 Gabriela Lopes Martins1
Gabriela Lopes Martins1 Rita Carolina Figueiredo Duarte1Érica Leandro Marciano Vieira1
Rita Carolina Figueiredo Duarte1Érica Leandro Marciano Vieira1 Natalia Pessoa Rocha2
Natalia Pessoa Rocha2 Estêvão Lanna Figueiredo3Francisco Rezende Silveira4José Raymundo Sollero Caiaffa5Rodrigo Pinheiro Lanna4Maria das Graças Carvalho1
Estêvão Lanna Figueiredo3Francisco Rezende Silveira4José Raymundo Sollero Caiaffa5Rodrigo Pinheiro Lanna4Maria das Graças Carvalho1 András Palotás6,7*Cláudia Natália Ferreira1
András Palotás6,7*Cláudia Natália Ferreira1 Helton José Reis1*
Helton José Reis1*- 1Neurofar Laboratory, Departamento de Farmacologia, ICB, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
- 2Department of Neurology, The University of Texas Health Science Center at Houston, Houston, TX, United States
- 3Hospital Lifecenter, Belo Horizonte, Brazil
- 4Hospital Semper, Belo Horizonte, Brazil
- 5Centro de Especialidades Médicas Ipsemg, Belo Horizonte, Brazil
- 6Asklepios-Med, Szeged, Hungary
- 7Kazan Federal University, Kazan, Russia
Background: Atrial fibrillation (AF) is the most common arrhythmia associated with high risk of venous thromboembolism. Inflammatory mechanisms may be involved in the pathophysiology of AF and in the AF-related thrombogenesis, and patients with AF might benefit from the use of anticoagulants with anti-inflammatory properties. However, the evidence is still scarce, and it points out the need of trials seeking to investigate the levels of inflammatory mediators in patients with AF under different anticoagulant therapies. Therefore, this study was designed to define whether patients with AF treated either with an activated coagulation factor X (FXa) inhibitor (rivaroxaban) or with a vitamin K inhibitor (warfarin) present changes in peripheral levels of inflammatory mediators, mainly cytokines and chemokines.
Methods: A total of 127 subjects were included in this study, divided into three groups: patients with non-valvular atrial fibrillation (NVAF) using warfarin (N = 42), patients with NVAF using rivaroxaban (N = 29), and controls (N = 56). Plasma levels of inflammatory mediators were quantified by immunoassays.
Results: Patients with AF (both warfarin and rivaroxaban groups) presented increased levels of inflammatory cytokines in comparison with controls. The use of rivaroxaban was associated with decreased levels of inflammatory cytokines in comparison with warfarin. On the other hand, patients with AF using rivaroxaban presented increased levels of the chemokines (MCP-1 in comparison with warfarin users; MIG and IP-10 in comparison with controls).
Conclusions: AF is associated with an inflammatory profile that was less pronounced in patients on rivaroxaban in comparison with warfarin users. Further studies are necessary to assess the clinical implications of our results and whether patients with AF would benefit from rivaroxaban anti-inflammatory effects.
Introduction
Atrial fibrillation (AF) is the most frequent cardiac arrhythmia in clinical practice. AF prevalence is estimated to be about 1–2% in the general population, increasing significantly with age (1). AF is associated with a considerable risk of mortality and morbidity due to venous thromboembolism (VTE). People with AF have increased risk of mortality compared to those without it, as demonstrated by the Framingham Heart Study (2). Noteworthy, AF remained significantly associated with an increased risk of death even after controlling for cardiovascular comorbidities (2, 3). AF is also associated with an estimated incremental cost of US$18,601 in hospital and clinical care in the year after diagnosis, even after accounting for age, time period, and comorbidities (4).
For clinical risk stratification, the CHA2DS2-VASc1 score has been widely accepted for predicting VTE in patients with AF and used as a surrogate for starting anticoagulant therapy based on the individuals' assessment (5–8). Warfarin is an inhibitor of vitamin K activity, being highly effective in preventing stroke and VTE in patients with AF and is the most used oral anticoagulant in clinical practice (9). However, due to the narrow therapeutic index and interactions with several drugs and foods, warfarin use requires frequent coagulation monitoring and dose adjustment (10). As an attempt to mitigate this problem, new oral anticoagulants have been developed, including rivaroxaban, which is a direct inhibitor of the activated coagulation factor X (FXa). Rivaroxaban has been proved to be non-inferior to warfarin in preventing stroke and VTE, with the great advantage of providing a more consistent and predictable pharmacological profile (11). FXa may play an important role in the activation of inflammatory responses (12), thus yielding another potential advantage of anti-FXa drugs, i.e., their anti-inflammatory effects (13, 14).
