 Hui Jan Tan1*
Hui Jan Tan1* Abdool Alleem Hj Shahren1
Abdool Alleem Hj Shahren1 Ching Soong Khoo1
Ching Soong Khoo1 Chen Fei Ng1
Chen Fei Ng1 Wan Asyraf Wan Zaidi1
Wan Asyraf Wan Zaidi1 Najma Kori1
Najma Kori1 Petrick Periyasamy1
Petrick Periyasamy1 Choon Leng Eu2†
Choon Leng Eu2† Alvin Oliver Payus3
Alvin Oliver Payus3 Rozita Hod4
Rozita Hod4- 1Department of Medicine, Faculty of Medicine, The National University of Malaysia, Kuala Lumpur, Malaysia
- 2Department of Psychiatry, Faculty of Medicine, The National University of Malaysia, Kuala Lumpur, Malaysia
- 3Department of Medicine, Faculty of Medicine, University Malaysia Sabah, Kota Kinabalu, Malaysia
- 4Department of Community Health, Faculty of Medicine, The National University of Malaysia, Kuala Lumpur, Malaysia
Introduction: Anxiety has been increasingly recognized as part of the psychosocial health issues in COVID-19 patients. However, the impact of this topic may be underestimated in low- and middle-income countries. This study aimed to estimate the prevalence of and risk factors of anxiety in COVID-19 patients compared to controls in a local tertiary teaching hospital in Malaysia.
Methods: In this case–control study, we analyzed data on adult patients aged 18 years and above hospitalized for COVID-19 infection with matched hospitalized controls. The demographic, clinical data and anxiety measures using the Generalized Anxiety Disorder-7 questionnaire were analyzed using univariate and multivariate analysis.
Results: 86.6% in the COVID-19 group had anxiety, significantly higher than 13.4% in the control group (p = 0.001). The COVID-19 group was significantly associated with the GAD-7 severity (p = 0.001). The number of COVID-19 patients in the mild, moderate, and severe anxiety groups was 48 (84.2%), 37 (86%), and 18 (94.7%), respectively. Multiple logistic regression showed significant predictors for anxiety, including COVID-19 diagnosis and neurological symptoms. Anxiety was found 36.92 times higher in the patients with COVID-19 compared to those without COVID-19 (OR 36.92;95% CI 17.09, 79.78, p = 0.001). Patients with neurological symptoms were at risk of having anxiety (OR 2.94; 95% CI 1.03, 8.41, p = 0.044).
Discussion: COVID-19 patients experience a significant disruption in psychosocial functioning due to hospitalization. The burden of anxiety is notably high, compounded by a diagnosis of COVID-19 itself and neurological symptomatology. Early psychiatric referrals are warranted for patients at risk of developing anxiety symptoms.
1. Introduction
There has been a growing recognition of neuropsychiatric manifestations since the declaration of the COVID-19 pandemic. The two most prevalent disabling mental disorders were depressive and anxiety disorders. A meta-analysis of mental health burden following the impact of COVID-19 showed that the prevalence of anxiety was 27.77% (CI: 24.47–31.32) (1). Previous studies have reported prevalence rates of anxiety between 18.6% (2) –34.72% (3). Hospitalized COVID-19 patients invariably have high anxiety levels from multifactorial etiology. This has been reflected following high anxiety levels in hospitalized COVID-19 patients in Turkey (4) and Iran (5). Anxiety is associated with specific stressors in hospitalized patients, which the additional burden of COVID-19 may further compound. Factors such as uncertainty, the inadequacy of explanation, isolation from family, physical effects of the illness, and financial worries may cause formidable barriers in this vulnerable group.
The South East Asia region had recorded 57 million confirmed cases and more than half a million deaths from COVID-19 infections (6). Malaysia had reported approximately 30,000 deaths by December 2021 (7). The impact of COVID-19 has not only resulted in a financial burden but also caused a sharp rise in psychological disorders in the population. Previous studies in Malaysia have focused on specific groups: healthcare workers (8, 9), children with autism (10), women (11), general population (12), urban and rural communities (13) and university students (14). There is a paucity of literature that compared anxiety levels between COVID-19 patients and other hospitalized medical patients, especially from this region.
Determining variables associated with anxiety in COVID-19 patients may be impeded by several issues, such as coexisting medical illnesses, clinical features, the severity and complications of the disease, and the duration of hospitalization or quarantine period. However, it is crucial to determine factors associated with developing anxiety so that we can address them earlier. This knowledge gap remains problematic as it is more challenging to perform studies in hospitalized COVID-19 patients who may also suffer from complications of the disease and its psychological effects. To address this gap, we embark on this study to determine the prevalence and risk factors of anxiety in COVID-19 patients compared to non-COVID-19 patients as controls in a tertiary teaching hospital in Malaysia.
2. Materials and methods
2.1. Study design and study population
This case–control study was conducted between 1 June 2021 and 31 December 2022 at Hospital Canselor Tuanku Muhriz, National University of Malaysia. This tertiary teaching hospital has received COVID-19 cases since the pandemic began in 2020.
The study population was recruited via simple random sampling and patients had to fulfill the following criteria: (1) Patients more than 18 years old with a diagnosis of COVID-19 via qualitative reverse transcription polymerase chain reaction (RT-PCR) from nasopharyngeal and/or oropharyngeal swab, and (2) Hospitalized patients. The controls were matched to the cases by gender and age. They were hospitalized patients in the medical wards due to other medical conditions apart from COVID-19 infection.
2.2. Data collection
Upon admission, consent was taken from the patients or the next of kin/caregivers. The patients/caregivers were given a set of questions to be answered on a virtual questionnaire according to their suited language (English and Bahasa Malaysia). The clinical and laboratory investigation data were further collated.
2.3. Ethical statement
This study was conducted following the guidelines in the Declaration of Helsinki and was approved by the Ethics and Research Board of the Faculty of Medicine, the National University of Malaysia FF-2021-379.
2.4. Questionnaire sections
2.4.1. Demographic variables
This section explored demographic and occupational characteristics. The demographic variables included age, gender, marital status, occupation, habits (smoking and alcohol), and education level.
