 Daniela P. Mendes-de-Almeida1,2,3
Daniela P. Mendes-de-Almeida1,2,3 Fernanda S. G. Kehdy4
Fernanda S. G. Kehdy4 Remy Martins-Gonçalves5
Remy Martins-Gonçalves5 Joanna Bokel1,6
Joanna Bokel1,6 Eduarda Grinsztejn7
Eduarda Grinsztejn7 Patrícia Mouta Nunes de Oliveira2
Patrícia Mouta Nunes de Oliveira2 Maria de Lourdes de Sousa Maia2
Maria de Lourdes de Sousa Maia2 Brenda Hoagland8Sandra Wagner Cardoso8
Brenda Hoagland8Sandra Wagner Cardoso8 Beatriz Grinsztejn8
Beatriz Grinsztejn8 Marilda M. Siqueira9
Marilda M. Siqueira9 Pedro Kurtz10
Pedro Kurtz10 Patricia T. Bozza5,†
Patricia T. Bozza5,† Cristiana C. Garcia9,11*†
Cristiana C. Garcia9,11*†
- 1Department of Hematology, Evandro Chagas National Institute of Infectious Diseases, Fundação Oswaldo Cruz (FIOCRUZ), Rio de Janeiro, Brazil
- 2Department of Medical Affairs, Clinical Studies, and Post-Registration Surveillance (DEAME), Institute of Technology in Immunobiologicals/Bio-Manguinhos, Fundação Oswaldo Cruz (FIOCRUZ), Rio de Janeiro, Brazil
- 3Research Center, Instituto Nacional de Câncer (INCA), Rio de Janeiro, Brazil
- 4Laboratório de Hanseníase, Instituto Oswaldo Cruz, Fundação Oswaldo Cruz (FIOCRUZ), Rio de Janeiro, Brazil
- 5Laboratory of Immunopharmacology, Instituto Oswaldo Cruz, Fundação Oswaldo Cruz (FIOCRUZ), Rio de Janeiro, Brazil
- 6Onco-Hematology Unit, Clínica São Vicente, Rio de Janeiro, Brazil
- 7Department of Medicine, Hematology and Oncology Division, University Hospitals, Case Western University, Cleveland, OH, United States
- 8Laboratory of Clinical Research on STD/AIDS, Evandro Chagas National Institute of Infectious Diseases Oswaldo Cruz Foundation (FIOCRUZ), Rio de Janeiro, Brazil
- 9Laboratório de Vírus Respiratórios, Exantemáticos, Enterovírus e Emergências Virais, Instituto Oswaldo Cruz, Fundação Oswaldo Cruz (FIOCRUZ), Rio de Janeiro, Brazil
- 10Intensive Care Department, Instituto D’Or de Pesquisa e Ensino, Rio de Janeiro, Brazil
- 11Grupo Integrado de Pesquisas em Biomarcadores, Instituto René Rachou, Fundação Oswaldo Cruz (FIOCRUZ-Minas), Belo Horizonte, Brazil
The emergence of the rare syndrome called vaccine-induced immune thrombocytopenia and thrombosis (VITT) after adenoviral vector vaccines, including ChAdOx1 nCov-19, raises concern about one's predisposing risk factors. Here we report the case of a 56-year-old white man who developed VITT leading to death within 9 days of symptom onset. He presented with superior sagittal sinus thrombosis, right frontal intraparenchymal hematoma, frontoparietal subarachnoid and massive ventricular hemorrhage, and right lower extremity arterial and venous thrombosis. His laboratory results showed elevated D-dimer, C-reactive protein, tissue factor, P-selectin (CD62p), and positive anti-platelet factor 4. The patient's plasma promoted higher CD62p expression in healthy donors' platelets than the controls. Genetic investigation on coagulation, thrombophilia, inflammation, and type I interferon-related genes was performed. From rare variants in European or African genomic databases, 68 single-nucleotide polymorphisms (SNPs) in one allele and 11 in two alleles from common SNPs were found in the patient genome. This report highlights the possible relationship between VITT and genetic variants. Additional investigations regarding the genetic predisposition of VITT are needed.
