 Andreas Schaefer1*
Andreas Schaefer1* Till Joscha Demal1
Till Joscha Demal1 Oliver D. Bhadra1
Oliver D. Bhadra1 David Grundmann2Lisa Voigtländer2Lara Waldschmidt2Johannes Schirmer1
David Grundmann2Lisa Voigtländer2Lara Waldschmidt2Johannes Schirmer1 Simon Pecha1Yvonne Schneeberger1
Simon Pecha1Yvonne Schneeberger1 Niklas Schofer2
Niklas Schofer2 Nils Sörensen2Stefan Blankenberg2Hermann Reichenspurner1
Nils Sörensen2Stefan Blankenberg2Hermann Reichenspurner1 Moritz Seiffert2
Moritz Seiffert2 Lenard Conradi1
Lenard Conradi1
- 1Department of Cardiovascular Surgery, University Heart and Vascular Center Hamburg, Hamburg, Germany
- 2Department of Cardiology, University Heart and Vascular Center Hamburg, Hamburg, Germany
Background: Valve-in-valve (ViV) transfemoral transcatheter aortic valve implantation (TAVI) for failing aortic surgical bioprostheses or transcatheter heart valves (THV) has demonstrated a reasonable clinical and hemodynamic efficacy. Traditionally, self-expanding (SE) supra-annular THV are considered to result in superior hemodynamics compared with balloon-expandable intra-annular THV after ViV. However, so far no data are found on latest-generation intra-annular SE THV for aortic ViV procedures which might be superior with regard to coronary access or subsequent valve reintervention.
Aim: We herein aim to evaluate a latest-generation SE intra-annular THV for aortic ViV procedures.
Materials and methods: Between May 2022 and November 2022, five consecutive patients (4/5 female with mean age of 76.2 years and mean Society of Thoracic Surgeons predicted risk of mortality score of 2.9%) received ViV TAVI using the Navitor system (Abbott, Chicago, IL, USA) for treatment of failing surgical bioprostheses or THV. Data were retrospectively analyzed according to updated Valve Academic Research Consortium 3 (VARC-3) definitions.
Results: At 30 days, absence of mortality and VARC-3 adjudicated clinical endpoints were documented. Echocardiography at 30 days revealed complete absence of paravalvular leakage and single-digit mean transvalvular gradients (mean of 6.0 mmHg) in all patients.
Conclusion: The investigated intra-annular SE THV results in excellent 30-day outcomes for aortic ViV procedures for failing surgical bioprostheses or THV. Despite the intra-annular design, hemodynamic results were excellent, even in small bioprostheses. Ease of use of this valve platform is reflected by only two cycles of resheathing in five ViV procedures with hemodynamic stability during all steps of valve deployment.
Introduction
Valve-in-valve (ViV) transfemoral (TF) transcatheter aortic valve implantation (TAVI) for failing aortic surgical bioprostheses or transcatheter heart valves (THV) has demonstrated a reasonable clinical and hemodynamic efficacy in patients not suitable for redo surgical aortic valve replacement (SAVR) (1, 2). Therefore, this technique was implemented in international guidelines for treatment of valvular heart disease (3, 4). However, certain drawbacks of this procedure were especially described concerning suboptimal hemodynamic results in patients with small bioprostheses or risk of coronary occlusion in patients with low coronary ostia take-off (5, 6). In the past, several procedural steps were introduced to overcome these possible complications including bioprosthetic valve fracture (BVF) to optimize hemodynamic results and intentional leaflet laceration to mitigate the risk of coronary occlusion (7, 8). In terms of postinterventional hemodynamic results, traditionally self-expanding (SE) supra-annular THV are considered to present superior hemodynamics compared with balloon-expandable (BE) intra-annular THV (9, 10). However, apart from a single-case report (11), so far no data are found on the use of a latest-generation SE intra-annular THV for ViV TF-TAVI in failing aortic surgical bioprostheses or THV. The Navitor THV (Abbott, Chicago, IL, USA) consists of a bovine pericardium bioprosthesis mounted in a nitinol frame covering an annulus range from 19 mm to 27 mm. The FlexNav Delivery integrated sheath system presents a True ID of 18 Fr. for the 23 and 25 mm THV and 19 Fr. for the 27 and 29 mm THV and is compatible with 14/15 Fr. sheathes. We herein report our first experience with aortic ViV procedures using this latest-generation intra-annular SE THV.
