 Barbara E. Stähli1,2*
Barbara E. Stähli1,2* Markus Reinthaler1,2David M. Leistner1,2,3Ulf Landmesser1,2,3
Markus Reinthaler1,2David M. Leistner1,2,3Ulf Landmesser1,2,3 Alexander Lauten1,2
Alexander Lauten1,2- 1Department of Cardiology, Charité - Universitätsmedizin Berlin, Berlin, Germany
- 2Partner Site Berlin, Deutsches Zentrum für Herz-Kreislaufforschung (DZHK), Berlin, Germany
- 3Berlin Institute of Health, Berlin, Germany
Mitral regurgitation frequently coexists in patients with severe aortic stenosis. Patients with moderate to severe mitral regurgitation at the time of transcatheter aortic valve replacement are at increased risk of future adverse events. Whether concomitant mitral regurgitation is independently associated with worse outcomes after TAVR remains a matter of debate. The optimal therapeutic strategy in these patients—TAVR with evidence-based heart failure therapy, combined TAVR and transcatheter mitral valve intervention, or staged transcatheter therapies—is ill-defined, and guideline-based recommendations in patients at increased risk for open heart surgery are lacking. Hence, a thorough evaluation of the aortic and mitral valve anatomy and function, along with an in-depth assessment of the patients' baseline risk profile, provides the basis for an individualized treatment approach. The aim of this review is therefore to give an overview of the current literature on mitral regurgitation in TAVR, focusing on different diagnostic and therapeutic strategies and optimal clinical decision making.
Introduction
Concomitant mitral regurgitation is frequently observed in patients with severe aortic stenosis (1–3). About 20% of patients undergoing transcatheter (TAVR) or surgical (SAVR) aortic valve replacement for severe aortic stenosis have concomitant more than mild mitral regurgitation (1–3). Whether concomitant mitral regurgitation is independently associated with worse outcomes after aortic valve replacement is uncertain (4). A thorough evaluation of the aortic and mitral valve anatomy and function is important in these patients and mainly based on transthoracic and transesophageal echocardiography. An in-depth understanding of the underlying pathophysiological mechanism provides the basis for an individualized treatment approach and optimal procedural planning. Emerging minimally invasive surgical and transcatheter treatment strategies offer novel, less-invasive therapeutic options for combined, staged or hybrid procedures when severe aortic stenosis and mitral regurgitation do coexist, particularly in elderly patients, obviating the need for open heart surgery (5). The treatment of first choice in these patients, however, remains a matter of debate, and guideline-based recommendations are lacking.
The aim of this review is therefore to give an overview of the current literature on mitral regurgitation in TAVR, with particular focus on the different diagnostic and therapeutic strategies available and on the clinical decision-making process in patients at increased surgical risk.
Assessment of Mitral Regurgitation in Patients With Severe Aortic Stenosis
In mitral regurgitation, besides the grading of the regurgitation severity, identification of the underlying etiology, particularly the distinction between primary and secondary mitral regurgitation, is of great importance to guide therapeutic management. The assessment of the mitral valve apparatus and the type of dysfunction is mainly based on transthoracic and/or transesophageal echocardiography with multimodality imaging used in specific situations (6, 7). Although transthoracic echocardiography is diagnostic in most cases, transesophageal echocardiography complements the assessment when transthoracic image quality is suboptimal and further diagnostic refinement is required (6, 7). Transesophageal echocardiography not only provides additional important information on the etiology of the disease, but also helps to determine the feasibility of dedicated transcatheter mitral valve procedures. Three-dimensional (3D) echocardiography facilitates anatomic and functional interpretation, particularly in patients with complex valvular pathologies (6–9).
Mitral regurgitation may either be primary/degenerative due to abnormalities of the valvular apparatus itself such as mitral valve prolapse, flail leaflets, and chordal rupture, or secondary/functional due to restricted leaflets, mostly caused by left ventricular dilatation and dysfunction in ischemic cardiomyopathy and chronic pressure overload related to aortic stenosis (10). Annular dilatation and left atrial enlargement causing insufficient leaflet closure, e. g., in patients with long-standing atrial fibrillation, may also be an underlying cause. Mixed forms exist when both pathologies overlap. As the mitral valvular apparatus is often calcified in patients with degenerative aortic stenosis, pure secondary mitral regurgitation is unlikely in this context (4).
An integrated approach using qualitative, semi-quantitative, and quantitative echocardiographic parameters allows for a comprehensive assessment of mitral regurgitation (9, 11, 12). Color flow imaging is the most common way to detect mitral regurgitation, with quantification based on the integration of further measures such as vena contracta width, PISA radius, regurgitation volume and effective regurgitant orifice area (EROA) (6). The evaluation of mitral regurgitation in aortic stenosis may, however, be challenging as jet velocity may be increased due to high left ventricular pressures (4). On the other hand, concomitant mitral regurgitation impacts on transvalvular gradient and flow in severe aortic stenosis, which may hamper echocardiographic assessment (13).
A thorough echocardiographic evaluation of the mitral valve apparatus is needed to determine the feasibility of transcatheter mitral valve interventions (14–16). Unfavorable echocardiographic criteria for percutaneous edge-to-edge mitral valve repair include severe leaflet calcifications in the grasping area, rheumatic leaflet thickening, perforated leaflets or clefts, and a mobile length of the posterior mitral valve leaflet of <7 mm, along with insufficient mechanical coaptation in functional (coaptation depth >11 mm, coaptation length <2 mm) and excessive flail gap in degenerative disease (fail gap >10 mm and flail width >15 mm, Table 1) (15–17). A pre-procedural mitral valve area of >4 cm2 is recommended in order to reduce the risk of post-procedural mitral valve stenosis (17). Advanced imaging modalities such as multidetector computed tomography (MDCT) complement the assessment of these patients. Besides the evaluation of the aorto-iliacal axis in TAVR patients, MDCT provides important information on the mitral valve apparatus, particularly on annular dimensions, the extent and localization of calcifications, and the spacial relationship to adjacent structures (16, 18, 19).
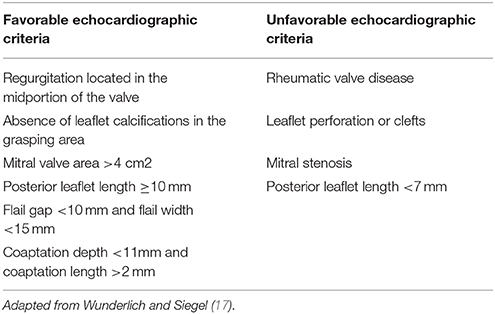
Table 1. Favorable echocardiographic criteria for transcatheter edge-to-edge mitral valve repair with the MitraClip® system.
