 Astrid Versluis
Astrid Versluis Thuy-My Le1,2
Thuy-My Le1,2 André C. Knulst
André C. Knulst Harmieke Van Os-Medendorp
Harmieke Van Os-Medendorp- 1Department of Dermatology and Allergology, University Medical Centre Utrecht, University Utrecht, Utrecht, Netherlands
- 2Center for Translational Immunology, University Medical Centre Utrecht, University Utrecht, Utrecht, Netherlands
- 3TNO, Netherlands Organization for Applied Scientific Research, Utrecht, Netherlands
- 4School of Health, Saxion University of Applied Sciences, Enschede, Netherlands
Accidental allergic reactions to food are one of the major problems in adult patients diagnosed with food allergy. Such reactions occur frequently, are often severe and are associated with higher medical and non-medical costs. The aim of this Perspective is to provide insight into the different factors involved in the occurrence of accidental allergic reactions and to present an overview of practical implications for effective preventive measures. Several factors affect the occurrence of accidental reactions. These factors are related to the patient, health care, or food. The most important patient-related factors are age, social barriers to disclosing their allergy and non-adherence to the elimination diet. With regards to healthcare, the degree to which clinical practice is tailored to the individual patient is an important factor. The major food-related factor is the absence of adequate precautionary allergen labeling (PAL) guidelines. Since many factors are involved in accidental allergic reactions, different preventive strategies are needed. It is highly recommended that health care be tailored to the individual patient, with regard to education about the elimination diet, support on behavioral and psychosocial aspects, usage of shared decision-making and taking into account health literacy. In addition, it is crucial that steps are taken to improve policies and guidelines for PAL.
Introduction
Food allergy affects 0.3%–6% of the adults in Europe (1). At present, no curative treatment is available. The key interventions after diagnosing a food allergy are an elimination diet and emergency medication to treat accidental allergic reactions (2). Despite specific dietary advice, accidental reactions to food still occur in the daily life of food-allergic individuals (3, 4). A prospective study showed that approximately half of all food allergic adults experienced on average, two accidental reactions per year (4). The severity of accidental allergic reactions varies from mild to severe (3, 4), and is sometimes even fatal (3). Even with severe reactions, patients often fail to adequately use their emergency medication and do not always seek medical treatment (3, 4). This increases morbidity and the risk of fatal outcomes (5). In addition, accidental allergic reactions have a significant impact on costs: food allergic patients with accidental allergic reactions had sevenfold higher direct and indirect costs than food allergic patients without these reactions (6). In all subcategories (hospital admissions, primary care consultations, outpatient consultations, travel costs to healthcare facilities and sick leave costs due to accidental reactions), patients with accidental allergic reactions were shown to have higher costs than patients without accidental allergic reactions (6).
Given the impact of accidental allergic reactions on costs and their frequency and severity, increased prevention of these accidental reactions is needed. To be able to prevent accidental allergic reactions, it is important to identify factors that affect their occurrence. The aim of this Perspective is to give insight into the different factors involved in the occurrence of accidental allergic reactions and to provide an overview of practical implications for effective preventive measures.
Many factors affect the occurrence of accidental allergic reactions
Factors which influence the occurrence of accidental allergic reactions can be grouped into three categories: (1) patient-related, (2) health care-related and (3) food-related (Figure 1).
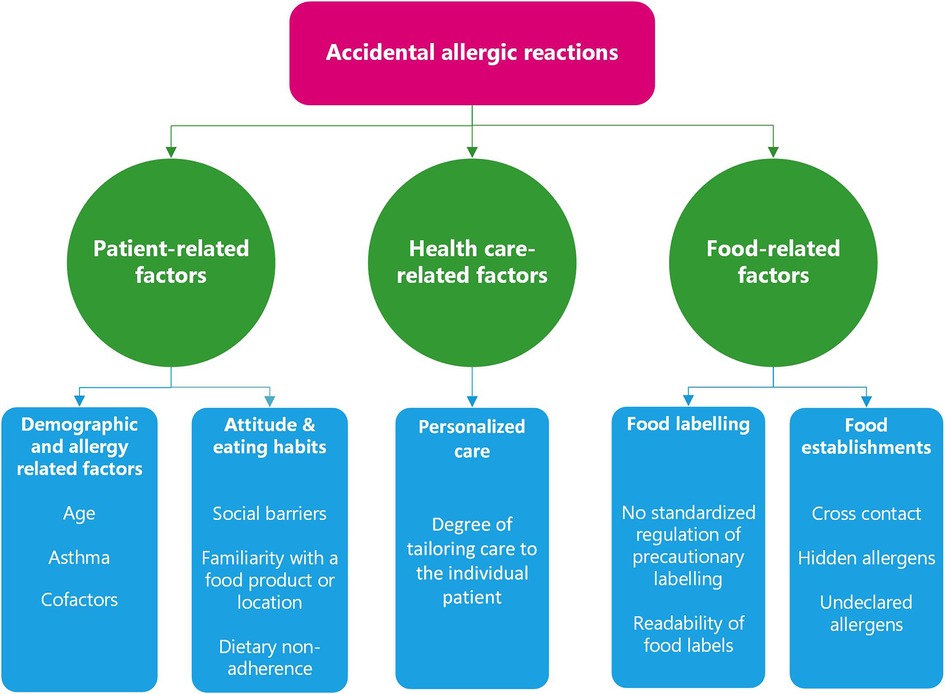
Figure 1. Factors affecting the occurrence of accidental allergic reactions.
