 Stéphane Odet1
Stéphane Odet1 Lauriana Solecki2Christophe Meyer1,3
Lauriana Solecki2Christophe Meyer1,3 Elise Weber1Brice Chatelain1Edouard Euvrard1,2
Elise Weber1Brice Chatelain1Edouard Euvrard1,2 Aude Barrabé1
Aude Barrabé1 Thomas Gualdi4
Thomas Gualdi4 Anne-Laure Parmentier4Laurent Tatu5,6Fabienne Pouthier7,8Aurélien Louvrier1,8
Anne-Laure Parmentier4Laurent Tatu5,6Fabienne Pouthier7,8Aurélien Louvrier1,8 Florelle Gindraux1,3*
Florelle Gindraux1,3*- 1Service de chirurgie maxillo-faciale, stomatologie et odontologie hospitaliéère, CHU Besançon, Besançon, France
- 2Service d’ophtalmologie, CHU Besançon, Besançon, France
- 3Laboratoire de Nanomédecine, Imagerie, Thérapeutique EA 4662, Université Bourgogne Franche-Comté, Besançon, France
- 4INSERM Centre d’Investigation Clinique 1431, CHU Besançon, Besançon, France
- 5Service de neurologie, CHU Besançon, Besançon, France
- 6Laboratoire d’anatomie, Université Bourgogne Franche-Comté, Besançon, France
- 7AICT, Établissement français du sang Bourgogne Franche-Comté, Besançon, France
- 8Université Bourgogne Franche-Comté, INSERM, EFS BFC, UMR1098, RIGHT Interactions Greffon-Hôte-Tumeur/Ingénierie Cellulaire et Génique, Besançon, France
Objectives: The purpose of this pilot porcine study was to explore and illustrate the surgical application of human amniotic membrane (hAM) in an ex vivo model of medication-related osteonecrosis of the jaw (MRONJ).
Material and methods: Five oral and maxillofacial surgeons participated to this study. MRONJ was simulated on porcine mandible specimens. hAM was applied using four different techniques: implantation with complete coverage, implantation with partial coverage, apposition and covering graft material. At the same time, the surgeons evaluated how well the hAM handled and its physical properties during the surgery.
Results: Surgeons found that hAM had suitable mechanical properties, as it was easy to detach from the support, handle, bind to the defect and bury. hAM was also found to be strong and stable. The “implantation with complete coverage” and “implantation with partial coverage” techniques were the preferred choices for the MRONJ indication.
Conclusion: This study shows that hAM is a graft material with suitable properties for oral surgery. It is preferable to use it buried under the gingiva with sutures above it, which increases its stability. This technical note aims to educate surgeons and provide them with details about the handling of hAM in oral surgery.
Clinical relevance: Two surgical techniques for hAM application in MRONJ were identified and illustrated. hAM handling and physical properties during surgery were reported.
Introduction
Human amniotic membrane (hAM) is the innermost layer of fetal membranes. It is composed of a single layer of epithelial cells, a basement membrane, and an avascular stroma containing amniotic mesenchymal stem cells, underlayered by the chorion. Its thickness (70–180 µm) varies among individuals (Chen et al., 2012; Gremare et al., 2019). The beneficial effects of hAM use have been widely described in the literature. To date, ophthalmology is one of the most popular applications of hAM (John, 2003).
Since the mid-1990s, there has been a growing interest in using hAM for oral surgery to accelerate tissue regeneration. One systematic review of literature explored the different indications for hAM use in oral surgery (Fenelon et al., 2018). In this line, two hAM configurations were identified (Odet et al., 2021): “implanted graft material” and “covering graft material”. The first one was applied to gingival recession, bone defects in the furcation, bone defects in interproximal areas and surgical wounds after implant surgery. The second one was applied to mandibular vestibuloplasty and mucosal defects. Whereas hAM use in ophthalmology has been accompanied by informative surgical illustrations (Dua and Azuara-Blanco, 1999; Letko et al., 2001; John, 2003), its use in oral surgery is not described to the same extent, specifically its handling and surgical application. As a consequence, a specific nomenclature beyond the previously mentioned terms—“implanted graft material” and “covering graft material”—was necessary (Odet et al., 2021). Along these lines, four theorical types of hAM surgeries are proposed:
1) “implantation”, where the hAM is buried and completely covered by the gingiva
2) “apposition”, where the hAM is applied against the site to be treated, not sutured, left exposed in the mouth and stabilized by any means (cross stitches, pressure dressing, palatal plates, etc.)
3) “whole covering graft material”, where the hAM is applied against the site to be treated, sutured to adjacent mucosa or underlying mucosa, fully left exposed in the mouth and protected by any means (cross stitches, pressure dressing, palatal plates, etc.)
