Corrigendum: Influence of clinical and neurocognitive factors in psychosocial functioning after a first episode non-affective psychosis: differences between males and females
 Maria Serra-Navarro1,2†
Maria Serra-Navarro1,2† Silvia Amoretti1,2,3,4†
Silvia Amoretti1,2,3,4† Norma Verdolini1,2,5María Florencia Forte1,3
Norma Verdolini1,2,5María Florencia Forte1,3 Ana M. Sánchez-Torres6,7
Ana M. Sánchez-Torres6,7 Eduard Vieta1,2*Derek Clougher1
Eduard Vieta1,2*Derek Clougher1 Antonio Lobo2,8
Antonio Lobo2,8 Ana González-Pinto2,9,10Rocío Panadero2,11Alexandra Roldán2,12
Ana González-Pinto2,9,10Rocío Panadero2,11Alexandra Roldán2,12 André F. Carvalho13
André F. Carvalho13 Elena de la Serna2,14Alba Toll2,15J. A. Ramos-Quiroga2,4,16,17
Elena de la Serna2,14Alba Toll2,15J. A. Ramos-Quiroga2,4,16,17 Carla Torrent1,2*Manuel J. Cuesta6,7
Carla Torrent1,2*Manuel J. Cuesta6,7 Miguel Bernardo2,3 PEPs Group
Miguel Bernardo2,3 PEPs Group- 1Bipolar and Depressive Disorders Unit, Hospital Clinic of Barcelona, Institute of Neurosciences, IDIBAPS, University of Barcelona, Barcelona, Catalonia, Spain
- 2Biomedical Research Networking Center for Mental Health Network (CIBERSAM), Barcelona, Spain
- 3Barcelona Clinic Schizophrenia Unit, Hospital Clinic of Barcelona, Neuroscience Institute, August Pi I Sunyer Biomedical Research Institute (IDIBAPS), University of Barcelona, Barcelona, Spain
- 4Psychiatric Genetics Unit, Group of Psychiatry, Mental Health and Addictions, Vall d’Hebron Research Institute (VHIR), Barcelona, Catalonia, Spain
- 5Local Health Unit Umbria 1, Department of Mental Health, Mental Health Center of Perugia, Perugia, Italy
- 6Department of Psychiatry, Complejo Hospitalario de Navarra, Pamplona, Spain
- 7IdiSNA, Navarra Institute for Health Research, Pamplona, Spain
- 8Department of Medicine and Psychiatry, Instituto de Investigación Sanitaria Aragón (IIS Aragón), Zaragoza University, Zaragoza, Spain
- 9Araba University Hospital, Bioaraba Research Institute, Vitoria-Gasteiz, Spain
- 10Department of Psychiatry, University of the Basque Country (UPV-EHU), Vitoria-Gasteiz, Spain
- 11Department of Child and Adolescent Psychiatry, Hospital General Universitario Gregorio Marañón, School of Medicine, Institute of Psychiatry and Mental Health, Universidad Complutense, IiSGM, Madrid, Spain
- 12Department of Psychiatry, Hospital de la Santa Creu i Sant Pau, Institut d’Investigació Biomèdica-Sant Pau (IIB-SANT PAU), Universitat Autònoma de Barcelona (UAB), Barcelona, Spain
- 13Innovation in Mental and Physical Health and Clinical Treatment (IMPACT), School of Medicine, Barwon Health, The Institute for Mental and Physical Health and Clinical Translation, Deakin University, Geelong, VIC, Australia
- 14Department of Child and Adolescent Psychiatry and Psychology, 2017SGR881, Institut Clínic de Neurociències, Hospital Clínic Universitari, CIBERSAM, Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Department of Medicine, University of Barcelona, Barcelona, Spain
- 15Hospital del Mar Medical Research Institute (IMIM), Universitat Autònoma de Barcelona (UAB), Barcelona, Spain
- 16Department of Psychiatry, Hospital Universitari Vall d’Hebron, Barcelona, Catalonia, Spain
- 17Department of Psychiatry and Legal Medicine, Universitat Autònoma de Barcelona, Barcelona, Catalonia, Spain
Background: Deficits in psychosocial functioning are present in the early stages of psychosis. Several factors, such as premorbid adjustment, neurocognitive performance, and cognitive reserve (CR), potentially influence functionality. Sex differences are observed in individuals with psychosis in multiple domains. Nonetheless, few studies have explored the predictive factors of poor functioning according to sex in first-episode psychosis (FEP). This study aimed to explore sex differences, examine changes, and identify predictors of functioning according to sex after onset.
Materials and methods: The initial sample comprised 588 individuals. However, only adults with non-affective FEP (n = 247, 161 males and 86 females) and healthy controls (n = 224, 142 males and 82 females) were included. A comprehensive assessment including functional, neuropsychological, and clinical scales was performed at baseline and at 2-year follow-up. A linear regression model was used to determine the predictors of functioning at 2-year follow-up.
Results: FEP improved their functionality at follow-up (67.4% of both males and females). In males, longer duration of untreated psychosis (β = 0.328, p = 0.003) and worse premorbid adjustment (β = 0.256, p = 0.023) were associated with impaired functioning at 2-year follow-up, while in females processing speed (β = 0.403, p = 0.003), executive function (β = 0.299, p = 0.020) and CR (β = −0.307, p = 0.012) were significantly associated with functioning.
Conclusion: Our data indicate that predictors of functioning at 2-year follow-up in the FEP group differ according to sex. Therefore, treatment and preventative efforts may be adjusted taking sex into account. Males may benefit from functional remediation at early stages. Conversely, in females, early interventions centered on CR enhancement and cognitive rehabilitation may be recommended.
Introduction
Psychosocial functioning deficits are present in the early stages of psychosis (1, 2). Impairments are commonly observed in daily life activities. Although symptomatic remission was considered the critical treatment goal for a long time, and was the main focus in previous studies rather than functional recovery, there is increasing interest in addressing functional impairment. In terms of functional and clinical improvement, a recent meta-analysis found that long-term remission rate after a first psychotic episode was 58% and the recovery rate was 38% (3). According to the literature, several factors influence functionality. Certain factors are modifiable, including duration of untreated psychosis (DUP), negative symptoms (4–6), family environment, neurocognitive performance and cognitive reserve (CR) (1, 7, 8) and ergo are of potential clinical importance for therapeutic interventions. CR is defined as the coping capacity of the adult brain for pathology that minimizes symptomatology (9). Recently, it has been studied in severe mental disorders and interventions are being developed to enhance it given its potential protective properties (10–12). However, younger age, poorer premorbid adjustment, and male sex, are non-modifiable and represent a challenge to treatment, given the non-modifiable and represent a challenge to treatment, given their potential impact on psychosocial functioning (13–16).
Specific sex differences in neuroanatomy, neurofunctionality, gender and hormonal steroids have been reported in schizophrenia (SZ) individuals (17–19). Men show more severe gross neuroanatomical abnormalities than females (20) and these differences have even been observed in individuals with high genetic risk for the development of SZ; males have more neuroanatomical alterations than females when compared to same sex controls (18). In relation to hormonal steroids, Li et al. (21) found that estrogen deficiency is highly related to severity. Moreover, Mendrek et al. (20) identified an association between hormonal status and performance in neurocognitive domains. Regarding gender, a study from Lewine et al. (22) showed that female participants, independent of sex and diagnosis, performed better than males on neurocognition, with the exception of attention and executive function.
To date, males with SZ present more cognitive impairments than females and differences are less pronounced in the early stages of illness (20). Although, sex differences have been extensively described in first-episode psychosis (FEP), mixed results have been found in neurocognitive performance. For example, research has found that females demonstrate better premorbid adjustment (14, 23–25) and neurocognitive performance (14, 23) than their male counterparts. Conversely, higher severity of negative symptoms and higher rates of substance use were more frequent in males (23). Moreover, lower educational level, earlier age at onset, more severe illness course, poorer insight, more hospitalizations, and longer DUP were more frequent in male subjects with psychosis (13, 15, 23, 25–27). Regarding cognitive factors, females demonstrated better social cognition and verbal memory than men (25, 27), whilst males in the FEP group showed better performance on visuospatial (27) and working memory tasks (13).
A limited number of studies have explored the predictive factors of poor psychosocial functioning according to sex in FEP. Mattsson et al. (24) examined sex differences in the prediction of long-term outcomes in a group of 81 male and 72 females with FEP, and found that lower educational attainment level was the primary predictor of unfavorable outcome in females and a low premorbid level of functioning in males. Nevertheless, a notable limitation of this study was the lack of cognitive assessment despite cognitive performance being recognized as a reliable predictor of unfavorable outcomes in individuals with psychosis. Moreover, Willhite et al. (28) investigated sex differences in individuals at ultra-high-risk for developing a psychotic disorder and found that negative symptoms mediated differences in functioning between male and female subjects with FEP. These findings suggest that sex-based symptom presentation and functional outcome may predate conversion to psychosis (28). Therefore, identifying specific predictors according to sex may have important clinical implications for offering more personalized and targeted treatment in FEP.
There are two potential hypotheses that could explain these sex differences: hormone status and sex chromosomes. The first hypothesis is supported by the two peaks of incidence in females and the finding that females with SZ have more severe symptoms during the lower estrogen phase of their menstrual cycle (21, 29). Moreover, a study by Kaneda and Ohmori (30) showed that estradiol levels, a form of estrogen, are associated with severity of negative symptoms in males and may be a biological marker. The second hypothesis is based on recent genetic studies, which show that x-chromosome instability is involved and may contribute to the development of psychosis (21, 31).
Therefore, although research in the field is expanding, there remains a limited number of studies exploring sex differences in FEP, particularly in terms of clinical, neurocognitive, and psychosocial functioning. The present study addresses this gap in the literature by exploring these outcomes, while also identifying predictors of functionality in males and females, following a first episode non-affective psychosis. Specifically, and based on the research to date, we propose the following hypotheses: (1) differences will be found between males and females in clinical and neurocognitive outcomes; (2) changes from baseline to 2-year follow-up will be observed; and (3) we expect negative symptoms, neurocognition, CR and DUP to be predictors of psychosocial functioning. Specific sex differences are not hypothesized and will be explored accordingly. Similarly, the aims of the study were: (1) to explore sex differences in clinical, psychosocial functioning and neurocognitive outcomes; (2) to examine changes in neurocognition and functionality from baseline to 2-year follow-up; and (3) to identify predictors of functionality in males and females after a first episode non-affective psychosis.