Impact of Mitral Regurgitation on Outcomes in Patients With Severe Aortic Stenosis
Patients with aortic stenosis and coexisting moderate to severe mitral regurgitation are known to have a worse clinical risk profile as compared to those without, which is also reflected by higher surgical risk scores (20, 21). They are older, have a higher prevalence of atrial fibrillation and prior myocardial infarction, and poorer left ventricular systolic function (LVEF) (20–22). Whether concomitant mitral regurgitation independently affects outcomes in patients undergoing AVR remains an ongoing matter of debate, particularly whether secondary mitral regurgitation is related with outcomes irrespective of left ventricular dysfunction. While some studies did not observe any association between the presence of mitral regurgitation and adverse events after SAVR (23, 24), others demonstrated an increased risk of mortality, heart failure, and need for future mitral valve repair/replacement when mitral regurgitation was treated medically (2, 25, 26). While in some studies, mitral regurgitation did not emerge as independent predictor of mortality after TAVR (2, 20, 27), the majority of studies clearly pointed toward an increased risk of mortality when coexistent moderate to severe mitral regurgitation was present at the time of TAVR (28–34). In a meta-analysis including 4,839 TAVR patients, all-cause mortality was significantly higher in patients with moderate to severe mitral regurgitation (29). Similarly, in a multicenter registry including 1,007 patients undergoing TAVR with the CoreValve Revalving System, 1-year mortality was significantly higher in patients with moderate or severe mitral regurgitation as compared to those without (31). Differences in the grading methodology of mitral regurgitation which was based on qualitative echocardiographic measures in most studies, along with varying inclusion criteria, mainly regarding the etiology and severity of mitral regurgitation, may hamper comparisons among studies. Most interestingly, in the PARTNER (Placement of AoRTic TraNscathetER Valve) trial, patients with moderate to severe mitral regurgitation seemed to experience an even greater benefit from TAVR than those without, as reflected in a smaller number needed to treat to prevent a fatality (35).
Treatment Strategies in Patients With Severe Aortic Stenosis and Mitral Regurgitation
As double valve surgery is associated with an increased mortality as compared to SAVR or combined SAVR and coronary artery bypass grafting (36), transcatheter therapeutic options represent promising less-invasive treatment alternatives to open heart surgery in high-risk patients. Despite the high prevalence of concomitant mitral regurgitation in patients with severe aortic stenosis and the associated substantial morbidity and mortality, randomized trials investigating different therapeutic strategies are lacking. Whether concomitant mitral regurgitation should be treated medically or addressed in combined or staged procedures is ill-defined, and optimal patient selection and timing of interventions need to be determined. The evidence in this field is mostly stemming from observational data and case series, which precludes firm conclusions. Given the lack of guideline-based recommendations, personalized treatment strategies based on associated symptoms, the individual valvular pathology, the comorbid burden, and the estimated procedural risk are advocated (10). Irrespective of attempted surgical or transcatheter approaches to mitral regurgitation, guideline-based heart failure management is essential in these patients before evaluating the regurgitation severity.
The Guideline-Based Heart Team Approach
All patients with severe symptomatic aortic stenosis and concomitant mitral regurgitation, who are at increased surgical risk, are evaluated by a multidisciplinary Heart Team to ensure comprehensive risk stratification and optimal patient selection. Besides technical aspects, associated symptoms, the burden of comorbidities, patient's life expectancy, patient's frailty, and the quality of life need to be taken into account to deliver best quality of care (10). Thereby, a balanced decision on the optimal treatment strategy is taken for each individual patient.
Guideline-based indications for mitral valve procedures are summarized in Table 2. The distinction between primary and secondary mitral regurgitation is emphasized in this context. Although mitral valve repair/replacement is considered the gold standard in patients with symptomatic severe mitral regurgitation (10), benefits in those with secondary forms are less clear as lack of survival benefit and an increased risk of recurrence have been reported (37), finally resulting in lower levels of evidence for treatment recommendations in this patient subgroup. According to current guidelines of the European Society of Cardiology (ESC) (10), intervention for severe chronic primary mitral regurgitation is indicated in symptomatic patients with preserved left ventricular ejection fraction (LVEF >30%, class of recommendation I, level of evidence B) with valve repair being the preferred treatment approach. Surgery is further indicated in asymptomatic patients with left ventricular dysfunction as mirrored by a reduced left ventricular systolic function [LVEF ≤ 60%] or increased left ventricular dimensions (left ventricular end-systolic diameter ≥45 mm, class of recommendation I, level of evidence B), and should be considered in patients with new onset of atrial fibrillation or increased pulmonary pressures (systolic pulmonary pressure ≥50 mmHg, class of recommendation IIa, level of evidence B), and flail leaflet or significant left atrial dilatation (class of recommendation IIa, level of evidence C) (10). Percutaneous edge-to-edge repair may be considered by the Heart Team for symptomatic patients at high surgical risk (class of recommendation IIb, level of evidence C). Currently, there is no indication to intervene for moderate mitral regurgitation.