4) “partial covering graft material”, where the hAM is applied against the bone, buried under the wound edges, sutured to adjacent mucosa or underlying mucosa, left partially exposed in the mouth and protected by any means (cross stitches, pressure dressing, palatal plates, etc.).
However, no study has provided details about how to handle cryopreserved hAM which is more challenging to cut, orient (mesenchymal versus epithelial side), manipulate and apply than the lyophilized or dehydrated amnion or amnion-chorion often used in oral surgery (Fenelon et al., 2018; Gulameabasse et al., 2020; Odet et al., 2021).
As previously investigated by Ragazzo et al. (Ragazzo et al., 2018; Ragazzo et al., 2021), our team wanted to use hAM to manage medication-related osteonecrosis of the jaw (MRONJ) in a compassionate clinical trial (Odet et al., 2022). Despite our extensive experience with hAM banking, its in vitro/in vivo osteogenic potential, and its use in oral, bone and nerve surgeries (Gindraux and Obert, 2010; Obert et al., 2012; Gindraux et al., 2013; Laurent et al., 2014a; Laurent et al., 2014b; Laurent et al., 2014c; Gindraux et al., 2017; Laurent et al., 2017; Fénelon et al., 2018; Bourgeois et al., 2019; Fenelon et al., 2019; Gualdi et al., 2019; Fenelon et al., 2020; Etchebarne et al., 2021; Fénelon et al., 2021; Fenelon et al., 2021; Odet et al., 2021), we failed to identify how to handle and apply hAM during surgery in the oral cavity. Thus, an ex vivo pilot study was required to fill these voids and train the surgeons.
Porcine jaw specimens are common in vivo models for oral and maxillofacial surgery, as the bone, teeth and mucosa have similar appearance, size and structure as the human jaw (Deppe et al., 2018; Kniha et al., 2021). So, MRONJ was simulated in fresh porcine mandible specimens to investigate 1) the handling of cryopreserved hAM and its related physical properties for oral surgery, and 2) the four previously listed theorical types of hAM surgeries. No specific MRONJ grade was targeted in this study. A questionnaire was developed to collect surgeon feedback. Thus, this technical note only defines hAM handling, its physical properties and surgical application in an ex vivo MRONJ model. It provides surgeons with tips and tricks for hAM application in oral surgery or more broadly, in soft tissue regeneration.
Material and methods
The work for this technical note was performed at the anatomy laboratory of the University of Franche-Comté (Besançon, France). Five maxillofacial and oral surgeons (CM, EE, EW, AB, SO), one ophthalmologist and one methodologist participated in the training. The fresh porcine mandible specimens were provided by Chevillotte Breeders (Valdahon, France). All the hAM application techniques were filmed by the group “Tête de Com”, and all the illustrations were made by Mr. Thomas Gualdi, a scientific illustrator.
hAM suitable for scientific purposes were provided by the AICT bank from the French Blood Institute (Etablissement Français du Sang). A 4.7-cm diameter cryopreserved hAM stored in glycerol on a nitrocellulose support (epithelial layer facing the support) was thawed for 2 h at room temperature. After three 5 min rinses in saline or hypotonic injection solution, the hAM was cut either on the nitrocellulose support or after being detached from it.
MRONJ simulation
A sulcular incision on two adjacent teeth was made in the premolar area of the porcine mandible (Figures 1A–C). Two teeth were extracted, and a 3-mm wide defect was created by resecting the mucosa on the vestibular edge of the incision, simulating MRONJ. The alveolar bone was resected over approximately 3 mm using a rongeur. Here, no specific MRONJ grade was targeted.
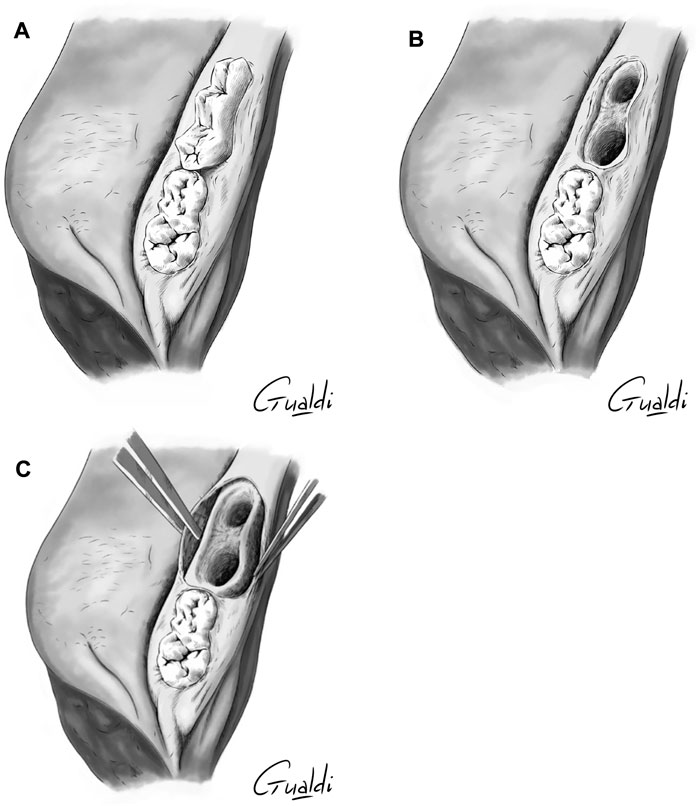
FIGURE 1. Simulation of MRONJ on porcine mandible specimen (upper view illustration): (A) Before premolar extraction; (B) After premolar extraction; (C) After gingival detachment from the alveolar bone.
