 Alexandre Blassiau1†
Alexandre Blassiau1† Matthias Gawlitza1*†
Matthias Gawlitza1*† Pierre-François Manceau1Serge Bakchine2Isabelle Serre2Sébastien Soize1Laurent Pierot1*
Pierre-François Manceau1Serge Bakchine2Isabelle Serre2Sébastien Soize1Laurent Pierot1*- 1Department of Neuroradiology, Hôpital Maison-Blanche, Reims, France
- 2Department of Neurology, Hôpital Maison-Blanche, Reims, France
Background: Mechanical thrombectomy (MT) is of clinical benefit for patients with extracranial-intracranial tandem lesions of anterior circulation. However, the optimal approach to the cervical lesion of the internal carotid artery (ICA) during MT has yet to be established. Data on a conservative approach for the proximal lesion during the acute phase are scarce.
Methods: A retrospective study on an institutional, prospective database was conducted. We included patients with anterior circulation stroke presenting with a tandem lesion that was approached conservatively during MT.
Results: Thirty-five 35 patients were included, of whom 25 (71.4%) had an atheromatous ICA lesion and 10 (28.6%) a dissection. Despite implementing a conservative strategy, acute percutaneous transluminal angioplasty (PTA) and/or stenting was necessary in 8 (22.9%) and 3 patients (8.6%), respectively. Of 27 surviving patients, 7 (25.9%) underwent delayed treatment of the ICA lesion. No new embolic events occurred between MT and delayed treatment. A favorable clinical outcome (mRS ≤ 2) was achieved in 15/35 patients (45.7%) and was associated with higher baseline ASPECTS (OR 1.62, 95% CI 1.08–2.45, p = 0.002) and successful recanalization (OR 9.39, 95% CI 1.92–45.80, p = 0.0005). Successful recanalization (TICI ≥ 2B) itself was observed in 54.3% of patients and was more likely with acute treatment of the proximal ICA lesion (OR 6.3, 95% CI 11–35.67, p = 0.03) and, more importantly, by the use of distal access catheters (OR 16.25, 95% CI 3.06–86.41, p = 0.0001).
Conclusion: A conservative approach for ICA lesions during MT is feasible and offers favorable outcomes and successful recanalization for a significant proportion of patients. However, acute treatment of the cervical lesion is often necessary (31.4%) to make the distal occlusion accessible. Clinical outcome is influenced by the size of the baseline ischemic core and by successful recanalization; the latter is strongly favored by the use of distal access catheters to pass the proximal lesion. The fact that acute treatment of the ICA lesion favored intracranial recanalization but had no effect on clinical outcome is probably due to sample size, emphasizing the need for large scale, randomized studies to determine the optimal treatment strategy for this pathology.
Introduction
Tandem extracranial-intracranial lesions of the anterior circulation, i.e., the simultaneous occurrence of an intracranial large vessel occlusion and a high-grade stenosis or occlusion of the ipsilateral proximal internal carotid artery (ICA), account for 10–20% of large vessel strokes (1, 2). This pathology is particularly challenging as response rates to intravenous thrombolysis are low and the prognosis is often poor (1, 3).
Although patients with tandem lesions have been excluded from the majority of randomized studies in recent years, the HERMES analysis confirmed the beneficial effect of mechanical thrombectomy (MT) for this pathology (4). Thus, evidence indicates that patients with tandem lesions should not be excluded from MT.
Nonetheless, it has yet to be established how the proximal ICA lesion should be approached during MT. There are several possibilities, i.e., stenting, percutaneous transluminal angioplasty (PTA) alone or no treatment of the lesion; yet, all approaches present advantages and drawbacks. Stenting in the acute phase offers a definitive treatment in one step, but necessitates antiplatelet therapy–often in conjunction with intravenous thrombolysis–putting the patient at potentially elevated risk of intracranial hemorrhage or reperfusion injury (5–8). While simple PTA of the carotid lesion obviates acute antiplatelet therapy, a risk of reperfusion injury persists and the rate of significant restenosis is high (9). However, delayed treatment of the lesion by endarterectomy or stenting can be utilized in patients with favorable clinical outcomes, which may also help to reduce the number of unnecessary procedures (10). Not treating the cervical lesion at all has similar potential advantages and in addition may be faster, while eliminating the risk of reperfusion injury. Nevertheless, this strategy must be balanced against the drawback of a potential risk of recurrent cerebral embolism (11).
Recent meta-analyses did not find significant differences in clinical outcomes between patients treated with stenting and patients treated with PTA alone in the acute phase (12, 13). Wilson et al. concluded that most studies “have entirely or partly treated extracranial occlusion with stenting during initial treatment” and that very few focus on angioplasty-only approaches (12). To the best of our knowledge, data on a completely conservative approach for the proximal ICA lesion are even scarcer (14), which is why we aimed to augment the existing literature with our retrospective case series.
Materials and Methods
Study Design and Ethics
The present paper is a retrospective study on our institutional, prospectively assembled thrombectomy database between October 2010 and October 2017. Inclusion criteria were patients with anterior circulation stroke presenting with a tandem extracranial and intracranial lesion (defined as a carotid stenosis of ≥90% or occlusion of the proximal carotid artery with simultaneous occlusion of an intracranial vessel of the anterior circulation), pretreatment imaging (MRI or CT) and clinical follow—up with 90 day modified Rankin Scale (mRS) assessment. Demographic data, vascular risk factors, admission National Institutes of Health Stroke Scale scores (NIHSS), stroke side, symptom onset to groin puncture and onset to reperfusion, MRI/CT and angiographic variables, information about delayed treatment of the carotid lesion by stenting or endarterectomy and the mRS score at 3 months were collected. Favorable outcome was defined as mRS 0–2. In line with French law, retrospective studies do not require ethics committee approval.