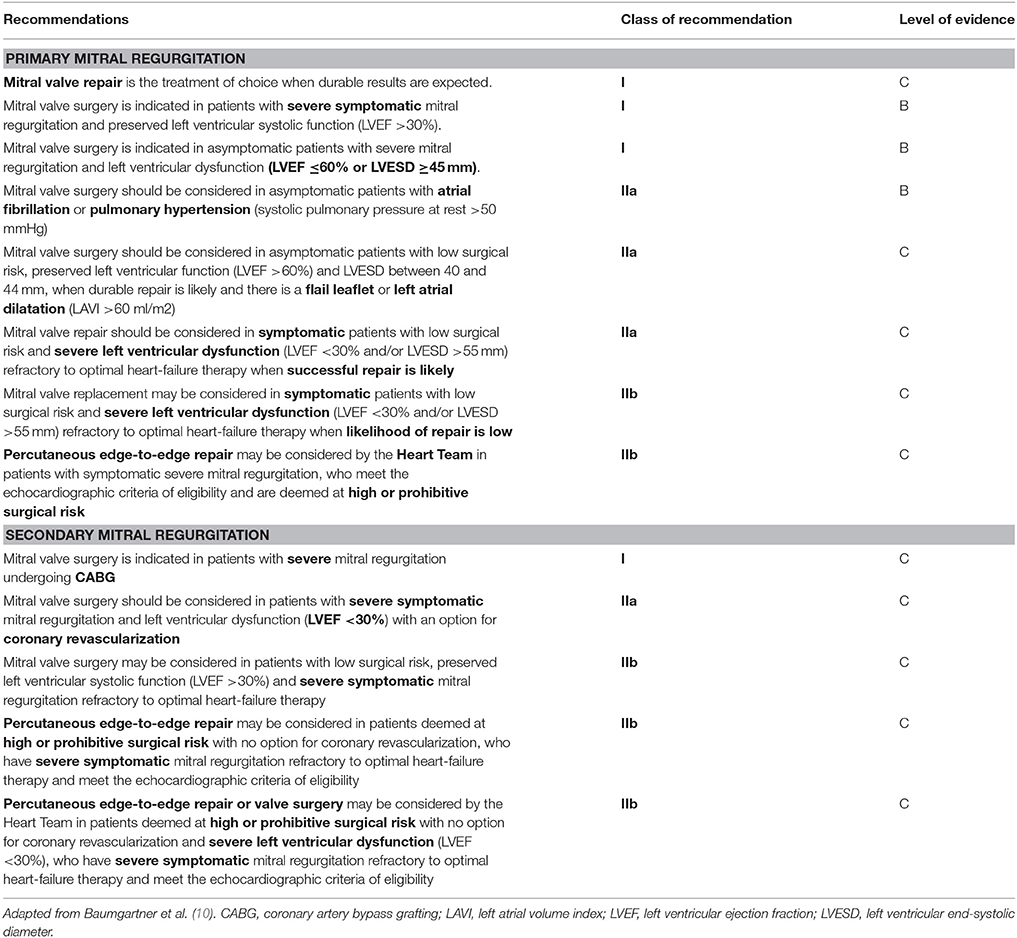
Table 2. Recommendations for the treatment of chronic mitral regurgitation according to the 2017 European Society of Cardiology (ESC) and European Association for Cardio-Thoracic Surgery (EACTS) guidelines for the management of valvular heart disease.
In patients with severe secondary mitral regurgitation, optimal guideline-recommended heart failure therapy, including optimal medical therapy and coronary revascularization or cardiac resynchronization as indicated, is of particular importance (10, 38). For the treatment of severe secondary mitral regurgitation, a class I recommendation for mitral valve surgery with valve repair being the method of first choice exists in patients undergoing coronary artery bypass graft surgery, when LVEF is preserved (level of evidence C). In symptomatic patients with reduced left ventricular systolic function (LVEF <30%), surgery should be considered when coronary revascularization is indicated (class of recommendation IIa, level of evidence C). When there is no option for coronary revascularization, mitral valve surgery may be considered in patients with preserved LVEF and low surgical risk (class of recommendation IIb, level of evidence C). A percutaneous edge-to-edge procedure may be considered when echocardiographic criteria of eligibility are met and surgical risk deemed prohibitive (class of recommendation IIb, level of evidence C). Although transcatheter percutaneous mitral valve procedures were shown to substantially reduce the degree of mitral regurgitation, beneficially affect left ventricular reverse remodeling, and significantly decrease the symptomatic burden (15, 39–41), it remains uncertain whether survival benefits are achieved. Emerging interventional procedures such as transcatheter annuloplasty or transapical valve replacement complement the therapeutic armamentarium for severe mitral regurgitation in high risk patients. Experience with these procedures is, however, still limited and guideline-based recommendations lacking.
TAVR and Natural Course of Mitral Regurgitation
Most studies report on a significant improvement of mitral regurgitation after AVR, which has mostly been attributed to reverse left ventricular remodeling and improved left ventricular function. Indeed, in a meta-analysis including 8,927 patients undergoing TAVR, the severity of mitral regurgitation significantly improved in about 60% of patients (42). In the PARTNER trial, moderate to severe mitral regurgitation was observed in 21% of SAVR and 20% of TAVR patients, and improvement was reported in 69% of SAVR and 58% of TAVR patients at 30 days (2). Similar results were reported in other studies (32, 43, 44). These effects may be particularly predominant in patients with secondary mitral regurgitation as structural valve alterations obviously persist after TAVR. A significant improvement in mitral regurgitation severity is more likely to occur in patients without severe pulmonary hypertension and atrial fibrillation (31) Interestingly, acute improvement in mitral regurgitation has been reported following TAVR and was related to immediate post-procedural changes in left ventricular hemodynamics and improved mitral leaflet tethering (45). Whether the design of the implanted transcatheter heart valve influences the post-procedural course of mitral regurgitation needs to be delineated in future studies. Observational studies point toward a greater degree of reduction of mitral regurgitation in patients treated with balloon-expandable as compared to self-expandable transcatheter heart valves (28).
Combined TAVR and Transcatheter Mitral Valve Procedure
In comparison to a single valve procedure, surgical double valve replacement/repair is associated with increased morbidity and mortality (36, 46). Indeed, mortality rates of about 10% have been reported for double valve aortic and mitral surgery as compared to 3% for isolated SAVR (36). Over the last decades, transcatheter techniques have evolved and offer less-invasive treatment alternatives to double valve surgery in patients deemed at high or prohibitive surgical risk. Transcatheter mitral valve replacement (TMVR) offers a less invasive treatment alternative to redo cardiac surgery, particularly in high-risk patients with degenerated mitral bioprostheses and failed annuloplasty rings (47). Clinical experience with bivalvular transcatheter procedures, however, is still limited (48, 49). The success of a combined approach with transcatheter mitral valve repair performed at the time of TAVR has been reported in several studies (50, 51). Different transcatheter mitral valve repair technologies may be used in this context such as the MitraClip® device (Abbott Vascular Inc., Menlo Park, CA, USA), the Carillon Mitral Contour System® (Cardiac Dimensions, Kirkland, WA, USA), and the Cardioband® (Valtech, Edwards Lifescience Corp, Irvine, CA, USA) (52) An overview of current devices for transcatheter mitral valve repair is provided in Table 3.