For the “hAM implantation with complete coverage” technique (see below), a horizontal periosteum incision was made on the two full thickness vestibular and lingual flaps to allow tensionless closure on the mucosal edges.
hAM applications
Two surgeons were needed to separate the hAM from its support: one detached the hAM with two forceps (without teeth) while the other held the support with another set of forceps (Figure 2A). The hAM tended to fold upon itself once detached from the support. Two options were used to unfold and apply it. The first one needed two surgeons: one held the membrane while the second unfolded it using two forceps without teeth. Later, both surgeons applied it on the surgical site (“with four hands”) in the desired orientation (Figure 2B). In the second option, only one surgeon was required: once the hAM was detached from the support, it was directly applied on the surgical site, and then unfolded using two forceps. The hAM’s orientation was quite difficult to maintain in this case.
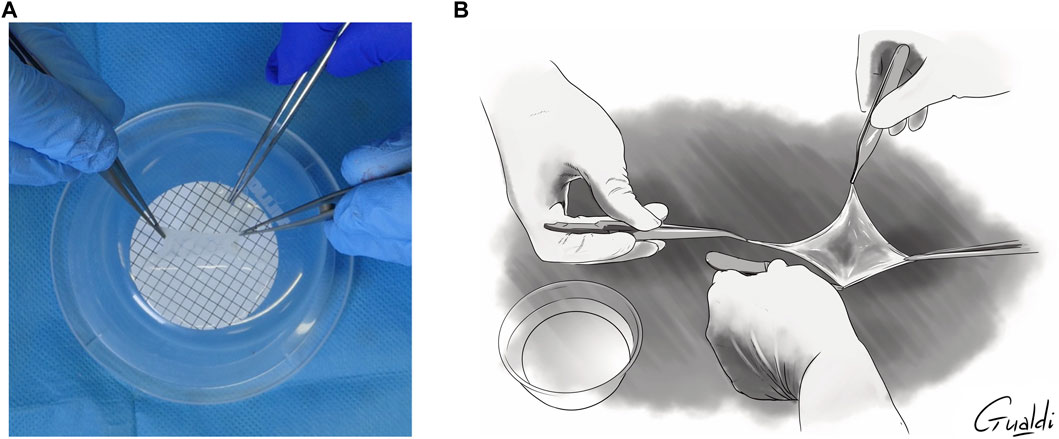
FIGURE 2. (A) hAM detachment from the nitrocellulose support. (B) “Four hands” application of hAM.
The four theoretical techniques identified by Odet et al. (Odet et al., 2021) were attempted and adapted to this experimental study. After hAM application at the MRONJ site (Figure 3A), hAM was buried between bone and gingiva when necessary (Figure 3B). In all cases, hAM could be cut into the desired shape and size and then applied with the mesenchymal side facing the bone and the epithelial side facing the gingiva. One to two hAM units were manipulated by the surgeon.
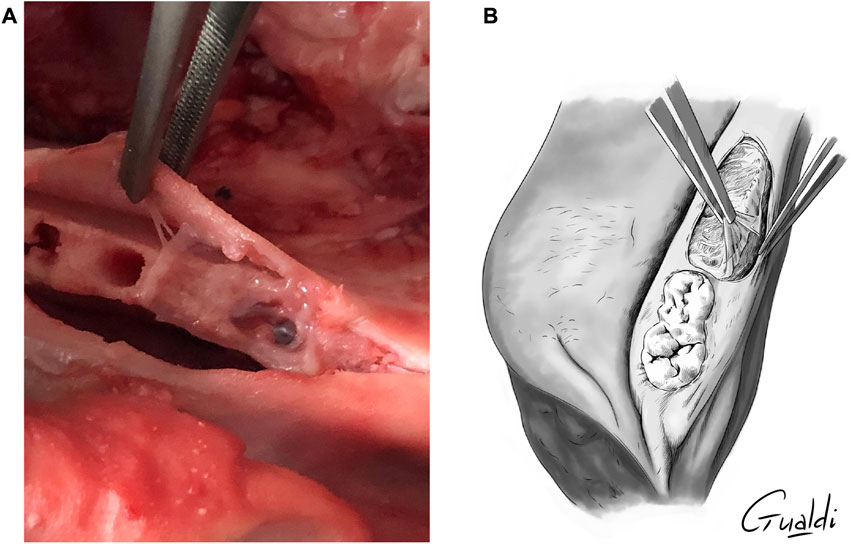
FIGURE 3. (A) hAM application on MRONJ simulation site. (B) hAM burying between bone and gingiva (upper view illustration).