Introduction
Mass vaccination against SARS-CoV-2 was the main measure to mitigate hospitalizations, long-term health outcomes, and death due to the COVID-19 pandemic. However, after millions of doses were administered, reports of a very rare syndrome called vaccine-induced immune thrombocytopenia and thrombosis (VITT) began to rise (1). The hallmark features are thrombocytopenia, thrombosis within 5–30 days of adenoviral SARS-CoV-2 vaccination, with strikingly elevated levels of D-dimer, hypofibrinogenemia, and positive antibodies against platelet factor 4 (PF4) (2). The clinical presentation depends on the thrombosis site. The typical targets are the cerebral venous sinus or splanchnic vein, arterial, or multiple beds (1–3).
The underlying mechanism of the syndrome is similar to heparin-induced thrombocytopenia (HIT), with the formation of aggregates of PF4 and the ChAdOx1 adenovector in an inflammatory environment induced by vaccination, with subsequent generation of high-avidity anti-PF4 IgG, which triggers platelet activation, prothrombotic cascade, and release of neutrophil extracellular traps (NETs) (4). However, the interplay between anti-PF4 antibodies and platelet activation is complex. A longitudinal study showed a slight but transient thrombin generation after ChadOx1 nCov-19. In addition, 19.6% (12/61) samples were positive for anti-PF4 before vaccination and 3.2% (2/61) were considered strong. Low titers of anti-PF4 remained unchanged after vaccination, and no seroconversion was detected. No thrombotic events occurred in this study (5).
Differences in incidence among countries and detection of oligoclonal anti-PF4 antibodies raised the suspicion of a genetic predisposition in VITT (6, 7). Individual factors like genetic ancestry might play a critical role in disease pathogenesis. Here, we report a fatal case of a Brazilian male who developed VITT 4 days after vaccination with ChAdOx1 nCov-19, its platelet activation profile, and genetic analysis.
Case description
A 56-year-old white man with a history of essential hypertension controlled with atenolol received the first ChAdOx1 nCov-19 vaccine in early May 2021. Four days after vaccination, he developed fever, malaise, and persistent headache. On the fifth day following vaccination, he presented with nausea, vomiting, fall from his height, generalized skin rash on the lower limbs, and ecchymosis. He was promptly admitted. His platelet count was 17,000/mm3 (150,000–450,000/mm3), D-dimer 41,000 ng/ml (<500 ng/ml), and fibrinogen 121 mg/dl (200–400 mg/dl). Peripheral smear showed no platelet clumps or schistocytes. Brain computed tomography (CT) examination identified right frontal heterogeneous intraparenchymal hematoma, measuring approximately 6.4 cm × 5.2 cm × 4.8 cm with a thin hypodense halo, causing mass effect with a local reduction in the amplitude of the sulci, compression over the right lateral ventricle resulting in contralateral deviation of midline structures by 0.7 cm, in addition to areas of bilateral frontoparietal subarachnoid hemorrhage. He also presented with a massive ventricular hemorrhage filling in the right lateral ventricle, the posterior horn of the left lateral ventricle, and the fourth ventricle, and bleeding in the right Sylvian cistern and perimesencephalic cistern. There was no evidence of aneurysmal dilatation. The CT angiogram the following day identified thrombosis in the superior sagittal sinus. Also, a lower extremities Doppler ultrasound showed right arterial and venous thrombosis. He underwent urgent neurosurgery for hematoma drainage and decompressive craniectomy. A few hours after the procedure, he developed new bleeding and bilateral cerebral edema and received plasma, cryoprecipitate, fibrinogen concentrate, platelet transfusions, and 70 g (1 g/kg) intravenous immunoglobulin. Despite all measures, the patient died with refractory intracranial hypertension on day 13 after vaccination.
Laboratory and clinical investigation
Patient’s relatives and healthy unvaccinated controls provided written informed consent approved by the local Ethics Committee for clinical and laboratory investigations (CAAE #68118417.6.0000.5248 and #48532621.8.0000.5262, respectively). SARS-CoV-2 RT-PCR of the nasopharyngeal swab and serology to dengue, Chikungunya, Zika, HIV, hepatitis B and C, Cytomegalovirus (CMV), Epstein-Barr virus (EBV), toxoplasmosis, and rubella were negative. Relatives denied any past COVID-19 infection or heparin exposure. There was no personal or family history of thrombosis or miscarriages.