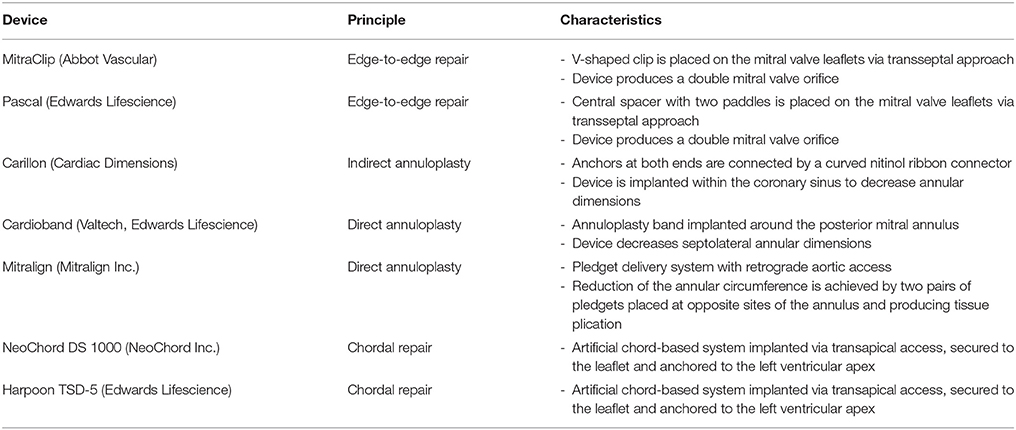
Table 3. Overview of devices for transcatheter mitral valve repair.
The most advanced percutaneous mitral valve repair system is the MitraClip® device which allows for introducing a V-shaped clip on the mitral valve leaflets via a transseptal approach under transesophageal echocardiographic and fluoroscopic guidance (Figure 1). Thereby, a double or multiple orifice is created (14–16). High procedural success rates of percutaneous edge-to-edge mitral valve repair have not only been reported for primary, but also secondary mitral regurgitation (41, 53), and safety and efficacy was also demonstrated in patients who did not meet the key echocardiographic eligibility criteria as determined by the EVEREST (Endovascular Valve Edge-to-Edge Repair) studies (54).
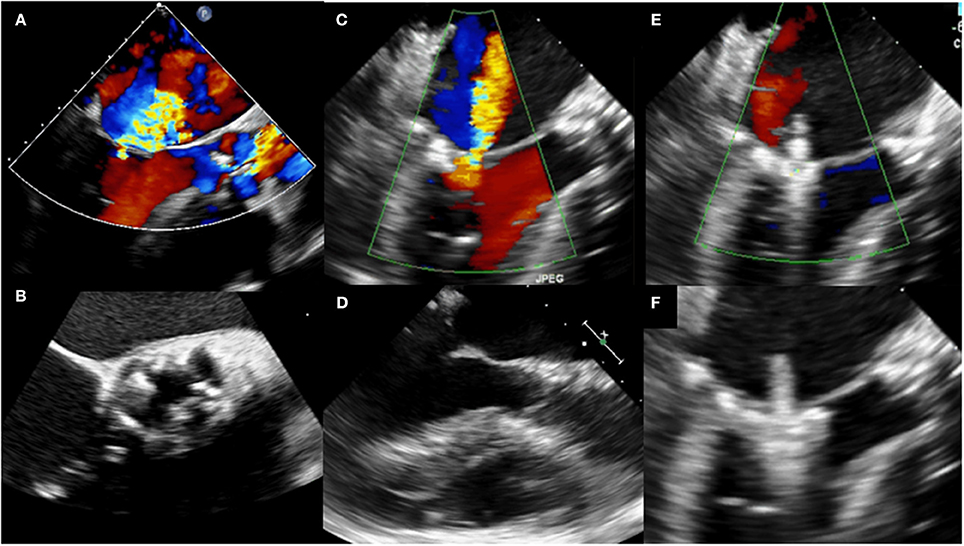
Figure 1. Pre- and post-procedural transesophageal echocardiography in a patient undergoing staged transcatheter aortic valve replacement (TAVR) and edge-to-edge mitral valve repair with the MitraClip® system. (A) Transesophageal color Doppler echocardiography at baseline (three-chamber view) showing severe aortic stenosis and concomitant severe mitral regurgitation. (B) Transesophageal echocardiography at baseline (aortic valve short-axis view) showing severe aortic stenosis. (C) Two-dimensional transesophageal color Doppler echocardiography (three chamber view) showing persistent severe mitral regurgitation following TAVR. (D) Two-dimensional transesophageal echocardiography (three chamber view) following TAVR. (E) Two-dimensional transesophageal color Doppler echocardiography (three-chamber view) during staged percutaneous edge-to-edge mitral valve repair with the MitraClip® system (grasping). (F) Two-dimensional transesophageal echocardiography (three-chamber view) during staged percutaneous edge-to-edge mitral valve repair with the MitraClip® system (grasping).
Percutaneous indirect mitral annuloplasty was developed to improve leaflet coaptation by reducing mitral annular dimensions using dedicated transcatheter devices such as the Carillon Mitral Contour System®. The Carillon Mitral Contour System® consists of anchors at both ends, which are connected by a curved nitinol ribbon connector. The device is implanted within the coronary sinus to reduce the severity of mitral regurgitation by annular placation (14, 55). Safety and feasibility of the procedure, along with clinical benefits in terms of heart failure symptoms, quality of life, and exercise tolerance have been shown for patients with dilated cardiomyopathy and functional mitral regurgitation in different studies such as the AMADEUS (the Carillon Mitral Annuloplasty Device European Union Study) and the TITAN (Transcatheter Implantation of Carillon Mitral Annuloplasty Device) trials (40, 55). The direct annuloplasty Cardioband® system represents a similar interventional transseptal approach for the treatment of secondary mitral regurgitation (56) The annuloplasty band is implanted around the posterior mitral annulus, aiming at reducing mitral regurgitation by decreasing septolateral annular dimensions.
Besides minimally invasive surgical valve repair or replacement, TMVR has emerged as less-invasive treatment alternative for patients deemed at high or prohibitive surgical risk, with several prostheses already introduced in clinical practice (57–59). Although feasibility and safety of valve-in-valve, valve-in-ring, and valve-in-native ring procedures have been demonstrated for transcatheter heart valve implantation in the mitral position (60), future randomized studies are needed to determine the role of TMVR in patients with severe mitral regurgitation.