Materials and methods
Study design and population
The sample was obtained from the “Phenotype-genotype interaction. Application of a predictive model in first psychotic episodes” (PEPs Project) study (32, 33). This is a multicenter, naturalistic, and longitudinal project under the umbrella of the Spanish Research Network on Mental Health (CIBERSAM) (34). The background, rationale and study design have been previously presented (32, 33). All participants were evaluated at two different time points. Individuals with FEP completed the full test battery of sociodemographic, clinical, functional, and neurocognitive assessments at both baseline and two-year follow-up. The same evaluation was administered to HCs at both stages, however, for the clinical assessment only the SCID-I-II was assessed.
Initially, the sample was composed of 588 individuals: 335 participants with a FEP and 253 healthy controls (HC). Inclusion criteria were: (1) aged between 7 and 35 years at the time of first evaluation; (2) duration of psychotic symptoms ≤1 year; (3) signed informed consent and (4) ability to speak Spanish. Exclusion criteria were as follows: (1) intellectual deficit according to DSM-IV criteria (including not only an IQ below 70 but also impaired functioning); (2) history of head injury with loss of consciousness and (3) organic disease with mental impact.
To ensure sample homogeneity, only adults with non-affective FEP and HCs were included. At two-year follow-up and according to DSM-IV-TR, non-affective FEP diagnosis was considered as: schizophrenia, schizophreniform, schizoaffective disorders, and other psychoses not otherwise specified. Supplementary Figure 1 shows the flowchart for the selection of the 247 non-affective FEP at baseline.
The FEP group was matched by age (±10%), gender and parental socioeconomic status (±1 level). The exclusion criteria for HC were the same as the FEP group, but also included the presence of a current or past psychotic disorder, major depression or other psychiatric illness and having a first-degree relative with psychotic disorder history. In this study, 224 adult HC were included.
Ethical approval was granted by the Hospital Clinic Ethics and Research Board. The study followed the ethical principles of the Declaration of Helsinki and Good Clinical Practices. All participants provided written informed consent.
Assessments
Clinical and sociodemographic assessment
Sociodemographic and clinical data from all participants were collected at baseline and at two years follow-up. Hollingshead’s Two-Factor Index of Social Position (35) was used to define parental socioeconomic status (SES); Duration of Untreated Psychosis (DUP) was estimated considering the number of days between the presence of the first psychotic symptoms and the beginning of adequate treatment, and antipsychotic mean doses were calculated by chlorpromazine equivalents (CPZ) based on international consensus (36). Drug misuse habits were gathered using an adapted version of the European Adaptation of a Multidimensional Assessment Instrument for Drug and Alcohol Dependence scale (37). The Structured Clinical Interview for DSM (SCID-I-II) was used to establish diagnoses according to DSM-IV criteria (38, 39) in the FEP group. Conversely, the SCID-I-II was administered to assess HC’s mental health to ensure that they met the inclusion criteria and to rule out the exclusion criteria of the study.
In the FEP group, psychotic symptoms were assessed with the Positive and Negative Syndrome Scale (PANSS) (40), and affective symptoms with the Montgomery-Asberg Depression Rating Scale (MADRS) (41) and the Young Mania Rating Scale (YMRS) (42). A total score was obtained from each scale. Higher scores correspond to greater severity.
Functional assessment
The Functioning Assessment Short Test (FAST) was used to evaluate functional outcome (43, 44) from all participants. Higher scores represent higher disability.
Neurocognitive assessment
A neurocognitive battery was used to evaluate different cognitive domains through standardized instruments. The neuropsychological assessment was made in the second month of evaluation in order to ensure the psychopathologic stability of individuals with FEP and was repeated in the two-year follow-up visit. The neurocognitive battery measured the following cognitive domains: (1) Sustained attention was tested with the Continuous Performance Test–II (CPT-II) (45), version 5; (2) Verbal learning and memory, assessed with the Verbal Learning Test Spain Complutense for adults (TAVEC) (46); (3) Working memory was assessed by the Digit Span Subtest and the Letter-Number Sequencing Subtest of the Wechsler Adult Intelligence Scale (WAIS-III) (47); (4) Processing speed was assessed with the Trail making test (Form A) (TMT-A) (48); (5) The executive functions were evaluated using the Wisconsin Card Sorting Test (49), corrected by age and educational level; (6) Verbal fluency was evaluated using semantic fluency (animals) (50) and F-A-S tests (51); and (7) Managing Emotions was assessed with the Mayer-Salovey-Caruso Emotional Intelligence Test (MSCEIT) (52). All neurocognitive measures were transformed into T-scores. Higher scores correspond to better performance in all neurocognitive domains except for attention.
Cognitive reserve and premorbid adjustment assessment
Premorbid adjustment, namely levels of functioning before the onset of psychosis, was assessed with The Premorbid Adjustment Scale (PAS) (53). Only childhood and early adolescence life periods have been taken into account since they are the two periods answered by all the participants. Higher scores indicate worse premorbid adjustment.
Cognitive reserve (CR) was assessed using the three proposed proxy indicators of CR in FEP as described in previous literature (10, 54–56). Proxy indicators include education, estimated premorbid IQ, leisure, social, and physical activities. Education was measured with: patient’s completed years of study, performance during school, and parents’ educational level. Estimated premorbid IQ and crystallized intelligence were evaluated with the vocabulary subtest of WAIS-III which appears to remain stable during disease progression (57). A “cognitive reserve score” was created using a Principal Components Analysis (PCA) for each subject. Higher scores correspond to better performance for each subject. Higher scores correspond to better performance.
Statistical analysis
Neurocognitive variables were grouped using PCA. The resulting cognitive domains were: sustained attention, verbal learning and memory, working memory, processing speed, executive functions, fluency, and emotion management (see Supplementary Table 1). Firstly, a multivariate analysis of variance with two factors: (1) sex (female vs. male) and (2) group (patients vs. HC) was conducted for demographic variables and for cognitive functions. For cognitive functions, a multivariate analysis of covariance with age and chlorpromazine equivalent as covariates was performed because FEP females and males were statistically different in these variables. In a second step, repeated measures multivariate analysis of covariance was used to check the differences and changes in cognitive functions with three factors: (1) sex (female vs. male), (2) group (patients vs. HC), and (3) assessment (baseline and follow-up). In patients, change scores were calculated using the reliable change index (RCI). To check changes for psychosocial functioning, RCI was calculated following this formula: (T2 − T1)/SED, where T1 and T2 are the individual’s observed baseline and 2-years follow-up scores, and SED is the standard error of the difference. For cognitive measures, corrections for measurement error and practice effects were then calculated for each participant using the RCI, calculated as (T2 − T1) − (M2 − M1)/SED, where T1 and T2 are the individual’s observed baseline and 2-year follow-up scores, M1 and M2 are the control group mean baseline and follow-up scores, and SED is the standard error of difference. An RCI [alpha set to 0.10 (two-tailed)] greater than +1.645 is considered a significant change, while reliable decline occurs when values fall below −1.645 (58–60). In the third step, in individuals with FEP, partial correlations controlling for chlorpromazine equivalent at baseline were computed for the continuous variables. The association between binary variables and the FAST score at 2-year follow-up was examined using a t-test, controlling again for the chlorpromazine equivalent effects. Finally, variables that were significantly correlated with FAST (p < 0.05) were included in two linear regression models with backward elimination in both sexes. In this way, we explored factors that predict psychosocial functioning at baseline and at 2-year follow-up, according to sex.
Statistical Package for the Social Sciences (SPSS v26) was used to analyze data. All statistical tests were carried out two-tailed, with an alpha level of significance set at p < 0.05.
Results
Sociodemographic, clinical, functional and cognitive characteristics of the sample and sex differences
A total of 247 FEP subjects (161 males and 86 females) and 224 HC (142 males and 82 females) were enrolled in this study. At two-year follow-up 145 individuals with FEP and 152 HC were re-evaluated as 102 subjects with FEP and 72 HC participants had withdrawn from the study due to a loss of follow-up or refusal of re-evaluation. The follow-up sample of the FEP group (n = 145) did not differ from the baseline sample in terms of sociodemographic, clinical, functional, and neurocognitive performance. Similarly, HCs assessed at follow-up (n = 152) showed no differences to the total sample of baseline HCs in terms of sociodemographic, functional, and the majority of cognitive domains.
A summary of the baseline sociodemographic and clinical characteristics of individuals with FEP and HC is shown in Table 1. There were main effects of group for SES (χ2 = 23.165, p < 0.001), tobacco and cannabis use (χ2 = 35.732, p < 0.001 and χ2 = 39.332, p < 0.001, respectively), psychosocial functioning (t = 437.177, p < 0.001), cognitive reserve (F = 155.857, p < 0.001), premorbid adjustment (F = 252.087, p < 0.001) and all cognitive measures. The male group was younger (F = 6.572, p = 0.011), reported higher tobacco and cannabis use (χ2 = 9.832, p = 0.007 and χ2 = 31.307, p < 0.001, respectively), higher CPZ (F = 5.720, p = 0.017), better attention (F = 11.466, p = 0.001) and processing speed (F = 12.640, p < 0.001), higher CR (F = 6.160, p = 0.013), and worse premorbid adjustment (F = 4.058, p = 0.045). No significant effect for GroupXSex was observed.
