 Anja Kalch1*
Anja Kalch1* Constanze Küchler1
Constanze Küchler1 Aliscia Rebecca Albani1
Aliscia Rebecca Albani1 Helena Bilandzic1
Helena Bilandzic1 Simone Fischer2,3
Simone Fischer2,3 Inge Kirchberger2,3
Inge Kirchberger2,3- 1Department for Media, Knowledge and Communication, University of Augsburg, Augsburg, Germany
- 2Epidemiology, Medical Faculty, University of Augsburg, Augsburg, Germany
- 3Institute for Medical Information Processing, Biometry and Epidemiology (IBE), LMU München, Munich, Germany
The inclusion of narratives in evidence-based patient information is a heavily discussed topic in literature. Narratives elicit intense engagement and emotional insights, but may also cause unintended persuasion effects. There is mixed evidence that adding narratives to non-narrative factual patient information is valuable for patients. In addition, providing patients with narratives about the outcome of treatments has been found to bias treatment decisions, in line with the direction implied by the narratives. This may counteract informed decision making of patients. However, narratives about the process of a treatment and personal experiences with treatments may support the well-being of patients in tertiary prevention. In order to investigate patients' views on narratives and their function in patient information, we conducted 26 semi-structured qualitative interviews with pulmonary embolism patients. Answers were coded using thematic analysis. Results show that patients are especially interested in experience and process narratives when combined with evidence-based patient information. We identified four main functions of experience and process narratives that patients ascribe to these narratives: (1) motivating self-reflection and reflection on the recovery process, (2) reducing the feeling of loneliness, (3) reducing emotional distress, and (4) inspiring mindful mastery.
Introduction
After stroke and myocardial infarction, pulmonary embolism is the third most frequent acute heart-related disease worldwide (Wendelboe and Raskob, 2016; Barco et al., 2021). About 50% of the patients surviving pulmonary embolism suffer from long-term physical limitations (6 months to 3 years), in particular from ongoing dyspnea, difficulties in physical performance and an overall reduced health status (Klok et al., 2010a, 2014; Klok and Barco, 2018). Related to these physical limitations, pulmonary embolism also affects patients' psychological well-being considerably (Noble et al., 2014; Erickson et al., 2019; Tran et al., 2021). Even if the awareness about the relevance of well-being of pulmonary embolism patients has increased in the last years (Rolving et al., 2020), knowledge on how to support patients is still underdeveloped (Tran et al., 2021).
Given that patients express high informational deficits after the acute treatment, research agrees that providing evidence-based information would be a first relevant step for improving patient care after hospital release (Kirchberger et al., 2020). In addition to providing patients with information related to the illness in general, research indicates that information that addresses patients' psychological and emotional needs has promising effects (Feehan et al., 2017; Hunter et al., 2017; Kirchberger et al., 2020). It is argued that this information helps patients reflect on their existing anxieties and worries as well as creates a sense of positive mindfulness (Feehan et al., 2017; Hunter et al., 2017; Kirchberger et al., 2020). A combination of non-narrative factual information (that is typical for patient information) and narratives seems to be a good approach to both, address the information deficit and (via the narratives) “provide important emotional or social information which is typically lacking in routine health information resources” (Bennett et al., 2015, p. 2033).
Narratives are broadly defined as “the representation of an event or series of events” (Abbott, 2001, p. 13), and includes at least one character who is involved in the events (Bilandzic and Busselle, 2013). In addition to this plot-focused perspective, an experience-oriented perspective on narratives is important (Fludernik, 1996), in which the narratives provide insight into feelings, thoughts, and goals of characters. This corresponds to the patients' need for emotional information (Bennett et al., 2015). Overall, this definition includes a great variety of narratives, ranging from short patient testimonials about treatment procedures to complex book-length stories, written by patients about their health-related experiences (Green, 2006). In this paper, we focus on patient narratives that give insight into patient experiences with treatment procedures, a specific illness or the recovery process and that are used as examples in health brochures or other similar types of health information (Shaffer and Zikmund-Fisher, 2013).
However, guidelines for the development of patient information are rather skeptical about narratives and do not recommend their inclusion in evidence-based health information (Lühnen et al., 2017; Shaffer et al., 2021). Evidence-based patient information “intends to incorporate science and rigor of evidence-based medicine with the personal values of consumers and patients” (Bunge et al., 2010, p. 316). Therefore, evidence-based patient information should be easy to read and use as well as contain relevant, comprehensive, up-to-date factual information reflecting “the highest standards of scientific accuracy” (Coulter, 1998; see also Goldsmith et al., 2007; Bunge et al., 2010). Evidence-based patient information is usually non-narrative, but has an objective and factual form of presentation. Narratives often do not reach the high-quality requirements for evidence-based patient information, and they run the risk of biasing persuasion toward a single case. In addition, there is limited evidence for beneficial effects (Shaffer et al., 2021). However, this criticism insufficiently considers the multidimensionality of narratives, “varying systematically in their purpose, content, and evaluative valence” (Shaffer and Zikmund-Fisher, 2013, p. 10). Taking into account the diversity of narratives, different sub-dimensions of patient narratives need to be discussed separately (Shaffer and Zikmund-Fisher, 2013; Shaffer et al., 2021). Based on such a differentiation of narratives, the criticism mainly applies to “outcome narratives” (stories addressing the question whether treatments were successful or not, Shaffer et al., 2013a) in decision aids and their potential to bias patients' treatment decisions (Shaffer et al., 2021). While it is plausible that narrative biases are problematic for decision behavior since they may influence a decision in a specific direction, other subjective patient-centered outcomes that are unrelated to decisional behavior, such as patients' well-being, are not at risk to be negatively affected in this regard. Similarly, while narratives focusing on treatment outcomes are prone to influence decision behavior of patients, this is not the case for narratives that neither give information about treatment decisions nor its outcomes, but give insights into the diagnosis, experiences with an illness or the recovery process. Specifically, we suggest that two types of stories may serve relevant functions above and beyond outcome narratives: Stories that inform patients about the process of diagnosis and treatment (“process narratives”) and stories that give an account of experiences of other patients, their thoughts and feelings (“experience narratives”) (Shaffer and Zikmund-Fisher, 2013; Shaffer et al., 2013a). However, these effects are rarely investigated, and specific recommendations do not exist yet. The present study addresses this research gap and investigates (1) what types of narratives patients experience as helpful in evidence-based patient information and (2) what well-being related functions patients associate with narratives.
Given that evidence-based patient information is subject to strict quality standards, qualitative research offering insights into the types and their functions of narratives is the first step to develop and finally include patient narratives in patient information on pulmonary embolism (Shaffer et al., 2021). We therefore conducted a two-stage qualitative interview study. In the first stage, we interviewed patients about their own experiences and their expectations toward patient narratives in patient information; in the second stage, patients received a prototype of an evidence-based patient information including 12 patient narratives from the first stage and evaluated the prototype in general, and patient narratives in particular.
Psychological well-being of pulmonary embolism patients
In existing medical research on pulmonary embolism, well-being is mainly addressed from a pathological perspective (Ryff, 1989a; Huppert and So, 2013), focusing on anxieties and depression of patients (Tran et al., 2021) as well as a reduced quality of life (Klok et al., 2010a; van Es et al., 2013). This focus partly corresponds to a hedonic well-being perspective (also discussed under the term “subjective well-being;” Ryan and Deci, 2001). In this line of research, well-being is considered “in terms of pleasure vs. pain” (Ryan and Deci, 2001, p. 144), focusing on the potential to increase happiness and the cognitive evaluation of life while at the same time minimizing negative affective experiences (Diener and Lucas, 1999; Diener et al., 2011). Typically, three different facets of hedonic well-being are differentiated: life-satisfaction, the absence of negative affect and the presence of positive affect (Andrews and Withey, 1976; Diener and Lucas, 1999; Ryan and Deci, 2001; Diener et al., 2011). Even if positive mood is hardly regarded in research on pulmonary embolism, the two other dimensions of hedonic well-being are addressed. While perceived quality of life closely relates to life-satisfaction (Pavot and Diener, 2008), anxiety and depression include the presence of negative mood states and are both well-established indicators for subjective well-being (Reer et al., 2019).
Apart from this strong focus on negative aspects of hedonic well-being, qualitative studies on psychological consequences of pulmonary embolism (e.g., Noble et al., 2014; Kirchberger et al., 2020) also implicitly address aspects of eudaimonic well-being (also discussed as psychological well-being; Ryan and Deci, 2001). In contrast to hedonic well-being, eudaimonic well-being refers to well-being not as the presence of happiness (Ryan and Deci, 2001) but as the “realization of human potential” (Ryff, 2018, p. 375). Eudaimonic well-being often is divided into six different facets: self-acceptance, personal growth, autonomy, purpose in life, environmental mastery, and positive relatedness to others (Ryff, 1989a,b). Of these six, self-acceptance is conceptualized as one of the key facets of eudaimonic well-being, reflecting a persons' positive attitude toward the self, awareness about personal strength but also acceptance of existing weaknesses (Ryff, 1989a,b, 2018). This is also related to personal growth, the feeling that the self continues to grow and develop further (Ryff, 1989b, 2018). Autonomy covers to what extent people have an internal focus of self-evaluation and act in a self-determined way (Ryff, 2018). In contrast, environmental mastery focuses on processes outside of the self and asks how well people are able to adapt to changes in the surroundings (Ryff, 2018). Related to this, purpose in life refers to the feeling that life is relevant and appreciated (Ryff, 1989b). Finally, positive relationships to others refer to the ability to have warm relationships, including friendships as well as love (Ryff and Keyes, 1995; Ryff, 2018). While self-acceptance and environmental mastery have been shown to empirically correlate with indicators for hedonic well-being (for example depression and life satisfaction), the four other dimensions are only weakly related or not at all (Ryff and Keyes, 1995). Thus, literature calls for a distinct consideration of hedonic and eudaimonic aspects of well-being (Ryan and Deci, 2001; Reinecke and Oliver, 2016).
Hedonic well-being of pulmonary embolism patients
In qualitative studies about psychological effects of pulmonary embolism, patients frequently report anxiety and depression, which are markers of a reduced well-being of patients (Feehan et al., 2017; Hunter et al., 2017; Rolving et al., 2019; Kirchberger et al., 2020). Compared to population-based controls, pulmonary embolism patients show significantly higher levels of depression and anxiety (Liu et al., 2011; Chuang et al., 2019; Erickson et al., 2019). Studies also show that several mental health related dimensions of quality of life (for example emotional health limitations, mental health, social functioning) are substantially weaker for pulmonary embolism patients than for the overall population, especially immediately after diagnosis (Klok et al., 2010a; van Es et al., 2013; Kahn et al., 2017; Erickson et al., 2019). Some patients even develop posttraumatic stress disorder following the life-threatening experience (Noble et al., 2014; Hunter et al., 2017).