TAVR and Staged Transcatheter Mitral Valve Procedure
As significant improvements in mitral regurgitation severity have been observed after AVR (26, 43, 44), a staged approach may be favored over a combined procedure with the aortic valve being addressed first and the mitral valve treated only in patients who remain symptomatic in spite of successful TAVR (50, 61). Patients with prior AVR undergoing transcatheter mitral valve repair, however, represent a complex patient subgroup with a high comorbid burden at increased risk of adverse events. One-year survival in these patients was reported to be below 50% (62).
Given the lack of randomized comparisons between surgical and transcatheter double valve interventions vs. medical management of mitral regurgitation in the context of severe aortic stenosis, evidence-based recommendations on patient selection and optimal timing of interventions cannot be made. For predominantly secondary mitral regurgitation, when no major structural mitral valve defects exist, a staged approach may be reasonable to tailor mitral interventions to patients with persistent symptomatic mitral regurgitation, who may benefit most. Bivalvular interventions may be advocated when concomitant predominantly primary mitral regurgitation is present.
Based on our experience, we strongly advocate a stepwise approach in this high-risk patient population, with TAVR being performed first and percutaneous mitral valve repair considered by the Heart Team only when severe mitral regurgitation persists after TAVR. A close clinical and echocardiographic follow-up of these patients following TAVR is mandatory, with functional tests used when grading of mitral regurgitation is challenging.
Cost-Effectiveness of Transcatheter Valve Procedures
Although procedural costs of TAVR exceed those of SAVR, cost-effectiveness of TAVR in patients at increased surgical risk has been demonstrated when shorter hospital stay and reduced need for post-acute rehabilitation services are taken into account, particularly when a transfemoral access is suitable (63–66). In heart failure patients with moderate-to-severe mitral regurgitation, therapy with the MitraClip® device was shown to be cost-effective compared to medical management alone (67). Direct economic comparisons between different transcatheter mitral valve repair systems and mitral valve surgery are, however, lacking. A staged approach with TAVR performed first and percutaneous mitral valve repair tailored to patients who do not experience any improvement in mitral regurgitation following TAVR seems to be cost-effective, as thereby the number of mitral valve interventions is reduced in comparison to simultaneous procedures.
Conclusion
Risk assessment and optimal patient selection, along with a personalized treatment approach defined by the Heart Team, is important to ensure best patient care in symptomatic aortic stenosis and concomitant mitral regurgitation. Given the heterogeneity and complexity of mitral valve disease in these high-risk patients, individualized treatment concepts are needed. Although the feasibility and safety of bivalvular transcatheter procedures have been demonstrated, the treatment of first choice—TAVR only, staged TAVR and transcatheter mitral valve procedures, or combined bivalvular transcatheter therapy vs. minimally-invasive surgical treatment—remains to be determined. Randomized trials investigating benefits of mitral valve procedures vs. guideline-based heart failure therapy in TAVR patients with concomitant mitral regurgitation will help to define optimal treatment approaches. Refinements of transcatheter mitral valve concepts including the combination of different approaches will probably enter clinical practice in near future and further improve patient outcomes.
Author Contributions
BS analysis and interpretation of the literature, drafting of the manuscript. BS, MR, DL, UL, and AL revising the manuscript critically for important intellectual content, final approval of the manuscript submitted. AL analysis and interpretation of the literature.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Moazami N, Diodato MD, Moon MR, Lawton JS, Pasque MK, Herren RL, et al. Does functional mitral regurgitation improve with isolated aortic valve replacement? J Card Surg. (2004) 19:444–8. doi: 10.1111/j.0886-0440.2004.00362.x
2. Barbanti M, Webb JG, Hahn RT, Feldman T, Boone RH, Smith CR, et al. Impact of preoperative moderate/severe mitral regurgitation on 2-year outcome after transcatheter and surgical aortic valve replacement: insight from the Placement of Aortic Transcatheter Valve (PARTNER) Trial Cohort A. Circulation (2013) 128:2776–84. doi: 10.1161/CIRCULATIONAHA.113.003885
3. Nombela-Franco L, Ribeiro HB, Urena M, Allende R, Amat-Santos I, DeLarochelliere R, et al. Significant mitral regurgitation left untreated at the time of aortic valve replacement: a comprehensive review of a frequent entity in the transcatheter aortic valve replacement era. J Am Coll Cardiol. (2014) 63:2643–58. doi: 10.1016/j.jacc.2014.02.573
4. Sannino A, Grayburn PA. Mitral regurgitation in patients with severe aortic stenosis: diagnosis and management. Heart (2018) 104:16–22. doi: 10.1136/heartjnl-2017-311552
5. Figulla HR, Webb JG, Lauten A, Feldman T. The transcatheter valve technology pipeline for treatment of adult valvular heart disease. Eur Heart J. (2016) 37:2226–39. doi: 10.1093/eurheartj/ehw153
6. Lancellotti P, Tribouilloy C, Hagendorff A, Popescu BA, Edvardsen T, Pierard LA, et al. Recommendations for the echocardiographic assessment of native valvular regurgitation: an executive summary from the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging (2013) 14:611–44. doi: 10.1093/ehjci/jet105