2.4.2. Clinical variables
The second section explored the clinical characteristics of comorbidities, presenting symptoms, and laboratory parameters. The presenting symptoms were divided into respiratory symptoms (fever, runny nose, sore throat, shortness of breath, and cough), gastrointestinal symptoms (diarrhea, vomiting, abdominal pain, and poor oral intake), neurological symptoms (seizures, limb weakness, headache, and dizziness), and musculoskeletal symptoms (muscle and joint pains). The severity of patients with COVID-19 was divided to five clinical categories according to our local guidelines (15): 1—asymptomatic, 2—symptomatic, 3—evidence of pneumonia, 4—oxygen supplement requirement, and 5—intubated and/or multiorgan failure. In addition, the laboratory data were retrieved from the hospital’s data management system.
2.4.3. Anxiety variable
The third section consists of the study instrument which was a questionnaire on General Anxiety Disorder-7 (GAD-7) in English (16) and the validated Bahasa Malaysia version (17). The patients had the alternative to answer in English or the Bahasa Malaysia version. The GAD-7 questionnaire is a 7-item, self-reporting anxiety questionnaire designed to evaluate mental health symptoms. The questionnaire inquires about the degree to which the patient has been bothered by feeling nervous, anxious, on edge; not being able to stop or control worrying; worrying too much about different things; having trouble relaxing; being so restless that it is hard to sit still; becoming easily annoyed or irritable; and feeling afraid as if something awful might happen. This scale consists of 7 questions responded on a four-point Likert scale ranging from 0 (not at all), 1 (several days), 2 (more than half the days) to 3 (nearly every day). GAD-7 total score for the seven items ranged from 0 to 21. A total score of 0–4 indicates minimal anxiety, 5–9 indicates mild anxiety, 10–14 indicates moderate anxiety, and 15–21 indicates severe anxiety. The GAD-7 is a valid and efficient tool for screening for GAD and assessing its severity in clinical practice and research with 89% sensitivity and 82% specificity. Previous studies that employed similar tools showed a prevalence rate of 17.9–22.6% for GAD during the COVID-19 outbreak (18, 19).
2.5. Statistical analysis
Data were analyzed using the software SPSS Statistic for Windows, version 25. Data normality was evaluated using one-sample Kolmogorov–Smirnov presented as median ± interquartile range for skewed data and frequency (percentage) for nominal data. The demographic factors and clinical characteristics (categorical variables) were analyzed using the Chi-square test. The variables were divided into demographic, clinical (clinical characteristics and laboratory investigations), and anxiety variables. The multivariate logistic regression analysis was performed by including the variables with a value of p less than 0.05 from the simple logistic regression analysis.
3. Results
3.1. Demographic variables
The distribution of the demographic characteristics is shown in Table 1. Of the 223 patients, 118 were COVID-19 positive, and 105 were in the control group. Overall, the median (IQR) age of the COVID-19 and control groups was 54 (40.75, 65) years and 56 (37.50, 68) years, respectively (p = 0.975; Table 2). There was no significant difference in patients’ age, gender, marital status, race, habits, and education level. Only the employment status was significantly different between both groups, where the number of those who were employed in the COVID-19 group was higher (57, 67.1%) compared to the control group (28, 32.9%; p = 0.001). The median (IQR) length of hospitalization was significantly higher in the COVID-19 group, 12 (8.00, 20.25) compared to the control group, 10 (5.00, 17.50; p = 0.032; Table 2).
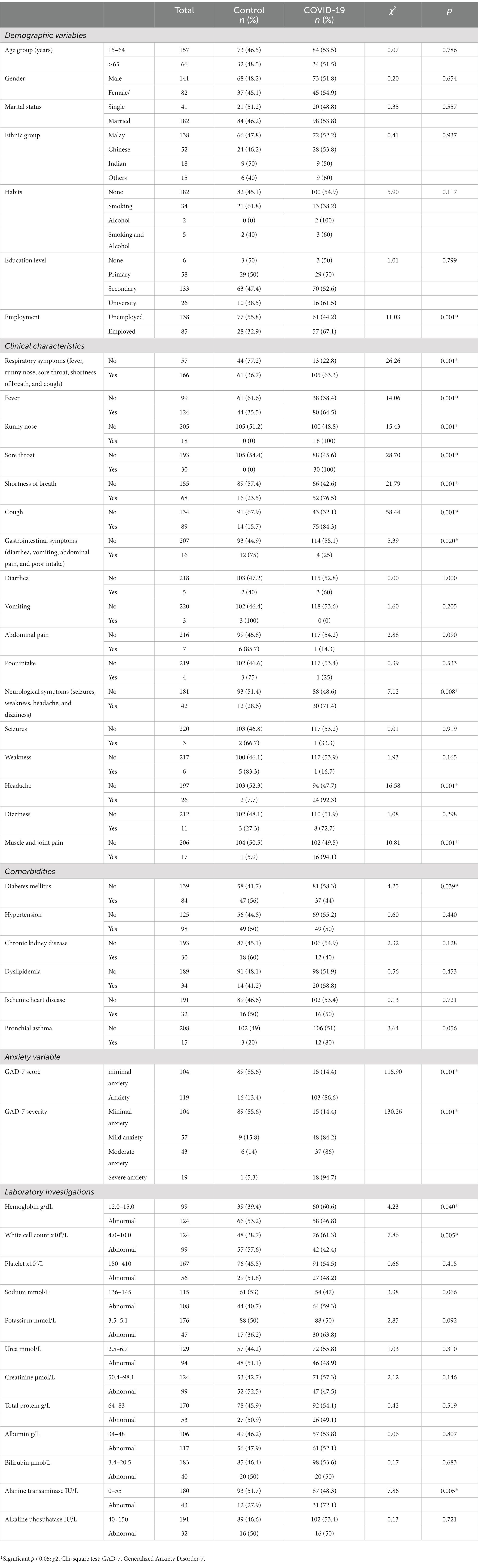
Table 1. Demographic, clinical characteristics, GAD-7 score, and laboratory investigations of the study population and controls.