TABLE 1
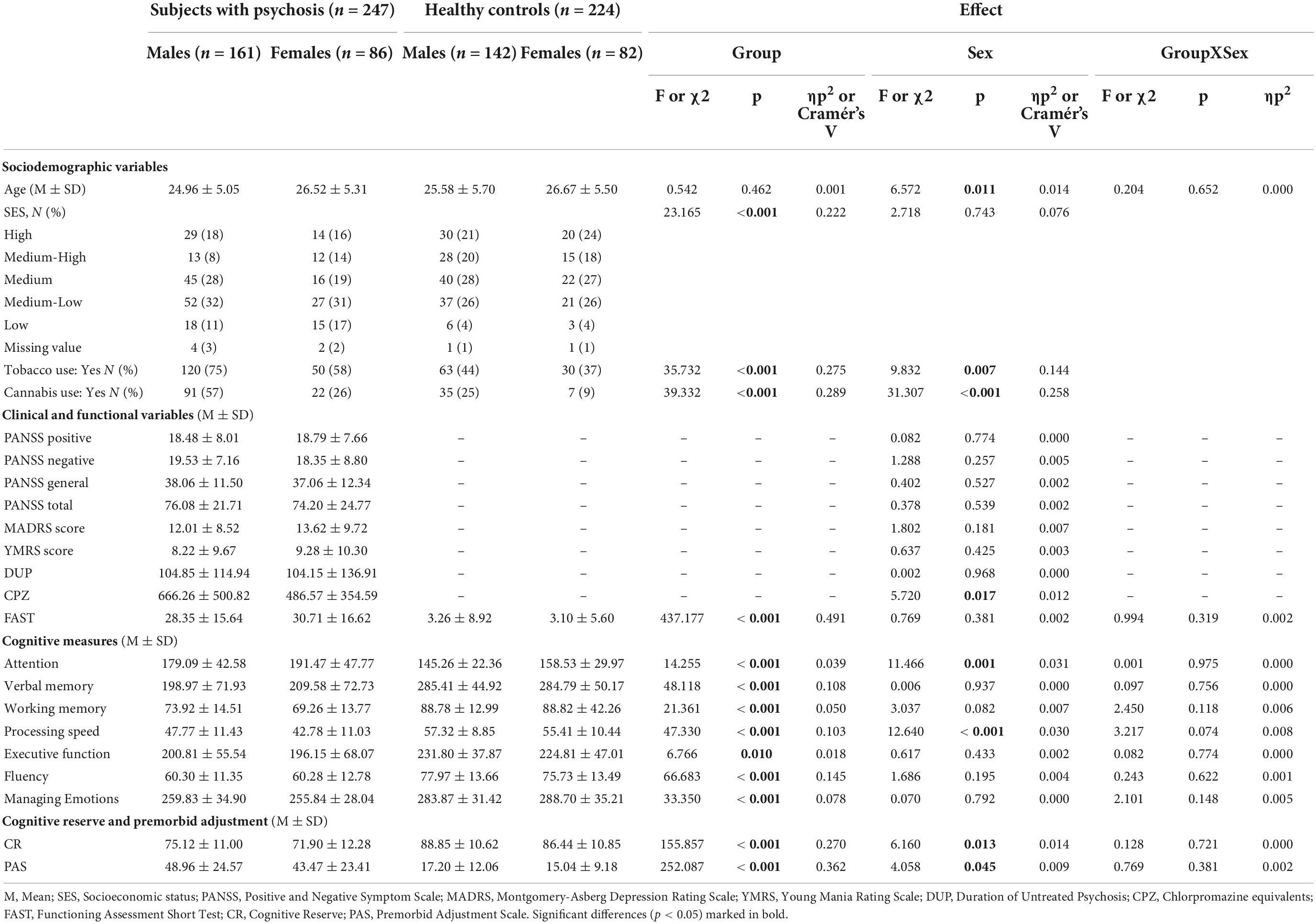
Table 1. Sex differences in sociodemographic, clinical and functional characteristics at baseline for subjects with psychosis and healthy controls.
At two-year follow-up, there were main effects of group for tobacco use, psychosocial functioning and all cognitive measures. The female group presented worse attention (F = 24.176, p < 0.001) and processing speed (F = 8.402, p = 0.004). Finally, there was a group x sex interaction for attention (F = 10.028, p = 0.002) (for more details see Supplementary Table 2). Supplementary Figure 2 shows the mean psychosocial functioning and cognitive scores with error bars in males and females with psychosis at baseline and follow-up.
Changes in cognitive and clinical characteristics and psychosocial functioning
Results from the repeated measures ANOVA revealed a time effect for psychosocial functioning (p < 0.001, ηp2 = 0.065) and all cognitive domains (values of partial eta squared range from 0.021 to 0.144) except attention (p = 0.097), indicating an improvement for both groups from baseline to the 2-year follow-up. An improvement in clinical status was also observed (values of partial eta squared range from 0.200 to 0.396). There was a significant time x group effect observed only for psychosocial functioning (p < 0.001, ηp2 = 0.085), indicating a significantly different effect in the FEP group over time compared with the HC group. No significant effect for TimeXGroupXSex was observed (see Table 2).
TABLE 2
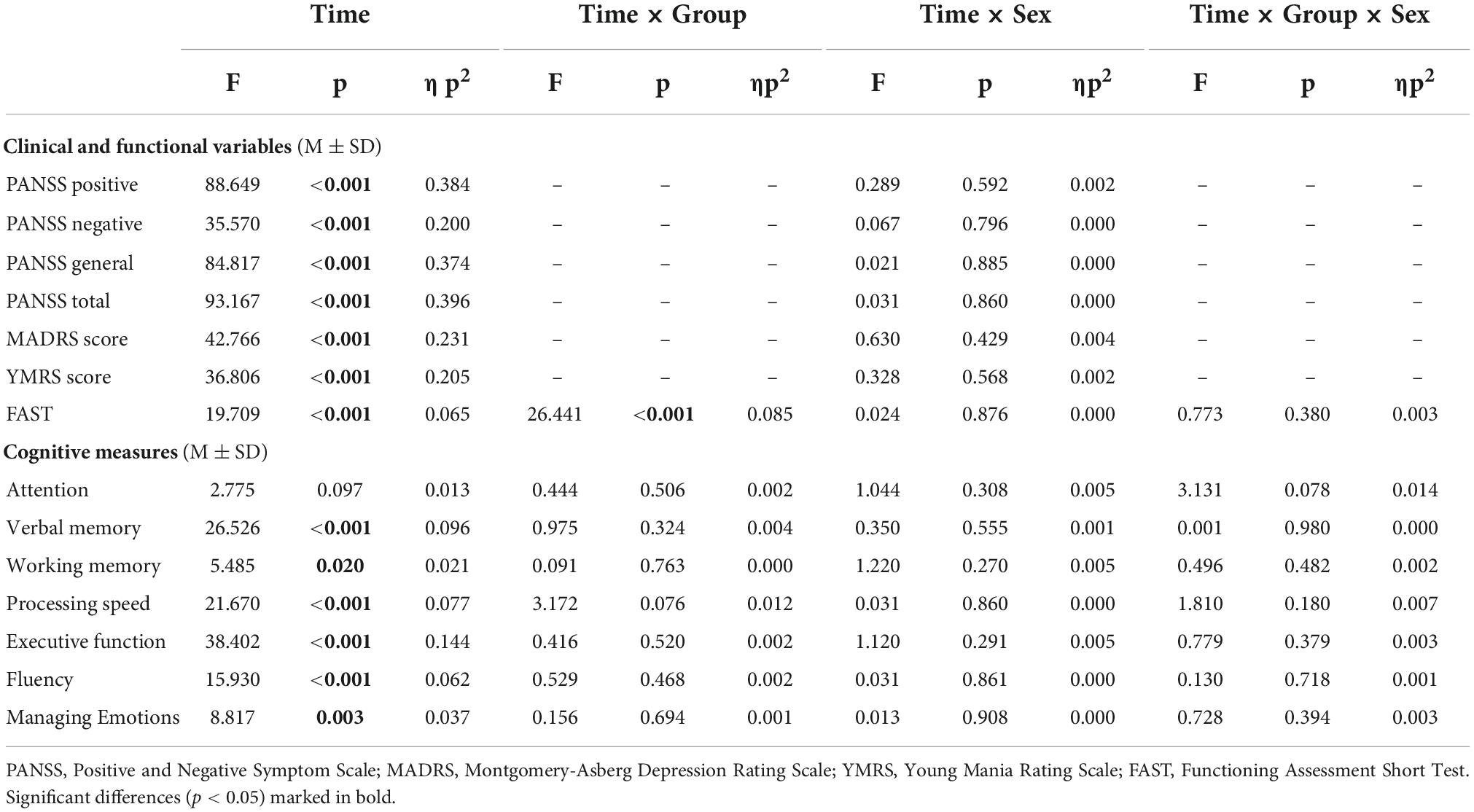
Table 2. Changes in clinical, cognitive functions and psychosocial functioning.
Supplementary Table 3 displays the percentage rates of improvements, declines and stability on all cognitive domains and psychosocial functioning as determined by the RCI. Most of the FEP improved their functionality on follow-up (67.4% of both males and females). Results herein indicate that although working memory improved over time, females improved less than males (p < 0.001, Cramer’s V = 0.403). No other significant group differences were observed.
Predictors of psychosocial functioning
At baseline, in males with FEP, worse psychosocial functioning correlated with higher positive (r = 0.308, p < 0.001), negative (r = 0.234, p = 0.004), depressive (r = 0.287, p < 0.001) and manic symptoms (r = 0.231, p = 0.005), poorer performance in processing speed (r = –0.183, p = 0.035) and social cognition (r = –0.213, p = 0.017), and worse premorbid adjustment (r = 0.228, p = 0.006). In females, FAST was also correlated with positive (r = 0.467, p < 0.001), negative (r = 0.613, p < 0.001), depressive (r = 0.358, p = 0.001), manic symptoms (r = 0.272, p = 0.017), and premorbid adjustment (r = 0.433, p < 0.001). However, regarding neurocognitive performance, a significant correlation was observed in sustained attention only (r = 0.299, p = 0.025). For HCs, FAST correlated with premorbid adjustment (r = 0.324, p < 0.001) in males and in verbal memory (r = –0.345, p = 0.003), verbal fluency (r = –0.281, p = 0.018), and premorbid adjustment (r = 0.426, p < 0.001) in females. No other variables correlated with FAST at baseline (see Supplementary Table 4). At follow-up, worse psychosocial functioning in FEP males correlated with higher negative symptoms at baseline (r = 0.295, p = 0.003), longer DUP (r = 0.272, p = 0.010), higher CPZ (r = 0.295, p = 0.003), worse sustained attention (r = 0.346, p = 0.003), and worse premorbid adjustment (r = 0.359, p < 0.001). In FEP females, FAST was correlated with worse performance in processing speed (r = –0.424, p = 0.005), executive function (r = –0.350, p = 0.029) and lower cognitive reserve (r = –0.312, p = 0.032). In HCs none of the baseline variables were associated with psychosocial functioning at follow-up (Table 3).