Evaluation by surgeons
hAM handling and physical properties during the surgery were evaluated with a questionnaire. The studied parameters were:
1) ease of detaching the hAM from the nitrocellulose support
2) hAM handling
3) hAM adhesion once applied on the defect (bone)
4) hAM strength
5) ease of suturing the hAM
6) ease of burying the hAM between the bone and mucosa.
These parameters were evaluated on a scale of 0–10 (0 = impossible to handle the hAM/failure of the procedure; 10 = perfect handling/success of the procedure). Grading was left up to each surgeon.
Additional parameters included
1) easiest way to cut the hAM: when still bound to the support or after being detached
2) easiest way to apply the hAM on the surgical site: flat or folded on itself
3) stability of hAM during suturing once applied on the surgical site.
Results
hAM applications
The four theoretical techniques previously mentioned were attempted and adapted to this practical study as follows:
1) Implantation with complete coverage (Figures 4A–C): the hAM was applied and buried between the bone and mucosa (Figure 3B). The mucoperiosteal flap was reapplied over the hAM and sutured hermetically above it, using simple or cross stitches.
2) Implantation with partial coverage (Figures 5A–C): the hAM was applied and buried between the bone and mucosa (Figure 3B). The mucoperiosteal flap was then sutured above it, non-hermetically. In this case, the hAM was left exposed in the oral cavity.
3) Apposition: the hAM was simply applied “in apposition” against the defect, without burying it between the bone and mucosa. The mucosa was then closed above it as hermetically as possible, using simple or cross stitches. Compared to the initial nomenclature, the hAM was not sutured.
4) Covering graft material: The hAM was cut into the desired shape, applied on the defect and sutured directly to the adjacent mucosa, using single stitches.

FIGURE 4. hAM implantation with complete coverage. The sutures were realized above the implanted hAM which was thus not visible. (A) Photography; (B) Sagittal section illustration; (C) Upper view illustration.
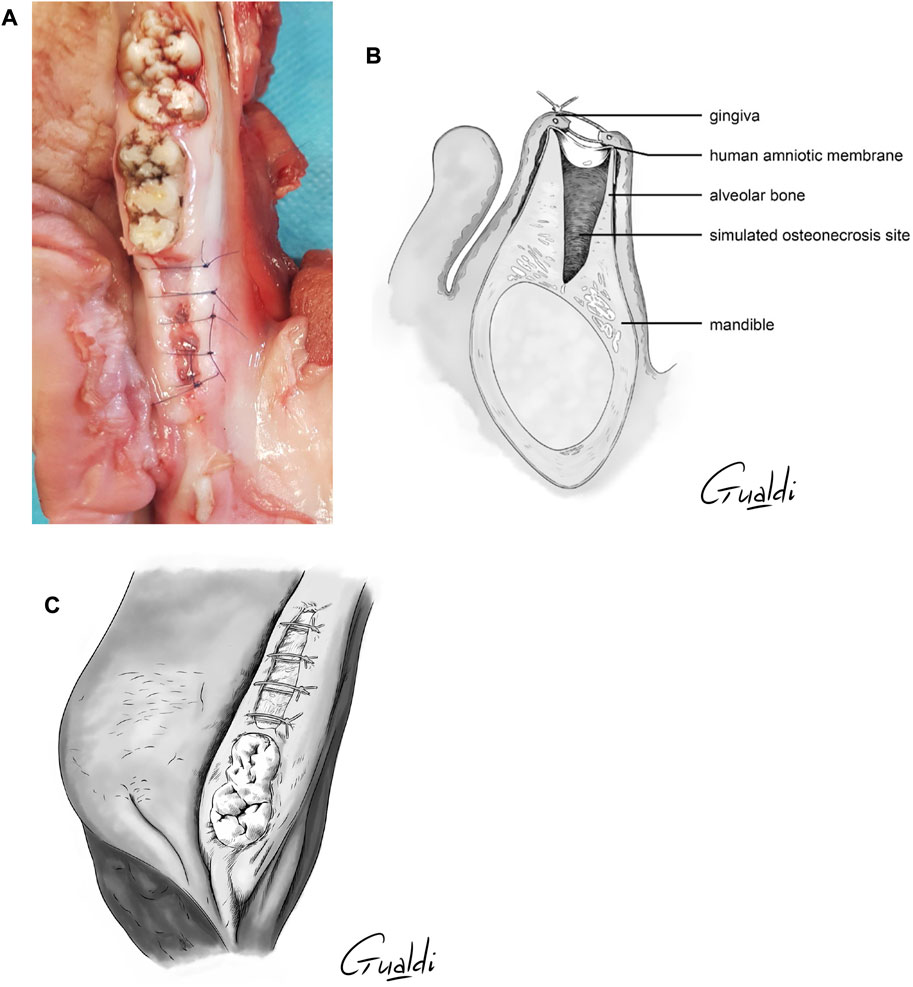
FIGURE 5. hAM implantation with partial coverage. The gingiva was sutured above the hAM, but leaving the hAM exposed in the oral cavity. (A) Photography; (B) Sagittal section illustration; (C) Upper view illustration.