Imaging Evaluation
Brain MR examinations were performed on a 3-T MR unit (Skyra, Siemens, Erlangen, Germany; Achieva 2.1, Philips Healthcare, Best, The Netherlands) and included at least DWI, FLAIR, T2* and TOF-MRA. CT scans were obtained on a tomograph with 64 slices using helicoid acquisition (General Electrics, Chicago, IL, United States).
Two interventional neuroradiologists, each with 8 years of experience, analyzed preinterventional cross-sectional imaging. Preinterventional CT- and DWI-ASPECT scores were evaluated and discrepancies resolved by consensus between readers. Additionally, all postinterventional neuroimaging studies performed during the patients' hospital stays were evaluated for the presence of intracranial hemorrhage (parenchymal hematoma PH1 and PH2) according to the European Cooperative Acute Stroke Study 3 (ECASS3) (15).
The cervical lesion was categorized on DSA as either atheromatous stenosis or dissection, according to typical angiographic imaging characteristics.
For the purpose of the study, two readers (8 and 20 years of experience), blinded from clinical and MRI data, assessed the intracranial occlusion site and initial and final thrombolysis in cerebral infarction (TICI) score on anonymized angiographic records. Successful recanalization was defined as TICI 2B-3 (more than two-thirds of the middle cerebral artery (MCA) territory) (16).
Mechanical Thrombectomy
Patients with acute ischemic stroke, presenting within 6 h of symptom onset with occlusion of a large intracranial vessel (ICA and/or MCA) and without initial intracranial hemorrhage were eligible for MT. Thrombectomy was performed after neuroradiologists and vascular neurologists made a multidisciplinary decision; in exceptional cases, the time window was extended beyond 6 h post symptom onset. Procedures were performed under conscious sedation using 6 F or 8 F catheters introduced via the common femoral artery. An initial angiographic run with the catheter placed in the common carotid artery confirmed the presence of a cervical ICA lesion. Our institutional protocol has evolved over time in line with technical advances. At the outset of the inclusion period, we passed the tandem lesion either with the guide catheter or, if the former was not possible, with the microcatheter, and performed an intracranial thrombectomy using a stent-retriever (Solitaire, FR, Medtronic, Minneapolis, MN, United States) in conjunction with syringe-aided aspiration on the guide catheter. The advent of flexible distal access and aspiration catheters changed this practice and treatment was modified by attempting to pass the stenosis with the distal access catheter, occasionally preceded by an aspiration maneuver at the level of the cervical lesion; intracranial stent-retriever thrombectomy was sometimes preceded or followed by a direct aspiration maneuver with 5 MAX, ACE 64, or ACE 68 reperfusion catheters aided by a mechanical pump providing continuous negative pressure (Penumbra, Alameda, CA, United States).
Our institutional protocol favors minimal treatment for the proximal ICA lesion and prefers balloon angioplasty using over-the-wire (Gateway, Boston Scientific, Fremont, CA, United States) or rapid-exchange (Sterling, Boston Scientific, Fremont, CA, United States) non-compliant PTA balloons only for patients in whom intracranial access through the proximal carotid lesion is not possible. Carotid stenting in the setting of a thrombectomy is considered only for patients (a) in whom intracranial access is not possible even after balloon angioplasty, and (b) in whom hemodynamic compromise due to insufficient collateral flow through the anterior and posterior communicating arteries is to be expected, which is typically investigated on preinterventional cross-sectional imaging studies and, in case of doubt, on a vertebral artery and a contralateral ICA angiogram after intracranial thrombectomy. Emergent carotid stenting can also be considered by the treating physician in case of a floating intraluminal thrombus in the ICA.
Delayed treatment of the cervical lesion by endarterectomy or stenting is typically considered in case of a favorable clinical outcome and with regard to the patient's comorbidities, life expectancy, compliance and personal preferences.
Anticoagulation/Antiaggregation
In case of an entirely conservative treatment and in case of balloon angioplasty of an atheromatous cervical lesion, antiaggregation with 75 mg of acetylsalicylic acid per day is started at discretion of the stroke neurologist and is maintained lifelong in the setting of a secondary prophylaxis.
Medical treatment of non-stented carotid artery dissection is conducted complying with the publication of Engelter et al. (17) and the duration of antiplatelet or anticoagulation therapy is guided by MRI control images.
In case of extracranial carotid stenting, the institutional protocol consists of intravenous administration of 250 mg of acetylsalicylic acid before deploying the stent. The day after the procedure, a cranial computed tomography and a craniocervical computed tomography angiography are conducted and in the absence of stent occlusion, intracranial hemorrhage and complete hemispheric infarction a loading dose of 300 mg of clopidogrel is administered per os. Oral dual antiplatelet therapy with 75 mg of both acetylsalicylic acid and clopidogrel is maintained during 3 months and acetylsalicylic acid monotherapy is continued thereafter.