Inflammatory responses, as evidenced by increased circulating levels of inflammatory mediators such as C-reactive protein (CRP), promote the persistence of AF (15, 16). In addition, the number of T lymphocytes and monocytes/macrophages is increased in the atrial myocardium of patients with AF (17). Regarding thrombus formation, higher plasma levels of CRP and interleukin (IL)-6 have been independently associated with stroke risk (18–20). Taken together, these data demonstrate that patients with AF might benefit from the use of anticoagulants with anti-inflammatory properties. Accordingly, a recent study has demonstrated that the treatment with rivaroxaban (43–98 days, depending on cardioconversion) was associated with reductions in both CRP and IL-6 in comparison with baseline levels (21). However, the evidence is still scarce, and it points out the need for trials seeking to investigate the levels of inflammatory mediators in patients with AF under different anticoagulant therapies. Therefore, this study was designed to define whether patients with AF treated with rivaroxaban (FXa inhibitor) or warfarin (vitamin K inhibitor) present changes in peripheral levels of inflammatory mediators, mainly cytokines and chemokines. We hypothesize that the use of rivaroxaban is associated with a decrease in the levels of inflammatory mediators.
Methods
Study Population
A total of 127 participants were enrolled in the study, 71 patients with non-valvular atrial fibrillation (NVAF) and 56 controls with comparable age and sex distribution. Participants were recruited from the outpatient clinics of the Hospitals Lifecenter, Semper, and Ipsemg (Belo Horizonte, Minas Gerais, Brazil). Patients were selected if they (i) presented with a history of AF, whose diagnosis was confirmed by electrocardiography, and (ii) had a prescription for chronic oral anticoagulation (CHA2DS2-VASC ≥ 2). Patients with AF were further categorized according to anticoagulant treatment: N = 42 were on warfarin with international normalized ratio (INR) between 2.00 and 3.00, and N = 29 were on rivaroxaban treatment, at a dose of 20 mg once daily. Controls were recruited from the local community and consist of a group of individuals with no previous diagnosis of AF or use of any anticoagulant drug.
Subjects were excluded if they have used any antiplatelet agent, non-steroidal anti-inflammatory drugs, heparin, hormone replacement therapy, antifibrinolytics, amiodarone, verapamil, quinidine, azole antifungals, and ritonavir in the 4 weeks prior to the study. In addition, participants with current diagnosis of alcohol use disorder; chronic kidney disease (creatinine clearance <30 ml/min); severe dyslipidemia; acquired or hereditary bleeding disorders; liver disease; thyroid disease; infectious, inflammatory, autoimmune, and malignant diseases; pregnancy; puerperium; and breast-feeding were excluded from this study.
The present study was approved by the Research Ethics Committees of Universidade Federal de Minas Gerais (UFMG–CAAE: 12603413.0.0000.5149), Lifecenter, Semper, and Ipsemg Hospitals and was performed in accordance with the principles provided in the Declaration of Helsinki. All participants received information about the research, and read and signed a written informed consent prior to any study procedures.
Biological Samples
Peripheral blood samples were drawn by venipuncture into tubes containing ethylenediamine tetraacetic acid (EDTA) and into tubes without anticoagulant in the Hospitals Lifecenter, Semper, and Ipsemg. Plasma and serum samples were obtained by centrifuging blood at 1,100 g for 15 min, at 25°C, within 4 h of collection. The samples were labeled and stored in aliquots at −80°C until analysis.
Laboratory Characterization
Serum samples were used for the assessment of the following biochemical markers: CRP, total cholesterol, high-density lipoprotein (HDL), low-density lipoprotein (LDL), triglycerides, aspartate transaminase (AST), alanine aminotransferase (ALT), gamma-glutamyl transferase (GGT), creatinine, and uric acid, using a Vitros 250 system (Johnson & Johnson®) in the Laboratory of Hospital Risoleta Tolentino Neves (Belo Horizonte, Minas Gerais, Brazil). In addition, white blood cell (WBC) count was assessed in whole blood samples by using the Coulter T-890® hematological analyzer in the Laboratório de Hematologia Clínica, Faculdade de Farmácia, UFMG.
Analysis of Inflammatory Mediators
Plasma samples were used for the assessment of inflammatory markers by Cytometric Bead Array (CBA, BD Bioscience, San Diego, CA, USA), using the following kits: Cytokines Th1/Th2 [IL-2, IL-4, IL-10, tumor necrosis factor (TNF), and interferon-gamma (IFN-γ)], Chemokines [CCL5/regulated on activation, normal T cell expressed and secreted (RANTES), CXCL9/monokine induced by interferon-gamma (MIG), CCL2/monocyte chemoattractant protein (MCP)-1, CXCL10/interferon-gamma-induced protein (IP)-10], and human transforming growth factor-beta (TGF-β)-1 Single Plex Flex Set. In addition, multiplex immunoassay (Merck Millipore, Billerica, MA, USA) was used to assess the levels of cardiovascular disease-related proteins, using the Human Cardiovascular Disease-Panel II kit [a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13 (ADAMTS13), growth differentiation factor (GDF)-15, myoglobin, soluble intercellular adhesion molecule (sICAM)-1, p-selectin, neutrophil gelatinase-associated lipocalin (lipocalin-2/NGAL), soluble vascular cell adhesion protein (sVCAM)-1, and serum amyloid A (SAA)].