The diagnosis itself, the life-threatening experience, as well as limiting physical consequences are known to evoke negative mood responses and depression (Liu et al., 2011; Hunter et al., 2017; Tran et al., 2021). In addition, the ongoing symptoms and physical limitations cause fatigue in patients, which is related to depression (Rolving et al., 2019). As emergent stressors, patients report fears about recurring events, potential bleeding risks due to anticoagulant treatment, uncertainties about the cause of the pulmonary embolism as well as insecurities about the long-term health consequences (Noble et al., 2014; Feehan et al., 2017; Hunter et al., 2017; Kirchberger et al., 2020).
Eudaimonic well-being of pulmonary embolism patients
Eudaimonic well-being is not directly addressed in literature about psychological effects of pulmonary embolism, but various results of qualitative studies with patients relate to its sub-dimensions.
Pulmonary embolism patients describe the need to accept physical weaknesses and perceived vulnerability as an obstacle (Rolving et al., 2019). Patients also struggle with their identity after experiencing pulmonary embolism (Noble et al., 2014; Hunter et al., 2017).
Related to life purpose, patients experience pulmonary embolism as a fundamentally life-changing event. Patients also tend to compare their current situation to their life before the pulmonary embolism as well as to other people in their age group, giving them the feeling that they are not able keep up with them (Noble et al., 2014). This upwards social comparison is related to a reduced autonomy (Ryff, 2018).
To some extent, patients also emphasize a decrease of positive relationships with others. In qualitative studies, they report feelings of social isolation (Hunter et al., 2017, 2019; Kirchberger et al., 2020) and identify the lack of emotional support. Other patients, however, also complained about feeling overprotected by their social environment (Rolving et al., 2019; Kirchberger et al., 2020).
Environmental mastery encompasses whether people are able to use their environment well and adapt it to their personal needs (Ryff, 1989b, 2018). Especially in the time following the acute pulmonary embolism event, this adaptation process is a barrier for patients (Noble et al., 2014). Instead of adapting and reorienting, highly anxious patients report avoiding adaptation efforts (Hunter et al., 2017).
Apart from these negative facets of eudaimonic well-being, most qualitative studies also describe that patients experience a positive re-evaluation of life (Hunter et al., 2017, 2019; Rolving et al., 2019). Specifically, the possibility of changing their life and setting new preferences are emphasized as positive consequences of the pulmonary embolism event (Noble et al., 2014; Feehan et al., 2017). This appreciation of a new orientation in life has parallels to personal growth as sixth subdimension of eudaimonic well-being (Ryff, 1989a).
Information deficit and patients' well-being
After the acute pulmonary embolism event, patients experience a general lack of information about various aspects of their illness, the treatment, the recovery process, as well as how the illness is going to impact their life, which decreases patients' well-being (Bennett et al., 2016; Kirchberger et al., 2020). Typically, patients are treated in hospital for the acute event and clinical guidelines recommend a follow-up check-up after 3–6 months (Konstantinides et al., 2020). This fits well to the medical-physiological needs. However, results from empirical studies show that patients perceive a lack of care precisely because they lack information after leaving the hospital (Hunter et al., 2017; Kirchberger et al., 2020). While results about patients' satisfaction with general information about symptoms, medication or risk factors are mixed (Bennett et al., 2016; Hunter et al., 2017; Kirchberger et al., 2020), empirical studies in particular show that patients lack information on emotional and psychological consequences as well as their long-term health prognosis (Bennett et al., 2016; Feehan et al., 2017).
Given that patients with a decreased well-being complain about a lack of information about psychological long-term consequences (Kirchberger et al., 2020), it is likely that reduced well-being and information deficits are related. Researchers recommend that patient information help patients accept their situation, deal with the ongoing risks, reflect on their situation and develop a sense of positive mindfulness (Bennett et al., 2016; Feehan et al., 2017). In other words, they seek to improve their well-being. At the same time, patient information should be high in quality and easily accessible (Erickson et al., 2019). While adding narratives to factual evidence-based patient information seems to be a promising strategy to satisfy these informational needs (Bennett et al., 2015) and to support patients' well-being, guidelines do not recommend narratives in patient information (Elwyn et al., 2006; Shaffer et al., 2021). In order to address this conflict, we consider the criticism of narratives in detail.
Critical arguments against using narratives in patient information
Guidelines and recommendations for the development of patient information are skeptical about including narratives (Elwyn et al., 2006; Lühnen et al., 2017; Shaffer et al., 2021). They either do not recommend narratives at all (Lühnen et al., 2017), question their usefulness (Elwyn et al., 2006) or do not consider them as a required element (Bekker et al., 2013; Shaffer et al., 2021). The reasons for this skepticism can be seen in (1) the risk of persuasion biases and potential harmful effects, (2) limited evidence for beneficial effects of adding narratives to health information, and (3) the strict quality requirements for narratives in patient information. We will discuss these points in the following sections.
Persuasion biases of narratives in patient information
The first critical point of using narratives in patient information relates to its persuasive potential and the risk to cause biases in decision making and behavior (Winterbottom et al., 2008; Betsch et al., 2015; Haase et al., 2015; Drewniak et al., 2020). While a neutral comparison of two treatment options based on medical facts may help patients to weigh pros and cons, an emotional and engaging patient story about a decision for a specific treatment and against the other treatment options may persuade patients and prevent a rational weighing up of the two treatment options. Such a bias is contrary to guidelines for the development of patient information, and their standard to provide neutral evidence-based information without decisional biases (Bekker et al., 2013; Lühnen et al., 2017; Shaffer et al., 2021). Patients should be supported in informed decision making by high quality evidence-based health information and protected from harmful effects due to negative persuasion effects (Shaffer et al., 2021).
Theoretically, the high persuasive power of narratives is explained with the potential of narratives to intensely engage readers or viewers with the story and to reduce defensive processes (for an overview see Bilandzic and Busselle, 2013) as well as to facilitate affective modes of information processing and risk decisions (for an overview see Shaffer et al., 2014). There is indeed a great amount of research showing the persuasive potential of health messages empirically, particularly in the context of primary health prevention and detection behavior on different outcome variables. For example, a systematic review by de Graaf et al. (2016) shows that narrative health messages are more influential for health-related behavioral intentions (for example intentions for physical activity) than control conditions (either statistical messages, or other non-narrative conditions) when a healthy behavior is depicted in the narratives. Similarly, a meta-analysis by Shen et al. (2015), two systematic reviews (Perrier and Martin Ginis, 2017, 2018) and a meta-analysis focusing only on Afro-American women (Ballard et al., 2021) found small but robust persuasion effects of narratives on health behavior and intentions for different types of detection and prevention measures.
The persuasive power of narratives is seen as particularly problematic when treatment decisions are biased, especially when this bias contradicts medical treatment recommendations (Haase et al., 2020), or when decisional conflicts are present (Syrowatka et al., 2016). A systematic review on computer-based decision aids shows that decisional conflict increases and knowledge decreases when decision aids include patient narratives (Syrowatka et al., 2016).
Even if such a bias does not automatically occur (Shaffer et al., 2014), there is ample empirical evidence that narratives may have unwanted negative persuasive effects (Winterbottom et al., 2008; Ziebland and Wyke, 2012). Several studies show that narratives about adverse effects may override statistical information on vaccination risks and thus negatively affect vaccination intentions (Betsch et al., 2011, 2013, 2015; Haase et al., 2020). Similar biasing effects of narratives overriding statistical information were also shown in the context of hypothetical treatment choices against angina (Ubel et al., 2001). Apart from this narrative bias in comparison to statistical data, single narratives have also been shown to unintentionally influence patients' decisions. In this vein, a newspaper story about rare side-effects of over-the-counter medication (Shaffer et al., 2018b), decreased readers' medication use. Relating to the source of the narrative, patient stories about dialysis modalities also have been shown to influence other patients' decisions more than treatment information provided by a doctor (Winterbottom et al., 2012).
Given the interplay of beneficial as well as unwanted persuasion effects, narratives are perceived as a double-edged sword: “while a compelling, persuasive narrative can save lives (for example by increasing uptake of cancer screening), an equally compelling, but misinformed, narrative can cost lives (for example decrease vaccinations)” (Shaffer et al., 2018a, p. 438).
Limited evidence for beneficial effects of adding narrative information
The second criticism of including narratives in patient information concerns the limited evidence of beneficial effects of adding narratives to patient information (Bekker et al., 2013; Lühnen et al., 2017; Shaffer et al., 2021). In this line of reasoning, narratives are typically compared to statistical evidence. Indeed, empirical evidence about the comparison of narratives and statistical information is mixed and effects vary for example depending on the dependent variables in question (Zebregs et al., 2015). For example, a meta-analysis by Zebregs et al. (2015) shows that narratives have a stronger effect on intentions compared to statistical evidence (Zebregs et al., 2015), which again is in line with the persuasive potential and the risk for decision biases. However, the effect is reversed for attitudes and beliefs (Zebregs et al., 2015). In contrast to this, a systematic review by Perrier and Martin Ginis (2017) does not find evidence for a greater efficacy of narrative health messages over statistical messages on intentions for detection behavior. The studies included in the systematic review only show an effect of narratives over no message conditions (Perrier and Martin Ginis, 2017). Similarly, a second systematic review focusing on health promotion behavior (Perrier and Martin Ginis, 2018) did not find evidence for differential effects of narratives and statistical information on health related attitudes as well as knowledge and only mixed evidence for effects on intentions (Perrier and Martin Ginis, 2018).
Given this limited evidence for a potential advantage of narrative over statistical information, and the risk for decision biases or unwanted persuasion effects, guidelines do not issue a recommendation for using narratives as an integral part of patient information (Lühnen et al., 2017; Shaffer et al., 2021).
High quality requirements
Developing evidence-based patient information is a complex process that involves meeting high quality standards overall (Lühnen et al., 2017; Shaffer et al., 2021). Consequently, compiling and editing patient stories for information materials requires a process that corresponds with these high quality standards and considers ethical guidelines in particular (Shaffer et al., 2021). Otherwise, patient stories run the risk of causing a distorted and unbalanced impression and may lead to negative psychological outcomes like confusion and anxiety, and ultimately to worse decision making (Ziebland and Wyke, 2012). Patients themselves emphasize the need of narratives to correspond with high quality standards and report on the danger of unreliable or misinformation through patient stories (Osaka and Nakayama, 2017). In this vein, patients emphasize the relevance that patient experiences be precise, reliable, and balanced (Newman et al., 2009). In order to reflect these quality requirements, the checklist to assess the quality of patient information from the international decision aids standard collaboration (IPDAS), lists three additional criteria for information material including patient stories (O'Connor et al., 2005). Following these requirements, patient information using stories should include a declaration of potential financial benefits patients received for sharing their stories, provide evidence that patients agreed to use their stories and use a range of positive as well as negative patient stories (O'Connor et al., 2005). Regarding the content of the stories used, Shaffer et al. (2021) also recommend clarifying which elements of the IPDAS checklist the patient story supports as well as how narrative dimensions (for example narrators point of view, resolution) are presented (see also Thompson and Kreuter, 2014). In order to develop patient information including narratives it is therefore recommended to base the development on qualitative research, that enables detailed insights into patients' experiences, their needs and expectations (Lühnen et al., 2017; Shaffer et al., 2021).