Materials and methods
Patients
Between May 2022 and November 2022, five consecutive patients [4/5 female with mean age of 76.2 years and mean Society of Thoracic Surgeons predicted risk of mortality (STS PROM) score of 2.9%] received ViV TAVI using this SE intra-annular THV for the treatment of failing surgical bioprostheses or THV as determined by transthoracic (TTE) and/or transesophageal echocardiography (TEE). Decision to implant this particular THV as well as application of concomitant procedures such as intentional leaflet laceration or BVF was left to operators’ discretion, and no specific anatomical criteria for using this platform were noted. However, aspects included in decision-making for utilization of BVF consisted of size of index valve and anticipated hemodynamic result, height of coronary ostia take-off, sinotubular junction width, and anticipated risk of sinotubular junction sequestration. In particular, in two patients (patient no. 1 and 3) with a labeled size of the index valve of 21 and 23 mm, BVF was performed to optimize hemodynamic results. In these patients, a wide sinotubular junction and high coronary ostia take-off were seen, and therefore risk for coronary occlusion was mostly absent. Contrarily, in a patient with a labeled size of 23 mm (patient no. 5), no BVF was conducted since a narrow sinotubular junction and low coronary ostia take-off were seen. In this particular patient, BVF would have increased the risk for coronary occlusion.
Allocation of patients to ViV TAVI followed current international recommendations (3) after consensus of the local dedicated heart team. According to the Valve Academic Research Consortium 3 (VARC)-3 criteria, a type of bioprosthetic valve dysfunction was structural valve deterioration in all patients (12) with the echocardiographic correlates of significant stenosis in four out of five patients and severe regurgitation in one patient.
Diagnostic work-up
The preprocedural diagnostic work-up followed institutional standards and was previously described (13): by routine, all patients received preoperative TTE and TEE for evaluation of cardiac functional status. Furthermore, diagnostic work-up included contrast-enhanced, electrocardiogram-gated multislice computed tomography (MSCT). Datasets were analyzed using the 3mensio Medical Imaging Software (3mensio, Medical Imaging, Bilthoven, Netherlands) for determination of adequate THV size as well as assessment of aortic root anatomy and morphology with an emphasis on the distance of coronary arteries to the aortic annulus and sinus width and assessment of aorto-iliac and peripheral vascular status.
All procedures were performed in a specially equipped hybrid operating suite by a dedicated team of cardiologists, cardiac surgeons, and anesthesiologists. THV function was assessed by invasive measurements of hemodynamics, aortic root angiography, and TTE.
Study procedure
Institutional standards for aortic ViV procedures were previously described (14). In brief, all herein described procedures were performed via TF access with local anesthesia as first-line approach, except for patients in which intentional leaflet laceration was performed where general anesthesia was used to enable TEE guidance. Utilized vascular closure systems consisted of suture-based devices (ProGlide/ProStyle; Abbott, Chicago, IL, USA) or a collagen plug-based device (MANTA; Teleflex, Wayne, PA, USA). In all patients without intentional leaflet laceration, a single femoral puncture as interventional access was performed, and non-interventional access was conducted via the right-sided radial artery. In one patient (patient no. 4), a single-puncture ViV TAVI without non-interventional access was performed. Target height for THV valve deployment was alignment of both lower stent rims to create optimal postinterventional hemodynamics with full stent deployment of the THV. In one patient with low coronary ostia take-off, intentional deep implantation into a Sapien 3 Ultra (Edwards Lifesciences, Irvine, CA, USA) was performed to protect against coronary occlusion. Intentional leaflet laceration was performed as previously described (15). BVF was performed prior to THV implantation and independently from the anticipated hemodynamic result. Following the procedure, all patients were transferred to a postoperative holding area until the first postoperative day and further stayed until discharge was completed on the ward.
Statistical analyses
Baseline and intraprocedural data were retrospectively collected, entered into a standardized database, and analyzed. Clinical endpoints were adjudicated in accordance with the updated standardized VARC-3 definitions (12). Patients were presented isolated in tables. For summarized data, absolute numbers were given for categorical variables and mean values for continuous variables.
Results
Baseline demographics
Patients presented with a moderate co-morbidity burden (one patient with concomitant coronary artery disease, one patient with s/p stroke, one patient with clinically significant chronic obstructive pulmonary disease) as reflected by the low mean STS PROM score of 2.9%. Three out of five patients were severely symptomatic in New York Heart Association (NYHA) functional class ≥III. Left ventricular function was preserved in all cases. Implanted bioprostheses during index procedures consisted of two surgical bovine pericardial valves [Perimount 21 and 23 mm (Edwards Lifesciences, Irvine, CA, USA)], two surgical porcine valves [Hancock 27 mm and Mosaic 23 mm (Medtronic, Minneapolis, MS, USA)], and one THV (Sapien 3, 26 mm). The range of time interval to ViV procedure was 70–165 months.