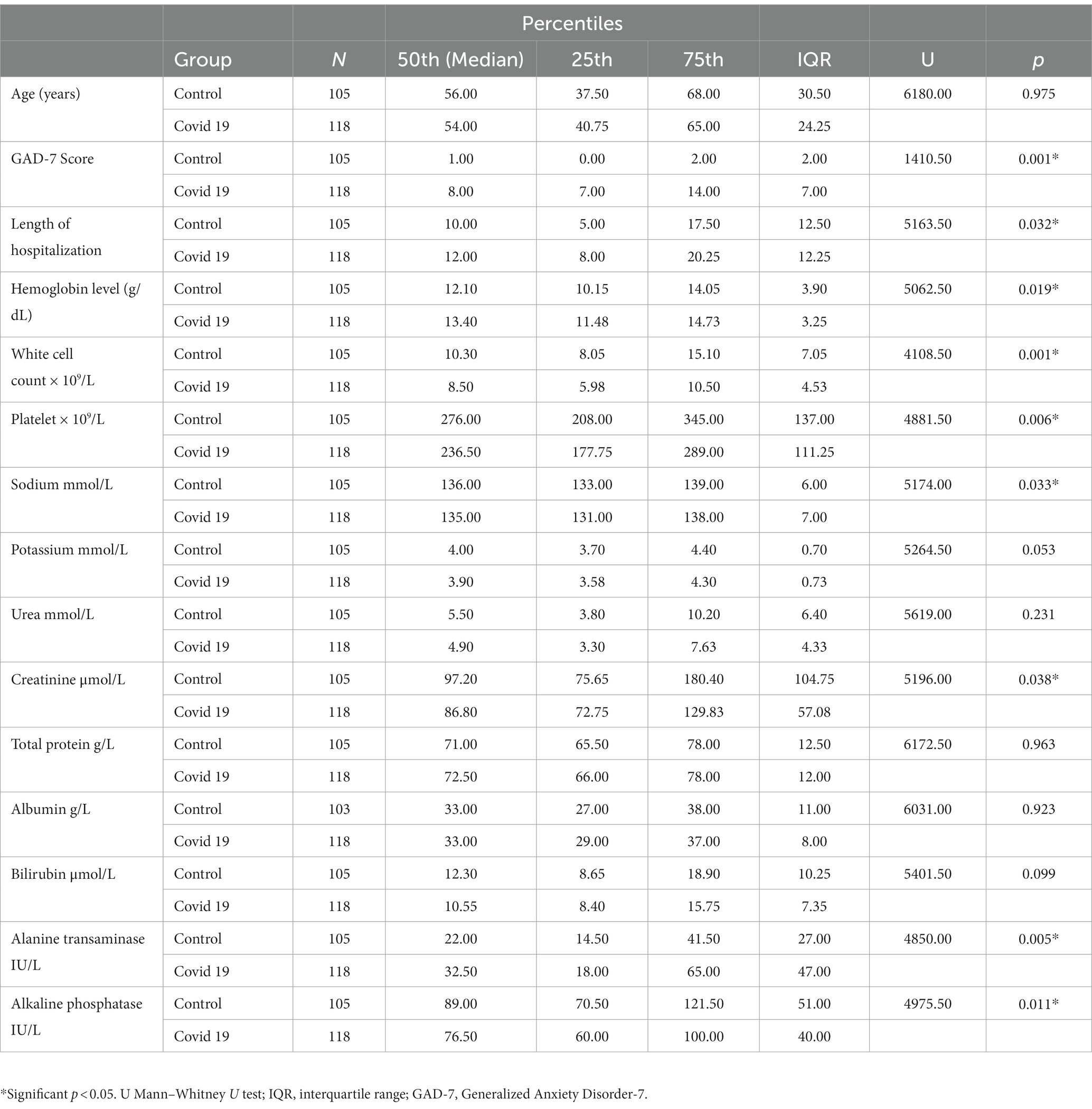
Table 2. Comparison of the variables between the study population and controls.
3.2. Clinical variable
In terms of the clinical parameters, there were more patients in the COVID-19 group with respiratory symptoms (p = 0.001), gastrointestinal symptoms (p = 0.02), neurological symptoms (p = 0.008), and musculoskeletal symptoms (muscle and joint pain; p = 0.001) compared to controls.
3.3. Anxiety variable
The median (IQR) GAD score was significantly higher in the COVID-19 group, 8 (7,14) compared to the control group, 1 (0,2; p = 0.001). The proportion of the COVID-19 group who had anxiety was significantly higher (103, 86.6%) compared to the control group (16,13.4%; p = 0.001). The COVID-19 group had a significant association with the GAD-7 severity (p = 0.001). The number of COVID-19 patients in the mild, moderate, and severe anxiety groups was 48 (84.2%), 37 (86%), and 18 (94.7%), respectively. In comparison, the proportion of the control group who were in the mild, moderate, and severe categories were 9 (15.8%), 6 (14%), and 1 (5.3%), respectively.
In the laboratory parameters, the COVID-19 group had a significant association with hemoglobin (p = 0.04), white cell count levels (p = 0.005), and alanine transaminase level (p = 0.005; Table 1).
Table 3 shows the association between the variables and anxiety. Among the demographic factors, only employment (p = 0.001) and COVID-19 (p = 0.001) diagnoses had a significant association with anxiety. Those employed in the COVID-19 group were higher (57, 67.1%) compared to the control group (15, 12.7%). The proportion of COVID-19 patients with anxiety was higher (103, 87.3%) than the control group (15, 12.7%).

Table 3. Distribution of the demographic, clinical characteristics, and laboratory investigations of the study population with anxiety.
The proportion of COVID-19 patients with anxiety was higher (103, 87.3%) compared to the control group (15, 12.7%; p = 0.001). Among the COVID-19 categories, category 3 had the highest proportion of patients (24, 92.3%) with anxiety (p = 0.001). The clinical symptoms that had a significant association with anxiety were respiratory symptoms (p = 0.001), neurological symptoms (p = 0.001), and musculoskeletal symptoms (p = 0.003). Among the investigations, only sodium level was associated with anxiety, where the number of COVID-19 patients with low sodium levels was 65(60.2%) compared to 43 (47.6%) in the control group (p = 0.048).