Patient-related factors
Patient-related factors which influence the risk of accidental allergic reactions include patient age (7), history of asthma (2, 8), attitude and eating habits (3, 9), and cofactors (10–14) (Figure 1).
Age-related factors
Adolescents and young adults are at high risk of fatal reactions to food: among 32 fatalities, 69% occurred in patients between 13–21 years of age (7). This high percentage may be due to higher risk-taking behavior with regard to the management of the elimination diet by teenagers and adolescents (3). Adolescence is known as a period of heightened vulnerability to risk-taking behavior (15). Only 61% of adolescents always carry their adrenaline auto-injector, meaning that 39% do not (16). Adolescence is the period in which responsibility for dietary management transfers from the parents or carer to the patient. Specific strategies for this transition are important. Such strategies include: an early start of the transition process (11–13 years), using a multidisciplinary approach, discussing self-management in everyday contexts such as school/work and actively evaluating adherence (17).
Asthma
Food-allergic patients with asthma appear to be at higher risk of severe and even fatal reactions (2, 8). Of 16 fatalities in adult patients, all individuals for whom data was available had asthma (8). In a study about fatal and near fatal reactions to food in 13 children and adolescents, all had asthma, whereof 12 had asthma that was well controlled (18). The EAACI guidelines (2) recommend the use of an adrenaline auto-injector in food-allergic patients with persistent or severe asthma and short-acting beta agonists for every patient with co-existing asthma. Healthcare professionals should monitor asthmatic patients carefully, including training on when and how to treat reactions.
Attitude and eating habits: social barriers, familiarity with food/location and dietary change
Patients often experience social barriers to the disclosure of their allergy when eating outside their home, due to fear of potential social embarrassment (3). They may avoid situations that might lead to them being perceived as on overly fussy eater (19). It is important that patients communicate information about the food allergens they avoid, because then the person who prepares or provides the food can take this into account. Accidental reactions often (63%–74%) occur at locations outside the home (3, 20). In only 54% of the allergic reactions which occurred in restaurants had the customer informed restaurant staff of their food allergy (20). Healthcare professionals should therefore openly discuss social embarrassment with food allergic individuals, and emphasize the importance of disclosing their food allergy and associated restrictions when eating out.
Food-allergic consumers sometimes estimated the risk of eating a certain food product based on the type of food product or brand in combination with prior experiences, instead of reading the complete food label (3, 9). This approach may lead to individuals missing possible changes in ingredients.
Barriers to changing dietary behavior might play a role. A study which evaluated dietary adherence after 58 positive food challenges, showed that 52% of the patients followed a less strict diet than advised (9). Patients who were advised to change their diet following a positive food challenge, more often not adhered to the dietary advice compared to patients to whom no dietary change was advised (9). It has been shown in other chronic diseases that adherence to specific dietary patterns is challenging because of many barriers, such as higher costs, overall restrictive nature of the diet, social support and practical factors (21–23). Food-allergic individuals who were advised to strictly avoid the culprit food [meaning avoidance of the allergenic food and ingredients, including products with precautionary allergen labeling (PAL)] more often failed to adhere to dietary advice compared to patients who received less strict dietary advice (9). This might be explained by the fact that a strict elimination diet has more impact on food choices than a less strict diet. Another factor might be that many patients do not consider PAL credible and therefore ignore these labels (24, 25) (see paragraph Food labeling issues are a main cause of accidental allergic reactions). The high frequency of non-adherence to dietary advice, especially by patients advised to strictly avoid allergens, indicates that more guidance with regard to dietary behavior is needed.
