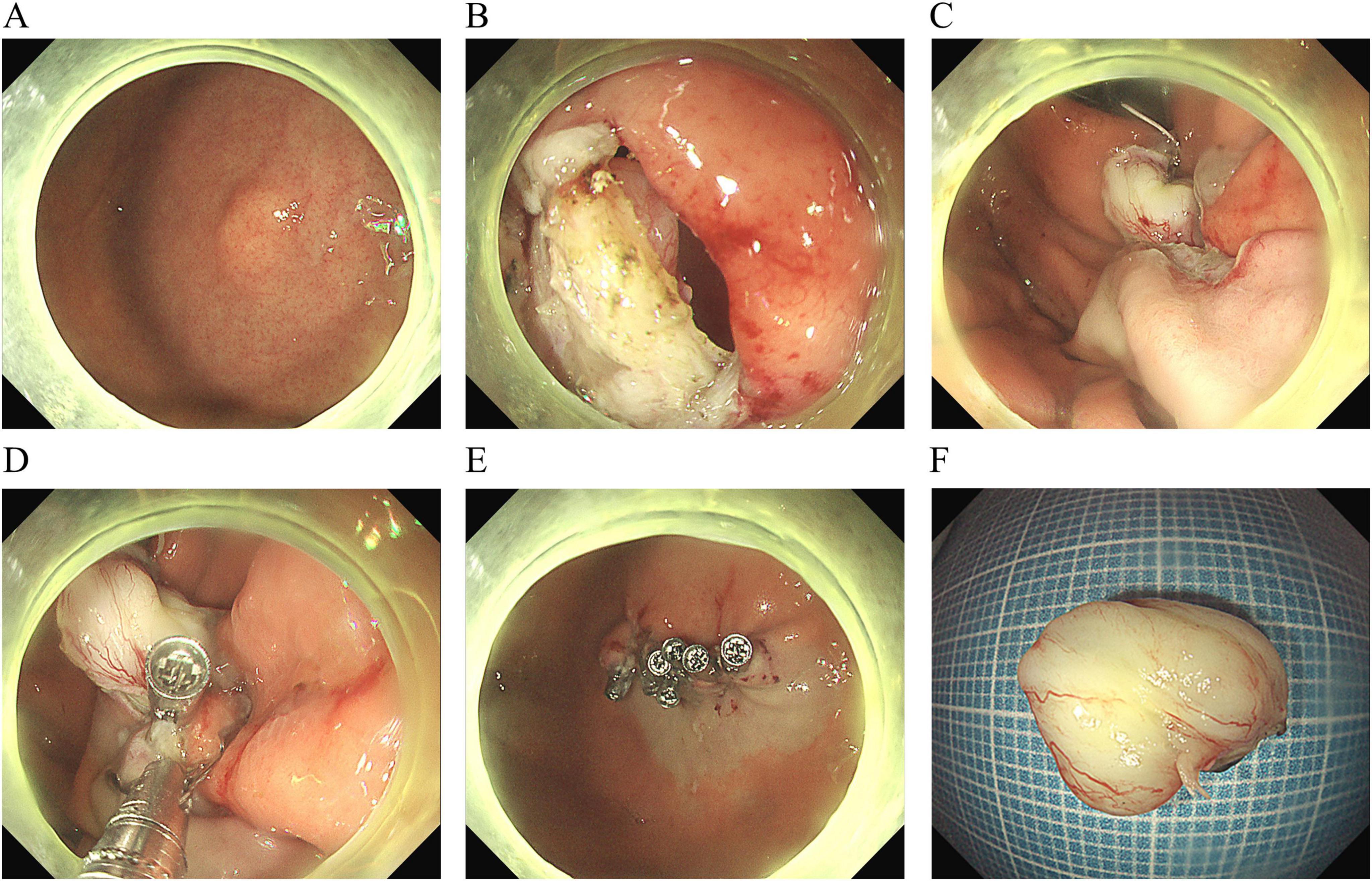
Figure 1. The procedural steps of endoscopic full-thickness resection with “single traction combined with pre-clamping.” (A) A submucosal tumor in the gastric fundus. (B) The exposed full-thickness incision. (C) Single traction using the dental floss. (D) Pre-clamping with three titanium clips. (E) Closure of the wound. (F) Macroscopic appearance of the resected tumor (measuring 15.0 × 11.0 mm).
only 12 min, and the tumor was pulled out (Figure 1F). The patient was discharged on the third day without any complications. Postoperative pathology showed a low-grade stromal tumor (Figures 2A–D).