TABLE 3
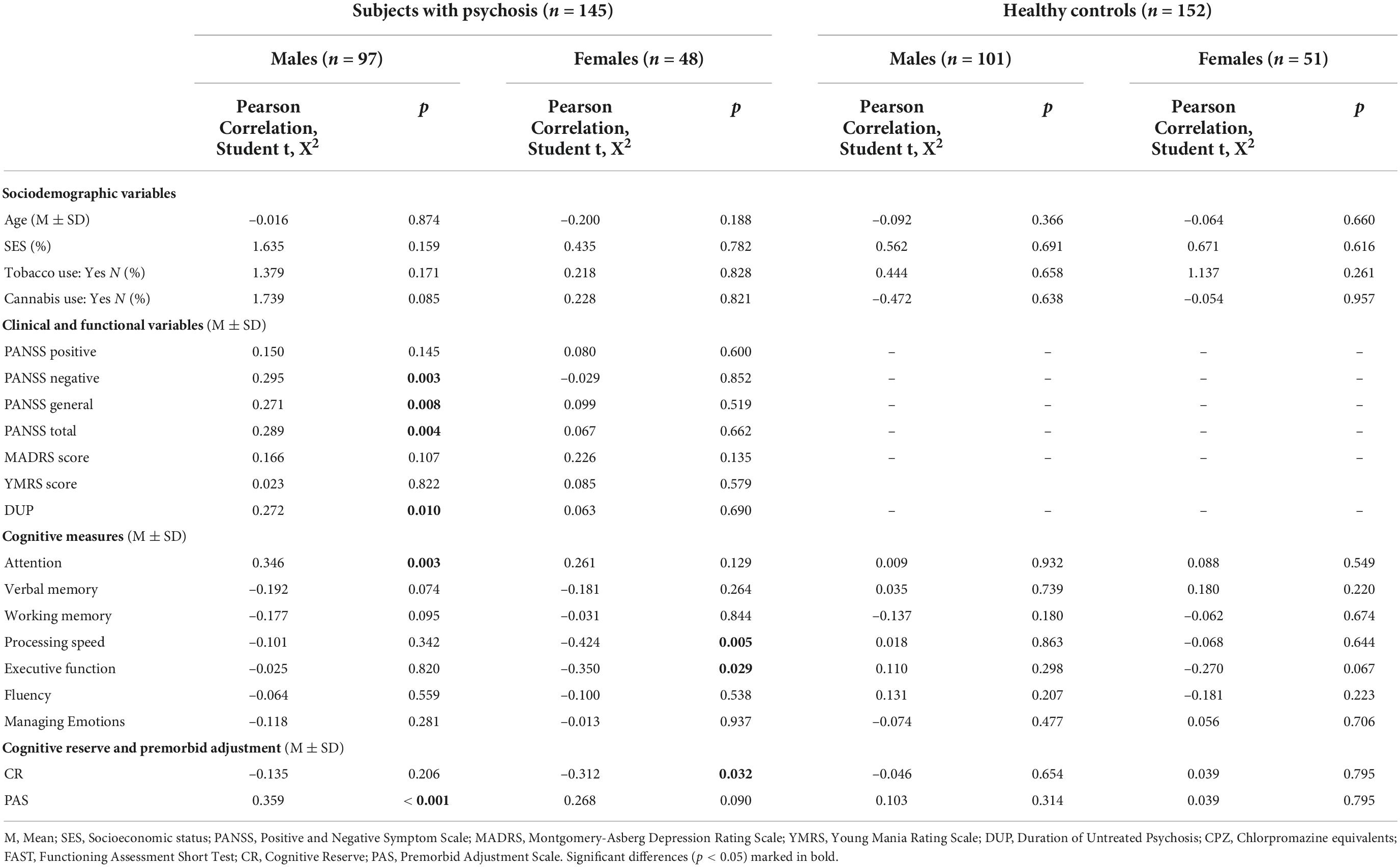
Table 3. Correlations between psychosocial functioning (FAST) at follow-up and socio-demographic and clinical variables at baseline in subjects with psychosis and healthy controls.
Results for linear regression are reported in Table 4. At baseline in FEP males, after including the variables that reached statistical significance in bivariate analyses in the regression model and controlling for chlorpromazine equivalent, positive (β = 0.285, p < 0.001), depressive symptoms (β = 0.195, p = 0.014) and adjustment (β = 0.213, p = 0.006) were significantly associated with worse FAST, with a higher effect exerted by positive symptoms. At follow-up, longer DUP (β = 0.328, p = 0.003) and worse premorbid adjustment (β = 0.256, p = 0.023) were associated with impaired psychosocial functioning.
TABLE 4

Table 4. Linear regression of the socio-demographic, clinical and neuropsychological variables associated with psychosocial functioning in males and females with psychosis.
In females, at baseline, negative (β = 0.655, p < 0.001), manic symptoms (β = 0.412, p < 0.001) and worse attention performance (β = 0.248, p = 0.012) were significantly associated with worse functioning, while at follow-up processing speed (β = –0.403, p = 0.003), executive function (β = –0.299, p = 0.020) and CR (β = –0.307, p = 0.02) were significantly associated with FAST, with a higher effect exerted by processing speed.
Discussion
Two main findings emerged from the present study. Firstly, individuals with FEP had higher substance abuse, lower SES, worse psychosocial functioning and neurocognitive performance in all cognitive domains in relation to the HC group (27, 61). As expected, individuals with FEP present more difficulties and impairments than the HC group. Secondly, different effects of sex were found regardless of the group. The male group uses more tobacco and cannabis, are younger, have higher CR and CPZ doses, worse premorbid adjustment and perform better in attention and processing speed. These differences have been found in individuals with schizophrenia. Males tend to show a higher incidence of the disorder, an earlier age at onset, poorer premorbid adjustment, higher rates of substance abuse, worse psychosocial functioning, and a more severe course of the disease, especially in negative symptoms, while in the FEP group mixed results have been found (14, 62, 63). In addition, males with psychosis require higher doses of antipsychotic than females (21). In terms of premorbid adjustment, no significant differences were found in our study, failing to replicate the results of Cotton et al. (64). Previous literature suggests that males have greater negative symptoms than females with FEP, especially related to emotional withdrawal, blunted affects, and avolition-apathy (13, 25, 65, 66). However, in our study, no significant differences were found in this regard. These results might be interpreted in the light of different models that explain SZ spectrum disorders. The neurodevelopmental model of SZ posits that the illness is the end stage of abnormal neurodevelopmental processes that began years before the onset of the illness (64). Within this theoretical framework, an attempt to describe relationships between sex/gender and indicators of neurodevelopment compromise in SZ has been made, but no associations regarding sex were found (62).
There are some possible explanations for the inconsistency in results. First, no specific scale was used to assess negative symptoms as the PANSS was the chosen measurement in this study. Similar to our results, González-Rodríguez et al. (65) found no significant gender differences in psychopathology assessed by the PANSS in FEP. Secondly, Willhite et al. (28) found no differences at baseline in negative symptoms when they studied gender differences in a simple of high-risk individuals. Regarding processing speed, it has been shown that females with schizophrenia have poorer processing speed when evaluated using the TMT-A (67). However, these findings were not replicated by Zanelli et al. (68) who found no sex differences in neurocognition among FEP. The female group showed worse sustained attention performance than males. Research has shown differences between sex, for example, females showed slower reaction times (69) and were less aroused than males (70). Similar results were described by Hsieh et al. (71) who evaluated sustained attention with the CPT in a sample of 900 adults and found that males outperformed females. Thus, sex differences in neurocognitive performance are a controversial issue as results remain inconclusive. The heterogeneity in the results may be partly explained by differences in the studied populations, namely FEP or schizophrenia, as well as the subtest used to measure each domain. To compare the results and generalize the findings, future research should endeavor to homogenize evaluation tools to assess the neurocognitive domains and the stage of the illness.
Regarding changes, both groups improved at follow-up and no differences were found between males and females. According to previous literature, FEP individuals improve in functional outcomes, achieved recovery and demonstrated symptom remission (54, 72). With reference to gender, we found that men improved significantly more than women in working memory. To the best of our knowledge, this has not yet been documented in the current literature.
Although no clinical or psychosocial functioning differences have been found between sexes, it seems that the variables associated with poorer functioning differ according to sex. For the prediction of psychosocial functioning, worse premorbid adjustment and higher were predictors of worse psychosocial functioning in males. The relationship between premorbid adjustment and DUP with psychosocial functioning have been widely reported (73). Premorbid adjustment is also considered a predictor of clinical severity, especially for subjects with FEP presenting negative symptoms (5, 10).
In females, worse processing speed, worse executive function and lower CR level predicted worse psychosocial functioning. In severe mental illness, CR has a significant influence on cognitive, clinical and functional outcomes (11, 74). In FEP, individuals with CR perform better in neurocognitive scales and functioning (1, 10, 54). A lower educational level predicted worse results in females but not in males (24). Regarding processing speed, Lindgren et al. (75), reported that it was associated with 1-year remission, occupational status, and maintaining of life goals and Milev et al. (76) found that in FEP, verbal memory, processing speed, and attention were potential targets for psychosocial interventions to improve outcome. In fact, it has been shown that processing speed is related to functioning in individuals with ultra-high-risk for psychosis (77). In line with our results, a recent meta-analysis found that there is a positive association between executive function and psychosocial function (78).
Thus, it seems that the predictors of psychosocial functioning at 2-year follow-up in the FEP group differ according to sex (see Figure 1). These sex differences could have important clinical implications, not only in terms of diagnosis, but also in terms of therapeutic approach. In the case of the former, and in order to improve psychosocial functioning, the present study supports the need to perform a thorough assessment of CR, premorbid adjustment, DUP, and neurocognitive status. In terms of therapeutic options, based on these results, we propose that males with FEP may benefit from a functional remediation from early stages. Conversely, in females, the implementation of early interventions centered on CR enhancement and cognitive rehabilitation may be beneficial, as CR has been associated with better cognitive performance and psychosocial functioning (1, 10, 54) and is a reliable predictor of functionality in this group.