The influence of cofactors on the threshold and severity of accidental allergic reactions seems to be limited
Cofactors are reported as factors which might influence the threshold and/or severity of allergic reactions in some patients. These include physical exercise, use of nonsteroidal anti-inflammatory drugs (NSAIDs), and consumption of alcohol (10, 11). A recent prospective study found that cofactors are often present during accidental allergic reactions (74%), but no significant correlation was found between the presence of cofactors and the severity of accidental allergic reactions (14). A number of studies found some, but only limited, influence of cofactors on the threshold and severity of allergic reactions to food (10, 11, 13). Recently, Dua et al. (12) published a prospective study in peanut-allergic patients who underwent three open peanut challenges: combined with exercise, combined with sleep deprivation, and with no intervention. This study reported that both sleep deprivation and exercise caused a reduction of the individuals’ threshold to peanut-related allergic reactions. Turner et al. (26) assessed the results of this study and concluded that this decrease is well within the intra-individual variability in reaction thresholds. Furthermore, the clinical center at which patients were evaluated had the largest impact on threshold variability (12, 26). Therefore, although cofactors can have some effect on threshold and severity of the reaction in some individuals, this does not appear to be any greater than the inherent shift in both clinical thresholds and risk of anaphylaxis identified in the wider food-allergic population, nor does it appear that such effects are predictable. The limited impact of cofactors is also indicated by the fact that population Eliciting Dose (ED) values calculated from reaction thresholds in the presence of the cofactors (12) were not lower than those based on the largest worldwide threshold dataset (27, 28), indicating that the variability caused by these cofactors does not exceed the population ED covered in this large threshold database. In conclusion, cofactors are frequently present in daily life, but the influence on thresholds and severity of accidental reactions seems to be limited. The exact influence and impact of cofactors on food-allergic reactions remains to be elucidated. Therefore, cofactors need to be considered when assessing a patient's medical history. If there is any suspicion of a role of cofactors in the occurrence of (severe) accidental reaction, it is advisable to inform patients about the possible role that cofactors can have in accidental reactions and how to manage these factors in daily life.
Healthcare-related factors: a more patient-tailored approach is needed
While several patient-related factors can influence the occurrence of accidental allergic reactions, which factors are involved differ per patient. Therefore, in clinical practice, it is important that healthcare professionals investigate which factors apply for each individual. Based on the described patient-related factors, we formulated the following recommendations to tailor health care to the individual patient (Table 1):
1. Education: Education is a key intervention for management of food allergy and should cover allergen avoidance, symptoms recognition and when and how to treat reactions (2). It has been shown that patients do not always carry their self-injectable adrenaline and that self-injectable adrenaline had often not been immediately administered in fatal reactions (7, 18). Therefore, specific attention to the use of self-injectable adrenaline is important. The type of education materials can be tailored to the individual patient. Different tools can be combined, such as group sessions, written materials, mobile apps, video and online self-management programs (29–33). Furthermore, education of family and close relatives about potentially risky situations should be considered (2).
2. Behavior change aspects: It is important that support regarding behavioral aspects is tailored to the individual patient. For instance, specific attention and guidance is needed for patients who are advised to change their diet after diagnosis, and therefore need to change their dietary behavior. In these patients, extra follow-up consultations are important for supporting dietary and behavioral change (21). Furthermore, extra attention is needed for adolescents due to higher risk-taking behavior. Adolescents should be positively encouraged to self-manage their condition whilst still in a “semi-protected” environment, in preparation for adulthood (34). Specific attention to carrying the adrenaline auto-injector is important, for example by discussing the emotional effect of feeling different, offering strategies for carrying auto-injectors (e.g., purse) and emphasizing the importance of carrying the adrenaline auto-injector (16).
3. Psychosocial aspects: It is important to recognize psychosocial aspects like anxiety and social embarrassment, and tailor interventions to patients’ needs. Healthcare professionals can support patients with psychosocial aspects/issues by: (1) providing appropriate education via knowledgeable healthcare professionals about coping with the risks associated with allergen exposure, allergic symptoms and treatment of reactions, (2) enhancing self-efficacy, for instance by practicing assertiveness about avoidance of allergens, (3) assessing social concerns, for example discussing problems that patients and family encounter with regard to managing the food allergy and (4) meaning making, for instance by reflecting on the positive growth patients make due to the challenges of managing food allergy (35). Mental health professionals can help to address psychosocial concerns in case there is a greater need for support (36).
4. Shared decision-making: Shared decision-making is defined as a patient-centered approach wherein the healthcare professional and patient work together. It involves a mutual discussion about management and treatment options, which take into account the patient’s underlying preferences and values (37). This empowers patients to make decisions that they find most acceptable (37–39). Within the care for patients with food allergy, this can be applied, for instance, when deciding whether or not to undertake a food challenge or the type of tools to use in the education process.
5. Health literacy: Low health literacy is linked to poor health behavior and outcomes (43, 44). Approaches to address health literacy are: shared decision-making, using patient-friendly education materials (e.g., simple pictures, key points), using eHealth interventions (videos, interactive self-help tools), avoiding jargon, focusing on the key messages, repetition and using the “teach-back” method (ask the patient to recall what they have been told) (40–42).
6. Multidisciplinary team: A multidisciplinary team including allergists and/or immunologists, allergy-specialized dieticians, clinical nurse specialists, nurses and mental health professionals may provide and coordinate the healthcare regarding the needs of the individual patient (2, 36). It is important that each discipline attends to inter-professional collaboration and understands its own role and responsibilities and those of other team members (45, 46).