Statistical Analysis
Continuous variables are described as mean ± SD or median with interquartile range (IQR) and categorical variables as number and percentage. Contingency analyses for categorical variables were performed using the exact Chi-square test. Continuous study parameters were compared among patients by either Student's t-test in case of a normal distribution or by the Mann-Whitney U-test in case of a non-normal distribution. To identify markers of favorable clinical outcome and successful revascularization, group comparisons and univariate logistic regression analyses were carried out. Due to the rather small sample size with resulting large confidence intervals, multivariate logistic regression models were not applied. All analyses were conducted using the JASP 9.0 freeware for Mac OS X (http://www.jasp-stats.com) and MedCalc for Windows (MedCalc Software, Ostend, Belgium).
Results
Study Population
During the study period, 269 patients underwent MT in our department. Of these, 36 patients (13.4%) presented with an extracranial/intracranial tandem occlusion. One patient with a tandem lesion did not undergo MT due to an anesthesiology complication and was removed from the study population leaving 35 patients for statistical analysis. Demographic aspects of the study population are detailed in Table 1. Twenty patients (57.1%) presented with a left hemispheric stroke. Median baseline ASPECTS was 6. MT was performed in conjunction with IVT in 23 patients (65.7%) with a mean onset-to-groin time of 255.5 ± 53 min. The mean NIHSS was 17.3 ± 4.5. Intracranial occlusion sites were the carotid-T in 15 patients (42.9%), the MCA M1 segment in 19 patients (54.3%) and the MCA M2 segment in 1 patient (2.8%), respectively.
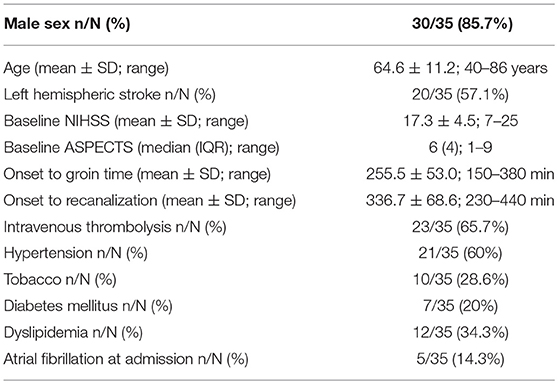
Table 1. Demographic characteristics of the study population.
Clinical and Angiographic Outcomes
At 3 months, mRS scores were 0 in 3 (8.6%), 1 in 7 (20%), 2 in 6 (17.1%), 3 in 5 (14.3%), 4 in 5 (14.3%), and 5 in 1 (2.9%) patients. Eight patients did not survive, resulting in a mortality rate of 22.9%. A favorable outcome (mRS 0–2) was achieved in 16 of 35 patients (45.7%).
TICI 3 was achieved in 5 (14.3%), TICI 2B in 14 (40%), TICI 2A in 10 (28.6%) and TICI 0-1 in 6 patients (17.1%). The rate of successful intracranial recanalization was thus 54.3%. Distal access catheters were employed in 18 patients (51.4%). Emboli to previously unaffected territories occurred in 5 patients (14.3%) of which 2 were observed in patients treated without (2 of 17; 11.8%) and 3 in patients treated with a distal access catheter (3 of 18; 16.7%). The rate of postinterventional parenchymal hematoma was 5.7% (2/35) for PH1 and 5.7% (2/35) for PH2.
Management of Tandem Lesions
Twenty-five patients (71.4%) were diagnosed with an atheromatous lesion and 10 patients (28.6%) with a dissection of the cervical ICA.
In 24 patients no acute treatment of the cervical lesion was performed (68.6%), whereas PTA only or stenting with or without concomitant PTA was carried out in 8 (22.9%) and 3 patients (8.6%), respectively. No statistically significant difference was observed for rates of acute treatment of the carotid lesions in atheromatous (9 of 25; 36%) or dissecting (2 of 10; 20%) lesions (p = 0.357).
Of 27 surviving patients, 7 (25.9%) underwent delayed treatment of the cervical lesion after a mean period of 41.7 ± 38.4 days (range 5–118). Delayed treatment consisted of carotid endarterectomy in 6 of 27 (22.2%) and carotid stenting in 1 of 27 patients (3.7%) and was only performed for atheromatous lesions of the ICA (7 of 20; 35%). The flowchart of the study population is depicted in Figure 1.
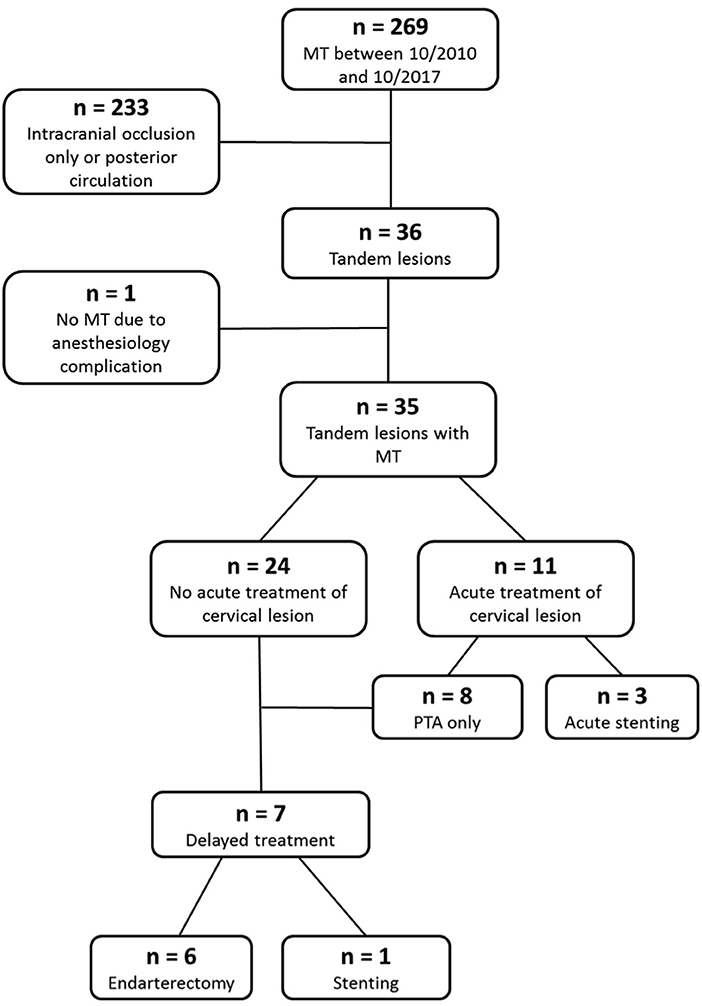
Figure 1. Flowchart of the study population.