In sum, the practical implementation process may be challenging and the effort should be in a reasonable relation to the expected benefit (Shaffer et al., 2021). Given that the expected added value is questioned by guidelines and recommendations, it follows that the costs for the implementation and development process are also questioned. This is in particular the case, when narratives need to be extensively recorded and edited; statistical data, on the other hand, is more easily available. However, this comparison of narratives and statistical information implies that both types of evidence have the same function and therefore can be used interchangeably. While this may be the case for narratives focusing on treatment outcomes and statistics (Shaffer and Zikmund-Fisher, 2013), stories giving insight into the inner world of patients, their feelings, thoughts and experiences of the illness may not be adequately be replaced by statistical information, for example frequencies of depression and anxieties.
Beyond persuasion effects of outcome narratives in patient information
Most ongoing discussions about using narratives in patient information are limited to specific health decision situations. The focus is on situations where treatment decisions are made and on narratives that provide information about treatment outcomes. However, various different purposes and types of narrative effects in health communication have been identified beyond persuasion, including for example patient engagement, provision of information, modeling behavior or providing comfort (for an overview see Green, 2006; Shaffer et al., 2018a; Drewniak et al., 2020). In this vein, research suggests that pulmonary embolism patients do not primarily lack information about specific treatments or patient experiences with these treatments but search for information that helps to improve their well-being (Bennett et al., 2016; Feehan et al., 2017). In order to address such needs, it is necessary to have (1) a multi-faceted view on narrative content beyond outcome-related narratives as well as (2) a differentiated concept of narrative outcomes.
Differentiating types of patient narratives and their specific effects
Shaffer and Zikmund-Fisher (2013) provided a taxonomy of narratives, differentiating outcome narratives, experience narratives and process narratives to reflect the various effects of narratives, their content and purpose. While outcome narratives directly address physical and psychological consequences of treatment decisions, and run the risk of causing unwanted persuasion biases, this is not the case for experience and process narratives (Shaffer and Zikmund-Fisher, 2013; Shaffer et al., 2013a). On the one hand, process narratives offer insights into processes and strategies patients use during their illness and in particular give information about decisional steps as well as cognitive decision dimensions. They are described as means to model patient behavior as well as to inform and engage patients (Shaffer and Zikmund-Fisher, 2013; Shaffer et al., 2018a). On the other hand, experience narratives focus on patients' experiences with a disease and emphasize feelings and thoughts related to how patients deal with their illness. As such, they are perceived as useful to engage and inform patients as well as to satisfy patients' emotional needs (Shaffer et al., 2013a, 2018a). However, empirical evidence about this assumed effect is rather scarce. So far, only one experimental study by Shaffer et al. (2013a) empirically tested the effects of these different narratives by contrasting process and experience narratives about breast cancer treatments. While process narratives motivated a more intense information search behavior, experience narratives enabled healthy women to imagine how the treatment can be experienced. These women also evaluated their hypothetical treatment decision more positively (Shaffer et al., 2013a).
Although studies comparing effects of different narrative types are missing, there are some empirical results supporting the assumptions by Shaffer and Zikmund-Fisher (2013) that specific types of narratives are useful to increase specific patient outcomes. Regarding the effect of process narratives, a study on narrative effects in web-decision aids about breast cancer showed that video narratives including process descriptions increased information search times (Shaffer et al., 2013b).
In terms of experience narratives, studies show that insights into patients' feelings and experiences of medical procedures can reduce affective forecasting errors as well as negative emotions related to these procedures and their consequences (Angott et al., 2013; Shaffer et al., 2016). This is also true for studies using a combination of process and experiential narratives (Woudstra and Suurmond, 2019). Similarly, beneficial effects of narratives providing emotional insights have also been shown for restorative narratives (Fitzgerald et al., 2019). In contrast to a narrative that includes negative experiences, a recovery narrative about a cancer patient focusing on hope and strength decreases negative emotions and increases positive emotional responses of unaffected readers as well as their willingness to help patients with rare diseases (Fitzgerald et al., 2019).
Similarly, related to the concept of experience narratives, Kalch (2019) compared the effect of narratives that give intense insights into emotions and cognitions of patients (narratives high in experientiality) to narratives where these insights were reduced (narratives low in experientiality). For different types of prevention behavior (for example physical activity), narratives high in experientiality increase perceived emotions, identification as well as narrative engagement with the narratives and as a consequence also positively influence readers' self-efficacy about performing the preventive behaviors and intentions. In addition, various results on emotional narratives (narratives including emotional arguments or making emotions explicit) support the assumption that emotions in narratives increase their effectiveness (de Graaf et al., 2016; Shaffer et al., 2021). In this regard, emotional narratives are for example shown to decrease negative affect about colorectal cancer screening and to increase screening intentions (Gavaruzzi et al., 2018) or to reduce binge drinking intentions (Keer et al., 2013). While the results of these studies referring to experientiality or emotional narratives also point in the same direction as studies using experience narratives, there is one important difference: In these narratives, an outcome of specific procedures is included (for example screening decision and the relief afterwards) and they have a persuasive intent, thus they are not singular experience narratives but a mixture of outcome narratives and experience narratives. Similar to outcome narratives, they may again be at risk to cause biases in decision making. As shown in a study by Betsch et al. (2011), narratives high in emotionality that address side-effects of vaccinations increase risk perceptions more than narratives low in emotionality.
Summing up, using process and experience narratives seems promising to support patients' well-being. However, we do not know at this stage whether these are also the kinds of narratives that pulmonary embolism patients would like to read in information materials. We therefore ask the following research question:
RQ1: What type of narratives are patients interested to read in evidence-based information materials?
Well-being related effects of narratives in patient information
Most systematic reviews and meta-analyses focusing on effects of narratives in health communication typically classify effects along decision-related dimensions (for example knowledge), behavior-related dimensions (for example attitudes) and behavior (Winterbottom et al., 2008; Zebregs et al., 2015; de Graaf et al., 2016; Perrier and Martin Ginis, 2017). Effects of narratives in patient information related to the psychological well-being of patients, in contrast, are hardly considered.
Only two systematic reviews have included aspects of hedonic well-being (Rennick-Egglestone et al., 2019b; Drewniak et al., 2020). Focusing on health recovery narratives, a systematic review by Rennick-Egglestone et al. (2019a) identified two qualitative studies showing that recovery narratives about eating disorder (Thomas et al., 2006) as well about psychosis (Williams et al., 2018) have the potential to increase hope and decrease psychological distress. Similar effects of patient narratives on optimistic feelings were also reported by another qualitative study on health recovery narratives for a broad variety of psychological disorders (Rennick-Egglestone et al., 2019b) as well as a qualitative study on the role of patient experiences in health-decision making (Entwistle et al., 2011). However, Osaka and Nakayama (2017) did not find differences between an information booklet including patient narratives and a booklet without patient experiences on early-breast cancer patients' anxieties. Also, a systematic review by Drewniak et al. (2020) shows more heterogeneous results for the effect of narratives to reduce psychological distress and anxiety.
Even if research on specific effects of patient narratives on hedonic well-being is relatively scarce and heterogeneous, it is overall well-documented in literature that narratives have a great potential to evoke emotions consistent with the story (Green et al., 2004; Green, 2006; Dunlop et al., 2010; Volkman and Parrott, 2012). For example, narratives aimed at breast cancer awareness and screening behavior are shown to increase breast cancer-related fears, risk perceptions and mammography intentions (Kreuter et al., 2010; McQueen et al., 2011). Similarly, a study by Volkman and Parrott (2012) on osteoporosis narratives shows that expressed emotions (either positive or negative) in narratives result in an even more intense perception of the same expressed emotions by recipients. In addition, the potential of narratives for emotional coping was investigated in the context of self-effects, using narratives in different medical contexts, such as cancer care therapy (Carlick and Biley, 2004) or trauma therapy (Kaminer, 2006). Writing about one's own experiences has been shown to decrease patients' fears and anxieties and to increase positive emotions (Carlick and Biley, 2004).
Apart from such effects of narratives on hedonic aspects of well-being, a few studies also describe narrative effects on dimensions of eudaimonic well-being, especially regarding positive relationships with others. Different studies on mental health recovery narratives show that stories how other patients managed their illness creates a positive feeling of connectedness to other people and decrease feelings of loneliness in patients (Rennick-Egglestone et al., 2019a,b). Similar results were also obtained using qualitative focus groups on treatment decisions for different focal health issues (Entwistle et al., 2011). These results parallel research on online-support groups for patients that also emphasizes the role of other users' experiences to feel connected and supported (Ziebland and Wyke, 2012). However, at the same time, patients that are still experiencing mental problems may be disconnected from patients that already recovered (Rennick-Egglestone et al., 2019b).
Summing up, research on well-being related effects of adding narratives to health information material is relatively scarce and results are mixed. This may be traced back to the great variation of health domains and research designs. In particular, narratives are presented in very different settings and formats, but hardly any study exists that uses narratives as additional content to evidence-based patient information and investigates how these are related to the well-being of patients. We therefore ask the following research question:
RQ2: What functions related to well-being do pulmonary embolism patients expect from narratives in evidence-based patient information?
Methods
Design and participants
In this research, we collected data in a two-stage process conducting 26 semi-structured interviews with 20 different people (6 people participated in both rounds of interviews1). Participants were recruited via a PE-patient database (PE = pulmonary embolism) at a university hospital (n = 16) and social media (n = 4). We used reflexive thematic analysis (Braun and Clarke, 2006, 2022) to analyze all data. In stage one, we conducted 15 interviews from September to December 2020. We interviewed six female and nine male patients, 19–79 years of age. Participants had several different educational qualifications, ranging from “Hauptschulabschluss” (completion of junior high school) to baccalaureate (or similar). Patients suffered from PE between June 2012 and September 2020, three patients had two PEs, one patient had three PEs, 12 are still on anticoagulation drugs, and 11 have comorbidities, such as hypertension, coagulation disorder, psychological disease, diabetes mellitus or cancer. In stage two, we were able to interview 11 PE patients (of which six participants already participated in stage one) from June 2021 to August 2021. We interviewed six female and five male patients, 20–71 years of age where nine have a baccalaureate (or similar). Patients suffered from PE between July 2013 and September 2020, two patients had two PEs, eight are still on anticoagulation drugs, four have comorbidities, such as hypertension, coagulation disorder, psychological disease, or cancer. The first part of the interview dealt with general views of the patients on health literacy regarding PE, and the second part dealt with expectation toward information materials. For this paper, the second portion of the interview was used. Twenty-four interviews were conducted by teams of two–one researcher from the communication group and one from the epidemiology group (two interviews were only carried out by one interviewer). In all, four researchers were involved in conducting the interviews.