Detailed patient demographics are summarized in Table 1.
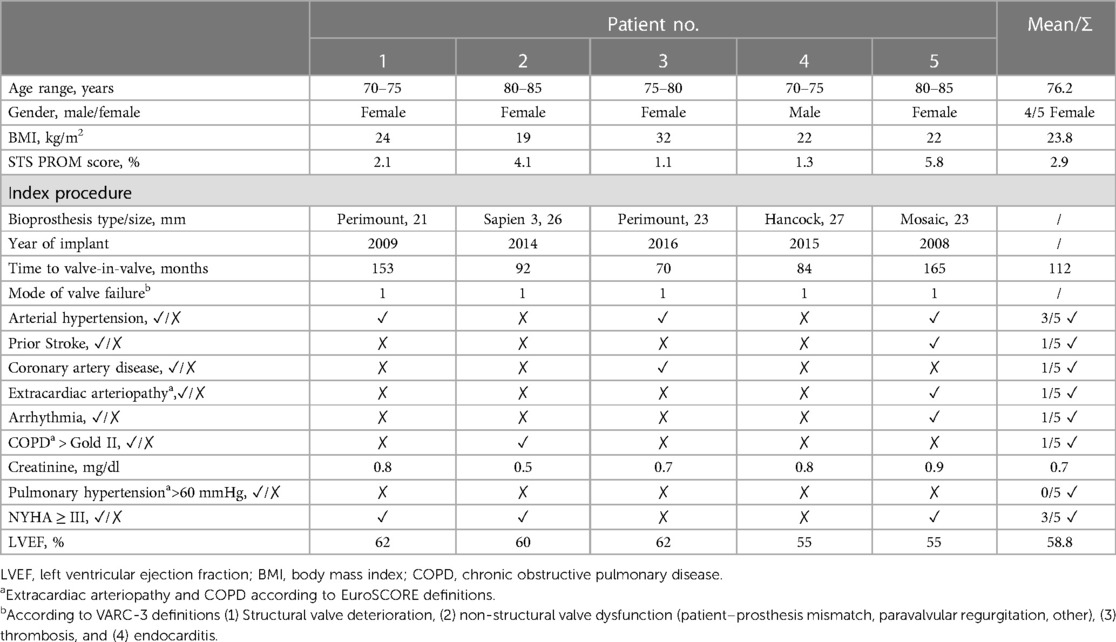
Table 1. Baseline data.
Periprocedural data
Mean peak/mean pressure gradients of degenerated bioprostheses with stenosis were 59.8/37.0 mmHg as determined by preprocedural TTE and/or TEE. In one patient, the leading cause for ViV procedure was severe valvular regurgitation. The range of procedure time, fluoroscopy time, and contrast agent used were 14–93 min, 8–28 min, and 50–143 ml, respectively. A cerebral protection system (SENTINEL™ Cerebral Protection System, Boston Scientific Co., Marlborough, MS, USA) was utilized in two patients. Intentional leaflet laceration was performed in one patient and BVF in two patients prior to THV deployment. Balloon pre- and postdilation were performed in one and two patients, respectively. Invasive measurements of mean pre- and post-implant pressure gradients revealed a decrease of peak gradient from 45.2 to 3.8 mmHg and decrease of mean gradient from 51.4 to 13.4 mmHg. Detailed periprocedural data are summarized in Table 2. For an illustration of ViV procedures using this SE intra-annular THV in surgical bovine, porcine valves, and THV, see Figures 1–3.
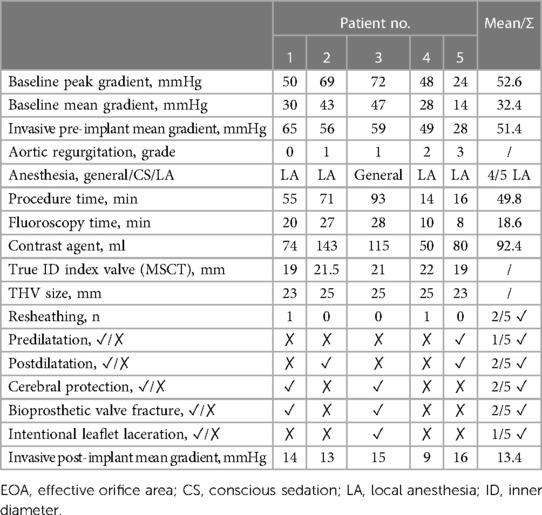
Table 2. Periprocedural data.