FIGURE 1
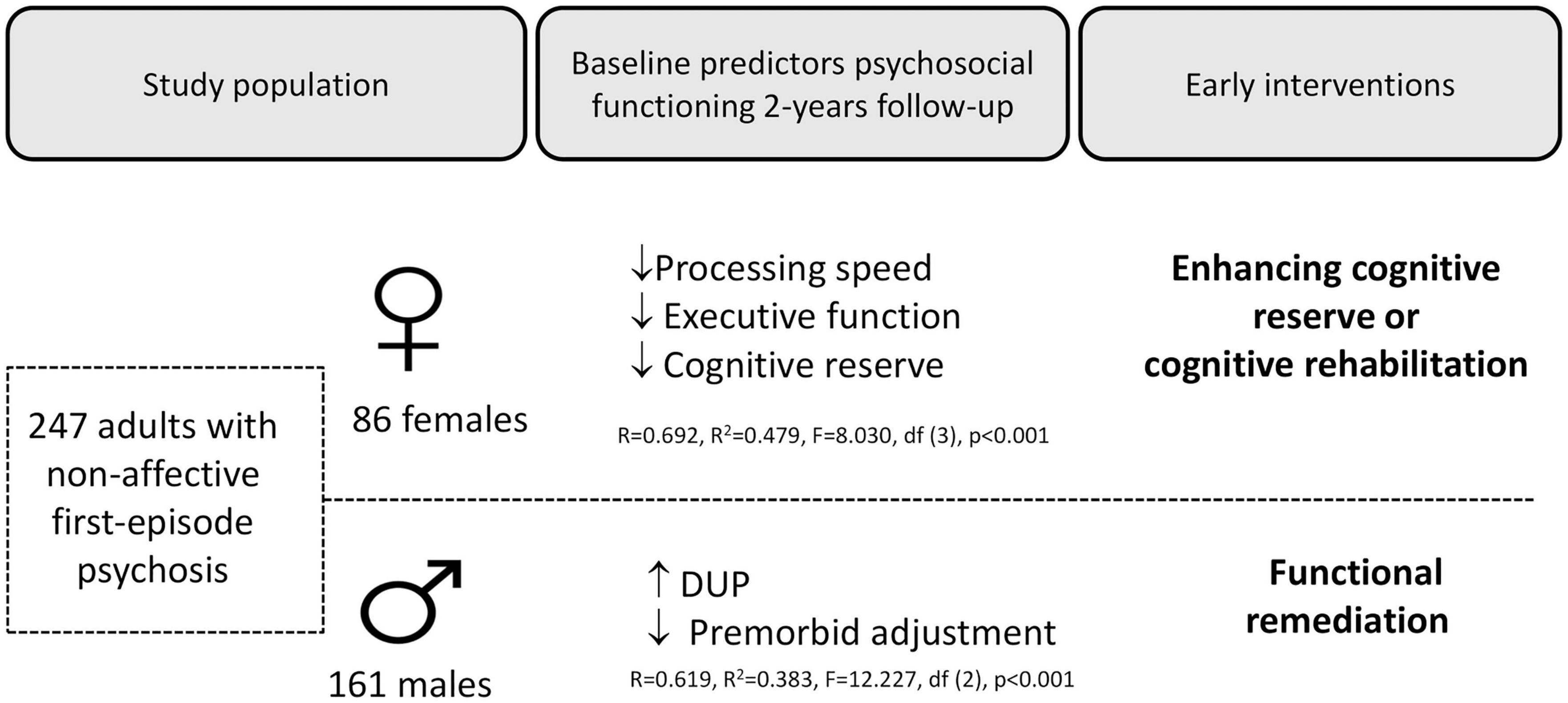
Figure 1. Overview of the study population, the main results, and the recommended intervention.
This study has certain limitations which must be taken into account. Firstly, when participants were evaluated, there was no validated instrument to measure CR so criteria established and replicated in previous studies were followed. Secondly, no specific scale was used to assess negative symptomatology. Future studies making use of newer and improved negative symptom scales — such as the Brief Negative Symptom Scale (BNSS) (79) or the Clinical Assessment Interview for Negative Symptoms (CAINS) (80) — may be more appropriate for their evaluation. Thirdly, another limitation is the difference between the group size of males and females. In the female group, the small sample size may have interfered with the results (low statistical power). This is possibly due to the naturalistic and multicentric nature of the study with a representative sample of non-affective FEP in a stable clinical phase recruited from the whole Spanish territory. Thus, further studies with larger sample sizes are required to confirm these findings.
In conclusion, this study identified premorbid adjustment, and DUP as risk factors in males with FEP. Similarly, processing speed, executive function and CR were recognized as modifiable factors in females. These results suggest that the enhancement of modifiable factors may improve functional outcomes and could be beneficial in the development of early intervention programs. Future studies, using larger sample sizes are needed to determine which factors might influence the relationship between neurocognitive or clinical outcomes and functioning depending on sex. Finally, longitudinal studies would help to understand the long-term impact of these findings.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Hospital Ethics Committee (2008/4232), according to the Declaration of Helsinki principles and Good Clinical Practice guidelines, within the requirements of the Spanish Law and the State Regulatory Authority. The patients/participants provided their written informed consent to participate in this study.
PEPs Group
Jairo González-Díaz: Barcelona Clinic Schizophrenia Unit, Hospital Clinic of Barcelona, Neuroscience Institute, August Pi I Sunyer Biomedical Research Institute (IDIBAPS), University of Barcelona, Barcelona, Spain; UR Center for Mental Health - CERSAME, School of Medicine and Health Sciences, Universidad del Rosario, Bogota DC, Colombia; Clínica Nuestra Señora de la Paz, Bogota DC, Colombia. Lucila Barbosa: Barcelona Clinic Schizophrenia Unit, Hospital Clinic of Barcelona, Neuroscience Institute, August Pi I Sunyer Biomedical Research Institute (IDIBAPS), University of Barcelona, Barcelona, Spain. Covadonga M. Diaz-Caneja and Marta Rapado-Castro: Biomedical Research Networking Center for Mental Health Network (CIBERSAM), Barcelona, Spain; Department of Child and Adolescent Psychiatry, Hospital General Universitario Gregorio Marañón, School of Medicine, Institute of Psychiatry and Mental Health, Universidad Complutense, IiSGM, Madrid, Spain. Carlo Alemany and Aina Avila-Parcet: Biomedical Research Networking Center for Mental Health Network (CIBERSAM), Barcelona, Spain; Department of Psychiatry, Hospital de la Santa Creu i Sant Pau, Institut d’Investigació Biomèdica-Sant Pau (IIB-SANT PAU), Universitat Autònoma de Barcelona (UAB), Barcelona, Spain. Iñaki Zorrilla and Itxasco Gonzalez-Ortega: Biomedical Research Networking Center for Mental Health Network (CIBERSAM), Barcelona, Spain; Araba University Hospital, Bioaraba Research Institute, Vitoria-Gasteiz, Spain; University of the Basque Country (UPV-EHU), Vitoria-Gasteiz, Spain. Concepción De-la-Cámara and Pedro Saz: Biomedical Research Networking Center for Mental Health Network (CIBERSAM), Barcelona, Spain; Department of Medicine and Psychiatry, Instituto de Investigación Sanitaria Aragón (IIS Aragón), Zaragoza University, Zaragoza, Spain. Juan Nacher: Biomedical Research Networking Center for Mental Health Network (CIBERSAM), Barcelona, Spain; Neurobiology Unit, Program in Neurosciences and Interdisciplinary Research Structure for Biotechnology and Biomedicine (BIOTECMED), Universitat de València, Biomedical Research Institute INCLIVA, Valencia, Spain. Esther Lorente: Neurobiology Unit, Program in Neurosciences and Interdisciplinary Research Structure for Biotechnology and Biomedicine (BIOTECMED), Universitat de València, Biomedical Research Institute INCLIVA, Valencia, Spain. Teresa Legido: CIBERSAM, IDIBAPS, Department of Medicine, University of Barcelona, Barcelona, Spain. Francesc Casanovas: CIBERSAM, IDIBAPS, Department of Medicine, University of Barcelona, Barcelona, Spain. Nestor Arbelo: Barcelona Clinic Schizophrenia Unit, Hospital Clinic of Barcelona, Neuroscience Institute, August Pi I Sunyer Biomedical Research Institute (IDIBAPS), University of Barcelona, Barcelona, Spain. Lidia Ilzarbe: Department of Psychiatry and Psychology, Institute of Neuroscience, Hospital Clinic de Barcelona, Barcelona, Spain. Josefina Castro-Fornieles: Biomedical Research Networking Center for Mental Health Network (CIBERSAM), Barcelona, Spain; Department of Child and Adolescent Psychiatry and Psychology, 2017SGR881, Hospital Clínic Universitari, Institut Clinic de Neurociències, Barcelona, Spain. Immaculada Baeza: Biomedical Research Networking Center for Mental Health Network (CIBERSAM), Barcelona, Spain; Department of Child and Adolescent Psychiatry and Psychology, 2017SGR881, Hospital Clínic Universitari, Institut Clinic de Neurociències, Barcelona, Spain. Fernando Contreras: Biomedical Research Networking Center for Mental Health Network (CIBERSAM), Barcelona, Spain; Bellvitge University Hospital, IDIBELL, Barcelona, Spain. Teresa Bobes Bascarán: Biomedical Research Networking Center for Mental Health Network (CIBERSAM), Barcelona, Spain; Servicio de Salud del Principado de Asturias (SESPA) Oviedo, Instituto de Investigación Sanitaria del Principado de Asturias (ISPA), Instituto Universitario de Neurociencias del Principado de Asturias (INEUROPA), Oviedo, Spain; Department of Psychology, Universidad de Oviedo, Oviedo, Spain. Leticia González-Blanco: Biomedical Research Networking Center for Mental Health Network (CIBERSAM), Barcelona, Spain; Servicio de Salud del Principado de Asturias (SESPA) Oviedo, Instituto de Investigación Sanitaria del Principado de Asturias (ISPA), Instituto Universitario de Neurociencias del Principado de Asturias (INEUROPA), Oviedo, Spain; Department of Psychiatry, Universidad de Oviedo, Oviedo, Spain. Rafael Segarra Echevarría and Arantzazu Zabala Rabadán: Biomedical Research Networking Center for Mental Health Network (CIBERSAM), Barcelona, Spain; Cruces University Hospital, BioCruces Health Research Institute, University of the Basque Country (UPV/EHU), Vizcaya, Spain. Roberto Rodriguez-Jimenez: Biomedical Research Networking Center for Mental Health Network (CIBERSAM), Barcelona, Spain; Instituto de Investigación Sanitaria Hospital 12 de Octubre (imas12), Madrid, Spain; CogPsy Group, Universidad Complutense de Madrid (UCM), Madrid, Spain. Luis Sanchez-Pastor: Instituto de Investigación Sanitaria Hospital 12 de Octubre (imas12), Madrid, Spain. Judith Usall: Parc Sanitari Sant Joan de Déu, Teaching, Research & Innovation Unit, Institut de Recerca Sant Joan de Déu, Sant Boi de Llobregat. Anna Butjosa: Biomedical Research Networking Center for Mental Health Network (CIBERSAM), Barcelona, Spain; Hospital Infanto-juvenil Sant Joan de Déu, Institut de Recerca Sant Joan de Déu, Esplugues de Llobregat, Barcelona. Salvador Sarró and María Ángeles García León: Biomedical Research Networking Center for Mental Health Network (CIBERSAM), Barcelona, Spain; FIDMAG Germanes Hospitalàries Research Foundation, Barcelona, Spain. Ángela Ibáñez: Biomedical Research Networking Center for Mental Health Network (CIBERSAM), Barcelona, Spain; Department of Psychiatry, Hospital Universitario Ramón y Cajal, IRYCIS, Universidad de Alcalá, Madrid, Spain. Lucía Moreno-Izco: Department of Psychiatry, Complejo Hospitalario de Navarra, Pamplona, Spain; IdiSNA, Navarra Institute for Health Research, Pamplona, Spain. Vicent Balanzá-Martinez: Biomedical Research Networking Center for Mental Health Network (CIBERSAM), Barcelona, Spain; Department of Medicine, University of Valencia, Valencia, Spain.