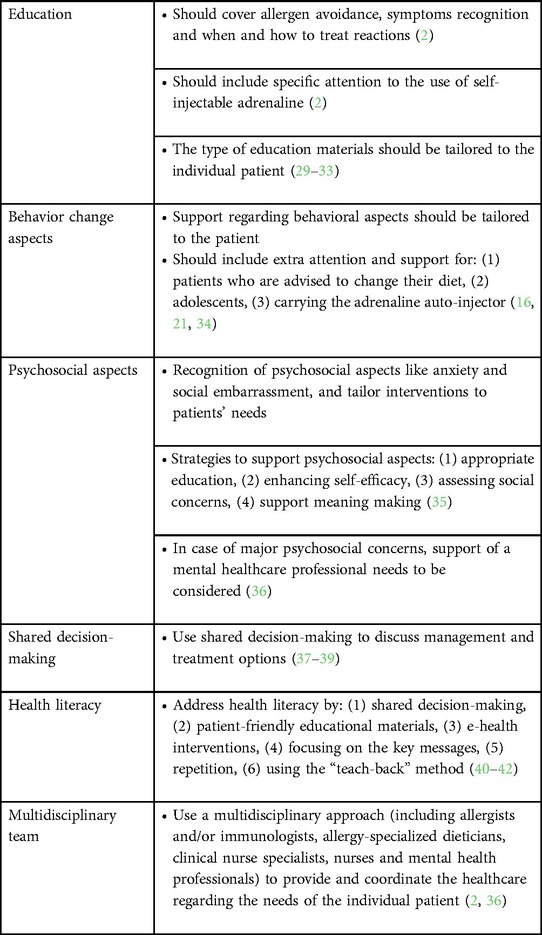
Table 1. Key points for a patient-centered approach.
Applying the above-detailed recommendations will help to ensure that healthcare is better-tailored to the individual patient and contribute to decreasing the occurrence of accidental reactions. For future research, it would be interesting to evaluate the effectiveness of these recommendations with regard to the occurrence of accidental reactions.
Food-related factors: better regulation of food labeling and food establishments needed
Food labeling issues are a main cause of accidental allergic reactions
A major issue affecting the occurrence of accidental allergic reactions, is the poor regulation regarding when and when not to use a PAL statement on prepackaged foods. PAL is used by manufacturers to give information about the possible occurrence of allergen contamination during the production process of food products. PAL is however poorly regulated and therefore is not always nor uniformly applied on food products. It is reported that 17%–68% of all manufactured foods contain PAL (47, 48). Chocolate, sweets and biscuits have such a description on more than 50% of the labels (49). Only 10% of prepackaged food products with a precautionary statement about peanuts had a detectable level of this allergen (50). This corroborates the notion that avoidance of products with PAL leads to major unnecessary dietary restrictions, with all their nutritional and social consequences. On the other hand, it was reported that there are prepackaged food products with clinically relevant levels of unlabeled allergens, which is a major concern because of the risk of severe accidental reactions (51, 52). In 37% of food products which caused accidental reactions, a non-ingredient allergen was detected (53).
Usage of PAL on prepackaged food products is often not based on a standardized risk assessment process. The current practice of deciding on when and how to use PAL has resulted in non-uniform application of PAL and generated more confusion and uncertainty than benefit for food allergic patients (54, 55). Many patients do not consider PAL credible and therefore ignore these labels (24, 25). Previously, several promising recommendations were given to improve these labels, including to only use PAL when there was a possibility that the allergen could be present at levels that might result in intakes in excess of a relevant reference dose (55, 56). Adoption of these recommendations will strongly contribute to global harmonization of risk-based allergen management and PAL. Educating food-allergic consumers (or those providing food for them, including food business operators) and other relevant stakeholders (e.g., risk assessors, healthcare providers) is critical, to ensure understanding of the applied principles and the implications of the chosen phraseology (55).
Issues with the readability of food labels also affect the occurrence of accidental reactions (3). It has been shown that less than 50% of patients considered allergy information to be clear (57). Furthermore, patients attributed different risk levels of unintended presence of allergens in prepackaged food products to different wordings of PAL, especially patients with higher levels of health literacy (57). There is a wide variety of ways in which allergen presence is currently communicated (58), which increases the risk of misinterpretation. Several recommendations have been proposed to improve allergen information on food labels including: ensuring readability of food information, presenting allergens in the ingredient list in bold, presenting topic order in a uniform manner on the label, providing an allergen information section, and using allergen icons (58). Moreover, it is recommended that there is a universally agreed upon uniform wording of PAL, that would unambiguously convey that the product is not suitable for individuals allergic to the specific allergen potentially contained in the product (55, 58). It is important that steps are taken to improve policies and guidelines, to translate such improvements into practice.