Statistical Analyses
Associations between categorical variables were assessed by the Pearson chi-square test. The Shapiro–Wilk normality test was used to assess whether or not the continuous variables follow a normal distribution. Three groups (warfarin vs. rivaroxaban vs. controls) were compared using the one-way ANOVA or the Kruskal–Wallis test, when data were determined to follow or not a normal distribution. Significant results for three-group comparisons were followed by post hoc analyses (Tukey's or Dunn's pairwise comparisons, in case of ANOVA or Kruskal–Wallis test, respectively). Significant values have been adjusted by the Bonferroni correction for multiple tests. All statistical tests were two-tailed and a significance level of p < 0.05 was set. Statistical analyses were performed using SPSS software version 25.0 (SPSS Inc., Chicago, IL, USA).
Results
Demographic, Clinical, and Laboratory Characteristics
Demographic, clinical, and laboratory characteristics of participants enrolled in this study are shown in Table 1. There were no differences between groups regarding age, sex, diagnosis of type II diabetes mellitus. The frequency of hypertension was higher among patients with AF (both warfarin and rivaroxaban groups) in comparison with controls. The percentage of patients using statins was higher in the warfarin group, in comparison with controls and with patients on rivaroxaban. There was no significant difference between patients on warfarin or rivaroxaban regarding the CHA2DS2-VASc score. Only 6 out of the 127 participants reported tobacco use (3/56 controls, 1/42 patients with AF on warfarin, and 2/29 patients on rivaroxaban). Due to the low expected frequencies, chi-square analysis for smoking status was not appropriate.
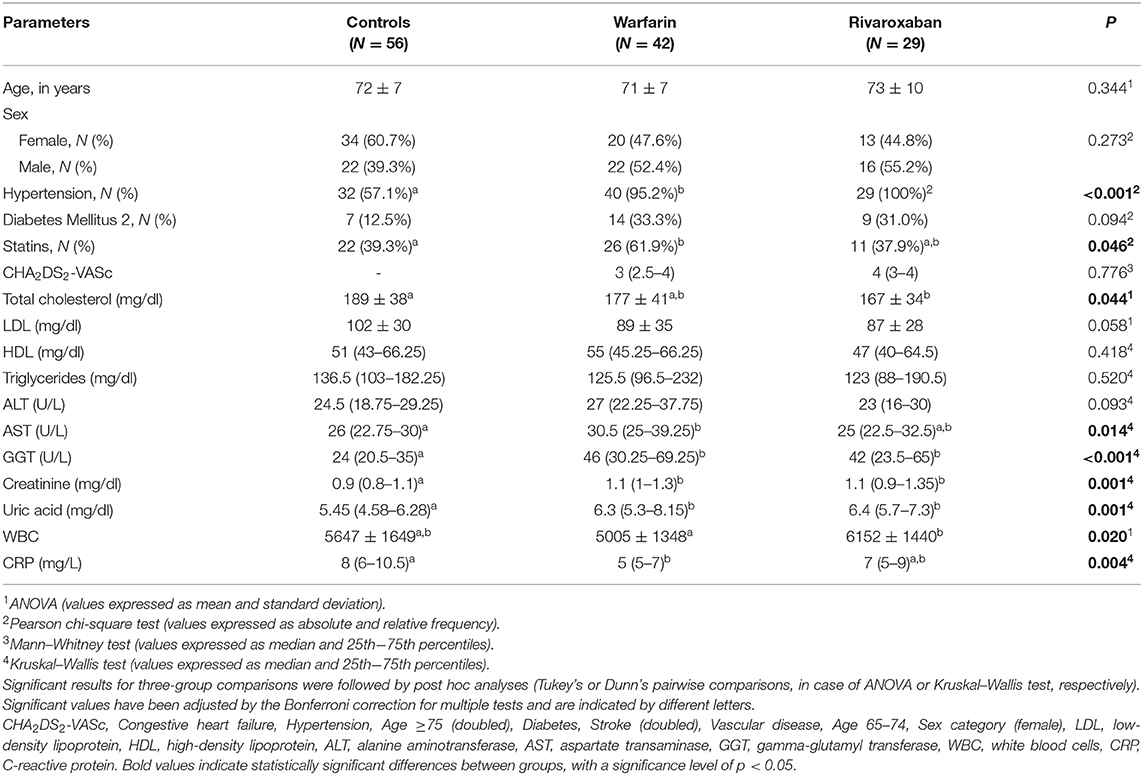
Table 1. Demographic, clinical, and laboratory characteristics of participants.