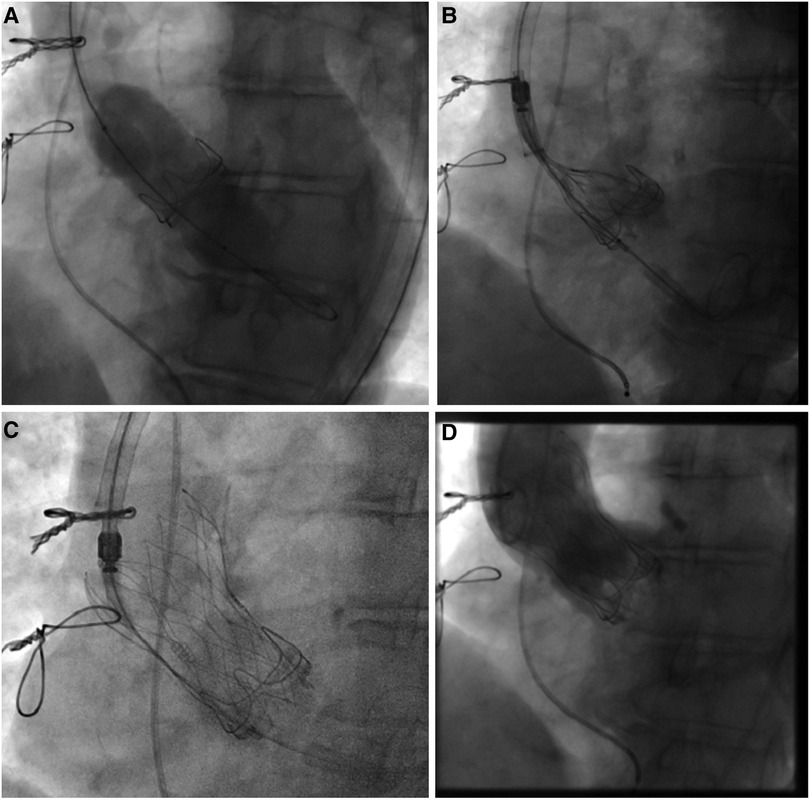
Figure 1. Valve-in-valve procedure using a self-expanding intra-annular transcatheter heart valve for treatment of a failing bovine surgical bioprosthesis. (A) Bioprosthetic valve fracture of a 21 mm (True ID: 19 mm) Perimount surgical bioprosthesis using a 22 mm True Dilatation Balloon. (B) Placement of a 23 mm self-expanding intra-annular transcatheter heart valve into the surgical bioprosthesis and alignment of both stent inflows. (C) Final position with (D) absence of any paravalvular leakage.
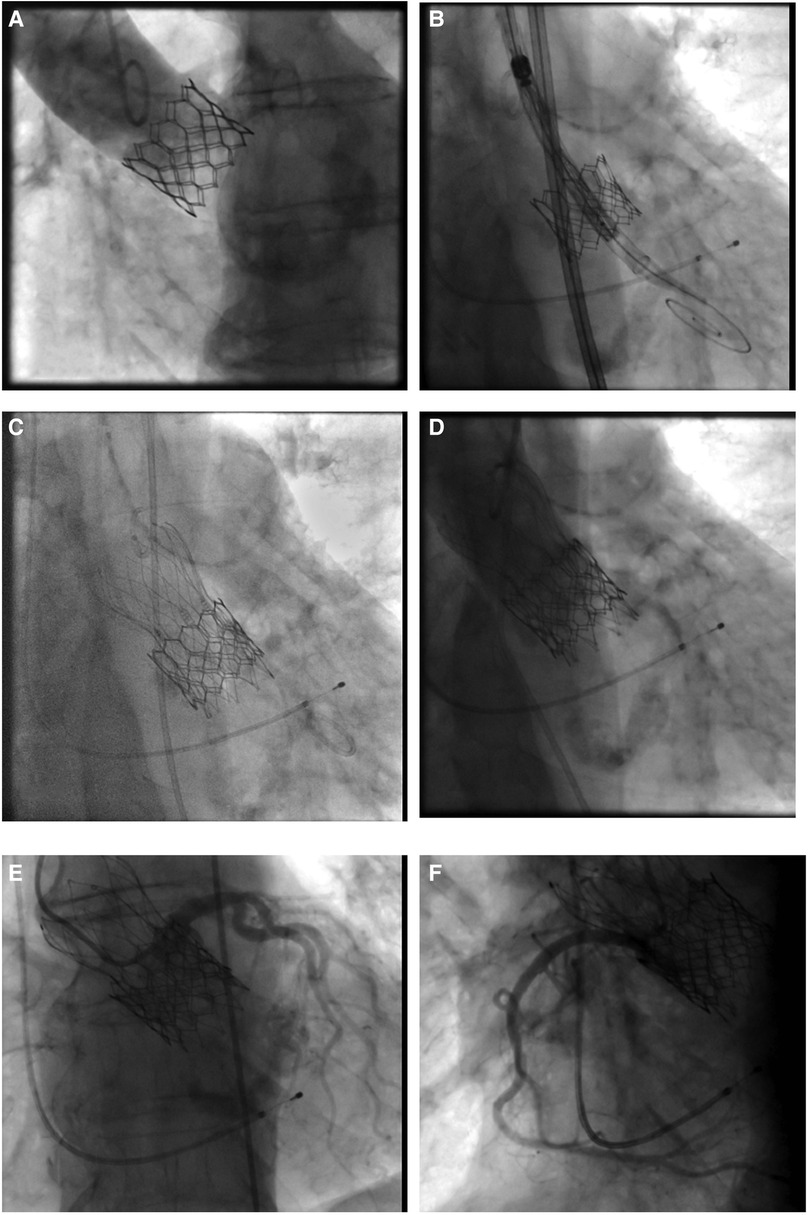
Figure 2. Valve-in-valve procedure using a self-expanding intra-annular transcatheter heart valve for treatment of a failing balloon-expandable transcatheter heart valve. (A) Failing balloon-expandable transcatheter heart valve in fluoroscopy with adequate distance of coronary arteries to the aortic annulus and marginal sinus width. (B) Placement of a 25 mm self-expanding intra-annular transcatheter heart valve into the Sapien 3, 26 mm (True ID: 21.5 mm) in deep position to protect against coronary occlusion. (C) Final position with (D) absence of paravalvular leakage. (E,F) Sufficient coronary perfusion in selective angiography of coronary arteries.