No neurological deterioration between the acute phase and the time of the delayed treatment was observed, and no neurological complications occurred during or after delayed treatment of the carotid stenosis.
Factors Influencing Outcome and Recanalization
The comparison of patients with favorable and unfavorable outcome at 3 months of follow-up is shown in Table 2. Notably, patients with favorable outcome had higher median ASPECTS on preinterventional imaging (7.5 vs. 5; p = 0.013) and experienced successful recanalization more often (81.3 vs. 31.6%; p = 0.006). All other cofactors were not statistically different between groups; specifically, no differences with respect to the etiology of the carotid lesion, the baseline NIHSS and the symptom onset to groin time were observed. Similar results were obtained by univariate logistic regression analysis (Table 3): The only significant factors associated with a favorable patient outcome were higher baseline ASPECTS values (OR 1.62, 95% CI 1.08–2.45, p = 0.02) and successful recanalization (OR 9.39, 95% 1.92–45.80, p = 0.0005). Moreover, a trend toward improved patient outcomes was observed when IV thrombolysis was employed (OR 3.09, 95% CI 0.89–18.28, p = 0.08).
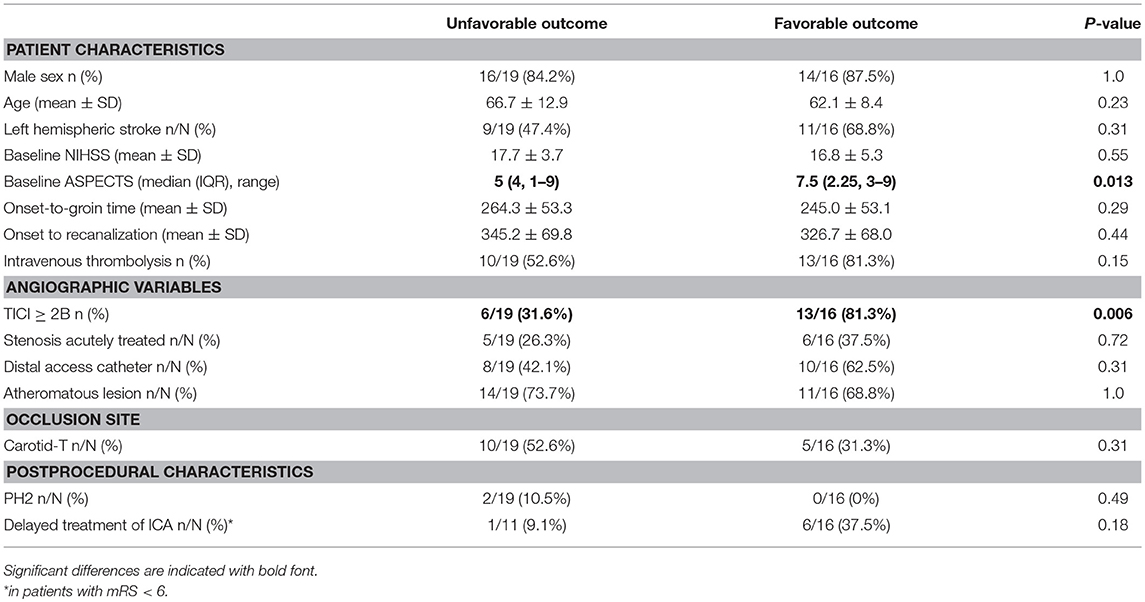
Table 2. Favorable vs. unfavorable outcome.