Food establishments
Miscommunication and poor knowledge of restaurant staff appears to be an important cause of increased risk of accidental allergic reactions. In food establishments, cross-contact can easily occur, for example by hands and cooking equipment (59). Hidden and undeclared allergens in menus may result in the occurrence of accidental reactions (20, 60). It is known that risks are higher in specific types of restaurants like Asian restaurants and ice cream shops (60). A study in the United States showed that only 73% of the servers correctly identified hen's egg as a major allergen and about 10% of managers and staff erroneously believed that a small amount of an allergen can be safely consumed by food allergic consumers (61). It can be assumed that this lack of knowledge leads to less careful working practices with regards to preventing cross-contact. A study in the United States showed that only 41% of the workers who primarily prepare or cook the food received food allergy training while working at their current restaurant (59). An American workgroup (60) has recommended measures for food establishments to lower cross-contact including educating staff that minimal cross-contact can cause allergic reactions, providing knowledge about cleaning methods to remove food allergens, creating a special allergen-free area in the kitchen and creating a separate pick-up area for allergen-free meals. However, several barriers are reported for implementation of food allergy training such as: high turnover of staff, lack of interest in food allergy training and high costs (60). Repeatedly offered food allergy training seems important to improve the knowledge of restaurant staff. To make this feasible, it seems necessary to reduce barriers, for example by making food allergy training easily and freely accessible by developing eLearnings or mobile apps.
Conclusion
Accidental allergic reactions occur frequently and are associated with high costs. Their occurrence is affected by many factors, related to the patient, healthcare and food. The most important factors related to the patient are age-related, social barriers to disclosing their allergy and non-adherence to the elimination diet. With regard to healthcare-related factors, the degree to which clinical practice is tailored to the individual patient is important, especially with regard to education and support of behavioral and psychosocial aspects. A major food-related factor is absence of harmonized regulation regarding PAL. Therefore it is of great importance that steps are taken to improve policies and guidelines for PAL.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Ethics statement
Ethical review and approval was not required for this study in accordance with the local legislation and institutional requirements.
Author contributions
All authors have contributed to the design and conception of the study, revised the manuscript and have read and approved the final manuscript.
Acknowledgments
We would like to thank all colleagues who contributed to the PhD research (3, 6, 9, 13, 14) upon which this Perspective is based.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Lyons SA, Burney PGJ, Ballmer-Weber BK, Fernandez-Rivas M, Barreales L, Clausen M, et al. Food allergy in adults: substantial variation in prevalence and causative foods across Europe. J Allergy Clin Immunol Pract. (2019) 7(6):1920–8. doi: 10.1016/j.jaip.2019.02.044
2. Muraro A, Werfel T, Hoffmann-Sommergruber K, Roberts G, Beyer K, Bindslev-Jensen C, et al. EAACI food allergy and anaphylaxis guidelines: diagnosis and management of food allergy. Allergy. (2014) 69(8):1008–25. doi: 10.1111/all.12429
3. Versluis A, Knulst AC, Kruizinga AG, Michelsen A, Houben GF, Baumert JL, et al. Frequency, severity and causes of unexpected allergic reactions to food: a systematic literature review. Clin Exp Allergy. (2015) 45(2):347–67. doi: 10.1111/cea.12328
4. Michelsen-Huisman AD, van Os-Medendorp H, Blom WM, Versluis A, Castenmiller JJM, Noteborn HPJM, et al. Accidental allergic reactions in food allergy: causes related to products and patient's management. Allergy. (2018) 73(12):2377–81. doi: 10.1111/all.13560
5. Dhami S, Panesar SS, Roberts G, Muraro A, Worm M, Bilò MB, et al. Management of anaphylaxis: a systematic review. Allergy. (2014) 69(2):168–75. doi: 10.1111/all.12318