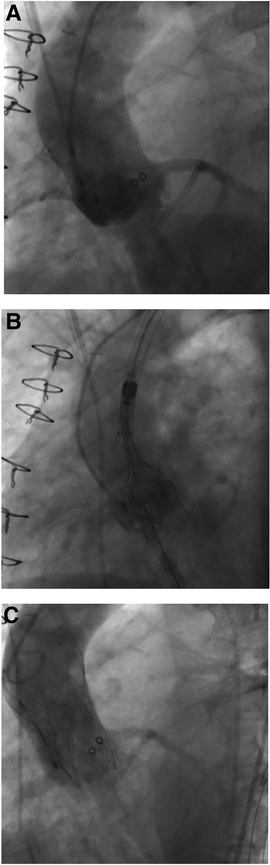
Figure 3. Valve-in-valve procedure using a self-expanding intra-annular transcatheter heart valve for treatment of a failing porcine surgical bioprosthesis. (A) Failing 23 mm (True ID: 19 mm) Mosaic surgical bioprosthesis with severe valvular regurgitation. (B) Placement of a 23 mm self-expanding intra-annular transcatheter heart valve into the surgical bioprosthesis and alignment of both lower stent parts. (C) Final position with absence of any paravalvular leakage.
Echocardiographic and clinical outcome data at 30 days
In the study group, peak and mean transvalvular gradients as determined by TTE decreased from 52.6 to 11.6 mmHg and from 32.4 to 6.0 mmHg, respectively. Complete absence of paravalvular leakage (PVL) was documented in all patients.
All-cause 30-day mortality was 0%. Device success, technical success, and early safety were reported to be 100%, respectively. No VARC-3 adjudicated clinical endpoints (disabling stroke, myocardial infarction, acute kidney injury, PPI, access site complication, bleeding) occurred. The range of holding area and hospital stay were 1 and 5–15 days, respectively.
Detailed echocardiographic and clinical outcome data are summarized in Table 3.