7. Lancellotti P, Moura L, Pierard LA, Agricola E, Popescu BA, Tribouilloy C, et al. European Association of Echocardiography recommendations for the assessment of valvular regurgitation. Part 2: mitral and tricuspid regurgitation (native valve disease). Eur J Echocardiogr. (2010) 11:307–32. doi: 10.1093/ejechocard/jeq031
8. Lang RM, Badano LP, Tsang W, Adams DH, Agricola E, Buck T, et al. EAE/ASE recommendations for image acquisition and display using three-dimensional echocardiography. Eur Heart J Cardiovasc Imaging (2012) 13:1–46. doi: 10.1093/ehjci/jer316
9. Grayburn PA, Weissman NJ, Zamorano JL. Quantitation of mitral regurgitation. Circulation (2012) 126:2005–17. doi: 10.1161/CIRCULATIONAHA.112.121590
10. Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, et al. ESC/EACTS Guidelines for the management of valvular heart disease: the task force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. (2017) 38:2739–91. doi: 10.1093/eurheartj/ehx391
11. Zoghbi WA, Adams D, Bonow RO, Enriquez-Sarano M, Foster E, Grayburn PA, et al. Recommendations for noninvasive evaluation of native valvular regurgitation: a report from the american society of echocardiography developed in collaboration with the society for cardiovascular magnetic resonance. J Am Soc Echocardiogr. (2017) 30:303–71. doi: 10.1016/j.echo.2017.01.007
12. Grayburn PA, Carabello B, Hung J, Gillam LD, Liang D, Mack MJ, et al. Defining “severe” secondary mitral regurgitation: emphasizing an integrated approach. J Am Coll Cardiol. (2014) 64:2792–801. doi: 10.1016/j.jacc.2014.10.016
13. Katte F, Franz M, Jung C, Figulla HR, Leistner D, Jakob P, et al. Impact of concomitant mitral regurgitation on transvalvular gradient and flow in severe aortic stenosis: a systematic ex vivo analysis of a subentity of low-flow low-gradient aortic stenosis. EuroIntervention (2018) 13:1635–44. doi: 10.4244/EIJ-D-17-00476
14. Delgado V, Kapadia S, Marsan NA, Schalij MJ, Tuzcu EM, Bax JJ. Multimodality imaging before, during, and after percutaneous mitral valve repair. Heart (2011) 97:1704–14. doi: 10.1136/hrt.2011.227785
15. Feldman T, Foster E, Glower DD, Kar S, Rinaldi MJ, Fail PS, et al. Percutaneous repair or surgery for mitral regurgitation. New Engl J Med. (2011) 364:1395–406. doi: 10.1056/NEJMoa1009355
16. Feldman T, Kar S, Rinaldi M, Fail P, Hermiller J, Smalling R, et al. Percutaneous mitral repair with the MitraClip system: safety and midterm durability in the initial EVEREST (Endovascular Valve Edge-to-Edge REpair Study) cohort. J Am Coll Cardiol. (2009) 54:686–94. doi: 10.1016/j.jacc.2009.03.077
17. Wunderlich NC, Siegel RJ. Peri-interventional echo assessment for the MitraClip procedure. Eur Heart J Cardiovasc Imaging (2013) 14:935–49. doi: 10.1093/ehjci/jet060
18. Blanke P, Naoum C, Webb J, Dvir D, Hahn RT, Grayburn P, et al. Multimodality imaging in the context of transcatheter mitral valve replacement: establishing consensus among modalities and disciplines. J Am Coll Cardiol Cardiovasc Imaging (2015) 8:1191–208. doi: 10.1016/j.jcmg.2015.08.004
19. Eleid MF, Foley TA, Said SM, Pislaru SV, Rihal CS. Severe mitral annular calcification: multimodality imaging for therapeutic strategies and interventions. J Am Coll Cardiol Cardiovasc Imaging (2016) 9:1318–37. doi: 10.1016/j.jcmg.2016.09.001
20. Toggweiler S, Boone RH, Rodes-Cabau J, Humphries KH, Lee M, Nombela-Franco L, et al. Transcatheter aortic valve replacement: outcomes of patients with moderate or severe mitral regurgitation. J Am Coll Cardiol. (2012) 59:2068–74. doi: 10.1016/j.jacc.2012.02.020
21. D'Onofrio A, Gasparetto V, Napodano M, Bianco R, Tarantini G, Renier V, et al. Impact of preoperative mitral valve regurgitation on outcomes after transcatheter aortic valve implantation. Eur J Cardiothorac Surg. (2012) 41:1271–6; discussion 1276–7. doi: 10.1093/ejcts/ezr236
22. Lauten A, Ferrari M, Goebel B, Rademacher W, Schumm J, Uth O, et al. Microvascular tissue perfusion is impaired in acutely decompensated heart failure and improves following standard treatment. Eur J Heart Fail. (2011) 13:711–7. doi: 10.1093/eurjhf/hfr043
23. Absil B, Dagenais F, Mathieu P, Metras J, Perron J, Baillot R, et al. Does moderate mitral regurgitation impact early or mid-term clinical outcome in patients undergoing isolated aortic valve replacement for aortic stenosis? Eur J Cardiothorac Surg. (2003) 24:217–22; discussion 222. doi: 10.1016/S1010-7940(03)00251-3
24. Schubert SA, Yarboro LT, Madala S, Ayunipudi K, Kron IL, Kern JA, Ailawadi G, et al. Natural history of coexistent mitral regurgitation after aortic valve replacement. J Thorac Cardiovasc Surg. (2016) 151:1032–9, 1042 e1. doi: 10.1016/j.jtcvs.2015.12.006
25. Barreiro CJ, Patel ND, Fitton TP, Williams JA, Bonde PN, Chan V, Alejo DE, et al. Aortic valve replacement and concomitant mitral valve regurgitation in the elderly: impact on survival and functional outcome. Circulation (2005) 112:I443–7. doi: 10.1161/CIRCULATIONAHA.104.526046
26. Ruel M, Kapila V, Price J, Kulik A, Burwash IG, Mesana TG. Natural history and predictors of outcome in patients with concomitant functional mitral regurgitation at the time of aortic valve replacement. Circulation (2006) 114:I541–6. doi: 10.1161/CIRCULATIONAHA.105.000976
27. Lauten A, Figulla HR, Mollmann H, Holzhey D, Kotting J, Beckmann A, et al. TAVI for low-flow, low-gradient severe aortic stenosis with preserved or reduced ejection fraction: a subgroup analysis from the German Aortic Valve Registry (GARY). EuroIntervention (2014) 10:850–9. doi: 10.4244/EIJV10I7A145