Procedure
The data were collected using an existing database of PE patients at a large hospital in Germany2. Patients in this sample had consented to be contacted for study purposes. For the first stage of interviews, we contacted the 100 most recently added patients in the database by mail. The PE patient database was only accessible through authorized personnel to ensure a confidential handling of all personal data. After agreeing to participate, a researcher contacted them to arrange the interview. We aimed for a sample of participants with diverse backgrounds and socio-demographic data. The theoretical sampling included variation in age groups, gender, formal education, presence of comorbidities, passage of time since their last PE as well as number of PEs suffered. Since PE patients are older on average, our sample was not as diverse as intended after the database recruiting process. Consequently, we recruited younger people through other channels. We posted a call for study participation on the Instagram page of the chair of epidemiology. We further contacted the administrators of a Facebook group and asked them to post our call for study participants. Additionally, a German influencer sharing her life with thrombosis posted our call on Instagram without any financial compensation.
If patients were not chosen for the first stage of interviews, we informed them that they were added to a waiting list for the next stage. Patients were offered the choice to carry out the interview in person (n = 9), via Zoom (n = 4), or via telephone (n = 2). If interviews were carried out in person, they were done at an office at the university hospital while complying to COVID-19 contact restrictions. After agreeing on a date and time, patients received information on the study and its goal as well as data privacy documents via mail. For stage two, we were able to contact patients of our waiting list who could not participate in stage one. Due to COVID-19 regulations we carried out n = 7 interviews via Zoom and n = 4 in person. All interviewees received 20 Euros compensation for participating in the interviews.
Interview material and data analysis
In our study, we asked PE-patients about their own experiences and the helpfulness of narratives to overcome psychological or physical barriers after leaving the hospital. In the first stage, patients were encouraged to express their own experiences and needs. They were asked whether patient narratives are interesting or considered helpful, and which of their own experiences they would share with future patients when dealing with post-illness life changes. We also asked patients about their ideas for a brochure and their informational needs that should be covered in a potential brochure. In the second stage, we provided patients with a prototype of a brochure (24 pages) that we developed in between the two rounds of interviews (example page see Supplementary Figure 1). The brochure summarized information on topics that patients have to deal with throughout their illness journey, for example diagnosis, emotional and psychological challenges, CTEPH and recidivism risk. Every chapter provided factual, evidence-based information as well as one (n = 4 chapters) or two (n = 4 chapters) patient narratives matching the topic of the chapter. All in all, n = 12 patient narratives were extracted from the first round of interviews, according to their fit to the respective chapter topic. All patient narratives used in the brochure are a mixture of experience and process narratives but not outcome narratives. While all experiences used are real-life experiences, we sometimes combined patient narratives from different patients into one (if they had similar experiences) to enrich the narratives. This is also declared in the brochure. Patients received the brochure before attending the interview and were asked to read the brochure carefully before the interview appointment. During the interview, we then asked again about the implemented patient narratives' helpfulness to deal with patients' challenges after suffering from PE. Interviews were transcribed by a professional transcription agency or student research assistants. Interview duration ranged between 20 and 75 min in stage one, and 40 and 100 min in stage two.
Data analysis was carried out by three researchers in collaboration following reflexive thematic analysis (Braun and Clarke, 2006, 2022) using MaxQDA software. Two researchers began with data familiarization. Since both authors attended the interviews themselves, inductive codes as well as notes were already assigned while re-familiarizing with the data. After discussing their impressions of the data and codes, the two researchers engaged in inductive and deductive coding of a set of interviews each. They discussed codes and problems throughout the process. Three authors then collaboratively generated initial themes by clustering codes after the first round of coding. The second round of coding was carried out a few months later by the same researchers who coded the first round. Again, they engaged in inductive coding, re-analyzing the existing codes, developing the existing themes, and adding new ones. Three authors then discussed the revised themes. Coding was done iteratively and repeatedly. Throughout the whole process, we revised the coding scheme, respectively. We worked with all interviews from stages one and two and analyzed them simultaneously. While in the first round we spoke hypothetically about a brochure for PE patients leaving the hospital which included patient narratives, participants in the second round worked with such a brochure, we developed in between the two rounds of interviews. During data analysis, we found that the themes were congruent between the first and the second round of interviews; they even complemented each other3.
Results
Types of patient narratives
Throughout the interviews, we found that it is important to patients that a variety of patient narratives is presented: “Simply everything, positive, negative, neutral, simply everything. Because it is always so different. While I was in a hell of a lot of pain, my dad didn't feel anything. … There are different variations on how it can happen and if you only read about one variation, but you don't have it yourself, then you can't imagine how it is. So actually the more the better. That is definitely very helpful.” (R1-P13). One patient described the diversity of patient narratives as a form of introduction round where the whole range of symptoms is presented showing the extent of an illness: “You are sitting in such a round, if I remember, at the round of introductions, you always have this comparison with your illness. So, with your disease, with one gentleman it was so similar, so he described how it developed, with the others it was completely different. But you can get a different picture, you can just skim this whole range of symptoms. Or you also store it [note: the information].” (R1-P2). This is extremely valuable to patients, because of the general lack of information they face after leaving the hospital.
Patients find it helpful to be provided with socio-demographic information of other patients, for example age, gender and how much time has passed since the PE, because it helps to compare themselves to them (see next section).
Regarding the content of patient narratives, patients are, on the one hand, interested in other patients' feelings after the PE: “How it happened and how you felt about it. Or above all, how you felt after the pulmonary embolism. I think that is perhaps always one of those things where many people who are discharged from the hospital are initially uncertain: What will happen next? And how will I feel, I don't know, 5, 6, 7, 8 months after the embolism?” (R1-P15).
On the other hand, they are also interested in the different milestones a patient reaches during recovery, especially when they struggle with certain things: “How the patient fared after all that stuff, after treatment or after rehab and so on. How he continued or how things improved.” (R1-P5). Or, “Yes, my God, how does it go on now for the time being? And can I go back to work normally at all? And also go to work at all with the anticoagulation and so on and immediately. No? Those were the first points where it was a bit difficult for me. Where I thought: Yes, and who will answer all this for me now?” (R1-P15).
Patients find narratives that give insight into other patients' emotions and treatment experiences as helpful to get a sense of manifold illness experiences: “I don't know anyone who has more severe limitations due to a pulmonary embolism. It would be very interesting to find out how it is with people who were saved just before they died and what limitations they have. Be it physical, mental, psychological or whatever, how they are treated with medication. So, I have to say, I would be interested if you could read about that somewhere.” (R1-P2).
While most patients would agree that it is important to represent several courses of illness in patient narratives and that successes as well as setbacks should be reported, it is important that the general message of patient narratives is positive and shows that setbacks or problems can be addressed: “The setbacks are very important. Because, as I said, not every day is like the other. And if I only read reports where it goes, oh great, after 3 weeks this worked, after five this and today everything is like before, that's not helpful. So, a healthy mixture would be good. … I mean, a brochure like this shouldn't just talk things up. It should really inform and also show what can still happen.” (R1-P10).
This interest in process and experience narratives is also reflected in the narratives patients like to share. When searching for narratives to include in the brochure for the prototype that should be used, no outcome narratives were shared by patients but instead a great amount was a combination of process and experience narratives. Referring to a variety of topics (including diagnosis, symptoms, treatment procedures, rehabilitation, physical and psychological limitations, daily living), most patients consequently tended to describe how they experienced and managed existing challenges, made progress and give insights into their feelings during that process: “For me, this sounds a bit strange, but for me it was actually a relatively pleasant disease. Because once you have it, once it has occurred, then the therapy is actually relatively clear…. it doesn't need any intervention, so you don't need a surgery or anything like that. That was my first concern, because that was my first hospital stay at that time. I thought, oh God, if I go to the hospital now, will they open my lungs or what are they going to do? So, there is, I have to say, no panic at first. If the diagnosis is there and if you have survived the first moment, then it is actually a disease that is relatively easy to live with, compared to many others. And yes, otherwise the only tip is really not to go crazy, so don't think about it any further.” (R1-P3) Or: “And I think that's also very important, that even if you don't feel like doing something, you say to yourself: ‘I just want to put my feet up and do nothing'…. Be lazy. So, after this was actually a near-death experience / I take a lot of things no longer so important. I think to myself: ‘In the past I would have been upset about it. No. I don't get upset about it at all now.' …Be a little more calm. Appreciate life a bit more.” (R1-P7).
This mixture of experience and process narratives often refers to the time after hospital release: “I was discharged immediately after the diagnosis, heparin injection in, catheter out, intravenous line out and then sent home. And the next day then to the general practitioner, so from there it was already very strange to be sent home again with this diagnosis and it occupied my head quite a bit. Not that evening, but afterwards, because you become so aware that you have just jumped from the brink of death, because pulmonary embolism is also a fairly common cause of death. So for me it was in any case psychologically difficult. I struggled with it quite a long time or even still struggle with it now.” (R1-P1).
In addition, a few narratives had a clear focus on the process only. In particular, some male patients had a stronger focus on different steps in the treatment process and their recovery without giving much insights into their feelings: “I would just say that you go to a lung specialist once a year or once every 2 years. So you go to a specialist and just have it checked again. And what would be important is that you pay attention to any symptoms. The simplest example is, you can't get up a flight of stairs anymore. That stays in everybody's mind when you walk up one floor and stand at the top and pump for 2 min. So these have to be warning signals that everyone should have in mind. That's what I would pass on.” (R1-P2) Some patients just list steps to follow: “Stay positive, stay active, get out, get in nature, get general information, like I said, check blood levels, watch your diet more, maybe reduce weight a little bit and that's it.” (R1-P6).
Only when directly asked about psychological consequences, some of the patient stories have a clear focus on emotional insights, for example “Before I suffered from PE, I was 20 years old, I was athletic, I was fit, and now I felt like an 80-year-old woman and that's because you can't get up and you have to take breaks every few steps… you just don't feel like yourself anymore.” (R2-P4).