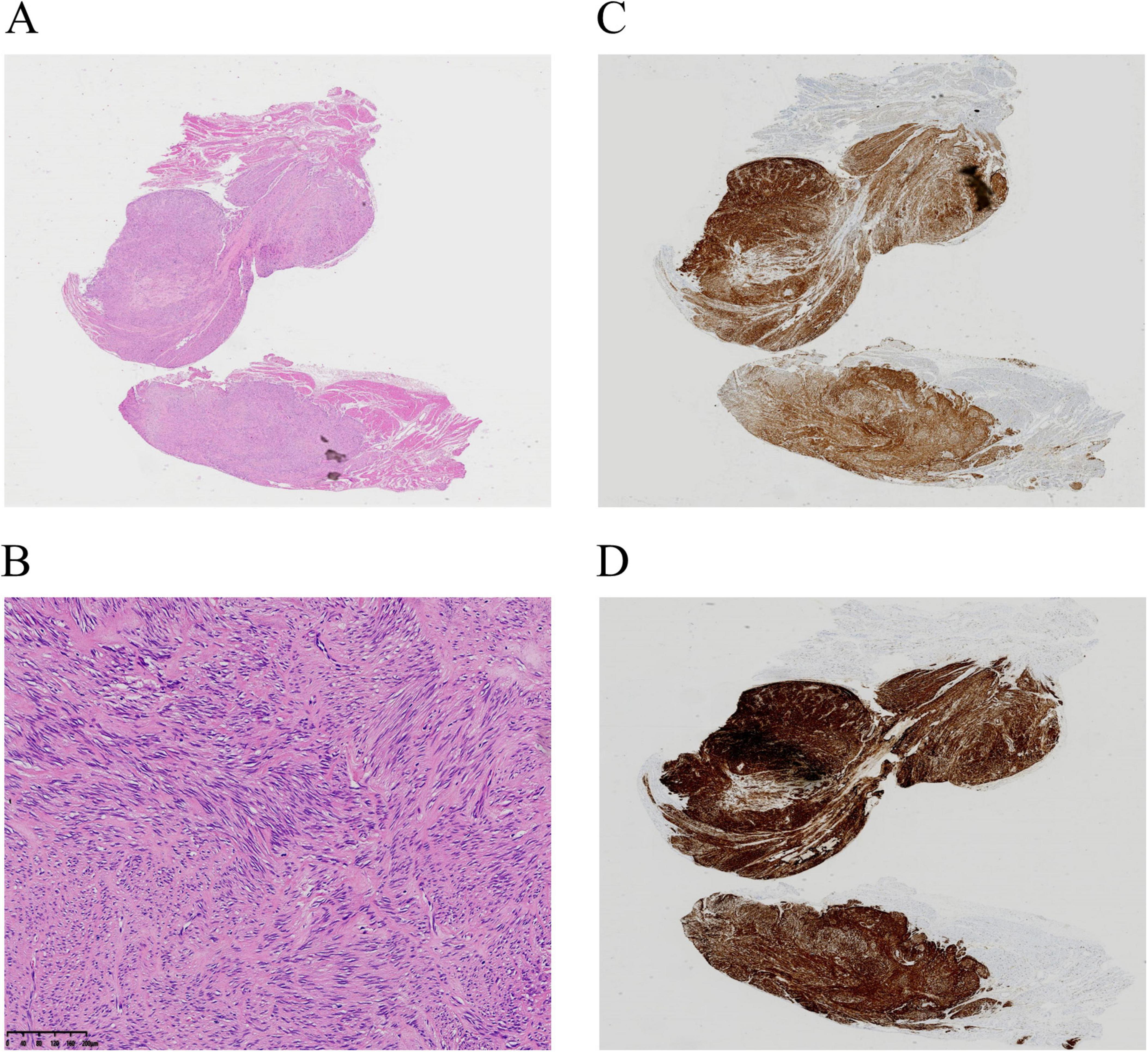
Figure 2. Pathologic examination. (A,B) Hematoxylin–eosin. Magnification: ×20 (A), ×100 (B). (C,D) Immunohistochemistry showing positive areas for CD117 (C) and DOG-1 (D).