Table 1 shows the mixed array of biochemical markers in the three groups of participants. It also shows that patients on warfarin presented lower levels of CRP compared to controls. In addition, patients on rivaroxaban showed higher values in WBC count compared to the warfarin group. Of note, these parameters were determined in order to exclude patients presenting with acute inflammatory response and/or severe dyslipidemia or liver disease.
Evaluation of Inflammatory Mediators
Increased levels of inflammatory cytokines were found in individuals with AF in comparison with controls. Patients on warfarin, compared with those on rivaroxaban and controls, presented with increased plasma levels of IL-2, IL-4, IL-10, TNF, and IFN-γ. Moreover, increased levels of these markers were found in the rivaroxaban group in comparison with controls (Figures 1A–E, respectively). Regarding the cardiovascular disease-related proteins, patients on warfarin and rivaroxaban presented similar levels of GDF-15 and both groups higher than controls (Figure 1F).

Figure 1. Plasma levels of inflammatory cytokines IL-2 (A), IL-4 (B), IL-10 (C), TNF (D), IFN-γ (E), and GDF-15 (F), comparing control (N = 56), warfarin (N = 42), and rivaroxaban (N = 29) groups. The dosage of IL-2, IL-4, IL-10, TNF, and IFN-γ was performed by Cytometric Bead Array; GDF-15, by Multiplex Immunoassay. The groups were compared by the Kruskal–Wallis test followed by Dunn's multiple comparison test. Significant values have been adjusted by the Bonferroni correction for multiple tests and are indicated by different letters. The horizontal bars show the mean and the standard error of the mean. IL, interleukin; TNF, tumor necrosis factor; IFN-γ, interferon-gamma; GDF-15, growth differentiation factor-15.
On the other hand, the rivaroxaban group had significantly higher levels of MCP-1 in comparison with the warfarin group (Figure 2A). In addition, patients on rivaroxaban presented increased levels of MIG and IP-10 in comparison with controls (Figures 2B,C).
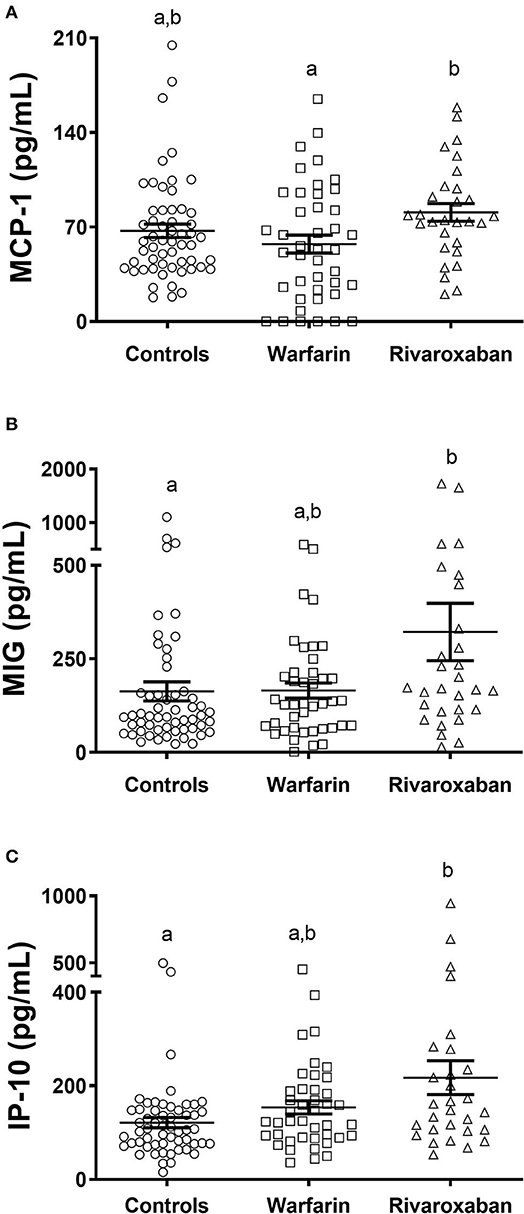
Figure 2. Plasma levels of inflammatory chemokines MCP-1 (A), MIG (B), and IP-10 (C), comparing control (N = 56), warfarin (N = 42), and rivaroxaban (N = 29) groups. The dosage of these markers was performed by Cytometric Bead Array. The groups were compared by the Kruskal–Wallis test followed by Dunn's multiple comparison test. Significant values have been adjusted by the Bonferroni correction for multiple tests and are indicated by different letters. The horizontal bars show the mean and the standard error of the mean. MCP-1, monocyte chemoattractant protein-1; MIG, monokine induced by interferon-gamma; IP-10, interferon-gamma-induced protein.
For the other analyzed parameters (RANTES, TGF-β, ADAMTS13, myoglobin, sICAM-1, p-selectin, lipocalin-2/NGAL, sVCAM-1, and SAA), no significant differences were found when comparing the three groups (data not shown).