Functions of patient narratives
Based on thematic analysis, we identified four functions related to well-being that patients ascribe to narratives in evidence-based patient information: (1) motivating self-reflection and reflection on the recovery process, (2) reducing the feeling of loneliness, (3) reducing emotional distress, and (4) inspiring mindful mastery (see Table 1, see Supplementary Table 1 for codes and themes).
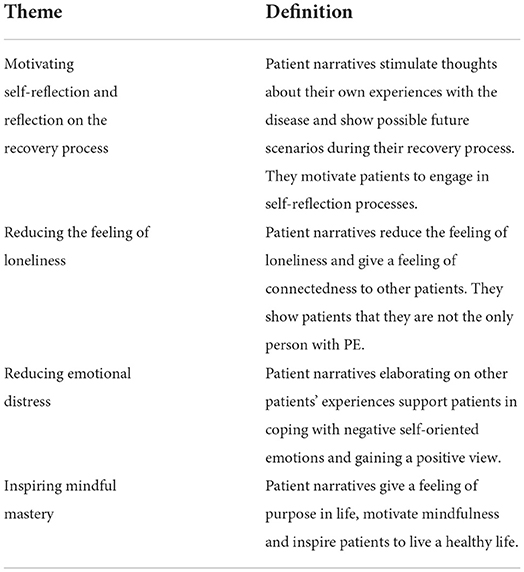
Table 1. Themes and definitions.
Motivating self-reflection and reflection on the recovery process
A truly recurrent theme within the interviews is that patient narratives provide references so that patients can compare others' situations to their own: “I can imagine that when I read such a report [note: patient narrative] from someone else, I could imagine, oh yes, that sounds almost like me. I can imagine that it is helpful for a patient. If it says, oh, I dealt with it this way, and the other person describes how he or she dealt with it that way, then I, as the person affected, can somehow say, yes, that's how it was for me too. … Yes, I can imagine that some people can get help from that, yes.” (R1-P8). As consequence of these comparisons, a reflection on personal well-being becomes possible: “And then you can also assess your own, your own well-being. Because that is exactly the problem. You can't always assess it. And then I see ‘ah yes, that's quite normal,' ‘ah yes, that's actually quite normal for this phase”' (R2-P8).
Comparisons with other patients through patient narratives are perceived as helpful to reflect their own recovery progress: “So I had a very severe embolism, I could no longer do anything, neither walk and talk, have had to learn everything again, but then you see already, it's okay. Some [people] need longer, with others it goes faster. They [the narratives] already describe how it is at the beginning, how you feel.” (R2-P3). In this vein, patient narratives give a feeling of development and self-assurance of what is possible: “They are highly interesting. So, I found personal examples highly interesting that show how to deal with it, what you can achieve and how far you can get as well.” (R2-P6). In this vein, patients emphasize the motivational potential: “And as I said, hearing how others cope sometimes gives a bit of a push.” (R1-P10) or “Hey look, they did this; look, they are doing this; look, there is a field report, they did this. Well, some of them have died, which is not so nice, of course. But you can also see that the brochure motivates. Because you have these reports from people who have managed to get back on their feet to some extent.” (R2-P3).
These insights into other patients achievements and their development are in particular perceived as helpful for the time following hospitalization: “who is just now being discharged from the hospital with a pulmonary embolism” I think it's more important for him to rather see 2, 3 years [from now], …, because if he has achieved that, then the other things are also, is nice to have, …, but for him it's more important to know, it takes time, but I can, …, in a year's time, if everything goes well, also climb the stairs normally again to the fourth floor or so.” (R1-P1). But long-term experiences too are perceived as useful in this regard: “What I also found interesting was to see how long ago these people had the pulmonary embolism. And to see once again how long-term consequences can actually play out, so, yes, I think it's a very good thing in itself.” (R2-P10).
However, for references to be helpful they must include socio-demographic as well as meta-data (for example severity of PE, time of PE). This helps patients to categorize the impressions and predict how long it might take to be able to get back to their everyday life, for example hobbies: “It has to be backed up a little bit with data, especially if it's such a severe course and it's, let's say, after half a year he was able to climb stairs again wonderfully, for example. After 2 years he is doing five-kilometer runs, for example.” (R1-P1).
Reducing the feeling of loneliness
A second recurrent function of patient narratives is their potential to reduce the feeling of loneliness: “What I found totally great … is that you included the experiences of pulmonary embolism patients. That still gives you the feeling that you are not the only one who has been around with this disease at some point, so I found that very appealing. I enjoyed reading these. I then took the brochure again at some point and went through all the green boxes again [authors' note: patient narratives were presented in green boxes in the brochure].” (R2-P2). In order to reduce the feeling of loneliness, it does not matter, whether the other patients have the same type of PE: “I think that it conveys that there are other people who have had the same symptoms, but with different manifestations or a different degree of severity.” (R2-P5). This is supported by another patients' statement: “Yes, I would definitely like that, especially because it means that you don't feel alone. You see, it hits different people, especially when people of different genders, different ages are presented. Then you see: ‘I'm just one of many and there are many others who struggle with this.”' (R1-P12).
The potential of patient narratives to provide references to other patients and thus reduce the feeling of loneliness is experienced as support by patients: “Exactly, so I also think it's important because when you read a brochure like this, you immediately think to yourself ‘okay, there's also someone else who had to go through something like this and … I'm not the only person in the world who now has to take medication for life'. It's nice when you get a bit of support like this” (R2-P9). In this vein, patients indicate that the patient stories provide a psychological benefit: “For me, the personal burden was simply because I couldn't categorize this illness at all. And because there was nothing, I think a brochure like that, you really shouldn't underestimate it, is something that gives you a certain support. And if I get that kind of support, then it doesn't become as much of a burden psychologically as if I feel left alone.” (R1-P14). One patient even went so far as to say that he considered patient narratives in patient information material as a substitute for a support group: “I don't go to a support group. I don't need to. I've been alone all my life, in charge of a huge engine room, with no one to ask, …. That's what I have your brochure for.” (R2-P11).
Reducing emotional distress
The third theme is the potential of narratives to reduce emotional distress. Patients expect that the brochure with patient narratives reduces fear and anxiety by providing a first-hand account of living a life with PE: “Because you often have no idea what's going on. And if you can read a little bit about it, it often takes the fear out of it. Because often people are afraid: ‘What now? What happens next?' If you can already read something, then it simplifies the whole thing a bit.” (R1-P13).
This aspect of reducing fear was also emphasized when patients were asked what experiences they would like to share with other patients: “that they should not worry so much in this respect.” (R1-P15) or “But do not ascribe too much [authors' note: attention or meaning] to the experience of a pulmonary embolism, otherwise you will of course also go crazy in everyday life. Because, then you pay attention yes at every step, if you cough or take a deep breath once and that does not work out so properly, then you can panic.” (R1-P9).
Patient narratives giving insight into other patients' emotions are also described as source of positive feelings in readers: “If someone else says, I feel the same way, then that gives me a good feeling and then I don't need to spend my energy on something like that, because it's quite normal that I have this emotion.” (R1-P14).
In addition, patient narratives are also described as source for self-confidence that enables patients to regain trust in the self and the body: “That gives you security again, because I just lack a bit of security. You've lost trust in your body at the moment and now you have to get security again and create trust again. And that's where I think this brochure absolutely contributes.” (R2-P8).
Inspiring mindful mastery
We identified the fourth theme, inspiring mindful mastery, when patients were asked about their most relevant patient experience they would like to share. Several patients emphasized the need to communicate in patient stories that life goes on and the disease should not take over: “And that giving up is simply not a solution, yes, definitely. That's the worst thing you can do, to give up, yes, that would actually be the most important thing I would say to him (laughs).” (R1-P13) or “Yes. Go on living your life as it was before. Get through the disease … and then continue to live your life simply. Don't let it get the upper hand. It must never get the upper hand, it must simply run with you. And you can't lose yourself, you have to look in any case that you continue.” (R1-P7) or “Maybe that you should already notice the signals of your body, but that you should nevertheless quickly try to resume your old active life.” (R1-P15).
In this vein, it is also perceived as important to communicate a positive mindset about life in patient stories: “So when I'm in a good mood, I try to pull the positive out of the whole thing in terms of the psyche. Then I say to myself: ‘Okay, I'm going to live with this or I'm going to have to live with this and I'm going to make the best of it.”' (R1-P2).
Others emphasize the relevance of mindfulness and relaxation: “Be a little more relaxed. Appreciate life a little more.” (R1-P7) or “Above all, that this was good, that you have discovered this [the PE] now and that you could help and that this is now again a beginning to look back at yourself and practically, life goes on, but with a little more attentiveness to yourself.” (R1-P11).
Discussion
This study is the first to investigate patients' perceptions of narratives in evidence-based patient information material for tertiary prevention of pulmonary embolism patients.
Promoting the well-being of pulmonary embolism patients is important after hospital release. Therefore, providing evidence-based patient information that include patient stories may be a first step in order to support post-hospital care. However, given the risk to bias patients' decisions as well as limited evidence for beneficial effects, their inclusion is contested (Shaffer et al., 2021). Two shortcomings of this critical view are identified: (1) the focus on persuasive effects of outcome narratives in decision situations as well as (2) the dominance of classical persuasive outcomes, such as intentions, attitudes and knowledge. Adding on this ongoing discussion, this paper argues that process and experience narratives (Shaffer and Zikmund-Fisher, 2013; Shaffer et al., 2013a) may be in particular influential to support patients' well-being. In order to explore this assumption, our aim was to identify what types of narratives patients find helpful in patient information and what well-being-related functions these narratives fullfill from patients' point of view. We therefore interviewed 20 patients who informed us about their own struggles with pulmonary embolism and the role of narratives in patient information.
Overall, patients were grateful for the narratives provided within the prototype of patient information material. A broad integration of very different narratives that reflect the heterogenous sociodemographical background of patients but also their various disease processes was perceived as important. In this vein, patients were not so much looking for one exemplar that best represented their own experiences, but appreciated the full bandwith of possible illness phases and progresses. Given that former research on the role of similarity and character-related engagement processes (for example self-referencing, identification) in patient information (de Graaf, 2014; Ooms et al., 2019) typically focuses on only one character or exemplar, research is needed that investigates such processes when multiple characters are present.
Regarding the type of narratives, we find evidence that patients appreciate insights into the recovery process, which steps other patients had to take and whether they succeded or not, as well as their feelings and emotions. This corresponds well with the understanding of process and experience narratives (Shaffer and Zikmund-Fisher, 2013). These narrative types also mirror the stories patients would like to pass on to other patients. However, both types of narratives are usually mixed in our patients' stories. This raises the question if sole descriptions of a treatment process without a description of experiences during that process or descriptions of experiential insights without any process elements are typical for real patient stories.