IgG anti-PF4 antibodies were detected with a 3.33 optical density (reference ≤ 0.4). A flow cytometry-based assay to detect platelet-activating antibodies was performed according to Handtke et al. (8) (Figure 1A). When added to healthy donor platelets, patient plasma elicited increased expression of CD62p to a greater extent than plasma from healthy heterologous donors. However, in the presence of high concentrations of heparin, which can destabilize PF4/adenovector aggregates due to its higher affinity to PF4, platelet activation levels were reduced to control levels, confirming the presence of platelet-activating immunocomplexes in the patient's plasma. Elevated plasmatic levels of CD62p, released by activated platelets and endothelial cells, and of tissue factor (TF, coagulation factor III), the primary activator of the extrinsic pathway of the coagulation cascade, corroborate the extensive platelet activation and clot formation (Figures 1B,C). Additional laboratory results are characterized in Table 1. The results of other blood tests were unremarkable except for increased alanine aminotransferase, C-reactive protein, IL-1β, and caspase-1. Antinuclear antibodies, anti-cardiolipin IgG and IgM, lupus anticoagulant, and beta-2 glycoprotein 1 IgG were not detected.
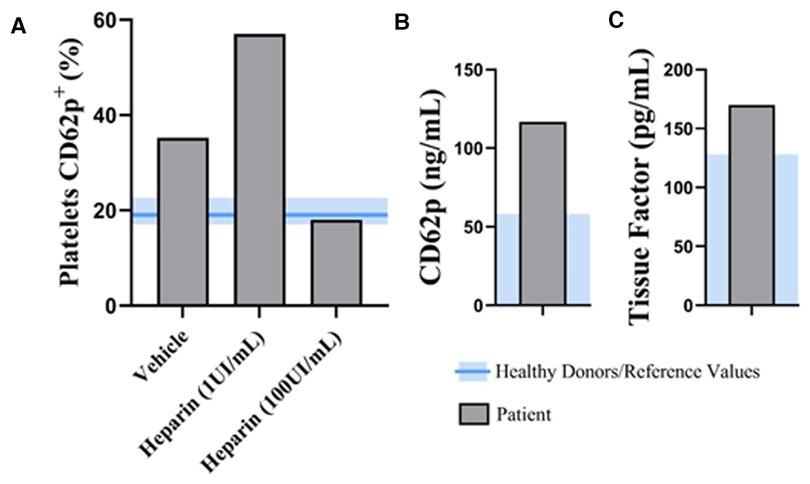
Figure 1. Functional VITT test, markers of platelet activation and coagulation. (A) A flow cytometry-based assay to detect platelet-activating antibodies was performed according to Handtke et al. Levels of CD62p surface expression in healthy donor's platelets stimulated with plasma from the patient in the presence of low (1 UI/ml) and high (100 UI/ml) concentrations of heparin. Plasmatic levels of CD62p (B) and tissue factor (C). The blue area represents the reference range of healthy donors. VITT, vaccine-induced immune thrombocytopenia and thrombosis;
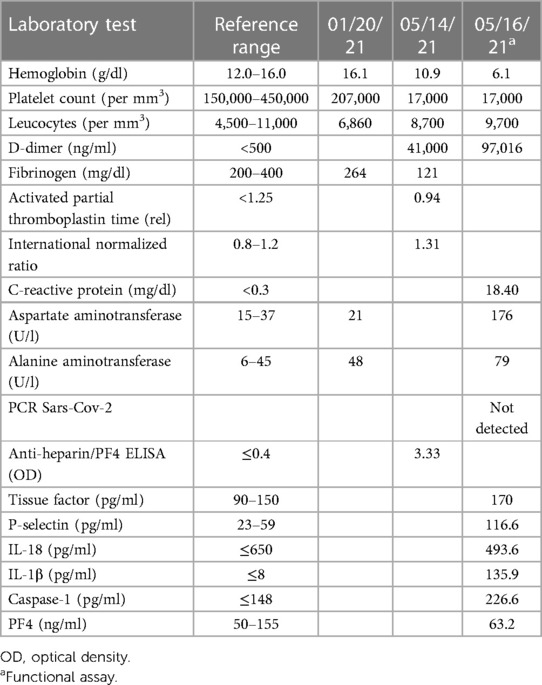
Table 1. Patient’s laboratory data.