6. Versluis A, Knulst AC, Michelsen-Huisman AD, Houben GF, Blom WM, Le TM, et al. Accidental food-allergic reactions are associated with higher costs and more sick leave but not with quality of life. Clin Exp Allergy. (2021) 51(4):627–30. doi: 10.1111/cea.13839
7. Bock SA, Munoz-Furlong A, Sampson HA. Fatalities due to anaphylactic reactions to foods. J Allergy Clin Immunol. (2001) 107(1):191–3. doi: 10.1067/mai.2001.112031
8. Bock SA, Munoz-Furlong A, Sampson HA. Further fatalities caused by anaphylactic reactions to food, 2001-2006. J Allergy Clin Immunol. (2007) 119(4):1016–8. doi: 10.1016/j.jaci.2006.12.622
9. Versluis A, Le TM, Erp FCV, Blankestijn MA, Houben GF, Knulst AC, et al. Low dietary adherence after a positive food challenge in food allergic adults. Clin Transl Allergy. (2022) 12(2):e12119. doi: 10.1002/clt2.12119
10. Wolbing F, Fischer J, Koberle M, Kaesler S, Biedermann T. About the role and underlying mechanisms of cofactors in anaphylaxis. Allergy. (2013) 68(9):1085–92. doi: 10.1111/all.12193
11. Niggemann B, Beyer K. Factors augmenting allergic reactions. Allergy. (2014) 69(12):1582–7. doi: 10.1111/all.12532
12. Dua S, Ruiz-Garcia M, Bond S, Durham SR, Kimber I, Mills C, et al. Effect of sleep deprivation and exercise on reaction threshold in adults with peanut allergy: a randomized controlled study. J Allergy Clin Immunol. (2019) 144(6):1584–94.e2. doi: 10.1016/j.jaci.2019.06.038
13. Versluis A, van Os-Medendorp H, Kruizinga AG, Blom WM, Houben GF, Knulst AC. Cofactors in allergic reactions to food: physical exercise and alcohol are the most important. Immun Inflamm Dis. (2016) 4(4):392–400. doi: 10.1002/iid3.120
14. Versluis A, van Os-Medendorp H, Blom WM, Michelsen-Huisman AD, Castenmiller JJM, Noteborn HPJM, et al. Potential cofactors in accidental food allergic reactions are frequently present but may not influence severity and occurrence. Clin Exp Allergy. (2019) 49(2):207–15. doi: 10.1111/cea.13282
15. Icenogle G, Cauffman E. Adolescent decision making: a decade in review. J Res Adolesc. (2021) 31(4):1006–22. doi: 10.1111/jora.12608
16. Sampson MA, Munoz-Furlong A, Sicherer SH. Risk-taking and coping strategies of adolescents and young adults with food allergy. J Allergy Clin Immunol. (2006) 117(6):1440–5. doi: 10.1016/j.jaci.2006.03.009
17. Roberts G, Vazquez-Ortiz M, Knibb R, Khaleva E, Alviani C, Angier E, et al. EAACI guidelines on the effective transition of adolescents and young adults with allergy and asthma. Allergy. (2020) 75(11):2734–52. doi: 10.1111/all.14459
18. Sampson HA, Mendelson L, Rosen JP. Fatal and near-fatal anaphylactic reactions to food in children and adolescents. N Engl J Med. (1992) 327(6):380–4. doi: 10.1056/NEJM199208063270603
19. Leftwich J, Barnett J, Muncer K, Shepherd R, Raats MM, Hazel Gowland M, et al. The challenges for nut-allergic consumers of eating out. Clin Exp Allergy. (2011) 41(2):243–9. doi: 10.1111/j.1365-2222.2010.03649.x
20. Oriel RC, Waqar O, Sharma HP, Casale TB, Wang J. Characteristics of food allergic reactions in United States restaurants. J Allergy Clin Immunol Pract. (2021) 9(4):1675–82. doi: 10.1016/j.jaip.2020.12.018
21. Tapsell LC. Dietary behaviour changes to improve nutritional quality and health outcomes. Chronic Dis Transl Med. (2017) 3(3):154–8. doi: 10.1016/j.cdtm.2017.06.005
22. Hall KD, Kahan S. Maintenance of lost weight and long-term management of obesity. Med Clin North Am. (2018) 102(1):183–97. doi: 10.1016/j.mcna.2017.08.012
23. Makharia GK, Singh P, Catassi C, Sanders DS, Leffler D, Ali RAR, et al. The global burden of coeliac disease: opportunities and challenges. Nat Rev Gastroenterol Hepatol. (2022) 19(5):313–27. doi: 10.1038/s41575-021-00552-z
24. Barnett J, Muncer K, Leftwich J, Shepherd R, Raats MM, Gowland MH, et al. Using ‘May contain’ labelling to inform food choice: a qualitative study of nut allergic consumers. BMC Public Health. (2011) 11:734. doi: 10.1186/1471-2458-11-734
25. Marchisotto MJ, Harada L, Kamdar O, Smith BM, Waserman S, Sicherer S, et al. Food allergen labeling and purchasing habits in the United States and Canada. J Allergy Clin Immunol Pract. (2017) 5(2):345–51.e2. doi: 10.1016/j.jaip.2016.09.020
26. Turner PJ, Patel N, Ballmer-Weber BK, Baumert JL, Blom WM, Brooke-Taylor S, et al. Peanut can be used as a reference allergen for hazard characterization in food allergen risk management: a rapid evidence assessment and meta-analysis. J Allergy Clin Immunol Pract. (2022) 10(1):59–70. doi: 10.1016/j.jaip.2021.08.008