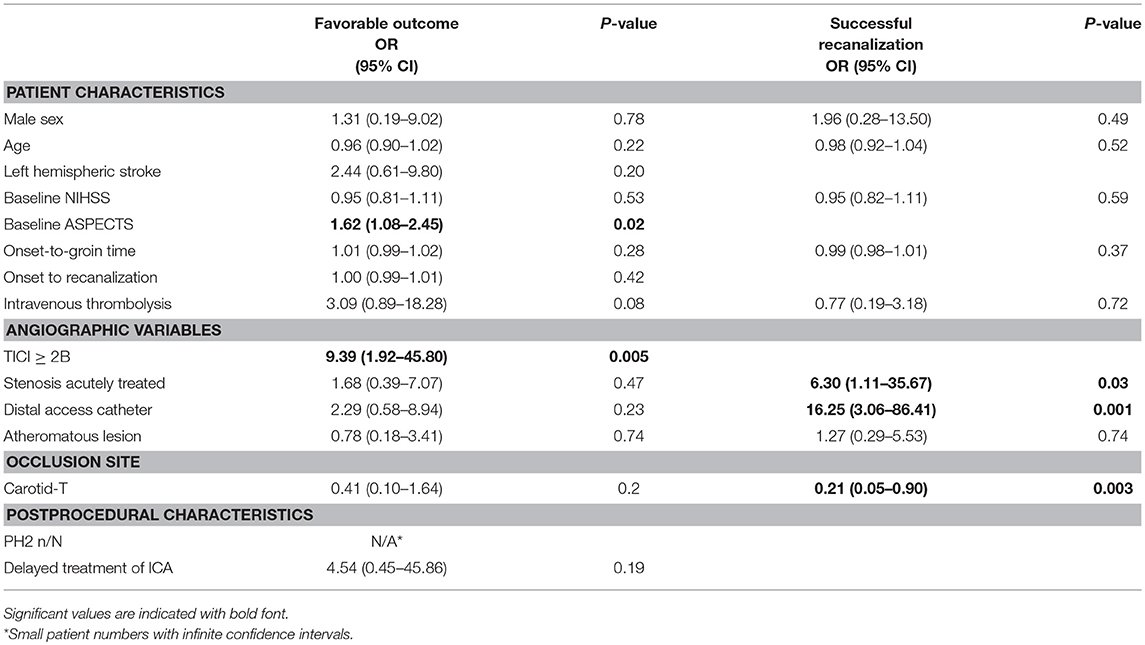
Table 3. Univariate logistic regression analyses with odds ratios for favorable outcome and successful recanalization.
Table 4 shows the analysis of factors in patients with successful and unsuccessful recanalization. Of note, distal access catheters were used more often in patients with successful recanalization (78.9 vs. 18.8%; p = 0.0006) and in those in whom the cervical lesion was treated more often in the acute phase by PTA with or without stenting (47.4 vs. 18.8%; p = 0.035). Thrombus localization at the carotid-T was observed more frequently in patients with unsuccessful recanalization (62.5 vs. 26.3%; p = 0.0442). The etiology of the cervical lesion (dissecting vs. atheromatous) was not significantly different between patients with successful and unsuccessful recanalization (p = 1.0). Univariate regression analysis confirmed these results as the only factors significantly associated with successful revascularization with acute treatment of the stenosis by stenting and/or PTA (OR 6.3, 95% CI 11–35.67, p = 0.03) and, even more importantly, the use of distal access catheters (OR 16.25, 95% CI 3.06–86.41, p = 0.001). Occlusion of the carotid-T hindered successful recanalization compared to occlusion of the MCA (OR 0.21, 95% CI 0.05–0.90, p = 0.003).
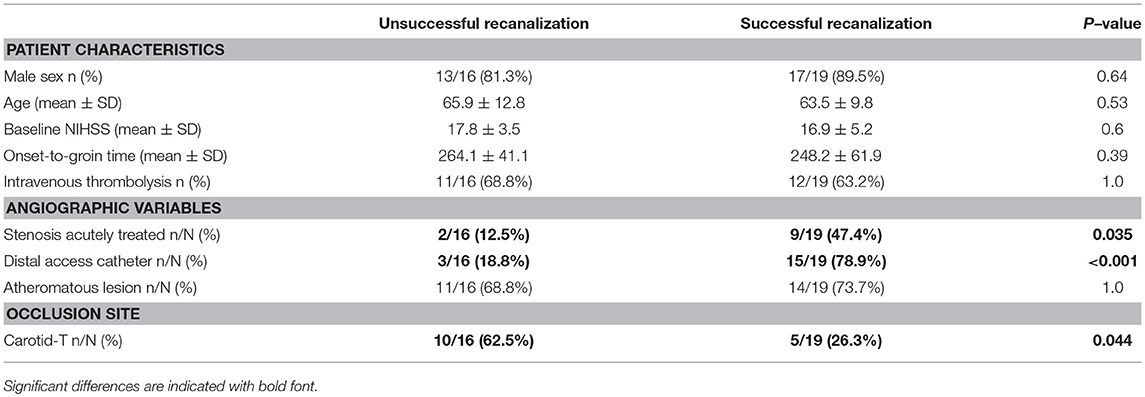
Table 4. Successful vs. unsuccessful recanalization.
Discussion
While the indication for MT of acute tandem occlusions of the anterior circulation is generally undisputed (4), it remains unclear how the cervical lesion should be treated. The vast majority of publications to date focus on stenting of the cervical lesion, with little data on the results of PTA-only and conservative approaches during the acute phase (and, where indicated, delayed treatment of the lesion), as noted by Wilson et al. (12) in their recent meta-analysis.