3.4. Risk factors for anxiety
Results of the univariate and multiple logistic regression analysis are shown in Table 4. In the univariate analysis, several factors showed significance for anxiety. These factors include the presence of diagnosis, employment, diabetes mellitus, respiratory symptoms, neurological symptoms, gastrointestinal symptoms, and musculoskeletal symptoms (p < 0.05). Further analysis by multiple logistic regression showed significant predictors for anxiety, including COVID-19 diagnosis and neurological symptoms. The diagnosis of COVID-19 was more likely to have anxiety compared to non-COVID-19 diseases (OR 36.92; 95% CI 17.09, 79.78, p = 0.001). We also found that patients with neurological symptoms were 2.94 times likely to have anxiety (OR 2.94; 95% CI 1.03, 8.41, p = 0.044; Table 4).
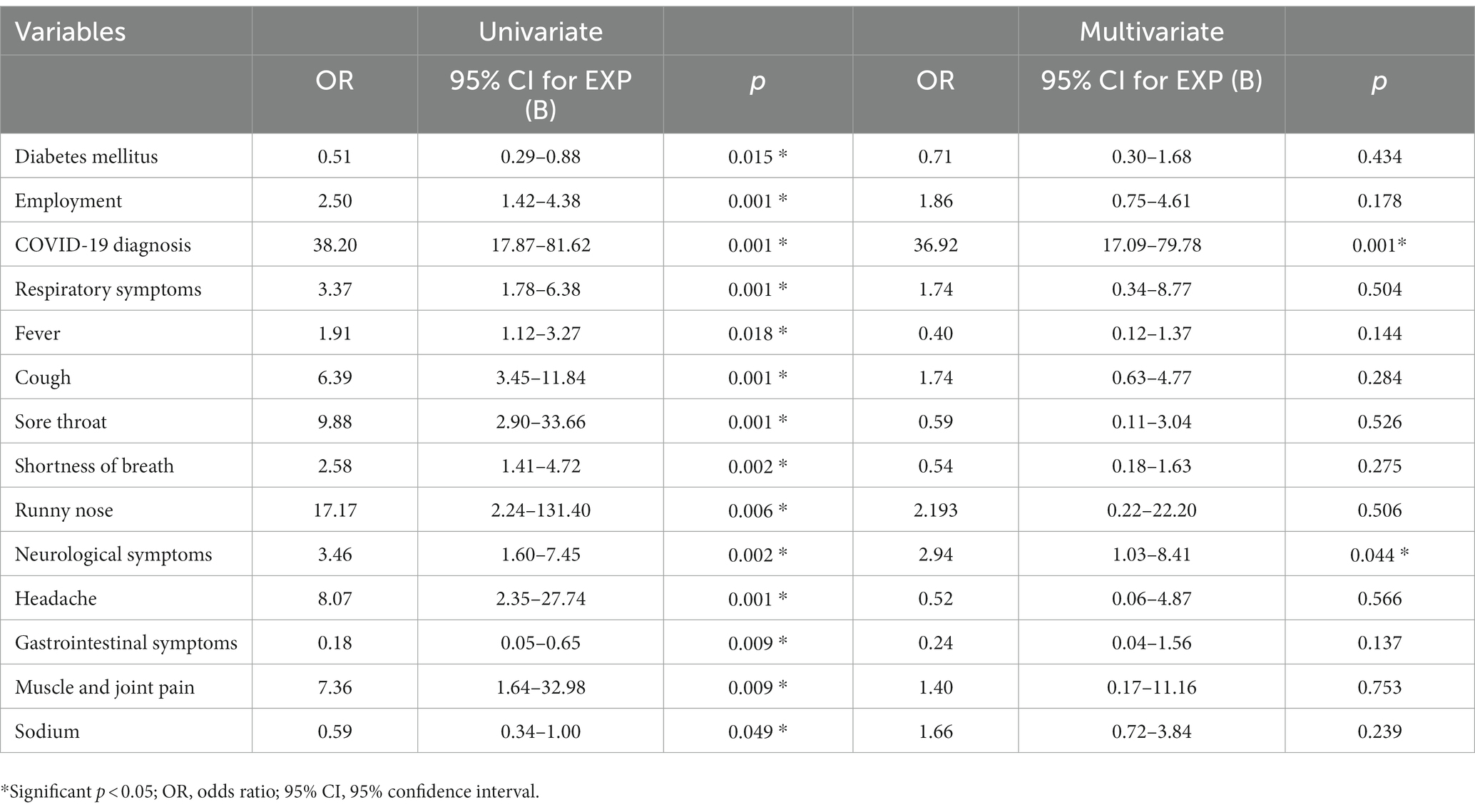
Table 4. Univariate and multivariate logistic regression analysis for anxiety.
4. Discussion
4.1. Prevalence of anxiety
The impact of the COVID-19 pandemic has caused a resultant increase in the psychological burden, including anxiety disorders. Mental health issues have emerged in general society but have also affected hospitalized patients (20, 21). The reported prevalence of anxiety in hospitalized COVID-19 patients ranged from 34.72% (2) to 60.35% (20, 21). A study performed in an urban hospital in Bangladesh showed that 30.7% of hospitalized patients with anxiety (22). A systemic review found that patients experience symptoms of anxiety (30–39%), depression (9–26%), and insomnia (24–40%) during and 3 months post-COVID-19 hospitalization (23).
A study from a local hospital in Malaysia regarding the psychological impact of COVID-19 patients found that the proportions of depressed, moderately anxious, and stressed patients were 20.5, 38.9, and 17.3%, respectively (24). This study was carried out in Ipoh, the capital of the Malaysian state of Perak, which is situated about 180 km north of Kuala Lumpur, the capital of Malaysia. Another local study reported a prevalence rate of 7% among stable hospitalized patients (25). On the contrary, our data from an urban tertiary teaching hospital in Kuala Lumpur revealed a higher prevalence of anxiety in hospitalized COVID-19 patients at 86.6%. The presence of COVID-19 has a 36 higher odds ratio to developing anxiety. This is in keeping with the predicted increment in anxiety disorders, posttraumatic stress disorders, obsessive–compulsive disorders, and the aversive social effects of isolation in Malaysia (26). An earlier community survey of anxiety in 2015, before the COVID-19 pandemic, only showed a prevalence of 8.2% in Malaysia (27). Following the pandemic, the prevalence of depression and anxiety is higher in the urban population compared with the rural population in Malaysia. The proportion of the participants with depressive symptoms was 23.9%; anxiety symptoms, 41.7%; and depression with comorbid anxiety symptoms, 19.9% (13). The discrepancy in the prevalence of anxiety in hospitalized COVID-19 patients between our study and other studies may be attributed to the emergence of psychosocial health problems in a middle-income country. This is supported by the reports emphasizing that the lack of financial and health resources and overcrowding may contribute to more dire consequences in low- and middle-income countries (28).