We performed genetic analysis using the Axiom™ Human Genotyping SARS-CoV-2 Research Array, which genotypes more than 870,000 single-nucleotide polymorphisms (SNPs) in the human genome. The first strategy consisted of screening mutations in 232 autosomal genes essential for thrombotic syndromes, to inflammatory disorders, and related to type I interferon (IFN) signaling (Table 2). Aiming to select rare variants, the minor allele frequency up to 0.01 in European or African populations was settled as a cutoff. Six thousand four hundred sixty-six related SNPs were present in the array, and 5,953 are described in the 1KGP database. From the selected SNPs, 689 and 845 rare putative variants were found in databases of African and European populations, respectively. Among them, 68 were found in heterozygosity in the patient. From these, seven SNPs have been studied in clinical conditions; four were considered benign; one likely benign; one, rs116667976, in the Factor XI gene (F11) with conflicting interpretations of pathogenicity (9); and the last one, rs2884737, in the VKORC1 gene, associated with Warfarin drug response. A descriptive analysis of the SNPs is depicted in Table 3.

Table 2. List of autosomal genes and number of SNPs investigated in the case of VITT.
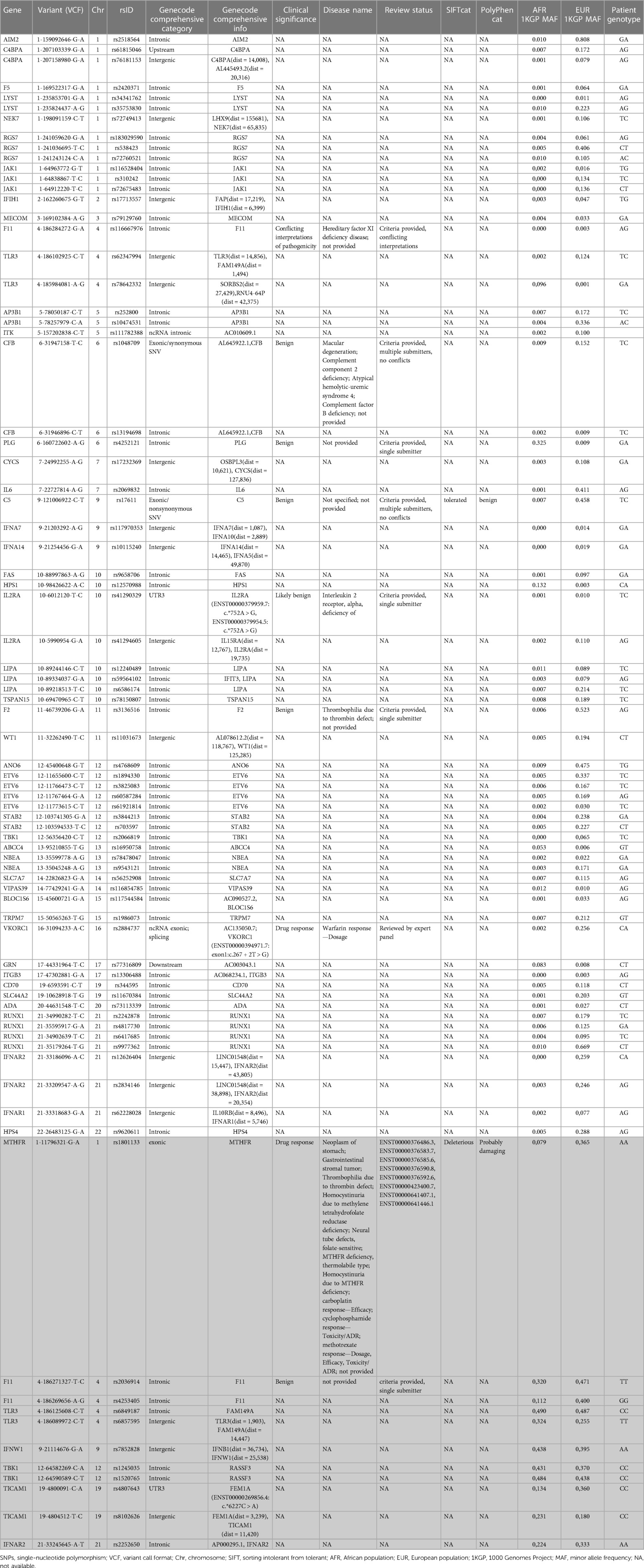
Table 3. Annotation of rare SNPs found in heterozygosity and common SNPs in homozygosity (gray) in the patient.