Our single center series suggests that a conservative approach for the ICA lesion is feasible and that the rate of clinically favorable outcome (45.7%) is within the range of previously published large-scale data on MT (18). Of note, neither group comparisons nor logistic regression analyses indicated that the treatment approach for cervical lesion during MT affected the patient's clinical outcome. Favorable outcome was predicted by a higher preinterventional ASPECT score and even more importantly by successful recanalization of the intracranial occlusion, which was achieved in 54.3% of the included patients. Successful recanalization was strongly favored by the use of distal access catheters, which, when these devices were employed, resulted in successful recanalization in 78.9% of patients, However, it should be noted that successful recanalization was also significantly more frequent when the carotid lesion was treated by stenting and/or balloon PTA during the acute phase. In a recent paper by Papanagiotou et al. (14) on the Thrombectomy In Tandem Lesions (TITAN) study collective, a multicentric registry on patients with MT for tandem stroke, successful recanalization was observed more frequently in patients with acute treatment of the ICA lesion (stent and/or PTA during MT) than in those with conservative management (79.4 vs. 60%) (14). The authors also found that patients without acute treatment of the cervical lesion were less likely to experience a favorable outcome after 3 months (42 vs. 58%). The results of another study on the same patient population were similar to ours, as extracranial carotid stenting had no significant impact on patient outcome which was, among other factors, predicted by age, NIHSS and baseline ASPECTS (19). However, that study confirmed a link between acute carotid stenting and successful reperfusion. Nevertheless, the assumption that stenting is definitively associated with successful reperfusion and that “the ICA lesion should be always treated” (14) during MT should be viewed with caution as both our single-center series and the TITAN study are entirely retrospective data with self-reported clinical outcome measures. One should bear in mind that neurointerventionists are probably more aggressive in treating large vessel occlusions—both intra- and extra-cranially—when a favorable outcome is anticipated so that these results are likely subject to selection bias (20). Moreover, there are multiple personal preferences in the performance of MT that may vary between institution and physicians; additionally, a physician's preference likely continually adapts as a result of personal experience. The way we interpret our data is that a conservative approach for the ICA lesion during MT with delayed treatment offers favorable outcomes for a significant proportion of patients. Successful recanalization is, however, crucial for clinical success and if the ICA lesion cannot be passed with a distal access catheter, the interventionist's threshold for performing a PTA with our without concomitant stenting should be low. Even with a conservative protocol, PTA or stenting of the cervical lesion was still considered necessary in 22.9 and 8.6% of patients, respectively. Furthermore, the fact that acute treatment of the proximal ICA lesion was carried out in 11 patients precludes definitive statements on this treatment strategy.
Unfortunately, most studies do not provide data on the delayed management of the ICA lesion if it was not stented during MT. Our data indicate that a conservative approach for the ICA lesion during the acute phase may reduce the number of overtreatments. Treatment outside the acute phase by endarterectomy or stenting was indicated in only 35% of surviving patients with an atheromatous ICA lesion. In another publication on carotid stenting after MT, the rate of delayed ICA stenting was 66.4%, which led the authors to conclude that this approach may help to prevent futile treatments (10). However, the hemorrhagic risks of stenting during MT must be balanced with the risk of leaving a “non-protected,” potentially emboligenic cervical lesion behind. This risk may be particularly high in patients with a free floating thrombus (21). In our study, no recurrent ischemic events were observed between the acute phase and the definitive treatment of the carotid stenosis after a mean of 41.7 days. Another study postulated that the risk of recurrent ipsilateral ischemic stroke in patients with symptomatic carotid artery stenosis awaiting endarterectomy is as high as 11.5% at 14 days and 18.8% at 90 days (22). However, disabling or fatal strokes at 90 days occurred in only 16 of 377 patients in that analysis (4.2%). A possible explanation for the differences between the latter series and our data may be the rather small sample size of our study. One could also hypothesize that in patients after MT, in whom—depending on the inclusion criteria—considerable infarcts may be present, recurrent emboli may stay silent if they find their way in the already infarcted territory. Another explanation is that we also included 10 patients with carotid artery dissections in whom the risk of recurrent embolism is known to be low (23). Furthermore, even if no active treatment of the ICA lesion by PTA or stenting is performed, passing the lesion with large-bore aspiration or guide catheters may result in a partial dilatation of the stenosis, akin to the Dotter technique (24).
Parenchymal hematoma occurred in 11.4% of our patients (5.7% PH1 and PH2 each), which is within the range of larger series on carotid stenting during MT. For example, Gory et al. (19) observed rates of 8.7% for PH1 and 5.1% for PH2 in the TITAN collective (66.2% received a carotid stent during MT), whereas Behme et al. (5) reported rates of 8 and 9% of PH1 and PH2 in a study in which all patients underwent carotid stenting during MT. Papanagiotou et al. (14) did not report on diminished hematoma occurrence in non-stented patients. Whether the avoidance of stenting effectively diminishes the risk of intracranial hemorrhage thus remains to be proven.
No effect of the proximal lesion's etiology (dissection vs. atheroma) on outcome or recanalization was observed in the present study, which is in line with a previous publication on the TITAN patient collective data (25).
We observed a trend toward a favorable outcome when IV thrombolysis was used, which may support the results of another recent publication (19). However, interpretation of this finding is likely limited by significant selection bias. Moreover, with the Solitaire With the Intention For Thrombectomy Plus Intravenous t-PA Versus DIRECT Solitaire Stent-retriever Thrombectomy in Acute Anterior Circulation Stroke (SWIFT DIRECT) trial actively recruiting (www.ClinicalTrials.gov NCT03192332), a randomized controlled trial will hopefully help to define the current role of IV thrombolysis in stroke treatment.