Author contributions
SA and MS-N designed the study, managed the literature searches and analyses, undertook the statistical analysis, and wrote the first draft of the manuscript. CT and EV revised the first draft and added critical comments to guide the redaction of the final manuscript. NV, MF, AS-T, DC, AL, AG-P, RP, AR, AC, ES, AT, MC, and MB revised the second draft of the article and provided critical comments to guide the redaction of the final manuscript. All authors within the PEPs Group recruited individuals with FEP and healthy controls at their centers, provided the anonymous data and revise the final manuscript and approved the final manuscript.
Funding
This study was funded with the projects PI17/01066 and PI20/00344 by the Instituto de Salud Carlos III and co-funded by the Unión Europea (FEDER) “Una manera de hacer Europa”.
Acknowledgments
We are extremely grateful to all participants. This study is part of a coordinated-multicentre Project, funded by the Ministerio de Economía y Competitividad (PI08/0208; PI11/00325; PI17/01066; PI20/00344; and PI14/00612), Instituto de Salud Carlos III – Fondo Europeo de Desarrollo Regional, Unión Europea, Una manera de hacer Europa, Centro de Investigación Biomédica en Red de salud Mental, CIBERSAM, by the CERCA Programme/Generalitat de Catalunya and Secretaria d’Universitats i Recerca del Departament d’Economia I Coneixement (2017SGR1355). Departament de Salut de la Generalitat de Catalunya, en la convocatoria corresponent a l’any 2017 de Concessió de Subvencions del Pla Estratègic de Recerca i Innovació en Salut (PERIS) 2016–2020, Modalitat Projectes de Recerca Orientats A l’Atenció Primària, Amb el Codi d’Expedient SLT006/17/00345. MB is also grateful for the support of the Institut de Neurociències, Universitat de Barcelona. SA has been supported by a Sara Borrell (CD20/00177), funded by Instituto de Salud Carlos III (ISCIII), and co-funded by European Social Fund “Investing in your future”. NV thanks the BITRECS project, which has received funding from the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie grant agreement No. 754550 and from “La Caixa” Foundation (ID 100010434), under the agreement LCF/PR/GN18/50310006. CT has been supported by a ‘Miguel Servet’ postdoctoral contract (CPI14/00175), and Miguel Servet II contract (CPII19/00018). EV thanks the support of the Spanish Ministry of Science, Innovation and Universities (PI15/00283; PI21/00787) integrated into the Plan Nacional de I + D + I y cofinanciado por el ISCIII-Subdirección General de Evaluación y el Fondo Europeo de Desarrollo Regional (FEDER); CIBERSAM; and the Comissionat per a Universitats i Recerca del DIUE de la Generalitat de Catalunya to the Bipolar Disorders Group (2017 SGR 1365) and the SLT006/17/00357 project, from PERIS 2016-2020 (Departament de Salut). CERCA Programme/Generalitat de Catalunya. A. Ibáñez thanks the support of the Madrid Regional Government and European Union Structural Funds (S2017/BMD3740; AGES-CM 2-CM), and the support of CIBERSAM. We also would like to thank the authors of the PEPs group who participated in the development of this manuscript.
Conflict of interest
EV has received grants and served as consultant, advisor or CME speaker for the following entities (unrelated to the present work): AB-Biotics, Abbott, Allergan, Angelini, Dainippon Sumitomo Pharma, Ferrer, Gedeon Richter, Janssen, Lundbeck, Otsuka, Sage, Sanofi-Aventis, and Takeda. JR-Q was on the speakers’ bureau and/or acted as consultant for Eli-Lilly, Janssen-Cilag, Novartis, Shire, Takeda, Bial, Shionogui, Lundbeck, Almirall, Braingaze, Sincrolab, Medice and Rubió, Raffo in the last 5 years. He also received travel awards (air tickets + hotel) for taking part in psychiatric meetings from Janssen-Cilag, Rubió, Shire, Takeda, Shionogui, Bial, Medice and Eli- Lilly. The Department of Psychiatry chaired by him received unrestricted educational and research support from the following companies in the last 5 years: Eli-Lilly, Lundbeck, Janssen-Cilag, Actelion, Shire, Ferrer, Oryzon, Roche, Psious, and Rubió. MB has been a consultant for, received grant/research support and honoraria from, and been on the speakers/advisory board of ABBiotics, Adamed, Angelini, Casen Recordati, Janssen-Cilag, Menarini, Rovi and Takeda. NV has received financial support for CME activities and travel funds from the following entities (unrelated to the present work): Angelini, Janssen-Cilag, Lundbeck, Otsuka. CDLC received financial support to attend scientific meetings from Janssen, Almirall, Lilly, Lundbeck, Rovi, Esteve, Novartis, Astrazeneca, Pfizer and Casen Recordati. IB has received honoraria or travel support to attend conferences from Angelini, Janssen and Otsuka-Lundbeck; and grants from Instituto de Salud Carlos III, Spanish ministry of Health. LG-B has received honoraria for lecturing and/or travel grants for attending conferences from the Spanish Foundation of Psychiatry and Mental Health, Otsuka, Lundbeck, Janssen-Cilag, Servier, Angelini and Pfizer. NA has received CME-related financing from Janssen-Cilag, Lundbeck, Adamed, Pfizer and Boston Scientific, outside the submitted work. LI has received medical education support from Otsuka-Lundbeck, and training courses support from Otsuka-Lundbeck, Adamed and Janssen. RR-J has been a consultant for, spoken in activities of, or received grants from: Instituto de Salud Carlos III, Fondo de Investigación Sanitaria (FIS), Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM), Madrid Regional Government (S2010/BMD-2422 AGES; S2017/BMD-3740), JanssenCilag, Lundbeck, Otsuka, Pfizer, Ferrer, Juste, Takeda, Exeltis, Casen-Recordati, Angelini. JG-D was partly funded by a grant from Ministerio de Ciencia y Tecnologia – Republica de Colombia (Convocatoria 885/2020) and has been an advisor/speaker for, or received travel support from Janssen, Eurofarma, Servier, Sanofi, Lilly, and Pfizer. AI has received research support from or served as speaker or advisor for Janssen-Cilag, Lundbeck and Otsuka. MR-C is a Ramon y Cajal Research Fellow (RYC-2017-23144), Spanish Ministry of Science, Innovation and Universities and was supported by a NARSAD independent investigator grant (no. 24628) from the Brain and Behavior Research Foundation. MC has received grant support from Instituto de Salud Carlos III, Spanish Ministry of Science and Innovation (PI18/00753, PI21/00701) and the Alicia Koplowitz Foundation. CMD-C has received grant support from Instituto de Salud Carlos III, Spanish Ministry of Science and Innovation (PI17/00481, PI20/00721, JR19/0024) and honoraria from Exeltis and Angelini.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.982583/full#supplementary-material
References
1. Amoretti S, Rosa AR, Mezquida G, Cabrera B, Ribeiro M, Molina M, et al. The impact of cognitive reserve, cognition and clinical symptoms on psychosocial functioning in first-episode psychoses. Psychol Med. (2020) 52:526–37. doi: 10.1017/S0033291720002226
2. Ayesa-Arriola R, Manuel Rodríguez-Sánchez J, Pérez-Iglesias R, González-Blanch C, Pardo-García G, Tabares-Seisdedos R, et al. The relevance of cognitive, clinical and premorbid variables in predicting functional outcome for individuals with first-episode psychosis: A 3 year longitudinal study. Psychiatry Res. (2013) 209:302–8. doi: 10.1016/j.psychres.2013.01.024
3. Lally J, Ajnakina O, Stubbs B, Cullinane M, Murphy KC, Gaughran F, et al. Remission and recovery from first-episode psychosis in adults: Systematic review and meta-analysis of long-term outcome studies. Br J Psychiatry. (2017) 211:350–8. doi: 10.1192/bjp.bp.117.201475
4. Lepage M, Bodnar M, Raucher-Chéné D, Lavigne KM, Makowski C, Joober R, et al. Neurocognitive functions in persistent negative symptoms following a first episode of psychosis. Eur Neuropsychopharmacol. (2021) 47:86–97. doi: 10.1016/j.euroneuro.2021.02.008