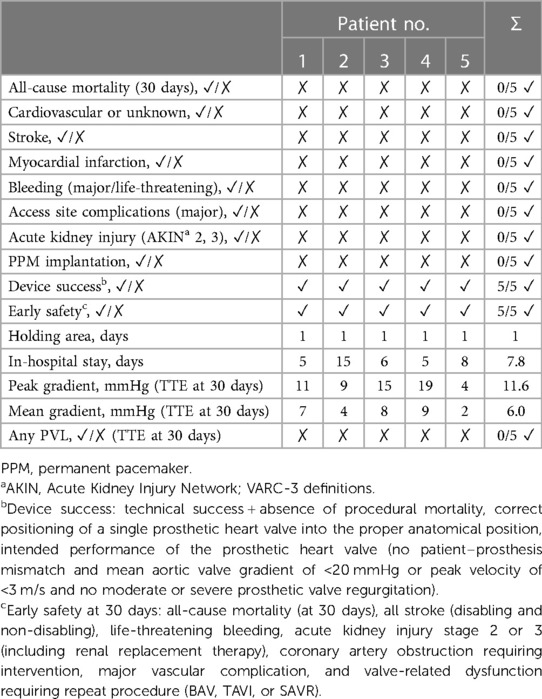
Table 3. Clinical and echocardiographic results at discharge.
Discussion
The main findings of the herein investigated patient series are as follows: (1) this SE intra-annular THV for ViV procedures resulted in excellent acute outcomes with the absence of mortality or VARC-3 adjudicated clinical endpoints; (2) despite the intra-annular design, hemodynamic results were excellent with no PVL and postinterventional single-digit mean transvalvular pressure gradients in all patients even in a bioprosthesis with a diameter of 21 mm; and (3) ease of use of this THV platform in aortic ViV procedures was reflected by only two cycles of resheathing in five ViV procedures with hemodynamic stability during all steps of valve deployment in the herein investigated patients.
Hemodynamic advantages of supra-annular THV for aortic ViV procedures, especially in small aortic bioprostheses with a diameter of ≤21 mm, are well documented by recent prospective randomized data (9). In the VIVID Registry investigating 1,006 patients, postprocedural peak/mean transvalvular pressure gradients of 27.1 ± 13.6/14.7 ± 8.2 mmHg for SE THV and 30.8 ± 15.8/17.7 ± 9.5 mmHg for BE THV (p < 0.001 for both values) were reported. Although this may not directly translate into increased mortality in the long term, higher incidences of patient–prosthesis mismatch with consecutive inadequate relief of valve stenosis and symptoms are likely with BE intra-annular THV. Furthermore, an increase of reintervention rates with intra-annular valves, especially in small aortic bioprostheses due to pin-wheeling effects caused by stent underexpansion, and possibility of early valve thrombosis were documented (1). The same is true for TAVI in TAVI procedures. A recent study demonstrated superior device success with SE THV in THV procedures compared with BE THV in THV procedures due to lower postprocedural mean transvalvular gradients with SE devices [SE THV: 10.3 mmHg (8.9–11.7 mmHg) vs. BE THV: 15.2 mmHg (13.2–17.1 mmHg); p < 0.001] (16). However, whether superiority of supra-annular SE THV in ViV procedures is an effect of the supra-annular valve design itself or is caused by different design properties of the respective THV still needs to be clarified. Although the herein investigated patient collective is small, postoperative hemodynamics are exceptionally favorable for ViV procedures using an intra-annular THV, even though it has to be emphasized that the herein documented hemodynamic results may be prone to bias since in two patients BVF was performed prior to THV implantation and hemodynamic performance of the utilized THV was determined after BVF. Furthermore, recent data suggest a beneficial impact of BVF after THV implantation with superior long-term effective orifice area (7), while still a patient-specific approach regarding utilization of BVF should be made for every patient to balance the anticipated hemodynamic result against the risk of coronary occlusion. However, these results suggest that not only valve position is crucial for postinterventional hemodynamics in ViV procedures but also the stent design itself. Here, the non-tapered stent and the low nitinol density and large stent cell design of the presented THV may contribute to single-digit mean gradients in all herein investigated cases. This assumption is further underlined by the good hemodynamic results of the predecessor THV platform in small native aortic annuli with severe aortic valve stenosis (17).
This finding may be of special importance for future concepts of lifetime management of aortic valve stenosis. Several concepts were introduced to provide patients with aortic valve stenosis a reasonable treatment strategy when multiple treatments of the aortic valve become necessary, consisting of SAVR-redo SAVR-TAVI or SAVR-TAVI-TAVI sequences (18). Especially in the latter concept, an initial ViV procedure using an intra-annular BE THV might be advantageous to facilitate a possible second ViV procedure using SE THV. In this scenario, a possibly unfavorable hemodynamic result with early THV failure after the first ViV treatment is accepted to enable a second ViV procedure. With the herein utilized intra-annular valve system, it seems possible to combine excellent acute hemodynamic results and anticipated extended valve durability of SE THV with preservation of valve reintervention, i.e., a second ViV procedure. Nevertheless, these preliminary results have to be confirmed in larger patient cohorts, and proof of concept of placing a supra-annular SE THV in an intra-annular SE THV is pending.