Our study has limitations, the retrospective design and rather small sample size being most important, which limits the generalizability of the findings. The combined report on atheromatous lesions and carotid artery dissection may contribute to a less homogeneous patient sample. However, the two entities are commonly reported together in the literature (14) and both our results and another study confirm that angiographic and clinical outcomes after MT do not differ between both lesion types (25). Furthermore, the rate of complete recanalization obtained at our center appears low compared to the recent literature; however, this can be explained by a very strict independent evaluation and the use of the stricter TICI scale instead of the modified TICI scale. Importantly, an evolution in practitioners' experience and in technology is highly likely as the first patients in our database were treated in 2010. Unfortunately, we did not have clinical data on the symptomatology of post-interventional intracranial hemorrhage available to us. Nonetheless, it was later shown that PH2 is a reliable, entirely imaging-based predictor of unfavorable outcome (26).
Conclusion
Our study shows that a conservative approach for the ICA lesion during MT is feasible and offers favorable outcomes for a significant number of patients. Factors influencing patient outcome are the size of the baseline ischemic core and particularly the result of recanalization. The utilization of distal access catheters seems highly beneficial for successful recanalization; however, if the cervical lesion cannot be passed with such a device, the threshold for PTA with our without concomitant stenting should be low as it may facilitate intracranial revascularization. Acute treatment of the proximal ICA lesion had no positive effect on clinical outcome, which may be explained by our sample size and probable selection bias. Even if a conservative treatment is planned, acute PTA or stenting of the cervical lesion in order to gain access to the intracranial vasculature may be necessary in a considerable proportion of patients. Beyond that, avoiding treatment of the proximal ICA lesion during the acute phase may help to reduce overtreatments. Altogether, our study provides valuable information on a much-debated pathology and highlights the lack of clarity, which will only be resolved with a properly designed randomized controlled trial.
Author Contributions
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Conflict of Interest Statement
LP consults for Balt, Cerenovus, Microvention, Penumbra and Vesalio.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Rubiera M, Ribo M, Delgado-Mederos R, Santamarina E, Delgado P, Montaner J, et al. Tandem internal carotid artery/middle cerebral artery occlusion: an independent predictor of poor outcome after systemic thrombolysis. Stroke (2006) 37:2301–5. doi: 10.1161/01.STR.0000237070.80133.1d
2. Grau AJ, Weimar C, Buggle F, Heinrich A, Goertler M, Neumaier S, et al. Risk factors, outcome, and treatment in subtypes of ischemic stroke: the German stroke data bank. Stroke (2001) 32:2559–66. doi: 10.1161/hs1101.098524
3. Kim YS, Garami Z, Mikulik R, Molina CA, Alexandrov AV, CLOTBUST Collaborators. Early recanalization rates and clinical outcomes in patients with tandem internal carotid artery/middle cerebral artery occlusion and isolated middle cerebral artery occlusion. Stroke (2005) 36:869–71. doi: 10.1161/01.STR.0000160007.57787.4c
4. Goyal M, Menon BK, Zwam WH van, Dippel DWJ, Mitchell PJ, Demchuk AM, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet (2016) 387:1723–31. doi: 10.1016/S0140-6736(16)00163-X
5. Behme D, Mpotsaris A, Zeyen P, Psychogios MN, Kowoll A, Maurer CJ, et al. Emergency stenting of the extracranial internal carotid artery in combination with anterior circulation thrombectomy in acute ischemic stroke: a retrospective multicenter study. AJNR Am. J. Neuroradiol. (2015) 36:2340–5. doi: 10.3174/ajnr.A4459
6. Zinkstok SM, Roos YB. Early administration of aspirin in patients treated with alteplase for acute ischaemic stroke: a randomised controlled trial. Lancet (2012) 380:731–737. doi: 10.1016/S0140-6736(12)60949-0
7. Mpotsaris A, Kabbasch C, Borggrefe J, Gontu V, Soderman M. Stenting of the cervical internal carotid artery in acute stroke management: the karolinska experience. Interv. Neuroradiol. (2017) 23:159–65. doi: 10.1177/1591019916681983
8. Mpotsaris A, Bussmeyer M, Buchner H, Weber W. Clinical outcome of neurointerventional emergency treatment of extra- or intracranial tandem occlusions in acute major stroke: antegrade approach with wallstent and solitaire stent retriever. Clin. Neuroradiol. (2013) 23:207–15. doi: 10.1007/s00062-013-0197-y
9. McCabe DJH, Pereira AC, Clifton A, Bland JM, Brown MM, CAVATAS Investigators. Restenosis after carotid angioplasty, stenting, or endarterectomy in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS). Stroke (2005) 36:281–6. doi: 10.1161/01.STR.0000152333.75932.fe
10. Cetin K, Akpinar Erdem Gürkaş, Emrah Aytac. Carotid angioplasty-assisted mechanical thrombectomy without urgent stenting may be a better option in acute tandem occlusions. Interv. Neuroradiol. (2017) 23:405–411. doi: 10.1177/1591019917701113
11. Gory B, Sivan-Hoffmann R, Riva R, Labeyrie PE, Huguet N, Nighoghossian N, et al. Repeated Solitaire mechanical thrombectomy in an acute anterior stroke patient. Rev. Neurol (Paris). (2015) 171:682–4. doi: 10.1016/j.neurol.2015.03.013
12. Wilson MP, Murad MH, Krings T, Pereira VM, O'Kelly C, Rempel J, et al. Management of tandem occlusions in acute ischemic stroke – intracranial versus extracranial first and extracranial stenting versus angioplasty alone: a systematic review and meta-analysis. J. NeuroInterventional Surg. (2018). 10:721–8. doi: 10.1136/neurintsurg-2017-013707
13. Coelho A, Lobo M, Gouveia R, Silveira D, Campos J, Augusto R, et al. Overview of evidence on emergency carotid stenting in patients with acute ischemic stroke due to tandem occlusions: a systematic review and meta-analysis. J. Cardiovasc. Surg (Torino). (2018) doi: 10.23736/S0021-9509.18.10312-0. [Epub ahead of print].