Video of the procedure:
https://https://youtu.be/GKy3I-n3NRQ
Surgeon evaluation
The surgeons noted that hAM was easy to work with overall (Table 1).
1) To detach from the nitrocellulose support: mean of 7.4 (6–8)
2) To handle: mean of 7.0 (4–8)
3) To bind to the defect: mean of 7.4 (6–9)
4) To bury between the bone and mucosa once applied on the defect: mean of 7.6 (5–9).
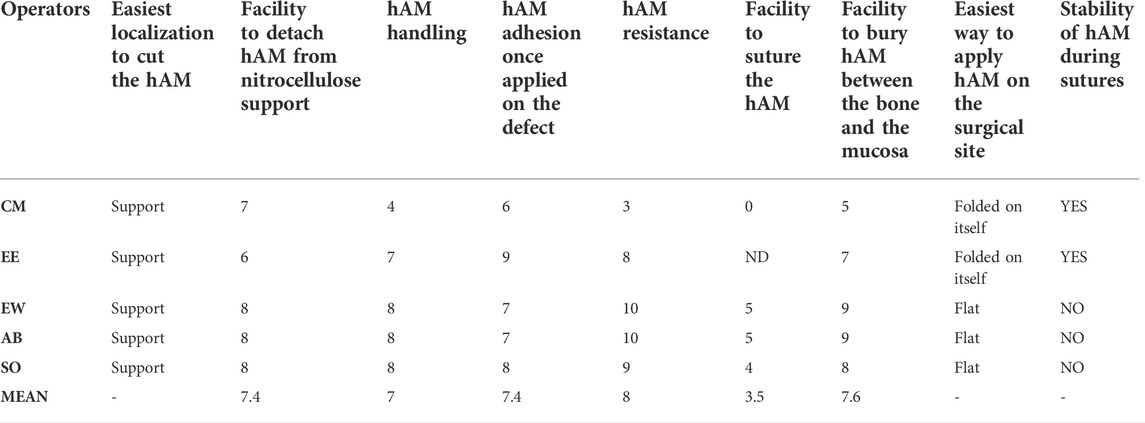
TABLE 1. Evaluation by the surgeons. ND: not done.
With a mean of 8 (3–10), surgeons found the hAM was very strong during manipulation, particularly when detached from the nitrocellulose support. However, all surgeons had difficulties when suturing it due to its fragility (because the stitch caused a crack during tightening) and its tendency to fold upon itself, making it hard to suture. After thawing and rinsing, wet hAM tended to fold on itself, making it difficult to manipulate and cut it from its nitrocellulose support. All surgeons agreed that it was easier to cut hAM when it was still bound to its support.
Two surgeons mentioned that hAM was easier to apply on the surgical site when it was folded upon itself. They noticed that the folding increased its thickness but that it was impossible to maintain its orientation. The other surgeons found that it was easier to use it flat and mentioned two advantages: hAM orientation and burying between the bone and mucosa.
hAM was found to be unstable at the surgical site during suturing by three surgeons. In these cases, hAM tended to rise up between the stitches when the mucosal edges were approximated. However, it was stable enough that it was not expelled from the surgical site. In contrast, two surgeons found that hAM was quite stable during suturing, without any movement or oral exposition from the hAM.
Discussion
The aim of this pilot porcine study was to reproduce MRONJ in fresh porcine mandible specimens and to describe hAM handling and physical properties during surgery. First it allowed us to refine the theorical nomenclature previously proposed for MRONJ (Odet et al., 2021). Second it assisted us in the practical aspects of our clinical study (Odet et al., 2022).
Of the four techniques evaluated, only two proved to be useful in MRONJ surgery: implantation with complete coverage and implantation with partial coverage. In both techniques, the hAM was very stable as it adhered to the bone and did not move when placing sutures above it. The common aspect of these the two techniques was that wet hAM was buried between the bone and mucosa, which increased its stability.