For some specific types of content, it seems plausible that patients have a more profound focus on one of the two types (for example when decribing their treatment procedure, a focus on process was recognizable). However, for most topcis patients addressed themselves, these facets were intertwined. Thus, research is needed investigating the relationship of those narrative types in more detail and disentangling their combined effects from their distinct effects.
While we are not able to answer the question of negative or positive effects of such narratives on patients' well-being directly, we are able to illustrate different functions that patients expect from narratives in patient information. By using thematic analysis, we identified four main functions of patient narratives patients emphasized: (1) motivating self-reflection and reflection on the recovery process, (2) reducing the feeling of loneliness, (3) reducing emotional distress, and (4) inspiring mindful mastery.
Comparing the four functions to aspects of hedonic and eudaimonic well-being, we detect parallels. Motivating self-reflection and reflection on the recovery process was the most overarching topic patients associate with narratives. In particular, insights into the progress of other patients were perceived as important for patients, as these were evaluated as motivational cues and supported a positive evaluation of future developments. The focus on the developmental perspective has parallels with personal growth as sub-dimension of eudaimonic well-being and its emphasis on openness, new experiences and continuous growing in contrast to stagnation (Ryff and Keyes, 1995). Given that medical research so far has predominantly focused on negative aspects of hedonic well-being of pulmonary embolism patients (Klok et al., 2010b; van Es et al., 2013; Tran et al., 2021), it is remarkable that the most relevant aspect detected in the interviews relates to dimensions of eudaimonic well-being.
Reduction of loneliness, the second function identified, covers patients' perceptions that narratives from other patients help to feel less alone with the illness but as part of a community. In some cases, this need was so strong that patients stated that they read the stories several times for this reason. The relevance of narratives for connectedness and feeling less lonely is in line with prior research on mental health (Rennick-Egglestone et al., 2019a,b) as well as treatment decisions (Entwistle et al., 2011). However, less is known about how connectedness is established. Further research therefore should investigate whether the connectedness patients experience is based on processes of parasocial interaction (Horton and Wohl, 1956) that are hardly investigated for health contexts. In addition, it is a worthwhile goal to seek for connections between parasocial interaction and eudaimonic well-being. While the patients in our study could not feel a real sense of connectedness, because there is hardly any PE-community they could feel connected to, our results stress the potential of narratives as a substitute for in-person interaction. Even if such parasocial interaction processes are different to intense social interactions, they may help patients with their loneliness.
The theme reducing emotional distress has a clear reference to hedonic well-being. It includes the potential of narratives to reduce negative affective states, such as anxiety and illness-related fears, but also to induce more positive feelings about the illness and the recovery process, in particular hope. This finding is in line with existing research in other health domains showing that narratives may decrease negative illness-related emotions and increase hope (Entwistle et al., 2011; Rennick-Egglestone et al., 2019a,b). Related to these positive feelings, patients also referred to the potential of narratives to regain trust and increase self-confidence in their own body. This may add on patients self-acceptance as aspect of eudaimonic well-being (Ryff and Keyes, 1995; Ryff, 2018).
Giving the high levels of depression and anxiety in pulmonary embolism patients (Liu et al., 2011; Chuang et al., 2019; Erickson et al., 2019), this reduction of emotional distress function seems promising to help patients suffering from a reduced mental health related quality of life (Klok et al., 2010b; van Es et al., 2013; Kahn et al., 2017; Erickson et al., 2019). Further research should also elaborate on the potential of patient stories for patients still suffering from post-traumatic stress-disorder due to pulmonary embolism. Interestingly, assumed relationships with hedonic and eudaimonic aspects of well-being are strongly intertwined in patients' descriptions, which questions a strict dichotomy of hedonic and eudaimonic well-being (Disabato et al., 2016). This relationship of both aspects is also in line with empirical results showing that eudaimonic and hedonic well-being are highly correlated and do not have a high discriminant validity but rather relate to well-being as a single overarching construct (Disabato et al., 2016).
Inspiring mindful mastery, the fourth function, includes the assumption that narratives can transport a positive message and support the appreciation of life even in the face of illness-related barriers. This may be related to purpose in life as part of eudaimonic well-being (Ryff and Keyes, 1995; Ryff, 2018). Given that research about well-being related aspects of pulmonary embolism patients already shows that patients tend to positively re-evaluate life as the recovery process is progressing (Hunter et al., 2017, 2019; Rolving et al., 2019), it is interesting for further research whether patient narratives have the potential to speed up this process. Particularly patients having difficulties to keep up with their daily lives and to accept their situation (Noble et al., 2014) are assumed to benefit from this function of patient narratives.
Even if we focused our research on pulmonary embolism, it seems plausible to assume that similar results are observable for other life-threatening diseases, where first-hand experiences are scarce. In particular directly after hospital release patient narratives may benefit from first-hand insights into a patient community to which patients may connect to and the potential to provide emotional release. Furthermore, we assume that they play a key-role in starting the self-management process of various diseases by motivating reflection and by providing inspiration about how barriers could be mastered.
In sum, all four identified topics show references to well-being related dimensions and thus may be helpful as elements in patient information. However, patient interviews cannot provide evidence for causal effects of patient narratives on well-being related dimensions, and this is the most relevant limitation of our research. In order to explore effects of narratives, future research should use experimental designs and test the effects of narratives for the four functions we identified. A second limitation refers to the cross-sectional character of both interview waves.
Overall, patients appreciate process and experience narratives. Using such narratives in evidence based-patient information that do not refer to treatment decisions but tertiary prevention and illness self-management, seems to provide an additional benefit for patients that is not covered by traditional persuasive outcomes.
Data availability statement
The datasets used in the analysis for this article are only available with restrictions. Participants of the studies did not agree to publicly share all their data. Requests to access the datasets should be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the Augsburg University Hospital. The patients/participants provided their written informed consent to participate in this study.
Author contributions
AK: conceptualization, writing-original draft preparation, funding acquisition, and investigation. CK: methodology and results, investigation, and writing-original draft preparation. AA: writing-original draft preparation, investigation, and methodology. HB: conceptualization, writing-original draft preparation, funding acquisition, and supervision. SF: methodology and investigation. IK: conceptualization, funding acquisition, and project administration. All authors contributed to the article and approved the submitted version.
Funding
This research was funded by Gemeinsamer Bundesausschuss (Grant No. 01VSF19023).
Acknowledgments
We thank all of our reviewers for their valuable remarks and feedback throughout the review process.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcomm.2022.990819/full#supplementary-material
Footnotes
1. ^The study was part of a larger research project in which communication scientists and epidemiologists collaborated. Within this project we accompanied the process of creating and evaluating a patient information brochure. This process involved several stages of interviews. We collaborated with a large university hospital in Germany that maintains a database of PE-patients. Registered patients agreed to be invited to participate in different studies and self-select in case they want to participate. If participants met our inclusion criteria, we decided to allow multi-participation. In stage one of the interviews patients expressed their informational needs and wishes for the brochure. In stage two patients were exposed to a prototype of the brochure and their evaluation was captured.
2. ^Interviews were conducted in German. All citations from the interviews were translated with deepl.com and revised by the authors. For better readability, we mended linguistic irregularities.
3. ^In the results section, we mark all quotes with R# - P#, which is a shortcut we use to anonymize our interviewees. At the same time these abbreviations help us to identify the person who stated the quote. R# marks the round of interviews, P# is the number we assigned to the respective participant.
References
Andrews, F. M., and Withey, S. B. (1976). Social Indicators of Well-Being: Americans' Perceptions of Life Quality. Plenum Press.
Angott, A. M., Comerford, D. A., and Ubel, P. A. (2013). Imagining life with an ostomy: does a video intervention improve quality-of-life predictions for a medical condition that may elicit disgust? Patient Educ. Councel. 91, 113–119. doi: 10.1016/j.pec.2012.10.015
Ballard, A. M., Davis, A., and Hoffner, C. A. (2021). The impact of health narratives on persuasion in African American women: a systematic review and meta-analysis. Health Commun. 36, 560–571. doi: 10.1080/10410236.2020.1731936
Barco, S., Valerio, L., Gallo, A., Turatti, G., Mahmoudpour, S. H., Ageno, W., et al. (2021). Global reporting of pulmonary embolism-related deaths in the World Health Organization mortality database: vital registration data from 123 countries. Res. Prac. Thromb. Haemostasis 5, e12520. doi: 10.1002/rth2.12520
Bekker, H. L., Winterbottom, A. E., Butow, P., Dillard, A. J., Feldman-Stewart, D., Fowler, F. J., et al. (2013). Do personal stories make patient decision aids more effective? A critical review of theory and evidence. BMC Med. Informatics Decision Making 13, 1–9. doi: 10.1186/1472-6947-13-S2-S9
Bennett, K. F., von Wagner, C., and Robb, K. A. (2015). Supplementing factual information with patient narratives in the cancer screening context: a qualitative study of acceptability and preferences. Euro. J. Cancer Care 24, 14–14. doi: 10.1111/hex.12357
Bennett, P., Patterson, K., and Noble, S. (2016). Predicting post-traumatic stress and health anxiety following a venous thrombotic embolism. J. Health Psychol. 21, 863–871. doi: 10.1177/1359105314540965
Betsch, C., Haase, N., Renkewitz, F., and Schmid, P. (2015). The narrative bias revisited: what drives the biasing influence of narrative information on risk perceptions? Judge. Decision Making 10, 241–264.