Anxiety was found to be associated with the severity of COVID-19 in the study, where the prevalence of mild, moderate, and severe anxiety was 84.2, 86, and 94.7%, respectively. This finding was in line with a previous study of hospitalized patients with severe and very severe anxiety (14). Signs and symptoms of anxiety and depression, such as irritability, despair, abnormally low mood, and discomfort, were demonstrated by COVID-19 patients in isolation wards (29). This is invariably evident in the increased vulnerability to stress and negative emotions from confined conditions and social isolation. Earlier studies from Wuhan, China, revealed that patients with low oxygen saturation related to the severe COVID-19 category were likely to have higher anxiety scores (2). There was a significant association between the severity of COVID-19 infection with anxiety in this study, whereby category 3 had the highest proportion of anxiety (92.3%) followed by category 5 (90.9%) and category 2 (87.5%), respectively. Although this study did not specifically ascertain the level of oxygen saturation during the study recruitment, the category of the patient’s severity was a more objective determinant as oxygen saturation may show a variable fluctuation during the course of the hospitalization.
4.2. Risk factors for anxiety
Anxiety symptoms result in clinically significant distress in the social and occupational life domains. Thus, it was not surprising that this study found that employment status was significantly different between the COVID-19 group and the controls, whereby the employed group had higher anxiety levels. Employment is crucial for psychological wellbeing as it fulfills essential needs such as social support, self-development, self-efficacy, and quality of life (30). Psychological health analysis among Chinese employees following the COVID-19 outbreak found a positive and significant impact of job insecurity on depression and anxiety (30). A cross-sectional online survey found that about 50.5% of Japanese workers felt anxious about being infected with COVID-19 in the workplace (31). A similar pattern of work-related distress was reported by employees in Serbia, where 63.4% of participants expressed increased levels of distress. This was related to moderately or highly insecure employment (30.4%) and losing their jobs (15.1%) (32). Higher distress scores were seen with increasing job insecurity, intolerance of uncertainty, and fear of COVID-19. A study in the United States gleaning the mental health burden among young adults found that job insecurity stemming from the loss of jobs and expected job loss could increase symptoms of anxiety and depression (33). The relationship between the effects of COVID-19 on the impact on employment invariably leads to poorer mental health worldwide. Further analysis of the subtypes of employment in this study may elucidate the moderating effect of intolerance of uncertainty on individual psychological factors.
Although most of the clinical features of COVID-19 are respiratory, cardiac, or gastrointestinal, many patients also experience neuropsychiatric manifestations. These manifestations stem from the direct effects on the nervous system or para-infectious/postinfectious immune-mediated disorders. Psychological stressors occur from social isolation, fear of illness, stigma, and future uncertainty from the disease. Several postulated mechanisms that have been proposed for nervous system damage by SARS-CoV-2 infection include direct infection (34), hypoxia injury (35), immune injury (36), and interaction with the angiotensin-converting enzyme receptors (37).
Several papers have explored the various COVID-19 neurological manifestations from China (38), ALBACOVID in Spain (39), the United States (40), France (41), and Malaysia (42). A systemic review of the literature revealed common neurological manifestations: myalgia, taste impairment, smell impairment, headache, and dizziness (43, 44). More severe complications include encephalopathy, encephalitis, cerebrovascular diseases (41, 45) and Guillain–Barre syndrome (46). Mao et al. retrospectively analyzed COVID-19 patients from 3 hospitals (38). They found 36.4% of patients with neuropsychiatric symptoms, which were differentiated into central (dizziness, headache), peripheral (dysgeusia, anosmia, and muscle pain), and psychological (anxiety, depression, and delirium) (38). Similarly, this study revealed that the main neurological symptoms were seizures, weakness, headache, and dizziness.
Previous literature on mental health in COVID-19 was primarily derived from observational studies (5, 47). The common psychological reactions to the COVID-19 pandemic showed symptoms of anxiety and depression (16–28%) and self-reported stress (8%) and may be associated with disturbed sleep (48). In this study, we evaluated that neurological symptoms had almost thrice the odds of developing anxiety symptoms. The currently available data broadly describe the neuropsychological COVID-19 manifestations but do not explore the association between both aspects. Our study demonstrated the possibility that anxiety might also be likely related to the underlying complex interplay of neurological features. Several proposed mechanisms that interlink psychopathological factors and immune systems include neuronal injury (49), disruption of the blood–brain barrier, peripheral immune cell invasion into the central nervous system (50) and maladaptive immune systems ( 51).
Anxiety is often associated with negative outcomes such as poorer prognosis of physical diseases, longer hospitalization, and increased readmission rates in non-psychiatric settings (52). The consequences of anxiety may affect the quality of life of the individual and negatively affect the individual’s work, family, and social life, and even lead to suicide (53). The effects of anxiety are often seen in isolation and quarantine wards. The unfavorable psychological effects of quarantine may lead to post-traumatic stress symptoms, bewilderment, and rage (54). The impact of the pandemic on anxiety needs to be apprehended in order to tailor the appropriate psychological and social support.
4.3. Strengths and limitations
The case–control study measured the variables between the cases and controls to evaluate the significant risk factors. We identified that COVID-19 patients with neurological symptoms had a higher risk to develop anxiety, which is a novel finding.
This study was carried out at a single center, which may not be a representative of the wider population of COVID-19 patients. This significant limitation may underestimate the true prevalence of anxiety among this patient group. Moreover, the study cannot determine the temporal relationship between exposure and outcome, which is a key consideration in understanding the development of anxiety. The lack of follow-up of patients after discharge from the hospital precludes any assessment of whether anxiety levels persist over time. The use of only one anxiety assessment questionnaire limits the ability to compare anxiety levels with other validated tools.