The size of the tumors ranged from 0.7 × 0.6 cm to 2.0 × 1.8 cm, with procedural durations spanning 25–123 min (Table 1). None of the patients experienced postoperative bleeding or infection. Pathology in all patients showed a low-grade stromal tumor. No recurrence occurred during the follow-up period (3–6 months).
Discussion
While most SMTs exhibit benign behavior, malignant transformation potential persists in up to 13% of muscularis propria-originating lesions (5). EFTR is an effective, economical, and minimally invasive technique for SMTs originating from deep muscularis propria layer (4, 6). The traction method facilitated wound edge inversion, enabling effective pre-clamping and mitigating serosal bleeding risks. Proactively identifying and managing exposed serosal hemorrhagic vessels might effectively minimize the risk of postoperative bleeding. In addition, controlled traction maneuvers facilitated optimal tumor retraction into the gastric lumen, enabling direct visualization and en bloc resection under endoscopic surveillance.
Traction assistance is a practical technique for EFTR without severe perioperative adverse events. Double traction assistance was used in EFTR for the resection of a gastric submucosal tumor (4). Prior studies report operative times of 28–89 min using clip-assisted traction (7) and 25–130 min with snare-assisted methods (8), both without severe adverse events. Notably, snare traction demonstrated significantly shorter operative durations and a lower incidence of intraoperative bleeding versus conventional EFTR (53.6 ± 16.6 min vs 67.7 ± 33.4 min, P < 0.001) (9). In addition, traction assistance was used to remove an embedded gastric fishbone (10).
Our technique achieved comparable efficiency (25–123 min), with variability attributable to the size and location of the tumor, as well as the proficiency level of the endoscopist. The EFTR case with 123 min was performed by a novice operator, whereas experienced endoscopists completed the procedure in 25–83 min. Notably, when excluding the case involving the duodenal bulb, an anatomically challenging location, procedural durations were further streamlined to 25–60 min.
Clip-based traction modalities (e.g., clip-line, clip-snare, clip-rubber band) and non-clip alternatives (external forceps, gravity-based traction) have been extensively utilized (11–15). Our protocol uniquely integrates single traction with pre-clamping, offering dual advantages of time reduction and risk mitigation.
Data availability statement
The original contributions presented in this study are included in this article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
JL: Writing – original draft, Writing – review and editing. JX: Methodology, Writing – review and editing. LW: Methodology, Writing – review and editing. XG: Investigation, Writing – review and editing. XZ: Conceptualization, Writing – review and editing. ZZ: Investigation, Writing – review and editing. CZ: Investigation, Writing – review and editing. LY: Validation, Writing – review and editing, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the General Project (2025ZL078) of Zhejiang Provincial Administration of TCM.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1581544/full#supplementary-material
Supplementary Video 1 | Single traction with the dental floss and pre-clamping with three titanium clips.