28. Nombela-Franco L, Eltchaninoff H, Zahn R, Testa L, Leon MB, Trillo-Nouche R, et al. Clinical impact and evolution of mitral regurgitation following transcatheter aortic valve replacement: a meta-analysis. Heart (2015) 101:1395–405. doi: 10.1136/heartjnl-2014-307120
29. Sannino A, Losi MA, Schiattarella GG, Gargiulo G, Perrino C, Stabile E, et al. Meta-analysis of mortality outcomes and mitral regurgitation evolution in 4,839 patients having transcatheter aortic valve implantation for severe aortic stenosis. Am J Cardiol. (2014) 114:875–82. doi: 10.1016/j.amjcard.2014.06.022
30. Zahn R, Gerckens U, Linke A, Sievert H, Kahlert P, Hambrecht R, et al. Predictors of one-year mortality after transcatheter aortic valve implantation for severe symptomatic aortic stenosis. Am J Cardiol. (2013) 112:272–9. doi: 10.1016/j.amjcard.2013.03.024
31. Bedogni F, Latib A, De Marco F, Agnifili M, Oreglia J, Pizzocri S, et al. Interplay between mitral regurgitation and transcatheter aortic valve replacement with the CoreValve Revalving System: a multicenter registry. Circulation. (2013) 128:2145–53. doi: 10.1161/CIRCULATIONAHA.113.001822
32. Cortes C, Amat-Santos IJ, Nombela-Franco L, Munoz-Garcia AJ, Gutierrez-Ibanes E, De La Torre Hernandez JM, et al. Mitral regurgitation after transcatheter aortic valve replacement: prognosis, imaging predictors, and potential management. J Am Coll Cardiol Cardiovasc Interv. (2016) 9:1603–14. doi: 10.1016/j.jcin.2016.05.025
33. O'Sullivan CJ, Stortecky S, Butikofer A, Heg D, Zanchin T, Huber C, et al. Impact of mitral regurgitation on clinical outcomes of patients with low-ejection fraction, low-gradient severe aortic stenosis undergoing transcatheter aortic valve implantation. Circ Cardiovasc Interv. (2015) 8:e001895. doi: 10.1161/CIRCINTERVENTIONS.114.001895
34. Selle A, Figulla HR, Ferrari M, Rademacher W, Goebel B, Hamadanchi A, et al. Impact of rapid ventricular pacing during TAVI on microvascular tissue perfusion. Clin Res Cardiol. (2014) 103:902–11. doi: 10.1007/s00392-014-0728-9
35. Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. New Engl J Med. (2010) 363:1597–607. doi: 10.1056/NEJMoa1008232
36. Iung B, Baron G, Butchart EG, Delahaye F, Gohlke-Barwolf C, Levang OW, et al. A prospective survey of patients with valvular heart disease in Europe: the Euro Heart Survey on Valvular Heart Disease. Eur Heart J. (2003) 24:1231–43. doi: 10.1016/S0195-668X(03)00201-X
37. Mihaljevic T, Gillinov AM, Sabik JF III. Functional ischemic mitral regurgitation: myocardial viability as a predictor of postoperative outcome after isolated coronary artery bypass grafting. Circulation (2009) 120:1459–61. doi: 10.1161/CIRCULATIONAHA.109.893347
38. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. (2016) 37:2129–200. doi: 10.1093/eurheartj/ehw128
39. Siminiak T, Hoppe UC, Schofer J, Haude M, Herrman JP, Vainer J, et al. Effectiveness and safety of percutaneous coronary sinus-based mitral valve repair in patients with dilated cardiomyopathy (from the AMADEUS trial). Am J Cardiol. (2009) 104:565–70. doi: 10.1016/j.amjcard.2009.04.021
40. Siminiak T, Wu JC, Haude M, Hoppe UC, Sadowski J, Lipiecki J, et al. Treatment of functional mitral regurgitation by percutaneous annuloplasty: results of the TITAN Trial. Eur J Heart Fail. (2012) 14:931–8. doi: 10.1093/eurjhf/hfs076
41. Glower DD, Kar S, Trento A, Lim DS, Bajwa T, Quesada R, et al. Percutaneous mitral valve repair for mitral regurgitation in high-risk patients: results of the EVEREST II study. J Am Coll Cardiol. (2014) 64:172–81. doi: 10.1016/j.jacc.2013.12.062
42. Chakravarty T, Van Belle E, Jilaihawi H, Noheria A, Testa L, Bedogni F, et al. Meta-analysis of the impact of mitral regurgitation on outcomes after transcatheter aortic valve implantation. Am J Cardiol. (2015) 115:942–9. doi: 10.1016/j.amjcard.2015.01.022
43. Coutinho GF, Correia PM, Pancas R, Antunes MJ. Management of moderate secondary mitral regurgitation at the time of aortic valve surgery. Eur J Cardiothorac Surg. (2013) 44:32–40. doi: 10.1093/ejcts/ezs676
44. Almasood A, Al Ahmari S, El-Shurafa H, Alotaibi M, Al Kasab S, AlAbdallah M, et al. The change in mitral regurgitation severity after trans-catheter aortic valve implantation. J Saudi Heart Assoc. (2015) 27:10–7. doi: 10.1016/j.jsha.2014.05.002
45. Shibayama K, Harada K, Berdejo J, Mihara H, Tanaka J, Gurudevan SV, et al. Effect of transcatheter aortic valve replacement on the mitral valve apparatus and mitral regurgitation: real-time three-dimensional transesophageal echocardiography study. Circ Cardiovasc Imaging. (2014) 7:344–51. doi: 10.1161/CIRCIMAGING.113.000942
46. Galloway AC, Grossi EA, Baumann FG, LaMendola CL, Crooke GA, Harris LJ, et al. Multiple valve operation for advanced valvular heart disease: results and risk factors in 513 patients. J Am Coll Cardiol. (1992) 19:725–32. doi: 10.1016/0735-1097(92)90509-L
47. Yoon SH, Whisenant BK, Bleiziffer S, Delgado V, Schofer N, Eschenbach L, et al. Transcatheter mitral valve replacement for degenerated bioprosthetic valves and failed annuloplasty rings. J Am Coll Cardiol. (2017) 70:1121–1131. doi: 10.1016/j.jacc.2017.07.714
48. Yaryura R, Rehman A, Morsli H, Hussain N. Transcatheter aortic and mitral valve replacement in a patient with critical aortic and mitral valve in-ring stenosis. JACC Cardiovasc Interv. (2015) 8:e155–7. doi: 10.1016/j.jcin.2015.03.040
49. Weich H, Janson J, Pecoraro A, van Wyk J, Rocher A, Dempers J, et al. First case of transcatheter native mitral and aortic valve replacement. EuroIntervention (2016) 12:1196. doi: 10.4244/EIJV12I9A195