5. Conclusion
This study compared patients’ characteristics, clinical features, and anxiety levels concerning COVID-19 patients compared to controls from a tertiary teaching hospital setting. We identified that the burden of anxiety is high among hospitalized COVID-19 patients compared to controls. Those with the presence of neurological symptoms were more likely to suffer from anxiety. Early psychiatric referrals are warranted for patients at risk of having symptoms of anxiety. In addition, the availability of support groups to provide counseling assistance to hospitalized COVID-19 patients may help to facilitate support intervention programs.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Research and Ethics Board, Faculty of Medicine, National University of Malaysia. The patients/participants provided their written informed consent to participate in this study.
Author contributions
AS and HT: conceptualization, methodology, investigation, formal analysis, and writing—original draft. CK: investigation, formal analysis, and writing—original draft. CN: methodology, investigation, formal analysis, and writing—review and editing. WZ: methodology, investigation, and writing—review and editing. NK and PP: data acquisition, formal analysis, and writing—review and editing. CE and AP: data acquisition and writing—review and editing. RH and HT: methodology and writing—review and editing. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by the National University of Malaysia Research Grant (FF-2021-379).
Acknowledgments
The authors would like to thank the Infection Disease team for their support and the Dean of the Faculty of Medicine at the National University of Malaysia for his permission to publish this article.
Conflict of interest
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1148019/full#supplementary-material
Abbreviations
COVID-19, Coronavirus disease 2019; GAD-7, General Anxiety Disorder-7; SARS-CoV-2, Severe Acute Respiratory Syndrome Coronavirus 2; MERS-CoV, Middle East respiratory syndrome–related coronavirus.
References
1. de Sousa, GM, Tavares, VDO, de Meiroz Grilo, MLP, Coelho, MLG, Lima-Araújo, GL, Schuch, FB, et al. Mental health in COVID-19 pandemic: a meta-review of prevalence Meta-analyses. Front Psychol. (2021) 12:703838. doi: 10.3389/fpsyg.2021.703838
2. Dai, LL, Wang, X, Jiang, TC, Li, PF, Wang, Y, Wu, SJ, et al. Anxiety and depressive symptoms among COVID-19 patients in Jianghan Fangcang shelter Hospital in Wuhan, China. PLoS One. (2020) 15:15. doi: 10.1371/journal.pone.0238416
3. Kong, X, Zheng, K, Tang, M, Kong, F, Zhou, J, Diao, L, et al. (2020). Prevalence and factors associated with depression and anxiety of hospitalized patients with COVID-19. medRxiv 2020.03.24.20043075; doi: 10.1101/2020.03.24.20043075 [Epub ahead of print].
4. Tokur Kesgin, M, Hançer Tok, H, Uzun, LN, and Pehlivan, Ş. Comparison of anxiety levels of hospitalized COVID-19 patients, individuals under quarantine, and individuals in society. Perspect Psychiatr Care. (2022) 58:149–58. doi: 10.1111/ppc.12857
5. Zandifar, A, Badrfam, R, Yazdani, S, Arzaghi, SM, Rahimi, F, Ghasemi, S, et al. Prevalence and severity of depression, anxiety, stress and perceived stress in hospitalized patients with COVID-19. J Diabetes Metab Disord. (2020) 19:1431–8. doi: 10.1007/s40200-020-00667-1
6. Lancet Regional Health–Southeast Asia T. New vision for a healthier Southeast Asia-NC-ND license. Lancet Regional Health–Southeast Asia. (2022) 1:100020. doi: 10.1016/j.lansea.2022.100020
7. Lim, PY, Md Said, S, Kadir Shahar, H, Azman, AZF, Mokhtar, SA, and Mahmud, A. COVID-19 inpatient deaths and brought-in-dead cases in Malaysia. Front Public Health. (2022) 10:10. doi: 10.3389/fpubh.2022.872838
8. Narendra Kumar, MK, Francis, B, Hashim, AH, Zainal, NZ, Abdul Rashid, R, Ng, CG, et al. Prevalence of anxiety and depression among psychiatric healthcare workers during the COVID-19 pandemic: a Malaysian perspective. Healthcare (Basel). (2022) 10:532–47. doi: 10.3390/healthcare10030532
9. Nordin, S, Yaacob, NA, Kelak, J, Ilyas, AH, and Daud, A. The mental health of Malaysia’s northwest healthcare workers during the relaxation of COVID-19 restrictions and its associated factors. Int J Environ Res Public Health. (2022) 19:7794–7803. doi: 10.3390/ijerph19137794
10. Fong, HX, Cornish, K, Kirk, H, Ilias, K, Shaikh, MF, and Golden, KJ. Impact of the COVID-19 lockdown in Malaysia: An examination of the psychological well-being of parent-child dyads and child behavior in families with children on the autism spectrum. Front Psych. (2021) 12:12. doi: 10.3389/fpsyt.2021.733905
11. Abdul Latif, NI, Mohamed Ismail, NA, Loh, SYE, Nur Azurah, AG, Midin, M, Shah, SA, et al. Psychological distress and COVID-19 related anxiety among Malaysian women during the COVID-19 pandemic. Int J Environ Res Public Health. (2022) 1:19. doi: 10.3390/ijerph19084590
12. Marzo, RR, Vinay, V, Bahari, R, Chauhan, S, Ming, DAF, Nelson Fernandez, SFA/P, et al. Depression and anxiety in Malaysian population during third wave of the COVID-19 pandemic. Clin Epidemiol Glob Health. (2021) 12:100868. doi: 10.1016/j.cegh.2021.100868
13. Leong Bin Abdullah, MFI, Ahmad Yusof, H, Mohd Shariff, N, Hami, R, Nisman, NF, and Law, KS. Depression and anxiety in the Malaysian urban population and their association with demographic characteristics, quality of life, and the emergence of the COVID-19 pandemic. Curr Psychol. (2021) 40:6259–70. doi: 10.1007/s12144-021-01492-2
14. Woon, LSC, Leong Bin Abdullah, MFI, Sidi, H, Mansor, NS, and Nik Jaafar, NR. Depression, anxiety, and the COVID-19 pandemic: severity of symptoms and associated factors among university students after the end of the movement lockdown. PLoS One. (2021) 16:16. doi: 10.1371/journal.pone.0252481
15. Ministry of Health Malaysia. Clinical management of confirmed COVID-19 case in adult. Ministry of Health Malaysia. (2020). Available at: https://covid-19.moh.gov.my/garis-panduan/gp-umum-covid19 (Accessed Dec 20, 2022).