In addition to the search for rare variants, a second strategy was employed. We performed a screening of common mutations in the European or African populations that were in homozygosity in the patient. We assessed classical hereditary thrombophilia-associated mutations: Factor V Leiden G1691A (rs6025), Factor II G20210A (rs1799963), and methylenetetrahydrofolate reductase (MTHFR), C677T (rs1801133) and A1298C (rs1801131), in addition to distinct mutations on F11 and genes related to type I IFN. The patient was homozygous for the missense MTHFR variant c.665C > T chr1-11856378 G > A p.Ala222Val NM_005957.5 rs1801133, with clinical relevance for methotrexate drug response, with a general population frequency of approximately 0.3. His medical records from January 2021 and 2008 showed normal levels of folic acid and homocysteine, respectively. Also, he was not on vitamin B12 supplementation or had ever had hemolysis. Furthermore, he was homozygous for the variants in FXI rs2036914 and rs4253405; in TLR3 rs6849187 and rs6857595; in IFNW1 rs7852828; in TBK1/RASSF3 rs1245035 and rs1520765; in TICAM1 rs4807643 and rs8102626; and in IFNAR2 rs2252650. Besides rs2036914, classified as benign, none of these variants have been described as associated with clinical diseases (Table 3 in gray).
Discussion
VITT is a rare but life-threatening disease described after the COVID-19 vaccination rollout with the adenoviral platform (2). The regulatory agencies use thrombosis with thrombocytopenia syndrome (TTS) as a descriptive term for VITT, not necessarily caused by vaccination (10). Herein, we describe a patient who developed a clinical condition consistent with the Level 1 TTS Brighton Collaboration case definition after the first dose of ChAdOx1 nCoV-19 (11). Our patient was one of the 39 VITT cases described in Brazil after primary vaccination in 2021 (12). According to the UK Expert Hematology Panel published by Pavord et al. (2), he was also classified as a definite VITT case. This series of 220 VITT British patients identified platelet counts of less than 30,000/mm3 and the presence of intracranial hemorrhage as being independently associated with death, with 73% mortality if they coexist (2). Our patient presented both poor prognostic factors and succumbed despite proper healthcare assistance.
Differences in VITT incidence worldwide support distinct genetic ancestries on pathogenesis, although other explanations, such as underreporting and health systems inequalities, should be addressed. The highest incidence was reported in Norway after ChAdOx1 nCoV-19, with five cases among 130,000 individuals, suggesting an incidence of 1 in 26,000 (13). In the United States, the VAERS surveillance system identified 54 cases of TTS from among over 14 million recipients of Ad26.COV2.S, for an incidence of 3.8 per million (approximately 1 in 263,000) (14). In addition to age below 50 years and first exposure to the COVID-19 adenovirus vaccine within 30 days, VITT risk factors are unknown and seem to differ from the traditional prothrombotic conditions. Unlike HIT, VITT is caused by monoclonal or oligoclonal anti-PF4 antibodies (7). This finding also indicates a potential role for the genetic predisposition in VITT pathophysiology. Thus, further studies characterizing anti-PF4 antibody–producing cells are needed.