Limitations
Limitations are inherent in the retrospective, single-center study design with limited patient numbers: patients were not randomized to a specific treatment or valve; therefore, patient preselection with hidden confounders may apply.
Conclusion
The investigated SE intra-annular THV resulted in reasonable 30-day outcomes in aortic ViV procedures for failing surgical bioprostheses or THV in this small series. Despite the intra-annular design, hemodynamic results were good in the herein investigated failing bioprostheses. Ease of use of this valve platform is reflected by only two cycles of resheathing in five ViV procedures with hemodynamic stability during all steps of valve deployment. A further advantage of using this particular THV in aortic ViV procedures may be the possibility for a second ViV procedure using a supra-annular THV, which is a concept that has to be validated in the future.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
AS and LC substantially contributed to the conception and design of the work and the acquisition, analysis, and interpretation of data for the work; drafted the work; and provided approval for the publication of the content. TD, OB, DG, LV, LW, JS, SP, YS, NSc, NSö, SB, HR, and MS critically revised the manuscript for important intellectual content and provided approval for the publication of the content. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors contributed to the article and approved the submitted version.
Conflict of interest
AS received speaker honoraria from Abbott. LC is an advisory board member for Abbott, Medtronic, JenaValve, and MicroPort and has received honoraria from Edwards Lifesciences, Boston Scientific, Neovasc, Highlife, PiCardia, and MicroInterventions. MS received speaker honoraria from Abbott Vascular, Abiomed, Amgen, AstraZeneca, Boston Scientific, BMS/Pfizer, Daiichi Sankyo, Edwards Lifesciences, Inari, Medtronic, Philips, Shockwave Medical, and Siemens.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
BE, balloon-expandable; BVF, bioprosthetic valve fracture; PPI, permanent pacemaker implantation; SAVR, surgical aortic valve replacement; SE, self-expanding; TAVI, transcatheter aortic valve implantation; TEE, transesophageal echocardiography; TF, transfemoral; THV, transcatheter heart valve; TTE, transthoracic echocardiography; VARC, Valve Academic Research Consortium; ViV, valve-in-valve.
References
1. Bleiziffer S, Simonato M, Webb JG, Rodés-Cabau J, Pibarot P, Kornowski R, et al. Long-term outcomes after transcatheter aortic valve implantation in failed bioprosthetic valves. Eur Heart J. (2020) 41(29):2731–42. doi: 10.1093/eurheartj/ehaa544
2. Schaefer A, Treede H, Seiffert M, Deuschl F, Schofer N, Schneeberger Y, et al. Repeat transcatheter aortic valve implantation using a latest generation balloon-expandable device for treatment of failing transcatheter heart valves. J Cardiothorac Surg. (2016) 11:2. doi: 10.1186/s13019-016-0398-y
3. Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease. EuroIntervention. (2022) 17(14):e1126–96. doi: 10.4244/EIJ-E-21-00009
4. Writing Committee Members, Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP 3rd, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. J Thorac Cardiovasc Surg. (2021) 162(2):e183–353. doi: 10.1016/j.jtcvs.2021.04.002
5. Pingpoh C, Schroefel H, Franz T, Czerny M, Kreibich M, Moser M, et al. Transcatheter valve-in-valve implantation in degenerated aortic bioprostheses: are patients with small surgical bioprostheses at higher risk for unfavourable mid-term outcomes? Ann Cardiothorac Surg. (2020) 9(6):478–86. doi: 10.21037/acs-2020-av-fs-0124
6. Gao Z, Wang Y, Qian D, Jin J. Incidence, risk factors, and outcomes of coronary obstruction following valve-in-valve transcatheter aortic valve replacement. Int Heart J. (2021) 62(1):104–11. doi: 10.1536/ihj.20-401
7. Meier D, Payne GW, Mostaço-Guidolin LB, Bouchareb R, Rich C, Lai A, et al. Timing of bioprosthetic valve fracture in transcatheter valve-in-valve intervention: impact on valve durability and leaflet integrity. EuroIntervention. (2023) 18(14):1165–77. doi: 10.4244/EIJ-D-22-00644