Discussion
In the current study, we evaluated plasma levels of inflammatory mediators in patients with AF on two different anticoagulant therapies, i.e., warfarin and rivaroxaban. Previous studies have demonstrated that in addition to the anticoagulant effects, FXa inhibitors such as rivaroxaban have anti-inflammatory properties (12, 13). We then hypothesized that rivaroxaban would be associated with decreased levels of inflammatory cytokines. We found that patients with AF (both warfarin and rivaroxaban groups) presented increased levels of inflammatory cytokines in comparison with controls. Corroborating our hypothesis, the use of rivaroxaban was associated with decreased levels of inflammatory cytokines in comparison with warfarin (Figure 1). Interestingly, patients with AF using rivaroxaban presented increased levels of the chemokines [MCP-1 in comparison with warfarin users; MIG and IP-10 in comparison with controls (Figure 2)].
Our results are in line with findings from previous studies, which reported increased plasma levels of inflammatory cytokines in patients with AF (22–25). Inflammatory mechanisms have been associated with the pathogenesis and maintenance of AF, as well as in the AF-related thrombogenesis (19). Furthermore, comorbidities shared by AF and increased risk of stroke, such as hypertension and diabetes, are also associated with inflammation (26). Thus, it is reasonable to hypothesize that patients with AF would benefit from drugs exerting anti-inflammatory properties.
IL-2 is a pro-inflammatory cytokine produced by T-helper type 1 (Th1) lymphocytes, which can activate T and natural killer (NK) cells and plays a crucial role in the regulation of T cells (25, 27). In a previous study, this cytokine was considered an independent predictive factor for recurrence of AF, once elevated plasma levels of IL-2 were detected in patients with AF who presented recurrence of AF after catheter ablation therapy, in comparison with control subjects in sinus rhythm (28). IL-4, in turn, is a cytokine expressed and produced by activated T-helper type 2 (Th2) lymphocytes and basophils, which has regulatory actions on allergic responses, as well as anti-tumor and anti-inflammatory effects (22). This mediator was considered as a predictive marker of the incidence of AF since high levels of this cytokine were found in patients admitted to the hospital with AF in comparison with controls (22). IL-10, an anti-inflammatory cytokine produced by monocytes and Th2 lymphocytes, and IFN-γ, an immunomodulatory cytokine produced by NK cells and Th1 lymphocytes, were associated with the development of AF after coronary artery bypass grafting (24). Finally, TNF, a pro-inflammatory cytokine synthesized by monocytes, macrophages, and Th1 lymphocytes, has been described as a predictive factor for the development of ischemic stroke in patients with chronic NVAF (29). Our results showed that the increase in levels of these cytokines in patients with AF was blunted in the rivaroxaban group, thus concluding that the use of this drug may be beneficial over warfarin in the context of inflammatory mechanisms.
The anti-inflammatory effects of FXa inhibitors were further demonstrated by a study in which the 6-months treatment with rivaroxaban or apixaban reduced the values of pentraxin-related protein (PTX-3), a protein produced primarily by macrophages and endothelial vasculature cells in response to early pro-inflammatory signals. The authors then suggested that PTX-3 would respond rapidly to endothelial changes in the left atrium and vessels, serving as a useful marker to determine the anti-inflammatory effect of FXa inhibitors (13). The anti-inflammatory activity of rivaroxaban was found to be associated with the inhibition of FXa-activated inflammatory response. When human atrial tissue slices were exposed to FXa, the expression of ICAM-1 and IL-8 increased. The combination of rapid pacing and FXa (mimicking AF) has promoted the significant up-regulation of the protease-activated receptor (PAR-1), PAR-2, ICAM-1, and IL-8. Rivaroxaban prevented the up-regulation of PARs, ICAM-1, and IL-8. In summary, these results indicate that FXa mediates inflammatory signaling in atrial tissue, possibly by the activation of protease-activated receptors (12). Considering the evidence that FXa can bind to PARs, activating them (30), the potential anti-inflammatory effect of rivaroxaban may be because of a direct FXa inhibition.
Contrary to the cytokines, the levels of chemokines were higher in rivaroxaban users in comparison with warfarin (MCP-1) and controls (MIG and IP-10, Figure 2). Chemokines are chemoattractant cytokines that play a vital role in cell migration to the damaged tissue, needed for after-injury remodeling. MCP-1 is a chemokine produced by several cell types, either constitutively or after induction by oxidative stress, cytokines, or growth factors. MCP-1 acts as a potent chemotactic factor for monocytes/macrophages, and it has been associated with cardiac fibrosis and remodeling in ischemic cardiomyopathy, and after myocardial infarction (31). This may be due to its effects on the recruitment and activation of mononuclear cells and fibroblast progenitors, with subsequent release of collagen, fibronectin, and other extracellular matrix components (32). The inhibition of MCP-1 in infarcted mice has been shown to impair the myocardial repair process after injury (33). MCP-1 appears to be involved not only in cell recruitment but also in the modulation of cardiac homeostasis after injury (34). Regarding IP-10, this is a chemokine with pro-inflammatory, anti-angiogenic, and anti-fibrotic properties. It was demonstrated that IP-10 is up-regulated in myocardial infarction in mice, acting as an inhibitor of growth factor-induced fibroblast migration, which protects the heart from excessive fibrotic remodeling (35, 36). In the same way, MIG is a pro-inflammatory chemokine induced by IFN-γ, with proven anti-fibrotic effects in in vitro liver cells (37). Therefore, the increase in chemokine levels observed in the rivaroxaban group can be regarded as beneficial, as chemokines are vital for tissue remodeling and resolution of inflammatory responses. Further investigations are required to evaluate if the use of rivaroxaban is directly associated with an increase of plasmatic levels of these chemokines in patients with AF and the related clinical implications.