In contrast, there was no burying of hAM in the apposition technique. Compared to the initial nomenclature, the hAM was not sutured due to its fragility. Thus, wet hAM applied without burying on mucosa/bone nor suturing was unstable and the instability increased with suturing of the gingiva above it. Similarly, the absence of burying in the covering graft technique made hAM unstable on mucosa/bone. In this last technique, suturing of hAM to the gingiva was the hardest part. Suturing of hAM to the mucosa shifted the allograft from the surgical site and made it fold upon itself. This makes hAM unsuitable for the suturing performed during oral surgery. Indeed, the dimensions of the suture material usually range from 3/0 (largest) to 6/0 (thinnest). These types of sutures lacerated the hAM because it is relatively thin. This is in contrast with hAM use in ophthalmology where the allograft is always sutured with smaller suture material—10/0 nylon or 8/10 to 10/0 VICRYL or PROLENE sutures (Sippel et al., 2001)—which produce less cracking of the hAM.
Odet’s review of literature distinguished two types of hAM application in the oral cavity (Odet et al., 2021). First, hAM could be used as an “implanted graft material” in periodontology and implantology. In these cases, the procedure was similar to our “implantation with complete coverage” technique, as the hAM was completely covered by the mucosa. Second, hAM was used as a “covering graft material” in mucosal defects of the oral cavity or in mandibular vestibuloplasties. In these cases, hAM was either directly sutured to the adjacent mucosa or simply applied on the defect to be filled and secured by any means (splints, sutured gauze, etc.) (Samandari et al., 2004; Arai et al., 2012; Amemiya et al., 2015). Here, this second type of surgery involves suturing of hAM which makes it unsuitable to MRONJ.
This technical note supplements the existing literature (Dua and Azuara-Blanco, 1999; Letko et al., 2001; John, 2003) and provides information on how to handle cryopreserved hAM in MRONJ. Detailed and novel illustrations are provided to assist maxillofacial and oral surgeons who want to use hAM in this application.
Conclusion
This technical note showed that hAM implantation with complete or partial coverage techniques is the preferred choice in an ex vivo MRONJ model. Directly suturing to the adjacent mucosa is hardly feasible because of the suture size and the relative thinness of hAM. In oral surgery, cryopreserved hAM has adequate adherence to both bone and mucosa and good stability once applied. This technical note also describes tips and tricks on hAM handling and provides practical illustrations to assist maxillofacial and oral surgeons in hAM application.
Data availability statement
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical review and approval was not required for the animal study because porcine jaw specimens.
Author contributions
FG, CM, LT, and SO elaborated the design of the study and organized the educational school at the University. FG supervised the training. SO and LS taught the technique to the surgeons. CM, EW, BC, EE, AB, and AL did the experimentations. TG elaborated the illustrations. AP studied the methodology to transfer it to clinical situation. FP provided the hAM. SO and FG wrote the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
This study was supported by a grant from the French Ministry of Health (PHRCI-2020). This publication is based upon work from COST Action 17116 “SPRINT”, supported by COST (European Cooperation in Science and Technology)—www.cost.eu.
Acknowledgments
The authors are grateful to Éleveurs de la Chevillotte (Valdahon, Besançon) and Société Bisontine d'Abattage-SBA (Besançon, France) for porcine mandible specimens; Hughes Grandin (Laboratoire d’Anatomie, Université de Franche-Comté, Besançon) for his high availability; TG (thomas-gualdi.fr) for the high quality of his illustrations and Franck Daval (Bibliothèque Universitaire Santé, Université Bourgogne Franche-Comté, Besançon, France) for the very helpful bibliographic support. The authors acknowledge the language support provided by Joanne Archambault.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Amemiya, T., Nakamura, T., Yamamoto, T., Kinoshita, S., and Kanamura, N. (2015). Autologous transplantation of oral mucosal epithelial cell sheets cultured on an amniotic membrane substrate for intraoral mucosal defects. PLoS One 10, e0125391. doi:10.1371/journal.pone.0125391
Arai, N., Tsuno, H., Okabe, M., Yoshida, T., Koike, C., Noguchi, M., et al. (2012). Clinical application of a hyperdry amniotic membrane on surgical defects of the oral mucosa. J. Oral Maxillofac. Surg. 70, 2221–2228. doi:10.1016/j.joms.2011.09.033