5. Mezquida G, Cabrera B, Bioque M, Amoretti S, Lobo A, González-Pinto A, et al. The course of negative symptoms in first-episode schizophrenia and its predictors: A prospective two-year follow-up study. Schizophr Res. (2017) 189:84–90. doi: 10.1016/j.schres.2017.01.047
6. Fraguas D, Del Rey-Mejías A, Moreno C, Castro-Fornieles J, Graell M, Otero S, et al. Duration of untreated psychosis predicts functional and clinical outcome in children and adolescents with first-episode psychosis: A 2-year longitudinal study. Schizophr Res. (2014) 152:130–8. doi: 10.1016/j.schres.2013.11.018
7. Amoretti S, Ramos-Quiroga JA. Cognitive reserve in mental disorders. Eur Neuropsychopharmacol. (2021) 49:113–5. doi: 10.1016/j.euroneuro.2021.04.011
8. Verdolini N, Amoretti S, Mezquida G, Cuesta MJ, Pina-Camacho L, García-Rizo C, et al. The effect of family environment and psychiatric family history on psychosocial functioning in first-episode psychosis at baseline and after 2 years. Eur Neuropsychopharmacol. (2021) 49:54–68. doi: 10.1016/j.euroneuro.2021.03.015
9. Stern Y. What is cognitive reserve? Theory and research application of the reserve concept. J Int Neuropsychol Soc. (2002) 8:448–60. doi: 10.1017/S1355617702813248
10. Amoretti S, Bernardo M, Bonnin CM, Bioque M, Cabrera B, Mezquida G, et al. The impact of cognitive reserve in the outcome of first-episode psychoses: 2-year follow-up study. Eur Neuropsychopharmacol. (2016) 26:1638–16348. doi: 10.1016/j.euroneuro.2016.07.003
11. Amoretti S, Cabrera B, Torrent C, Bonnín CDM, Mezquida G, Garriga M, et al. Cognitive reserve assessment scale in health (CRASH): Its validity and reliability. J Clin Med. (2019) 8:586. doi: 10.3390/jcm8050586
12. de la Serna E, Montejo L, Solé B, Castro-Fornieles J, Camprodon-Boadas P, Sugranyes G, et al. Effectiveness of enhancing cognitive reserve in children, adolescents and young adults at genetic risk for psychosis: Study protocol for a randomized controlled trial. Rev Psiquiatr Salud Ment. (2021) S1888–9891:00029–X. doi: 10.1016/j.rpsm.2021.02.003
13. Li AWY, Hui CLM, Lee EHM, Chang WC, Chan SKW, Chen EYH. Gender differences in correlates of cognition in first-episode psychosis. Psychiatry Res. (2019) 271:412–20. doi: 10.1016/j.psychres.2018.12.011
14. Ochoa S, Usall J, Cobo J, Labad X, Kulkarni J. Gender differences in schizophrenia and first-episode psychosis: A comprehensive literature review. Schizophr Res Treatment. (2012) 2012:1–9. doi: 10.1155/2012/916198
15. Thorup A, Petersen L, Jeppesen P, Ohlenschlæger J, Christensen T, Krarup G, et al. Gender differences in young adults with first-episode schizophrenia spectrum disorders at baseline in the Danish OPUS study. J Nerv Ment Dis. (2007) 195:396–405. doi: 10.1097/01.nmd.0000253784.59708.dd
16. Hall MH, Holton KM, Öngür D, Montrose D, Keshavan MS. Longitudinal trajectory of early functional recovery in patients with first episode psychosis. Schizophr Res. (2019) 209:234–44. doi: 10.1016/j.schres.2019.02.003
17. Riel H, Lee JB, Fisher DJ, Tibbo PG. Sex differences in event-related potential (ERP) waveforms of primary psychotic disorders: A systematic review. Int J Psychophysiol. (2019) 145:119–24. doi: 10.1016/j.ijpsycho.2019.02.006
18. Riecher-Rössler A, Butler S, Kulkarni J. Sex and gender differences in schizophrenic psychoses-a critical review. Arch Womens Ment Health. (2018) 21:627–48. doi: 10.1007/s00737-018-0847-9
19. Guma E, Devenyi GA, Malla A, Shah J, Chakravarty MM, Pruessner M. Neuroanatomical and symptomatic sex differences in individuals at clinical high risk for psychosis. Front psychiatry. (2017) 8:291. doi: 10.3389/fpsyt.2017.00291
20. Mendrek A, Mancini-Marïe A. Sex/gender differences in the brain and cognition in schizophrenia. Neurosci Biobehav Rev. (2016) 67:57–78. doi: 10.1016/j.neubiorev.2015.10.013
21. Li R, Ma X, Wang G, Yang J, Wang C. Why sex differences in schizophrenia? J Transl Neurosci. (2016) 1:37–42.
22. Lewine RRJ, Thurston-Snoha B-J, Ardery R. Sex, gender, and neuropsychological functioning in schizophrenia. J Clin Exp Neuropsychol. (2006) 28:1362–72. doi: 10.1080/13803390500473738
23. Ayesa-Arriola R, de la Foz VOG, Setién-Suero E, Ramírez-Bonilla ML, Suárez-Pinilla P, van Son JM, et al. Understanding sex differences in long-term outcomes after a first episode of psychosis. npj Schizophr. (2020) 6:1–8. doi: 10.1038/s41537-020-00120-5
24. Mattsson M, Flyckt L, Edman G, Nyman H, Cullberg J, Forsell Y. Gender differences in the prediction of 5-year outcome in first episode psychosis. Int J Methods Psychiatr Res. (2007) 16:208–18. doi: 10.1002/mpr.228
25. Pu C, Qiu Y, Zhou T, Yang F, Lu Z, Wang C, et al. Gender differences of neurocognitive functioning in patients with first-episode schizophrenia in China. Compr Psychiatry. (2019) 95:152132. doi: 10.1016/j.comppsych.2019.152132
26. Cocchi A, Lora A, Meneghelli A, La Greca E, Pisano A, Cascio MT, et al. Sex differences in first-episode psychosis and in people at ultra-high risk. Psychiatry Res. (2014) 215:314–22. doi: 10.1016/j.psychres.2013.11.023
27. Danaher H, Allott K, Killackey E, Hester R, Cotton S. An examination of sex differences in neurocognition and social cognition in first-episode psychosis. Psychiatry Res. (2018) 259:36–43. doi: 10.1016/j.psychres.2017.09.053
28. Willhite RK, Niendam TA, Bearden CE, Zinberg J, O’Brien MP, Cannon TD. Gender differences in symptoms, functioning and social support in patients at ultra-high risk for developing a psychotic disorder. Schizophr Res. (2008) 104:237–45. doi: 10.1016/j.schres.2008.05.019
29. McEwen BS, Milner TA. Understanding the broad influence of sex hormones and sex differences in the brain. J Neurosci Res. (2017) 95:24–39. doi: 10.1002/jnr.23809
30. Kaneda Y, Ohmori T. Relation between estradiol and negative symptoms in men with schizophrenia. J Neuropsychiatry Clin Neurosci. (2005) 17:239–42. doi: 10.1176/jnp.17.2.239
31. Goldstein JM, Cherkerzian S, Seidman LJ, Petryshen TL, Fitzmaurice G, Tsuang MT, et al. Sex-specific rates of transmission of psychosis in the New England high-risk family study. Schizophr Res. (2011) 128:150–5. doi: 10.1016/j.schres.2011.01.019
32. Bernardo M, Bioque M, Parellada M, Ruiz JS, Cuesta MJ, Llerena A, et al. Assessing clinical and functional outcomes in a gene–environment interaction study in first episode of psychosis (PEPs). Rev Psiquiatr Salud Ment. (2013) 6:4–16. doi: 10.1016/j.rpsmen.2012.11.001
33. Bernardo M, Cabrera B, Arango C, Bioque M, Castro-Fornieles J, Cuesta MJ, et al. One decade of the first episodes project (PEPs): Advancing towards a precision psychiatry. Rev Psiquiatr Salud Ment. (2019) 12:135–40. doi: 10.1016/j.rpsm.2019.03.001
34. Salagre E, Arango C, Artigas F, Ayuso-Mateos JL, Bernardo M, Castro-Fornieles J, et al. CIBERSAM: Ten years of collaborative translational research in mental disorders. Rev Psiquiatr Salud Ment. (2019) 12:1–8. doi: 10.1016/j.rpsmen.2018.10.001
35. Hollingshead AB, Redlich FC. Social class and mental illness. New York, NY: Wiley (1958). doi: 10.1037/10645-000
36. Gardner DM, Murphy AL, O’Donnell H, Centorrino F, Baldessarini RJ. International consensus study of antipsychotic dosing. Am J Psychiatry. (2010) 167:686–93. doi: 10.1176/appi.ajp.2009.09060802
37. Kokkevi A, Hartgers C. EuropASI: European adaptation of a multidimensional assessment instrument for drug and alcohol dependence. Eur Addict Res. (1995) 1:208–10. doi: 10.1159/000259089
38. First M, Spitzer R, Gibbon M, Williams JBW, Benjamin LS. Structured Clinical Interview for DSM IV Axis I Disorder, Research Version. New York, NY: Biometrics Research (1997).
39. First MB, Gibbon M, Spitzer RL, Williams JBW, Benjamin LS. Structured clinical interview for DSM-IV® axis ii personality disorders SCID-II. Washington, DC: American Psychiatric Association (1997).
40. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. (1987) 13:261–76. doi: 10.1093/schbul/13.2.261
41. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. (1979) 134:382–9. doi: 10.1192/bjp.134.4.382
42. Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale for mania. Br J Psychiatry. (1978) 133:429–35. doi: 10.1192/bjp.133.5.429
43. Amoretti S, Mezquida G, Rosa AR, Bioque M, Cuesta MJ, Pina-Camacho L, et al. The functioning assessment short test (FAST) applied to first-episode psychosis: Psychometric properties and severity thresholds. Eur Neuropsychopharmacol. (2021) 47:98–111. doi: 10.1016/j.euroneuro.2021.02.007
44. Rosa AR, Sánchez-Moreno J, Martínez-Aran A, Salamero M, Torrent C, Reinares M, et al. Validity and reliability of the Functioning Assessment Short Test (FAST) in bipolar disorder. Clin Pract Epidemiol Ment Health. (2007) 3:5. doi: 10.1186/1745-0179-3-5
45. Conners CK. Conners’ continuous performance test II. Tonawanda, NY: Multi-Health System Inc (2004).
47. Weschler D. Wechsler adult intelligence scale-III (WAIS-III). San Antonio, TX: Psychological Association (1997).
48. Reitan RM, Wolfson D. Category Test and Trail Making Test as measures of frontal lobe functions. Clin Neuropsychol. (1995) 9:50–6. doi: 10.1080/13854049508402057
49. Heaton R. Wisconsin card sorting test manual. Odessa, FL: Psychological Assessment Resources (1993).
51. Loonstra AS, Tarlow AR, Sellers AH. COWAT metanorms across age, education, and gender. Appl Neuropsychol. (2001) 8:161–6. doi: 10.1207/S15324826AN0803_5
52. Mayer JD, Salovey P, Caruso DR, Sitarenios G. Measuring emotional intelligence with the MSCEIT V2.0. Emotion. (2003) 3:97. doi: 10.1037/1528-3542.3.1.97
53. Cannon-Spoor HE, Potkin SG, Wyatt RJ. Measurement of premorbid adjustment in chronic schizophrenia. Schizophr Bull. (1982) 8:470–84. doi: 10.1093/schbul/8.3.470
54. Amoretti S, Cabrera B, Torrent C, Mezquida G, Lobo A, González-Pinto A, et al. Cognitive reserve as an outcome predictor: First-episode affective versus non-affective psychosis. Acta Psychiatr Scand. (2018) 138:441–55. doi: 10.1111/acps.12949
55. Anaya C, Torrent C, Caballero FF, Vieta E, Bonnin Cdel M, Ayuso-Mateos JL, et al. Cognitive reserve in bipolar disorder: Relation to cognition, psychosocial functioning and quality of life. Acta Psychiatr Scand. (2016) 133:386–98. doi: 10.1111/acps.12535
56. de la Serna E, Andrés-Perpiñá S, Puig O, Baeza I, Bombin I, Bartrés-Faz D, et al. Cognitive reserve as a predictor of two year neuropsychological performance in early onset first-episode schizophrenia. Schizophr Res. (2013) 143:125–31. doi: 10.1016/j.schres.2012.10.026
57. De Oliveira MO, Nitrini R, Yassuda MS, Brucki SMD. Vocabulary is an appropriate measure of premorbid intelligence in a sample with heterogeneous educational level in Brazil. Behav Neurol. (2014) 2014:875960. doi: 10.1155/2014/875960
58. Duff K. Evidence-based indicators of neuropsychological change in the individual patient: Relevant concepts and methods. Arch Clin Neuropsychol. (2012) 27:248–61. doi: 10.1093/arclin/acr120
59. Barbu RM, Berard JA, Gresham LM, Walker LAS. Longitudinal stability of cognition in early-phase relapsing-remitting multiple sclerosis: Does cognitive reserve play a role? Int J MS Care. (2018) 20:173–9. doi: 10.7224/1537-2073.2016-073
60. Barker-Collo SL, Purdy SC. Determining the presence of reliable change over time in multiple sclerosis: Evidence from the PASAT, adjusting-PSAT, and stroop test. Int J MS Care. (2013) 15:170–8. doi: 10.7224/1537-2073.2013-007
61. Vila-Badia R, Del Cacho N, Butjosa A, Ochoa S, Serra-Arumí C, Esteban-Sanjusto M, et al. Cognitive functioning in first episode psychosis. Gender differences and relation with clinical variables. Early Interv Psychiatry. (2021) 15:1667–76. doi: 10.1111/eip.13110
62. Navarra-Ventura G, Vicent-Gil M, Serra-Blasco M, Massons C, Crosas JM, Cobo J, et al. Group and sex differences in social cognition in bipolar disorder, schizophrenia/schizoaffective disorder and healthy people. Compr Psychiatry. (2021) 109:152258. doi: 10.1016/j.comppsych.2021.152258
63. Choi JS, Chon MW, Kang DH, Jung MH, Kwon JS. Gender difference in the prodromal symptoms of first-episode Schizophrenia. J Korean Med Sci. (2009) 24:1083–8. doi: 10.3346/jkms.2009.24.6.1083
64. Cotton SM, Lambert M, Schimmelmann BG, Foley DL, Morley KI, McGorry PD, et al. Gender differences in premorbid, entry, treatment, and outcome characteristics in a treated epidemiological sample of 661 patients with first episode psychosis. Schizophr Res. (2009) 114:17–24. doi: 10.1016/j.schres.2009.07.002
65. González-Rodríguez A, Studerus E, Spitz A, Bugra H, Aston J, Borgwardt S, et al. Gender Differences in the Psychopathology of Emerging Psychosis. Isr J Psychiatry Relat Sci. (2014) 51:85–92.
66. Hui CLM, Leung CM, Chang WC, Chan SKW, Lee EHM, Chen EYH. Examining gender difference in adult-onset psychosis in Hong Kong. Early Interv Psychiatry. (2016) 10:324–33. doi: 10.1111/eip.12167
67. Lahera G, Ruiz A, Brañas A, Vicens M, Orozco A. Reaction time, processing speed and sustained attention in schizophrenia: Impact on social functioning. Rev Psiquiatr Salud Ment. (2017) 10:197–205. doi: 10.1016/j.rpsmen.2017.10.006
68. Zanelli J, Morgan K, Dazzan P, Morgan C, Russo M, Pilecka I, et al. Gender differences in neuropsychological performance across psychotic disorders – a multi-centre population based case-control study. PLoS One. (2013) 8:1–8. doi: 10.1371/journal.pone.0077318
69. Roivainen E. Gender differences in processing speed: A review of recent research. Learn Individ Dif. (2011) 21:145–9. doi: 10.1016/j.lindif.2010.11.021
70. Giambra LM, Quilter RE. Sex differences in sustained attention across the adult life Span. J Appl Psychol. (1989) 74:91–5. doi: 10.1037/0021-9010.74.1.91
71. Hsieh PC, Chu CL, Yang YK, Yang YC, Yeh TL, Lee IH, et al. Norms of performance of sustained attention among a community sample: Continuous performance test study. Psychiatry Clin Neurosci. (2005) 59:170–6. doi: 10.1111/j.1440-1819.2005.01353.x
72. Austin SF, Mors O, Budtz-Jørgensen E, Secher RG, Hjorthøj CR, Bertelsen M, et al. Long-term trajectories of positive and negative symptoms in first episode psychosis: A 10year follow-up study in the OPUS cohort. Schizophr Res. (2015) 168:84–91. doi: 10.1016/j.schres.2015.07.021
73. Stefanopoulou E, Lafuente AR, Fonseca AS, Keegan S, Vishnick C, Huxley A. Global assessment of psychosocial functioning and predictors of outcome in schizophrenia. Int J Psychiatry Clin Pract. (2011) 15:62–8. doi: 10.3109/13651501.2010.519035
74. Camprodon-Boadas P, de la Serna E, Baeza I, Puig O, Ilzarbe D, Sugranyes G, et al. Cognitive reserve in patients with first-episode psychosis as outcome predictor at 5-year follow-up. Eur Child Adolesc Psychiatry. (2021) 30:1959–67. doi: 10.1007/s00787-020-01668-4
75. Lindgren M, Birling H, Kieseppä T, Tuulio-Henriksson A. Is cognitive performance associated with anxiety and depression in first-episode psychosis? J Affect Disord. (2020) 263:221–7. doi: 10.1016/j.jad.2019.11.161
76. Milev P, Ho B-C, Arndt S, Andreasen NC. Predictive values of neurocognition and negative symptoms on functional outcome in schizophrenia: A longitudinal first-episode study with 7-year follow-up. Am J Psychiatry. (2005) 162:495–506. doi: 10.1176/appi.ajp.162.3.495
77. Sawada K, Kanehara A, Sakakibara E, Eguchi S, Tada M, Satomura Y, et al. Identifying neurocognitive markers for outcome prediction of global functioning in individuals with first-episode and ultra-high-risk for psychosis. Psychiatry Clin Neurosci. (2017) 71:318–27. doi: 10.1111/pcn.12522
78. Cowman M, Holleran L, Lonergan E, O’Connor K, Birchwood M, Donohoe G. Cognitive predictors of social and occupational functioning in early psychosis: A systematic review and meta-analysis of cross-sectional and longitudinal data. Schizophr Bull. (2021) 47:1243–53. doi: 10.1093/schbul/sbab033
79. Kirkpatrick B, Strauss GP, Nguyen L, Fischer BA, Daniel DG, Cienfuegos A, et al. The brief negative symptom scale: Psychometric properties. Schizophr Bull. (2011) 37:300–5. doi: 10.1093/schbul/sbq059
Keywords: first episode non-affective psychosis, psychosocial functioning, sex differences, cognition, negative symptoms
Citation: Serra-Navarro M, Amoretti S, Verdolini N, Forte MF, Sánchez-Torres AM, Vieta E, Clougher D, Lobo A, González-Pinto A, Panadero R, Roldán A, Carvalho AF, de la Serna E, Toll A, Ramos-Quiroga JA, Torrent C, Cuesta MJ, Bernardo M and PEPs Group (2022) Influence of clinical and neurocognitive factors in psychosocial functioning after a first episode non-affective psychosis: differences between males and females. Front. Psychiatry 13:982583. doi: 10.3389/fpsyt.2022.982583
Received: 30 June 2022; Accepted: 28 September 2022;
Published: 20 October 2022.
Edited by:
Wing Chung Chang, The University of Hong Kong, Hong Kong SAR, ChinaReviewed by:
Ellie Brown, The University of Melbourne, AustraliaErnest Marek Tyburski, Pomeranian Medical University in Szczecin, Poland
Copyright © 2022 Serra-Navarro, Amoretti, Verdolini, Forte, Sánchez-Torres, Vieta, Clougher, Lobo, González-Pinto, Panadero, Roldán, Carvalho, de la Serna, Toll, Ramos-Quiroga, Torrent, Cuesta, Bernardo and PEPs Group. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eduard Vieta, evieta@clinic.cat; Carla Torrent, ctorrent@clinic.cat
†These authors share first authorship