Study Limitations
The results of the current study should be interpreted taking into account its limitations. First, our results cannot be extrapolated to patients with AF using other oral anticoagulants. Second, the use of other drugs (such as antihypertensive and oral hypoglycemic agents) was very common in our sample, and it cannot be terminated for the sake of scientific research for obvious ethical considerations. Therefore, the observed findings might also be influenced by their ongoing treatments. Third, the fact the data were not normally distributed (even after attempts to data transformation) prevented the use of more sophisticated analyses. Lastly, the sample size and the cross-sectional design hampered any statements about the potential anti-inflammatory effect of rivaroxaban and the clinical implications of our results. Prospective studies with larger sample size are needed to validate the current findings.
Conclusion
We demonstrated that patients with AF presented with increased levels of inflammatory cytokines. This profile was different when we compared patients treated with warfarin or rivaroxaban. It is possible that rivaroxaban has a potential anti-inflammatory effect. However, the cross-sectional nature of our study prevents this assumption. Further prospective studies involving a greater number of participants are required to confirm the effects of oral anticoagulants in relation to the inflammatory response in individuals with AF. Altogether, our results point to new perspectives for the treatment of patients AF with oral anticoagulants with anti-inflammatory effects.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee from UFMG. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
GM, CF, and HR worked on the conception and organization of the research project. Material preparation, data collection, and analysis were performed by GM, CF, RD, ÉV, NR, EF, FS, JC, and RL. GM wrote the first draft of the manuscript. RD, ÉV, NR, EF, FS, JC, RL, MC, AP, CF, and HR reviewed the manuscript. All authors read and approved the final version of the manuscript.
Funding
This work was supported by Fundação de Amparo à Pesquisa do Estado de Minas Gerais [APQ 02196-16] and Conselho Nacional de Desenvolvimento Científico e Tecnológico [304.779/2014-8].
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to thank the study participants for their immeasurable contribution and the Brazilian government research-funding agencies: Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG), Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), and Pró-Reitoria de Pesquisa (PRPq)-UFMG. GM is currently a Ph.D. student CNPq fellowship recipient. HR was a CNPq fellowship recipient.
Footnotes
1. ^Congestive heart failure, Hypertension, Age ≥75 (doubled), Diabetes mellitus, prior Stroke/transient ischemic attack/thromboembolism (doubled), Vascular disease, Age 65–74, Sex category (female).
References
1. Chugh SS, Havmoeller R, Narayanan K, Singh D, Rienstra M, Benjamin EJ, et al. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 study. Circulation. (2014) 129:837–47. doi: 10.1161/CIRCULATIONAHA.113.005119
2. Benjamin EJ, Wolf PA, D'Agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham heart study. Circulation. (1998) 98:946–52. doi: 10.1161/01.CIR.98.10.946
3. Bassand J-P, Virdone S, Goldhaber SZ, Camm AJ, Fitzmaurice DA, Fox KA, et al. Early risks of death, stroke/systemic embolism, and major bleeding in patients with newly diagnosed atrial fibrillation: results from the GARFIELD-AF registry. Circulation. (2019) 139:787–98. doi: 10.1161/CIRCULATIONAHA.118.035012
4. Delaney JA, Yin X, Fontes JD, Wallace ER, Skinner A, Wang N, et al. Hospital and clinical care costs associated with atrial fibrillation for medicare beneficiaries in the cardiovascular health study and the Framingham heart study. SAGE Open Med. (2018) 6:2050312118759444. doi: 10.1177/2050312118759444
5. January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, et al. 2019 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American college of cardiology/American heart association task force on practice guidelines and the heart rhythm society. J Am Coll Cardiol. (2014) 64:104–32. doi: 10.1016/j.jacc.2019.01.011