Betsch, C., Renkewitz, F., and Haase, N. (2013). Effect of narrative reports about vaccine adverse events and bias-awareness disclaimers on vaccine decisions: a simulation of an online patient social network. Med. Decis. Making 33, 14–25. doi: 10.1177/0272989X12452342
Betsch, C., Ulshöfer, C., Renkewitz, F., and Betsch, T. (2011). The influence of narrative v. statistical information on perceiving vaccination risks. Med. Decis. Making 31, 742–753. doi: 10.1177/0272989X11400419
Bilandzic, H., and Busselle, R. W. (2013). “Narrative persuasion,” in The Sage Handbook of Persuasion. Developments in Theory and Practice, eds J. P. Dillard and L. Shen (London: Sage), 200–219. doi: 10.4135/9781452218410.n13
Braun, V., and Clarke, V. (2006). Using thematic analysis in psychology. Qual. Res. Psychol. 3, 77–101. doi: 10.1191/1478088706qp063oa
Bunge, M., Mühlhauser, I., and Steckelberg, A. (2010). What constitutes evidence-based patient information? Overview of discussed criteria. Patient Educ. Counsel. 78, 316–328. doi: 10.1016/j.pec.2009.10.029
Carlick, A., and Biley, F. C. (2004). Thoughts on the therapeutic use of narrative in the promotion of coping in cancer care. Euro. J. Cancer Care 13, 308–317. doi: 10.1111/j.1365-2354.2004.00466.x
Chuang, L.-H., Gumbs, P., van Hout, B., Agnelli, G., Kroep, S., Monreal, M., et al. (2019). Health-related quality of life and mortality in patients with pulmonary embolism: a prospective cohort study in seven European countries. Qual. Life Res. 28, 2111–2124. doi: 10.1007/s11136-019-02175-z
Coulter, A. (1998). Evidence based patient information. BMJ 317, 225–226. doi: 10.1136/bmj.317.7153.225
de Graaf, A. (2014). The effectiveness of adaptation of the protagonist in narrative impact: similarity influences health beliefs through self-referencing. Human Commun. Res. 40, 73–90. doi: 10.1111/hcre.12015
de Graaf, A., Sanders, J., and Hoeken, H. (2016). Characteristics of narrative interventions and health effects: a review of the content, form, and context of narratives in health-related narrative persuasion research. Rev. Commun. Res. 4, 88–131. doi: 10.12840/issn.2255-4165.2016.04.01.011
Diener, E., and Lucas, R. E. (1999). “Personality and subjective well-being,” in Well-Being: Foundations of Hedonic Psychology, eds D. Kahneman, E. Diener, and N. Schwarz (New York, NY: Sage), 213–229.
Diener, E., Oishi, S., and Lucas, R. E. (2011). “Subjective well-being: the sciene of happiness and life satisfaction,” in The Oxford Handbook of Positive Psychology, eds S. J. Lopez and C. R. Snyder (Oxford: Oxford University Press), 187–192.
Disabato, D. J., Goodman, F. R., Kashdan, T. B., Short, J. L., and Jarden, A. (2016). Different types of well-being? A cross-cultural examination of hedonic and eudaimonic well-being. Psychol. Assessment 28, 471–482. doi: 10.1037/pas0000209
Drewniak, D., Glässel, A., Hodel, M., and Biller-Andorno, N. (2020). Risks and benefits of web-based patient narratives: systematic review. J. Med. Internet Res. 22, e15772. doi: 10.2196/15772
Dunlop, S. M., Wakefield, M., and Kashima, Y. (2010). Pathways to Persuasion: cognitive and experiential responses to health-promoting mass media messages. Commun. Res. 37, 133–164. doi: 10.1177/0093650209351912
Elwyn, G., O'Connor, A., Stacey, D., Volk, R., Edwards, A., Coulter, A., et al. (2006). Developing a quality criteria framework for patient decision aids: online international Delphi consensus process. BMJ 333, 417. doi: 10.1136/bmj.38926.629329.AE
Entwistle, V. A., France, E. F., Wyke, S., Jepson, R., Hunt, K., Ziebland, S., et al. (2011). How information about other people's personal experiences can help with healthcare decision-making: a qualitative study. Patient Educ. Counsel. 85, e291–e298. doi: 10.1016/j.pec.2011.05.014
Erickson, R. M., Feehan, M., Munger, M. A., Tak, C., and Witt, D. M. (2019). Understanding factors associated with quality of life in patients with venous thromboembolism. Thromb. Haemostasis 119, 1869–1876. doi: 10.1055/s-0039-1696717
Feehan, M., Munger, M. A., Johnson, S. A., Walsh, M., Fleming, R., and Witt, D. M. (2017). Emotional impact of venous thromboembolism: a qualitative study of patients' journeys. Inside Patient Care 5.
Fitzgerald, K., Paravati, E., Green, M. C., Moore, M. M., and Quian, J. L. (2019). Restorative narratives for health promotion. Health Commun. 35, 356–363. doi: 10.1080/10410236.2018.1563032
Gavaruzzi, T., Sarlo, M., Giandomenico, F., Rumiati, R., Polato, F., De Lazzari, F., et al. (2018). Assessing emotions conveyed and elicited by patient narratives and their impact on intention to participate in colorectal cancer screening: a psychophysiological investigation. PLoS ONE 13, e0199882. doi: 10.1371/journal.pone.0199882
Goldsmith, M. R., Bankhead, C. R., and Austoker, J. (2007). Synthesising quantitative and qualitative research in evidence-based patient information. J. Epidemiol. Commun. Health 61, 262–270. doi: 10.1136/jech.2006.046110
Green, M. C. (2006). Narratives and cancer communication. J. Commun. 56, S163–S183. doi: 10.1111/j.1460-2466.2006.00288.x
Green, M. C., Brock, T. C., and Kaufman, G. E. (2004). Understanding media enjoyment: the role of transportation into narrative worlds. Commun. Theory 14, 311–327. doi: 10.1111/j.1468-2885.2004.tb00317.x
Haase, N., Betsch, C., and Renkewitz, F. (2015). Source credibility and the biasing effect of narrative information on the perception of vaccination risks. J. Health Commun. 20, 920–929. doi: 10.1080/10810730.2015.1018605
Haase, N., Schmid, P., and Betsch, C. (2020). Impact of disease risk on the narrative bias in vaccination risk perceptions. Psychol. Health 35, 346–365. doi: 10.1080/08870446.2019.1630561
Horton, D., and Wohl, R. R. (1956). Mass communication and para-social interaction: observation on intimacy at a distance. Psychiatry 19, 185–206. doi: 10.1080/00332747.1956.11023049
Hunter, R., Lewis, S., Noble, S., Rance, J., and Bennett, P. D. (2017). “Post-thrombotic panic syndrome”: a thematic analysis of the experience of venous thromboembolism. Br. J. Health Psychol. 22, 8–25. doi: 10.1111/bjhp.12213
Hunter, R., Noble, S., Lewis, S., and Bennett, P. (2019). Long-term psychosocial impact of venous thromboembolism: a qualitative study in the community. BMJ Open 9, e024805. doi: 10.1136/bmjopen-2018-024805
Huppert, F. A., and So, T. T. C. (2013). Flourishing across europe: application of a new conceptual framework for defining well-being. Soc. Indicat. Res. 110, 837–861. doi: 10.1007/s11205-011-9966-7
Kahn, S. R., Akaberi, A., Granton, J. T., Anderson, D. R., Wells, P. S., Rodger, M. A., et al. (2017). Quality of life, dyspnea, and functional exercise capacity following a first episode of pulmonary embolism: results of the ELOPE cohort study. Am. J. Med. 130, 990.e9–990.e21. doi: 10.1016/j.amjmed.2017.03.033
Kaminer, D. (2006). Healing processes in trauma narratives: a review. Soutch Afr. J. Psychol. 36, 481–499. doi: 10.1177/008124630603600304
Keer, M., van den Putte, B., de Wit, J., and Neijens, P. (2013). The effects of integrating instrumental and affective arguments in rhetorical and testimonial health messages. J. Health Commun. 18, 1148–1161. doi: 10.1080/10810730.2013.768730
Kirchberger, I., Ruile, S., Linseisen, J., Haberl, S., Meistinger, C., and Berghaus, T. (2020). The lived experience with pulmonary embolism: a qualitative study using focus groups. Respir. Med. 167, 105978. doi: 10.1016/j.rmed.2020.105978
Klok, F. A., and Barco, S. (2018). Follow-up after acute pulmonary embolism. Predicting chronic thromboembolic pulmonary hyperten- sion and post-pulmonary embolism syndrome. H?mostaseologie 38, 22–32. doi: 10.5482/HAMO-17-06-0020
Klok, F. A., van der Hulle, T., den Exter, P. L., Lankeit, M., Huisman, M. V., and Konstantinides, S. (2014). The post PE-syndrome: a new concept for chronic complications of pulmonary embolism. Blood Rev. 28, 221–226. doi: 10.1016/j.blre.2014.07.003
Klok, F. A., van Kralingen, K. W., van Dijk, A. P. J., Heyning, F. H., Vliegen, H. W., and Huisman, M. V. (2010a). Prevalence and potential determinants of exertional dyspnea after actue pulmonary embolism. Respir. Med. 104, 1744–1749. doi: 10.1016/j.rmed.2010.06.006
Klok, F. A., van Kralingen, K. W., van Dijk, A. P. J., Heyning, F. H., Vliegen, H. W., Kaptein, A. A., et al. (2010b). Quality of life in long-term survivors of acute pulmonary embolism. CHEST 138, 1432–1440. doi: 10.1378/chest.09-2482
Konstantinides, S. V., Meyer, G., Becattini, C., Bueno, H., Geersing, G.-J., Harjola, V.-P., et al. (2020). 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Euro. Heart J. 41, 543–603. doi: 10.1093/eurheartj/ehz405
Kreuter, M. W., Holmes, K., Alcaraz, K., Kalesan, B., Rath, S., Richert, M., et al. (2010). Comparing narrative and informational videos to increase mammography in low-income African American women. Patient Educ. Counsel. 81, S6–S14. doi: 10.1016/j.pec.2010.09.008
Liu, C., Li, X., Chen, H., Cui, J., Niu, L., He, Y., et al. (2011). Depression, anxietey and influencing factors in patients with acute pulmonary embolism. Chin. Med. J. 124, 2438–2442. doi: 10.3760/cma.j.issn.0366-6999.2011.16.007
Lühnen, J., Albrecht, M., Mühlhauser, I., and Steckelberg, A. (2017). Leitlinien evidenzbasierte Gesundheitsinformationen. Available online at: http://www.leitlinie-gesundheitsinformation.de/
McQueen, A., Kreuter, M. W., Kalesan, B., and Alcaraz, K. I. (2011). understanding narrative effects: the impact of breast cancer survivor stories on message processing, attitudes, and beliefs Among African American women. Health Psychol. 30, 674–682. doi: 10.1037/a0025395
Newman, M. A., Ziebland, S., and Barker, K. L. (2009). Patients' views of a multimedia resource featuring experiences of rheumatoid arthritis: pilot evaluation of www.healthtalkonline.org. Health Informatics J. 15, 147–159. doi: 10.1177/1460458209102974
Noble, S., Lewis, R., Whithers, J., lewis, S., and Bennett, P. (2014). Long-term psychological consequences of symptomatic pulmonary embolism: a qualitative study. Br. Med. J. Open 4, e004561. doi: 10.1136/bmjopen-2013-004561
O'Connor, A., Elwyn, G., Barratt, A., Barry, M., Coulter, A., Holmes-Rovner, M., et al (2005). IPDAS 2005: Criteria for Judging the Quality of Patient Decision Aids. Available online at: http://ipdas.ohri.ca/IPDAS_checklist.pdf
Ooms, J., Hoeks, J., and Jansen, C. (2019). “Hey, that could be me”: the role of similarity in narrative persuasion. PLoS ONE 14, e0215359. doi: 10.1371/journal.pone.0215359
Osaka, W., and Nakayama, K. (2017). Effect of a decision aid with patient narratives in reducing decisional conflict in choice for surgery among early-stage breast cancer patients: a three-arm randomized controlled trial. Patient Educ. Counsel. 100, 550–562. doi: 10.1016/j.pec.2016.09.011
Pavot, W., and Diener, E. (2008). Satisfaction with life scale and the emerging construct of life satisfaction. J. Positive Psychol. 3, 137–152. doi: 10.1080/17439760701756946
Perrier, M. J., and Martin Ginis, K. A. (2017). Narrative interventions for health screening behaviours: a systematic review. J. Health Psychol. 22, 375–393. doi: 10.1177/1359105315603463
Perrier, M. J., and Martin Ginis, K. A. (2018). Changing health-promoting behaviours through narrative interventions: a systematic review. J. Health Psychol. 23, 1499–1517. doi: 10.1177/1359105316656243
Reer, F., Tang, W. Y., and Quandt, T. (2019). Psychosocial well-being and social media engagement: the mediating roles of social comparison orientation and fear of missing out. New Media Soc. 21, 1486–1505. doi: 10.1177/1461444818823719
Reinecke, L., and Oliver, M. B. (2016). “Media use and well-being: status quo and open questions,” in The Routledge Handbook of Media Use and Well-Being: International Perspectives on Theory and Research on Positive Media Effects, eds L. Reinecke and M. B. Oliver (New York, NY: Routledge), 3–13.