Bourgeois, M., Loisel, F., Obert, L., Pluvy, I., and Gindraux, F. (2019). Can the amniotic membrane be used to treat peripheral nerve defects? A review of literature. Hand Surg. Rehabilitation 38, 223–232. doi:10.1016/j.hansur.2019.05.006
Chen, B., Jones, R. R., Mi, S., Foster, J., Alcock, S. G., Hamley, I. W., et al. (2012). The mechanical properties of amniotic membrane influence its effect as a biomaterial for ocular surface repair. Soft Matter 8, 8379–8387. doi:10.1039/c2sm26175h
Deppe, H., Wolff, C., Bauer, F., Ruthenberg, R., Sculean, A., and Mücke, T. (2018). Dental implant surfaces after insertion in bone: An in vitro study in four commercial implant systems. Clin. Oral Investig. 22, 1593–1600. doi:10.1007/s00784-017-2262-4
Dua, H. S., and Azuara-Blanco, A. (1999). Amniotic membrane transplantation. Br. J. Ophthalmol. 83, 748–752. doi:10.1136/bjo.83.6.748
Etchebarne, M., Fricain, J.-C., Kerdjoudj, H., Di Pietro, R., Wolbank, S., Gindraux, F., et al. (2021). Use of amniotic membrane and its derived products for bone regeneration: A systematic review. Front. Bioeng. Biotechnol. 9, 661332. doi:10.3389/fbioe.2021.661332
Fenelon, M., B Maurel, D., Siadous, R., Gremare, A., Delmond, S., Durand, M., et al. (2019). Comparison of the impact of preservation methods on amniotic membrane properties for tissue engineering applications. Mater. Sci. Eng. C 104, 109903. doi:10.1016/j.msec.2019.109903
Fenelon, M., Catros, S., and Fricain, J. C. (2018). What is the benefit of using amniotic membrane in oral surgery? A comprehensive review of clinical studies. Clin. Oral Investig. 22, 1881–1891. doi:10.1007/s00784-018-2457-3
Fénelon, M., Catros, S., Meyer, C., Fricain, J.-C., Obert, L., Auber, F., et al. (2021). Applications of human amniotic membrane for tissue engineering. Membranes 11, 387. doi:10.3390/membranes11060387
Fénelon, M., Chassande, O., Kalisky, J., Gindraux, F., Brun, S., Bareille, R., et al. (2018). Human amniotic membrane for guided bone regeneration of calvarial defects in mice. J. Mat. Sci. Mat. Med. 29, 78. doi:10.1007/s10856-018-6086-9
Fenelon, M., Etchebarne, M., Siadous, R., Grémare, A., Durand, M., Sentilhes, L., et al. (2021). Comparison of amniotic membrane versus the induced membrane for bone regeneration in long bone segmental defects using calcium phosphate cement loaded with BMP-2. Mater. Sci. Eng. C 124, 112032. doi:10.1016/j.msec.2021.112032
Fenelon, M., Etchebarne, M., Siadous, R., Grémare, A., Durand, M., Sentilhes, L., et al. (2020). Assessment of fresh and preserved amniotic membrane for guided bone regeneration in mice. J. Biomed. Mat. Res. A 108, 2044–2056. doi:10.1002/jbm.a.36964
Gindraux, F., Laurent, R., Nicod, L., De Billy, B., Meyer, C., Zwetyenga, N., et al. (2013). Human amniotic membrane: Clinical uses, patents and marketed products. Recent Pat. Regen. Med. 3, 193–214. doi:10.2174/22102965113039990021
Gindraux, F., and Obert, L. (2010). “Human amniotic membranes: Benefits for bone repair/regeneration,” in Bioreconstruction : De l’os à la peau tome 2. Editor S. M. France, 85–91.
Gindraux, F., Rondot, T., De Billy, B., Zwetyenga, N., Fricain, J.-C., Pagnon, A., et al. (2017). Similarities between induced membrane and amniotic membrane: Novelty for bone repair. Placenta 59, 116–123. doi:10.1016/j.placenta.2017.06.340
Gremare, A., Jean-Gilles, S., Musqui, P., Magnan, L., Torres, Y., Fenelon, M., et al. (2019). Cartography of the mechanical properties of the human amniotic membrane. J. Mech. Behav. Biomed. Mat. 99, 18–26. doi:10.1016/j.jmbbm.2019.07.007
Gualdi, T., Laurent, R., Moutarlier, V., Fenelon, M., Nallet, A., Pouthier, F., et al. (2019). In vitro osteodifferentiation of intact human amniotic membrane is not beneficial in the context of bone repair. Cell Tissue Bank. 20, 435–446. doi:10.1007/s10561-019-09778-3
Gulameabasse, S., Gindraux, F., Catros, S., Fricain, J. C., and Fenelon, M. (2020). Chorion and amnion/chorion membranes in oral and periodontal surgery: A systematic review. J. Biomed. Mat. Res. 109, 1216–1229. doi:10.1002/jbm.b.34783
John, T. (2003). Human amniotic membrane transplantation: Past, present, and future. Ophthalmol. Clin. North Am. 16, 43–65. vi. doi:10.1016/s0896-1549(02)00110-4
Kniha, K., Buhl, E. M., Hermanns-Sachweh, B., Al-Sibai, F., Bock, A., Peters, F., et al. (2021). Implant removal using thermal necrosis—An in vitro pilot study. Clin. Oral Investig. 25, 265–273. doi:10.1007/s00784-020-03361-x
Laurent, R., . Brennan, M., . Renaud, A., . D'arros, C., . Obert, L., . Layrolle, P., et al. (2014b). Osteodifferenciation of intact human amniotic membrane through a jet sprayed polycaprolactone nanofibre scaffold. Orthop. Proc. 96, 113.