The effect of MTHFR variants on thrombotic risk is controversial. Recent guidelines state that MTHFR polymorphisms should not be a part of inherited thrombophilia testing due to a lack of clinical evidence (15, 16). However, a meta-analysis based on case-control studies found that the rs1801133 MTHFR C677T polymorphism—the same identified in our patient—could increase ischemic stroke susceptibility in Asian, male, and young-middle age populations (17). Another meta-analysis enrolled 99 genetic association studies, including Brazilians, concluded that the MTHFR rs1801133 polymorphism might be implicated in developing deep vein thrombosis and pulmonary embolism in non-VITT patients and may serve as a potential biological marker for venous thromboembolism in Caucasians, East Asians, and West Asians (18). Yet, the frequency of MTHFR polymorphisms in VITT is unexplored. A heterozygous MTHFR C677T rs1801133 variant has been identified in an Italian patient with cerebral sinus thrombosis with thrombocytopenia after COVID-19 vaccination and increased levels of homocysteine and folate deficiency (19). This description was a probable VITT case, given the lack of anti-PF4 positivity. Another paper from Germany has reported two women presenting with cerebral sinus vein thrombosis after the ChAdOx1 vaccine, each carrying an MTHFR variant (heterozygous A1298C and homozygous MTHFR C677T variant) (20).
The F11 variant rs116667976 found in heterozygosity in the patient is classified as likely benign by ACMG and presented as having conflicting interpretations of pathogenicity in the ClinVar database. It has been selected as a potentially functional mutation in thrombosis without functional analysis available (21). The same SNP was described in 2 out of 49 women with heavy menstrual bleeding. However, functional data are still missing for assessing the involvement of this very rare variant in thrombotic diseases (22). The other F11 variants that were presented in two alleles of the patient, rs2036914 and rs4253405, African and European, have been evaluated in studies of percutaneous coronary intervention and venous thrombosis, respectively, but the genotype found in the patient from our study has not been described to be associated with any disease (23). The high allele frequency of these SNPs makes it difficult to find any associations.
Type I IFNs are induced by exposure of cells to pathogen-associated molecular patterns (PAMPs) detected by receptors like toll-like receptors (TLRs). By distinct mechanisms, type I IFN signaling leads to inflammasome activation, pyroptosis, and, lately, the release of proinflammatory molecules and prothrombotic mediators, like TF, initiating the extrinsic coagulation pathway (24). Due to the involvement of type I IFN response to thrombotic processes, we also evaluated SNPs in the related genes. We found eight variants in homozygosity in the patient. However, none of them are found in exons or have been studied for thrombotic diseases.
Early recognition and treatment are essential for a favorable outcome in VITT. Risk factors are still poorly understood. We described a case report of VITT in an individual harboring a benign rs1801133 homozygous variant in MTHFR and the rs116667976, rs2036914, and rs4253405 in the F11, apart from homozygous mutations in IFNAR2, IFNW1, TBK1, TICAM1, and TLR3 genes without reported clinical significance. Although these findings could favor a genetic predisposition, most of the variants found are frequent, and further genomic research is needed to establish a causal association.
Patient perspective
This work is of value for alerting healthcare professionals to the early signs and symptoms of VITT and adding information about a possible genetic background related to the disease development.
Data availability statement
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Comitê de Ética em Pesquisa com Seres Humanos do Isntituto Oswaldo Cruz. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the patient's brother for the publication of this case report.
Author contributions
DPMA and CCG: conceptualizing and writing the original draft. DPMA and PK: attending to the patient and analyzing the clinical data. RMG and PTB: performing and analyzing the platelet functional assay and writing; JB, EG, BH, SWC, and BG: recruiting controls for platelet functional assay comparison and revising the manuscript. PMNO and MMLSM: revising the manuscript. FSGK: performing genetic data analysis. MMS, BG, PTB, and CCG: supervising the study, funding acquisition, writing review, and editing. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by INOVA Covid-19 Geração de Conhecimento FIOCRUZ/Fundação Oswaldo Cruz (Grant number 48402179262880) and FAPERJ. Instituto Oswaldo Cruz was in charge of the publication fee.