14. Papanagiotou P, Haussen DC, Turjman F, Labreuche J, Piotin M, Kastrup A, et al. Carotid stenting with antithrombotic agents and intracranial thrombectomy leads to the highest recanalization rate in patients with acute stroke with tandem lesions. JACC Cardiovasc. Interv. (2018) 11:1290–9. doi: 10.1016/j.jcin.2018.05.036
15. Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N. Engl. J. Med. (2008) 359:1317–29. doi: 10.1056/NEJMoa0804656
16. Higashida RT, Furlan AJ, Radiology for the TAC of the AS of I and TN and the S of I. Trial design and reporting standards for intra-arterial cerebral thrombolysis for acute ischemic stroke. Stroke (2003) 34:e109–37. doi: 10.1161/01.STR.0000082721.62796.09
17. Engelter ST, Brandt T, Debette S, Caso V, Lichy C, Pezzini A, et al. Antiplatelets versus anticoagulation in cervical artery dissection. Stroke (2007) 38:2605–11. doi: 10.1161/STROKEAHA.107.489666
18. Friedrich B, Gawlitza M, Fahnert J, Quäschling U, Kahn T, Lobsien D, et al. Interventional ischemic stroke treatment – A (R)evolution. RöFo - Fortschritte Auf Dem Geb. Röntgenstrahlen Bildgeb. Verfahr. (2016) 188:259–67. doi: 10.1055/s-0041-10689
19. Gory B, Haussen DC, Piotin M, Steglich-Arnholm H, Holtmannspötter M, Labreuche J, et al. Impact of intravenous thrombolysis and emergent carotid stenting on reperfusion and clinical outcomes in patients with acute stroke with tandem lesion treated with thrombectomy: a collaborative pooled analysis. Eur. J. Neurol. (2018) 25:1115–20. doi: 10.1111/ene.13633
20. Spiotta AM, Arthur AS, Fiorella D, Frei D, Baxter B, Mocco J, et al. Is discretion the better part of valor? J. Neurointerventional Surg. (2018) 10:719–20. doi: 10.1136/neurintsurg-2018-013938
21. Labeyrie MA, Ducroux C, Civelli V, Reiner P, Cognat E, Aymard A, et al. Endovascular management of extracranial occlusions at the hyperacute phase of stroke with tandem occlusions. J. Neuroradiol. (2018) 45:196–201. doi: 10.1016/j.neurad.2017.10.003
22. Johansson E, Cuadrado-Godia E, Hayden D, Bjellerup J, Ois A, Roquer J, et al. Recurrent stroke in symptomatic carotid stenosis awaiting revascularization: a pooled analysis. Neurology. (2016) 86:498–504. doi: 10.1212/WNL.0000000000002354
23. Markus HS, Hayter E, Levi C, Feldman A, Venables G, Norris J. Antiplatelet treatment compared with anticoagulation treatment for cervical artery dissection (CADISS): a randomised trial. Lancet Neurol. (2015) 14:361–7. doi: 10.1016/S1474-4422(15)70018-9
24. Woodward K, Wegryn S, Staruk C, Nyberg EM. The Dotter method revisited: early experience with a novel method of rapid internal carotid artery revascularization in the setting of acute ischemic stroke. J. Neurointerventional Surg. (2016) 8:360–366. doi: 10.1136/neurintsurg-2014-011587
25. Gory B, Piotin M, Haussen DC, Steglich-Arnholm H, Holtmannspötter M, Labreuche J, et al. Thrombectomy in acute stroke with tandem occlusions from dissection versus atherosclerotic cause. Stroke (2017) 48:3145–8. doi: 10.1161/STROKEAHA.117.018264
Keywords: tandem lesions, ischemic stroke, mechanical thrombectomy, carotid artery stenting, large vessel occlusion, conservatory approach, percutaneous transluminal angioplasty (PTA)
Citation: Blassiau A, Gawlitza M, Manceau P-F, Bakchine S, Serre I, Soize S and Pierot L (2018) Mechanical Thrombectomy for Tandem Occlusions of the Internal Carotid Artery—Results of a Conservative Approach for the Extracranial Lesion. Front. Neurol. 9:928. doi: 10.3389/fneur.2018.00928
Received: 15 August 2018; Accepted: 12 October 2018;
Published: 05 November 2018.
Edited by:
Daniel Behme, Universitätsmedizin Göttingen, GermanyReviewed by:
Christoph Kabbasch, Uniklinik Köln, GermanyAnnika Kowoll, Universitätsklinikum Knappschaftskrankenhaus Bochum, Germany
Copyright © 2018 Blassiau, Gawlitza, Manceau, Bakchine, Serre, Soize and Pierot. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Matthias Gawlitza, bWF0dGhpYXNnYXdsaXR6YTIxNUBnbWFpbC5jb20=
Laurent Pierot, bHBpZXJvdEBnbWFpbC5jb20=
†These authors have contributed equally to this work