8. Kitamura M, Wilde J, Dumpies O, Richter I, Obradovic D, Krieghoff C, et al. Risk assessment of coronary obstruction during transcatheter aortic valve replacement: insights from Post-BASILICA computed tomography. JACC Cardiovasc Interv. (2022) 15(5):496–507. doi: 10.1016/j.jcin.2022.01.003
9. Rodés-Cabau J, Abbas AE, Serra V, Vilalta V, Nombela-Franco L, Regueiro A, et al. Balloon- vs self-expanding valve systems for failed small surgical aortic valve bioprostheses. J Am Coll Cardiol. (2022) 80(7):681–93. doi: 10.1016/j.jacc.2022.05.005
10. Ochiai T, Yoon SH, Sharma R, Miyasaka M, Nomura T, Rami T, et al. Outcomes of self-expanding vs. balloon-expandable transcatheter heart valves for the treatment of degenerated aortic surgical bioprostheses—a propensity score-matched comparison. Circ J. (2018) 82(10):2655–62. doi: 10.1253/circj.CJ-18-0157
11. Wong I, Bieliauskas G, De Backer O, Søndergaard L. Cusp overlap technique during valve-in-valve TAVI using the novel Navitor transcatheter heart valve. EuroIntervention. (2022) 17(16):1298–9. doi: 10.4244/EIJ-D-21-00592
12. VARC-3 Writing Committee, Généreux P, Piazza N, Alu MC, Nazif T, Hahn RT, et al. Valve academic research consortium 3: updated endpoint definitions for aortic valve clinical research. Eur Heart J. (2021) 42(19):1825–57. doi: 10.1093/eurheartj/ehaa799
13. Schaefer A, Linder M, Treede H, Deuschl F, Schofer N, Seiffert M, et al. Applicability of next generation balloon-expandable transcatheter heart valves in aortic annuli exceeding formally approved dimensions. Clin Res Cardiol. (2016) 105(7):585–91. doi: 10.1007/s00392-015-0954-9
14. Conradi L, Silaschi M, Seiffert M, Lubos E, Blankenberg S, Reichenspurner H, et al. Transcatheter valve-in-valve therapy using 6 different devices in 4 anatomic positions: clinical outcomes and technical considerations. J Thorac Cardiovasc Surg. (2015) 150(6):1557–65. 1567.e1–3; discussion 1565–7. doi: 10.1016/j.jtcvs.2015.08.065
15. Westermann D, Ludwig S, Kalbacher D, Spink C, Linder M, Bhadra OD, et al. Prevention of coronary obstruction in patients at risk undergoing transcatheter aortic valve implantation: the Hamburg BASILICA experience. Clin Res Cardiol. (2021) 110(12):1900–11. doi: 10.1007/s00392-021-01881-4
16. Landes U, Richter I, Danenberg H, Kornowski R, Sathananthan J, De Backer O, et al. Outcomes of redo transcatheter aortic valve replacement according to the initial and subsequent valve type. JACC Cardiovasc Interv. (2022) 15(15):1543–54. doi: 10.1016/j.jcin.2022.05.016
17. Voigtländer L, Kim WK, Mauri V, Goßling A, Renker M, Sugiura A, et al. Transcatheter aortic valve implantation in patients with a small aortic annulus: performance of supra-, intra- and infra-annular transcatheter heart valves. Clin Res Cardiol. (2021) 110(12):1957–66. doi: 10.1007/s00392-021-01918-8
Keywords: transcatheter aortic valve implantation, bioprostheses, aortic valve, valve-in-valve, self-expandable aortic valve
Citation: Schaefer A, Demal TJ, Bhadra OD, Grundmann D, Voigtländer L, Waldschmidt L, Schirmer J, Pecha S, Schneeberger Y, Schofer N, Sörensen N, Blankenberg S, Reichenspurner H, Seiffert M and Conradi L (2023) Valve-in-valve procedures for degenerated surgical and transcatheter aortic valve bioprostheses using a latest-generation self-expanding intra-annular transcatheter heart valve. Front. Cardiovasc. Med. 10:1209184. doi: 10.3389/fcvm.2023.1209184
Received: 20 April 2023; Accepted: 7 August 2023;
Published: 1 September 2023.
Edited by:
Fabien Praz, University Hospital of Bern, SwitzerlandReviewed by:
Alberto Guido Pozzoli, Ospedale Regionale di Lugano, SwitzerlandAugusto D’Onofrio, University of Padua, Italy
© 2023 Schaefer, Demal, Bhadra, Grundmann, Voigtläender, Waldschmidt, Schirmer, Pecha, Schneeberger, Schofer, Sörensen, Blankenberg, Reichenspurner, Seiffert and Conradi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andreas Schaefer YW5kLnNjaGFlZmVyQHVrZS5kZQ==