Rennick-Egglestone, S., Morgan, K., Llewellyn-Beardsley, J., Ramsay, A., McGranahn, R., Gillard, S., et al. (2019a). Mental health recovery narratives and their impact on recipients: systematic review and narrative synthesis. Can. J. Psychiatry 64, 669–697. doi: 10.1177/0706743719846108
Rennick-Egglestone, S., Ramsay, A., McGranahn, R., Llewellyn-Beardsley, J., Hui, A., Pollock, K., et al. (2019b). The impact of mental health recovery narratives on recipients experiencing mental health problems: qualitative analysis and change model. PLoS ONE 14, e0226201. doi: 10.1371/journal.pone.0226201
Rolving, N., Brocki, B., Bloch-Nielsen, J. R., Mikkelsen, H. R., Ravn, P., and Frost, L. (2020). Effect of a physiotherapist-guided home-based exercise intervention on physical capacity and patient-reported outcomes among patients with acute pulmonary embolism. A randomized clinical trial. Phys. Med. Rehabil. 3, e200064. doi: 10.1001/jamanetworkopen.2020.0064
Rolving, N., Brocki, B. C., and Andreasen, J. (2019). Coping with everyday life and physical activity in the aftermath of an acute pulmonary embolism: a qualitative study exploring patients' perceptions and coping strategies. Thromb. Res. 182, 185–191. doi: 10.1016/j.thromres.2019.06.007
Ryan, R. M., and Deci, E. L. (2001). On happiness and human potentials: a review of research on hedonic and eudaimonic well-being. Annu. Rev. Psychol. 52, 141–166. doi: 10.1146/annurev.psych.52.1.141
Ryff, C. D. (1989a). Beyond Ponce de Leon and life satisfaction: new directions in quest of successful aging. Int. J. Behav. Dev. 12, 35–55. doi: 10.1177/016502548901200102
Ryff, C. D. (1989b). Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J. Personal. Soc. Psychol. 57, 1069–1081. doi: 10.1037/0022-3514.57.6.1069
Ryff, C. D. (2018). “Eudaimonic well-being. Highlichts from 25 years of inquiry,” in Diversity in Harmony: Insights From Psychology - Proceedings of the 31st International Congress of Psychology, eds K. Shigemasu, S. Kuwano, T. Sato, and T. Matsuzawa (Hoboken, NJ: Wiley), 375–395.
Ryff, C. D., and Keyes, C. L. M. (1995). The structure of psychological well-being revisited. J. Personal. Soc. Psychol. 69, 719–727. doi: 10.1037/0022-3514.69.4.719
Shaffer, V. A., Brodney, S., Gavaruzzi, T., Zisman-Ilani, Y., Munro, S., Smith, S. K., et al. (2021). Do personal stories make patient decision aids more effective? Update from the international patient decision aids standards. Med. Decis. Making. 41, 897–906. doi: 10.1177/0272989X211011100
Shaffer, V. A., Focella, E. S., Hathaway, A., Scherer, L. D., and Zikmund-Fisher, B. J. (2018a). On the usefulness of narratives: an interdisciplinary review and theoretical model. Ann. Behav. Med. 52, 429–442. doi: 10.1093/abm/kax008
Shaffer, V. A., Focella, E. S., Scherer, L. D., and Zikmund-Fisher, B. J. (2016). Debiasing affective forecasting errors with targeted, but not representative, experience narratives. Patient Educ. Councel. 99, 1611–1619. doi: 10.1016/j.pec.2016.04.004
Shaffer, V. A., Hulsey, L., and Zikmund-Fisher, B. J. (2013a). The effects of process-focused versus experience-focused narratives in a breast cancer treatment decision task. Patient Educ. Counsel. 93, 255–264. doi: 10.1016/j.pec.2013.07.013
Shaffer, V. A., Owens, J., and Zikmund-Fisher, B. J. (2013b). The effect of patient narratives on information search in a web-based breast cancer decision aid: an eye-tracking study. J. Med. Internet Res. 15, e2784. doi: 10.2196/jmir.2784
Shaffer, V. A., Scherer, L. D., Focella, E. S., Hinnant, A., Len-Ríos, M. E., and Zikmund-Fisher, B. J. (2018b). What is the story with narratives? How using narratives in journalism changes health behavior. Health Commun. 33, 1151–1157. doi: 10.1080/10410236.2017.1333562
Shaffer, V. A., Tomek, S., and Hulsey, L. (2014). The effect of narrative information in a publicly available patient decision aid for early-stage breast cancer. Health Commun. 29, 64–73. doi: 10.1080/10410236.2012.717341
Shaffer, V. A., and Zikmund-Fisher, B. J. (2013). All stories are not alike: a purpose-, content-, and valence-based taxonomy of patient narratives in decision aids. Med. Decis. Making 33, 4–13. doi: 10.1177/0272989X12463266
Shen, F., Sheer, V. C., and Li, R. B. (2015). Impact of narratives on persuasion in health communication: a meta-analysis. J. Advertis. 44, 105–113. doi: 10.1080/00913367.2015.1018467
Syrowatka, A., Krömker, D., Meguerditchian, A. N., and Tamblyn, R. (2016). Features of computer-based decision aids: systematic review, thematic synthesis, and meta-analyses. J. Med. Internet Res. 18, e20. doi: 10.2196/jmir.4982
Thomas, J. J., Judge, A. M., Brownell, K. D., and Vartanian, L. R. (2006). Evaluating the effects of eating disorder memoirs on readers' eating attitudes and behaviors. Int. J. Eat Disord. 39, 418–425. doi: 10.1002/eat.20239
Thompson, T., and Kreuter, M. W. (2014). Using written narratives in public health practice: a creative writing perspective. Prev. Chronic Dis. 11, E94. doi: 10.5888/pcd11.130402
Tran, A., Redley, M., and de Wit, K. (2021). The psychological impact of pulmonary embolism: a mixed-methods study. Res. Prac. Thromb. Haemostasis 5, 301–307. doi: 10.1002/rth2.12484
Ubel, P. A., Jepson, C., and Baron, J. (2001). The inclusion of patient testimonials in decision aids: effects on treatment choices. Med. Decis. Making 21, 60–68. doi: 10.1177/0272989X0102100108
van Es, J., den Exter, P. L., Kaptein, A. A., Andela, C. D., Erkens, P. M. G., Klok, F. A., et al. (2013). Quality of life after pulmonary embolism as assessed with SF-36 and PEmb-QoL. Thromb. Res. 132, 500–505. doi: 10.1016/j.thromres.2013.06.016
Volkman, J. E., and Parrott, R. L. (2012). Expressing emotions as evidence in osteoporosis narratives: effects on message processing and intentions. Human Commun. Res. 38, 429–458. doi: 10.1111/j.1468-2958.2012.01433.x
Wendelboe, A. M., and Raskob, G. E. (2016). Global burden of thrombosis. Epidemiologic aspects. Circul. Res. 118, 1340–1347. doi: 10.1161/CIRCRESAHA.115.306841
Williams, A., Fossey, E., Farhall, J., Foley, F., and Thomas, N. (2018). Recovery after psychosis: qualitative study of service user experiences of lived experience videos on a recovery-oriented website. JMIR Ment. Health 5, e37. doi: 10.2196/mental.9934
Winterbottom, A., Bekker, H. L., Conner, M., and Mooney, A. (2008). Does narrative information bias individual descision making? A systematic review. Soc. Sci. Med. 67, 2079–2088. doi: 10.1016/j.socscimed.2008.09.037
Winterbottom, A., Bekker, H. L., Conner, M., and Mooney, A. F. (2012). Patient stories about their dialysis experience biases others' choices regardless of doctor's advice: an experimental study. Nephol. Dialyis Transplant. 27, 325–331. doi: 10.1093/ndt/gfr266
Woudstra, A. J., and Suurmond, J. (2019). How narratives influence colorectal cancer screening decision making and uptake: a realist review. Health Expect. 22, 327–337. doi: 10.1111/hex.12892
Zebregs, S., van den Putte, B., Neijens, P., and de Graaf, A. (2015). The differential impact of statistical and narrative evidence on beliefs, attitude, and intention: a meta-analysis. Health Commun. 30, 282–289. doi: 10.1080/10410236.2013.842528
Keywords: qualitative interviews, experience, types of narratives, evidence-based patient information, thematic analysis, well-being
Citation: Kalch A, Küchler C, Albani AR, Bilandzic H, Fischer S and Kirchberger I (2022) On the need for narratives in patient information: Differentiating types and functions of narratives from pulmonary embolism patients' point of view. Front. Commun. 7:990819. doi: 10.3389/fcomm.2022.990819
Received: 10 July 2022; Accepted: 05 September 2022;
Published: 29 September 2022.
Edited by:
Victoria Team, Monash University, AustraliaReviewed by:
Roma Subramanian, University of Nebraska Omaha, United StatesLik Sam Chan, The Chinese University of Hong Kong, China
Bryan Abendschein, Western Michigan University, United States
Copyright © 2022 Kalch, Küchler, Albani, Bilandzic, Fischer and Kirchberger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anja Kalch, anja.kalch@phil.uni-augsburg.de