16. Spitzer, RL, Kroenke, K, Williams, JB, and Löwe, B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
17. Sidik, SM, Arroll, B, and Goodyear-Smith, F. Validation of the GAD-7 (Malay version) among women attending a primary care clinic in Malaysia. J Prim Health Care. (2012) 4:5–11. doi: 10.1071/HC12005
18. Cordaro, M, Grigsby, TJ, Howard, JT, Deason, RG, Haskard-Zolnierek, K, and Howard, K. Pandemic-specific factors related to generalized anxiety disorder during the initial COVID-19 protocols in the United States. Issues Ment Health Nurs. (2021) 42:747–57. doi: 10.1080/01612840.2020.1867675
19. Chen, H, Gao, J, Dai, J, Mao, Y, Wang, Y, Chen, S, et al. Generalized anxiety disorder and resilience during the COVID-19 pandemic: evidence from China during the early rapid outbreak. BMC Public Health. (2021) 21:1830. doi: 10.1186/s12889-021-11877-4
20. Hao, F, Tam, W, Hu, X, Tan, W, Jiang, L, Jiang, X, et al. A quantitative and qualitative study on the neuropsychiatric sequelae of acutely ill COVID-19 inpatients in isolation facilities. Transl Psychiatry. (2020) 10:355. doi: 10.1038/s41398-020-01039-2
21. Ngasa, SN, Tchouda, LAS, Abanda, C, Ngasa, NC, Sanji, EW, Dingana, TN, et al. Prevalence and factors associated with anxiety and depression amongst hospitalised COVID-19 patients in Laquintinie hospital Douala, Cameroon. PLoS One. (2021) 16:e0260819. doi: 10.1371/journal.pone.0260819
22. Nabi, SG, Rashid, MU, Sagar, SK, Ghosh, P, Shahin, M, Afroz, F, et al. Psychological impact of COVID-19 pandemic: a cross-sectional study of hospitalized COVID-19 patients in an urban setting, Bangladesh. Heliyon. (2022) 8:e09110. doi: 10.1016/j.heliyon.2022.e09110
23. Veazie, S, Lafavor, B, Vela, K, Young, S, Sayer, NA, Carlson, KF, et al. Mental health outcomes of adults hospitalized for COVID-19: a systematic review. J Affect Disord Rep. (2022) 8:100312. doi: 10.1016/j.jadr.2022.100312
24. Loo, TH, Arvinder-Singh, HS, Ang, YC, Kong, YH, Vikram Suarn, S, and Rakesh, S. Psychological impact amongst patients with COVID-19 in Perak state. Med J Malaysia. (2022) 77:643–9.
25. Bin Adnan, MAA, Bin Kassim, MSA, Bt Sahril, N, et al. Prevalence and predictors of anxiety among stable hospitalized COVID-19 patients in Malaysia. Int J Environ Res Public Health. (2023) 20:586. doi: 10.3390/ijerph20010586
26. Shanmugam, H, Ariff, JJ, Nair, P, Ken, CS, and Guan, NC. Impacts of COVID-19 pandemic on mental health in Malaysia: a single thread of hope. Malays J Psychiatry. (2020) 29:78–84.
27. Maideen, SFK, Sidik, SM, Rampal, L, and Mukhtar, F. Prevalence, associated factors and predictors of anxiety: a community survey in Selangor. Malaysia BMC Psychiatry. (2015) 15:262–273. doi: 10.1186/s12888-015-0648-x
28. Bong, CL, Brasher, C, Chikumba, E, McDougall, R, Mellin-Olsen, J, and Enright, A. The COVID-19 pandemic: effects on low- and middle-income countries. Anesth Analg. (2020) 131:86–92. doi: 10.1213/ANE.0000000000004846
29. Rahman, J, Muralidharan, A, Quazi, SJ, Saleem, H, and Khan, S. Neurological and psychological effects of coronavirus (COVID-19): An overview of the current era pandemic. Cureus. (2020) 12:e8460. doi: 10.7759/cureus.8460
30. Khudaykulov, A, Changjun, Z, Obrenovic, B, Godinic, D, Alsharif, HZH, and Jakhongirov, I. The fear of COVID-19 and job insecurity impact on depression and anxiety: An empirical study in China in the COVID-19 pandemic aftermath. Curr Psychol. (2022) 9:1–14. doi: 10.1007/s12144-022-02883-9
31. Eguchi, H, Hino, A, Inoue, A, Tsuji, M, Tateishi, S, Ando, H, et al. Effect of anxiety about COVID-19 infection in the workplace on the association between job demands and psychological distress. Front Public Health. (2021) 9:722071. doi: 10.3389/fpubh.2021.722071
32. Blanuša, J, Barzut, V, and Knežević, J. Intolerance of uncertainty and fear of COVID-19 moderating role in relationship between job insecurity and work-related distress in the republic of Serbia. Front Psychol. (2021) 12:647972. doi: 10.3389/fpsyg.2021.647972
33. Ganson, KT, Tsai, AC, Weiser, SD, Benabou, SE, and Nagata, JM. Job insecurity and symptoms of anxiety and depression among U.S. Young adults during COVID-19. J Adolesc Health. (2021) 68:53–6. doi: 10.1016/j.jadohealth.2020.10.008
34. Leber, AL, Everhart, K, Balada-Llasat, JM, Cullison, J, Daly, J, Holt, S, et al. Multicenter evaluation of biofire filmarray meningitis/encephalitis panel for detection of bacteria, viruses, and yeast in cerebrospinal fluid specimens. J Clin Microbiol. (2016) 54:2251–61. doi: 10.1128/JCM.00730-16
35. Guo, YR, Cao, QD, Hong, ZS, Tan, YY, Chen, SD, Jin, HJ, et al. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak - an update on the status. Mil Med Res. (2020) 7:11. doi: 10.1186/s40779-020-00240-0