Laurent, R., Nallet, A., De Billy, B., Obert, L., Nicod, L., Meyer, C., et al. (2017). Fresh and in vitro osteodifferentiated human amniotic membrane, alone or associated with an additional scaffold, does not induce ectopic bone formation in Balb/c mice. Cell Tissue Bank. 18, 17–25. doi:10.1007/s10561-016-9605-2
Laurent, R., Nallet, A., Obert, L., Nicod, L., and Gindraux, F. (2014c). Storage and qualification of viable intact human amniotic graft and technology transfer to a tissue bank. Cell Tissue Bank. 15, 267–275. doi:10.1007/s10561-014-9437-x
Laurent, R., . Nicod, L., . Layrolle, P., . de Billy, B., . Obert, L., and . Gindraux, F. (2014a). Osteogenic potential and immunogenicity of human amniotic membrane: In vitro and in vivo studies. Orthop. Proc. 96-B, 112.
Letko, E., Stechschulte, S. U., Kenyon, K. R., Sadeq, N., Romero, T. R., Samson, C. M., et al. (2001). Amniotic membrane inlay and overlay grafting for corneal epithelial defects and stromal ulcers. Arch. Ophthalmol. 119, 659–663. doi:10.1001/archopht.119.5.659
Obert, L., Genestier, L., Froidevaux, L., Averlant, E., Laurent, R., Wajszczak, L., et al. (2012). “Amniotic membrane for bone repair? Reflection around of the masquelet technique to one stage/membrane amniotique pour la réparation osseuse ? Réflexion autour de la simplification de la technique de Masquelet à une chirurgie,” in Technique de Masquelet. Sauramps médical.
Odet, S., Louvrier, A., Meyer, C., Nicolas, F. J., Hofman, N., Chatelain, B., et al. (2021). Surgical application of human amniotic membrane and amnion-chorion membrane in the oral cavity and efficacy evaluation: Corollary with ophthalmological and wound healing experiences. Front. Bioeng. Biotechnol. 9, 685128. doi:10.3389/fbioe.2021.685128
Odet, S., Meyer, C., Gaudet, C., Weber, E., Quenot, J., Derruau, S., et al. (2022). Tips and tricks and clinical outcome of cryopreserved human amniotic membrane application for the management of medication-related osteonecrosis of the jaw (MRONJ): A pilot study. Front. Bioeng. Biotechnol. 10, 936074. doi:10.3389/fbioe.2022.936074
Ragazzo, M., Trojan, D., Spagnol, L., Paolin, A., and Guarda Nardini, L. (2018). Use of amniotic membrane in the treatment of patients with BRONJ: Two case reports. J. Surg. Case Rep. 2018, rjy073. doi:10.1093/jscr/rjy073
Ragazzo, M., Val, M., Montagner, G., Trojan, D., Fusetti, S., and Guarda Nardini, L. (2021). Human amniotic membrane: An improvement in the treatment of medication-related osteonecrosis of the jaw (MRONJ)? A case–control study. Cell Tissue Bank. 23 (1), 129–141. doi:10.1007/s10561-021-09922-y
Samandari, M. H., Yaghmaei, M., Ejlali, M., Moshref, M., and Saffar, A. S. (2004). Use of amnion as a graft material in vestibuloplasty: A preliminary report. Oral Surg. Oral Med. Oral Pathology, Oral Radiology, Endodontology 97, 574–578. doi:10.1016/j.tripleo.2003.10.031
Keywords: amniotic membrane, porcine jaw, oral mucosa, xenograft, ex vivo, osteonecrosis of the jaw and illustrations
Citation: Odet S, Solecki L, Meyer C, Weber E, Chatelain B, Euvrard E, Barrabé A, Gualdi T, Parmentier A-L, Tatu L, Pouthier F, Louvrier A and Gindraux F (2022) Human amniotic membrane application in oral surgery—An ex vivo pilot study. Front. Bioeng. Biotechnol. 10:968346. doi: 10.3389/fbioe.2022.968346
Received: 13 June 2022; Accepted: 23 September 2022;
Published: 24 October 2022.
Edited by:
Heinz Redl, Institute for Experimental and Clinical Traumatology (LBG), AustriaReviewed by:
Jingang An, Peking University Hospital of Stomatology, ChinaJochen Salber, Ruhr-University Bochum, Germany
Copyright © 2022 Odet, Solecki, Meyer, Weber, Chatelain, Euvrard, Barrabé, Gualdi, Parmentier, Tatu, Pouthier, Louvrier and Gindraux. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Florelle Gindraux, ZmdpbmRyYXV4QGNodS1iZXNhbmNvbi5mcg==