6. Wann LS, Curtis AB, January CT, Ellenbogen KA, Lowe JE, Estes NA 3rd, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (Updating the 2006 Guideline): a report of the American college of cardiology foundation/American heart association task force on practice guidelines. Circulation. (2011) 123:104–23. doi: 10.1161/CIR.0b013e3181fa3cf4
7. Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. (2010) 137:263–72. doi: 10.1378/chest.09-1584
8. Sulzgruber P, Wassmann S, Semb AG, Doehner W, Widimsky P, Gremmel T, et al. Oral anticoagulation in patients with non-valvular atrial fibrillation and a CHA2DS2-VASc score of 1: a current opinion of the European society of cardiology working group on cardiovascular pharmacotherapy and European society of cardiology council on stroke. Eur Heart J Cardiovasc Pharmacother. (2019) 5:171–80. doi: 10.1093/ehjcvp/pvz016
9. Ageno W, Gallus AS, Wittkowsky A, Crowther M, Hylek EM, Palareti G. Oral anticoagulant therapy: antithrombotic therapy and prevention of thrombosis: American college of chest physicians evidence-based clinical practice guidelines. Chest. (2012) 141(2 Suppl.):e44S−88S. doi: 10.1378/chest.11-2292
10. Harter K, Levine M, Henderson SO. Anticoagulation drug therapy: a review. West J Emerg Med. (2015) 16:11–7. doi: 10.5811/westjem.2014.12.22933
11. Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. (2011) 365:883–91. doi: 10.1056/NEJMoa1009638
12. Bukowska A, Zacharias I, Weinert S, Skopp K, Hartmann C, Huth C, et al. Coagulation factor Xa induces an inflammatory signalling by activation of protease-activated receptors in human atrial tissue. Eur J Pharmacol. (2013) 718:114–23. doi: 10.1016/j.ejphar.2013.09.006
13. Katoh H, Nozue T, Michishita I. Anti-inflammatory effect of factor-Xa inhibitors in Japanese patients with atrial fibrillation. Heart Vessels. (2017) 32:1130–6. doi: 10.1007/s00380-017-0962-y
14. Terry CM, He Y, Cheung AK. Rivaroxaban improves patency and decreases inflammation in a mouse model of catheter thrombosis. Thromb Res. (2016) 144:106–12. doi: 10.1016/j.thromres.2016.06.008
15. Bruins P, te Velthuis H, Yazdanbakhsh AP, Jansen PG, van Hardevelt FW, de Beaumont EM, et al. Activation of the complement system during and after cardiopulmonary bypass surgery: postsurgery activation involves C-reactive protein and is associated with postoperative arrhythmia. Circulation. (1997) 96:3542–8. doi: 10.1161/01.CIR.96.10.3542
16. Chung MK, Martin DO, Sprecher D, Wazni O, Kanderian A, Carnes CA, et al. C-reactive protein elevation in patients with atrial arrhythmias: inflammatory mechanisms and persistence of atrial fibrillation. Circulation. (2001) 104:2886–91. doi: 10.1161/hc4901.101760
17. Smorodinova N, Bláha M, Melenovský V, Rozsívalová K, Pridal J, Durišová M, et al. Analysis of immune cell populations in atrial myocardium of patients with atrial fibrillation or sinus rhythm. PLoS ONE. (2017) 12:e0172691. doi: 10.1371/journal.pone.0172691
18. Roldan V, Marin F, Diaz J, Gallego P, Jover E, Romera M, et al. High sensitivity cardiac troponin T and interleukin-6 predict adverse cardiovascular events and mortality in anticoagulated patients with atrial fibrillation. J Thromb Haemost. (2012) 10:1500–7. doi: 10.1111/j.1538-7836.2012.04812.x
19. Hu YF, Chen YJ, Lin YJ, Chen SA. Inflammation and the pathogenesis of atrial fibrillation. Nat Rev Cardiol. (2015) 12:230–43. doi: 10.1038/nrcardio.2015.2
20. Lip GY, Patel JV, Hughes E, Hart RG. High-sensitivity C-reactive protein and soluble CD40 ligand as indices of inflammation and platelet activation in 880 patients with nonvalvular atrial fibrillation: relationship to stroke risk factors, stroke risk stratification schema, and prognosis. Stroke. (2007) 38:1229–37. doi: 10.1161/01.STR.0000260090.90508.3e
21. Kirchhof P, Ezekowitz MD, Purmah Y, Schiffer S, Meng IL, Camm AJ, et al. Effects of Rivaroxaban on biomarkers of coagulation and inflammation: a post hoc analysis of the X-VeRT trial. TH Open. (2020) 4:e20–e32. doi: 10.1055/s-0040-1701206