27. Houben GF, Baumert JL, Blom WM, Kruizinga AG, Meima MY, Remington BC, et al. Full range of population eliciting dose values for 14 priority allergenic foods and recommendations for use in risk characterization. Food Chem Toxicol. (2020) 146:111831. doi: 10.1016/j.fct.2020.111831
28. Remington BC, Westerhout J, Meima MY, Blom WM, Kruizinga AG, Wheeler MW, et al. Updated population minimal eliciting dose distributions for use in risk assessment of 14 priority food allergens. Food Chem Toxicol. (2020) 139:111259. doi: 10.1016/j.fct.2020.111259
29. Jones CJ, Llewellyn CD, Frew AJ, Du Toit G, Mukhopadhyay S, Smith H. Factors associated with good adherence to self-care behaviours amongst adolescents with food allergy. Pediatr Allergy Immunol. (2015) 26(2):111–8. doi: 10.1111/pai.12333
30. Armitage LC, Kassavou A, Sutton S. Do mobile device apps designed to support medication adherence demonstrate efficacy? A systematic review of randomised controlled trials, with meta-analysis. BMJ Open. (2020) 10(1):e032045. doi: 10.1136/bmjopen-2019-032045
31. Watson PW, McKinstry B. A systematic review of interventions to improve recall of medical advice in healthcare consultations. J R Soc Med. (2009) 102(6):235–43. doi: 10.1258/jrsm.2009.090013
32. van Os-Medendorp H, van Leent-de Wit I, de Bruin-Weller M, Knulst A. Usage and users of online self-management programs for adult patients with atopic dermatitis and food allergy: an explorative study. JMIR Res Protoc. (2015) 4(2):e57. doi: 10.2196/resprot.4134
33. Matricardi PM, Dramburg S, Alvarez-Perea A, Antolín-Amérigo D, Apfelbacher C, Atanaskovic-Markovic M, et al. The role of mobile health technologies in allergy care: an EAACI position paper. Allergy. (2020) 75(2):259–72. doi: 10.1111/all.13953
34. Muraro A, Agache I, Clark A, Sheikh A, Roberts G, Akdis CA, et al. EAACI food allergy and anaphylaxis guidelines: managing patients with food allergy in the community. Allergy. (2014) 69(8):1046–57. doi: 10.1111/all.12441
35. Rubeiz CJ, Ernst MM. Psychosocial aspects of food allergy: resiliency, challenges and opportunities. Immunol Allergy Clin North Am. (2021) 41(2):177–88. doi: 10.1016/j.iac.2021.01.006
36. Engel ML, Bunning BJ. The unmet needs of patients with food allergies. Immunol Allergy Clin North Am. (2021) 41(2):321–30. doi: 10.1016/j.iac.2021.01.005
37. Greenhawt M. Shared decision-making in the care of a patient with food allergy. Ann Allergy Asthma Immunol. (2020) 125(3):262–7. doi: 10.1016/j.anai.2020.05.031
38. Elwyn G, Frosch D, Thomson R, Joseph-Williams N, Lloyd A, Kinnersley P, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. (2012) 27(10):1361–7. doi: 10.1007/s11606-012-2077-6
39. Miller TA. Health literacy and adherence to medical treatment in chronic and acute illness: a meta-analysis. Patient Educ Couns. (2016) 99(7):1079–86. doi: 10.1016/j.pec.2016.01.020
40. Jacobs RJ, Lou JQ, Ownby RL, Caballero J. A systematic review of eHealth interventions to improve health literacy. Health Informatics J. (2016) 22(2):81–98. doi: 10.1177/1460458214534092
41. Edison K, Staiculescu I, Hudson S. Educate your patients and improve outcomes: health literacy for the dermatologist. Clin Dermatol. (2012) 30(4):459–63. doi: 10.1016/j.clindermatol.2011.09.004
42. Dunn P, Conard S. Improving health literacy in patients with chronic conditions: a call to action. Int J Cardiol. (2018) 273:249–51. doi: 10.1016/j.ijcard.2018.08.090
43. Stellefson M, Paige SR, Alber JM, Chaney BH, Chaney D, Apperson A, et al. Association between health literacy, electronic health literacy, disease-specific knowledge, and health-related quality of life among adults with chronic obstructive pulmonary disease: cross-sectional study. J Med Internet Res. (2019) 21(6):e12165. doi: 10.2196/12165
44. Sansom-Daly UM, Lin M, Robertson EG, Wakefield CE, McGill BC, Girgis A, et al. Health literacy in adolescents and young adults: an updated review. J Adolesc Young Adult Oncol. (2016) 5(2):106–18. doi: 10.1089/jayao.2015.0059
45. van Dongen JJJ, van Bokhoven MA, Goossens WNM, Daniels R, van der Weijden T, Beurskens A. Development of a customizable programme for improving interprofessional team meetings: an action research approach. Int J Integr Care. (2018) 18(1):8. doi: 10.5334/ijic.3076