References
1. Shi M, Zhang J, Ullah S, Liu D. Endoscopic full-thickness resection preserving the mucosa: More is better. Endoscopy. (2023) 55:E330–1. doi: 10.1055/a-1976-1988
2. Chu Y, Xu M. A real-world promising result of endoscopic full-thickness resection: It’s time for endoscopic full-thickness resection to be widely used. Am J Gastroenterol. (2020) 115:1972–3. doi: 10.14309/ajg.0000000000001028
3. Zhang Q, Cai J, Xiang L, Wang Z, de Liu S, Bai Y. Modified submucosal tunneling endoscopic resection for submucosal tumors in the esophagus and gastric fundus near the cardia. Endoscopy. (2017) 49:784–91. doi: 10.1055/s-0043-111236
4. Song Y, Sun X, Ge C, Li R. A modified endoscopic full-thickness resection technique: Double traction-assisted resection. Endoscopy. (2024) 56:E269–70. doi: 10.1055/a-2277-0540
5. Polkowski M. Endoscopic ultrasound and endoscopic ultrasound-guided fine-needle biopsy for the diagnosis of malignant submucosal tumors. Endoscopy. (2005) 37:635–45. doi: 10.1055/s-2005-861422
6. Granata A, Martino A, Ligresti D, Tuzzolino F, Lombardi G, Traina M. Exposed endoscopic full-thickness resection without laparoscopic assistance for gastric submucosal tumors: A systematic review and pooled analysis. Dig Liver Dis. (2022) 54:729–36. doi: 10.1016/j.dld.2021.09.014
7. Ru N, Li L, Bi Y, Gao F, Zhang B, Chai N, et al. A modified exposed endoscopic full-thickness resection: Traction-assisted resection while defect closing. J Dig Dis. (2023) 24:305–10. doi: 10.1111/1751-2980.13199
8. Ni L, Liu X, Wu A, Yu C, Zou C, Xu G, et al. Endoscopic full-thickness resection with clip- and snare-assisted traction for gastric submucosal tumours in the fundus: A single-centre case series. Oncol Lett. (2023) 25:151. doi: 10.3892/ol.2023.13737
9. Gu L, Wang X, Ouyang M, Li F, Wu Y, Liu X. Facilitating endoscopic full-thickness resection for gastric submucosal tumors with a novel snare traction method (with video). J Gastroenterol Hepatol. (2024) 39:535–43. doi: 10.1111/jgh.16428
10. Chen S, Ying S, Xian C, Li Y, Jiang W. Removal of an embedded gastric fishbone by traction-assisted endoscopic full-thickness resection. Endoscopy. (2024) 56:E232–3. doi: 10.1055/a-2268-5934
11. Yoshida M, Takizawa K, Nonaka S, Shichijo S, Suzuki S, Sato C, et al. Conventional versus traction-assisted endoscopic submucosal dissection for large esophageal cancers: A multicenter, randomized controlled trial (with video). Gastrointest Endosc. (2020) 91:55–65.e2. doi: 10.1016/j.gie.2019.08.014
12. Yamada S, Doyama H, Ota R, Takeda Y, Tsuji K, Tsuji S, et al. Impact of the clip and snare method using the prelooping technique for colorectal endoscopic submucosal dissection. Endoscopy. (2016) 48:281–5. doi: 10.1055/s-0034-1393241
13. Nomura T, Kamei A, Sugimoto S, Oyamada J. Colorectal endoscopic submucosal dissection using a clip-on-clip traction method. Endoscopy. (2018) 50:E197–8. doi: 10.1055/a-0605-2868
14. Imaeda H, Hosoe N, Ida Y, Kashiwagi K, Morohoshi Y, Suganuma K, et al. Novel technique of endoscopic submucosal dissection using an external grasping forceps for superficial gastric neoplasia. Dig Endosc. (2009) 21:122–7. doi: 10.1111/j.1443-1661.2009.00842.x
Keywords: endoscopic full-thickness resection, submucosal tumor, single traction, pre-clamping, en bloc resection
Citation: Liu J, Xu J, Wang L, Gu X, Zhang X, Zhang Z, Zhang C and Yu L (2025) Case Report: A novel strategy of endoscopic full-thickness resection: single traction combined with pre-clamping. Front. Med. 12:1581544. doi: 10.3389/fmed.2025.1581544
Received: 22 February 2025; Accepted: 02 June 2025;
Published: 02 July 2025.
Edited by:
Hung Leng Kaan, National University Hospital, SingaporeReviewed by:
Cherry Bansal, Tantia University, IndiaMeng-Yuan Shen, Zhejiang Chinese Medical University, China
Copyright © 2025 Liu, Xu, Wang, Gu, Zhang, Zhang, Zhang and Yu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Liangliang Yu, eXVkYW55dUB6anUuZWR1LmNu