22. Negreva M, Georgiev S, Prodanova K, Vitlianova K, Arabadzhieva D. Interleukin-4 and paroxysmal atrial fibrillation. Merit Res J Med Sci. (2015) 3:271–7. doi: 10.2147/JIR.S10095
23. Hak L, Mysliwska J, Wieckiewicz J, Szyndler K, Siebert J, Rogowski J. Interleukin-2 as a predictor of early postoperative atrial fibrillation after cardiopulmonary bypass graft (CABG). J Interferon Cytokine Res. (2009) 29:327–32. doi: 10.1089/jir.2008.0082.2906
24. Li J, Solus J, Chen Q, Rho YH, Milne G, Stein CM, et al. Role of inflammation and oxidative stress in atrial fibrillation. Heart Rhythm. (2010) 7:438–44. doi: 10.1016/j.hrthm.2009.12.009
25. Rizos I, Tsiodras S, Rigopoulos AG, Dragomanovits S, Kalogeropoulos AS, Papathanasiou S, et al. Interleukin-2 serum levels variations in recent onset atrial fibrillation are related with cardioversion outcome. Cytokine. (2007) 40:157–64. doi: 10.1016/j.cyto.2007.08.013
26. Harada M, Van Wagoner DR, Nattel S. Role of inflammation in atrial fibrillation pathophysiology and management. Circ J. (2015) 79:495–502. doi: 10.1253/circj.CJ-15-0138
27. Guo Y, Lip GY, Apostolakis S. Inflammation in atrial fibrillation. J Am Coll Cardiol. (2012) 60:2263–70. doi: 10.1016/j.jacc.2012.04.063
28. Cabrera-Bueno F, Medina-Palomo C, Ruiz-Salas A, Flores A, Rodriguez-Losada N, Barrera A, et al. Serum levels of interleukin-2 predict the recurrence of atrial fibrillation after pulmonary vein ablation. Cytokine. (2015) 73:74–8. doi: 10.1016/j.cyto.2015.01.026
29. Pinto A, Tuttolomondo A, Casuccio A, Di Raimondo D, Di Sciacca R, Arnao V, et al. Immuno-inflammatory predictors of stroke at follow-up in patients with chronic non-valvular atrial fibrillation (NVAF). Clin Sci. (2009) 116:781–9. doi: 10.1042/CS20080372
30. Steinberg SF. The cardiovascular actions of protease-activated receptors. Mol Pharmacol. (2005) 67:2–11. doi: 10.1124/mol.104.003103
31. Deshmane SL, Kremlev S, Amini S, Sawaya BE. Monocyte chemoattractant protein-1 (MCP-1): an overview. J Interferon Cytokine Res. (2009) 29:313–26. doi: 10.1089/jir.2008.0027
32. Dobaczewski M, Frangogiannis NG. Chemokines and cardiac fibrosis. Front Biosci (Schol Ed). (2009) 1:391. doi: 10.2741/s33
33. Dewald O, Zymek P, Winkelmann K, Koerting A, Ren G, Abou-Khamis T, et al. CCL2/Monocyte Chemoattractant Protein-1 regulates inflammatory responses critical to healing myocardial infarcts. Circ Res. (2005) 96:881–9. doi: 10.1161/01.RES.0000163017.13772.3a
34. Dusi V, Ghidoni A, Ravera A, De Ferrari GM, Calvillo L. Chemokines and heart disease: a network connecting cardiovascular biology to immune and autonomic nervous systems. Mediators Inflamm. (2016) 2016:5902947. doi: 10.1155/2016/5902947
35. Bujak M, Dobaczewski M, Gonzalez-Quesada C, Xia Y, Leucker T, Zymek P, et al. Induction of the CXC chemokine interferon-γ-inducible protein 10 regulates the reparative response following myocardial infarction. Circ Res. (2009) 105:973–83. doi: 10.1161/CIRCRESAHA.109.199471
36. Saxena A, Bujak M, Frunza O, Dobaczewski M, Gonzalez-Quesada C, Lu B, et al. CXCR3-independent actions of the CXC chemokine CXCL10 in the infarcted myocardium and in isolated cardiac fibroblasts are mediated through proteoglycans. Cardiovasc Res. (2014) 103:217–27. doi: 10.1093/cvr/cvu138
Keywords: atrial fibrillation, inflammation, warfarin, rivaroxaban, cytokines, chemokines
Citation: Martins GL, Duarte RCF, Vieira ÉLM, Rocha NP, Figueiredo EL, Silveira FR, Caiaffa JRS, Lanna RP, Carvalho MdG, Palotás A, Ferreira CN and Reis HJ (2020) Comparison of Inflammatory Mediators in Patients With Atrial Fibrillation Using Warfarin or Rivaroxaban. Front. Cardiovasc. Med. 7:114. doi: 10.3389/fcvm.2020.00114
Received: 25 March 2020; Accepted: 02 June 2020;
Published: 24 July 2020.
Edited by:
Pietro Enea Lazzerini, University of Siena, ItalyReviewed by:
Harry Staines, Independent Researcher, York, United KingdomSteve Bibevski, Joe DiMaggio Children's Hospital, United States
Copyright © 2020 Martins, Duarte, Vieira, Rocha, Figueiredo, Silveira, Caiaffa, Lanna, Carvalho, Palotás, Ferreira and Reis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: András Palotás, cGFsb3Rhc0Bhc2tsZXBpb3MtbWVkLmV1; Helton José Reis, aGVsdG9uanJAaWNiLnVmbWcuYnI=