Acknowledgments
We thank the patient's relatives and controls for consenting to the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Greinacher A, Thiele T, Warkentin TE, Weisser K, Kyrle PA, Eichinger S. Thrombotic thrombocytopenia after ChAdOx1 nCov-19 vaccination. N Engl J Med. (2021) 384(22):2092–101. doi: 10.1056/NEJMoa2104840
2. Pavord S, Scully M, Hunt BJ, Lester W, Bagot C, Craven B, et al. Clinical features of vaccine-induced immune thrombocytopenia and thrombosis. N Engl J Med. (2021) 385(18):1680–9. doi: 10.1056/NEJMoa2109908
3. Buoninfante A, Andeweg A, Baker AT, Borad M, Crawford N, Dogné JM, et al. Understanding thrombosis with thrombocytopenia syndrome after COVID-19 vaccination. npj Vaccines. (2022) 7(1):141. doi: 10.1038/s41541-022-00569-8
4. Greinacher A, Selleng K, Palankar R, Wesche J, Handtke S, Wolff M, et al. Insights in ChAdOx1 nCoV-19 vaccine-induced immune thrombotic thrombocytopenia. Blood. (2021) 138(22):2256–68. doi: 10.1182/blood.2021013231
5. Campello E, Bulato C, Simion C, Spiezia L, Radu CM, Gavasso S, et al. Assessing clinically meaningful hypercoagulability after COVID-19 vaccination: a longitudinal study. Thromb Haemost. (2022) 122(08):1352–60. doi: 10.1055/a-1788-5206
6. Arepally GM, Ortel TL. Vaccine-induced immune thrombotic thrombocytopenia: what we know and do not know. Blood. (2021) 138(4):293–8. doi: 10.1182/blood.2021012152
7. Kanack AJ, Bayas A, George G, Abou-Ismail MY, Singh B, Kohlhagen MC, et al. Monoclonal and oligoclonal anti-platelet factor 4 antibodies mediate VITT. Blood. (2022) 140(1):73–7. doi: 10.1182/blood.2021014588
8. Handtke S, Wolff M, Zaninetti C, Wesche J, Schönborn L, Aurich K, et al. A flow cytometric assay to detect platelet-activating antibodies in VITT after ChAdOx1 nCov-19 vaccination. Blood. (2021) 137(26):3656–9. doi: 10.1182/blood.2021012064
9. NM_000128.4(F11):c.1304+12G>A and hereditary factor XI deficiency disease [Internet]. National Library of Medicine. (2023). Available at: https://www.ncbi.nlm.nih.gov/clinvar/RCV001151016.4/ (Accessed March 10, 2023).
10. Makris M, Pavord S. Most cases of thrombosis and thrombocytopenia syndrome (TTS) post ChAdOx-1 nCov-19 are vaccine-induced immune thrombotic thrombocytopenia (VITT). Lancet Reg Health Eur. (2022) 12:100274. doi: 10.1016/j.lanepe.2021.100274
11. Chen RT. Updated proposed Brighton collaboration process for developing a standard case definition for study of new clinical syndrome X, as applied to thrombosis with thrombocytopenia syndrome (TTS) [Internet]. (2021). Available at: https://brightoncollaboration.us/wp-content/uploads/2021/05/TTS-Interim-Case-Definition-v10.16.3-May-23-2021.pdf (cited October 4, 2021).