50. Rudolph V, Schirmer J, Franzen O, Schluter M, Seiffert M, Treede H, et al. Bivalvular transcatheter treatment of high-surgical-risk patients with coexisting severe aortic stenosis and significant mitral regurgitation. Int J Cardiol. (2013) 167:716–20. doi: 10.1016/j.ijcard.2012.03.060
51. Puls M, Seipelt R, Schillinger W. Complete interventional heart repair of multiple concomitant cardiac pathologies in a staged approach. Catheter Cardiovasc Interv. (2013) 81:896–900. doi: 10.1002/ccd.24448
52. Maisano F, Alfieri O, Banai S, Buchbinder M, Colombo A, Falk V, et al. The future of transcatheter mitral valve interventions: competitive or complementary role of repair vs. replacement? Eur Heart J. (2015) 36:1651–9. doi: 10.1093/eurheartj/ehv123
53. Braun D, Lesevic H, Orban M, Michalk F, Barthel P, Hoppe K, et al. Percutaneous edge-to-edge repair of the mitral valve in patients with degenerative versus functional mitral regurgitation. Catheter Cardiovasc Interv. (2014) 84:137–46. doi: 10.1002/ccd.25331
54. Attizzani GF, Ohno Y, Capodanno D, Cannata S, Dipasqua F, Imme S, et al. Extended use of percutaneous edge-to-edge mitral valve repair beyond EVEREST (Endovascular Valve Edge-to-Edge Repair) criteria: 30-day and 12-month clinical and echocardiographic outcomes from the GRASP (Getting Reduction of Mitral Insufficiency by Percutaneous Clip Implantation) registry. J Am Coll Cardiol Cardiovasc Interv. (2015) 8:74–82. doi: 10.1016/j.jcin.2014.07.024
55. Schofer J, Siminiak T, Haude M, Herrman JP, Vainer J, Wu JC, et al. Percutaneous mitral annuloplasty for functional mitral regurgitation: results of the CARILLON Mitral Annuloplasty Device European Union Study. Circulation (2009) 120:326–33. doi: 10.1161/CIRCULATIONAHA.109.849885
56. Maisano F, La Canna G, Latib A, Denti P, Taramasso M, Kuck KH, Colombo A, et al. First-in-man transseptal implantation of a “surgical-like” mitral valve annuloplasty device for functional mitral regurgitation. J Am Coll Cardiol Cardiovasc Interv. (2014) 7:1326–8. doi: 10.1016/j.jcin.2014.08.003
57. Rodes-Cabau J. Transcatheter mitral valve replacement: first steps on a long road. J Am Coll Cardiol. (2018) 71:22–4. doi: 10.1016/j.jacc.2017.11.015
58. Regueiro A, Granada JF, Dagenais F, Rodes-Cabau J. Transcatheter mitral valve replacement: insights from early clinical experience and future challenges. J Am Coll Cardiol. (2017) 69:2175–92. doi: 10.1016/j.jacc.2017.02.045
59. Bapat V, Rajagopal V, Meduri C, Farivar RS, Walton A, Duffy SJ, et al. Early experience with new transcatheter mitral valve replacement. J Am Coll Cardiol. (2018) 71:12–21. doi: 10.1016/j.jacc.2017.10.061
60. Wilbring M, Alexiou K, Tugtekin SM, Arzt S, Ibrahim K, Matschke K, et al. Pushing the limits-further evolutions of transcatheter valve procedures in the mitral position, including valve-in-valve, valve-in-ring, and valve-in-native-ring. J Thorac Cardiovasc Surg. (2014) 147:210–9. doi: 10.1016/j.jtcvs.2013.09.021
61. D'Ancona G, Paranskaya L, Oner A, Kische S, Ince H. Mitro-aortic pathology: a point of view for a fully transcatheter staged approach. Neth Heart J. (2017) 25:605–8. doi: 10.1007/s12471-017-1028-6
62. D'Ancona G, Kische S, Senges J, Ouarrak T, Puls M, Bekeredjian R, et al. Combined mitro-aortic pathology: impact of previous aortic valve replacement upon outcomes of MitraClip therapy (from the German transcatheter mitral valve interventions registry). EuroIntervention (2017) 13:475–82. doi: 10.4244/EIJ-D-17-00222
63. Reynolds MR, Magnuson EA, Wang K, Lei Y, Vilain K, Walczak J, et al. Cost-effectiveness of transcatheter aortic valve replacement compared with standard care among inoperable patients with severe aortic stenosis: results from the placement of aortic transcatheter valves (PARTNER) trial (Cohort B). Circulation (2012) 125:1102–9. doi: 10.1161/CIRCULATIONAHA.111.054072
64. Reynolds MR, Magnuson EA, Lei Y, Wang K, Vilain K, Li H, et al. Cost-effectiveness of transcatheter aortic valve replacement compared with surgical aortic valve replacement in high-risk patients with severe aortic stenosis: results of the PARTNER (Placement of Aortic Transcatheter Valves) trial (Cohort A). J Am Coll Cardiol. (2012) 60:2683–92. doi: 10.1016/j.jacc.2012.09.018
65. Reynolds MR, Baron SJ, Cohen DJ. Economic implications of transcatheter aortic valve replacement in patients at intermediate surgical risk. Circulation (2016) 134:1416–8. doi: 10.1161/CIRCULATIONAHA.116.021962
66. Tam DY, Hughes A, Wijeysundera HC, Fremes SE. The cost-effectiveness of self-expandable transcatheter aortic valves in intermediate risk patients. Ann Thorac Surg. (2018). doi: 10.1016/j.athoracsur.2018.03.069. [Epub ahead of print].
67. Armeni P, Boscolo PR, Tarricone R, Capodanno D, Maggioni AP, Grasso C, et al. Real-world cost effectiveness of MitraClip combined with medical therapy versus medical therapy alone in patients with moderate or severe mitral regurgitation. Int J Cardiol. (2016) 209:153–60. doi: 10.1016/j.ijcard.2016.01.212
Keywords: transcatheter aortic vave replacement, mitral valve insufficiency, mitral valve repair, aortic stenosis, aortic valve, mitral valve
Citation: Stähli BE, Reinthaler M, Leistner DM, Landmesser U and Lauten A (2018) Transcatheter Aortic Valve Replacement and Concomitant Mitral Regurgitation. Front. Cardiovasc. Med. 5:74. doi: 10.3389/fcvm.2018.00074
Received: 30 March 2018; Accepted: 30 May 2018;
Published: 19 June 2018.
Edited by:
Maurizio Taramasso, UniversitätsSpital Zürich, SwitzerlandReviewed by:
Masahiko Asami, Bern University Hospital, SwitzerlandPaolo Denti, San Raffaele Hospital (IRCCS), Italy
Copyright © 2018 Stähli, Reinthaler, Leistner, Landmesser and Lauten. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Barbara E. Stähli, YmFyYmFyYS1lbGlzYWJldGguc3RhZWhsaUBjaGFyaXRlLmRl