36. Klein, RS, Garber, C, and Howard, N. Infectious immunity in the central nervous system and brain function. Nat Immunol Nat Publish Group. (2017) 18:132–41. doi: 10.1038/ni.3656
37. Wrapp, D, Wang, N, Corbett, KS, Goldsmith, JA, Hsieh, CL, Abiona, O, et al. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science. (2020) 367:1260–3. doi: 10.1126/science.abb2507
38. Mao, L, Jin, H, Wang, M, Hu, Y, Chen, S, He, Q, et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. Arch Neurol. (2020) 77:683–90. doi: 10.1001/jamaneurol.2020.1127
39. Romero-Sánchez, CM, Díaz-Maroto, I, Fernández-Díaz, E, Sánchez-Larsen, Á, Layos-Romero, A, García-García, J, et al. Neurologic manifestations in hospitalized patients with COVID-19: the ALBACOVID registry. Neurology. (2020) 95:E1060–70. doi: 10.1212/WNL.0000000000009937
40. Iosifescu, AL, Hoogenboom, WS, Buczek, AJ, Fleysher, R, and Duong, TQ. New-onset and persistent neurological and psychiatric sequelae of COVID-19 compared to influenza: a retrospective cohort study in a large new York City healthcare network. Int J Methods Psychiatr Res. (2022) 31:e1914. doi: 10.1002/mpr.1914
41. Meppiel, E, Peiffer-Smadja, N, Maury, A, Bekri, I, Delorme, C, Desestret, V, et al. Neurologic manifestations associated with COVID-19: a multicentre registry. Clin Microbiol Infect. (2021) 27:458–66. doi: 10.1016/j.cmi.2020.11.005
42. Tan, HJ, Goh, CH, Khoo, CS, Ng, CF, Tan, JK, Wan Zaidi, WA, et al. Neurological manifestations in SARS-CoV -2 infection: a single-center cross-sectional study in Malaysia. Neurol Clin Neurosci. (2023) 11:17–26. doi: 10.1111/ncn3.12677
43. Yassin, A, Nawaiseh, M, Shaban, A, Alsherbini, K, el-Salem, K, Soudah, O, et al. Neurological manifestations and complications of coronavirus disease 2019 (COVID-19): a systematic review and meta-analysis. BMC Neurol. (2021) 21:138. doi: 10.1186/s12883-021-02161-4
44. Pinzon, RT, Wijaya, VO, Buana, RB, al Jody, A, and Nunsio, PN. Neurologic characteristics in coronavirus disease 2019 (COVID-19): a systematic review and meta-analysis. Front Neurol. (2020) 11:565. doi: 10.3389/fneur.2020.00565
45. Ellul, MA, Benjamin, L, Singh, B, Lant, S, Michael, BD, Easton, A, et al. Neurological associations of COVID-19. Lancet Neurol. (2020) 19:767–83. doi: 10.1016/S1474-4422(20)30221-0
46. Payus, AO, Jan, TH, Ibrahim, A, et al. Autoimmune polyradiculopathy in SARS-CoV-2: a narrative review of Guillain-Barre syndrome in novel coronavirus disease (COVID-19). Acta Med Mediterranea. (2020) 36:3781–5. doi: 10.19193/0393-6384_2020_6_599
47. Liu, S, Yang, L, Zhang, C, Xiang, YT, Liu, Z, Hu, S, et al. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry. (2020) 7:e17–8. doi: 10.1016/S2215-0366(20)30077-8
48. Rajkumar, RP. COVID-19 and mental health: a review of the existing literature. Asian J Psychiatr. (2020) 52:102066. doi: 10.1016/j.ajp.2020.102066
49. Desforges, M, le Coupanec, A, Dubeau, P, Bourgouin, A, Lajoie, L, Dubé, M, et al. Human coronaviruses and other respiratory viruses: underestimated opportunistic pathogens of the central nervous system? Viruses. (2019) 12:14. doi: 10.3390/v12010014
50. Wu, Y, Xu, X, Chen, Z, Duan, J, Hashimoto, K, Yang, L, et al. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav Immun. (2020) 87:18–22. doi: 10.1016/j.bbi.2020.03.031
51. Najjar, S, Pearlman, DM, Alper, K, Najjar, A, and Devinsky, O. Neuroinflammation and psychiatric illness. J Neuroinflammation. (2013) 10:43. doi: 10.1186/1742-2094-10-43
52. Guo, WJ, Wang, HY, Deng, W, Huang, MJ, Dong, ZQ, Liu, Y, et al. Effects of anxiety and depression and early detection and management of emotional distress on length of stay in hospital in non-psychiatric inpatients in China: a hospital-based cohort study. Lancet. (2019) 394:S83. doi: 10.1016/S0140-6736(19)32419-5
53. Wang, C, Pan, R, Wan, X, Tan, Y, Xu, L, Ho, CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. (2020) 17:1729. doi: 10.3390/ijerph17051729
Keywords: anxiety, COVID-19, hospitalized, case control, Generalized Anxiety Disorder-7
Citation: Tan HJ, Shahren AAH, Khoo CS, Ng CF, Zaidi WAW, Kori N, Periyasamy P, Eu CL, Payus AO and Hod R (2023) Anxiety among hospitalized COVID-19 patients: a case–control study from a tertiary teaching hospital in Malaysia. Front. Psychiatry. 14:1148019. doi: 10.3389/fpsyt.2023.1148019
Edited by:
Baojuan Ye, Jiangxi Normal University, ChinaReviewed by:
Mario J. Valladares-Garrido, Norbert Wiener Private University, PeruGellan Ahmed, Assiut University, Egypt
Copyright © 2023 Tan, Shahren, Khoo, Ng, Zaidi, Kori, Periyasamy, Eu, Payus and Hod. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hui Jan Tan, tanhuijan@ukm.edu.my
†ORCID: Choon Leng Eu, https://orcid.org/0000-0002-0531-7790