12. Mouta Nunes de Oliveira P, Mendes-de-Almeida DP, Bertollo Gomes Porto V, Crespo Cordeiro C, Vitiello Teixeira G, Saraiva Pedro R, et al. Vaccine-induced immune thrombotic thrombocytopenia after COVID-19 vaccination: description of a series of 39 cases in Brazil. Vaccine. (2022) 40(33):4788–95. doi: 10.1016/j.vaccine.2022.06.014
13. Schultz NH, Sørvoll IH, Michelsen AE, Munthe LA, Lund-Johansen F, Ahlen MT, et al. Thrombosis and thrombocytopenia after ChAdOx1 nCoV-19 vaccination. N Engl J Med. (2021) 384(22):2124–30. doi: 10.1056/NEJMoa2104882
14. See I, Lale A, Marquez P, Streiff MB, Wheeler AP, Tepper NK, et al. Case series of thrombosis with thrombocytopenia syndrome after COVID-19 vaccination-United States, December 2020 to August 2021. Ann Intern Med. (2022) 175(4):513–22. doi: 10.7326/M21-4502
15. Hickey SE, Curry CJ, Toriello HV. ACMG Practice guideline: lack of evidence for MTHFR polymorphism testing. Genet Med. (2013) 15(2):153–6. doi: 10.1038/gim.2012.165
16. Deloughery TG, Hunt BJ, Barnes GD, Connors JM, Ay C, Barco S, et al. A call to action: MTHFR polymorphisms should not be a part of inherited thrombophilia testing. Res Pract Thromb Haemost. (2022) 6(4):e12739. doi: 10.1002/rth2.12739
17. Chen M, Mao BY, Wang D, Cheng X, Xu CX. Association between rs1801133 polymorphism and risk of adult ischemic stroke: meta-analysis based on case–control studies. Thromb Res. (2016) 137:17–25. doi: 10.1016/j.thromres.2015.11.037
18. Zeng J, Zeng Q. Correlations between methylenetetrahydrofolate reductase gene polymorphisms and venous thromboembolism: a meta-analysis of 99 genetic association studies. Eur J Prev Cardiolog. (2019) 26(2):120–34. doi: 10.1177/2047487318799467
19. Castelli GP, Pognani C, Sozzi C, Franchini M, Vivona L. Cerebral venous sinus thrombosis associated with thrombocytopenia post-vaccination for COVID-19. Crit Care. (2021) 25(1):137. doi: 10.1186/s13054-021-03572-y
20. Fousse M, Schub D, Merzou F, Fassbender K, Sester M, Kettner M, et al. Case report: cerebral sinus vein thrombosis in two patients with AstraZeneca SARS-CoV-2 vaccination. J Neurol. (2022) 269(2):583–6. doi: 10.1007/s00415-021-10731-2
21. Martin-Fernandez L, Gavidia-Bovadilla G, Corrales I, Brunel H, Ramírez L, López S, et al. Next generation sequencing to dissect the genetic architecture of KNG1 and F11 loci using factor XI levels as an intermediate phenotype of thrombosis. PLoS One. (2017) 12(4):e0176301. doi: 10.1371/journal.pone.0176301
22. Wiewel-Verschueren S, Mulder AB, Meijer K, Mulder R. Factor 11 single-nucleotide variants in women with heavy menstrual bleeding. J Obstet Gynaecol. (2017) 37(7):912–8. doi: 10.1080/01443615.2017.1312303
23. Campo G, Lunghi B, Pavasini R, Ferraresi P, Punzetti S, Malagù M, et al. Factor XI rs2036914 gene polymorphism and occurrence of adverse events after percutaneous coronary intervention. A prospective evaluation. Int J Cardiol. (2014) 177(2):711–3. doi: 10.1016/j.ijcard.2014.10.014
Keywords: vaccine-induced thrombotic thrombocytopenia, ChAdOx1 nCoV-19 vaccine, genetic predisposition, polymorphisms, anti-PF4 antibodies, VITT
Citation: Mendes-de-Almeida DP, Kehdy FSG, Martins-Gonçalves R, Bokel J, Grinsztejn E, Mouta Nunes de Oliveira P, Maia Maria de Lourdes de Sousa, Hoagland B, Wagner Cardoso S, Grinsztejn B, Siqueira MM, Kurtz P, Bozza PT and Garcia CC (2023) A case report of vaccine-induced immune thrombotic thrombocytopenia (VITT) with genetic analysis. Front. Cardiovasc. Med. 10:1189320. doi: 10.3389/fcvm.2023.1189320
Received: 18 March 2023; Accepted: 24 April 2023;
Published: 19 May 2023.
Edited by:
Luca Spiezia, University of Padua, ItalyReviewed by:
Omer Iqbal, Loyola University Chicago, United StatesAriela Hoxha, University Hospital of Padua, Italy
© 2023 Mendes-de-Almeida, Kehdy, Martins-Gonçalves, Bokel, Grinsztejn, Mouta Nunes de Oliveira, Maia, Hoagland, Wagner Cardoso, Grinsztejn, Siqueira, Kurtz, Bozza and Garcia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cristiana C. Garcia Y3Jpc3RpYW5hLmdhcmNpYUBmaW9jcnV6LmJy
†These authors have contributed equally to this work