46. McLaney E, Morassaei S, Hughes L, Davies R, Campbell M, Di Prospero L. A framework for interprofessional team collaboration in a hospital setting: advancing team competencies and behaviours. Healthc Manage Forum. (2022) 35(2):112–7. doi: 10.1177/08404704211063584
47. Pieretti MM, Chung D, Pacenza R, Slotkin T, Sicherer SH. Audit of manufactured products: use of allergen advisory labels and identification of labeling ambiguities. J Allergy Clin Immunol. (2009) 124(2):337–41. doi: 10.1016/j.jaci.2009.05.032
48. Zurzolo GA, Mathai ML, Koplin JJ, Allen KJ. Hidden allergens in foods and implications for labelling and clinical care of food allergic patients. Curr Allergy Asthma Rep. (2012) 12(4):292–6. doi: 10.1007/s11882-012-0263-6
49. Pele M, Brohee M, Anklam E, Van Hengel AJ. Peanut and hazelnut traces in cookies and chocolates: relationship between analytical results and declaration of food allergens on product labels. Food Addit Contam. (2007) 24(12):1334–44. doi: 10.1080/02652030701458113
50. Hefle SL, Furlong TJ, Niemann L, Lemon-Mule H, Sicherer S, Taylor SL. Consumer attitudes and risks associated with packaged foods having advisory labeling regarding the presence of peanuts. J Allergy Clin Immunol. (2007) 120(1):171–6. doi: 10.1016/j.jaci.2007.04.013
51. Remington BC, Baumert JL, Blom WM, Houben GF, Taylor SL, Kruizinga AG. Unintended allergens in precautionary labelled and unlabelled products pose significant risks to UK allergic consumers. Allergy. (2015) 70(7):813–9. doi: 10.1111/all.12625
52. Spanjersberg MQ, Knulst AC, Kruizinga AG, Van Duijn G, Houben GF. Concentrations of undeclared allergens in food products can reach levels that are relevant for public health. Food Addit Contam Part A Chem Anal Control Expo Risk Assess. (2010) 27(2):169–74. doi: 10.1080/19440040903317513
53. Blom WM, Michelsen-Huisman AD, van Os-Medendorp H, van Duijn G, de Zeeuw-Brouwer ML, Versluis A, et al. Accidental food allergy reactions: products and undeclared ingredients. J Allergy Clin Immunol. (2018) 142(3):865–75. doi: 10.1016/j.jaci.2018.04.041
54. Fiocchi A, Risso D, DunnGalvin A, Gonzalez Diaz SN, Monaci L, Fierro V, et al. Food labeling issues for severe food allergic patients. World Allergy Organ J. (2021) 14(10):100598. doi: 10.1016/j.waojou.2021.100598
55. Ad hoc Joint FAO/WHO expert consultation on risk assessment of food allergens. Part 3: review and establish precautionary labelling in foods of the priority allergens (2021).
56. Taylor SB, Christensen G, Grinter K, Sherlock R, Warren L. The allergen bureau VITAL program. J AOAC Int. (2018) 101(1):77–82. doi: 10.5740/jaoacint.17-0392
57. Holleman BC, van Os-Medendorp H, van den Bergh H, van Dijk LM, Linders YFM, Blom WM, et al. Poor understanding of allergen labelling by allergic and non-allergic consumers. Clin Exp Allergy. (2021) 51(10):1374–82. doi: 10.1111/cea.13975
58. Blom WM, van Dijk LM, Michelsen-Huisman A, Houben GF, Knulst AC, Linders YFM, et al. Allergen labelling: current practice and improvement from a communication perspective. Clin Exp Allergy. (2021) 51(4):574–84. doi: 10.1111/cea.13830
59. Radke TJ, Brown LG, Faw B, Hedeen N, Matis B, Perez P, et al. Restaurant food allergy practices - six selected sites, United States, 2014. Morb Mortal Wkly Rep. (2017) 66(15):404–7. doi: 10.15585/mmwr.mm6615a2
60. Carter CA, Pistiner M, Wang J, Sharma HP. Food allergy in restaurants work group report. J Allergy Clin Immunol Pract. (2020) 8(1):70–4. doi: 10.1016/j.jaip.2019.09.013
Keywords: food allergy, accidental allergic reactions, prevention, factors, accidental reactions
Citation: Versluis A, Le T-M, Houben GF, Knulst AC and Van Os-Medendorp H (2023) Accidental allergic reactions to food in adolescents and adults: An overview of the factors involved and implications for prevention. Front. Allergy 4:1062049. doi: 10.3389/falgy.2023.1062049
Received: 5 October 2022; Accepted: 21 February 2023;
Published: 10 March 2023.
Edited by:
Joyce Yu, Columbia University Irving Medical Center, United StatesReviewed by:
Isabel Janet Skypala, Royal Brompton & Harefield NHS Foundation Trust, United KingdomMarion Elizabeth Groetch, Icahn School of Medicine at Mount Sinai, United States
© 2023 Versluis, Le, Houben, Knulst and Van Os-Medendorp. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Astrid Versluis YS52ZXJzbHVpcy03QHVtY3V0cmVjaHQubmw= Harmieke Van Os-Medendorp aC52YW5vc0BzYXhpb24ubmw=
Specialty Section: This article was submitted to Food Allergy, a section of the journal Frontiers in Allergy